managing problems complications
TRANSCRIPT

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 1/66
MANAGING PROBLEMS AND
COMPLICATIONS
PART I IIKhaled Q Al Hamad
BDS MSc MRD RCSEd
4 th
year, Dent 445

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 2/66
References
1. Complete Prosthodonticsproblems, diagnosis, and management
(Grant, Heath, McCord)
Chapter: Problem solving
2. Lecture notes

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 3/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
► Lack of peripheral seal.► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit► Denture not sited in optimal space( also neuro muscular control)
Problems in occlusion Support problems
1. Lack of ridge
2. Bony prominence
► Non- resilient soft tissue► Pain- avoidance mechanisms
• Comfort
• Speech
• Psychological
• Other.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 4/66
Appearance
►May arise at the delivery visit !
► Arise when communication has broken down.
►May arise. when relative dislikes the results.
The the try-in home
Or ask the pt to bring his relative at the try-in
►Solutions:
Shade: staining or resetting
Teeth positions: grinding or repositions
Polished surface: grinding
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 5/66
Looseness of dentures
► especially in the lower.
Due to atrophic Mandibular ridge
Solved may be by placing implants.
►Patients may describe this as:
Rocking
Falling
Lifting or rising
Too big
Bulky and occupy too much space..

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 6/66
► Upper denture mostpossess a seal to preventeasy access of air andsaliva to impressionsurface. Seal has two
components: Buccal & labial flanges
should fill functional depthand width of the sulci.
Seal across posterior bordershould be effective.
► It may be possible todevelop similar seal aroundthe lower.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 7/66
Examining the seal
►Upper:
Labial & buccal border: pull down on anteriorteeth
Post dam: pull out on incisors
Distobuccal sulcus and tuberosity: pull out oncanine on the contra lateral side.
►Lower: Left with tip of probe placed in the anterior
interdental area.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 8/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
► Lack of peripheral seal.► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit► Denture not sited in optimal space( also neuro muscular control)
Problems in occlusion Support problems
1. Lack of ridge
2. Bony prominence
► Non- resilient soft tissue► Pain- avoidance mechanisms
• Comfort
• Speech
• Psychological
• Other.
L k f i h l l

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 9/66
Lack of peripheral sealborder under extension in length &
width►Presentation
On delivery
When speaking
When eating When opening wide
After adjustment
►Examination:
Direct vision
Diagnostic addition oftracing compound

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 10/66
► Overcoming
Adding tracing compond torelevant borders, mould andtrim excess. Send to the lab
for the compound to bereplaced with acrylic.
For semi-permanent option:modify in a similar mannerby adding butyl
methacrylate resin-providebutt joint between old andnew resin
► Avoiding:
Proper primary & secondary
impression. Proper pouringand re aration of the cast-

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 11/66
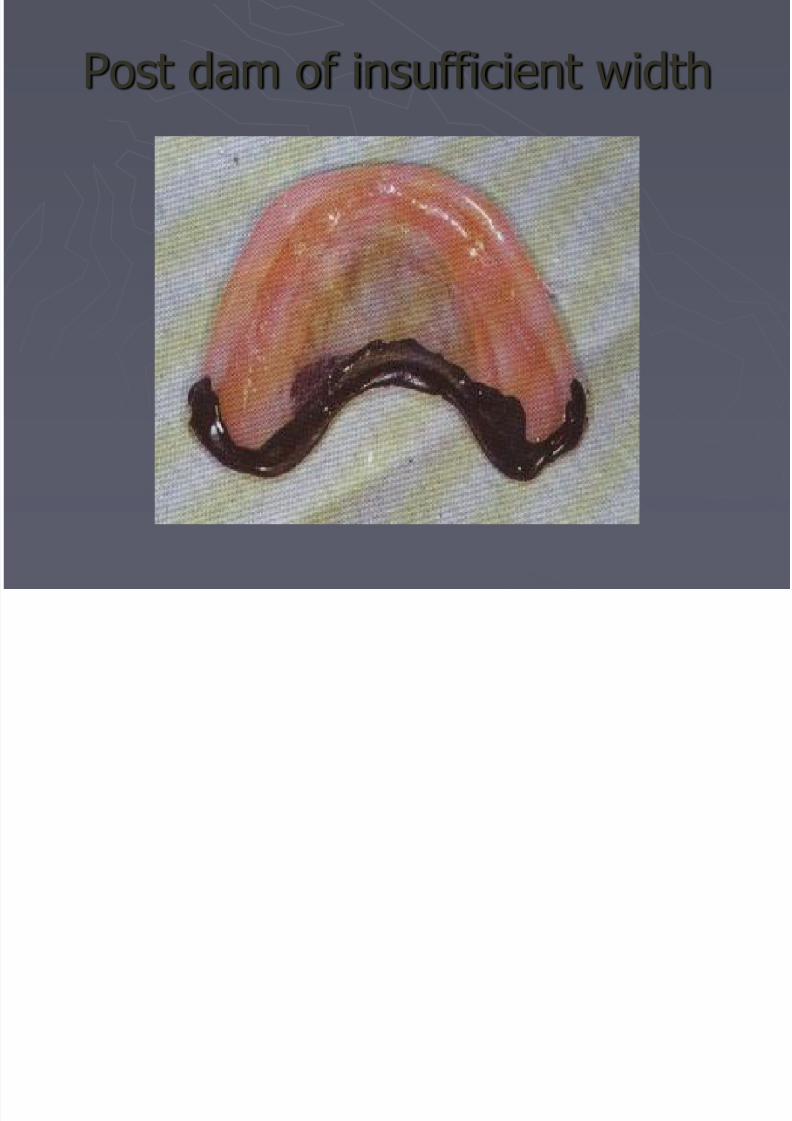
Posterior border of upper denture
► Recognizing
Observe soft palate movementwhen say “aah”
Diagnostic addition of tracingcompound
► Management Over-extension: adjust the add
post dam as below
Under-extension: extend borderwith tracing compound andrefine fit with wash impression.
Cut grooves for post dam inmaster cast.
► Avoiding
See picture
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 12/66
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 13/66
►Causes of Lack of Retention
Decreased retentive forces
►Lack of peripheral seal.
► Air beneath the impression surface
►Xerostomia
►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )
►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 14/66
Decreased retentive forces- lack ofseal
►Torus where the post dam should be sited.
Note junction line between mobile and non mobiletissues. Palpate to determine size of torus and
displaceability of tissues anterior and posterior to it. Adjust borders until optimal seal achieved. Replace postdam.
►Resorption of residual ridge
Recognizing:►Lapse of time
►Denture may rock with finger pressure
►Fibrous displasia due to denture overextension

