management of lower gi bleeding m k alam ms; frcs almaarefa college
TRANSCRIPT
Management of lower GI bleeding
M K Alam MS; FRCS
ALMAAREFA COLLEGE

Learning objectives (ILOs)
At the end of this presentation students will be able to:
Define lower GI haemorrhage (LGIB). Enumerate the causes of LGIB. Describe the pathophysiology of LGIB Describe the symptoms and signs Describe the diagnostic work up. Describe the resuscitative measures. Describe the management- non-surgical and
surgical interventions.
Introduction
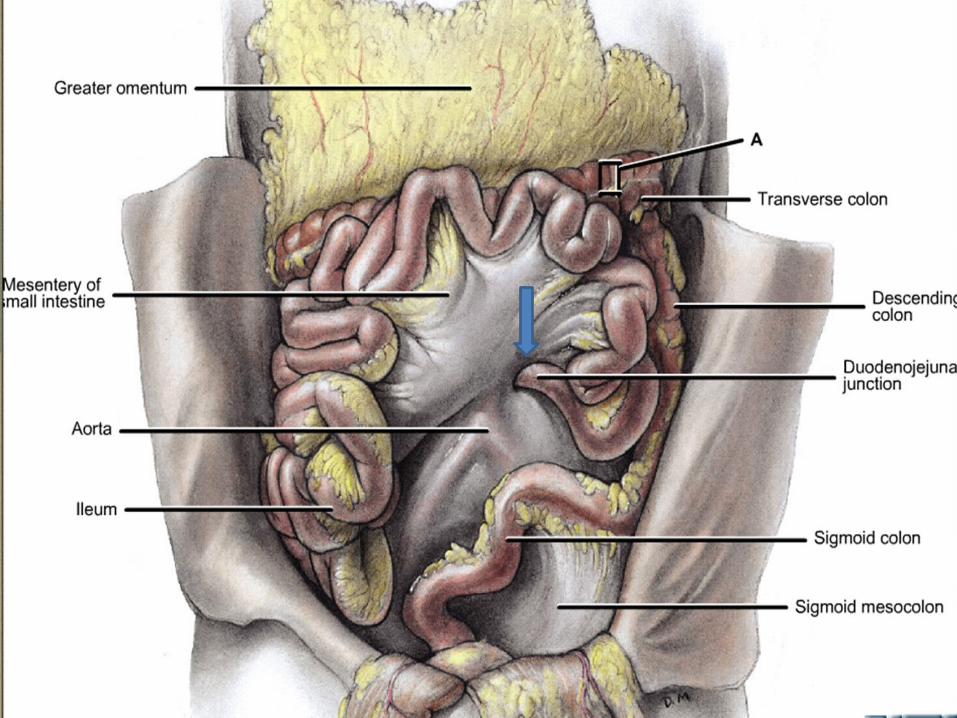
• Definition: Bleeding distal to DJ flexure- ligament of Treitz
• Frequent cause of hospital admission, morbidity & mortality.
• 20-33% of all gastrointestinal bleeding.
• Proximal to caecum- melena
• Right colon- maroon color
• Left colon- bright red bleeding
• Brisk UGI bleeding- bright red color

