managing bone metastases in crpc: click to edit master ... · pdf filemanaging bone metastases...
TRANSCRIPT

Click to edit Master title style
This program has been accredited by the CUA as a Group Learning Activity (Section 1) as defined by the
Maintenance of Certification Program of the Royal College of Physicians and Surgeons of Canada. Completion of this program enables participants to
claim a maximum of two (2) Section 1 credits
Managing Bone Metastases in CRPC: From Bone-targeted Therapies to Radiopharmaceuticals: Update 2016

The scientific content of this
program was developed by the
Canadian Urological Association

Disclosure of Commercial Support
• This program has received financial support from Bayer Inc. and Amgen Inc. in the form of an educational grant.
• This program has received in-kind support from Bayer Inc. and Amgen Inc. in the form of logistical support.

Editorial Committee
• Fred Saad, MD, FRCSC (Program Lead) Professor and Chief, Urology Director of G-U Oncology Centre Hospitalier l’Université de Montréal Université de Montréal Endowed Chair in Prostate Cancer Research Montreal Cancer Institute Montreal, Quebec
• Robert J. Hamilton, MD, MPH, FRCSC
Urologist Division of Urology University Health Network – Princess Margaret Hospital Toronto, Ontario
• Alan So, MD, FRCSC Associate Professor Department of Urologic Sciences University of British Columbia Research Scientist Prostate Centre Vancouver General Hospital Vancouver, British Columbia
• Shawn Malone, MD, FRCSC Associate Professor University of Ottawa Radiation Oncologist The Ottawa Hospital Ottawa, Ontario

All Faculty have adhered to the:
• CMA Code of Ethics (Update 2004)
• CMA Guidelines for Physician Interactions with Industry (2007)
• Innovative Medicines Canada Code of Ethical Practices (2016)

Disclosure of Commercial Support
• Potential for conflict(s) of interest:
• Insert speakers name has received funding from Bayer.
• Insert speakers name has received funding from Amgen.
• Bayer benefits from the sale of a product that will be discussed in this program: Radium-223 (Xofigo)
• Amgen benefits from the sale of a product that will be discussed in this program: denosumab (Xgeva)

Faculty/Presenter Disclosures Company/ Organization
Details
I am a member of an Advisory Board or equivalent with a commercial organization.
I am a member of a Speakers bureau.
I have received payment from a commercial organization (including gifts or other consideration or ‘in kind’ compensation).

Faculty/Presenter Disclosures Company/ Organization
Details
I have received a grant(s) or an honorarium from a commercial organization.
I hold a patent for a product referred to in the CME/CPD program or that is marketed by a commercial organization.
I hold investments in a pharmaceutical organization, medical devices company or communications firm.
I am currently participating in or have participated in a clinical trial within the past two years.

The CUA is committed to providing high-quality CPD programs that are fair and balanced. If you have perceived any bias in this presentation or
have any feedback, please contact:
Tal Erdman Coordinator, CPD Programs and Accreditation,
Office of Education 185 Dorval, #401, Dorval, QC - H9S 5J9
T: (514) 395-0376 ext. 43 - F: (514) 395-1664 [email protected]

Learning Objectives
By participating in this educational session, health care providers can expect to:
• Discuss the rationale for the use of radiopharmaceuticals in the management of castrate-resistant prostate cancer (CRPC)
• Review the evidence for the use of radium-223 as monotherapy and in combination for the treatment of men with metastatic CRPC (mCRPC)
• Discuss practical considerations for the use of radium-223 in clinical practice

Rationale for the Use of Bone-targeted Therapy/Radiopharmaceuticals
• > 90% of patients with advanced prostate cancer have bone metastases1
– Negative impact on survival2-4
– Associated with bone pain and the need for opioids5,6
• Bone metastases can lead to a variety of SREs: Fracture, radiation to bone, spinal cord compression, surgery to bone
– Associated with significant morbidity and lower QOL7
1. Tannock IF, et al. N Engl J Med 2004;351:1502-12; 2. DePuy et al. Support Care Cancer 2007;15:869-76;
3. Norgaard et al. J Urol 2010;184:162-7; 4. Oefelein MG, et al. J Urol 2002;168:1005-7;
5. Goh P, et al. Curr Onc 2007;14:9-12; 6. Inoue T, et al. Urology 73:1104–9, 2009; 7. Weinfurt KP, et al. Ann Onc 2005;16:579-84
QOL = Quality of life
SRE = Skeletal-related event

Bone Metastases Associated with SREs in CRPC*†
Saad F, et al. J Natl Cancer Inst 2002;94:1458-68
Saad F, et al. J Natl Cancer Inst 2004;96:879-82
Saad F. Personal communication. 2008
*Placebo patients from the pivotal zoledronic acid trial. Patients may have
experienced more than one SRE. †Note for each group a number of patients who
had SREs were asymptomatic
33%
26%
8%
4%
0
10
20
30
40
50
Radiation to
bone
Pathologic
fracture
Spinal cord
compression
Surgery
to bone
Pa
tie
nts
(%
)
24 Months

SREs Associated with Decreased Survival
• Among patients with ≥ 1 SRE, survival at 360 days was worse in those with multiple SREs (22.4%) vs. those with 1 SRE (29.8%) (p < 0.01)
De Puy V, et al. Support Care Cancer 2007;15:869-76
0
1
Pro
bab
ility
Survival (days)
No SREs ≥ 1 SREs 0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
90 180 270 360
Survival at 360 days
P HR
Patients with no SREs 49.7% 0.02 1.30
Patients with ≥ 1 SRE 28.2%

Burden of Metastatic Bone Disease: Retrospective Cohort Study (Quebec)
• Cohort study of RAMQ database: Men with PCa diagnosis and ≥ 1 health care claim
• 626 MBD patients and 1,671 controls (no MBD)
• Adjusted mean all-cause healthcare costs were $11,820 higher in MBD patients vs. controls
• MBD-related costs were $3,091 higher in MBD patients vs. controls
– Most common SRE = radiotherapy (received by 85% of MBD patients)
Perrault L, et al. Can Urol Assoc J 2015;9:307-14
MBD = Metastatic bone disease
RAMQ = Régie de l’Assurance Maladie du Québec

