lvot obstruction: patients at risk - casecag …casecag.com/education/lecture pdfs/lvot...
TRANSCRIPT

LVOT Obstruction: Patients at Risk
Edwin G. Avery, M.D.
Chief, Case Cardiac Anesthesia Group
Fall 2011 Cardiac Anesthesia TEE Conference

Disclosures
Covidien: funded research, consultant
Alere: funded research
The Medicines Company: funded research, speaker’s
bureau


Overview
Discuss the most common perioperative clinical
presentations of LVOT obstruction associated with
Hypertrophic Cardiomyopathy (HCM) and the
interventional options available to treat this
pathology
Present a clinical case of HCM with LVOT
obstruction as assessed with intraoperative TEE

HCM and LVOT Obstruction
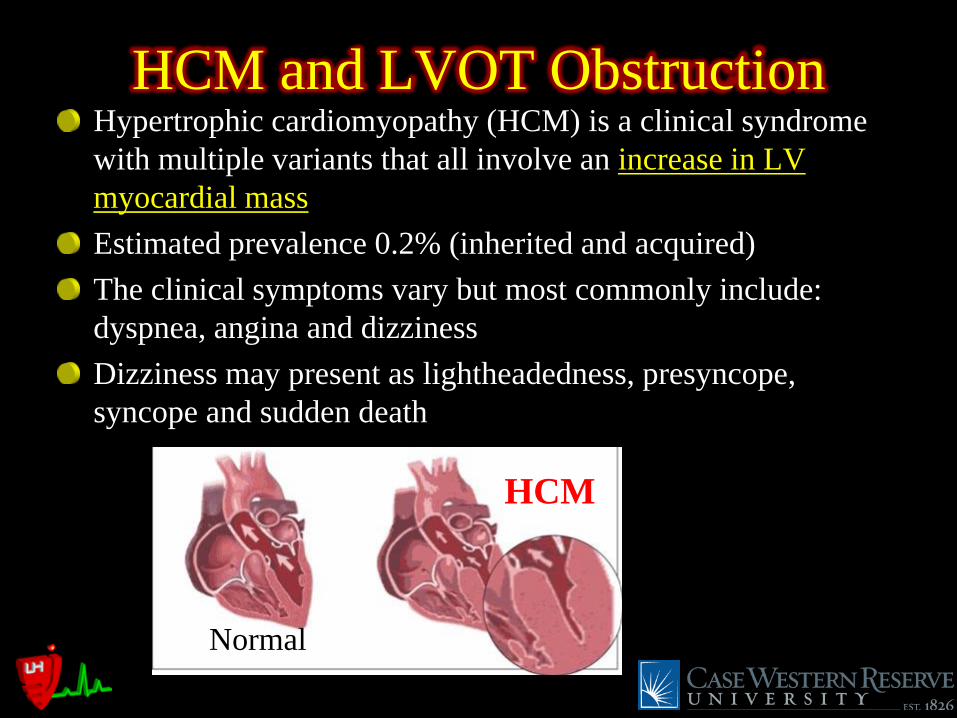
HCM and LVOT Obstruction Hypertrophic cardiomyopathy (HCM) is a clinical syndrome
with multiple variants that all involve an increase in LV
myocardial mass
Estimated prevalence 0.2% (inherited and acquired)
The clinical symptoms vary but most commonly include:
dyspnea, angina and dizziness
Dizziness may present as lightheadedness, presyncope,
syncope and sudden death
HCM
Normal

HCM and LVOT Obstruction
HCM variants include:
Concentric LVH (RV may also be involved)
Asymmetric upper septal hypertrophy (ASH)
ASH with or without systolic anterior motion of the
anterior mitral leaflet (SAM)
SAM with or without mitral regurgitation (commonly a
posteriorly directed jet of variable severity)
Malposition of the anterior papillary muscle
Mid-cavitary hypertrophy (with or without a gradient)
Apical hypertrophy
LV free wall hypertrophy

HCM and LVOT Obstruction TEE presentation of HCM concentric LVH (PWT or SWT ≥ 11 mm)