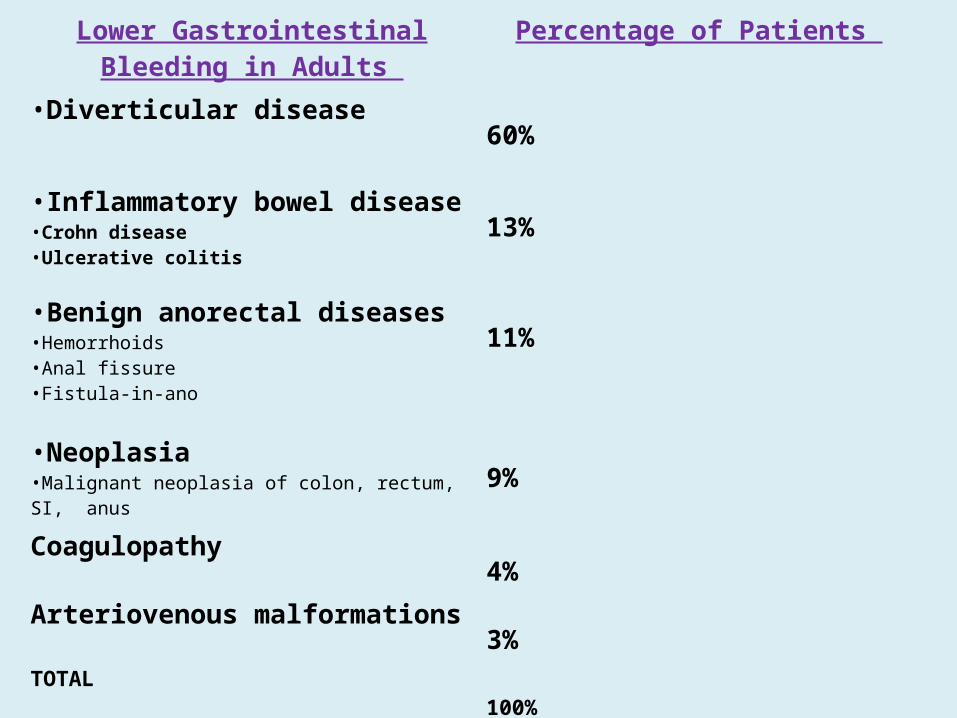
Lower Gastrointestinal Bleeding in Adults
Percentage of Patients
•Diverticular disease 60%
•Inflammatory bowel disease •Crohn disease•Ulcerative colitis
13%
•Benign anorectal diseases•Hemorrhoids•Anal fissure•Fistula-in-ano
11%
•Neoplasia•Malignant neoplasia of colon, rectum, SI, anus
9%
Coagulopathy 4%
Arteriovenous malformations 3%TOTAL 100%
Source: Vernava AM, Longo WE, Virgo KS. A nationwide study of the incidence and etiology of lower gastrointestinal bleeding. Surg Res Commun. 1996;18:113-20.[8]

Diverticulosis
• Dominant cause of LGIB
• Saclike protrusion through the circular muscle fibers at a point
where the vessel has perforated.
• Vessel becomes draped over the dome of the diverticulum
• Most commonly located in the sigmoid and descending colon
• Bleeding originates from vasa rectae in the submucosa
• Risk factors: Lack of dietary fiber, constipation, advanced age, and
use of NSAIDs and aspirin.

Angiodysplasia
• Most common A-V malformations found in the GIT
• Most common site- cecum and ascending colon;
• Acquired lesions, affect elderly persons >60 years
• Bleeding is venocapillary in origin.
• Generally less vigorous than diverticular bleeding.
• 80% untreated angiodysplasia experience rebleeding.

Colitis (IBD)• Massive hemorrhage-due to IBD is rare
• Ulcerative colitis- bloody diarrhea in most, mild to moderate LGIB in up to 50%.
• Crohn disease -LGIB is not as common. Bleeding more common with colonic involvement than small bowel involvement.
• Ischemic colitis- elderly with abdominal pain and bloody diarrhea. Involves splenic flexure and the rectosigmoid. Not associated with significant blood loss or hematochezia.
Neoplasm
• Polyps and carcinoma
• Occult bleeding
• Low grade and frequent bleeding- common
• Massive bleeding- unusual

