managing asthma in primary care: putting new guideline recommendations into context
TRANSCRIPT

707
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
Managing Asthma in Primary Care: Putting New Guideline Recommendations Into Context
REVIEW
Michael E. Wechsler, MD
Many patients with asthma are treated in the primary care set-
ting. The primary care physician is therefore in a key position to
recognize poorly controlled asthma and to improve asthma man-
agement for these patients. However, current evidence continues
to show that, for a substantial number of patients, asthma control
is inadequate for a wide variety of reasons, both physician-related
and patient-related. The most recently updated treatment guide-
lines from the National Asthma Education and Prevention Program
were designed to help clinicians, including primary care physi-
cians, manage asthma more effectively with an increased focus
on achieving and maintaining good asthma control over time. The
current review is intended to assist primary care physicians in
improving asthma control among their patients; this review clari-
fies the new guidelines and provides a specialist’s perspective
on diagnosis, appropriate therapy, disease control surveillance,
and appropriate referral when necessary. This discussion is based
primarily on the new guidelines and the references cited therein,
supplemented by the author’s own clinical experience.
Mayo Clin Proc. 2009;84(8):707-717
ACT = Asthma Control Test; EPR3 = Expert Panel Report 3; FeNO =
fractionated exhaled nitric oxide; ICS = inhaled corticosteroid; LABA =
long-acting β-agonist; NAEPP = National Asthma Education and Preven-
tion Program; RAST = radioallergosorbent test
From the Division of Pulmonary and Critical Care Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA.
From 2007 to 2009, Dr Wechsler consulted for or participated in advisory boards or speakers bureaus for AstraZeneca, GlaxoSmithKline, Schering-Plough, Novartis, Genentech, Merck, MediciNova, and Sepracor.
This article is freely available on publication, because the authors have cho-sen the immediate access option.
Individual reprints of this article are not available. Address correspondence to Michael E. Wechsler, MD, Pulmonary and Critical Care Medicine, Brigham and Women’s Hospital, Harvard Medical School, 15 Francis St, PBB Lobby, Boston, MA 02115 ([email protected]).
© 2009 Mayo Foundation for Medical Education and Research
Primary care physicians treat a considerable number of patients with asthma. These physicians are well-
positioned to recognize inadequately controlled asthma and to improve disease management for many patients with asthma. However, evidence continues to show that, for a substantial number of patients, asthma control is inadequate.1-4 In a study of US national administrative claims data, nearly three-fourths of patients with asthma (73%; 46,227/63,324) met the criteria for uncontrolled disease at least once during a 3-year period.3
A wide range of factors, physician-related and patient-related, can contribute to poor asthma control. One aspect of this problem, as revealed by data from patient surveys, is that many patients overestimate their level of disease control, often tolerating substantial asthma symptoms and having low expectations about the degree of control that is possible.5,6 Patients also frequently exhibit poor adherence to prescribed controller medications7; additional patient-related factors affecting asthma control include self-management abilities, smoking status, inhaler technique, ability to remember doses, access to prescriptions, and costs of medication.6
Physician practices can also contribute to inadequate asthma control. Physicians have a tendency to underestimate the prevalence of asthma symptoms and to overestimate the degree to which their patients’ asthma is controlled1,6;
therefore, they may not always prescribe adequate controller medication therapy.7 Physicians may also have an inadequate understanding of disease etiology or may not communicate well with patients, and these problems make it difficult to establish a pharmacotherapeutic regimen that the patient is willing and able to follow.5
In light of the complexities inherent in the long-term management of asthma, national and international guidelines have been developed over the years to assist clinicians in caring for their patients. The use of guideline-based treatment strategies has been shown to favorably affect asthma outcomes, but there has also been increasing recognition that previous guidelines were not adequately followed and did not lead to acceptable levels of asthma control.8 In 2007, the National Asthma Education and Prevention Program (NAEPP) issued updated guidelines for the diagnosis and management of asthma (the Expert Panel Report 3 [EPR3]),9 which, among other changes, shifted the focus to ongoing assessment of disease control with the goal of improving the management of asthma over time. The current review is intended to assist primary care physicians in improving their patients’ asthma control, in part through an improved understanding of the new guidelines, and to provide a specialist’s perspective on diagnosing asthma and prescribing appropriate therapy, monitoring disease control, and providing appropriate and timely referrals. As such, this review is based primarily on the NAEPP guidelines, the references therein, and the author’s clinical experience.
OVERVIEW OF THE UPDATED NAEPP GUIDELINES
The NAEPP, initiated by the National Heart, Lung, and Blood Institute in 1989 in response to the worsening asth-
For editorial
comment,
see page 673

708
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
ma epidemic, issued its first set of asthma management guidelines in 1991. A revised set of guidelines—the Expert Panel Report 2—was published in 1997 and was updated in 2002. These guidelines first introduced the stepwise approach to asthma therapy that is based on a 4-part classification scheme of disease severity (mild intermittent, mild persistent, moderate persistent, or severe persistent). Although this approach is useful, its limitations have been clearly recognized, particularly the need to more clearly address the fluctuating severity of asthma symptoms over time.8,10,11 Thus, the EPR3 guidelines, published in 2007, were based on the overall stepwise treatment model but incorporated some fundamental changes. A key modification in the EPR3 guidelines is the emphasis on distinguishing between asthma severity, which is intrinsic to the disease process, and a patient’s level of asthma control, which fluctuates over time. Classifying disease severity is the first step in initiating therapy for a patient who has not been taking long-term control medication. Once therapy is initiated, the emphasis shifts to the assessment of asthma control, which will guide decisions about maintaining or adjusting therapy and evaluating the patient’s responsiveness to various asthma medications.9 The new guidelines also added a distinction between the
