maternal-child health policy
DESCRIPTION
MATERNAL-CHILD HEALTH POLICY. DR. RENE CASTRO S. Regional Forum on Social Protection in Health for Women, Newborn and Child Populations in LAC – Lessons learned to prompt the way forward. Tegucigalpa, 8 -10 November 2006. - PowerPoint PPT PresentationTRANSCRIPT
MATERNAL-CHILD HEALTH POLICY
Regional Forum on Social Protection in Health for Women, Newborn and Child Populations in LAC –
Lessons learned to prompt the way forward.Tegucigalpa, 8 -10 November 2006
DR. RENE CASTRO S.
“Maternal and child mortality is
one of the demographic facts that
can be influenced in a more or less
serious way since it depends a great
deal on the care that the mother
and child receive before, during and
after birth.”
Dr. Salvador Allende, Minister of Health
(1940)

LA REALIDAD
MEDICO – SOCIAL
CHILENA
“Chilean Medical – Social Reality”

Maternal, perinatal and child health indicators reflect a country’s economic, cultural, social and health development.
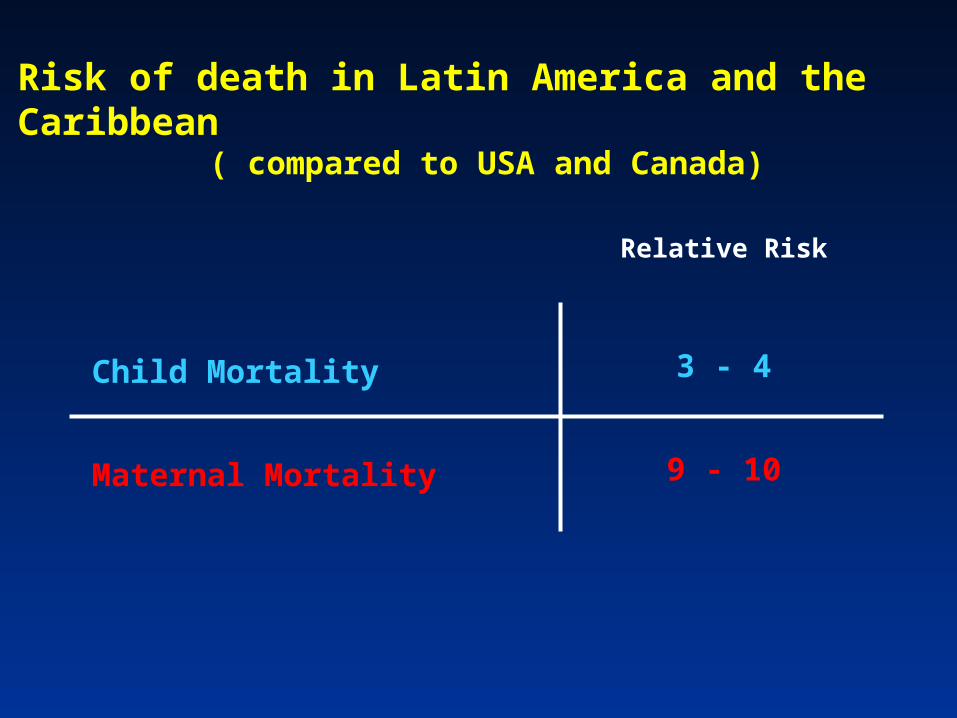
Risk of death in Latin America and the Caribbean
( compared to USA and Canada)
Child Mortality
Maternal Mortality
Relative Risk
3 - 4
9 - 10
Until 1920, the health situation in Chile
qualified as a “savage state”: the
highest child mortality in the world.
1952: Life expectancy at birth - 54.9
years – among the lowest at the global
level, reflecting the poor living conditions
in the country.
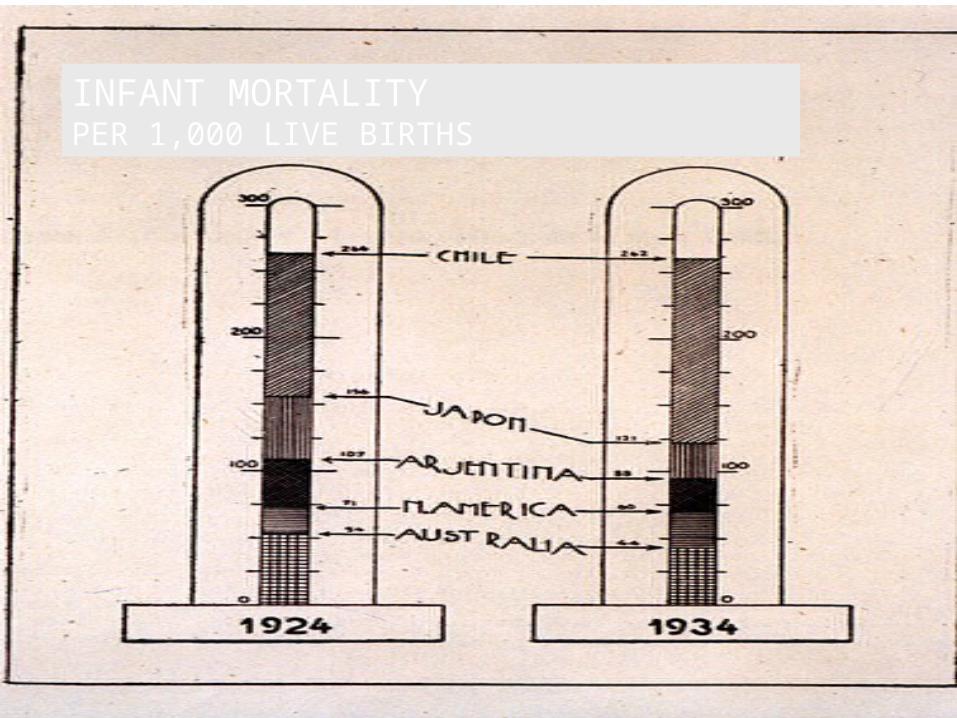
INFANT MORTALITYPER 1,000 LIVE BIRTHS
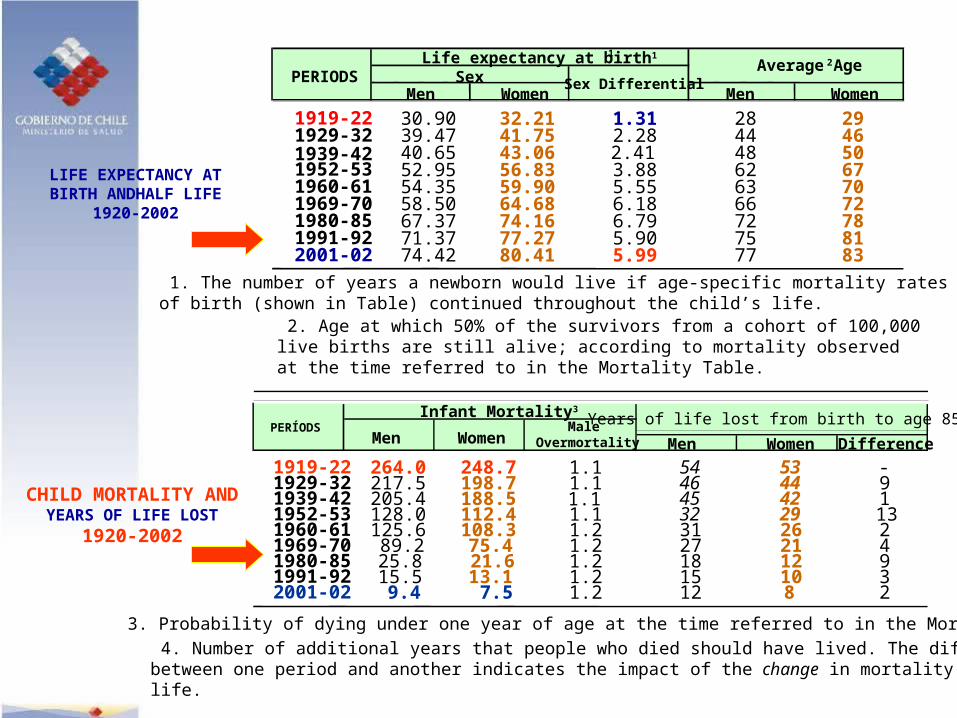
CHILD MORTALITY AND YEARS OF LIFE LOST
1920-2002
LIFE EXPECTANCY AT BIRTH ANDHALF LIFE
1920-2002
Men Women Difference
1919-22 264.0 248.7 1.1 54 53 -1929-32 217.5 198.7 1.1 46 44 91939-42 205.4 188.5 45 42 11952-53 128.0 112.4 1.1 32 29 131960-61 125.6 108.3 1.2 31 26 21969-70 89.2 75.4 1.2 27 21 41980-85 25.8 21.6 1.2 18 12 91991-92 15.5 13.1 1.2 15 10 32001-02 9.4 7.5 1.2 12 8 2