SSEs vs. SREs
Symptomatic skeletal events (SSEs)
Skeletal-related events (SREs)
Radiation to bone Radiation to bone
Symptomatic pathologic fracture Pathologic fracture
Surgery to bone Surgery to bone
Symptomatic spinal cord compression
Spinal cord compression

Burden of SSEs in CRPC with Bone Metastases: Real-World Canadian Data
• Retrospective chart review of 393 patients at CHUM, PMCC, VGH
• Median survival from onset of MBD = 23.9 months
• 833 SSEs in 275 patients
• Mean of 2.12 SSEs per patient
• 70% of MBD patients had ≥ 1 documented SSE
• Mean MBD-related HRU costs:
– ≥ 1 SSE: $22,191 (observed) to $34,670 (adjusted)
– 0 SSEs: $9,550
Saad F, et al. AUA 2016 (Abstr 16-2136)
CHUM = Centre Hospitalier de l'Université de Montréal;
HRU = Health care resource use; PMCC = Princess Margaret Cancer Centre;
VGH = Vancouver General Hospital

BTT Use Varies Among Canadian Centres
• Centre Hospitalier de l'Université de Montréal (CHUM) had fewer SSEs, longer median time to first SSE and smaller proportion of patients received palliative radiation vs. Princess Margaret Cancer Centre (PMCC) or Vancouver General Hospital (VGH)
• Similar proportions of patients at CHUM (64%) and PMCC (60%) received BTTs: – ZA given predominantly on monthly schedule at CHUM (77%) and
every 3 mos at PMCC (70%)
• Few patients received a BTT at VGH (24%)
• Standardization of BTT practices needed
Saad F, et al. AUA 2016 (Abstr MP50-17) BTT = Bone-targeted therapy

Time to SSE in Three Canadian Sites
Saad F, et al. AUA 2016 (Abstr MP50-17)
1.0
0.8
0.6
0.4
0.2
0.0 0 50 100
Time to SSE (months)
Even
t P
rob
abili
ty
150 200
Median time to SSE, months (95% CI)
25.0 (18.5, 32.6) 14.6 (9.7, 16.8) 17.3 (14.8, 24.0)
CHUM (n = 130 PMCC (n = 154) VGH ( n = 109)

Multiple SSEs in Three Canadian Sites
Saad F, et al. AUA 2016 (Abstr MP50-17)
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Nu
mb
er
of
Pati
ents
Number of SSEs
CHUM (n = 130) PMCC (n = 154) VGH (n = 109)

Bone-targeted Agents
• Inhibit the activity of osteoclasts involved in osteolysis and bone resorption at bone metastatic sites:
– Bisphosphonates (ie, zoledronic acid)1
– RANKL inhibitors (eg, denosumab)
• Monoclonal antibody that binds to and inhibits the activity of RANKL2
1. Saad F, et al. J Natl Cancer Inst 2004;96:879-82
2. Fizazi K, et al. Lancet 2011;377:813-22 RANKL = Receptor activator of nuclear factor-kappa B ligand

Mode of Action of Denosumab and Bisphosphonates
Adapted from Fornier MN. J Clin Oncol 2010;28:5127-31
BMP = Bone morphogenetic proteins; FGFs = Fibroblast growth factors; IGFs = Insulin-like growth factors;
IL = Interleukin; PDGF = Platelet-derived growth factor; PGE2 = Prostaglandin E2; PTHrP = Parathyroid hormone-related
protein; TGF-b = Transforming growth factor-beta; TNF = Tumour necrosis factor;
M-CSF = Macrophage colony-stimulating factor; RANK = Receptor activator of Nuclear Factor κ B;
RANKL = RANK ligand
Tumour cell Tumour cell
Tumour cell
PTHrP IL-1,6,8 PGE2
TNF M-CSF
Proteoclast
RANK
Denosumab
RANKL
Osteoclast RANK
Osteoclast in apoptosis
BMP PDGF FGFs IGFs TGF-b
Denosumab 1. Binds to RANKL and neutralizes its
activity 2. Reduces osteoclast activity and bone
resorption
Bisphosphonates 1. Inhibit tumour cell adhesion
to bone 2. Inhibit osteoclast activity 3. Induce osteoclast apoptosis
Differentiation
PTHrP

Bone-targeted Agents Reduce Complications but Have No Proven Survival Benefit
1. Saad F, et al. J Natl Cancer Inst 2002;94:1458-68
2. Fizazi K, et al. Lancet 2011;377:813-22
Therapeutic Primary end point
Primary end point efficacy
Zoledronic acid vs placebo
Reduced SREs p = 0.0211
Denosumab vs zoledronic acid
Prevention of SREs
p = 0.0082

