management of urinary incontinence. depends on the patient! age effect on quality of life type of...
TRANSCRIPT
Management of Urinary Incontinence
Depends on the patient!• Age• Effect on quality of life• Type of incontinence• Presence of prolapse

Activity!
• Sort the cards into management options for stress incontinence or overactive bladder.
• Line them up in the order that you would offer them, there may be more than one at the same time.
• Of course, not every option is suitable for every patient.
Stress incontinence
Conservative• Lifestyle
interventions• Pelvic floor
exercises +/- biofeedback
• Vaginal cones• Ring pessary
Medical• Vaginal oestrogen• Duloxetine
Surgical• TVT• Pelvic floor repair

Overactive Bladder
Conservative• Lifestyle
interventions• Bladder
retraining• Pelvic floor
exercises
Medical• Vaginal
oestrogen• Anti-muscarinics
Surgical • Sacral nerve
root stimulation• Botox• Detrusor
myomectomy• Augmentation
cystoplasty
Lifestyle Interventions
Pelvic Floor Exercises
• More effective if supervised• +/- biofeedback• Refer to community continence services• Vaginal cones
Bladder Retraining
• To re-establish cortical control over voiding• Regular voiding, gradually increasing
intervals.• Using distraction and relaxation techniques• Bladder diary will show improvement
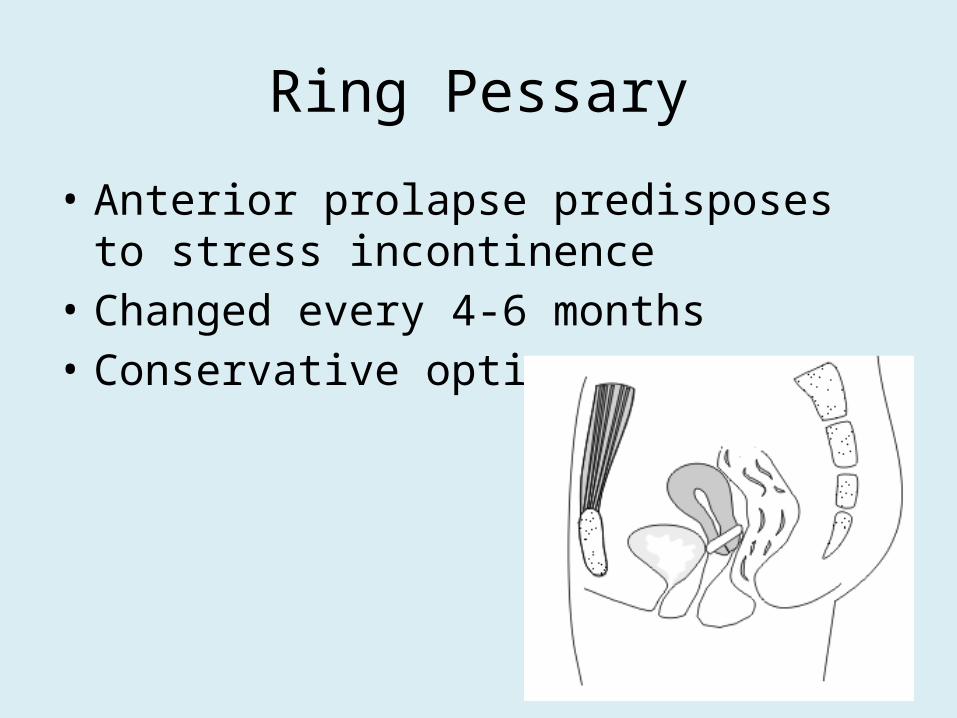
Ring Pessary
• Anterior prolapse predisposes to stress incontinence
• Changed every 4-6 months• Conservative option
Anti-muscarinic medication
• Oxybutinin 2.5mg, 5mg• Tolterodine (Detrusitol), Trospium (Regurin)• CI: myasthenia gravis, significant bladder outflow obstruction or urinary
retention, severe ulcerative colitis, toxic megacolon, and in gastro-intestinal obstruction or intestinal atony.
• SE: dry mouth, gastro-intestinal disturbances including constipation, flatulence, taste disturbances, blurred vision, dry eyes, drowsiness, dizziness, fatigue, difficulty in micturition (less commonly urinary retention)
• Try several before giving up
Other medications
DuloxetineSNRIIncreases urethral closure pressure20-40mg bdSE: GI disturbance, headache, dry mouth, rarely suicidal ideation
Vaginal Oestrogense.g. Ovestin, Vagifem, Ortho-gynestAll postmenopausal women not on HRTOestrogen breaks advised (?endometrial Ca risk)
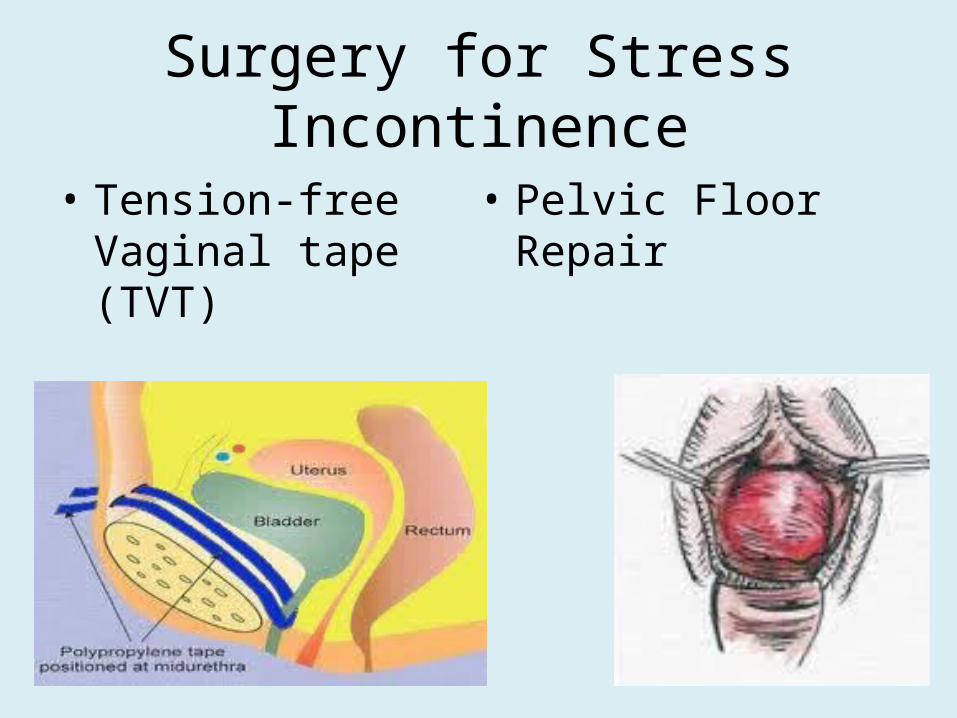
Surgery for Stress Incontinence
• Tension-free Vaginal tape (TVT)
• Pelvic Floor Repair

Surgery for Overactive Bladder
• A last resort!• Sacral nerve root stimulation• Botox• Detrusor Myomectomy• Augmentation Cystoplasty
Any Questions?