malaria programme in afghanistan -...
TRANSCRIPT

1
Malaria Programme
Review
in
Afghanistan
________________________
2dt Draft
6 December 2016

2
CCOONNTTEENNTTSS
AAcckknnoowwlleeddggeemmeennttss
AAbbbbrreevviiaattiioonnss
KKeeyy FFiinnddiinnggss aanndd AAccttiioonn PPooiinnttss 99
IInnttrroodduuccttiioonn 1177
Rationale
Objectives
Thematic Areas Reviewed
Expected Outputs, Outcomes and Timelines
Review Process
Part 1: 20
Geography and Climate
Population and Demography
Political Structure and Administration
Part 2: 23
Health Profile and Policies
Overview of Health Services
History of Malaria Control
National Malaria and Leishmaniasis Control Programme
National Strategic Plan on Malaria Control and
Elimination & Malaria Elimination Plan, 2013-2017
Part 3: 27
Malaria Epidemiology
Recent Trends and Present Situation
Conclusions
Recommendations
Part 4: (Programme Performance by Thematic Areas) 37
4.1. Case Management 37
Current Situation & Existing Challenges
Conclusions

3
Recommendations
4.2. Vector Control and Entomological Surveillance 42
Current Situation & Existing Challenges
Conclusions
Recommendations
4.3. Malaria Surveillance 53
Current Situation & Existing Challenges
Conclusions
Recommendations
4.4. Epidemic Preparedness and Response (EPR) 59
Current Situation & Existing Challenges
Conclusions
Recommendations
4.5. Programme Management 62
Current Situation & Existing Challenges
Conclusions
Recommendations
4.6. Procurement Supply Management (PSM) 66
Current Situation & Existing Challenges
Conclusions
Recommendations
4.7. Monitoring and Evaluation (M&E) 68
Current Situation & Existing Challenges
Conclusions
Recommendations
4.8. Advocacy, Information, IEC and Community Mobilization 71
Current Situation & Existing Challenges
Conclusions
Recommendations
4.9. Operational Research 73
Current Situation & Existing Challenges
Conclusions

4
Recommendations
Part 5: 76
Main Conclusions
Main Recommendations (to be considered in the short and medium run)
The Way Forward
The Way Forward 89
References 90
Annexes 93

5
ACKNOWLEDGEMENTS
The Malaria Programme Review carried out in Afghanistan would not have been possible without
the guidance and support of national health authorities. Since it is impossible to mention them
individually, we would like to thank in this way all those who have been committed to and involved
in malaria control and elimination in the country, particularly H.E. Dr Ferozudin Feroz, the
Minister of Health, Ministry of Public Health; Dr Ahmad Jan Naeem, Deputy Minister of Health,
Ministry of Public Health; Dr Naimullah Safi; Dr Mohammad Sami Nahzat; Dr Hamida Hamid;
Dr Naeem Habib and others.
We are indebted to all international experts and national consultants - Dr Mikhail Ejov (Team
Review Leader, Epidemiology/Recent Trends/Present Situation/Surveillance/M&E/EPR), Dr
Abul Faiz (Case Management); Dr Ahmad Ali Enayati (Vector Control/Entomological
Surveillance); Dr Ahmad Raeisi (Epidemiology/ Operational Research); Dr Delwar Hussain
(Programme Management/Advocacy, IEC, Community Mobilization/PSM); Dr M. Nader (Vector
Control); Dr M. Asif Alokozai (Operational Research/M&E); Dr A. Aziz Rasoli
(Epidemiology/EPR/Surveillance); Dr Mirwais Mansoor (Case Management); Dr Mirza Khan
Basharmal (Programme Management/PSM) and Dr Sohrab Safi (Advocacy, IEC & Community
Mobilization) recruited by UNDP/GF/Afghanistan - who have contributed their time and expertise
to make this review successful.
We are grateful to UNDP/GF staff in Afghanistan (Dr Alim Atarud, Ms Madelena Monoja, Dr
Ahmad Walid Sediqi, Mr Sardar Mohammad Asif, Mr Rasool Zahedi, Mr Nazar Muhammad
Shinwari and others) for their overall guidance and coordination as well as indispensable funding
provided without which this Review would not have been possible.
We would equally like to extend our special thanks to WHO staff in Afghanistan (Dr Rick
Peeperkorn and Dr Supriya Warusavithana) and EMRO (Dr Atta Hoda and Dr Ghasem Zamani)
for their valuable advice and support, which is acknowledged with gratitude.

6
ABBREVIATIONS
ABER Annual Blood Examination Rate
ACT Artemisinin combination therapy
ACD Active Case Detection
ANDS Afghanistan National Development Strategy
API Annual Parasite Incidence
APfI Annual P. falciparum Incidence
APvI Annual P. vivax Incidence
ANDS Afghanistan National Development Strategy
AS Artesunate
BCC Behaviour Change Communication
BHCs Basic Health Centers
BPHS Basic Package of Health Services
BRAC Bangladesh Rural Advancement Committee
BTi Bacillus thuringiensis israelensis
CBMM Community Based Management of Malaria
CCM Country Coordination Mechanism
CDC Communicable Diseases Control
CFR Case Fatality Ratio
CHCs Comprehensive Health Centres
CHSs Community Health Supervisors
CHWs Community Health Workers
CQ Chloroquine
DDT Dichlorodiphenyltrichloroethane
DEWS Disease Early Warning system
DHs District Hospitals
EQA External Quality assurance
EC European Commission
ELISA Enzyme-Linked Immunosorbent Assay
EMRO Eastern Mediterranean Regional Office
EPHS Essential Package of Hospital Services
EPR Epidemic Preparedness and Response
EDL Essential Drug List
EPHS Essential Package of Hospital Service
GCMU Grant Contract Management Unit
GIS Geographical Information System
GF Global Fund
GFATM Global Fund to fight AIDS, Tuberculosis and Malaria
G6PD Glucose-6-Phosphate Dehydrogenase deficiency
HSCs Health Sub-Centres
HPs Health Posts
HMIS Health Management Information System
HNI Health Net International
IEC Information Education and Communication

7
IPD In-Patient Department
IRS Indoor Residual Spraying
IVM Integrated Vector Management
IRM Insecticide Resistance Management
ITNs Insecticide Treated Nets
IV Intravenous injection
IM Intramuscular injection
KAP Knowledge Attitude practice
HPLC High Performance Liquid Chromatography
LLINs Long Lasting Insecticide Treated Nets
LTA Long Term Agreement
MNTs Mobile Health Teams
M&E Monitoring and Evaluation
MIS Malaria Indicator Survey
MoPH Ministry of Public Health
MPR Malaria Programme Review
NCDs Noncommunicable Diseases
NGOs Non-Governmental Organisations
NMLCP National Malaria and Leishmaniasis Control Programme
NMSP National Strategic Plan for Malaria Control and Elimination
MEP Malaria Elimination Plan
NTCC National Technical Coordination Committee
NTG National Treatment Guideline
NFM New Funding Module
PCR Polymerase Chain Reaction
PMLCP Provincial Malaria and Leishmaniasis Control Programme
PPR Parasite Prevalence Rate
PPHD Provincial Public Health Directorate
PR Principle Recipient
PSM Procurement Supply Management
PHs Provincial Hospitals
PQ Primaquine
RHs Regional Hospitals
RDT Rapid Diagnostic Test
QA Quality Assurance
QAS Quality Assurance System
OPD Out-Patient Department
QC Quality Control
SCM Severe and Complicated Malaria
SP Sulfadoxine-Pyrimethamine
SOPs Standard Operating Procedures
SPR Slide Positivity Rate
SWAP Sector Wide Approach
TPR Test Positivity Rate
TTT Technical Task Team

8
UNDP United Nations Development Programme
USAID United States Agency for International Development
VCNA Vector Control Needs Assessment
WB World Bank
WHO World Health Organization
WHOPES World Health Organization Pesticide Evaluation Scheme
WMR World Malaria Report
WMD World Malaria Day
UM Uncomplicated Malaria
9
KEY FINDINGS AND ACTION POINTS
Malaria Programme Review
The MPR was conducted by UNDP/GFATM, the NMLCP of the MoPH and WHO in November-
December 2016 to evaluate the performance of national malaria control programme and
recommend priority areas for revision of the existing national strategic plan which will be done in
2017. Moreover, this MPR was also an in-depth assessment of the GFATM NFM grant for malaria
control program in Afghanistan. The following thematic areas including (1) epidemiology, recent
trends and present situation; (2) case management; (3) vector control and entomological
surveillance; (4) malaria surveillance; (5) epidemic preparedness and response; (6) programme
management; procurement and supply management; (7) monitoring and evaluation; (8) advocacy,
IEC and community mobilization; and (9) operational research were reviewed.
Health Profile and Policies
Significant progress in Afghanistan’s health services over the last decade has translated into
substantial declines in infant, child and maternal mortality rates. However, many of Afghanistan’s
health indicators remain extremely worrisome. There is a high burden of communicable diseases,
which account for more than 60% of all outpatient visits and more than half of all deaths. Some
of the major challenges and constraints faced by the health sector include: inadequate financing
for many key programmes and heavy reliance on external sources of funding; insufficient and
inadequately trained health workers; lack of access to healthcare due to dispersed populations and
insecurity; quality-compromised services; constrained national capacities for health planning and
management, especially in the areas of governance, healthcare financing, human resource
development, monitoring, evaluation and analysis of the health situation at central and especially
at the provincial level.
Local Epidemiology
Malaria is still a major public health problem in Afghanistan. Referring to WMR 2015, 24% of
Afghan population lives in areas at high risk for malaria, 49% at medium risk and the remaining
27% live in areas with no risk or very low risk of malaria transmission. Malaria is a complex
disease and its distribution in Afghanistan varies largely from place to place, and is dependent
upon a variety of factors related to parasites, vectors and human populations under different
geographical, ecological and socio-economic conditions. Using a combination of available malaria
and environmental data, all districts in Afghanistan were classified into four main strata with high,
medium, low and very low risk of malaria transmission or its absence in malaria free areas.
At present, P. vivax malaria is the most prevalent species accounting for almost 95% of all
parasitologically confirmed cases, with less than 5% of total cases attributed to P. falciparum with
a decrease in its proportion over the past years. Malaria transmission is seasonal from June to
November. The P. falciparum peak is in August to October, a few months after the summer peak
of P. vivax. Many Plasmodium vivax infections relapse during the spring season and this may give
rise to a vivax peak around July Transmission of P. falciparum, at the edge of its geographical
range, is unstable, and can fluctuate markedly from year to year. The distribution of Anopheline
mosquitoes in Afghanistan varied by ecological zones, and includ An. stephensi, An. culicifacies,
An. fluviatilus, An. annularis, An. pulcherrimus, An. superpictus and An. hycranus. There is a
profound diversity in ethnic groups residing across the country. The genotypic study of the

10
Mediterranean variant of G6PD deficiency in males in nine provinces in Afghanistan confirms that
the 563C.T mutation reaches its highest frequencies in Pashtuns and Pashais (8.9%), with lower
prevalence in groups historically associated with northern provinces and countries to the north of
Afghanistan.
Recent trends and Present Situation
In some northern, western and southern provinces the number of malaria cases, particularly P.
falciparum has dropped significantly and these provinces became eligible for malaria elimination.
It is becoming evident that some provinces have already interrupted and other provinces could
interrupt transmission of P. falciparum malaria in the years ahead. However, in some eastern
provinces along the border with Pakistan, continuous outbreaks have caused a severe epidemic
malaria in 2014-2016. In 2015, more than 70% of reported confirmed cases were reported from 3
eastern provinces such as Nangarhar, Kunar and Laghman, and almost 90% of all confirmed P.
falciparum cases were registered in 5 provinces (Nangarhar, Laghman, Kunar, Khost and Paktika)
with 49 reported deaths due to malaria from Nangarhar and Kunar. Since 2013, the proportion of
malaria cases confirmed by RDTs and/or microscopy has substantially increased from 14.4% in
2013 to 28.2% in 2015. However, the majority (more than 70%) of reported malaria cases are still
diagnosed on clinical ground in 2015. Because of continuous improvement in access to
parasitological diagnosis across the country between 2013 and 2015, API increased from 1.79 to
3.82 cases per 1000 population at risk per year with the highest API of 27 cases reaching 42 cases
per 1000 population at risk reported in three eastern provinces of the country (Kunar, Laghmar
and Nangarhar).
Malaria control and elimination in Afghanistan is the responsibility of NMLCP in the CDC
Department of the General Directorate of Preventive Medicine in MoPH. The goal of National
Strategic Plan on Malaria Control and Elimination, 2013-2017 is to contribute to the improvement
of the health status in Afghanistan through the reduction of morbidity and mortality associated
with malaria with a vision to completely interrupt transmission of P. falciparum by 2020. NMLCP
has 34 PMLCP units operating in 34 endemic provinces. Key functions of them are to provide
coordination with NMLCP, facilitate capacity building of the health staff, monitoring and
evaluation of malaria activities like surveillance, diagnosis treatment etc. National malaria control
efforts are mainly supported by the external donors with major funding support from the GFATM.
The main conclusions that have been made for each thematic area and priority issues that should
be addressed immediately (2017) are listed below:
CASE MANAGEMENT
Conclusions
Parasitological confirmation of all clinically-suspected cases of malaria by RDT or
microscopy is not in place yet.
There is insufficient information from the private sector on diagnosis of malaria.
Lack of quality assurance for malaria diagnosis by microscopy and/or RDT at different
levels.

11
Treatment of cases (P. vivax, P. falciparum, management of severe and complicated
malaria, pre-referral treatment of severe and complicated cases) are not always done as per
existing national treatment protocol/drug policy.
Despite the radical treatment of vivax cases and provision of a single dose of primaquine
for P. falciparum malaria patients are recommended, this approach has to be put into
practice.
Lack of training on case management of different health care providers including the
private sector.
Recommendations
Wide scale deployment of RDTs through multiple public, private and community-based
channels and strengthening/setting up of existing/new laboratory facilities should be
actively promoted to reach universal coverage of case management including remote,
inaccessible, ‘security compromised’ and internally displaced populations.
Training on malaria diagnosis and treatment with updated training materials and SOPs
should be provided to different categories of health care providers at all public, private and
community-based health sector facilities.
National malaria treatment guidelines should be updated based on the new 2015 WHO
Guidelines for Treatment of Malaria.
EDL for treating malaria should be revisited and a minimum set of essential drugs is
required for areas where cases are drastically reduced to avoid medicine’s wastage and to
ensure that quality-assured efficacious antimalarial drugs provided in both public and
private sectors.
VECTOR CONTROL AND ENTOMOLOGICAL SURVEILLANCE
Conclusions
Distribution of LLINs is based on the official numbers of country’s population provided
by the National Statistics Services that is not always update, so that the number of LLINs
distributed is always behind the national target.
Malaria entomological data is not used along with epidemiological and HMIS data for the
decision making regarding malaria control and elimination.
Number of entomology staff in NMLCP and especially at provincial level is none or
minimal, and their training on vector control and entomological surveillance is inadequate.
A proper plan for entomological surveillance is not in place. As an important component
of entomological surveillance, insecticide susceptibility status of malaria vectors should
be conducted under rigorous standards to ensure the reliability of the results for decision
making.
Recommendations
National policy and funding for procurement and distribution of LLINs should be adequate
and sufficient to cover all population groups at risk of malaria within the country:
o A better estimate of the total populations at provincial, district and lower levels
should be made to calculate the sufficient quantities of LLINs to be procured and
distributed within each province. If the target is one LLIN for 2 people, the
benchmark of a maximum of two LLINs per household should be lifted.

12
o Timely procurement of LLINs should always be a priority so that distribution
can start well before transmission season.
o Distribution of LLINs should be coupled with locally appropriate and gender
sensitive IEC/BCC to ensure community participation and correct LLIN usage.
There is a desperate need for strengthening the entomological component of NMLCP at
central and provincial levels:
o The inventory of existing entomology staff and assessment for the staff needed and
relevant posts to be filled at each level should be made.
o The entomological capacity of NMLCP should be strengthened. Training should be
“task-oriented” and “problem-solving” and supplemented by regular supervision
and refresher training courses.
o A core NMLCP technical group on vector control with a good representation of
competent staff in medical entomology and vector control at provincial level should
be maintained or established to play a greater role in the decision-making process
on malaria control and elimination.
MALARIA SURVEILLANCE
Conclusions
Based on available malaria and environmental data and reflecting a risk of malaria, all
districts in Afghanistan were classified into four main strata with high, medium, low and
very low risk of malaria transmission or its absence in malaria free areas to provide
strategic guidance for planning anti-malaria interventions.
Routine malaria surveillance is presently conducted through HMIS, and malaria reporting
from BPHS and EPHS is integrated with HMIS. Malaria sentinel surveillance is currently
carried out through three types of sentinel sites to show malaria trend, to monitor drug
efficacy and to detect epidemics/outbreaks.
Recommendations
1. Based on the 2016 reported API as a primary criterion for selection and other criteria such
as the reported number of malaria cases per health facility; the reported ratio of P.
falciparum to P. vivax; determinants of local epidemiology and degree of development of
health system within a given province, the entire country should be sub-divided into three
Categories (1) where malaria is still widespread and the primary objective is to reduce the
remaining malaria burden further; (2) where malaria shows a focal distribution of
indigenous cases and which are eligible for malaria elimination and (3) where all reported
cases of malaria have an imported nature, and particular focus should be placed on
maintenance of the results achieved by prevention of re-establishing local malaria
transmission. NMLCP may request WHO to provide the necessary technical assistance in
relation to this task.
In the malaria elimination phase, malaria must be a notifiable disease, and every
symptomatic and asymptomatic infection should be detected and mandatory notified.
Surveillance activities should be enhanced so that every focus (village, or sub-village or
working site) with indigenous case(s) of malaria is targeted for action.
13
EPIDEMIC PREPAREDNESS AND RESPONSE (EPR)
Conclusions
At present, EPR is one of the strategic directions of the NMSP 2013-2017, and malaria
outbreaks are detected through functional DEWS which is covering the entire country.
However, the existing epidemic preparedness and response mechanism is obviously not
adequate to prevent and contain the ongoing outbreaks/epidemic of malaria in the eastern
provinces.
There is no a built-in mechanism for forecasting and early warning for malaria epidemics.
There is no link between malaria control program and hydro-metrology and other relevant
departments regarding forecasting.
The existing malaria stratification is lacking to identify properly epidemic-prone areas
within the country.
The existing epidemic prevention mechanism is insufficient, and epidemic preparedness is
lacking.
EPR teams were established at central and provincial levels, and the system for epidemic
detection and investigation is in place, but are not fully functional especially at provincial
and lower levels.
Recommendations
The NMLCP capacity to judge the abnormality of the situation, decide on the
epidemiological diagnosis of outbreaks/epidemic and have the authority to plan and
implement epidemic containment measures should be strengthened, particularly at
provincial level.
Epidemic-prone situations should be identified during the process of stratification of the
malaria problem into discrete areas and populations based on various data from health and
non-health sectors.
It is expected that emergency situations within epidemic-prone areas or population groups
in Afghanistan are likely occur. The application of effective vector control methods
including focal IRS if technically feasible/operationally applicable should be seriously
considered to contain on-going outbreaks/epidemic and their further spread and recurrence
in subsequent years. In epidemic-prone areas, where LLINs and other sustainable vector
control measures are already used may be the most effective way of reducing transmission
and preventing epidemic spread to new areas or resurgence in subsequent years.
PROGRAMME MANAGEMENT
Conclusions
Almost all the departments of NMLCP are lacking manpower, financial resources and
coordination to make the programme more productive and fully functional at all levels.
There is a lack of competent programme staff in most programme departments, particularly
at provincial level at present. It has been noted that many of the professional and technical
staff of NMLCP have frequently moved out to search for a better job.
14
There are insufficient capacities/capabilities of the core technical groups, particularly at
provincial level to provide adequate guidance and assistance in planning, implementation,
monitoring and evaluation of malaria control and elimination activities.
There are a lack of coordination and no regular meetings between central programme and
provincial teams.
The programme’s budget has no adequate reserve provisions to meet possible problems
that are liable to occur during its implementation.
Recommendations
2. Emphasizing the need to address the emerging elimination and remaining challenges, the
current NMSP/MEP 2013-2017 should be revised to reflect changes in programme
priorities, targets, strategic approaches and key interventions, considering that malaria
elimination in Afghanistan should be carried out in a phased manner by parasite species
with a priority to be given to elimination of P. falciparum and by geographical area (sub-
national elimination) with different parts of the county being at different programme phases
simultaneously. NMLCP may request WHO to provide the necessary technical assistance
in relation to this task.
For relatively large and heterogeneous country like Afghanistan, the emphasis should be
given to assessing major administrative units, typically Provinces. Some provinces have
already become eligible for elimination. If their health systems are strong enough, it is
rational to pilot surveillance and other elimination activities focusing on setting up
adequate surveillance, databases and quality assurance systems, preparing and testing
relevant SOPs and training for different categories of health staff.
To ensure achieving programme objectives and targets the roles and responsibilities of
departments of the NMLCP should be revisited to ensure their proper guidance, continuous
coordination and synchronization of their work.
Assessment of the NMLCP’s capacity in terms of human resources available at central and
provincial levels should be carried out to make the inventory of programme staff, and on
this basis to decide on the number and categories of professional personnel to be trained
or re-trained.
PROCUREMENT SUPPLY MANAGEMENT (PSM)
Conclusions
Procurement supply management of NMLCP in Afghanistan is implemented by
UNDP/GFATM and UNDP collaborates with NMLCP for quantification and
specification.
Besides UNDP as GF grant PR, BPHS/EPHS is another big channel for PSM, which
includes mostly malaria supplies. The main challenges include unavailability of
information on quantity, quality, costing, etc. of supplies procured and distributed by this
system with NMLCP.
Recommendations
Establishment of a mechanism to regularly exchange the PSM information with NMLCP
is required for a timely action in procurement and supplying of the medicines or materials

15
based on updated policy, proper allocation of the needed supplies, avoiding the gaps of
required supplies, etc.
MONITORING AND EVALUATION (M&E)
Conclusions
The national malaria M&E plan has been recently updated and is being presently used to
guide and coordinate malaria M&E activities among all parties involved.
There are too many outcome/impact indicators being reported as recommended by NMSP
and MEP 2013-2017, and they are not properly specified in relation to the stage on the
continuum to malaria elimination.
Lack of adequate analytical capacity for data interpretation, particularly at the provincial
level.
Malaria-related trainings on malaria M&E are insufficient at all levels.
Recommendations
To streamline the reporting process, the existing outcome and impact indicators should be
re-examined considering maintaining a minimum set of indicators per an objective. The
decision on selection of the minimum set of realistic indicators should be taken by NMLCP
in close collaboration with WHO and other partners concerned. NMLCP may request
WHO to provide the necessary technical assistance in relation to this task.
Different set of outcome and impact indicators are required depending on the stage on the
continuum to malaria elimination, which should be routinely tracked by NMLCP. Indicators on impact and adequacy of surveillance are central to verification about
interruption of malaria transmission, its elimination and maintenance of malaria-free
status.
ADVOCACY, IEC & COMMUNITY MOBILIZATION
Conclusions
There is a lack of understanding how local communities perceived malaria and what kind
of preventive practices are currently in place at grassroots level.
There are shortages of updated IEC materials on malaria available in public health facilities
across the country.
There are no operational plans available at provincial level to conduct advocacy and social
mobilization related to malaria prevention.
Recommendations
In the context of the national plan for malaria elimination, NMLCP should map all the
current IEC/BCC strategies and revise them, if necessary, to align with existing strategies
on case management, disease prevention and surveillance.
To improve coordination, NMLCP may convene a meeting to share with all partners
involved progress on IEC/BCC activities, identify best practices and challenges in
implementation, update key messages and develop new IEC/BCC materials/messages in
the context of malaria elimination.

16
OPERATIONAL RESEACH
Conclusions
Designing and conducting operational research is entirely dependent upon provision of
external funds, but there is lack of donors’ commitment.
Despite the National Institute for Health has some capacity for planning/conducting
operational research related to malaria, the overall national operational research
capabilities are insufficient in Afghanistan.
Recommendations
Operational research on malaria should be prioritized in the donors’ mandate for allocation
of human/financial resources.
A national core group of researchers should be formed to address malaria-related issues,
and some of them should attend international training courses on designing research
protocols and conducting relevant studies.

17
INTRODUCTION
RRaattiioonnaallee
Based on WHO recommendation, the MPR should be conducted every 3–5 years as part of the
mid-term and end-of-term evaluations before the strategic plans are revised and updated and, if
possible, as part of the evaluation preceding a new GF proposal. Consequently, the NMLCP of the
MoPH and partners planned to conduct MPR at end of 2016 or early 2017 to evaluate the
performance of national malaria control programme and recommend priority areas for revision of
the existing national strategic plan which will be done in 2017. Moreover, this MPR is an in-depth
assessment of the GF NFM grant for malaria control program in Afghanistan. Under this review
the national response to malaria in Afghanistan will be evaluated in a comprehensive manner by
external and internal experts who have extensive expertise in different areas of malaria control and
elimination, order to identify the existing gaps/challenges and advise on possible solutions with
the aim to improve the performance of national malaria programme, revise the existing national
strategic plan on malaria control and elimination and assist NMLCP in resource mobilization.
Objectives
General objectives
To assess national malaria programme by identifying achievements, critical issues, problems and
their underlying causes as well as to provide technical recommendations with a view of revising
of the existing strategic plan to address the emerging and remaining challenges.
Specific objectives
To review the epidemiology of malaria in Afghanistan
To review the structure, organization, and management framework of NLMCP within the
national health system and development agenda;
To assess progress towards achievement of national, regional and global targets;
To review the current programme performance by major thematic areas and by service
delivery levels;
To define the next steps on re-defining the strategic direction and focus, including revision
of the existing policies and strategies.
Thematic areas reviewed
Epidemiology, surveillance, monitoring, evaluation;
Programme management;
Diagnosis and case management;
Vector control;
Epidemic preparedness and response;
Malaria commodities procurement supply management;
Advocacy, information, education, communication and community mobilization;
Operational research.

