lymph node staging - duke university · pdf filelung cancer 1 lymph node staging ebus, eus,...
TRANSCRIPT
Lung Cancer 1
Lymph Node Staging EBUS, EUS, Navigational Bronchoscopy
Daniel L Miller MD
Kamal A. Mansour Professor of Surgery
Emory University School of Medicine
Chief, General Thoracic Surgery
Emory University Healthcare
Atlanta, Georgia
Lung Cancer 2
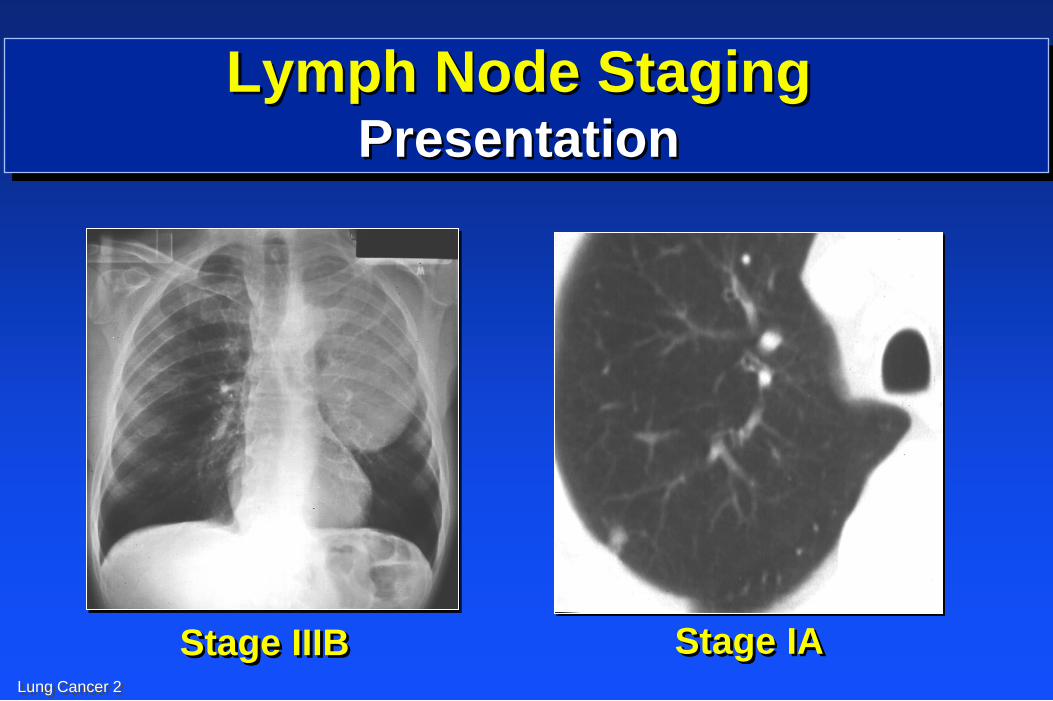
Lymph Node Staging Presentation
Stage IIIB Stage IA
Lung Cancer 3
0
200
400
600
800
1000
1200
1400
1600
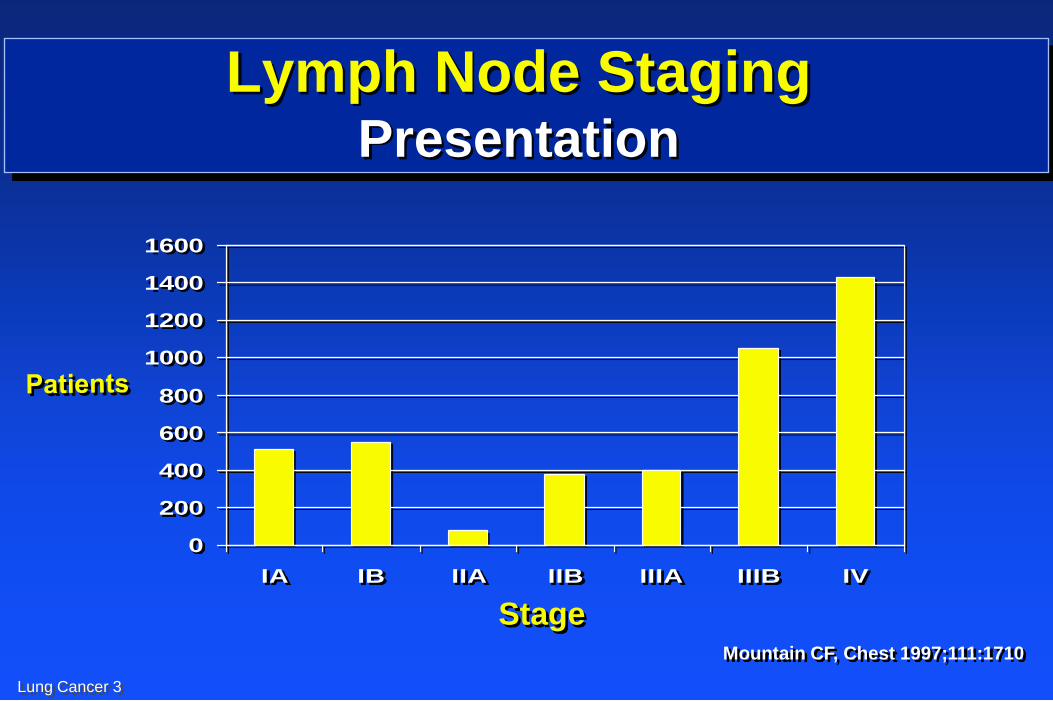
IA IB IIA IIB IIIA IIIB IV
Stage Mountain CF, Chest 1997;111:1710
Lymph Node Staging Presentation
Lung Cancer 4
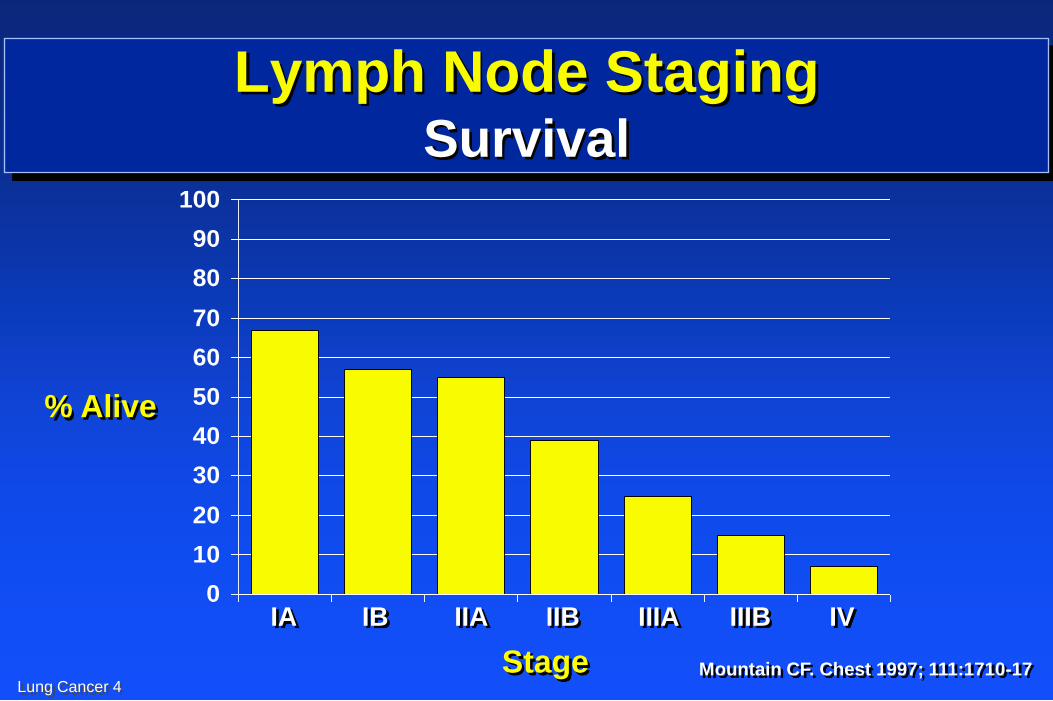
Lymph Node Staging Survival
0
10
20
30
40
50
60
70
80
90
100
% Alive
IA IB IIA IIB IIIA IIIB IV
Stage Mountain CF. Chest 1997; 111:1710-17

Lung Cancer 5
Lung Cancer
Lymph Node Evaluation
Lung Cancer 6
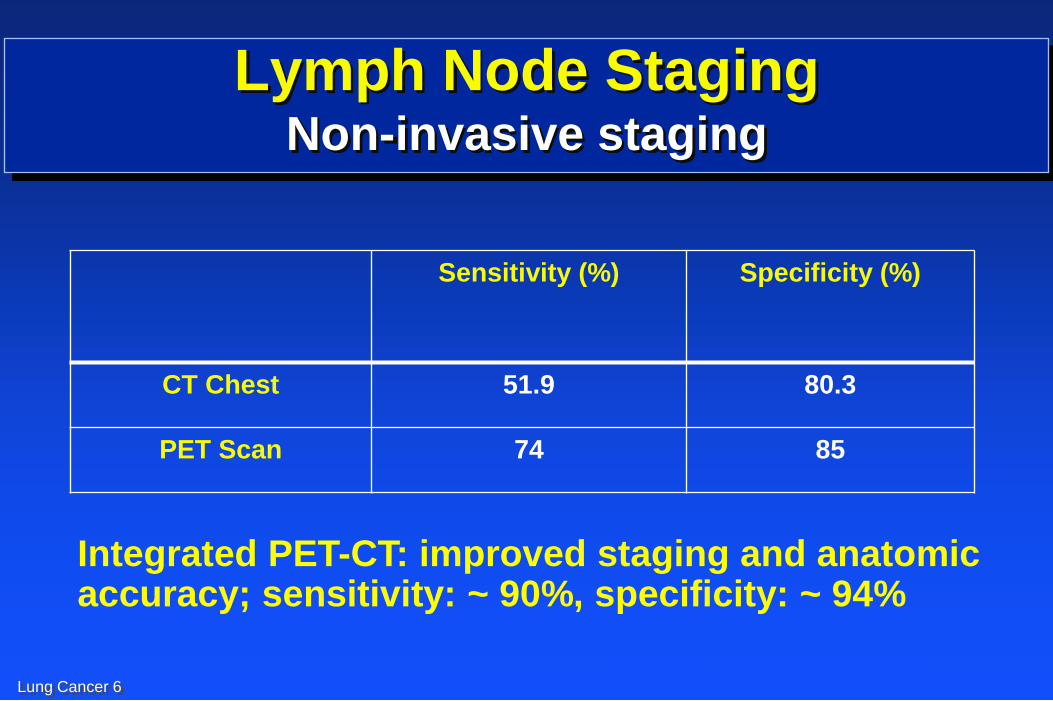
Lymph Node Staging Non-invasive staging
Sensitivity (%) Specificity (%)
CT Chest 51.9 80.3
PET Scan 74 85
Silvestri et al. Chest 2007;132:178S-201S
Integrated PET-CT: improved staging and anatomic accuracy; sensitivity: ~ 90%, specificity: ~ 94%
Lung Cancer 7
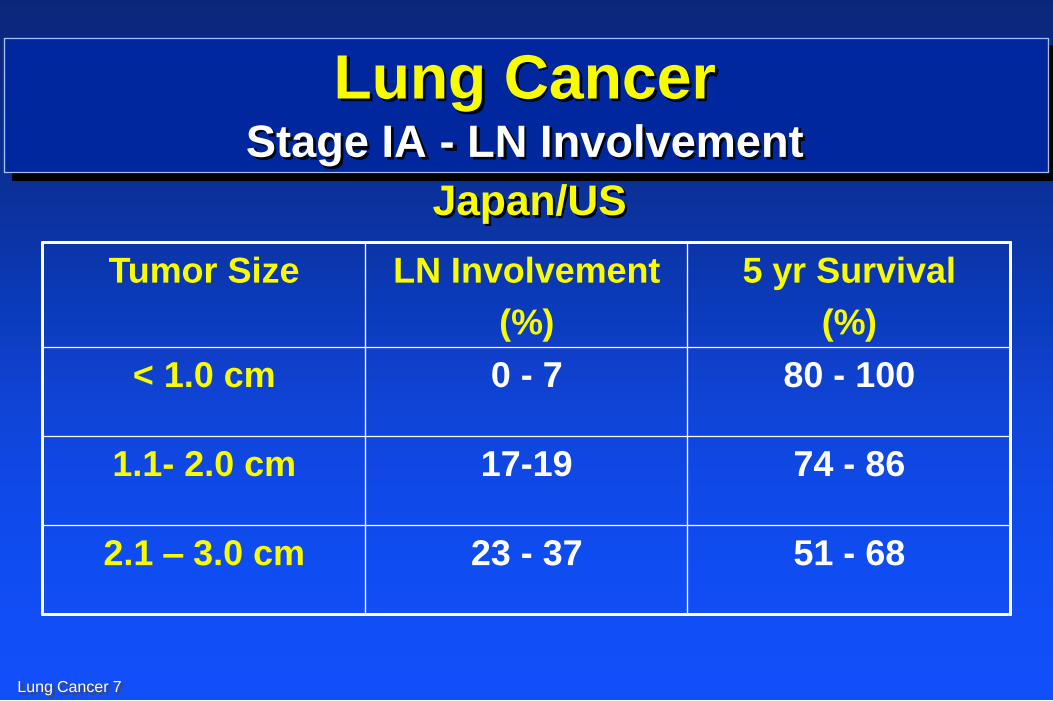
