maryann walsh master's research project 2011
TRANSCRIPT

1
Weight Loss on WIC: Assessing the Level of Interest and Weight Loss
Success When a Weight Loss Program is Offered to Mothers Receiving
Benefits from the Women, Infants and Children Program
Maryann Walsh
Master Project
Submitted to the Graduate College of Bowling Green State University in partial
fulfillment of the requirements for the degree of
MASTER OF FOOD AND NUTRITION
April 2011
Project Committee:
Dr. Younghee Kim

2
Table of Contents
Introduction…………………………………………………………………………….4
Significance of the Problem……………………………………………………………4
Statement of the Problem……………………………………………………………...5
Significance of the Study………………………………………………………………6
Purpose of the Study…………………………………………………………………...6
Literature Review………………………………………………………………………6
The Women, Infants and Children Program………………………………....6
Behaviors/ Barriers to Weight Loss In Low-Income Women………………..8
Food Choices and Grocery Shopping Habits…………………………………11
The Use of Pedometers in Weight Loss………………………………………..13
The Use of Weight- Ins…………………………………………………………15
Weight Loss Protocol Design…………………………………………………..16
Methods………………………………………………………………………………….20
Overview………………………………………………………………………...20
Recruitment……………………………………………………………………..20
Inclusion Criteria……………………………………………………………….21
Exclusion Criteria………………………………………………………………21
Initial Contact with Participants……………………………………………....21
Secondary Contact with Participants………………………………………….23
Final Contact with Participants………………………………………………..24
Results…………………………………………………………………………………...24
Table 1…………………………………………………………………………...24

3
Table 2………………………………………………………………………….25
Sources………………………………………………………………………………….27
Appendix 1: Recruitment Flyer……………………………………………………….32
Appendix 2: Weight Loss on WIC Introductory Survey…………………………….33
4
Introduction
Before the advent of overly processed convenience and fast foods, being food
insecure typically meant being underweight and malnourished. In the present day with an
abundance of inexpensive, calorie dense foods available, the opposite has come to
fruition. As of 2008, the CDC has reported that 34% of the U.S. population is considered
obese (BMI of 30 or greater) (31). Government food assistance programs such as the
Supplemental Nutrition Assistance Program (Snap, formerly Food Stamps) and Women,
Infants and Children (WIC) help those that are food insecure by providing supplemental
foods (1)
The major difference in the foods offered by SNAP and WIC is that SNAP
provides an electronic funds transfer card which can be used to purchase any food item
the client desires (1). WIC however provides specific healthy food items including
protein sources (beans, peanut butter), whole grains (whole grain bread or brown rice and
cereals) fruits and vegetables, 100% juices and milk, cheese and eggs (2). Unfortunately,
even with food assistance programs like these that provide access to healthy foods, there
is still a prevalence of obesity in those with a low socioeconomic status (3).
Significance of the Problem
Due to insufficient access to affordable weight loss counseling/programs, women
with low socioeconomic status do not have the ability to receive weight loss guidance and
education. These women belonging to the lower socioeconomic groups also tend to be the
most in need of accessible weight loss/weight management programs.

5
Black and others at New York University critically reviewed ninety studies
published between 1997 through 2007 on neighborhood determinants of obesity through
the PubMed and PsychInfo databases. Their findings were that neighborhoods with
decreased economic and social resources have higher incidences of obesity. They also
found that residents of low-income urban areas would typically report greater barriers to
physical activity, such as limited opportunities for daily walking exercise and reduced
access to stores that sell healthy foods, especially large supermarkets (3).
The National Longitudinal Survey of Youth 1979 was utilized in a study
conducted at the City University of New York. The data showed that low-income women
who participated in the food stamp program demonstrated a 9.1% increase in the
predicted probability of current obesity (4). Possible explanations for this could be that by
having supplemental foods to have in the household, this leaves more funds available for
fast food and convenience food consumption.
This study will provide education as well as guidance for women on the WIC
program who desire to lose weight and make healthier choices each day.
Statement of the Problem
The less access that low-income individuals have to weight loss programs the
more likely this group is to remain overweight or obese. In turn, conditions that result
from overweight and obesity such as heart disease, diabetes, high blood pressure, etc. will
be more prevalent amongst the low-income; this will lead to higher public health care
expenses as well as many low-income individuals utilizing government funded health
care.

6
Significance of the Study
There is currently an insufficiency of studies examining the desire for low-income
women to lose weight and the success of these women to loss weight after a weight loss
program is initiated. The significance of this study is to gauge the success of a weight
loss program within the WIC program and if a weight loss program should be offered
within local WIC agencies.
Purpose of the Study
The purpose of this study is to design a weight loss protocol for either post-
partum women or mothers of children receiving WIC benefits. The protocol would
provide education on how to utilize the healthy foods that WIC offers as well as
education on meal planning and calorie consumption. A group of women would then be
recruited within the WIC agency to participate in the study. It is hoped that this study will
be able to demonstrate that it is possible for low income women to achieve a healthy
weight without having to spend money on expensive “diet food” including special
shakes, bars, frozen meals, etc.
