managing progressive ms · managing major changes managing progressive ms es 6009 4/07 $1.50 the...
TRANSCRIPT
Managing Major Changes
Managing Progressive MS
ES 6009 4/07 $1.50
The National Multiple Sclerosis Societyis dedicated to ending the devastating
effects of multiple sclerosis.
� � � �
Programs and Services DepartmentNational Multiple Sclerosis Society
700 Broadway, Suite 810Denver, CO 80203Tel: (303) 813-1052Fax: (303) 813-1513National Web site:
nationalmssociety.org
For Information: 1-800-FIGHT-MS (1-800-344-4867)Website: nationalmssociety.org
For Information: 1-800-FIGHT-MS (1-800-344-4867)Website: nationalmssociety.org

The National Multiple Sclerosis Society isproud to be a source of information aboutmultiple sclerosis. Our comments arebased on professional advice, publishedexperience, and expert opinion, but do notrepresent individual therapeutic recom-mendations or prescription. For specificinformation and advice, consult your per-sonal physician.
The Society publishes many other pamphletsand articles about various aspects of MS. Toask for these, or for other information, call theNational MS Society at 1-800-FIGHT-MS(1-800-344-4867).
All our publications are on our Web site, alongwith handouts called "Basic Facts" on varioustopics. For a list, click the bar on our homepage called “Living with MS”; then click“Library & Literature”. If you have no accessto the Internet, just call your chapter and askfor a copy of the latest Publications List.
Some of our popular pamphlets include:
� A Guide for Caregivers� Choosing the Right Health-Care Provider� At Home with MS: Adapting Your
Environment� So You Have Progressive MS?
Kaye Hooper has worked in the field of MSfor over ten years, primarily as nurse consult-ant and manager of the MS Clinic at RoyalBrisbane Hospital, Australia where she wasinvolved in clinical care, patient education,research and MS education for other nursesand health professionals. She has served onmany international MS boards and councilsand continues to be involved in MS projects.
Cover: Nancy Chamberlayne, MEd, is a vol-unteer telephone counselor for the BritishColumbia MS Society. Photograph by GaryNeilson.
Inside photos by Mark Kiryluk (pp. 13, 35,43, 47), Forest McMullin (pp. 5, 11), GaryNeilson (p. 21), Bill Stanton (pp. 9, 17).
This publication is supported by contribu-tions to the National Multiple SclerosisSociety from its members and friends.
Reviewed by members of the ClientEducation Committee of the NationalMultiple Sclerosis Society’s Medical AdvisoryBoard.
© 2007 National Multiple Sclerosis Society
ManagingProgressive MS
by Kaye Hooper, RN, MPH, MSCN
This booklet aims to document some ofthe strategies for living with severe MS inindependent or supported home environ-ments. It will point you to people andservices that may help you make choices,establish a comfortable and safe place tolive, and plan your future. Your needsand circumstances will probably changeover time, so what is a good solution foryou now may require another answer at alater time.
For basic information on MS we’d like torefer you to the Society’s booklets, avail-able online at nationalmssociety.org(go to “Library”) or from the nearestNational MS Society chapter. Throughoutthis booklet there will be references to lit-erature on specific topics, helpful organi-zations, and Web sites. Call 1-800-344-4867 to be connected.
INTRODUCTION
Most people reading this booklet will havelived for years with relapsing-remittingMS and are now facing a progressivecourse of MS without remission. Otherreaders may have had progressive MSfrom the onset (primary-progressive MS)but now face new problems, and worsen-ing symptoms. Everyone is different andeach person travels a unique road livingwith MS.
This road can be rough and unpre-dictable, challenging, frustrating, andexhausting. But it may lead to deepmeaning and self-discovery. Developingand strengthening personal coping strate-gies enables many people to appreciatelife and maintain a sense of purposedespite this chronic illness.
It is important for everyone to strive for apositive outlook—and to recognize andapplaud one’s own personal victories andachievements.
2 Managing Progressive MS 3
strategies and treat-ments. It is possible toalleviate many symp-toms, to improve somefunctions and—just asimportant—there areways to compensatefor disabilities andthus lessen theirimpact on your life.
Primary symptoms,directly caused by MS,include weakness,numbness, tremor,loss of vision, pain,mobility problems,poor balance, bladderand bowel dysfunction,sexual dysfunction, and cognition changes.These symptoms, common in relapsing-remitting MS, continue in progressive MS.They tend to worsen gradually over time. Thisdownward course may stabilize at any point.This doesn’t mean it goes away, but ratherthat adjustments and accommodations havecome to feel natural.
Permanent functional losses occur in progres-sive MS. Some permanent losses may occur
5
WHAT HAPPENS INPROGRESSIVE MS?
Even in the earliest stages of MS, damageoccurs within the central nervous system—which is comprised of the brain, optic nerves,and spinal cord. Myelin, a fatty material thatinsulates nerve fibers called axons, is attackedand the axons are sometimes damaged. Areasof demyelination tend not to repair themselvessufficiently, and with each attack morelesions, or areas of damage, tend to occur.
Progressive MS manifests itself differently ineveryone. Whether your MS is “secondary-progressive” which followed a period of“relapsing-remitting” MS or “primary-progressive” meaning it has been slowlyprogressive from the beginning, it is importantto realize that “progressive” does not necessar-ily mean severe disability. But it does meanthat there are few or no relapses, and few orno recovery or remission periods when majorsymptoms abate.