Other diseases
• Benign anorectal disease (eg, hemorrhoids, anal fissures, anorectal fistulas) cause intermittent rectal bleeding. 11% of patients with LGIB had hemorrhage from anorectal disease.[8]
• Small intestinal conditions (Peutz-Jeghers syndrome, hemangiomas, and adenocarcinomas) may cause bleeding, but are usually occult in nature.
Signs and symptoms
• Variable- depending on the etiology
• Mild and intermittent- angiodysplasia, colon carcinoma
• Colon carcinoma rarely causes significant LGIB.
• Moderate/ severe: Diverticula-related bleeding.
Signs and symptoms
• Young patients with infectious or noninfectious (idiopathic) colitis : • Fever• Dehydration• Abdominal cramps• Hematochezia
• Older patients with diverticular bleeding or angiodysplasia: Painless
bleeding and minimal symptoms.
• Ischemic colitis: Abdominal pain, and varying degrees of bleeding
• Massive lower GI bleeding usually in ≥65 years.

Massive LGIB
• Age > 65
• Hematochezia or bright red blood PR
• Hemodynamically unstable
• Diverticulosis, angiodysplasia
Lower GI bleeding rate
• Moderate bleeding: Hematochezia or melena. Hemodynamically stable. Benign anorectal conditions, IBD, neoplasia.
• Occult bleeding: Microcytic hypochromic anemia.
Benign anorectal conditions, IBD, neoplasia.

Diagnosis
• History & physical examination in all patients
• Nasogastric tube insertion
• Digital rectal examination, and anoscopy /proctoscopy
• Complete blood cell (CBC) count
• Serum electrolytes levels
• Coagulation profile: aPTT, PT, platelet count

