maximum medical therapy of chronic...
TRANSCRIPT

Maximum Medical Therapy
of Chronic Rhinosinusitis
Riyadh Alhedaithy
R5 ENT Resident, Combined KSUF and SB.
30/12/2015
ARTICLE REVIEW
INTRODUCTION
Chronic rhinosinusitis (CRS) is a common, debilitating, and
expensive chronic inflammatory disease.
Despite appropriate medical therapy, a subset of patients with CRS
will have persistent symptoms and be considered candidates for
endoscopic sinus surgery (ESS).
ESS is associated with improvements in patient symptoms, quality of
life, and is the economically wise choice compared to continued
medical therapy alone.

INTRODUCTION
The decision on when to offer surgery is poorly defined.
There is no consensus on what the ‘appropriate’ or
maximal medical therapy (MMT) should be provided to
patients prior to considering them candidates for ESS.
In order to improve the appropriateness and value of care
for CRS, it is important to define appropriate evidence-
based indications for ESS.
OBJECTIVES
To define the MMT criteria used as an indication for
ESS in patients with persistent symptoms of CRS.
MATERIALS AND METHODS
Databases (Jan 2009-Dec 2014):
Ovid MEDLINE, EM-BASE, Cochrane Central
register of Controlled Trials, Cochrane Database of
Systematic Reviews, Science Citation Index,
Database of Abstracts and Reviews of Effects, CAB
Abstracts, and the Cumulative Index to Nursing and
Allied Health Literature (CINAHL)

MATERIALS AND METHODS
Inclusion criteria:
Adult patient population (>18 years of age) with a
diagnosis of CRS and received ESS.
Exclusion criteria:
CF, granulomatous and autoimmune disease,
immotile ciliary diseases, acute complications of
rhinosinusitis, or other non-CRS indications for ESS.

MATERIALS AND METHODS
Extracted Data:
Type of medical therapies
Mean duration of use for each therapy
Disease characteristics (including polyp status)
Diagnostic criteria utilized,
Subjective patient outcomes criteria used (if any)
MATERIALS AND METHODS
Primary outcome:
MMT criteria was defined as the medical therapy protocol
that must have been trialed and failed prior to being considered
a candidate for ESS.
Duration of each therapy involved in the MMT criteria was
synthesized in a quantitative manner by calculating means
with standard deviations and 95% confidence intervals.
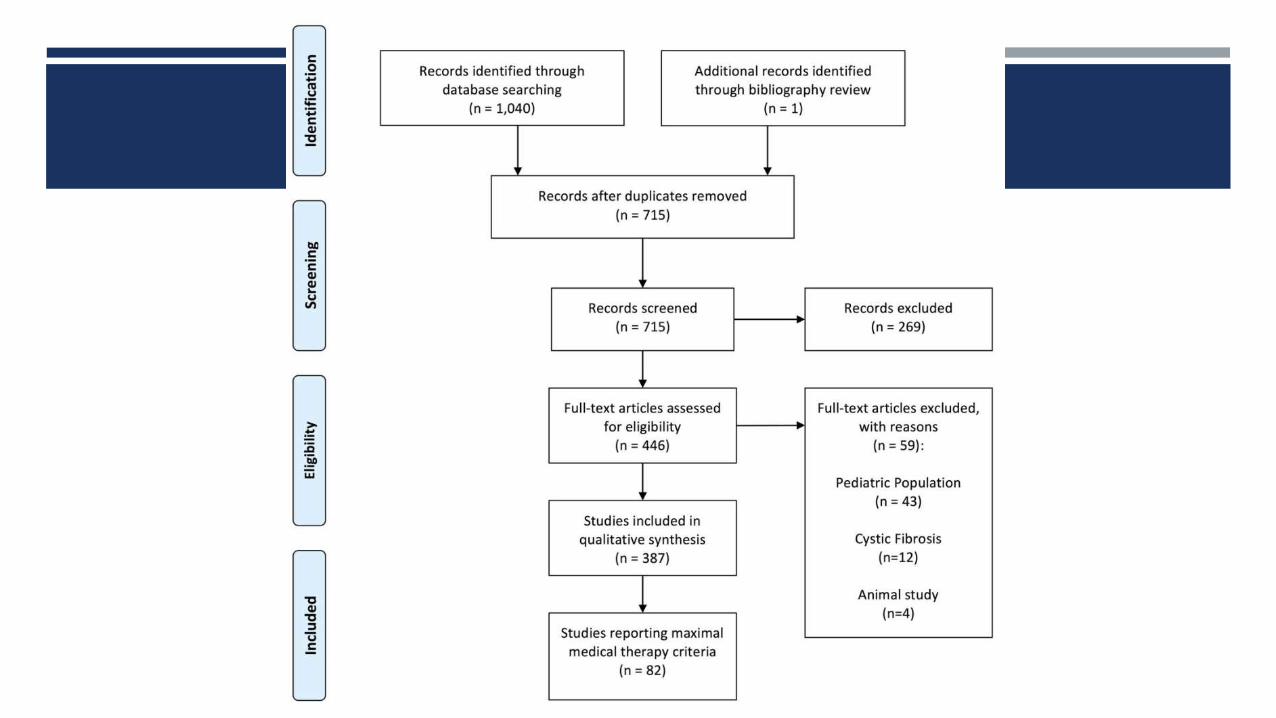
RESULTS

