managing hypertension and obesity through and … files/syllabus files fall... · managing...
TRANSCRIPT

Managing Hypertension and Obesity through Therapeutics and Lifestyle Modifications
December 4, 2013
Baltimore, Maryland
Educational Partner:
The American Society for Preventive Cardiology

Session 2
Session 2: Managing Hypertension and Obesity Through Therapeutics and Lifestyle Modifications Learning Objectives: 1. Outline current guidelines on the diagnosis, management, and treatment of patients who are obese. 2. Identify the constellation of cardiovascular risk markers in diabetic, insulin-resistant, metabolic syndrome and/or
obese patients. 3. Understand the comprehensive approach to the treatment of obesity and hypertension. Faculty
James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA Diplomate, American Board of Clinical Lipidology Clinical Assistant Professor of Medicine New York University (NYU) Medical School NYU Center for Cardiovascular Disease Prevention Director Bellevue Hospital Lipid Clinic New York, New York
Dr Underberg is a clinical assistant professor of medicine in the division of general internal medicine at New York University (NYU) Medical School and the NYU Center for Cardiovascular Disease Prevention. He is the director of the Bellevue Hospital Primary Care Lipid Management Clinic and is also a member of the executive committee of the division of general internal medicine. His clinical focus is preventive cardiovascular medicine. He is an American Society of Hypertension (ASH)-certified specialist in clinical hypertension and a diplomate of the American Board of Clinical Lipidology. Dr Underberg is the founder and president of the New York Preventive Cardiovascular Society and a founding member of the board of directors of the Northeast Chapter of the National Lipid Association (NLA). He serves on the editorial board of the Journal of Clinical Lipidology, co-chairs the communication committee of the NLA, and is the co-editor of the NLA quarterly newsletter Lipid Spin. He currently serves on the CME committee of the ASH. He graduated from Yale University with a BS and MS and from the University of Pennsylvania Medical School. His internship and residency were completed at NYU-Bellevue Hospital Medical Center. He has been elected a fellow of the American College of Preventive Medicine, the Society of Vascular Medicine, the NLA, the American College of Physicians, and the ASH. He is currently involved in several clinical trials in the areas of hypertension, lipids, diabetes, and cardiovascular disease prevention. He sees patients both in a university-based referral practice and in the Bellevue Hospital Lipid Clinic.
Robert K. Gleeson, MD, FACP, FNLADiplomate, American Board of Clinical Lipidology Assistant Professor, Medicine Froedtert and The Medical College of Wisconsin Milwaukee, Wisconsin
Dr Gleeson is an assistant professor in the department of general medicine at the Medical College of Wisconsin. He is director of the preventive cardiology and lipid management program, which is part of the college’s Heart and Vascular Center, and director of the executive physical program, which is part of the college's Clinical Ventures Group.
Session 2
He is a diplomate of the American Board of Clinical Lipidology and along with Michael Davidson, the co-author of Lipidology, a Primer: The What, Why, and How of Better Lipid Management. Their second book, Conversations with a Preventive Cardiologist, was published in the late fall of 2012. He authored What Healthy People Know: And the 7 Things They Do To Stay Healthy and Live Long (2006), a book promoting a heart-healthy lifestyle. His professional interests are promoting a heart-healthful lifestyle and the use of easily understood lipid treatment protocols to improve compliance. Faculty Financial Disclosure Statements The presenting faculty reports the following: Dr Underberg serves on a speaker bureau for Abbott Laboratories, Aegerion Pharmaceuticals, Amarin Pharma Inc., AstraZeneca, Daiichi Sankyo, Inc., GlaxoSmithKline, Kowa Pharmaceuticals, LipoScience, Merck & Co., Inc., and Sanofi. Dr Gleeson has no financial relationships to disclose. Education Partner Financial Disclosure Statement The content collaborators at the American Society for Preventive Cardiology have no financial relationships to disclose. Suggested Reading List Sica D, Toth P. Clinical Challenges in Hypertension II. Oxford, UK: Clinical Publishing; 2010. Tonkin A. Therapeutic Strategies in Lipid Disorders. Oxford, UK: Clinical Publishing; 2009. Toth P, Sica D. Clinical Challenges in Lipid Disorders. Oxford, UK: Clinical Publishing; 2008.
1
Managing Hypertension and Obesity through Therapeutics and Lifestyle Modifications
SPEAKERsJames A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA
Robert K. Gleeson, MD, FACP, FNLA
SESSION 29:15–10:45am
Presenter Disclosure Information
►Dr Underberg serves on a speaker bureau for Abbott Laboratories, Aegerion Pharmaceuticals, Amarin Pharma Inc., AstraZeneca, Daiichi Sankyo, Inc., GlaxoSmithKline, KowaPharmaceuticals, LipoScience, Merck & Co., Inc., and Sanofi.
►Dr Gleeson has no financial relationships to disclose.
The following relationships exist related to this presentation:
Off-Label/Investigational Discussion
► In accordance with pmiCME policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
New Strategies for Obesity Management & Cardiometabolic Risk Reduction:
Proven Strategies in Different Patient Populations
James A. Underberg MD, MS, FACPM, FACP, FASH, FNLA
Clinical Assistant Professor , NYU School of Medicine
NYU Center for Cardiovascular Disease Prevention
Director, Bellevue Hospital Lipid Clinic, New York, NY
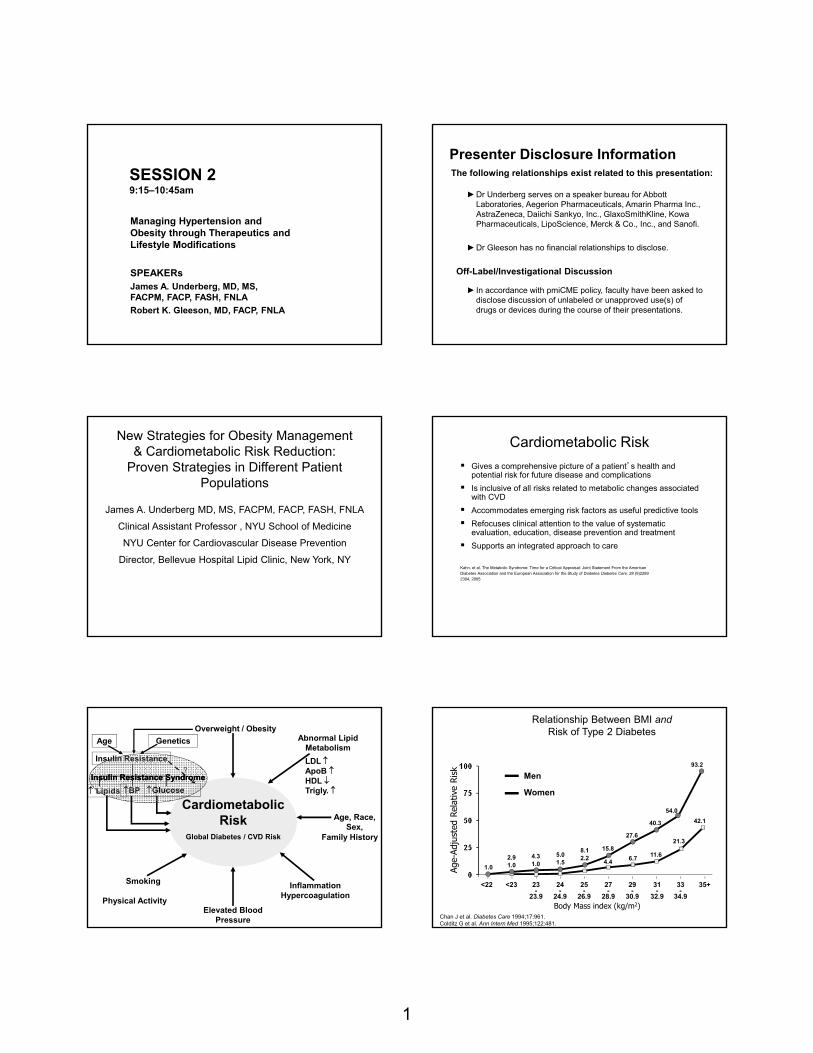
Cardiometabolic Risk
Gives a comprehensive picture of a patient’s health and potential risk for future disease and complications
Is inclusive of all risks related to metabolic changes associated with CVD
Accommodates emerging risk factors as useful predictive tools
Refocuses clinical attention to the value of systematic evaluation, education, disease prevention and treatment
Supports an integrated approach to care
Kahn, et al. The Metabolic Syndrome: Time for a Critical Appraisal: Joint Statement From the AmericanDiabetes Association and the European Association for the Study of Diabetes Diabetes Care. 28 (9)22892304, 2005
Abnormal Lipid Metabolism
LDL ApoB HDL Trigly.