While there are still no effective medical treat-ments to repair nerves or reverse permanentlosses of function, there are many useful
4 Managing Progressive MS
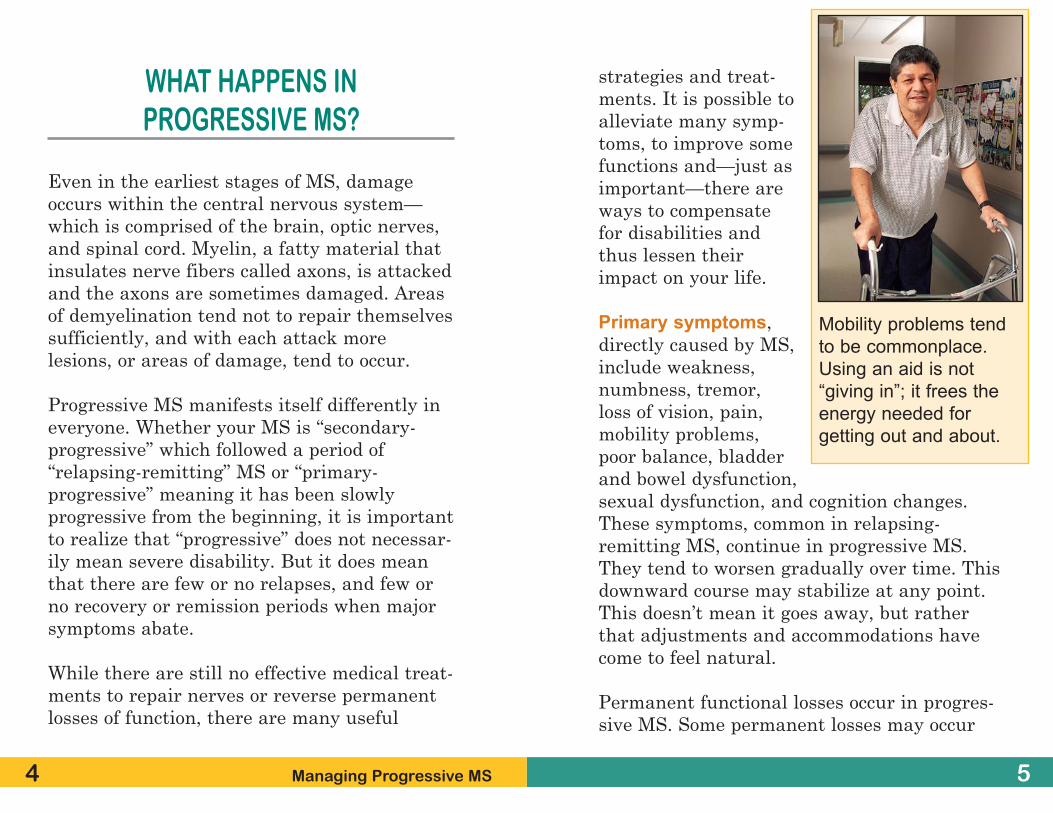
Mobility problems tend
to be commonplace.
Using an aid is not
“giving in”; it frees the
energy needed for
getting out and about.
7
in relapsing-remitting MS, as well, as every-one does not recover completely following anacute attack (or relapse). However, relapsing-remitting MS is known for periods of improve-ment. These will not be as apparent in pro-gressive MS.
Secondary symptoms are complications thatarise from the primary symptoms. Urinarytract infections can be a result of bladder dys-function, for example; poor balance and inac-tivity can cause problems with posture, jointmobility, or bone health. Paralysis or poormobility creates a risk for skin breakdown(pressure sores). Problems with swallowingmay cause respiratory infections and poornutrition.
The repercussions of these symptoms hit hard.Increased effort is required to deal with them,which can take a toll on your energy. It is nor-mal to feel stressed and fatigued when facedwith such challenges.
Tertiary symptoms are the “trickle down”effects of the disease on your life. These symp-toms include social, vocational, and psycholog-ical complications. For example, if you are nolonger able to drive or walk, you may not beable to hold the job you are used to. The stress
6 Managing Progressive MS
and strain of dealing with MS often alterssocial networks and sometimes fracturesrelationships. Problems with bladder control,tremor, or swallowing may cause people towithdraw from social interactions and becomeisolated.
Depression is fairly common in people withMS. Depression may be a primary or a terti-ary symptom as it can be caused by the dis-ease process itself or be triggered by the bur-dens of the added baggage discussed above.
MEDICAL ISSUES
The Health-Care Team—who does what
Let’s start by clarifying the professionals youmay need to help you handle MS symptoms.Whether MS is progressive or not, it is a com-plex and unpredictable condition—and oftenrequires the attention of many specialists.
You may receive care at a multidisciplinaryMS center. If you do not, you need to create amultidisciplinary team, working with yourneurologist or primary-care physician and
aware of preventivehealth issues. TheSociety has devel-oped guidelineswhich can beobtainedon our Web site orby calling yourchapter.
� MS nurse—coordi-nates health-careservices. The nurseoversees initial andlong-term manage-ment issues, teachesself-care, includingadministration ofmedications, andadvocates for needs with insurance compa-nies and other agencies.
� Physical Therapist (PT)—focuses on exer-cise programs to reduce and prevent seriouscomplications such as contractures (frozenjoints) and osteoporosis, and to ease spastic-ity and tremor. PTs provide information onequipment such as wheelchairs, scooters,hoists, canes, braces, and walkers. Theyteach safe, effective ways to use these
9
within the limits of your insurance coverage.Possibly, for certain needs, you may seek careoutside your coverage, if that can be managed.If you have created your own team, you mayalso need to initiate coordination among themembers. Your nurse and your chapter of theNational MS Society will help. Many chaptersprovide “case management” programs or refer-rals to community care managers. All chaptersare familiar with the MS specialists practicingin your area.
These are the key professional roles:
� Neurologist—in addition to establishing theinitial diagnosis, prescribes treatments forMS and symptom management. Regularannual visits to the neurologist are recom-mended for assessment and monitoring ofMS. The neurologist will refer you to otherspecialists such as a urologist, gastroen-terologist, gynecologist, psychiatrist, or painspecialist.
� Family physician—provides primary healthcare, including general health checkups,immunizations, and preventive care.Society research suggests that people withmore severe progressive MS tend to rely ontheir neurologists for primary health care.Be sure you (and your neurologist) are
8 Managing Progressive MS
Knowledgeable health-
care professionals play a
key role in plans for living
well with progressive MS.
Dr. Aaron Miller is head of
the Society’s Medical
Advisory Board.
11
devices, including the best ways to transferin and out of bed, a car, a shower, andmore. PTs help their clients create personalexercise programs for increasing stamina,optimizing mobility, and preventing unnec-essary complications.
� Occupational Therapist (OT)—focusesmainly on skills that require upper bodyfunction. OTs are specialists in tools, tech-niques, or equipment to conserve energyand compensate for disabilities that inter-fere with dressing, grooming, personalhygiene, eating, driving, using computers,and other ordinary activities. They mayconsult with architects or builders aboutrenovations and home adaptations to sup-port independence. OTs may also evaluateand treat cognitive problems.
