managing emotional and behavioural problems in … · problems in children with autism spectrum...
TRANSCRIPT

S
Managing Emotional and Behavioural
Problems in Children with Autism
Spectrum Disorders: Programs with
School Trials
Associate Professor Kate Sofronoff
School of Psychology
University of Queensland
Acknowledgements

What has an Evidence-Base?
S Behaviour therapy
S Applied Behaviour Analysis (Lovaas)
S Use of visual supports
S Social Stories, Comic Strip Conversations (Gray)
S Use of environmental supports
S Quiet spaces
S Cognitive Behavioural Interventions
S Anxiety, anger management, friendship, social-emotional skills

What do Parents and Teachers
Typically Report as Difficult?
S Managing challenging behaviours S Head banging, self harm, screaming
S Managing emotional problems S Anxiety, social problems, anger, depression
S Increasing independence S What can the child do for themselves?
S Skill building S Self care, tolerance, social skills
S Nurturance traps S It’s the disorder, he/she doesn’t understand

High Rates of Multiple Problem
Areas
S Recent UK study – children in mainstream schools
S Anxiety, fears and phobias (N=188; 43.3%)
S Behavioural problems (N=201; 46.3%)
S Eating problems (N=241; 55.5%)
S Sensory Issues (N=221; 50.9%)
S Maskey, Warnell, Parr, Le Couteur, & McConachie (2013), JADD,43: 851-859.

Evidence-Based Programs
S Programs that have been subjected to rigorous evaluation
S Programs that follow best practice guidelines for working with autism spectrum disorders
S Some of these are now taking a transdiagnostic approach
S Taking account of other likely diagnoses or problems that will interfere with a child’s capacity to learn new skills
S Behavioural problems in relation to new situations
S Anxiety in relation to social interaction
S Anger in relation to social interaction

Where to Start?
S Parents and teachers often ask for social skills
S Child needs to be able to regulate emotions
S To cope with frustration
S To cope being told ‘not your turn’ and ‘wait’
S To behave appropriately in different situations
S Often working with parents first is likely to produce better results

Parenting Programs
S Aim to work collaboratively with parents to establish goals that parents want to achieve
S Acknowledge the parent as expert
S Allow parent to select strategies that will work for their family and circumstances
S Aim to empower parents
S What does this have to do with schools???

Stepping Stones Triple P
S Developed specifically for parents with a child with a developmental disability
S Targets creating a positive parent-child relationship
S Creating a positive learning environment
S How to teach new skills
S Using assertive discipline
S Encouraging child to learn emotion management strategies

Evidence Base S Sanders, M.R., Mazzucchelli, T., & Studman, L. (2004). Stepping Stones Triple P: The theoretical basis and development of an
evidence-based positive parenting program for families with a child who has a disability. Journal of Intellectual and
developmental Disability, 29, 265-283.
S Roberts, C., Mazzucchelli, T., Studman, L., & Sanders, M.R. (2006). Behavioral family Intervention for children with
developmental disabilities and behavioral problems. Journal of Clinical Child and Adolescent Psychology, 35, 180-193.
S Whittingham, K., Sofronoff, K., & Sheffield, J. (2006). Stepping Stones Triple P: A pilot study to evaluate acceptability of the
program by parents of a child diagnosed with an autism spectrum disorder. Research in Developmental Disabilities, 27, 364-380.
S Plant, K., & Sanders, M. (2007). Reducing problem behavior during care-giving in families of preschool-aged children with
developmental disabilities. Research in Developmental Disabilities, 28, 362-385.
S Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M.R. (2009). Do parental attributions affect treatment outcome in a
parenting program? An exploration of the effects of parental attributions in an RCT of Stepping Stones Triple P for the ASD
population. Research in Autism Spectrum Disorders, 3, 129-144.
S Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M.R. (2009). An exploration of parental attributions within the Autism
Spectrum Disorders population. Behaviour Change, 25, 201-214.
S Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M.R. (2009). Stepping Stones Triple P: An RCT of a parenting program
with parents of a child diagnosed with an autism spectrum disorder. Journal of Abnormal Child Psychology, 37, 469-480.
S Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M.R. (2010). Behavioural Family Intervention with parents of children
with ASD: What do they find useful in the parenting program Stepping Stones Triple P? Research in Autism Spectrum
Disorders,3, 868-875.
S Sofronoff, K., Jahnel, D., & Sanders, M. (2011). The Stepping Stones Triple P Seminars for parents of a child with a
developmental disability: A randomized controlled trial. Research in Developmental Disabilities, 32, 2253-2262.
S Roux, G., Sofronoff, K., & Sanders, M. (2013). A randomized controlled trial of Group Stepping Stones Triple P for families of
children with disabilities. Family Process, 52(3), 411-424.
S Brown, F., Whittingham, K., Boyd, R., McKinlay, L., & Sofronoff, K. (in press). Improving child and parent outcomes following
pediatric acquired brain injury: A randomized controlled trial of Stepping Stones Triple P plus Acceptance and Commitment
therapy. Journal of Child Psychology and Psychiatry.
S Tellegen, C., & Sanders, M.R. (2013). Stepping Stones Triple P-Positive Parenting Program for children with disability: A
systematic review and meta-analysis. Research in Developmental Disabilities, 34, 1556-1571.