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 15/66
►Management If polished surface acceptable, teeth in neutral
zone, free way space not more than 6mm, and
occlusion satisfactory, then reline denture► Avoiding
Prolong wearable life of immediate denture byrepeated relining with tissue conditioner (3
weeks maximum ). Review complete denture yearly to determine
the need for reline/remake.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 16/66
►Inelasticity of cheeks (aging, scleroderma,
submucous fibrosis)
Recognizing
►Patient medical history
►Observation of mobility of tissues
►Palpation of displaceability of lips and cheeks Management
► Adjust borders by adding tracing compound and thenreplacing it with acrylic.
Avoiding►Proper border moulding
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 17/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
►Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 18/66
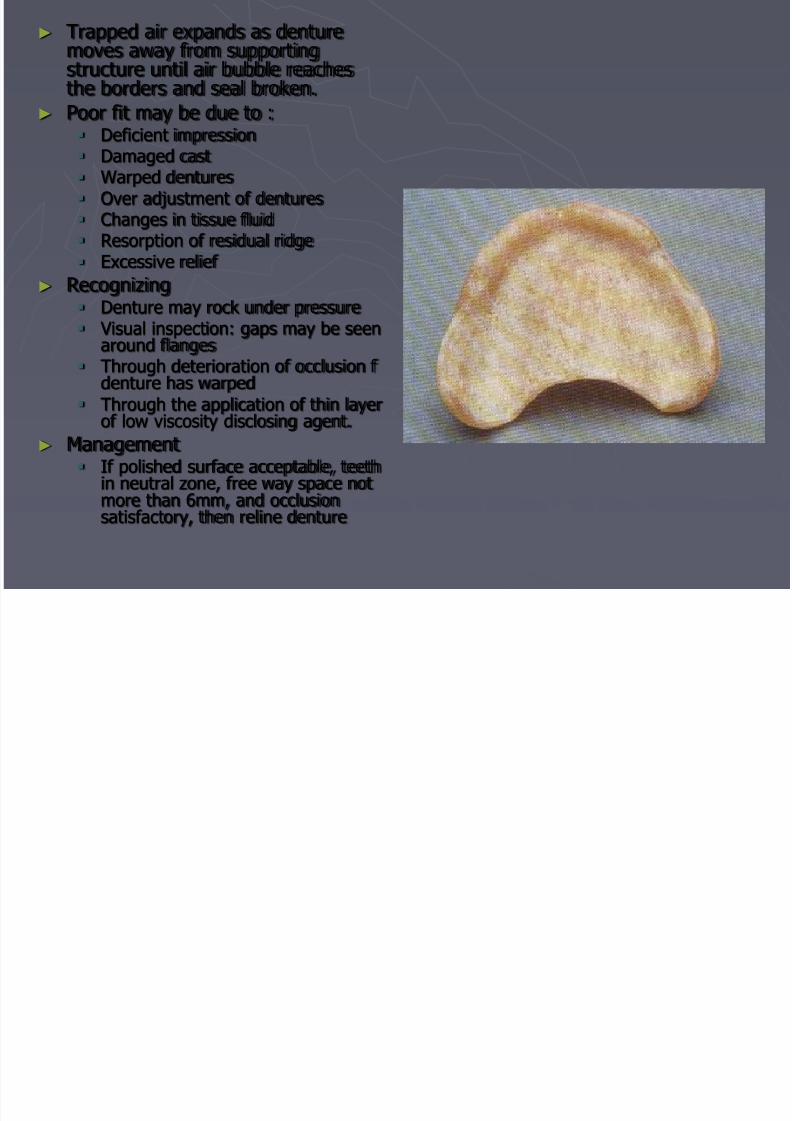
► Trapped air expands as denturemoves away from supportingstructure until air bubble reachesthe borders and seal broken.
► Poor fit may be due to :
Deficient impression Damaged cast Warped dentures Over adjustment of dentures Changes in tissue fluid Resorption of residual ridge Excessive relief
► Recognizing Denture may rock under pressure Visual inspection: gaps may be seen
around flanges Through deterioration of occlusion f
denture has warped Through the application of thin layer
of low viscosity disclosing agent.► Management
If polished surface acceptable, teethin neutral zone, free way space notmore than 6mm, and occlusionsatisfactory, then reline denture

