maternal health disparities: economic & psychosocial hardships during pregnancy may 18-19, 2005...
TRANSCRIPT

Maternal health disparities: Economic & psychosocial hardships
during pregnancy
May 18-19, 2005Jacob’s Institute For Women’s Health
Paula Braveman, MD, MPHProfessor of Family & Community Medicine
Director, Center on Social Disparities in Health

Hardships during pregnancy
Major economic and psychosocial hardships are not rare during pregnancy
Large disparities But hardships are prevalent among all groups except
the most affluent (22% with highest incomes) Of concern in itself, re maternal well-being If reflects chronic stress, also could adversely affect
maternal & infant health, thus health over life course Need to re-assess prenatal services And policies across the life course

Acknowledgements
Collaborators Soowon Kim & Kristen Marchi, Center on Social
Disparities in Health, UCSF Tonya Stancil, CDC Div. of Repro. Health (PRAMS) Marilyn Metzler, CDC Coordinating Center on
Health Promotion, Adult & Community Health Moreen Libet & Shabbir Ahmad, CA Dept Health
Services MCAH Branch Funding
Division of Reproductive Health, CDC Coordinating Center on Health Promotion

CA. Maternal and Infant Health Assessment, 2002-03
Statewide postpartum survey on maternal and infant health and health care, yearly since 1999
Collaborative effort of CA. Dept. Health Services MCH Branch & UCSF CSDH
Modeled on CDC’s PRAMS survey Mail/telephone in English and Spanish N = 7,206, with > 70% response Generally representative but under-
representation of most disadvantaged is likely

Most women (53%) had low incomes (were poor or near-poor)
Poor:at or under the
poverty line33%
High income:over 400% of poverty
22%
Moderate: 3-4 x poverty
7%
Low-moderate: 2-3 x poverty
10%
Near-poor:101-200% of poverty
20%

Very hard to get by on her income: disparities by income,2002 - 2003
0
4
8
12
16
20
24
28
% o
f w
om
en
Overall 0-100% 101-200% 201-300% 301-400% >400%% of Federal Poverty Level

Very hard to get by on her income: racial/ethnic disparities, 2002 - 2003
0
4
8
12
16
20
24
Afr Amer API - US API - notUS
EuroAmer
Latina US Latina notUS
AmerIndian
% o
f w
om
en
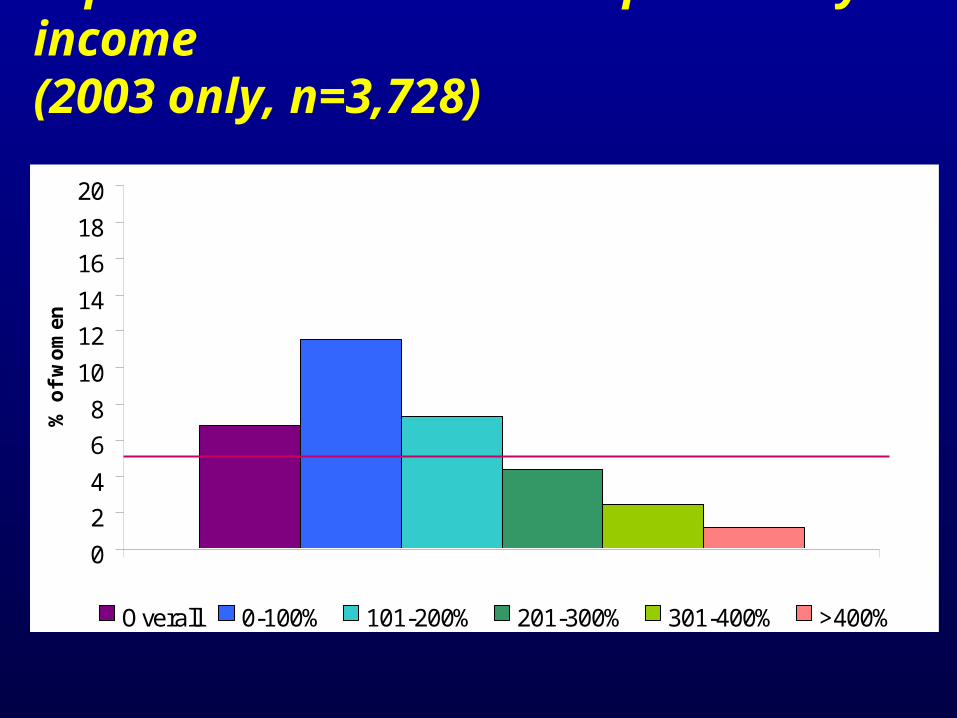
Separated or divorced: disparities by income(2003 only, n=3,728)
0
2
4
6
8
10
12
14
16
18
20
% o
f w
om
en
Overall 0-100% 101-200% 201-300% 301-400% >400%
% of Federal Poverty Level

Separated or divorced: racial/ethnic disparities (2003 only, n=3,728)
0
2
4
6
8
10
12
14
16
18
Afr Amer API - US API - notUS
EuroAmer
Latina US Latina notUS
AmerIndian
% o
f w
om
en

