malignant hyperthermia and dantrolene sodium
TRANSCRIPT
Malignant Hyperthermia and Dantrolene Sodium
R.Srihari
Topics for Discussion
• Introduction• Pathophysiology• Triggering Agents• Clinical Presentation• Clinical Features• Laboratory Findings• Clinical Diagnosis• Differential diagnosis• Management
Introduction
• Malignant hyperthermia(MH) manifests manifests clinically as a hypermetabolic crises when an MH susceptible individual – exposed to volatile anesthetic or succinyl choline
• Incidence – estimated to be 1:100000 anesthetics administered –Males > Females– Children less than 19 contribute to ~ 50%
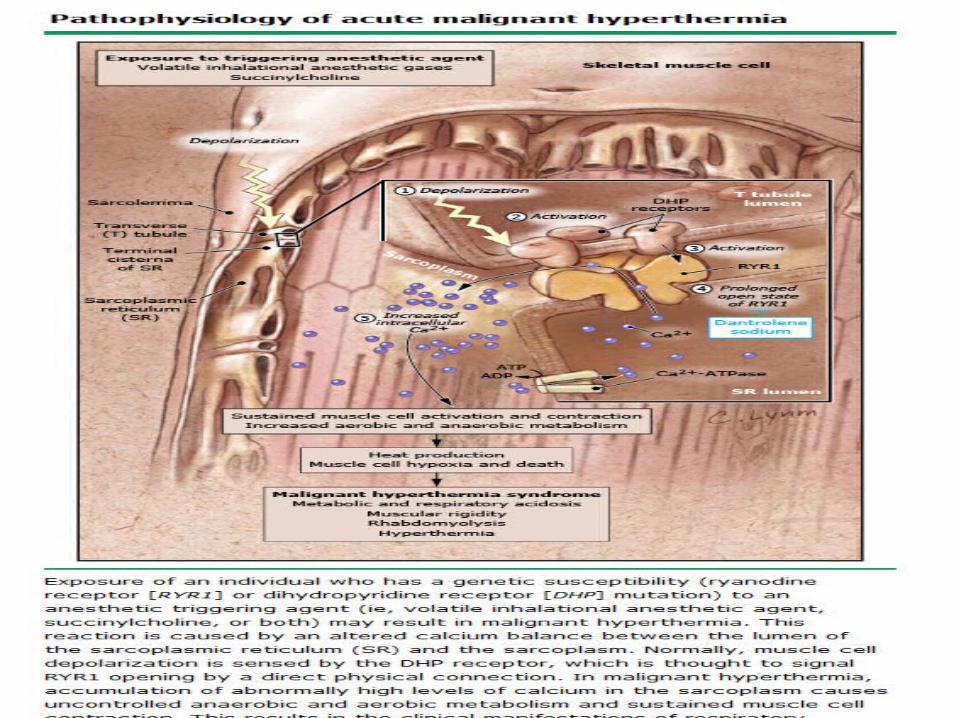
Pathophysiology
• MH susceptible patients have genetic skeletal muscle receptor abnormalities allowing excessive calcium accumulation in presence of certain anesthetic triggering agents
• Mechanism how anesthetic triggers MH by interacting with the receptors – Unknown
• Due to an episode of MH Clinical manifestations are due to cellular hypermetabolism sustained muscle contraction and breakdown( rhabdomyolysis) anaerobic metabolism acidosis sequelae
• Normal Muscle Physiology:– Depolarization spreads throughout the muscle cell
via t-tubule system
Activates Dihydropyridine(DHP) receptors located in t-tubule membrane
These receptors are coupled to ryanodine receptors which are calcium channels embedded In the wall of Sarcoplasmic reticulum