Lung Cancer Stage IA - LN Involvement
Tumor Size LN Involvement
(%)
5 yr Survival
(%)
< 1.0 cm 0 - 7 80 - 100
1.1- 2.0 cm 17-19 74 - 86
2.1 – 3.0 cm 23 - 37 51 - 68
Japan/US
Lung Cancer 8
Lymph Node Staging Invasive Staging
Mediastinoscopy
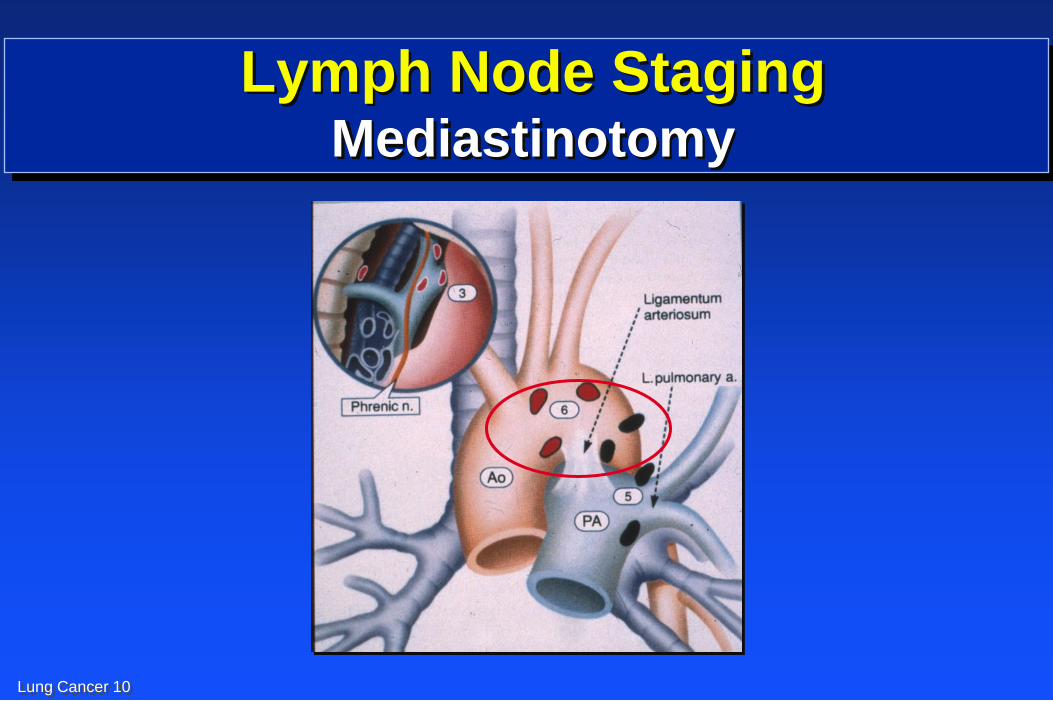
Mediastinotomy (Chamberlain procedure)
Video-assisted Thoracic Surgery (VATS)
Thoracotomy
Transthoracic needle aspiration (CT)
Endobronchial Ultrasound (EBUS)
Endoscopy Ultrasound (EUS)
Navigational Bronchoscopy (SD)
Lung Cancer 9
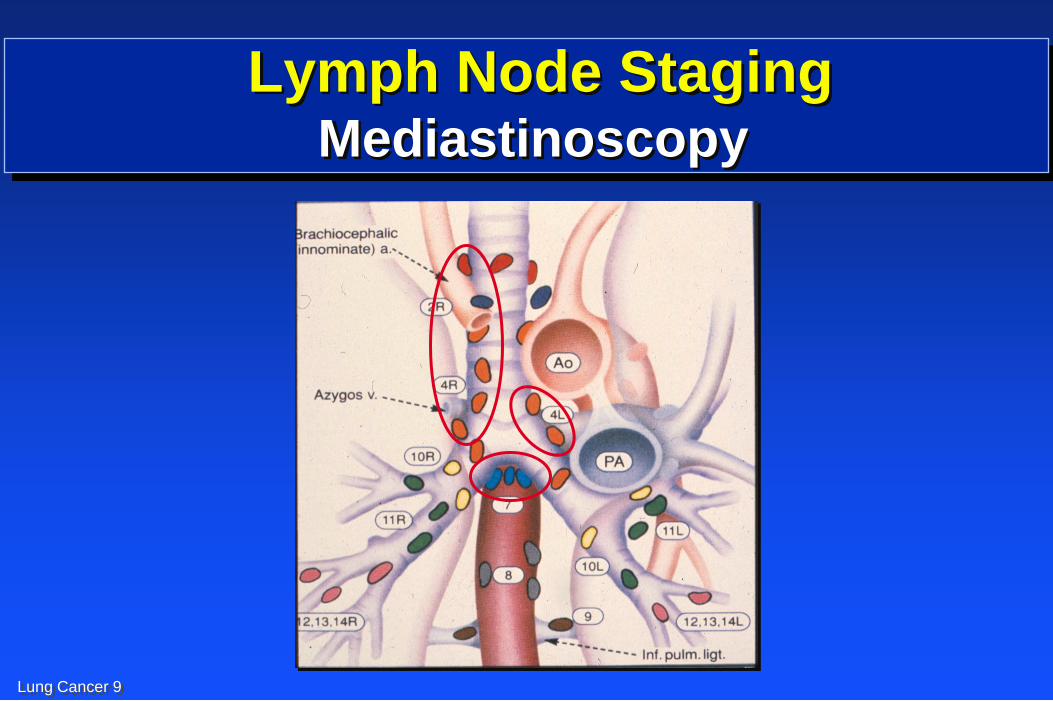
Lymph Node Staging Mediastinoscopy
Lung Cancer 10
Lymph Node Staging Mediastinotomy
Lung Cancer 11
Lung Cancer
American College of Surgeons Survey
In 2001, patient care survey of 729 hospitals
40,090 NSCLC pts; 11,668 pts (29%) had surgery
Surgery only – 74%; Stage I – 60%; Lobe - 75%
Mediastinoscopy (27%); LN biopsied 47%
N2 LN removed (58%); N1 with specimen (42%)
Positive surgical margin 8%; Frozen section 65%
Mortality – wedge (5%), Lobe (5%), Pneumo (9%)
Current surgical treatment of lung cancer is poor
There is no standard of care
Lung Cancer 12
Lung Cancer
Society Thoracic Surgeons Database
In 2008, GTS database (1999 – 2006)
49,029 operations; 9033 pulmonary resections
