malignant hyperthermia- the heat is on
TRANSCRIPT

1
Malignant Malignant Hyperthermia-Hyperthermia- The The
Heat is ONHeat is ON
Dr. Manish Singhal
KGH, Tralee,Ireland
2
Anaesthetic Deaths in a Anaesthetic Deaths in a FamilyFamily
Denborough MA, Forster JFA, Lovell RRH, et al
Royal Melbourne Hospital
British J. Anaesth. 1962;34,395
3
Some Landmarks in theSome Landmarks in theEvolution of Understanding Evolution of Understanding
MHMH
1960/611960/61 -- Denborough and Lovell describe Denborough and Lovell describe “Anesthetic deaths in a family” “Anesthetic deaths in a family”
1960s1960s -- Gordon (?) Names the syndrome “Malignant Gordon (?) Names the syndrome “Malignant Hyperthermia”Hyperthermia”Porcine Stress Syndrome related to MH Porcine Stress Syndrome related to MH
19711971 -- First International symposium on MH,Toronto First International symposium on MH,Toronto Caffeine contracture test identifiedCaffeine contracture test identifiedHalothane contracture test Halothane contracture test
1970s1970s -- Relation of masseter muscle rigidity to MHRelation of masseter muscle rigidity to MH
4
Some Landmarks in theSome Landmarks in theEvolution of Understanding Evolution of Understanding
MHMH
19751975 -- Second International Symposium of MH, Denver Second International Symposium of MH, Denver Clinical presentation of MH Clinical presentation of MH Dantrolene as treatment for MHDantrolene as treatment for MH
19791979 -- FDA approval of Dantrolene FDA approval of Dantrolene
19811981 -- Formation of MHA and MHAUS Formation of MHA and MHAUS
19821982 -- MH hotline formed MH hotline formed
1980s1980s -- End tidal COEnd tidal CO22 as an early sign as an early sign
5
Some Landmarks in the Some Landmarks in the Evolution of Understanding of Evolution of Understanding of
MHMH
1980s1980s: European and North American : European and North American
MH groups. Patient organizations MH groups. Patient organizations
North American MH Registry North American MH Registry
1990s1990s: Identification of ryanodine receptor gene as causal in : Identification of ryanodine receptor gene as causal in pigs, some humans pigs, some humans
1990s1990s: MH without anesthetics? : MH without anesthetics? More than 30 mutations are causal in humans More than 30 mutations are causal in humans
20002000- Introduction of molecular genetic testing - Introduction of molecular genetic testing
New tests proposed New tests proposed
6
DefinitionDefinition
Malignant hyperthermia is a Malignant hyperthermia is a pharmacogeneticpharmacogenetic
disorder of skeletal muscle triggered in disorder of skeletal muscle triggered in
susceptiblessusceptibles (human or animal) (human or animal) in most instancesin most instances
by inhalation agents, and/or succinylcholine by inhalation agents, and/or succinylcholine
resulting in resulting in hypermetabolism, skeletal muscle hypermetabolism, skeletal muscle
damage, hyperthermia and death damage, hyperthermia and death if untreatedif untreated. .
7
Trigger Agents for MHTrigger Agents for MH
MH Trigger AgentsMH Trigger Agents
Potent Volatile Potent Volatile Anesthetics (eg. Anesthetics (eg. halothane, halothane, sevoflurane, sevoflurane, desflurane) desflurane)
Succinylcholine Succinylcholine
Not MH TriggersNot MH Triggers
Intravenous agents Intravenous agents
Opioids Opioids
Non-depolarizing agents Non-depolarizing agents
Ketamine Ketamine
Propofol Propofol
Anxiolytics Anxiolytics
8
Spectrum of Presentations of Spectrum of Presentations of Malignant HyperthermiaMalignant Hyperthermia
The classic case The classic case
Masseter muscle rigidity Masseter muscle rigidity
Associated with muscle disorders Associated with muscle disorders
MH without anesthesiaMH without anesthesia
9
10
What are the Clinical What are the Clinical Manifestations of MH?Manifestations of MH?
Original ConceptsOriginal Concepts: :
All patients have muscle rigidity All patients have muscle rigidity
High fever, acidosis High fever, acidosis
High death rate High death rate
Current ConceptsCurrent Concepts
Muscle rigidity may or may not be present Muscle rigidity may or may not be present
Temperature is a late sign Temperature is a late sign
End tidal COEnd tidal CO22 is an early sign is an early sign
MH may occur at any point during anesthesia - or an emergence MH may occur at any point during anesthesia - or an emergence
Recrudescence despite treatmentRecrudescence despite treatment
11
Signs of Malignant Signs of Malignant HyperthermiaHyperthermia
SpecificSpecific
– Muscle Rigidity Muscle Rigidity
– Increased COIncreased CO22
Production Production
– Rhabdomyolysis Rhabdomyolysis
– Marked Marked Temperature Temperature ElevationElevation
Non SpecificNon Specific
– Tachycardia Tachycardia
– Tachypnea Tachypnea
– Acidosis Acidosis (Resp/Metabolic) (Resp/Metabolic)
– Hyperkalemia Hyperkalemia
12
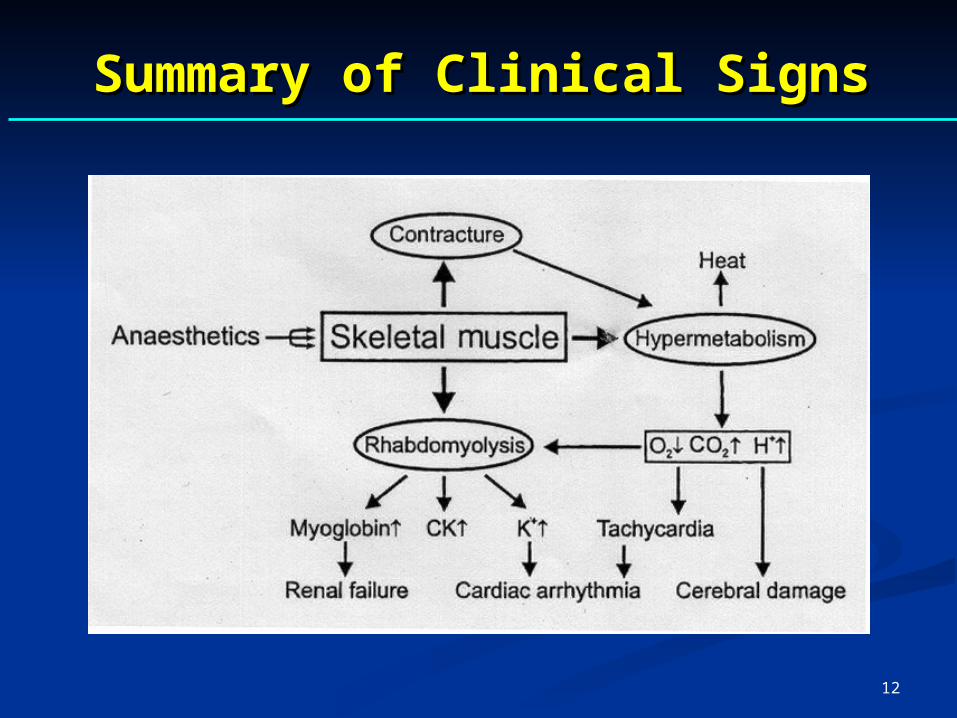
Summary of Clinical SignsSummary of Clinical Signs

13
10
5
% expired CO2
Acta Anaesthesiol Scand. 1984;28:1-8.