Literature Review
The Women, Infants and Children Program
The WIC program is a supplemental food program that was created to serve those
women, infants and children in need of food assistance (5). Along with receiving food
vouchers (typically 3 months at a time in check form), prenatal and postpartum moms can
receive breastfeeding advice and all clients receive nutrition counseling regularly

7
(typically every 3-6 months). WIC currently serves over 9.1 million individuals in the
US. The goal of WIC is to enhance the nutrition status of Women, Infants and Children
with low income (1) In order to receive WIC a family must be at 185% of poverty,
receiving state cash assistance (TANF), receiving food stamps (SNAP) or be receiving
state medical assistance which are all indicators of a low family income. Therefore, when
a woman is actively receiving WIC’s services they fit the description of being low-
income.
When a woman is on WIC and she provides proof of a confirmed pregnancy and
that she is under prenatal care (typically a doctor’s note stating this information) then she
begins receiving WIC benefits. The food package for a pregnant woman varies from state
to state but generally looks like this: 5.5 gallons of milk (16 ounces can be used towards
cheese), 1 jar of peanut butter, 4 cans of beans (or 1 pound of dried beans), 2 cans of
concentrated juice, 2 dozen eggs, 36 ounces of select cereals, choice of 2 loaves of whole
grain bread or 2 one pound bags of brown rice, and a $10 voucher for fresh, frozen or
canned fruits and vegetables (2).
Once a pregnant woman on WIC gives birth, she then is eligible to receive the
following: the same food package as a pregnant woman, minus 1.5 gallons of milk, 1
dozen eggs and minus the bread/rice option. If the woman is partially breastfeeding she
receives the same as the non-breastfeeding client but with additional milk and juice and
she also receives bread. Lastly, when a woman is fully breastfeeding she receives the
largest food package: The same as a pregnant woman with the addition of 6 cans of tuna,
pink salmon or sardines (2).
8
In 1974, years after the initiation of the WIC program, the food packages began to
follow guidelines that coincided with the Dietary Guidelines for Americans. This came
about when the USDA found that when proper nutrition (including the dietary guidelines
of macro and micronutrients) was provided for low-income mothers, Medicaid cost
savings averaged $12-15,000 per infant. This was exciting news that further emphasized
the importance of the WIC program. In 2009, the WIC program upgraded their food
packages again replacing items like 2% and whole milk for children over 2 with 1% and
skim milk as well as replacing white breads with whole grain breads. These changes were
in place to emphasize the importance of the prevention of obesity, which since 1974 had
reached epidemic proportions (6)
Behaviors/ Barriers to Weight Loss In Low-Income Women
While it may be clear that a large number of women participating in the WIC
program are overweight (BMI of 25-29.9), not all may have the desire or interest to lose
weight. An important element of designing the protocol is to include an initial evaluation
of reservations/barriers and motivators. In previous studies of weight loss programs in
low-income women, participants identified higher self-esteem, the ability to be more
physically active, better health, and less societal prejudices toward them as benefits to
losing weight. Barriers to weight loss included lack of personal effort, lack of social
support, inadequate finances, and low self-esteem. Participants believed that group
support weight loss programs modeled after Weight Watchers® would be beneficial (7).
Another factor to consider in post partum weight loss is the amount of stress that
the mother may be under. One study showed that stressful experiences triggered
9
emotional eating and reduced participants' ability to practice healthy eating behaviors (8).
Other factors—for example, wanting quick weight-loss results—made it difficult for
these mothers to follow recommended healthful lifestyle practices. Nutritionists/dietitians
can address these concerns by including information about ways to deal with stress and
emotional eating and emphasizing the benefits of healthful eating and physical activity in
their program plans.
The mental health status of the participant must be considered as well when
initiating a weight loss program. The prevalence of post partum depression is
significantly higher in lower-income women compared to more affluent women (29).
Two hundred and nineteen families were examined by self-reporting depression for low-
income rural women experiencing depressive symptoms. Just over one half (52.5%) of
respondents who were experiencing depressive symptoms self-reported depression,
whereas 47.5% of respondents self-reported no depression. Women reporting depression
were significantly likelier to report physical health problems, injury/illness, and more
frequent physician visits. Women reporting no depression were significantly likelier to
have been pregnant in the previous 3 years. The study concluded that women reporting
depression had more health care system exposure and perhaps depressive symptomology
knowledge. Public health campaigns should educate about depressive symptoms,
including postpartum depression, to reduce stigma and increase treatment seeking (9).
In Sonoma Country California (an area with a high Hispanic population) a study
was done to assess depression symptoms in women under 45 years old in five California
counties. A significant negative association was found between the number of people in
the household and depressive symptom scores, that is, with fewer people in the household
10
depression increased (15). This result may indicate the need for a support system that is
more accessible to individuals in smaller households or it may be an artifact of Hispanics
having larger families and lower depression scores. The results indicated that there is a
critical need to provide mental health resources to low-income women, especially those
with young children as well as consider the mental health of a participant of a weight loss
program.
Eating habits in early post-partum need to be considered when conducting a
weight loss study on post-partum women. In a study focusing on early post-partum
women, The Eating Stimulus Index (ESI) was given to participants in order to determine
the relationship between motivations to eat with diet quality and food intake in 115
overweight/obese, low-income women in early postpartum (10). Regression analysis
indicated that convenience-eating resistance was the strongest predictor of diet quality in
the post partum women, followed by vegetable taste preference, and the availability of
fruits and vegetables. Convenience eating resistance was also the strongest predictor of
discretionary energy intake. This study was valid because it showed the importance of
knowing your clients ability to access certain foods before expecting them to eat these
certain foods. This study also showcased the validity of the ESI as a useful tool in dietary
behavior assessment.
