maid in newfoundland - arnnl.ca in newfoundland...maid in newfoundland assisted death as part of the...
TRANSCRIPT

MAiD in Newfoundland
ASSISTED DEATH AS PART OF THE SPECTRUM OF END OF L IFE OPTIONS
-PAIN AND SYMPTOM MANAGEMENT
-ACTIVE TREATMENT WITHDRAWAL
-PALLIATIVE SEDATION
-ASSISTED DEATH

OBJECTIVES:To summarize the Canadian MAiD Data to date
To outline the Medical Assistance in Dying (MAiD) process as it currently stands in Newfoundland.
To discuss individual rights, and the safeguards in place to protect those rights.
To review several cases of MAiD which have occurred in the province
To discuss future considerations- process map, breakdown of the numbers, knowledge translation.

Regarding Medical Assistance in Dying:The Spectrum of care- where are you now?
1 No willingness to deal with Hastened death at all- help patient to find another practitioner
2 Discussion of medical condition, prognosis, treatment options, side effects
3 Discussion of maid process
4 Evaluate the Eligibility of the patient- Do they meet all the criteria?
5 Evaluate the capacity of the patient – Do they understand options and forseableconsequence
6 Able to act as Secondary Physician- oversight role- ensure pt. meets criterion for MAiD
7 Able to act as Primary Physician- assessments, administer medication protocol, death certificate
8 Other ways to participate: (eg. Act as independent witness, share information, etc.)
Please list: ____________________________________________________________________

Federal Data: the first 6 months:




Most Recent Federal Data:As of Aug. 31st, 2017….

Sept. 2017 national data
80
3
11
79
21
49
JUNE 17 -D EC 31ST 2016 JA N1 -JUNE 30 , 2017 D EC. 10TH, 2015 - JUNE 30 , 2017
NUMBER OF MAID DEATHS IN CANADA
Number of MAiD deaths in Canada

Table 2. Profile of Medically Assisted Deaths in Participating Jurisdictions (Excludes QC, NU, YT, NWT)
June 17 toDecember 31, 2016
January 1 to June 30, 2017
Total number of medically assisted deaths 507 875
Number of clinician-administered deaths (voluntary euthanasia)
506 875
Number of self-administered deaths (assisted suicide)
1 0
Number of medically assisted deaths by provider
N/A837 (95.4%) physician
38 (4.6%) nurse practitioner
Settings in which assistance in dying occurred:In hospital
HomeLTC facility or Nursing home
Other
249 (50%)182 (37%)
30 (6%)37 (7%)
368 (41.5%)350 (40.7%)
78 (9.0%)79 (9.0%)
Average age of persons receiving assisted death
72.27 years of age 73 years of age