Resection: Wedge – 18%, Segment – 4%,
Lobe – 67%, Bilobe – 4%, and Pneumo – 7%
Mediastinal LN evaluate 65%; Mediastinoscopy – 21%
LN Dissection - 41%, Sampling – 21%, Biopsy – 8%
Operative mortality 2.5%
Postoperative complications 32%
Lung Cancer 13
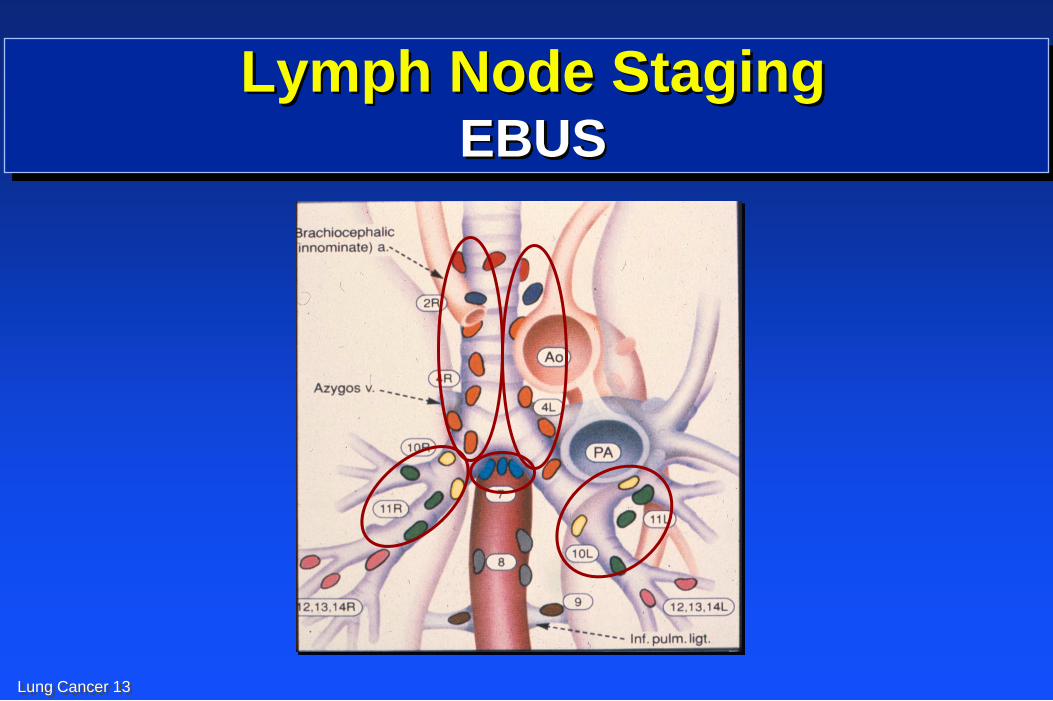
Lymph Node Staging EBUS
Lung Cancer 14
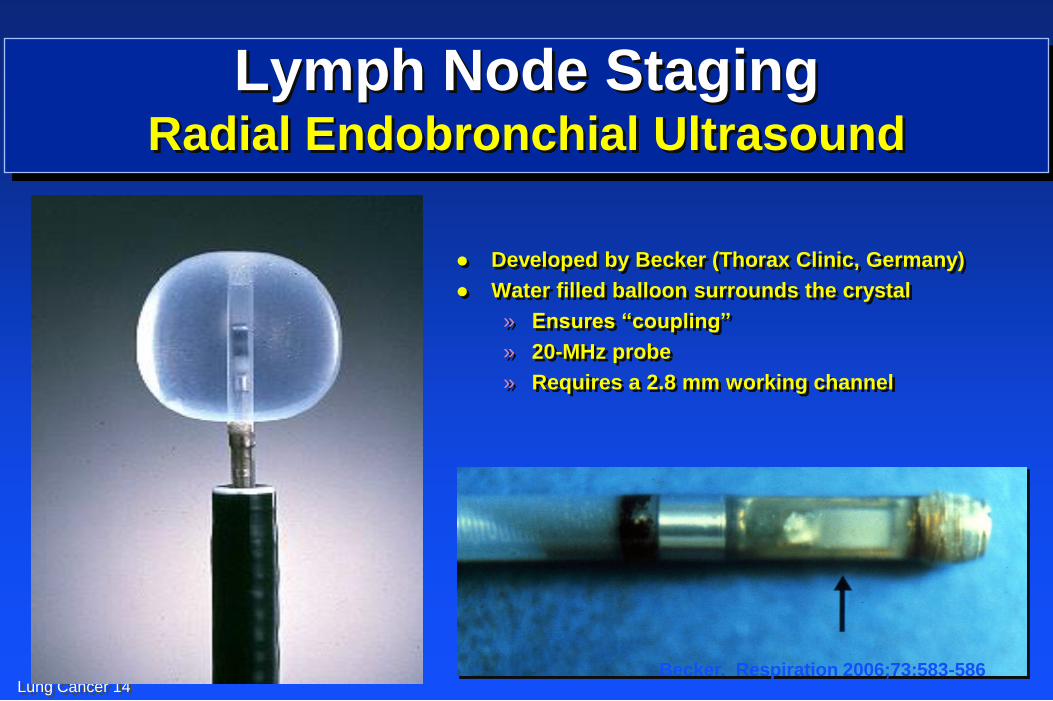
Developed by Becker (Thorax Clinic, Germany)
Water filled balloon surrounds the crystal
» Ensures “coupling”
» 20-MHz probe
» Requires a 2.8 mm working channel
Lymph Node Staging Radial Endobronchial Ultrasound
Becker. Respiration 2006;73:583-586
Lung Cancer 15
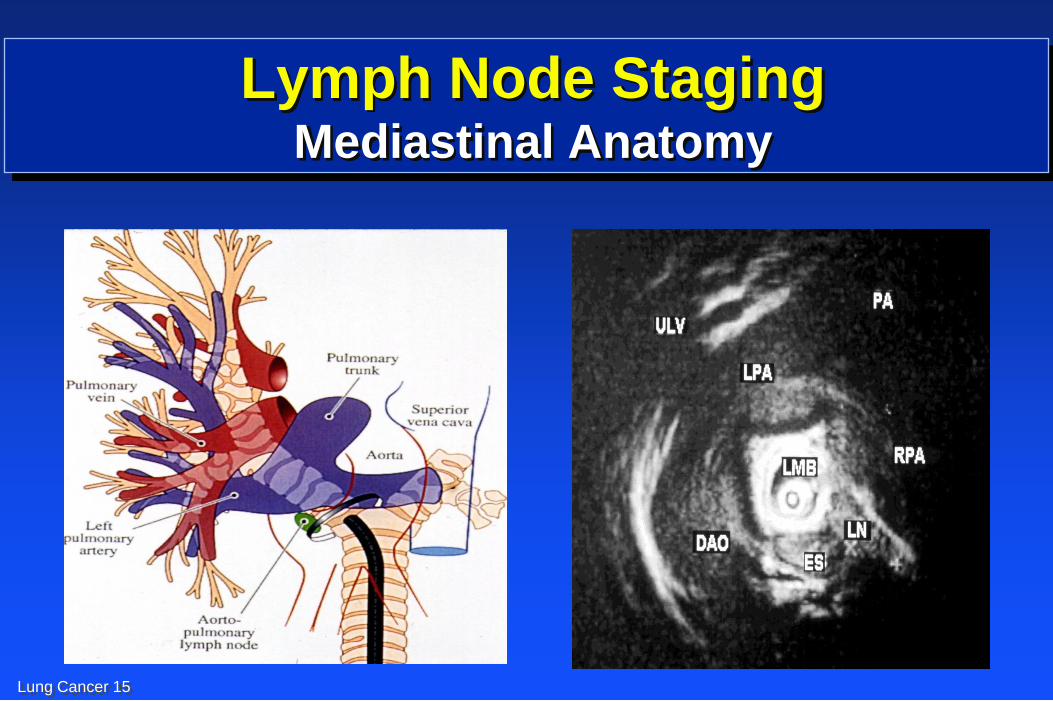
Lymph Node Staging Mediastinal Anatomy
Lung Cancer 16
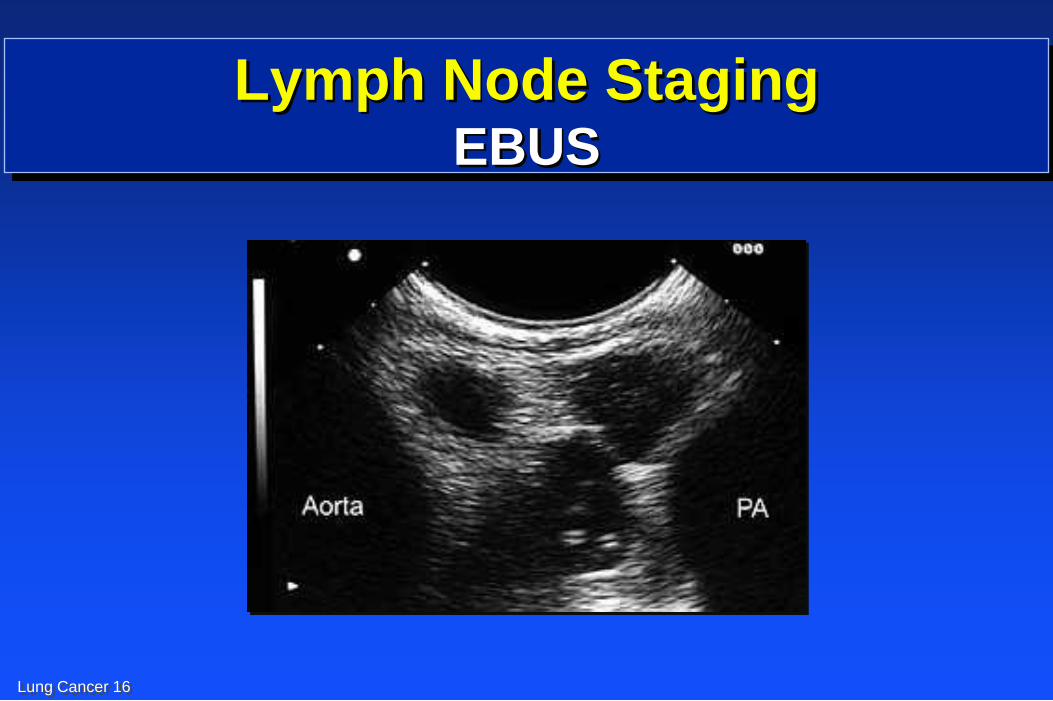
Lymph Node Staging EBUS
Lung Cancer 17
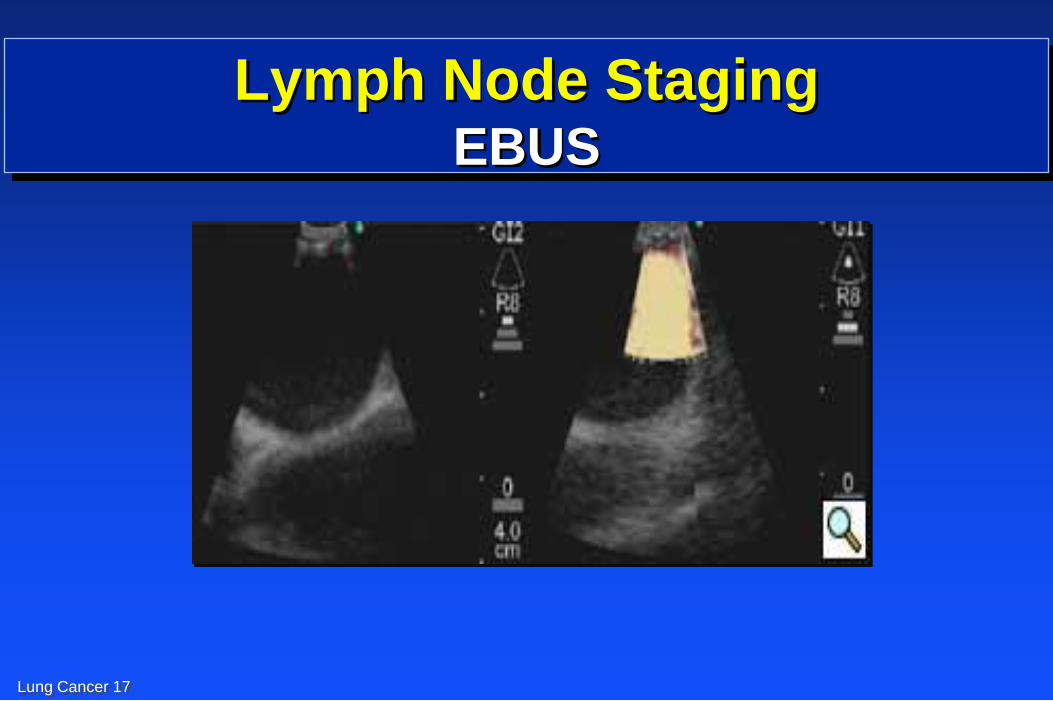
Lymph Node Staging EBUS
Lung Cancer 18
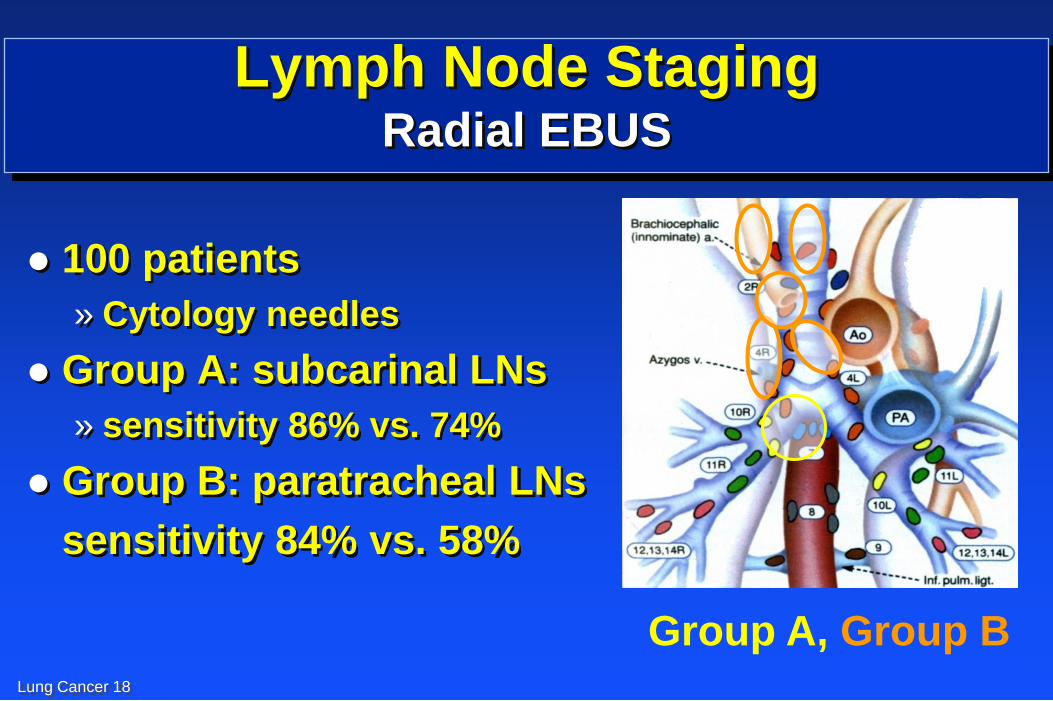
Lymph Node Staging Radial EBUS
100 patients
» Cytology needles
Group A: subcarinal LNs
» sensitivity 86% vs. 74%
Group B: paratracheal LNs
sensitivity 84% vs. 58%
Group A, Group B Chest 2004; 125: 322
Lung Cancer 19
Lymph Node Staging Clinical staging differ from pathologic staging
24% clinically over staged