Another barrier to consider in healthy eating habits among low-income women is
their ability to budget their resources, whether it is a combination of personal income and
food vouchers or just food vouchers (food stamps, WIC checks, etc). Tarasuk and others
found that a woman's intakes of energy, milk products, and vegetables decreased
significantly as the time since she received income increased (16). When their food

11
security status was considered, women who were food secure or marginally insecure
showed no significant within-month patterns, but significant declines in energy,
carbohydrate, vitamin B-6, and fruit and vegetable intake were observed for women with
moderate or severe adult food insecurity. The food intakes of women in deprived
circumstances are sensitive to the decline in household resources following the receipt of
a monthly check. This indicates that it is necessary to provide education in meal planning
and in budgeting one’s food allowance within a weight loss program.
Food Choices and Grocery Shopping Habits
A crucial aspect of initiating any weight loss protocol is to evaluate the food
selection and consumption behaviors of the participants in the program. Wiig and Smith
set out to investigate factors affecting food choice and health beliefs among low income
women taking into consideration their weight and socioeconomic status (11). Ninety-two
low-income women ages 18-65 with at least 1 child age 9-13 were asked to participate in
focus groups. The results were extremely interesting: 75% had a BMI over 25 and most
were in charge of doing the grocery shopping for the families. Many of the women
blamed their health problems such as hypertension, overweight/obesity and diabetes on
genetics or their metabolism. Many of the women claimed they enjoyed eating fruits and
vegetables but the cost was what deferred them from eating more of them. This clearly
shows that there needs to be more adequate education on how to better stretch one’s food
dollar especially when supplemental nutrition programs are being utilized.
Wiig and Smith also set out to examine grocery shopping behaviors and food
stamp usage of low-income women with children to identify factors that influence their
food choices on a limited budget (12). This study also utilized focus groups. Ninety-two
12
women, of whom 76% were either overweight or obese with a mean age of 37 were given
a grocery list consisting of 177 items. Each participant was asked to prioritize the items if
they only had $50 to spend (this number was taken from the average amount of food
stamp allotment). Surprisingly meats were given highest priority, and the biggest barriers
to buying, and transportation and store accessibility were listed as most common barriers
to shopping frequency. Participants used various strategies to make their food dollars
stretch by buying what was on sale (even if these items were not the healthiest of
choices). This study clearly showed that the participants needed to be taught strategies to
prepare meals without as much meat, which is typically expensive and can be high in
saturated fat and cholesterol. Also, it appeared to be necessary to better educate the
participants on how to purchase fruits and vegetables more cost effectively (frozen or
canned instead of fresh).
Wiig and Smith most recently conducted a cross-sectional study that investigated
low-income, urban Minnesotan women's past-month food purchases and their
associations with race, homelessness, and aspects of the food system, including food
shelf (food pantry) and food store usage (13). These associations were factors believed to
influence food choice and grocery shopping behavior. The subjects were surveyed on
demographics, the US Department of Agriculture’s 18-item Household Food Security
Survey Module, and grocery shopping questions related to food purchases and food
stores visited in the past month. Participants consisted of a convenience sample of 448
low-income, urban Minnesotan women, and the data was collected from February
through May 2008. The sample breakdown was as follows: 44% African American, 35%
American Indian, 10% white, and 11% other/mixed race; 37% were homeless. The rate of
13
“less healthy” food group purchases were higher compared to “healthy” food group
purchases. One extremely interesting finding was that food shelf (food pantry) usage
increased the odds of purchasing less healthy choices at supermarkets. Also, it was seen
that race has a direct relationship to protein choices but not to fruit, vegetable and whole
grain choices. This information solidifies the fact that in a research study such as the one
being conducted it is necessary to help develop strategies on how any money available
for food should be spent.
Another important factor to consider is the ambition of the women to go and
utilize her supplemental food checks. In a rather large study focusing on 454 participants
86% were Hispanic, 7% non-Hispanic black, and 7% of other ethnic backgrounds.
Participants reported purchasing a wide variety of items (14). The 10 most frequently
mentioned items were oranges, apples, bananas, peaches, grapes, tomatoes, carrots,
lettuce, broccoli, and potatoes. In conclusion, low-income women used the supplement
provided almost fully, and purchased a wide variety of fresh fruits and vegetables for
their families. No particular barriers arose to redemption of the vouchers by either the
participants or the retail vendors.
The Use of Pedometers in Weight Loss
The plan for the study is to make it as convenient as possible for the clients
participating in the study to fully participate. Pedometers are being given to each
participant as well as instructions on how to use the pedometer and how to incorporate
them into their everyday lives. In a meta-analysis focused on the use of pedometers in
weight loss interventions participants lost an average of 1.27 kg (.05 kg per week) during
the interventions (17).
14
When pedometers were given to sedentary office workers, average steps per day
went from 7,029 ± 3,100 (SD) at baseline to a plateau of 10,480 ± 3,224 steps/day by
3.96 ± 3.28 weeks of the intervention. On average, participants experienced significant
decreases in BMI, waist girth, and resting heart rate. Reductions in waist girth and heart
rate were significantly related to the increase in steps per day. In addition, reductions in
BMI were predicted by the initial steps per day (18).
Another systematic review showed very similar results when adding a pedometer
to a weight loss program: pedometer users significantly increased their physical activity
by 2183 steps per day over baseline (95% CI, 1571-2796 steps per day, P < .0001) (19).