Cardiometabolic Risk
Global Diabetes / CVD Risk
Overweight / Obesity
Inflammation Hypercoagulation
Elevated Blood Pressure
Smoking
Age, Race, Sex,
Family History
GlucoseBP Lipids
Age Genetics
Insulin Resistance?
Insulin Resistance SyndromeInsulin Resistance Syndrome
Physical Activity
Relationship Between BMI and Risk of Type 2 Diabetes
Chan J et al. Diabetes Care 1994;17:961.Colditz G et al. Ann Intern Med 1995;122:481.
Age-
Adju
sted
Rel
ativ
e Ri
sk
Body Mass index (kg/m2)
Men
Women
<22 <23 23-
23.9
24-
24.9
25-
26.9
27-
28.9
29-
30.9
31-
32.9
33-
34.9
35+
1.0
2.91.0
4.31.0
5.01.5
8.12.2
15.8
4.4
27.6
40.3
54.0
93.2
6.711.6
21.3
42.1
2
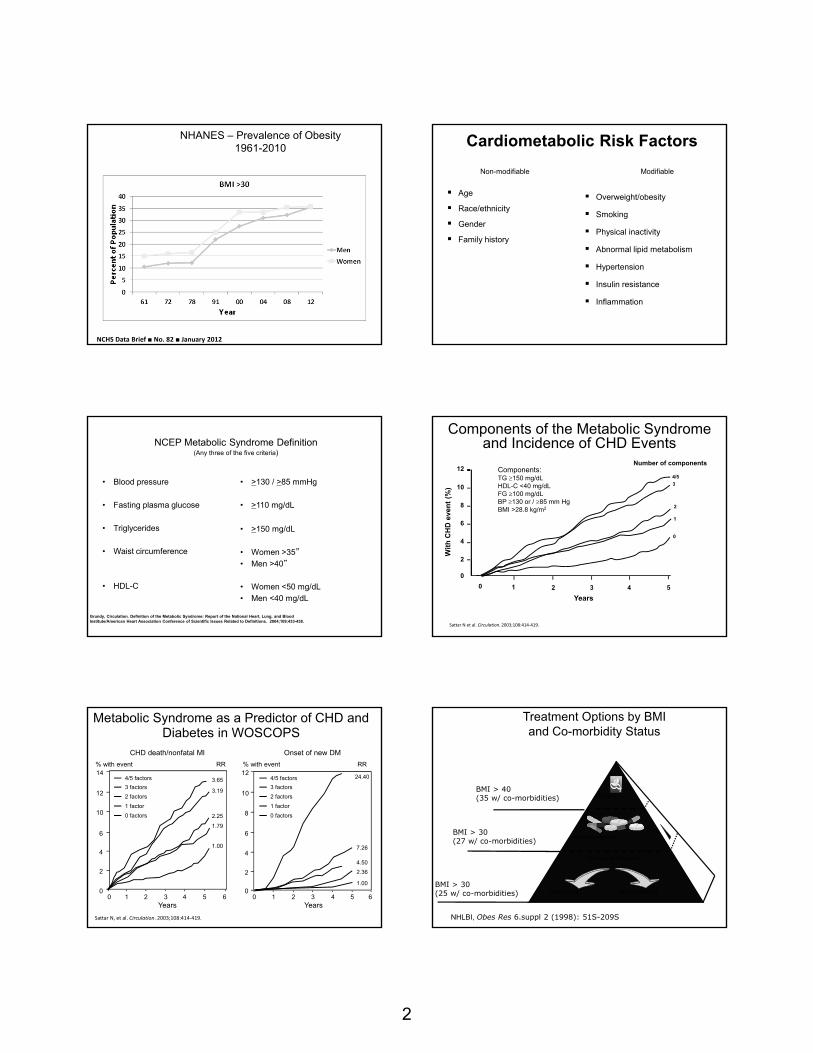
NHANES – Prevalence of Obesity1961-2010
NCHS Data Brief ■ No. 82 ■ January 2012
Non-modifiable Modifiable
Age
Race/ethnicity
Gender
Family history
Overweight/obesity
Smoking
Physical inactivity
Abnormal lipid metabolism
Hypertension
Insulin resistance
Inflammation
Cardiometabolic Risk Factors
NCEP Metabolic Syndrome Definition(Any three of the five criteria)
• Blood pressure
• Fasting plasma glucose
• Triglycerides
• Waist circumference
• HDL-C
• >130 / >85 mmHg
• >110 mg/dL
• >150 mg/dL
• Women >35”
• Men >40”
• Women <50 mg/dL
• Men <40 mg/dL
Grundy, Circulation. Definition of the Metabolic Syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference of Scientific Issues Related to Definitions. 2004;109:433-438.
Components of the Metabolic Syndrome and Incidence of CHD Events
12
10
8
6
4
2
0
0 1 2 3 4 5
Years
Wit
h C
HD
eve
nt
(%)
0
1
2
3
4/5Components:TG 150 mg/dLHDL-C <40 mg/dLFG 100 mg/dLBP 130 or / 85 mm HgBMI >28.8 kg/m2
Sattar N et al. Circulation. 2003;108:414‐419.
