management of type 2 diabetes in youth cindy cain rn, pnp phil zeitler md, phd university of...
Post on 21-Dec-2015
216 views
TRANSCRIPT
Management of Type 2 diabetes in Youth
Cindy Cain RN, PNPPhil Zeitler MD, PhD
University of Colorado DenverAurora, CO

Progression of insulin resistance to glucose intolerance
ObesityObesity with
Insulin resistanceGeneticslifestyle
Obesity and hyperinsulinemia
NGT
Compensatorysecretion
Obesity and hyperinsulinemia
IGT
Worseningresistance
Obesity and hyperinsulinemia
IFG cell failureHGO
T2DM
cell failure
Metabolic syndrome

Metabolic Syndrome
A clustering of cardiovascular risk factors first noted in large epidemiologic studies
Visceral adiposity Insulin resistance Low HDL Systemic pro-inflammatory state
Subsequently also associated with Elevated triglycerides dysglycemia PCOS Fatty liver disease

Mortality Associated With Metabolic "syndrome"
Lakka H-M et al. JAMA. 2002;288:2709-2716.
18
9
6
8
32
0
2
4
6
8
10
12
14
16
18
20
All-cause mortality* CVD mortality* CHD mortality*
Metabolic "syndrome"
No metabolic "syndrome"
Mo
rtal
ity
(% o
f p
atie
nts
)
2003 PPS®
*Adjusted for known CHD risk factors.
POWERSEARCH PLUG-IN™ 2.0Copyright © 2001-02 Accent Graphics, Inc.
Slide Source: "R:\NDEI-2\2004 Grant\T108\ARS\T095 ARS Case 2 FINAL-Baton Rouge 12-09-03.ppt" <OPEN>Last Modified: December 9, 2003 2:17:25 PMSlide Number: 19
POWERSEARCH PLUG-IN™ 2.0Copyright © 2001-02 Accent Graphics, Inc.
Slide Source: "R:\NDEI-2\2004 Grant\T108\ARS\T095 ARS Case 2 FINAL-Baton Rouge 12-09-03.ppt" <OPEN>Last Modified: December 9, 2003 2:17:25 PMSlide Number: 19
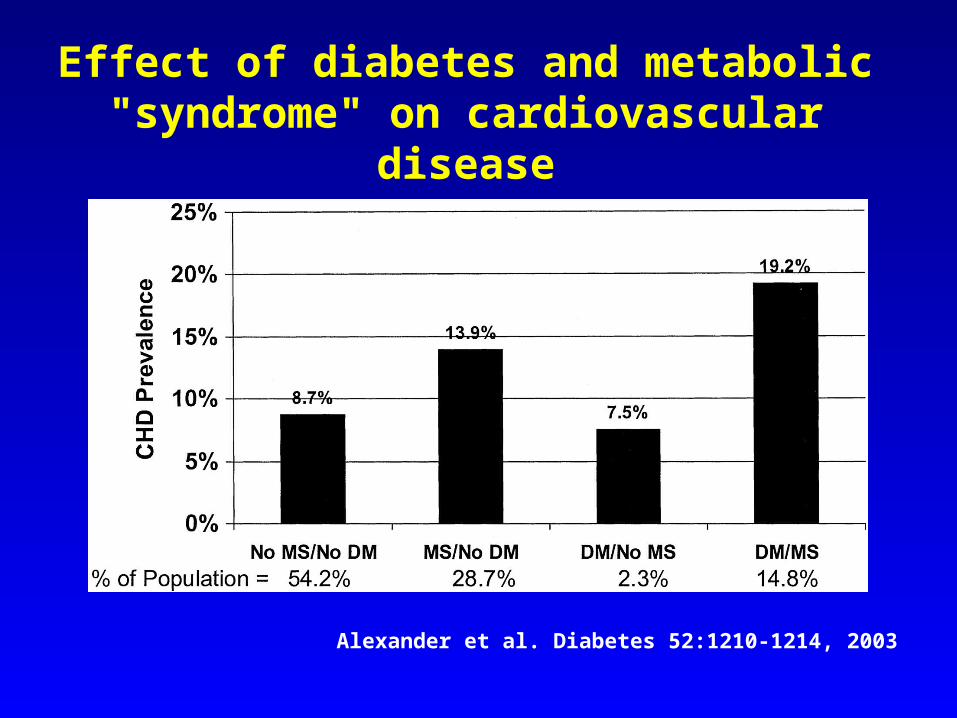
Effect of diabetes and metabolic "syndrome" on cardiovascular disease
Alexander et al. Diabetes 52:1210-1214, 2003
Metabolic syndrome and vascular complications
in type 2 youth
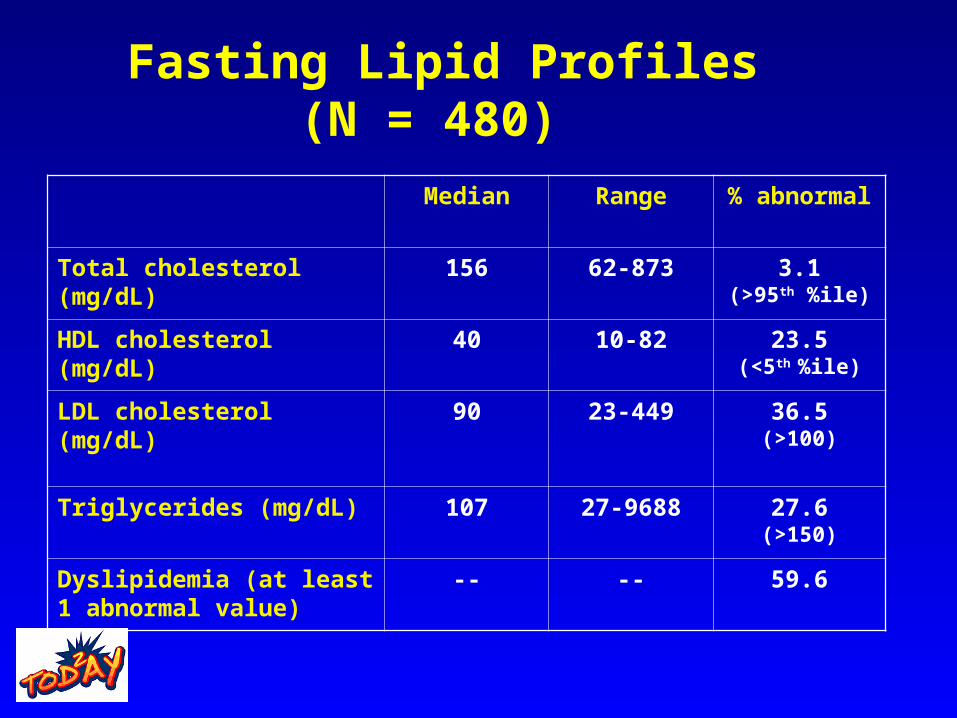
Fasting Lipid Profiles (N = 480)
Median Range % abnormal
Total cholesterol (mg/dL) 156 62-873 3.1(>95th %ile)
HDL cholesterol (mg/dL) 40 10-82 23.5(<5th %ile)
LDL cholesterol (mg/dL) 90 23-449 36.5(>100)
Triglycerides (mg/dL) 107 27-9688 27.6(>150)
Dyslipidemia (at least 1 abnormal value)
-- -- 59.6