20% clinically under staged
ATS/ERS: Obtain pathologic evaluation in all
patients thought to be surgical candidates
prior to VATS or thoracotomy
Lung Cancer 20
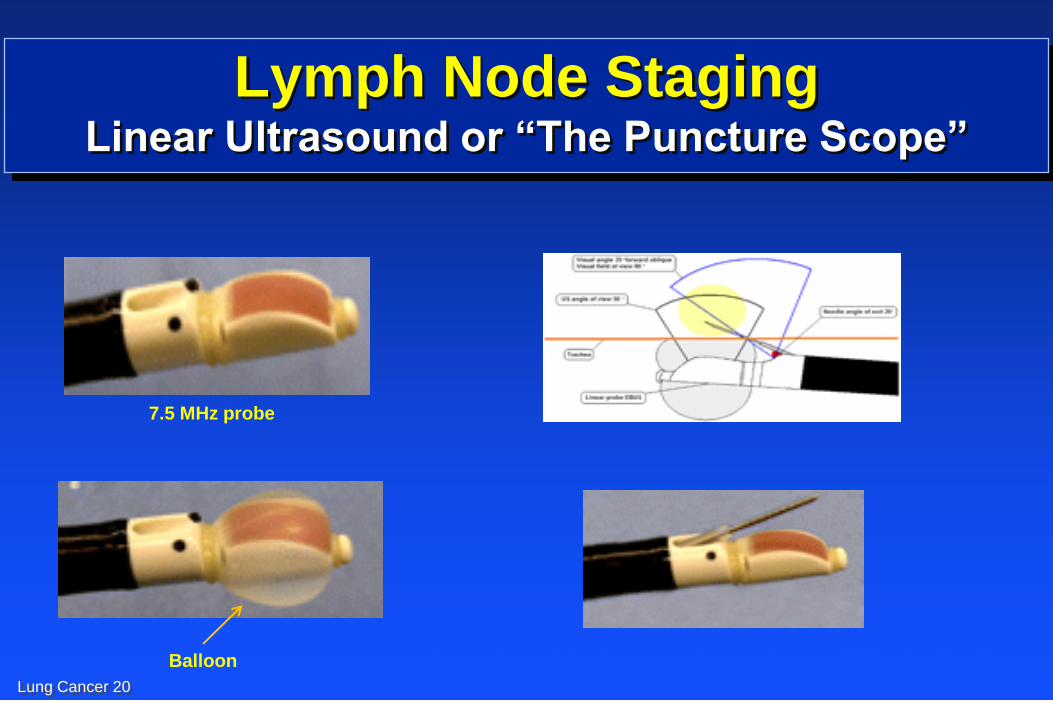
Lymph Node Staging Linear Ultrasound or “The Puncture Scope”
7.5 MHz probe
Balloon Gomez et al. Proceedings of the American thoracic Society 2009;6(2):180-186

Lung Cancer 21
Operator
end of
scope
Lymph Node Staging Linear Ultrasound or “The Puncture Scope”
Lung Cancer 22
Lymph Node Staging Real-time EBUS
Herth et al. Endoscopy 2006;38 Suppl 1:S105-109
502 patients with any size LN
Sensitivity
96%
Specificity
100%
Accuracy
97%
Linear
EBUS TBNA
Lung Cancer 23
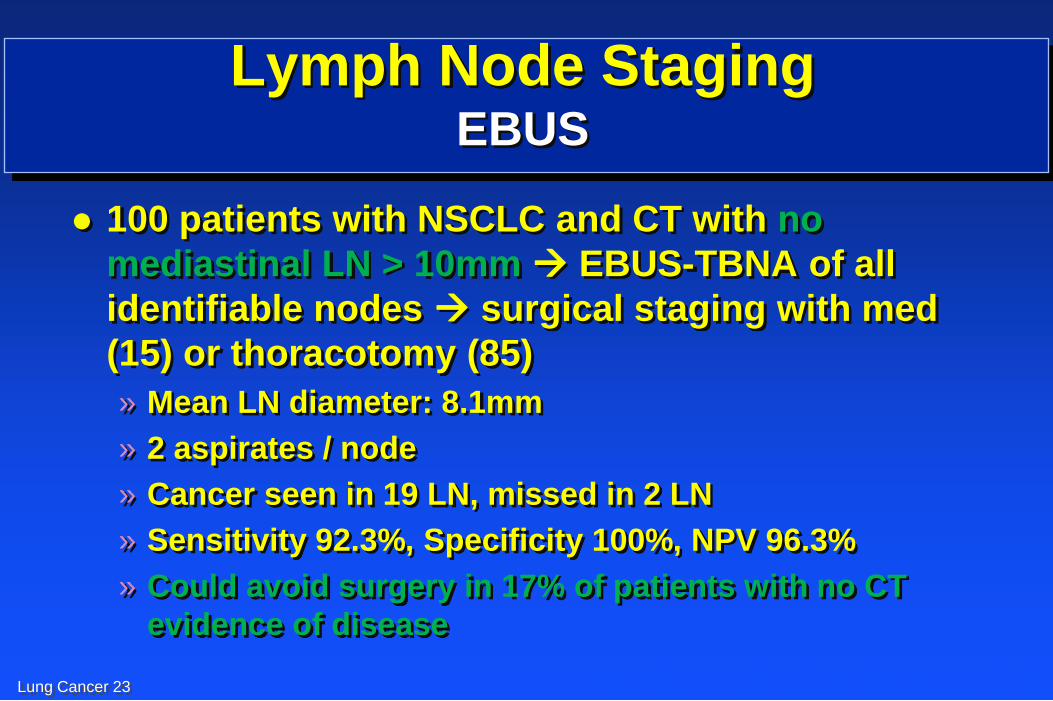
Lymph Node Staging EBUS
100 patients with NSCLC and CT with no
mediastinal LN > 10mm EBUS-TBNA of all
identifiable nodes surgical staging with med
(15) or thoracotomy (85)
» Mean LN diameter: 8.1mm
» 2 aspirates / node
» Cancer seen in 19 LN, missed in 2 LN
» Sensitivity 92.3%, Specificity 100%, NPV 96.3%
» Could avoid surgery in 17% of patients with no CT
evidence of disease
Herth et al, Eur Respir J 2006; 28: 910
Lung Cancer 24
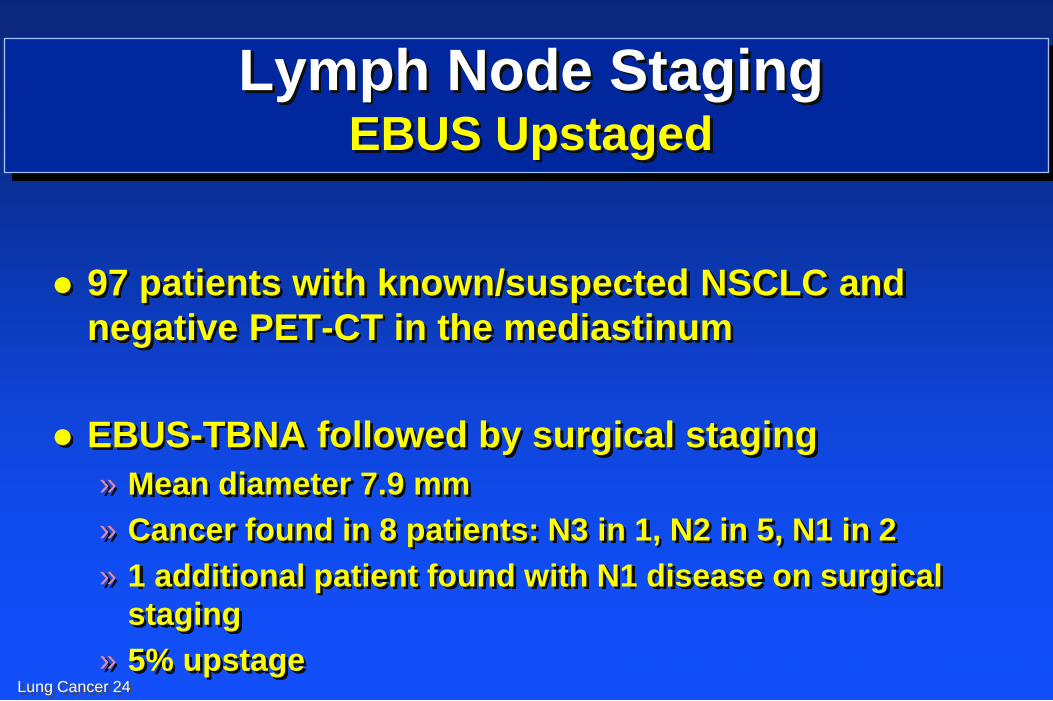
Lymph Node Staging EBUS Upstaged