Number of components
Metabolic Syndrome as a Predictor of CHD and Diabetes in WOSCOPS
Sattar N, et al. Circulation. 2003;108:414‐419.
14
12
10
6
01
% with event
0 32 64Years
1 32 65
12
6
4
2
00
Years
4
2
5 4
% with event
CHD death/nonfatal MI Onset of new DM
8
10
RR RR
24.40
7.26
4.50
2.36
1.00
3.65
3.19
2.25
1.79
1.00
4/5 factors
3 factors
2 factors
1 factor
0 factors
4/5 factors
3 factors
2 factors
1 factor
0 factors
Treatment Options by BMI and Co-morbidity Status
Lifestyle Modification
Healthy Diet Physical Activity
Pharmacotherapy
Surgery
BMI > 30(25 w/ co-morbidities)
BMI > 30(27 w/ co-morbidities)
BMI > 40(35 w/ co-morbidities)
NHLBI, Obes Res 6.suppl 2 (1998): 51S-209S
3
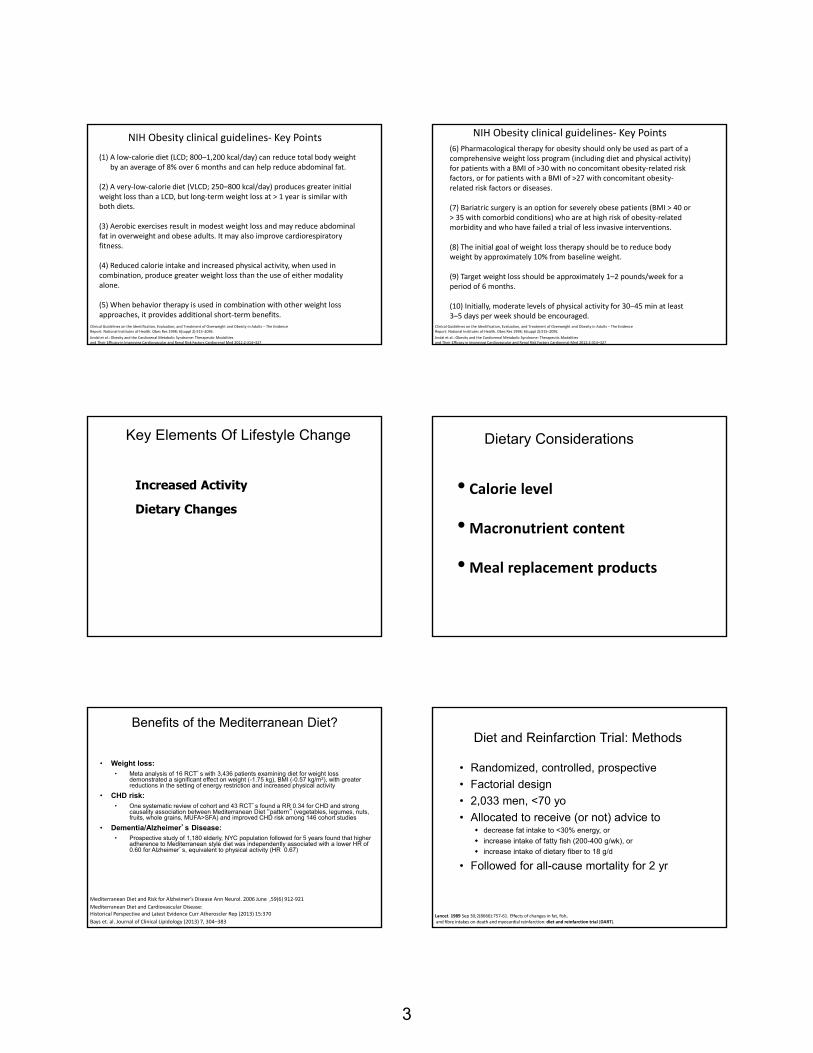
(1) A low‐calorie diet (LCD; 800–1,200 kcal/day) can reduce total body weight by an average of 8% over 6 months and can help reduce abdominal fat.
(2) A very‐low‐calorie diet (VLCD; 250–800 kcal/day) produces greater initial weight loss than a LCD, but long‐term weight loss at > 1 year is similar with both diets.
(3) Aerobic exercises result in modest weight loss and may reduce abdominal fat in overweight and obese adults. It may also improve cardiorespiratory fitness.
(4) Reduced calorie intake and increased physical activity, when used in combination, produce greater weight loss than the use of either modality alone.
(5) When behavior therapy is used in combination with other weight loss approaches, it provides additional short‐term benefits.
NIH Obesity clinical guidelines‐ Key Points
Jindal et al.: Obesity and the Cardiorenal Metabolic Syndrome: Therapeutic Modalitiesand Their Efficacy in Improving Cardiovascular and Renal Risk Factors Cardiorenal Med 2012;2:314–327
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The EvidenceReport. National Institutes of Health. Obes Res 1998; 6(suppl 2):51S–209S.
(6) Pharmacological therapy for obesity should only be used as part of a comprehensive weight loss program (including diet and physical activity) for patients with a BMI of >30 with no concomitant obesity‐related risk factors, or for patients with a BMI of >27 with concomitant obesity‐related risk factors or diseases.
(7) Bariatric surgery is an option for severely obese patients (BMI > 40 or > 35 with comorbid conditions) who are at high risk of obesity‐related morbidity and who have failed a trial of less invasive interventions.
(8) The initial goal of weight loss therapy should be to reduce body weight by approximately 10% from baseline weight.
(9) Target weight loss should be approximately 1–2 pounds/week for a period of 6 months.
(10) Initially, moderate levels of physical activity for 30–45 min at least 3–5 days per week should be encouraged.
NIH Obesity clinical guidelines‐ Key Points
Jindal et al.: Obesity and the Cardiorenal Metabolic Syndrome: Therapeutic Modalitiesand Their Efficacy in Improving Cardiovascular and Renal Risk Factors Cardiorenal Med 2012;2:314–327
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The EvidenceReport. National Institutes of Health. Obes Res 1998; 6(suppl 2):51S–209S.
Key Elements Of Lifestyle Change
Increased Activity
Dietary Changes
Dietary Considerations
• Calorie level
•Macronutrient content
•Meal replacement products
Benefits of the Mediterranean Diet?