3. Probability of dying under one year of age at the time referred to in the Mortality Table.
Years of life lost from birth to age 854Male
Overmortality
Infant Mortality3
Men WomenPERÍODS
Men Women Men Women
1919-22 30.90 32.21 1.31 28 291929-32 39.47 41.75 2.28 44 461939-42 40.65 43.06 2.41 48 501952-53 52.95 56.83 3.88 62 671960-61 54.35 59.90 5.55 63 701969-70 58.50 64.68 6.18 66 721980-85 67.37 74.16 6.79 72 781991-92 71.37 77.27 5.90 75 812001-02 74.42 80.41 5.99 77 83
1. The number of years a newborn would live if age-specific mortality rates at timeof birth (shown in Table) continued throughout the child’s life.
SexAverage Age2
PERIODSLife expectancy at birth11
Sex Differential
2. Age at which 50% of the survivors from a cohort of 100,000 live births are still alive; according to mortality observed at the time referred to in the Mortality Table.
4. Number of additional years that people who died should have lived. The differencebetween one period and another indicates the impact of the change in mortality on human life.
1.1
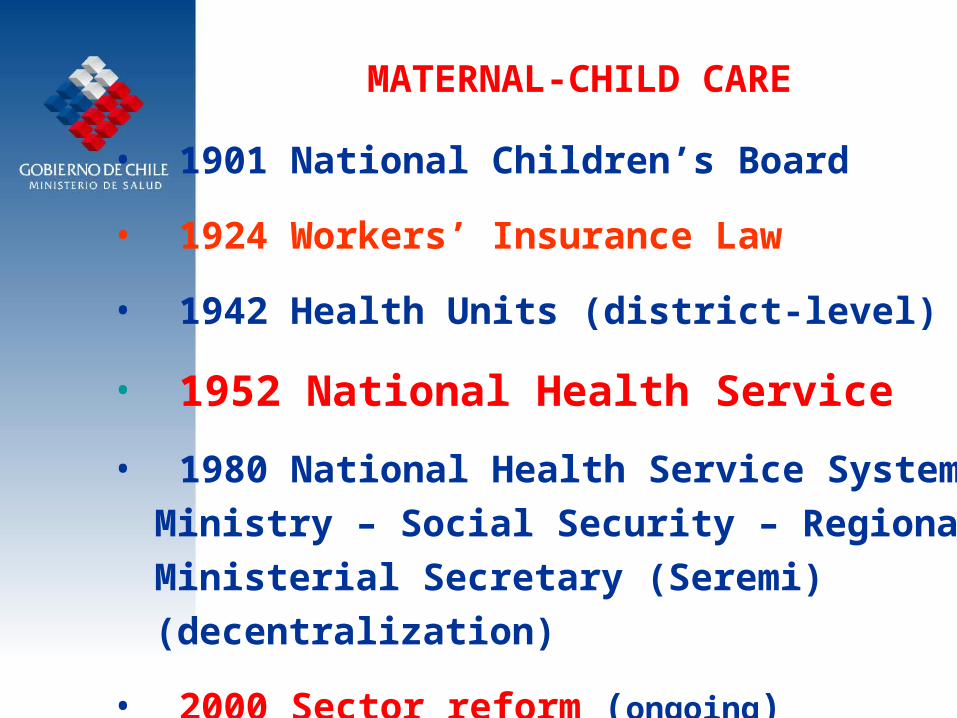
MATERNAL-CHILD CARE
• 1901 National Children’s Board
• 1924 Workers’ Insurance Law
• 1942 Health Units (district-level)
• 1952 National Health Service
• 1980 National Health Service System:Ministry – Social Security – RegionalMinisterial Secretary (Seremi)(decentralization)
• 2000 Sector reform (ongoing)
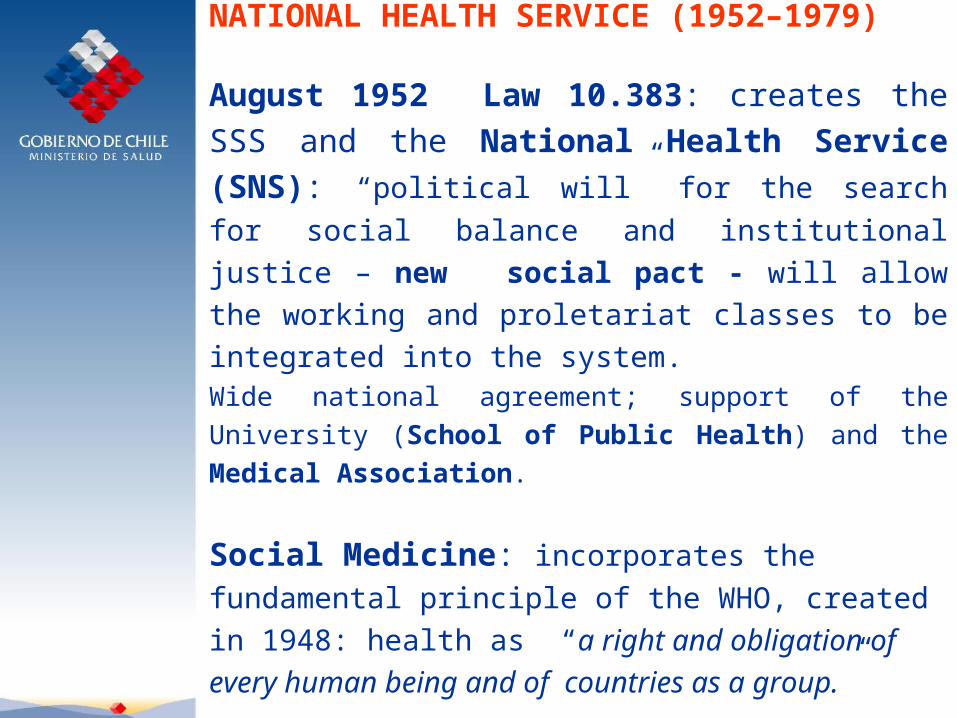
August 1952 Law 10.383: creates the SSS and the National Health Service (SNS): “political will” for the search for social balance and institutional justice – new social pact - will
allow the working and proletariat classes to be integrated
into the system.Wide national agreement; support of the University (School of Public Health) and the Medical Association.