97 patients with known/suspected NSCLC and
negative PET-CT in the mediastinum
EBUS-TBNA followed by surgical staging
» Mean diameter 7.9 mm
» Cancer found in 8 patients: N3 in 1, N2 in 5, N1 in 2
» 1 additional patient found with N1 disease on surgical
staging
» 5% upstage Herth et al, Chest 2008; 133:887
Lung Cancer 25
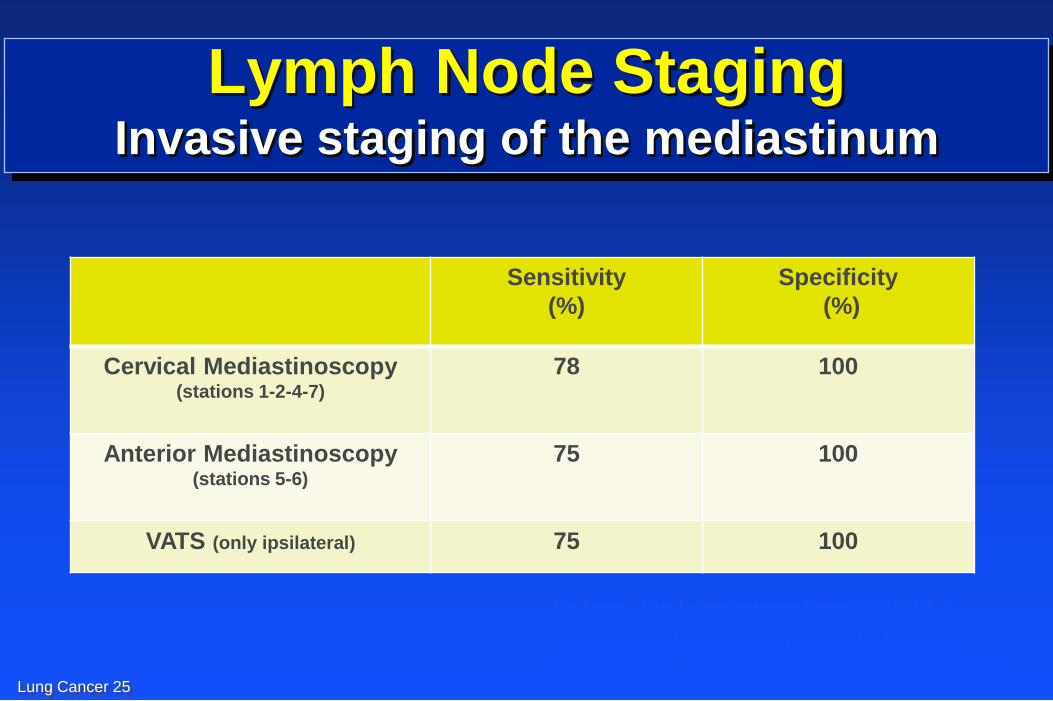
Lymph Node Staging Invasive staging of the mediastinum
Sensitivity
(%)
Specificity
(%)
Cervical Mediastinoscopy (stations 1-2-4-7)
78 100
Anterior Mediastinoscopy (stations 5-6)
75 100
VATS (only ipsilateral) 75 100
De Leyn. Eur L Cardiothrac Surg 2007;32:1-8
Lemaire et al. Ann Thorac Surg 2006;82:1185-1189
Yasufuku et al. Respirology 2007;12:173-183
Lung Cancer 26
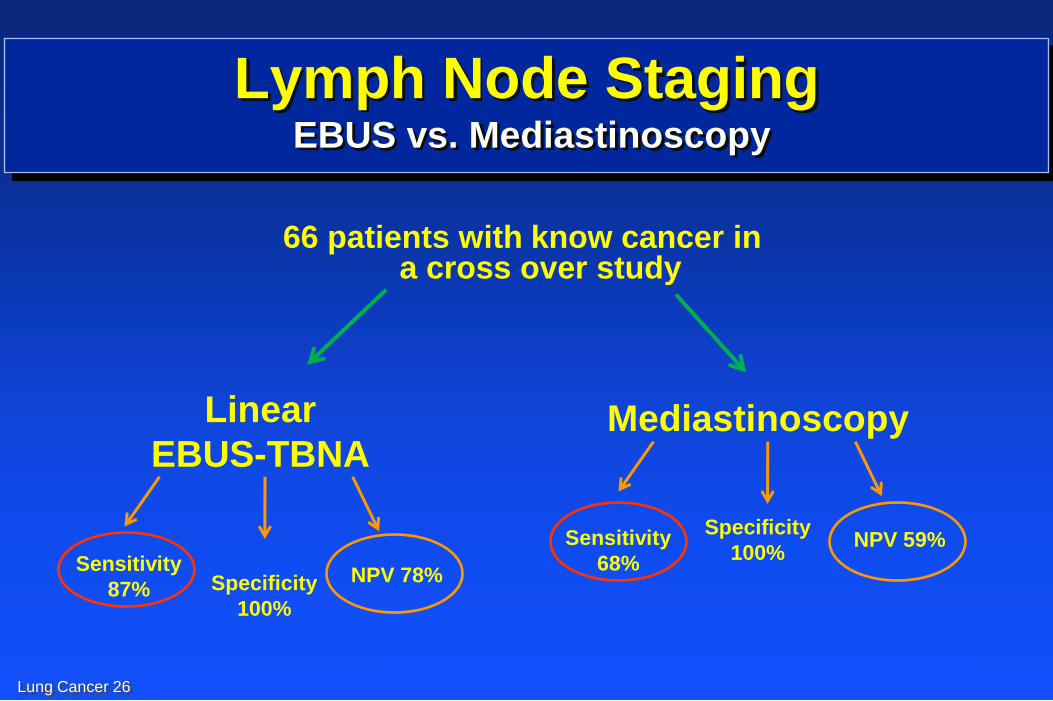
Lymph Node Staging EBUS vs. Mediastinoscopy
Ernst A. et al. Journal of Thoracic Oncology: 3(6):577-82, 2008 Jun
66 patients with know cancer in a cross over study
Sensitivity
68%
Specificity
100% NPV 59%
Mediastinoscopy
Sensitivity
87% Specificity
100%
NPV 78%
Linear
EBUS-TBNA
Lung Cancer 27
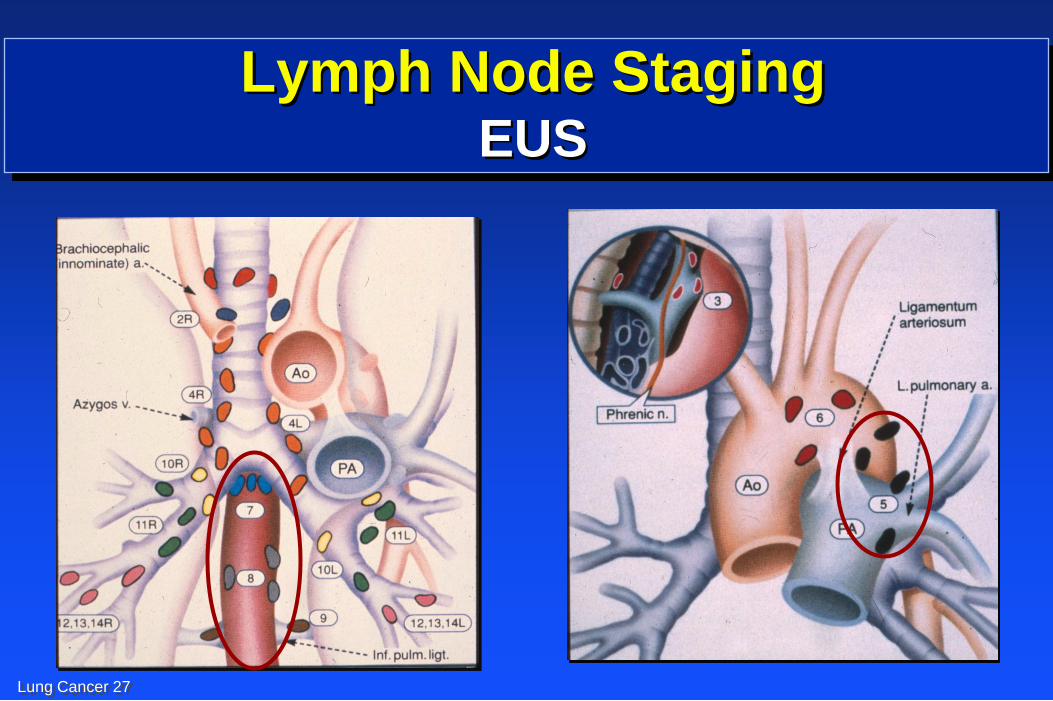
Lymph Node Staging EUS
Lung Cancer 28
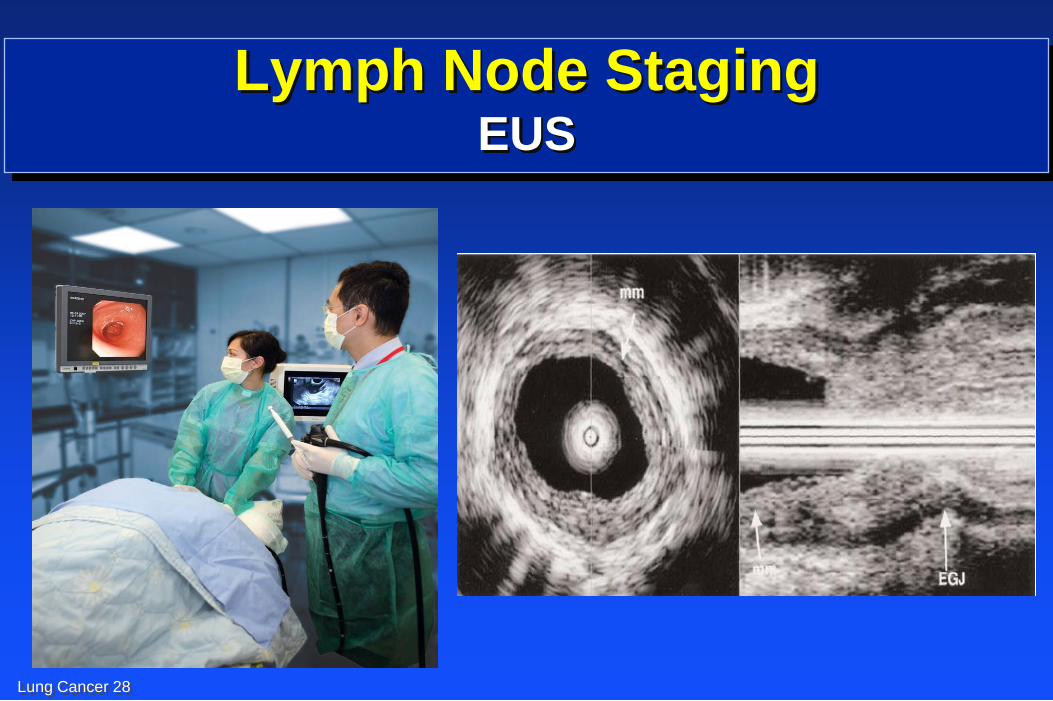
Lymph Node Staging EUS
Lung Cancer 29
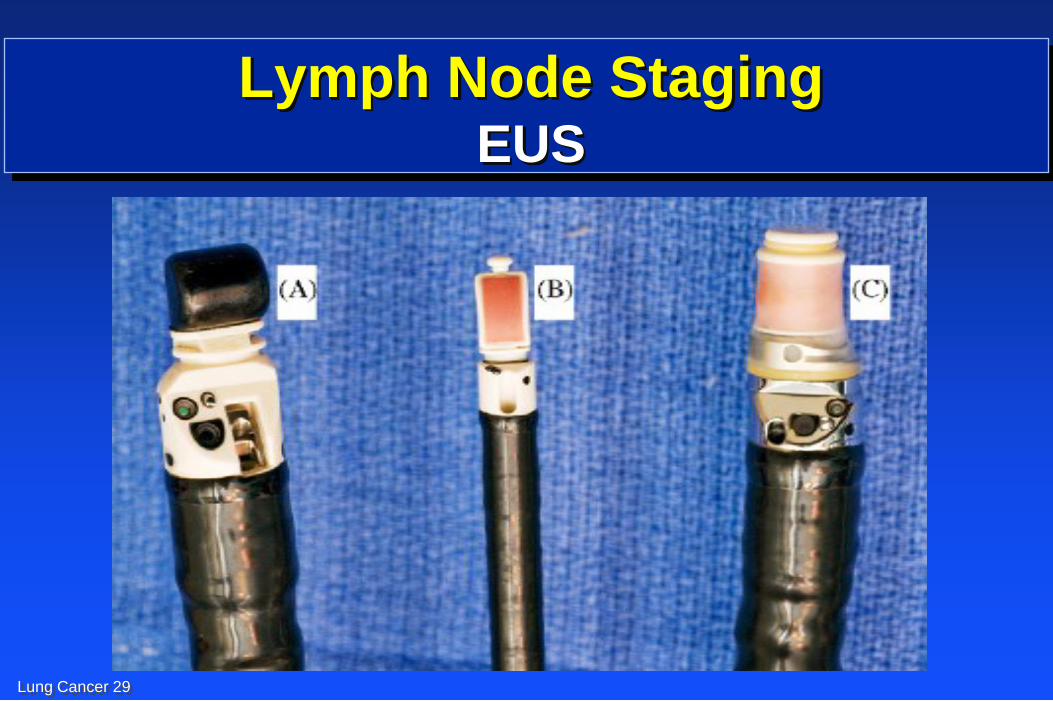