Marked increase in End-Tidal Marked increase in End-Tidal Carbon Dioxide in an MH crisisCarbon Dioxide in an MH crisis
14
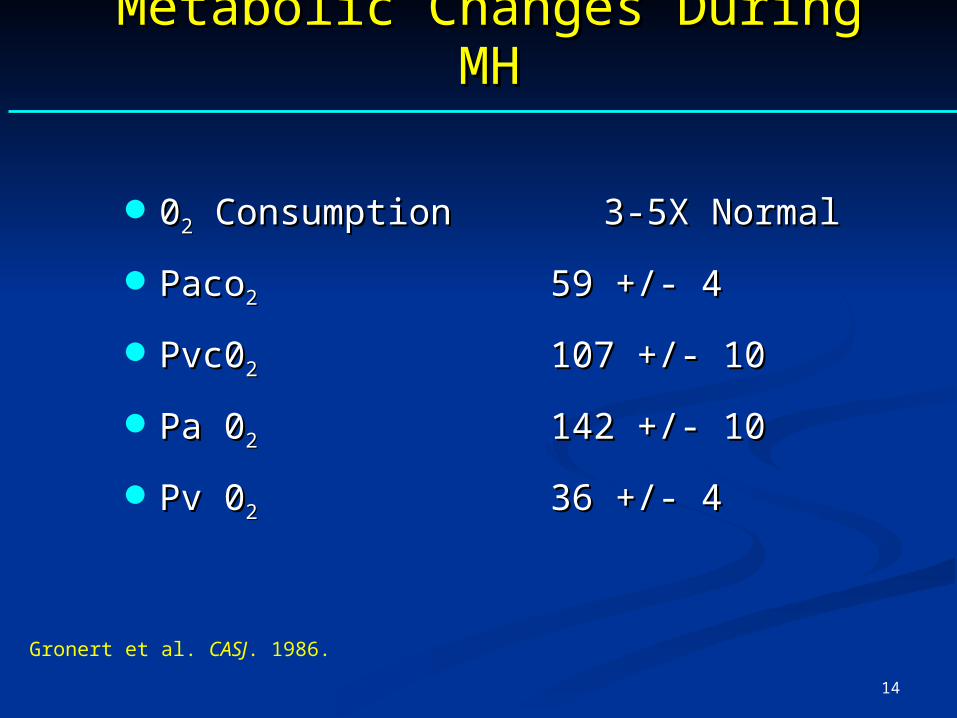
Metabolic Changes During MHMetabolic Changes During MH
0022 Consumption Consumption 3-5X Normal 3-5X Normal
PacoPaco22 59 +/- 4 59 +/- 4
Pvc0Pvc022 107 +/- 10 107 +/- 10
Pa 0Pa 022 142 +/- 10 142 +/- 10
Pv 0Pv 022 36 +/- 436 +/- 4
Gronert et al. CASJ. 1986.
15
Death from MHDeath from MH
16 year old female 16 year old female
4 hour TM joint surgery 4 hour TM joint surgery
Forane and vecuronium Forane and vecuronium
Precipitous rise in end tidal COPrecipitous rise in end tidal CO2 2
Arrhythmias and cardiac arrest Arrhythmias and cardiac arrest
Temperature 42.2 C Temperature 42.2 C
Dantrolene, 10mg/kg Dantrolene, 10mg/kg
Died from DIC after two daysDied from DIC after two days
16
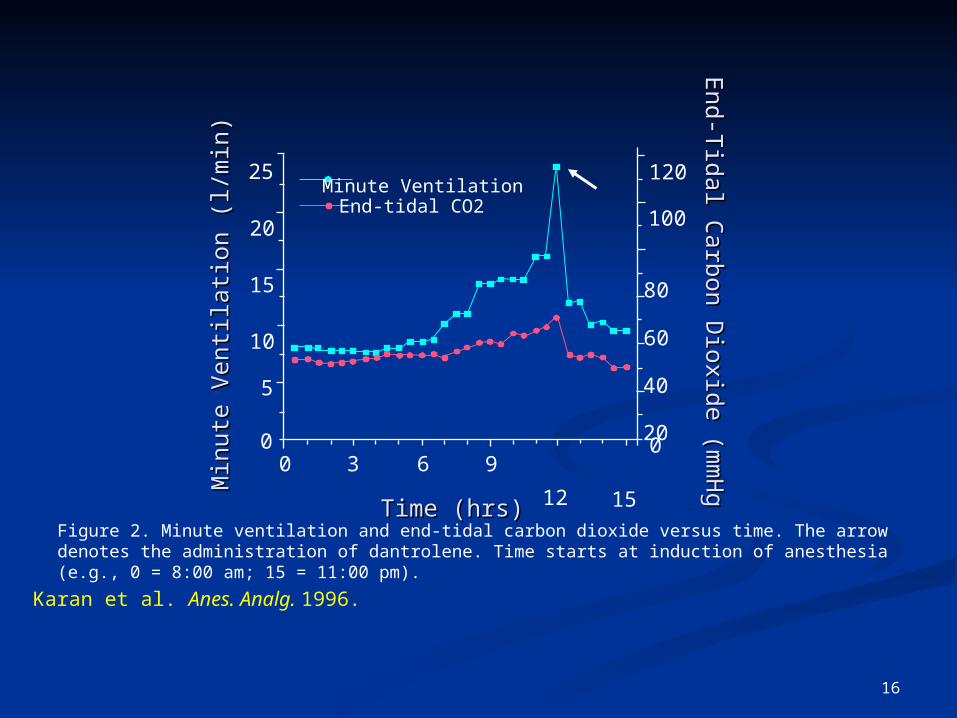
Figure 2. Minute ventilation and end-tidal carbon dioxide versus time. The arrow denotes the administration of dantrolene. Time starts at induction of anesthesia (e.g., 0 = 8:00 am; 15 = 11:00 pm).
25
12 15 0
20
40
60
80
100
10
15
20
Time (hrs)Time (hrs)
End-tidal CO2 Minute Ventilation 120
96300
5
Karan et al. Anes. Analg. 1996.
End-T
idal Carbon D
ioxide (mm
Hg
End-T
idal Carbon D
ioxide (mm
Hg
Min
ute
Ven
tilat
ion
(l/m
in)
Min
ute
Ven
tilat
ion
(l/m
in)
17
Muscle Rigidity and MHMuscle Rigidity and MH
Jaw muscle rigidity may occur after succinylcholine Jaw muscle rigidity may occur after succinylcholine
More common in children More common in children
Presages MH in 20-30% Presages MH in 20-30%
Generalized rigidity not always present Generalized rigidity not always present
When present, regularly associated with MH When present, regularly associated with MH susceptibility susceptibility
With muscle breakdown and creatine kinase above With muscle breakdown and creatine kinase above 20,00IU, the likelihood of MH is very high.20,00IU, the likelihood of MH is very high.

