maternal mental illness antenatal and postnatal depression dr andrew mayers...
TRANSCRIPT
2
Maternal Mental Illness
Overview What is maternal mental illness? Consequences for child and the mother Effect on relationship between them Types of illness
Antenatal depression Antenatal anxiety Postnatal depression
We will look at these illnesses in this session Serious illnesses (later session)
Postpartum psychosis Maternal OCD
3
Who am I? What am I doing here?
First worked in Hampshire perinatal MH unit in 2003
Co-ordinated research programme
Now associated with Dorset MBU in Bournemouth
Formerly, Director of PANDAS
National pre- and postnatal mental illness charity
Member of Maternal Mental Health Alliance
Member of Perinatal Mental Health Partnership
Commissioned by NHS in Hampshire and IOW to ‘train’ health profs
Presented at CPHVA conference, York (Oct 2013)
For more information:
http://www.andrewmayers.info/perinatal-mental-health.html
Follow me on Twitter @DrAndyMayers
4
Postnatal period
Correlation between antenatal mental distress and postnatal maternal distress and antenatal attachment and postnatal attachment...PREVENTION!!
Change/transition Psychological distress (anxiety, stress, low
mood) Stress, daily
hassles of bring up an infant,
change in identity, relationship
changes, loss of control …
5
Impact on developing child
Significant intellectual deficits found in children (aged 4) whose mothers had suffered with depression (Cogill, et al., 1986)
Postnatal depression may be associated with later difficulties in child’s adjustment-problems when starting school
Anxiety in girls; conduct problems in boys
Affects child’s social and emotional development
Ability to form relationships
Depression in fathers associated with emotional and behavioural outcomes in children aged 3½ years
Increased risk of conduct problems in boys
Effects remain after controlling for maternal postnatal depression (Ramchandani et al., 2005)
6
Impact of postnatal depression
PND associated with several negative outcomes Increased marital stress Disturbances in child’s emotional and cognitive
development (Cogill, et al., 1986)
Children of dep mums more likely to be associated with: Insecure attachment Eating difficulties Sleep disturbance Being overly clinging
PND affects mum’s ability to cope with care of baby See Murray, et al., 2003
7
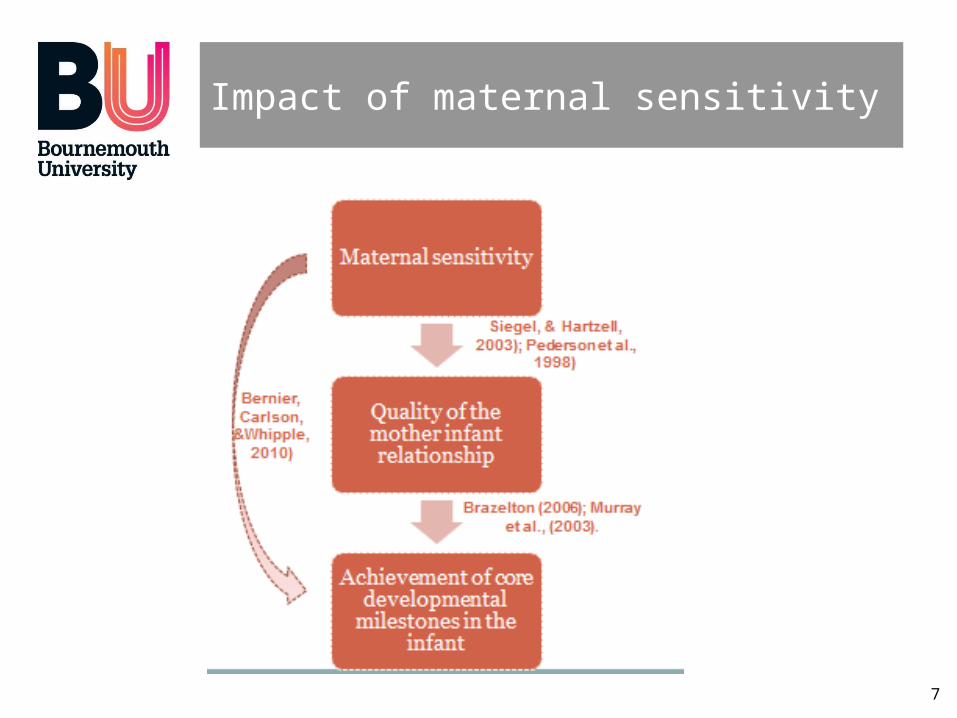
Impact of maternal sensitivity
8
The importance of attachment
Why is attachment important between mother and infant? Early mother–infant bond may have sig. impact on
developing infant (e.g. Bowlby, 1953; Ainsworth, 1993) Infant’s internal working model (IWM) is very important
Expectations about themselves in relation to others Model of self and of other
If infant’s carer attends positively and responds to needs Infant has positive IWM:
High self-worth, availability of others, resolution of crises
Infant’s carer inconsistent response and attention Infant’s has negative IWM:
Low or ambivalent self-worth, unavailable others, crises not resolved
9
What can health visitors do?