Calcium release through DHP receptor trigger RYR1 receptors to release calcium from SR into intracellular space
Calcium combines with troponin to cross link actin and myosin resulting in muscle cell contraction
Reuptake of calcium by Sarcoplasmic reticulum ATPase leads to muscle cell relaxation
• Malignant Hyperthermia:– MH susceptible patients have mutations for
abnormal RYR1 or DHP receptors
unregulated passage of calcium from sarcoplasmic reticulum into intracellular space
ACUTE MH CRISIS
Accelerated levels of aerobic metabolism sustain muscle for a time, but produce CO2 and cellular acidosis and deplete oxygen and ATP
Early signs: Hypercarbia + Respiratory/ Metabolic acidosis
A change to anaerobic metabolism worsens acidosis with production of lactate
– Once energy stores are depleted , rhabdomyolysis occurs and results in hyperkalemia and myoglobinuriaHyperkalemia occurs early in Muscular patients
– Overtime sustained contractions generates more heat than the body is able to dissipate
Marked hyperthermia occurs minutes to hours following onset of symptoms
Core body temperature may increase rise 1 C every few minutes
Severe hyperthermia leads to increase in CO2 production and increased Oxygen consumption with widespread organ dysfunction DIC
Triggering Agents
• Vast majority of patients developed MH while patient was receiving volatile anesthetic agent with or without succinylcholine
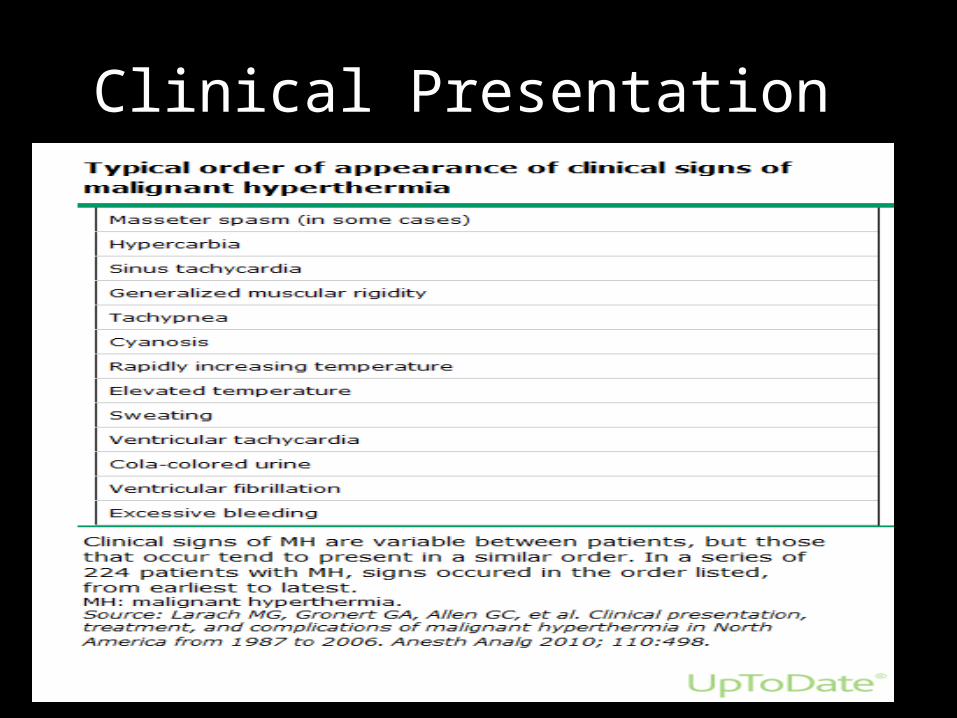