Age range of persons receiving medical assistance in dying
N/A±
# of Cases Age range
Less than 71
39150144124119102886823
18-35 36-45 46-55 56-64 65-7071-75 76-80 81-85 86-90
90+Unkno
wn‡Proportion of men/women receiving assisted death‡
49% Men51% Women
463 (53%) Men412 (47%) Women
Proportion of individuals receiving assisted death in large urban centres vs. smaller population centresv‡
65.8% Large urban centres34.2 % Smaller population
centres
500 (57.1%) Large urban centres
375 (42.9%) Smallerpopulation centres
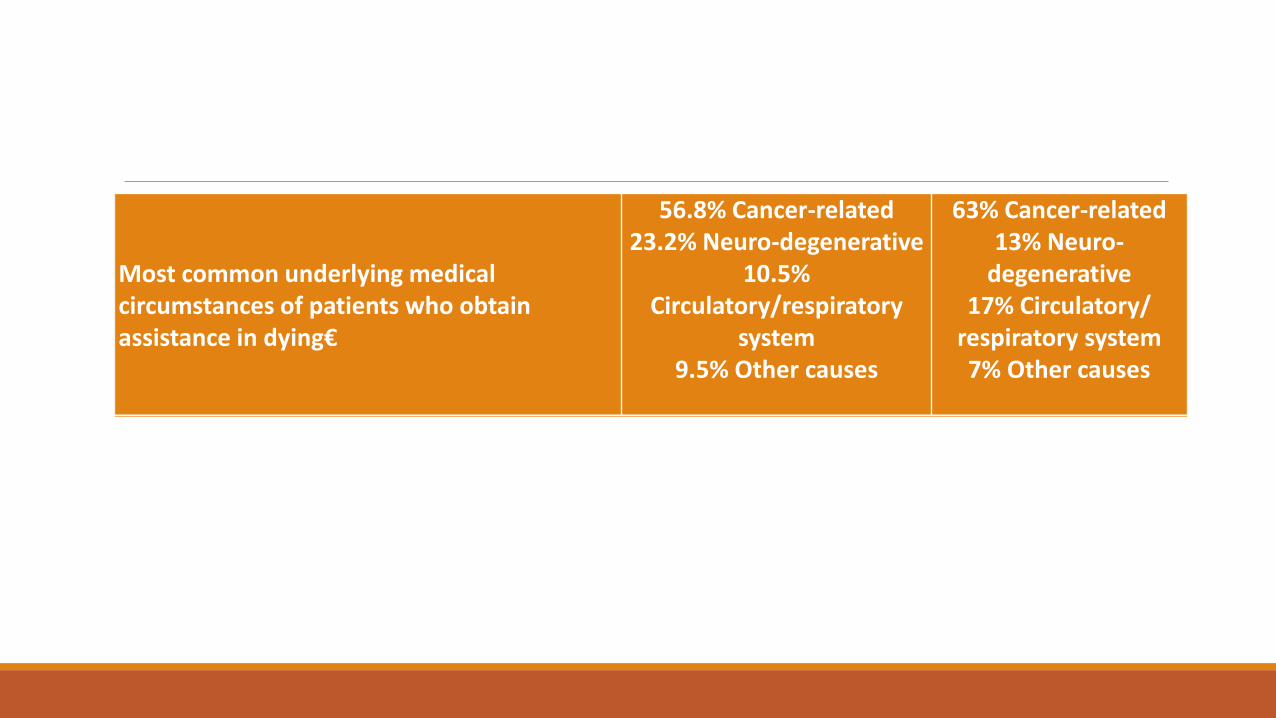
Most common underlying medical circumstances of patients who obtain assistance in dying€
56.8% Cancer-related23.2% Neuro-degenerative
10.5% Circulatory/respiratory
system9.5% Other causes
63% Cancer-related13% Neuro-
degenerative17% Circulatory/
respiratory system7% Other causes

Kay Carter- 89y.o. Canadian woman traveled to“Dignitas” in Switzerland and became the 10thcanadian to die from assisted suicide there.

2015- “The Carter Decision”-no longer illegal to help someone die
It took nearly a year and a half for the federal government to draft new legislation outlining the specifics.
June 2016- Medical Assistance in Dying became law.

Key Legislative Objectives
Recognize personal autonomy and dignity
Recognize inherent and equal value of every life
Include robust safeguards to protect vulnerable persons and guard against errors or abuse
Set out eligibility for competent adults where death is reasonable foreseeable and who are suffering intolerably
Balance different interests, including personal autonomy toward the end of life and the protection of vulnerable persons
Encourage consistent approach across Canada

Newfoundland Response
Extensive consultation by Government between August 2015 and early 2017.
High degree of consensus in province
“ability of people to start from a position of compassion and empathy for patients, families and health care”.
Government interest in “providing coherent programming with equitable access to patients across the province”.

Newfoundland ResponseGovernmental Correspondence - June 2017
Appointment of Provincial Medical Assistance in Dying (MAiD) Coordinator.
◦ Working with RHAs ---------MAiD Coordinating team
◦ The development of provincial standards for operational polices and protocol
◦ The development and delivery of education and training for health professionals.

THE N.L. NUMBERS: so far…As of June 2016 to March 1, 2018:
Newfoundland: 28 requests, 22 completed
Eastern- 22 requests, 14 assisted, 1 did not meet criteria, 5 died prior, 4 pending.
Central- 6 requests, 6 assisted
Western- 2 requests, 2 assisted
Labrador/Grenfell - 0

How many? (What will be the workload?)In countries with an established MAiD process…
Out of 100 deaths:◦ On average about 7 people will apply for HD
◦ Of those only ~3 will get approval
◦ Less than half (1) will actually complete HD
According to Statistics Canada:
2016-17- N.L. had 5,280 estimated deaths (increasing by ~120/year)
Assessments: about 7% = 370 /y
Assisted deaths: about 1% = 53/y
Actual number: June 2016-June 2017 0.25% = 13/y

MAiD in NL Pathway- linear- (Patient)Initial inquiry- requirement for a “fulsome discussion”- Ontario case regarding referral
Formal Request-
Primary assessment (first physician/NP)- Skype/telehealth OK
Secondary assessment (Second Doc/NP) –attestation
Waiting period of 10 “CLEAR” days
Final determination of capacity – day of procedure
Administration of med protocol- peer to peer debrief- immediate
Formal debrief- days-weeks later- Systems improvement

MAiD Pathway NL1) Pt’s initial inquiry- to clinician – obligation of a
◦ “Fulsome conversation”- done by health care provider-Social Work: Discussion of end of life- advanced directives, SDM- standard of practice- OK to have discussion
2) Ensure Pt informed of Dx, prognosis, Tx, Sfx to ensure INFORMED consent- done by health care provider
ISSUE OF INFORMED CONSENT- need to know options and consequences of options
3)Eligibility?
- Canadian Health care, 18yo, capacity, voluntary, informed consent to MAiD- Done by MRP or MAiD physician (soon NP?)

