management of endovascular graft infections
TRANSCRIPT

Barbara Hasse, MD
Division of Infectious Diseases and Hospital EpidemiologyUniversity Hospital of Zurich
University of ZurichZurich, Switzerland
Management of endovascular graft infections
ESCMID eLibrary
by a
uthor

Agenda
Introduction
Cases
Vasgra Cohort
Diagnosis
Treatment: Surgical treatment approach, Antimicrobial therapy
PET/CT for treatment response
ESCMID eLibrary
by a
uthor

Background
Vascular graft infections are associated with a significant mortality and
morbidity.
Femoropopliteal grafts: 4% Aortic grafts: 0.5-2%
Darouiche et al. N Engl J Med 2004; 350:1422-9
Legout et al Clin Microbiol Infect 2012:18:352:18: 352-8
Hasse et al. Swiss Medical Weekly 2013ESCMID eLibrary
by a
uthor

Aortic aneurysm: open surgery vs endovascular treatment
ESCMID eLibrary
by a
uthor

Aortic endograft are often used in patients who are unfit for open
procedures
EVARTEVAR
Infection rate < 1%ESCMID eLibrary
by a
uthor

Economic consequences
Switzerland: 9 /100’000 persons hospitalized with vascular graft infection
Hospitalization costs 72’350 sFr (DRG)
Source: Swiss federal office of Statistics, 2013
Darouiche et al. N Engl J Med 2004; 350:1422-9 ESCMID eLibrary
by a
uthor

Vascular graft infection: interaction microorganisms, host and prosthetic factors
Polyethylenterephthalate (Dacron®)
coated with gelatin or collagen
Woven
Knitted
Polytetrafluoroethylen (Gore-Tex®)
Blood-tight, smooth surface, prevents
blood clotsESCMID eLibrary
by a
uthor

Foreign bodys are devoid of microcirculation
Synthetic material
‒ PET Polyethylenterephthalate Dacron
‒ PTFE Polytetrafluoroethylen Gore-Tex
Biological material
‒ Animal Heterologous Xenografts
‒ Cryopreserved Homologous Homograft
cadaveric arteries
‒ Produced naturally Autologous Autograft
in the body
Susceptib
ilityto
infe
ctio
n
ESCMID eLibrary
by a
uthor

Role of the biofilm
http://www2.binghamton.edu/biology/faculty/davies/research.htmESCMID eLibrary
by a
uthor

Typical organisms
Staphylococcus aureus 20-50%
Coagulase negative Staphylococci 15%
Enterobacteriaceae 14-41%
Anaerobes 5%
Fungi 1-2%
Polymicrobial infections 20%
FitzGerald et al. Journal of Antimicrobial Chemotherapy (2005) 56, 996–999
Revest et al. Int Journal of Antimicr Agents Chemother 2015ESCMID eLibrary
by a
uthor

Case #1 | 61-year-old male
2010 EVAR
06/2012 Fever, night sweats, belt-shaped
abdominal pain; CRP 89 mg/L
07/2012 Dx of aortic endograft infection
Endograft infection
CoNS, S. agalactiaeESCMID eLibrary
by a
uthor

Criteria for vascular graft infections
Positive bacterial culture of intraoperative
specimens or blood samples
Clinical signs of infection
Biological signs of infection or other
radiological signs of infection (perigraft air
or fluid persisting for more than 8 weeks
postoperatively, abscess)
FitzGerald et al; Journal of Antimicrobial Chemotherapy (2005) 56, 996–999ESCMID eLibrary
by a
uthor
No treatment guidelines
Surgical treatment
Antimicrobial therapy
Empirical therapy?
Use of the same treatment approach for
o Endovascular/ open surgery
o Abdominal/ thoracic or peripheral vascular surgery
Duration unclear – how long is long enough?
ESCMID eLibrary
by a
uthor

Vascular graft cohort Study (VASGRA)
Prospective, observational cohort study, single centre, May 2013
Infectious Diseases specialists, microbiology, vascular surgery, radiology
ESCMID eLibrary
by a
uthor

