mca latest
DESCRIPTION
middle cerebral artery slidesTRANSCRIPT

MIDDLE CEREBRAL ARTERY
SHARMINIY A/P MUNIANDY1000356AIMST UNIVERSITY
MIDDLE CEREBRAL ARTERY (MCA)DEFINITIONS Middle cerebral artery syndrome
is a condition whereby the blood supply from the middle cerebral artery (MCA) is restricted, leading to a reduction of the function of the portions of the brain supplied by that vessel: the lateral aspects of frontal, temporal and parietal lobes, the corona radiata, globus pallidus, caudate and putamen. The MCA is the most common site for the occurrence of ischemic stroke.
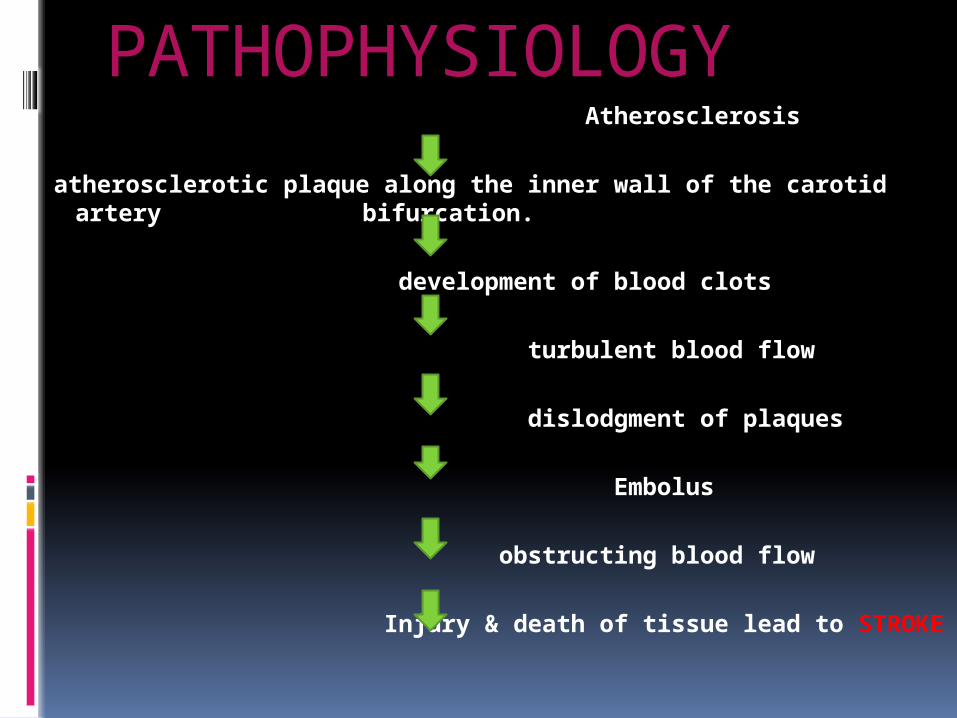
PATHOPHYSIOLOGY Atherosclerosis
atherosclerotic plaque along the inner wall of the carotid artery
bifurcation.
development of blood clots
turbulent blood flow
dislodgment of plaques
Embolus
obstructing blood flow
Injury & death of tissue lead to STROKE

CLINICAL FEATURES
Contralateral hemiparesis involving mainly the upper limb and face ( lower limb is more spared)
Contralateral hemisensory loss involving mainly the upper limb and face (lower limb is more spared)
Motor speech impairment : broca’s or nonfluent aphasia with limited vocabulary and slow,hesitant speech
Receptive speech impairment:wernicke’s or fluent aphasia with impaired auditory comprehension and fluent speech with normal rate and melody.
Global apahasia : nonfluent speech with poor comprehension
Perceptual deficits: unilateral neglect,depth perception,spatial relations,agnosia
Limb kinetic apraxia Contralateral homonymous hemianopsia Loss of conjugate gaze to the opposite side Ataxia of contralateral limbs (sensory ataxia) Pure motor hemiplegia (lacunar stroke) Difficulity in reading,writing and calculating