� Speech/Language Pathologist (SLP)—evaluates and treats speech and swallowingproblems by training the person with MSand caregivers/family members about eat-ing safety, how to prepare easy-to-swallowfood, and how to manage feeding tubes ifnecessary. They teach the use of speechamplifiers or telephone aids, and, like OTs,may evaluate and treat cognitive problems.
10 Managing Progressive MS
� Social Worker—assesses social needs andlinks clients to appropriate resources inareas of income maintenance, insurance,entitlement programs, housing, long-term care options, living wills, and estateplanning.
� Counselor—mental health professionalshelp individuals and family members devel-op problem-solving skills, grieve for losses,recreate self-esteem, handle changing rela-tionships, learn to live with uncertainty,and find ways to be productive.
� Neuropsychologist—specializes in cogni-tion problems. The neuropsychologist willset up programs to compensate for weak-nesses identified in comprehensive neu-ropsychological testing.
Rehabilitation pays
off even when MS
has become more
severe. Sarah
Davidson attends
the MS Achieve-
ment Center (a
day program) in
Rochester.
experiencing relapses. Natalizumab (Tysabri®)is also FDA-approved for all relapsing forms ofMS. Mitoxantrone (Novantrone®) is approvedfor secondary-progressive, progressive-relapsing and worsening relapsing-remittingdisease. Although not specifically approved forMS, methotrexate, and cyclophosphamidehave also been used with varying degrees ofsuccess. Tysabri, Novantrone, and methotrex-ate and cyclophosphamide all pose the risk ofpossible serious side effects.
Experimental treatments, including bone mar-row transplantation and a procedure calledplasmapheresis, have had very mixed results.These approaches have many risks andbecause they are experimental they may notbe reimbursable by your insurance policies. Todate, primary-progressive MS has been themost resistant to all of these treatments.
13
� Spiritual advisors—may help make sense ofMS within a personal worldview. The choiceof advisors and the sources of support areintensely personal matters but the need topay attention to this aspect of life with MScannot be overemphasized.
In MS, effective health care is best achieved bycoordinated input from a range of specialistproviders. It is important to contact the rele-vant professional early and to put a plan intoaction. Prompt attention to a problem can oftenreduce the impact it might have on your life.
What medical treatments helpprogressive MS?
This is an important question to discuss witha knowledgeable MS specialist. Although thereare some treatments for progressive MS, youmay or may not be a suitable candidate forthem, depending on your particular situation.Your physician may suggest starting or stay-ing with one of the disease-modifying drugs.
The interferon medications (Avonex®,Betaseron®, and Rebif®) are approved by theFood and Drug Administration (FDA) for allrelapsing forms of MS, including secondary-progressive MS in those people who are still
12 Managing Progressive MS
As director of
Living in HopeMinistries in
Colorado and a
person with MS
herself, Tracey
Kimball values giv-
ing and receiving
spiritual support.

14 Managing Progressive MS 15
Among the more interesting therapies in clini-cal trials are those using monoclonal antibod-ies—products of the biomedicine revolution.(They include CamPath® 1H [alemtuzumab],Zenapax® [daclizumab], and others.) For themost up to date information, be in touch withyour chapter of the Society or go to www.nationalmssociety.org/ProgressiveMS onour Web site in addition to having a full dis-cussion with your physician.
Should you volunteer fora clinical trial?
Clinical trials are essential for scientists tounderstand MS, to develop better treatments,and ultimately to find a cure. Because MS issuch a complex disease and affects individualsso differently, it is expected that people partic-ipating in trials will have different outcomes.In other words, some individuals may benefitmore than others. Moreover, only some peoplewill receive the test treatment and every effortwill be made to prevent anyone from knowingwho receives what while the trial continues.
Volunteering in a clinical trial is an invaluablecontribution to the MS knowledge bank butmay offer only limited personal benefit.
And many trials are limited to people withrelapsing-remitting MS.
Some people with progressive MS feelresearch ignores them. Progressive MS movesvery slowly, and presents far fewer clear“markers” by which to measure the effective-ness of a new treatment. Therefore, many clin-ical trials are structured for volunteers withrelapsing-remitting MS, where the benefits, ifany, will be seen sooner and more clearly.
Ultimately, the knowledge gained from clinicaltrials helps everyone. Even if you never partic-ipate in a trial, there are reasons to be hope-ful. Researchers around the world are at workon the whole spectrum of MS and importantadvances are being made every year.
To find out if there is a clinical trial for whichyou could volunteer, talk to your doctor, con-tact your National MS Society chapter, andvisit the Research section on the Society’s Website. This site is also an excellent way of keep-ing up with the newest developments in MSresearch and treatments.

periods. Most do sowith the help and sup-port of family andfriends. They reportjoys and a deep senseof achievement alongthe way. Spiritualadvisors and/or profes-sional counselors maybe a critical resourcein helping individualsand their family mem-bers—who also livewith the MS—toexplore ways to adapt.
You may not be ableto be on one of theinjectable disease-modifying therapies, but there are manythings you can do to minimize the impact ofsymptoms on your life, guard your health,improve your quality of life, and maximizeyour ability to function.
Complementary and alternativemedicines (CAMs)
People with MS are frequent consumers ofvarious types of CAM—and with care and cau-
17
HANDLING MS DAY TO DAY
The emotional roller coaster
Some days you feel up to the challenge whileother days you want to retreat. Feelings ofgrief, loss, anger, disbelief, fear, sadness, andguilt can be constant companions. You thinkyou have gotten over a challenge and then itraises its head again.
Living with MS is a process—and you have toarm yourself for the hard days and allow your-self to celebrate the good days.
Severe disability may occur despite the bestmanagement, interventions, and treatmentstaken early on in the disease. Despite yourbest efforts and those of your health profes-sionals and family, the disease may take itsown course.
Finding ways to be productive and fulfilled, toreshape your life, and regain self-esteem thatmay have been lost because of MS, ofteninvolves developing mental, emotional, andspiritual “muscles” you may not have usedbefore. These goals are not achieved quickly.But people can and do pass through crisis
16 Managing Progressive MS
A New York City class in
adapted tai chi allows
people to participate in
this mind-body practice
at their own levels.

19
tion this is appropriate. CAM should alwaysbe used alongside prescribed medicines andtherapies. When you decide to try any comple-mentary or alternative therapy, your health-care team needs to be fully informed.