RADIOPHARMACEUTICALS

Alpha- vs. Beta-emitting Particles Alpha-emitters Beta-emitters
High-LET a-particles produce double-strand DNA breaks1,2
• Difficult to repair1,2 • Repair failure leads to apoptosis
(programmed cell death)1
• Misrepairs create chromosomal aberrations that result in mitotic cell death1
Low-LET b-radiation produces single-strand DNA breaks1
• Easily repaired using the opposite strand as a template1
• Less likely to induce cell death1
Examples: • Strontium-89 • Samarium-153:
Rhenium-186:
1. Hall E, Giaccia A. Radiobiology for the Radiologist. 6th Ed.
Philadelphia: Lippincott William & Wilkins; 2006
2. Bruland Ø, et al. Clin Cancer Res. 2006;12:6250s-6257s. LET = Linear energy transfer.
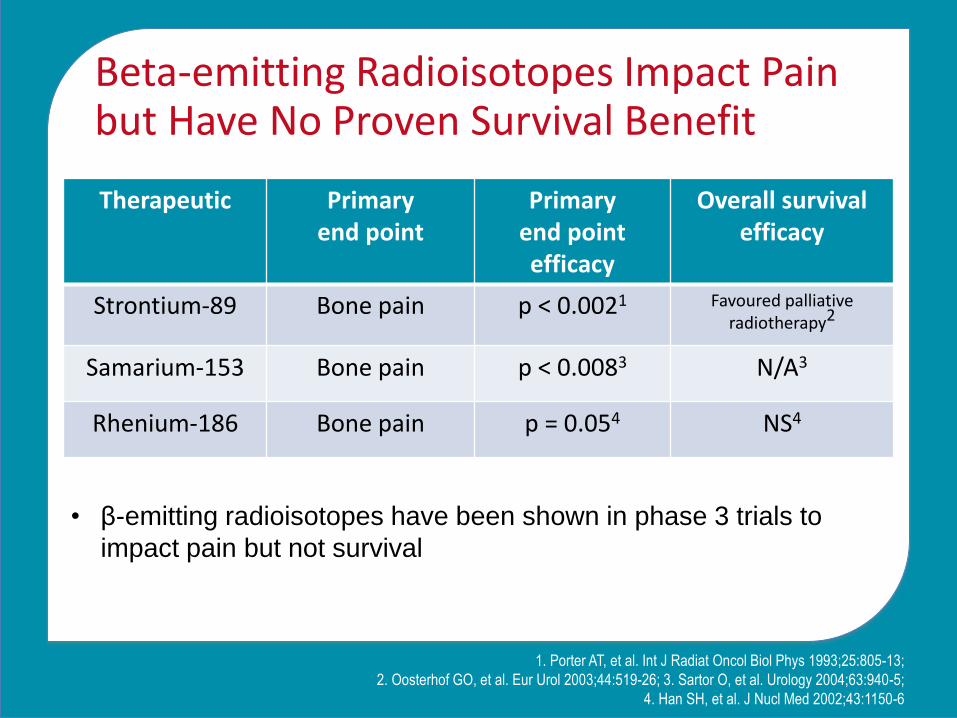
Beta-emitting Radioisotopes Impact Pain but Have No Proven Survival Benefit
1. Porter AT, et al. Int J Radiat Oncol Biol Phys 1993;25:805-13;
2. Oosterhof GO, et al. Eur Urol 2003;44:519-26; 3. Sartor O, et al. Urology 2004;63:940-5;
4. Han SH, et al. J Nucl Med 2002;43:1150-6
Therapeutic Primary end point
Primary end point efficacy
Overall survival efficacy
Strontium-89 Bone pain p < 0.0021 Favoured palliative radiotherapy2
Samarium-153 Bone pain p < 0.0083 N/A3
Rhenium-186 Bone pain p = 0.054 NS4
• β-emitting radioisotopes have been shown in phase 3 trials to
impact pain but not survival

Radium-223 Dichloride (223 RaCl2)
• Calcium mimetic
• Targets new bone growth in and around metastases
20
Ca 38
Sr 56
Ba 88
Ra

Properties of Radium-223
• Ra-223 dichloride
• t ½ - 11.43 days
• 4 α particles
– ~28 MeV, ~ 95%
• 2 β particles
• Multiple X/γ emissions allow imaging
Sartor O, et al. J Nucl Med Radiat Ther 2012;3:1-8

CLINICAL EFFICACY OF RADIUM-223
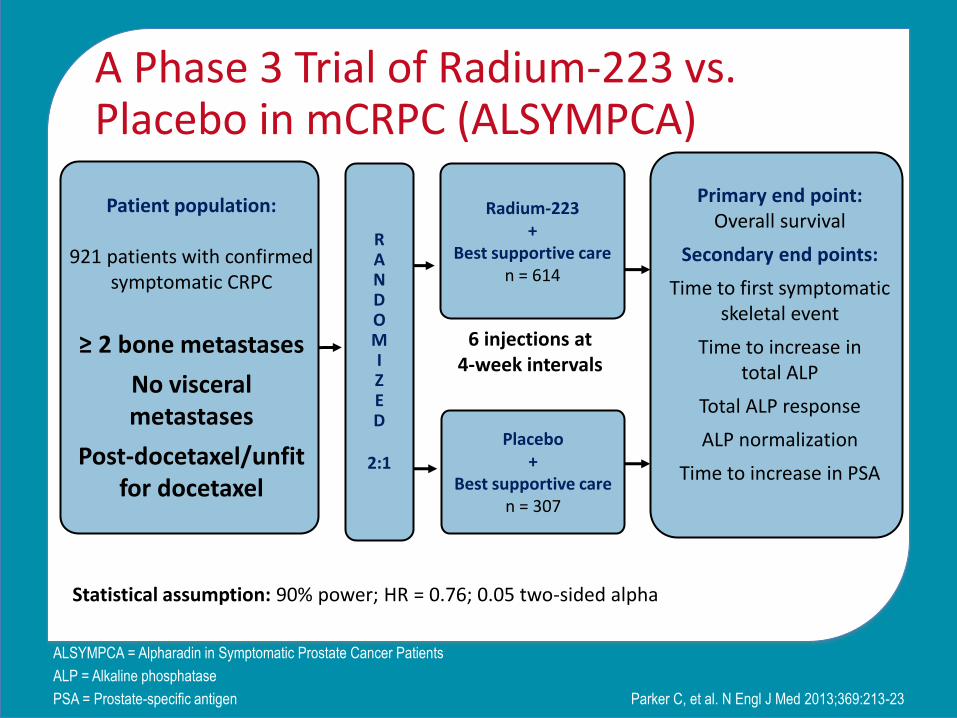
A Phase 3 Trial of Radium-223 vs. Placebo in mCRPC (ALSYMPCA)
Parker C, et al. N Engl J Med 2013;369:213-23
ALSYMPCA = Alpharadin in Symptomatic Prostate Cancer Patients
ALP = Alkaline phosphatase
PSA = Prostate-specific antigen
R A N D O M I Z E D
2:1
Radium-223 +
Best supportive care n = 614
Placebo +
Best supportive care n = 307
Patient population:
921 patients with confirmed symptomatic CRPC
≥ 2 bone metastases
No visceral metastases
Post-docetaxel/unfit for docetaxel
Primary end point: Overall survival
Secondary end points:
Time to first symptomatic skeletal event
Time to increase in total ALP
Total ALP response
ALP normalization
Time to increase in PSA
6 injections at 4-week intervals
Statistical assumption: 90% power; HR = 0.76; 0.05 two-sided alpha