Diagnosis (COLONOSCOPY)
• Flexible colonoscopy: Initial diagnostic method of choice.
• Hemodynamically stable.
• Colonoscopy following a rapid bowel preparation.
• Bowel prep colonoscopy- higher diagnostic/ therapeutic
yields than unprepped colonoscopic evaluation.
• Successfully identify the origin of severe LGIB in 80-90% .
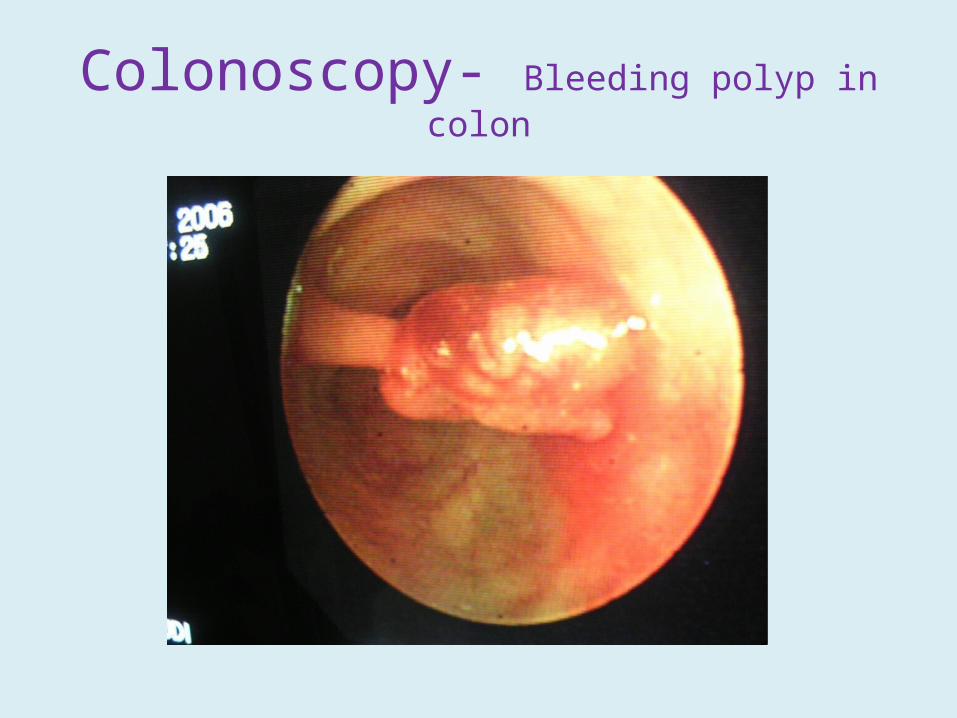