18
EExxppeecctteedd OOuuttppuuttss,, OOuuttccoommeess aanndd TTiimmeelliinneess
Outputs
Programme thematic area reviews and provincial review reports
Programme Review Aide Memoire
Programme Review Report
Outcomes
Updated knowledge on epidemiology of malaria, recent trends and present malaria
situation in Afghanistan;
Re-define malaria risk mapping, populations at different risk, and malaria risk factors;
Identify areas for revision in the existing strategic and operational plans on malaria control
and elimination; and
Recommend areas for revision in the existing malaria guidelines for various categories of
interventions.
Timelines
On 7th of November: preliminary findings (current situation, existing challenges and
possible solutions) by the thematic areas have been presented by the MPR international
consultants and thoroughly discussed;
On 8th of November: a consolidated presentation and draft of the aide memoire have been
prepared and shared with all concerned for their comments;
On 9th of November: a consolidated presentation has been made by the MPR international
consultants and the draft of the aide memoire has been submitted;
Between 8th and 15th of November: preparation and finalisation of the Thematic Area
Reviews;
On 15th of November: submission of the Thematic Area Reviews to the Team Leader;
Between 16th and 25th of November: preparation of and discussions on the Draft
Programme Review Report;
Between 26th of November and 1st of December: finalization of the Final Programme
Review Report and its submission to UNDP/GF and MoPH in Afghanistan.
RReevviieeww PPrroocceessss
Coordinator
Director, NMLCP acted as the review coordinator. The role of the programme manager was to
lead, plan and organize the review as well as conduct it with the support of the technical team
appointed for this purpose. Tasks of the review coordinator and the technical team were the
following:
Prepare a review proposal and plan;
Prepare a budget and secure financing;
Set up a review secretariat, and review task force, supported by national and international
facilitators or consultants;
Identify internal and external review team members;

19
Prepare background documents, conduct a desk review and collect the necessary materials;
Arrange the logistics of the review;
Support the preparation of presentations;
Support the preparation of the aide-memoire, slide presentation and press release;
Support preparation of the report and its printing and dissemination; and
Follow up the recommendations of the review and implement the plan of action.
Secretariat
A secretariat to provide the necessary logistic, secretarial and communication support was set up
by the national malaria control programme. The review secretariat provided technical,
organizational and logistic support for all phases of the review.
Taskforce
The national malaria control programme and its partners appointed a malaria programme review
taskforce who oversaw the review. The recommended team included the review coordinator and
malaria control programme staff who constituted the core secretariat with both technical and
programmatic knowledge and skills in malaria control and public health service delivery. Members
from the GF Country Team participated as observers during the review. A TTT was established to
closely oversee the planning, implementation and completion of the MPR.
MMethodology
The MPR involved a mixture of methods, including desk reviews of technical thematic areas based
on programme data, reports, documents and published literature; updating country databases and
country profiles; mapping of populations at risk; estimating burden and making projections; policy
and management analysis; special studies; and group work, individual consultations and provincial
and district field visits with interviews and observations.
20
PART 1
Geography and Climate
The geography and climate in Afghanistan are highly variable and generally characterized by
rugged topography, patchy rainfall and extreme aridity in large parts of the country. Almost half
of the country land surface lies above altitudes of more than 2000 meters. In the northeast, the
country is dominated by the Hindu Kush mountain range which is prone to earthquakes and
comprises the Wakhan Corridor-Pamir Knot, Badakhshan, Central Mountains, Eastern Mountains,
Northern Mountains and Foothills, Southern Mountains and Foothills. The Turkistan Plains, Herat-
Farah Lowlands, Sistan Basin-Helmand Valley, Western Stony Desert, and Southwestern Sandy
Desert surround the Mountains in the north, west and southwest.
During the winter, temperatures in the central highlands of the country, the area around Nuristan
and the Wakhan corridor, drop to below -15 °C while in the summer in July the low-lying areas of
the Sistan Basin of the southwest, the Jalalabad basin in the east, and the Turkistan plains along
the Amu River in the north temperatures average over 35 °C. The Sistan Basin is one of the driest
areas in the world while much of the south and south west has desert climate. Average rainfall in
the country is approximately 210 mm per year with the main rainy season from December to April,
although some areas in the south-east receive monsoonal summer rain. The country drainage
system is dominated by four main rivers: Amu (Oxus) to the north, the Hari Rud to the west, the
Helmand River in the south and the Kabul River in the east. Forests, found mainly in the eastern
provinces of Nuristan and Paktiya, cover barely 2.9% of the country's area although these are
diminishing. In the eastern and north eastern provinces, irrigated rice cultivation is widely
practiced and is a major contributor to anopheles breeding (Safi et al., 2009).
PPooppuullaattiioonn aanndd DDeemmooggrraapphhyy
As of 1 January 2016, the population of Afghanistan was estimated to be 33 045 440 people within
a total geographical area of 647,500 sq. km. Approximately 76% of the population lives in rural
areas. About 2.7 million Afghan refugees are living in Pakistan and Iran. The sex ratio of the total
population was 1.072 males per 1 000 females, which is higher than global sex ratio. During 2016
Afghanistan population is projected to increase by 997 642 people and reach 34 043 082 in the
beginning of 2017. Afghanistan population density is 50.7 people per square kilometre as of
November 2016. Total life expectancy (both sexes) at birth for Afghanistan is 61 years. Literacy
rate for adult male population is 51.99% and this rate for adult female population is 24.15%. The
key health indicators for Afghanistan are shown in Table 1 below.
Table 1: The key health indicators, Afghanistan
Indicator Value World Ranking
Crude Birth Rate 32.504 births/thousand 38th

21
Indicator Value World Ranking
Crude Death Rate 7.857 deaths/thousand 88th
Life Expectancy (Both Sexes) 61.041 years 176th
Life Expectancy (Male) 59.851 years 175th
Life Expectancy (Female) 62.32 years 176th
Total Fertility Rate 4.477 children/woman 28th
Infant Mortality Rate 65.684 deaths/1,000 live births 14th
Under Five Mortality 89.935 deaths/thousand 18th
The population of Afghanistan includes many different ethnic groups. The Pashtuns, who make
up more then half the population, have traditionally been the dominant ethnic group. Their
homeland lies south of the Hindu Kush, but Pashtun groups live in all parts of the country. Many
Pashtuns also live in northwestern Pakistan, where they are called Pathans. Pashtuns are usually
farmers, though many them are nomads, living in tents made of black goat hair. The Pashtuns
speak Pashto, which is an Indo-European language and one of the two official languages of
Afghanistan. The Tajiks, are the second largest ethnic group in Afghanistan. They live in the
valleys north of Kabul and in Badakhshan. They are farmers, artisans, and merchants. The Tajiks
speak Dari, also an Indo-European language and the other official language of Afghanistan. Dari
is more widely spoken than Pashto in most of the cities. In the central ranges live the Hazaras.
Although their ancestors came from the Xinjiang region of northwestern China, the Hazaras speak
an archaic Dari. Most are farmers and sheepherders. In the east, north of the Kabul River, is an
isolated wooded mountainous region known as Noristan. The Noristani people who live there
speak a wide variety of Indo-European dialects. In the far south live the Baluchi, whose Indo-
European language (called Baluchi) is also spoken in southwestern Pakistan and southeastern Iran.
To the north of the Hindu Kush, on the steppes near the Amu Darya, live several groups who speak
Turkic languages. The Uzbeks are the largest of these groups, which also include Turkmen and, in
the extreme northeast Vakhan Corridor, the Kyrgyz people. These groups are settled farmers,
merchants, and seminomadic sheepherders. The nomads live in yurts, or round, felt-covered tents
of the Mongolian or Central Asian type.
22
Agriculture is the backbone of the Afghan economy, the rugged topography and low rainfall are
severe constraints on productivity. Rice is intensively cultivated through snow-fed irrigation in
the eastern and northeastern provinces and is a major contributor to anopheline breeding sites.
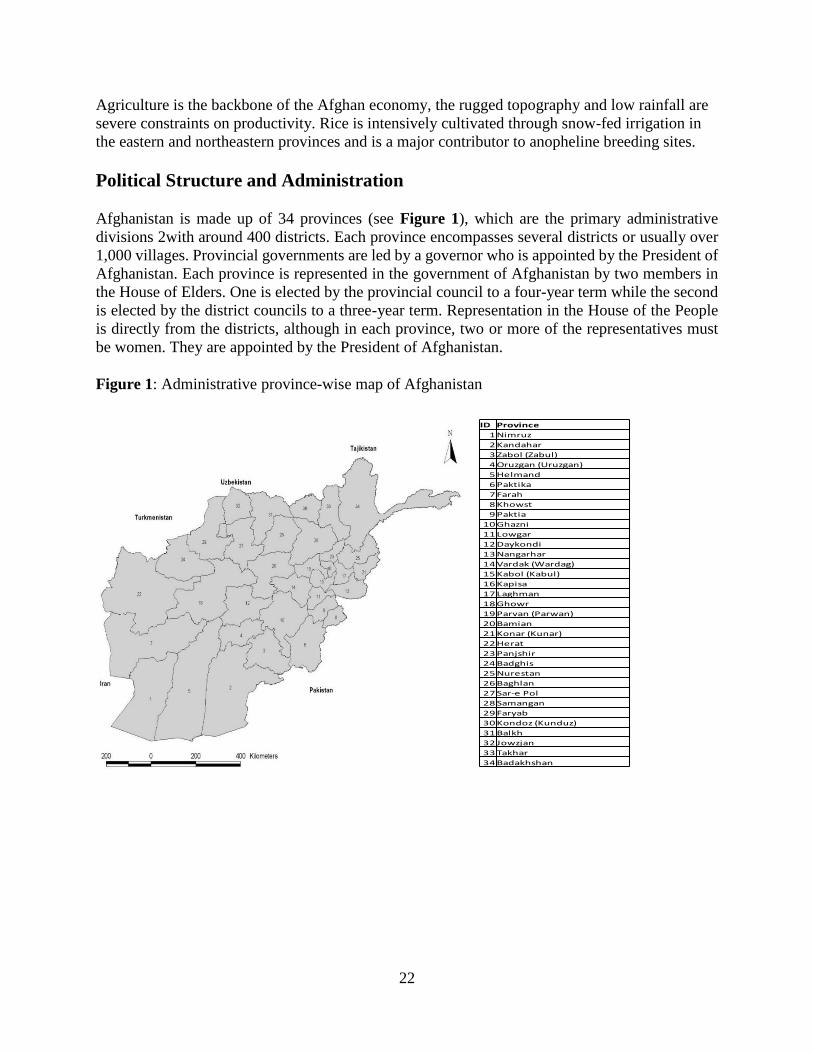
Political Structure and Administration
Afghanistan is made up of 34 provinces (see Figure 1), which are the primary administrative
divisions 2with around 400 districts. Each province encompasses several districts or usually over
1,000 villages. Provincial governments are led by a governor who is appointed by the President of
Afghanistan. Each province is represented in the government of Afghanistan by two members in
the House of Elders. One is elected by the provincial council to a four-year term while the second
is elected by the district councils to a three-year term. Representation in the House of the People
is directly from the districts, although in each province, two or more of the representatives must
be women. They are appointed by the President of Afghanistan.
Figure 1: Administrative province-wise map of Afghanistan
ID Province
1 Nimruz
2 Kandahar
3 Zabol (Zabul)
4 Oruzgan (Uruzgan)
5 Helmand
6 Paktika
7 Farah
8 Khowst
9 Paktia
10 Ghazni
11 Lowgar
12 Daykondi
13 Nangarhar
14 Vardak (Wardag)
15 Kabol (Kabul)
16 Kapisa
17 Laghman
18 Ghowr
19 Parvan (Parwan)
20 Bamian
21 Konar (Kunar)
22 Herat
23 Panjshir
24 Badghis
25 Nurestan
26 Baghlan
27 Sar-e Pol
28 Samangan
29 Faryab
30 Kondoz (Kunduz)
31 Balkh
32 Jowzjan
33 Takhar
34 Badakhshan

23
PPAARRTT 22
Health Profile and Policies
Significant progress in Afghanistan’s health services over the last decade has translated into
substantial declines in infant, child and maternal mortality rates. However, many of Afghanistan’s
health indicators remain extremely worrisome. Progress seems to be stagnating, and surveys show
large imbalances across socio-economic levels with a clear urban/rural divide. Gender inequality
is a pervasive problem and women and girls experience avoidable morbidity and mortality because
of gender-based discrimination and harmful practices, including many different forms of gender-
based violence. Afghanistan is frequently hit by natural disasters causing significant loss of lives,
livelihoods and infrastructure. In 2015, 7.4 million people needed humanitarian assistance, an
increase of 37% from the previous year.
Life expectancy is low at 61 years, and despite a significant decline, infant, under-five and maternal
mortality are still high, respectively at 66 per 1000 live births, 91 per 1000 live births and 396 per
100,000 live births. There is an extremely high prevalence of chronic malnutrition, with 39% of
all children under five years of age being malnourished. Micro-nutrient deficiencies are
widespread: around 46% of children under five suffer from vitamin A deficiency.
NCDs contribute to more than 35% of overall mortality. Major causes of mortality due to NCDs
include cardiovascular disease, cancer and diabetes.
There is a high burden of communicable diseases, which account for more than 60% of all
outpatient visits and more than half of all deaths. Tuberculosis continues to be a major public
health challenge – there are around 58,000 cases of tuberculosis every year with around 13,000
deaths. Over 75% of Afghans live in areas at risk of malaria transmission. While Afghanistan
remains one of the two polio-endemic countries globally, progress has been achieved in polio
eradication. In 2015, 20 polio cases were reported, compared to 28 in 2014. Overall immunization
coverage remains low – only 51% of all children receive all antigens before the age of 1 and around
one fifth of Afghan women and children have never been immunized against diseases. Currently
10 antigens are included in the immunization programme.
Some of the major challenges and constraints faced by the health sector include: inadequate
financing for many key programmes and heavy reliance on external sources of funding;
insufficient and inadequately trained health workers and a lack of qualified female health workers,
particularly in the rural areas; lack of access to healthcare due to dispersed populations and
insecurity; quality-compromised services; constrained national capacities for health planning and
management, especially in the areas of governance, healthcare financing, human resource
development, monitoring, evaluation and analysis of the health situation at central and especially
at the provincial level.
The BPHS and EPHS have been developed by the MoPH, and partners and health services are
delivered through an innovative contracting-out mechanism by international NGOs and MoPH in
selected provinces. There has been considerable progress under difficult circumstances in
increasing the number of health facilities and developing and implementing strategic health

24
policies and plans with the financial and technical assistance from bilateral and multilateral
development partners.
The coverage of the BPHS/EPHS public health system is around 60% with a compromised quality
of service delivery. There is a lack of or very limited provision of public health services in security-
compromised areas that make up over 30% of the country. There is a substantial health workforce
which is unbalanced in terms of capacity, gender as well as geographic distribution. The private
sector is unregulated and expanding.
The MoPH and partners developed a new National Health Policy for 2015-2020 with five key
policy areas including governance, institutional development, public health, health services and
human resources. The Ministry is currently in the process of developing its new Health Sector
Strategic Plan 2016-2020 based on the new policy with active involvement of partners. Total health
expenditure roughly equals to US$55 per capita per year, of which 20-25% is covered by
development partners and 4-6% by the government budget: out-of-pocket share is more than 70%.
OOvveerrvviieeww ooff HHeeaalltthh SSeerrvviicceess
MoPH is one of the leading Ministries in the Government of the Islamic Republic of Afghanistan.
Building on recent achievements and based on the new policy with active involvement of partners,
the Ministry has developed a National Health Strategic Plan for 2016-2020.
In 2003, the MoPH made the decision with the support of donors, to change its role to a stewardship
role. That decision resulted in the development and implementation of the BPHS. Provision
primary health care services based on this package has been contracted out to nongovernmental
organizations (NGOs). “The goal in developing the BPHS was to provide a standardized package
of basic health services that would form the core of service delivery in all health care facilities.
The BPHS was further revised in 2010. For secondary health care services, the EPHS was later
added, focusing on hospitals, improving their facilities and equipment, staff training and
development and enhancing the referrals between different levels of the health system.
Contracting out to NGOs has worked well in Afghanistan and has proven to be enormously
successful in expanding service coverage and improving quality of care. Currently the vast
majority of the entire population lives in districts where primary health care services are being
provided by NGOs either under contract with the MoPH or through direct grants from donors and
through the MoPH Strengthening Mechanism. The MoPH has used this system to ensure that all
providers are implementing the BPHS and EPHS in accordance with technical guidelines and that
all providers are clearly responsible and held accountable for defined geographical areas and
populations. As a result, health indicators for Afghanistan have dramatically improved since the
introduction of the BPHS and EPHS. The standardized classification of health facilities that
provide the basic health services includes (1) HPs; (2) HSCs; (3) BHCs; (4) MHTs; (5) CHCs, and
(6) DHs. Hospitals are classified into three groups (DHs, PHs and RHs) per size of the referral
population, number of beds, workload and complexity of patient services offered. Another group
of hospitals are located mostly in Kabul, and they provide education and training for health workers
and act as referral hospitals for the provincial and regional hospitals. This group of hospitals is
being directly managed by MoPH or Ministry of Higher Education.

25
History of Malaria Control
Organized malaria control programme was established in 1947 after an epidemiological
assessment conducted by WHO. Starting from 1949 a nation-wide spraying campaign was
organized. In 1956 malaria eradication was set as the goal and DDT indoor residual spraying (rural
areas) and anti-larval measures (urban areas) were the main malaria vector control interventions
applied in the country. In 1970 insecticide resistance to prevailing vector species was developed
and since 1973, eradication programme reverted to malaria control programme making the
diagnosis and treatment of malaria patients as one of the main strategic approaches. During 1992-
93 use of insecticide treated mosquito nets was adopted as a main malaria vector control approach.
Plasmodium falciparum developed resistance to chloroquine in early 1990s, and by 2001,
resistance levels exceeded 80%. The use of ACT for treating P. falciparum patients has been
started since 2003, and the use of RDTs kits expanded to confirm the malaria diagnosis.
National Malaria and Leishmaniasis Control Programme
Malaria control and elimination in Afghanistan is the responsibility of NMLCP in the CDC
Department of the General Directorate of Preventive Medicine in MoPH (See Annexes: Chart 1).
The main roles of NMLCP are to:
develop and disseminate evidence based effective policy and strategies;
develop national guidelines for all components of the national malaria strategy;
monitor malaria drug efficacy and insecticide resistance in the country;
recommend and support efficient malaria control and elimination activities;
monitor and evaluates the implementation and impact of malaria control and elimination
program in the country;
support capacity building of national health staff;
NMLCP has 34 PMLCP units operating in 34 endemic provinces. Key functions of them are to
provide coordination with NMLCP, facilitate capacity building of the health staff, monitoring and
evaluation of malaria activities like surveillance, diagnosis treatment etc. Introduction of the BPHS
has improved case management and data flow through HMIS systematized the national reporting
system.
At the provincial level vector control activities are managed through regional entomology
departments located in five provinces of the country including: Takhar, Kundoz, Badakhshan,
Nanagarhar and Balkh. Entomology departments in Nangarhar and Kundoz have 3 staff
(entomology officer, entomology supervisor and a technician) but the rest of the provinces have
only two entomology staff including an entomology officer and a technician. Most of these staff
do not carry out any entomological activities and are assigned for other task by the provincial
directors.
National malaria control efforts are mainly supported by the external donors with major funding
support from the GFATM.

26
National Strategic Plan on Malaria Control and Elimination/Malaria
Elimination Plan, 2013-2017
Vision:
Malaria-free Afghanistan.
Mission:
The NMLCP is to lead efforts to control malaria through coordinated approaches with multiple
partners, using evidence-based national policies and guidelines to reduce the burden of malaria
as a public health problem in Afghanistan.
Goal: To contribute to the improvement of the health status in Afghanistan through the reduction of
morbidity and mortality associated with malaria.
Objectives:
To reduce malaria morbidity by 85% in all malaria stratum by the end of 2017 (baseline
total cases (confirmed plus clinical) = 19.5 cases per 1000 population; 5.5 estimated
confirmed cases per 1000 population, 2011 data);
To reduce malaria mortality to 99% by the end of 2017 (nationally malaria reported deaths
40, in 2011);
To reduce the incidence of P. falciparum malaria to sporadic cases by the end of 2017 with
a vision to completely interrupt transmission of Pf by 2020; and
To reduce malaria morbidity in high risk (stratum one districts) by 80% by the end of
2017 (baseline total cases [clinical plus confirmed] = 146.7 per 1000; estimated
confirmed cases, 38 per 1000 from 2009-2010 figures).
Strategic Directions:
Case Management; prompt and reliable diagnosis and effective treatment;
P. falciparum elimination and reduction of deaths from malaria to zero and P. vivax by
90% by 2017 in northern, north-eastern and north-western provinces;
Application of preventive measures in the framework of IVM with a focus on LLINs;
Detection and control of malaria epidemics;
Strengthening of the health system and malaria control programme;
Malaria control and border areas;
Quality assurance;
Information, Education and Communication for malaria prevention; and
Operational Research.

27
PART 3
Malaria Epidemiology
Malaria is still a major public health problem in Afghanistan. Referring to WMR 2015, 24% of
Afghan population lives in areas at high risk for malaria, 49% at medium risk and the remaining
27% live in areas with no risk or very low risk of malaria transmission. Malaria is a complex
disease and its distribution in Afghanistan varies largely from place to place, and is dependent
upon a variety of factors related to parasites, vectors and human populations under different
geographical, ecological and socio-economic conditions. Using a combination of available malaria
and environmental data, all districts in Afghanistan were classified into four main strata with high,
medium, low and very low risk of malaria transmission or its absence in malaria free areas (see
Figure 2).
Figure 2: District-wise stratification of Afghanistan by high, medium, low risk of malaria and
areas with no risk
The natural extent of malaria transmission in Afghanistan is limited by the combination of high
altitude and the consequent reduced temperatures and aridity which affect both development of the
malaria mosquitos and parasites. Malaria occurs at altitudes below 2000 metres above sea (see
Figure 3), and most prevalent in river valleys and rice-growing fields across the country. In a
recent analysis of the temperature suitability to support parasite sporogony, an index ranging from
0 (not suitable) to 1 (most suitable) (Gething P. et al., 2011) has showed that most of the
temperature-suitable areas were coincident with altitude of ≥2000m (Figure 4).

28
Figure 3: Malaria altitude limits, Afghanistan
Figure 4: Temperature Suitability Index for malaria parasite sporogony, Afghanistan
At present, P. vivax malaria is the most prevalent species accounting for almost 95% of all
parasitologically confirmed cases, with less than 5% of total cases attributed to P. falciparum with
a decrease in its proportion over the past years. Malaria transmission is seasonal from June to
November. The P. falciparum peak is in August to October (see Figure 5), a few months after the
summer peak of P. vivax (see Figure 6). Many Plasmodium vivax infections relapse during the
spring season and this may give rise to a vivax peak around July Transmission of P. falciparum,
at the edge of its geographical range, is unstable, and can fluctuate markedly from year to year.

29
Recent surveys have highlighted the diverse distribution of Anopheline mosquitoes in Afghanistan
(see Figure 7). Abundance and species composition varied by ecological zones, and included the
following malaria vector species: An. stephensi, An. culicifacies, An. fluviatilus, An. annularis, An.
pulcherrimus, An. superpictus and An. hycranus. During the rainy months, small collections of
water exposed to sunlight formed suitable breeding habitats for An. stephensi. An. superpictus was
found to breed commonly in canals. The study positively incriminated An. stephensi as the
predominant vector, exhibiting strong zoophilic behaviour, with a strong presence in animal sheds
than in human habitations. An. pulcherimus was found to be mostly an outdoor feeder and its peak
of activity was before midnight. An. superpictus with a minority of An. stephensi is found in Balkh
and Herat. An. pulcherimus, An. hycranus and An. stephensi are revealed in Badakshan and
Kunduz including An. superpictus in the latter province. It should be noted that aside from An.
stephensi being the incriminated vector in Nangarhar, the vector status, predominance, seasonal
distribution and behaviors of other anopheline species such as An. subpictus and An. culcifacies
have yet to be confirmed (Eshgy N. & Nushin M. 1978; Rowland M. et al., 2002; Safi N. et al.,
2009)
0
1000
2000
3000
4000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Figure 5: Seasonal pattern of P. falciparum, 2013-2015
2013 2014 2015
0
20000
40000
60000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Figure 6: Seasonal pattern of P. vivax, 2013-2015
2013 PV 2014 PV 2015 PV

30
Figure 7: Geographical distribution of malaria vectors within Afghanistan
Analysis of species composition amongst Anopheles mosquitoes has shown that An. stephensi
(Leslie, Mohammed et al. 2008) remains the dominant species in Nangahar Province (see
Figure 8).
Figure 8: Species composition of Anopheline mosquitoes collected during entomological
surveillance in Nangarhar Province, 2008.

31
There is a profound diversity in ethnic groups residing across the country. The genotypic study of
the Mediterranean variant of G6PD deficiency in males in nine provinces in Afghanistan confirms
that the 563C.T mutation reaches its highest frequencies in Pashtuns and Pashais (8.9%), with
lower prevalence in groups historically associated with northern provinces and countries to the
north of Afghanistan (Natsuda J. et al., 2014).
Recent Trends and Present Situation
In some northern, western and southern provinces cases of malaria, particularly P. falciparum have
dropped significantly and these provinces became eligible for malaria elimination. It is becoming
evident that some provinces have already interrupted and other provinces could interrupt
transmission of P. falciparum malaria in the years ahead. However, in some eastern provinces
along the border with Pakistan, continuous outbreaks have caused a severe epidemic malaria in
2014-2016.
In 2015, more than 70% of reported confirmed cases were reported from 3 eastern provinces such
as Nangarhar, Kunar and Laghman, and almost 90% of all confirmed P. falciparum cases were
registered in 5 provinces (Nangarhar, Laghman, Kunar, Khost and Paktika) with 49 reported deaths
due to malaria from Nangarhar and Kunar, reflecting a focal distribution of the malaria problem
in Afghanistan (see Figures 9 & 10).
Figure 9: Annual Malaria Parasite Incidence by districts, Afghanistan, 2015

32
Figure 10: Annual P. falciparum Parasite Incidence by districts, Afghanistan, 2015
In 2015 several outbreaks of P. vivax and P. falciparum malaria were reported in eastern provinces
of the country resulted in the increase of the number of reported clinically-suspected and confirmed
cases of malaria (see Figures 11, 12, 13, 14 & 15).