Social Medicine: incorporates the fundamental
principle of the WHO, created in 1948: health as “a right and obligation of every human being and of countries as a group.”
NATIONAL HEALTH SERVICE (1952–1979)
NATIONAL HEALTH SERVICE (1952–1979)
Chile was the second country at the global level (4 years after England); it integrated 6 institutions that addressed different areas of social security and health management.
Objectives:
- reduction of maternal and child mortality,
- control of infectious diseases,
- eradication of malnutrition and,
- coordination with other social sectors that have links to health determinants.
0
5
10
15
20
25
30
35
1951
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
YEAR
RA
TE
PE
R 1
0000
LB
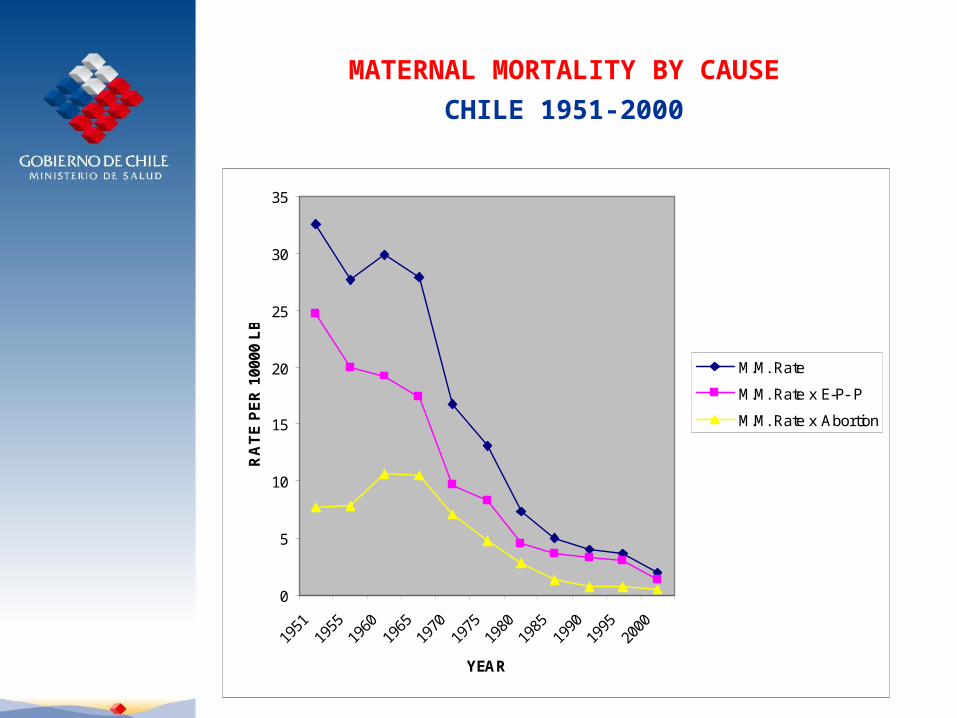
M.M. Rate
M.M. Rate x E-P- P
M.M. Rate x Abortion
MATERNAL MORTALITY BY CAUSE
CHILE 1951-2000
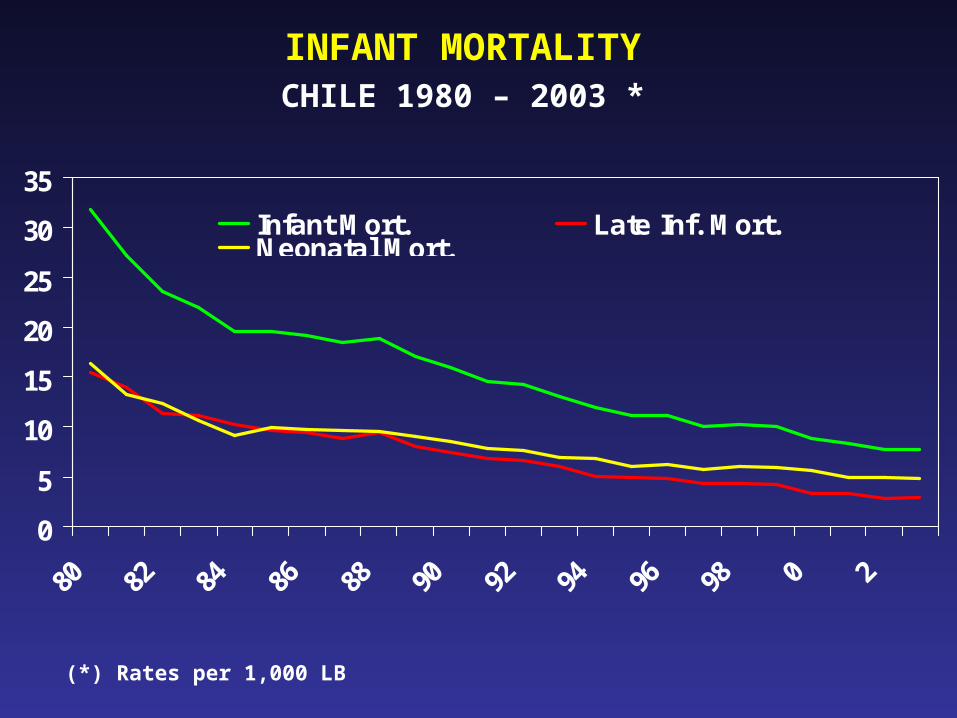
INFANT MORTALITYCHILE 1980 – 2003 *
0
5
10
15
20
25
30
35
Infant Mort. Late Inf. Mort.Neonatal Mort.
(*) Rates per 1,000 LB
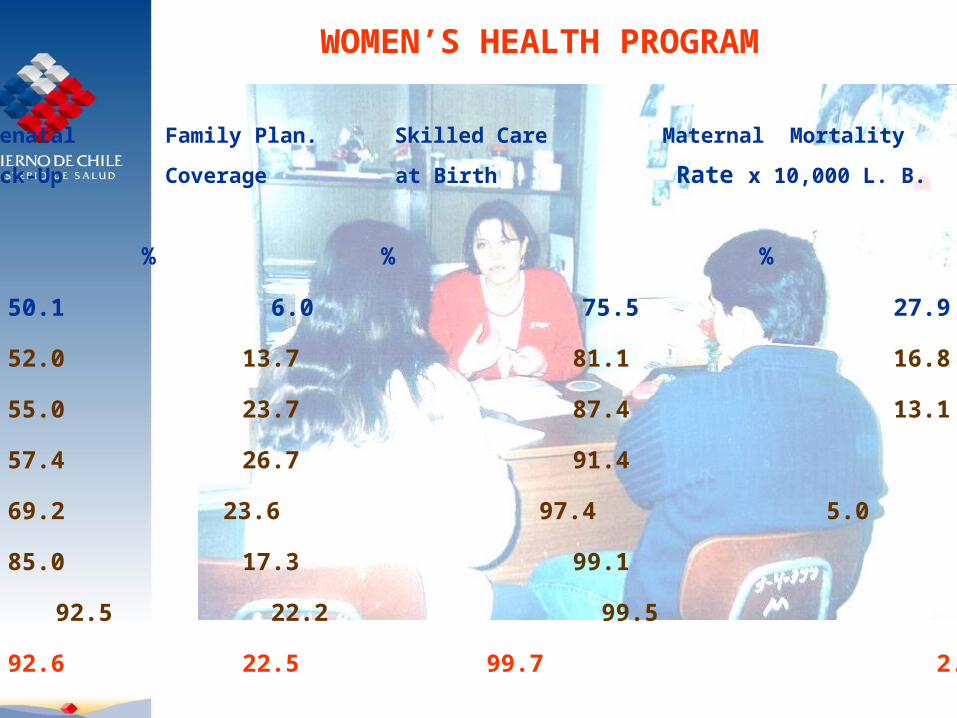
WOMEN’S HEALTH PROGRAM
Years Prenatal Family Plan. Skilled Care Maternal Mortality
Check-Up Coverage at Birth Rate x 10,000 L. B.
