major clinical trials in diabetic retinopathy
TRANSCRIPT

Major Clinical Trials in Diabetic Major Clinical Trials in Diabetic Retinopathy Retinopathy
Joseph T. Fan, M.D.Joseph T. Fan, M.D.Loma Linda UniversityLoma Linda University

Diabetic RetinopathyDiabetic Retinopathy
How are the present treatment How are the present treatment choices shaped by results of past choices shaped by results of past clinical trials? clinical trials?
What are important questions yet be What are important questions yet be answered by new clinical trials? answered by new clinical trials?
Diabetic RetinopathyDiabetic Retinopathy
Major cause of legal blindnessMajor cause of legal blindness
Two Types: NonTwo Types: Non--proliferative, proliferative, proliferativeproliferative
Intense glucose control results in Intense glucose control results in reduction in diabetic retinopathyreduction in diabetic retinopathy
Laser surgery for retinopathy is most Laser surgery for retinopathy is most effective before visual loss occurseffective before visual loss occurs

Diabetic RetinopathyDiabetic Retinopathy
Five multicenter clinical trials have Five multicenter clinical trials have established the basis for the management established the basis for the management
of diabetic retinopathyof diabetic retinopathy
•• Diabetes Control and Complications TrialDiabetes Control and Complications Trial•• United Kingdom Prospective Diabetes StudyUnited Kingdom Prospective Diabetes Study•• Early Treatment Diabetic Retinopathy StudyEarly Treatment Diabetic Retinopathy Study•• Diabetic Retinopathy StudyDiabetic Retinopathy Study•• Diabetic Retinopathy Vitrectomy StudyDiabetic Retinopathy Vitrectomy Study
NonNon--PorliferativePorliferative Diabetic Diabetic RetinopathyRetinopathy
Does intense glucose control reduce Does intense glucose control reduce diabetic retinopathy?diabetic retinopathy?
•• Diabetes Control and Complications TrialDiabetes Control and Complications Trial•• United Kingdom Prospective Diabetes United Kingdom Prospective Diabetes
StudyStudy

NonNon--Proliferative Diabetic Retinopathy:Proliferative Diabetic Retinopathy:
MicroaneurysmsMicroaneurysms
EdemaEdemaHard exudatesHard exudatesIntraretinalIntraretinal hemorrhageshemorrhages




Diabetes Diabetes Control and Complications Control and Complications Trial (DCCT) 1983Trial (DCCT) 1983--19931993
1441 Patients1441 Patients–– Absence of hypertension, hypercholesterolemia, and Absence of hypertension, hypercholesterolemia, and
severe diabetic complicationssevere diabetic complications
2 groups2 groups–– Type 1 diabetes and no diabetic retinopathyType 1 diabetes and no diabetic retinopathy–– Type 1 diabetes and mild to moderate diabetic Type 1 diabetes and mild to moderate diabetic
retinopathyretinopathy
Study questionsStudy questions–– Primary prevention study:Primary prevention study:
Will intensive blood glucose control slow the development of Will intensive blood glucose control slow the development of progression to diabetic retinopathy?progression to diabetic retinopathy?
–– Secondary prevention study:Secondary prevention study:Will intensive blood glucose control slow progression of Will intensive blood glucose control slow progression of diabetic retinopathy?diabetic retinopathy?

DCCT: 1983DCCT: 1983--19931993
Primary prevention group: Type 1 Diabetes Primary prevention group: Type 1 Diabetes with no retinopathy (726 patients)with no retinopathy (726 patients)Secondary preventions group: Type 1 Secondary preventions group: Type 1 Diabetes with mild to moderate NPDR (715 Diabetes with mild to moderate NPDR (715
patients)patients)
Patients randomized to conventional Patients randomized to conventional treatment or intensive treatment groups.treatment or intensive treatment groups.

DCCT: 1983DCCT: 1983--19931993
Conventional Treatment GroupConventional Treatment Group–– Insulin injections (once or twice a day)Insulin injections (once or twice a day)–– Daily self monitoring of glucoseDaily self monitoring of glucose–– Clinic visits every 3 monthsClinic visits every 3 months–– Diet and exercise educationDiet and exercise education
Intensive Treatment GroupIntensive Treatment Group–– Insulin pump or 3 or more insulin shots a dayInsulin pump or 3 or more insulin shots a day–– Self monitoring of blood glucose four or more times a Self monitoring of blood glucose four or more times a
dayday–– Diet and exercise planDiet and exercise plan–– Initial hospitalization to implement treatmentInitial hospitalization to implement treatment–– Weekly to monthly clinic visitsWeekly to monthly clinic visits
DCCT Results: Primary DCCT Results: Primary Prevention GroupPrevention Group
Intensive blood sugar control 27% Intensive blood sugar control 27% reduction in development of Diabetic reduction in development of Diabetic Retinopathy and 78% reduction in Retinopathy and 78% reduction in progression of Diabetic Retinopathy, progression of Diabetic Retinopathy, with a mean followwith a mean follow--up 6.5 years.up 6.5 years.

