management of diffuse tissue argyria subsequent to endodontic
TRANSCRIPT
Endodontics
Management of diffuse tissue argyria subsequent to endodontic therapy:Report of a case
Gary D, Rusch-Behrend*/James L, Gutmann**
A case of severe mucogingival argyria secondary to leakage around and corrosion of silvercone root canal obturations and apical amalgam restorations is presented. Following removalof the silver points and re-treatment of tlie root canais, periradicular surgery was performedto remove t¡ie amalgam root-end restorations and reduce the amoutit of dispersed metallicparticles in the subctitaneous ti.^sues. Subsequent free gingival grafting created an estlieticatlypleasing and biologically acceptable result. (Quintessence Int ¡995:26:553-557.)
Introduction
Arg}'ria has been defined as a permanent pigmentationofthe sldn and mucous membranes following chronicexposure to silver compounds through occupationalhazards or exposure to systematically administeredsilver-containing therapeutics. ' The discoloration maybe generalized, as a slate-blue discoloration ofthe skin,conjunctiva, and/or internal organs, closely mimickingcyanosis.- Argyria may be pronounced in tissue areasexposed to the sun, when colorless silver salts arereduced to metallic salts, ̂ A common form, frequentlytermed amalgam pigmentation or amalgam tattoo, iscaused by the inadvertant embedding of silver-con-taining amalgam patiicles in the oral mucosa after oralsurgical or operative dental procedures, A locahzedform of argyria has been attributed to the use ofsilver-containing root canal sealers or silver cones.""-̂ Itmay also present following the corrosion of amalgamsuigical root-end restorations.^"*
* Gradúale Endodontic Studenl, Departmeni of Rebturative Sciences,Baylor College of Dentistr>', Dallas, Texas.
" Professor and Director of Graduate Endodontics, Department ofRestorative Sciences, Baylor College of Dentistij, Dallas, Texas,
Reprint requests: Dr J, L. Gutmann, Professor and Director of GraduateEndodontics, Department uf Restorative Sciences, Baylor College ofDenlistry, 3302 Gaston Avenue, Dailas, Tesas 75246.
Management of argyria caused by the accidentalpresence of amalgam in the oral tissues may requirereconstructive mucogingival surgery in the form oftissue excision and free gingival grafting,'^ When theetiology is attributed to materials used in nonsurgicaland/or surgical root canal treatment, a thoroughremoval of these substances is indicated before graftingprocedures are undertaken,'
Case report
A 26-year-old white woman presented with a chiefcomplaint of severely discolored soft oral tissuesoverlying the maxillary central incisors. Her presenthealth and past medical history were unremarkableand noncontributory to her chief complaint. Likewise,no dental symptoms were present. The patient couldnot specify when the discoloration first appeared otherthan to report that it was noticed after previousnonsurgical and surgical root canal treatment. She wasuncertain whether or not the discolorations hadchanged in shape or size since first noticed. The rootcanal treatment had been pertbrmed subseqtient totrauma to the anterior maxilla.
Clinical examination revealed amorphous blue-black, nonraised, nonindurated discoloration ofthealveolar mucosa su pe ri or-late ral to the root apices ofthe maxillary central incisors (Fig 1), The maxillaryanterior teeth were not tender to percussion orpalpation. Radiographie examination revealed that thecanal of the right central incisor was obturated with
9R, Miimhpr 8/1995 553

Endodonîics
Fig 1 (above) The intense tissue staining in the attachedgingiva of the anterior maxilla radiates into the mucogingivaltissues.
Fig 2 (rigtit) A radiograph of the maxillary centra) incisorsreveals large amalgam root-end restorations and the pre-sence of a silver cone obturation in each tooth
Fig 3 Reflection of a full-thickness mucoperiosfeal fissuefiap reveals intense staining along with tissue fibrosis.
gutta-percha, a silver cone, and an amalgam root-endrestoration. The left central incisor was obturated witha silver cone and an amalgam root-end restoration(Fig 2). Significant lateral voids were present and acrescentic radiolucent area was evident around theroot-end obturation of the left central incisor. Somesmail radiopaque inclusions (smaller than or equal to1 mm) were also evident on the radiograph within 5 mmofthe apices of both teeth (Fig 2). On the basis ofthedentai history, the soft tissue pigmentation was deter-mined to be caused by corrosion ofthe silver cone inthe canal of the left central incisor and from thesilver-containing amalgam placed in the root ends
following root-end resection. Both nonsurgical andsurgical intervention were identified as necessary toeliminate the source of the silver products and theresultant tissue argyria.