domains of current impairment and future risk, which are to be noted by the physician during the assessment of both asthma severity and disease control, so that asthma’s effects on quality of life and functional capacity in the present and its risks for the future are considered separately.9
Regarding medication management, the most sub-stantive changes in the EPR3 guidelines are the separate recommendations for 3 age groups of patients (children aged birth to 4 years, children aged 5 to 11 years, or patients aged 12 years or older) and the expansion of treatment steps from 4 to 6 so that the action within each step can be simplified.9,11,12 In terms of specific medications, the important role of inhaled corticosteroids (ICSs) in asthma therapy continues to be supported. On the basis of new safety data for long-acting β-agonists (LABAs), guidelines recommend equal consideration for either increasing the ICS dose to a medium dose or adding a LABA to low-dose ICS therapy for patients aged 12 years or older whose asthma is inadequately controlled by low-dose ICS therapy. LABAs should not be used as monotherapy. Finally, the use of allergy immunotherapy has been included in steps 2 through 4 for patients aged 5 years or older, and omalizumab has been included for consideration in therapy steps 5 and 6 for patients aged 12 years or older.9
MAKING THE DIAGNOSIS
Correctly diagnosing asthma is the first step toward attain-ing disease control. In general, a diagnosis of asthma is established if episodic symptoms of airflow obstruction or airway hyperresponsiveness are present, airflow obstruction is at least partially reversible, and alternative diagnoses are excluded. The guidelines recommend the use of a detailed medical history, the results of a physical examination (focusing on the upper respiratory tract, chest, and skin), and the results of spirometry (for patients aged 5 years or older) in making the diagnosis. Any additional studies necessary for excluding alternative diagnoses or identifying other potential causes of symptoms should also be performed (eg, chest radiography, specific blood tests).9 However, primary care physicians may choose to refer patients to a specialist for spirometry or other testing. Table 1 lists some key indicators of a diagnosis of asthma, including wheezing; a history of recurrent cough, wheezing, difficulty in breathing, or chest tightness; and symptoms that occur or worsen in the presence of specific triggers.9 Particularly important factors that should be addressed as part of the medical history include the overall pattern of symptoms (eg, perennial, seasonal, or both; continual, episodic, or both; diurnal variations), precipitating factors (such as the presence of allergic triggers), and a family history of asthma, allergy, or other atopic disorders.9
TABLE 1. Key Indicators for Considering a Diagnosis of Asthmaa
Wheezing High-pitched whistling sounds when breathing out, especially in children. (Lack of wheezing and normal findings on chest examination do not exclude asthma.)History of any of the following Cough, worse particularly at night Recurrent wheeze Recurrent difficulty in breathing Recurrent chest tightnessSymptoms occur or worsen in the presence of the following Exercise Viral infection Animals with fur or hair House-dust mites (in mattresses, pillows, upholstered furniture, carpets) Mold Smoke (tobacco, wood) Pollen Changes in weather Strong emotional expression (laughing or crying hard) Airborne chemicals or dusts Menstrual cyclesSymptoms occur or worsen at night, awakening the patient
a Consider a diagnosis of asthma and performing spirometry if any of these indicators is present. These indicators are not diagnostic in themselves, but the presence of multiple key indicators increases the probability of a diagno sis of asthma. Spirometry is needed to establish a diagnosis of asth-ma. Eczema, hay fever, and a family history of asthma or atopic diseases are often associated with asthma, but they are not key indicators.
From Expert Panel Report 3: Guidelines for the Diagnosis and Manage-ment of Asthma.9

709
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
Although recurrent cough and wheezing are often due to asthma, other causes of airway obstruction should be considered in the initial diagnosis or if the patient does not respond to initial therapy. Table 2 lists the most common possibilities included in the differential diagnosis of asthma, according to the EPR3 guidelines. Vocal cord dysfunction—characterized by episodic dyspnea and wheezing caused by intermittent paradoxical vocal cord adduction during inspiration—often mimics asthma and can be difficult to diagnose. A diagnosis is best made with indirect or direct vocal cord visualization during an episode, and treatment generally consists of speech therapy and relaxation techniques. Several other conditions may coexist with asthma or complicate the diagnosis or management of asthma. Cough-variant asthma, in particular, is easily overlooked because chronic cough can be a sign of a wide variety of health problems. Conversely, chronic cough may also be the principal (or only) manifestation of asthma, especially among young children. The diagnosis of cough-variant asthma is confirmed by a positive response to asthma medication, and treatment should follow the usual stepwise approach to asthma management. Other common comorbid conditions that complicate the diagnosis of asthma are chronic sinusitis, gastroesophageal reflux disease, obstructive sleep apnea, and respiratory
tract infections. Because it is often accompanied by symptoms similar to those of asthma and by elevated IgE levels, allergic bronchopulmonary aspergillosis should also be excluded.9,13 Although rare, Churg-Strauss syndrome is another comorbid condition that should be considered in the assessment of patients with difficult-to-control asthma. It is a serious disorder characterized by eosinophilic inflammation of the respiratory tract and necrotizing vasculitis of small and medium vessels. Laboratory results demonstrate eosin-ophilia, and symptoms include asthma, rhinosinusitis, pul-monary infiltrates, peripheral neuropathy, and skin, heart, or gastrointestinal involvement.14