Clinical Presentation
• Clinical signs present perioperatively in several possible patterns– Intraoperatively during any phase of anesthetic
manifested by gradually worsening hypercarbia, tachycardia, metabolic acidosis and generalised rigidity
– Perioperatively with isolated rhabdomyolysis in otherwise asymptomatic patients
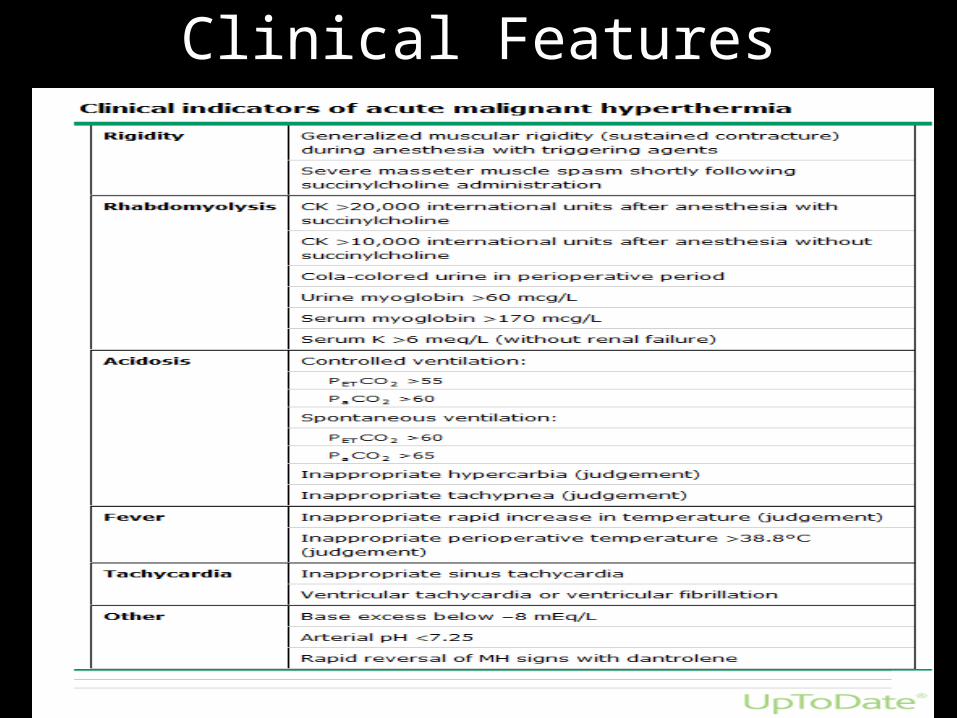
Clinical Features
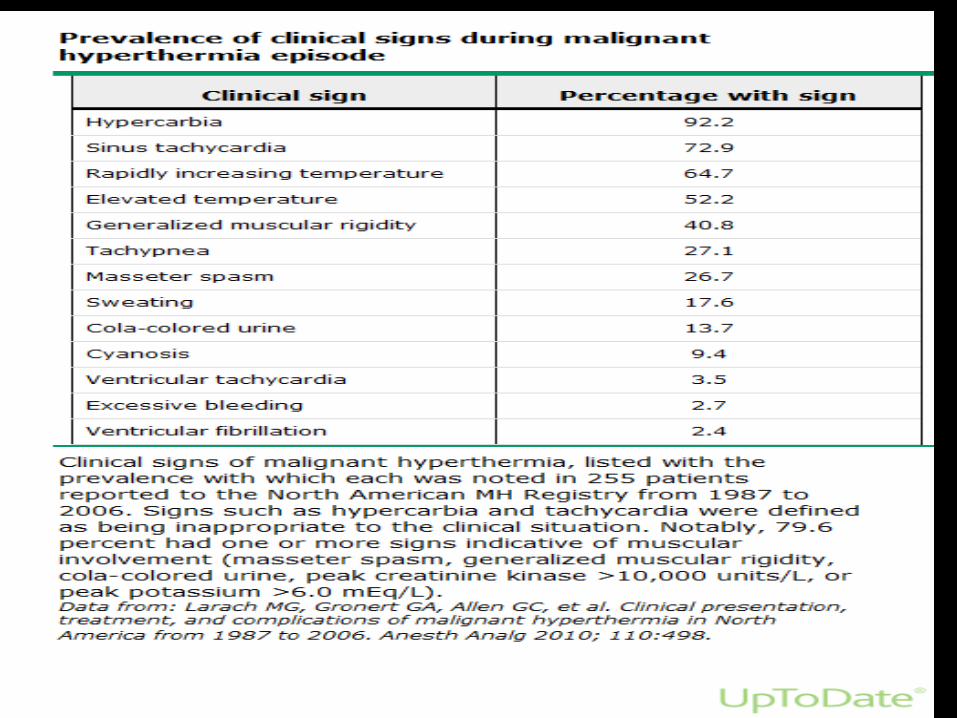
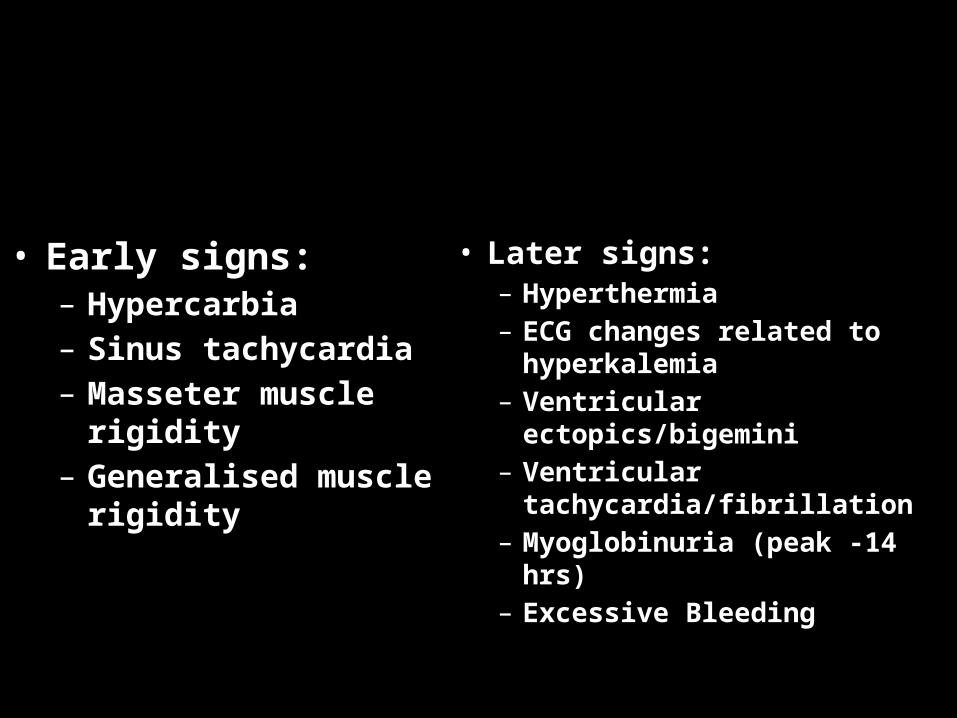
• Early signs:– Hypercarbia – Sinus tachycardia – Masseter muscle
rigidity– Generalised muscle
rigidity
• Later signs:– Hyperthermia– ECG changes related to
hyperkalemia– Ventricular
ectopics/bigemini– Ventricular
tachycardia/fibrillation– Myoglobinuria (peak -
14 hrs)– Excessive Bleeding
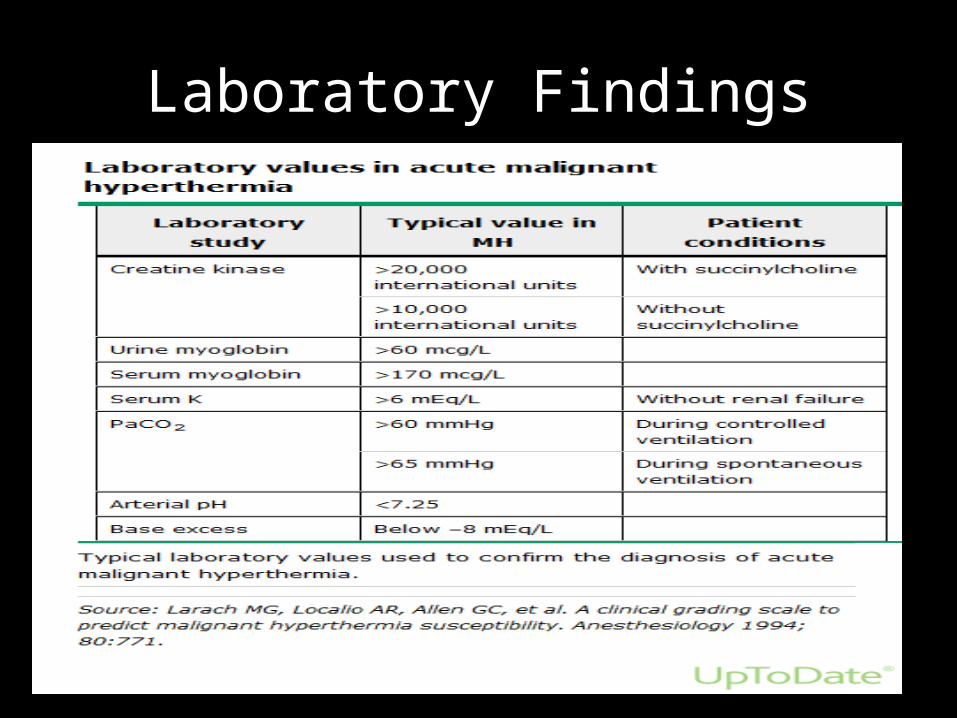
Laboratory Findings
Clinical Diagnosis
• During an acute event, diagnosis of MH is presumptive, based on 1 or more clinical findings a/w MH
• Diagnosis must be considered in all patients receiving triggering agents as 90% have negative family history for MH
• Treatment is initiated emergently as soon as diagnosis of MH is considered
• Clinical signs:– Increased EtCo2– Generalised muscle
rigidity– Hyperkalemia related
arrhythmias– Tachycardia– Tachypnea– Myoglobinuria– Hyperthermia
• Lab Studies:– ABG –pH <7.25– K> 6– CK >100000 units– CK>20000 units (with
SCh)– Serum myogoblin >170
mcg/L– Urine Myoglobin >60
mcg/L