Type 2 youth with Hypertension and Dyslipidemia (N=480)
Dyslipidemia
No
Dyslipidemia
Yes
TOTAL
BP <95th %ile 154
(32%)
202
(42%)
356
(74%)
BP >95th %ile 42
(9%)
82
(17%)
124
(26%)
TOTAL 196
(41%)
284
(59%)
480
(100%)
MIC at
DX
Yrs
F/U
HT at
F/U
MIC at
F/U
MAC at
F/U
Age at Dx/
comparison
Pt #
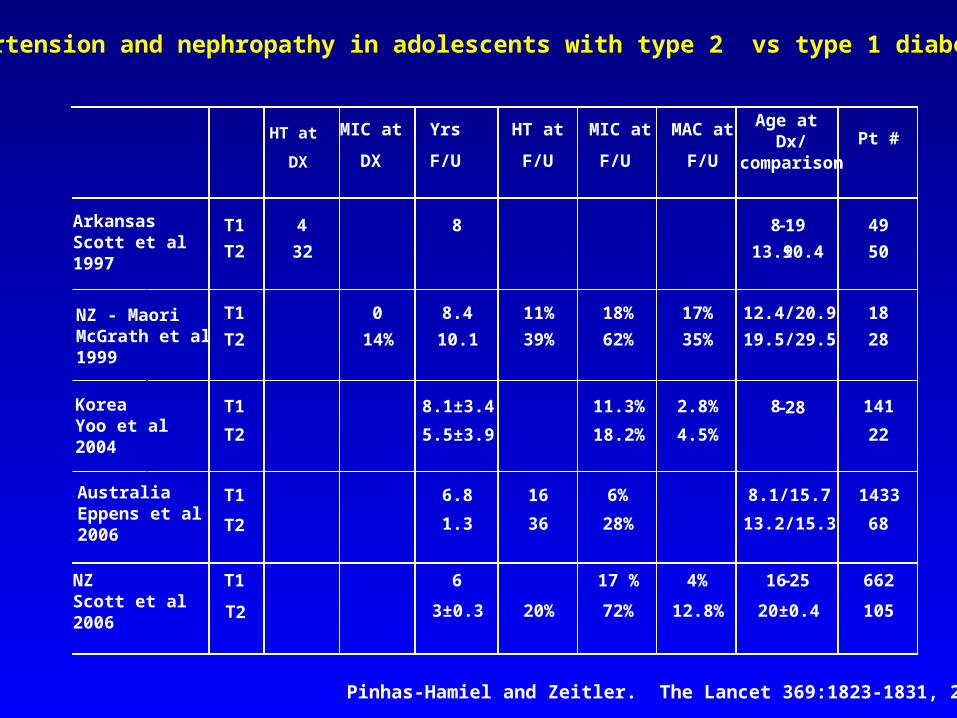
ArkansasScott et al1997
T1
T2
4
32
8
8-19
13.9±0.4 49
50
NZ - MaoriMcGrath et al1999
T1
T2
0
14%
8.4
10.1
11%
39%
18%
62%
17%
35%
12.4/20.9
19.5/29.5
18
28
KoreaYoo et al 2004
T1
T2
8.1±3.4
5.5±3.9
11.3%
18.2%
2.8%
4.5%
8-28
141
22
AustraliaEppens et al2006
T1
T2
6.8
1.3
16
36
6%
28%
1433
68
8.1/15.7
13.2/15.3
NZScott et al2006
T1
T2
6
3±0.3 20%
17 %
72%
4%
12.8%
16-25
20±0.4
662
105
Hypertension and nephropathy in adolescents with type 2 vs type 1 diabetes
HT at
DX
Pinhas-Hamiel and Zeitler. The Lancet 369:1823-1831, 2007

