maternal mortality dr tucker obgyn
TRANSCRIPT
Maternal MortalityBY SHANNON LARATONDA, MHS

Definition and statistics
Maternal mortality: deaths due to complications
from pregnancy or childbirth (UNICEF)
Death of a woman during pregnancy or within 1 yr. of pregnancy termination (CDC)
From 1990 to 2013, rate declined 45% 1990 – 377,000 deaths 2013 – 293,000 deaths
Average annual rate of reduction 2.6% 5.5% annual decline rate needed to
achieve United Nations’ Millenium Development Goal 5 To ↓ rate by 75% by 2015

Maternal mortality ratio
Maternal mortality ratio: maternal deaths per 100,000 live births in women aged 15-49, by region, 1990, 2005, and 2013
Remains unacceptably high in sub-Saharan Africa
Huge disparities found between richest and poorest countries serve as evidence that almost all maternal deaths can be prevented

Facts from World Health Organization
Every day approx. 800 women die from preventable causes related to pregnancy and childbirth (worldwide) 650 per year in U.S.
99% of all mortality deaths occur in developing countries More than half occur in sub-Saharan
Africa Almost 1/3 occur in South Asia
Maternal mortality is higher in women living in rural areas and among poor communities
Females <15yo. & >35yo. face highest risk of complications and death from pregnancy Leading cause of death among
adolescent girls in developing countries
1/160 lifetime risk of maternal death in developing countries; 1/3700 developed
Skilled care BEFORE, DURING, and AFTER childbirth can save the lives of women and newborns

Causes of Maternal Mortalities Worldwide in 2014

Causes of Maternal Mortalities in the U.S. in 2011

Infection → Sepsis (14% U.S.)
Mother should practice good hygiene Helps if early signs of infection are
recognized and treated in a timely manner Chills, pus draining from uterus,
fever, lower abdominal pain, malaise, uterine tenderness, uterus does not return to normal size
Puerperal sepsis: infection related to giving birth Chlamydia, C. tetani, C. welchii, E.
coli, gonococci, staph, strep Endometritis Breast infections
ie. mastitis – 1 in 20 nursing mothers
Wounds from childbirth Urinary tract infections Unsafe abortions

Postpartum Hemorrhage (11.3% U.S.)
Severe bleeding after birth can kill a healthy woman within hours if unattended
Approx. 4% of women More likely with a C-section #1 cause is uterine atony Other causes:
Retained products of conception (RPOC)
Uterine tear Poor clotting
Maternal hemorrhage is the third most likely cause of death for women in low income countries; behind HIV/AIDS and TB (WHO, 2008)
Oxytocin immediately after childbirth effectively reduces the risk of bleeding

Postpartum Hemorrhage
Symptoms Uncontrolled bleeding Decreased BP Increased HR Low Hct Swelling and pain in tissues in the
vaginal and perineal areas
Diagnosis Medical hx, PE, and labs
Estimation of blood loss PR and BP Hct Clotting factors in blood

Postpartum Hemorrhage
Treatment IV fluids Blood transfusion to prevent shock Oxytocin, Misoprostol, Ergotamine Oxygen mask Stop the cause
Manual massage of the uterus to stimulate contractions
Removal of placental pieces Pack the uterus with sponges or other
sterile materials Tie-off bleeding blood vessels Laparotomy to ID source of bleeding hysterectomy

Postpartum Hemorrhage
Risk factors Placental abruption Placenta previa Overdistended uterus from
excess amniotic fluid, large fetus or multiple pregnancy
Gestational hypertension or preeclampsia
More than 5 previous births General anesthesia
Prolonged labor Infection Obesity Medications to induce labor Medications to stop
contractions for preterm labor
Use of forceps or vacuum-assisted delivery
Peripartum Cardiomyopathy (10.1% U.S.)
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2612110/ Increased blood volume → increases CO