Under the Criminal Code:Counselling or aiding suicide
241 (1) Everyone is guilty of an indictable offence and liable to imprisonment for a term of not more than 14 years who, whether suicide ensues or not,
◦ (a) counsels a person to die by suicide or abets a person in dying by suicide; or
◦ (b) aids a person to die by suicide.
Marginal note : Exemption for medical assistance in dying
(2) No medical practitioner or nurse practitioner commits an offence under paragraph (1)(b) if they provide a person with medical assistance in dying in accordance with section 241.2.

Federal Legislation- Bill C-14
“Clarification
(5. 1) For greater certainty, no social worker, psychologist, psychiatrist, therapist, medical practitioner, nurse practitioner or other health care professional commits an offence if they provide information to a person on the lawful provision of medical assistance in dying.”
The whole purpose of C14 was to amend the criminal code to exclude Health professionals from prosecution under the old subsection 241(1)(a) of the Criminal Code.

ARNNL – guidelines regarding MAiD“RN and NP may aid in providing nursing care and perform activities within their scope of practice such as:
Providing information about MAiD upon the client’s request to clients/families;”

MAiD NL ctd4) Grievous and irremediable condition?
◦ Serious and incurable condition
◦ Advanced state of irreversible decline
◦ Causing enduring suffering, intolerable to the individual, no acceptable relief.
◦ Natural death “reasonably foreseeable” or “on the downward trajectory” or more specifically “Advanced state of irreversible decline in capability”◦ Note: In the Carter decision there was no requirement of “foreseeable death”

Advanced state of irreversible decline in capability
When combined with the requirements that death be reasonably foreseeable and that the person be suffering intolerably, the requirement to be in an advanced state of irreversible decline ensures that medical assistance in dying would be available to those who are in an irreversible decline towards death, even if that death is not anticipated in the short term. This approach to eligibility gives individuals who are in decline toward death the autonomy to choose their preferred dying process

Reasonably foreseeable death
In the context of medical assistance in dying, it means that there is a real possibility of the patient’s death within a period of time that is not too remote. In other words, the patient would need to experience a change in the state of their medical condition so that it has become fairly clear that they are on an irreversible path toward death, even if there is no clear or specific prognosis. Each person’s circumstances are unique, and life expectancy depends on the nature of the illness, and the impacts of other medical conditions or health-related factors such as age or frailty. Physicians and nurse practitioners have the necessary expertise to evaluate each person’s unique circumstances and can effectively judge when a person is on a trajectory toward death. While medical professionals do not need to be able to clearly predict exactly how or when a person will die, the person’s death would need to be foreseeable in the not too distant future.

http://www.health.gov.nl.ca/health/faq/pdf/medical_assistance_dying.pdf

MAiD NL- Administration of meds Prescription to Pharmacist: Informed by Dr. of MAiD intention, and time-frame for use
Dispense meds to administering physician ONLY (Pharmacy Board) 2 kits dispensed – Hospital vs Community pharmacy
***One final opportunity given to Pt to withdraw request and demonstrate capacity. (Signature-if possible)
Administer Meds-
unused meds returned
Death Certificate-