Type 1 versus Type 2 Outcomes in Youth
Results Type 1 n-1433 Type 2 n-68
Retinopathy 20% 4% p<0.0001Microalbuminuria 6% 28% p<0.0001
Hypertension 16% 36% p<0.0001Neuropathy, peripheral 27% 21%
Neuropathy, autonomic 61% 57%
A1c 8.5% 7.3%Hypertriglyceridemia 53%
Hypercholesterolemia 32%
Eppen, et al Diabetes Care 29:1300,06
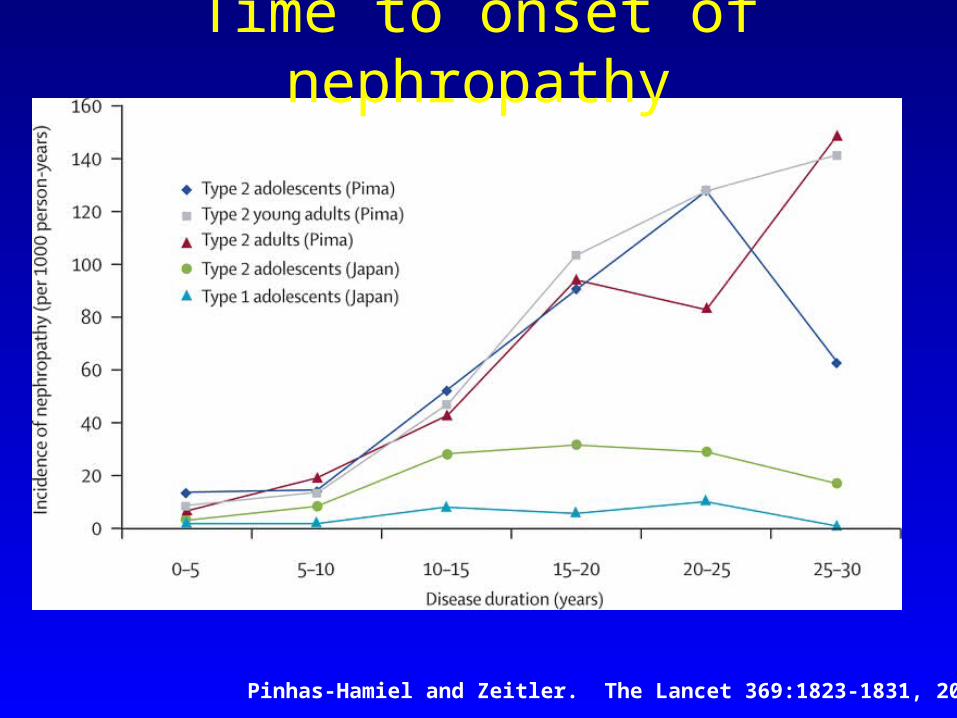
Time to onset of nephropathy
Pinhas-Hamiel and Zeitler. The Lancet 369:1823-1831, 2007