When you are considering using any form ofCAM, it’s a good idea to ask the same kinds ofquestions you would ask when starting a newtreatment prescribed by a physician. In otherwords, it’s best to approach CAMs withhealthy, informed caution. CAMs may make areal contribution to coping successfully withsymptoms, but they are not totally risk-free.Be particularly cautious—and skeptical—about any CAM that claims to cure your MS.
The booklet, “Clear Thinking AboutAlternative Therapies” is a good place tostart your exploration. It is available from theSociety or can be accessed on the Society Website. The Web site managed by the RockyMountain MS Center (www.ms-cam.org) isdevoted to CAMs used by people with MS andthe Society recommends it as a good source ofinformation.
18 Managing Progressive MS
SYPMTOM MANAGEMENT WHENTHE ROAD GETS ROUGHER
Some of the more difficult symptoms of MSare not tied to progressive disease—and maybe familiar to you. But symptoms may becomeharder to manage if problems mount up.
Fatigue
An overwhelming tiredness, without any tiringactivity, affects about 85% of people with anytype of MS.
Primary fatigue is a direct result of damagewithin the central nervous system.
Secondary fatigue stems from indirect factors.Examples include sleeplessness because ofspasms, pain, or too many nighttime trips tothe bathroom; infections that cause body tem-perature to increase; medications with fatigueas a side effect.
Even though this may seem counter to goodsense, a regular exercise program has beenproven to reduce fatigue. Certain medications,including amantadine and modafinil (Provigil®)
21
may also be beneficial. And, most importantly,fatigue can be managed by using energy-saving techniques. If your disability hasincreased, saving energy is now vitally impor-tant. In addition to self-help and medications(explained in the Society publication,“Fatigue: What You Should Know”) yourneurologist, your nurse, an occupational thera-pist, a physical therapist, a mental healthcounselor, and independent living specialistscan all contribute to the development of yourpersonal energy-saving plan. Ask your doctoror call your chapter for referrals.
It’s true about keeping cool
With MS, an increase in body temperature cancause a temporary increase in symptoms suchas fatigue, spasms, slurred speech, visual dis-turbances, or weakness. Nerve conductivityslows down when an individual’s body temper-ature rises even a very small amount.
Use fans, air conditioners, cool water, icydrinks, cool showers—anything that works.And keep out of the sun in the middle of theday. Commercially available cooling garments,including special vests, hats, wristbands andjackets, can also reduce the risk of worseningsymptoms on hot days, while making outside
20 Managing Progressive MS
activities outside moreenjoyable.
Discuss exerciseoptions with youroccupational therapist,physical therapist, orMS nurse, to findways to exercise andkeep the heat down atthe same time.
Stress anddepression
Stress is a fact of life.Sometimes it makesus spring into action,but other times it crushes us. Managing stressis part of successful living for everyone withMS—including the person newly-diagnosedwith relapsing-remitting MS and the personliving with very severe, progressive MS.
Depression, on the other hand, is not a fact oflife, but it is extremely common among peoplewith MS at any stage. Symptoms of depressioncan look a lot like stress symptoms, anddepression can also be confused with lack ofdeep sleep, fatigue, or cognitive issues.
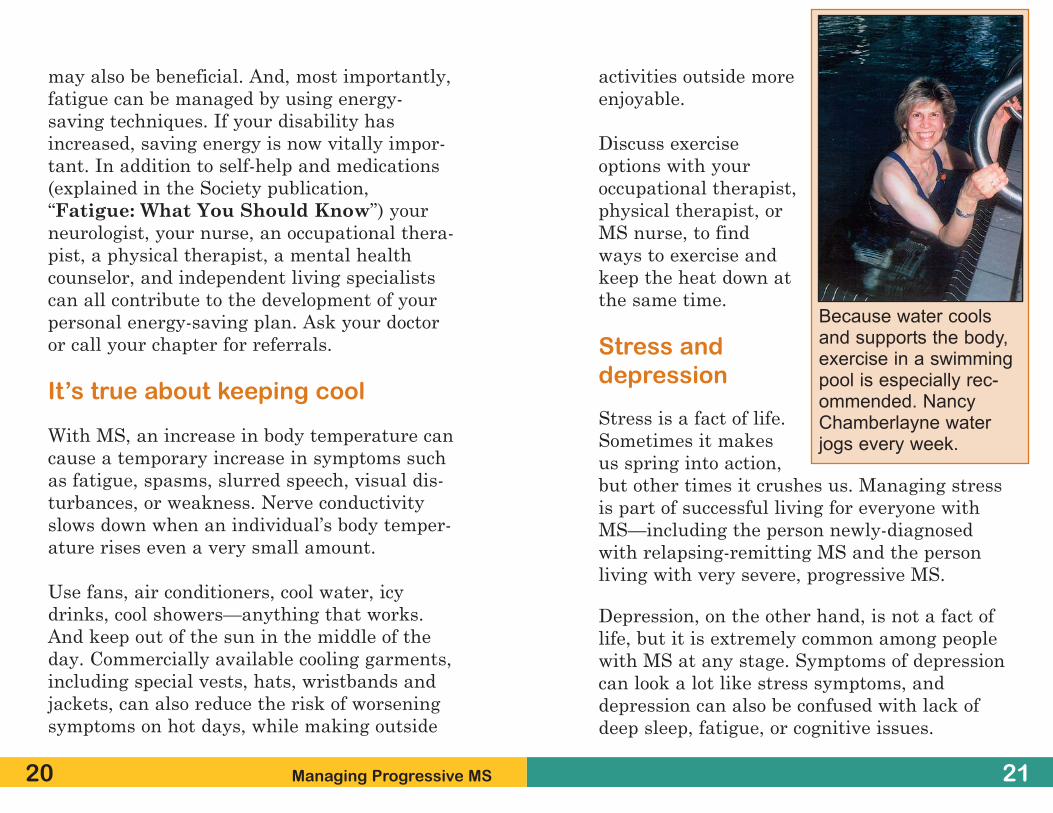
Because water coolsand supports the body,exercise in a swimmingpool is especially rec-ommended. NancyChamberlayne waterjogs every week.

2322 Managing Progressive MS
Pain
As with cognitive problems, MS pain is alsonot related to the degree of disability or thestage of the disease. People with mild relaps-ing-remitting disease may have stubborn MSpain while those with severe progressive MSand many disabilities may have little or none.