MANAGING ASTHMA
HOW ARE ASTHMA SEVERITY AND CONTROL ASSESSED AND MONITORED?Once the diagnosis of asthma has been established, the focus shifts to classifying asthma severity so that therapy can be initiated and to monitoring control over time so that therapy can be adjusted. According to the new guidelines, severity and control should be assessed separately, but both are classified on the basis of the domains of current impairment and future risk. Impairment is defined as “the frequency and intensity of symptoms and functional limitations the patient is experiencing currently or has recently experienced,” whereas risk is defined as “the likelihood of either asthma exacerbations, progressive decline in lung function (or, for children, lung growth), or risk of adverse effects from medication.” The new guidelines stress that the impairment domain and the risk domain may respond differently to treatment.9
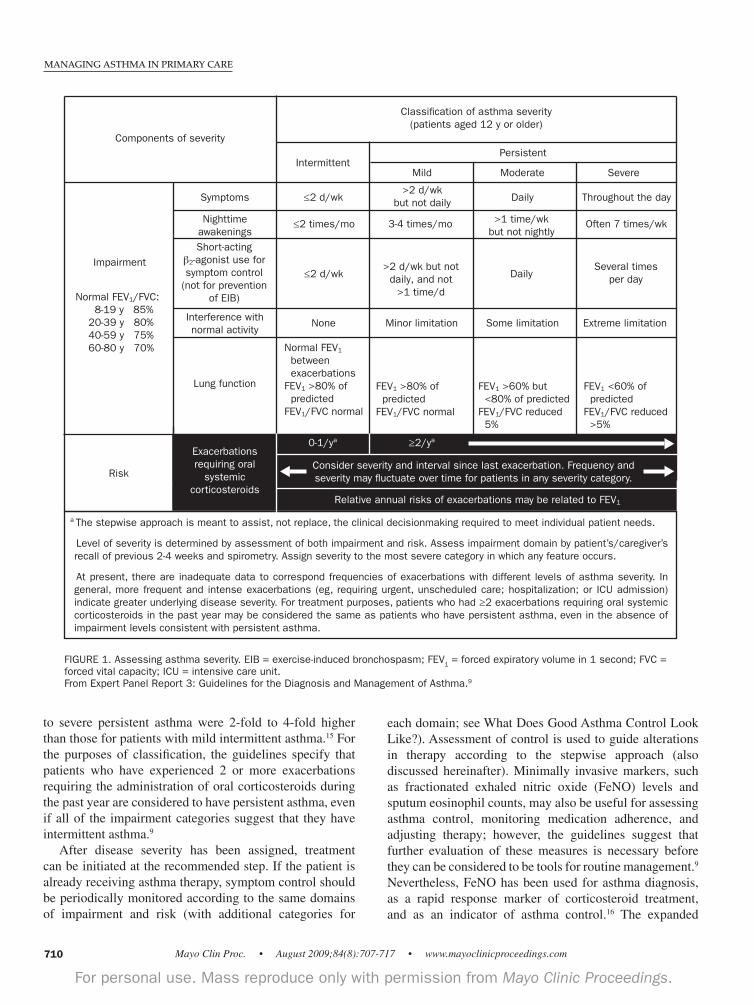
In assessing impairment, asthma severity should be evaluated using the categories outlined in Figure 1.9 Severity should be assigned according to the most severe category of impairment. Assessment of future risk, which is based on the frequency of exacerbations requiring the administration of oral systemic corticosteroids, is another important facet of asthma severity. The occurrence of exacerbations can vary widely (from rare to frequent) among patients and for each individual patient. Because patients at any level of disease severity, including intermittent asthma, can experience severe exacerbations, the current version of the guidelines has omitted the word from the former classification of asthma. Although the current guidelines state that evidence is insufficient to confirm an association between the frequency of exacerbations and the level of asthma severity, in general, the more frequent and the more intense the exacerbations, the greater the degree of underlying disease severity.9,15 One study found that the rates of hospitalizations, urgent care visits, and absenteeism for patients with moderate
TABLE 2. Differential Diagnostic Possibilities for Asthma
Infants and children Upper airway diseases Allergic rhinitis and sinusitis Obstructions involving large airways Foreign body in trachea or bronchus Vocal cord dysfunction Vascular rings or laryngeal webs Laryngotracheomalacia, tracheal stenosis, or bronchostenosis Enlarged lymph nodes or tumor Obstructions involving small airways Viral bronchiolitis or obliterative bronchiolitis Cystic fibrosis Bronchopulmonary dysplasia Heart disease Other causes Recurrent cough not due to asthma Aspiration due to dysfunction of the swallowing mechanism or to gastroesophageal refluxAdults Chronic obstructive pulmonary disease (eg, chronic bronchitis or emphysema) Congestive heart failure Pulmonary embolism Mechanical obstruction of the airways (benign and malignant tumors) Pulmonary infiltration with eosinophilia Cough resulting from administration of drugs (eg, angiotensin- converting enzyme inhibitors) Vocal cord dysfunction
From Expert Panel Report 3: Guidelines for the Diagnosis and Manage-ment of Asthma.9
710
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
to severe persistent asthma were 2-fold to 4-fold higher than those for patients with mild intermittent asthma.15 For the purposes of classification, the guidelines specify that patients who have experienced 2 or more exacerbations requiring the administration of oral corticosteroids during the past year are considered to have persistent asthma, even if all of the impairment categories suggest that they have intermittent asthma.9
After disease severity has been assigned, treatment can be initiated at the recommended step. If the patient is already receiving asthma therapy, symptom control should be periodically monitored according to the same domains of impairment and risk (with additional categories for
each domain; see What Does Good Asthma Control Look Like?). Assessment of control is used to guide alterations in therapy according to the stepwise approach (also discussed hereinafter). Minimally invasive markers, such as fractionated exhaled nitric oxide (FeNO) levels and sputum eosinophil counts, may also be useful for assessing asthma control, monitoring medication adherence, and adjusting therapy; however, the guidelines suggest that further evaluation of these measures is necessary before they can be considered to be tools for routine management.9 Nevertheless, FeNO has been used for asthma diagnosis, as a rapid response marker of corticosteroid treatment, and as an indicator of asthma control.16 The expanded
≥2/y0-1/y
Components of severity
Classification of asthma severity(patients aged 12 y or older)
PersistentIntermittent
Throughout the day
SevereModerateMild
Symptoms ≤2 d/wk>2 d/wk
but not daily Daily
Nighttime awakenings
≤2 times/mo 3-4 times/mo >1 time/wk but not nightly
Often 7 times/wk
Short-acting 2-agonist use for
symptom control (not for prevention
of EIB)
≤2 d/wk>2 d/wk but not
daily, and not >1 time/d
DailySeveral times
per day
Interference with normal activity
None Minor limitation Some limitation Extreme limitation
Lung function
Normal FEV1 between exacerbationsFEV1 >80% of predictedFEV1/FVC normal
Risk
FEV1 >80% of predictedFEV1/FVC normal
Impairment
FEV1 >60% but <80% of predictedFEV1/FVC reduced 5%
FEV1 <60% of predictedFEV1/FVC reduced >5%
Normal FEV1/FVC: 8-19 y 85% 20-39 y 80% 40-59 y 75% 60-80 y 70%
Exacerbations requiring oral
systemic corticosteroids
Consider severity and interval since last exacerbation. Frequency and severity may fluctuate over time for patients in any severity category.
Relative annual risks of exacerbations may be related to FEV1
≥2/ya0-1/ya
a The stepwise approach is meant to assist, not replace, the clinical decisionmaking required to meet individual patient needs.
Level of severity is determined by assessment of both impairment and risk. Assess impairment domain by patient’s/caregiver’s recall of previous 2-4 weeks and spirometry. Assign severity to the most severe category in which any feature occurs.
At present, there are inadequate data to correspond frequencies of exacerbations with different levels of asthma severity. In general, more frequent and intense exacerbations (eg, requiring urgent, unscheduled care; hospitalization; or ICU admission) indicate greater underlying disease severity. For treatment purposes, patients who had ≥2 exacerbations requiring oral systemic corticosteroids in the past year may be considered the same as patients who have persistent asthma, even in the absence of impairment levels consistent with persistent asthma.