MEDICAL MANAGEMENT
antiplatelet (aspirin ,Thienopyridines or anticoagulant (warfarin) at first diagnosis.
SURGICAL MANAGEMENT
Carotid endarterectomy or carotid angioplasty can be used to remove atherosclerotic narrowing (stenosis) of the carotid artery.
Endarterectomy for a significant stenosis has been shown to be useful in the secondary prevention after a previous stroke
Hemicraniectomy

DIAGNOSIS
Ultrasonography Magnetic Resonance Imaging CT ANGIOGRAPHY

EVIDENCE BASED JOURNALS
Emilia MikołajewskaNDT-Bobath Method in Normalization of Muscle
Tone in Post-Stroke Patients 2012
In all cases with recovery, this level of recovery was grade 1. The greatest number of recoveries was observed from grade 1 to grade 0 on the Ashworth
Scale. It implicates the conclusion that, in the area of
muscle tension normalization, the NDT-Bobath method is most efficient in cases of mid-range increased muscle tension.
Constraint-Induced Movement Therapy During Early Stroke Rehabilitation Corwin Boake, Elizabeth A. Noser, Tony Ro, Sarah Baraniuk, Mary Gaber, Ruth Johnson, Eva T. Salmeron, Thao M. Tran 2007
On all measures of motor function of the affected arm and hand, patients who received
CIMT showed an apparent advantageous trend over patients who received intensive traditional therapy.
Relative to the control group, the CIMT group reported significantly greater improvement in quality of performing daily activities using the affected hand.
PHYSIOTHERAPY MANAGEMENT
Flaccidity stage weightbearing, passive range of motion,
proper positioning of limbs, and facilitation techniques such as tapping, quick stretch, and electrical stimulation.
Scapular mobilization is important during the spastic stage to help reduce stiffness of scapula and increase shoulder range of motion.
A hand or wrist splint may also be useful, particularly at night.
Heat or cold therapy can temporarily decrease spasticity and allow the muscle to be stretched.
Electromyographic biofeedback EMGBF:

Weight bearing can be done by the caregiver placing the patient's open hand on a flat surface (i.e. mat, bed, book), supporting the patient's elbow so the arm won't buckle, and having the patient lean and put weight down through the flaccid arm and hand. One can also tap the muscles to try an initiate movement.
Sensation Interventions
Encourage pt to use the more involved side to increase awareness and function.
Stroking involved extremity using textured fabrics, pressing objects into hand, or drawing shapes and letters on the skin.
Approximation through weight bearing in sitting/modified plantigrade/standing
Stretching Superficial and Deep pressure stimulation

Motor Function Interventions AROM and PROM daily in all jts and
motions. (scapula is very important to prevent impingement in subacromial space during overhead movements)
arm cradling, table top polishing, sitting leaning forward and reaching both hands down to the floor.
Positioning strategies w/ proper jt alignment –splints may be necessary

Manage Spasticity
Prolonged pressure on long flexor tendons in arm
Kneeling or quadruped to reduce spasticity in the quadriceps
Hooklying w/ lower trunk rotation or PNF chops to reduce tone in the trunk
Ice wraps or ice packs can be used temporarily to reduce spasticity.
splints to provide for early wb and break up synergy patterns
Strength Interventions
Free Weights Step-ups while wearing ankle
weights Functional Activities PNF
Postural and Functional Mobility Interventions
Rolling to both side Supine <>Sit – from both sides- shift
LE’s over edge of bed and use UE’s to push up.
Sitting – with symmetrical posture and proper spine and pelvic alignment. Progress from stability>dynamic stabilty> reaching. Practice trunk flex/ext, lateral flex, and rotation.

Standing, Modified Plantigrade
Standing with unilateral support on the affected side.
transfer towards the less affected side, but it is important to practice transferring using both sides.

Balance Interventions Achieve postural alignment and static
stability, progress to weight shifting within limits of stability, maintain symmetrical weight bearing.
Increase the difficulty by applying perturbations, standing on a less stable surface, narrow BOS, extend UE or LE out to side, add head movements, add dual tasks, move from a closed environment to an open environment.
Gait Training Interventions Overhead harness on treadmill Parallel bars and ambulation aids Maintain Natural rhythm of walking and
speed. Encourage Pt to take even steps. Recognize gait abnormalities and correct. Position UE in extension and abduction with
the hand open to break up synergy pattern. Practice walking
forward/backward/sideward/cross-stepping, step-ups, stair climbing, step-overs/travel training in environment.