Currently
S This program is being offered FREE across Queensland and
Victoria – many facilitators are teachers
S In NSW the My Say survey is currently underway
S Training of professionals will begin towards the end of this
year in NSW
S Programs (levels 2 and 3) will be available via these
professionals in 2015



S
Cognitive Behaviour
Therapy for Children
with ASD
Anxiety

Can CBT be used?
S Moree & Davis (2010)
S Modification trends
S Rotheram-Fuller & MacMullen (2011)
S Adaptations for use in schools
S Scarpa & Reyes (2011)
S Emotion regulation strategies
S Reaven, Blakeley-Smith,Culhane-Shelburne, & Hepburn (2012)
S Group CBT for anxiety
S Attwood & Sofronoff (2013)
S CBT for anxiety
S Beaumont & Sofronoff (2013)
S Social-emotional skills
S Sofronoff, Beaumont & Weiss (in press)
S Transdiagnostic processes in ASD interventions

CBT for Anxiety Sofronoff, Attwood & Hinton (2005). A randomised controlled trial of a CBT intervention for anxiety in children with
Asperger syndrome. Journal of Child Psychology and Psychiatry, 46, 1152-1160.
S Program developed by Tony Attwood
S Exploring Feelings
S Multiple Randomised Controlled Trials
S Trial in Newcastle, UK (McConachie et al in press)
S Six 2 hour sessions – 3 children with 2 therapists
S Original trial evaluated 3 conditions
S Child only
S Child + Parent
S Waitlist
S Child + Parent condition showed best results
S Parents also preferred to be involved

Results
S Significant improvement reported by parents on measures of anxiety
S Child + Parent group superior to Child Only group and both intervention groups superior to Treatment as Usual
S Significant increase in knowledge of how to manage anxiety by child report
S Qualitative information from parents very useful
S Some generalisation to school reported by parents

Social Worries
0
2
4
6
8
10
12
14
Time 1 Time 2 Time 3
Intervention Control Int. + ParentsS main effect for Time S F2,78 =13.82, p<.0001
S no main effect for Group
S Time x Group Interaction
F4,158=14.15, p<.0001
S Post hoc tests S Intervention groups showed S significantly lower parent S ratings between T1 and T3 S Difference between S intervention groups at T3 S approached significance
S Both interventions different S from wait-list at T3

Separation Anxiety
0
1
2
3
4
5
6
7
8
9
10
Time 1 Time 2 Time 3
Intervention Control Int. + Parents S main effect for Time S F2,78 =13.69, p<.0001 S main effect for Group S F2,78 =5.24, p<.01
S Time x Group Interaction
F4,158=10.65, p<.0001
S Post hoc tests S Intervention groups reported
significantly lower parent ratings at T3
S Difference between intervention groups at T3 significant

Obsessive Compulsive
Symptoms
0
1
2
3
4
5
6
Time 1 Time 2 Time 3
Intervention Control Int. + Parents S Main effect for Time F2,78 =16.69, p<.0001
S No main effect for Group
S Time x Group Interaction F4,158=10.13, p<.0001
S Post hoc tests of simple interaction effects
S Both intervention groups significantly lower at T2 and T3 compared with T1
S Intervention groups reported significantly lower parent ratings compared with WL at T3
S No difference between intervention
group 1 and control at T2