HCM and LVOT Obstruction TEE presentation of HCM concentric LVH ± RVH

HCM and LVOT Obstruction TEE presentation of HCM concentric LVH (PWT or SWT ≥ 11 mm)
PWT = 21 mm
End diastole

HCM and LVOT Obstruction TEE presentation of ASH SWT:PWT ≥ 1.3

HCM and LVOT Obstruction TEE presentation of ASH SWT:PWT ≥ 1.3
SWT = 34 mm
SWT:PWT = 34 / 21 = 1.62
End Diastole
LV long axis
(SWT measured perpendicular
to LV long axis)
Distance to maximal septal
thickness from aortic annulus

HCM and LVOT Obstruction TEE presentation of HCM ASH with or without SAM

HCM and LVOT Obstruction TEE presentation of HCM ASH with or without SAM†
†Mild posteriorly directed MR

HCM and LVOT Obstruction TEE presentation of HCM HOCM: LVOT gradient (latent or provocative)†
†Latent ≥30 mmHg, Provocative ≥50 mmHg

HCM and LVOT Obstruction TEE presentation of HCM HOCM: LVOT gradient (latent or provocative)†
†Latent ≥30 mmHg, Provocative ≥50 mmHg
Peak 92 mmHg
Mean 53 mmHg Note sharper peak associated
with dynamic obstruction

HCM and LVOT Obstruction HOCM: LVOT gradient (dynamic obstruction)
Characteristic
“Spike and
Dome” A-line
tracing in
dynamic
obstruction

HCM-LVOT Obstruction:Treatment Medical therapy: β-blockers, verapmil, disopyramide
Permanent pacemaker (DDD) or ICD implantation
Ethanol injection for septal ablation (1st septal perforator
coronary artery)
Mitral valve replacement with low profile mechanical
prosthesis (e.g., St. Jude bileaflet tilting disc)
Surgical myectomy

HCM-LVOT Obstruction:Treatment TEE exam of patients undergoing septal myectomy should include
a complete multiplanar assessment of the aortic valve for evidence
of AI as the surgical approach to the septum may result in damage
to the valve

HCM-LVOT Obstruction:Treatment
Pre-Myectomy Post-Myectomy
Minor AV Injury

HCM-LVOT Obstruction Summary
In some cases, even aggressive septal myectomy may
not relieve the resting or provocative gradient (even
when combined with medical therapy).
In such cases the implantation of a low profile mitral
mechanical prosthesis can be helpful in relieving the
gradient.
There is no evidence that ANY therapy alters the
progressive course of this disease.

Edwin G. Avery, M.D.
Chief, Case Cardiac Anesthesia Group
University Hospitals Case Medical Center
You’re the Intraoperative Echocardiography Consultant


Preinduction Hemodynamics

Induction
Systemic BP: 75/37
Pulmonary BP: 82/44
Fentanyl + Versed + Cisatracurium
Diagnosis? Treatment?