DCCT Results: Secondary DCCT Results: Secondary Prevention GroupPrevention Group
Intensive blood sugar control had a 54% Intensive blood sugar control had a 54% reduction in progression of Diabetic reduction in progression of Diabetic retinopathy. 47% reduction in Proliferative retinopathy. 47% reduction in Proliferative Diabetic Retinopathy and severe NonDiabetic Retinopathy and severe Non--Proliferative Diabetic Retinopathy, 56% Proliferative Diabetic Retinopathy, 56% reduction in Pan Retinal Laser reduction in Pan Retinal Laser Photocoagulation, 23% reduction in Photocoagulation, 23% reduction in macular edema, with a mean followmacular edema, with a mean follow--up of up of 6.5 years.6.5 years.

United Kingdom Prospective Diabetes United Kingdom Prospective Diabetes Study (UKPDS): 1977Study (UKPDS): 1977--19991999
4209 Patients: 4209 Patients:
–– Cohort 1: Newly Diagnosed type 2 Cohort 1: Newly Diagnosed type 2 Diabetes Mellitus with no diabetic Diabetes Mellitus with no diabetic retinopathyretinopathy
–– Cohort 2: Newly Diagnosed type 2 Cohort 2: Newly Diagnosed type 2 Diabetes Mellitus with mild diabetic Diabetes Mellitus with mild diabetic retinopathyretinopathy

United Kingdom Prospective Diabetes United Kingdom Prospective Diabetes Study (UKPDS): 1977Study (UKPDS): 1977--19991999
Study questions:Study questions:
–– Will intensive control of blood glucose Will intensive control of blood glucose with type 2 diabetes reduce the risk of with type 2 diabetes reduce the risk of retinopathy progression?retinopathy progression?
–– Will intensive control of blood pressure Will intensive control of blood pressure in patients with type 2 diabetes reduce in patients with type 2 diabetes reduce the risk of retinopathy progression?the risk of retinopathy progression?

UKPDS: 1977UKPDS: 1977--19991999Patients randomized to conventional Patients randomized to conventional or intensive treatment groupsor intensive treatment groups
Conventional treatmentConventional treatment––Diet control followed by Diet control followed by sulphonylureasulphonylurea, ,
insulin, insulin, metforminmetforminIntensive treatmentIntensive treatment
––SulphonylureaSulphonylurea, Insulin, or if overweight , Insulin, or if overweight MetforminMetformin

UKPDS Conclusions:UKPDS Conclusions:
Intensive blood glucose control slowed Intensive blood glucose control slowed progression of retinopathy with average progression of retinopathy with average followfollow--up of 10 years.up of 10 years.–– 27% Reduction in clinically meaningful 27% Reduction in clinically meaningful
retinopathy retinopathy –– 29% Reduction in need for Laser29% Reduction in need for Laser–– 23% Reduction in vitreous hemorrhage23% Reduction in vitreous hemorrhage–– 16% Reduction in Legal Blindness16% Reduction in Legal Blindness

UKPDS Conclusions:UKPDS Conclusions:
Intensive blood pressure control Intensive blood pressure control independently slowed progression of independently slowed progression of retinopathy and reduced the risk of other retinopathy and reduced the risk of other microvascularmicrovascular complications of diabetes. complications of diabetes. No difference was found between No difference was found between AngiotensinAngiotensin Converting Enzyme inhibitors Converting Enzyme inhibitors and Beta blockers. and Beta blockers.


Diabetic Macular EdemaDiabetic Macular Edema
Standard Care: Focal Laser Standard Care: Focal Laser TreatmentTreatment


Early Treatment Diabetic Early Treatment Diabetic Retinopathy Study Retinopathy Study
(ETDRS): 1979(ETDRS): 1979--19901990Eligible patients:Eligible patients:Diabetic patients with VA Diabetic patients with VA >> 20/400 with mild to 20/400 with mild to severe nonsevere non--proliferative diabetic retinopathy and/or proliferative diabetic retinopathy and/or non highnon high--risk proliferative diabetic retinopathy risk proliferative diabetic retinopathy ++macular edema.macular edema.
Study questions:Study questions:–– Is focal laser treatment effective in treating diabetic Is focal laser treatment effective in treating diabetic
macular edema?macular edema?–– Is pan retinal laser photocoagulation effective for slowing Is pan retinal laser photocoagulation effective for slowing
the progression of diabetic retinopathy?the progression of diabetic retinopathy?

ETDRS: 1979ETDRS: 1979--19901990
3711 patients3711 patients
–– One eye of each patient assigned to One eye of each patient assigned to early photocoagulation and the other to early photocoagulation and the other to close monitoring.close monitoring.

ETDRS: 1979ETDRS: 1979--19901990Defined Clinically Significant Macular Edema as Defined Clinically Significant Macular Edema as any one of the following:any one of the following:–– Retinal edema at or within 500 microns of the Retinal edema at or within 500 microns of the
center of the maculacenter of the macula–– Hard exudates at or within 500 microns of the Hard exudates at or within 500 microns of the
center if associated with thickening of adjacent center if associated with thickening of adjacent retinaretina
–– A zone of thickening larger than 1 disc area if A zone of thickening larger than 1 disc area if located within 1 disc diameter of the center of located within 1 disc diameter of the center of the maculathe macula



ETDRS Conclusions: Macular ETDRS Conclusions: Macular EdemaEdema
Focal photocoagulation for diabetic Focal photocoagulation for diabetic macular edema reduced the risk of macular edema reduced the risk of moderate vision loss by moderate vision loss by >> 50% and 50% and increased the chance of small increased the chance of small improvement in visual acuity and reduced improvement in visual acuity and reduced retinal thickening. retinal thickening.

