maryland county health team -...
TRANSCRIPT
MARYLAND COUNTY HEALTH TEAM
2017 ANNUAL REVIEW PRESENTATION
PRESENTED BY: CYRUS B. SNEH

OVERVIEW OF THE COUNTY HEALTH SYSTEM
Maryland has a current population of 163,898
25 health facilities (1 hospital, 4 health centers, 20 clinics)
Private: 3 Public: 22
Six(6) health districts (Harper, Pleebo , Karluway 1&2 and Barrobo
Whojah and Farjah) currently combined to form 4 District Health
Teams (DHTs)
57% of the population has access to healthcare within 5km or 1
hour walk
Health facility per 10,000 population ratio is 2.5 (Global target is 2)
513 health workers (26% core clinicians)
8.5 clinicians per 10,000 population (Global target is 23)
Private sector contribution/involvement:
This sector contributes to availability of drugs where drugs are
stocked-out or unavailable in county depot or at health facility via
transport of medicines from NDS or direct provision of these
medicines and supplies
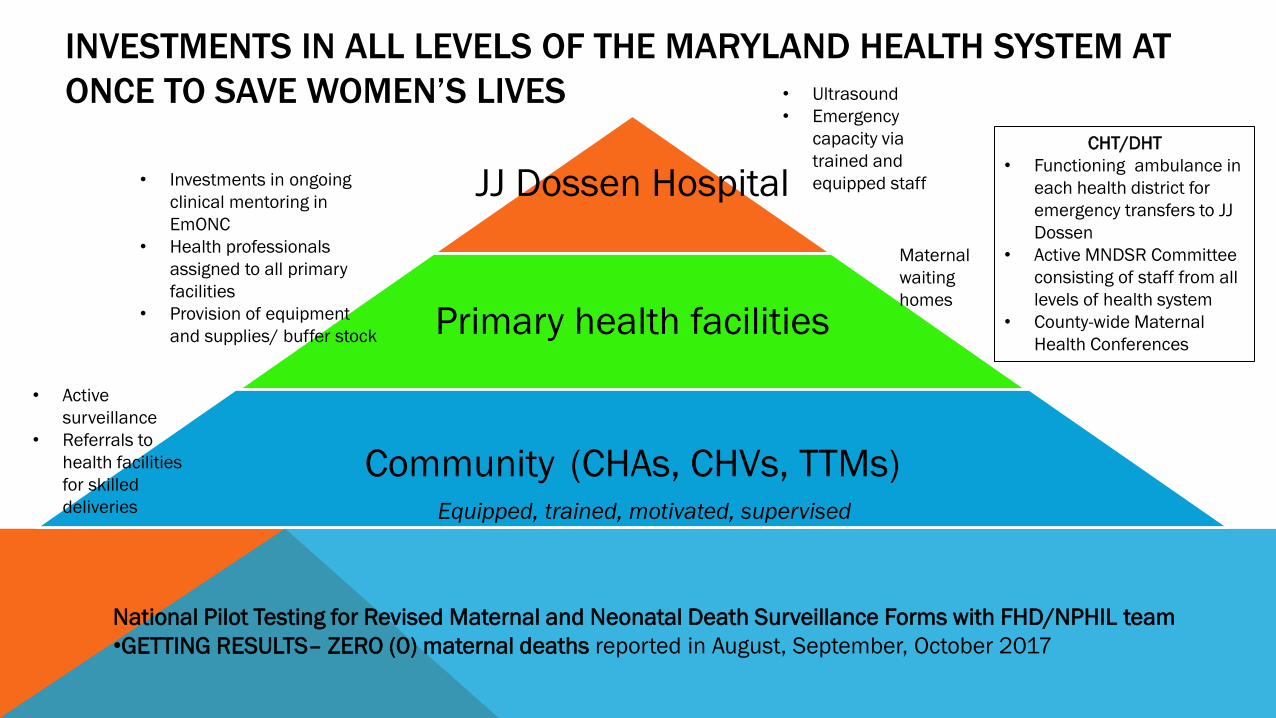
INVESTMENTS IN ALL LEVELS OF THE MARYLAND HEALTH SYSTEM AT
ONCE TO SAVE WOMEN’S LIVES
JJ Dossen Hospital
Primary health facilities
Community (CHAs, CHVs, TTMs)
CHT/DHT
• Functioning ambulance in
each health district for
emergency transfers to JJ
Dossen
• Active MNDSR Committee
consisting of staff from all
levels of health system
• County-wide Maternal
Health Conferences
Equipped, trained, motivated, supervised
• Active
surveillance
• Referrals to
health facilities
for skilled
deliveries
• Investments in ongoing
clinical mentoring in
EmONC
• Health professionals
assigned to all primary
facilities
• Provision of equipment
and supplies/ buffer stock
• Ultrasound
• Emergency
capacity via
trained and
equipped staff
Maternal
waiting
homes
National Pilot Testing for Revised Maternal and Neonatal Death Surveillance Forms with FHD/NPHIL team
•GETTING RESULTS– ZERO (0) maternal deaths reported in August, September, October 2017
2016/2017 KEY ACHIEVEMENTS • Launching of National Community Health Assistant Program
• 20 CHSS and 114 CHA recruited, trained and compensated and 208 active Community Health Committees holding monthly meetings(UNICEF support)
• Rollout of CBIS (reporting started since August 2017) through current partnership with PIH (through UNICEF support)
• Launching of NCD clinic at JJ Dossen Hospital as proof of concept for national NCD program
• 170 active patients followed through twice weekly clinic for diabetes, hypertension, sickle cell disease, splenomegaly, CHF, COPD, epilepsy, etc; growing wait list of patients
• Strengthening of Mental Health Services
• 669 patients actively in care and support for mental illness at JJ Dossen, Pleebo Health Center, and Harper Prison
• 40 homeless and formerly homeless patients with mental illness currently in ongoing treatment; a few patients who’ve made dramatic recovery are currently working with PIH
2016/2017 KEY ACHIEVEMENTS
Surveillance: Surveillance is functional at all levels beginning with the community/HF, district and county levels in all 4 health districts.