FIGURE 1. Assessing asthma severity. EIB = exercise-induced bronchospasm; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; ICU = intensive care unit.From Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9

711
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
availability of portable FeNO monitors, combined with an improved ability to interpret the clinical meaning of the measurements, is likely to expand the role of minimally invasive markers in the future.
WHAT ARE THE OBSTACLES TO ACHIEVING GOOD ASTHMA CONTROL?Ongoing monitoring of symptom control is a key component of asthma management over time and helps ensure that treatment goals are met and necessary adjustments to therapy are made. However, one of the difficulties of asthma management is that both patients and physicians tend to underestimate the severity of symptoms or overestimate the patient’s level of disease control. Many patients may assume that a certain level of symptoms or some limitation of activity is an inevitable consequence of having asthma. In fact, 39% to 70% of respondents to the Asthma Insights and Reality (AIR) surveys reported that their asthma was well controlled or completely controlled even though they were experiencing moderate symptoms.2 Thus, patients whose asthma is poorly controlled may not always receive a prescription for adequate controller medication therapy or may not adhere to a daily controller medication regimen. Fewer than one-third of the respondents to the AIR surveys, including those with severe persistent asthma, reported regular use of preventive asthma medication; usage rates ranged from 26% in Western Europe to 9% in Japan.2 A review of several different patient surveys found that at least 40% of patients reported underusing their prescribed medications, in terms of either frequency or dosing, largely because of discomfort with long-term ICS therapy. In fact, when higher ICS doses were prescribed for regaining asthma control, at least 50% of patients reported that they refused to fully adhere to the higher dosage regimen because of concerns about adverse effects.5 In other circumstances, patients do not even use their inhalers with proper technique, further preventing them from gaining the benefit of these therapies or from achieving control. Other obstacles to achieving good asthma control include the presence of exacerbating factors, such as ongoing occupational or allergen exposures, which should be identified and eliminated when possible. Occupational history should be considered for adults with uncontrolled asthma, especially if symptoms improve on weekends and holidays. Perhaps the environmental factor that contributes most to the development, persistence, and severity of asthma is viral respiratory infection. Although influenza vaccination is recommended for patients with asthma because of their risk of influenza-associated complications, vaccination should not be expected to reduce the frequency or severity of exacerbations during influenza season.9 Asthma can also be exacerbated by certain drugs, such as nonsteroidal anti-inflammatory drugs and β-blockers.
Aspirin-sensitive asthma is frequently associated with a genetic sequence variation and is relatively common in Eastern Europe and Japan. Although the mechanism involved in β-blocker–induced asthma is not completely understood, antagonism of the β
2-adrenoreceptor, even with
β1-selective medications, should be avoided for patients
with asthma.17 Asthma may also be difficult to control in the presence of untreated gastroesophageal reflux disease or other comorbid conditions.
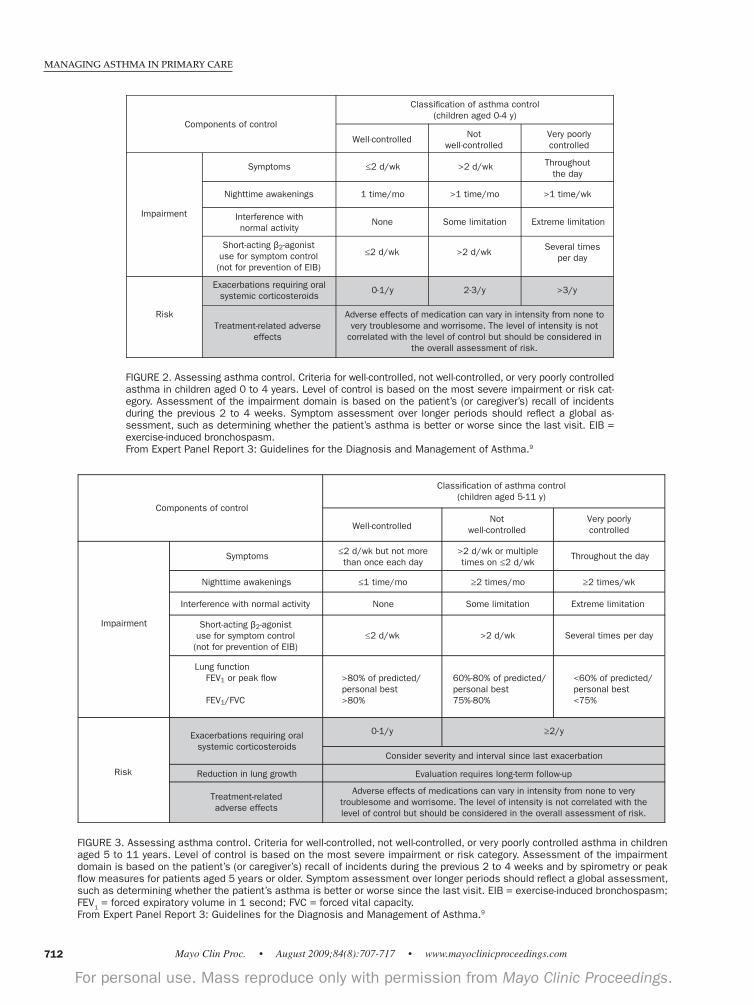
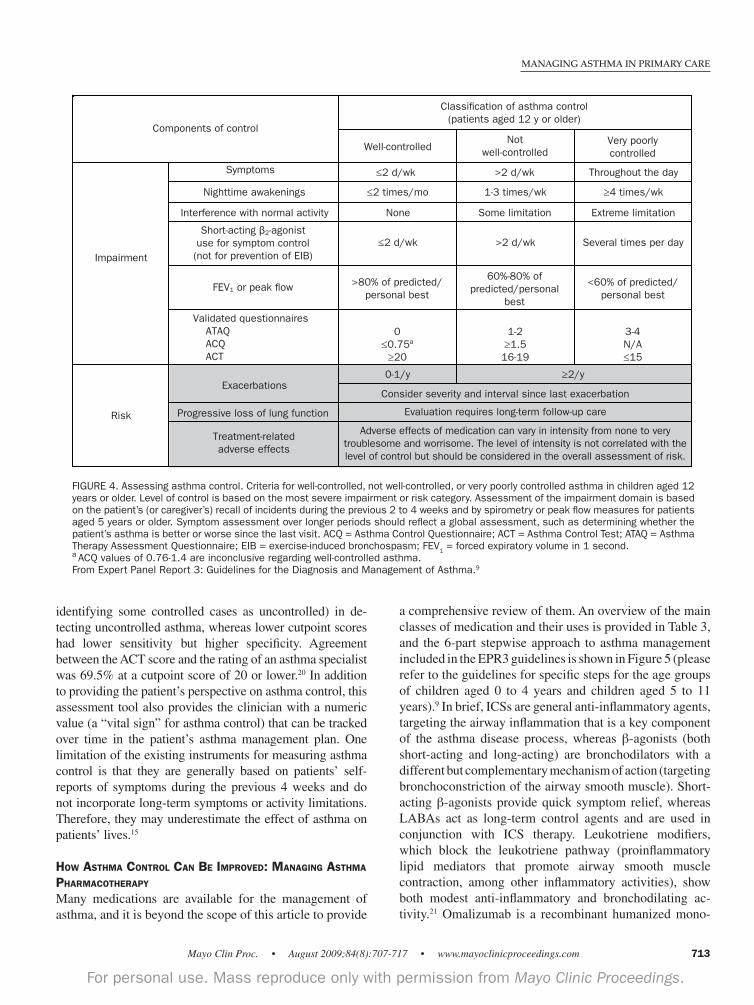
WHAT DOES GOOD ASTHMA CONTROL LOOK LIKE?Both patients and their physicians should understand exactly what constitutes good asthma control. Physicians must be able to recognize good control, or the lack thereof, so that they can adjust the management plan. Patients should be educated so that they do not accept a certain level of ongoing symptoms, short-acting inhaler use, and reduced activity as “normal” for someone with asthma. Figures 2, 3, and 4 detail the impairment and risk criteria that are used in the EPR3 guidelines to classify asthma as well-controlled, not well-controlled, or very poorly controlled for patients in 3 age groups. A patient aged 12 years or older who has well-controlled asthma should have symptoms no more than twice per week, should experience nighttime awakenings no more than twice per month, should use a short-acting β-agonist no more than twice per week, should experience no interference with normal activity, should have a forced expiratory volume in 1 second or peak flow levels higher than 80% of the predicted or personal best, and should have had no more than 1 exacerbation during the past year.9 If any aspect of the patient’s asthma control does not meet these criteria, the patient does not have good asthma control, and the clinician should consider changing the patient’s asthma management plan. In addition to clinician assessment, several validated self-assessment tools can be used during follow-up visits to quickly