ETDRSETDRS
Defined Mild NonDefined Mild Non--Proliferative Diabetic Proliferative Diabetic Retinopathy:Retinopathy:
At least one At least one microaneurysmmicroaneurysm

ETDRS: Moderate Diabetic ETDRS: Moderate Diabetic RetinopathyRetinopathy

ETDRSETDRS
Defined Severe NonDefined Severe Non--Proliferative Diabetic Proliferative Diabetic Retinopathy as any one of the followingRetinopathy as any one of the following
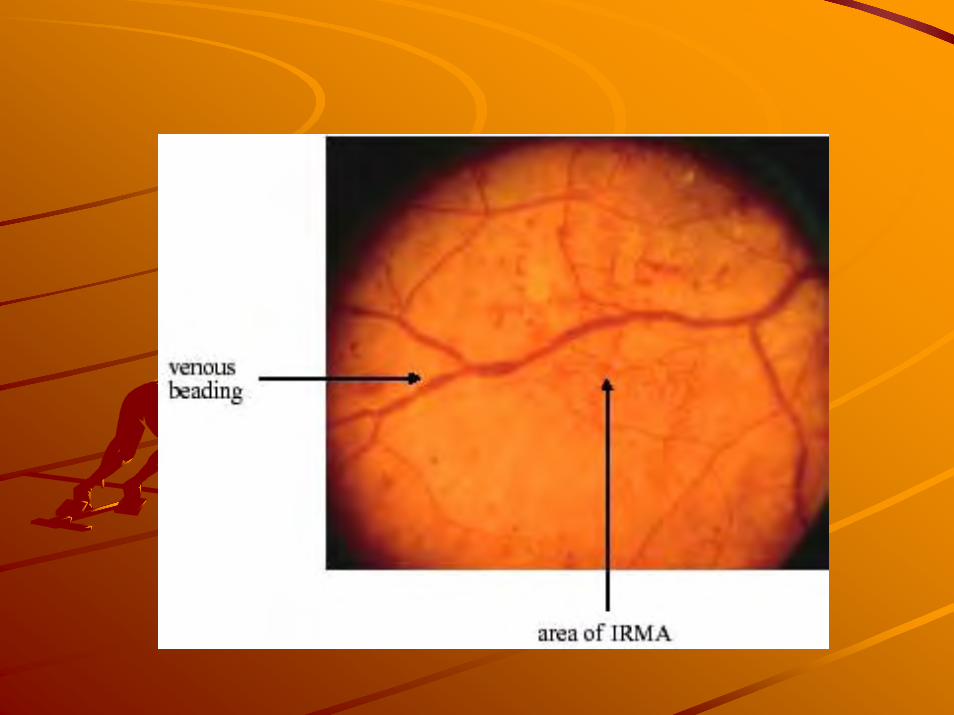
4 quadrants of diffuse 4 quadrants of diffuse intraretinalintraretinalhemorrhages and hemorrhages and microaneurysmsmicroaneurysms2 quadrants of venous beading2 quadrants of venous beading1 quadrant of 1 quadrant of intraretinalintraretinalmicrovascularmicrovascular abnormalitiesabnormalities


ETDRSETDRS
Defined Very Severe NonDefined Very Severe Non--Proliferative Proliferative Diabetic Retinopathy as any two of the Diabetic Retinopathy as any two of the followingfollowing
4 quadrants of diffuse 4 quadrants of diffuse intraretinalintraretinalhemorrhages and hemorrhages and microaneurysmsmicroaneurysms2 quadrants of venous beading2 quadrants of venous beading1 quadrant of 1 quadrant of intraretinalintraretinalmicrovascularmicrovascular abnormalitiesabnormalities

ETDRSETDRS
Defined Proliferative Diabetic Retinopathy Defined Proliferative Diabetic Retinopathy as any of the following:as any of the following:
Retinal NeovascularizationRetinal NeovascularizationDisc Neovascularization Disc Neovascularization Vitreous Vitreous HemorrahgeHemorrahgeFibrous Tissue ProliferationFibrous Tissue Proliferation




ETDRS ResultsETDRS Results
Progression to PDRProgression to PDR–– Severe NPDRSevere NPDR had a 15% chance of had a 15% chance of
progression to highprogression to high--risk PDR within 1 risk PDR within 1 year and 60% progression in 5 years.year and 60% progression in 5 years.
–– Very Severe NPDRVery Severe NPDR (any 2 criteria for (any 2 criteria for severe NPDR) had a 45% chance of severe NPDR) had a 45% chance of progression to highprogression to high--risk PDR within 1 risk PDR within 1 year and 75% progression in 5 years. year and 75% progression in 5 years.