RESULTS
1041
Articles
82
Articles
60 (73%)
CRSwNP
CRSsNP
19 (24%)
CRSwNP
3 (4%)
CRSsNP
4 (5%)
Not
mentioned

RESULTS
MMT Criteria:
None of the studies specified the type of topical
corticosteroid therapy used in the MMT criteria.
Selection of oral antibiotic was typically described
as “broad spectrum” or “culture-directed
antibiotic”,
4 studies (5%) specified amoxicillin/clavulanate.
Prednisone and methylprednisolone were the
steroid agents used in the MMT criteria.

RESULTS
Of the 19 studies that evaluated CRSwNP patients,
14 (74%) included systemic corticosteroids as part of MMT criteria.
Of the 3 studies that evaluated CRSsNP patients,
All 3 (100%) included systemic corticosteroids in the MMT criteria.
Of the 60 studies that evaluated both CRSwNP and
CRSsNP patients,
31 (52%) included systemic corticosteroids.
RESULTS
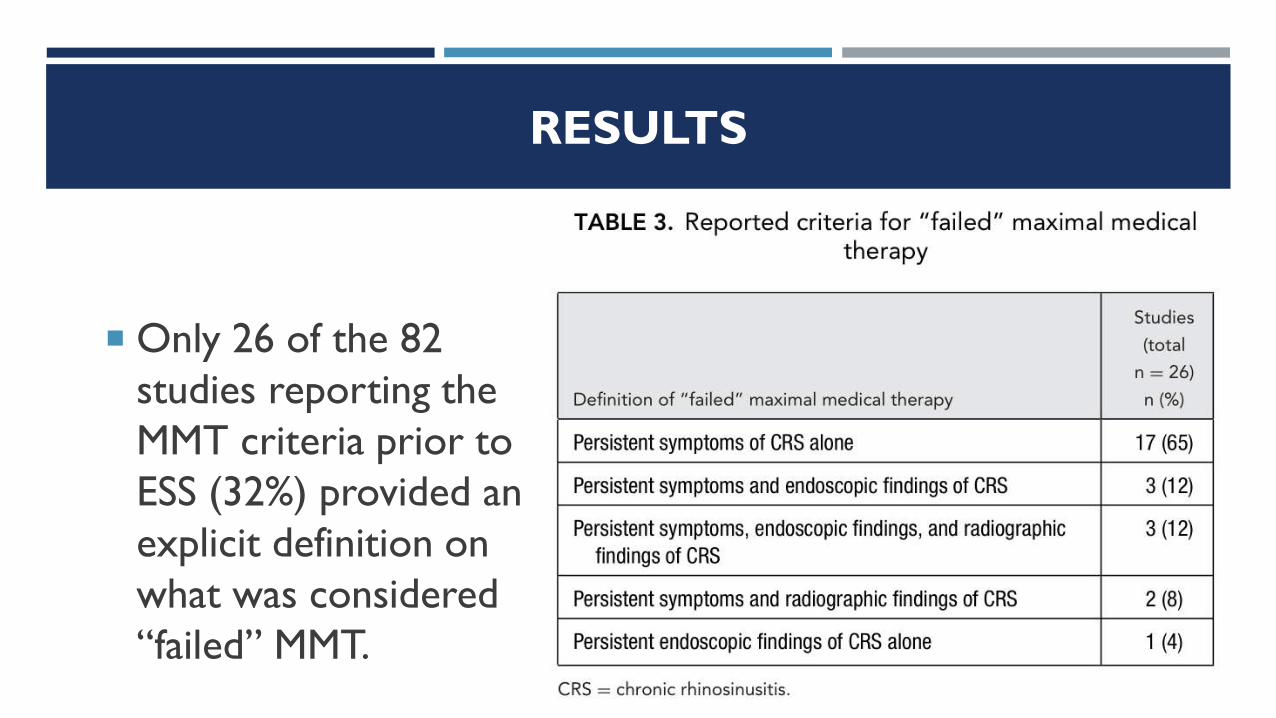
Only 26 of the 82
studies reporting the
MMT criteria prior to
ESS (32%) provided an
explicit definition on
what was considered
“failed” MMT.
DISCUSSION
In the 82 studies that explicitly reported MMT criteria
prior to ESS:
The most common MMT criteria were:
8-week course of topical intranasal corticosteroids (91%) and
3-week course of broad-spectrum or culture-directed oral antibiotic (89%).
The use of systemic corticosteroids was often included (61%), with
the mean duration being a 2-week course.
Evidence supports the use of systemic corticosteroids in CRSwNP,
but remains less conclusive for CRSsNP.