Methodology
Prospective n=72
ESCMID eLibrary
by a
uthor

Systematic microbiological/histopathological work up
Use of PET/CT scan at diagnosis/ during follow-up
Microbiology
Deep tissue cultures
Broad range PCR
Blood cultures
Cultures of negative pressure wound therapy foams
Histopathology
PET/CT
At diagnosis, during FUP, 3 month after stop of antimicrobial therapy
ESCMID eLibrary
by a
uthor

Risk factors
ESCMID eLibrary
by a
uthor

Postoperative wound complications are the most important risk factors for
abdominal vascular graft infection
365 patients with 599 vascular grafts; 46 Prosthetic vascular graft infections
Incidence 6 (95% 4-10) per 100 PYFUP
Variable Hazard Ratio 95% Confidence interval P Value
Endovascular operation 0.32 0.13-0.76 0.010
Postoperative wound infection 4.8 1.7-14 0.004
Other wound complications 1.8 0.71-4.8 0.209
Duration of operation in hours 1.2 1.0-1.3 0.012
Cox regression, MV Model
ESCMID eLibrary
by a
uthor

Diagnosis
ESCMID eLibrary
by a
uthor

Diagnostic work-up: Broad range PCR adds to the diagnostic accuracy
Review of discordant samples:
PCR positive samples added to clinical diagnosis
Culture positive/PCR negative samples
among isolates with low bacterial load/
contaminants
Bloemberg G et al. unpublished
Culture
negative
Culture
positive
Total
PCR
negative
103 43 146
PCR
positive
22 29 57
Total 125 72 197
ESCMID eLibrary
by a
uthor

Bacterial cultures from NPWT foams do not improve diagnostics
Scherrer AU et al. submittedESCMID eLibrary
by a
uthor

FDG uptake in non-infected graft as a confounder for PET/CT scan
Keidar Z, et al. J Nucl Med. 2014;55:392-395
Diffuse FDG-uptake
No focal uptake
Intensity not changing over time
SUV 1.9 (0.4-6.3)
ESCMID eLibrary
by a
uthor

PET/CT scan is very accurate for vascular graft infections
Sah BR et al. European Journal of Vascular and Endovascular Surgery; 49: 455-464
Accuracy: 94%
No antibiotics: 100%
ESCMID eLibrary
by a
uthor

Treatment
ESCMID eLibrary
by a
uthor

Surgical treatment: Removal of the infected endograft
More proximal aortic cross-clamping than index surgery
Associated with high risk of operative complications or death, or both.
Extraanatomic reconstructionIn-line reconstruction
Cernohorsky P et al. Journal of Vascular Surgery,2011;54:327-33ESCMID eLibrary
by a
uthor

Surgical treatment and outcomes of aortic endograft infections
206 Endograft infections (180 EVAR; 26 TEVAR)
Surgical management: 96% patients after mean 153 days.
90% In situ replacement (cryopreserved allograft, neoaortoiliac system, abx-
soaked prosthesis)
6% Axillary-bifemoral bypass
Outcome (mean FUP 21 month):
11% 30 day mortality, 30 % 1-year mortality, 35% 2-year mortality
15% Reinfections
Smeds et al. Journal of Vascular Surgery, Feb 2016ESCMID eLibrary
by a
uthor