ETDRS Conclusion: Early Pan ETDRS Conclusion: Early Pan Retinal Laser PhotocoagulationRetinal Laser Photocoagulation
Early Pan Retinal Laser Photocoagulation Early Pan Retinal Laser Photocoagulation is not indicated for mild to moderate Nonis not indicated for mild to moderate Non--Proliferative Diabetic Retinopathy, but Proliferative Diabetic Retinopathy, but should be considered for those with severe should be considered for those with severe or very severe Nonor very severe Non--Proliferative Diabetic Proliferative Diabetic Retinopathy. Retinopathy.
Pan Retinal Laser Photocoagulation should Pan Retinal Laser Photocoagulation should be performed in eyes with highbe performed in eyes with high--risk risk characteristics of proliferative diabetic characteristics of proliferative diabetic retinopathy andretinopathy and

ETDRS: HighETDRS: High--Risk Proliferative Risk Proliferative Diabetic RetinopathyDiabetic Retinopathy
Any disc neovascularization with vitreous Any disc neovascularization with vitreous hemorrhagehemorrhage
>=1/3 disc area of disc neovascularization >=1/3 disc area of disc neovascularization with or without vitreous hemorrhagewith or without vitreous hemorrhage
>=1/2 disc area of retinal >=1/2 disc area of retinal neovascularization with vitreous neovascularization with vitreous hemorrhagehemorrhage
+ Pan Retinal Laser Photocoagulation+ Pan Retinal Laser Photocoagulation

ETDRSETDRS
Defined Severe NonDefined Severe Non--Proliferative Diabetic Proliferative Diabetic Retinopathy as any one of the followingRetinopathy as any one of the following
4 quadrants of diffuse 4 quadrants of diffuse intraretinalintraretinalhemorrhages and hemorrhages and microaneurysmsmicroaneurysms2 quadrants of venous beading2 quadrants of venous beading1 quadrant of 1 quadrant of intraretinalintraretinalmicrovascularmicrovascular abnormalitiesabnormalities
+/+/-- Pan Retinal Laser PhotocoagulationPan Retinal Laser Photocoagulation

ETDRSETDRSDefined Very Severe NonDefined Very Severe Non--Proliferative Proliferative Diabetic Retinopathy as any two of the Diabetic Retinopathy as any two of the followingfollowing
4 quadrants of diffuse 4 quadrants of diffuse intraretinalintraretinalhemorrhages and hemorrhages and microaneurysmsmicroaneurysms2 quadrants of venous beading2 quadrants of venous beading1 quadrant of 1 quadrant of intraretinalintraretinalmicrovascularmicrovascular abnormalitiesabnormalities
+/+/-- Pan Retinal Laser PhotocoagulationPan Retinal Laser Photocoagulation

PAN RETINAL Laser PAN RETINAL Laser PHOTOCOAGULATIONPHOTOCOAGULATION
–– 1000 to 3000 burns1000 to 3000 burns–– Outpatient procedureOutpatient procedure–– 1 to 3 sessions1 to 3 sessions–– Standard Treatment for Standard Treatment for
Proliferative Diabetic RetinopathyProliferative Diabetic Retinopathy




Diabetic Retinopathy Study (DRS): Diabetic Retinopathy Study (DRS): 19711971--19751975
First multiFirst multi--centered, randomized, clinical centered, randomized, clinical trial in Ophthalmology, and provided trial in Ophthalmology, and provided
evidence for treatment of proliferative evidence for treatment of proliferative diabetic retinopathy with pan retinal diabetic retinopathy with pan retinal
laser photocoagulation.laser photocoagulation.

Diabetic Retinopathy StudyDiabetic Retinopathy Study
EligibilityEligibility–– Proliferative diabetic retinopathy or Proliferative diabetic retinopathy or
bilateral severe nonproliferative diabetic bilateral severe nonproliferative diabetic retinopathy with visual acuity retinopathy with visual acuity >> 20/100 20/100 in each eye.in each eye.
Study questionStudy question–– Is photocoagulation (argon or xenon Is photocoagulation (argon or xenon
arc) effective for treating proliferative arc) effective for treating proliferative diabetic retinopathy?diabetic retinopathy?

Diabetic Retinopathy Study: Diabetic Retinopathy Study: 19711971--19751975
EligibilityEligibility–– Proliferative diabetic retinopathy or Proliferative diabetic retinopathy or
bilateral severe nonproliferative diabetic bilateral severe nonproliferative diabetic retinopathy with visual acuity retinopathy with visual acuity >> 20/100 20/100 in each eye.in each eye.
Study questionStudy question–– Is photocoagulation (argon or xenon Is photocoagulation (argon or xenon
arc) effective for treating diabetic arc) effective for treating diabetic retinopathy?retinopathy?

DRSDRS
Design features Design features –– 1742 patients1742 patients–– One eye of each patient was assigned to One eye of each patient was assigned to
randomly to photocoagulation (scatter for new randomly to photocoagulation (scatter for new vessels), and focal (for macular edema). vessels), and focal (for macular edema).
–– Other eye assigned to monitoring without Other eye assigned to monitoring without laser.laser.
–– Eye assigned to treatment was randomly given Eye assigned to treatment was randomly given argon laser or xenon arc photocoagulation.argon laser or xenon arc photocoagulation.