--CHA,CHSS operate at the community/ HF,
--Surveillance officers at district and county levels.
--CHSS function as surveillance focal persons at the health facility
• Quality of health services: Improvement in the quality of care at facilities by :
• Provision of regular staff capacity building and on-the-job coaching and mentoring
• Formalization of Standard Operating Procedures, protocols and treatment guidelines
• HMIS: Through regular monthly review meetings and timely submission of HMIS reports, health information is being utilized in programmatic decision making
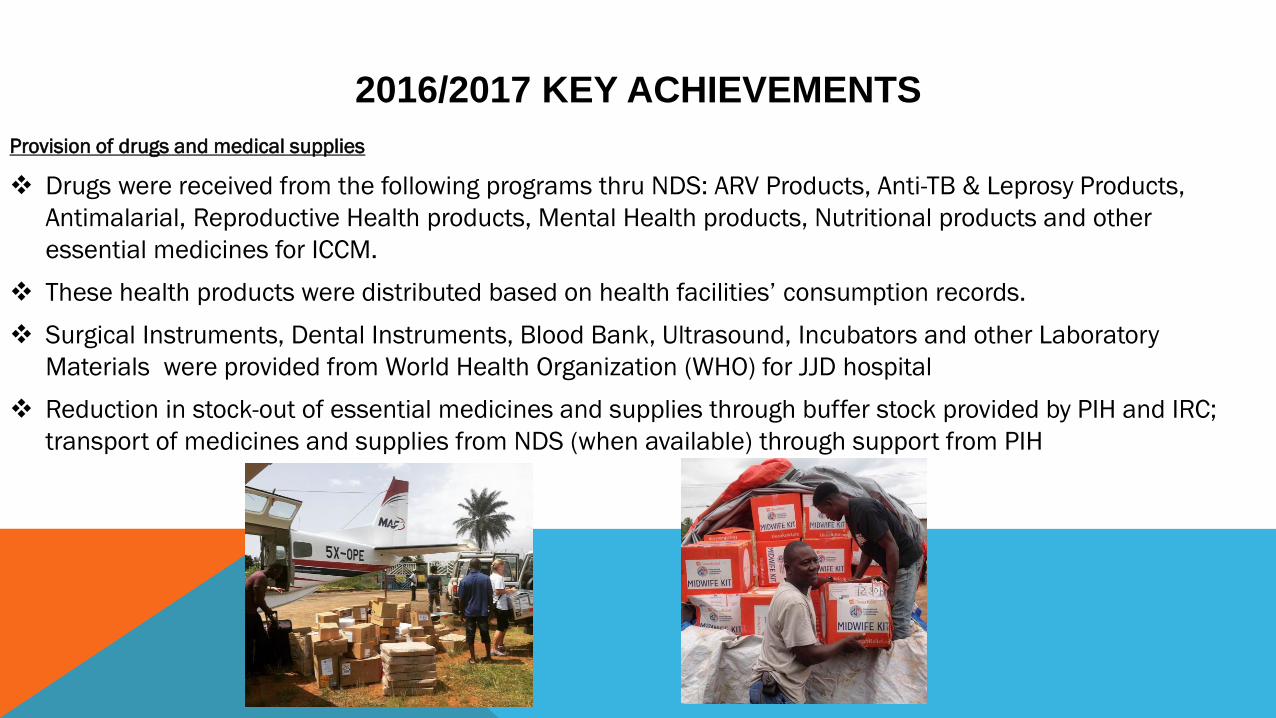
Provision of drugs and medical supplies
Drugs were received from the following programs thru NDS: ARV Products, Anti-TB & Leprosy Products,
Antimalarial, Reproductive Health products, Mental Health products, Nutritional products and other
essential medicines for ICCM.
These health products were distributed based on health facilities’ consumption records.