33
Figure 11: Confirmed malaria cases reported in Nangarhar province, 2012-2015
Figure 12: Confirmed malaria cases reported in Laghman province, 2012-2015
Figure 13: Confirmed malaria cases reported in Kunar province, 2012-2015
84 50 49 88220 345 474 451
697
1043 971
344168 98 46 196629
1,196
3,224
4,2283,995
2,076
1,458
470
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Av 12-14 2015

34
Figure 14: Seasonal pattern of P. vivax cases reported in Nangarhar, Kunar, Laghman eastern
provinces, 2015
138 105 187 192
595
1,039 1,0741,209
1,5861,258
816
252115
35 92
261
1,138
1,7741,892
2,101
2,590
1,167
705
280
0
500
1000
1500
2000
2500
3000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Av 12-14 2015
0
2000
4000
6000
8000
10000
12000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Kunar Laghman Nangarhar

35
Figure 15: Seasonal pattern of P. falciparum cases reported in Badakhshan province, 2015
Since 2013, the proportion of malaria cases confirmed by RDTs and/or microscopy has
substantially increased from 14.4% in 2013 to 28.2% in 2015. However, the majority (more than
70%) of reported malaria cases are still diagnosed on clinical ground in 2015 (see Figure 16).
During 2013-2015, a somewhat increase in the number of confirmed malaria cases has been
observed for both P. vivax and P. falciparum due to improved access to and use of parasitological
0
5
10
15
20
25
30
35
40
45
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Pf malaria
626839585602
273377
326694
414407
461283
467123
390729392463
482748
391365
319742295050
366526
0
100000
200000
300000
400000
500000
600000
700000
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Figure 16: Total number of clinically-suspected and parasitologically
confirmed cases in Afghanistan, 2002-2015
Confirm + Clinical

36
diagnosis. There was a tiny proportion (4.9-7.1%) of P. falciparum cases during 2013-2015 (see
Figure 17).
Figure 17: The number of clinically-suspected and parasitoilogically confirmed cases of P. vivax
and P. falciparum in Afghanistan, 2002-2015
Because of continuous improvement in access to parasitological diagnosis across the country
between 2013 and 2015, API increased from 1.79 to 3.82 cases per 1000 population at risk per
year with a wide province-wise range (0.01 to 41.94 cases per 1000 population). The highest API
of 27-42 cases per 1000 population at risk was reported in three eastern provinces of the country
(Kunar, Laghmar and Nangarhar).
Over the past three years (2013-2015), ABER has not significantly changed and remained at a
relatively low level (2.0-2.5%) with considerable fluctuations from 0.05% to 18.7% by provinces.
In 2015, the highest ABER (12.4%-18.1%) was reported in three eastern provinces of the country
(Kunar, Laghmar and Nangarhar) where the most P. falciparum and P. vivax cases of malaria were
reported. SPR has increased from 9.1% to 19.2% with the highest SPR/TPR of over 20% was
reported in the same eastern provinces in 2015 (see Annexes: Tables 2 & 3).
212,228224,662
31,355
210,250
328,278
369,081385,549
325,849 323,066
405,199
336,525
273,628
211,130
263,149
330,083316,697
229,233
110,527
79,913 85,919 77,21960,854 63,255 71,968
53,609 43,842
77,93798,357
84,528 44,243
12,789 5,917 6,216 6,283 4,355 4,026 6,142 5,581 1,231 2,272 5,983 5,020
0
50000
100000
150000
200000
250000
300000
350000
400000
450000
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Total Clinical Cases Pv Pf

37
PART 4 (Programme Performance by Thematic Areas)
4.1. Case Management
Current Situation & Existing Challenges
Clinical diagnosis was practiced in the country due to limited capacity for diagnostic confirmation.
Many of the clinically diagnosed cases receiving CQ were not malaria (Leslie T et al. 2012).
Despite change in the policy advocating parasitological diagnosis for all suspected cases majority
cases are still diagnosed clinically (71%), and only 29% are diagnosed by microscopy or by using
rapid diagnostic test (Annual Malaria Report 2015, MoPH/Afghanistan). RDT-based diagnosis has
good sensitivity and specificity in P. falciparum malaria in comparison with P. vivax. At present
bivalent RDTs are used which can detect P. vivax, P. falciparum and mixed infection. Previously
there was no report of mixed infection was found from Afghanistan, in a recent RDT based
diagnosis ~6% were found to have mixed P. vivax and P. falciparum infections (Annual Malaria
Report 2015, MoPH/Afghanistan). In neighbouring Iran and Pakistan mixed P. falciparum and P.
vivax malaria were reported earlier as well (Shaikh S et al. 2012: Zakeri S et al. 2012).
Diagnosis and treatment of malaria has been integrated into the BPHS, EPHS and there is initiative
for the CBMM (A BPHS for Afghanistan, MoPH/Afghanistan, 2009; The EPHS for Afghanistan,
MoPH/Afghanistan, 2005: National Strategy for Community-based Management in Afghanistan,
2016-2020, MoPH/Afghanistan, 2016). An attempt for making good coordination has been
observed between NMLCP, BPHS, EPHS and NGOs. EPHS and EPHS Programmes including
malaria activities are performed by contracted out implementers.
The public health system providing PHC is relatively weak but despite limitations management of
malaria has been found to be one of the example of ‘best practice’ in health care delivery in
Afghanistan. Health Sector Strategy of Afghanistan 2016-2020 implementing 1st SWAP, and
NMSP 2013-2017 committed to ‘promote prompt diagnosis and effective treatment of malaria’ as
one of the 14 key interventions (National Health Strategy 2016-2020, MoPH/Afghanistan, 2016;
National Strategic Plan for Malaria Control and Elimination 2013-2017, MoPH/Afghanistan,
2013). In fact, major cornerstone of control of malaria is prompt diagnosis and treatment.
Major components of the current malaria diagnosis and treatment guidelines (updated 2014,
previous one is 2010) are as follows:
Clinically diagnosed cases to receive 3-day CQ;
P. vivax cases to receive 3 day CQ + PQ for 14 days if G6PD test is available;
P. falciparum cases to receive ACT, AS+SP (1st line drug) plus single dose of PQ; quinine
plus doxycycline or clindamycin (2nd line drug);
Severe malaria-injection quinine; pre-referral treatment for severe malaria - IV/IM AS or
artemether.
Specific recommendations for treatment of cases during pregnancy are also provided in the
guidelines. Complete treatment of P. vivax malaria requires treatment of both blood and liver stage,
to achieve clinical cure, and to prevent relapses, onward transmission and progression to severe

38
disease (WHO guidelines for the treatment of malaria, 3rd edition, Geneva, 2015; Control and
Elimination of Plasmodium vivax malaria: A Technical Brief, WHO, 2015). At present, there is no
user-friendly test at point of care to detect G6PD deficiency reflecting that no wide scale use of
PQ has occurred. There is a variable proportion of G6PD deficiency among Afghan population
with highest among the Pashtun/Pashai group (8.9%) and 2% in rest of the population
(Jamornthanyawat N et al. 2014). A study comparing 14 day PQ and its weekly dose for 8 weeks
is presently being conducted. There is an ongoing study to provide PQ in GPD deficient vivax
cases at the level of district hospital after referral although majority of the cases are expected to be
diagnosed at the peripheral level by community based health workers. Provision of PQ after doing
G6PD test at DHs will limit access to the quick treatment. In Afghan refugees residing in Pakistan
weekly dose of PQ for 8 weeks has been found to be better than CQ alone in preventing relapse
and not associated with major side effects (WHO Malaria Microscopy: Quality Assurance Manual,
version 2, 2015).
Training materials for confirming diagnosis by using RDTs and microscopy, and treatment
provision by various health care professionals were developed by NMLCP.
QAS for diagnosis and treatment of malaria has been adopted by NMCLP. QAS requires the
national reference laboratory to set up standard operating procedures (SOPs), provide training per
standard and reference materials (including slide bank, bench aids) available to all staff. SOPs
describe below in detail the activities to be performed in laboratories providing malaria
microscopy/RDT services Leslie T et al. 2008).
Box: SOP for Malaria Microscopy
1. Microscope use and Preventive Maintenance
2. Cleaning and Storing of Microscope Slides
3. Bio-safety in Handling Blood Specimens and Disposal of Infectious Waste Materials
4. Preparation of Thick and Thin Blood Film
5. Preparation of Giemsa Stock Solution
6. Preparation of Giemsa Working Solution and Staining of Malaria Blood Films
7. Reading of Malaria Blood Smear and Parasite Quantification
8. Interpretation, Recording and Reporting of Results
9. Cross-checking of Malaria Blood Smear
10. Feed backing of cross-checked slides
11. On-site Supervisory and Monitoring Visits in Microscopy Centers
12. Conduct of Basic Malaria Microscopy Training
13. Conduct of Proficiency Assessment
The SOPs aim to provide uniformity, consistency and reliability in each of the laboratory activities
performed, to ensure high quality diagnosis (accuracy, sensitivity, and specificity of smear reading
results) and provides training and reference for old and new staff. Structured standard QAS was
not found in the laboratories visited/or activities reported; although specific proportion of
‘positive’ and ‘negative’ slides were cross checked, refresher’s training conducted but few
technologists had the formal microscopy training and the refreshers’ course for the microscopists
was mostly unstructured.

39
IEC/BCC materials and clinical algorithm were made widely available at different tiers of care.
The displayed algorithm and posters on IEC was slightly different from each other.
Although parasitological diagnosis has been encouraged clinical diagnosis was widely practiced
until recently to introduce parasitological diagnosis by RDT in community based malaria program,
by microscopy/RDT in BPHS, EPHS facilities. Investigation report sometime are not considered
in decision making for providing treatment (20-30% patients get CQ despite negative results).
Single dose Primaquine is yet to be used for the treatment of Pf malaria, and 14 day PQ is yet to
use for radical cure of vivax.
Quick treatment seeking has been promoted by the NMLCP guidelines as per WHO
recommendation of diagnosis within 24-48 hours of onset of fever, but no time frame was
mentioned. Survey conducted in 2011 found that still only 59% febrile cases seek treatment within
48 hours, 33% within 24 hours (The 2nd MIS in Afghanistan 2011, MoPH/Afghanistan, 2012).
Most of the falciparum malaria occurred in 5 Eastern provinces (4461 out of 5020 falciparum
cases) but descriptive information is inadequate. There is little information about severe malaria
although 49 reported deaths happened in 2015 in two states (Malaria deaths by health facility,
NMLCP/MoPH/Afghanistan, 2016).
Limited observation from Afghanistan and a recent meta-analysis could not detect severe
manifestation following vivax infection, however a careful close clinical and laboratory
investigation is required to exclude such case in view of report of severe malaria in neighbouring
Pakistan (Rahimi B et al. 2014).
The health-seeking behaviour suggests that 34% patients go to private sector in stratum I and 26%
used to get self-medication for malaria (The 2nd MIS in Afghanistan 2011, MoPH/Afghanistan,
2012).
Adherence to treatment guideline is not optimal, for example in some places S-P alone is used for
the treatment of uncomplicated malaria, AS alone and even halofantrine, mefloquine are found to
be available in limited medicine shops visited by local consultants. Drugs not recommended in
NTG or by WHO were reported to be available in private sectors.
Drug quality assessment, pharmacovigilance, prohibiting the drugs not approved in NTG is yet to
be started by drug regulatory authority.
Several therapeutic efficacy studies were conducted for the treatment of vivax and falciparum
malaria in the previous decade. So far there is no resistance of vivax infection to chloroquine was
found. Despite continued use of ACT, AS+SP for long ten years it has been found to be effective
in limited study although in some early reports found resistance to S-P (Awab G et al. 2016). SP
from WHO qualified sources are difficult to be obtained now. Falciparum malaria in Afghanistan
has been found to be sensitive to ACT, artemether-lumefantrine (Awab G et al. 2015).

40
Conclusions
Diagnosis:
1. Parasitological confirmation of all clinically-suspected cases of malaria by RDT or
microscopy are not in place yet.
2. Many laboratory staff do not have standardized and recommended training on malaria
microscopy.
3. There is insufficient information from the private sector about diagnosis of malaria using
microscopy/RDT.
4. Lack of quality assurance for malaria diagnosis by microscopy and/or RDT in relation to
adhering to the tools developed/to be developed including using SOPs at different levels
including central malaria reference laboratory, NMLCP and PMLCP.
5. Lack of descriptive information about uncomplicated and severe/complicated cases of
malaria including deaths due to malaria.
6. G6PD deficiency test is not currently available.
Treatment:
1. Treatment of cases (P. vivax, P. falciparum, management of severe and complicated
malaria, pre-referral treatment of severe and complicated cases) are not always done as per
existing national treatment protocol/drug policy.
2. Despite the radical treatment of vivax cases and provision of a single dose of primaquine
for all P. falciparum malaria patients are recommended as per existing national treatment
policy, this approach has to be put into practice across the country.
3. Lack of training on case management based on updated curriculum for malaria diagnosis
and treatment of different health care providers including private sector and health staff of
CBMM, BPHS and EPHS facilities
4. There is insufficient training on management of severe and complicated malaria.
5. There is poor access to prompt/adequate diagnosis and effective treatment of malaria in
remote and border areas and at complex emergencies.
Recommendations
Diagnosis:
1. Wide scale deployment of (a) RDT through multiple channels- public and private sector
hospitals and lab, NGOs, at the community and (b) strengthening of existing microscopy

41
centres and setting up new microscopy centres should be considered to reach universal
coverage of case management including remote, inaccessible, ‘security compromised’ and
internally displaced populations.
2. Training on malaria diagnosis with updated training materials and SOPs should be
provided to different health care providers paying particular attention to CHWs and
providers based on new Malaria Microscopy QA manual of WHO (2nd edition, 2015).
3. Central and regional malaria reference laboratories should be strengthened or established
for (1) QA/QC for microscopy and RDT; (2) supervision and monitoring; (3)
implementation and use of standard training curriculum and SOPs for microscopy and
RDT; (4) prevention, maintenance, and repair of microscopes; and (5) resolving
discordance results linked to molecular testing.
4. External Quality Assurance system (EQA) for malaria microscopy and RDT should be set
up.
5. Long-term human capacity strengthening and sustainability of reference laboratories
should be ensured with a capacity building plan based on standardized training curriculum.
6. Death verification system of malaria by structured auditing all cases of death following
severe malaria should be established.
Treatment:
1. National malaria treatment guidelines should be updated based on the new 2015 WHO
Guidelines for the Treatment of Malaria.
2. Fourteen-day primaquine treatment, if G6PD test is available or 0.75 mg/kg primaquine
weekly for 8 weeks under close medical supervision should be put into practice at all
public, private and community-based health sector facilities, considering that policy
decision on the use of primaquine for radical cure of P. vivax pending further local new
evidence.
3. Standardized training curriculum on malaria treatment should be developed with
special emphasis on the use of primaquine and its side effects; using injectable
artesunate for treating severe and complicated malaria considering its superiority over
quinine; pre-referral management of severe and complicated malaria, and promoting
‘prompt’ treatment-seeking behaviour by the community.
4. Training materials and modules on case management should updated, relevant national
capacity building development plan should be agreed and training courses should be
regularly conducted for different categories of health care providers, private
practitioners and CHWs at different level.

42
5. QA of case management services and antimalarial diagnostics/drugs should be
established and functional covering the public, private and community-based health
sectors throughout the entire country.
6. Essential drug list for treating malaria should be revisited and a minimum set of
essential drugs is required for areas where cases are drastically reduced to avoid
wastage, to ensure that the antimalarial medicines provided in both public and private
sectors are of acceptable quality, through regulation, inspection and law enforcement.
7. Capacities of referral hospitals for and health personnel involved into management of
severe and complicated malaria should be improved and all severe and complicated
cases of malaria should be properly registered and reported.
8. Access to and quality of malaria diagnosis and treatment services should be improved
at remote, inaccessible and ‘security compromised’ areas and among mobile and
migrant populations.
9. Malaria case management at community level should be scaled up and supportive
supervision should be regularly provided.
10. The therapeutic efficacy studies should be continued with focus on highly endemic
areas and their outcomes should be considered while updating a national treatment
policy.
11. Case management practices should be part of a national strategy on Information,
Education, and Communication.
12. Pharmacovigilance system which will allow improvement in knowledge of drug safety
and increase the ability to detect rare side effects of primaquine should be set up,
initially in public referral hospitals and other public health facilities.
4.2. Vector Control and Entomological Surveillance
Current Situation & Existing Challenges
Malaria vectors in Afghanistan
An. superpictus Grassi was the first species identified in the country. Larvae of the species were
collected from Northern parts of Afghanistan in 1947. In latter surveys, more culicine mosquitoes
were identified from other areas of the country. A checklist of Anophelines of Afghanistan
reported 21 Anopheles species in the country (Ward 1972). Historically, An. superpictus used to
be the main malaria vector in Afghanistan. However, after successful completion of the trials of
DDT application in rural areas of Afghanistan followed by nationwide spraying campaigns, it had
been almost eradicated by 1970, but replaced by An. stephensi and An. culicifacies, which had
become resistant to DDT in the East and South of Afghanistan, and by the outdoor resting An.
hyrcanus and An. pulcherrimus in the problematic rice-growing areas in the North of the
country (Kolaczinski, Graham et al.). The earlier success in controlling P. falciparum malaria was

43
because of the use of DDT against malaria vectors, when the freshwater An. superpictus was
suppressed. P. vivax malaria remained highly endemic and is associated with rice-growing areas,
where it is transmitted by the endophilic and exophilic rice-field breeders, An. pulcherrimus and
An. hyrcanus (Faulde, Hoffmann et al. 2007).
Today, the main malaria vectors in Afghanistan are An. stephensi and A.n culicifacies in the eastern
parts of the country from where most malaria cases are reported including Nangarhar, Kunar and
Laghman. An. superpictus in Balkh and Herat, An. hyrcanus, and An. pulchrimus in Kunduz and
Badakshan are playing the secondary role (Rowland, Mohammed et al. 2002). A recent survey
highlighted the diverse distribution of mosquitoes in Afghanistan: An. superpictus in Balkh and
Herat, with a minority of An. stephensi. An. pulcherrimus, An. hycranus, and An. stephensi in
Badakshan and Kunduz including An. superpictus in the latter province, An. stephensi, An.
subpictus, An. splendidus, and An. culcifacies in Nangarchar. During the rainy months, small
collections of water on flat land, hoof prints, ponds, pit burrows, small canals and others exposed
to sunlight formed suitable breeding habitats for An. stephensi. An. superpictus was found to breed
commonly in canals. The study positively incriminated An. stephansi as the predominant vector,
exhibiting strong zoophilic behaviour, with a strong presence in animal sheds than in human
habitations. An. pulcherrimus was found to be mostly an outdoor feeder and its peak of activity
was before midnight. (Rowland, Mohammed et al. 2002; Barwa 2011; MoPH 2014). Distribution
of different species of Anopheles in Afghanistan is summarized in Figure 2 (Safi, Hameed et al.
2009). Recent efforts to improve data on vectors and vector control have enhanced knowledge of
the vector bionomics in Afghanistan. A survey conducted in 2010 highlighted the diverse
distribution of mosquitoes (incrimination of vectors unconfirmed) amongst the entomological
sentinel sites in Afghanistan: An. superpictus in Balkh and Herat, An. pulcherrimus, An. hycranus
and An. superpictus in Kunduz and Badakshan, An. stephensi, An. subpictus and An. culcifacies in
Nangarhar (MoPH 2013).
Strategy for Vector Control and its Coordination The Vector-Borne Disease Task Force coordinates and oversees the strategy for implementation
of vector control. The taskforce is chaired by the NMLCP/MoPH, with representation from
partners i.e., WHO, BPHS implementing NGOs and perhaps major donors’ representatives
(USAID, EC, WB). Potentially important inter sectorial partners are: the Ministry of Education,
the Ministry of Information, the Chamber of Commerce, the Ministry of Finance, and the Ministry
of Agriculture. Provincial Malaria Task Forces would be mandated the responsibility of
implementing the operational aspects of the LLINs strategy.
In summary, the main intervention for malaria vector control is LLINs. Other vector control
strategic approaches (e.g. in elimination-oriented areas in the North) include additional
components (e.g. environmental management, larviciding, IRS, livestock sponging). IRS as
malaria vector control is only recommended for controlling malaria epidemics and outbreaks. Anti-
larval measures (temephos) is considered when house spraying is impractical around urban areas
or when there are limited, recognizable and accessible numbers of breeding sites making these
larval source management interventions more cost effective and time efficient. However, these
require some additional evidence of effectiveness through operational research. IVM strategies
and its framework needed for coordination and legislation have been put in place (MoPH 2013).

44
However, if elimination is on the national health and development agenda, IRS, LLINs, source
reduction and larviciding should be considered and planned for (Enayati, Lines et al. 2009).
As insecticide resistance in the main malaria vectors in Afghanistan is evident, implementation of
the IVM strategies in vector control including larval source management (community participation
is helpful here), larviciding (using temephos and/or BTi), using alternative insecticide(s) for IRS,
and implementing insecticide resistance management strategies are highly recommended.
Based on the National Malaria Strategic Plan 2013-1017, strategies have been put in place to make
sure that IVM components are strengthened and operational through regular meetings of IVM
steering committee, establishment of subnational IVM steering committee, introducing pesticide
legislation and monitoring of public health pesticide usage and training for farmers in the
community regarding vector control and use of pesticide jointly with IVM member ministries,
especially Ministry of Agriculture (MoPH 2013). Also as LLINs distribution has been the mainstay
of malaria vector control, mechanisms for ensuring their adequate distribution and proper
utilization were envisaged including: provision and house to house free distribution of LLINs in
strata one and two districts, (at least 85% coverage), community awareness regarding proper usage
of LLINs, regular monitoring of LLINs supply and distribution procedure, susceptibility test of
LLINs at field level (PMLCP), quality test of LLINs by WHOPES recommended lab to comply
WHOPES specification, conduct LLINs utilization survey and provision of LLINs for replacement
of distributed LLINs after three year of distribution (MoPH 2013).
Long Lasting Insecticidal Nets
According to the Basic Package of Health Services for Afghanistan 2009, Insecticide-treated
mosquito nets (based on availability and seasonal variations) would be promoted and distributed
in all levels of health system including HPs, HSCs, BHCs, MPHSs, CHC and DHs (MoPH 2009).
Also, based on the malaria strategic plan 2013-2017, distribution of LLIN to every 2 persons in
districts of the strata 1 and 2, and also to pregnant women in the rest of the strata were the envisaged
control measure. According to the plan, the coverage of the LLINs to everyone in the strata 1 and
2 should be more than 90%, and 85% for pregnant women in the rest of the strata (MoPH 2013).
LLIN distribution mechanisms
MoPH has adopted a revised strategy for insecticide treated nets in 2009, to focus on free
distribution of LLINs to attain rapid high coverage in malaria target areas (Strata 1 and 2
provinces). An estimated 7.5 million nets would be required to cover the entire at-risk population
if 2 people sleep under each net (strata one and two districts). When accounting for the three-year
life-span of LLINs and a population growth rate of 1.9%, 18 million LLINs were needed till 2017
to achieve at least 85% coverage of these populations, in line with national targets (MoPH 2013).
A phased implementation through house to house distribution of LLINs and distribution to
pregnant women through ANC clinic in strata 1 and 2 accompanied by intensive community
awareness program continue to provide the desired coverage. Security, logistics and geographical
barriers were big challenges for house to house LLINs distribution. To overcome these challenges
the program involved community and local partners in the process of LLINs distribution.
Communities and local partners engaged to assist with security, monitoring, and logistics and
supply in their local areas. The commercial private sector provided an alternative system for
efficient distribution of nets in towns and cities and in insecure areas where access by government

45
officials and NGO workers is difficult and restricted. This would be conducted through service
contracts with local businesses to distribute the LLINs for free to households (MoPH 2013).
Coverage of LLIN
According to the NMSP 2013-1017, the target coverage of LLINs was set to be 90% by 2016.
Based on MISs (MISs 2008, 2011 and 2014), household ownership of LLINs increased from 10%
in 2008 to 20% in 2011 and 40% in 2014. The coverage in stratum 1 was 43% in 2011. In 2014,
2015 and 2016, about 4,580,000 LLINs were distributed in strata 1 and 2, and also through ANC
throughout the country. However, due to the inconsistency in data, the true picture of the LLIN
coverage can not be calculated. Having said that, as the LLINs distributed before 2014 would lose
their effectiveness by the end of 2016, the total number of LLINs in use in Afghanistan are those
distributed in 2014 (3.8 million), in 2015 (80,000) and in 2016 (700,000), would be about 4.6
million. The number of populations in the strata 1 and 2 are about 15,000,000 (MoPH 2013), and
considering one LLIN for every 2 people (based on national malaria strategic plan 2013-2017
(MoPH 2013), the present coverage of LLINs is about 61%. Therefore, distribution of 2.15 million
LLINs are required for 90% coverage of 15,000,000 people of the strata 1 and 2. However, it must
be considered that 2016 is coming to its end and by 2017, all the LLINs distributed in 2014 would
lose their effectiveness, therefore to reach a coverage of 90% in 2017, about 7 million LLINs is
required (MoPH 2013). Overall net ownership was higher in rural residences and high risk malaria
strata. Female headed households had higher ownership of ITNs and LLINs. Balkh and Khost
Provinces had the highest and lowest ownership of ITNs 41.7% and 10.3% respectively. High
ownership of LLINs was recorded in Laghman (92.4%) and Paktya (83.8%) (MoPH 2008; MoPH
2011; MoPH 2014). To compensate for the WHO standard of one LLIN per 1.8 people (Kilian,
Boulay et al. 2010, WHO 2014) and also the underestimation of the true number of population as
well as the population growth, an increase of 20% in the procurement and distribution of LLINs is
recommended.
LLINs utilization The proportion of people sleeping under LLINs was 2% in 2008, 14% in 2011 and 16.7% in 2014.
In detailes, based on MIS 2014, sleeping under LLINs last night in households with at least one
net was 54% in 2011 and 38.2% in 2014, sleeping under LLINs last night of children under 5
years of age was 19.4% in 2011 and 43.6% in 2014, sleeping under LLINs last night of pregnant
woman was 19.2% in 2011 and 23.6% in 2014. The proportion of people sleeping under an LLIN
the night before slightly increased from 14% to 17% between 2011 and 2014, and in households
with at least one LLIN decreased from 54% to 38% (MoPH 2014). About 82% of the LLINs in
the studied areas were of acceptable quality (MoPH 2014).
Quality control of PermaNet 2.0:
Twelve samples 001 to 012 from the batches 1280 13, 1281 13, 1283 13 and 1285 13 of PermaNet
2.0 fully comply with the requirements of the WHO specification 333/LN/1 (July 2013) for
appearance, deltamethrin content, deltamethrin wash resistance index, netting mesh size,
dimensional stability to washing and bursting strength. More than 50% of the nets were aged less
than 6 months and also about 80% of the households acquired the nets from either NGOs or
through campaign (MoPH 2014).