DRS ResultsDRS Results
50% or greater reduction in the rates 50% or greater reduction in the rates of severe vision loss in eyes treated of severe vision loss in eyes treated with Pan Retinal Laser with Pan Retinal Laser Photocoagulation compared to Photocoagulation compared to untreated control eyes over 5 years of untreated control eyes over 5 years of followfollow--upup

VITRECTOMYVITRECTOMY
To remove vitreous To remove vitreous hemorrhagehemorrhageTo treat or prevent To treat or prevent retinal detachmentretinal detachment



Diabetic Retinopathy Vitrectomy Study Diabetic Retinopathy Vitrectomy Study (DRVS): 1979(DRVS): 1979--1990, 1990,
Group 1: Recent severe vitreous Group 1: Recent severe vitreous hemorrhage (within 5 months) from hemorrhage (within 5 months) from PDR with VA PDR with VA << 5/200, macula 5/200, macula attached. attached. Group 2: Advanced very severe PDR Group 2: Advanced very severe PDR VA VA >> 10/200 with extensive 10/200 with extensive neovascular or neovascular or fibrovascularfibrovascularproliferations, macula attached. proliferations, macula attached.
Diabetic Retinopathy Vitrectomy Study Diabetic Retinopathy Vitrectomy Study (DRVS): 1979(DRVS): 1979--19901990
Study questionsStudy questions–– What is the benefit of early (1What is the benefit of early (1--6 months 6 months
after onset of vitreous hemorrhage) after onset of vitreous hemorrhage) versus late (at 1 year) vitrectomy in versus late (at 1 year) vitrectomy in eyes with severe vitreous hemorrhage eyes with severe vitreous hemorrhage and visual loss.and visual loss.
–– What is the role of vitrectomy in What is the role of vitrectomy in managing eyes with very severe PDR?managing eyes with very severe PDR?

DRVS ResultsDRVS Results
Group 1 (617 Eyes): Recent severe Group 1 (617 Eyes): Recent severe vitreous hemorrhage vitreous hemorrhage –– Chance of visual acuity Chance of visual acuity >> 10/20 10/20
increased by early vitrectomy in increased by early vitrectomy in patients with type 1 diabetes, younger patients with type 1 diabetes, younger and had more severe proliferative and had more severe proliferative diabetic retinopathy.diabetic retinopathy.
Group 2 (370 Eyes): Very severe Group 2 (370 Eyes): Very severe PDR with useful vision group PDR with useful vision group –– Chance of visual acuity Chance of visual acuity >> 10/20 10/20
increased by early vitrectomy only in increased by early vitrectomy only in eyes with very severe new vessels.eyes with very severe new vessels.
DRVSDRVSAdvances in vitreoretinal surgical techniques Advances in vitreoretinal surgical techniques have changed some of the recommendations of have changed some of the recommendations of the DRVS.the DRVS.
–– Patients with preexisting complete PRP with Patients with preexisting complete PRP with vitreous hemorrhage can have a longer vitreous hemorrhage can have a longer observation period.observation period.
–– Patients who have not had prior PRP or incomplete Patients who have not had prior PRP or incomplete PRP should have early intervention if vitreous PRP should have early intervention if vitreous hemorrhage is secondary to PDR regardless of the hemorrhage is secondary to PDR regardless of the type 1 or 2 diabetes.type 1 or 2 diabetes.

The Diabetic Retinopathy Clinical The Diabetic Retinopathy Clinical Research NetworkResearch Network
A Randomized Trial Comparing A Randomized Trial Comparing Intravitreal Intravitreal Triamcinolone AcetonideTriamcinolone Acetonide
to Focal/Grid Photocoagulationto Focal/Grid Photocoagulationfor Diabetic Macular Edemafor Diabetic Macular Edema
Sponsored by the National Eye Institute, Sponsored by the National Eye Institute, National Institutes of Health, U.S. Department of Health and HumNational Institutes of Health, U.S. Department of Health and Human an
Services.Services.
60

61
Primary Study ObjectivePrimary Study Objective
To compare the efficacy and safety of preservative-free IVT (1 mg or 4 mg) with focal/grid laser

62
Study DesignStudy Design
1 mg IVT
Focal/Grid Laser
4 mg IVT
Multicenter, randomized clinical trial
Major Eligibility Criteria Assessed:Major Eligibility Criteria Assessed:
•>18 years old•Type 1 or type 2 diabetes•Center-involved DME (with OCT CSF >250 µm)•VA letter score 73 to 24 (20/40 to 20/320)
Eligible eyes randomizedSubjects with 2 study eyes assigned alternative treatment in 2nd eye

Laser4 mg
Median Visual Acuity inLaser and 4 mg IVT Treated Eyes
Median Visual Acuity inLaser and 4 mg IVT Treated Eyes
63Months
VisualAcuityScore
20/80
20/50
20/32
20/40
20/63
0 12 16 20 244 8

64
Median Central Subfield Thickness Median Central Subfield Thickness in Laser and 4mg Treated Eyesin Laser and 4mg Treated Eyes
200
250
300
350
400
450
0 4 8 12 16 20 24
Laser
4 mg
Months
Central Subfield
Thickness(microns)