Overall, pedometer users increased their physical activity by 26.9% over baseline. An
important predictor of increased physical activity was having a step goal such as 10, 000
steps per day (P = .001). When data from all studies were combined, pedometer users
significantly decreased their body mass index by 0.38 (95% CI, 0.05-0.72; P = .03).
These studies are encouraging because using pedometers is a convenient,
inexpensive and fun way to track steps and to encourage additional steps (such as using
the stairs instead of the elevator). Having a pedometer can significantly cause an increase
in physical activity when goals are set for the number of steps per day, and the fact that a
client’s own home or place of employment can be their “stepping ground” makes
pedometers a very convenient weight loss aid (20). An amount of 10,000 steps a day
(which is equivalent to about 5 miles) done by a 175lb male walking 2 mph burns 398
calories, which is an impressive amount of calories to burn while going about one’s day
(21).
15
The use of Weigh Ins
Monitoring of the participant’s progress is a crucial aspect of any weight-loss
program. With self-reporting of progress comes the occurrence of over and under
reporting, and not all participants may own scales so scheduled weigh-ins are often
necessary. Haq and others found that there was a significant difference between measured
and reported weight (mean difference=−3.75 lb, p=0.0001) and height (mean
difference=+0.35 in., p=0.0007). The mean difference between measured and reported
BMI was −1.14 kg/m2 (p=0.0001) (22). Unemployed, retired, or disabled women were
more likely to under-report their BMI than employed women (p=0.001). This is relevant
information because many of the clients of WIC are unemployed. Another interesting
finding within this study is that six percent of subjects who were initially considered
eligible for the study on the basis of the self-report were eventually excluded from the
study because they did not meet the inclusion criterion for BMI. This shows that it is
important to do an in-person weigh in when pre-screening the clients for participation,
without relying on self-reporting.
The frequency of weigh-ins is an aspect that needs to be considered. Butryn found
that 36.2% of study participants reported weighing themselves at least once per day, and
more frequent weighing was associated with lower BMI and higher scores on
disinhibition and cognitive restraint (23). Other participants who did not weigh daily still
showed favorable results; therefore this is an element that will have to be discussed with
the participant. The psychological outcome of weighing one’s self everyday (especially
without seeing results) can deter weight loss efforts for some, so this is an area that needs
to be explored with the participant individually.
16
Wing and others randomly assigned 314 participants who had lost a mean of 19.3
kg of body weight in the previous 2 years to one of three groups: a control group, which
received quarterly newsletters (105 participants), a group that received face-to-face
intervention (105), and a group that received Internet-based intervention (104) (24). The
content of the programs in the two intervention groups was the same, emphasizing daily
self-weighing and self-regulation, as was the frequency of contact with the groups. The
primary outcome was weight gain over a period of 18 months. As compared with
receiving quarterly newsletters, and the internet based interventions, a self-regulation
program based on daily weighing improved maintenance of weight loss, particularly
when delivered face to face, it was the most successful approach to weight loss
monitoring and maintenance.
Weight Loss Protocol Design
The creation of an effective weight-loss protocol requires careful planning and
consideration of the demographic involved. Gustafson and others set out to assess the
cost-effectiveness of a 16-week weight loss intervention (it was named “Weight-Wise”)
for low-income midlife women (25). The study design was a randomized controlled trial
conducted in North Carolina in 2007. It tested a weight loss intervention among 143
women (40–64 years old, mean BMI=35.1 kg/m). The participants were randomized to
one of two groups: special intervention (n = 72) and a wait-listed control group (n = 71).
The effectiveness of the study was measured in changes in weight, systolic and diastolic
blood pressure, total cholesterol, and HDL cholesterol.
Cost-effectiveness was measured by calculating life years gained (LYG) from
changes in weight, based on a years life lost (YLL) algorithm. The results showed that
17
intervention participants had statistically significant decreases in weight (kg) (−4.4 95%
CI=− 5.6, −3.2) and in systolic blood pressure (− 6.2 mm Hg, 95% CI=− 10.6, −1.7)
compared to controls. The total cost of conducting Weight-Wise was $17,403, and the
cost per participant in the intervention group was $242. (Both were funded by the
University of North Carolina School of Medicine and Public Health.) The incremental
cost per life year gained from a decrease in obesity was $1862. These results showed that
the “Weight-Wise” protocol is effective and could be considered for use in future group
weight loss programs for women with low income.
Often evidence-based interventions may not match the specific population or
health concern of interest. The Multisource Method (MSM), which, in combination with
a workshop format, may be used by health professionals and researchers in health
promotion program development (26). The MSM draws on deviating from past protocols
and processes, focus groups, community advisors, behavioral change theory, and
evidence-based strategies. The MSM can be a useful method to follow when you are
creating a protocol/program for a demographic which has not been previously
represented and when you have no earlier information to draw from.
Klohe-Lehman and others set out to examine if greater nutrition knowledge vs.
gains in knowledge promote more successful weight loss in low-income, overweight and
obese mothers with young children. The design consisted of a convenience sample of
mothers and their children who were measured for height and weight; mothers completed
demographic and nutrition knowledge questionnaires pre- and post intervention (27). The
141 participants were recruited from government and public health clinics and
elementary schools. Inclusion criteria for mothers were: family income <200% federal
18
poverty level; overweight/obese; and Hispanic, African-American, or white
race/ethnicity.
