mcdowell county schools employer administration manual€¦ · mcdowell county schools employer...
TRANSCRIPT

Metropolitan Life Insurance Company
New York, NY
McDowell County Schools
Employer Administration
Manual

Contents
Employer Administration Manual 01/09/13 i
Introduction ................................................................................................................... 1
Contacts ......................................................................................................................... 2 Customer Service Center Contacts ......................................................................................... 2 Life Contacts ........................................................................................................................... 3 Life Disability Contacts ............................................................................................................ 4 Dental Eligibility Contacts ........................................................................................................ 4 Dental Claim Contacts ............................................................................................................ 4 Additional Services Contacts .................................................................................................. 5
Reporting Structure ...................................................................................................... 6 Claims Structure ...................................................................................................................... 6 Billing Branches ...................................................................................................................... 6
Enrollment Procedures ................................................................................................. 7 Eligibility .................................................................................................................................. 7
Actively at Work Requirements ........................................................................................................................ 7 Deferred Effective Date for Disabled Dependents ........................................................................................... 7 Handicapped Dependent Children ................................................................................................................... 7 Common-Law Spouses as Dependents ........................................................................................................... 9
New Enrollments ................................................................................................................... 13 Late Enrollments ................................................................................................................... 16
Waiting Period ............................................................................................................................................... 16 Processing Coverage Changes ............................................................................................ 17
Change in Dependent Coverage ................................................................................................................... 17 Cancellation of Coverage Requested by an Employee .................................................................................. 17 Termination of Employment ........................................................................................................................... 17 Temporary Layoff or Leave of Absence, Disability, or Retirement ................................................................. 18 Death of an Employee ................................................................................................................................... 18
Beneficiary Designation ........................................................................................................ 19 Choosing a Beneficiary .................................................................................................................................. 19 Designating or Changing a Beneficiary .......................................................................................................... 20 Allocation of Payment .................................................................................................................................... 22
Sending Enrollment Data to MetLife .......................................................................... 23 Updating through MetLink® ................................................................................................... 23
Billing ........................................................................................................................... 24 Self Billing through MetLink® ................................................................................................. 24 Late Payments ...................................................................................................................... 29
Results of Late Premium and Fees and Invoices ........................................................................................... 29 Cancelled Coverage ...................................................................................................................................... 29 Reinstatement Rules...................................................................................................................................... 29 Rehire Rules .................................................................................................................................................. 29
Guidelines for Claims Submission ............................................................................ 32 Life Claims ............................................................................................................................ 32
Life Claims ..................................................................................................................................................... 32 Life Disability Claims ...................................................................................................................................... 40 Accelerated Benefits Option (ABO) Claims .................................................................................................... 46
Contents
Employer Administration Manual 01/09/13 ii
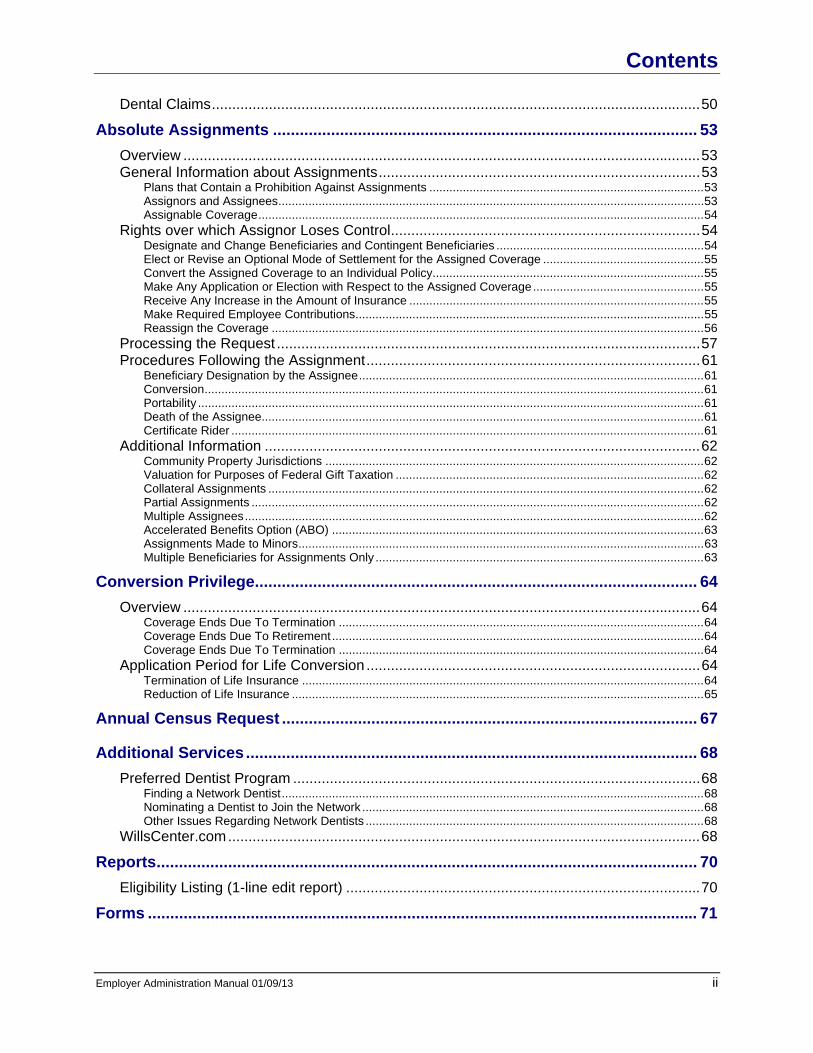
Dental Claims ........................................................................................................................ 50 Absolute Assignments ............................................................................................... 53