18
Incidence of MMRIncidence of MMR
Retrospective in ChildrenRetrospective in Children
Halothane/Succ.Halothane/Succ. 0.33-1.03% 0.33-1.03%
All AnesthesiaAll Anesthesia 0.12% 0.12%
Prospective in ChildrenProspective in Children
Halothane/Succ.Halothane/Succ. 0.9% 0.9%
Halo/STP/Succ.Halo/STP/Succ. 0.4% 0.4%
Retrospective - Adults and ChildrenRetrospective - Adults and Children
All AnestheticsAll Anesthetics 0.008%0.008%
19
Disorders Associated with MH Disorders Associated with MH SusceptibilitySusceptibility
Central Core Disease Central Core Disease
Evans Myopathy Evans Myopathy
Hypokalemic Periodic Paralysis Hypokalemic Periodic Paralysis
?sodium channel myotonias ?sodium channel myotonias

20
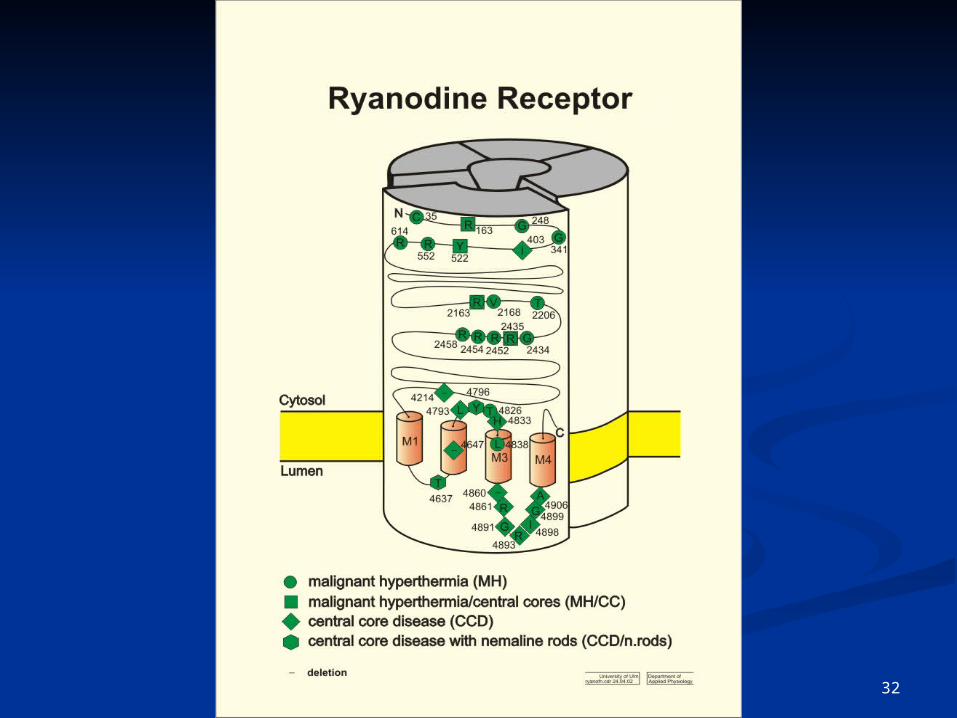
MHS mutations CCD mutations
transmembranedomains
4000 2000
T4826I
1 5038 aaI3916M
15364 pb
Y4796C
LS4647del
F4860del
RQF4214del
L4793P
I4898T
R4861H/C
R4893W
R4914G/T
G4899E/RG4638V
H4651P
G4907E
F4922L
Y4631N
R4825C
H4887Y
I4937M
T4637A
L4838V
A4906V
A4940TR4136S
V4234L
P4668SR4737W
P4973L
I403M
R552WR614C/L
C35R
G341R
G248RY522S
R401C/H
R163C/LD166N
R533C/H
R44C
R328W
R2163C/H/P
T2206M/R
R2435H/L
R2458C/H
G2434R/H
V2168M
R2454C/H
D2129E
V2214IE2347del
A2367T
D2431N
R2676W/T2787S
R2355W
R2401HR2428T
R2452W
V2117L
Mutations causing CCD are concentrated in the transmembrane domains of RYR1
21
Mimics of Malignant HyperthermiaMimics of Malignant Hyperthermia
Fever (without rigidity)Fever (without rigidity) – Thyrotoxicosis Thyrotoxicosis – Sepsis Sepsis – Pheochromocytoma Pheochromocytoma – Iatrogenic overheating Iatrogenic overheating – Anticholinergic Anticholinergic
syndrome syndrome – Faulty equipment Faulty equipment – Tourniquet (children)Tourniquet (children)
Fever and muscleFever and muscle symptoms symptoms – NMSNMS – Hypoxic encephalopathy Hypoxic encephalopathy – Ionic contrast agents Ionic contrast agents
in CSF in CSF – Cocaine, amphetamine, Cocaine, amphetamine,
ecstasyecstasy
22
Neurolept Malignant Neurolept Malignant SyndromeSyndrome
NMS is a potentially fatal, idiopathic NMS is a potentially fatal, idiopathic hypermetabolic response to a variety of hypermetabolic response to a variety of neuroleptics and dopamine receptor blocking neuroleptics and dopamine receptor blocking agentsagents. Although peripheral manifestations . Although peripheral manifestations include rhabdomyolysis and rigidity, the include rhabdomyolysis and rigidity, the pathophysiologic changes occur in the CNS pathophysiologic changes occur in the CNS Treatment with dantrolene, benzodiazepines, Treatment with dantrolene, benzodiazepines, dopamine agonists have been effectivedopamine agonists have been effective