The intervention consisted of eight weekly weight- loss classes emphasizing diet,
physical activity, and behavior modifications based on the Social Cognitive Theory and
were administered to the mothers. The outcomes measured were: Improvements in
maternal nutrition knowledge and weight loss. Statistical Analyses Performed were:
Paired-samples t tests, repeated measures analysis of variance, analysis of covariance,
Pearson correlations, and x2 statistics. The results were that nutrition knowledge of
mothers increased in all areas. Participants with weight loss ≥2.27 kg (responders) had
greater knowledge than those who did not; the drawback however was that the actual net
gain was similar for those who lost and did not lose weight. Weight gainers only
improved in two areas on the test, whereas weight-loss responders increased knowledge
in all six.
Responders appeared more aware of diet, weight loss, and health information.
This study is an important reference because it shows that weight-management programs
should include a strong component of nutrition education to alleviate knowledge
inequalities and promote more effective weight control. In low-income mothers, greater
initial knowledge may be more predictive of weight loss than gains in knowledge during
an intervention. This is great knowledge to have going in to the said study that will be
conducted.
Jordan and others discussed the evaluation of a nutrition and physical activity
program for reducing body weight and improving nutrition attitudes in mothers of young
children. A convenience sample of 114 intervention mothers and 33 comparison mothers

19
was recruited from public health clinics and community centers (28). Eligibility criteria
included Hispanic, African American, or white ethnicity; body mass index of at least 25
kg/m, low income (<200% of the federal poverty index); and youngest child aged 1 to 4
years. For intervention participants, height, weight, percentage of body fat, waist
circumference, demographics, nutrition attitudes, and dietary intake were measured at
weeks 0 and 8; height, weight, percentage of body fat, and waist circumference were
reassessed at 6 months. Overweight mothers in the comparison group provided
anthropometric and demographic data at weeks 0 and 8. Changes in anthropometrics,
attitudes, and dietary intake were evaluated in intervention mothers. Anthropometric data
of intervention vs. comparison group mothers were examined. Differences in
anthropometrics and attitude scores between weight loss responders (≥2.27 kg) and non-
responders (<2.27 kg) were assessed at week 8. Intervention participants lost weight, an
average of −2.7 kg. Comparison mothers gained a slight amount of weight, an average of
.1 kg by week 8. Weight loss responders had healthier eating attitudes and fewer
perceived barriers than the non-responders post-intervention. In conclusion, the dietary
and physical activity curriculum studied is a valuable resource for weight management
programs serving low-income women.
A meta-analysis found thirteen study interventions centered solely on diet
modification, five focused only on physical activity, and five concentrated on a
combination of both (30). The preponderance of studies targeted WIC and urban
recipients. While the majority of intervention studies supported the use of the
Transtheoretical Model of Change (TTM) for weight loss and preventing weight gain,
researchers noted that challenges still exist and further interventions are needed.
20
Methods
Overview
The study will take place from mid-January to mid-March and will focus on providing
informal, individualized weight loss education and recommendations for mothers who
participate in the WIC program. By using an open-ended approach it will allow the
women to talk one on one with a nutritionist and ask questions and gain insight as to how
they can change their eating habits in order to lose weight.
Due to the varying levels of financial resources and access to safe venues for exercise
among the mothers, pedometers are being given to the mothers. The pedometers will be
provided in order to provide a simple to use, inexpensive way for the women to track
their daily steps and make them aware of opportunities for daily exercise within their
individual lives. The researcher is providing funding for the pedometers. Reporting of
steps will not be required from the women, however at the end of the study the women
will be required to disclose how often and to what extent they used the pedometers.
Recruitment
Recruitment of participants will begin the project. Information flyers will be posted in
two WIC office locations, both of which are run by the same agency (Tri-Town
Community Action Agency of Johnston, RI). Contact information in the form of both e-
mail and office phone number of the student who is conducting the project will be given
on the flyer. This sign will be posted at the beginning of December and recruitment will
take place from December to mid January (Appendix 1). All data recorded during contact
with the participants will be recorded in Table 1.
21
Inclusion Criteria
The following is the inclusion criteria for the program:
Must either be on WIC as a post-partum or breastfeeding mother –or-
Must have at least 1 child on WIC
Must be either a client of the two office’s participating in the program or must be
able to travel to either of the offices.
Must be able to walk (for the pedometer portion of the program)
Exclusion Criteria
The following is exclusion criteria for the program:
Not being on WIC or having a child on WIC
Those who are currently pregnant or are planning on becoming pregnant between
mid January to the end of March.
Initial Contact with Participants
Initial contact will begin with the planning of 2-3 initial meeting times. The woman will
choose a meeting date and time that works best with their schedule. Those who cannot
make it to the set meeting times will then be offered an individual appointment with the
administrator of the study.
During the initial meeting, participants’ height, weight and waist circumference will be
taken as the baseline data. The participants will then be asked to write down their biggest
barrier to weight loss and to also fill out a short informative survey (Appendix 1). While
they are filling out the survey the administrator will calculate the basal metabolic rate of
22
each participant and then multiply by 1.2 (sedentary) for every participant, regardless of
what they may self report for their typical daily exercise.
Next the participants will each be given a pedometer and will be instructed how to
use it to incorporate physical activity into their daily routines. Afterwards, the
participants will be given a general “pep talk” about healthier eating focusing on whole
grains, fruits and vegetables (the importance of them and how to stretch one’s food
budget to include more of them) as well limiting sugars and watching caloric intake.