Surgical Instruments, Dental Instruments, Blood Bank, Ultrasound, Incubators and other Laboratory
Materials were provided from World Health Organization (WHO) for JJD hospital
Reduction in stock-out of essential medicines and supplies through buffer stock provided by PIH and IRC;
transport of medicines and supplies from NDS (when available) through support from PIH
2016/2017 KEY ACHIEVEMENTS

2016/2017 KEY ACHIEVEMENTS • Strengthening of Emergency Referral Pathway
• 1 Ambulance stationed in each of 4 health districts
• Referrals for specialized care via ambulance or flight via direct partnership with Jackson F Doe Hospital in Tappita
and JFK and ELWA in Monrovia through partnership between JJ Dossen Hospital leadership and PIH
• 1 surgeon at JJ Dossen providing emergency and elective surgeries along with JJ Dossen team
• 1 OB/GYN was present through beginning of 2017; another arriving next week
• Major improvements in TB case detection and treatment outcomes-
• 67 trained, supervised and compensated CHVs focused on TB/HIV/Leprosy active case finding, treatment support,
and linkages to clinical care, psychosocial support, monthly food packages in Harper and Pleebo districts
• Thanks to their strong efforts 774 patients were newly enrolled in TB treatment between June 215 and June 2017,
with 95% treatment success
• Establishment of MDR-TB treatment ward and rollout of Genexpert for regional testing and treatment for MDRTB in
the Southeast (part of NLTCP Decentralization strategy) at JJ Dossen
2016/2017 KEY ACHIEVEMENTS
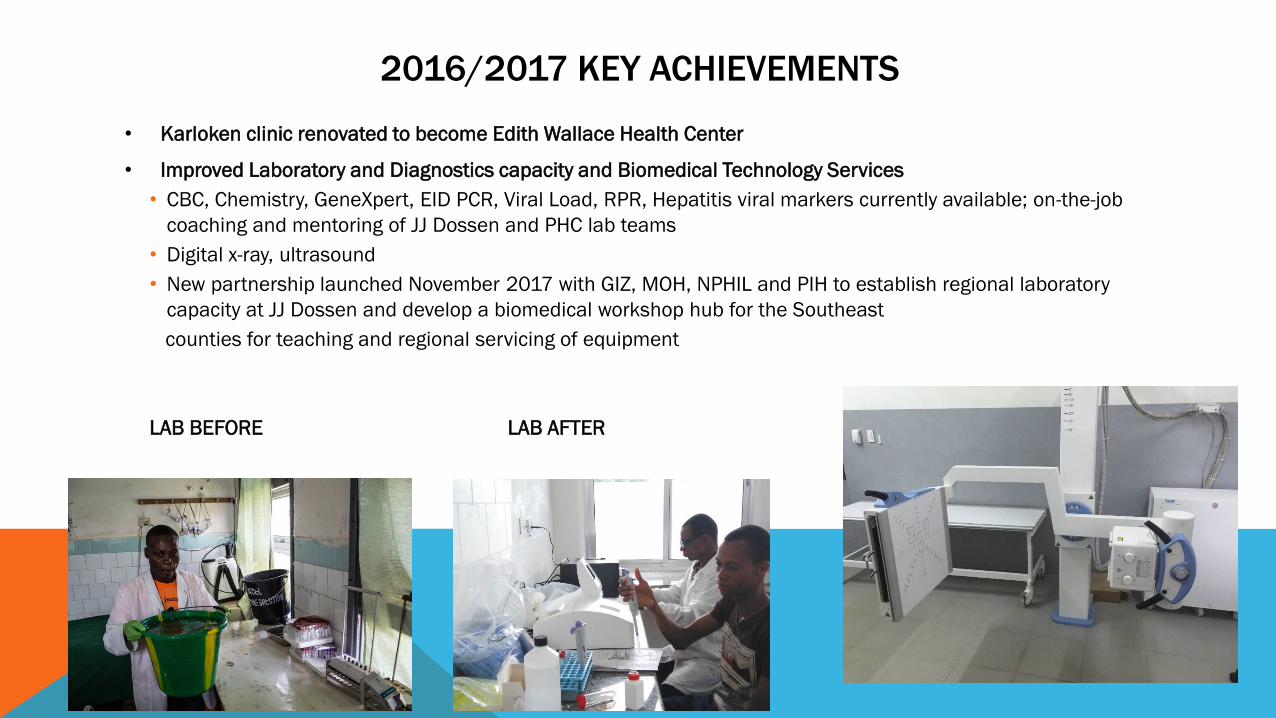
• Karloken clinic renovated to become Edith Wallace Health Center
• Improved Laboratory and Diagnostics capacity and Biomedical Technology Services
• CBC, Chemistry, GeneXpert, EID PCR, Viral Load, RPR, Hepatitis viral markers currently available; on-the-job
coaching and mentoring of JJ Dossen and PHC lab teams
• Digital x-ray, ultrasound
• New partnership launched November 2017 with GIZ, MOH, NPHIL and PIH to establish regional laboratory
capacity at JJ Dossen and develop a biomedical workshop hub for the Southeast
counties for teaching and regional servicing of equipment
LAB BEFORE LAB AFTER

NEW MATERNAL WAITING HOME
0
50
100
150
200
250
2015 2016 2017
Nu
mb
er
of
De
live
rie
s
YEAR
Glofaken Delivery 2015-2016
unskilled Delivery
Skilled Delivery