Health visitors CAN play a crucial role in identifying mental health difficulties Spotting signs and risk factors Early intervention Signposting to relevant services
For the well-being of mother AND the developing infant
Important to: Acknowledge distress Offer an empathic response Assess risk
But WHAT are we looking for?
10
Antenatal depression
“At any one time during pregnancy one in every ten women will be depressed and around one in every thirty will be depressed in pregnancy and the postnatal period” Dr Vivette Glover
Symptoms Chronic anxiety Guilt Incessant crying Lack of energy Relationship worries
Worrying their partner may leave once the baby is born
Conflict with parents Isolation Fear to seek help
11
Causes of antenatal depression
Physical Body changes!
Weight gain (only clothes that fit are tatty or were previous used for ‘painting’), swollen breasts, dizziness and nausea, bladder issues, exhaustion, heart rate, blood pressure, swollen ankles/wrists...
Hormonal changes Nausea – morning sickness
For some mums-to-be these experiences (and/or perception of them) worse than for others
12
Causes of antenatal/postnatal depression
Emotional causes
Mood swings
First-time mum experience
Change of identity
Previous pregnancy difficulties
Complications, difficult labour, miscarriage, stillbirth…
Chronic anxiety
Especially new mums
NEVER ‘dismiss’ anxiety - EMPATHISE
13
Causes of antenatal depression
Social causes Antenatal depression is NOT new (despite only being
recognised relatively recently) Mums just did not have chance to talk about it then
Family support Families often lived closer together than they do now
Work and finance Greater pressure for mum to work in modern age
Expectations Media perceptions of perfect nursery/bedroom Pressure to live to societal standard
Good enough mum
NOTE: Majority of cases of antenatal depression disappear at birth BUT - one third of these mums develop postnatal depression
14
Post-natal depression (PND)
Baby blues (see O’Hara, 2009)
Two to four days after birth (quite normal – but not PND) Emotional/liable to burst into tears, for no apparent
reason Difficult sleeping (even when baby permits) Loss of appetite Feeling anxious, sad, or guilty Questioning maternal skills
Effects up to 75% of mums May relate to changes in post-birth hormone levels
Or could be related to being in hospital Key is that this doesn't last long – usually only a few days
If it persists it may develop into PND
15
PND: DSM-5 diagnosis
PND needs same DSM-5 diagnosis as major depressive disorder But relates specifically to the peripartum period
Pregnancy and/or within 4 weeks of birth Five (or more) of (but at least one of symptom 1 or 2)
1. Depressed mood (for most of day, nearly every day…)
2. Markedly diminished interest in all/almost all activities
3. Significant weight loss (not dieting) or decease/increase appetite
4. Insomnia or hypersomnia
5. Psychomotor agitation/retardation (observable)
6. Fatigue or loss of energy
7. Feelings of worthlessness or excessive/inappropriate guilt
8. Diminished ability to think/concentrate or indecisiveness
9. Recurrent thoughts of death… suicidal ideation/attempt/plan
16
PND: Features
Additional features may also indicate presence Sense of inadequacy, inability to cope Feeling guilty Being unusually irritable
Which makes the guilt worse Being hostile/indifferent to husband/partner/baby Losing interest in sex Panic attacks Excessive unwarranted anxiety
Such as being alone in the house Obsessive fears about the baby's health or wellbeing
17
PND: Prevalence
PND affects about 10% of new mums Compare to baby blues (25-75%)
Although DSM-5 states ‘must be within 4 weeks of birth’ Most clinicians/researchers extend this to several months
Vulnerable mums usually referred in ‘perinatal’ period During pregnancy up until baby is 1 year
Can come on gradually or all of a sudden Can range from being relatively mild to very hard-hitting About 50% PND women afraid to tell health professionals
about it Scared it will lead to social services taking child away Or that they would be seen as bad mothers
See O’Hara (2009) for good overview of PND
18
PND: Causes
Causes of PND uncertain But there are a number of known risk factors (Kim, et al.