Pain can be a direct result of nerve damage inthe brain and spinal cord or it may be a sideeffect of walking problems, abnormal posture,or immobility. Nerve pain and musculoskeletalpain require completely different treatments,so accurate diagnosis is the key first step.Either kind of pain can be so severe and con-stant that it limits daily life.
Musculoskeletal pain usually responds well tophysical therapy and the use of adaptivedevices. However, chronic nerve pain—whichcan sometimes resist the existing medications—may warrant a workup at a specialty pain clin-ic. There, a multidisciplinary team with expert-ise in the management of complex pain, willcreate an individualized treatment plan to meetyour needs. If a multidisciplinary pain clinic isnot an option—due to expense or distance—communicate your needs to your neurologistand to staff at your Society chapter for help inidentifying all available local resources.
Consult your health-care professional if youfind yourself sleeping too much, not sleepingenough, losing appetite, gaining weight, orfeeling agitated, irritable, worthless, or bluemost of the day for more than two weeks. Callimmediately if you are having thoughts ofdeath or suicide. Stress can be managed—anddepression can be treated with medication andcounseling.
Cognition
Cognitive changes are not linked to progres-sive disease. They affect up to 50% of everyonewith MS and can occur at any time in thecourse of the disease. The changes are mild formost people and involve short-term memorylapses, slowed response time, and the like. Buteven mild problems may affect employment,driving, communication, and relationships.
About 5-10% of people with MS experiencesevere cognitive impairment. They mayrequire structured environments and supervi-sion. Those who are severely impaired mayhave great difficulty recognizing the extent oftheir problems. The Society booklet, “SolvingCognitive Problems” presents a compre-hensive overview and discusses testing andcognitive rehabilitation.

way toward ensuring confidence and prevent-ing accidental injury.
Spastic limbs also benefit from exercise pro-grams in a cool swimming pool. A temperatureof 85 degrees or less is best. Water supportsbody weight enabling wider motions than canbe done on dry land.
Baclofen is the most commonly used anti-spas-ticity medication, but in higher doses oralbaclofen becomes increasingly sedating. Apump, about three inches across, can be surgi-cally implanted in the abdomen to deliverbaclofen (and sometimes drugs to controlpain), in very small doses via a thin tubedirectly into the intrathecal space surroundingthe spinal cord. A test dose is required beforethe pump can be implanted.
This delivery method limits sedating sideeffects. There are potential risks includinginfection, pump failure, and dislodgement ofthe tube. The pump needs to be refilled by adoctor or nurse at regular intervals with a pro-fessional assessment of the dosing level ateach refill.
Other spasticity medications that may behelpful include diazepam, dantrolene, and
25
Spasticity
Spasticity is also common in MS and is man-aged with a combination of medications, physi-cal therapy, exercise, stretching, adaptivedevices, and rehabilitation. The Society book-let, “Controlling Spasticity in MS” providesa good overview.
Severe spasticity can cause serious problemswith positioning, sitting or lying down, andmay impede personal care. This in turnincreases the risk of pressure sores and otherskin problems. Untreated spasticity may causepermanent joint contractures (stiff or frozenjoints). However a certain amount of spasticitymay also help people with severe MS. Theincreased stiffness in the arms or legs canhelp stabilize a person during transfers ordaily chores. This advantage needs to be bal-anced against the benefits of the medicationsthat make the limbs looser.
Regular stretching is just as effective whetherit is active (you move independently) or pas-sive (when a helper moves your limbs). If youneed a helper, you probably need a sessionwith a physical therapist or an MS nurse toteach your helper. A little training goes a long
24 Managing Progressive MS
27
tizanidine. Botulinum toxin (Botox®) injec-tions, which are used to reduce spasticity inan individual muscle, temporarily paralyzesthe selected muscle to allow free movement,This therapy, which is costly and may not becovered by insurance, is not appropriate forlarge groups of muscles. The effects of a Botoxinjection last three to six months.
Spasticity at night may require special posi-tioning or the use of splints or padded braces.If you or your partner notice spasticity or peri-odic leg movements at night, be sure to dis-cuss this with an MS nurse. A partner may bemore aware of this than the person with MSwho wakes up tired but is not quite aware ofhow frequently deep sleep is being disrupted.
Very rarely, surgery is recommended forpainful spasticity that does not respond toother measures.
Bladder problems
Many people with MS know every bathroomfacility along all their frequently traveledroutes. If problems are continual, a person mayfeel tied to the house and be wary about goinganywhere. During the day, repeated journeys to
26 Managing Progressive MS
the bathroom use upprecious energy.Frequent nighttimetrips (even to a bedsidecommode) increasefatigue and irritabilityfor individuals andtheir partners. Loss ofbladder control canalso increase the riskof pressure sores andskin breakdown.
Good bladder manage-ment is the answer.Depending on the indi-vidual, it is usually acombination of man-agement strategieswith prescription medication such as oxybu-tynin, tolterodine, trospium chloride, or solfeni-cen succinate. A urologist, MS nurse or a conti-nence specialist should be involved in ongoingmanagement of bladder issues if they aresevere or persistent.
Some of the strategies include:
� Bladder “training” and scheduled voiding.(Ask your nurse.)