23
Principle Features of NMSPrinciple Features of NMS
Hypermetabolic response to potent neuroleptics Hypermetabolic response to potent neuroleptics and to dopamine receptor blocking drugs and to dopamine receptor blocking drugs
Incidence 0.2% of those taking Incidence 0.2% of those taking neuroleptics/antipsychotics neuroleptics/antipsychotics
Onset may be gradual or slow Onset may be gradual or slow
• Not inherited Not inherited
• No animal model No animal model
• Responsive to a variety of drug treatmentsResponsive to a variety of drug treatments
24
Drugs that May Precipitate Drugs that May Precipitate NMSNMS
Antipsychotics ,e.g. phenothiazines,Resperidal, Olanzapine, Quietepine
Neuroleptics e.g. haloperidol, droperidol
Acute withdrawal of anti parkinson drugs
Dopamine blocking agents e.g. metoclopramide, promethazine, trifluoroperazine
25
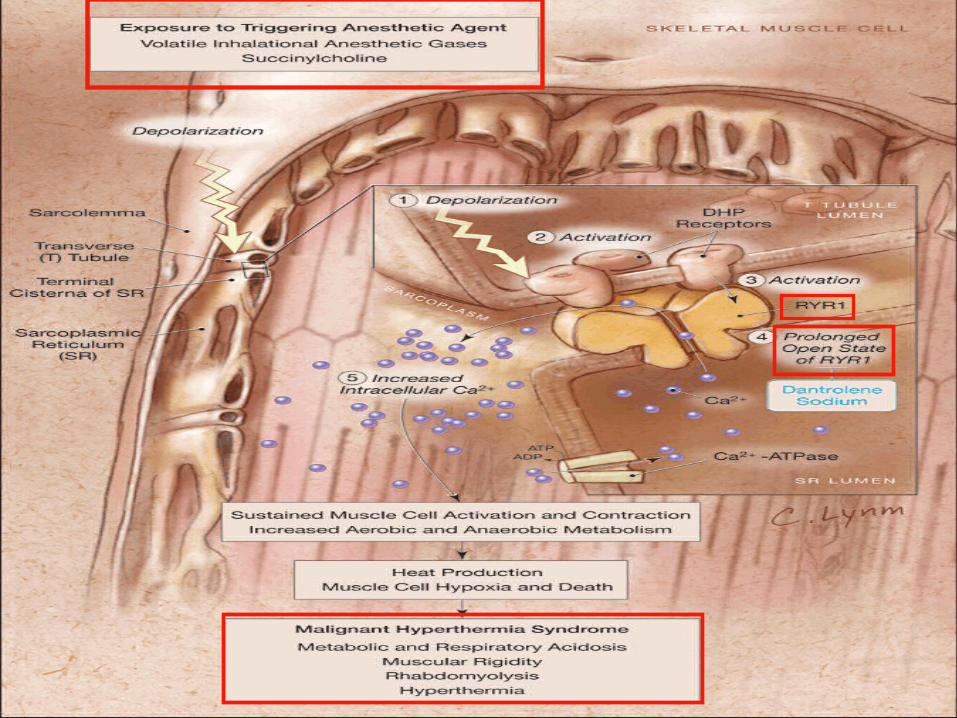
Pathophysiology of MHPathophysiology of MHand Molecular Geneticsand Molecular Genetics
26
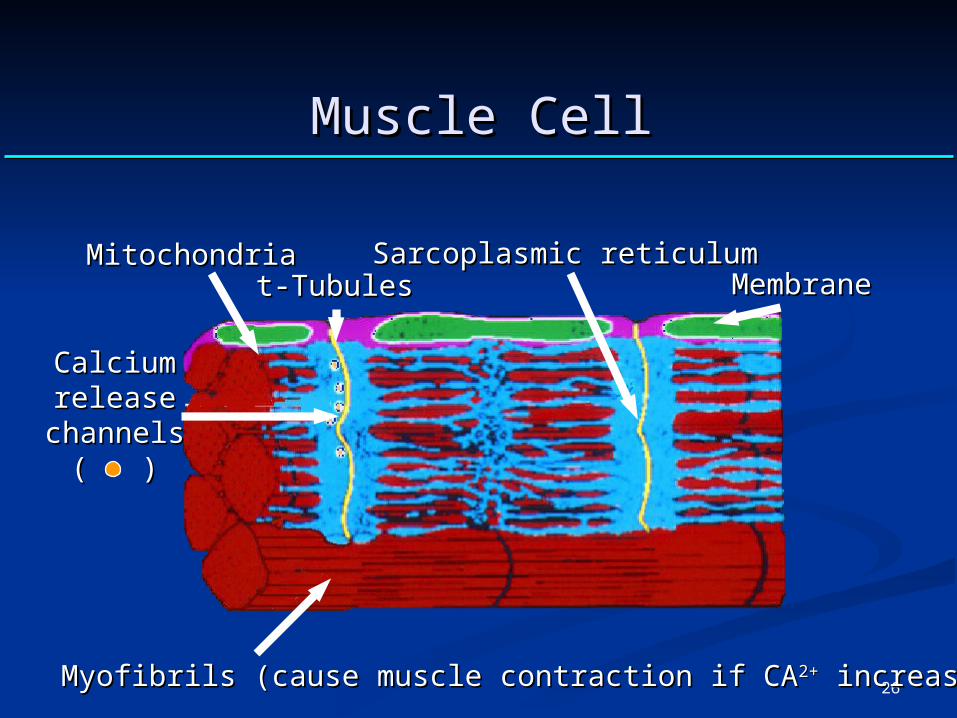
Muscle CellMuscle Cell
MitochondriaMitochondriat-Tubulest-Tubules MembraneMembrane
Sarcoplasmic reticulumSarcoplasmic reticulum
CalciumCalciumreleaserelease
channelschannels( )( )
Myofibrils (cause muscle contraction if CAMyofibrils (cause muscle contraction if CA2+2+ increases) increases)
27
28
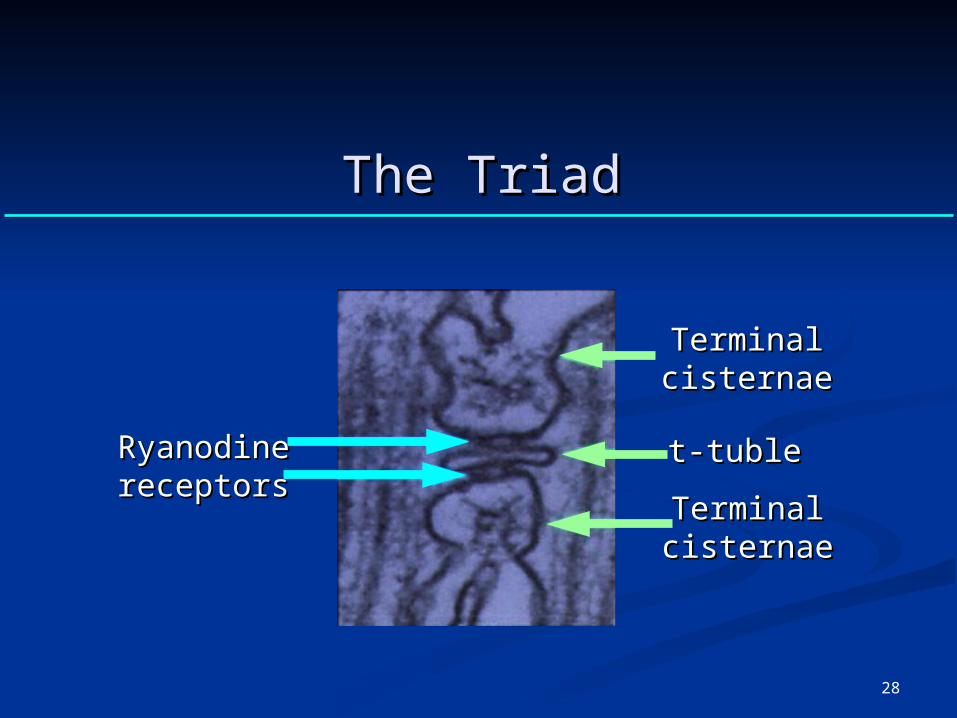
RyanodineRyanodinereceptorsreceptors
TerminalTerminalcisternaecisternae
t-tublet-tuble
TerminalTerminalcisternaecisternae
The TriadThe Triad
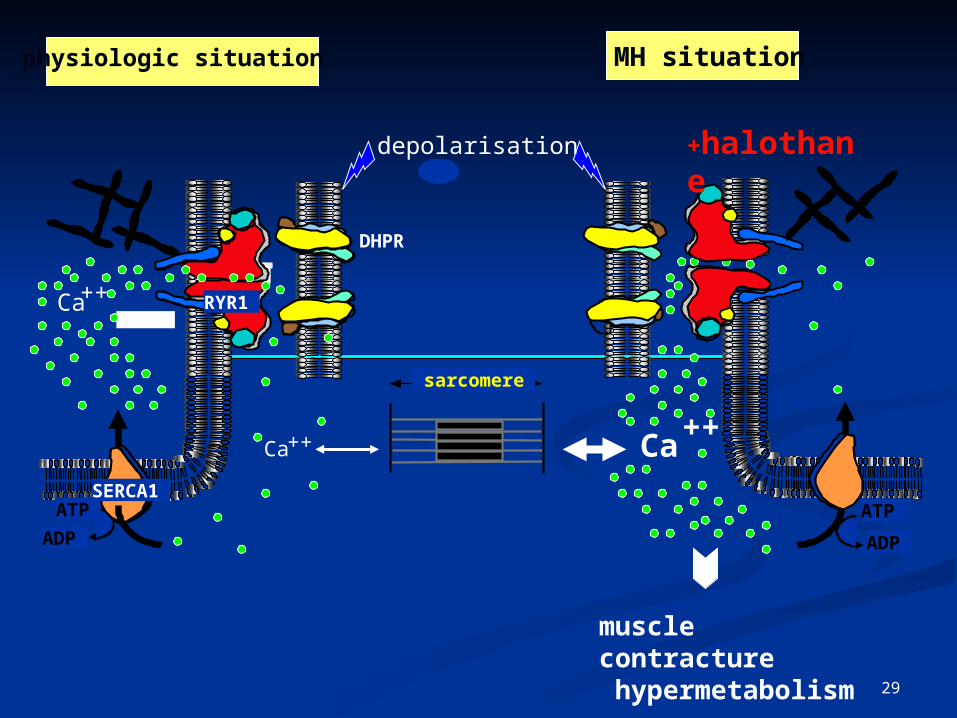
29
DHPR
RYR1 Ca++
ATP
ADP
SERCA1
sarcomere
Ca++
ATP
ADP
Ca++
physiologic situation MH situation
+halothane
muscle contracture hypermetabolism
depolarisation
30
Ryanodine receptor gene is a candidate Ryanodine receptor gene is a candidate for predisposition to malignant for predisposition to malignant
hyperthermiahyperthermia
David H. MacLennan*, Catherine DuffDavid H. MacLennan*, Catherine Duff††, , Francesco Zorzato*, Junichi Fujii*, Michael Francesco Zorzato*, Junichi Fujii*, Michael Phillips*, Robert G. KornelukPhillips*, Robert G. Korneluk‡‡, Wanda Frodis, Wanda Frodis§§, , Beverley A. BrittBeverley A. Britt§§ & Ronald G. Worton & Ronald G. Worton† †
Nature. V. 343; 1990.