% % %
1965 50.1 6.0 75.5 27.9
1970 52.0 13.7 81.1 16.8
1975 55.0 23.7 87.4 13.1
1980 57.4 26.7 91.4 7.3
1985 69.2 23.6 97.4 5.0
1990 85.0 17.3 99.1 4.0
1995 92.5 22.2 99.5 3.1
1998 92.6 22.5 99.7 2.0
S.N.S.S. CARE NETWORK
•PRIMARY CARE
General Doctor’s Offices• Urban 250• Rural 150• Rural Posts > 1,100
• HOSPITAL-BASED CARE : 162/177
FAMILY PLANNING IN CHILE
1967: POLICY BASED ON HEALTH OBJECTIVES
a. Reduce Maternal Mortality due to Induced Abortion(Avoid Unwanted Pregnancy) ;
b. Reduce Child Mortality associated with high fertility;
c. Promote Family Well-being (Responsible Parenting)
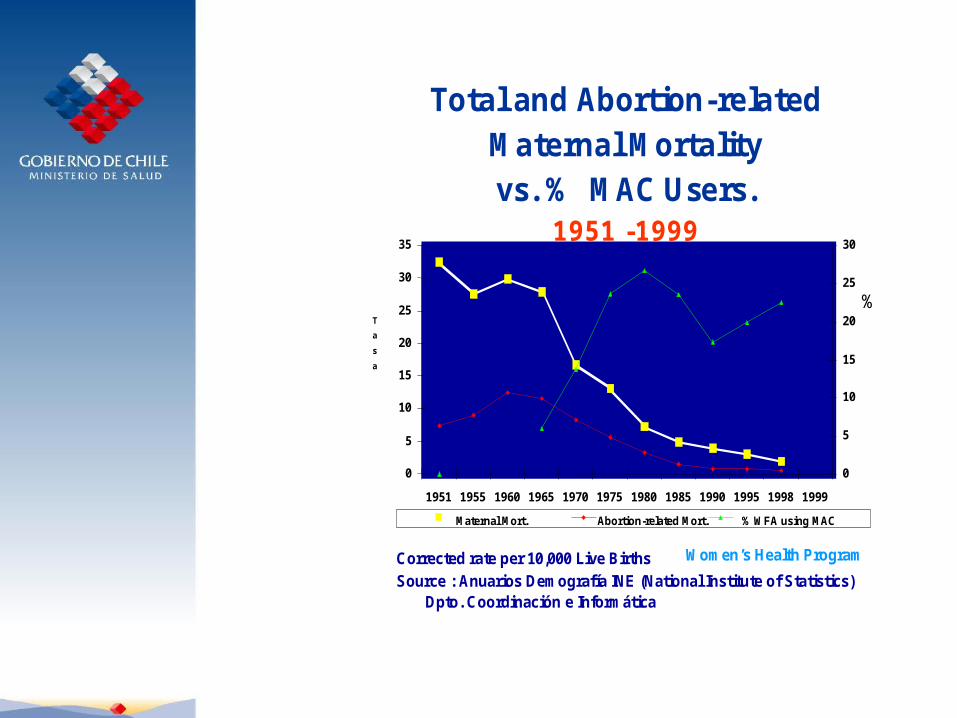
Total and Abortion-related Maternal Mortalityvs. % MAC Users.
1951 -1999
0
5
10
15
20
25
30
35
1951 1955 1960 1965 1970 1975 1980 1985 1990 1995 1998 1999
0
5
10
15
20
25
30
Maternal Mort. Abortion-related Mort.
Corrected rate per 10,000 Live BirthsSource : Anuarios Demografía INE (National Institute of Statistics)
Dpto. Coordinación e Informática
Women’s Health Program
T
a
s
a
%
% WFA using MAC
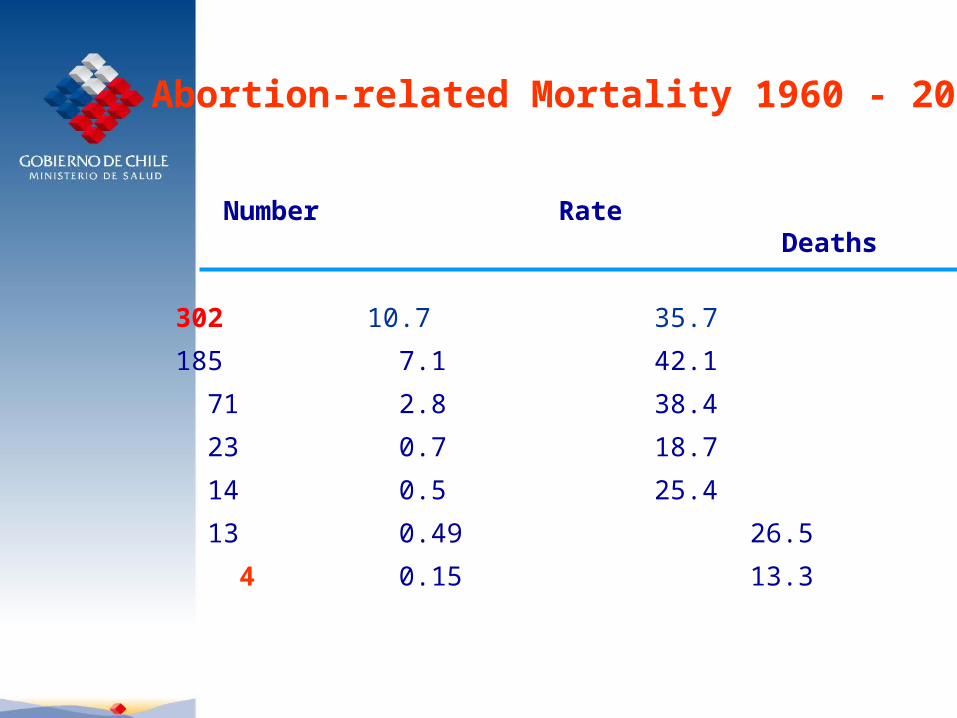
Abortion-related Mortality 1960 - 2000
Year Number Rate % Maternal Deaths
1960 302 10.7 35.7
1970 185 7.1 42.1
1980 71 2.8 38.4
1990 23 0.7 18.7
1998 14 0.5 25.4
2000 13 0.49 26.5
2001 4 0.15 13.3
Foundation for a Family Planning Policy
“The Government of Chile recognizes the
benefit
that the population achieves through Family
Planning activities, which allow individuals to
have the number of children with the desired
spacing and timing. For this reason, it
maintains its support for Family Planning
activities in order to promote the
achievement of adequate comprehensive
reproductive health.”