2016/2017 KEY ACHIEVEMENTS
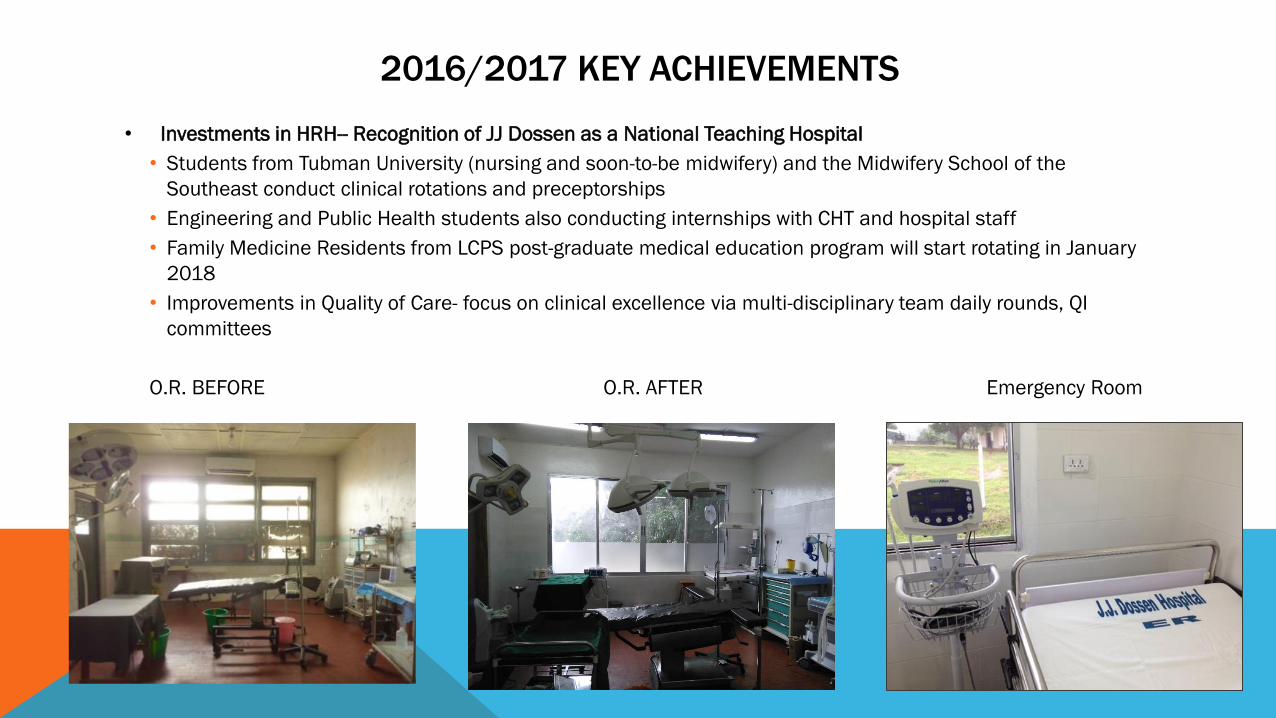
• Investments in HRH-- Recognition of JJ Dossen as a National Teaching Hospital
• Students from Tubman University (nursing and soon-to-be midwifery) and the Midwifery School of the
Southeast conduct clinical rotations and preceptorships
• Engineering and Public Health students also conducting internships with CHT and hospital staff
• Family Medicine Residents from LCPS post-graduate medical education program will start rotating in January
2018
• Improvements in Quality of Care- focus on clinical excellence via multi-disciplinary team daily rounds, QI
committees
O.R. BEFORE O.R. AFTER Emergency Room

COUNTY PERFORMANCE 2016/2017
Maternal and Child Health
• Increase in % of Skilled Deliveries from 41% to 52% and drop in number of maternal deaths by 50%
• Increase in the immunization coverage from 47% fully immunized previous year to 56.7%
• Decrease in the dropout rates from 32% to 27%
• Human Resource for Health: 7 midwives hired for selected facilities
• Improved Timeliness of LMIS and HMIS Reports submission of 100%
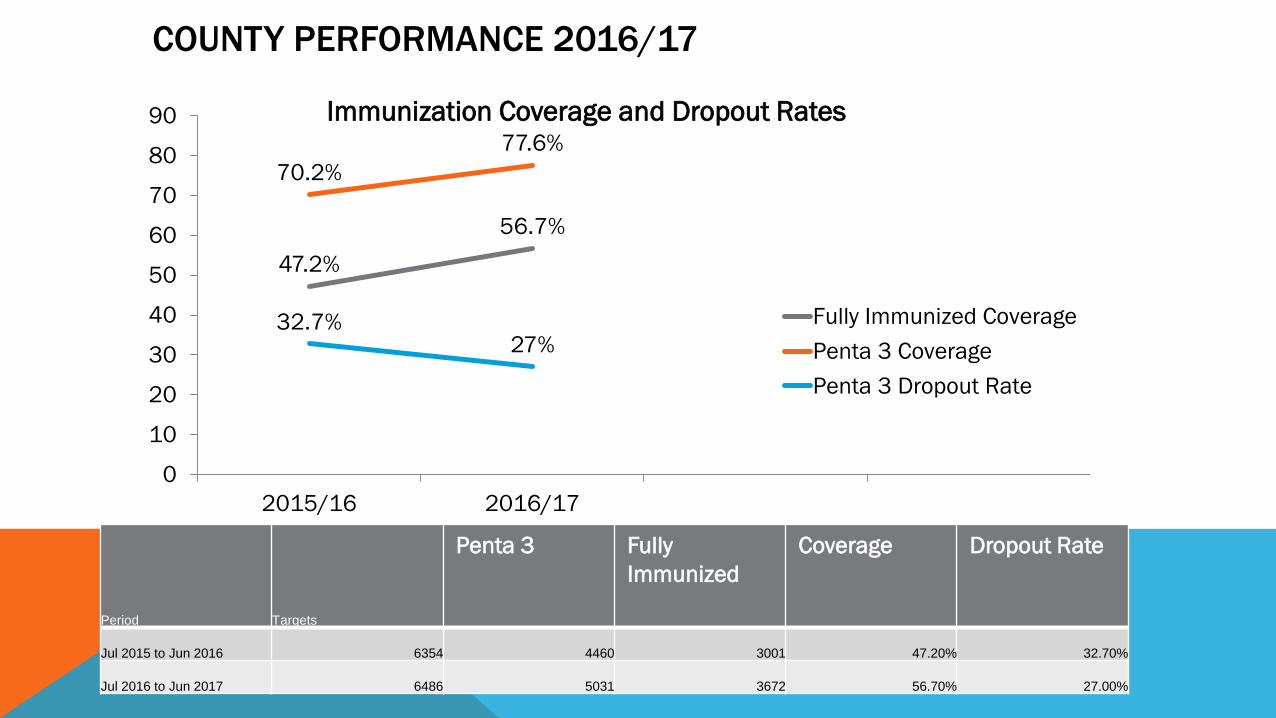
47.2%
56.7%
70.2%