DISCUSSION
Majority of studies (65%) considered “failure” of MMT to
involve “persistence of CRS symptoms alone, without the
need for repeat radiologic imaging”
As there is currently a lack of a uniform definition of what
constitutes a “failure” of MMT, we feel authors need to
include this information in future studies evaluating ESS for
CRS.
DISCUSSION
Several mailed surveys have been performed
in an attempt to characterize which therapies
are included in MMT

DISCUSSION
In 2007, a survey study by Dubin et al. was selectively
mailed to members of the American Rhinologic Society
(ARS) and obtained 308 responses:
The most common response indicated that practitioners would
“always” include topical nasal corticosteroids and oral antibiotics
in their MMT regimen.
Saline irrigations and systemic corticosteroids were “usually”
included.

DISCUSSION
67% of respondents considered failure to involve an
“persistent symptoms with unchanged CT”
24% considered a failure to involve “persistent
abnormal CT despite complete resolution of
symptoms”.
DISCUSSION
The most recent survey study mailed questionnaires to all
members of ENT-UK (https://www.entuk.org) in 2012:
Majority (61%) of the 167 respondents self-identified as rhinologists.
Majority of respondents would “always” include topical
corticosteroid sprays (61%, 0-5 months duration) and oral
antibiotics (92%, 1-2 weeks duration).
Systemic corticosteroids (0-5 days duration) were “rarely” included.

DISCUSSION
Clarithromycin and amoxicillin-clavulanate were the
most broad-spectrum antibiotics used, in that order.
Majority of respondents would also consider routine
allergy testing with use of oral antihistamines, if
indicated by a positive test.

CONCLUSION
A minority of studies explicitly report MMT criteria before
considering a patient with CRS a candidate for ESS.
When reported, the MMT criteria varied widely with the majority
of protocols involving a minimum 8-week course of topical
intranasal corticosteroids and 3-week course of oral
antibiotics.
A 2-week course of systemic corticosteroids was also included as
part of MMT in more than one-half of the reviewed studies.

ARTICLE REVIEW

OBJECTIVE
Evaluate the effects of oral glucocorticoids and
doxycycline on symptoms and objective clinical
and biological parameters in patients with
CRSwNP.