Lymph Node Staging EUS
Lung Cancer 30
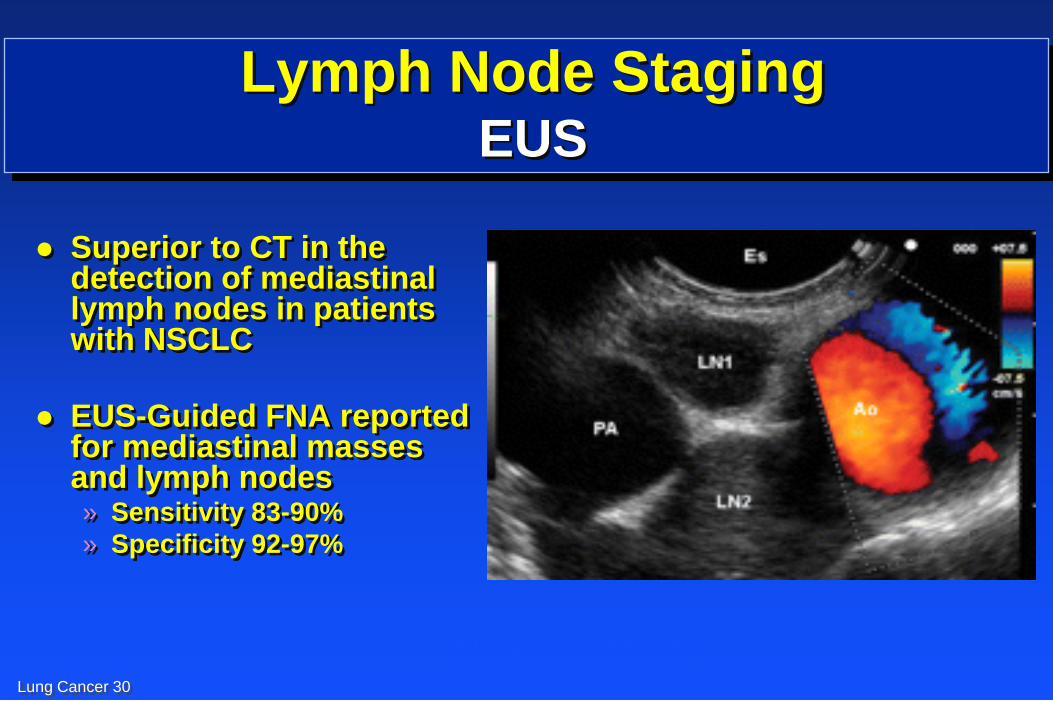
Lymph Node Staging EUS
Superior to CT in the detection of mediastinal lymph nodes in patients with NSCLC
EUS-Guided FNA reported for mediastinal masses and lymph nodes » Sensitivity 83-90%
» Specificity 92-97%
Micames et al CHEST 2007
Ann Int Med 1997; 127:604, Ann Thor Surg 1996; 61:1441
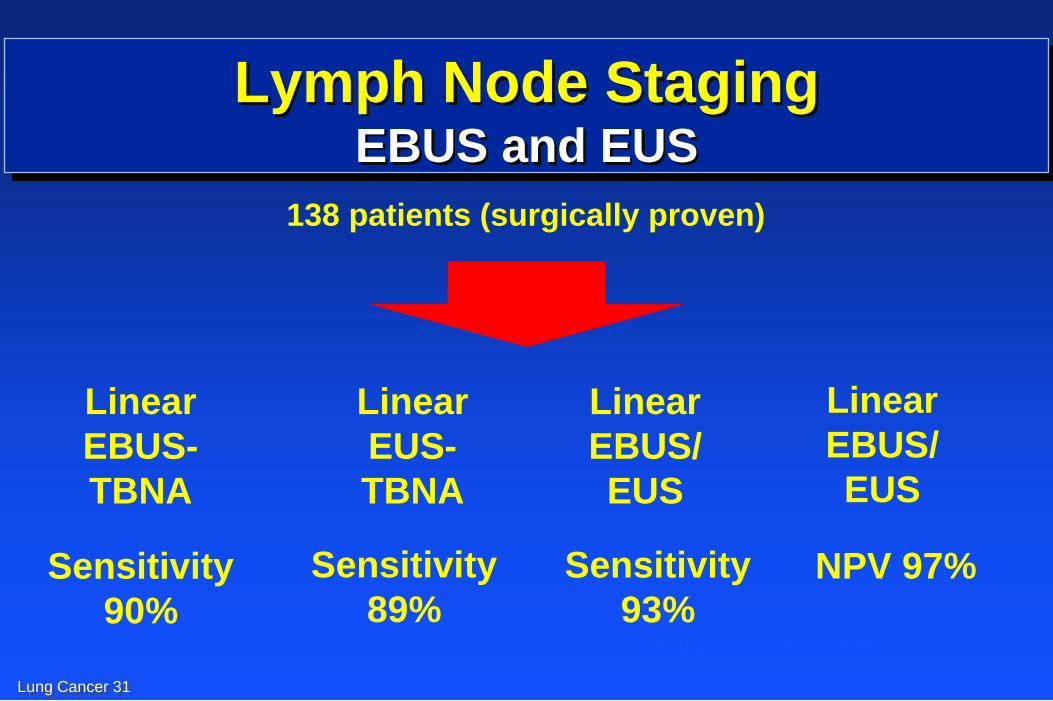
Lung Cancer 31
Lymph Node Staging EBUS and EUS
138 patients (surgically proven)
Sensitivity
90%
NPV 97% Sensitivity
89%
Linear
EBUS-
TBNA
Linear
EBUS/
EUS
Linear
EUS-
TBNA
Linear
EBUS/
EUS
Sensitivity
93% Wallace et al. JAMA, 2008
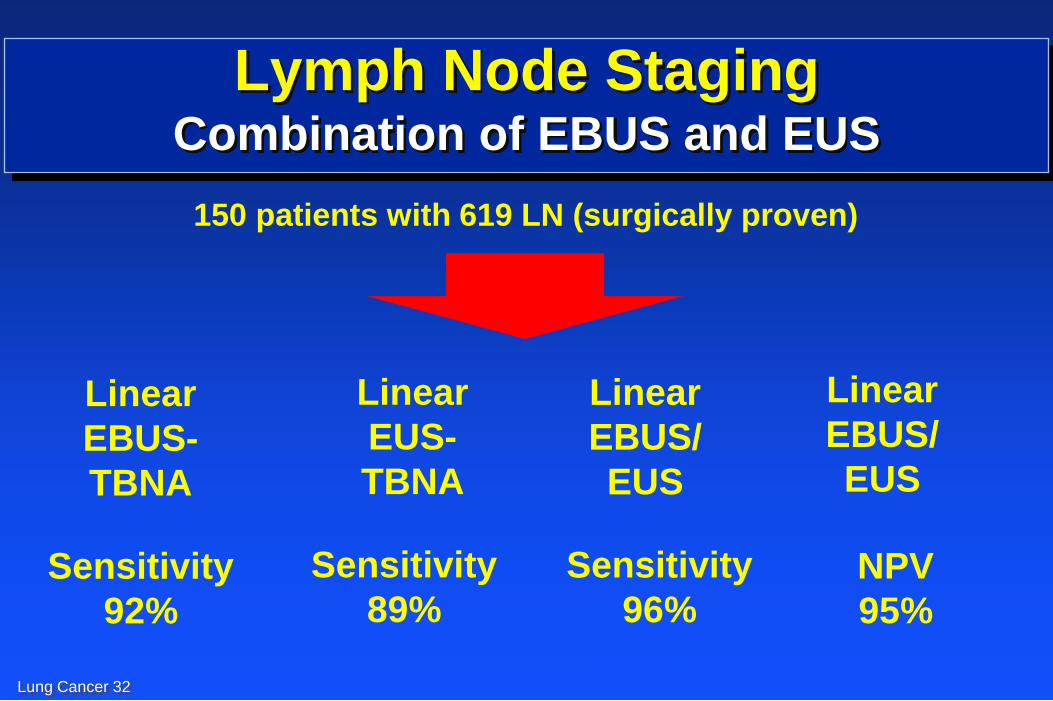
Lung Cancer 32
Lymph Node Staging Combination of EBUS and EUS
150 patients with 619 LN (surgically proven)
Sensitivity
92%
NPV
95%
Sensitivity
89%
Linear
EBUS-
TBNA
Linear
EBUS/
EUS
Linear
EUS-
TBNA
Linear
EBUS/
EUS
Sensitivity
96%
Herth et al, CHEST 2010; 138(4). 790-794
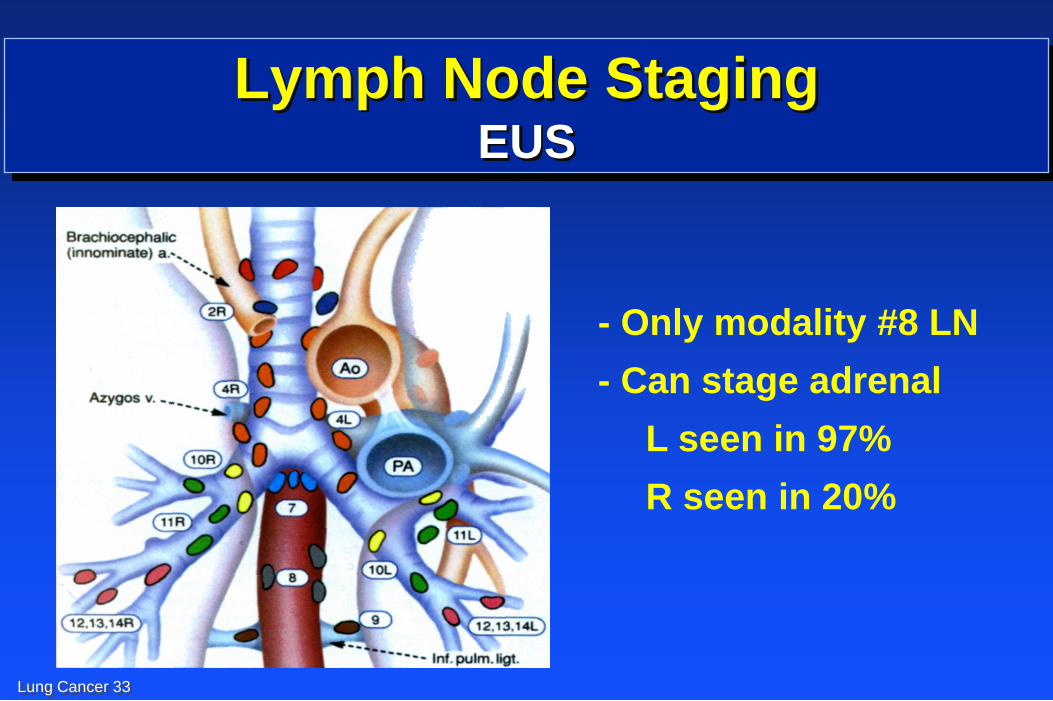
Lung Cancer 33
Lymph Node Staging EUS
- Only modality #8 LN
- Can stage adrenal
L seen in 97%
R seen in 20%
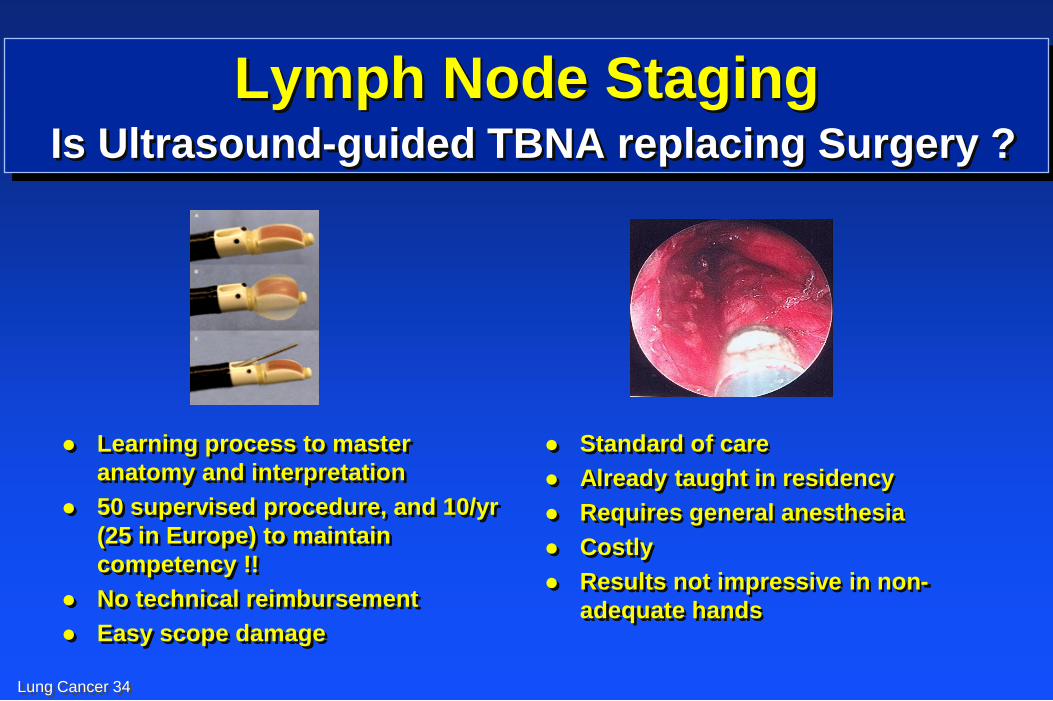
Lung Cancer 34
Lymph Node Staging Is Ultrasound-guided TBNA replacing Surgery ?