James and the Maths Test
0
1
2
3
4
5
6
Time 1 Time 2 Time 3
Intervention Control Int. + Parents S main effect for Time S F2,78 =104.76, p<.0001
S main effect for Group S F2,78 =38.19, p<.0001
S Time x Group Interaction F4,158=28.31,
p<.0001
S Post hoc tests
S Both intervention groups significantly higher at T2 and T3 compared with T1
S Intervention groups significantly different from waitlist at T2 and T3
S Intervention groups significantly different from each other at T2 and T3

Conclusions
S Intervention effective in changing some behaviours for some children
S Parents very positive about the groups
S Many children made friends
S Many parents formed support groups
S Greater parent involvement led to better child outcomes
S Many changes not captured by standard measures
S Population likely to benefit from ongoing contact
S About 55% reported change in the school setting as well as at home

S
Anger Management Sofronoff, Attwood, Hinton, Levin (2007)

Sofronoff, Attwood, Hinton & Levin (2007). A randomized controlled trial of a cognitive behavioural
intervention for anger management in children diagnosed with Asperger syndrome. Journal of Autism and
Developmental Disorders, 37, 1203-1214.
S Randomised controlled trial
S 52 children aged 10-14 years (mean age 10.79)
S 2 children did not meet criteria
S 5 families withdrew after assignment to wait-list
S 45 participated
S Boys in Intervention 23, girls 1 (wait-List 20 boys, 1 girl)
S All children diagnosed ASD by paediatrician
S Diagnosis checked by semi-structured interview with parents
S Childhood Asperger Syndrome Test (CAST; Scott, Baron-Cohen et al.)
S No children excluded on basis of co-morbid disorder
S ADHD 11 (46%) in Intervention and 9 (43%) in wait-list

Parent Reports of Anger
90
92
94
96
98
100
102
104
106
108
110
Intervention Wait-list
pre
post
follow-up
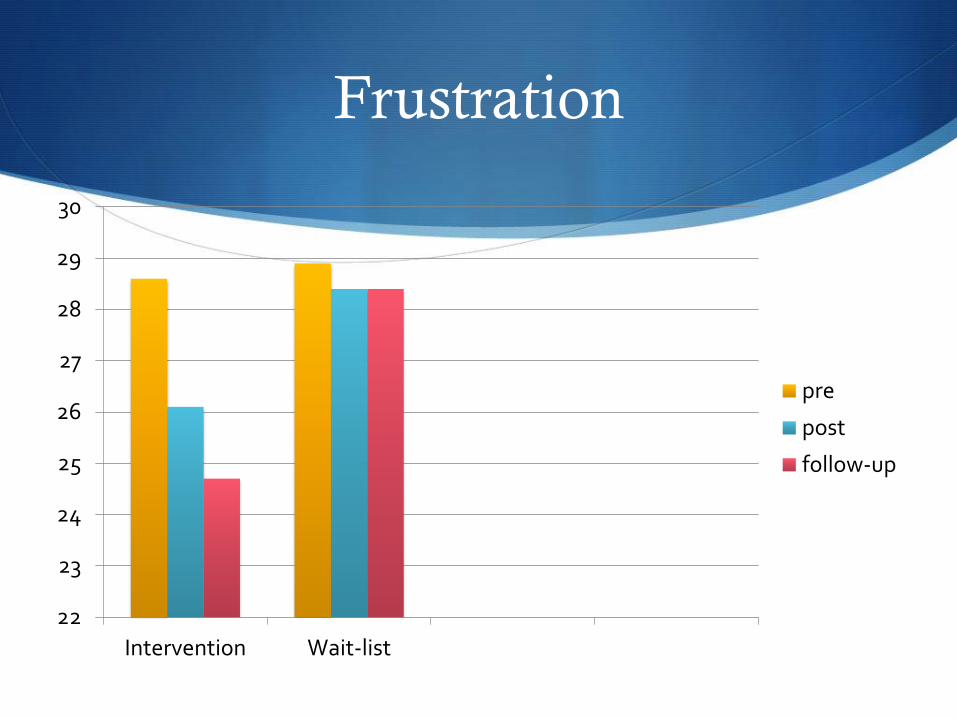
Frustration
22
23
24
25
26
27
28
29
30
Intervention Wait-list
pre
post
follow-up

Parent Monitoring of Anger
0
1
2
3
4
5
6
7
8
9
10
Intervention Wait-list
pre
post
follow-up