Differential Diagnosis• Anesthesia/Surgery related:
– Insufficient anesthesia/ analgesia– Insufficient ventilation/ fresh gas flow– Overheating– Increased CO2 absorption during laparoscopy
• Drug related:– Anaphylaxis – low BP ; high PCO2; no muscle signs– Transfusion reactions- fever; brown urine; hyperkalemia– Drugs of abuse: Cocaine, Ecstasy,Metamphetamine- sudden cardiovascular collapse ;
tachypnea
• Alcoholic withdrawal syndrome – delirium, high HR, BP• NMS- slow onset ; fever, rigidity, autonomic instability• Serotonin syndrome – fever, high BP, muscle rigidity• EPS sideeffects of antipsychotics – Rigidity• Pheochromocytoma• Thyroid storm
Management
• Approach to management of suspected MH crisis:– Evaluate and manage hypercarbia
• Increase minute ventilation• Eliminate obstruction of ventilation• Seek sources of increased CO2
– Confirm other signs of MH:• Generalised rigidity• PVC (or other signs of hyperkalemia)• Tachycardia• Unstable hemodynamic stability (high or low)• Masseter spasm• Unexplained metabolic acidosis
• Initiate MH protocol:– Optimize oxygenation and ventilation:
• Increase FiO2 to 100%• Increase RR and TV to maximise ventilation and reduce
etCO2• If not intubated ETT done and NDMR given
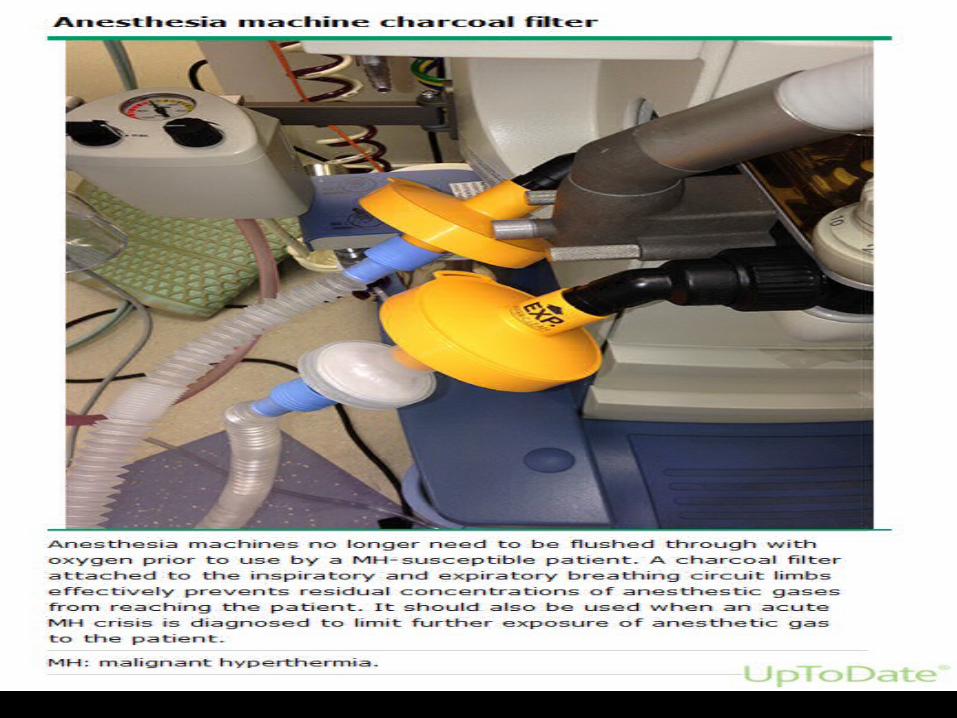
– Discontinue triggering agents• Inform surgeon of the diagnosis• Surgical procedure should be terminated if not possible
to be finished under intravenous anesthesia• Charcoal filter to be placed at expiratory and inspiratory