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 19/66
►Management If polished surface acceptable, teeth in neutral zone,
free way space not more than 6mm, and occlusion
satisfactory, then reline denture. Before taking theimpression, relieve heavy contacts.
► Avoiding When making the 2nd impression ensure:
►Uniform thickness of impression material achieved►No pressure from tray
►Impression poured before distortion occurs.
►Borders are adequately supported
Cast must not be over trimmed or damaged
Optimum curing cycle used.
Denture must not be heated when trimmed and not becleaned through boiling.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 20/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
►Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 21/66
► Changes in tissue fluid Lack of recovery from old
denture(90 min gap)
Medications (diuretics)
Heart failure
► management If prolonged seating
pressure by cotton pelletsrestore retention,reline/rebase using minimumpressure technique.
consult with the physician Ensure old denture not worn
for 90 minutes before theimpression

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 22/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
►Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 23/66
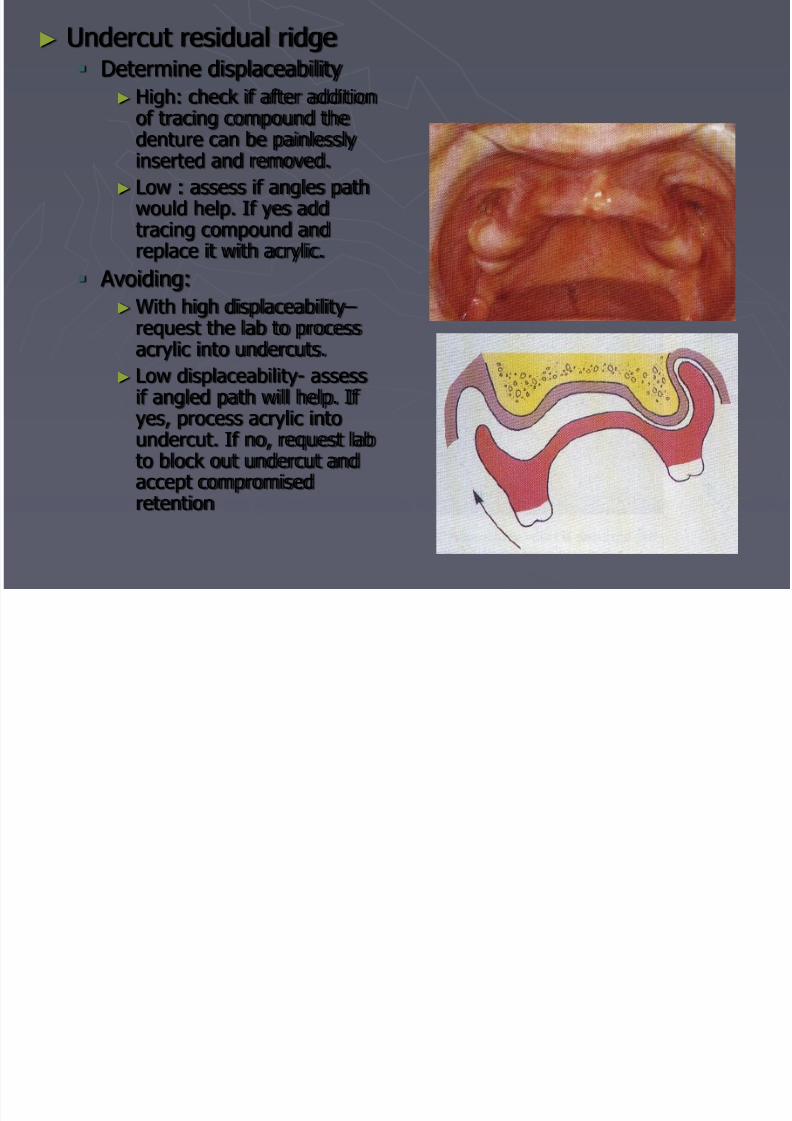
► Undercut residual ridge Determine displaceability
► High: check if after additionof tracing compound the
denture can be painlesslyinserted and removed.
► Low : assess if angles pathwould help. If yes addtracing compound andreplace it with acrylic.
Avoiding:►With high displaceability –
request the lab to processacrylic into undercuts.
► Low displaceability- assessif angled path will help. If
yes, process acrylic intoundercut. If no, request labto block out undercut andaccept compromisedretention