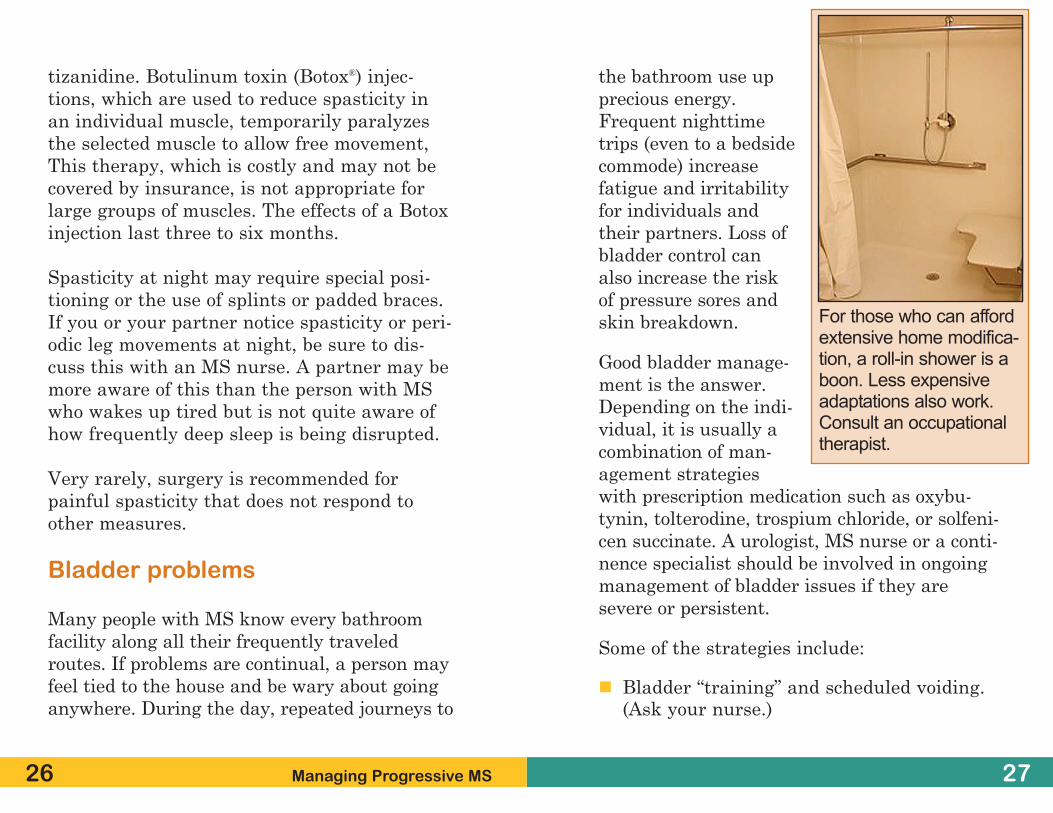
For those who can affordextensive home modifica-tion, a roll-in shower is aboon. Less expensiveadaptations also work.Consult an occupationaltherapist.

to drain into the toilet. The process takes lessthan 10 minutes. It is done every four to sixhours throughout the day and then just priorto sleep. This schedule can vary with individu-als. There is little risk of infection, and afterovercoming initial natural reluctance, IC isnot painful or upsetting. IC allows a personwith MS to remain dry.
Difficulties with hand function, weakness ortremor, or problems transferring on and off atoilet may make IC inappropriate for somepeople.
Indwelling Catheter
For people who are unable to manage IC, anindwelling catheter may be the safest or mostpractical next choice. Once the health-careprofessional has inserted the catheter into thebladder through the urethra, an indwellingcatheter remains in place draining the urineinto a disposable collection bag. The urinedrains by gravity so the collection bag shouldalways remain lower than the person’s bladderto avoid backflow.
Indwelling catheters require monitoring andcare so complications such as infections andbladder stones are avoided. Silicone catheters
2928 Managing Progressive MS
� Limiting alcohol and caffeinated drinksthat can irritate the bladder.
� Avoiding constipation with a good bowelprogram. (See below.)
� Daily cranberry tablets. Cranberry preventsbacteria from sticking to the bladder liningand helps prevent infections.
� Drinking six to eight glasses of water a day.Fluids are essential to keeping the bladderfunctioning properly and avoiding infec-tions, dehydration, and constipation.
� The use of pads and absorbent products forsecurity.
� Catherization to drain the bladder. This isa highly effective management techniqueand there are several options depending onyour need.
Intermittent catherization (IC)
This quick, efficient way of emptying the blad-der can be done independently by the individ-ual, or by a caregiver. In both cases, an MSnurse can provide the necessary training.
A small tube (catheter) is inserted into thebladder through the urethra. This allows urine
If MS makes personal hygiene difficult
We all need daily cleansing with soap andwater. Showers, bed baths, or sponge bathsare essential to keep skin clean and healthy.So too are daily dental hygiene, hair care, andtoileting. Should MS compromise the strengthand coordination skills needed to accomplishthem, there are assistive devices that helpindividuals remain independent or ease theburden on caregivers.
Occupational therapists are the experts in thearea of assistive devices for personal hygieneand bathroom adjustments that make toiletfunctions more effective and safe. They haveextensive practical information on bothdevices and techniques.
If you need a caregiver or a visiting nurse tohelp with basic activities, get advice andinform yourself about all available options.Working together you and your caregiver candevelop a hygiene system that works for you,while allowing you to maintain as much inde-pendence and privacy as possible.
Here are a few bathroom devices to discusswith your OT or other professional advisors.Some have a minimal cost, while others areexpensive.
31
are changed every three to four weeks or atregular intervals to avoid infections.
The same fluid intake recommended above (6-8 glasses) is essential in order to irrigate thebladder and reduce the risk of infection andstone formation. Carbonated drinks should beavoided as they make the urine alkaline,which encourages stones.
Low-grade infections are common withindwelling catheters and long-term antiseptictreatment or short-term antibiotics may berequired.
Suprapubic catheters
For those with more advanced MS bladderproblems, a suprapubic catheter can be theanswer. This involves minor surgery. A flexi-ble tube is inserted into the bladder throughan incision in the lower abdomen. The bladderempties via this tube into a collection bagwhich is usually fastened to the leg. This tech-nique may be more appropriate for long-termmanagement as it is associated with fewercomplications than an indwelling catheter.
A urologist will need to assess your bladderproblems and discuss the options and manage-ment strategies that would be best for you.
30 Managing Progressive MS
MS can also make having a bowel movementmore difficult.
A bowel program may include use of stool sof-teners with bulk-forming laxatives, supposito-ries, or enemas. Some of the other strategiesare similar to the bladder checklist above:
� Follow the practice of having a bowel move-ment at the same time every day, usuallyafter breakfast, when the normal reflex forbowel activity takes place.
� Reduce caffeine and alcohol—these canworsen bowel problems.
� Increase fluids by drinking water, dilutedfruit juices, non-caffeinated hot drinks.
� Use protective undergarments with dispos-able linings.
� Be patient. It takes time to establish regu-lar bowel habits—often weeks before youcan feel comfortable with your daily routine.
If constipation is severe, there may be a needfor manual stimulation to empty the boweland this will require wearing a plastic glove.Insert a gloved finger into the rectum androtate it gently around the anus rim. This can
33
� Hoists or lifts for transferring betweenchair/bed/toilet/shower.
� Grab rails for stability and mobility, so thatyou can move, roll, transfer, and access allareas of your body.
� Long handled scrubbers and body washersfor reaching far-away parts more easily.
� Raised toilet—which requires less bending,extensive movements, or leg strength.
� Toilet railings for safely getting on and off.