October 1990
PROFESSIONAL DELIVERY CARE
YEAR %
1965 74.3
1975 87.4
1985 97.4
1998 99.6
“ From empiricism to professionalismin delivery care”
Prof. F. Mardones-Restat
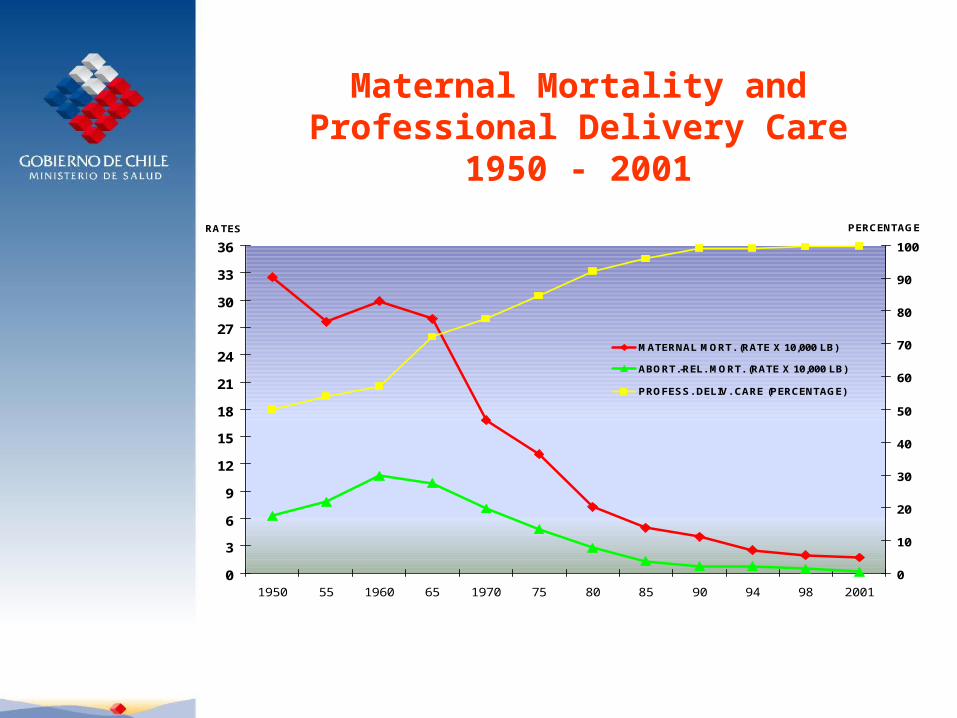
0
3
6
9
12
15
18
21
24
27
30
33
36
1950 55 1960 65 1970 75 80 85 90 94 98 2001
RATES
0
10
20
30
40
50
60
70
80
90
100
PERCENTAGE
MATERNAL MORT. (RATE X 10,000 LB)
ABORT.-REL. MORT. (RATE X 10,000 LB)
PROFESS. DELIV. CARE (PERCENTAGE)
Maternal Mortality andProfessional Delivery Care
1950 - 2001

MATERNAL-CHILD HEALTH 1960 – 2000
Rates per 1,000 LB1960 2000
Birth Rate 35.5 17.2
Total Maternal Mort. 2.99 0.2
M.M. due to Abortion 1.07 0.05
Infant Mortality 125.1 8.9
Neonatal Mort. < 28 d. 36.2 5.6
REDUCTION OF MATERNAL MORTALITY IN CHILE :
LESSONS LEARNED
1950-2000
Ministry of Health, CHILEUniversidad de la FronteraPan American Health OrganizationPAHO/USAID
Steps for Reducing Maternal Mortality• Consider M.M. to be a human rights and social justice problem.
• Recognize that every pregnancy has some level of risk.
• Assure that skilled personnel attend births.
• Promote maternal health as a vital economic and
social investment : Postpone motherhood. Prevent unwanted pregnancy. Prevent unsafe abortion.
• Facilitate access to maternal health services.
• Improve the quality of maternal health services.
• Supervise and evaluate changes.
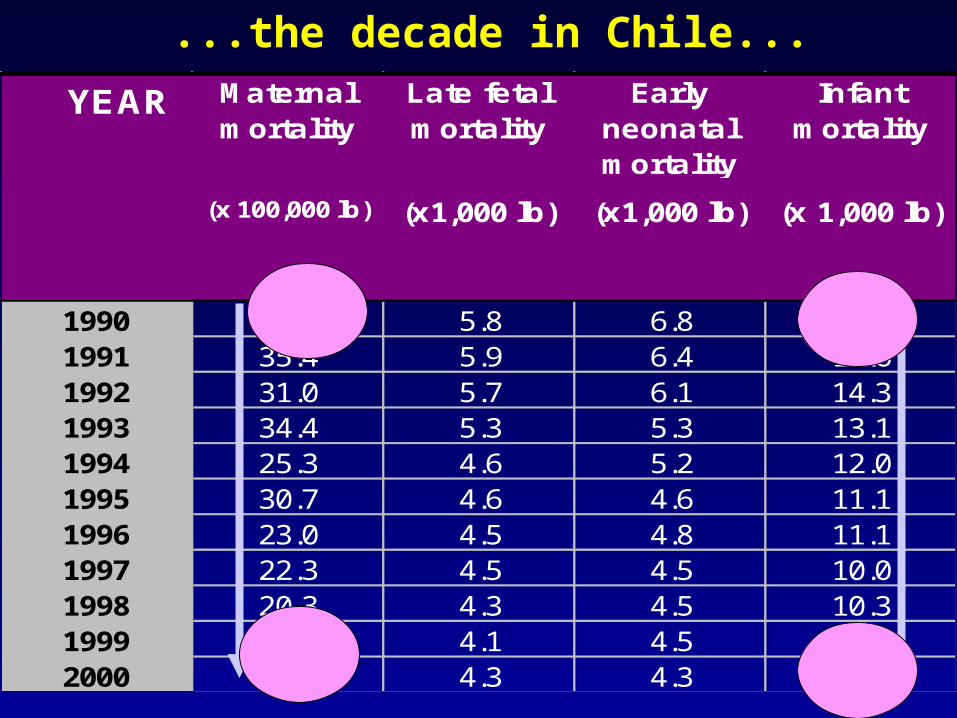
Maternal mortality
Late fetal mortality
Early neonatal mortality
Infant mortality
(x 100,000 lb) (x1,000 lb) (x1,000 lb) (x 1,000 lb)
1990 40.0 5.8 6.8 16.01991 35.4 5.9 6.4 14.61992 31.0 5.7 6.1 14.31993 34.4 5.3 5.3 13.11994 25.3 4.6 5.2 12.01995 30.7 4.6 4.6 11.11996 23.0 4.5 4.8 11.11997 22.3 4.5 4.5 10.01998 20.3 4.3 4.5 10.31999 22.7 4.1 4.5 10.12000 18.7 4.3 4.3 8.9
YEAR
...the decade in Chile...