Endograft infection
More proximal aortic cross-clamping than index surgery
Associated with high risk of operative complications or death, or both.
Other surgical technique?ESCMID eLibrary
by a
uthor
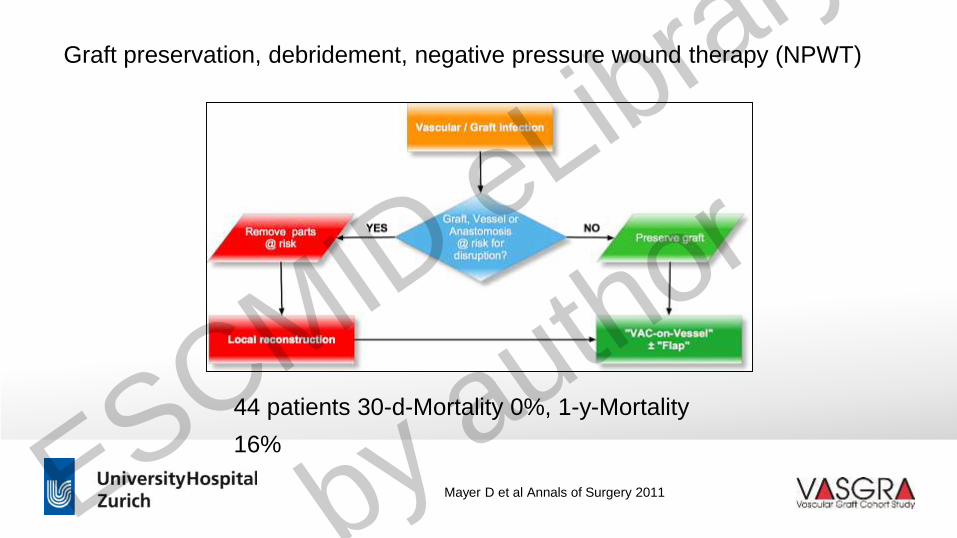
Graft preservation, debridement, negative pressure wound therapy (NPWT)
44 patients 30-d-Mortality 0%, 1-y-Mortality
16%
Mayer D et al Annals of Surgery 2011ESCMID eLibrary
by a
uthor

Endograft infection is a challenge for medical therapy
No blood flow
No vasa vasorum
Antibiotics do no reach the thrombus/ site of infection
Biofilm acts as barrier against antibiotic penetration
Evidence ?
ESCMID eLibrary
by a
uthor

Abdominal aortic graft infection - empirical therapy
Revest et, al Int Journal of Antimicr Agents 2015
Coverage of Gram positive, Gram negative and Anaerobes
Coverage of Methicillin resistant Staphylococci
Bactericidal against bacteria in stationary growth phase
Good tissue- and biofilm-penetration and safety profile
ESCMID eLibrary
by a
uthor

Do we always need antibiotics in endograft infection?
VAC VeraFlo TM
Instillation of antiseptics
ESCMID eLibrary
by a
uthor

Do we always need antibiotics in endograft infection?
Antibiotics
28 NPWT
ESCMID eLibrary
by a
uthor

Type of microorganism influences surgical treatment and vice versa
Endovascular graft infetions with barely no blood flow, withhold antibiotics in
case of instillation
If graft retention/ NPWT therapy prolongation of therapy needed
Surgical excision of infected material and extraanatomic reconstruction
recommended:
Pseudomonas aeruginosa, MRSA, Rifampicin-resistant Staphylococci
Fungi
Mycobacterium chimaera
ESCMID eLibrary
by a
uthor

Case #2 | 61-year-old male
2014 EVAR (PTFE)
04/2015 Fever, night sweats, belt-shaped
abdominal pain; CRP 65 mg/L
05/2015 Dx of aortic endograft infection
Mycobacterium chimaera
CoNS
Endograft infection
ESCMID eLibrary
by a
uthor

Extraanatomic reconstruction: axillobifemoral bypass
ESCMID eLibrary
by a
uthor

Treatment duration
ESCMID eLibrary
by a
uthor

Case #3 | 70-year-old male
Belt-shaped pain in abdomen without fever
EVAR six weeks before…
Stationary aortic aneurysm (5.5 cm)
Focal FDG-uptake on graft, SUVmax12.4
Dx: Aortic graft infection
Coagulase neg Staphylococci
Endograft infection
ESCMID eLibrary
by a
uthor