Overview ............................................................................................................................... 53 General Information about Assignments ............................................................................... 53
Plans that Contain a Prohibition Against Assignments .................................................................................. 53 Assignors and Assignees ............................................................................................................................... 53 Assignable Coverage ..................................................................................................................................... 54
Rights over which Assignor Loses Control ............................................................................ 54 Designate and Change Beneficiaries and Contingent Beneficiaries .............................................................. 54 Elect or Revise an Optional Mode of Settlement for the Assigned Coverage ................................................ 55 Convert the Assigned Coverage to an Individual Policy................................................................................. 55 Make Any Application or Election with Respect to the Assigned Coverage ................................................... 55 Receive Any Increase in the Amount of Insurance ........................................................................................ 55 Make Required Employee Contributions ........................................................................................................ 55 Reassign the Coverage ................................................................................................................................. 56
Processing the Request ........................................................................................................ 57 Procedures Following the Assignment .................................................................................. 61
Beneficiary Designation by the Assignee ....................................................................................................... 61 Conversion ..................................................................................................................................................... 61 Portability ....................................................................................................................................................... 61 Death of the Assignee.................................................................................................................................... 61 Certificate Rider ............................................................................................................................................. 61
Additional Information ........................................................................................................... 62 Community Property Jurisdictions ................................................................................................................. 62 Valuation for Purposes of Federal Gift Taxation ............................................................................................ 62 Collateral Assignments .................................................................................................................................. 62 Partial Assignments ....................................................................................................................................... 62 Multiple Assignees ......................................................................................................................................... 62 Accelerated Benefits Option (ABO) ............................................................................................................... 63 Assignments Made to Minors ......................................................................................................................... 63 Multiple Beneficiaries for Assignments Only .................................................................................................. 63
Conversion Privilege ................................................................................................... 64 Overview ............................................................................................................................... 64
Coverage Ends Due To Termination ............................................................................................................. 64 Coverage Ends Due To Retirement ............................................................................................................... 64 Coverage Ends Due To Termination ............................................................................................................. 64
Application Period for Life Conversion .................................................................................. 64 Termination of Life Insurance ........................................................................................................................ 64 Reduction of Life Insurance ........................................................................................................................... 65
Annual Census Request ............................................................................................. 67
Additional Services ..................................................................................................... 68 Preferred Dentist Program .................................................................................................... 68
Finding a Network Dentist .............................................................................................................................. 68 Nominating a Dentist to Join the Network ...................................................................................................... 68 Other Issues Regarding Network Dentists ..................................................................................................... 68
WillsCenter.com .................................................................................................................... 68 Reports ......................................................................................................................... 70
Eligibility Listing (1-line edit report) ....................................................................................... 70 Forms ........................................................................................................................... 71