Learning process to master
anatomy and interpretation
50 supervised procedure, and 10/yr
(25 in Europe) to maintain
competency !!
No technical reimbursement
Easy scope damage
Standard of care
Already taught in residency
Requires general anesthesia
Costly
Results not impressive in non-
adequate hands
Lung Cancer 35
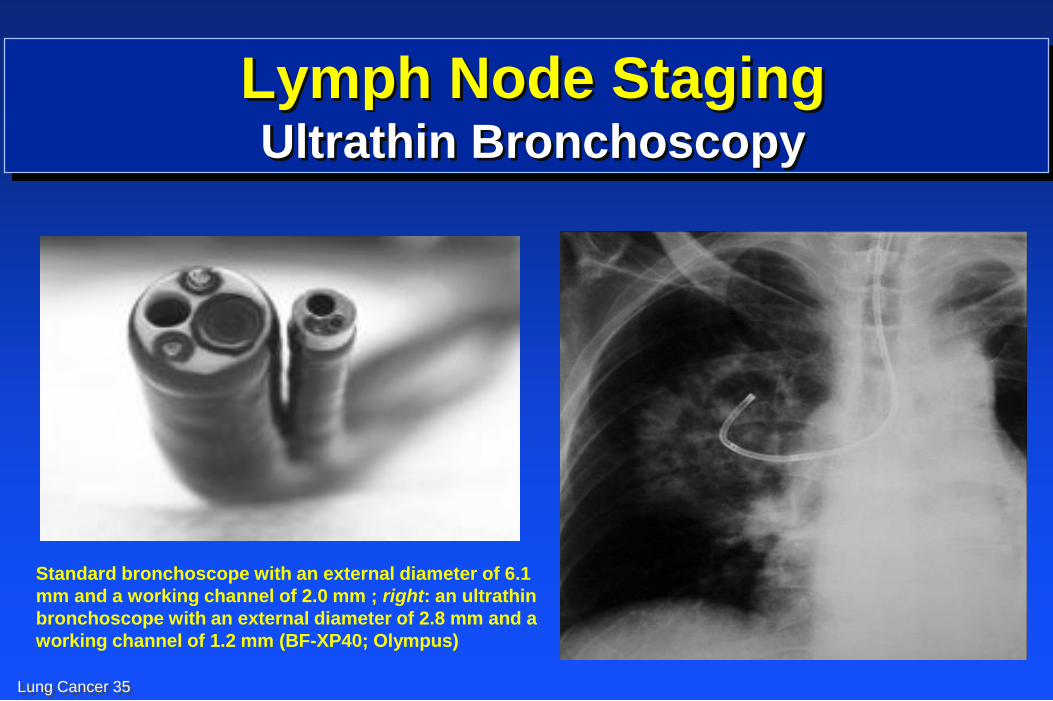
Lymph Node Staging Ultrathin Bronchoscopy
Standard bronchoscope with an external diameter of 6.1
mm and a working channel of 2.0 mm ; right: an ultrathin
bronchoscope with an external diameter of 2.8 mm and a
working channel of 1.2 mm (BF-XP40; Olympus)
Lung Cancer 36
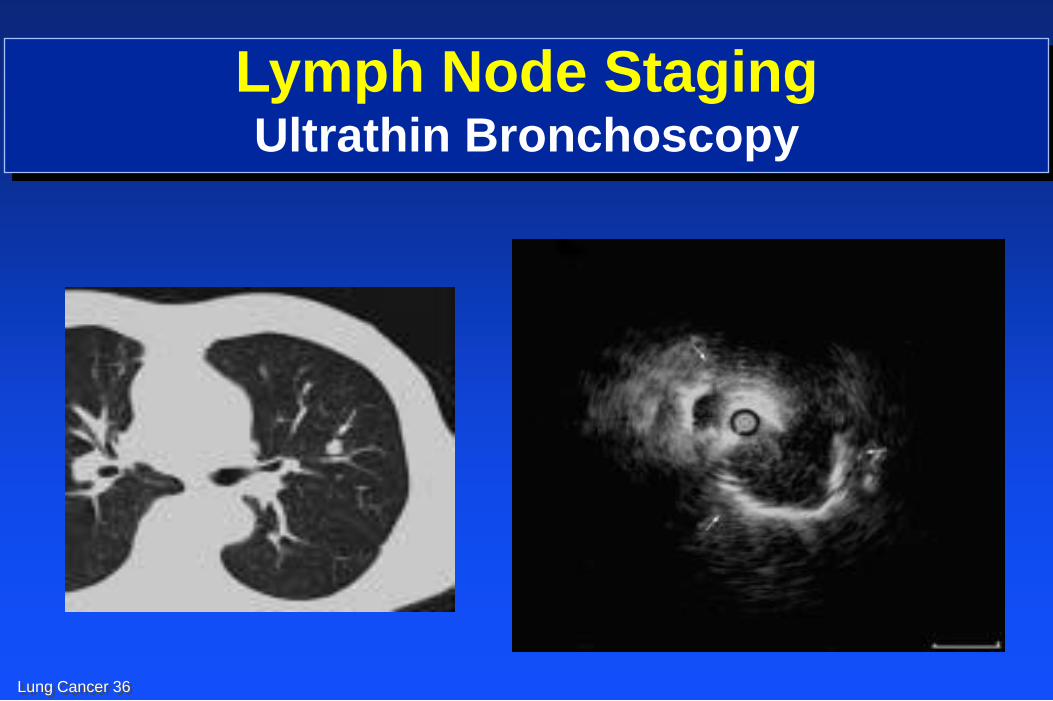
Lymph Node Staging Ultrathin Bronchoscopy
Lung Cancer 37
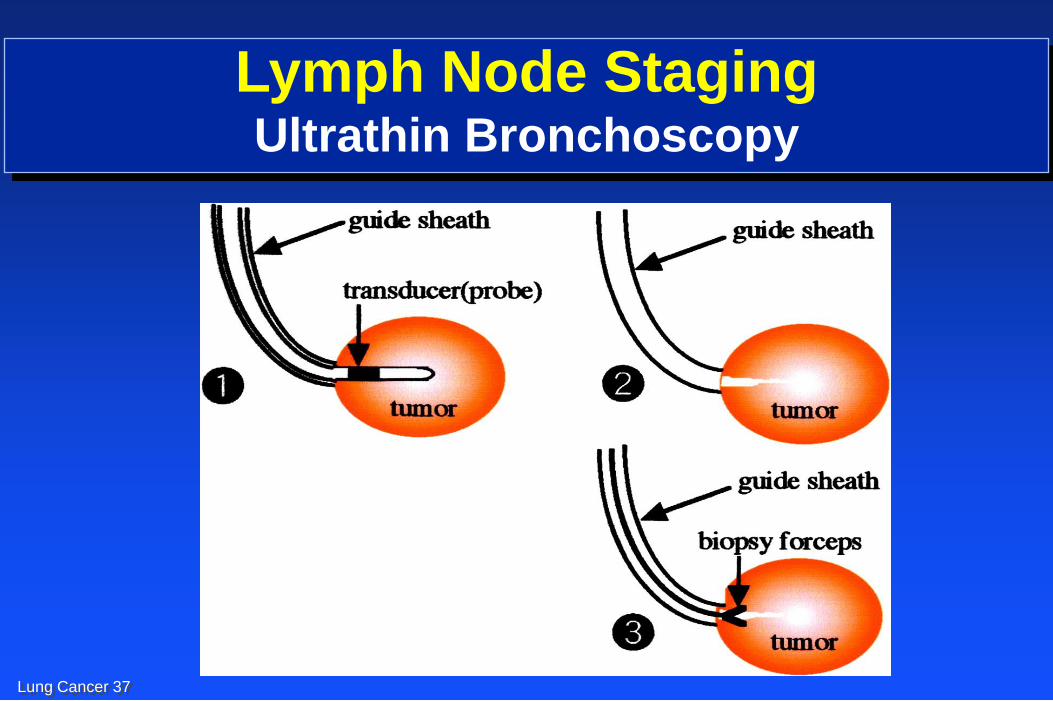
Lymph Node Staging Ultrathin Bronchoscopy
Lung Cancer 38
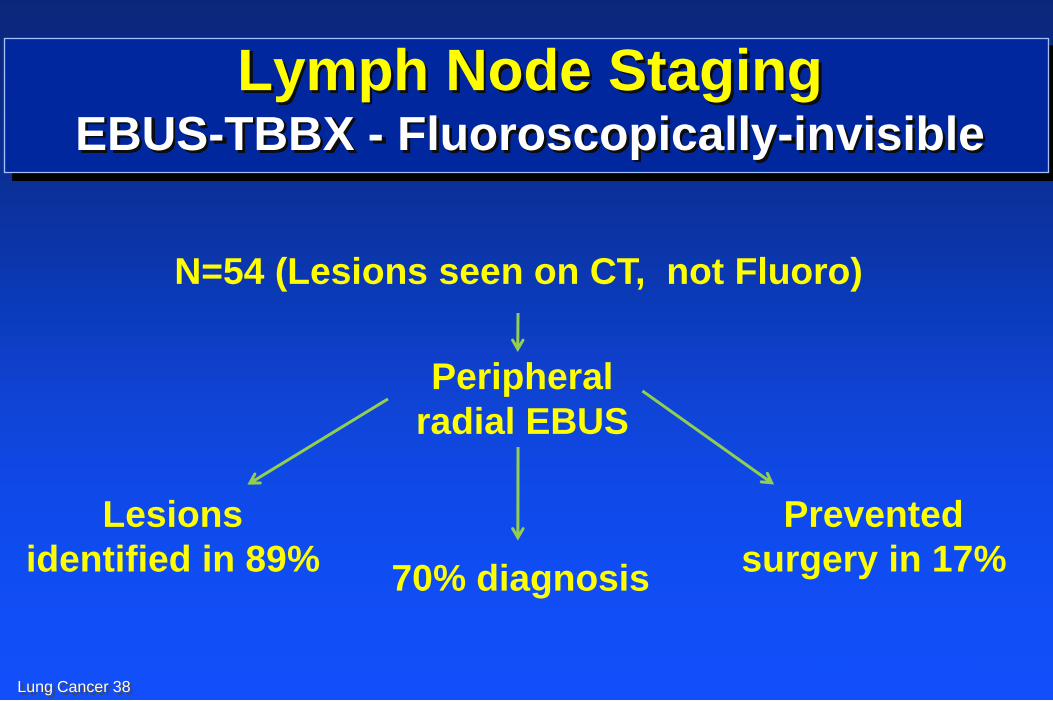
Lymph Node Staging EBUS-TBBX - Fluoroscopically-invisible
N=54 (Lesions seen on CT, not Fluoro)
Peripheral
radial EBUS
Lesions
identified in 89% 70% diagnosis
Prevented
surgery in 17%
Herth et al. Chest 2006;129:147-150
Lung Cancer 39