capture the overall level of asthma control from the patient’s perspective. These tools are based on current impairment and do not address the risk domain of control. The most commonly used tools are the Asthma Control Questionnaire,18 the Asthma Therapy Assessment Questionnaire,19 and the Asthma Control Test (ACT).20 The ACT is an easy-to-use questionnaire consisting of 5 questions, each scored by the patient on a scale from 1 to 5, regarding activity levels, frequency of daytime or nighttime symptoms, rescue inhaler use, and the patient’s perception of asthma control during the past 4 weeks. The result is a total numeric score ranging from 5 to 25; a cutpoint score of 20 or higher generally indicates well-controlled asthma (in conjunction with the physician’s clinical assessment). A validation study of the ACT found that higher cutpoint scores had higher sensitivity but lower specificity (falsely
712
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
FIGURE 3. Assessing asthma control. Criteria for well-controlled, not well-controlled, or very poorly controlled asthma in children aged 5 to 11 years. Level of control is based on the most severe impairment or risk category. Assessment of the impairment domain is based on the patient’s (or caregiver’s) recall of incidents during the previous 2 to 4 weeks and by spirometry or peak flow measures for patients aged 5 years or older. Symptom assessment over longer periods should reflect a global assessment, such as determining whether the patient’s asthma is better or worse since the last visit. EIB = exercise-induced bronchospasm; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity.From Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9
FIGURE 2. Assessing asthma control. Criteria for well-controlled, not well-controlled, or very poorly controlled asthma in children aged 0 to 4 years. Level of control is based on the most severe impairment or risk cat-egory. Assessment of the impairment domain is based on the patient’s (or caregiver’s) recall of incidents during the previous 2 to 4 weeks. Symptom assessment over longer periods should reflect a global as-sessment, such as determining whether the patient’s asthma is better or worse since the last visit. EIB = exercise-induced bronchospasm.From Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9
713
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
identifying some controlled cases as uncontrolled) in de-tecting uncontrolled asthma, whereas lower cutpoint scores had lower sensitivity but higher specificity. Agreement between the ACT score and the rating of an asthma specialist was 69.5% at a cutpoint score of 20 or lower.20 In addition to providing the patient’s perspective on asthma control, this assessment tool also provides the clinician with a numeric value (a “vital sign” for asthma control) that can be tracked over time in the patient’s asthma management plan. One limitation of the existing instruments for measuring asthma control is that they are generally based on patients’ self-reports of symptoms during the previous 4 weeks and do not incorporate long-term symptoms or activity limitations. Therefore, they may underestimate the effect of asthma on patients’ lives.15
HOW ASTHMA CONTROL CAN BE IMPROVED: MANAGING ASTHMA PHARMACOTHERAPY
Many medications are available for the management of asthma, and it is beyond the scope of this article to provide
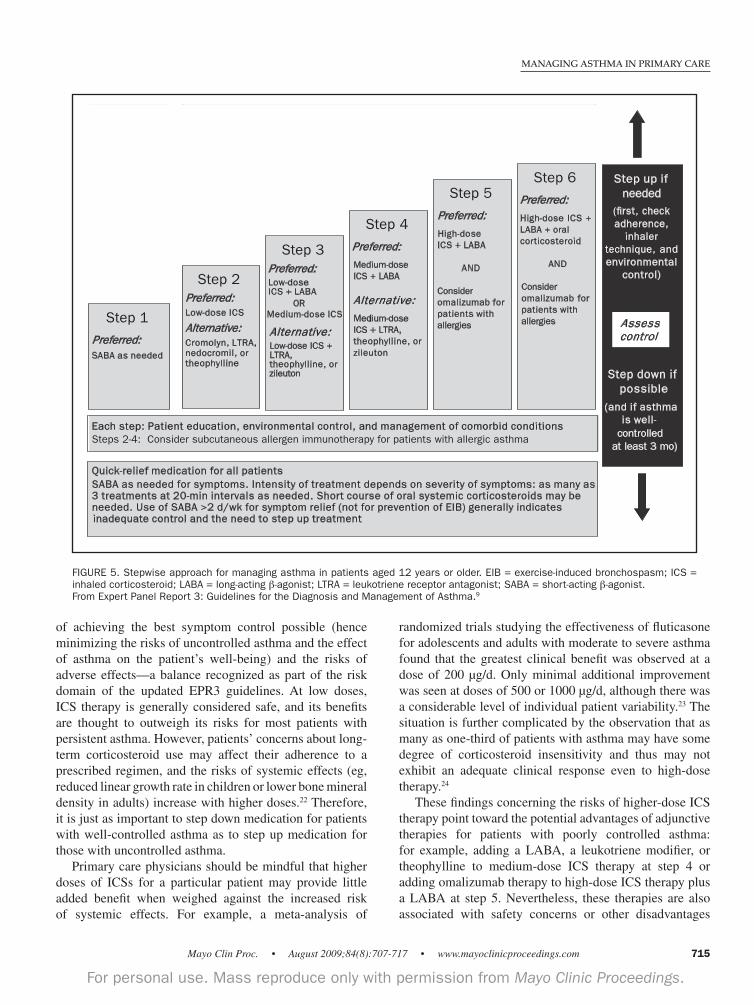
a comprehensive review of them. An overview of the main classes of medication and their uses is provided in Table 3, and the 6-part stepwise approach to asthma management included in the EPR3 guidelines is shown in Figure 5 (please refer to the guidelines for specific steps for the age groups of children aged 0 to 4 years and children aged 5 to 11 years).9 In brief, ICSs are general anti-inflammatory agents, targeting the airway inflammation that is a key component of the asthma disease process, whereas β-agonists (both short-acting and long-acting) are bronchodilators with a different but complementary mechanism of action (targeting bronchoconstriction of the airway smooth muscle). Short-acting β-agonists provide quick symptom relief, whereas LABAs act as long-term control agents and are used in conjunction with ICS therapy. Leukotriene modifiers, which block the leukotriene pathway (proinflammatory lipid mediators that promote airway smooth muscle contraction, among other inflammatory activities), show both modest anti-inflammatory and bronchodilating ac-tivity.21 Omalizumab is a recombinant humanized mono-
FIGURE 4. Assessing asthma control. Criteria for well-controlled, not well-controlled, or very poorly controlled asthma in children aged 12 years or older. Level of control is based on the most severe impairment or risk category. Assessment of the impairment domain is based on the patient’s (or caregiver’s) recall of incidents during the previous 2 to 4 weeks and by spirometry or peak flow measures for patients aged 5 years or older. Symptom assessment over longer periods should reflect a global assessment, such as determining whether the patient’s asthma is better or worse since the last visit. ACQ = Asthma Control Questionnaire; ACT = Asthma Control Test; ATAQ = Asthma Therapy Assessment Questionnaire; EIB = exercise-induced bronchospasm; FEV1 = forced expiratory volume in 1 second. a ACQ values of 0.76-1.4 are inconclusive regarding well-controlled asthma. From Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9