• Weight loss:• Meta analysis of 16 RCT’s with 3,436 patients examining diet for weight loss
demonstrated a significant effect on weight (-1.75 kg), BMI (-0.57 kg/m2), with greater reductions in the setting of energy restriction and increased physical activity
• CHD risk:• One systematic review of cohort and 43 RCT’s found a RR 0.34 for CHD and strong
causality association between Mediterranean Diet “pattern” (vegetables, legumes, nuts, fruits, whole grains, MUFA>SFA) and improved CHD risk among 146 cohort studies
• Dementia/Alzheimer’s Disease:• Prospective study of 1,180 elderly, NYC population followed for 5 years found that higher
adherence to Mediterranean style diet was independently associated with a lower HR of 0.60 for Alzheimer’s, equivalent to physical activity (HR 0.67)
Bays et. al. Journal of Clinical Lipidology (2013) 7, 304–383
Mediterranean Diet and Cardiovascular Disease:Historical Perspective and Latest Evidence Curr Atheroscler Rep (2013) 15:370
Mediterranean Diet and Risk for Alzheimer’s Disease Ann Neurol. 2006 June ,59(6) 912‐921
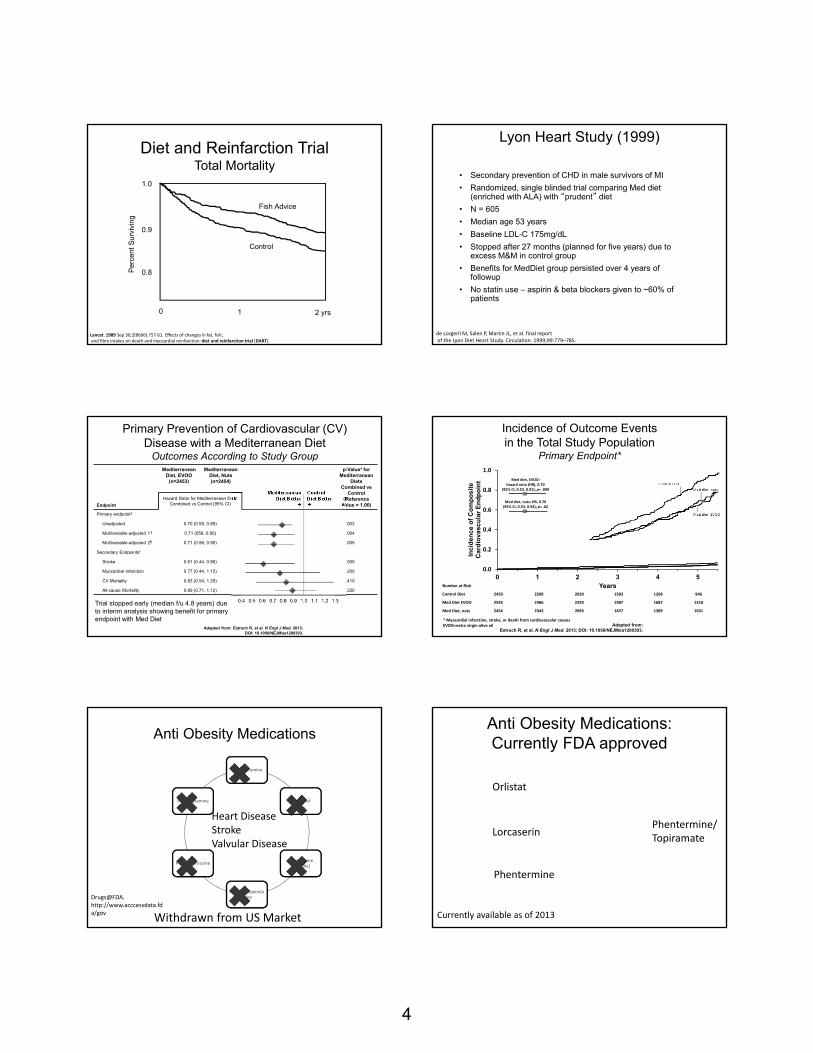
Diet and Reinfarction Trial: Methods
• Randomized, controlled, prospective
• Factorial design
• 2,033 men, <70 yo
• Allocated to receive (or not) advice to decrease fat intake to <30% energy, or
increase intake of fatty fish (200-400 g/wk), or
increase intake of dietary fiber to 18 g/d
• Followed for all-cause mortality for 2 yr
Lancet. 1989 Sep 30;2(8666):757‐61. Effects of changes in fat, fish,and fibre intakes on death and myocardial reinfarction: diet and reinfarction trial (DART).
4
1.0
0.9
0.8
0 1 2 yrs
Control
Fish Advice
Diet and Reinfarction TrialTotal Mortality
Per
cent
Sur
vivi
ng
Lancet. 1989 Sep 30;2(8666):757‐61. Effects of changes in fat, fish,and fibre intakes on death and myocardial reinfarction: diet and reinfarction trial (DART).
Lyon Heart Study (1999)
• Secondary prevention of CHD in male survivors of MI
• Randomized, single blinded trial comparing Med diet (enriched with ALA) with “prudent” diet
• N = 605
• Median age 53 years
• Baseline LDL-C 175mg/dL
• Stopped after 27 months (planned for five years) due to excess M&M in control group
• Benefits for MedDiet group persisted over 4 years of followup
• No statin use – aspirin & beta blockers given to ~60% of patients
de Lorgeril M, Salen P, Martin JL, et al. final reportof the Lyon Diet Heart Study. Circulation. 1999;99:779–785.
Endpoint
Mediterranean Diet, EVOO
(n=2453)
Mediterranean Diet, Nuts(n=2454)
Mediterranean Diet Better
Control Diet Better
p-Value† for Mediterranean
Diets Combined vs
Control(Reference
Value = 1.00)Hazard Ratio for Mediterranean Diets
Combined vs Control (95% CI)
Primary endpoint‡
Unadjusted 0.70 (0.55, 0.89) .003
Multivariable-adjusted 1§ 0.71 (056, 0.90) .004
Multivariable-adjusted 2¶ 0.71 (0.56, 0.90) .005
Secondary Endpointsǁ
Stroke 0.61 (0.44, 0.86) .005
Myocardial Infarction 0.77 (0.44, 1.15) .200
CV Mortality 0.83 (0.54, 1.29) .410
All-cause Mortality 0.89 (0.71, 1.12) .320
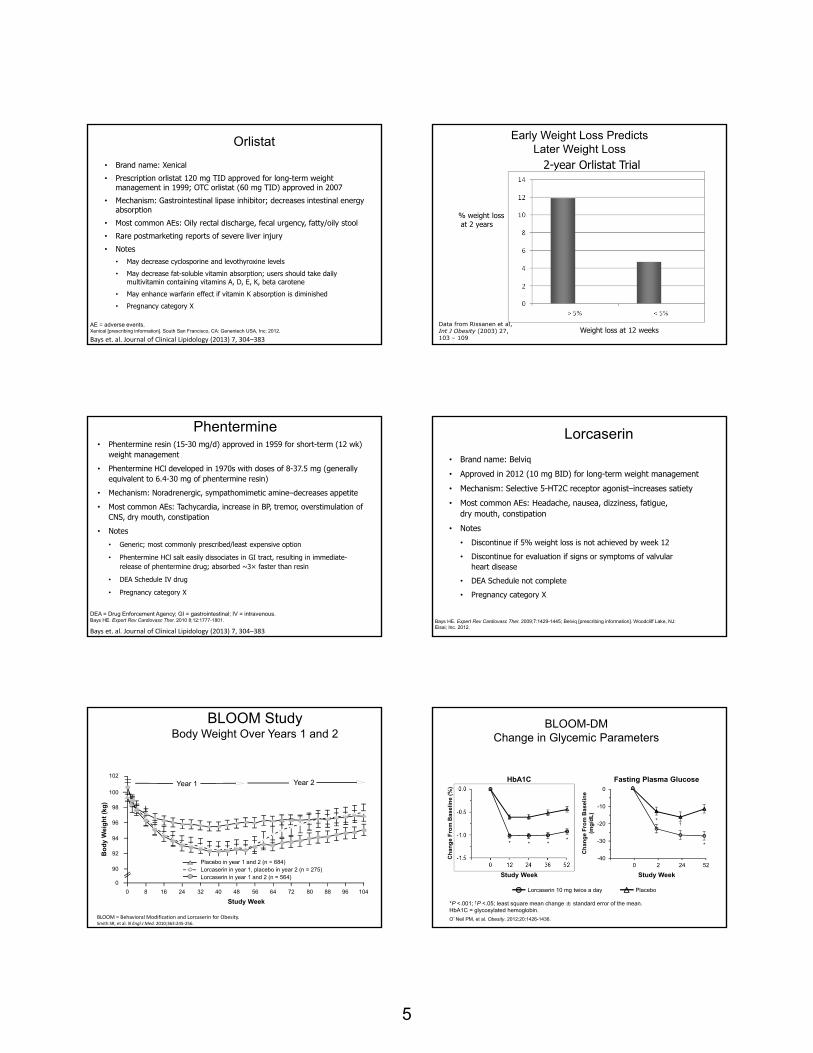
Primary Prevention of Cardiovascular (CV) Disease with a Mediterranean Diet
Outcomes According to Study Group
Adapted from: Estruch R, et al. N Engl J Med. 2013;DOI: 10.1056/NEJMoa1200303.