The “pep talk” will be an interactive, open-forum group conversation outlined as follows:
1. Swapping refined, white breads for whole grain versions
a. Why whole grains are healthier
b. Why they aid in weight loss
c. How to find inexpensive whole grain products
2. Incorporating fruits and vegetables into one’s daily diet
a. Why fruits and vegetables are so important to human health
b. Why fruits and vegetables aid in weight loss
c. How to stretch one’s dollar when buying fruits and vegetables
3. Limiting sugars in one’s diet
a. The importance of cutting out sugar sweetened beverages completely
b. How to choose foods low in sugar
c. Why excessive sugar hinders weight loss
23
4. Calorie counting/watching
a. Why calorie counting is an effective way to keep one’s diet under control
b. How to count calories easily while practicing portion control
c. How calorie counting equates to weight loss
The purpose of the pep talk is to educate and provide a forum for the participants to ask
questions and learn. The participants will not be tested in any way on the information
given. It is hoped that the 24-hour recall taking place in the second contact will reflect the
initiation of practicing the habits associated with the education provided. After the brief
educational portion of the initial contact session, the participants will be given contact
information, both email and office telephone number of the program administrator. They
will be encouraged to call the administrator whenever questions should arise or if they
just need some motivational words or ideas. The participants will be sent on their way
and will be given a date approximately 1 month from the present date to come to the WIC
office for a weigh in. Monthly weigh ins will be scheduled 2 times throughout the
program after the initial weigh in, 1 to mark the mid-way point and 1 more for the final
assessment.
Secondary Contact with Participants
Secondary contacts will be arranged by appointment with each participant. The
participant’s weight will be taken and then the participant will have time to discuss how
the first month went and what they think they need help improving upon. Each
24
participants will also be asked to provide a 24 hour recall. It is hoped that this 24 hour
recall will help assess the participant’s compliance with the healthy eating habits
discussed at the initial contact.
Final Contact with Participants
The third and final contact with the participants will be scheduled as a group meeting like
the first contact and will take place after 2 months. At this time weight and waist
circumference will be taken. The participants will be given an opportunity to discuss as a
group how they feel about their weight loss (if any weight was lost).
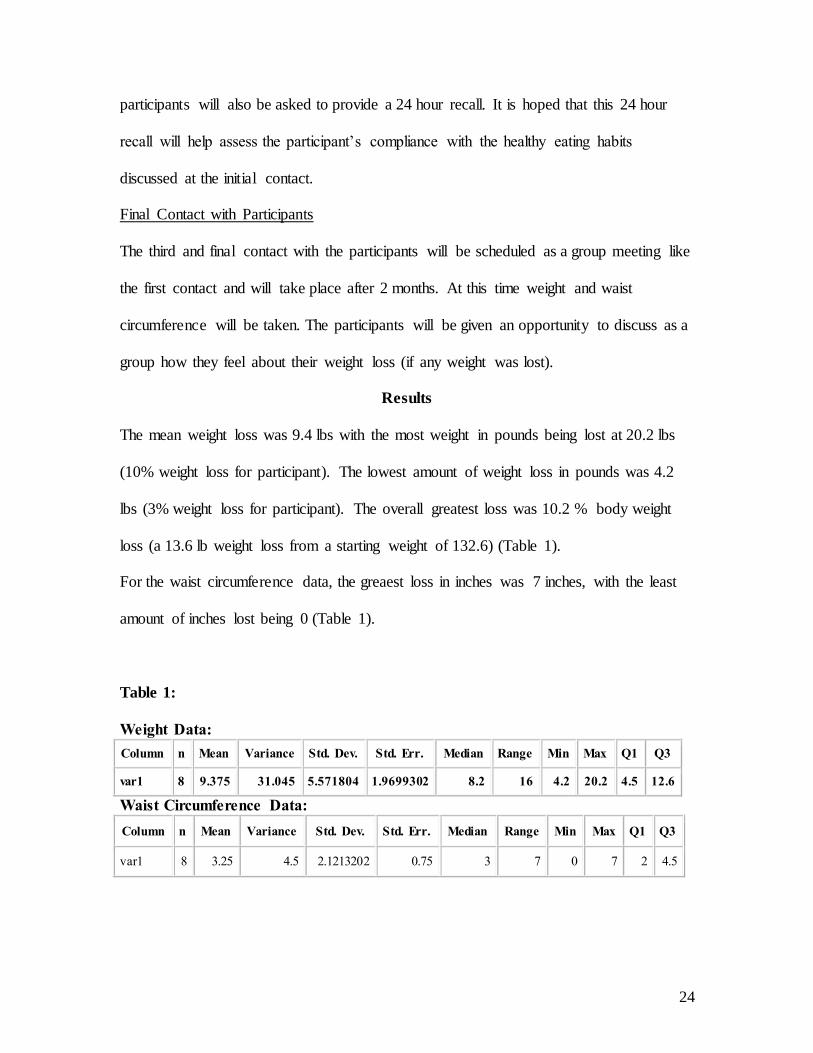
Results
The mean weight loss was 9.4 lbs with the most weight in pounds being lost at 20.2 lbs
(10% weight loss for participant). The lowest amount of weight loss in pounds was 4.2
lbs (3% weight loss for participant). The overall greatest loss was 10.2 % body weight
loss (a 13.6 lb weight loss from a starting weight of 132.6) (Table 1).
For the waist circumference data, the greaest loss in inches was 7 inches, with the least
amount of inches lost being 0 (Table 1).