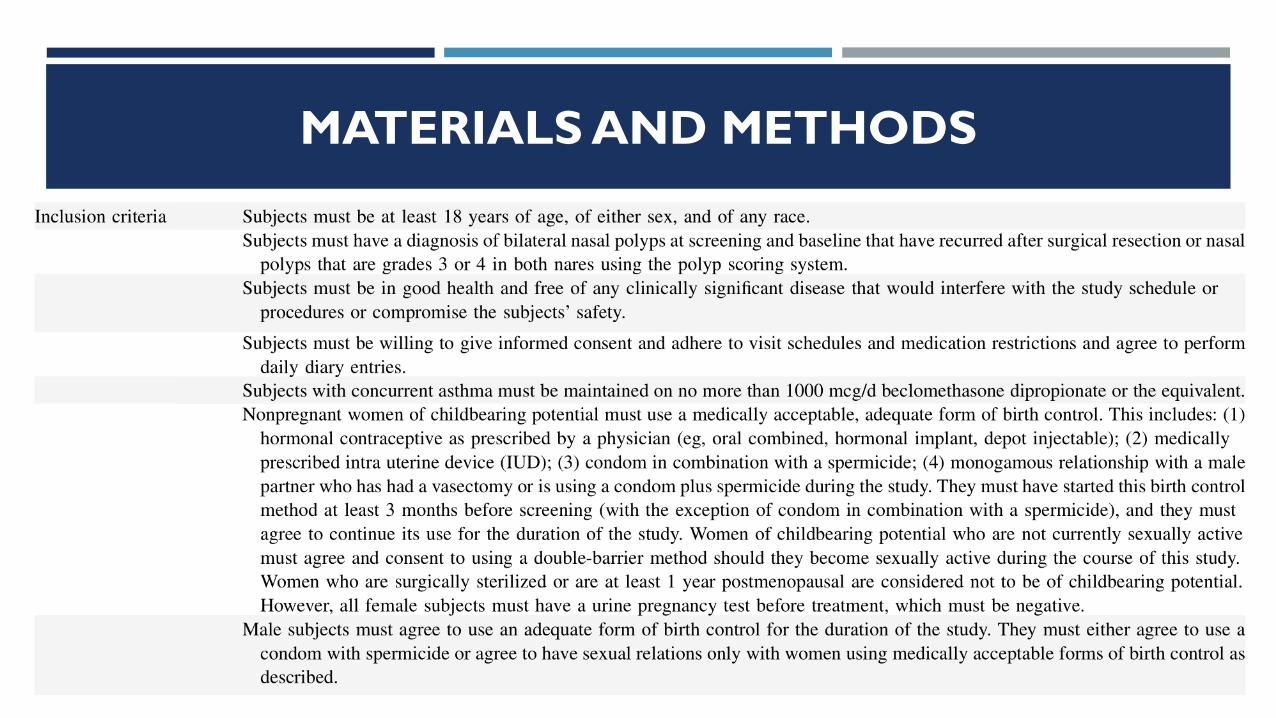
MATERIALS AND METHODS
Double-blind, placebo-controlled, multicenter trial.
Randomly assigned 47 patients with bilateral nasal polyps to
receive either (for 20 days):
Methylprednisolone in decreasing doses (32–8 mg once daily)
Doxycycline (200 mg on the first day, followed by 100 mg once
daily)
Placebo
MATERIALS AND METHODS
Patients were followed for 12 weeks and were assessed for:
1. Symptoms and signs by nasal endoscopy.
2. Nasal peak inspiratory flow.
3. Markers of inflammation in nasal secretions (eosinophilic cationic
protein (ECP), IL-5, myeloperoxidase, matrix metalloproteinase 9,
and IgE).
4. Peripheral blood level concentrations of (eosinophils, ECP, and
soluble IL-5 receptor)
MATERIALS AND METHODS

MATERIALS AND METHODS

RESULTS

RESULTS
Methylprednisolone
Group:
Significant reduction of
polyp size after one week
compared to placebo p= 0.002
Maximal reduction was
after two weeks P< 0.0001

RESULTS
Methylprednisolone
Group:
Polyps began to recur after
2 weeks, but still has
significant reduction in
polyp score compared
with the placebo until
month 2.

RESULTS
Methylprednisolone
Group:
After 3 months, NO
significant effect of
methylprednisolone on
polyp size was observed
compared with placebo
and baseline values.

RESULTS
Doxycycline Group:
Significant reduction in
polyp size starting at week
two compared with
placebo and remained
significantly reduced upto
3 months after dosing.

RESULTS
Effect of Methylprednisolone on
patients symptoms compared to
placebo:
Significant decrease in nasal congestion ,
PND and hyposmia after 1 week until 4
week.
Symptoms scores worsened
progressively after week 4 and returned
to baseline values.
No significant effect on rhinorrhea

RESULTS
Effect of Doxycycline on patients
symptoms compared to placebo:
Significant reduction in PND at week 2
and significant reduction in rhinorrhea
at week 8.

RESULTS
Anti-inflammatory effects of Methylprednisolone:
Significant decrease of eosinophils in blood samples compared with
placebo starting at week 1, with a maximal decrease at 2 weeks.
Blood eosinophils counts returned to baseline levels at month 1.
Rebound eosinophilia (above baseline level) observed levels at
month 2 and 3.
Significant reduction in IL-5 and IgE at weeks 1,2,and 4.
No change in MMP-9 levels in nasal secretion
RESULTS
Anti-inflammatory effects of Doxycycline :
No effect on eosinophils level in blood samples.
No effect on IL-5 level in nasal secretions.
Significant reduction in IgE at weeks 1,2,and 4.
Significant decrease in levels of myeloperoxidase and MMP-9 in
nasal secretions.

CONCLUSION
Methylprednisolone and doxycycline each significantly decreased
nasal polyp size compared with placebo.
Oral doxycycline causes a long-term reduction in nasal polyp size
(lasting for 12 weeks), whereas methylprednisolone causes an
initial reduction in polyp size (maximal after week 2) but complete
recurrence after 2 months.
Treatment of CRSwNP with oral corticosteroids is of limited value
unless it is associated with surgery or therapy with intra nasal
corticosteroids.