Trial stopped early (median f/u 4.8 years) due to interim analysis showing benefit for primary endpoint with Med Diet
Med diet, EVOO: hazard ratio (HR), 0.70
(95% CI, 0.53, 0.91); p= .009
Med diet, nuts: HR, 0.70(95% CI, 0.53, 0.94); p= .02
Incidence of Outcome Events in the Total Study Population
Primary Endpoint*
Adapted from:Estruch R, et al. N Engl J Med. 2013; DOI: 10.1056/NEJMoa1200303.
Number at Risk
Control Diet 2450 2268 2020 1583 1268 946
Med Diet EVOO 2543 2486 2320 1987 1687 1310
Med Diet, nuts 2454 2343 2093 1657 1389 1031
* Myocardial infarction, stroke, or death from cardiovascular causesEVOO=extra virgin olive oil
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5
Inc
ide
nc
e o
f C
om
po
sit
e
Car
dio
vasc
ula
r E
nd
po
int
Years
Control Diet
Med diet, nuts
Med diet, EVOO
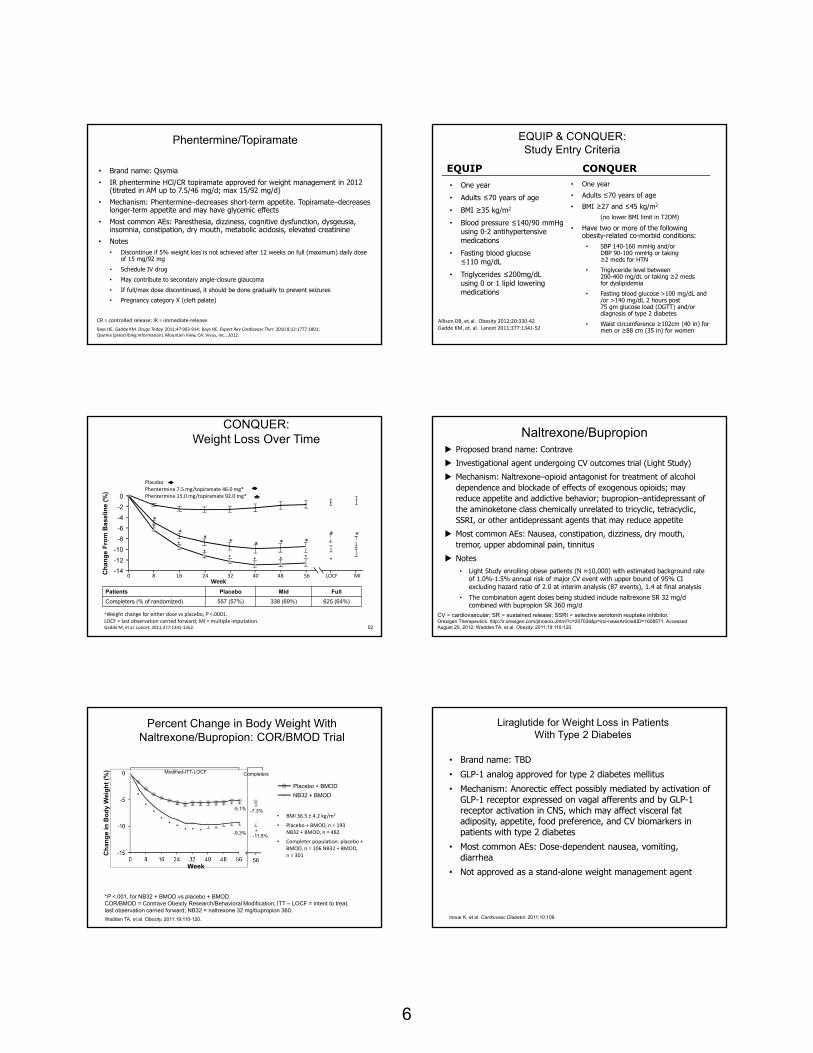
Anti Obesity Medications
D‐Fenfluramine
Mazindol
Sibutramine(Meridia)
Phenylpropanolamine
Phendimetrazine
Benzphetamine
Heart DiseaseStrokeValvular Disease
Withdrawn from US Market
Drugs@FDA. http://www.acccessdata.fda/gov
Anti Obesity Medications: Currently FDA approved
Orlistat
Lorcaserin
Phentermine
Currently available as of 2013
Phentermine/Topiramate
5
Orlistat
• Brand name: Xenical
• Prescription orlistat 120 mg TID approved for long-term weight management in 1999; OTC orlistat (60 mg TID) approved in 2007
• Mechanism: Gastrointestinal lipase inhibitor; decreases intestinal energy absorption
• Most common AEs: Oily rectal discharge, fecal urgency, fatty/oily stool
• Rare postmarketing reports of severe liver injury
• Notes• May decrease cyclosporine and levothyroxine levels
• May decrease fat-soluble vitamin absorption; users should take daily multivitamin containing vitamins A, D, E, K, beta carotene
• May enhance warfarin effect if vitamin K absorption is diminished
• Pregnancy category X
AE = adverse events.Xenical [prescribing information]. South San Francisco, CA: Genentech USA, Inc; 2012.