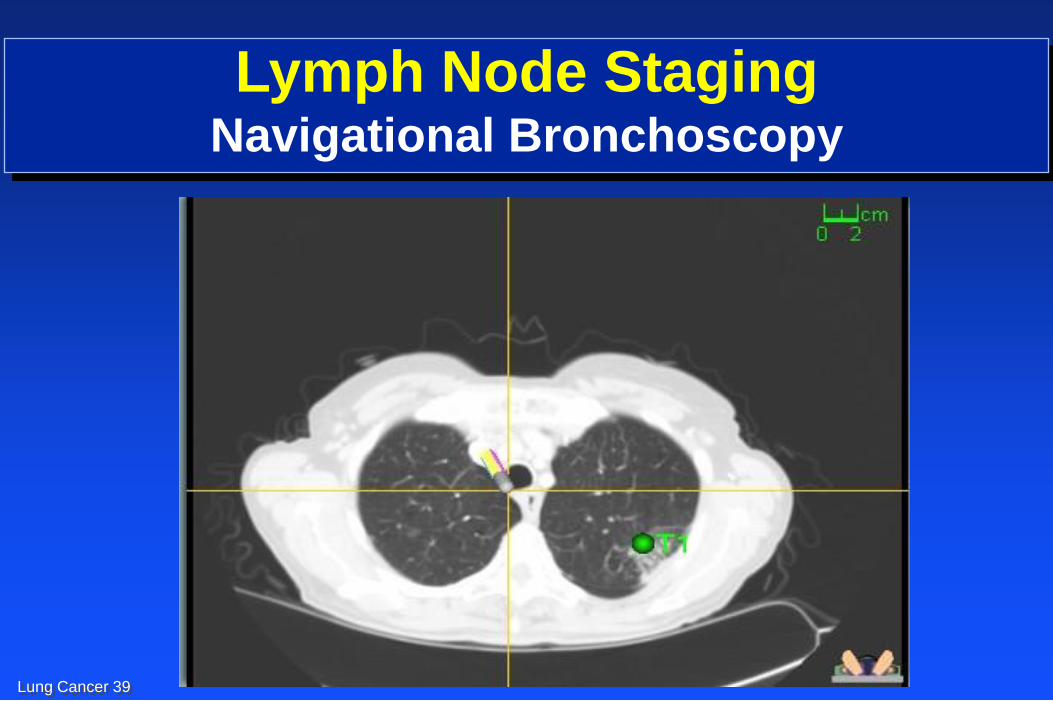
Lymph Node Staging Navigational Bronchoscopy
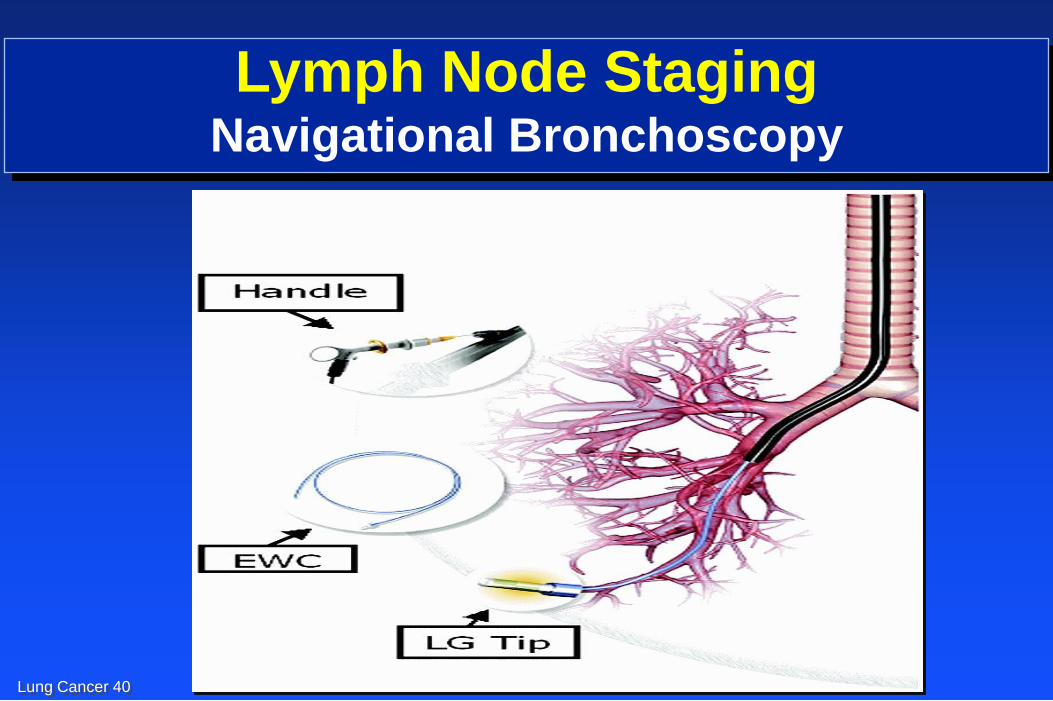
Lung Cancer 40
Lymph Node Staging Navigational Bronchoscopy
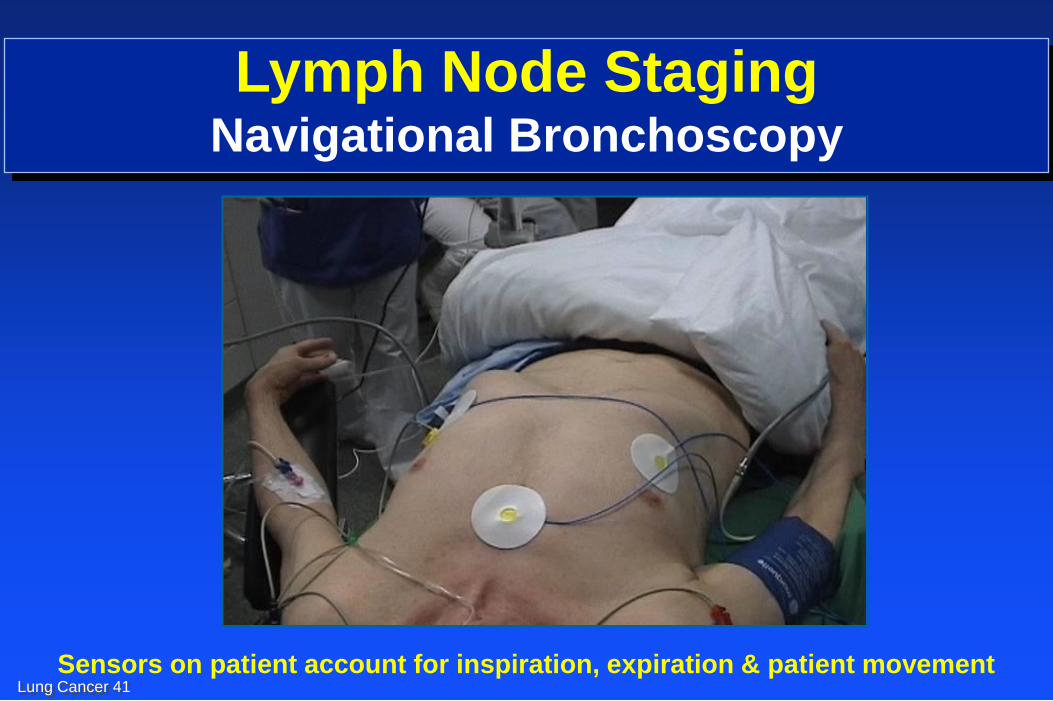
Lung Cancer 41
Sensors on patient account for inspiration, expiration & patient movement
Lymph Node Staging Navigational Bronchoscopy
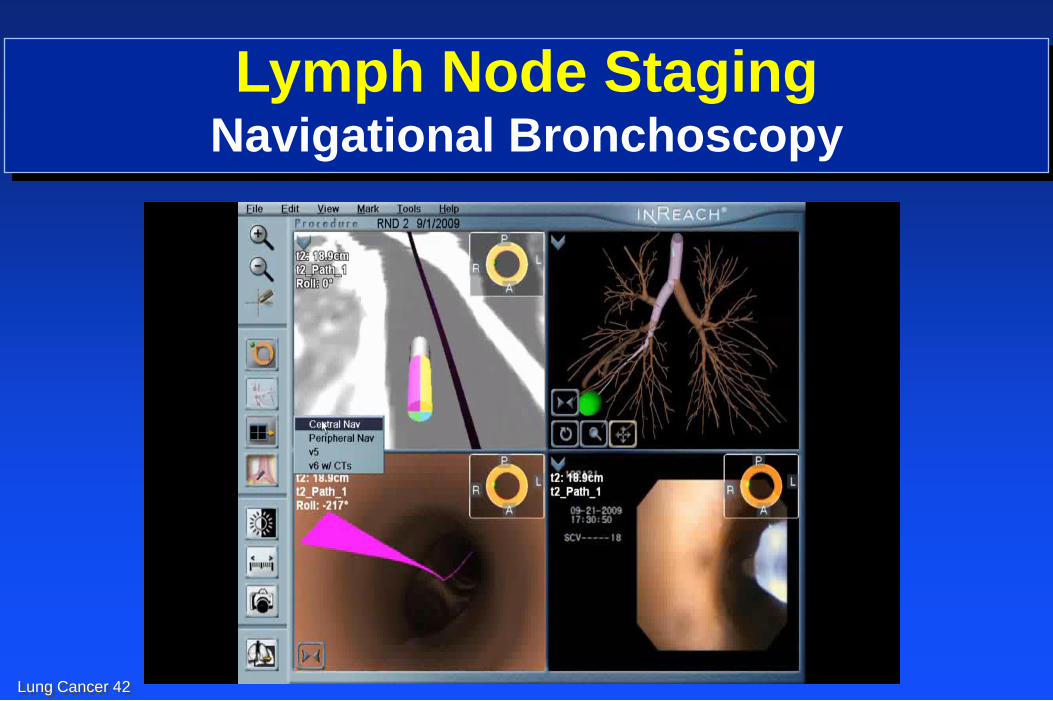
Lung Cancer 42
Lymph Node Staging Navigational Bronchoscopy
Lung Cancer 43
Lymph Node Staging Navigational Bronchoscopy
N=60 (LN and peripheral lesions)
75% yield from
peripheral lesions
100% yield from
lymph node
Final diagnosis obtained in
80% of cases (75% cancer)
Mehta et al. Am J of Resp and Crit Care Med 2007 No Rhythm issues or Fluoro required
Lung Cancer 44
Lymph Node Staging Conclusions
Lymph node metastasis can occur in any size NSCLC
tumor
Accurate clinical staging is essential to provide the
best treatment for patients with NSCLC
Endoscopic staging (EBUS, EUS, SD) methods are
proving to be reliable for staging of the mediastinum
Lung Cancer 45
Lung Cancer
Smoking Cessation