PEDIATRICS, 10 April 2006

MATERNAL – CHILD HEALTH SITUATION
Stable health policies during the last 50
years
Institutionalized National Health System
Human resources that are committed to
their work
Culture of health among the population

“Chile is better - Health Reform”
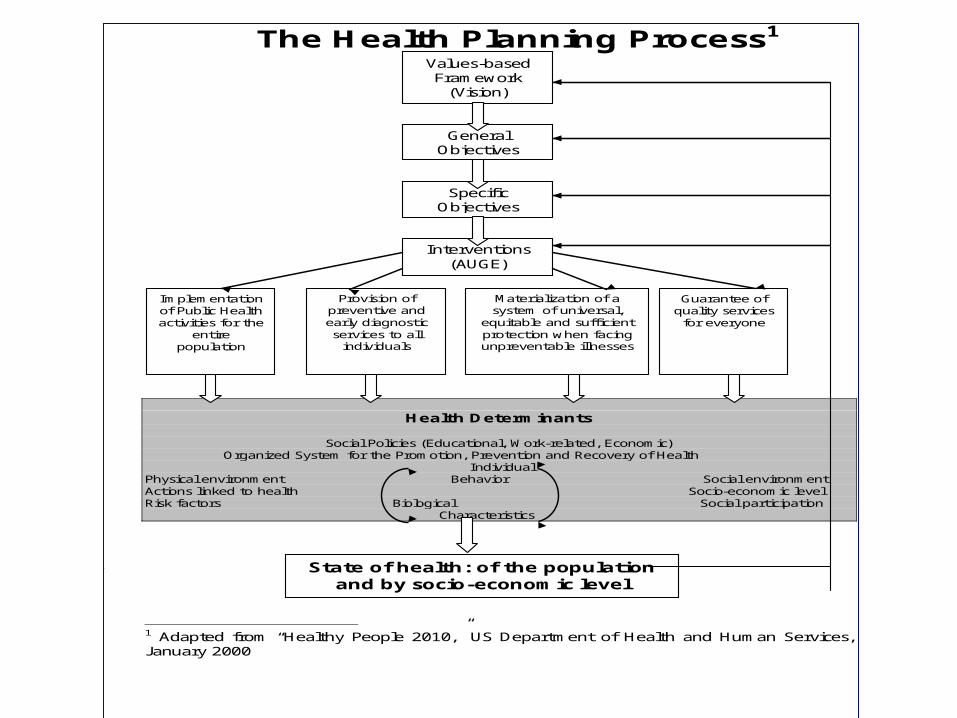
The Health Planning Process1
Health Determinants
Social Policies (Educational, Work-related, Economic) Organized System for the Promotion, Prevention and Recovery of Health
Individual Physical environment Behavior Social environment Actions linked to health Socio-economic level Risk factors Biological Social participation
Characteristics
1 Adapted from “Healthy People 2010,” US Department of Health and Human Services, January 2000
Values-based Framework
(Vision)
General Objectives
Specific Objectives
Interventions (AUGE)
Implementation of Public Health activities for the
entire population
Provision of preventive and early diagnostic services to all
individuals
Materialization of a system of universal,
equitable and sufficient protection when facing unpreventable illnesses
Guarantee of quality services for everyone
State of health: of the population and by socio-economic level
SEXUAL AND REPRODUCTIVE HEALTH
“DESIGN AND IMPLEMENTATION OF HEALTH PRIORITIESChilean Programmatic Reform”
REPRODUCTIVE HEALTH
PRECON-CEPTION
CARE
PRENATAL CARE
DELIVERY ANDPOSTPARTUM
CARE
HEALTHY MOTHERSAND NEWBORNS
NEONATALCARE
++ ++
==
++

•Improve the health objectives attained
–Child health, women’s health, infectious diseases
•Confront the challenges that result from aging and other changes in society
–Determinants of the health situation, primary causes of death and disability
•Reduce health inequalities
–Living conditions and determinants, health situation, access to health
•Provide services according to the population’s expectations
–Financial justice, care according to expectations, quality of care
Health Objectives: Cornerstone of the Reform
“Health Objectives for the Decade 2000-2010”
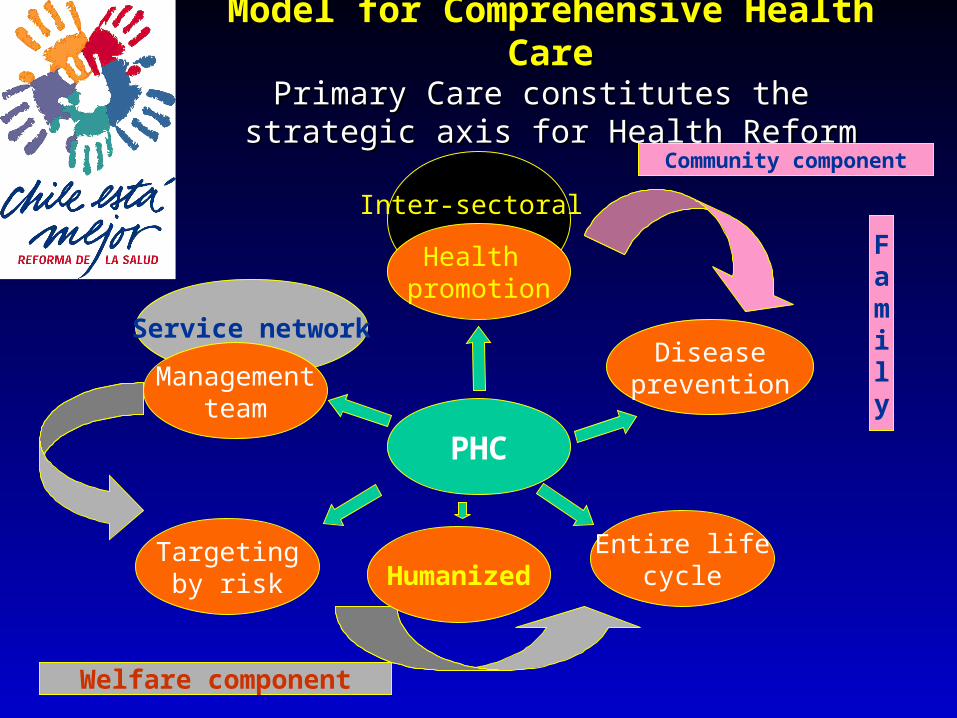
Model for Comprehensive Health Model for Comprehensive Health CareCare
Primary Care constitutes the Primary Care constitutes the strategic axis for Health Reformstrategic axis for Health Reform
Entire lifecycle
Inter-sectoral
Service networkDisease
prevention
Targetingby risk
PHC
Welfare component
Community component
Health promotion
Managementteam
Family
Humanized
Unwanted Pregnancies
Health Objectives and Goals for Unwanted Pregnancies
Impact Goals:
•Decrease the gap between desired and observed fertility: the gap between desired and observed fertility should be under 20%