46
LLIN chemical analyses
Assays were conducted using HPLC at a WHO collaboration center in India and the concentration
of insecticides in LLINs was in compliance with the product specifications for each individual
LLIN (MoPH 2015).
Indoor Residual Spraying (IRS)
Based on the NMSP 2013-1017, the IRS is used as vector control measure only for outbreaks
control, also as focal use in the elimination areas to control active foci. In 2015, NMLCP with
support of partners implemented IRS with bendiocarb in response to the P. vivax malaria outbreaks
occurred in eastern Provinces (Nangarhar, Kunar and Laghman) and P. falciparum malaria
outbreak which occurred in Taskhan district of Badakhshan Province (MoPH 2015). Based on the
field visits and reports from provinces involving outbreaks, this strategy has not been practiced
much, hence, the increasing epidemics in Eastern Provinces of Laghman, Kunar and Nangarhar.
Integrated Vector Management (IVM) In 2015 NMLCP developed the National IVM strategy with the technical support from WHO
EMRO. A workshop was conducted with the participation of IVM steering committee
representing different line ministries and partner organizations - Ministries of Agriculture,
Environmental Health Directorate (Municipality), Women’s Affairs, Water and Power, Haj and
Religious Affairs, Education, Rural and Rehabilitation, Environmental Health Directorate
(MoPH), National Environmental Protection Agency and Provincial Malaria Program Managers.
During this workshop draft VCNA report comprising vector control needs assessment for all vector
borne diseases, including malaria was finalized. Then the IVM as well as IRM strategies for
Afghanistan developed (MoPH 2015).
An IVM steering committee has been established, comprising of members from key line ministries
such as agriculture, water and power and environmental health agencies. The committee provide
a consultative forum that can effectively promote cost efficient, effective, ecologically safe and
sustainable interventions for vector borne disease control in Afghanistan. Efforts are geared
towards establishing a public health pesticide registration scheme, which strengthens the
institutional and legal framework for public health pesticide legislation in the country. A pesticide
registration working group will make the necessary recommendations to ensure adequate control
over and sale of public health pesticides, including introducing pesticide legislation and monitoring
of public health pesticide usage (MoPH 2015).
Sentinel sites for vector surveillance
Entomological sentinel sites were established in 3 additional provinces (Balkh, Badakshan, and
Herat) to increase the total number to 5 (there are sites already established in Kunduz and
Nangarhar) for systematic collation, analysis and interpretation of vector related parameters to
allow for improved planning, implementation and evaluation of disease vector control
interventions. The plan was to collect specific entomological parameters (human blood index,
human biting rate, vector density, and vector behaviour and insecticide susceptibility status) at
these sites. Insectaries in Kabul, Jalalabad, and Kunduz are used for conducting operational
research, and each insectary is run by an entomologist. It is planned to collect mosquito specimens
pyrethrum spray catches, exit window traps and light traps from cattle sheds and households, and
identified morphologically by field personnel in their respective districts using a standardized

47
identification key verified by sending random sub-samples to experienced entomology staff at
NMLCP in Kabul. Dissections to determine parity rates and mosquito age grading are also planned
to be performed bimonthly in the three provinces at insectary facilities (i.e., Kunduz, Nangarhar
and Kabul). The central entomology team was planned to make bimonthly visits to assess the parity
rates in provinces without insectaries. Sub-samples of mosquitoes collected bimonthly from the
four collection methods performed in Kabul, Kunduz and Nangarhar were planned to be analyzed
using ELISA to detect Plasmodium presence and blood-meal analysis. Mosquitoes were going to
be collected and reared to adults in selected provinces, to be tested for resistance to four classes of
insecticides (i.e., organochlorine, carbamate, organophosphate and pyrethroids) following
standard WHO guidelines. Insecticide resistance testing were going to be conducted once annually
in each province. Additional resistance analysis were also planned to follow susceptibility tests
(MoPH 2013). However, the desk and field review performed during the national malaria program
review did not reflect all the entomological surveillance activities mentioned above.
Many attempts have been made in vector surveillance in Afghanistan. In a study in 2008, four
sampling methods were used to collect mosquitoes (MoPH 2013):
Space spraying: A non-persistent insecticide was sprayed in the main sleeping room of
houses and animal sheds at dawn.
Cattle baited net catches: A big animal net was used to collect mosquitoes. Two cows were
kept under the net over a night. The collection of mosquitoes was conducted for 12 hours,
over a night. Live samples were collected for later use in species identification.
CDC light-traps: CDC light traps were hung inside sleeping rooms, in animal sheds and
outside the compound from dusk-dawn. Samples were collected after dawn for later use
in sporozoite analysis and species identification.
Larval sampling: Mosquito breeding sites in each ecological zone were examined by field
teams. Those found to have Anopheles larvae were included in the survey. Anopheles
larvae collected from each site and bred to adulthood for later insecticide resistance testing.
Insecticide resistance
NMLCP with the assistance of WHO and HealthNet TPO conducted the country’s first
comprehensive assessment on the status of vector susceptibility in 2010. The survey examined the
susceptibility of wild caught anopheles to 3 classes of insecticides: Pyrethroid, carbamate and
organochlorines in 5 provinces. The survey observed reduced susceptibility to all 3 classes of
insecticides in Afghanistan, originating mainly in the Eastern Region (Nangarhar). Intense efforts
to preserve insecticide susceptibility and deescalate the evolution of resistance is needed to avoid
reduction in the effective lifespan of any malaria intervention (Barwa 2011; MoPH 2013). In 2011,
76 susceptibility teste have been performed on different Anopheles species in Provinces of
Badakshan, Takhar, Herat, Kunduz and Nangarhar, the results of which are summarized in Table
4. The results clearly shows reduced susceptibility to pyrethroids in Anopheline mosquitoes in the
provinces (Ahmadhi, Zahid Safi et al. 2015).

48
Table 4: Results of susceptibility bioassays on adult Anopheles in Badakshan, Takhar, Herat,
Kunduz and Nangarhar, 2011
As per the plan of NMLCP, susceptibility bioassays have been performed in 2014 on the main
Anopheles vector species of malaria against all four classes of insecticides in 5 provinces. Analysis
of the mortality rates has revealed the presence of resistance to the 4 classes of insecticides in
Nangarhar, Kunar, Ghazni and Laghman where An. stephensi was the dominant species found. An.
superpictus in Badakhshan province is susceptible to all classes of insecticides except for
deltamethrin for which resistance was observed. Kdr genotyping of An. stephensi mosquitoes
revealed the presence of kdr mutations (L1014S and L1014F) with a higher frequency of the
L1014S form. As it can be seen in the following figure, the main Anopheles species in high risk
areas are resistant to some insecticides including and most importantly deltamethrin, the only
pyrethroid used in LLINs (Ahmad, Buhler et al. 2016).
Another study on insecticide resistance and susceptibility was performed in six provinces
(Nangarhar, Kunar, Laghman, Herar, Takhar and Badakhshan) from August to October 2015. A
total of 144 susceptibility tests (including controls) were conducted using 5% malathion, 0.05%
deltamethrin, 0.75% permethrin, and 0.1% bendiocarb. Dominant species tested were An.
stephensi in Kunar, Laghman and Nangarhar, An. pulcherrimus from Badakhshan and Takhar and
An. superpictus from Herat. The mortality for deltamethrin was 100%, 99%, 100%, 85% and 95%
for mosquitoes collected from Herat, Takhar, Badakshan, Kunar and Nangarhar respectively.
However, these results contradict with the study conducted in 2014 (HealthNet 2015).
Although there is evidence of insecticide resistance emerging in Afghanistan, it is unclear what
the epidemiological impact will be on malaria situation. Resistance management strategies should
be put in place at the early stages of resistance development, when it is rare rather than when it
has become widespread. An integral component of a basic entomological monitoring programme
is monitoring insecticide resistance. To preserve the effectiveness of malaria vector control
interventions further investigations are needed to confirm physiological insecticide resistance
mechanisms (metabolic and target site insensitivity), gene frequency, distribution and strength of
resistance conferred by genes. To bolster local capacity, technical experts will provide necessary
support, training and mentoring of local laboratory staff to develop much needed molecular
diagnostic skills. Susceptible and resistant specimens following susceptibility tests will be assayed

49
for target site modification using allele specific PCR diagnostic kits designed for knock down
resistance mechanisms. Biochemical assays will be used to identify biochemical mechanisms
involved and quantify levels of monoxygenases, esterase and Glutathione-S transferases.
It should be noted that higher confidence is in the data of susceptibility bioassays performed in
2014 on mosquitoes, as the tests were carried out by expert members of staff, performed in a better
environmental condition, the data is in accord with other rounds of bioassays, the results were
verified and supported by molecular analysis of kdr genotype (with frequency of about 11%)
(Ahmad, Buhler et al. 2016) as well as further analysis by biochemical assays of the enzymes
involved in insecticide resistance including alfa- and beta-esterases, pNPA, glutathione S-
transferases and cytochrome P450 (a difference in enzyme ratios of about 2-fold when compared
with those in the susceptible strain).
Cone assays on LLIN
Long lasting insecticide treated nets are the intervention of choice for malaria control in
Afghanistan thus regular bioassays are mandatory to check the efficacy of insecticide. NMLCP
as part of its planned activity in 2013 and 2016 conducted bioassays of the LLINs distributed in
the past two years. The nets were collected from 4 Provinces of Nangarhar, Kunar, Khust and
Kunduz. The bioassay tests were conducted using WHO standard kit and guidelines. The
knockdown rates of the tested mosquitoes were 98.6%, 95.7%, 87% and 85.6% for Khost, Kunduz,
Kunar and Nangarhar respectively. The mortality rates of the tested mosquitoes to LLINs were
92.8%, 90.8%, 85.5% and 94.5% in Khost, Kunduz, Kunar and Nangarhar respectively (MoPH
2015).
Capacity building in vector control and entomological surveillance
Entomologists and vector control specialists at national level provide evidence on vector
bionomics, behavior and insecticide susceptibility, although the provinces are currently
experiencing a severe shortage of staff. There are two Entomologists (with Master degree in
medical entomology under the WHO fellowship programme) in NMLCP and 9 entomology
technicians and one entomology supervisor at the provincial level. During spraying campaigns,
temporary spray men (50) were hired and trained for IRS operations in three Northeastern
provinces. The provinces have also organized in service training of personnel in vector control
with support from NMLCP; in 2011, 8 staff members were trained on vector control from Kunduz
and Nangarhar provinces. Entomology training for 21 health staff of central and provincial units
of NMLCP was conducted by WHO expert. Staff was trained on vector surveillance, insecticide
resistance monitoring and insecticide resistance management, practical training on sample
collection, vector and entomological surveillance, susceptibility and bioassay test of mosquitos
was also provided. Two senior entomology staff of NMLCP were trained in biochemical analysis
for identification of resistance mechanisms in anopheline mosquitoes in Mazandaran University
of Medical Sciences at Sari, of Iran in December 2015. The purpose of this training was to enable
NMLCP to conduct biochemical analysis of mosquitoes in the country (MoPH 2015).
Conclusions
1. At present, LLINs is a core intervention that is widely used to reduce transmission and
prevent malaria in local communities and high-risk population groups. IRS is now
50
restricted to the control of outbreaks, however, the actual use of IRS is rarely seen in
practice. No other malaria vector control interventions such as source reduction and
larviciding are being presently implemented.
2. Allocation of LLINs is based on the official numbers of country’s population provided by
the National Statistics Services that is not always update and in some provinces seriously
underestimates their actual numbers, so that the number of planned LLINs for distribution
would not cover even half of the population (Nangarhar, as an example).
3. The number of LLINs distributed is always behind the national target. As there are families
with more than 10-15 members, distribution of a maximum of two LLINs for a household
is largely insufficient. Due to discrepancy in the data regarding LLINs distribution, the
actual coverage of LLINs is not possible to estimate.
4. Malaria entomological data is not used along with epidemiological and MHIS data for the
decision making regarding malaria control and elimination. As an example, distribution of
LLINs in a highly-affected province like Nangarhar was started in the middle of
transmission season.
5. PMLCP staff including public health care providers do not seem to have embraced the vital
importance of entomological surveillance in malaria control and elimination. Private sector
providers do not systematically share the information regarding LLINs distribution with
the PMLCP and its entomology department.
6. Number of entomological staff in NMLCP and especially at provincial level (PMLCP) is
none or minimal, and their training on vector control and entomological surveillance is
inadequate.
7. A proper plan for entomological surveillance is not in place. As an important component
of entomological surveillance, insecticide susceptibility status of malaria vectors has been
carried out. However, this monitoring should be conducted under rigorous standards to
ensure the reliability of the results for decision making. Adequate operational research is
not conducted on vector control and entomological surveillance.
Recommendations
1. Various eco-epidemiological types of malaria with different principal and secondary
vectors within the country should be properly defined and technically/operationally
feasible vector control measures/options for different malaria settings based on local
epidemiology should be selected.
2. Achieving and maintaining universal coverage with LLINs to ensure that each household
has sufficient nets in line with WHO standards) and every inhabitant at risk sleeps under a
LLIN every night is critical to reduce transmission in high-transmission settings. In high-
transmission settings, particularly with An. stephensi and An. culicifacies, transmission

51
reduction through universal coverage and usage of LLINs and other sustainable vector
control including protective personal measures should be recommended.
3. National policy and funding for procurement and distribution of LLINs should be adequate
and sufficient to cover all population groups at risk of malaria within the country:
A better estimate of the total populations at provincial, district and lower levels
should be made to calculate the sufficient quantities of LLINs to be procured and
distributed within each province. If the target is one LLIN for 2 people, the
benchmark of a maximum of two LLINs per household should be lifted.
Timely procurement of LLIN should always be a priority so that distribution can
start well before transmission season.
Distribution of LLINs should be coupled with locally appropriate and gender
sensitive IEC/BCC to ensure community participation and correct LLIN usage.
4. It is logical to assume that a combination of different vector control options suiting
Afghanistan’s conditions and responding to local needs and based on Integrated Vector
Management (IVM) principles may compensate for deficiencies of each individual
method:
Vector control options including LLINs, larval source management and larviciding
(temephos and BTi) should be actively promoted through community participation
in high-transmission settings to bring malaria transmission down.
The application of vector control measures and their combinations should be always
guided by consideration of their technical feasibility, operational applicability,
sustainability, and some of them are in need of better QA.
Environmental management (drainage, filling, land levelling, vegetation removal
etc.), which deserves to be used more often by communities for collective
protection from malaria vectors can be recommended, and can be applied in
combination with other vector control measures. An inter-sectorial collaboration is
required for deployment of environmental management at local level.
5. The programme should consider conducting focal IRS in the event of outbreaks and in
areas eligible for elimination where case/focus investigations are in place, and
entomological evidence and other factors indicate that interruption of transmission can be
expected:
Focal IRS should be applied on a strict total coverage of all active foci of malaria,
with a view to interrupting transmission as soon as possible all over the target area.
The choice of insecticide should consider safety, efficacy, cost, availability and
susceptibility of vectors as well as using alternative insecticide(s) for IRS.
To be effective IRS requires careful planning, well-organized operations with
skilled technical staff, very strong supervision and community mobilization to
achieve the high level of IRS coverage to maximize impact of this measure.
The well-defined SOPs should be developed for IRS planning, implementation, and
monitoring.
Malaria entomology and health staff should be trained on IRS to support its
application and monitor quality of IRS operations.

52
6. There is a desperate need for strengthening the entomological component of NMLCP at
central and provincial levels:
The inventory of existing entomology staff and assessment for the staff needed and
relevant posts to be filled at each level should be made.
The entomological capacity of NMLCP should be strengthened. Training should be
“task-oriented” and “problem-solving” and supplemented by regular supervision
and refresher training courses.
A core NMLCP technical group on vector control with a good representation of
competent staff in medical entomology and vector control at provincial level should
be maintained or established to play a greater role in the decision-making process
on malaria control and elimination.
7. The necessary capacity of national malaria programme for entomological surveillance
should be built:
Training on entomological surveillance and its role in malaria control and
elimination should be organized for the NMLCP and PMLCP staff.
SOPs related to entomological monitoring and surveillance should be developed:
Entomological surveillance should include identification of vector species,
monitoring vector behaviors and bionomics, mapping species distribution and
density, identification of host preference, seasonal fluctuation of species, and
assessment of an area’s receptivity.
Entomological surveillance should also be carried out in epidemic-prone areas
based on set outbreak thresholds.
Insecticide resistance is one of the greatest threats to any concerted or prolonged
attempt at malaria transmission control, and monitoring and management of
insecticide resistance should be regularly conducted.
All existing and possible breeding sites of Anopheles mosquitoes should be
properly mapped in relation to active foci of malaria in areas eligible for
elimination.
Considering different malaria transmission settings, an operational plan for
entomological surveillance should be worked out, and adequate training on
entomological surveillance should be conducted to strengthen a national capacity
of entomological services.
8. Vector biology and control research is of particular interest, which has been neglected, but
should be re-considered to make vector control more effective in producing desired results.
National capability/capacity to undertake operational research on issues of direct relevance
to vector control should be strengthened. The following studies can be considered:
KAP studies on barriers for LLINs ownership and utilization.
KAP studies on existing/potential preventive measures.
Technical feasibility and operational applicability of various vector control
measures and their combinations in different malaria settings.
Feeding and resting behaviour of malaria vectors.
Insecticide susceptibility of malaria vectors.
Biochemical/molecular mechanisms of insecticide resistance.

53
Vector control impact assessment.
4.3. Malaria Surveillance
Current Situation & Existing Challenges
A malaria surveillance system consists of the tools, procedures, people and structures that generate
information on malaria cases and deaths, which can be used for planning, monitoring and
evaluating malaria control and elimination programme.
The design of malaria surveillance system depends on the level of malaria transmission, the
implementing strategy and its goal and the resources available to conduct surveillance. In the
control phase, surveillance is based on aggregate numbers, and indicators such as
mortality/morbidity rates, API, incidence of severe/complicated cases, CFR etc. are calculated to
measure the impact of programme malaria interventions (1). In the elimination phase, as a
transmission is progressively reduced, it becomes increasingly possible and necessary to track and
respond to each individual case (2). In the phase of prevention of re-establishment of local
transmission, a priority should be given to the immediate notification of imported cases and the
occurrence of possible introduced because of onward transmission from imported cases and
indigenous cases.
Now, when there are still many cases of malaria and is not possible to investigate and react to each
confirmed case individually – the main objectives of the NMSP, 2013-2017 are to reduce malaria
morbidity by 85% with a priority to high risk districts and malaria mortality to 99% by the end of
2017. In addition, the reduction of P. falciparum incidence to sporadic cases by the end of 2017 is
another objective with a vision to completely interrupt indigenous transmission of P. falciparum
by 2030.
Malaria stratification
Malaria is a complex disease and its distribution in Afghanistan varies largely from place to place,
and is dependent upon a variety of factors related to parasites, vectors and human populations
under different geographical, ecological and socio-economic conditions. Referring to WMR 2015,
24% of Afghan population lives in areas at high risk for malaria, 49% at medium risk and the
remaining 27% live in areas with no risk or very low risk of malaria transmission.
Based on available malaria and environmental data and reflecting a risk of malaria, all districts in
Afghanistan were classified into four main strata with high (2 944 800 people); medium (12 133
500 people), low (5 023 200 people) and very low risk of malaria transmission or its absence in
malaria free areas (4 168 400 people) to provide strategic guidance for planning anti-malaria
interventions. The different district-wise maps are available for P. vivax and P. falciparum.
Case definition:
Although WHO now recommends that all suspected cases of malaria be confirmed with a
diagnostic test (microscopy or RDTs), this is not yet the practice in Afghanistan due to poor access
to diagnostic testing, which, however, has substantially improved in recent years. Thus, it is
necessary to distinguish between suspected malaria cases, presumed cases and confirmed cases:

54
Suspected malaria case: Patient illness is suspected by a health staff/CHWs to be due to
malaria. The criteria for suspected malaria usually include fever or a history of fever, but
the precise criteria are established by NMLCP.
Presumed (not tested) malaria case: In a suspected malaria case, the patient did not
receive a diagnostic test for malaria but was nevertheless treated for malaria. Such cases
have also been referred to as “probable” cases.
Confirmed malaria case: A suspected case of malaria in which malaria parasites have
been demonstrated by microscopy or a RDT, becomes a confirmed case.
As a high proportion of suspected and presumed malaria cases are not due to malaria (3), these
counts do not provide good indicators for malaria surveillance. In Afghanistan, where the majority
(more than 70%) of reported malaria cases are still diagnosed on clinical ground in 2015, the actual
magnitude of the malaria problem cannot be measured properly. Malaria surveillance should
therefore be based on confirmed malaria cases only, and the proportion of malaria cases confirmed
by RDTs and/or microscopy has substantially increased from 14.4% in 2013 to 28.2% in 2015. It
is important to report clinically-suspected and confirmed cases separately as their final values are
not comparable over time.
Malaria cases can be categorized as uncomplicated or severe/complicated. In general, people with
uncomplicated malaria are treated as out-patients, while those with severe/complicated malaria are
managed as in-patients. In the control phase, for surveillance purposes out-patient and in-patient
malaria cases can be considered proxies for uncomplicated and severe/complicated malaria,
respectively.
Routine malaria surveillance
Routine malaria surveillance is presently conducted through HMIS, and malaria reporting from
BPHS and EPHS is integrated with HMIS. Malaria diagnosis and treatment is integrated with
BPHS and EPHS services, malaria diagnosis and treatment are provided from health post level up
to regional hospitals. HMIS collects data on priority disease including malaria in pretested standard
form. The services and interventions that are monitored through the HMIS are limited to those that
focus on the priority target groups and conditions of the BPHS and EPHS.
Standard reporting formats with 102 indicators including 2 related to malaria are processed and
analysed monthly at health facility level and reports to provincial HMIS department. The HMIS
central department analyses the data and shares the analysed data with other departments and
BPHS implementers on quarterly basis.
Sentinel surveillance
The rationale for establishing malaria sentinel sites is to collect additional indicators on malaria at
health facility and community level. Malaria sentinel surveillance is presently conducted through
three types of sentinel sites including 20 sentinel sites to show malaria trend; 2 sentinel sites for
drug efficacy monitoring and 350 DEWS sentinel sites to detect epidemics/outbreaks.
Stakeholders involved in malaria control in Afghanistan are convinced that the use of malaria
sentinel sites would capture programme information that would otherwise be missed by HMIS,
DHS and MIS. The sentinel site data would be useful not only for M&E, but also for assessing

55
malaria mortality and morbidity trends, evaluating the programme effectiveness and determining
the progress towards malaria elimination.
There are sentinel sites identified by MoPH for drug efficacy studies in different malaria strata.
At present, malaria outbreaks detected through DEWS that has around 360 sentinel sites all over
the country. These sentinel sites are based in CHCs and DHs with microscopy facilities. Routine
health facilities data are reported to provincial/central levels on weekly basis. Health facilities of
the BPHS are requested to fill out the malaria weekly charts to assist in malaria surveillance by
tracking malaria trends at local level that can report unusual malaria situations through the DEWS,
BPHS or directly to malaria control programme. The registration book with case records from the
OPD, IPD and laboratory provides detailed information about each malaria case including its
diagnosis and treatment outcomes.
However, there are no clear guidelines on establishing, monitoring and evaluation of malaria
sentinel sites.
Malaria surveillance indicators
Malaria data are currently reported by the Health Management Information System (HMIS) from
BPHS and EPHS include:
Total number of suspected deaths due to malaria.
Total number of blood slides/RDTs taken and examined.
Total number of confirmed cases of P. falciparum and P. vivax by sex and age.
Total number of clinically-suspected and confirmed cases of malaria by sex and age.
Total number of in-patient cases of malaria (not reported as severe/complicated malaria)
Stock out of anti-malaria drugs except Quinine and PQ.
The following malaria surveillance indicators are presently calculated:
Total incidence of confirmed malaria cases as well as separately for P. falciparum (APfI)
and P. vivax (APvI) cases per 1000 population a year.
Total number of clinically-suspected and confirmed cases of malaria per 1000 population
a year.
Total number of deaths due to malaria (malaria mortality) per 100 000 population a year.
SPR by microscopy.
TPR by RDT.
ABER.
To determine malaria specific indicators and to continue to gather the reports from all BPHS/EPHS
and implementing partners, the NMLCP and HMIS taskforce agreed to develop Malaria and
Leishmaniasis Information System which should have standardised registration and reporting
forms on malaria and leishmaniasis to be used by all healthcare providers in the public health
sector. Partial vertical malaria surveillance should be set up for those indicators which are not
captured by the current HMIS. The following indicators to be added into Malaria Information
System (MIS) were proposed by NMLCP:
Number of patients treated with ACT.
Age and gender specific incidence rates.