Phenylephrine + Volume + Ventilation
Stable hemodynamics and ready for TEE

ME 4C View

ME 4C Color MV

ME Long Axis View

ME 4C View w/Color

TG Short Axis Mid-pap View
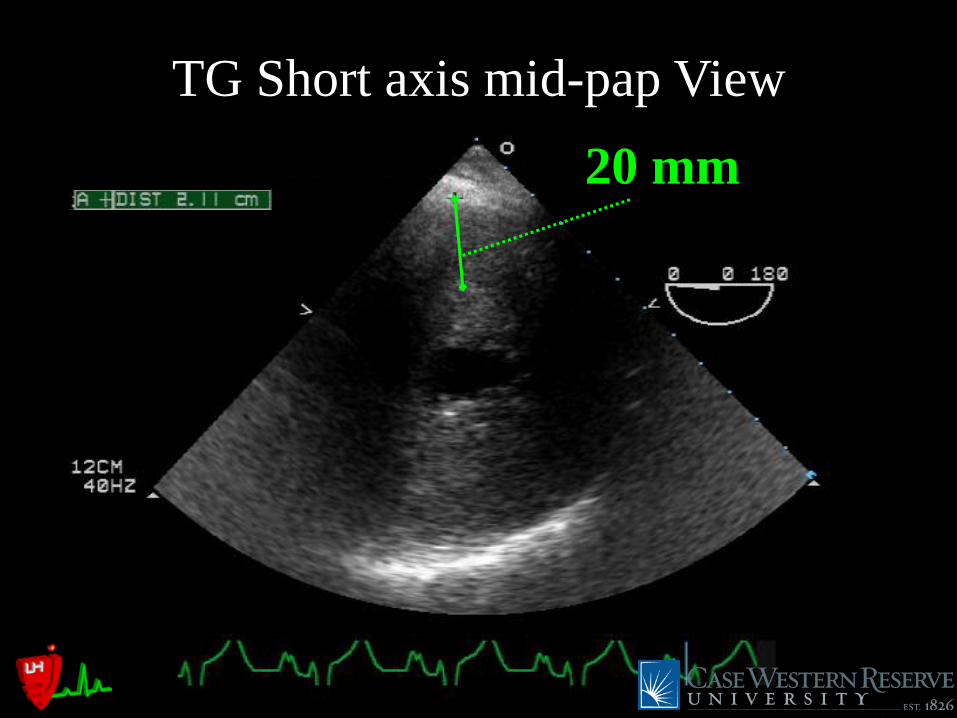
20 mm
TG Short axis mid-pap View
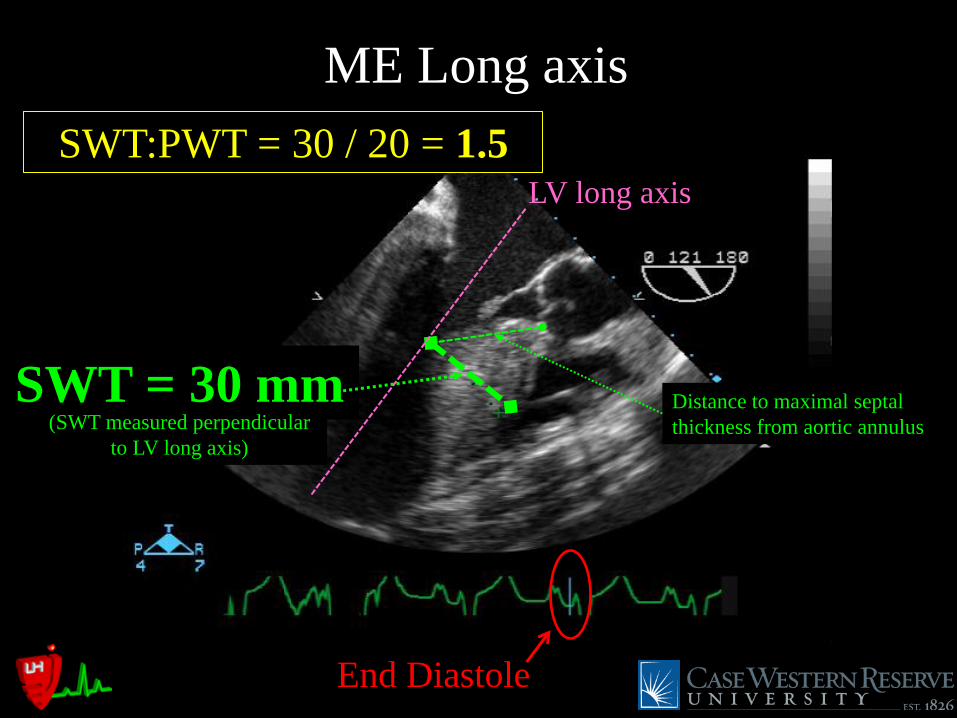
ME Long axis
SWT = 30 mm
End Diastole
LV long axis
(SWT measured perpendicular
to LV long axis)
Distance to maximal septal
thickness from aortic annulus
SWT:PWT = 30 / 20 = 1.5