•By age group, maternal educational level, socio-economic level, experience with use of contraceptive methods (methods used, duration of use)
•Reduce pregnancies in adolescents: see Chapter 2 on Risk Factors, Sexual Behavior
•Reduce abortion-related maternal mortality by 50% (over the level in 2000)
•Counseling on Sexual and Reproductive Health for the population at greatest risk of abortion (detected using predictive instrument)
•Coverage for Fertility Regulation: by five-year age groups
•Audit of complicated abortions by cause at the level of hospitals and/or primary care establishments
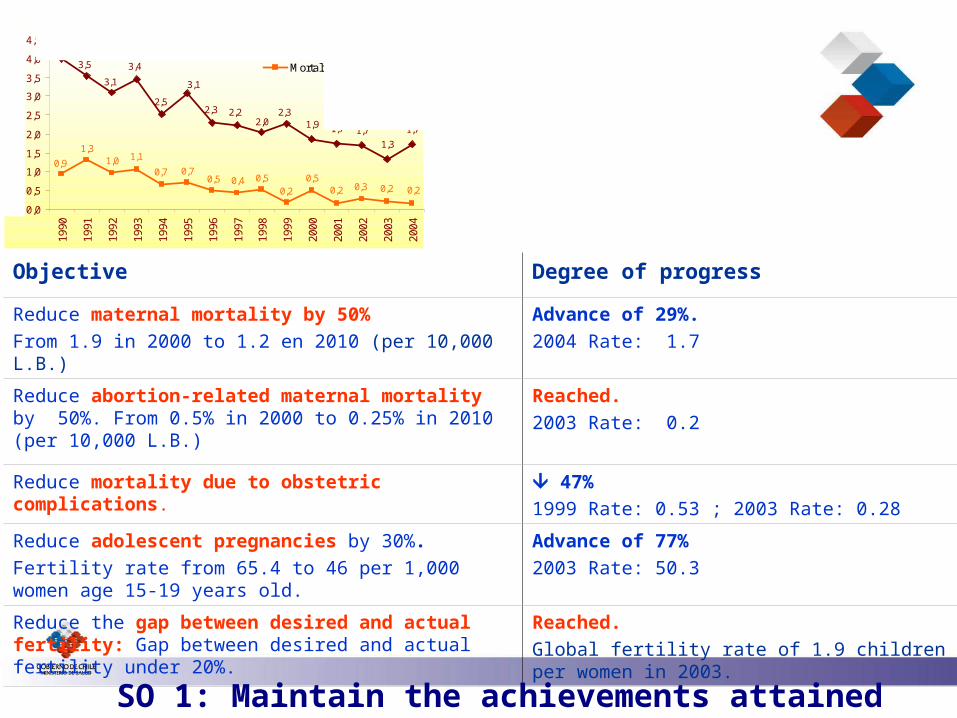
mortalidad materna y por aborto, Chile 1990-2004
1,9 1,7 1,7
1,3
1,7
4,0
3,5
2,32,0
2,22,3
3,1
2,5
3,4
3,1
0,20,20,30,20,5
0,20,50,40,5
0,70,7
1,11,01,3
0,9
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
4,0
4,5
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Tas
as p
or 1
0.00
0 N
V
Mortalidad Materna
Mortalidad por aborto
Objective Degree of progress
Reduce maternal mortality by 50%From 1.9 in 2000 to 1.2 en 2010 (per 10,000 L.B.)
Advance of 29%. 2004 Rate: 1.7
Reduce abortion-related maternal mortality by 50%. From 0.5% in 2000 to 0.25% in 2010 (per 10,000 L.B.)
Reached. 2003 Rate: 0.2
Reduce mortality due to obstetric complications.
47%1999 Rate: 0.53 ; 2003 Rate: 0.28
Reduce adolescent pregnancies by 30%. Fertility rate from 65.4 to 46 per 1,000 women age 15-19 years old.
Advance of 77%2003 Rate: 50.3
Reduce the gap between desired and actual fertility: Gap between desired and actual fertility under 20%.
Reached.Global fertility rate of 1.9 children per women in 2003.
SO 1: Maintain the achievements attained
Maternal and abortion-related mortality, Chile 1990-2004
Maternal Mortality
Abortion-related mortality
Rate
s x
10,0
00 L
B
SO 1: Maintain the achievements attained
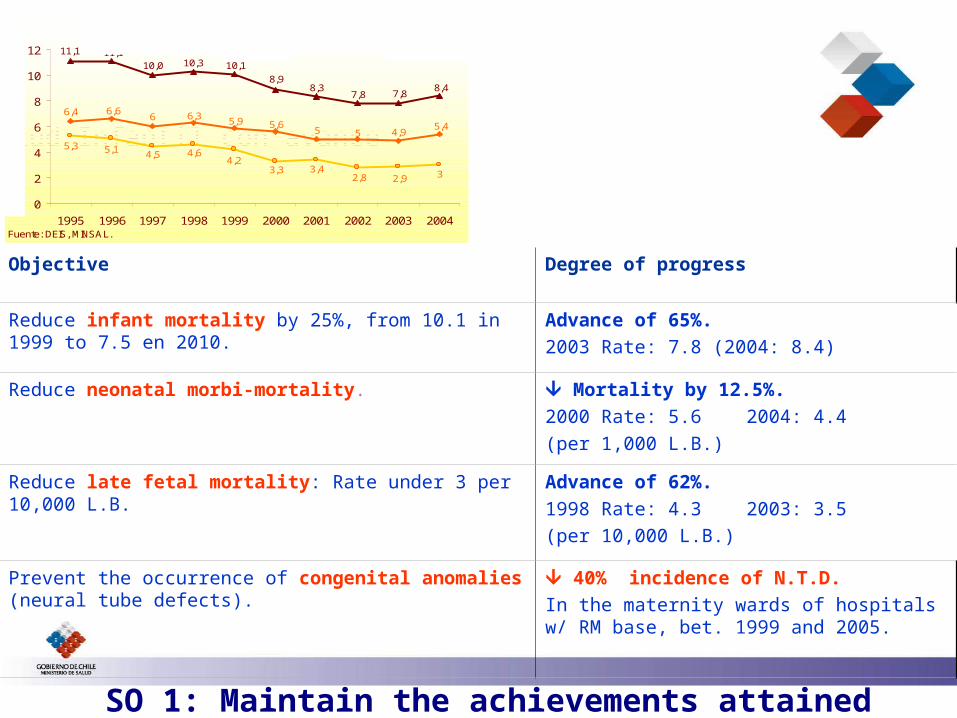
Salud Infantil con avance
Mortalidad Infantil y sus componentes, Chile 1995-2004
8,47,87,8
8,38,9
10,110,310,011,111,1
5,44,955
5,65,96,366,66,4
32,92,83,43,3
4,24,64,55,15,3
0
2
4
6
8
10
12
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Tasas p
or
1000 N
V
Infantil Neonatal Postneonatal
Fuente: DEIS, MINSAL.
Objective Degree of progress
Reduce infant mortality by 25%, from 10.1 in 1999 to 7.5 en 2010.
Advance of 65%.2003 Rate: 7.8 (2004: 8.4)
Reduce neonatal morbi-mortality. Mortality by 12.5%. 2000 Rate: 5.6 2004: 4.4(per 1,000 L.B.)
Reduce late fetal mortality: Rate under 3 per 10,000 L.B.
Advance of 62%. 1998 Rate: 4.3 2003: 3.5 (per 10,000 L.B.)
Prevent the occurrence of congenital anomalies (neural tube defects).
40% incidence of N.T.D. In the maternity wards of hospitals w/ RM base, bet. 1999 and 2005.