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 24/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
►Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 25/66
► Excessive relief over areasof reduced displaceability Recognizing
► Palpate area and compare itwith amount of relief
provided► Use disclosing material.
Management► Reline/rebase: outline area
to be relived on the casts oron the impression andindicate amount of relief.
Avoidance► outline area to be relived on
the casts or on theimpression and indicateamount of relief.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 26/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit
Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
► Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 27/66
XEROSTOMIA
► Lack of saliva due to or disease of salivary gland
Medications
Irradiation of the head and neck
►Reduce ability to form seal along borders.
►Management Consider prescribing
►Sugar free acidic sweets, chewing gums, artificial saliva. Consult with the physician.
Design denture to maximize retentive forces andminimize displacing forces.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 28/66
►Causes of Lack of Retention Decreased retentive forces
►Lack of peripheral seal.► Air beneath the impression surface
Poor fit
Changes in tissue fluid
Undercut residual ridge
Excessive relief over areas of reduced displaceability
►Xerostomia►Neuromuscular control
Increased displacing forces►Denture border problems (over extension )►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 29/66
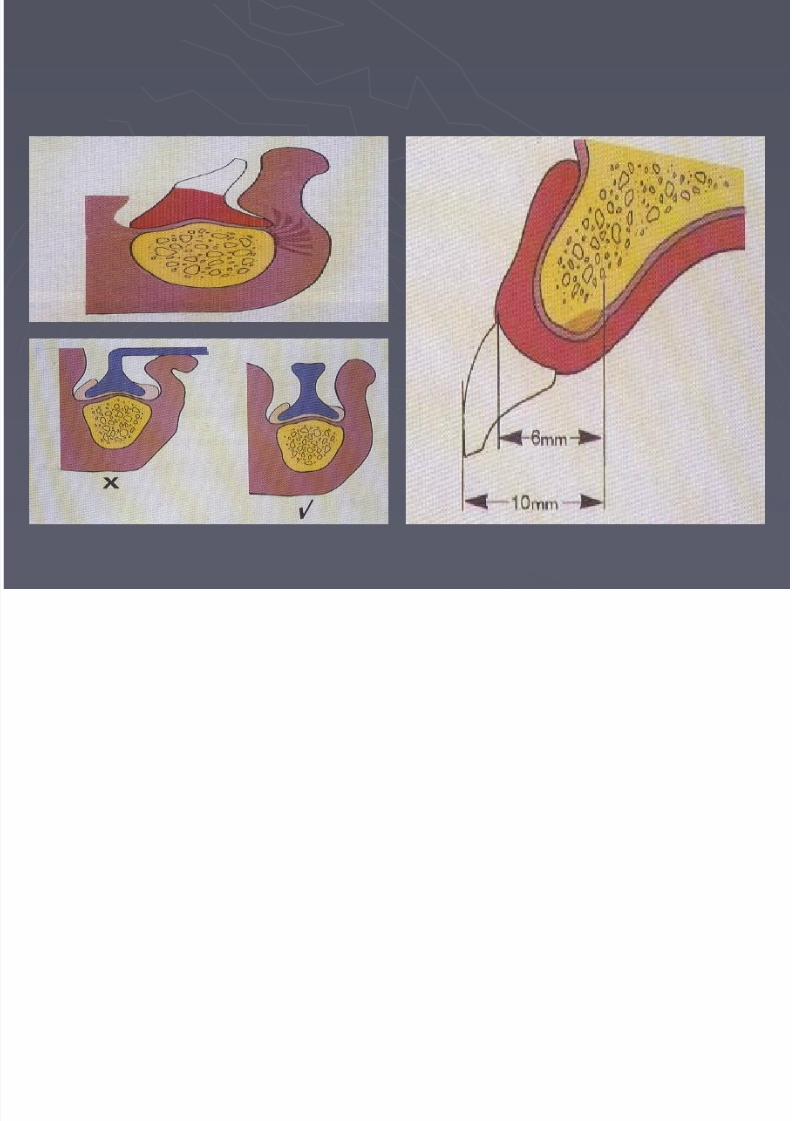
► Basic shape of dentureincorrect. cross section of theposterior region should betriangular. Occlusal surface sited
within confines of borders andpolished surfaces being slightlyconcave
► Recognizing
Lower molar too linguallyplaced.
Lingual polished surface convex
Upper buccal flangeinsufficiently wide.
► Management
Narrow lower teeth lingually
Adjust lingual polished surface
Add tracing compound to adjustbuccal flange
Decreased retentive

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 30/66
Decreased retentiveforces/Neuromuscular control
►Other causes Motor neuron disorder
►Presentation:
On delivery
On eating On speaking
After adjustment
Change in shape to the old dentures►Try to adjust dentures to be similar to the old ones.
►Consider template techniques
High Occlusal plane on lower denture
Patient des not appreciate the need for active control.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 31/66
High Occlusal plane
► Recognizing
Usually associated with high VD if the upper incisal levelis correct
► Management If upper occlusal plane
correct hen:
► If increased VD is under 1.5mm: mount on the
articulator and adjust lowerusing selective grinding
► If more than 1.5mm : resett the correct VD
Patient des not appreciate the need

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 32/66
Patient des not appreciate the needfor active control.
► Recognizing Ask patient to close on your
finger by the anterior teethand observe position of thetongue. Ideally should take
the position shown on thefigure.
► Management Train the patient to use his
tongue to retain the denture
by placing small beading ofresin on the posterior borderof the upper and lingual tothe anteriosr.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 33/66
► When patient has beenwith out posterior teeth,tongue adapts to increasedavailable space.
► Consider Use of small occlusal table
Remove most distal posteriorteeth
Consider using specialimpression techniques:neutral zone technique.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 34/66
► Causes of Lack of Retention Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface Poor fit
Changes in tissue fluid Undercut residual ridge Excessive relief over areas of reduced displaceability
► Xerostomia
►Neuromuscular control
Increased displacing forces
►Denture border problems (over extension in length & width)► Poor fit to supporting structures
► Deep post dam
►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 35/66
Increased Displacing Forces
► Overextension (in length) : Recognition
► Direct vision and gentle manipulation of cheeks and lips, andmovement of the tongue.
► Look for sign of inflammation t the reflection of the sulcus.
► Overextension (in width): Buccal to tuberosities (encroachment on coronoid)
Lingual & labial flanges: if thick could be lifted by the tongue andmentalis
► Management Reduce bulk- use disclosing agent if needed- and repolish
► Avoidance: Proper border moulding and impressioning.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 36/66
► Causes of Lack of Retention Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface Poor fit
Changes in tissue fluid Undercut residual ridge Excessive relief over areas of reduced displaceability
► Xerostomia
►Neuromuscular control
Increased displacing forces
► Denture border problems (over extension in length & width)►Deep post dam
► Poor fit to supporting structures
►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 37/66
►Deep post dam
Recoil of tissues pushes denture downwards
Recognizing►Pt complain of pain in region of the post dam.
►Deep groove in palatal tissues with inflammationranging from hyperemia to ulceration.
Management►Reduce depth-use disclosing agent if needed- be
aware of over reduction as the tissues may heal andlack of seal may develop