31
Identification of the Mutation in Porcine Identification of the Mutation in Porcine Ryanodine Receptor Associated with Malignant Ryanodine Receptor Associated with Malignant
HyperthermiaHyperthermia
JUNICHI FUJII,* KINYA OTSU, FRANCESCO ZORZATO,JUNICHI FUJII,* KINYA OTSU, FRANCESCO ZORZATO,†† STELLA STELLA DE LEON, VIJAY K. KHANNA, JANICE E. WEILER, PETER J. DE LEON, VIJAY K. KHANNA, JANICE E. WEILER, PETER J. O’BRIEN, DAVID H. MACLENNANO’BRIEN, DAVID H. MACLENNAN‡ ‡
Malignant hyperthermia (MH) causes neurological, liver, and kidney Malignant hyperthermia (MH) causes neurological, liver, and kidney damage and death in humans and major economic losses in the swine damage and death in humans and major economic losses in the swine
industry. industry. A single point mutation in the porcine gene A single point mutation in the porcine gene for the skeletal muscle ryanodine receptor (for the skeletal muscle ryanodine receptor (ryr1ryr1) ) was found to be correlated with MH in five major was found to be correlated with MH in five major breeds of lean, heavily muscled swinebreeds of lean, heavily muscled swine.. Haplotyping Haplotyping suggests that the mutation in all five breeds has a common origin. suggests that the mutation in all five breeds has a common origin. Assuming that this is the causal mutation for MH, the development of a Assuming that this is the causal mutation for MH, the development of a noninvasive diagnostic test will provide the basis for elimination of the noninvasive diagnostic test will provide the basis for elimination of the MH gene or its controlled inclusion in swine breeding programs. MH gene or its controlled inclusion in swine breeding programs.
Science. 1991.
32
33
Guidelines for Molecular Guidelines for Molecular Genetic Detection of Genetic Detection of
Susceptibility to Susceptibility to Malignant HyperthermiaMalignant Hyperthermia
Urwyler, A , Deufel T, McCarthy T et al Urwyler, A , Deufel T, McCarthy T et al
Br.J Anaesth. 86: 283,2001 Br.J Anaesth. 86: 283,2001
34
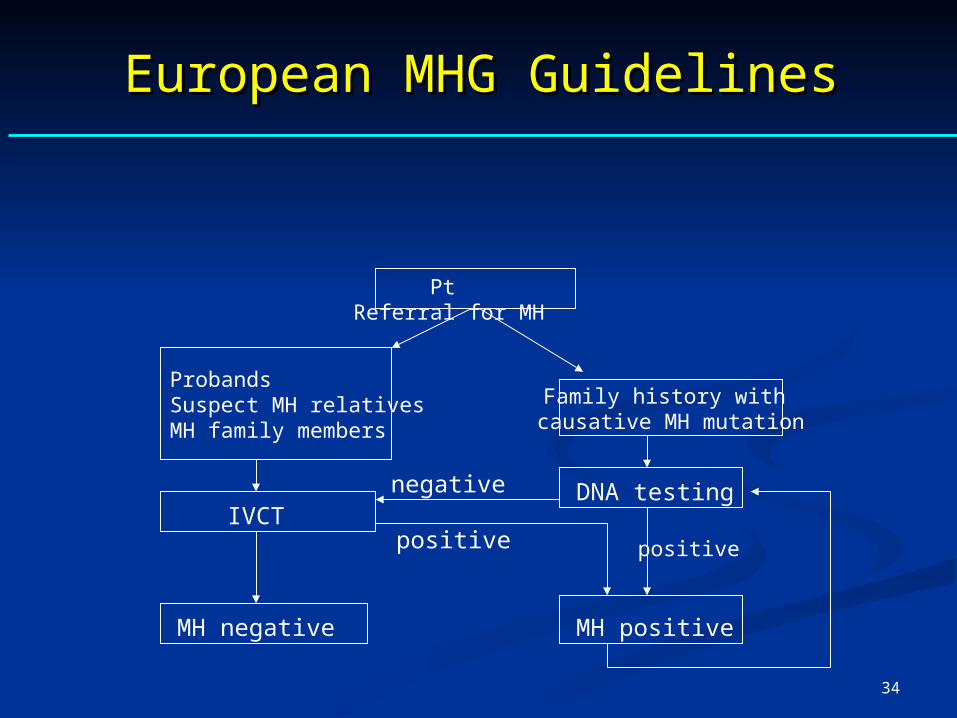
European MHG GuidelinesEuropean MHG Guidelines
Probands Suspect MH relatives MH family members
Family history with causative MH mutation
negative
positive
Pt Referral for MH
IVCT
MH negative
positive
DNA testing
MH positive

35
P & G – M Haus - 35
36
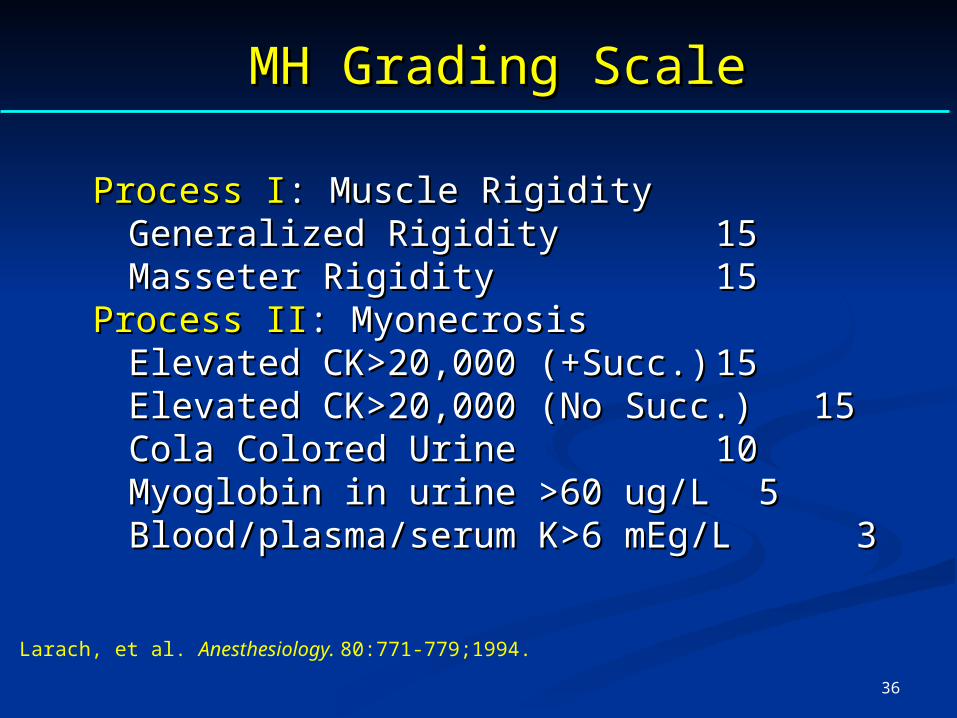
MH Grading ScaleMH Grading Scale
Process IProcess I: Muscle Rigidity : Muscle Rigidity Generalized RigidityGeneralized Rigidity 15 15 Masseter RigidityMasseter Rigidity 15 15
Process IIProcess II: Myonecrosis : Myonecrosis Elevated CK>20,000 (+Succ.)Elevated CK>20,000 (+Succ.) 15 15 Elevated CK>20,000 (No Succ.)Elevated CK>20,000 (No Succ.) 15 15 Cola Colored UrineCola Colored Urine 10 10 Myoglobin in urine >60 ug/LMyoglobin in urine >60 ug/L 5 5 Blood/plasma/serum K>6 mEg/LBlood/plasma/serum K>6 mEg/L 3 3
Larach, et al. Anesthesiology. 80:771-779;1994.