65
DiscussionDiscussionVisual acuity benefit in 4 mg IVT group at 4 months consistent with published case seriesNo visual acuity differences by 1 yearGreater visual acuity benefit and fewer side effects (IOP and cataract) in laser group at 2 yearsOCT results mirrored visual acuity resultsLaser or IVT likely improves VA over 2 years compared with expected untreated course

66
Consistency in SubgroupsConsistency in Subgroups
No clear benefit of intravitreal triamcinolone over laser: • With or without prior laser• Across baseline OCT thickness• Across baseline visual acuities

67
Importance of Focal/Grid Importance of Focal/Grid PhotocoagulationPhotocoagulation
Results re-affirm importance of laser in management of DMEIt was widely believed that the ETDRS showed laser reduces vision loss, but did not improve VA . . . however . . . majority of eyes in ETDRS were better than 20/40 (no room for substantial improvement)

68
Future Studies NeededFuture Studies Needed
Determine whether combining focal/grid and intravitreal triamcinolone results in better outcomes for DMEDetermine whether other treatments (e.g., anti-VEGF), with or without focal/grid, results in better outcomes for DME


LucentisLucentisTMTM
(ranibizumab, rhuFab V2)(ranibizumab, rhuFab V2)
rhuFab
Chen, et al. Journal of Molecular Biology, Vol. 293, No. 4( 865-881) Nov 1999
Kim …Ferrara Nature 362, 841-844.(1993)
HumanizedAntibody
Monoclonal Antibody
Human
Monoclonal AntibodyMouse
Presta…Ferrara Cancer Res. 47:
4593-4599.1997
Monoclonal AntibodyA.4.6.1
Humanization
V1 -> V2Improved VersionPreparing Fab
Chen, et al. Journal of Molecular Biology, Vol. 293, No. 4( 865-881) Nov 1999
AvastinTM
LucentisTM

Study SummaryStudy SummaryTrialsTrials TwoTwo Phase III studies , doublePhase III studies , double--masked, masked,
three randomized arms in each studythree randomized arms in each studyStudy 1: RIDE Study 1: RIDE Study 2: RISE Study 2: RISE
Duration:Duration: 36 Months for safety36 Months for safety24 Months for primary efficacy endpoint 24 Months for primary efficacy endpoint
PopulationPopulation CSMECSME--CI secondary to diabetes mellitus CI secondary to diabetes mellitus Type I/Type IIType I/Type II
Treatment Treatment assignmentassignment
Arm 1: 0.5 mg ranibisumab (N 122)Arm 1: 0.5 mg ranibisumab (N 122)Arm 2: 0.3 mg ranibizumab (N 122)Arm 2: 0.3 mg ranibizumab (N 122)Arm 3: Sham injection (N 122)Arm 3: Sham injection (N 122)
Sample sizeSample size 366 per trial366 per trial

LaserLaser--RanibizumabRanibizumab--Triamcinolone Triamcinolone for DME Studyfor DME Study
Diabetic Clinical Research Diabetic Clinical Research Network t Protocol INetwork t Protocol I

Treatment GroupsTreatment Groups
Randomization to one of the following 4 groups:Randomization to one of the following 4 groups:Group A: Group A: Sham injection + focal laserSham injection + focal laser
Group B: 0.5 mg injection of intravitreal Group B: 0.5 mg injection of intravitreal Ranibizumab + focal laserRanibizumab + focal laser
Group C: 0.5 mg injection of intravitreal Group C: 0.5 mg injection of intravitreal Ranibizumab + deferred focal laserRanibizumab + deferred focal laser
Group D: 4 mg injection of intravitreal Group D: 4 mg injection of intravitreal Triamcinolone + focal laserTriamcinolone + focal laser 7
3
Intravitreal Ranibizumab or Intravitreal Ranibizumab or Triamcinolone Acetonide as Triamcinolone Acetonide as
Adjunctive Treatment to Panretinal Adjunctive Treatment to Panretinal Photocoagulation for Proliferative Photocoagulation for Proliferative Diabetic Retinopathy (Diabetic Diabetic Retinopathy (Diabetic Retinopathy Research Network Retinopathy Research Network
Protocol J)Protocol J)

Protocol J: Treatment Groups Protocol J: Treatment Groups All groups receive focal photocoagulation All groups receive focal photocoagulation
and panretinal photocoagulation.and panretinal photocoagulation.
Randomization to one of the following 3 Randomization to one of the following 3 groups:groups:Intravitreal injection of 0.5 mg Intravitreal injection of 0.5 mg ranibizumabranibizumab (Lucentis(Lucentis™™) at baseline and 4 ) at baseline and 4 weeksweeksIntravitreal injection of 4 mg Intravitreal injection of 4 mg triamcinolone acetonidetriamcinolone acetonide at baseline and at baseline and sham injection at 4 weekssham injection at 4 weeksShamSham injection at baseline and 4 weeksinjection at baseline and 4 weeks

Diabetic RetinopathyDiabetic RetinopathyReview indications and results of Review indications and results of focal laser treatment for diabetic focal laser treatment for diabetic macular edemamacular edemaReview indications and results of pan Review indications and results of pan retinal laser photocoagulation for retinal laser photocoagulation for severe nonsevere non--proliferative diabetic proliferative diabetic retinopathy and for proliferative retinopathy and for proliferative diabetic retinopathydiabetic retinopathy
Diabetic Diabetic RetinoapthyRetinoapthyReview the results of monoReview the results of mono--therapy therapy comparing focal laser treatment and comparing focal laser treatment and intravitreal triamcinoloneintravitreal triamcinolone
Discussions on new clinical trialsDiscussions on new clinical trials

Questions?Questions?