Treatment

Treatment Approach – Diabetes
– Lifestyle change must be part of any
intervention
• Standard diabetes education
• Intensive intervention
– Little evidence that this is effective on its
own in children
– In patients with overt diabetes, lifestyle
change should be used in combination with
drug therapy

Glycemic Targets

Glucose– Target
• Primary - Hemoglobin A1c < 6.5%
• Secondary
– Fasting BG < 120
– Post-prandial BG < 140
– Monitoring (if not on insulin)
• Finger stick blood glucose
– Twice a day
– 3-5 days a week
– When ill

Metformin
• Mechanism of action– suppression of HGO
– Secondary decrease in insulin levels
– May have peripheral effects?
• Well-studied in adults and children – effective, safe, and inexpensive
• Most pediatric experience of oral agents– Approximately 45% of patients nationally
• Approved for pediatric use in diabetes

Metformin• Desirable properties –
– weight loss
– Mild improvement in lipids
– Improvement in menstrual irregularities/hirsutism
– ? Improvement in hepatic steatosis
• Minimal side effects – – GI - can be avoided with slow titration
– Lactic acidosis –metanalysis of 40,000 patients – no increased lactic acidosis - even when used with contraindications
• Salpeter et al Arch Intern Med. 2003 163:2594, 2003

Sulfonylureas
• Insulin secretagogues
• Well-studied in adults – effective, safe, inexpensive
• Side effects significant– Weight gain – hypoglycemia
• no effect on lipids• Rarely used in Pediatrics
– MODY

Thiazolidinediones• PPAR agonists
– Alter adipocyte and muscle metabolism to promote increased insulin sensitivity
– rosiglitazone, pioglitazone
• Well-studied in adults– Lower A1c ~1%
– Beneficial effects on lipids
• May prolong -cell function• Not approved in Youth
– Very limited pediatric Experience– One clinical trial – never published
Thiazolidinediones• Extensive Side effects
– Weight gain• Visceral vs subcutaneous fat • may not be deleterious
– Edema– Decreased bone density?– Increased cardiac dysfunction
• Implications for youth with “young” hearts but hypertension and dyslipidemia
– Macular edema– Liver dysfunction

Metaglinide analogs• Insulin secretagogues
– Short acting
– Glucose-dependent
– repaglinide, nateglinide
• May be helpful in control of post-prandial
hyperglycemia
• Compliance before meals difficult for adolescents

Insulin
• Not generally considered first line therapy for
type 2 in adults
– Weight gain
– Hypoglycemia
– management burden
– ? Increased cardiovascular risk

BUT
• It works!
• It may synergize with other therapies by reducing glucose toxicity
• Familiar to pediatricians and pediatric diabetologists– 25-30% of adolescent type 2 patients are being treated with insulin
alone.
• Patients often started on insulin – – ? Diagnosis, acute metabolic decompensation
• More serious illness = Better compliance?
• Preservation of b-cell function?

Treatment Algorithm: Treatment Algorithm: Current Practice Among Pediatric Current Practice Among Pediatric
EndocrinologistsEndocrinologists • No evidence• New onset
– “Reasonable” control (A1c <8–10, nonketotic)• Start metformin at 500 mg q/d• Titrate as tolerated (<500 mg/wk) to maximum
of 2000 mg/d• Initiate SDE, with additional focus on basic
lifestyle change and weight loss– Little evidence for efficacy of lifestyle alone
SDE = standard diabetes education.