Bays et. al. Journal of Clinical Lipidology (2013) 7, 304–383
Early Weight Loss Predicts Later Weight Loss
2-year Orlistat Trial
% weight lossat 2 years
Weight loss at 12 weeksData from Rissanen et al,Int J Obesity (2003) 27, 103 – 109
Phentermine• Phentermine resin (15-30 mg/d) approved in 1959 for short-term (12 wk)
weight management
• Phentermine HCl developed in 1970s with doses of 8-37.5 mg (generally equivalent to 6.4-30 mg of phentermine resin)
• Mechanism: Noradrenergic, sympathomimetic amine–decreases appetite
• Most common AEs: Tachycardia, increase in BP, tremor, overstimulation of CNS, dry mouth, constipation
• Notes
• Generic; most commonly prescribed/least expensive option
• Phentermine HCl salt easily dissociates in GI tract, resulting in immediate-release of phentermine drug; absorbed ~3× faster than resin
• DEA Schedule IV drug
• Pregnancy category X
DEA = Drug Enforcement Agency; GI = gastrointestinal; IV = intravenous.Bays HE. Expert Rev Cardiovasc Ther. 2010 8;12:1777-1801.
Bays et. al. Journal of Clinical Lipidology (2013) 7, 304–383
Lorcaserin
• Brand name: Belviq
• Approved in 2012 (10 mg BID) for long-term weight management
• Mechanism: Selective 5-HT2C receptor agonist–increases satiety
• Most common AEs: Headache, nausea, dizziness, fatigue, dry mouth, constipation
• Notes
• Discontinue if 5% weight loss is not achieved by week 12
• Discontinue for evaluation if signs or symptoms of valvularheart disease
• DEA Schedule not complete
• Pregnancy category X
Bays HE. Expert Rev Cardiovasc Ther. 2009;7:1429-1445; Belviq [prescribing information]. Woodcliff Lake, NJ: Eisai; Inc. 2012.
BLOOM Study Body Weight Over Years 1 and 2
Study Week
BLOOM = Behavioral Modification and Lorcaserin for Obesity. Smith SR, et al. N Engl J Med. 2010;363:245‐256.
Bo
dy
We
igh
t (k
g)
Year 1
Placebo in year 1 and 2 (n = 684)Lorcaserin in year 1, placebo in year 2 (n = 275)Lorcaserin in year 1 and 2 (n = 564)
Year 2
0
102
100
98
96
94
92
90
10472 806448 564024 32160 8 88 96
Fasting Plasma Glucose
-40
-30
-20
-10
0
0 2 24 52
BLOOM-DMChange in Glycemic Parameters
HbA1C
*P <.001; †P <.05; least square mean change ± standard error of the mean.HbA1C = glycosylated hemoglobin.
O’Neil PM, et al. Obesity. 2012;20:1426-1436.
Ch
ang
e F
rom
Bas
elin
e (m
g/d
L)
Ch
ang
e F
rom
Bas
elin
e (%
)
Study WeekStudy Week
PlaceboLorcaserin 10 mg twice a day
* * **
*†
*
6
Phentermine/Topiramate
• Brand name: Qsymia
• IR phentermine HCl/CR topiramate approved for weight management in 2012 (titrated in AM up to 7.5/46 mg/d; max 15/92 mg/d)
• Mechanism: Phentermine–decreases short-term appetite. Topiramate–decreases longer-term appetite and may have glycemic effects
• Most common AEs: Paresthesia, dizziness, cognitive dysfunction, dysgeusia, insomnia, constipation, dry mouth, metabolic acidosis, elevated creatinine
• Notes• Discontinue if 5% weight loss is not achieved after 12 weeks on full (maximum) daily dose
of 15 mg/92 mg
• Schedule IV drug
• May contribute to secondary angle-closure glaucoma
• If full/max dose discontinued, it should be done gradually to prevent seizures
• Pregnancy category X (cleft palate)
CR = controlled release; IR = immediate‐release.
Bays HE, Gadde KM. Drugs Today. 2011;47:903‐914; Bays HE. Expert Rev Cardiovasc Ther. 2010 8;12:1777‐1801;Qsymia [prescribing Information]. Mountain View, CA: Vivus, Inc.; 2012.
EQUIP & CONQUER: Study Entry Criteria
• One year
• Adults ≤70 years of age
• BMI ≥35 kg/m2
• Blood pressure ≤140/90 mmHg using 0-2 antihypertensive medications
• Fasting blood glucose ≤110 mg/dL
• Triglycerides ≤200mg/dL using 0 or 1 lipid lowering medications
• One year
• Adults ≤70 years of age
• BMI ≥27 and ≤45 kg/m2
(no lower BMI limit in T2DM)
• Have two or more of the following obesity-related co-morbid conditions:
• SBP 140-160 mmHg and/or DBP 90-100 mmHg or taking ≥2 meds for HTN
• Triglyceride level between 200-400 mg/dL or taking ≥2 meds for dyslipidemia
• Fasting blood glucose >100 mg/dL and /or >140 mg/dL 2 hours post 75 gm glucose load (OGTT) and/or diagnosis of type 2 diabetes
• Waist circumference ≥102cm (40 in) for men or ≥88 cm (35 in) for women
EQUIP CONQUER
Allison DB, et.al. Obesity 2012;20:330‐42Gadde KM, et. al. Lancet 2011;377:1341‐52
*
*****
*
* ****
* ***
0 8 16 24 32 40 48 56 LOCF MI
CONQUER: Weight Loss Over Time
52
*
*
Ch
an
ge
Fro
m B
as
elin
e (
%)
0
-2
-4
-6
-8
-10
-12
-14
Week
PlaceboPhentermine 7.5 mg/topiramate 46.0 mg*Phentermine 15.0 mg/topiramate 92.0 mg*
Patients Placebo Mid Full
Completers (% of randomized) 557 (57%) 338 (69%) 625 (64%)
*Weight change for either dose vs placebo, P <.0001.LOCF = last observation carried forward; MI = multiple imputation.Gadde M, et al. Lancet. 2011;377:1341‐1352.
Naltrexone/Bupropion Proposed brand name: Contrave
Investigational agent undergoing CV outcomes trial (Light Study)
Mechanism: Naltrexone–opioid antagonist for treatment of alcohol dependence and blockade of effects of exogenous opioids; may reduce appetite and addictive behavior; bupropion–antidepressant of the aminoketone class chemically unrelated to tricyclic, tetracyclic, SSRI, or other antidepressant agents that may reduce appetite
Most common AEs: Nausea, constipation, dizziness, dry mouth, tremor, upper abdominal pain, tinnitus
Notes• Light Study enrolling obese patients (N ≈10,000) with estimated background rate
of 1.0%-1.5% annual risk of major CV event with upper bound of 95% CI excluding hazard ratio of 2.0 at interim analysis (87 events), 1.4 at final analysis
• The combination agent doses being studied include naltrexone SR 32 mg/d combined with bupropion SR 360 mg/d
CV = cardiovascular; SR = sustained release; SSRI = selective serotonin reuptake inhibitor.Orexigen Therapeutics. http://ir.orexigen.com/phoenix.zhtml?c=207034&p=irol-newsArticle&ID=1608571. Accessed August 20, 2012; Wadden TA, et al. Obesity. 2011;19:110-120.