DIABETIC RETINOPATHY ANDDIABETIC RETINOPATHY ANDCADIOVACULAR DISEASECADIOVACULAR DISEASE
PDR risk indicator for MI, stroke, PDR risk indicator for MI, stroke, amputationamputationPDR elevates risk of developing PDR elevates risk of developing diabetic nephropathydiabetic nephropathyElevated serum lipid levels Elevated serum lipid levels associated with retinal hard associated with retinal hard exudatesexudates

PREGNANCY AND PREGNANCY AND DIABETIC RETINOPATHYDIABETIC RETINOPATHY
Discuss risks before Discuss risks before conception conception
••Retinopathy may worsenRetinopathy may worsen
••Regular ophthalmologic exam Regular ophthalmologic exam advisedadvised

SCREENING GUIDELINES:SCREENING GUIDELINES:DIABETES Dx DIABETES Dx < AGE 30< AGE 30
Annual ophthalmologic exams Annual ophthalmologic exams starting 5 years after Dxstarting 5 years after DxOphthalmoscopy by PCP for Ophthalmoscopy by PCP for signs signs at other intervalsat other intervals


SCREENING GUIDELINES:SCREENING GUIDELINES:DIABETES Dx DIABETES Dx > AGE 30> AGE 30
Annual ophthalmologic exams Annual ophthalmologic exams starting at time of Dxstarting at time of DxOphthalmoscopy by PCP for Ophthalmoscopy by PCP for signs at other intervalssigns at other intervals

SCREENING GUIDELINES:SCREENING GUIDELINES:CONCEPTION AND PREGNANCYCONCEPTION AND PREGNANCY
Ophthalmologic exam before Ophthalmologic exam before conceptionconceptionOphthalmologic exam at 3Ophthalmologic exam at 3--month intervals, beginning in month intervals, beginning in first trimesterfirst trimester

Ophthalmologic exam followOphthalmologic exam follow--up schedule determined by up schedule determined by ophthalmologist and primary ophthalmologist and primary care physician.care physician.

CONCLUSIONCONCLUSIONEarly treatment may prevent Early treatment may prevent blindnessblindnessImproved screening can Improved screening can ensure early treatmentensure early treatment

DIABETIC RETINOPATHY:DIABETIC RETINOPATHY:A PUBLIC HEALTH ISSUEA PUBLIC HEALTH ISSUEPrevalence may rise as % of Prevalence may rise as % of aged in population risesaged in population risesScreening is a costScreening is a cost--effective effective way to reduce the incidence of way to reduce the incidence of blindnessblindness
Diabetic Retinopathy Vitrectomy Study Diabetic Retinopathy Vitrectomy Study (DRVS)(DRVS)
Eligible patients (2 groups)Eligible patients (2 groups)–– Recent severe vitreous hemorrhage (within 5 months) Recent severe vitreous hemorrhage (within 5 months)
from PDR with VA from PDR with VA << 5/200, macula attached. 5/200, macula attached.
–– Advanced very severe PDR VA Advanced very severe PDR VA >> 10/200 with extensive 10/200 with extensive neovascular or neovascular or fibrovascularfibrovascular proliferations, macula proliferations, macula attached. attached.
Study questionsStudy questions–– What is the benefit of early (1What is the benefit of early (1--6 months after onset of 6 months after onset of
vitreous hemorrhage) versus late (at 1 year) vitrectomy vitreous hemorrhage) versus late (at 1 year) vitrectomy in eyes with severe vitreous hemorrhage and visual loss.in eyes with severe vitreous hemorrhage and visual loss.
–– What is the role of vitrectomy in managing eyes with What is the role of vitrectomy in managing eyes with very severe PDR?very severe PDR?

DRVSDRVS
Study DesignStudy Design–– Group with severe vitreous hemorrhage from Group with severe vitreous hemorrhage from
PDR (617 eyes) PDR (617 eyes) Eligible eyes assigned randomly to early vitrectomy Eligible eyes assigned randomly to early vitrectomy or conventional management (vitrectomy if center of or conventional management (vitrectomy if center of macula detaches or if vitreous hemorrhage persists macula detaches or if vitreous hemorrhage persists for 1 year; photocoagulation if possible)for 1 year; photocoagulation if possible)
–– Group with severe PDR and useful vision (370 Group with severe PDR and useful vision (370 eyes)eyes)
Eligible eyes assigned randomly to early vitrectomy Eligible eyes assigned randomly to early vitrectomy or conventional management (vitrectomy if center of or conventional management (vitrectomy if center of macula detaches or if vitreous hemorrhage persists macula detaches or if vitreous hemorrhage persists for 6 months)for 6 months)