Colonoscopy- Bleeding polyp in colon
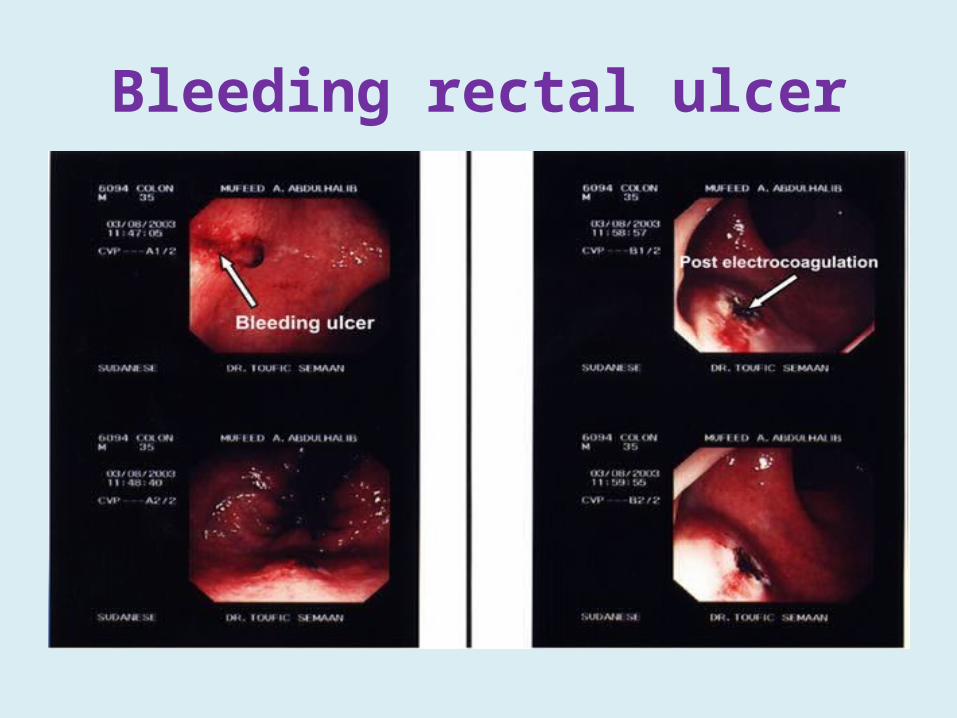
Bleeding rectal ulcer
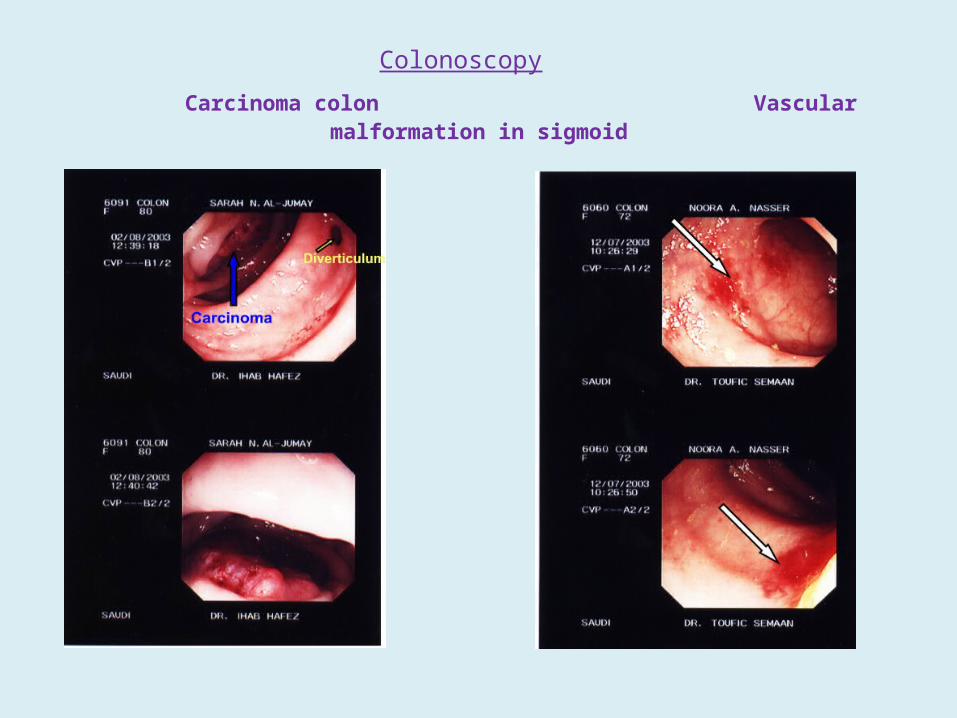
Colonoscopy Carcinoma colon Vascular malformation in sigmoid
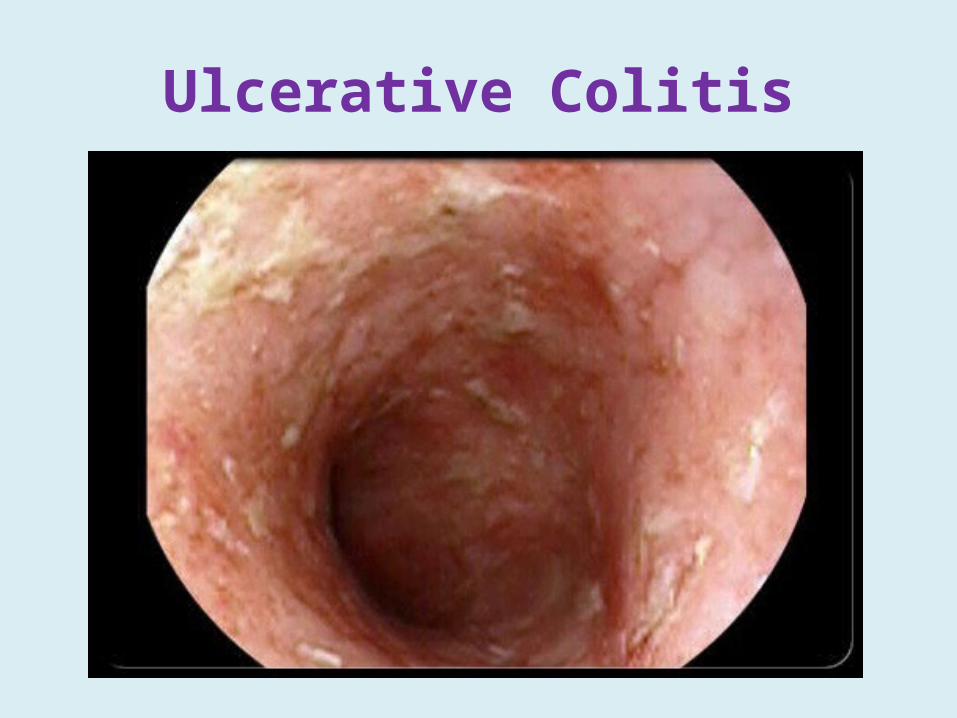
Ulcerative Colitis
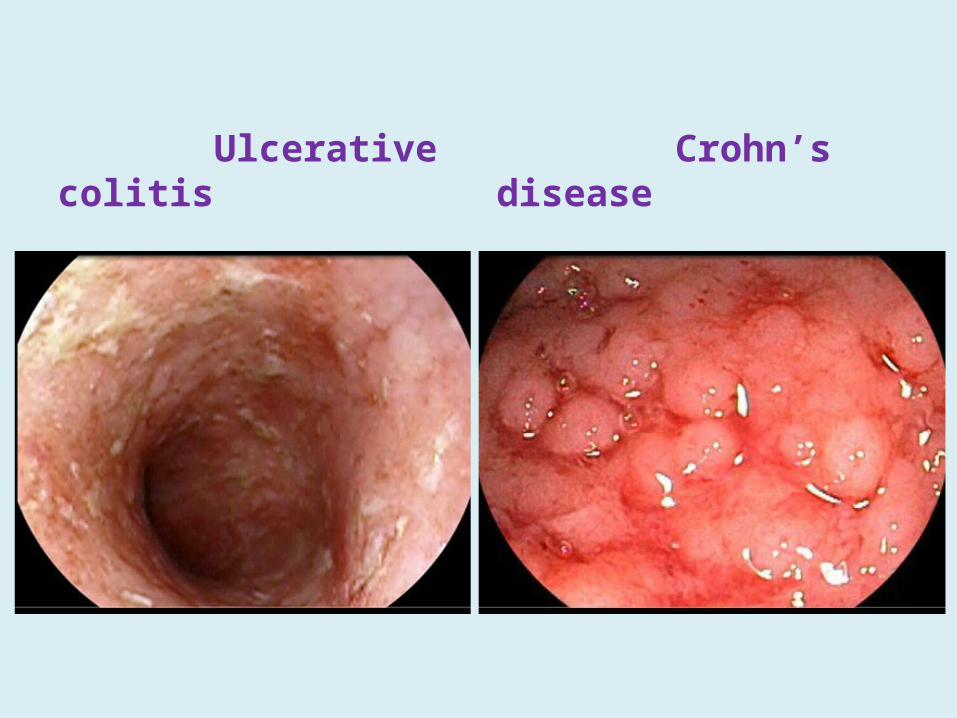
Ulcerative colitis Crohn’s disease