ALSYMPCA: Patient Demographics Parameter Radium-223
(n = 614) Placebo (n = 307)
Age, median (range) 71 (49-90) 71 (44-94)
Total alkaline phosphatase < 220 U/L, n (%) 348 (57) 169 (55)
Current use of bisphosphonates, n (%) 250 (41) 124 (40)
Any prior use of docetaxel, n (%) 352 (57%) 174 (57%)
PSA, μg/L 146 (3.8–6026) 173 (1.5–14500)
Hemoglobin, g/dL 12.2 (8.5–15.7) 12.1 (8.5–16.4)
Lactate dehydrogenase, U/L 315 (76–2171) 336 (132–3856)
ECOG performance-status score, n (%) 0 1 ≥ 2
165 (27) 371 (60) 77 (13)
78 (25)
187 (61) 41 (13)
Extent of disease, n (%) < 6 metastases 6–20 metastases > 20 metastases
100 (16) 262 (43) 195 (32)
38 (12)
147 (48) 91 (30)
Parker C, et al. N Engl J Med 2013;369:213-23 ECOG PS = Eastern Cooperative Oncology Group performance status
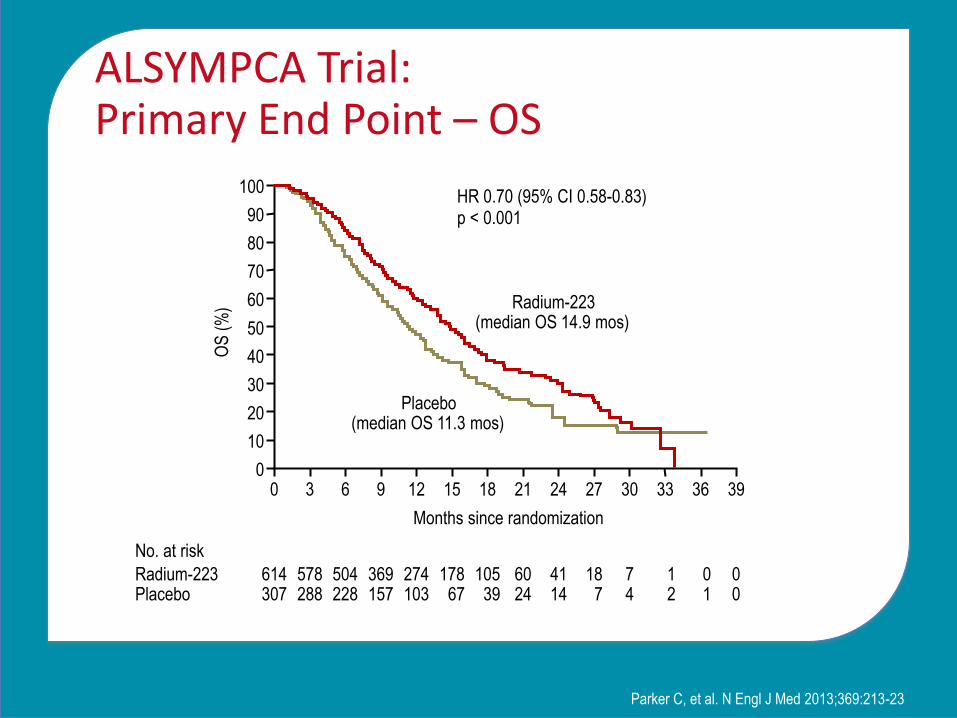
ALSYMPCA Trial: Primary End Point – OS
Parker C, et al. N Engl J Med 2013;369:213-23
100
80
90
70
60
40
30
10
50
20
0 0 3 6 9 12 15 39
Months since randomization
HR 0.70 (95% CI 0.58-0.83) p < 0.001
No. at risk
Radium-223 Placebo
614 307
578 288
504 228
369 157
274 103
178 67
18 21 24 27 30
105 39
60 24
41 14
18 7
7 4
33
1 2
36
0 1
0 0
Radium-223 (median OS 14.9 mos)
Placebo (median OS 11.3 mos)
OS
(%
)

ALSYMPCA: Previous Docetaxel Use and Survival
Previous docetaxel use No previous docetaxel use
Hoskin P, et al. Lancet Oncol 2014;15:1397-406
Radium-223, n = 352 Median: 14.4 months (95% CI 12.5–15.5)
Placebo, n = 174 Median: 11.3 months (95% CI 10.0-12.9)
HR 0.70 (95% CI 0.56–0.88; p = 0.002) 100
80
60
40
20
0 0 4 8 40
Treatment period
0 4 8 36 32
Treatment
period
Radium-223, n = 262 Median: 16.1 months (95% CI 13.9–17.8)
Placebo, n =1 33 Median: 11.5 months (95% CI 9.5–14.1)
HR 0.69 (95% CI, 0.52–0.92; p = 0.01)
36 32 28 24 20 16 12 28 24 20 16 12
352
174
327
152
238
104
0
0
262
133
236
113
168
74
0
0
1
1
0
1
1
1
5
4
27
5
45
15
88
35
157
61
7
3
14
9
31
14
70
24
120
42
Radium-223
Placebo
Number
at risk
Sur
viva
l (%
)
Months Months

ALSYMPCA Trial: Secondary End Point – Time to First Symptomatic Skeletal Event
Parker C, et al. N Engl J Med 2013;369:213-23
100
80
90
70
60
40
30
10
50
20
0 0 3 6 9 12 15 30
Months since randomization
HR 0.66 (95% CI 0.52-0.83) p < 0.001
No. at Risk
Radium-223 Placebo
614 307
496 211
342 117
199 56
129 36
63 20
18 21 24 27
31 9
8 7
8 4
1 1
0 0
Radium-223 (median time to first symptomatic
skeletal event, 15.6 mos)
Placebo (median time to first symptomatic
skeletal event, 9.8 mos)
Pat
ient
s w
ithou
t sym
ptom
atic
skel
etal
eve
nt(%
)