37
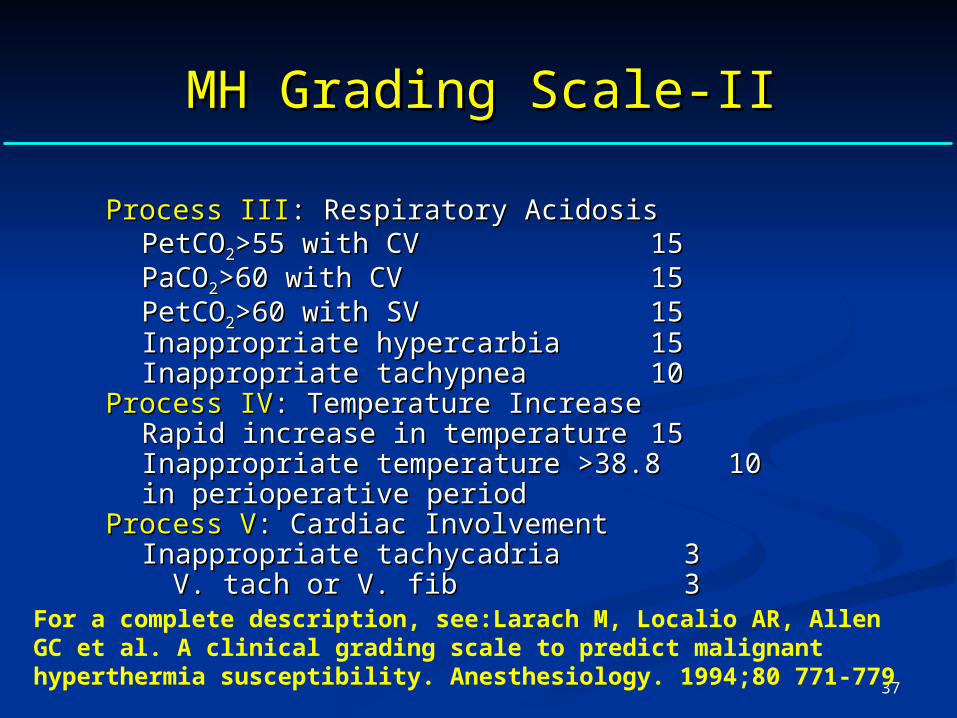
MH Grading Scale-IIMH Grading Scale-II
Process IIIProcess III: Respiratory Acidosis : Respiratory Acidosis PetCOPetCO22>55 with CV>55 with CV 15 15 PaCOPaCO22>60 with CV>60 with CV 15 15 PetCOPetCO22>60 with SV>60 with SV 15 15 Inappropriate hypercarbiaInappropriate hypercarbia 15 15 Inappropriate tachypneaInappropriate tachypnea 10 10
Process IVProcess IV: Temperature Increase : Temperature Increase Rapid increase in temperatureRapid increase in temperature 15 15 Inappropriate temperature >38.8Inappropriate temperature >38.8 10 10 in perioperative period in perioperative period
Process VProcess V: Cardiac Involvement : Cardiac Involvement Inappropriate tachycadriaInappropriate tachycadria 3 3
V. tach or V. fibV. tach or V. fib 3 3For a complete description, see:Larach M, Localio AR, Allen GC et al. A clinical grading scale to predict malignant hyperthermia susceptibility. Anesthesiology. 1994;80 771-779

38
What is the Incidence of MH?What is the Incidence of MH?
Original ConceptsOriginal Concepts: :
Rare. One in 50,000 anesthetics Rare. One in 50,000 anesthetics
Current ConceptsCurrent Concepts: :
Clinically based information:Clinically based information:
One in 20,000 to 50,000 anesthetics depending One in 20,000 to 50,000 anesthetics depending on drugs, population on drugs, population
Molecular Genetics based information:Molecular Genetics based information:
MH trait in 1 in 2,000-3,000 patients. Low MH trait in 1 in 2,000-3,000 patients. Low penetrance penetrance
39
Diagnostic ProceduresDiagnostic Procedures
40
What Tests Are UsedWhat Tests Are UsedTo Diagnose MH?To Diagnose MH?
Current Concepts:Current Concepts:
Halothane, caffeine contracture test (Halothane, caffeine contracture test (CHCTCHCT) is ) is
the only gold standard the only gold standard
Current InvestigationsCurrent Investigations: :
--Molecular genetics Molecular genetics
-Nuclear magnetic resonance for assessing ATP and creatine -Nuclear magnetic resonance for assessing ATP and creatine phosphate with/without exercise in vivo phosphate with/without exercise in vivo
-Calcium flux measurement in cultured muscle cells -Calcium flux measurement in cultured muscle cells
-Local increase in pC0-Local increase in pC022 following IM caffeine following IM caffeine
-EMG changes in MH patients-EMG changes in MH patients
41
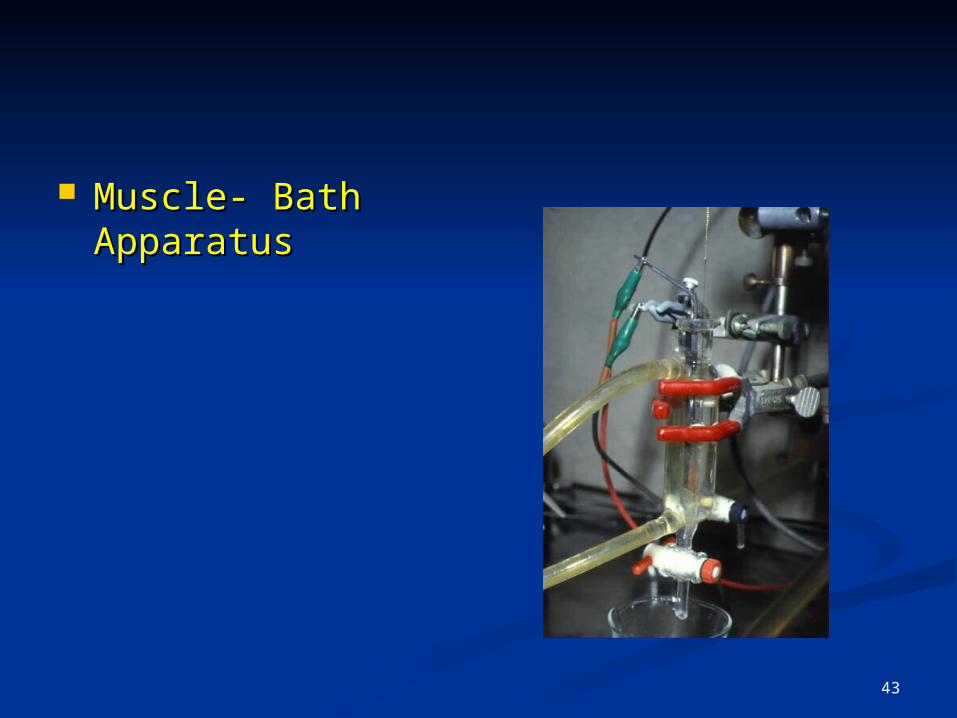
Muscle Contracture Muscle Contracture testingtesting
Expensive ( > $2500 ), invasive, non-routine Expensive ( > $2500 ), invasive, non-routine procedure done at specific diagnostic procedure done at specific diagnostic centers ( twelve in u.s.a. and canada ).centers ( twelve in u.s.a. and canada ).
Freshly biopsied skeletal muscle tissue.Freshly biopsied skeletal muscle tissue.
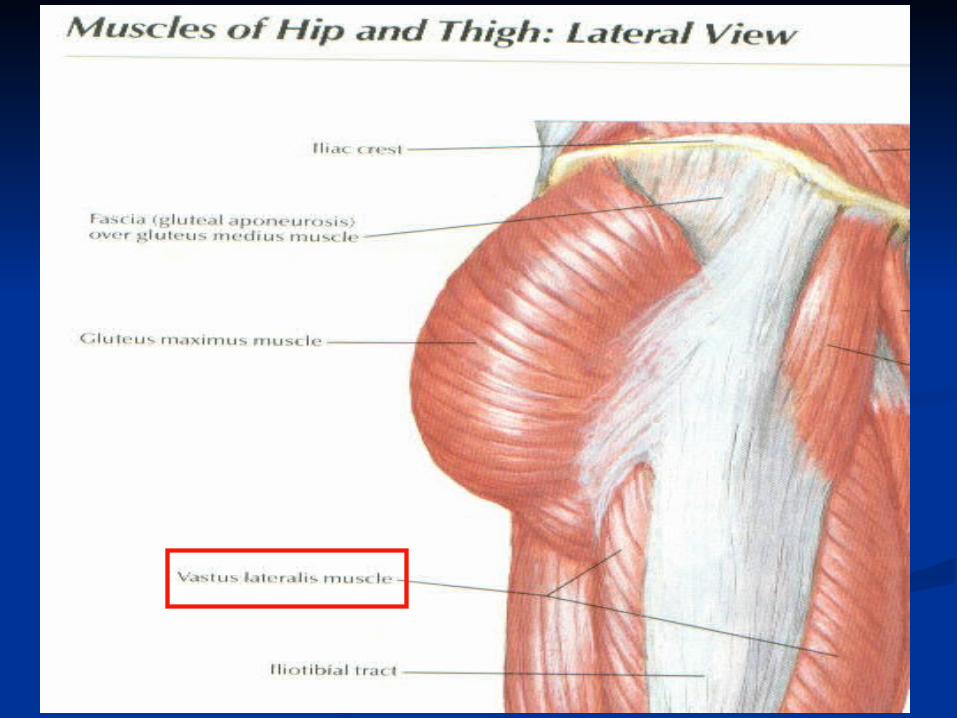
Muscle of choice is the vastus lateralis.Muscle of choice is the vastus lateralis.