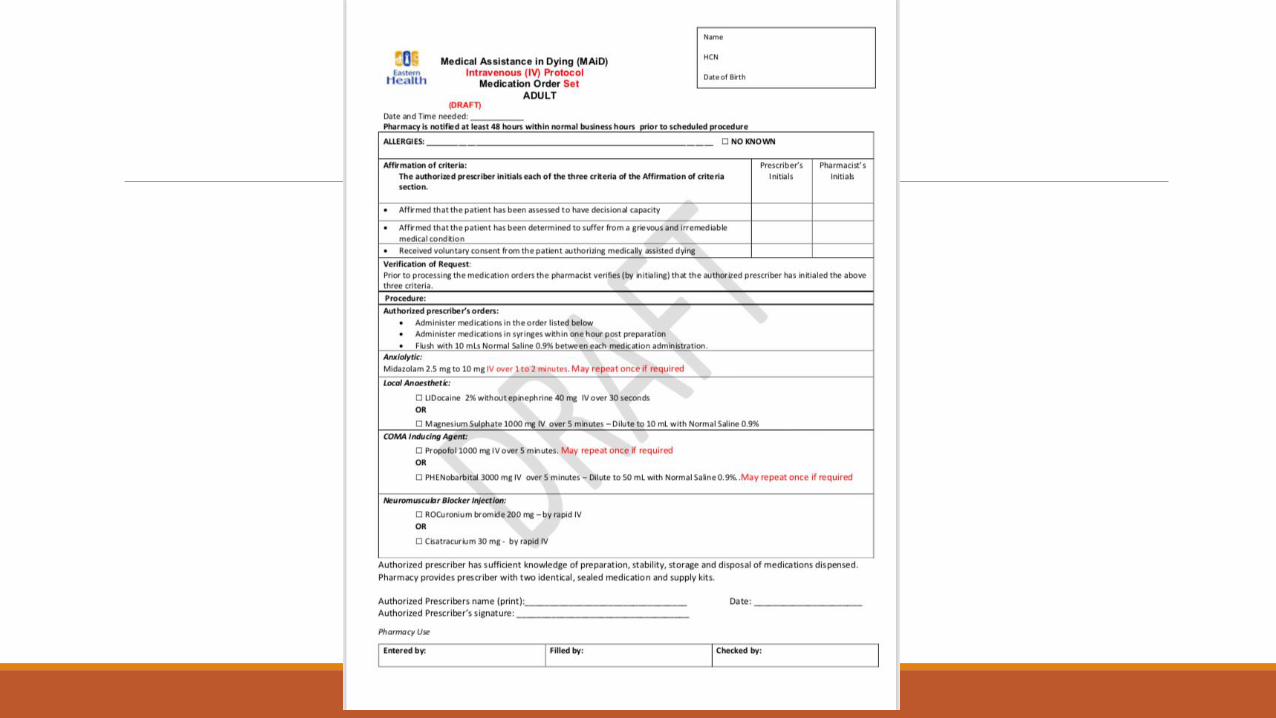
Med protocol:

Meds for Euthenasia
1)Sedative/ Anxiolytic (light): Benzodiazepine (Midazolam- 2.5 to 10mg over 30 seconds)
2) Sedation (deep):
Local anesthesia- Lidocaine or Mag sulph.
Coma- Barbiturate- Phenobarb, Propofol
3) Neuromuscular blocade:
Cisatracurium 30mg/15ml rapid IV or
Atracurium 100mg/10ml rapid IV
Rocuronium Bromide 200mg/20ml rapid IV ??Pentobarbita??
Death Certificate:No obligation to report MAiD on death certificate.- data will be tracked via federal reporting mechanism***
Provincial Recommendation: Underlying illness, MAiD does not need to be on the Death Cert.
Could lead to incorrect data collection-
Confidentiality requirements.
Other provinces differ- eg Ontario

Regional MAiD CoordinationLabrador/Grenfell:
◦ Regional Coordinator- Dr. Gabe Woollam [email protected]
◦ Referrals- [email protected] Fax: (709)896-4032 Questions- Tel: (709)897-2350
Western: ◦ Regional Coordinator-Dr. Jeff Cole [email protected]
◦ Referrals- Fax: (709)637-5159 Questions- Tel: (709)637-5000 ext. 5168
Central Health ◦ Regional Coordinator- Sueann Fry [email protected]
◦ Referrals- Fax: (709) 292-2249 Questions- Tel: (709) 292-2151
Eastern Health: ◦ Regional Coordinator- Judy Davidson [email protected]
◦ Referrals- [email protected] Fax: (709) 777-7774Questions- Tel: (709)777-7679
Provincial Coordinator: Dr. Aaron McKim [email protected]
Fax: (709) 729-0121 Tel: (709) 729-3103

Future considerations: provincialRegional Teams- responsible for setting up and maintaining regional MAiD database of assessors and providers, and coordination of requests.
Departmental/ Site leads- responsible for information dissemination, coordinating any requests and possibly assessments or provision of MAiD
Faith Based “opt outs”- update
Billing codes- sessional?
Training/certification?
Oral protocol?
Institutional vs at home?

Future considerations: NationalMental Illness only?
Emancipated youth?
Advanced directives?