56
Severe and complicated cases.
Number of cases among pregnant women.
Number of cases confirmed by RDT.
Stock out of all antimalarial drugs.
Data sources and collection
NMLCP relies on a diverse range of sources for provision of data and their reporting mechanisms
which include routine and integrated data from health facilities through HMIS and programmatic
vertical data through NMLCP departments and partners. Various measures have been undertaken
by each reporting entity to ensure a high standard of reporting. The main source of malaria data is
the HMIS. Malaria-related data is collected on monthly basis at provincial level and compiled at
central level, where malaria surveillance indicators are calculated. Some outcome indicators are
collected through MIS. The provincial service delivery reports are the source of information on
malaria and its control, and these reports include:
Malaria case management and treatment based on NTG monthly reports.
Monthly malaria morbidity reports.
Laboratory Quality Assurance report and cross checking of examined slides.
Quarterly supervision and monitoring report.
Malaria routine LLIN delivery reports.
Monthly CBMM reports.
Weekly report from sentinel sites.
Monthly training reports.
Conclusions
1. Based on available malaria and environmental data and reflecting a risk of malaria, all
districts in Afghanistan were classified into four main strata with high, medium, low and
very low risk of malaria transmission or its absence in malaria free areas to provide
strategic guidance for planning anti-malaria interventions. The different district-wise maps
are available for P. vivax and P. falciparum.
2. Routine malaria surveillance is presently conducted through HMIS, and malaria reporting
from BPHS and EPHS is integrated with HMIS. Malaria sentinel surveillance is currently
conducted through three types of sentinel sites to show malaria trend, to monitor drug
efficacy and to detect epidemics/outbreaks.
3. Malaria surveillance is based on aggregate numbers, and indicators such as
mortality/morbidity rates, API, APfI, APvI, SPR, TPR, ABER and others are calculated to
assess the present malaria situation and current trends and measure the impact of
programme malaria interventions.
4. API is best suited to measure the extent of the malaria problem and the impact of
interventions in areas where all or at least much of clinically-suspected cases confirmed by
quality-assured RDTs and/or microscopy. ABER (% of people examined for malaria by
microscopy and/or RDTs) is intended to measure the level of diagnostic surveillance

57
activity per administrative unit. SPR/TPR (% of people found positive for malaria by
microscopy/RDTs) is intended to measure the distribution of malaria infection in the
community over a period of time.
Recommendations
1. Considering the obvious differences and recent changes in malaria situation over space and
time, malaria stratification should be updated and the entire territory of the country should
be sub-divided into three Categories (1) where malaria is still widespread and the primary
objective is to reduce the remaining malaria burden further; (2) where malaria shows a
focal distribution of indigenous cases and which are eligible for malaria elimination and
(3) where all reported cases of malaria have an imported nature, and particular focus should
be placed on maintenance of the results achieved by prevention of re-establishing local
malaria transmission. NMLCP may request WHO to provide the necessary technical
assistance in relation to this task.
2. Based on the 2016 reported API as a primary criterion for selection and other criteria such
as the reported number of malaria cases per health facility; the reported ratio of P.
falciparum to P. vivax; determinants of local epidemiology and degree of development of
health system within a given province, the entire country should be sub-divided into three
distinct Categories, namely:
Category 1 with Provinces that are still in the transmission-reduction phase
where the reported API of 1 or above case per 1000 population at risk, elimination
of malaria does not appear to be feasible at present.
Category 2 with Provinces where the reported API of less than 1 case per 1000
population at risk per year and elimination of malaria supported by other criteria
is technically feasible and operationally applicable.
Category 3 with Provinces that presently free from malaria, prevention of re-
establishment of transmission is recommended.
3. Measuring PPR can be recommended as the Malaria Indicator Survey among children
(juveniles/schoolchildren of 5-9 years old) in high transmission settings of the eastern
provinces. The infant parasite rate of 6-11 months old is of special importance as it is a
good indicator of a recent local transmission of malaria.
4. Along with PPR, the incidence of UM (malaria out-patients) and SCM (malaria in-patients)
as well as SCM/UM ratio and CFR of SCM can be recommended as additional indicators
to measure the malaria burden and impact of control interventions in high transmission
settings, considering that:
from improved coverage of LLINs, a decrease in the incidence of UM and SCM
can be expected;
from improved management of UM, a decrease in the incidence of SCM and the
ratio of SCM to UM can be expected; and

58
from improved management of SCM before and after hospitalization, a decrease
in the CFR of SCM can be expected.
5. The target ABER should be well above 5%, and preferably 10% of the population at risk
for provinces under Category 1, and in the range between 2 and 4% of the population at
risk for provinces under Category 2, which are eligible for malaria elimination. The level
of diagnostic surveillance activity (ABER) and the distribution of malaria infection
(SPR/TPR) should be measured together in each administrative unit.
6. Coordination mechanisms between NMLCP, HMIS, BPHS and DEWS at provincial and
central levels to collect, process, analyse and share malaria-related data should be
improved. The current malaria surveillance should be reinforced to increase coverage and
completeness of reported data from health facilities throughout the entire territory of the
country. Existing database on malaria should be revisited and online reporting mechanism
should be set up.
7. Existing malaria surveillance and information systems should be strengthened to ensure
complete and timely reporting from all health sectors including the public facilities and
private sector, CHWs, military/police health services, and other parties concerned. Case-
based malaria surveillance system in the provinces under Category 1 should be established
and expanded in support of the move towards elimination.
8. A major surveillance paradigm change occurs when the country embarks on elimination:
Malaria must be a notifiable disease, and the country should concentrate on
detecting every symptomatic and asymptomatic infections and reacting to every
confirmed case.
Surveillance activities have to be enhanced so that every focus (village, or sub-
village or working site) with indigenous case(s) of malaria is targeted for action.
A case-based surveillance and response system, preferably based on GIS should be
established initially in priority provinces with low malaria incidence that are
eligible for malaria elimination, and later it should be expanded to other provinces
as appropriate.
9. Specific guidelines and SOPs on malaria surveillance should be developed, and relevant surveillance, databases and quality assurance systems should be set up and training different
categories of health staff should be conducted in the transition phase from control to elimination.
10. To ensure adherence to standard surveillance procedures and practices in line with national
SOPs, malaria control programme staff should lead trainings on surveillance for all
categories of health staff concerned and other partners involved. Such trainings can be
integrated into other malaria trainings if possible.

59
4.4. Epidemic Preparedness and Response (EPR)
Current Situation & Existing Challenges
Outbreaks of malaria of varying magnitudes may occur in areas where the intensity of malaria
transmission has been reduced to a low level because of control activities, but levels of receptivity
and vulnerability remain relatively high. The appearance and explosive development of outbreaks
indicates the failure on the part of national health services to forecast and prevent this kind of
events. The genesis and mechanisms of malaria outbreaks are usually complex and depend on both
qualitative and quantitative relationships between the human host, the parasite and its vector as
well as on the biological, physical, political and economic characteristics of the environment
(Najera J. et. al., 1998)
In most parts of Afghanistan where malaria transmission is unstable with most of the populations
having little or no immunity, malaria outbreaks can represent a major public health problem.
During 2013- 2015 in some districts of the eastern provinces of Nangarhar, Kunar, Laghman and
Badakhshan, malaria outbreaks caused by P. vivax and P. falciparum malaria were reported by
DEWS and Provincial MLCPs and investigated by technical unit staff of NMLCP in collaboration
with partners (see Annexes: Table 5).
Different factors may have contributed to development of these outbreaks, including lack of
effective vector control measures as well as timely diagnosis and adequate treatment of cases,
shortages of primaquine for anti-relapse therapy of P. vivax cases at health facilities, and
insufficient epidemic preparedness. The existing EPR mechanism is inadequate to prevent
outbreaks, and manpower/logistics and the mechanism for their rapid mobilization and deployment
are insufficient to curb the on-going epidemic. Distribution of LLINs was carried out in 2013 in
these areas, and the efficacy of the insecticide treatment in the LLINs might have diminished over
time. The use of LLINs was the only vector control tool.
To contain the reported outbreaks, the following interventions have been applied:
Strengthening case management at health facility and community levels through urgent
training of health staff in diagnosis, and ensuring the availability of RDTs at lower health
facility and community levels;
Introducing ACD to promptly diagnose and early treat cases of malaria;
Enhancing public awareness by using IEC materials on early treatment seeking behaviour
and controlling vector breeding sites;
Appling IRS of dwellings and distributing LLINs in the affected villages;
Regular monitoring of the malaria trend to assess the effectiveness of containment
interventions.
Ministry of Public Health with collaboration of its partners is responsible for all types of
emergency situations including malaria epidemics. EPR is one of the strategic directions of the
NMSP 2013-2017, which was emphasized on early detection and rapid response to malaria
epidemic. It stated that 85% of malaria epidemics should be detected and contained within two-
60
weeks of onset (National Strategic Plan for Malaria Control and Elimination 2013-2017,
MoPH/NMLCP, 2013).
National EPR guidelines have been prepared in 2010 to address epidemics detection, investigation
and control. EPR teams were trained and established at central level and 29 provinces. Along with
NMLCP other stockholders such as DEWS, HMIS, PPHD and BPHS are involved in epidemic
control.
At present, malaria outbreaks detected through DEWS that has around 360 sentinel sites all over
the country. These sentinel sites are based in CHCs and DHs with microscopy facilities. Routine
health facilities data are reported to provincial/central levels on weekly basis. In case of an unusual
increase in the number of cases, the health staff should inform malaria provincial unit immediately
and provincial EPR team should investigate it per approved EPR guidelines.
Based on local epidemiological situation of the affected area, characteristics of the epidemic and
availability of resources, epidemic control measures are selected. Epidemic response should be
within one week of its onset. The following containment measures are recommended:
Ensure that all health staff are aware of the outbreak and involved in its containment, and
maintain daily communication at all levels and among all concerned;
Ensure adequate stock of drugs and diagnostics supplies;
Enhance diagnostic and treatment services with support from mobile teams;
Consider the use of mobile clinics in remote or underserved areas;
Introduce active case detection in areas affected by the outbreak;
Enhance quality assurance of diagnosis through cross-checking of slides and training of
technicians where required;
Consider a directly observed treatment by health workers;
Improve local capacity for management of severe and complicated malaria;
Conduct intensive IEC campaigns;
Apply IVM including IRS, larviciding, chador impregnation and live-stock sponging and
consider targeted distribution of LLINs;
Ensure that stakeholders and policy makers are informed of the epidemic and assisted in
resource mobilisation.
Conclusions
At present, MoPH in collaboration with its partners is responsible for all types of emergency
situations including malaria epidemics. EPR is one of the strategic directions of the NMSP 2013-
2017, which was emphasized on early detection and rapid response to malaria epidemic. Malaria
outbreaks are detected through functional DEWS which is covering the entire country. However,
the existing epidemic preparedness and response mechanism is obviously not adequate to prevent
and contain ongoing outbreaks/epidemic of malaria in the eastern provinces. The existing EPR
should be enhanced considering that:
1. There is no a built-in mechanism for forecasting and early warning for malaria epidemics.

61
There is no link between malaria control program and hydro-metrology and other relevant
departments regarding forecasting.
2. The existing stratification is lacking to identify properly epidemic-prone areas within the
country.
3. The existing epidemic monitoring system and response mechanism are in place, but should
be strengthened.
4. The existing epidemic prevention mechanism is insufficient, and epidemic preparedness is
lacking.
5. EPR teams were established at central and provincial levels and system for epidemic
detection and investigation is in place, but are not fully functional especially at provincial
and lower levels.
6. There is no specific government budget for malaria epidemic detection and control, and
EPR is mainly depending on donor support.
Recommendations
1. The existing EPR guidelines should be revised to include the forecasting and early warning
mechanisms.
2. Epidemic-prone situations should be identified during the process of stratification of the
malaria problem into discrete areas and populations based on various data from health and
non-health sectors. Further analysis of epidemic-prone situations can define major
precipitating factors which cause epidemics so that in the future they can be monitored for
epidemic prediction purposes.
3. An outbreak monitoring system should constitute a part of national malaria
epidemiological surveillance system. Early signs of an impending epidemic related either
to a particular area or population group should be identified and tracked. The recognition
of early alarm signals heavily depends upon the adequacy of the variables chosen. Selection
of the set of variables and the range of their numerical values is determined by type of the
area regarding the local epidemiology, epidemic risk factors, existing health service
infrastructure, time lag in communication, etc.
4. Control of a malaria outbreak should involve an adequate package of measures aimed at
(1) minimizing clinical consequences; (2) containing transmission, if possible; (3)
preventing further spread of the epidemic; and (4) improving emergency preparedness to
prevent future epidemics. The first two objectives require the application, as soon as
possible, of effective containment measures, while the last two involve assessment of risk
and the application of preventive measures. IRS, if feasible, continues to be the most
effective measure to swiftly contain malaria transmission. IRS, to be fully effective, should
achieve total coverage of all houses within the affected area based on adequate provision

62
of insecticides, spraying equipment, transport and deployment of vector control
programme staff.
5. It is expected that emergency situations within epidemic-prone areas or population groups
in Afghanistan are likely occur. Prevention of outbreaks and their further spread and
recurrence in subsequent years requires the application of vector control methods including
IRS if technically feasible and operationally applicable. In epidemic-prone areas, where
LLINs and other sustainable vector control measures are already used may be the most
effective way of reducing transmission and preventing epidemic spread to new areas or
resurgence in subsequent years.
6. Preparedness for malaria outbreaks should be based on an understanding of the
epidemiology of malaria and epidemic risk factors. The more complete that understanding
and the more developed the information system and the monitoring of risk factors, the
higher is the level of preparedness, the more accurate the forecasting and the more adequate
the response. Malaria preparedness should be strengthened by identifying resources
(appropriate manpower, supplies, equipment and logistical arrangements including
administrative and technical procedures, responsibilities of health and other sectors) and
the required mechanisms for their rapid mobilization and deployment at provincial and
lower levels.
7. The NMLCP capacity to judge the abnormality of the situation, decide on the
epidemiological diagnosis of outbreaks/epidemic and have the authority to plan and
implement epidemic containment measures should be strengthened, particularly at
provincial level. While various levels of peripheral health services as well as CHWs should
be encouraged to report early any unusual rise in numbers of malaria cases and associated
mortality, it is also important that there is adequate expertise to sort out the information
from the periphery and distinguish between true and false alarm signals at the provincial
level.
8. The government allocations for epidemic preparedness and response should be considered.
4.5. Programme Management
Current Situation & Existing Challenges
Government of Islamic Republic of Afghanistan is committed to control and eliminate malaria
from this country. The goal of national malaria control programme is to contribute to the
improvement of the health status in Afghanistan through the reduction of morbidity and mortality
associated with malaria by reducing morbidity and mortality to 85% and 99% respectively by
2017.
NMLCP with its nine different departments under the leadership of MoPH coordinates the PMLCP
by providing managerial guidance and technical assistance in case management, disease
prevention, malaria surveillance, capacity building, community mobilization, operational research
and monitoring and evaluation. However, almost all the departments of NMLCP obviously require

63
more manpower and financial resources to make the programme more productive and fully
functional at all levels. NMLCP coordinates malaria control and elimination activities with
different local and international partners including BPHS implementers, UNDP, WHO, non-
governmental organizations and private health sectors. Country Coordination Mechanism, as a
body of members drawn from public health agencies, international institutions and donors, works
as oversight coordination committee to provide guidance and strategic direction of NMLCP and
to ensure its accountability. Malaria elimination to be successful requires concerted efforts from
various health and non-health sectors including health, education, information and
communication, finance and agriculture etc.
An existing national malaria strategic plan, 2013-2017 is used to guide stakeholders concerned on
programme goal, objectives, approaches and interventions that are uniformly undertaken for
effective programme management. Existing strategic approaches and specific/cross-cutting
interventions of the NMLCP should be re-considered and specified in detail to address the
emerging elimination challenges. Evidence should be provided that the interruption of
transmission can be achieved by the proposed package of interventions, and such evidence can be
obtained from the experience of pilot projects within the country or from the experience in
neighbouring countries. Other available documents include: a national treatment policy/protocol
for malaria; IEC and advocacy documents; action plan with milestones/targets to undertake social
mobilization in the community and procurement plan to follow standard guidelines for transparent
and accountable procurement.
To achieve the stated goals and objectives, the roles and responsibilities of departments of the
NMLCP should be revisited to ensure their proper guidance, continuous coordination and
synchronization of their work that does not seem to be happening at present. Engagement of the
country in malaria elimination increases the need for leadership, and this issue is a crucial element
for success of the elimination campaign.
There is a lack of competent senior programme staff in most programme departments, particularly
at provincial level at present. It has been noted that many of the professional and technical staff of
NMLCP has frequently moved out to search for a better job, and NMLCP should find the
way/incentives to retain the programme staff. Assessment of the NMLCP’s capacity in terms of
human resources available at central and provincial levels should be carried out to make the
inventory of programme staff, and on this basis to decide on the number and categories of
professional personnel to be trained or re-trained.
A considerable effort should be taken to increase human resources and train, motivate and sustain
health staff including the programme personnel at all levels until malaria eliminated across the
entire country. Although training for improvement of staff skills and competence can take place in
the country, some staff may require additional training abroad. Newly recruited programme
personnel need to be trained, and basic training should be supplemented by regular supervision
and refresher training courses. The core technical groups of professionals adequately trained on
malaria with the necessary epidemiological expertise should be maintained within national
programme, particularly at provincial level.

64
From the provincial MLCP managers and field observations have also underscored the importance
to hold regular regional coordination meetings either at regional or central level. Holding such
meeting in the malaria-affected regions could enable the programme managers from central level
to understand better malaria-related situations, problems, constraints and gaps that exist at the
regional and lower levels and to improve support for programme implementation. NMLCP should
pay special attention to field work for the central- and provincial-level programme staff aimed at
providing the necessary technical guidance and improving collaboration with BPHS implementers,
private health sector providers and other involved in programme implementation.
Since October 2015, UNDP Afghanistan has been awarded the contract as its PR to manage
national malaria control programme under NFM of GF. Before October 2015, NMLCP, HNTPO
and BRAC jointly as principal recipient led the malaria control programme from Jan 2010 to
February 2015 as awarded PR and then next three months till May 2015 as Non-Cost Extension
contractor. Currently, UNDP is the principal recipient for the malaria control programme in
Afghanistan under New Funding Model with the overall responsibility to manage the fund.
Procurement of supplies and drugs, commodities and services, training, research and finance are
the responsibilities of UNDP. It coordinates with WHO for technical issues and directly with
NMLCP and BPHS implementers for programme implementation.
The programme’s budget should include adequate reserve provisions to meet possible problems
that are liable to occur during its implementation due to security constraints in many of the
provinces where malaria burden is high, particularly in the bordering provinces along Pakistan;
insufficient numbers of technical skilled manpower and a high demand for local and international
trainings. There have not been such allocations in the budget for this type of training abroad.
Conclusions
1. A national malaria strategic plan, 2013-2017 is used to guide stakeholders concerned on
programme goal, objectives, approaches and interventions, however, its existing strategic
approaches and specific/cross-cutting interventions should be revised and specified in
detail to address the emerging elimination challenges
2. Almost all the departments of NMLCP are lacking manpower, financial resources and
coordination to make the programme more productive and fully functional, particularly at
provincial level at present. It has been noted that many of the professional and technical
staff of NMLCP have frequently moved out to search for a better job.
3. There are insufficient capacities/capabilities of the core technical groups, particularly at
provincial level to provide adequate guidance and assistance in planning, implementation,
monitoring and evaluation of malaria control and elimination activities.
4. There are a lack of coordination and no regular meetings between central programme and
provincial teams.
5. The programme’s budget has no adequate reserve provisions to meet possible problems
that are liable to occur during its implementation.

65
Recommendations
1. The government and MoPH should remain fully committed to malaria, and to make all
possible efforts required to achieve a greater impact on malaria situation in the country.
2. Emphasizing the need to address the emerging elimination and remaining challenges,
the current NMSP/MEP,2013-2017 should be revised to reflect changes in programme
priorities, targets, strategic approaches and key interventions, considering that malaria
elimination in Afghanistan should be carried out in a phased manner by parasite species
with a priority to be given to elimination of P. falciparum and by geographical area
(sub-national elimination) with different parts of the county being at different
programme phases simultaneously. NMLCP may request WHO to provide the
necessary technical assistance in relation to this task.
3. For relatively large and heterogeneous country like Afghanistan, the emphasis should
be given to assessing major administrative units, typically Provinces. Some provinces
have already become eligible for elimination. If their health systems are strong enough,
it is rational to pilot surveillance and other elimination activities focusing on setting up
adequate surveillance, databases and quality assurance systems, preparing and testing
relevant SOPs and training for different categories of health staff.
4. To ensure achieving programme objectives and targets the roles and responsibilities of
departments of the NMLCP should be revisited to ensure their proper guidance,
continuous coordination and synchronization of their work.
5. Coordination meetings with all stakeholders to guide planning, implementation and
evaluation of programme interventions on malaria should be held at regular intervals.
6. Assessment of the NMLCP’s capacity in terms of human resources available at central
and provincial levels should be carried out to make the inventory of programme staff,
and on this basis to decide on the number and categories of professional personnel to
be trained or re-trained.
7. The core technical groups of professionals adequately trained on malaria with the
necessary epidemiological expertise should be maintained/established, particularly at
provincial level.
8. Engagement of the country in malaria elimination increases the need for programme
leadership, and this issue that is a crucial element for success of the elimination
campaign should be seriously considered.
9. A considerable effort should be taken to increase human resources and train, motivate
and sustain health staff including the programme personnel at all levels until malaria
eliminated across the entire country.

66
10. NMLCP should increase interactive communication between NMLCP and PMLCP to
improve the programme performance and quality; to provide the necessary support; to
increase motivation and to facilitate handling the field issues. Holding regular quarterly
regional meetings between NMLCP and PMLCP should be conducted to improve
coordination.
11. Adequate legislative and administrative provisions to govern the elimination
programme should be considered to cover the programme’s requirements, including
the right of entry by malaria staff with the purpose of investigation or spraying,
mandatory notification and reporting of malaria cases etc.
12. Regulation of the private sector as a major elimination challenge in Afghanistan should
be properly addressed.
13. The programme’s budget should be sufficient and realistic, including adequate reserve
provisions to meet possible problems that are liable to occur during its implementation,
and the source(s) of funds should be clearly indicated.
4.6. Procurement Supply Management (PSM)
Current Situation & Existing Challenges
Procurement supply management of Global Fund Malaria Programme in Afghanistan is
implemented by UNDP, Afghanistan. UNDP collaborates with NMLCP for quantification and
specification. All other procedures are conducted by UNDP office.
Existing PSM system under Global Fund in Afghanistan has a procurement action plan which is
strictly managed and maintained by UNDP. Under current malaria grant major commodities that
are planned for procurement are LLINs, RDTs, anti-malarial drugs, laboratory equipment and
supplies, computers, printers, furniture and other IT equipment. Procurement action plan
specifically specifies each product with unit and exact quantification that should be procured.
Product specification with unit and exact quantity helps to determine price of the goods that should
be procured. Procurement action plan also has date when the goods will be received in the
warehouse on arrival in the country. Additionally, tentative customs clearance dates are marked
so that advance information and clearance can be delivered to the custom. Modes of transport, lead
time day and procurement partners are other important elements which are also planned in the
procurement action plan. Responsible person specified for each items of procurement keeps track
on the date of delivery. Once the goods are received, Programme and PSM check the items for
quality, numbers and specified items. If they miss out anything then they report, and in case there
is any damage then they report for replacement.
UNDP being the prime recipient of GF has already LTA with vendor, manufacturer and agencies
which are capable enough to provide the services for which they have LTA with UNDP. PSM of
UNDP maintains integrity of quality, accountability and transparency. To maintain quality,
accountability and transparency PSM passes through different steps including:

67
Defining the list of health products that will need to be procured. List are done
comprehensively for health and non-health products which are endorsed by donors.
Developing procurement action plan from the annual plan of the programme provide the
list of the items.
Preparing procurement request form is something a request form with all the items for
procurement.
Sending PRF to procurement partners. UNICEF, for example, is the procurement partner
for ACTs, LLINs and medicines. For RDTs and other equipment, the General Procurement
Unit of GF is responsible.
Specifying quantities for procurement and cost is provided by agencies.
Evaluating by UNDP specifications based on confirm specification, lead time and
transportation.
As per evaluation report, issuing by UNDP the Purchase Order.
Delivering by the vendor items as per agreed lead time and specification.
Receiving by UNDP the items ordered.
Confirming by UNDP receiving the items.
Checking by Programme and PSM the items for quality, numbers and specified items.
Transporting all the items received to wire house.
Distributing the items to the areas where they were planned for.
Besides UNDP as GF grant PR, BPHS/EPHS is another big channel for PSM, which includes
mostly malaria supplies. The main challenges include unavailability of information on quantity,
quality, costing, etc. of supplies procured and distributed by this system with NMLCP.
Conclusions
1. Procurement supply management of NMLCP in Afghanistan is implemented by
UNDP/GFATM and UNDP collaborates with NMLCP for quantification and specification.
2. UNDP being the prime recipient of Global Fund has already LTA with vendor,
manufacturer and agencies which are capable enough to provide the services for which
they have LTA with UNDP. PSM of UNDP maintains integrity of quality, accountability
and transparency.
3. Besides UNDP as GF grant PR, BPHS/EPHS is another big channel for PSM, which
includes mostly malaria supplies. The main challenges include unavailability of
information on quantity, quality, costing, etc. of supplies procured and distributed by this
system with NMLCP.
Recommendations
1. NMLCP should coordinate the estimation and procurement of malaria commodities with
GCMU, BPHS and EPHS and malaria partners.

68
2. NMLCP should regularly update on supplies used or in stock, and required for the next
year(s).
3. National programme staff should take active part in the process of PSM and they should
be trained along with the UN staff.
4. Establishment of a mechanism to regularly exchange the PSM information with NMLCP
is required for a timely action in procurement and supplying of the medicines or materials
based on updated policy, proper allocation of the needed supplies, avoiding the gaps of
required supplies, etc.
5. In the long-term MoPH and NMLCP should take care of the PSM.
4.7. Monitoring and Evaluation (M&E)
Current Situation & Existing Challenges
M&E is the central component of any anti-malaria programme. Through M&E, programme
impact, outcome, output and input indicators are measured to provide the basis for accountability
and informed decision making at both programme and policy level. In the elimination phase, the
main M&E requirement is to indicate exactly which administrative units have reached the
elimination target at a given point in time.
M&E Directorate within the General Directorate for Policy and Planning of the MoPH is the
departmental body responsible for implementing the M&E Strategic Plan of MoPH. The M&E
Directorate is closely linked to HMIS, DEWS, Information Technology and Research and
Informatics departments and Human Resource Database. M&E department coordinates and guides
all M&E activities among the various departments in MoPH, Provincial Public Health Directorate
and NGOs.
NMLCP is responsible for monitoring and evaluation of all malaria related activities by M&E
department of NMLCP at central level and the M&E officers of PMLCPs at provincial level. There
is lack of adequate technical capacity for data analysis and interpretation, particularly at the
provincial level. Besides the M&E department of NMLCP, which is responsible for M&E in the
field of malaria, Health Net TPO, BRAC and WHO also have M&E system to monitor and evaluate
their related malaria activities. Partners should submit their M&E finding to NMLCP.
M&E department is responsible to oversee the performance of programme implementation and
regularly conducts supervision visits to provinces to monitor the programme performance, detect
problems/constraints and provide on job training, if needed. In cooperation with NMLCP M&E
department, provincial malaria M&E officers are responsible for all M&E malaria-related
activities at their respective provinces. All PRs conduct joint supportive supervisory visits to
improve quality of malaria interventions and fill gaps.
The updated malaria M&E plan 2013-2017 has been prepared with support of the technical
working group composed of members from different NMLCP departments (Updated National

69
Malaria M&E Plan, 2013-2017, MoPH/NMLCP, 2013; National Strategic Plan for malaria Control
and Elimination, MoPH/NMLCP, 2013; National Elimination Plan, 2013-2017, MoPH/NMLCP,
2013). Numerous malaria indicators (see Table 6) along with data collection/reporting tools and
supervisory checklists that are used by BPHS implementers, HMIS, NMLCP and PRs for data
collection reflected in the updated malaria M&E plan, 2013-2017 are used by NMLCP, partners
and WHO.
Table 6: Malaria impact and outcomes indicators recommended
Indicators
Strategic Approaches
Impact Outcomes
National Strategic Plan for Malaria Control and Elimination, 2013-2017
Case Management 3 8
IVM - 8
EPR - 4
Capacity Building - 2
Involvement of Private Sector - 1
Cross-Border Coordination - 2
IEC/BCC - 2
Operational Research - 1
Sub-Total 3 28
Malaria Elimination Plan, 2013-2017
Case Management 2 6
Involvement of Private Sector - 1
IVM - 3
Sub-Total 2 10
TOTAL 5 38
NMLCP relies on a diverse range of sources for provision of data and its reporting mechanisms
which include routine and integrated data from health facilities through HMIS and programmatic
vertical data through NMLCP departments and partners. Various measures are undertaken by each
reporting entity to ensure a high standard of reporting. Malaria reporting and information systems
are in place and bulk of data on malaria is collected.
Routine data collected at health facilities level in standard HMIS forms are entered to HMIS
database and shared with PHD every month, and reported to national level (HMIS) at quarterly
basis. Data are analysed and feedback provided to BPHS implementers on quarterly basis. The
consolidated version of HMIS database is shared with all MoPH departments and partners.
Vertical programmatic data collected at field level and submitted to provincial level at weekly and
monthly basis. Data is entered to data sheet by provincial LMCP staff and reported to NMLCP at
monthly or quarterly basis. NMLCP enters data to malaria database which developed by
WHO/EMRO.
NMLCP collects additional malaria specific information through malaria MIS, periodic surveys
and sentinel sites. Quarterly malaria updates on epidemiological malaria profile and progress made

70
are disseminated at both national and provincial levels. There is a lack of evidence-based
documentation on progress made towards malaria elimination in the country.
Four main departments of Epidemiology/Surveillance, M&E, Entomology and QA of LMCP at
central and provincial level are responsible for QA of malaria data.
MoPH has established the Vector Borne Disease Task force meeting committee as an independent
focal body to coordinate malaria related issues among government entities, international partners,
NGOs, private sector and civil societies. This is a multi-sectorial structure which reflects the full
commitment and priorities of the government of Afghanistan and the development partners
responding to malaria in line with the ANDS. At the same time, Afghan CCM is also playing a
major role in coordinating HIV, TB and Malaria related issues in the country.
Conclusions
1. The national malaria M&E plan has been recently updated and is being presently used to
guide and coordinate malaria M&E among all parties involved.
2. There are too many outcome/impact indicators being reported as recommended by NMSP
and MEP 2013-2017, and they are not properly specified in relation to the stage on the
continuum to malaria elimination.
3. Lack of adequate technical capacity for data analysis and interpretation at the central and
provincial levels.
4. Malaria data collected by partners are not always shared with NMLCP.
5. Malaria-related trainings on malaria M&E are insufficient at all levels.
6. National malaria report is prepared and published annually, but there is lack of evidence-
based documentation on progress made towards malaria elimination within the country.
Recommendations
3. NMLCP should take overall responsibility for ensuring that data is analysed and interpreted
appropriately and the results are used effectively to ensure that any necessary action is
taken promptly to maximize programme performance and impact.
4. To streamline the reporting process, the existing outcome and impact indicators should be
re-examined considering maintaining a minimum set of indicators per an objective. The
decision on selection of the minimum set of realistic indicators should be taken by NMLCP
in close collaboration with WHO and other partners concerned. NMLCP may request
WHO to provide the necessary technical assistance in relation to this task.