*****
Percent Change in Body Weight With Naltrexone/Bupropion: COR/BMOD Trial
• BMI 36.5 ± 4.2 kg/m2
• Placebo + BMOD, n = 193 NB32 + BMOD, n = 482
• Completer population: placebo + BMOD, n = 106 NB32 + BMOD, n = 301
*P <.001, for NB32 + BMOD vs placebo + BMOD. COR/BMOD = Contrave Obesity Research/Behavioral Modification; ITT – LOCF = intent to treat, last observation carried forward; NB32 = naltrexone 32 mg/bupropion 360.
Wadden TA, et al. Obesity. 2011;19:110-120.
Ch
an
ge
in B
od
y W
eig
ht
(%)
Completers
NB32 + BMOD
Placebo + BMOD
56Week
Modified-ITT-LOCF
*
-7.3%
-11.5%
-5.1%
-9.3%
*
*****
**
*
Liraglutide for Weight Loss in Patients With Type 2 Diabetes
• Brand name: TBD
• GLP-1 analog approved for type 2 diabetes mellitus
• Mechanism: Anorectic effect possibly mediated by activation of GLP-1 receptor expressed on vagal afferents and by GLP-1 receptor activation in CNS, which may affect visceral fat adiposity, appetite, food preference, and CV biomarkers in patients with type 2 diabetes
• Most common AEs: Dose-dependent nausea, vomiting, diarrhea
• Not approved as a stand-alone weight management agent
Inoue K, et al. Cardiovasc Diabetol. 2011;10:109.

7
Effect of Obesity Drugs on LipidsAverage Changes from Baseline
Total Cholesterol LDL-C Triglycerides HDL-C
Orlistat ↓ 2% ↓ 4% ↑ 1% ↑ 9%
Lorcaserin ↓ 1% ↑ 2% ↓ 5% ↑ 2%
Phentermine/ Topiramate
↓ 6% ↓ 8% ↓ 5% ↑ 4%
Xenical Package Insert. Genentech USA, Inc., South San Francisco, CA: January 2012.Belviq Package Insert. Arena Pharmaceuticals, Woodcliff Lake, NJ: June 2012.
Qsymia Package Insert. VIVUS Inc., Mountain View, CA: July 2012. 58
Summary
• Obesity /Overweight continues to be a problem worldwide associated with Cardiometabolic Risk
• Theraputic interventions include lifestyle, bariatric surgery and pharmacologic therapies
• Weight loss vs. Preventing Weight Gain may be important issues
• Dietary Interventions can cause short term weight loss, and some long term CV benefits
• Pharmacologic intervention for weight loss should be used with an understanding of potential cardiometabolic benefits.
Hypertension and Obesity
Still Waters Run Deep
Robert Gleeson, MD, FACP, FNLA
Medical College of Wisconsin
Preventive Cardiology and Lipid Management
Does Preventive Cardiology Make a Difference?
Why does preventive cardiology matter?
1. Since 1960, has worked to identify the major causes of atherosclerosis and CAD
2. Identified treatments that lowered the risk factor and CAD
3. Wrote guidelines for best treatment
But cardiovascular disease remains the leading cause of premature
morbidity and mortality
The American Society for Preventive Cardiology is proud to continue the fight to prevent cardiovascular disease.
Please join us in our journey.
Together we can work to prevent atherosclerosis.
aspconline.org

8
Key Points about Obesity
1. Obesity increases risk of all CVD risk factors, events, and mortality
2. Obesity increases hypertension, which is largely untreated
3. Treating hypertension in the obese patient lowers risk of CVD events
4. Treating obesity lowers hypertension and improves other CV risk factors
Measuring BP in the Obese
• A standard BP cuff over-estimates BP in obese
• For every 5 cm increase in arm circumference, the BP increases 3/2 mm
• Standard cuff fits 9 to 13 inches circumference
• Large cuff fits 13 to 17 inches circumference
Regardless of etiology,hypertension increases
• CV deaths
• Coronary artery disease
• Stroke
• Peripheral artery disease
• Heart failure
• Valvular heart disease
Hypertension and CVD
• BP has a continuous, graded, and linear effect on CVD with a nadir of 115/75
• Above that, CVD events and mortality double for every
• 20 mm increase in systolic
• 10 mm increase in diastolic
• 66% of CHD deaths occur in men with systolic BP between 130 and 159
Stamler et al Lancet 2002
Obesity and Hypertension
• 75% of hypertension is related to obesity1
1. Krus et al e Circ 1998
BMI Prevalence of HBP %NHANES 2005 to 2008
< 25 15.3
25‐30 27.8
30 42.5
Hypertension in obesity
• Only 30% of hypertension in obese is treated adequately
Kurukulasuriya LR et al. Med Clin North Am 2011 Sep;95(5):903‐17
9
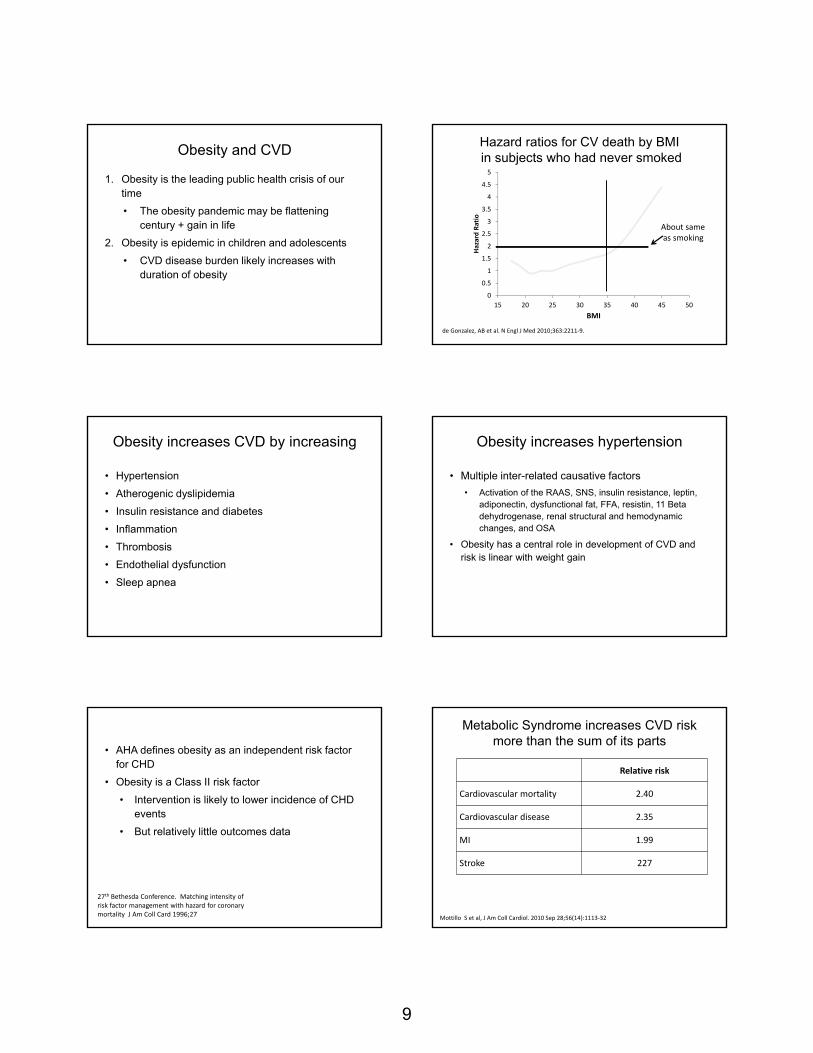
Obesity and CVD
1. Obesity is the leading public health crisis of our time
• The obesity pandemic may be flattening century + gain in life
2. Obesity is epidemic in children and adolescents
• CVD disease burden likely increases with duration of obesity
Hazard ratios for CV death by BMIin subjects who had never smoked
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
15 20 25 30 35 40 45 50
Hazard Ratio
BMI
de Gonzalez, AB et al. N Engl J Med 2010;363:2211‐9.