Treatment consisted of removal ofthe crowns fromboth teeth and removal ofthe gutta-percha and silvercones. Following thorough canal cleaning and shap-ing, the canals were obturated with injectible thermo-plasticized gutta-percha (Obtura, Texceed) and Seal-apex root canal sealer (Kerr/Sybron) prior to surgicalintervention. Surgically, a ftill-thickness mucoperio-steal tissue flap was reflected on the labial surface (Fig3). Curettage of the osseous tissues along with athinning of the refiected tissue removed some of thepigmented tissues. However, heavy tissue scarring andthe tenacious attachment of the fibrous connectivetissue to the bone minimized the removal of theaccumulated pigmentation. Root-end resection andremoval of the apical amalgam restorations ñirtherreduced the ptgmented tissues (Figs 4 and 5).
Microscopic analysis of sections of the apicallybiopsied tissues revealed soft tissue whh bone andmineralized debris. The connective tissues contained adifHise chronic inflammatory cell infiltrate that waspredominantly plasmocytic. Multiple aggregates of ablack foreign material were present (Fig 6).
Three to 4 weeks afier tissue healing followingendodontic sut^ical intervention, periodontal graftingprocedures were performed in an attempt to furtherreduce the tissue argyria (Fig 7). A ftili-thickness free
554 Quintessence International Volume 26, Number
Endodontics
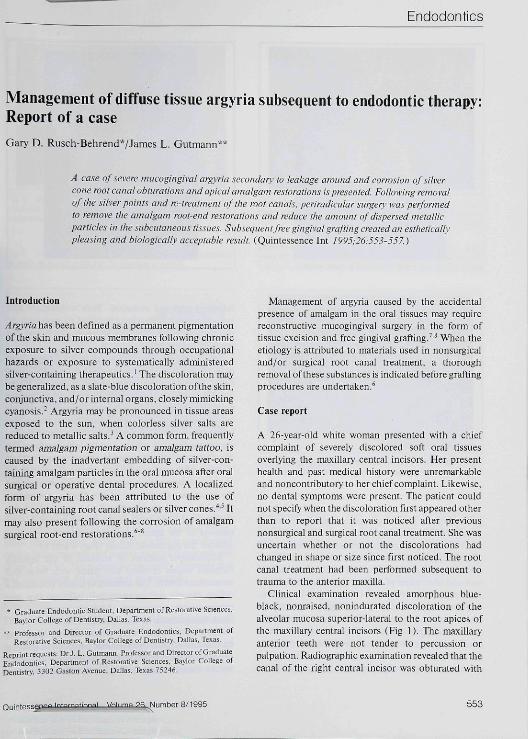
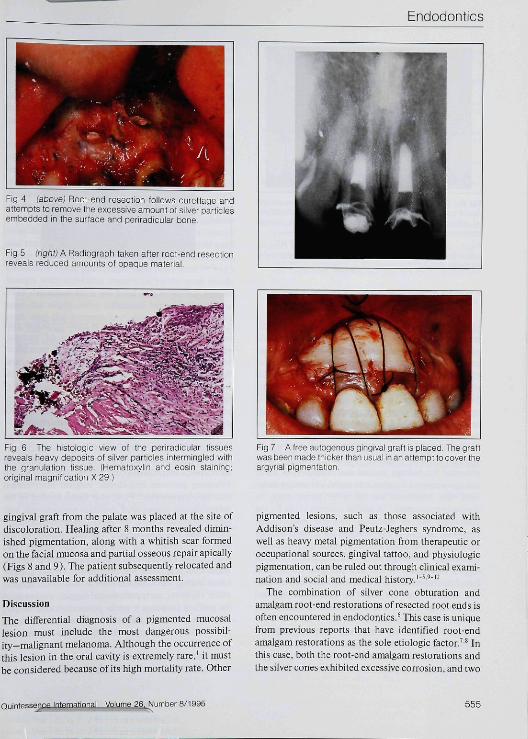
Fig 4 (above) Root-end resection follows curellage andattempts to remove the excessive amount oi silver particlesembedded in the surface and periradicular bone.
Fig 5 (right) A Radiograph taken atter root-end resectionreveals reduced amounts of opaque material.