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 38/66
► Causes of Lack of Retention Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface Poor fit
Changes in tissue fluid Undercut residual ridge Excessive relief over areas of reduced displaceability
► Xerostomia
►Neuromuscular control
Increased displacing forces
► Denture border problems (over extension in length & width)► Deep post dam
► Poor fit to supporting structures
►Occlusal problems
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 39/66
►Poor fit to supporting structures
Recoil of displaced tissues lifts denture.
Recognizing►Denture falls when teeth not in contact.( not to be
confused with overextension or denture not sited inoptimal space)
Management►If polished surface acceptable, teeth in neutral zone,
free way space not more than 6mm, and occlusionsatisfactory, then reline denture-using minimal
pressure technique. Before taking the impression,relieve heavy contacts and ensure old dentures notworn for 90 minutes before making the impression
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 40/66
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 41/66
► Causes of Lack of Retention Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface Poor fit
Changes in tissue fluid Undercut residual ridge Excessive relief over areas of reduced displaceability
► Xerostomia
►Neuromuscular control
Increased displacing forces
► Denture border problems (over extension in length & width)► Deep post dam
► Poor fit to supporting structures
►Occlusal problems

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 42/66
►Uneven Initial Contacts
causes dentures to tilt on supporting tissues, thusdisrupting retentive seal. Also prevents even seating of
loosening dentures on supporting tissues when teethoccluded.
Recognizing:
►ask patient to close slowly into RCP until teeth just touch
Management► Aim is to adjust occlusion until even contact in RCP is achieved.
Minor errors: use chair side techniques- difficult as dentures moveon supporting tissues producing errors in markings
Major errors: use laboratory techniques. Remount the maxillary
denture on semi adjustable articulator using a face bow and theMandibular denture with Pre-tooth contact registration. Thenadjust the occlusion on the articulator using articulating paper.
Gaps more than 1.5mm (vertically) or errors in antero-posteriorrelation more than half a cusp require cannot be adjusted by
selective grinding and requires re setting.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 43/66
k f f d b &

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 44/66
► Lack of freedom between RCP & ICP Patient with inaccurate control of Mandibular movement
may not adapt to exact cusp-fossa relationship casingdentures to move and disrupt peripheral seal.
Recognizing► Age/ medical history: patient has difficulty in achieving
reproducible occlusal relationship. Patient able to eat using olddentures with flattened, worn teeth.
Management►Remount dentures, adjust teeth to produce area of freedom. If
adjustment will result in loss of occlusal balance, reset/remakeusing cuspless teeth.
Avoidance► Always allow 1-1.5mm of easy anterior movement of mandible
from RCP.►Consider use of cuspless teeth (non-anatomic) teeth set in
occlusal balance during lateral and protrusive movement (thisproduces no vertical overlap- possible effect on aesthetics)
► Lack of occlusal balance in excursive movements