Treatment AlgorithmTreatment Algorithm• New onset • “Poor” control (A1c >8–10)
– Without acidosis• Start metformin at 500 mg q/d and basal insulin
(15-30 units qhs)– Titrate metformin as tolerated (<500 mg/wk)
to maximum of 2000 mg/d– Once glucose control is attained, wean insulin as tolerated
– With acidosis– Treat as you would in type 1 until acidosis resolved– Start metformin and subcutaneous insulin as needed– Wean insulin as tolerated

Treatment AlgorithmTreatment Algorithm• Intensification of therapy
– Failure to maintain A1c <6.5 – Add-on insulin
• Once-daily basal insulin (glargine or detemir) – start at 10–20 units a day
– Given whenever adherence and supervision are most likely
– Titrate as needed to maintain A1c <6.5
• Addition of short-acting insulin– Inability to maintain A1c in target despite 1 unit/kg long-acting
insulin
– Evidence for postprandial hyperglycemia

Treatment AlgorithmTreatment Algorithm• Intensification of therapy
– Other options1,2
• Exenatide – Incretin – GLP-1 analog
» Slows gastric emptying» Decreases appetite» Increases glucose-dependent insulin secretion» Injected bid before meals» Not FDA approved – pediatric trials pending
• DPP-4 inhibitors– Sitagliptin
» Inhibits GLP-1 inactivation» Actions similar to exenatide but no weight loss» Not FDA approved – pediatric trials pending
1. Holst JJ. Expert Opin Emerg Drugs. 2004;9(1):155-166. 2. Drucker DJ et al. Lancet. 2006;368(9548):1696-1705.

Non-glycemic targets

AHA/ADA Consensus
• Atherosclerotic lesions in youth correlate with established risk factors
• Risk factors track from childhood into adulthood
• Behaviors associated with risk acquired during childhood
• No controlled trial comparing risk reduction will ever be done
(Kavey et al, Circulation 114:2710-2738, 2006)
Lipids
• LDL < 160 mg/dl (?130) {<100 mg/dL in DM}
• LDL > goal – diet therapy (7% sat fat, < 200 mg chol)
• LDL > 160 mg/dl after 6 months of TLC
• “It may be appropriate to treat”
• TG < 150 mg/dl fasting
• TG > 400
• treat – to avoid postprandial > 1000 mg/dl
• HDL > 35 mg/dL

Treatment - lipids
• Same as in Adults– Efficacy in lipid lowering similar– No evidence for (or against)
cardioprotective effect with any intervention
• Statins
• Fish Oil/Omega 3 Fatty acids
• Ezetimibe
• Nicotinic acid
• Fibrates
Blood pressure
• Goal < 95%ile for age
• pharmacologic therapy may be appropriate if >
95%ile AND
• No improvement with lifestyle modification
• Evidence of target organ damage (microalbuminuria)
• ACE or ARB first line drug
• Titrate ACE until BP < 90th %ile

Microalbuminuria
• Random urine albumin/creatinine ratio
• Normal < 30
• Abnormal sample repeated fasting
• 2 of 3 abnormal is diagnostic
• Start therapy with ACE and titrate until
microalbumin normal

Treatment – BP, albumin
• Same as adults– ACE inhibitor
– Angiotensin receptor blocker (ARB)
– Diuretics
– Calcium channel blockers (CaCB)
– Beta adrenergic antagonists

CASE DISCUSSION

Dominick• 15 yo Hispanic male with long history of
overweight and newly diagnosed diabetes (Fasting glucose 289)
• Denies change in eating or activity habits– “Healthy” diet with large portions sizes– Fast food 2-3 times a week– Active in sports (football, lacrosse)
• No medications• ROS: Polyuria, polydipsia, fatigue for 3 months

Dominick
• Past Hx:
– BW 8 lbs, 2 oz, T2DM
• Fam Hx:
– Mother and father with T2DM (dx 45 and 43)
– T2DM in maternal and paternal grandparents
– Maternal grandfather with MI age 62

Dominick
• Exam– Ht 75%ile
– Wt > 95%ile
– BMI 32
– BP 120/58
– Acanthosis nigricans at neck, IP joints
– Tanner 5

Dominick
• Laboratory evaluation?
• Other evaluations?
• Interventions?
• Follow-up Care