Infant mortality and its components, Chile 1995-2004
Infant Post neonatal
Rate
s x
10,0
00 L
B

Millennium Development GoalsMillennium Development Goals
Eradicate extreme poverty and hunger
Achieve universal primary education
Promote gender equality and empower women
Reduce child mortality
Improve maternal health
Combat HIV/AIDS, malaria and other diseases
Ensure environmental sustainability
GOAL 1
GOAL 2
GOAL 3
GOAL 4
GOAL 5
GOAL 6
GOAL 7
“This is how the AUGE works: explicit health guarantees”
12 September 2004 “The regime of General Health Guarantees is a health regulation instrument that is an integral part of the Health Services Regime.”

12 September 2004“The Explicit Guarantees relate to access, quality, financial protection and timeliness.”
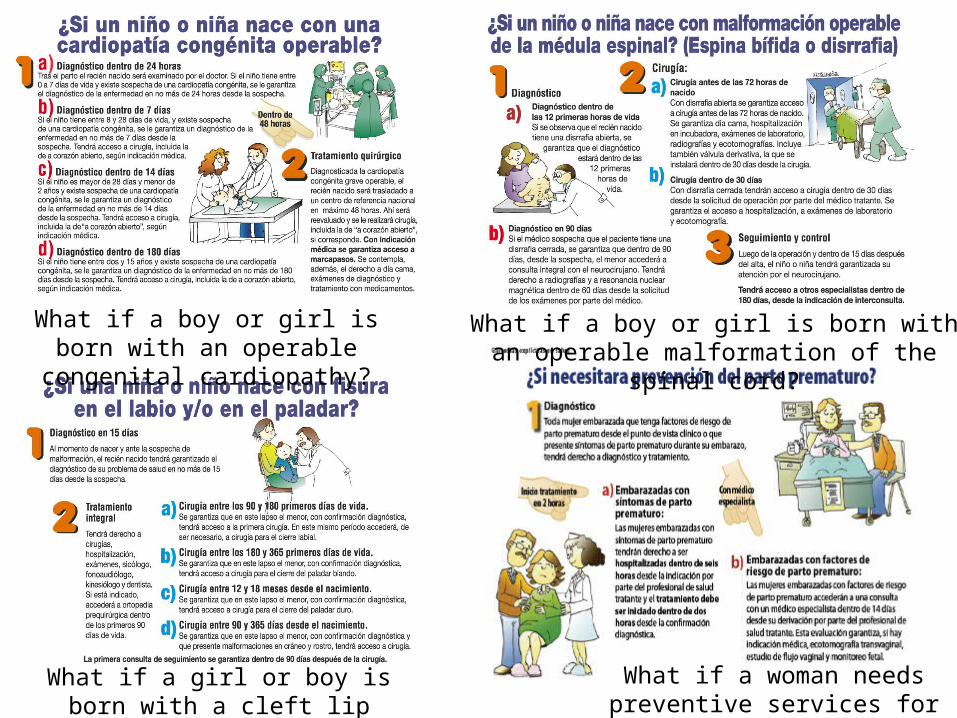
What if a boy or girl is born with an operable congenital cardiopathy?
What if a boy or girl is born with an operable malformation of the spinal cord?
What if a woman needs preventive services for a premature birth?
What if a girl or boy is born with a cleft lip and/or palate?

Government Program
“ A good social
protection system
accompanies people
throughout their life
cycle, protecting their
first steps, …”
“My goal, at the end of the Administration, is that we will have achieved the implementation of a child protection system aimed at leveling the development opportunities of Chilean children in the first eight years of life, independent of social origin, gender, geography or household structure.
A task of this magnitude far exceeds the reach of traditional social policy approaches and will require a set of programs and instruments...”
Constitution Ceremony of the Presidential Advisor for the Reform of Childhood Policies, 30 March 2006.
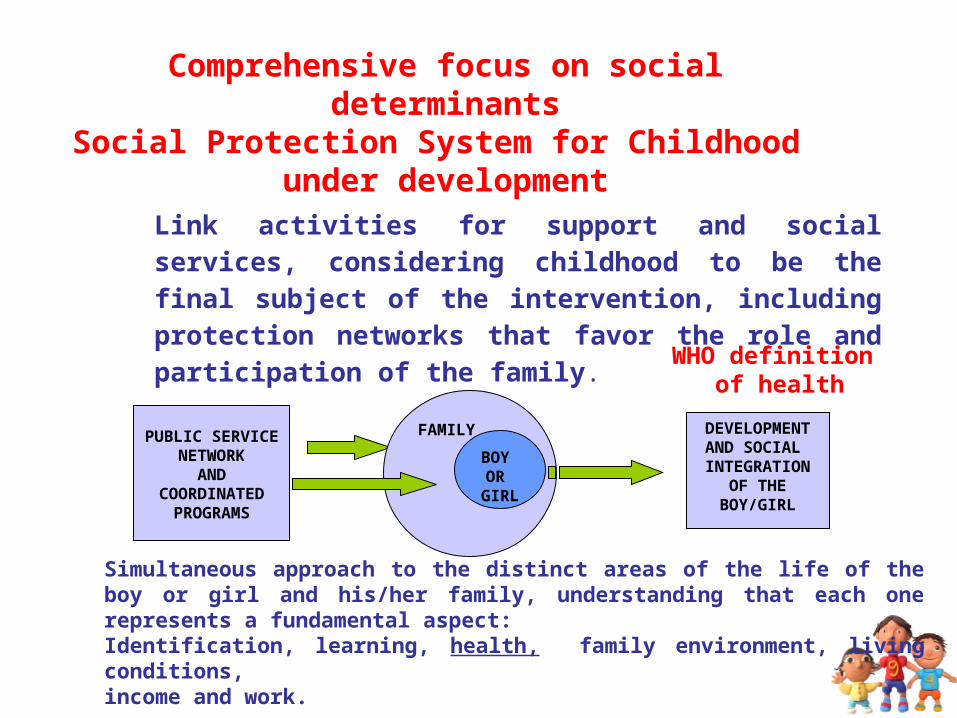
Comprehensive focus on social determinantsSocial Protection System for Childhood
under development
Link activities for support and social services, considering childhood to be the final subject of the intervention, including protection networks that favor the role and participation of the family.
PUBLIC SERVICENETWORK
ANDCOORDINATED
PROGRAMS
FAMILY DEVELOPMENTAND SOCIAL INTEGRATION
OF THEBOY/GIRL
BOY OR
GIRL
Simultaneous approach to the distinct areas of the life of the boy or girl and his/her family, understanding that each one represents a fundamental aspect:Identification, learning, health, family environment, living conditions,income and work.
WHO definition of health

The logic of the intervention
The following matrices have been developed for each stage of the boy’s or girl’s life cycle:
• Baby from gestation until 3 months.
• From 3 months to 3 years.
• From 4 to 5 years.
• From 6 to 10+ years (4th of basic).
The matrices have a logic of continuity: the boy/girl enters the System at the gestation stage and the System accompanies him/her from that moment throughout the different stages of the life cycle.

“The future of children is always todayProposals by the Presidential Advisor for the Reform of Childhood Policies”
13.10.06 “Chile grows with you”
System for the Protection of ChildhoodChile Grows With You
Pregnancy control will mark the entrance of women into the public health system.
Automatic one-time family subsidy for the entire gestational period (R.N. Subsidy).
Pregnancy and delivery manual, organized by weeks of gestation.
Program for the integrated development of doctor’s visits (complement to prenatal and healthy child controls). Humanized delivery care (AUGE 2007)