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 45/66
► Lack of occlusal balance in excursive movements Causes dentures to shift on supporting tissues and
disrupt retentive seal. Many patient wear denturesuccessfully without occlusal balance, however, as
retentive forces decreases , displacing forces generatedby lack of balance assume greater significance.
Recognizing►Hold the dentures in place on supporting tissues. Request
patient to close until teeth just touch, then to „rub‟ from one
side to side and forwards. By observation, note if teeth slideeasily without causing dentures to move over supportingtissues.
Lack of balance commonly associated excessive vertical overlap ofanterior teeth.
Management
► Adjust teeth until balancing contacts us achieved. Could bedone chair side, but remount procedures is preferred. Ifachievement of balancing contacts would necessitate mutilationof teeth ( excessive shortening of lower incisors) then resetteeth or remake dentures.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 46/66
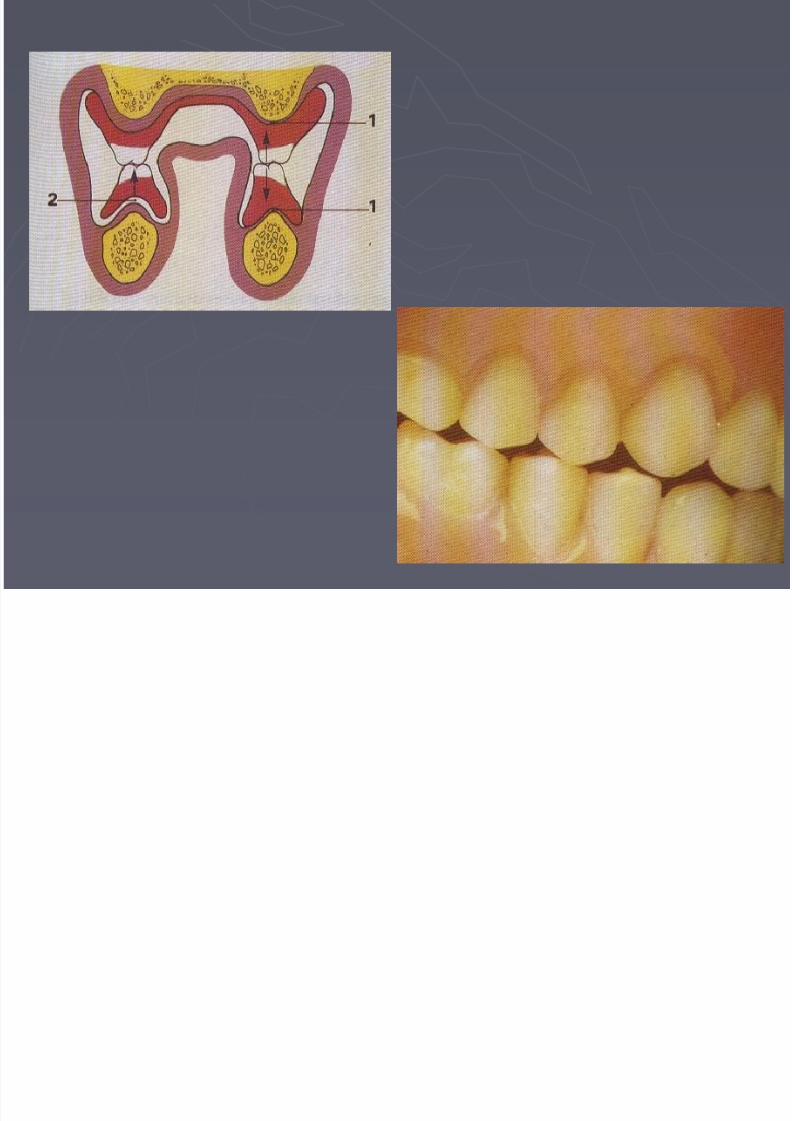
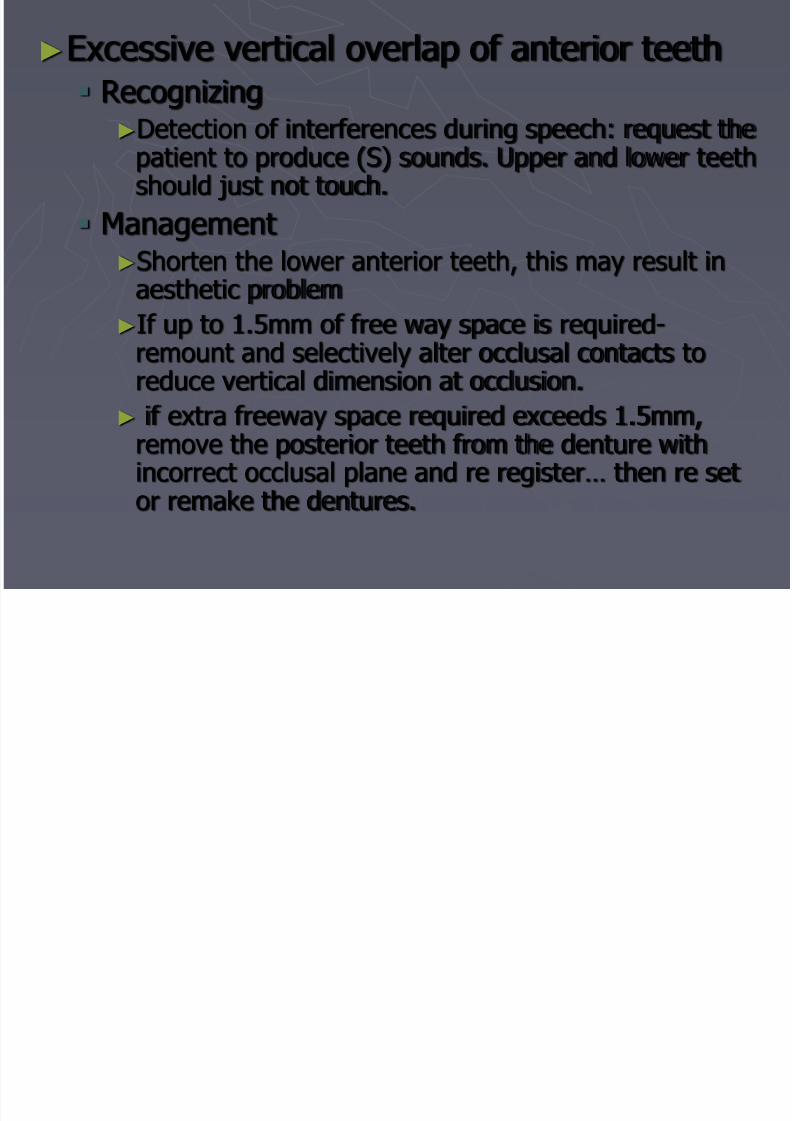
►Excessive vertical overlap of anterior teeth Recognizing►Detection of interferences during speech: request the
patient to produce (S) sounds. Upper and lower teethshould just not touch.
Management►Shorten the lower anterior teeth, this may result in
aesthetic problem►If up to 1.5mm of free way space is required-
remount and selectively alter occlusal contacts toreduce vertical dimension at occlusion.
► if extra freeway space required exceeds 1.5mm,remove the posterior teeth from the denture withincorrect occlusal plane and re register… then re setor remake the dentures.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 47/66