714
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
clonal anti-IgE antibody that specifically binds to free IgE, the immunoglobulin molecule that triggers the allergic cascade by binding to effector cells such as mast cells and basophils. Thus, for patients with allergic asthma, omalizumab blocks the subsequent downstream cascade of events triggered by IgE, including inflammatory effects in the airways.21
For patients with persistent asthma, regardless of age group, daily anti-inflammatory treatment with ICSs is still the cornerstone of therapy. As already discussed, one of the key changes in EPR3 from previous guidelines is the recognition of potential safety concerns associated with LABA therapy; therefore, at step 3 (for patients aged 5 years or older), patients whose asthma was not adequately controlled with low-dose ICSs should be stepped up to either medium-dose ICS therapy or low-dose ICS therapy plus a LABA. Most importantly, LABAs are to be used only in combination with ICS therapy; the Food and Drug Administration has issued a black-box warning against
the use of LABAs as monotherapy for long-term control of asthma.9 An additional change in the EPR3 guidelines is the addition of anti-IgE therapy with omalizumab at steps 5 and 6 (patients who are being treated with a high-dose ICS plus a LABA) as an option for patients aged 12 years or older who have IgE-mediated allergic asthma (patients with a clinical history of allergies and evidence of elevated IgE levels in conjunction with positive results from a skin test or a radioallergosorbent test [RAST]). Omalizumab is indicated for patients aged 12 years or older with moderate to severe persistent asthma whose symptoms are inadequately controlled with ICSs and who have exhibited a positive skin test reaction or in vitro reactivity to a perennial aeroallergen (via RAST). Although the cost of this biologic agent is higher than that of other asthma therapies, it has been shown to reduce the incidence of asthma exacerbations, even among patients with more severe asthma. Regardless of the therapy step, long-term management of asthma always involves a balance between the benefits
TABLE 3. Overview of Classes of Asthma Medications
Medication class Examples Mechanism Mode of administration
Long-term controller medications ICSs Budesonide Anti-inflammatory Inhaled once or twice daily Beclomethasone Ciclesonide Flunisolide Fluticasone Mometasone Triamcinolone LABAs Salmeterol Bronchodilator Inhaled twice daily Formoterol Combination Salmeterol/fluticasone Combination anti-inflammatory/ Inhaled twice daily LABA/ICS Formoterol/budesonide bronchodilator Inhaled twice daily Leukotriene modifiers Montelukast Anti-inflammatory and Oral (once daily for montelukast, Zileuton bronchodilatory effects twice daily for zileuton)
Immunomodulators Anti-IgE Omalizumab Immunomodulatory/ SC injection once every 2 anti-inflammatory or 4 weeks Mast cell stabilizers Cromolyn/nedocromil Anti-inflammatory (stabilizes Inhaled 4 times daily mast cells and interferes with chloride channel function) Methylxanthines Theophylline Bronchodilators; may have Oral (liquid, sustained-release mild anti-inflammatory effects tablets, and capsules)
Quick-relief agents SABAs Albuterol Bronchodilator Inhaled every 4-6 h as needed Levalbuterol Pirbuterol Anticholinergics Ipratropium bromide Bronchodilator (inhibits Inhaled every 6 h during moderate muscarinic cholinergic or severe asthma exacerbations receptors), reduces intrinsic vagal tone of the airways Oral corticosteroids Methylprednisolone Anti-inflammatory Oral (often given in short-course Prednisolone bursts during exacerbations) Prednisone
ICS = inhaled corticosteroid; LABA = long-acting β-agonist; SABA = short-acting β-agonist; SC = subcutaneous.Data from Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9
715
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
of achieving the best symptom control possible (hence minimizing the risks of uncontrolled asthma and the effect of asthma on the patient’s well-being) and the risks of adverse effects—a balance recognized as part of the risk domain of the updated EPR3 guidelines. At low doses, ICS therapy is generally considered safe, and its benefits are thought to outweigh its risks for most patients with persistent asthma. However, patients’ concerns about long-term corticosteroid use may affect their adherence to a prescribed regimen, and the risks of systemic effects (eg, reduced linear growth rate in children or lower bone mineral density in adults) increase with higher doses.22 Therefore, it is just as important to step down medication for patients with well-controlled asthma as to step up medication for those with uncontrolled asthma. Primary care physicians should be mindful that higher doses of ICSs for a particular patient may provide little added benefit when weighed against the increased risk of systemic effects. For example, a meta-analysis of