Regarding Medical Assistance in Dying:The Spectrum of care- where are you now?
1 No willingness to deal with Hastened death at all- help patient to find another practitioner
2 Discussion of medical condition, prognosis, treatment options, side effects
3 Discussion of maid process
4 Evaluate the Eligibility of the patient- Do they meet all the criteria?
5 Evaluate the capacity of the patient – Do they understand options and forseeableconsequence
6 Able to act as Secondary Physician- oversight role- ensure pt. meets criterion for MAiD
7 Able to act as Primary Physician- assessments, administer medication protocol, death certificate
8 Other ways to participate: (eg. Act as independent witness, share information, etc.)
Please list:______________________________________________________________________

Cases:

Case 165 y.o. woman
Advanced metastatic disease- Mets to Brain, Bone, liver, lung.
Saw a close relative die under similar circumstances- delirium, shouting, hallucinating. She wanted no part of it.
Requested MAiD- Urgent timeline.

Eligibility- Case 1Above 18? – yes
Covered for health care – yes
Capable of consenting - yes
Informed consent – partially, can be accomplished
Voluntary – yes
Grievous and irremediable medical condition?

Case 1 ctd.Developed confusion- delirium/drug toxicity
Capable of consenting – NO.
Decreased dose/med changes- regained capacity
“What are you waiting for?!?”
Quebec protocol- administered.

Case 274 y.o. man in assisted living- St John’s.
Metastatic mesothelioma- exhausted treatment options.
Palliative care involved. Getting hard to breath, feeling drained.
Wanted MAiD- didn’t know where to turn.
Contacted by daughter.
1st assessment- meets criteria.
Case 2 ctd.After initial assessment- stopped chemo
- Pt felt better. “Didn’t want to go just yet”
Time to coordinate the specifics: who, where, meds, IV access, timeline.
Initial call to oncologist and GP, palliative care doc.- not helpful
Weeks later-Called by daughter- nearly choked to death in the night- wants MAiD ASAP!
At the end-3 oncologists participated as physician learners. PC doc 2nd assessor.

Case 387 y.o. man with advanced pancreatic cancer- refractory to medical management.
June 23rd- Declaration of intent
June 26th Met with patient- Assessed Pt. and outlined his other options: ◦ pain and symptom management
◦ Palliative sedation
◦ Patient was not interested in these options. Determined he did meet the criterion for MAiD.
June 28th-Secondary assessment completed
“10 clear days” – Date set for July 4th, 2017

But then-June 30th (Friday AM) called by nurse in LTC facility: “He’s going downhill rapidly”
Initiated “expedited process”◦ Contacted second physician- would reassess situation- in agreement with expiditing
◦ Contacted CMPA- “Too short a time frame”
◦ Pharmacy- had meds ready.
After morning clinic- picked up meds, went to the LTC facility. Met with nursing staff.
Family physician in attendance- Patient had decided “not today- I feel too good”

Case 3 continuedPatient advised I was going out of town and would not be back until after the weekend.
July 4th (Tuesday)- Met with Care team at the LTC facility.
Patient somnolent, sleepy even though pain meds had been lightened up in an attempt to rows him. Able to nod “YES” when asked if he wanted MAiD- however when we asked him to indicate he knew what he was agreeing to- he could not reply. When asked if he would rather simply have pain meds and expire without assistance to die- he could not answer.
We tried with hand squeezing- and again he cold squeeze once for yes, but could not squeeze twice for no. Could not indicate with clarity that he was aware he could withdraw, or meaningfully indicate he comprehended what he was saying yes to.
Case 3 continuedPatient advised I was going out of town and would not be back until after the weekend.
July 4th (Tuesday)- Met with Care team at the LTC facility.
Patient somnolent, sleepy even though pain meds had been lightened up in an attempt to rows him. Able to nod “YES” when asked if he wanted MAiD- however when we asked him to indicate he knew what he was agreeing to- he could not reply. When asked if he would rather simply have pain meds and expire without assistance to die- he could not answer.
We tried with hand squeezing- and again he cold squeeze once for yes, but could not squeeze twice for no. Could not indicate with clarity that he was aware he could withdraw, or meaningfully indicate he comprehended what he was saying yes to.

Conclusions:Medical Assistance in Dying (MAiD) is now legal under specific circumstances
Safeguards are in place to ensure that individual choice and safety are protected.
If a person has lost capacity or is unable to give informed consent- they are not eligible for MAiD
Individuals rights are balanced against protecting vulnerable people
Each of the 4 health regions in Newfoundland and Labrador have their own MAiD coordination teams which can help individuals answer questions or address requests for MAiD