► last lower tooth tooposteriorly placed
Teeth overlies crest of theresidual ridge as this risestowards crest of theretromolar pad.
Pressure on these teethcauses denture to slip up.
► Recognize
Apply finger pressure on thelast tooth and observe ifdenture moves.
► Management Remove most posterior teeth
from dentures
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 48/66
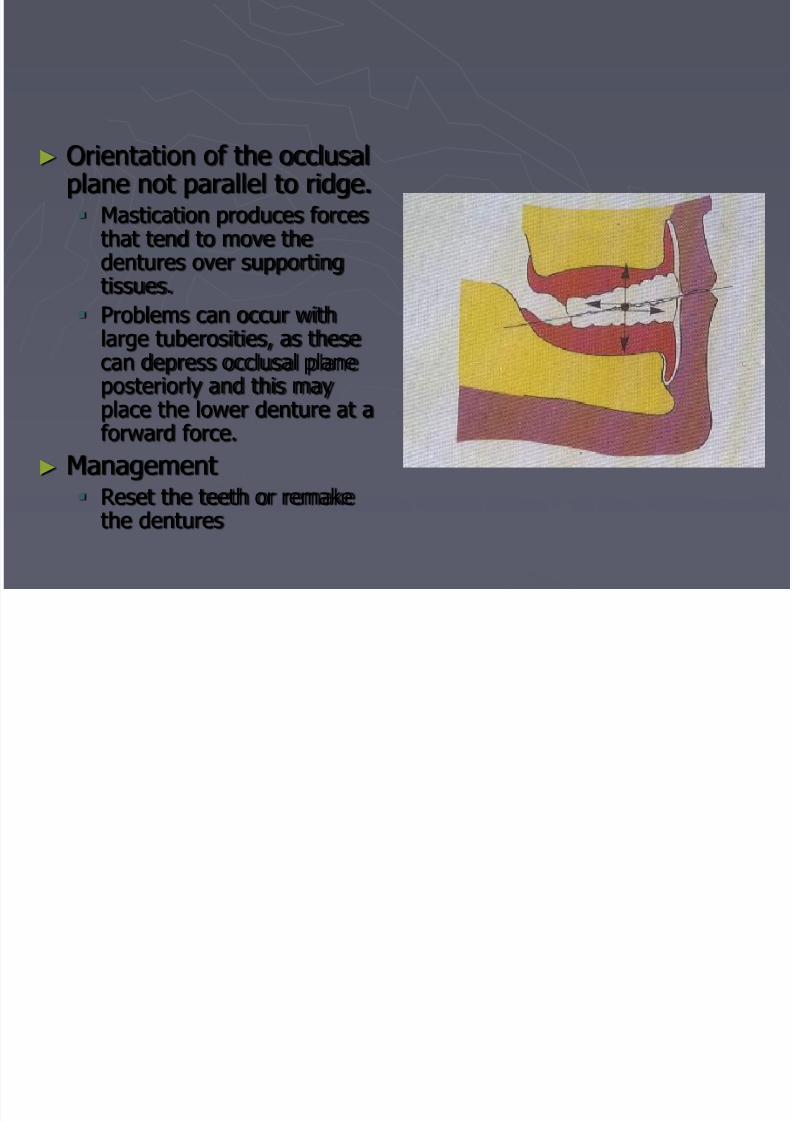
► Orientation of the occlusalplane not parallel to ridge. Mastication produces forces
that tend to move thedentures over supporting
tissues. Problems can occur with
large tuberosities, as thesecan depress occlusal planeposteriorly and this mayplace the lower denture at aforward force.
► Management Reset the teeth or remake
the dentures
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 49/66
Problems
► Appearance
►Function
Looseness of dentures
Problems in occlusion Support problems
►Comfort
►
Speech►Psychological
►Other.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 50/66
Support Problems
►Lack of ridge►Fibrous displaceable ridge
►Bony prominence covered by thinmucosa
►Non- resilient soft tissue
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 51/66
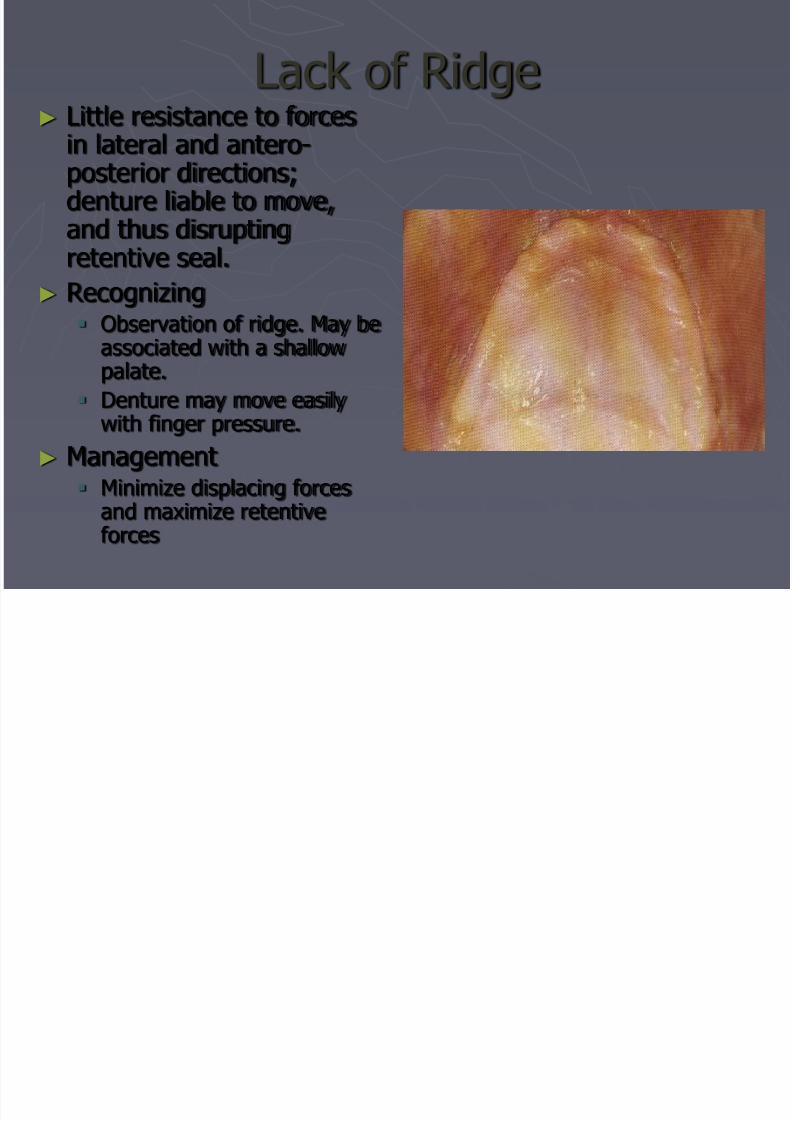
Lack of Ridge► Little resistance to forces
in lateral and antero-posterior directions;denture liable to move,and thus disruptingretentive seal.
► Recognizing Observation of ridge. May be
associated with a shallowpalate.
Denture may move easily
with finger pressure.► Management
Minimize displacing forcesand maximize retentiveforces
Fibrous displaceable ridge