Table 1:
Weight Data:
Waist Circumference Data:
Column n Mean Variance Std. Dev. Std. Err. Median Range Min Max Q1 Q3
var1 8 9.375 31.045 5.571804 1.9699302 8.2 16 4.2 20.2 4.5 12.6
Column n Mean Variance Std. Dev. Std. Err. Median Range Min Max Q1 Q3
var1 8 3.25 4.5 2.1213202 0.75 3 7 0 7 2 4.5

25
Table 2:
Initial Contact
Anthropometrics
1 (63in)
2 (65.5in)
3 (61in)
4 (59in)
5 (60in)
6 (68in)
7 (60.5in)
8 (62in)
Weight (lbs) 152 169.4 137.8 128.4 132 202.2 165.4 132.6
Waist
Circumference (inches)
33 37 41 29 28 44 39 26
Secondary Contact
Anthropometrics Use Pedometer?
1 (63in) Yes
2 (65.5in) Yes
3 (61in) No
4 (59in) Yes
5 (60in) Yes
6 (68in) No
7 (60.5in) Yes
8 (62in) Yes
Weight (lbs) 145.8 167.2 142.2 124 134.8 191 167.6 129.2
Waist
Circumference (inches)
32 37 42 28 28 41 39 26
Final Contact
Anthropometrics
Use Pedometer?
1 (63in)
2 (65.5in)
3 (61in)
4 (59in)
5 (60in)
6 (68in)
7 (60.5in)
8 (62in)
Weight (lbs) 140.4 164.6 133.6 120 127.8 182 157.4 119
Waist Circumference (inches)
28 37 39 26 26 37 35 23
Discussion
It is evident through the data that the program was a success. When the second
contact occurred and 3 of the 8 clients has gained weight, it prompted that student
researcher to ask each participant (including those who had lost weight) if there was
anything they would like to change/add to the program. Four of the 8 participants
mentioned that they felt their success could be greater if they could be “checked up on”
each week between the monthly weigh-ins. All participants, including those who had not
expressed initial interest in the weekly contacts from the researcher agreed to take part in
26
them. It was decided that due to the fact that all of the participants had cell phones with
text messaging capabilities (as well as the researcher) that weekly “text check-ins” would
be appropriate on Fridays to provide motivation to continue healthy eating habits
throughout the weekend. The researcher would text message each of the 8 participants
each Friday afternoon and ask how they were doing and what their plans were for the
weekend, if plans included a party or social situation where food was involved the
researcher would call the client to obtain more information and provide motivation and
tips on how to not overindulge while still enjoying themselves. The participants
expressed that these weekly “text check-ins” helped keep them on track with their healthy
eating and gave them motivational strategies to continue to stick with their healthy eating
habits.
Besides the weekly “text check-ins” a majority of the clients expressed approval
of the informal nutrition counseling sessions incorporated into their monthly weigh-in
contacts. It was hoped that the informality of the monthly contacts would initiate an open
forum for the participants to ask questions and discuss barriers to losing weight all while
helping to develop strategies for continuing their weight loss success or maintaining their
weight loss if their desired weight was reached.
Lastly, 6 of the 8 participants claimed that they used the pedometers between the
1st and 2nd contact, while none of the participants claimed to use the pedometers by the 3rd
contact. In hopes of keeping the process as simply and unintimidating as possible the
participants were not required to track their pedometer use, perhaps had they been
required to even greater weight loss results would have been seen. The pedometers main
purpose was to serve as an incentive and as a fun way to encourage physical activity
27
Sources
1. United States Department of Agriculture. “Supplemental Nutrition Assistance
Program” Accessed October 1, 2010. http://www.fns.usda.gov/snap/
2. United States Department of Agriculture. “ Women, Infants and Children
Program” Accessed October 1, 2010.
http://www.fns.usda.gov/wic/benefitsandservices/foodpkg.htm
3. Jennifer L Black, James Macinko (2008). Neighborhoods and obesity. Nutrition
Reviews 66 (1), 2–20. doi:10.1111/j.1753-4887.2007.00001.x
4. The American Society for Nutritional Sciences J. Nutr. 133:2225-2231, July 2003
5. United States Department of Agriculture. “The WIC Program: WIC Eligibi lity
Requirements” Accessed September 29, 2010.
http://www.fns.usda.gov/wic/howtoapply/eligibilityrequirements.htm
6. Gail C. Frank. Changes in WIC Food Packages: An Opportunity to Address
Obesity. Obesity Management. December 2008, 4(6): 333-337.
doi:10.1089/obe.2008.0245.
7. Lambert, Laurel, PhD,RD,etal. Perceived Benefits and Barriers Related to Post
Partum Weight of Overweight/Obese WIC Program Particpants. Topics in
Clinical Nutrition. January 2005, 20 (1): 16-27

28
8. Change, Mei Wei, PhD, RN ,etal. Motivators and Barriers to Healthful Eating and
Physical Activity Among Low Income Overweight and Obese Mothers. Journal
of the American Dietetic Association. June 2008, V. 108, (6) 1023-1028.
9. Simmons, LeeAann, PhD, etal. Low Income Rural Women and Depression:
Factors Associated with Self Reporting. American Journal of Health
Behavior,Novebmer 2007, V. 31 (6) 657-666.