TG LV Long axis

TG Modified LA View

TG Modified Long axis w/color

LVOT pre-CPB Gradient
Peak 92 mmHg
Mean 63 mmHg C.O. = 1.7 L/min
HCM patients may have low C.O. secondary to low stroke volumes as a result of
decreased LV chamber size and noncompliance/diastolic dysfunction
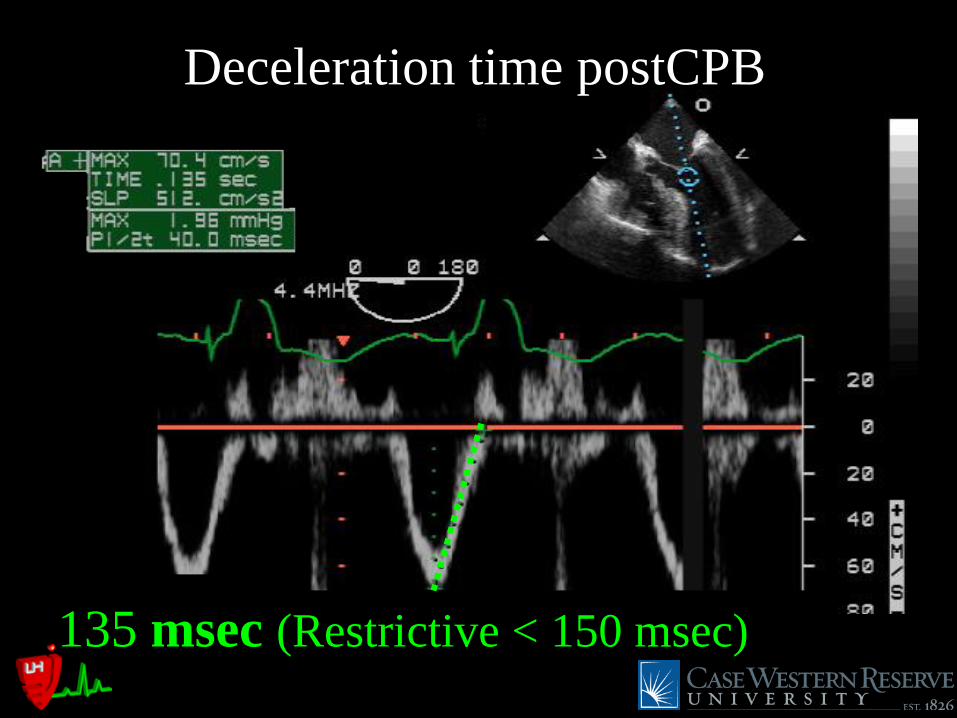
Deceleration time postCPB
135 msec (Restrictive < 150 msec)

8.6 cm/sec
TDI Lateral MV annulus

Vp post-CPB
Vp 39 cm/sec (Restrictive < 45 cm/sec)