Dylan is Being Teased
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Intervention Wait-list
pre
post
follow-up

Qualitative Teacher Reports
S 18 teachers were able to be contacted by phone for a brief interview and were asked a series of questions
S Firstly they were asked if they knew that the child had completed the program and if so who told them about this
S All had heard from the child’s mother
S In response to ‘have you noticed any change in the child’s ability to manage anger since completing the program?’ 16 (88%) responded “YES” and 2 (12%) said “NO”
S 3 themes emerged from the YES responders
S All were aware of the child trying to use strategies to manage anger at least sometimes
S 19% (3) said the child would ask to withdraw when feeling angry
S 56% (9) said the child now had a language with which to talk about anger and this helped reduce the number of outbursts

Parents and Teachers often ask
for Social Skills
S Can we teach social interaction skills in the context of
anxiety issues and emotion regulation issues
S Is there a logical progression of programs?
S Parenting
S Emotion recognition
S Anxiety/emotion regulation (anger, affection)
S Social interaction
S Depression
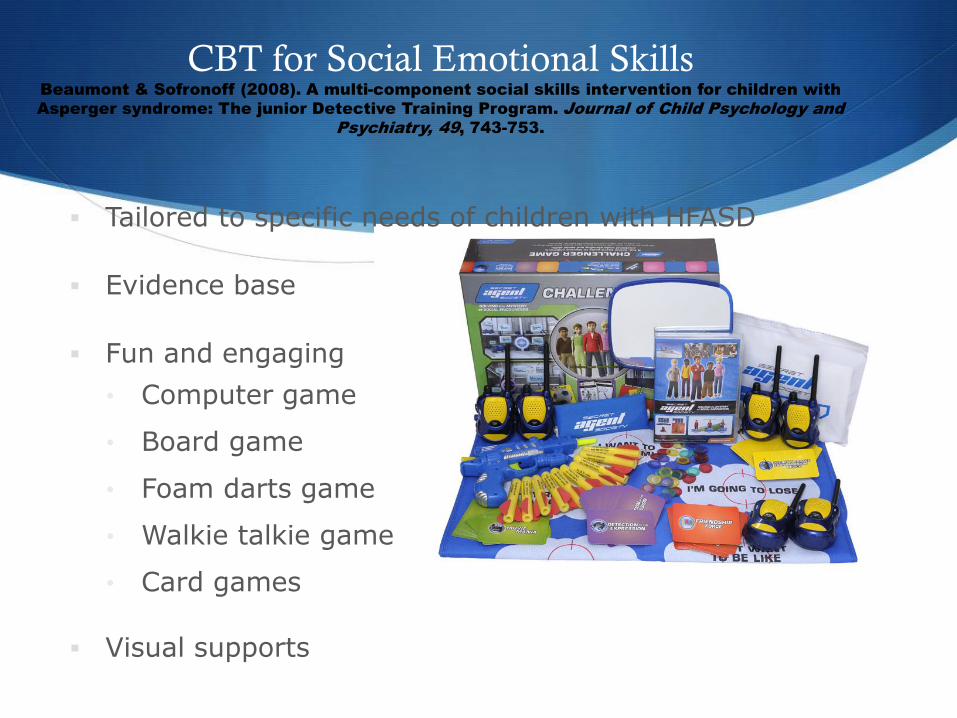
Tailored to specific needs of children with HFASD
Evidence base
Fun and engaging
• Computer game
• Board game
• Foam darts game
• Walkie talkie game
• Card games
Visual supports
CBT for Social Emotional Skills Beaumont & Sofronoff (2008). A multi-component social skills intervention for children with
Asperger syndrome: The junior Detective Training Program. Journal of Child Psychology and
Psychiatry, 49, 743-753.

Computer Game
Emotion regulation and social skills
• Anger management
• Anxiety management
• Apologizing
• Bullying and teasing
• Coping with mistakes
• Meeting new people
• Playing with others
• Talking to others
• Team work
• Trying new things
• Winning and losing

Conclusions and Future Research
Program appeared to be effective in improving children’s emotion regulation and social skills in original RCT.
Completed Trials
Autism Spectrum Australia (Renae Beaumont tomorrow)
Mainstream schools trial (paper in press)
Parent delivered (current trial)
Future Trials
Whole classroom program (CRC)
Adolescent program – school-based (CRC)
Adult program (CRC)