About sameas smoking
Obesity increases CVD by increasing
• Hypertension
• Atherogenic dyslipidemia
• Insulin resistance and diabetes
• Inflammation
• Thrombosis
• Endothelial dysfunction
• Sleep apnea
Obesity increases hypertension
• Multiple inter-related causative factors
• Activation of the RAAS, SNS, insulin resistance, leptin, adiponectin, dysfunctional fat, FFA, resistin, 11 Beta dehydrogenase, renal structural and hemodynamic changes, and OSA
• Obesity has a central role in development of CVD and risk is linear with weight gain
• AHA defines obesity as an independent risk factor for CHD
• Obesity is a Class II risk factor
• Intervention is likely to lower incidence of CHD events
• But relatively little outcomes data
27th Bethesda Conference. Matching intensity of risk factor management with hazard for coronary mortality J Am Coll Card 1996;27
Metabolic Syndrome increases CVD risk more than the sum of its parts
Relative risk
Cardiovascular mortality 2.40
Cardiovascular disease 2.35
MI 1.99
Stroke 227
Mottillo S et al, J Am Coll Cardiol. 2010 Sep 28;56(14):1113‐32

10
Is overweight with normal risk factors still a risk?
• Yes.
• They still had impaired vaso-reactivity, increased LV mass, impaired clotting1
• No
• 22.000 hypertensive patients with CHD2
1. Lind ATVB 2011;312. Uretsky Obesity Paradox Am J Med 2007;120
BMI HR
20-25 1.0
25 - 30 0.77
30 - 35 0.68
Overweight versus waist measurement
• At every BMI and in both men and women, the risk of cardiovascular disease is increased by increasing abdominal fat
• WHR is better predictor of CVD than BMI
Waist measurement
• Increased risk for HBP, diabetes, dyslipidemia if
• Caucasian and Blacks M > 40 F > 35
• S. Asian and Japanese M > 35 F > 31
• Most useful if BMI 25 to 35
• If BMI > 35, waist measurement adds little predictive value
Waist to hip ratio WHR fromNurses Health Study
• Normal
• Men: WHR < 0 .9
• Women < 0.8
• A larger WHR is always worse
• Females:
• WHR > 0.88 compared to WHR < 0.72 has HR of CHD = 3.2
• Even if BMI normal (20 to 25), a WHR > 0.76 compared to WHR < 0.76 has a HR of CHD = 2
Rexrode JAMA 1988;280
Treating obesity to lower blood pressure
1. Lose weight
2. Lose weight and exercise more
3. Treat BP and CV risk factors
4. Lose weight, exercise more, and treat the BP
5. Major social campaigns like the no smoking campaigns
6. All of the above
Weight-loss and BP mixed results
• Weight-loss diets lower BP best
• Diet weight loss of 4 kg lowers BP 6/3 mm Hg
• Some weight-loss meds lower BP, some raise
• Orlistat lowers BP but not as much as diet
• Sibutramine no effect
• Roux-en-Y gastric bypass lowers BP, but not as much as anticipated
• Liposuction no effect on BP
Horvath Arch Med 2008 commentary

11
Benefits of Weight Loss
• 5% weight loss is associated with reduction of
• angiotensinogen levels by 27%
• renin by 43%
• aldosterone by 31%
• angiotensin-converting enzyme activity by 12%
• angiotensinogen expression by 20% in adipose tissue
Engeli S et al. Hypertension. 2005 Mar;45(3):356‐62.
Weight loss options
• Commercial weight-loss programs
• Work quite well, may be sustainable
• Diet and exercise
• Necessary to do both, but sustaining is hard
• Pharmaceuticals
• All short-term and with side effects
• Surgery, esp. bariatric surgery
• Long-term benefit, but need compliant patient
National Weight Control Registry predictors of successful long-term weight control
1. Self-monitoring of weight
2. Consumption of a low-fat diet
• Different macronutrient components of diet are less important than over-all calorie restriction
3. Daily physical activity of approximately 60 minutes
4. Minimal sedentary “screen time”
5. Eating most meals at home
National Weight Control Registry
Major difficulty of weight loss
• “Body weight and body fat are tenaciously regulated.” emedicine on obesity options
• When patients lose weight by dieting, their total and resting energy expenditure also drop in an effort to conserve energy.
• The only way to counteract this drop is to increase activity levels
Treating hypertension in the obese
Anti-hypertensives in the obese
It’s the lower BP, not the drugs that matter
Treat high-risk obese when BP > 130/80
Landsberg et al J Clin Hyperten Jan 213

12
Anti-hypertensives in the obese
Most of the anti-hypertensive benefit comes from the lowest dose of the drug
Treating hypertension in obese according toJan 2013 statement of ASH and Obesity Society
• Target < 140/90 unless DM, CKD and then aim for < 130/80
• RAAS inhibition
• ACE or ARB
• CCB
• Diuretics
• Low-dose thiazide or thiazide like agents
• Loop diuretics if required
• Potassium sparing agents
• Avoid beta-blockers except for specific cardiac indication
• All agents are potentiated by weight loss
Treating hypertension in obese patients cont’d
• Beta-blockers and thiazides both increase insulin resistance and diabetes
• Thiazide diuretics increase dyslipidemia associated with obesity
• If use thiazides, use low dose like 12.5 to 25 mg of HCTZ or chlorthalidone
• Beta blockers cause insulin resistance and weight gain
• Limit beta blockers to post MI or HF
Summary
1. Obesity increases risk of hypertension
2. The combination substantially increases the risk of CVD
3. Treating hypertension in the obese requires treating the obesity as part of the therapeutic plan
1. Lifestyle management is required for every case
4. Lower HBP in the obese is essential to reduce risk of CVD
Question & Answer