Colonic Diverticulosis

Other diagnostic modalities
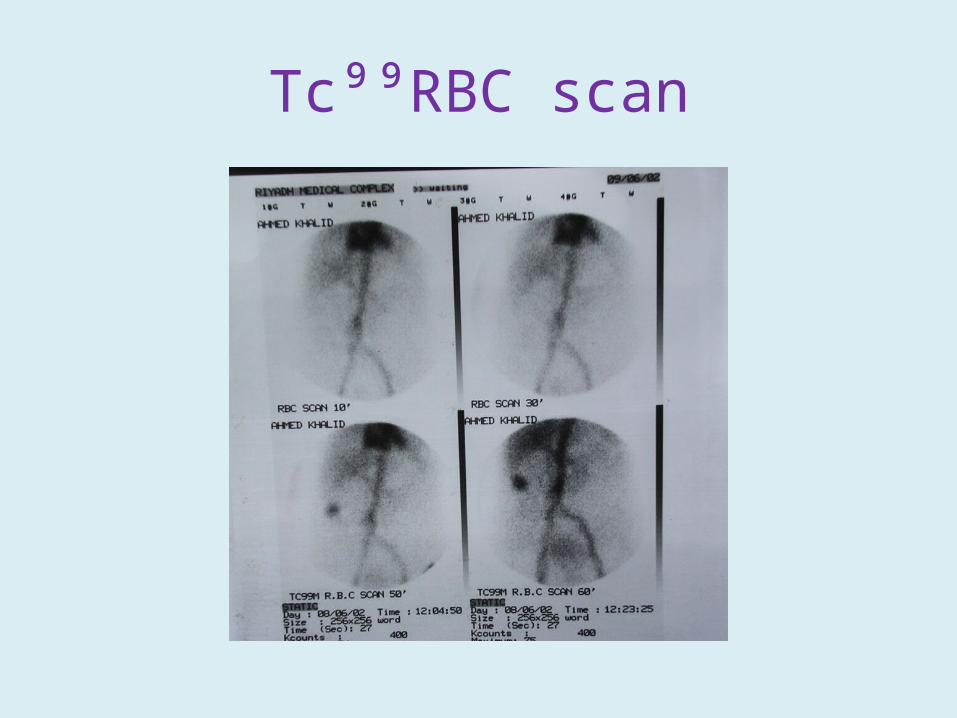
• RBC scan can detect hemorrhage at rates as low as 0.1-0.5
mL/min.
• Angiography: Detects bleeding at rates of 1-1.5 mL/min.
Indications: Brisk ongoing LGIB, hemodynamically unstable, with
or without a preceding radionuclide scan & failed colonoscopy.
• CT scanning (A & P): Routine workup failed- contrast
extravasation, bowel wall enhancement, vascular dilatation
• Exploratory laparotomy (rarely): Intraoperative push enteroscopy
in hemodynamically unstable patients.