limbs of circuit not necessary to change machine
• Administer Dantrolene:– Skeletal muscle relaxant –directly acting at cellular level– Chemical strucutre – consists of Hydantoin group– Only known antidote for MH – Dose :2.5mg/kg- continuous repeat dose of 1mg/kg until symptoms
subside or cumulative dose of 10mg/kg reached in large iv line– No renal/hepatic dose adjustments– Paediatric and Geriatric dosing – similar to adult dose
– Brand –Ryanodex (newer) supplied as 250mg vial reconstituted with 5ml sterile water
as it is hyperconcentrated it will achieve higher concentrations faster
• Older brands- Dantrium and Revonto– Present as 20mg vial to be reconstituted with 0.9%
NS or 5%D to 60 ml – After given iv – has to be flushed with saline
– Mechanism of action:• Acts directly on skeletal muscle by interfering with release of
calcium ion from sarcoplasmic reticulumPrevents or reduces increases in myoplasmic calcium ion
concentration that activates the acute catabolic process associated with malignant hyperthermia
– Pharmacokinetics:• Time to peak concentration : 1 min post iv • Metabolism: Hepatic; metabolites – 5-hydroxydantrolene• Half life elimination: 4-11 hours• Excretion: Feces (50%) and Urine(25% as unchanged drug)
– Side effects:• Flushing• A-V block• Tachycardia• Voice disorder• Dizziness• Dysphagia
–Monitor and treat hyperkalemia:Based on ECG changes to prevent life threatening