71
5. Different set of outcome and impact indicators are required depending on the stage on the
continuum to malaria elimination, which should be routinely tracked by NMLCP. Indicators on impact and adequacy of surveillance are central to verification about
interruption of malaria transmission, its elimination and maintenance of malaria-free status.
6. Central- and provincial-level programme staff should be trained in malaria data analysis
and interpretation. SOPs for data collection, recording and analysis should be revised to
improve the reporting process and its outcomes.
7. The mechanism of data sharing among stakeholders concerned should be re-examined and
coordinated by NMLCP in a proper manner.
8. Different training options on malaria M&E should be considered for various categories of
general health and programme staff and CHWs. Existing national training modules on
malaria M&E should be updated.
9. Progress towards malaria elimination should be documented. An annual malaria report as
a good epidemiological practice that provides a synthesis of all available information on
malaria, its control and elimination is required for the future verification/certification
process of malaria elimination.
10. A malaria elimination database should be established when a decision has been made to go
for elimination. Information on coverage and quality of interventions with mapping out
cases and foci of malaria is particularly important in provinces eligible for malaria
elimination.
4.8. Advocacy, IEC and Community Mobilization
Current Situation & Existing Challenges
The involvement of communities and their partnership with health sectors to empower then in their
own health development is crucial. Malaria prevention must go hand in hand with community
participation. Unless individuals in communities see the merits of preventing the illness, even the
best-designed prevention strategies might not be used.
NMLCP developed its IEC/BCC guidelines in 2008 aiming to inspire people who are at risks and
suffer from malaria to change their behaviours. The strategy is aimed at improving knowledge and
awareness on vector control, diseases management and prevention. As reflected from outcomes of
the Malaria Indicator Surveys conducted, only 32.9% and 33.4% of respondents sought early
treatment for fever in 2011 and 2014, respectively. Unless the targeted population has adopted a
positive behaviour change to seek early diagnosis of malaria, to have adequate treatment of malaria
and to use regularly LLIN to protect themselves, malaria control cannot be sustainable. Changing
behaviours of the population takes always time and requires huge efforts from the programme.
Different IEC approaches and methods should be undertaken through various mass media channels
to facilitate changing human behaviours in relation to malaria control and prevention.

72
Approaches and activities that are undertaken to translate the current IEC/BCC strategies in
Afghanistan include (1) community events with school students and in women shuraa; (2)
distribution of notebook, posters and brochures with messages on malaria control and prevention;
(3) informal discussions on prevention and control in the meeting with students, teachers; and (4)
TV and radio talk show with malaria experts to improve public awareness. During commemoration
of the World Malaria Day celebrated annually at the central level and some provinces, IEC
materials like posters, brochures, booklets with malaria messages are distributed to the health
facilities. IEC campaign should be also conducted before and during the malaria transmission
season. Community mobilization is the approach aimed to increase public awareness on malaria
control and prevention. Leaders of the society including Mollahs, Imams, school teachers, students
and community elders are regarded as persons who may influence others to adopt positive
behaviours regarding malaria control and prevention.
NMLCP has a plan and standard curriculum to conduct IEC activities every year, which are
communicated to provinces and down to district level. Topics to raise community awareness on
malaria include information on signs and symptoms of malaria, early diagnosis and treatment of
malaria, how to use LLINs, health seeking behaviours and health facilities where malaria can be
properly diagnosed and treated. Once the decision is made about launching malaria elimination, at
least in eligible northern provinces, it should be reflected in the national IEC/BCC strategies and
their mechanism to advocate for elimination. The same should be done for highly affected eastern
provinces of Afghanistan, where appropriate IEC/BCC strategies should be developed.
Conclusions
1. NMLCP developed its IEC/BCC guidelines in 2008 to facilitate changing behaviours of
local communities on malaria and its control and prevention.
2. At present, NMLCP has a plan and standard curriculum to conduct IEC activities, which
are communicated to provinces and down to district level.
3. There is a lack of understanding how local communities perceived malaria and what kind
of preventive practices are currently in place at community level.
4. There are shortages of updated IEC materials on malaria available in public health facilities
across the country.
5. There are no operational plans available at provincial level to conduct advocacy and social
mobilization related to malaria prevention.
Recommendations
1. In the context of the national plan for malaria elimination, NMLCP should map all the
current IEC/BCC strategies and revise them, if necessary, to align with existing strategies
on case management, disease prevention and surveillance.

73
2. There should be updated IEC/BCC national strategy to guide involvement and
empowerment of communities and their linkages with local health staff and partnership
with private sector to ensure the sustainability of malaria preventive activities.
3. KAP assessments should be conducted to evaluate the impact of IEC/BCC strategies and
assess compatibility of practices, customs and beliefs of various social groups and ethnic
groups with existing strategies, and based on results, IEC/BCC strategies and targeted
materials can be updated.
4. Strategies on community mobilization should be developed with an overall aim to deliver
quality malaria-related information on treatment and prevention at the community level.
5. To promote behaviour change related to health seeking and personal protection, NMLCP
should develop and disseminate widely IEC-related materials/messages to the public. The
messages should target the most at-risk and underserved populations. Different IEC/BCC
materials/messages should be harmonized across different ethnic groups and migrant
populations. A multi-media strategy to deploy messages via radio, television should be
broadly utilized.
6. To improve coordination, NMLCP may convene a meeting to share with all partners
involved progress on IEC/BCC activities, identify best practices and challenges in
implementation, update key messages and develop new IEC/BCC materials/messages in
the context of malaria elimination. NMLCP should include key IEC/BCC messages into
training modules and learning materials to be used for training purpose of public health
staff, private health providers and CHWs.
7. NMLCP along with general health staff and CHWs should work with community leaders
to mobilize communities and increase awareness about malaria prevention. Community
sensitization and training workshops should be organized by involving important
community actors including religious leaders, village elders, private sectors providers,
teachers and other stakeholders to strengthen the linkages between the key actors and
quality malaria service providers.
4.9. Operational Research
Current Situation & Existing Challenges
Afghanistan malaria control program in collaboration with other related agencies have conducted
some researches on malaria control interventions e.g. vector control, case management, new
intervention (treatment regimes, or case management), drug efficacy and program evaluation.
During years (2013-2016) two surveys, one of Malaria Indicators Survey (MIS) and another for
Long Lasting Insecticidal Treated Nets have been conducted. The MIS is a national level survey
which measures some important impact level indicators including (1) malaria prevalence; (2)
household ownership of LLIN; (3) treatment seeking behaviour, and (4) knowledge for malaria

74
prevention. Finding from MIS indicate that parasitologically confirmed prevalence is 3.4%
keeping in mind that data collection time is an important factor for measuring prevalence because
malaria has a seasonal nature. Ownership for LLIN at households is 31% while those who slept
last night under bed nets are 17%. Treatment seeking behaviour for participants when they had
fever; shows that using private or public health facilities are 5% and 11% while self- medication
or buying medicines from pharmacy is 32% and 37%. Knowledge on malaria prevention using bed
nets is around 41% while 30% has mentioned “don’t know”.
The survey of durability and efficacy of long lasting insecticidal nets was investigated the usability
of distributed nets after three years due to attrition and effectiveness of its insecticidal effect. Its
findings indicated higher endurance but low number of nets for some provinces while the usage in
other provinces was lower.
The prevalence of malaria infection in some provinces of the country is a significant public health
issue. Studies to inform the decision makers and renew policies and implement technically-sound
interventions to better curb the problem are in need. Although this operational research needs
extensive proficiency and is costly, but NMLCP with support of related NGOs and other donor
agencies has conducted such studies. Collaboration with national universities is absent probably
due to poor technical capabilities of these institutions or lack of communication and coordination.
The results of some operational research conducted are presented below.
The operational research/Cluster Randomised Trial on the use of malaria rapid diagnostic tests by
community health workers in Afghanistan revealed that RDT has lower operational sensitivity for
Falciparum parasite (53.1%, 50.3-56.0) and for P. vivax 47.6% (70/147) (p<0.0001).
A multicentre randomised, placebo-controlled comparison of short and long course primaquine
regimens is an ongoing research, and it is expected that the results to determine whether a 7-day
primaquine regimen is safe and not inferior to the standard 14-day regimen (total dose of 7mg/kg
in both arms) in preventing P. vivax relapse in G6PD normal patients will be available in years to
come.
The findings from the study on status of insecticide resistance in high-risk malaria provinces in
Afghanistan revealed that emerging resistance against all four classes of insecticides in the high-
risk provinces eastern and northern part of the country was observed in both An. stephensi and
Anopheles culicifacies, which are principal malaria vectors in these provinces.
The findings on malaria in pregnancy in Afghanistan have shown that prevalence of malaria was
lower among pregnant women in comparison of anaemia, while there was no association of
anaemia with age, gravidity, intestinal parasite prevalence, or low-birthweight at delivery, and
pregnant women were not willing to use preventive medication for malaria during pregnancy. It
has concluded that the use of LLINs is a best vector control intervention to prevent malaria among
pregnant women.
The initial results of efficacy and safety of Artemether-Lumefantrine (Coartem) for the treatment
of uncomplicated P. falciparum and P. vivax malaria in health facilities (Jalalabad, Ghanikhil,
Asadabad and Chawkai) in Nangarhar and Kunar provinces of Afghanistan have indicated that the

75
medicine is well tolerated by patients. Efficacy and safety of Coartem for parasitological clearance
was faster in vivax patients compared with falciparum malaria. Although this is not a superiority
study but this drug could be considered as a reserved second-line therapy.
Conclusions
1. Despite the desperate need for operational research on malaria and its control, there is no
specific budget for operational malaria research in the MoPH.
2. Designing and conducting operational research is entirely dependent upon provision of
external funds, but there is lack of donors’ commitment.
3. Despite the National Institute for Health has some capacity for planning/conducting
operational research related to malaria, the overall national operational research
capabilities are insufficient in Afghanistan.
Recommendations
1. Operational research on malaria should be prioritized in the donors’ mandate for allocation
of human/financial resources.
2. The national capacity/capability for operational research should be strengthened in the
National Institute for Health, and its personnel should attend international training courses
related to designing research protocols and conducting relevant studies.
3. A national core group of researchers should be formed to address malaria-related issues.
4. A budget line should be defined in MoPH for operational research including malaria.

76
Part 5
Main Conclusions
Over the recent years (2013-2015) Afghanistan has made a significant progress in reducing the
burden of malaria contributing to poverty alleviation as malaria is most prevalent in the poorest
segment of the population.
In some northern, western and southern provinces the number of malaria cases, particularly P.
falciparum has dropped significantly and these provinces became eligible for malaria elimination.
It is becoming evident that some provinces have already interrupted and other provinces could
interrupt transmission of P. falciparum malaria in the years ahead. The results achieved in some
parts of Afghanistan, where malaria transmission is limited and incidence/risk became extremely
low, need to be further consolidated with the goal of interrupting the transmission of malaria.
Despite visible progress in dealing with malaria in Afghanistan, however, the goal of eliminating
malaria in the entire country is still distant because of the remaining high burden of malaria with
ongoing severe epidemic of malaria in some eastern provinces, numerous technical and operational
constraints (lack of epidemic preparedness and response, vector behaviours, poor accessibility of
remote/border often endemic areas, uncontrolled population migration within the country and
between Afghanistan and neighbouring endemic countries, lack of involvement of private and
community-based health sectors etc.) and security problems.
The main conclusions that have been made for each thematic area are listed below:
Case Management
Parasitological confirmation of all clinically-suspected cases of malaria by RDT or
microscopy is not in place yet.
There is insufficient information from the private sector on diagnosis of malaria.
Lack of quality assurance for malaria diagnosis by microscopy and/or RDT at different
levels.
Treatment of cases (P. vivax, P. falciparum, management of severe and complicated
malaria, pre-referral treatment of severe and complicated cases) are not always done as per
existing national treatment protocol/drug policy.
Despite the radical treatment of vivax cases and provision of a single dose of primaquine
for P. falciparum malaria patients are recommended, this approach has to be put into
practice.
Lack of training on case management of different health care providers including the
private sector.
Vector Control and Entomological Surveillance
Distribution of LLINs is based on the official numbers of country’s population provided
by the National Statistics Services that is not always update, so that the number of LLINs
distributed is always behind the national target.

77
Malaria entomological data is not used along with epidemiological and HMIS data for the
decision making regarding malaria control and elimination.
Number of entomology staff in NMLCP and especially at provincial level is none or
minimal, and their training on vector control and entomological surveillance is inadequate.
A proper plan for entomological surveillance is not in place. As an important component
of entomological surveillance, insecticide susceptibility status of malaria vectors should
be conducted under rigorous standards to ensure the reliability of the results for decision
making.
Malaria Surveillance
Based on available malaria and environmental data and reflecting a risk of malaria, all
districts in Afghanistan were classified into four main strata with high, medium, low (5
023 200 people) and very low risk of malaria transmission or its absence in malaria free
areas to provide strategic guidance for planning anti-malaria interventions.
Routine malaria surveillance is presently conducted through HMIS, and malaria reporting
from BPHS and EPHS is integrated with HMIS. Malaria sentinel surveillance is currently
carried out through three types of sentinel sites to show malaria trend, to monitor drug
efficacy and to detect epidemics/outbreaks.
Epidemic Preparedness and Response (EPR)
At present, EPR is one of the strategic directions of the NMSP 2013-2017, and malaria
outbreaks are detected through functional DEWS which is covering the entire country.
However, the existing epidemic preparedness and response mechanism is obviously not
adequate to prevent and contain the ongoing outbreaks/epidemic of malaria in the eastern
provinces.
There is no a built-in mechanism for forecasting and early warning for malaria epidemics.
There is no link between malaria control program and hydro-metrology and other relevant
departments regarding forecasting.
The existing stratification is lacking to identify properly epidemic-prone areas within the
country.
The existing epidemic prevention mechanism is insufficient, and epidemic preparedness is
lacking.
EPR teams were established at central and provincial levels and the system for epidemic
detection and investigation is in place, but are not fully functional especially at provincial
and lower levels.
Programme Management
Almost all the departments of NMLCP are lacking manpower, financial resources and
coordination to make the programme more productive and fully functional at all levels.
There is a lack of competent programme staff in most programme departments, particularly
at provincial level at present. It has been noted that many of the professional and technical
staff of NMLCP have frequently moved out to search for a better job.

78
There are insufficient capacities/capabilities of the core technical groups, particularly at
provincial level to provide adequate guidance and assistance in planning, implementation,
monitoring and evaluation of malaria control and elimination activities.
There are a lack of coordination and no regular meetings between central programme and
provincial teams.
The programme’s budget has no adequate reserve provisions to meet possible problems
that are liable to occur during its implementation.
Procurement Supply Management (PSM)
Procurement supply management of Global Fund Malaria Programme in Afghanistan is
implemented by UNDP, Afghanistan and UNDP collaborates with NMLCP for
quantification and specification.
Besides UNDP as GF grant PR, BPHS/EPHS is another big channel for PSM, which
includes mostly malaria supplies. The main challenges include unavailability of
information on quantity, quality, costing, etc. of supplies procured and distributed by this
system with NMLCP.
Monitoring and Evaluation (M&E)
The national malaria M&E plan has been recently updated and is being presently used to
guide and coordinate malaria M&E activities among all parties involved.
There are too many outcome/impact indicators being reported as recommended by NMSP
and MEP, 2013-2017, and they are not properly specified in relation to the stage on the
continuum to malaria elimination.
Lack of adequate analytical capacity for data interpretation, particularly at the provincial
level.
Malaria-related trainings on malaria M&E are insufficient at all levels.
Advocacy, IEC and Community Mobilization
There is a lack of understanding how local communities perceived malaria and what kind
of preventive practices are currently in place at grassroots level.
There are shortages of updated IEC materials on malaria available in public health facilities
across the country.
There are no operational plans available at provincial level to conduct advocacy and social
mobilization related to malaria prevention.
Operational Research
Designing and conducting operational research is entirely dependent upon provision of
external funds, but there is lack of donors’ commitment.
Despite the National Institute for Health has some capacity for planning/conducting
operational research related to malaria, the overall national operational research
capabilities are insufficient in Afghanistan.

79
Main Recommendations
The main recommendations that have been made on a priority basis for each thematic area are
listed below:
Priority issues should be addressed immediately (2017):
Case Management
Wide scale deployment of RDTs through multiple public, private and community-based
channels and strengthening/setting up of existing/new laboratory facilities should be
actively promoted to reach universal coverage of case management including remote,
inaccessible, ‘security compromised’ and internally displaced populations.
Training on malaria diagnosis and treatment with updated training materials and SOPs
should be provided to different categories of health care providers at all public, private
and community-based health sector facilities.
National malaria treatment guidelines should be updated based on the new 2015 WHO
guidelines on treatment of malaria.
Essential drug list for treating malaria should be revisited and a minimum set of essential
drugs is required for areas where cases are drastically reduced to avoid medicine’s
wastage and to ensure that quality-assured efficacious antimalarial drugs provided in
both public and private sectors.
Vector Control and Entomological Surveillance
National policy and funding for procurement and distribution of LLINs should be adequate
and sufficient to cover all population groups at risk of malaria within the country:
o A better estimate of the total populations at provincial, district and lower levels
should be made to calculate the sufficient quantities of LLINs to be procured and
distributed within each province. If the target is one LLIN for 2 people, the
benchmark of a maximum of two LLINs per household should be lifted.
o Timely procurement of LLIN should always be a priority so that distribution can
start well before transmission season.
o Distribution of LLINs should be coupled with locally appropriate and gender
sensitive IEC/BCC to ensure community participation and correct LLINs usage.
There is a desperate need for strengthening the entomological component of NMLCP at
central and provincial levels:
o The inventory of existing entomology staff and assessment for the staff needed and
relevant posts to be filled at each level should be made.
o The entomological capacity of NMLCP should be strengthened. Training should be
“task-oriented” and “problem-solving” and supplemented by regular supervision
and refresher training courses.
o A core NMLCP technical group on vector control with a good representation of
competent staff in medical entomology and vector control at provincial level should
be maintained or established to play a greater role in the decision-making process
on malaria control and elimination.

80
Malaria Surveillance
11. Based on the 2016 reported API as a primary criterion for selection and other criteria such
as the reported number of malaria cases per health facility; the reported ratio of P.
falciparum to P. vivax; determinants of local epidemiology and degree of development of
health system within a given province, the entire country should be sub-divided into three
Categories (1) where malaria is still widespread and the primary objective is to reduce the
remaining malaria burden further; (2) where malaria shows a focal distribution of
indigenous cases and which are eligible for malaria elimination and (3) where all reported
cases of malaria have an imported nature, and particular focus should be placed on
maintenance of the results achieved by prevention of re-establishing local malaria
transmission. NMLCP may request WHO to provide the necessary technical assistance in
relation to this task.
In the malaria elimination phase, malaria must be a notifiable disease, and every
symptomatic and asymptomatic infection should be detected and mandatory notified.
Surveillance activities should be enhanced so that every focus (village, or sub-village or
working site) with indigenous case(s) of malaria is targeted for action.
Epidemic Preparedness and Response (EPR)
The NMLCP capacity to judge the abnormality of the situation, decide on the
epidemiological diagnosis of outbreaks/epidemic and have the authority to plan and
implement epidemic containment measures should be strengthened, particularly at
provincial level.
Epidemic-prone situations should be identified during the process of stratification of the
malaria problem into discrete areas and populations based on various data from health and
non-health sectors.
It is expected that emergency situations within epidemic-prone areas or population groups
in Afghanistan are likely occur. The application of vector control methods including focal
IRS if technically feasible/operationally applicable should be seriously considered to
contain the on-going outbreaks/epidemic and their further spread and recurrence in
subsequent years. In epidemic-prone areas, where LLINs and other sustainable vector
control measures are already used may be the most effective way of reducing transmission
and preventing epidemic spread to new areas or resurgence in subsequent years.
Programme Management
Emphasizing the need to address the emerging elimination and remaining challenges, the
current National Strategic Plan for Malaria Control and Elimination/Malaria Elimination
Plan, 2013-2017 should be revised to reflect changes in programme priorities, targets,
strategic approaches and key interventions, considering that malaria elimination in
Afghanistan should be carried out in a phased manner by parasite species with a priority to
be given to elimination of P. falciparum and by geographical area (sub-national
elimination) with different parts of the county being at different programme phases

81
simultaneously. NMLCP may request WHO to provide the necessary technical assistance
in relation to this task.
For relatively large and heterogeneous country like Afghanistan, the emphasis should be
given to assessing major administrative units, typically Provinces. Some provinces have
already become eligible for elimination. If their health systems are strong enough, it is
rational to pilot surveillance and other elimination activities focusing on setting up
adequate surveillance, databases and quality assurance systems, preparing and testing
relevant SOPs and training different categories of health staff.
To ensure achieving programme objectives and targets the roles and responsibilities of
departments of the NMLCP should be revisited to ensure their proper guidance, continuous
coordination and synchronization of their work.
Assessment of the NMLCP’s capacity in terms of human resources available at central and
provincial levels should be carried out to make the inventory of programme staff, and on
this basis to decide on the number and categories of professional personnel to be trained
or re-trained.
Procurement and Supply Management (PSM)
Establishment of a mechanism to regularly exchange the PSM information with NMLCP
is required for a timely action in procurement and supplying of the medicines or materials
based on updated policy, proper allocation of the needed supplies, avoiding the gaps of
required supplies, etc.
Monitoring and Evaluation (M&E)
To streamline the reporting process, the existing outcome and impact indicators should be
re-examined considering maintaining a minimum set of indicators per an objective. The
decision on selection of the minimum set of realistic indicators should be taken by NMLCP
in close collaboration with WHO and other partners concerned. NMLCP may request
WHO to provide the necessary technical assistance in relation to this task.
Different set of outcome and impact indicators are required depending on the stage on the
continuum to malaria elimination, which should be routinely tracked by NMLCP. Indicators on impact and adequacy of surveillance are central to verification about
interruption of malaria transmission, its elimination and maintenance of malaria-free
status.
Advocacy, IEC and Community Mobilization
In the context of the national plan for malaria elimination, NMLCP should map all the
current IEC/BCC strategies and revise them, if necessary, to align with existing strategies
on case management, disease prevention and surveillance.
To improve coordination, NMLCP may convene a meeting to share with all partners
involved progress on IEC/BCC activities, identify best practices and challenges in
implementation, update key messages and develop new IEC/BCC materials/messages in
the context of malaria elimination.
82
Operational Research
Operational research on malaria should be prioritized in the donors’ mandate for allocation
of human/financial resources.
A national core group of researchers should be formed to address malaria-related issues,
and some of them should attend international training courses on designing research
protocols and conducting relevant studies.
Important issues that should be taken into consideration in the short and medium run
(2017-2019):
Case Management
Central and regional malaria reference laboratories should be strengthened or established
for QA/QC of malaria diagnosis, supervision and monitoring etc.
EQA system for malaria diagnosis should be set up.
A substantial effort should be taken to ensure that primaquine treatment for 14 days (if
G6PD test is available) or 0.75 mg/kg primaquine weekly for 8 weeks for anti-relapse
treatment of P. vivax under close medical supervision and a single dose of primaquine
as a gametocytocide for P. falciparum have been put into practice.
QA of case management services, antimalarial diagnostics and drugs should be
established and functional covering the public, private and community-based health
sectors throughout the entire country.
Structured death verification system for malaria auditing all cases of deaths following
severe/complicated malaria should be established.
Capacities of referral hospitals for and health personnel involved into management of
severe/complicated malaria should be improved and all severe/complicated cases of
malaria should be properly registered and reported.
Access to and quality of malaria diagnosis and treatment services should be improved at
remote, inaccessible and ‘security compromised’ areas and among mobile and migrant
populations.
Malaria case management at community level should be scaled up and supportive
supervision should be regularly provided.
The therapeutic efficacy studies should be continued with focus on highly endemic areas
and their outcomes should be considered while updating a national treatment policy.
Case management practices should be part of a national strategy on Information,
Education, and Communication.
Pharmacovigilance system which will allow improvement in knowledge of drug safety
and increase the ability to detect rare side effects of primaquine should be set up, initially
in public referral hospitals and other public health facilities.
Vector Control and Entomological Surveillance
Various eco-epidemiological types of malaria with different principal and secondary
vectors within the country should be properly defined and technically/operationally