� A multipurpose commode—to be used as abedside commode, a shower chair, or placedover the toilet as an elevated toilet seat.
� Push-button self-cleansing device, installedon a toilet, which washes and dries theperianal area with jets of warm water andwarm air.
Bowel problems
Constipation, which is very common in MS, iscaused by decreased intestinal movement, lim-ited physical activity, poor diet, and decreasedfluid intake. Pelvic floor muscles weakened by
32 Managing Progressive MS
indwelling catheter or other bowel or bladderproblems, you will need to start the discus-sion—and you may find it easier to approachyour MS nurse about these problems.Depending on the type(s) of difficulties you areexperiencing, your neurologist or nurse mayrefer you to a urologist, who is a specialist inthe male and female urinary system and isalso trained to treat male erectile dysfunction.You may want to start your exploration withthe Society’s booklet, “MS and Intimacy”which contains helpful facts and resources.
Swallowing problems
This is a serious issue. Choking and coughingwhen eating or drinking can be dangerous aswell as disturbing. If you have these problems,you need to consult a speech pathologist toassess your needs.
35
stimulate the bowel and help open the analmuscles.
Diarrhea or fecal incontinence can occur as aconsequence of constipation. When a hardmass of stool presses on the internal sphincterand cannot pass through (known asimpaction), softer stool leaks out around thisimpacted stool. An enema or suppositoryshould be administered to empty the colon ofthe fecal mass. It may take a number of daysto completely empty an impacted bowel andthen it is important to establish a regular pat-tern of bowel emptying.
It is also important to remember that changesin bowel habits can be caused by other prob-lems. Colon cancer, allergies, viruses andother infections can cause diarrhea and consti-pation—so always discuss new bowel problemswith your health-care professional. Not everyproblem you have is caused by MS.
Sexual issues
Even in early MS, there may be physicalchanges that make sexual activity difficult oruncomfortable. Worsening MS may worsenproblems. Since your physician may not bringup the sexual issues related to having an
34 Managing Progressive MS
People with
swallowing diffi-
culties may need
to experiment
with smoothies
or pureed soups.
abilities to the fullest. Voice amplifiers may beuseful if a person’s articulation of words isadequate. Sometimes speech problems areeased when the individual learns to speakmore slowly, use shorter sentences, and choosewords that are easy to pronounce.
To express themselves more widely and toshare complex information, people with speechlimitations often need “assistive communica-tion devices.” This is a fancy term for toolsthat range from paper and pen, or “magicslates,” to sophisticated laptop computers.People with disabilities can control computersusing adapted keyboards, sticks held in themouth, or wireless devices worn on the heador eyeglasses. There are even computer con-trols that operate by eye blink. TTY/TT sys-tems and free translation services enable tele-phone use for those who speak too softly orslowly for a regular telephone. For those withprofound disabilities, there are communicationboards. The user gazes at alphabet letters,symbols, words, or phrases to communicatebasic messages.
Skin care
A pressure sore is any redness or break in theskin caused by too much pressure for too long
37
By choosing the right foods, preparing themproperly, and learning the best body posturesfor eating or drinking, you can avoid complica-tions such as respiratory infections (caused byfood particles in the lungs) and malnutrition.
People with MS-related swallowing problemsare often advised to choose thicker fluids andstewed, mashed, or blended foods that needless chewing, while avoiding foods that crum-ble easily. It may also be advisable to eatsmaller, more frequent meals, and to takesmaller bites to avoid fatigue from chewingand swallowing.
In rare situations, MS overwhelms swallowingreflexes. Then a feeding tube may be surgical-ly inserted to bring food and liquid directly tothe stomach. A decision about what type offeeding tube to use should be made in consul-tations with a knowledgeable MS specialist.
Speech problems
Some people with MS experience episodes ofspeech difficulties. These may come and go orthey may remain and perhaps worsen overtime. Consultation with a speech pathologist isimportant. With professional help, people canlearn how to use their existing communication
36 Managing Progressive MS
3938 Managing Progressive MS
� Treat spasticity with medication and regu-lar physical therapy.
� Wear appropriate clothing—soft andunbinding materials and roomy cuts toaccommodate sitting.
� Give bony prominences (like the hip orankle bones) protection by the use ofpadded boots or cushions and gently mas-sage these areas to help keep the skin andjoint healthy.
Some added ways to avoid pressure soresinclude:
� Do wheelchair pushups and positionchanges in the chair at regular intervals.Aim for an hourly push up or a roll fromside to side to relieve the area and allow airto flow. How frequently a person can do thisdepends on body weight, the wheelchairsupport and cushioning, upper limbstrength, and current skin condition (is itintact and dry?).
� Use appropriate cushions to relieve pres-sure—there are many types available.
a period of time. The pressure prevents bloodfrom getting to the skin—so the skin dies.Normally the nerves send messages of pain ordiscomfort to the brain to signal the need tochange position. Damage from MS interruptsthese signals. People with MS who are immo-bile most of the day, even if they are not inbed, are at risk of pressure sores—also knownas decubitus ulcers or bed sores.
� Shearing is a special kind of pressureinjury. It happens when the skin moves oneway and the bone underneath moves anoth-er. Shearing happens if you slouch or slidewhen you are seated, for example.
� An abrasion can occur when you are pulledor pull yourself across a surface instead oflifting. This is an example of friction injury.
� High pressure, such as a bump or fall, maycause damage to the skin which may notshow up right away.
A pressure care plan helps avoid these prob-lems. Speak to your physical therapist ornurse to get the best advice. You will learnthat the person with MS and the caregiverscan work together to prevent most skin prob-lems from occurring.
41
� Use lifts or hoists to make changing posi-tion easier, and to prevent “shear” duringtransfers.
� Inspect the whole body every day to detectany changes in color or broken areas—acaregiver is essential for checking areasthat are not visible to the individual.
40 Managing Progressive MS
� Treat any problem area immediately. Restthe area by removing all pressure and con-tact a physician or wound specialist.
� Eat an adequate diet. Good nutrition isessential for healthy skin.
� Manage bladder and bowel problems, tokeep skin dry and clean.
WHERE TO LIVE TO GET THE CAREONE NEEDS
Some people manage independent lives withmajor disabilities by employing personal careattendants, housekeepers, and home healthaids to maximum advantage. Others manage,and manage well, with the help of partnersand loved ones. Still others come to decidethat their needs are best met in a residentiallong-term care facility. In the middle are peo-ple whose arrangements are unstable, drain-ing, and even dangerous.