77.6%
32.7% 27%
0
10
20
30
40
50
60
70
80
90
2015/16 2016/17
Immunization Coverage and Dropout Rates
Fully Immunized Coverage
Penta 3 Coverage
Penta 3 Dropout Rate
Period Targets
Penta 3 Fully
Immunized
Coverage Dropout Rate
Jul 2015 to Jun 2016 6354 4460 3001 47.20% 32.70%
Jul 2016 to Jun 2017 6486 5031 3672 56.70% 27.00%
COUNTY PERFORMANCE 2016/17
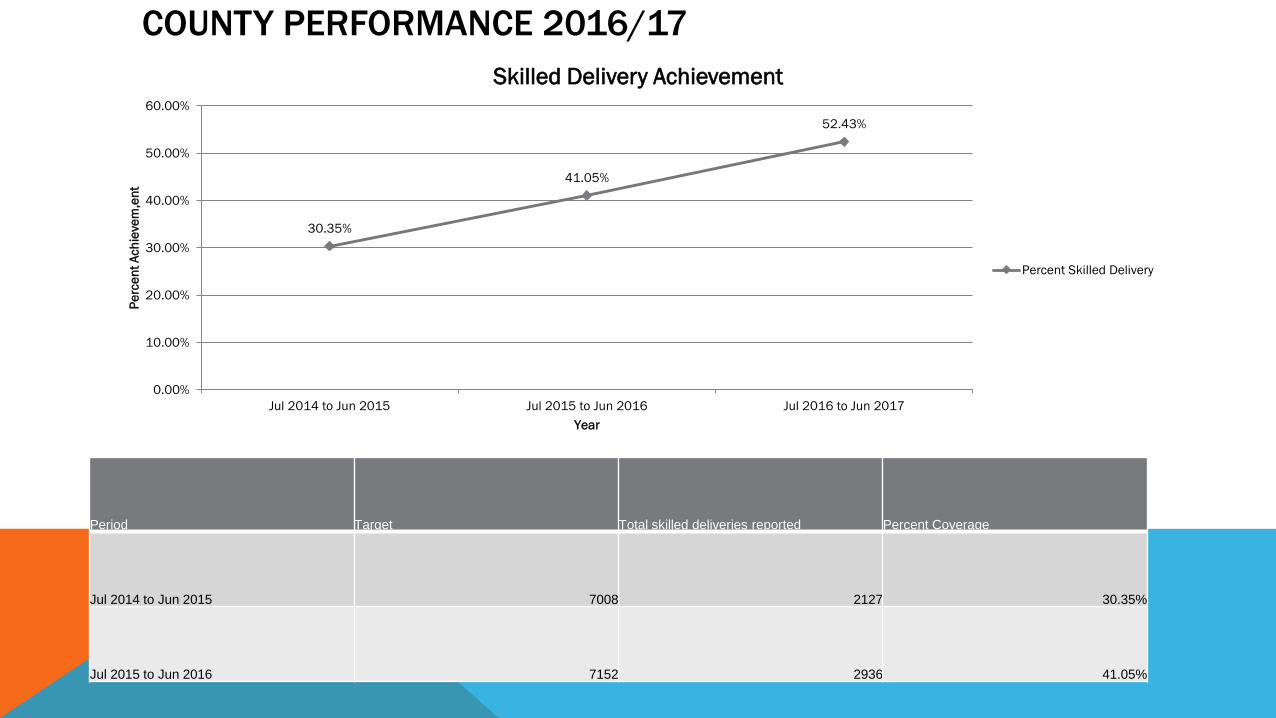
Period Target Total skilled deliveries reported Percent Coverage
Jul 2014 to Jun 2015 7008 2127 30.35%
Jul 2015 to Jun 2016 7152 2936 41.05%
30.35%
41.05%
52.43%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Jul 2014 to Jun 2015 Jul 2015 to Jun 2016 Jul 2016 to Jun 2017
Pe
rce
nt
Ach
ieve
m,e
nt
Year
Skilled Delivery Achievement
Percent Skilled Delivery
COUNTY PERFORMANCE 2016/17

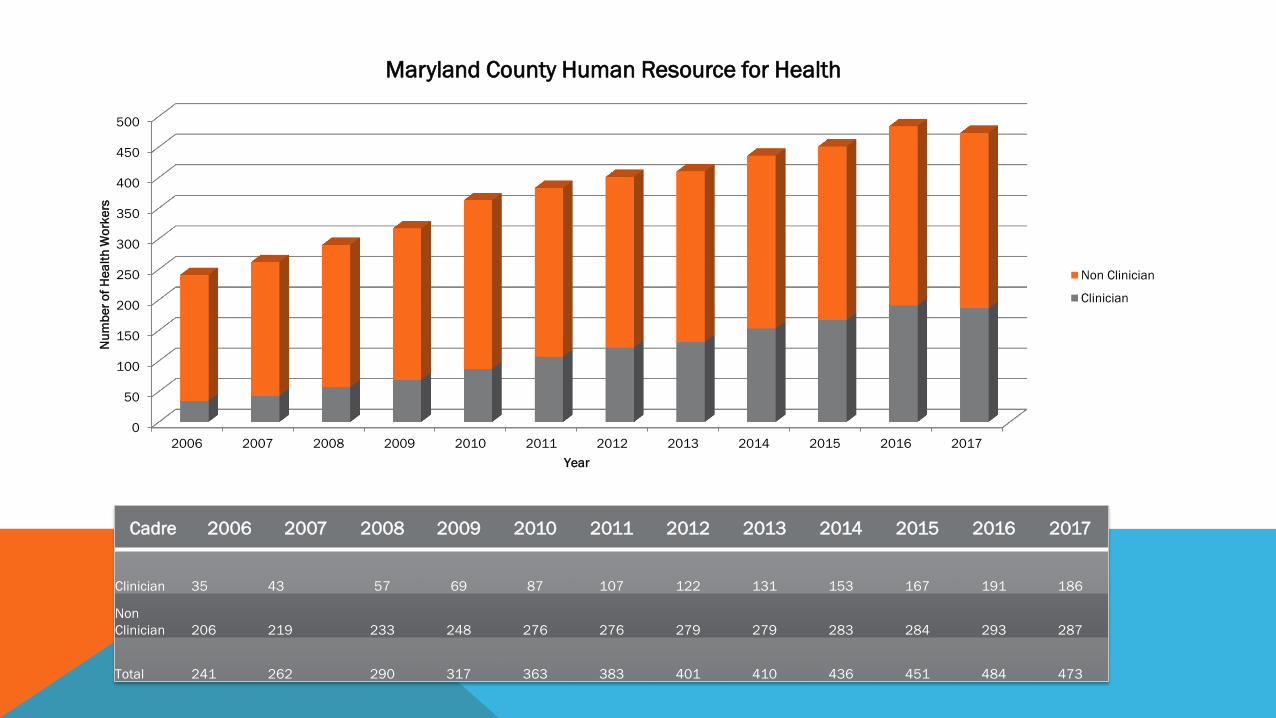
COUNTY PERFORMANCE 2006-2017
The Health Management Information System (HMIS) is one of
the vital components of the health system, in order to have
good Health Care Delivery, data must be collected and used
effectively in the various facilities
Data compiled in this report was received from the 25
functional health facilities within the county.