DRVS ResultsDRVS Results
Recent severe vitreous hemorrhage Recent severe vitreous hemorrhage groupgroup–– Chance of visual acuity Chance of visual acuity >> 10/20 10/20
increased by early vitrectomy in increased by early vitrectomy in patients with type 1 diabetes, younger patients with type 1 diabetes, younger and had more severe proliferative and had more severe proliferative diabetic retinopathy.diabetic retinopathy.
Very severe PDR with useful vision Very severe PDR with useful vision group group –– Chance of visual acuity Chance of visual acuity >> 10/20 10/20
increased by early vitrectomy only in increased by early vitrectomy only in

DRVSDRVSAdvances in vitreoretinal surgical techniques Advances in vitreoretinal surgical techniques have changed some of the recommendations of have changed some of the recommendations of the DRVS.the DRVS.
–– Patients with preexisting complete PRP with Patients with preexisting complete PRP with vitreous hemorrhage can have a longer vitreous hemorrhage can have a longer observation period.observation period.
–– Patients who have not had prior PRP or incomplete Patients who have not had prior PRP or incomplete PRP should have early intervention if vitreous PRP should have early intervention if vitreous hemorrhage is secondary to PDR regardless of the hemorrhage is secondary to PDR regardless of the type 1 or 2 diabetes.type 1 or 2 diabetes.

EDUCATION ISSUES FOR EDUCATION ISSUES FOR PHYSICIANS AND PATIENTSPHYSICIANS AND PATIENTS
Diabetic eye complicationDiabetic eye complicationExamination schedulesExamination schedulesTreatment optionsTreatment optionsScreening guidelinesScreening guidelines

Research resultsResearch results↓↓
Improved screening and treatmentImproved screening and treatment↓↓
Continuing education programContinuing education program↓↓
Ophthalmologist and medical Ophthalmologist and medical communitycommunity

Primary care Primary care physicianphysician
++OptometristsOptometrists
++OphthalmologyOphthalmology
↓↓Effective screening Effective screening timely treatmenttimely treatment



DCCT ResultsDCCT Results
Intensive blood sugar control Intensive blood sugar control reduced risk of developing reduced risk of developing retinopathy by 76% and slowed retinopathy by 76% and slowed progression of retinopathy by 54%. progression of retinopathy by 54%.
Intensive blood sugar control also Intensive blood sugar control also reduced risk of neuropathy by 60% reduced risk of neuropathy by 60% and and albuminuriaalbuminuria by 54%by 54%



DIABETIC RETINOPATHY:DIABETIC RETINOPATHY:EFFECTIVE SCREENINGEFFECTIVE SCREENING
Depends on retinal Depends on retinal examinationexamination
$62 million potential saving $62 million potential saving annuallyannually
DIABETIC MACULAR EDEMA:DIABETIC MACULAR EDEMA:PREVALENCEPREVALENCE
Diabetes Dx Diabetes Dx ≤≤ 5 yrs = 5%5 yrs = 5%Diabetes Dx Diabetes Dx ≥≥ 5 yrs = 15%5 yrs = 15%

Proliferative Diabetic Proliferative Diabetic Retinopathy: PREVALENCERetinopathy: PREVALENCE
Age of Diagnosis Age of Diagnosis
Duration of Diabetes MellitusDuration of Diabetes Mellitus

%PATIENT WITH PDR:%PATIENT WITH PDR:INSULIN USERS DxINSULIN USERS Dx<AGE 30<AGE 30
Years After DiagnosisYears After Diagnosis %%
5 05 01515 25 25 2020 5555

%PATIENT WITH PDR:%PATIENT WITH PDR:INSULIN USERS DxINSULIN USERS Dx>AGE 30>AGE 30
Yrs After DxYrs After Dx %%
20 20%20 20%

DRVS: 1979DRVS: 1979--19901990
Group 1: severe vitreous hemorrhage from PDR Group 1: severe vitreous hemorrhage from PDR (617 eyes) (617 eyes) –– Eligible eyes assigned randomly to early vitrectomy or Eligible eyes assigned randomly to early vitrectomy or
conventional management (vitrectomy if center of conventional management (vitrectomy if center of macula detaches or if vitreous hemorrhage persists for 1 macula detaches or if vitreous hemorrhage persists for 1 year; photocoagulation if year; photocoagulation if possible)spossible)s
Group 2: severe PDR and useful vision (370 Group 2: severe PDR and useful vision (370 eyes)eyes)–– Eligible eyes assigned randomly to early vitrectomy or Eligible eyes assigned randomly to early vitrectomy or
conventional management (vitrectomy if center of conventional management (vitrectomy if center of macula detaches or if vitreous hemorrhage persists for 6 macula detaches or if vitreous hemorrhage persists for 6 months)months)

Inclusion CriteriaInclusion CriteriaDecrease in vision is due to diabetic Decrease in vision is due to diabetic macular edema and not due to other macular edema and not due to other causescauses
Patient is able (in the opinion of the Patient is able (in the opinion of the investigator) and willing to return to investigator) and willing to return to all visits and assessments.all visits and assessments.