randomized trials studying the effectiveness of fluticasone for adolescents and adults with moderate to severe asthma found that the greatest clinical benefit was observed at a dose of 200 μg/d. Only minimal additional improvement was seen at doses of 500 or 1000 μg/d, although there was a considerable level of individual patient variability.23 The situation is further complicated by the observation that as many as one-third of patients with asthma may have some degree of corticosteroid insensitivity and thus may not exhibit an adequate clinical response even to high-dose therapy.24
These findings concerning the risks of higher-dose ICS therapy point toward the potential advantages of adjunctive therapies for patients with poorly controlled asthma: for example, adding a LABA, a leukotriene modifier, or theophylline to medium-dose ICS therapy at step 4 or adding omalizumab therapy to high-dose ICS therapy plus a LABA at step 5. Nevertheless, these therapies are also associated with safety concerns or other disadvantages
FIGURE 5. Stepwise approach for managing asthma in patients aged 12 years or older. EIB = exercise-induced bronchospasm; ICS = inhaled corticosteroid; LABA = long-acting β-agonist; LTRA = leukotriene receptor antagonist; SABA = short-acting β-agonist. From Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma.9
Step 1
Preferred:SABA as needed
Step 2Preferred:Low-dose ICS
Alternative:Cromolyn, LTRA,nedocromil, or theophylline
Step 3Preferred:Low-doseICS + LABA
ORMedium-dose ICS
Alternative:Low-dose ICS +LTRA,theophylline, or zileuton
Step 5
Preferred:
High-dose ICS + LABA
AND
Consider omalizumab forpatients with allergies
Step 6
Preferred:
High-dose ICS +LABA + oral corticosteroid
AND
Consider omalizumab forpatients with allergies
Step up ifneeded
Step down if possible
(and if asthmais well-
controlledat least 3 mo)
Step 4
Preferred:
Medium-dose ICS + LABA
Alternative:
Mediium-dose ICS + LTRA, theophylline, orzileuton
Assesscontrol
Quick-relief medication for all patients
SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: as many as
3 treatments at 20-min intervals as needed. Short course of oral systemic corticosteroids may be
needed. Use of SABA >2 d/wk for symptom relief (not for prevention of EIB) generally indicates
inadequate control and the need to step up treatment
Each step: Patient education, environmental control, and management of comorbid conditionsSteps 2-4: Consider subcutaneous allergen immunotherapy for patients with allergic asthma
(first, check adherence,
inhaler technique, and environmental
control)

716
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
that must be weighed against the clinical benefits. Liver function must be monitored when patients are taking zileuton, and the serum concentration of theophylline must also be monitored.9 The Food and Drug Administration has issued a black-box warning for omalizumab because of a small risk of anaphylaxis (corresponding to 0.09% in postmarketing surveillance studies).25 For this reason, clinicians who administer omalizumab must be prepared and equipped to treat anaphylaxis, to observe patients for an appropriate period of time after each injection, and to educate patients about the risks of anaphylaxis and the appropriate treatment if it occurs.26 Additionally, the EPR3 guidelines list malignant neoplasm as a potential adverse effect of omalizumab because the pivotal clinical trials found that the incidence of such neoplasms was higher among patients receiving omalizumab than among those receiving placebo. Subsequently, the increased occurrence of malignancies was deemed not to be due to omalizumab, and an expert panel of oncologists concluded that only 3 of the reported 25 neoplasms were even remotely related to the study drug.27,28 As the only approved biologic therapy for asthma, omalizumab is more expensive than other controller medications and is administered by subcutaneous injection in the physician’s office. A recent study showed that the adherence and persistence rates associated with omalizumab were substantially higher than those associated with the combination of an ICS and a LABA, perhaps because the requirement for subcutaneous injection by a health care professional translates into direct observation of adherence to therapy.29
For patients with allergic asthma, as indicated by positive results from a skin test or in vitro RAST testing for individual aeroallergens, specific allergen immunotherapy may be an appropriate adjunctive therapy when a clear relationship exists between asthma symptoms and allergen exposure. According to the EPR3 guidelines, the evidence for improved asthma control with immunotherapy is strongest when patients are affected by single allergens, especially house dust mites, cat dander, or pollen.9 A patient with persistent asthma that may be associated with allergy should probably be referred to an allergist for skin-prick testing and consideration of immunotherapy, omalizumab therapy, or both.