This information covers the period under review
0
50
100
150
200
250
300
350
400
450
500
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Nu
mb
er
of
He
alt
h W
ork
ers
Year
Maryland County Human Resource for Health
Non Clinician
Clinician
Cadre 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Clinician 35 43 57 69 87 107 122 131 153 167 191 186
Non
Clinician 206 219 233 248 276 276 279 279 283 284 293 287
Total 241 262 290 317 363 383 401 410 436 451 484 473
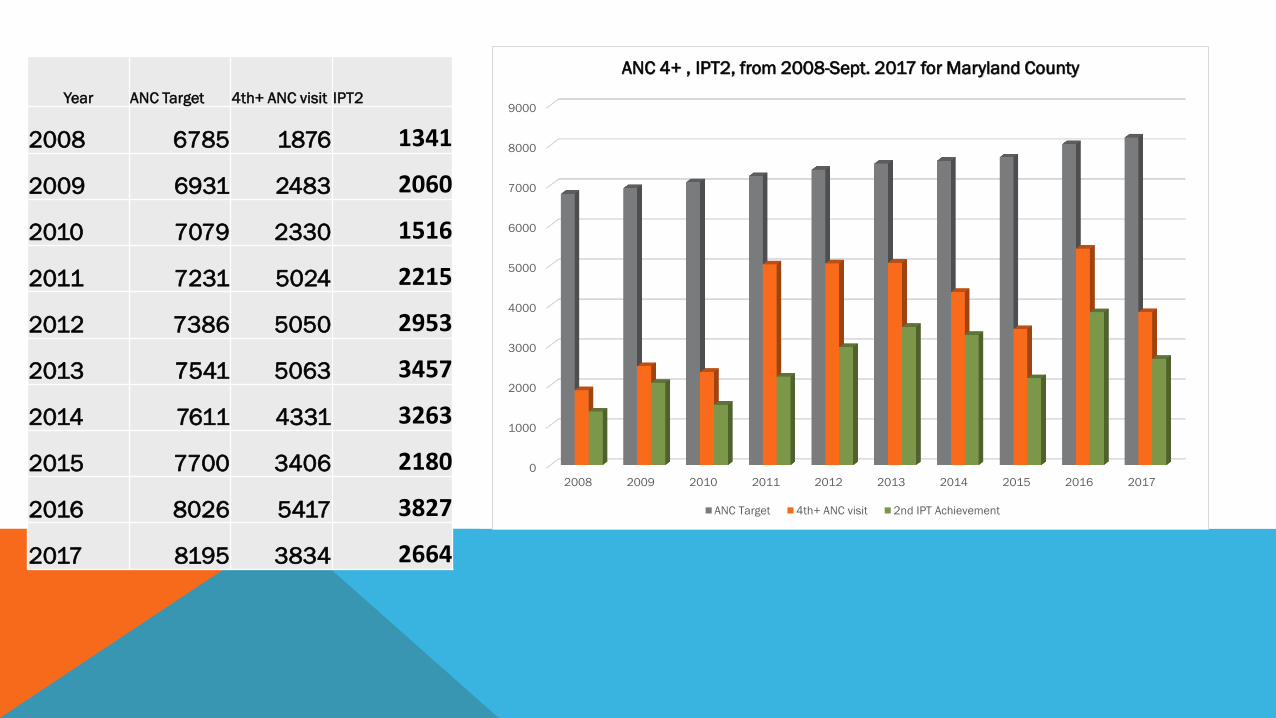
Year ANC Target 4th+ ANC visit IPT2
2008 6785 1876 1341
2009 6931 2483 2060
2010 7079 2330 1516
2011 7231 5024 2215
2012 7386 5050 2953
2013 7541 5063 3457
2014 7611 4331 3263
2015 7700 3406 2180
2016 8026 5417 3827
2017 8195 3834 2664
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
ANC 4+ , IPT2, from 2008-Sept. 2017 for Maryland County
ANC Target 4th+ ANC visit 2nd IPT Achievement

0
1000
2000
3000
4000
5000
6000
7000
8000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
13% 17% 20% 34% 32% 34% 34% 27% 48% 40%
Inst. Delivery Achievement from 2008-Sept. 2017
for Maryland CountyHealth Team
Skilled Del. Target Skilled Del. Achieve
Year Skilled Del.
Target Skilled Del.
Achieve Skilled Del.
Percentage %
2008 6106 822 13%
2009 6237 1034 17%
2010 6371 1260 20%
2011 6508 2236 34%
2012 6647 2095 32%
2013 6787 2293 34%
2014 6850 2295 34%
2015 6930 1892 27%
2016 7224 3441 48%
2017 7375 2940 40%
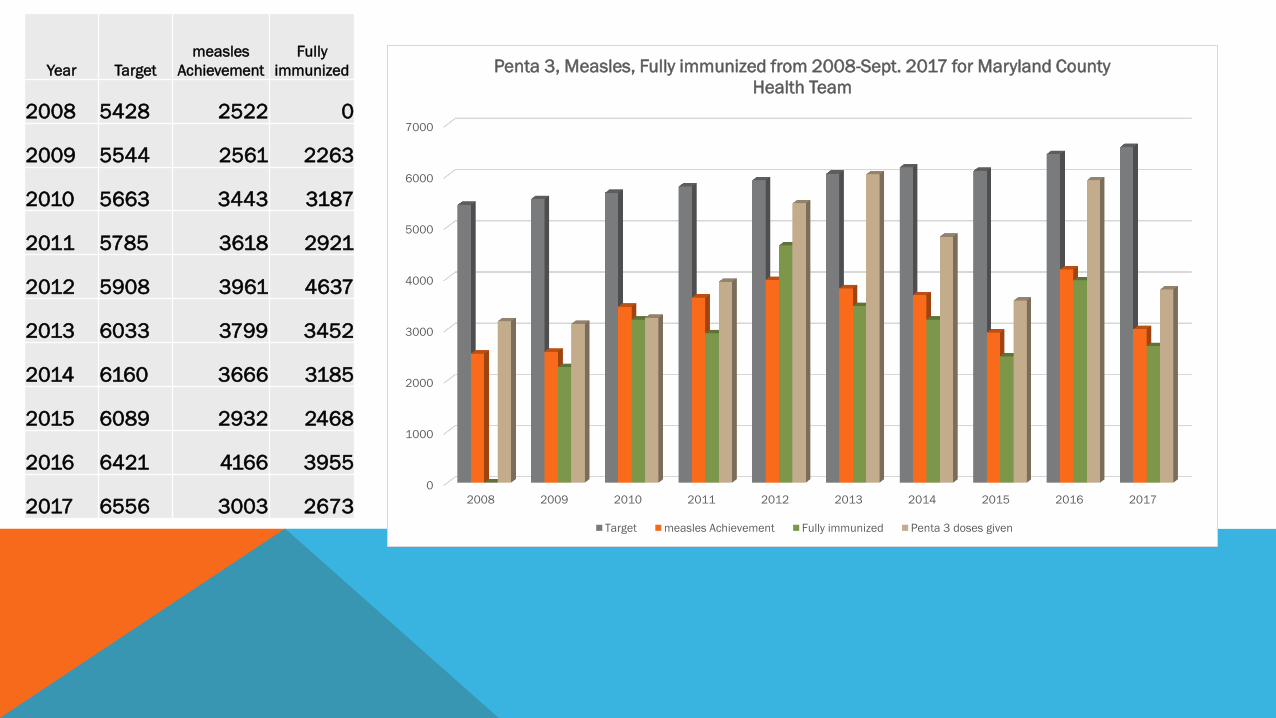
Year Target measles
Achievement Fully
immunized
2008 5428 2522 0
2009 5544 2561 2263
2010 5663 3443 3187
2011 5785 3618 2921
2012 5908 3961 4637
2013 6033 3799 3452
2014 6160 3666 3185
2015 6089 2932 2468
2016 6421 4166 3955
2017 6556 3003 2673 0
1000
2000
3000
4000
5000
6000
7000
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Penta 3, Measles, Fully immunized from 2008-Sept. 2017 for Maryland County
Health Team
Target measles Achievement Fully immunized Penta 3 doses given

KEY DRIVERS OF CHANGE
• Recruitment and assignment of professional staff to all health facilities across the county including the
introduction of the CHSS with a mandate to perform at both health facility and community and CHA/CHW at
community
• The establishment of a functional DHT with primary mandate to supervise health activities at the district
level
• Increase in the frequency of meetings with supervisors and program- leads on issues relevant to their
programs
• Weekly surveillance report and monthly IDSR bulletin of diseases collected across the county through
surveillance officers