10. Cahill,Jodi, Freeland-Graves, Jeanne, Bijal, Shah, Lu, Hongxiong Motivations to
eat are related to diet quality and food intake in overweight and obese, low-
income women in early postpartum. Appetite; Oct2010, Vol. 55 Issue 2, p263-
270, 8p
11. Dammann, Kristen Wiig; Smith, Chery. Factors Affecting Low-income Women's
Food Choices and the Perceived Impact of Dietary Intake and Socioeconomic
Status on Their Health and Weight. Journal of Nutrition Education & Behavior,
Jul/Aug2009, Vol. 41 Issue 4, p242-253, 12p, 2 Charts; DOI:
10.1016/j.jneb.2008.07.003;
12. Wiig, Kristen, Smith, Chery. The art of grocery shopping on a food stamp budget:
factors influencing the food choices of low-income women as they try to make
ends meet. Public Health Nutrition; Oct2009, Vol. 12 Issue 10, p1726-1734
13. Kristen Wiig; Smith, Chery . Race, Homelessness, and Other Environmental
Factors Associated with the Food-Purchasing Behavior of Low-Income Women.
29
Journal of the American Dietetic Association; Sep2010, Vol. 110 Issue 9, p1351-
1356, 6p
14. Herman, Dena, PhD, RD, MPH, etal. Choices made by Low Income Women
Provided with an Economical Supplement for Fresh Fruit and Vegetable
Purchase. Journal of the American Dietetic Association. May 2006, Vol. 106 (5)
740-744.
15. Block, Amy Joy, High Risk of Depression Among Low Income Women Raises
Awareness About Treatment Options. California Agriculture. January-March
2010. 64 (1) 22-25.
16. Tarasuk, Valerie, etal. Low Income Women’s Dietary Intakes are Sensitive to the
Depletion of Household Resources in One Month. The Journal of Nutrition,
August 2007. 137:1980-1987.
17. Richardson, Caroline, MD, etal. A Meta-Analysis of Pedometer Based Walking
Interventions and Weight-Loss. Annals of Family Medicine. 2008, 6:69-77
18. Chan, Catherine B. PhD, etal. Health Benefits of a Pedometer Based Physical
Activity Intervention in Sedentary Works. Preventative Medicine December 2004.
Volume 39, Issue 6,Pages 1215-122.
19. Bravada M Dina, MD,MD etal. Using Pedometers to Increase Physical Activity
and Improve Health. Journal of the American Medical Association, November
2007, 298(19):2296-2304.
30
20. WebMD. “Pedometers Get You Moving” Accessed on September, 29, 2010.
http://www.webmd.com/fitness-exercise/news/20071120/pedometers-get-you-
moving
21. About.com/Haskill etal. “Walking Calories Calculator”
http://walking.about.com/library/cal/uccalc1.htm
22. Haq, Nawaz MD,MPH, etal. Self Reported Height and Weight: Implications for
Obesity Research. American Journal of Preventative Medicine. May 2001,
Volume 20, Issue 4 , Pages 294-298.
23. Butryn, Megan, etal. Consistent Self Monitoring of Weight: A Key Component of
Successful Weight Loss Maintenance. Obesity,2007. 15, 3091–3096;
24. Wing, Rena, PhD, etal. A Self Regulation Program for Maintenance of Weight
Loss. New England Journal of Medicine, October 2006, 355:1563-1571.
25. Gustafson, Alison, etal. Cost-effectiveness of a behavioral weight loss
intervention for low-income women: The Weight-Wise Program.Preventive
Medicine; Nov2009, Vol. 49 Issue 5, p390-395, 6p
26. Walker, Lorraine O. etal. Developing Health Promotion Interventions: A
Multisource Method Applied to Weight Loss Among Low-Income Postpartum
Women. Public Health Nursing; Mar/Apr2010, Vol. 27 Issue 2, p188-195, 8p

31
27. Klohe-Lehman, Deborah M., etal. Nutrition Knowledge Is Associated with
Greater Weight Loss in Obese and Overweight Low-Income Mothers.Journal of
the American Dietetic Association; Jan2006, Vol. 106 Issue 1, p65-75, 11p
28. Jordan, Kristine C. etal. A nutrition and physical activity intervention promotes
weight loss and enhances diet attitudes in low-income mothers of young
children.Nutrition Research; Jan2008, Vol. 28 Issue 1, p13-20, 8p
29. Segre, Lisa, etal. The Prevalence of Post-Partum Depression: The Relative
Significance of Three Social Status Indices.Social Psychiatriy and Psychiatric
Epidemiology. October, 2007. 42 (4) 316-321
30. Judith S MacAlpine, "A review of effective weight loss and/or weight gain
prevention for disadvantaged populations" (January 1, 2009). Texas Medical
Center Dissertations.
31. Centers for Disease Control and Prevention. “Obesity and Overweight” Accessed
on October, 1, 2010. http://www.cdc.gov/nchs/fastats/overwt.htm
32
Appendix 1
Looking to shed some pounds in
2011?
Participate in the “Weight Loss on WIC Study” taking place this January through March.
Requirements to Participate:
Must be either a post-partum mom on WIC or a mom with children receiving WIC benefits.
Must be 18 or over.
Must be able to make it to this WIC office 3 times throughout the 2 month study.
Contact Maryann Walsh to register or for more info: [email protected]
401-519-1933
33
Appendix 2
Weight Loss on WIC Introductory Survey Name:__________________________
Email:____________________________
Phone:______________________________
Date of Birth:________________ Height:____________
Current Weight:_________
Goal Weight:_________
Current Waist Circumference:_________
Please briefly describe past weight loss efforts/programs which you have tried (if any):
What did you like/dislike about these methods/programs:
What is your biggest challenge to weight loss?
Do you have any medical conditions that would affect your weight loss on this program?