ALSYMPCA: Current Bisphosphonate Use and Symptomatic Skeletal Events
Current bisphosphonate use No current bisphosphonate use
Sartor O, et al. Lancet Oncol 2014;15:738-46
Number at risk
Radium-223
Placebo
0 4 8 12 16 20 24 28 32
250
124
193
71
115
29
61
17
25
10
8
3
3
3
1
1
0
0
Time (months)
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32
364
183
247
103
120
41
68
19
30
9
12
4
5
1
0
0
0
0
Time (months)
Placebo, n = 183
Median: 8.4 months
(95% CI 6.4–19.5)
HR = 0.77 (0.58–1.02)
p = 0.07
Treatment period
Pat
ient
s w
ithou
t
sym
ptom
atic
ske
leta
l eve
nts
(%)
Radium-223, n = 364
Median: 11.8 months (95% CI 9.3–13.6)
Treatment period
Placebo, n = 124
Median: 10.2 months
(95% CI 7.8–29.0)
HR = 0.49 (0.33–0.74)
p = 0.00048 Radium-223, n = 250
Median: 19.6 months
(95% CI 16.5 – not estimable)
0
20
40
60
80
100
Pat
ient
s w
ithou
t
sym
ptom
atic
ske
leta
l eve
nts
(%)

ALSYMPCA: Quality of Life
Nilsson S, et al. Ann Oncol 2016;27:868-74
*Response = Increase in score of ≥3 points from baseline at week 16 and/or week 24 for all
scales except pain, and an increase in score of ≥2 from baseline for the pain scale
34.9
24.5 24.7 26.5
22.5 24.7
17.9
21.9
16.5 14.9
0
5
10
15
20
25
30
35
40
45
Prostate Cancer
Subscale
Physical Well-Being Subscale
Social/Family Well-Being Subscale
Emotional Well-Being
Subscale
Functional Well-Being Subscale
Radium-223 (n = 434) Placebo (n = 191)
% R
esp
on
der
s* 30.2
20.1
Pain-Related Subscale
p = 0.012
p = 0.063 p = 0.446 p = 0.006
p = 0.029
p = 0.010

ALSYMPCA: Adverse Events
Parker C, et al. N Engl J Med 2013;369:213-23
All grades Grades 3 or 4
Adverse event Radium-223 (n = 600)
Placebo (n = 301)
Radium-223 (n = 600)
Placebo (n = 301)
Hematologic
Anemia 187 (31) 92 (31) 77 (13) 39 (13)
Neutropenia 30 (5) 3 (1) 13 (2) 2 (1)
Thrombocytopenia 69 (12) 17 (6) 38 (6) 6 (2)
Non-hematologic
Bone pain 300 (50) 187 (62) 125 (21) 77 (26)
Diarrhea 151 (25) 45 (15) 9 (2) 5 (2)
Nausea 213 (36) 104 (35) 10 (2) 7 (2)
Vomiting 111 (19) 41 (14) 10 (2) 7 (2)
Constipation 108 (18) 64 (21) 6 (1) 4 (1)
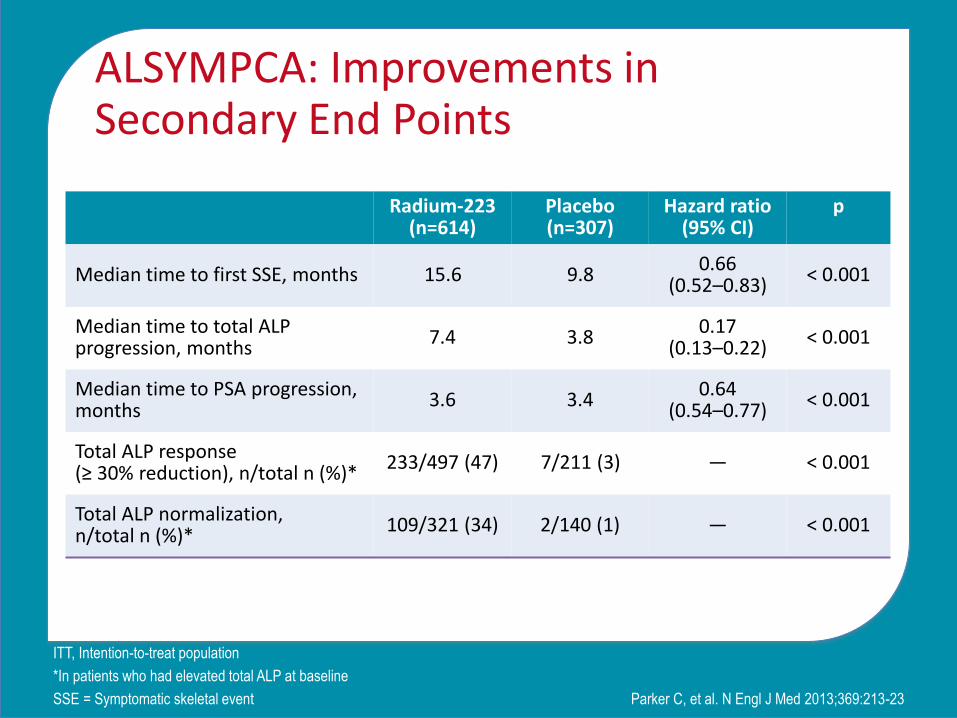
ALSYMPCA: Improvements in Secondary End Points
Parker C, et al. N Engl J Med 2013;369:213-23
ITT, Intention-to-treat population
*In patients who had elevated total ALP at baseline
SSE = Symptomatic skeletal event
Radium-223 (n=614)
Placebo (n=307)
Hazard ratio (95% CI)
p
Median time to first SSE, months 15.6 9.8 0.66 (0.52–0.83)
< 0.001
Median time to total ALP progression, months
7.4 3.8 0.17 (0.13–0.22)
< 0.001
Median time to PSA progression, months
3.6 3.4 0.64 (0.54–0.77)
< 0.001
Total ALP response (≥ 30% reduction), n/total n (%)*
233/497 (47) 7/211 (3) — < 0.001
Total ALP normalization, n/total n (%)*
109/321 (34) 2/140 (1) — < 0.001

ALSYMPCA: OS in Patients With and Without ALP Declines
Heinrich D, et al. EAU 2014
0
0
Ra-223 patients
without confirmed
tALP decline
n = 97
Median: 10.4 months
Ra-223 patients
with confirmed
tALP decline
n = 400
Median: 17.8 months
HR = 0.45
95% CI 0.34-61
p < 0.001
Months
Per
cent
age
of P
atie
nts
100
90
80
70
60
50
40
30
20
10
40 30 20 10