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 52/66
Fibrous displaceable ridge► Forces of mastication
cause denture to sink into
and tilt on supportingtissues, thus disruptingretentive seal.
► Observation Palpation of the residual
ridge to determinedisplaceability. Denture maysink into tissues under fingerpressure.
Presence of history of
presence of natural teeth(usually lower anteriors)
Teeth may appear to meetevenly under forcefulocclusion, but when theteeth just meet, incorrect
occlusion often appear.
M t

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 53/66
►Management Reline/rebase►Precautions
Remove acrylic from impression surface until no contact isevident-you could check with disclosing material.
Add vent holes in the labial /buccal flange of the dentures.
Use low viscosity material.
Provide best possible posterior teeth.
►Non- resilient soft tissue Does not adapt to impression surface
May be associated with Endocrine /Nutritional
deficiencies. Management is similar to fibrous displaceable
ridge
Bony prominence covered by thin

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 54/66
Bony prominence covered by thinmucosa
e.g. :Prominent maxillary midline
suture, denture rocks about fulcrumproduced by area of reduced tissuedisplaceability and thus disruptingthe seal.
► Recognizing Denture rocks on finger pressure. Inflammation of thin mucosa Palpation to determine degree of
displaceability
► Overcoming Remove acrylic from impression
surface (indicated by disclosingagent)► Beware of excessive creation of
space beneath the denture► Beware of over thinning of the
denture base-possible fracture
Provide optimal occlusal contacts.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 55/66
Pain Avoidance Mechanisms

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 56/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
►
Lack of peripheral seal.► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit
► Denture not sited in optimal space( also neuro muscular control)
Problems in occlusion Support problems
1. Lack of ridge
2. Bony prominence
► Non- resilient soft tissue
► Pain- avoidance mechanisms
• Comfort
• Speech
• Psychological
• Other.

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 57/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
►
Lack of peripheral seal.► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit
► Denture not sited in optimal space( also neuro muscular control)
► Occlusal errors
2. Problems in occlusion3. Support problems
1. Lack of ridge
► Bony prominence
► Non- resilient soft tissue
► Pain- avoidance mechanisms
• Comfort• Speech
• Psychological
• Other.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 58/66
Causes of Discomfort
►Related to
Impression surface
Polished surface
Occlusal surface
Discomfort Related to the
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 59/66
Discomfort Related to theImpression Surface
► Pressure areas due to: Faulty impression Damage to the working cast
Warping of the base during processing
Immersing in too hot water
► Denture base not relieved in a region of undercut► Pearls of acrylic or sharp ridges on the fitting surface of the
denture► Lack of appropriate relief over tori, atrophic mucosa.► Overextension of peripheries, unrelieved frenal /muscle
attachment► Pressure on mylohyoid ridge.► Atrophic mucosa, spiky ridge► Postdam too deep

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 60/66
►Discomfort Related to the Polished Surface
Maxillary denture constraining coronoid process.
►Discomfort Related to the occlusal Surface
Slide form RCP to ICP
Lack of incisal overjet
Lack of appropriate freeway space
Lack of occlusal contacts
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 61/66
Discomfort Related to Other Causes
►Instability of Dentures
►Burning Mouth Syndrome
►Xerostomia
►TMD
A

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 62/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit
► Denture not sited in optimal space( also neuro muscular control)
► Occlusal errors
2. Problems in occlusion3. Support problems
1. Lack of ridge
► Bony prominence
► Non- resilient soft tissue
► Pain- avoidance mechanisms
• Comfort
• Speech• Psychological
• Other.
►Noise on speaking:

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 63/66
►Noise on speaking: Recognizing:
►Excessive OVD►
Occlusal interferences►Loose dentures
►Sibilants, e.g. “S” Recognizing:
►Count from 60-70, anterior teeth should be just out of contact
►Bilabial sounds, e.g. “P” “B” Recognizing:
►Lip approximation: is it easily attained?►Incisal position: is it incorrect?
► Labio dental sounds, e.g. “F” “V” The vermilion border of mandibular lip rest against the
incisal edges of the upper teeth? On swallowing, does the Mandibular lip overlap the
labial surface of the maxillary incisors?
A
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 64/66
1. Appearance
2. Function1. Looseness of dentures Decreased retentive forces
► Lack of peripheral seal.
► Air beneath the impression surface
► Xerostomia
► Neuromuscular control
Increased displacing forces► Denture border problems (over extension in length & width)
► Post dame too deep
► Poor fit
► Denture not sited in optimal space( also neuro muscular control)
► Occlusal errors
2. Problems in occlusion3. Support problems
1. Lack of ridge
► Bony prominence
► Non- resilient soft tissue
► Pain- avoidance mechanisms
• Comfort
• Speech• Psychological
• Other.
8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 65/66
►Gagging
Desensitization programmes
►Use soft tooth brush
Hypnosis
Training plates
Fixatives
Professional psychological counselor

8/13/2019 Managing Problems Complications
http://slidepdf.com/reader/full/managing-problems-complications 66/66
►Other problem areas
Burning Mouth Syndrome
Denture Stomatitis/Angular chelitis
Allergy
Temporomandibular Joint Disorders (TMD)