Patients with multiple episodes of LGIB without a known source
• Elective mesenteric angiography• Upper and lower endoscopy• Meckel scanning (Tc⁹⁹)• Upper GI series with small bowel• Enteroclysis
Tc⁹⁹RBC scan
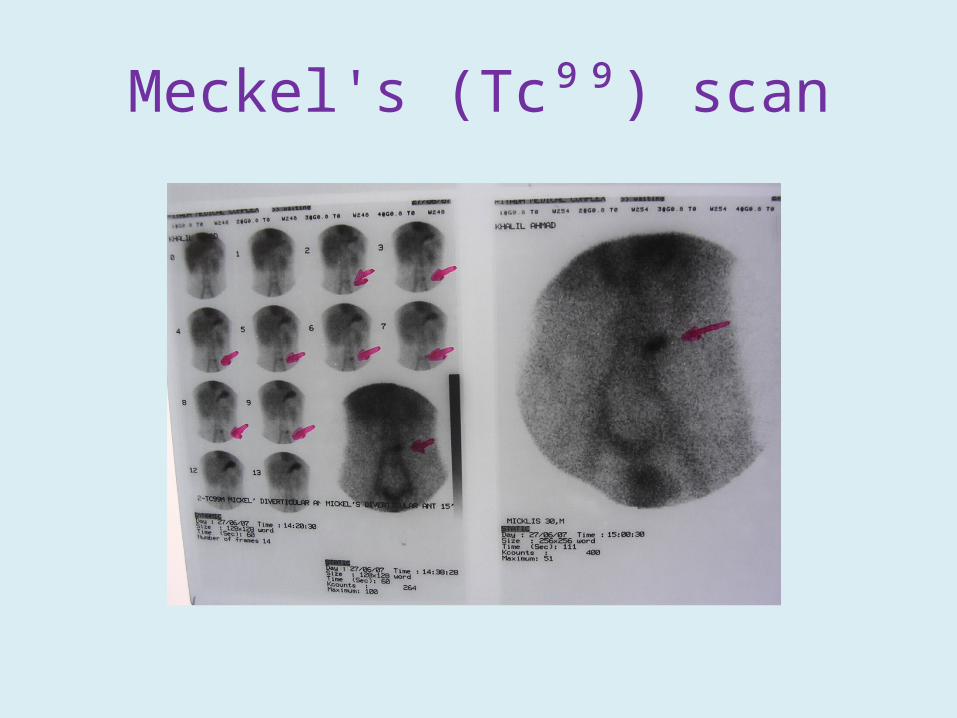
Meckel's (Tc⁹⁹) scan
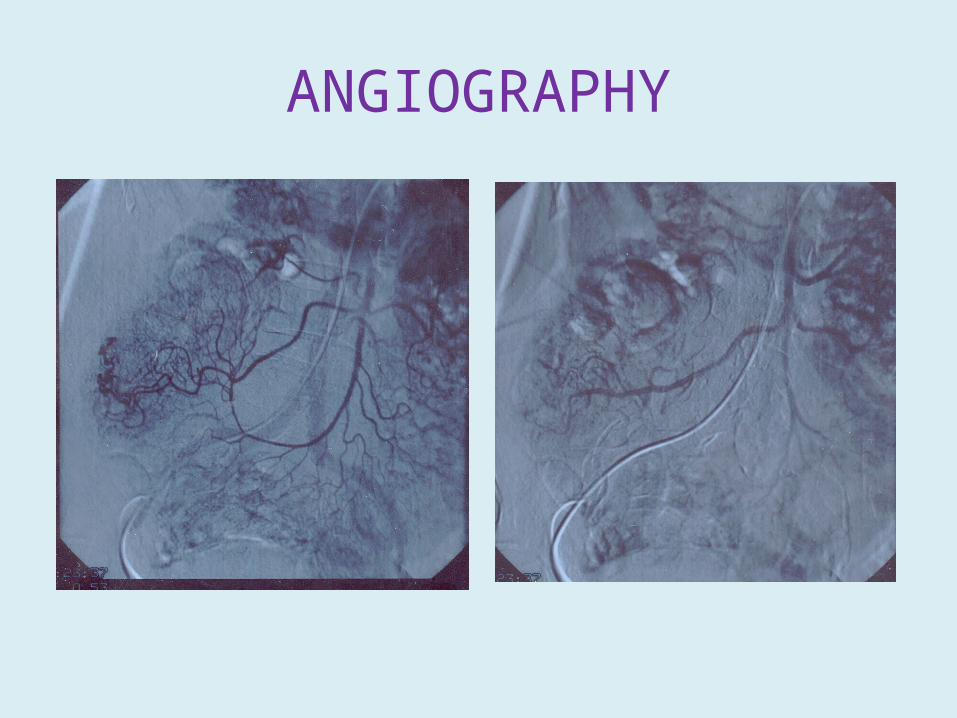
ANGIOGRAPHY