ALSYMPCA: Hematological Values in Patients Receiving Chemotherapy After Radium-223
Sartor O et al. Ann Oncol 2012;23(suppl. 9). Abstr 936P Post-hoc analysis
Placebo
Radium-223 Month 0 on the X axis =
the start of chemotherapy

Impact of Radium-223 on New Hormonal Therapies
• Favourable safety profile of radium-223 supports combination with other agents for additional beneficial effect1
• Hormonal agents abiraterone acetate and enzalutamide improved overall survival in CRPC patients with bone metastases2,3
– Safety profiles suggest nonoverlapping toxicity with rRadium-223
• Ongoing trials are studying the impact of radium-223 on new hormonal therapies1
1. Petrylak DP, et al. J Clin Oncol 2014;32(suppl):5S. Abstr TPS5103
2. De Bono JS, et al. N Engl J Med 2011;364:1995-2005
3. Scher HI, et al. N Engl J Med 2012;367:1187-97

Radium-223 Early Access Program: Study Design
Saad F, et al. Lancet Oncol 2016. [Epub ahead of print]
BPI-SF = Brief Pain Inventory-Short Form; HRPC = Hormone-refractory
prostate cancer; OS = Overall survival; SAE = Serious adverse events;
TEAE = Treatment-emergent adverse events
CRPC/HRPC patients with: • Bone
metastasis • ≥ 2 skeletal
metastases on imaging
• No lung/liver/ brain metastases
Radium-223 50 KBq/kg q4w x 6 injections Best standard of care (BSoC)
Treatment assessments each cycle Variables: Safety (SRE, TEAE, SAE, ECOG PS, Lab tests, QOL (BPI-SF) and OS Exploratory variables: SRE, ALP and PSA (changes in levels and time-to-event data)
Follow-up for safety data SRE, TEAE, SAE and secondary malignancies

Radium-223 Early Access Program: OS by Baseline Concomitant Use of Novel Endocrine Agents
NA = Not achieved
NE = Not estimated
OS = Overall survival
Concomitant use of abiraterone or enzalutamide
Yes No
Patients, n 189 507
Events, n (%) 42 (22%) 164 (32%)
Median OS, months (95% CI) NA (16–NE) 13 (12–16)
Saad F, et al. Lancet Oncol 2016. [Epub ahead of print]
0
0
4
3
48
75
142
296
Concomitant use of abi or enza
No concomitant use of abi or enza
Patients at risk
Concomitant use of abiraterone or enzalutamide
No concomitant use of abiraterone or enzalutamide
Time from start of treatment (months)
0 6 12 18 24 0
10
20
30
40
50
60
70
80
90
100
Ove
rall
surv
ival
(%
)
189
507

Radium-223 Early Access Program: OS by Baseline Concomitant Denosumab Use
NA = Not achieved
NE = Not estimated
OS = Overall survival
Concomitant use of denosumab
Yes No
Patients, n 136 560
Events, n (%) 34 (25%) 172 (31%)
Median OS, months (95% CI) NA (15–NE) 13 (12–NE)
Saad F, et al. Lancet Oncol 2016. [Epub ahead of print]
0
0
3
4
39
84
102
336
138
560
Concomitant use of denosumab
No concomitant use of denosumab
Patients at risk
Concomitant use of denosumab
No concomitant use of denosumab
0 6 12 18 24 0
10 20 30 40 50 60 70 80 90
100
Time from start of treatment (months)
Ove
rall
surv
ival
(%
)

Radium-223 Early Access Program: OS by Baseline Pain
*Measured by the Brief Pain Inventory Short Form (BPI-SF) questions 3 “Worst pain”,
4 “least pain”, 5 “average pain”, 6 “pain right now”
NA = Not achieved; NE = Not estimated; OS = Overall survival
Baseline pain* (n = 669)
No pain Mild Moderate-severe
Patients, n 139 370 158
Events, n (%) 23 (17%) 110 (30%) 64 (41%)
Median OS, months (95% CI) NA (16–NE) 14 (13–NE) 11 (9–13)
Saad F, et al. Lancet Oncol 2016. [Epub ahead of print]
0
0 0
2
4 1
32
66 20
94
238 88
139
370 158
No pain
Mild pain Moderate-severe pan
Patients at risk
No pain
Mild pain
Moderate-severe pain
0 6 12 18 24 0
10
20
30
40
50
60
70
80
90
100
Time from start of treatment (months)
Ove
rall
surv
ival
(%
)

Radium-223 Early Access Program: OS by Baseline ECOG PS
NE = Not applicable
OS = Overall survival
ECOG PS
0 1 ≥ 2
Patients, n 261 348 87
Events, n (%) 42 (16%) 117 (34%) 47 (54%)
Median OS, months (95% CI) NA (17–NA) 13 (11-NA) 7 (5-11)
0 0
4 3
62 55
183 226
261 348
ECOG 0 ECOG 1
Patients at risk
ECOG PS 0
ECOG PS ≥ 2
Saad F, et al. Lancet Oncol 2016. [Epub ahead of print]
0 0 6 29 87 ECOG ≥ 2
ECOG PS 1
0 6 12 18 24 0
10
20
30
40
50
60
70
80
90
100
Time from start of treatment (months)
Ove
rall
surv
ival
(%
)

PRACTICAL CONSIDERATIONS FOR THE USE OF RADIUM-223

Strategies to Minimize Hematological Effects of Radium-223
• Evaluate at baseline and prior to each injection:
• Discontinue treatment if counts do not recover to above values within 6-8 weeks despite supportive care (transfusions and growth factors)
Xofigo PM. March 2015
*Note: Patients may be accepted into clinical trials with hemoglobin
levels < 100 g/L
Before 1st administration
Before subsequent administrations
Absolute neutrophil count
≥ 1.5 x 109/L 1.0 x 109/L
Platelet count ≥ 100 x 109/L ≥ 50 x 109/L
Hemoglobin ≥ 100 g/L* ≥ 10 g/dL*

Radium-223: Instructions for Patients
• Remain well hydrated and monitor oral intake
• Report signs of bleeding or infection
• Report signs of dehydration, hypovolemia, urinary retention or renal failure/insufficiency
• For a least 1 week post-injection:
– Flush toilet several times after use
– Promptly wash soiled clothing separately
Xofigo PM. December 2013