Fig 6 The histoiogic view of the periradicular tissuesreveals heavy deposits of silver particles intermingled withthe granulation tissue. (Hematoxylin and eosin staining;original magnification X 29,]
Fig 7 A free autogenous gingival graft is placed The graftwas been made thicker than usual in an attempt to cover theargyrial pigmentation
gingival graft from the palate was placed at the site ofdiscoloration. Healing after 8 months revealed dimin-ished pigmentation, along with a whitish scar formedon the facial mucosa and partial osseous repair apicaliy(Figs 8 and 9), The patient subsequently relocated andwas unavailable for additional assessment.
Discussion
The differential diagnosis of a pigmented mucosallesion must include the most dangerous possibil-ity-mahgnant melanoma. Although the occurrence ofthis lesion in the oral cavity is extremeiy rare,' it mustbe considered because of its high mortality rate. Other
pigmented lesions, such as those associated withAddison's disease and Peutz-Jeghers syndrome, aswell as heavy metal pigmentation from therapeutic oroccupational sources, gingival tattoo, and physiologicpigmentation, can be ruled out through clinical exami-nation and social and medical history,'"'^"'-
The combination of silver cone obturation andamalgam root-end restorations of resected root ends isoften encountered in endodontics,^ This case is uniquefrom previous reports that have identified root-endamalgam restorations as the sole etiologic factor,'-* Inthis case, both the root-end amalgam restorations andthe silver cones exhibited excessive corrosion, and two
International Volume 26. Number 8/1995 555

Endodontics
Fig 8 (above) HeaUng atter 6 months reveáis a whitishtissue covering most ot the pigmented area. Some ieachingof silver precipitate is stiii evident. Prcvisional coronairestorations are present.Fig 9 (right) A radiograph of the maxiilary central incisors,taken 6 months postoperativeiy, reveals a smaii amount ofosseous repair.
previous endodontic surgical entries failed to preventthis occurrence. Because both materials will corrodewhen exposed to interstitial fluids and release silver-containing salts into the surrounding tissues,'-" thistype of etiology must be included in the differentialdiagnosis of pigmented lesions. It is important that thepotential for these materials to create an unestheticappearance ofthe mucosa be recognized prior to theirindiscriminate use.* Likewise, when amalgam is usedin the presence of exposed tissues, diligence must beexercised to remove metallic debris from all tissuestlirough copious irrigation. Further, given the greatpotential for leakage around and corrosion of silvercones, compared to other root canal-obturating mate-rials, the continued use of silver cones must beseriously questioned. " A similar concern exists for thecontinued use of amalgam root-end restorations,especially in light ofthe potential for coronal leakagethrough the root canal system to reach the periradicu-lar tissues.'^ Although no specific incidences of tissueargyria subsequent to root-end amalgam restorationshave been reported, use of alternative root-end restora-tive materials that are based on zinc oxide-eugenoland résistent to corrosion is advocated to minimize orprevent tissue discoloration.*
Studies examining excisionai biopsy specimensfrom amalgam tattoos with light and electron micro-scopy and microprobe analysis suggest that as corro-sion occurs, mercury and tin are lost, leaving silver and
tin in the macrophages and giant cellsJ^'^ Silver alsoremains in the basement membranes of mucosalepithelium, skeletal muscle Fibers, smooth muscles ofblood vessels, flbroblasts. collagen, elastic tissue, andSchwann"s cells. Once staining is deposited in the basallamina propria and collagen bundles, management ofthe staining with grafting procedures may be compro-mised, even on removal ofthe original source ofthesilver staining.
Free gingival grafting has been recommended tomanage esthetics, especially with aigydai staining.'''Although this procedure is generally quite predictablewhen used for correcting periodontal defects," its usefollowing previous endodontic surgical interventionmay be compromised. First, scar tissue formed in thesubcutaneous tissues after previous periradicular sur-gery complicates both the periodontal surgical tech-nique and the prerequisite vascular supply of theperiosteal tissues.' In this case, the patient hadexperienced two previous endodontic surgical entries.Significant scar tissue was present and further compli-cated healing was expected from an additional surgicalentry. However, early periodontal surgical interventionfor grafting purposes 4 weeks postendodontic surgerymay have minimized this concern because the collagenfiber density ofthe connective rissue was not yet tliilymature.'^
A second concern is the continued migration ofcorrosion products and staining ofthe grafted tissues,'
556 Quintessence International Voiume 26, Number

Endodontics
In this patient, the silver and amalgam particles werewidely disseminated and deeply embedded in both themucoperiosteal and osseous tissues. With thin grafts,continued staining may be the norm. With thickergrafts, as performed in this patient, the blood supply tothe grafted tissues as well as the esthetic result may becompromised.