WHEN SHOULD THE PRIMARY CARE PHYSICIAN REFER A PATIENT TO AN ASTHMA SPECIALIST?A referral to a specialist should be considered for any patient whose asthma is difficult to control, including patients who do not achieve good control with a combination of an ICS and a LABA and those who may be considered for therapy with omalizumab. More specifically, asthma management guidelines recommend that primary care physicians consider
referral for patients who have experienced more than 2 oral corticosteroid bursts per year or a recent exacerbation requiring hospitalization, those who required therapy at step 4 or higher to achieve adequate asthma control, or those for whom immunotherapy or therapy with omalizumab is being considered.9
CONCLUSION
Asthma is a chronic condition that often remains uncon-trolled for reasons that may be related to the disease process itself, the management decisions of clinicians, the patient’s perceptions of disease control or self-management behaviors, the cost of medications, or a combination of all of these factors. Whatever the reasons for poor control, efforts to improve it can achieve a notable positive effect on the lives of patients with asthma. The most recently updated treatment guidelines from the NAEPP (EPR3) were designed to help clinicians, including primary care physicians, manage asthma more effectively, with an increased focus on achieving and maintaining good asthma control over time. Proper diagnosis and regular assessment of asthma control are key components of an effective management strategy, but improving control depends on recognition by both the patient and the physician as to what constitutes good asthma control. To this end, patients with asthma should be educated not to accept a certain level of symptoms or activity limitations as an inevitable consequence of asthma. Both the levels of current impairment and the future risks (of asthma exacerbations or adverse medication effects) should be used to inform decisions about appropriate levels of asthma therapy, and physicians should be aware of the new medication recommendations included in the latest NAEPP guidelines. The revised guidelines emphasize the importance of assessing, achieving, and continually monitoring asthma control by focusing on the key domains of impairment and risk. The implementation of these recommendations by primary care physicians and other health professionals who are at the forefront of care is crucial to minimizing the incidence of uncontrolled asthma at a time when our knowledge of the disease and the availability of effective medications have fostered an opportunity for substantial improvement.
REFERENCES
1. Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. . 2008; 31(2):320-325. Epub 2007 Oct 24.

717
MANAGING ASTHMA IN PRIMARY CARE
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedingsa .
2. Rabe KF, Adachi M, Lai CK, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys.
. 2004;114(1):40-47. 3. Stempel DA, McLaughin TP, Stanford RH, Fuhlbrigge AL. Patterns of asthma control: a 3-year analysis of patient claims. . 2005; 115(5):935-939. 4. Sapra SJ, Broder MS and Chang E. Alignment with the revised NHLBI 2007 asthma guidelines, Expert Panel Report 3 (EPR 3) in a large payer data-base. . 2009;123(2)(suppl 1):S117. 5. Holgate ST, Price D, Valovirta E. Asthma out of control? A structured review of recent patient surveys. . 2006;6(suppl 1):S2. 6. Horne R, Price D, Cleland J, et al. Can asthma control be improved by understanding the patient's perspective? . 2007;7:8. 7. Barnes PJ. The size of the problem of managing asthma. . 2004; 98(suppl 2):S4-S8. 8. Ohar JA. Asthma treatment guidelines: current recommendations, future goals. . 2005;2(6):23-27. 9. US Department of Health and Human Services, National Institutes of Health, National Heart Lung and Blood Institute, National Asthma Educa-tion and Prevention Program. Expert Panel Report 3: Guidelines for the Di-agnosis and Management of Asthma. NIH Publication No. 07-40511-440. Bethesda, MD: US Dept of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute; 2007. http://www.nhlbi.nih .gov/guidelines/asthma/asthgdln.pdf. Accessed May 20, 2009. 10. Long AA. Addressing unmet needs in asthma care. . 2005;2(6): 16-22. 11. Schatz M. Pharmacotherapy of asthma: what do the 2007 NAEPP guide-lines say? . 2007;28(6):628-633. 12. Kelly HW. Rationale for the major changes in the pharmacotherapy sec-tion of the National Asthma Education and Prevention Program guidelines.
. 2007;120(5):989-994. 13. Berlow BA. Eight key questions to ask when your patient with asthma doesn't get better. . 1997;55(1):183-189, 192-194. 14. Lilly CM, Churg A, Lazarovich M, et al. Asthma therapies and Churg-Strauss syndrome. . 2002;109(1):S1-S19. 15. Fuhlbrigge AL, Adams RJ, Guilbert TW, et al. The burden of asthma in the United States: level and distribution are dependent on interpretation of the national asthma education and prevention program guidelines.
. 2002;166(8):1044-1049.
16. Kharitonov SA, Barnes PJ. Exhaled markers of pulmonary disease. . 2001;163(7):1693-1722.
17. Barnes PJ, Woolcock AJ. Difficult asthma. . 1998;12(5): 1209-1218. 18. Juniper EF, O'Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. . 1999;14(4):902-907. 19. Vollmer WM, Markson LE, O'Connor E, et al. Association of asthma control with health care utilization and quality of life. . 1999; 160(5, pt 1):1647-1652. 20. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. . 2004; 113(1):59-65. 21. Hanania NA. Targeting airway inflammation in asthma: current and fu-ture therapies. . 2008;133(4):989-998. 22. Irwin RS, Richardson ND. Side effects with inhaled corticosteroids: the physician's perception. . 2006;130(1)(suppl):41S-53S. 23. Masoli M, Weatherall M, Holt S, Beasley R. Clinical dose-response re-lationship of fluticasone propionate in adults with asthma. Thorax. 2004;59(1): 16-20. 24. Mjaanes CM, Whelan GJ, Szefler SJ. Corticosteroid therapy in asthma: predictors of responsiveness. . 2006;27(1):119-132, vii. 25. Cox L, Platts-Mills TA, Finegold I, Schwartz LB, Simons FE, Wallace DV. American Academy of Allergy, Asthma & Immunology/American College of Allergy, Asthma and Immunology Joint Task Force Report on omalizum-ab-associated anaphylaxis. . 2007;120(6):1373-1377. Epub 2007 Nov 9. 26. Prenner BM. Asthma 2008: targeting immunoglobulin E to achieve dis-ease control. . 2008;45(6):429-436. 27. Kuhn R. Immunoglobulin E blockade in the treatment of asthma. Phar
. 2007;27(10):1412-1424. 28. Corren J, Casale TB, Lanier B, Buhl R, Holgate S, Jimenez P. Safety and tolerability of omalizumab. . 2009;39(6):788-797. Epub 2009 Mar 17. DOI10.1111/j.1365-2222.2009.03214.x. 29. Broder M, Chang E, Ory C, Kamath T, Sapra S. Adherence and per-sistence with omalizumab and fluticasone/salmeterol within a managed care population. [published online ahead of print January 16, 2009].
. 2009 Mar-Apr; 30(2):148-157. Epub2009 Jan 16. DOI. 10.2500/aap.2009.30.3190