Monitoring of cancer therapy
Adeno-CA: cT1 pN3 cM0
05/2012
Cisplatin and Alimta
07/2012
Recurrence
11/2012ESCMID eLibrary
by a
uthor
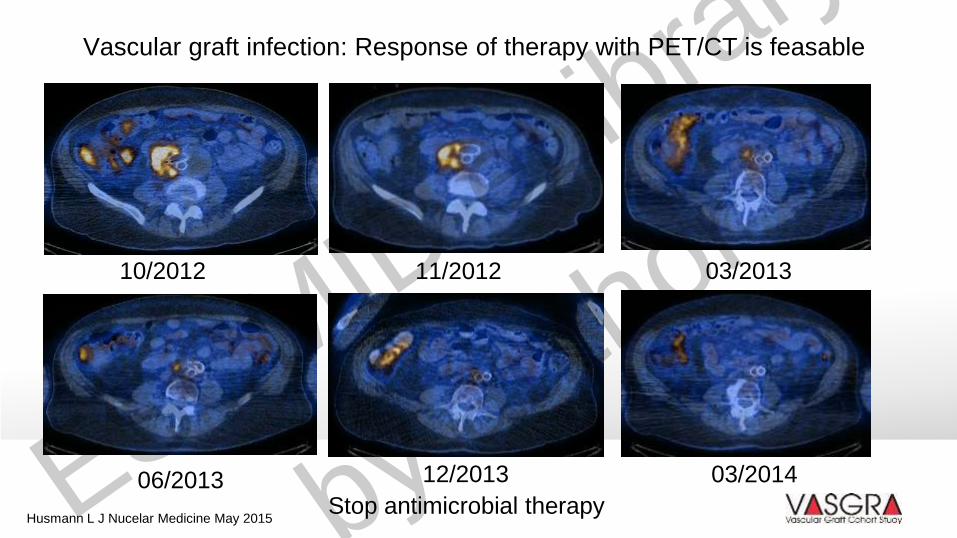
Vascular graft infection: Response of therapy with PET/CT is feasable
10/2012 11/2012 03/2013
06/2013 12/2013 03/2014
Stop antimicrobial therapyHusmann L J Nucelar Medicine May 2015ESCMID eLibrary
by a
uthor

Conclusions
Suggestions for treatment algorithms
ESCMID eLibrary
by a
uthor

Vascular graft infections qualifying for implant preservation
Implant, anastomosis
and soft tissue intact
Vascular graft infection
Implant, anastomosis
not intact
Preserve graft Remove parts risk
Prerequisites
• Condition of implant, anastomosis and soft tissue good
• Perioperative culture positive
• Susceptibility to antimicrobial agents with activity against surface-adhering
microorganisms
Negative pressure
wound therapy
+
Flap
ESCMID eLibrary
by a
uthor

Vascular graft infections not qualifying for implant preservation
Vascular graft infection
Aortoenteric fistula
Tissue defect
Supressive therapy In-situ
reconstruction
Extraanatomic
reconstruction
Recommended
• Difficult to treat microorganisms
• Severely compromised tissue
• Comorbidities, Drug abuse (?)
High risk for surgery
Comorbidities
Difficult-to-treat
organisms
ESCMID eLibrary
by a
uthor

Strategy antimicrobial therapy
Vascular graft infection
SIRS
Delayed surgeryNo SIRS
Immediate surgery
Start empirical therapy
immediatelyAwait microbiology
culture results
Adapt antimicrobial
therapy in accordance
with deep tissue and
blood cultureESCMID eLibrary
by a
uthor

Length of antimicrobial therapy depends on surgical strategy
171 patients (FUP 3.4), Healed 75%, Death due to PVGI 9.6 %
ESCMID eLibrary
by a
uthor

Dieter Mayer
Vascular surgeryAnnelies Zinkernagel
Translational Research
Caroline Müller
Study nurse
Lars Husmann
Nuclear medicine
Guido Bloemberg, Microbiologist Simone Bürgin, Study nurse
Alexandra Scherrer, Statistics Marisa Kälin & Ulrich Matt, Infectious Diseases Service
Zoran Rancic, Vascular surgery Rainer Weber, Infectious Disease Service
Mario Lachat , Vascular surgery Irene Burger & Bert-Ram Sah, Nuclear medicine
Vontobel Foundation
Rozalia StiftungESCMID eLibrary
by a
uthor