Ask your chapter of the National MS Society tosend you the handout called “Hiring Help atHome” or find it on the Society’s website in the“Library” section under “Brochures/Managing
� ABLEDATA, sponsored by the NationalInstitute on Disability and Rehabilitation
Research, U.S. Department of Education, is
a premier source of information on adaptive
technology on the Web. Go to www.able
data.com. The site lists more than 20,000
products, with descriptions, prices, order-
ing, and installation information.
� Centers for Independent Living. TheNational Council on Independent Living
links some 700 private, nonprofit commu-
nity organizations by and for people with
disabilities. These centers offer technical
advice, training, and advocacy to enable
people to live safely outside institutions.
Go to www.ncil.org. The site has a click-
able map for locating the nearby centers.
Or look in the telephone directory under
Independent Living Center.

Reorganize, refit, renovate, oreven consider moving!
Staying at home will mean making changes.Home adaptations do more than fight fatigue.They offer safety, ease of movement, and com-fort. Once again, an occupational therapist isthe specialist in assessing what can be done tomodify your home. It may not be as hopeless,expensive, or ugly as you might think at first.Some renovations—such as a roll-in shower—are costly; others, such as ramps, may beavailable as a volunteer project. Grab bars,available in attractive colors, require profes-sional installation, but replacing doorknobswith lever handles is a weekend do-it-your-selfer’s project.
42 Managing Progressive MS 43
Major Changes.” It includes checklists to helpassess needs, sample job description forms foruse in hiring, and a sample employment con-tract, along with suggestions on recruiting vol-untary or paid help at home.
If you are receiving long-term support services,either in the community or in a residentialsetting, be sure the supervisor of care has acopy of the Society’s publications developed toenhance quality of care in those settings.“Nursing Home Care for Individuals withMultiple Sclerosis,” “Assisted Living forIndividuals with Multiple Sclerosis,”“Serving Individuals with MultipleSclerosis in Adult Day Programs” and“Serving Individuals with MultipleSclerosis in the Home” are all available inthe “For Professionals” section of the Society’sWeb site (nationalmssociety.org/prcpublications), or printouts may berequested from your local chapter.
All the options require some degree offlexibility.
Taking an active
part in life away
from home is
possible—but
going places
requires planning
and patience.

The realities of the daily routine have a hugeimpact on both the person with MS—wholoses some degree of independence—and thecaregiver/family members who take on signifi-cant responsibility. MS is changeable andunpredictable and people experience good andbad days. One day the person with MS can’thelp with transferring from the bed to a chairbut can make the move easily on a better day.
If disability is significant, there is a great dealfor the caregivers to manage:
� Personal care such as dressing, bathing,grooming, eating, toileting, exercising,transportation, and taking medication.
� Daily activities such as work, recreation,entertainment, exercise, hobbies, privatetime, religious practice.
� Household tasks including general cleaning,shopping, cooking, laundry, bill-paying,childcare, yard work, house maintenance,transportation.
� Training and supporting other caregivers,whether paid or volunteers, family mem-bers or employees, to ensure comfort andsafety for all. No solitary caregiver can do itall!
45
The National MS Society booklet “At Homewith MS” is a good starting point. It listsresources for equipment, plans, andvolunteers.
Caregivers
Caring for a loved one with a disabling chronicdisease at home can be deeply satisfying andat the same time challenging and exhausting.
44 Managing Progressive MS
Money matters
Be sure to discuss equipment purchases and
renovations with your tax advisor, your
health-care provider, your insurance compa-
ny, and staff at your Society chapter. If you
are employed, discuss your needs with your
state vocational rehabilitation program.
Equipment and renovations to meet medical
needs, with documentation from health care
professionals, are usually tax-deductible
medical expenses. Equipment or renovations
that enable you to be gainfully employed may
be funded by a state vocational rehab pro-
gram—or by your insurance policy. Your
Society chapter may know about community
resources, including volunteers to help.

matters. When the issues are bought out intothe open it takes the burden off both partners.Open and honest communication about sexualneeds and pleasures without fear of ridicule orembarrassment is the crucial first step.
It’s a partnership
Even with good information and equipment,caregivers cannot do everything alone. Thepotential for frustration, burn-out, and evenabuse is too great. The person with MS andthe caregiver need to be there for each other.Feelings of anger and frustration need a safeoutlet. The caregiver needs emotional support,time off, and a trusted counselor or advisor.Finding these necessary resources shouldinvolve a call to the nearest Society chapter.Many have programs for family caregivers.
47
The medical team can provide tips and teachtechniques for bathing, dressing, toileting, andsafe transfers. The National MS Society andother area resources can provide education forcaregivers and individuals with MS so thatthe safest and best practices are used from thebeginning. The Society is also a source of self-help groups, peer counseling, volunteers, andreferral to area resources, such as homehealth service providers, adult day programs,and respite care.
Sexual issues for partners
When MS becomes more severe, caregiverswho are also spouses or partners face morehurdles in their sexual relationship. It’s hardto switch gears if the caregiver bathes, toilets,grooms, and dresses the partner. The couplemay need new “cues” to initiate intimacy andset the stage for romance.
Psychological and social issues may make theperson with MS feel inadequate and unlov-able. What can be done to manage these prob-lems? The Society booklet, “MS andIntimacy” recommends considering a trainedsexual counselor. Counselors can help coupleswork through these delicate and important
46 Managing Progressive MS
Caregivers need
to give them-
selves care too.
Plan some time
away. Both part-
ners benefit.

The Society booklet, “A Guide forCaregivers” includes a valuable resourcesection.
Living with severe MS is truly unpredictableand exhausting. But—for both the person withMS, the family members, and caregivers—meeting the challenges offers deep rewards.
Avonex is a registered trademark of Biogen Idec.Betaseron is a registered trademark of Berlex, Inc.Botox is a registered trademark of Allergan, Inc.CamPath is a registered trademark of Genzyme Corporation.Novantrone is a registered trademark of Serono.Provigil is a registered trademark of Cephalon, Inc.Rebif is a registered trademark of Serono Pfizer.Tysabri is a registered trademark of Biogen Idec and Elan.Zenapax is a registered trademark of Hoffmann-La Roche Inc.
48 Managing Progressive MS