CLINICAL VIGNETTES

PATIENT WHO HAS UNDERGONE CHEMOTHERAPY WITH DOCETAXEL
Clinical Vignette #1

Clinical Vignette #1
• 67 yo male, diagnosed with PCa in June 2008
– PSA 11 ng/mL, cT2a, GS 4+4 = 8 in 4/10 cores
– CT and bone scan –ve for metastases
• Sept 2008: Treated with radical prostatectomy
– pT3a, GS 4+4 = 8, N1 (lymph nodes in 2 regional LN)
– No adjuvant treatments initiated, ADT discussed
ADT = Androgen-deprivation therapy; CT = Computed tomography
GS = Gleason score; LN = Lymph node;
PSA = Prostate-specific antigen

Clinical Vignette #1 (cont’d)
• PSA rose quickly after surgery
• June 2009: Intermittent androgen blockade started
• Jan 2012: CRPC developed; PSA 22 ng/mL; bone scan showed metastases
0.4
3.2
5.5
0
2
4
6
Jan 2009 March 2009 May 2009
PSA
ng/
mL

Clinical Vignette #1 (cont’d)
• March 2012: Started on abiraterone acetate + prednisone and denosumab 120 mg q 4 weeks
– PSA continued to rise
• How would you have intervened over these 7 months?
• Bone scan showed worsening bony mets (spine, femur) (right and left), and multiple ribs; CT showed no visceral disease
24
33
45
0
10
20
30
40
50
July 2012 Oct 2012 Jan 2013
PSA
ng/
mL

Clinical Vignette #1 (cont’d)
• Sept 2014: Finished 10 cycles of docetaxel and prednisone
– PSA 23 ng/mL
– No change in bone scan
– CT scan shows no visceral disease
– Worsening bony pain, especially in spine

Discussion Questions
• Would you refer for consideration of a radiopharmaceutical for this patient?
• Why/why not?
• What other agent would you initiate at this time, if any? Why/why not?

PATIENT WHO HAS PROGRESSED ON DOCETAXEL AND IS ENROLLED IN A CLINICAL TRIAL
Clinical Vignette #2

Clinical Vignette #2
• July 2002: 65 yo male with high-risk prostate cancer
– cT2B, Gleason 8, PSA 38 ng/mL
– Staging –ve
– Radical external radiation therapy
– 3 years adjuvant LHRH
• Jan 2007: PSA relapse, staging –ve
• ADT initiated
ADT = Androgen-deprivation therapy
PSA = Prostate-specific antigen
LHRH = Luteinizing hormone-releasing hormone
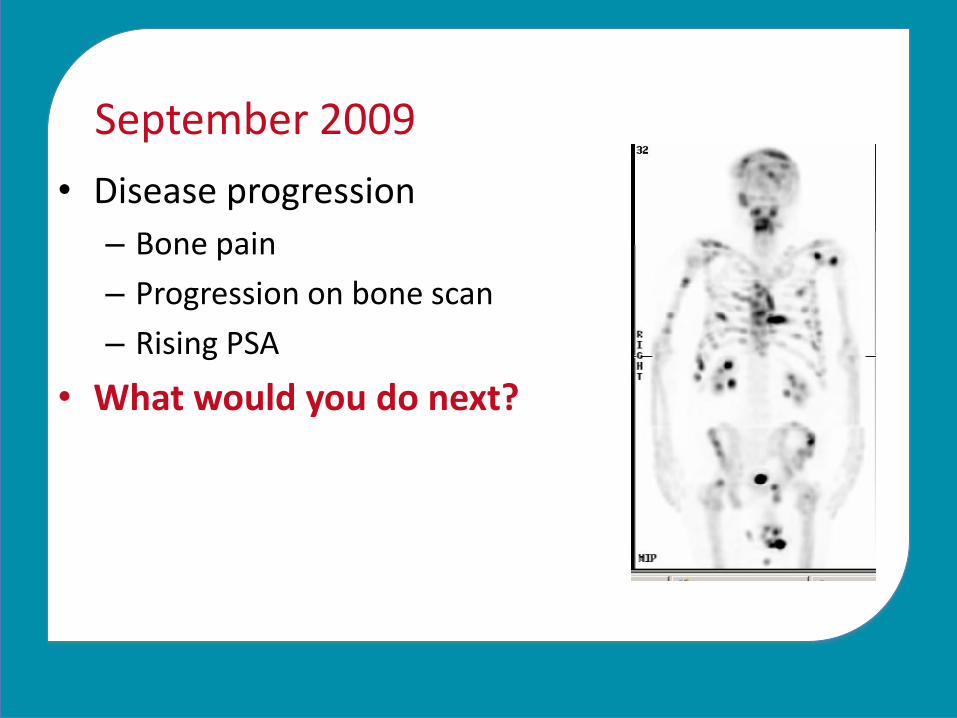
September 2009
• Disease progression
– Bone pain
– Progression on bone scan
– Rising PSA
• What would you do next?

November 2009
• Receives docetaxel
• Zoledronic acid started
• Docetaxel discontinued due to severe mucositis and bone marrow toxicity (2 cycles)

Discussion Question
What is your next step?
• Androgen receptor axis-targeted therapy?
• Initiate denosumab?
• Refer for chemotherapy (cabazitaxel)?
• Refer for radium-223?
Clinical Vignette #2 (cont’d)
• Nov 2009: Patient referred for radium-223
• At initiation:
– Diffuse bone pain/anorexia/fatigue
– PSA 785 ng/mL, ALP 448 U/L, hemoglobin 96 g/L
– PSADT 4 months
– Diffuse bone metastases
– Morphine sulfate (timed-release) 15 mg bid + breakthrough morphine
PSADT = PSA doubling time