2-3g muscle needed to perform TESTING2-3g muscle needed to perform TESTING
42
43
Muscle- Bath Muscle- Bath ApparatusApparatus
44
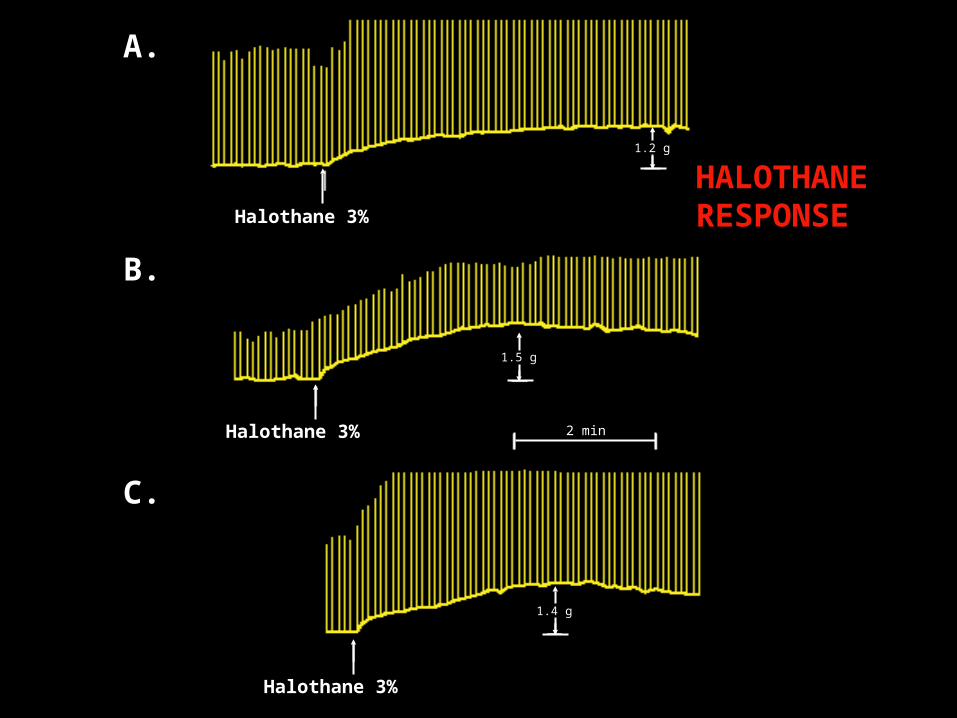
A.
B.
C.
Halothane 3%
Halothane 3%
Halothane 3%
1.4 g
1.5 g
1.2 g
2 min
HALOTHANE RESPONSE

45
2.0mM 4.0 8.0
+0.3g +2.6g
2.0 mM 4.0
+0.8 +2.1g
Normal
MH Susceptible
Caffeine Dose ResponseCaffeine Dose Response

46
Sensitivity and Specificity of Sensitivity and Specificity of Muscle Biopsy TestMuscle Biopsy Test
Sensitivity:Sensitivity: 100% 100%
Specificity:Specificity: 80%-80%-93% 93%
47
Problems with Contracture Problems with Contracture TestTest
Fresh muscle needed: Fresh muscle needed: InvasiveInvasive
Difficult to standardize completely Difficult to standardize completely
Difficult to develop knowns and unknowns Difficult to develop knowns and unknowns
How to interpret in face of myopathy How to interpret in face of myopathy
Expensive!Expensive!
Few , widely scattered biopsy centers Few , widely scattered biopsy centers
48
Other Tests Under Other Tests Under DevelopmentDevelopment
-Nuclear magnetic resonance for assessing -Nuclear magnetic resonance for assessing ATP and creatine phosphate with/without ATP and creatine phosphate with/without exercise in vivo exercise in vivo
-Calcium flux measurement in cultured -Calcium flux measurement in cultured muscle cells from needle biopsy with muscle cells from needle biopsy with caffeine caffeine
-Calcium flux in B lymphocytes with -Calcium flux in B lymphocytes with caffeine caffeine
-Local increase in pC0-Local increase in pC022 following IM caffeine following IM caffeine
49
Treatment and Treatment and ManagementManagement
50
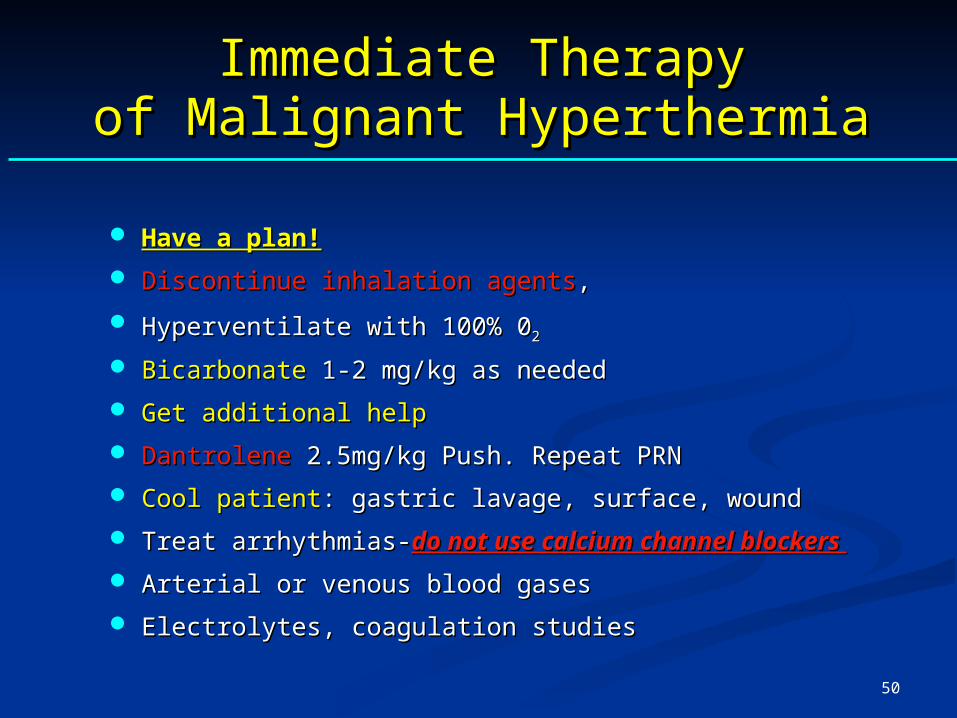
Immediate TherapyImmediate Therapyof Malignant Hyperthermiaof Malignant Hyperthermia
Have a plan!Have a plan!