For this patient, other periodontal techniquesemployed in mucogingival surgery to manage tissueesthetics were considered inappropriate, especiallybecause ofthe size ofthe defect to be resolved and thecharacter ofthe discoloration.'" Because ofthe widedissemination ofthe black foreign material, even aftercurettage ofthe osseous tissue and connective tissuebase of the mucoperiosteai flap, esthetic considera-tions dictated removal of the affected gingival tissuesand replacement with a free autogenous gingival graftdrawn from the palate. Although a subperiosteaiconnective tissue graft might have been used,̂ ''"̂ ^ anyforeign body remnants superficial to the graft wouldhave detracted from the final result. In the presentcase, the slight color difference between the palatalgraft and the surrounding attached gingiva of thealveolus was considered minor compared to theoriginal argydal staining.
References
1. ShafecWG, ttine MK, Levy BM, Oral Pathology, ed 3, Philadelphia:Saunders, 1963:528.
2, Tiramins AC, Morgan GAR, Argyna or cyanosis. Anesthesitilogy1988:43:755-756,
3. Shelley WB, Shelley ED, Bjrmeister V. Argyria: The intradermal"ptiotograph," a manifestation of passive photosensitivity. J AmAcadDermatol I987;16:2tl-2I7,
4, Kirchotr DA. Localized argyria after a surgical endodontie pro-cedure. Oral Surg Oral Med Oral Pathot 197t:32:613-6t7,
5, Büchner A, Hansen LS. Amalgam pigmentation ( amalgam talloo) oftlie oral mucosa. A elinicopathologic study of 26S eases. Oral SurgOral Med Oral Pathol 1980:49:139-147,
6, GutitiannJL,HarrisonJW, Surgical Endodontics. Boston: BlackwellScientific:, t99t:230-264.
7, Dello Russo NM, Esthelie use of a free gingival autograñ to cover anamalgam latloo; Report of case, J Am Dent Assoc 198hlO2:334-335,
8, Shitoah J. Covington JS, Schuman NJ, Reconstructive mueogingivalsurgery: Ttie management of amatgam tattoo, QuintEssenee tnt t938:19:489-492,
9, Mani NJ, Gingival tattoo, A tiitherto undescribed mucosal pigmen-(alion. Quinti^sencc Int I985;t6:l57-159,
10, Kin CA, Forrest WR, Indueed mucogingival pigmentation (lattoo),Compend Contin Edue Dent 1988:9:194.
11 Gazi MJ, Unusual pigmentation of the gingiva. Oral Siii^ Oral MedOral Pathol 1986:62:640-649.
12, Gorüky M, Buehner A, Fundoianu Dayan D, Aviv t. Physiologicpigmentation ofthe gingiva in tsraeli Jews of different ethnic origin.Oral Surg Oral Med Oral Palhol 1984:58:506-509,
13. Settzer S, Green DB, Weiner N, DeRenzis F. A scanning electronmicroscope examination of silver cones removed from endodonti-cally treated teeth. Oral Surg Oral Med Oral Pathol I972;33:5S9-605.
14, Swanson K, Madison S. An evaiuation of eoronal microleakage inendodontieally Ireated teeth. Part t. Time periods, J Endod1987:13:56-59.
15. tiarrison JD, RowteyPSA, Peters PD, Amalgam tattoo5: Light andelectron mieroscopy and electron probe microanalysis, J Pathol1977:121:83-92.
Id. Weathers DR, Fine RM. Amalgam tattoo of oral mucosa. ArchDermatol 1974:110:727-728,
t?, Allen EP Use of mucogingival surgical procedures to entianceesthetics. Dent Clin North Am I9SS;32:307-330.
IS, Harrison JW. Healing of surgical wounds in oral mucoperiosteaitissues. J Endod 199ht7:4OI-4O8,
19. Lange DE. tndication and procedures for mucogingival surgery, tn:Hosi E. Zachrisson BU, Baldaur A (edsl. Orthodontics andPeriodontics. Chicago: Quinlessence, 1985:79-103.
20. Ratzke PB. Covering tocalized areas of root exposure employing theenvelope technique, J Periodontol 1985:.S6:397-402.
21, Langer B. Langer L. Subepithelial connective tissue graft techniquefor root coverage. J Periodontol 1985:56:715-720,
22, Nelson SW. The sub-pedicle eonneetive tissue grat\. A bilaminarreconstructive procedure for the coverage of denuded root surfaces. JPeriodontol t987;58:95-102, •
Quintesserjc£ Number 8/1995 557