Thrombotic PE (9.8% U.S.)
Hypercoagulability Main reason - pregnancy is a
hypercoagulable state 4-5 fold increase risk of
thromboembolism during pregnancy and post partum
Highest risk in 3rd trimester 80% are venous thromboembolism
(VTE) Incidence 0.49-1.72 per 1,000
pregnancies
Risk factors Hx of thrombosis Inherited or acquired
thrombophilia Increased maternal age Complications of pregnancy and
childbirth
Hypertensive Disorder of Pregnancy (8.4% U.S.)
Preeclampsia Hypertension after 20 weeks,
edema, proteinuria, thrombocytopenia
Should be detected and managed before seizure onset (eclampsia)
HELLP syndrome Hemolysis, Elevated Liver enzymes,
Low Platelets 0.2-0.6% of all pregnancies Abnormal periph. smear, LD
>600U/L, bilirubin >1.2mg/dl, elevated AST/ALT, low platelets
DELIVER BABY!!! Rx magnesium sulfate to prevent seizures, blood transfusion To prolong pregnancy: bed rest, fetal monitor, antihypertensive and corticosteroids
Treatment
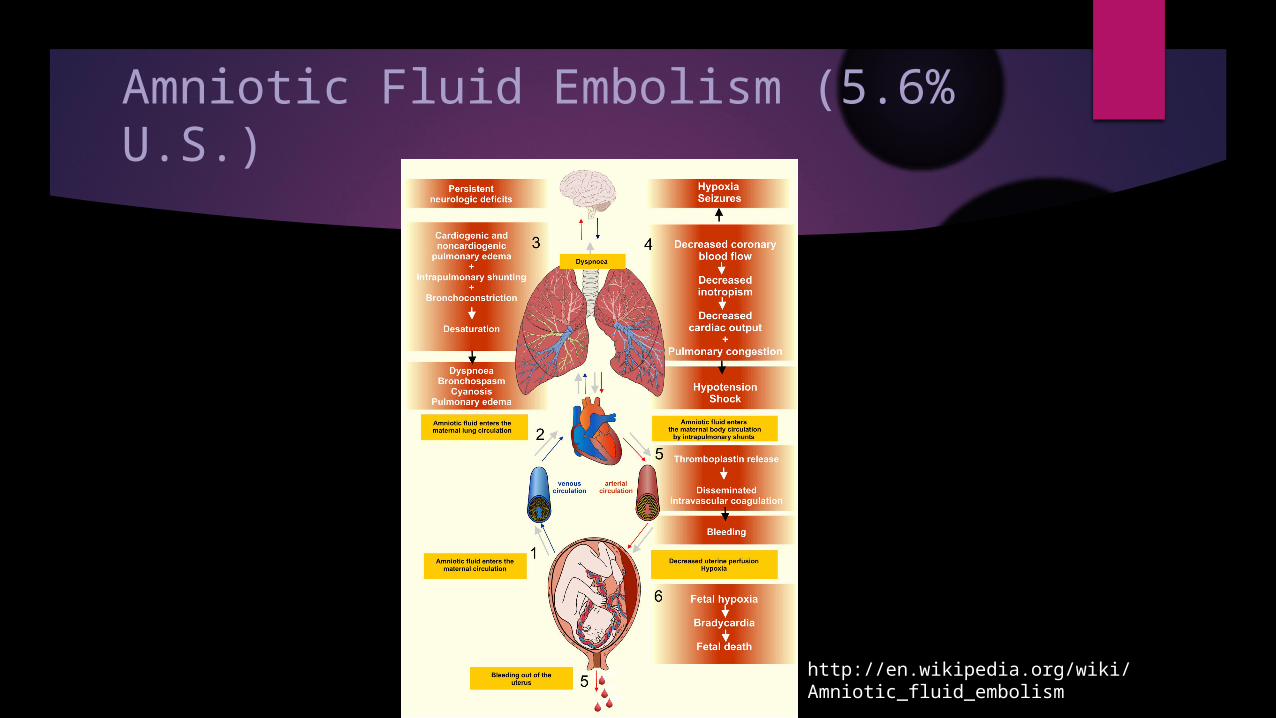
Amniotic Fluid Embolism (5.6% U.S.)
http://en.wikipedia.org/wiki/Amniotic_fluid_embolism

Avoid Maternal Deaths
Prevent unwanted pregnancies and young adolescent pregnancies Access to contraception Safe abortion services and post-abortion care Education and awareness

References
Centers for Disease Control and Prevention (2015). Pregnancy Mortality Surveillance System. Retrieved April 20, 2015 from http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/PMSS.html.
UNICEF (2015). Maternal Mortality. Retrieved April 20, 2015 from http://data.unicef.org/maternal-health/maternal-mortality.
World Health Organization (WHO), (May 2014). Maternal Mortality. Retrieved April 20, 2015 from http://www.who.int/mediacentre/factsheets/fs348/en/.