83
feasible vector control measures/options for different malaria settings based on local
epidemiology should be selected.
Achieving and maintaining universal coverage with LLINs to ensure that each household
has sufficient nets in line with WHO standards and every inhabitant at risk sleeps under a
LLIN every night is critical to reduce transmission in high-transmission settings. In high-
transmission settings, particularly with An. stephensi and An. culicifacies, transmission
reduction through universal coverage and usage of LLINs and other sustainable vector
control including protective personal measures should be recommended.
It is logical to assume that a combination of different vector control options suiting
Afghanistan’s conditions and responding to local needs and based on Integrated Vector
Management (IVM) principles may compensate for deficiencies of each individual
method:
o Vector control options including LLINs, larval source management and
larviciding (temephos and BTi) should be actively promoted through
community participation in high-transmission settings to bring malaria
transmission down.
o The application of vector control measures and their combinations should be
always guided by consideration of their technical feasibility, operational
applicability, sustainability, and some of them are in need of better QA.
o Environmental management (drainage, filling, land levelling, vegetation
removal etc.), which deserves to be used more often by communities for
collective protection from malaria vectors can be recommended, and can be
applied in combination with other vector control measures. An inter-sectorial
collaboration is required for deployment of environmental management at local
level.
The programme should consider conducting focal IRS (if technically
feasible/operationally applicable) in the event of outbreaks and in areas eligible for
elimination where case/focus investigations are in place, and entomological evidence and
other factors indicate that interruption of transmission can be expected:
o Focal IRS should be applied on a strict total coverage of all active foci of
malaria, with a view to interrupting transmission as soon as possible all over
the target area.
o The choice of insecticide should consider safety, efficacy, cost, availability and
susceptibility of vectors as well as using alternative insecticide(s) for IRS.
o To be effective IRS requires careful planning, well-organized operations with
skilled technical staff, very strong supervision and community mobilization to
achieve the high level of IRS coverage to maximize impact of this measure.
o The well-defined SOP should be developed for IRS planning, implementation,
and monitoring.
o Malaria entomological and health staff should be trained on IRS to support its
application and monitor quality of IRS operations.
The necessary capacity of national malaria programme for entomological surveillance
should be built:
o Training on entomological surveillance and its role in malaria control and
elimination should be organized for the NMLCP and PMLCP staff. SOPs
related to entomological monitoring and surveillance should be developed:

84
o Entomological surveillance should include identification of vector species,
monitoring vector behaviours and bionomics, mapping species distribution and
density, identification of host preference, seasonal fluctuation of species, and
assessment of an area’s receptivity.
o Entomological surveillance should also be carried out in epidemic-prone areas
based on set outbreak thresholds.
o Insecticide resistance is one of the greatest threats to any concerted or prolonged
attempt at malaria transmission control, and monitoring and management of
insecticide resistance should be regularly conducted.
o All existing and possible breeding sites of Anopheles mosquitoes should be
properly mapped in relation to active foci of malaria in areas eligible for
elimination.
o Considering different malaria transmission settings, an operational plan for
entomological surveillance should be worked out, and adequate training on
entomological surveillance should be conducted to strengthen a national
capacity of entomological services.
Vector biology and control research is of particular interest, which has been neglected, but
should be re-considered to make vector control more effective in producing desired results.
National capability/capacity to undertake operational research on issues of direct relevance
to vector control should be strengthened. The following studies can be considered:
o KAP studies on barriers for LLINs ownership and utilization.
o KAP studies on existing/potential preventive measures.
o Technical feasibility and operational applicability of various vector control
measures and their combinations in different malaria settings.
o Feeding and resting behaviour of malaria vectors.
o Insecticide susceptibility of malaria vectors.
o Biochemical/molecular mechanisms of insecticide resistance.
o Vector control impact assessment.
Malaria Surveillance
Measuring PPR can be recommended as the Malaria Indicator Survey among children
(juveniles/schoolchildren of 5-9 years old) in high transmission settings of the eastern
provinces. The infant parasite rate of 6-11 months old is of special importance as it is a
good indicator of a recent local transmission of malaria.
Along with PPR, the incidence of UM (malaria out-patients) and SCM (malaria in-patients)
as well as SCM/UM ratio and CFR of SCM can be recommended as additional indicators
to measure the malaria burden and impact of control interventions in high transmission
settings, considering that:
o from improved coverage of LLINs, a decrease in the incidence of UM and
SCM can be expected;
o from improved management of UM, a decrease in the incidence of SCM and
the ratio of SCM to UM can be expected; and

85
o from improved management of SCM before and after hospitalization, a
decrease in the CFR of SCM can be expected.
The target ABER should be well above 5%, and preferably 10% of the population at risk
for provinces under Category 1, and in the range between 2 and 4% of the population at
risk for provinces under Category 2, which are eligible for malaria elimination. The level
of diagnostic surveillance activity (ABER) and the distribution of malaria infection
(SPR/TPR) should be measured together in each administrative unit.
Coordination mechanisms between NMLCP, HMIS, BPHS and DEWS at provincial and
central levels to collect, process, analyse and share malaria-related data should be
improved. The current malaria surveillance should be reinforced to increase coverage and
completeness of reported data from health facilities throughout the entire territory of the
country. Existing database on malaria should be revisited and online reporting mechanism
should be set up.
Existing malaria surveillance and information systems should be strengthened to ensure
complete and timely reporting from all health sectors including the public facilities and
private sector, CHWs, military/police health services, and other parties concerned. Case-
based malaria surveillance system in the provinces under Category 1 should be established
and expanded in support of the move towards elimination.
A major surveillance paradigm change occurs when the country embarks on elimination,
and a case-based surveillance and response system, preferably based on GIS should be
established initially in priority provinces with low malaria incidence that are eligible for
malaria elimination, and later it should be expanded to other provinces as appropriate.
Specific guidelines and SOPs on malaria surveillance should be developed, and relevant surveillance, databases and quality assurance systems should be set up and training different
categories of health staff should be conducted in the transition phase from control to elimination.
To ensure adherence to standard surveillance procedures and practices in line with national
SOPs, malaria control programme staff should lead trainings on surveillance for all
categories of health staff concerned and other partners involved. Such trainings can be
integrated into other malaria trainings if possible.
Epidemic Preparedness and Response (EPR)
The existing EPR guidelines should be revised to include the forecasting and early warning
mechanisms.
An outbreak monitoring system should constitute a part of national malaria
epidemiological surveillance system. This system should identify and track early signs of
an impending epidemic related either to a particular area or population group. The
recognition of early alarm signals heavily depends upon the adequacy of the variables
chosen. Selection of the set of variables and the range of their numerical values should be
determined by type of the area regarding the local epidemiology, epidemic risk factors,
existing health service infrastructure, time lag in communication, etc.
Control of a malaria outbreak should involve an adequate package of measures aimed at
(1) minimizing clinical consequences; (2) containing transmission, if possible; (3)
preventing further spread of the epidemic; and (4) improving emergency preparedness to
prevent future epidemics. The first two objectives require the application, as soon as
possible, of effective containment measures, while the last two involve assessment of risk

86
and the application of preventive measures. IRS, if feasible, continues to be the most
effective measure to swiftly contain malaria transmission. IRS, to be fully effective, should
achieve total coverage of all houses within the affected area based on adequate provision
of insecticides, spraying equipment, transport and deployment of vector control
programme staff.
Preparedness for malaria outbreaks should be based on an understanding of the
epidemiology of malaria and epidemic risk factors. The more complete that understanding
and the more developed the information system and the monitoring of risk factors, the
higher is the level of preparedness, the more accurate the forecasting and the more adequate
the response. Malaria preparedness should be strengthened by identifying resources
(appropriate manpower, supplies, equipment and logistical arrangements including
administrative and technical procedures, responsibilities of health and other sectors) and
the required mechanisms for their rapid mobilization and deployment at provincial and
lower levels.
The government allocations for epidemic preparedness and response should be considered.
Programme Management
The government and MoPH should remain fully committed to malaria, and to make all
possible efforts required to achieve a greater impact on malaria situation in the country.
The core technical groups of professionals adequately trained on malaria with the
necessary epidemiological expertise should be maintained/established, particularly at
provincial level.
Engagement of the country in malaria elimination increases the need for programme
leadership, and this issue that is a crucial element for success of the elimination campaign
should be seriously considered.
A considerable effort should be taken to increase human resources and train, motivate and
sustain health staff including the programme personnel at all levels until malaria eliminated
across the entire country.
Coordination meetings with all stakeholders to guide planning, implementation and
evaluation of programme interventions on malaria should be held at regular intervals.
NMLCP should increase interactive communication between NMLCP and PMLCP to
improve the programme performance and quality; to provide the necessary support; to
increase motivation and to facilitate handling the field issues. Holding regular quarterly
regional meetings between NMLCP and PMLCP should be conducted to improve
coordination.
Adequate legislative and administrative provisions to govern the elimination programme
should be considered to cover the programme’s requirements, including the right of entry
by malaria staff with the purpose of investigation or spraying, mandatory notification and
reporting of malaria cases etc.
Regulation of the private sector as a major elimination challenge in Afghanistan should be
properly addressed.
The programme’s budget should be sufficient and realistic, including adequate reserve
provisions to meet possible problems that are liable to occur during its implementation,
and the source(s) of funds should be clearly indicated.

87
Procurement and Supply Management (PSM)
NMLCP should coordinate the estimation and procurement of malaria commodities with
GCMU, BPHS and EPHS and malaria partners.
NMLCP should regularly update on supplies used or in stock, and required for the next
year(s).
National programme staff should take active part in the process of PSM and they should
be trained along with the UN staff.
In the long-term MoPH and NMLCP should take care of the PSM.
Monitoring and Evaluation (M&E)
NMLCP should take overall responsibility for ensuring that data is analysed and
interpreted appropriately and the results are used effectively to ensure that any necessary
action is taken promptly to maximize programme performance and impact.
Central- and provincial-level programme staff should be trained in malaria data analysis
and interpretation. SOPs for data collection, recording and analysis should be revised to
improve the reporting process and its outcomes.
The mechanism of data sharing among stakeholders concerned should be re-examined and
coordinated by NMLCP in a proper manner.
Different training options on malaria M&E should be considered for various categories of
general health and programme staff and CHWs. Existing national training modules on
malaria M&E should be updated.
Progress towards malaria elimination should be documented. An annual malaria report as
a good epidemiological practice that provides a synthesis of all available information on
malaria, its control and elimination is required for the future verification/certification
process of malaria elimination.
A malaria elimination database should be established when a decision has been made to
go for elimination. Information on coverage and quality of interventions with mapping out
cases and foci of malaria is particularly important in provinces eligible for malaria
elimination.
Advocacy, IEC and Community Mobilization
There should be updated IEC/BCC national strategy to guide involvement and
empowerment of communities and their linkages with local health staff and partnership
with private sector to ensure the sustainability of malaria preventive activities.
KAP assessments should be conducted to evaluate the impact of IEC/BCC strategies and
assess compatibility of practices, customs and beliefs of various social groups and ethnic
groups with existing strategies, and based on results, IEC/BCC strategies and targeted
materials can be updated.
Strategies on community mobilization should be developed with an overall aim to deliver
quality malaria-related information on treatment and prevention at the grassroots level.
To promote behaviour change related to health seeking and personal protection, NMLCP
should develop and disseminate widely IEC-related materials/messages to the public. The
messages should target the most at-risk and underserved populations. Different IEC/BCC

88
materials/messages should be harmonized across different ethnic groups and migrant
populations. A multi-media strategy to deploy messages via radio, television should be
broadly utilized.
NMLCP along with general health staff and CHWs should work with community leaders
to mobilize communities and increase awareness about malaria prevention. Community
sensitization and training workshops should be organized by involving important
community actors including religious leaders, village elders, private sectors providers,
teachers and other stakeholders to strengthen the linkages between the key actors and
quality malaria service providers.
Operational Research
The national capacity/capability for operational research should be strengthened in the
National Institute for Health.
A budget line should be defined in MoPH for operational research including malaria.

89
The Way Forward
Welcoming the substantial progress made toward reducing the burden of malaria in Afghanistan
in recent years, the Government and MoPH should remain fully committed to malaria, and to make
all possible efforts required to achieve a greater impact on malaria situation in the country.
Emphasizing the need to address the emerging elimination and remaining challenges, the current
National Strategic Plan for Malaria Control and Elimination, 2013-2017 should be revised to
reflect changes in programme priorities, targets, strategic approaches and key interventions,
considering that malaria elimination in Afghanistan should be carried out in a phased manner by
parasite species with a priority to be given to elimination of P. falciparum and by geographical
area (sub-national elimination) with different parts of the county being at different programme
phases simultaneously.
In 2017, after developing and launching of the new National Strategic Plan for Malaria Elimination
2017-2020, a nation-wide planning exercise and orientation workshop should be carried out with
participation of all Provinces to agree jointly on milestones/targets as well as specific/cross-cutting
interventions, training needs and administrative/financial provisions that should be defined in
detail for each Province. Along with planning exercise a national orientation workshop should be
conducted for Provincial senior managerial and health staff to inform on organization and
management of the programme and agree upon their engagement in execution of the programme
at their respective administrative units.
Particular attention should be given to those Provinces that are already in the elimination phase,
and if their health systems are strong enough, it is rational to pilot surveillance and other
elimination activities focusing on setting up adequate surveillance, databases and quality assurance
systems, preparing and testing relevant SOPs and training. A substantial effort should be
considered to increase human capacity for malaria elimination and train, motivate and sustain
health staff of different categories and CHWs throughout the country, with special focus on areas
eligible for elimination.
Since surveillance and M&E will be a key component of measuring the progress towards
elimination, national reporting and information systems for disease surveillance and health
management should be further strengthened at central, provincial and district levels by
validation/assessment of existing systems at all levels before Provinces become eligible to enter
the elimination phase.
The NMLCP should establish a Working Technical Committee that will be responsible for overall
coordination and guidance of elimination activities. The Committee should periodically review the
programme to ensure that it remains on track, and the level of inputs required to see the desired
programme impact is provided and sustained, since there is always some risk that financial
provisions of the funding agencies and government could not be sufficient.
A mechanism for periodic external reviews of the programme to assess the progress against
milestones and targets, identify possible gaps and advise on actions to solve these problems should
be built-in.

90
References
Eshghy N, Nushin MK. Evaluation of malathion as a residual spray for the control of
Anopheles culicifacies in the province of Helmand, southeast Afghanistan. Mosquito News
1978; 38: 268–74.
Eshghy N, Nushin MK. Insecticide resistance of Anopheles culicifacies in the province of
Helmand, southeast Afghanistan. Mosquito News 1978; 38: 97–101.
Gething, PW, Van Boeckel, TP, Smith, DL, Guerra, CA, Patil, AP, Snow, RW and Hay,
SI (2011). Modelling the global constraints of temperature on transmission of Plasmodium
falciparum and P vivax. Parasites and Vectors 4: 92 doi:101186/1756-3305-4-92.
Safi N, Hameed H, Sediqi W, Himmat E (2009). NMLEP Annual Report 2008.
Afghanistan Annual Malaria Journal, issue 1: 8-14.
Safi N, Leslie T, Rowland M (2009). Progress and Challenges to Malaria Control in
Afghanistan. Afghanistan Annual Malaria Journal, issue 1: 15-29.
Rowland M, Mohammed N, Rehman H, et al. Anopheline vectors and malaria transmission
in eastern Afghanistan. Trans. R. Soc. Trop. Med. Hyg. 2002; 96: 620–26.
Rowland M, Rab MA, Freeman T, Durrani N, Rehman N. Afghan refugees and the
temporal and spatial distribution of malaria in Pakistan. Soc. Sci. Med. 2002; 55: 2065–76.
Rowland M, Webster J, Saleh P, et al. Prevention of malaria in Afghanistan through social-
marketing of insecticide-treated nets: evaluation of coverage and effectiveness by cross-
sectional surveys and passive surveillance. Trop. Med. Int. Health 2002; 7: 813–22.
Natsuda J. et al. A population survey of the G6PD 563T (Mediterranean) mutation in
Afghanistan, PLOS ONE, volume 9, issue 2, 2014.
Annual Malaria Report 2015. Islamic Republic of Afghanistan, Ministry of Public Health.
Leslie T, Mikhail A, Mayan I, Anwar M, Bakhtash S, Nader M, et al. (2012). Over
diagnosis and mistreatment of malaria among febrile patients at primary healthcare level
in Afghanistan: observational study. BMJ; 345: e4389; 1-13.
Shaikh S, Memon H, Iohano B, Shaikh A, Ahmed I et. al. (2012). Severe disease in children
hospitalized with a diagnosis of Plasmodium vivax in south-eastern Pakistan. Malaria J,
11:144.
Zakeri S, Najafabadi S T, Zare A, and Djadid N D (2012). Detection of malaria parasites
by nested PCR in south-eastern, Iran: Evidence of highly mixed infections in Chahbahar
district. Malaria J, 1:2.
A Basic Package of Health Services for Afghanistan – 2009/1388. Islamic Republic of
Afghanistan, Ministry of Public Health. July 2009.
The Essential Package of Hospital Services for Afghanistan. Islamic Republic of
Afghanistan, Ministry of Public Health. July 2005.
National Strategy for Community-based Management of Malaria (CBMM) in Afghanistan
(2016-2020). Islamic Republic of Afghanistan, Ministry of Public Health 2016.
National Health Strategy 2016‒2020. Islamic Republic of Afghanistan, Ministry of Public
Health. June 20, 2016.
National Strategic Plan for Malaria Control and Elimination 2013 - 2017. Islamic Republic
of Afghanistan, Ministry of Public Health.
WHO. Guidelines for the treatment of malaria, 3rd Edition, Geneva: WHO, 2015.

91
WHO (2015). Control and Elimination of Plasmodium Vivax Malaria- A Technical Brief.
1-53.
Jamornthanyawat N, Awab G R, Tanomsing N, Pukrittayakamee S, et al. (2014). A
Population Survey of the Glucose-6-Phosphate Dehydrogenase (G6PD) 563C.T
(Mediterranean) Mutation in Afghanistan. PLoS ONE; 9 (2): e88605; 1-8.
WHO (2015). Malaria Microscopy- Quality Assurance Manual, (Version 2); 1-120.
Leslie T, Mayan I, Mohammed N, Erasmus P, Kolaczinski J, Whitty CJ, Rowland M.
(2008). A randomised trial of an eight-week, once weekly primaquine regimen to prevent
relapse of Plasmodium vivax in Northwest Frontier Province, Pakistan. PLoS ONE;
6;3(8):e2861.
The Second Malaria Indicator Survey in the Islamic Republic of Afghanistan, 2011.
Islamic Republic of Afghanistan, Ministry of Public Health. 2012.
Malaria death by health facility 2016. National Malaria and Leishmaniasis Control
programe data. Islamic Republic of Afghanistan, Ministry of Public Health.
Rahimi B A, Thakkinstian A, White N J, Sirivichayakul C, Dondorp A M, and
Chokejindachai W (2014). Severe vivax malaria: a systematic review and meta-analysis of
clinical studies since 1900. Malaria J, 13:481.
Awab G R, Imwong M, Sasithon Pukrittayakamee, Alim F, Hanpithakpong W, et al.
(2016). Clinical trials of artesunate plus sulfadoxine‑pyrimethamine for Plasmodium
falciparum malaria in Afghanistan: maintained efficacy a decade after introduction. Malar
J; 15:121.
Awab G R, Nahzat M S, Habib M N and Baryalai S A (2015). Therapeutic Efficacy of
Anti-Malarial Drugs in the treatment of uncomplicated malaria in Afghanistan, 2007-2013.
Invest in the future: Defeat Malaria. (Afghanistan); P 86-90.
Ahmad, M., C. Buhler, et al. (2016). "Status of insecticide resistance in high-risk malaria
provinces in Afghanistan." Malaria Journal 15(1): 98.
Ahmadhi, A. A., N. H. Zahid Safi, et al. (2015). "Insecticide susceptibility survey in
Afghanistan, 2011 " Afghanistan Annual Malaria Journal 35-50.
Barwa, C. (2011). Status of insecticide susceptibility in Afghanistan, Islamic Republic of
Afghanistan, Ministry of Public Health, General Directorate of Preventive Medicine and
Primary Health Care, Communicable Disease Directorate
National Malaria and Leishmaniasis Control Program.
Enayati, A., J. Lines, et al. (2009). "Suppressing the vector." Shrinking the malaria map: a
prospectus on malaria elimination: 140-154.
Faulde, M. K., R. Hoffmann, et al. (2007). "Malaria Reemergence in Northern
Afghanistan." Emerging Infectious Diseases 13(9): 1402-1404.
HealthNet (2015). Evaluating insecticide resistance status in wild-caught Anopheles
mosquitoes in Afghanistan N. M. L. C. P. Healthnet TPO, Ministry of Public Health,
Afghanistan.
Kolaczinski, J., K. Graham, et al. (2005). "Malaria control in Afghanistan: progress and
challenges." The Lancet 365(9469): 1506-1512.
Leslie, T., N. Mohammed, et al. (2008). "Vector Surveillance in Nangahar Province,
Afghanistan; ." Afghanistan Annual Malaria Journal(1): 129-141.

92
MoPH (2008). Malaria Indicator Survey. M. o. P. H. Islamic Republic of Afghanistan,
General Directorate of Preventive Medicine and Primary Health Care, Communicable
Disease Directorate and A. National Malaria and Leishmaniasis Control Programme.
MoPH (2009). A Basic Package of Health Services for Afghanistan – 2009/1388. Islamic
Republic of Afghanistan. M. o. P. H. Islamic Republic of Afghanistan, General Directorate
of Preventive Medicine and Primary Health Care, Communicable Disease Directorate and
A. National Malaria and Leishmaniasis Control Programme.
MoPH (2011). Malaria Indicator Survey. M. o. P. H. Islamic Republic of Afghanistan,
General Directorate of Preventive Medicine and Primary Health Care, Communicable
Disease Directorate and A. National Malaria and Leishmaniasis Control Programme.
MoPH (2013). National Malaria Strategic plan 2013-1017. M. o. P. H. Islamic Republic of
Afghanistan, General Directorate of Preventive Medicine and Primary Health Care,
Communicable Disease Directorate and A. National Malaria and Leishmaniasis Control
Programme.
MoPH (2013). Updated National Malaria Monitoring and Evaluation Plan. M. o. P. H.
Islamic Republic of Afghanistan, General Directorate of Preventive Medicine and Primary
Health Care, Communicable Disease Directorate and A. National Malaria and
Leishmaniasis Control Programme.
MoPH (2014). Malaria Indicator Survey. M. o. P. H. Islamic Republic of Afghanistan,
General Directorate of Preventive Medicine and Primary Health Care, Communicable
Disease Directorate and A. National Malaria and Leishmaniasis Control Programme.
MoPH (2015). Annual Malaria report. M. o. P. H. Islamic Republic of Afghanistan,
General Directorate of Preventive Medicine and Primary Health Care, Communicable
Disease Directorate and A. National Malaria and Leishmaniasis Control Programme.
Rowland, M., N. Mohammed, et al. (2002). "Anopheline vectors and malaria transmission
in eastern Afghanistan." Trans R Soc Trop Med Hyg 96(6): 620-626.
Sabot, O., J. Tulloch, et al. (2009). "Getting to Zero." Shrinking the malaria map: a
prospectus on malaria elimination: 19-39.
Safi, N., H. Hameed, et al. (2009). "NMLEP Annual Report 2008. ." Afghanistan Annual
Malaria Journal(1): 8-14.
Ward, R. A. (1972). "Mosquitoes of Afghanistan - An Annotated Checklist " Mosquito
Systematics 4 (3): 93-97.
Disease Surveillance for Malaria Control: An Operational Manual, World Health
Organization, 2012.
Disease Surveillance for Malaria Elimination: An Operational Manual, World Health
Organization, 2012.
D’Acremont V, Lengeler C, Genton B. Reduction in the proportion of fevers associated
with Plasmodium falciparum parasitaemia in Africa: a systematic review. Malaria Journal,
2010, 9:240.
Najera J. et. Al. Malaria epidemics: Detection, Control, Forecasting and Prevention,
WHO/MAL98.1084, Geneva, 1998.
Updated National Malaria M&E Plan, 2013-2017, MoPH/NMLCP, 2013.
Malaria Elimination Plan 2013-2017, MoPH/NMLCP, 2013.