2008)
Having had depression before Especially PND
Not having a supportive partner Having a premature or sick baby Having lost your own mother as child Having had several recent life stresses
Bereavement, unemployment, housing or money problems
Poor sleep (see later)
19
PND: Causes
Some additional risk factors for PND Shock of becoming a mother
Women often unprepared for physical impact of childbirth
Plus new and daunting skills to learn New full time responsibility Helpless human being who cannot communicate
Other than cry (distressing in itself) Some mums get anxious when they don’t hear
crying! Lie awake listening out
Loss of freedom and independence Exhaustion and fatigue
20
PND: Causes
Hormones Oestrogen and progesterone affect emotions
Levels of progesterone are very high during pregnancy PND maybe due to sudden drop progesterone after
birth In one study women given progesterone to try prevent
PND But it had the reverse effect and got worse Oestrogen treatment via patch can be helpful
Otherwise, hormones not a major influence Diet
Lack of certain nutrients during pregnancy may cause PND Omega 3 oils (found in oily fish, seeds and nuts) Magnesium (leafy green vegetables and seeds) Zinc (seeds and nuts)
21
PND Treatment
Antidepressants Huge amount of evidence of benefit in treating
depression First line choice in most adults BUT it is not that simple in PND
Some antidepressants serious side effects and interaction
Consider this if mum is breastfeeding Some antidepressants are not safe for infants
22
Medication for PND – what is safe?
Tricyclic antidepressants Lower known risks than other antidepressants
But more dangerous in overdose SSRIs (after 20 weeks) greater risk hypertension in
neonate Fluoxetine fewer known risks of SSRIs Paroxetine (in 1st trimester) some risk foetal heart
defects Venlafaxine some risk high blood pressure (at high
doses) Most antidepressants pass into the breast milk
Imipramine, nortryptiline and sertraline - at relatively low levels
Citalopram and fluoxetine - at relatively high levels
23
PND Treatment
Counselling and talking therapies (CBT etc.) very effective
Group or individual care
BUT rare - can take time to get into a programme
We need more Perinatal Mental Health teams!
Self-help strategies
Counselling (listening visits)
Brief cognitive behavioural therapy
Interpersonal psychotherapy
24
Whooley questions
During the past month…
1. Have you often been bothered by feeling down, depressed or hopeless?
2. Have you often been bothered by having little interest or pleasure in doing things?
Consider a third question:
Is this something you feel you need or want help with?
25
What we have learned
We have examined several aspects of maternal mental illness What is maternal mental illness? Types of illness
Antenatal depression Antenatal anxiety Postnatal depression
26
Exercise
Group task Are Whooley questions enough? What are the risk factors? What signs should we watch out for? Why are mums reluctant to tell us about mental health
problems? How far should we pursue this?