arrhythmias and cardiac arrest
USE OF CCBS – CONTRAINDICATED IN MH AS IT CAN WORSEN HYPERKALEMIA AND HYPOTENSION
– Check labs:• Electrolytes, Blood gases, CK , serum myoglobin,
coagulation parameters and fibrin split products
• Initiate supportive care:– Monitor and treat acidosis:
• Bicarbonate
– Treat cardiac arrhythmias as per ACLS protocol
– Treat hyperthermia can precipitate DIC• >39 C should be cooled infuse cold saline intravenously, lavage open
body cavity, apply ice to surfaces till temp <38.5 C
– Insert bladder catheter to monitor urine color and volume.• Urine dipstick test + for heme myoglobinuria• Urine output >1ml/kg/hr
– Monitor muscle compartment for compartment syndrome
– Institute measures to prevent rhabdomyolysis induced renal failure • Hydration + Soda Bicarbonate + Diuretics
• Ongoing care:– When surgery over, patient should be transferred to
ICU for ventilatory support and hemodynamic monitoring for 24 hours
– Dantrolene can be stopped or interval between dosing increased to every 8-12 hours if the following criteria met:• Metabolic stability for 24 hours• Core temperature less than 38 C• CK is decreasing• No evidence of myoglobinura• Muscle no longer rigid
• Counselling after acute MH:– Not have anesthesia with triggering agents– Avoid exercises in excessive heat or humidity as
they can trigger event– Inform family members of possible MH episode
MH- genetic
Thank You