93
Annexes: Chart 1: NMLCP organogram 2010

94
Table 2: Malaria data 2002-2015, Afghanistan
Year Population
Confierm Malaria at Aomunity level Confierm Malaria
Hospitals, CHCs, BHCs Clinical Malaria
Cases Malaria Cases
Total Cases
Deaths All
Deaths Malaria
ABER SPR %
TPR %
Proportion of
Confirmed among
total slide examined
Incidence Rate/1000
P
Incidence Rate
Positive Cases/1000
P
Incidence Rate
PF/1000 P
Incidence Rate
Pv/1000 P
estimated confirmed
among clinical
estimated confirmed
Estimated incidence Positive
Cases/1000 P
RDT Consumed
RDT Mix
RDT PF Positive
RDT PV Positive
Slide Examin
Pf Pv Malaria
HPs CHC, BHC
Confirmed Clinical Confirm
+ Clinical
2002 20297800 NA NA NA NA NA 84528 330083 * 212228 414611 212228 626839 NA NA NA NA NA NA 3.09 2.04 4.16 16.26 NA NA NA
2003 20691400 NA NA NA NA NA 44243 316697 * 224662 360940 224662 585602 NA NA NA NA NA NA 2.83 1.74 2.14 15.31 NA NA NA
2004 21677700 NA NA NA NA NA 12789 229233 10307 21048 242022 31355 273377 NA NA NA NA NA NA 1.26 1.12 0.59 10.57 NA NA NA
2005 22097900 NA NA NA NA NA 5917 110527 78769 131481 116444 210250 326694 NA NA NA NA NA NA 1.48 0.53 0.27 5.00 NA NA NA
2006 22575900 NA NA NA NA NA 6216 79913 155110 173168 86129 328278 414407 NA NA NA NA NA NA 1.84 0.38 0.28 3.54 NA NA NA
2007 23038900 NA NA NA NA NA 6283 85919 182819 186262 92202 369081 461283 NA NA NA NA NA NA 2.00 0.40 0.27 3.73 NA NA NA
2008 23511400 NA NA NA NA 549494 4355 77219 159509 226040 81574 385549 467123
8,334 46 2.34 14.85 14.85 0.15 1.99 0.35 0.19 3.28 57236 138810 5.90
2009 23993500 NA NA NA NA 521817 4026 60854 148602 177247 64880 325849 390729
8,197 32 2.17 12.43 12.43 0.12 1.63 0.27 0.17 2.54 40514 105394 4.39
2010 23432900 NA NA NA NA 524523 6142 63255 137670 185396 69397 323066 392463
9,266 22 2.24 13.23 13.23 0.13 1.67 0.30 0.26 2.70 42743 112140 4.79
2011 24987700 NA NA NA NA 531053 5581 71968 193442 211757 77549 405199 482748
10,910 40 2.13 14.60 14.60 0.15 1.93 0.31 0.22 2.88 59171 136720 5.47
2012 25427322 NA NA NA NA 511408 1231 53609 177827 158698 54840 336525 391365
12,384 36 2.01 10.72 10.72 0.11 1.54 0.22 0.05 2.11 36087 90927 3.58
2013 25740700 NA NA NA NA 507145 2272 43842 114258 159370 46114 273628 319742
14,679 24 1.97 9.09 9.09 0.09 1.24 0.18 0.09 1.70 24881 70995 2.76
2014 26588632 155919 1566 1417 19575 514466 3000 58362 51386 159744 83920 211130 295050
15,991 32 2.52 16.31 12.52 0.13 1.11 0.32 0.23 2.93 26430 110350 4.15
2015 27101365 138026 700 316 15466 538789 4004 82891 50437 212712 103377 263149 366526
17,450 49 2.50 19.19 15.27 0.15 1.35 0.38 0.19 3.63 40193 143570 5.30

95
Table 3: Malaria data 2013-2015 by Provinces, Afghanistan
Province Year Population Clinical Malaria
HF
Malaria HP
RDT Consumed
RDT Mix
RDT PF Positive
RDT PV Positive
Total Malaria Slides
Examined
Slide PF Positive
Slide PV
Positive
Total Confirmed
Total Clinical
Total Malaria
ABER SPR %
TPR %
Proportion of
Confirmed among
total slide examined
Incidence Rate/1000
P
Incidence Rate
Positive Cases/1000
P
Incidence Rate
PF/1000 P
Incidence Rate
Pv/1000 P
estimated confirmed
among clinical
estimated confirmed
Estimated incidence Positive
Cases/1000 P
Badakhshan 2013 919900 5784 4808 14408 4 1140 1144 10592 11736 1.57 7.94 7.94 0.08 12.76 1.24 0.00 1.24 841.01 1985.01 2.16
Badakhshan 2014 935327 3544 2225 10516 103 131 1103 13149 5 1158 2500 5769 8269 2.53 19.01 10.56 0.11 8.84 2.67 0.15 2.42 609.44 3109.44 3.32
Badakhshan 2015 950953 3110 2526 5238 17 8 572 15408 52 1238 1887 5636 7523 2.17 12.25 9.14 0.09 7.91 1.98 0.06 1.90 515.12 2402.12 2.53
Badghis 2013 479800 1409 1686 1997 4 28 32 3095 3127 0.42 1.60 1.60 0.02 6.52 0.07 0.01 0.06 49.59 81.59 0.17
Badghis 2014 487838 2075 1075 955 2 13 15 3150 3165 0.20 1.57 1.57 0.02 6.49 0.03 0.00 0.03 49.48 64.48 0.13
Badghis 2015 495958 2658 1081 82 0 0 0 960 2 18 20 3739 3759 0.21 2.08 1.92 0.02 7.58 0.04 0.00 0.04 71.77 91.77 0.19
Baghlan 2013 855400 148 199 3246 3 21 24 347 371 0.38 0.74 0.74 0.01 0.43 0.03 0.00 0.02 2.57 26.57 0.03
Baghlan 2014 894838 39 504 4508 0 0 0 3398 1 8 9 543 552 0.88 0.26 0.11 0.00 0.62 0.01 0.00 0.01 0.62 9.62 0.01
Baghlan 2015 910784 89 6 3441 0 0 0 2010 5 31 36 95 131 0.60 1.79 0.66 0.01 0.14 0.04 0.01 0.03 0.63 36.63 0.04
Balkh 2013 1318000 832 2902 3680 4 138 142 3734 3876 0.28 3.86 3.86 0.04 2.94 0.11 0.00 0.10 144.08 286.08 0.22
Balkh 2014 1298247 467 720 7783 15 50 29 3737 0 124 218 1187 1405 0.89 5.83 1.89 0.02 1.08 0.17 0.04 0.12 22.46 240.46 0.19
Balkh 2015 1325659 869 588 7450 7 8 13 3811 10 142 180 1457 1637 0.85 4.72 1.60 0.02 1.23 0.14 0.01 0.12 23.29 203.29 0.15
Bamyan 2013 432700 360 331 804 7 34 41 691 732 0.19 5.10 5.10 0.05 1.69 0.09 0.02 0.08 35.24 76.24 0.18
Bamyan 2014 439899 289 289 223 0 2 12 729 7 46 67 578 645 0.22 9.19 7.04 0.07 1.47 0.15 0.02 0.13 40.68 107.68 0.24
Bamyan 2015 447218 528 145 1468 0 0 13 813 16 14 43 673 716 0.51 5.29 1.89 0.02 1.60 0.10 0.04 0.06 12.69 55.69 0.12
Dykundi 2013 378900 1359 597 2594 4 47 51 1956 2007 0.68 1.97 1.97 0.02 5.30 0.13 0.01 0.12 38.46 89.46 0.24
Dykundi 2014 417476 1256 773 755 0 0 13 1043 10 27 50 2029 2079 0.43 4.79 2.78 0.03 4.98 0.12 0.02 0.10 56.42 106.42 0.25
Dykundi 2015 424339 1088 668 244 1 0 16 1389 9 18 44 1756 1800 0.38 3.17 2.69 0.03 4.24 0.10 0.02 0.08 47.31 91.31 0.22
Farah 2013 490600 282 55 1186 5 15 20 337 357 0.24 1.69 1.69 0.02 0.73 0.04 0.01 0.03 5.68 25.68 0.05
Farah 2014 498951 284 26 658 1 17 18 310 328 0.13 2.74 2.74 0.03 0.66 0.04 0.00 0.03 8.48 26.48 0.05
Farah 2015 507405 343 38 815 7 13 20 381 401 0.16 2.45 2.45 0.02 0.79 0.04 0.01 0.03 9.35 29.35 0.06
Faryab 2013 964600 1360 2541 3527 3 26 29 3901 3930 0.37 0.82 0.82 0.01 4.07 0.03 0.00 0.03 32.08 61.08 0.06
Faryab 2014 981197 1005 1893 1991 98 0 895 3145 0 19 1012 2898 3910 0.52 32.18 19.70 0.20 3.98 1.03 0.00 0.93 571.02 1583.02 1.61
Faryab 2015 998147 1186 1275 1395 1 0 0 2413 0 0 1 2461 2462 0.38 0.04 0.03 0.00 2.47 0.00 0.00 0.00 0.65 1.65 0.00
Ghazni 2013 1188600 3549 452 14258 41 1307 1348 4001 5349 1.20 9.45 9.45 0.09 4.50 1.13 0.03 1.10 378.27 1726.27 1.45
Ghazni 2014 1240437 2553 688 1896 9 22 25 14710 52 1304 1412 3241 4653 1.34 9.60 8.50 0.09 3.75 1.14 0.06 1.07 275.58 1687.58 1.36
Ghazni 2015 1228831 2371 352 5405 13 21 99 11987 46 733 912 2723 3635 1.42 7.61 5.24 0.05 2.96 0.74 0.05 0.68 142.79 1054.79 0.86
Ghor 2013 668000 1095 491 585 29 15 44 1586 1630 0.09 7.52 7.52 0.08 2.44 0.07 0.04 0.02 119.29 163.29 0.24
Ghor 2014 679085 932 475 415 22 5 27 1407 1434 0.06 6.51 6.51 0.07 2.11 0.04 0.03 0.01 91.54 118.54 0.17
Ghor 2015 690296 662 342 339 29 7 36 1004 1040 0.05 10.62 10.62 0.11 1.51 0.05 0.04 0.01 106.62 142.62 0.21
Helmand 2013 867600 12126 813 10776 63 375 438 12939 13377 1.24 4.06 4.06 0.04 15.42 0.50 0.07 0.43 525.92 963.92 1.11
Helmand 2014 909395 11501 1344 3741 70 1 2 11099 33 202 308 12845 13153 1.63 2.78 2.08 0.02 14.46 0.34 0.04 0.22 266.59 574.59 0.63
Helmand 2015 924711 11210 1421 4495 3 0 7 8651 8 99 117 12631 12748 1.42 1.35 0.89 0.01 13.79 0.13 0.01 0.11 112.42 229.42 0.25
Hirat 2013 1816100 905 1886 2285 3 3 2791 2794 0.13 0.13 0.13 0.00 1.54 0.00 0.00 0.00 3.66 6.66 0.00
Hirat 2014 1852790 957 756 4181 1 0 16 1386 0 8 25 1713 1738 0.30 1.80 0.45 0.00 0.94 0.01 0.00 0.01 7.69 32.69 0.02
Hirat 2015 1890202 450 875 5202 0 0 0 1391 1 11 12 1325 1337 0.35 0.86 0.18 0.00 0.71 0.01 0.00 0.01 2.41 14.41 0.01
Jawzjan 2013 521400 1376 2591 2462 15 6 21 3967 3988 0.47 0.85 0.85 0.01 7.65 0.04 0.03 0.01 33.84 54.84 0.11
Jawzjan 2014 530751 245 1430 398 0 4 2 1559 0 9 15 1675 1690 0.37 0.96 0.77 0.01 3.18 0.03 0.01 0.02 12.84 27.84 0.05
Jawzjan 2015 540255 1763 1238 866 8 0 2 1924 0 22 32 3001 3033 0.52 1.66 1.15 0.01 5.61 0.06 0.00 0.04 34.42 66.42 0.12
Kabul 2013 4086500 6422 1019 23568 74 1133 1207 7441 8648 0.58 5.12 5.12 0.05 2.12 0.30 0.02 0.28 381.08 1588.08 0.39
Kabul 2014 4227261 7162 809 2371 1 1 294 25636 35 1719 2050 7971 10021 0.66 8.00 7.32 0.07 2.37 0.48 0.01 0.48 583.45 2633.45 0.62

96
Kabul 2015 4372977 9066 703 1690 0 20 583 28653 61 2811 3475 9769 13244 0.69 12.13 11.45 0.11 3.03 0.79 0.02 0.78 1118.78 4593.78 1.05
Kandahar 2013 1119000 3358 4577 6215 5 99 104 7935 8039 0.56 1.67 1.67 0.02 7.18 0.09 0.00 0.09 132.78 236.78 0.21
Kandahar 2014 1200929 3216 3332 5613 1 70 71 6548 6619 0.47 1.26 1.26 0.01 5.51 0.06 0.00 0.06 82.83 153.83 0.13
Kandahar 2015 1226593 2488 2371 2237 0 0 0 4851 1 150 151 4859 5010 0.58 3.11 2.13 0.02 4.08 0.12 0.00 0.12 103.51 254.51 0.21
Kapisa 2013 426800 1107 13 7527 1 275 276 1120 1396 1.76 3.67 3.67 0.04 3.27 0.65 0.00 0.64 41.07 317.07 0.74
Kapisa 2014 433867 720 0 5148 0 109 109 720 829 1.19 2.12 2.12 0.02 1.91 0.25 0.00 0.25 15.24 124.24 0.29
Kapisa 2015 441010 653 0 5855 0 140 140 653 793 1.33 2.39 2.39 0.02 1.80 0.32 0.00 0.32 15.61 155.61 0.35
Khost 2013 556000 4352 4666 14161 121 1298 1419 9018 10437 2.55 10.02 10.02 0.10 18.77 2.55 0.22 2.33 903.65 2322.65 4.18
Khost 2014 565211 3935 1272 7865 145 96 386 18359 45 1174 1846 5207 7053 4.64 10.06 7.04 0.07 12.48 3.27 0.25 2.76 366.54 2212.54 3.91
Khost 2015 574582 5008 1437 6884 298 110 407 12786 84 1028 1927 6445 8372 3.42 15.07 9.80 0.10 14.57 3.35 0.34 2.50 631.39 2558.39 4.45
Kunar 2013 436000 18667 20436 39298 173 5354 5527 39103 44630 9.01 14.06 14.06 0.14 102.36 12.68 0.40 12.28 5499.57 11026.57 25.29
Kunar 2014 443272 17653 5545 21625 299 504 4185 43731 474 8349 13811 23198 37009 14.74 31.58 21.13 0.21 83.49 31.16 2.21 28.28 4902.19 18713.19 42.22
Kunar 2015 450652 26040 6630 13678 26 33 3260 41970 249 8890 12458 32670 45128 12.35 29.68 22.39 0.22 100.14 27.64 0.63 26.96 7313.88 19771.88 43.87
Kunduz 2013 972200 1519 1961 9260 53 53 3480 3533 0.95 0.57 0.57 0.01 3.63 0.05 0.00 0.05 19.92 72.92 0.08
Kunduz 2014 990937 495 506 2430 4 1 8 7007 1 38 52 1001 1053 0.95 0.74 0.55 0.01 1.06 0.05 0.00 0.05 5.52 57.52 0.06
Kunduz 2015 1010037 177 317 1390 0 0 0 5505 0 21 21 494 515 0.68 0.38 0.30 0.00 0.51 0.02 0.00 0.02 1.50 22.50 0.02
Laghman 2013 431200 12226 12108 37810 49 2142 2191 24334 26525 8.77 5.79 5.79 0.06 61.51 5.08 0.11 4.97 1410.10 3601.10 8.35
Laghman 2014 438346 21353 1939 6217 63 94 1534 44210 643 6637 8971 23292 32263 11.50 20.29 17.79 0.18 73.60 20.47 1.68 18.64 4143.66 13114.66 29.92
Laghman 2015 445588 34543 3180 20847 75 51 3744 57512 776 14040 18686 37723 56409 17.59 32.49 23.85 0.24 126.59 41.94 1.86 39.91 8995.67 27681.67 62.12
Logar 2013 379400 902 311 2701 18 157 175 1213 1388 0.71 6.48 6.48 0.06 3.66 0.46 0.05 0.41 78.59 253.59 0.67
Logar 2014 385638 843 213 2028 11 8 451 3100 8 400 878 1056 1934 1.33 28.32 17.12 0.17 5.02 2.28 0.04 2.21 180.80 1058.80 2.75
Logar 2015 392045 1238 658 562 22 1 57 3966 12 485 577 1896 2473 1.15 14.55 12.74 0.13 6.31 1.47 0.03 1.38 241.61 818.61 2.09
Nangarhar 2013 1462600 49533 30624 236080 1441 25217 26658 80157 106815 16.14 11.29 11.29 0.11 73.03 18.23 0.99 17.24 9051.28 35709.28 24.41
Nangarhar 2014 1489787 47700 15332 43626 656 448 9188 235431 1438 32366 44096 63032 107128 18.73 18.73 15.80 0.16 71.91 29.60 1.27 27.89 9960.18 54056.18 36.28
Nangarhar 2015 1517388 79211 17996 22479 183 42 5272 252131 2357 47815 55669 97207 152876 18.10 22.08 20.27 0.20 100.75 36.69 1.58 34.99 19705.82 75374.82 49.67
Nimroz 2013 152800 262 45 82 2 2 307 309 0.05 2.44 2.44 0.02 2.02 0.01 0.00 0.01 7.49 9.49 0.06
Nimroz 2014 162135 198 43 81 0 1 1 241 242 0.05 1.23 1.23 0.01 1.49 0.01 0.00 0.01 2.98 3.98 0.02
Nimroz 2015 164978 207 39 197 5 1 6 246 252 0.12 3.05 3.05 0.03 1.53 0.04 0.03 0.01 7.49 13.49 0.08
Nooristan 2013 143200 2407 1005 4797 26 355 381 3412 3793 3.35 7.94 7.94 0.08 26.49 2.66 0.18 2.48 271.00 652.00 4.55
Nooristan 2014 145574 2513 527 705 0 0 128 5585 19 519 666 3040 3706 4.32 11.92 10.59 0.11 25.46 4.57 0.13 4.44 321.88 987.88 6.79
Nooristan 2015 147967 4009 323 1895 1 1 243 8239 41 1482 1768 4332 6100 6.85 21.46 17.45 0.17 41.23 11.95 0.28 11.66 755.77 2523.77 17.06
Paktika 2013 420700 12126 1979 16120 59 1351 1410 14105 15515 3.83 8.75 8.75 0.09 36.88 3.35 0.14 3.21 1233.75 2643.75 6.28
Paktika 2014 427692 16816 1752 1980 10 23 412 20799 98 1839 2382 18568 20950 5.33 11.45 10.46 0.10 48.98 5.57 0.28 5.26 1941.66 4323.66 10.11
Paktika 2015 434742 13513 1539 1930 8 5 510 22839 164 1530 2217 15052 17269 5.70 9.71 8.95 0.09 39.72 5.10 0.39 4.69 1347.26 3564.26 8.20
Paktya 2013 525500 3187 2364 10437 53 916 969 5551 6520 1.99 9.28 9.28 0.09 12.41 1.84 0.10 1.74 515.37 1484.37 2.82
Paktya 2014 542896 1861 1890 2213 50 9 373 12761 51 1032 1515 3751 5266 2.76 11.87 10.12 0.10 9.70 2.79 0.11 2.59 379.51 1894.51 3.49
Paktya 2015 551987 2105 917 3439 2 3 449 9837 33 931 1418 3022 4440 2.41 14.41 10.68 0.11 8.04 2.57 0.07 2.50 322.78 1740.78 3.15
Panjsher 2013 137700 224 15 3895 20 20 239 259 2.83 0.51 0.51 0.01 1.88 0.15 0.00 0.15 1.23 21.23 0.15
Panjsher 2014 151004 97 13 188 0 0 0 2377 0 21 21 110 131 1.70 0.88 0.82 0.01 0.87 0.14 0.00 0.14 0.90 21.90 0.15
Panjsher 2015 153487 141 8 263 0 0 0 1843 0 18 18 149 167 1.37 0.98 0.85 0.01 1.09 0.12 0.00 0.12 1.27 19.27 0.13
Parwan 2013 642300 392 105 2803 36 36 497 533 0.44 1.28 1.28 0.01 0.83 0.06 0.00 0.06 6.38 42.38 0.07
Parwan 2014 653362 427 92 798 0 0 1 1720 0 32 33 519 552 0.39 1.92 1.31 0.01 0.84 0.05 0.00 0.05 6.80 39.80 0.06
Parwan 2015 664502 436 74 1428 0 0 7 1558 0 47 54 510 564 0.45 3.47 1.81 0.02 0.85 0.08 0.00 0.08 9.22 63.22 0.10
Samangan 2013 335700 200 224 242 10 10 424 434 0.07 4.13 4.13 0.04 1.29 0.03 0.00 0.03 17.52 27.52 0.08
Samangan 2014 381459 533 302 1352 0 0 0 345 0 27 27 835 862 0.44 7.83 1.59 0.02 2.26 0.07 0.00 0.07 13.29 40.29 0.11
Samangan 2015 387928 366 315 1684 0 0 0 365 0 4 4 681 685 0.53 1.10 0.20 0.00 1.77 0.01 0.00 0.01 1.33 5.33 0.01
Sar-e-Pul 2013 451000 1425 1450 1591 3 92 95 2875 2970 0.35 5.97 5.97 0.06 6.59 0.21 0.01 0.20 171.67 266.67 0.59

97
Sar-e-Pul 2014 550238 928 994 0 0 0 0 1442 6 49 55 1922 1977 0.26 3.81 3.81 0.04 3.59 0.10 0.01 0.09 73.31 128.31 0.23
Sar-e-Pul 2015 559577 909 458 4797 0 0 2 1594 13 103 118 1367 1485 1.14 7.40 1.85 0.02 2.65 0.21 0.02 0.19 25.24 143.24 0.26
Takhar 2013 950100 2335 9615 8109 4 178 182 11950 12132 0.85 2.24 2.24 0.02 12.77 0.19 0.00 0.19 268.21 450.21 0.47
Takhar 2014 966576 1731 3058 14743 30 5 378 8067 2 214 629 4789 5418 2.36 7.80 2.76 0.03 5.61 0.65 0.01 0.61 132.06 761.06 0.79
Takhar 2015 983336 1107 1904 10481 33 2 107 9190 1 287 430 3011 3441 2.00 4.68 2.19 0.02 3.50 0.44 0.00 0.40 65.82 495.82 0.50
Urozgan 2013 339200 3007 739 4534 34 162 196 3746 3942 1.34 4.32 4.32 0.04 11.62 0.58 0.10 0.48 161.94 357.94 1.06
Urozgan 2014 380469 2461 654 3170 6 83 89 3115 3204 0.83 2.81 2.81 0.03 8.42 0.23 0.02 0.22 87.46 176.46 0.46
Urozgan 2015 386818 1812 602 1244 2 11 1 3150 2 94 110 2414 2524 1.14 3.49 2.50 0.03 6.53 0.28 0.03 0.25 60.43 170.43 0.44
Wardak 2013 577100 460 83 3660 4 160 164 543 707 0.63 4.48 4.48 0.04 1.23 0.28 0.01 0.28 24.33 188.33 0.33
Wardak 2014 586623 700 53 270 0 0 24 3518 13 305 342 753 1095 0.65 9.72 9.03 0.09 1.87 0.58 0.02 0.56 67.98 409.98 0.70
Wardak 2015 596287 849 24 699 0 0 90 4612 17 359 466 873 1339 0.89 10.10 8.77 0.09 2.25 0.78 0.03 0.75 76.60 542.60 0.91
Zabul 2013 294100 4674 1567 12447 25 1677 1702 6241 7943 4.23 13.67 13.67 0.14 27.01 5.79 0.09 5.70 853.39 2555.39 8.69
Zabul 2014 299125 3255 862 11516 1 18 116 10383 27 438 600 4117 4717 7.32 5.78 2.74 0.03 15.77 2.01 0.15 1.85 112.80 712.80 2.38
Zabul 2015 304126 2507 387 5113 0 0 12 10225 3 309 324 2894 3218 5.04 3.17 2.11 0.02 10.58 1.07 0.01 1.06 61.13 385.13 1.27

98
Table 5: Province-wise data on malaria outbreaks 2013-2015, Afghani
Re
po
rte
d D
ate
Inve
stig
atio
n D
ate
Epi W
ee
k
Ru
mo
r
Clin
ical
Co
nfi
rme
d
Lab
Co
nfi
rme
d
U5
Mal
e
O5
Mal
e
U5
Fem
ale
O5
Fem
ale
U5
de
ath
O5
de
ath
No
Clo
se C
on
tact
s
Vill
age
Dis
tric
t
Pro
vin
ce
Re
gio
n
Mal
e
Fem
ale
Ch
ildre
n_<
5
Re
po
rte
d%
Ass
ess
ed
%
No
Sp
eci
me
ns
Co
llect
ed
Dat
e S
pe
cim
en
s
sen
t
No
Po
siti
ve
Spe
cim
en
s
Dat
e r
esu
lt
Shar
ed
On
goin
g
Co
ntr
olle
d
Dat
e o
utb
reak
Star
ted
Dat
e o
utb
reak
d
ecl
are
d o
ver
Re
mar
ks
08-Jun-11 09-Jun-11 23 No Yes No 216 0 0 0 Daman Behsod Nangarhar East 408 498 181 0 5 4 Yes No
09-Jul-11 10-Jul-11 28 No Yes No 143 0 0 0 Lamatek Narang Kunar East 1118 1048 433 82 3 3 Yes No
16-Jul-11 21-Jul-11 29 Yes No No 359 0 0 0 Sheikhan Daman Behsod Nangarhar East 408 398 161 50 7 7 Yes No
03-Sep-11 04-Sep-11 40 Yes No No 33 62 0 0 0 Gultapa Alishang Laghman East 287 309 119 65 5 2 Yes No
30-Jun-12 01-Jul-12 27 No No Yes 0 0 0 245 0 0 Qalai Malakh Behsood Nangarhar East 507 446 191 564 245 No Yes
the team investigated the situation, SPR became 43.4% and team concluded the investigation as malaria peak incidence.
10-Jul-12 10-Jul-12 28 No Yes 0 0 0 0 6 0 0 Ahmad Shah Baba Center Kabul Central East 6 No Yes
30-Aug-14 31-Aug-14 35 No No Yes 47 34 57 4 0 0 0 Different villages of Shigal Shigal Kunar East 17200 16581 6756 186 100 02-Sep-14 No Yes 23-Aug-14 02-Sep-14
cases were treated by anti malaria drugs, proper HE messages provided and anti malaria steps have been taken.
08-Sep-14 08-Sep-14 36 No No Yes 23 37 16 21 0 0 0 Deffirent villages Watapoor Kunar East 440 380 164 88 No Yes 01-Sep-14 09-Oct-14 cases were treated by anti malaria drugs, proper HE messages provided and anti malaria steps have been taken.
15-Sep-14 16-Sep-14 37 No No Yes 16 70 19 64 0 0 0 Koz Kashkt Khiwa Nangarahr East 598 566 233 388 16-Sep-14 162 16-Sep-14 No Yes 10-Sep-14 20-Sep-14 cases were treated by anti malaria drugs, proper HE messages provided and anti malaria steps have been taken.
22-Dec-14 23-Dec-14 51 No Yes No 4 2 2 6 0 0 14 Sullah Tarinkot Urozgan South 280 280 140 80 30 9 24-Dec-14 No Yes 16-Dec-14 23-Dec-14
25-Aug-15 31-Aug-15 35 No No Yes 0 0 0 Sangarsaray CHC Kama Nangarhar East 17723 13000 6145 85 31-Aug-15 83 06-Sep-15 Yes No 25-Aug-15
"698 Cases were detected and treated during 3 Months(Jauza,Sartan and Asad) 1394 by anti malaria drugs,proper HE messages provided and anti malaria preventive steps have been taken by Sangarsray CHC "
25-Aug-15 02-Sep-15 35 No No Yes 0 0 0 Khiwa CHC Khiwa Nangarhar East 12790 8000 4158 70 02-Sep-15 69 06-Sep-15 Yes No 25-Aug-15
"713 Cases were detected and treated during 3 Months(Jauza,Sartan and Asad) 1394 by anti malaria drugs,proper HE messages provided and anti malaria preventive steps have been taken by Khiwa CHC "
25-Aug-15 26-Aug-15 34 No No Yes 6 2 0 7 0 0 Pestakhar Teshkan Badakhshan North East 5800 50 25-Aug-15 35 15-Aug-15 No 10-Aug-15