Clinical Vignette #2 (cont’d)
• 6 cycles of radium-223 (50 kBq/kg IV Q4 weekly)
• Subjective clinical benefit (discontinued narcotics within 6 weeks)
• Complete pain relief last 4 months
• PSA stabilized/ALP normalized (101 U/L)
• Single palliative external-beam radiation to humerus for pain
• Toxicity: – No gastrointestinal adverse effects
– No systemic reactions
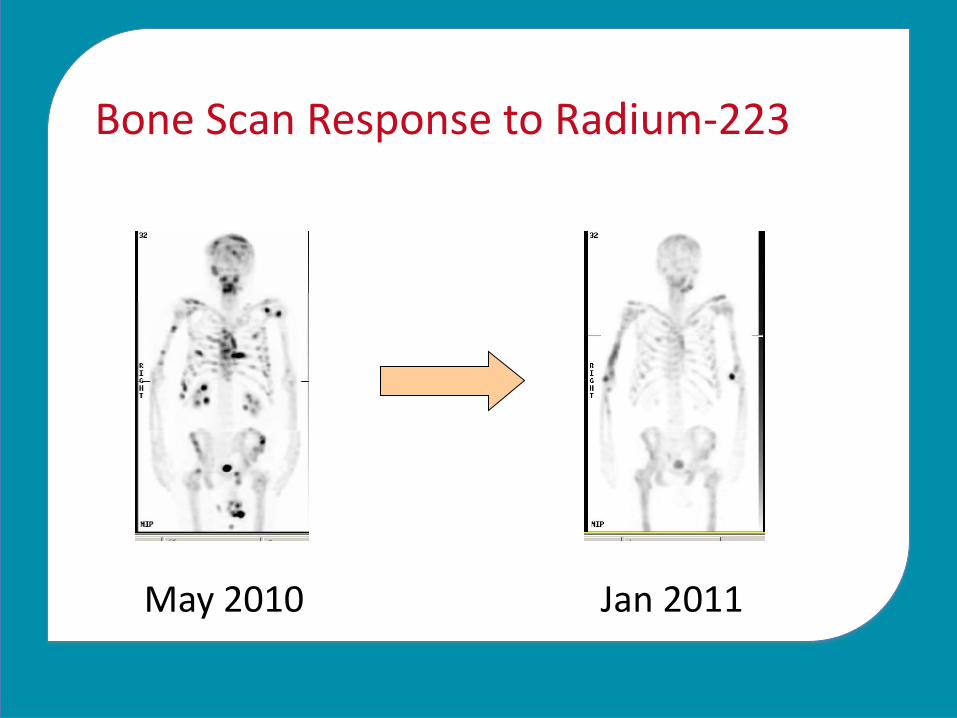
Bone Scan Response to Radium-223
May 2010 Jan 2011

Clinical Vignette #2 (cont’d)
• May 2010: Patient progresses – bones/nodes
• No response to abiraterone acetate + prednisone and discharged to palliative care hospital for supportive care
• What benefits could have been actualized if the patient had received a bone-targeted therapy?
• How else might you have sequenced therapy for this patient?

PATIENT WHO PROGRESSES ON ABIRATERONE ACETATE + PREDNISONE
Clinical Vignette #3

Clinical Vignette #3
• Aug 2011: 74-year-old man with PCa
– PSA: 420 ng/mL
– Biopsy: Gleason 8
• Multiple BM on bone scan, no visceral metastases in abdominal CT, clear chest X-ray
• Initial treatment: ADT = leuprolide and bicalutamide from time of diagnosis
• Question: This was 2011. What would you have done with this patient today?

PSA Rising: Indication for New Treatment
• May 12, 2013
– PSA 12 ng/mL, testosterone 0.6 nmol/L, ALP 95 IU/L, Hb 12.1 g/dL
– Multiple BM on bone scan, no visceral metastases in abdominal CT and chest X-Ray
• June 14, 2013
– PSA 25 ng/mL
• June 21, 2013
– Abiraterone acetate + prednisone initiated

PSA Rising: Indication for New Treatment (cont’d)
• March 2014 – Patient became symptomatic of progressive BM
needing NSAID and occasional codeine for pain relief
1.5
8 11
25
05
1015202530
Sept2013
Jan2014
Feb2014
March2014
PSA
ng/
mL

Symptoms
• Pain: variable intensity, regular NSAID with occasional codeine 30 mg on average 1-2/day when active
• Patient reduced activities but was able to continue regular walks with spouse with the use of codeine
• Sleep occasionally disturbed due to pain
• Bothered by constipation due to analgesic use

Clinical Vignette #3
• April 2014: PSA: 52 ng/mL, testosterone 0.6 nmol/L, ALP 312 IU/L
– Imaging:
• Bone metastases: multiple metastases (approximately 10-12) mainly in spine, sacrum and right hip - No evidence of visceral metastatic disease

Discussion Questions
• What are the options for this patient who has had symptomatic progression on abiraterone acetate + prednisone?
• What is your therapeutic sequence/clinical maneuver with this man?
• What are the characteristics of the right patient for:
– Radium-223?
– Chemotherapy?
– Bone-targeted therapy?

What We Did
• The patient was offered docetaxel or radium-223 given progression on abiraterone acetate + prednisone and the appearance of symptoms
• The patient selected radium-223 after discussing the advantages and disadvantages of each
• Patient made aware that chemotherapy could still be an option after radium-223 and vice versa
• April 2011: Radium-223 initiated (6 cycles)

Radium-223 Treatment
• Radium-223 was administered with no dose interruptions
• Concomitant treatment for PCa: leuprolide
• Comorbidities: well-controlled hypertension

Other Key Measures
Hb
g/L
WBC
x109/L
Platelets
/µL
ALP
U/L
PSA
ng/mL
After 1 cycle of
Radium-223
119 5.8 265,000 261 61
After 2 cycles of
Radium-223
117 5.6 241,000 243 75
After 3 cycles of
Radium-223
118 6.3 238,000 188 92
After 4 cycles of
Radium-223
111 4.9 244,000 155 113
After 5 cycles of
Radium-223
115 5.5 212,000 121 119
After 6 cycles of
Radium-223
108 4.7 198,000 99 126

• Oct 2014: Patient completed radium-223 treatment
• Dec 2014: Pain progressed, PSA 260 ng/mL
• What would you suggest at this point?
Clinical Vignette #3 (cont’d)

Clinical Vignette #3 (cont’d)
• Dec 2014: Patient started docetaxel (7 cycles)
• April 2015:
– No unexpected side effects or myelosuppression beyond what was expected
– Patient not on G-CSF

Patient Case – Overview
AA = Abiraterone acetate; ALP = Alkaline phosphatase;
BIC = Bicalutamide; BM = Bone metastases, DXT = Docetaxel;
LEU = Leuprolide; TT = Testosterone