IVRT 200 msec
(Restrictive < 60 msec; Delayed Relaxation > 100)
IVRT Post-CPB

TG SA RV

Membranous septum pre-CPB
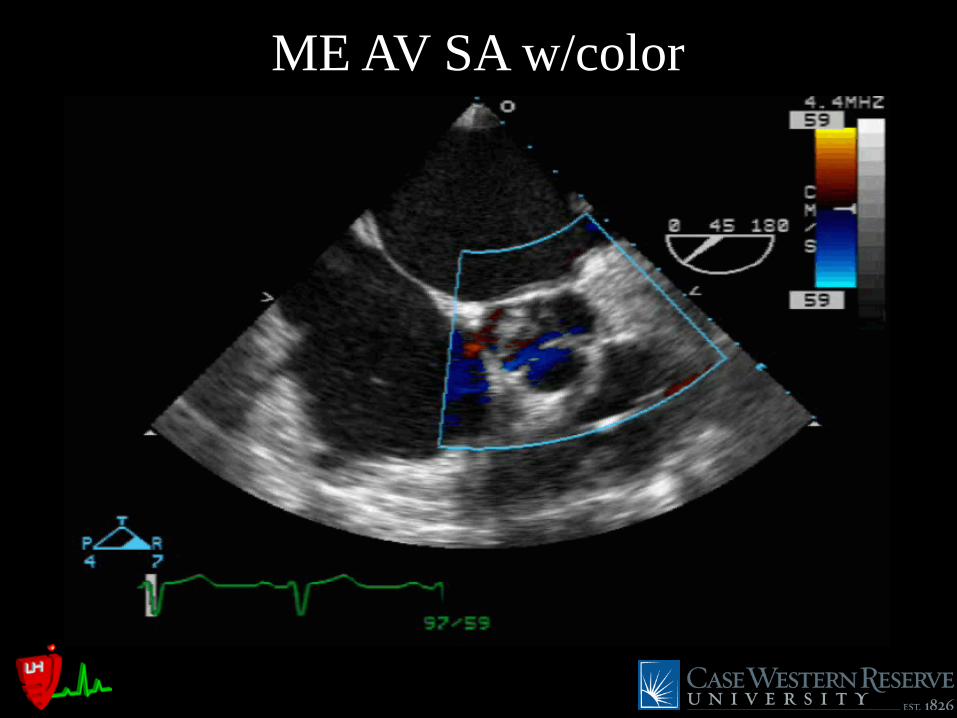
ME AV SA w/color

On CPB – Septal Myectomy

ME 4C View post-CPB

ME 4 C view w/color

TG Modified Long axis post-CPB

TG Modified long axis w/color post-CPB

Peak 5 mmHg
Mean 2 mmHg
Post-CPB LVOT gradient
C.O. = 2.0 L/min

Improved a-line tracing
Pre-CPB Post-CPB

TG SA RV post-CPB
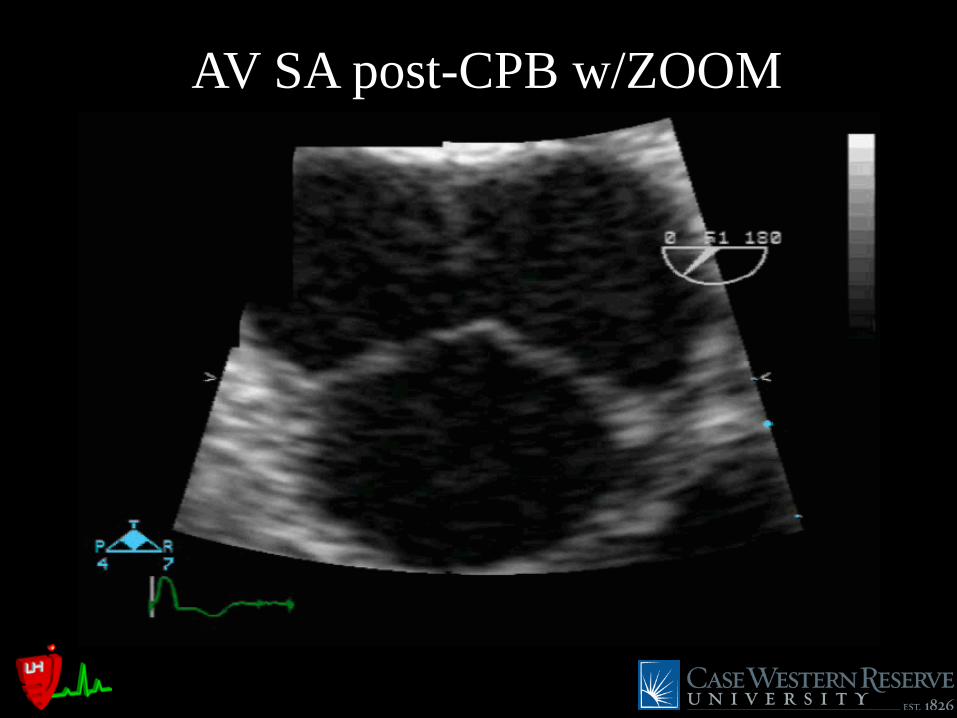
AV SA post-CPB w/ZOOM

AV LA Zoom post-CPB


The End – Thank You Please visit www.casecag.com for a copy of this presentation and
to view it in video format
Click
Here