Discontinue inhalation agentsDiscontinue inhalation agents, ,
Hyperventilate with 100% 0Hyperventilate with 100% 02 2
BicarbonateBicarbonate 1-2 mg/kg as needed 1-2 mg/kg as needed
Get additional helpGet additional help
DantroleneDantrolene 2.5mg/kg Push. Repeat PRN 2.5mg/kg Push. Repeat PRN
Cool patientCool patient: gastric lavage, surface, wound : gastric lavage, surface, wound
Treat arrhythmias-Treat arrhythmias-do not use calcium channel blockers do not use calcium channel blockers
Arterial or venous blood gases Arterial or venous blood gases
Electrolytes, coagulation studiesElectrolytes, coagulation studies
51
52
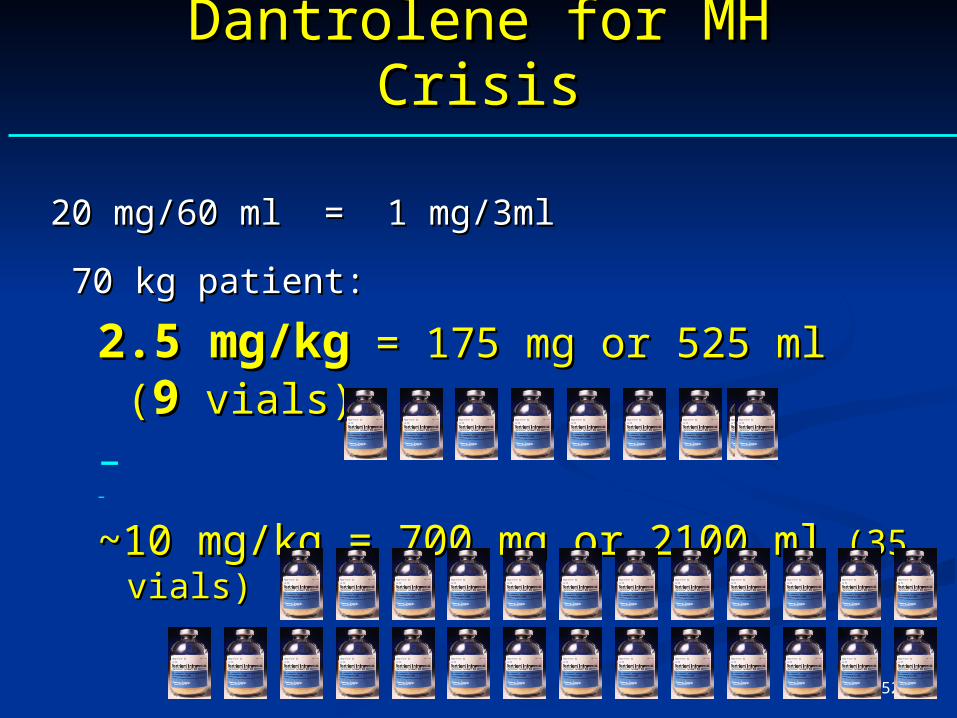
Dantrolene for MH CrisisDantrolene for MH Crisis
20 mg/60 ml = 1 mg/3ml 20 mg/60 ml = 1 mg/3ml
70 kg patient: 70 kg patient:
2.5 mg/kg2.5 mg/kg = 175 mg or 525 ml ( = 175 mg or 525 ml (99 vials) vials)
– –
~10 mg/kg = 700 mg or 2100 ml~10 mg/kg = 700 mg or 2100 ml (35 vials) (35 vials)
53
Treatment of Malignant Treatment of Malignant HyperthermiaHyperthermia
Dantrolene-2 Dantrolene-2
After crisis controlled, give dantrolene 1mg/kg After crisis controlled, give dantrolene 1mg/kg every 4-6 hours for 24 hours every 4-6 hours for 24 hours
Continue dantrolene for 36 hours Continue dantrolene for 36 hours
Recrudescence rate is 25%Recrudescence rate is 25%
54
Management of Malignant Management of Malignant HyperthermiaHyperthermia
Biochemical MarkersBiochemical Markers
Blood gases – esp pCOBlood gases – esp pCO22, pH, CK , pH, CK
Myoglobinuria Myoglobinuria
PT, PTT, INR, fibrin split products PT, PTT, INR, fibrin split products
Liver enzymes, BUNLiver enzymes, BUN
55
Morbidity and MortalityMorbidity and Mortality
RHABDOMYOLYSIS RHABDOMYOLYSIS
RENAL FAILURERENAL FAILURE
DIC if temp >41.5DIC if temp >41.500 C C
Hyperkalemia Hyperkalemia
Acidosis Acidosis
56
Prevention of Malignant Prevention of Malignant HyperthermiaHyperthermia
Preop personal/family history of anesthetic Preop personal/family history of anesthetic problems, neuromuscular disorders problems, neuromuscular disorders
Temperature/endtidal COTemperature/endtidal CO22 monitoring during monitoring during general anesthesia general anesthesia
Recognition of masseter rigidity Recognition of masseter rigidity
Investigation of unexplained tachycardia, Investigation of unexplained tachycardia, hypercarbia, hyperthermia hypercarbia, hyperthermia
Availability of Dantrolene Availability of Dantrolene
Avoiding MH triggers in MH susceptibles Avoiding MH triggers in MH susceptibles
Using Succinylcholine in indicationUsing Succinylcholine in indication
57
Principles of Management ofPrinciples of Management ofMH SusceptibleMH Susceptible
Dantrolene not necessary Dantrolene not necessary preoperatively (dantrolene available) preoperatively (dantrolene available)
Avoid succinylcholine Avoid succinylcholine
Avoid potent inhalation agents Avoid potent inhalation agents
Discharge after about 2 hours in the Discharge after about 2 hours in the recovery room if all signs are stablerecovery room if all signs are stable
58
Drug Safety in MHDrug Safety in MH
MH Trigger Agents MH Trigger Agents
Potent Volatile Potent Volatile Anesthetics (eg. Anesthetics (eg. halothane, halothane, sevoflurane, sevoflurane, desflurane) desflurane)
Succinylcholine Succinylcholine
Not MH Triggers Not MH Triggers
Intravenous agents Intravenous agents
Opioids Opioids
Non-depolarizing agents Non-depolarizing agents
Ketamine Ketamine
Propofol Propofol
Anxiolytics Anxiolytics
59
SummarySummary
MH is a metabolic myopathy affecting skeletal muscle MH is a metabolic myopathy affecting skeletal muscle
All potent inhalation agents and Succinylcholine are the All potent inhalation agents and Succinylcholine are the triggers for MH triggers for MH
Inheritance of MH in humans is autosomal dominant Inheritance of MH in humans is autosomal dominant
The basic defect in MH is an increase in intracellular The basic defect in MH is an increase in intracellular calcium of the skeletal muscle calcium of the skeletal muscle
MH effects all ages and races MH effects all ages and races
MH appears to be more common in children than adultsMH appears to be more common in children than adults

60
SummarySummary
Masseter muscle rigidity after Succinylcholine is Masseter muscle rigidity after Succinylcholine is associated with MH in 20-50% of cases associated with MH in 20-50% of cases
Endtidal COEndtidal CO22 increase is the most sensitive and specific increase is the most sensitive and specific clinical sign of MH clinical sign of MH
Although hyperthermia is a late sign of MH, it is an Although hyperthermia is a late sign of MH, it is an important confirmatory sign in some cases important confirmatory sign in some cases
Metabolic, respiratory acidosis are common Metabolic, respiratory acidosis are common
Myoglobinuria, elevation of CK are common during and Myoglobinuria, elevation of CK are common during and after MH after MH
MH may appear at any time during anesthesia and in MH may appear at any time during anesthesia and in the early part of the recovery periodthe early part of the recovery period

61
SummarySummary
Prompt treatment with dantrolene 2.5mg/kg or more effectively Prompt treatment with dantrolene 2.5mg/kg or more effectively treats MH treats MH
Dantrolene should be continued for 24-48 hours Dantrolene should be continued for 24-48 hours
Sudden cardiac arrest in young males with inhalation agents +/- Sudden cardiac arrest in young males with inhalation agents +/- Succ often indicates hyperkalemia and occult myopathy Succ often indicates hyperkalemia and occult myopathy
Only accepted diagnostic test is the halothane-caffeine Only accepted diagnostic test is the halothane-caffeine contracture test contracture test
MH testing indicated in patients and clinical episodes and their MH testing indicated in patients and clinical episodes and their family members family members
Help and assistance are available from mhaus and Help and assistance are available from mhaus and the hotlinethe hotline

62
STEPHANIE KULEBA
April 30, 2008 Wall Street Journal article "A Fresh Focus On a Rare Risk of Anesthesia" by Laura Landro.

63
HAVE A PLAN AND MOVEHAVE A PLAN AND MOVE
Thank you