Partner lost his job: disparities by income (2003 only, n=3,728)
0
2
4
6
8
10
12
14
16
18
20
% o
f w
om
en
Overall 0-100% 101-200% 201-300% 301-400% >400%
% of Federal Poverty Level

Partner lost his job: racial/ethnic disparities (2003 only, n=3,728)
0
2
4
6
8
10
12
14
16
18
20
22
Afr Amer API - US API - notUS
EuroAmer
Latina US Latina notUS
AmerIndian
% o
f w
om
en

Homeless: disparities by income(2003 only, n=3,728)
0
2
4
6
8
10
12
14
16
18
20
% o
f w
om
en
Overall 0-100% 101-200% 201-300% 301-400% >400%
% of Federal Poverty Level

Homeless: racial/ethnic disparities(2003 only, n=3,728)
0
2
4
6
8
10
12
14
Afr Amer API - US API - notUS
EuroAmer
Latina US Latina notUS
AmerIndian
% o
f w
om
en

Food insecurity: disparities by income,2002-2003, n=7206
0
4
8
12
16
20
24
28
32
36
40
% o
f w
om
en
Overall 0-100% 101-200% 201-300% 301-400% >400%% of Federal Poverty Level

Food insecurity: racial/ethnic disparities,2002-2003
0
4
8
12
16
20
24
28
32
Afr Amer API - US API - notUS
EuroAmer
Latina US Latina notUS
AmerIndian
% o
f w
om
en

Total Number of Hardships* Women Had During Pregnancy: by Income, MIHA 2003
0102030405060708090
100
Family income as a % of federal poverty level
% o
f p
reg
nan
t w
om
en
Five or more
Four
Three
Two
One
*Hardships included here are ‘hard to make ends meet’, ‘food insecurity’, ‘no practical support’, ‘no emotional support’, ‘separated/divorced during pregnancy’, ‘homeless’, ‘job loss of spouse/partner’, ‘involuntary job loss of herself’, ‘incarceration’, and ‘domestic violence’. Note that ‘poverty’ and ‘near-poverty’ are not included as hardships in this analysis by income groups.

Total number of hardships1 women had during pregnancy: by racial/ethnic group, MIHA 2003
0
20
40
60
80
100
% o
f p
reg
nan
t w
om
en Five or more
Four
Three
Two
One
1Hardships included here are ‘poverty’, ‘hard to make ends meet’, ‘food insecurity’, ‘no practical support’, ‘no emotional support’, ‘separated/divorced during pregnancy’, ‘homeless’, ‘job loss of spouse/partner’, ‘involuntary job loss of respondent, ‘incarceration of respondent or her spouse/partner’, and ‘domestic violence’.
2N=3,692; 3Born in the United States; 4Born outside the United States.
3 4 3 4
Race/Ethnicity
2

Big disparities, but hardships were prevalent overall
Black, Latina, and Am. Indian women had more hardships but all age and racial/ethnic groups had hardships
Poor & near-poor women had more hardships But women with incomes 201-300% of poverty also
had hardships (e.g., ~10%: hard to live on income, job loss, food insecurity…)
And women with incomes 301-400% of poverty had some hardships (~10% partner lost job)

Most women giving birth had low incomes
A third were poor (family income < 100% of federal poverty line)
Another fifth (20%) were near-poor (101-200% of poverty)
53% were low-income (up to 200% of poverty)
Who is the maternity mainstream?

California is not unique
Data from 17 PRAMS states (CDC survey, 2000-01) paint a similar picture Similar prevalence of poverty (32%) and low
income (53%) Hardships prevalent overall Big disparities But affected all social groups except high-
income women (28% of sample)

Impact on maternal & infant health?
Food insecurity & homelessness: maternal health impact is obvious
Poor maternal nutrition a known risk for LBW Homelessness: Threat to maternal nutrition,
and major stressor All other hardships are major stressors. If
chronic, evidence indicates could affect birth weight and prematurity

What is known about impact of stress on birth outcomes?
Stress can adversely impact birth outcomes through direct physiologic pathways:
Neuro-endocrine mechanisms Immune/inflammatory response Vascular effects
And stress adverse behaviors with impact on birth outcomes
Effects can be modified by social support

And what about values?
Compassion for suffering Ethical principles: justice Human rights:
Right to attain highest biologically possible state of health
Right to a standard of living adequate for health
Implications?
Prenatal care in US: a medical model More visits for low-risk women than in most
western European countries Very limited psychosocial/economic services
“Comprehensive” care: primarily adds health education
WIC Few low-income women qualify for TANF or
housing assistance

Are there other models?
Contrast with some western European countries that provide all pregnant women with: Universal, cradle-to-grave health insurance Income support (“prenatal allowance”) Housing assistance Range of services to reduce poverty and buffer
psychosocial consequences of low income Could deficiencies of US model help explain our
worse birth outcomes? What about policies & services affecting pre-
pregnancy conditions, including in childhood?
Conclusions
Many women experience major economic & psychosocial hardships during pregnancy
Most pregnant women are low-income Big disparities but diverse socioeconomic, age,
and racial/ethnic groups are affected Science & values support need to address these
hardships Need to re-assess content of prenatal care &
consider models used elsewhere – including policies affecting psychosocial & economic stressors across the life course