• Regular Health Partners coordination meetings, community engagement meetings and quarterly County
Health Board meetings
• Concerted investments in all levels of the Maryland health system (community, primary care, secondary
care) all at the same time allowing for fully functioning referral pathway leading to better patient outcomes
and trust in health system
CHALLENGES
Operational
• Delay in receiving operational support from Government
Programmatic
• Failure of some partners to be transparent on various aspects of program activities
• Failure of Program Unit to furnish CHT with documents signed with partners in a timely manner so as to guide
program implementation

CHALLENGES
Systemic
Supply:
• Difficult terrain in rainy season making receipt and distribution of materials challenging
• Failure of SCMU and NDS to fully utilize consumption data in supplying Maryland leading to inadequate
supplies of some antimalarial and other ICCM commodities
• Stock-out of Reproductive Health Products (Depo provera injectables, Jadell (Implant) and Microgynon pills)
Human Resources:
• Difficulty in recruiting or replacing staff due to freeze placed by MOH personnel, though Civil Service says otherwise.
PRIORITY ACTIONS/RECOMMENDATIONS
Short term actions (within 6 months) • Program strengthening: Mental Health, Emergency Services, Supply Chain and Surveillance System
• Maternal Health: Increase delivery by SBA, Increase IPT2 and FP uptake and establish youth friendly services in 7 health
facilities
and 4communities.
• Strengthen our community health program
• Quality Improvement: Clinical mentoring and supportive supervision
• Health information:Improve in information utilization at all levels of the CHT
Medium term actions ( 1- 2 years) • Increase facility-based deliveries with a skilled birth attendance from 57% to 68%
• Increase children under 1 year who received PENTA 3 from 63% to 76 %
• Reduce the Penta 3 Dropout rates from 27% to 18%
• Increase the facilities with at least 1 midwife from 65% to 80%
• Maintain LMIS and HMIS reporting rate 100%
• Expand TB services, and strengthen Mental Health services
•
•
PRIORITY ACTIONS/RECOMMENDATIONS
Long term actions ( 3- 5 years)
• Increase facility-based deliveries with a skilled birth attendant from 57% to 80%
• Increase children under 1 year who received PENTA3 from 63%to 95%
• Reduce the Penta 3 Dropout rates from 27% to 5%
• Increase the facilities with at least 1 midwife from 65% to 100%
• Maintain LMIS and HMIS reporting rate 100%
• Improve our health infrastructures and build new ones

PARTNERS 2016/2017



Thank you!!!!!!