Haemorrhoids Anal fistula
Principles of Management
• Resuscitation and initial assessment
• Localization of the bleeding site
• Therapeutic intervention to stop bleeding
Resuscitation and initial assessment
• Large-bore IV access and • Administration of normal saline.• Blood sample: CBC, electrolytes, coagulation
profile, crossmatch. • Patient's blood loss and hemodynamic status
should be ascertained.• In cases of severe bleeding-invasive
hemodynamic monitoring to direct therapy.

Localization of the bleeding site
• Flexible colonoscopy ( hemodynamic stability)
• RBC isotope scan
• Angiography
• CT scan
• Upper GI endoscopy

Therapeutic interventions
• Diverticular bleeding: Colonoscopy with bipolar probe
coagulation, epinephrine injection, or metallic clips. Recurrent
bleeding- resection of the affected bowel segment.
• Angiodysplasia: Thermal therapy (electrocoagulation, argon)
• Ischemic colitis : NPO and IV hydration.
• Bleeding site cannot be determined: Vasoconstrictive agents- vasopressin (Pitressin) used.
Vasopressin unsuccessful/contraindicated-
superselective embolization.
Superselective angiographic embolization
• The most feared complication of embolization of the mesenteric vessels is ischemic colitis.
• Has limited its use for GI bleeding.

SURGERY
• The indications for surgery include the following:
• Active persistent bleeding with hemodynamic instability that is refractory to aggressive resuscitation
• Persistent, recurrent bleeding• Transfusion of >4 units PRBC in a 24-hours with
active or recurrent bleeding• Transfusion of >6 units of PRBC during the same
hospitalization
Surgery• Segmental bowel resection following precise localization
of the bleeding point. Low morbidity and mortality when compared with subtotal colectomy.
• Subtotal (total abdominal) colectomy with temporary end ileostomy is the procedure of choice in patients who are actively bleeding from an unknown source.
• Blind segmental resection should not be performed because of a prohibitively high rebleeding rate, morbidity, and mortality rate.

Thank you!