Introduction
Employer Administration Manual 01/09/13 1
The Employer Administration Manual (EAM) is a reference tool developed to help your benefits department facilitate the administration of benefits. For insured benefits, the Group Insurance Policy, including all Certificates and other exhibits, and any Participation Agreement, if applicable, is the governing document. Legal requirements and terms and conditions of the governing document control in the event of any conflict with the EAM. Please note that all information contained in this document is proprietary to MetLife and should not be disclosed to third parties without the prior, written consent of MetLife. All information is subject to change without notice; however, MetLife will make an effort to provide advance notice where appropriate. This document illustrates guidelines for common administrative functions, including enrollment, billing and claims processing. The EAM also contains a detailed MetLife contact list and descriptions and samples of forms needed to administer your Group Benefits. The guidelines include example sections of each required form. Please note that these example sections are from MetLife’s standard forms. Your actual form may vary based on the state in which the Group Policy was issued or the Employee’s state of residence. Refer to Forms for actual samples of your applicable forms. If you have any questions regarding this document, contact your Account Specialist found in Contacts.

Contacts
Employer Administration Manual 01/09/13 2
Customer Service Center Contacts
Benefit Representative Use Only Roles and Responsibilities Contact
Management of day-to-day administration of benefit program
Customer problem resolution Billing issues Contract and renewal preparation Supplies (forms, billing invoices and
mailing envelopes)
Escalation of issues not resolved by MetLife contacts listed below
Mymetteam_se1 Dedicated Service Team MetLife Customer Service Center PO Box 2523 Aurora, IL 60507 Overnight carrier deliveries must be sent to 177 S. Commons Drive Aurora, IL 60504 Tel 1-800-708-5652 Ext. 3625 Fax 1-630-978-5897 Email [email protected]
Escalation of issues not resolved by Account Specialist
Regina Prochaska Southeast Manager MetLife Customer Service Center PO Box 2523 Aurora, IL 60507 Overnight carrier deliveries must be sent to 177 S. Commons Drive Aurora, IL 60504 Tel 1-800-708-5652 Ext. 7567 Fax 1-630-978-5873 Email [email protected]
• Renewal presentation to Customer and Broker
Assist Customer and Broker with products
Plan revisions
Jamie Madden Accopunt Executive MetLife 604 Green Valley Road #408 Greensboro, NC 27408 Tel 1-336-292-8551 Fax 1-336-294-2134 Email [email protected]

Contacts
Employer Administration Manual 01/09/13 3
In partnership with Account Executive (or Client Executive if applicable), serves as a local resource for customer and broker
Supports Account Executive and Account Manager to resolve escalated issues
Consultative partner for plan changes, product recommendations, and renewal planning
Participation and assistance in coordinating benefit fairs and enrollment meetings
Life Contacts
Employee Use Roles and Responsibilities Contact
• Employee inquiries Group Life Claims 1-800-638-6420
Benefit Representative and Employee Use Roles and Responsibilities Contact
Status of submitted, paid, or denied claim
Claim-specific claim interpretation Beneficiary designation verification
for a submitted claim Processing time
Metropolitan Life Insurance Company Group Life Claims PO Box 6100 Scranton, PA 18505-6100
Overnight carrier deliveries must be sent to Metropolitan Life Insurance Company Group Life Claims - 4th Floor 123 Wyoming Avenue Scranton, PA 18503 Tel 1-800-638-6420 Fax 570-558-8645
• Life conversions • Additional services available through
Financial Services Representatives
MetLife Advice Resource Center Tel 1-877-ASK-MET7 (1-877-275-6387) Fax 1-888-422-4272 Email [email protected]
Contacts
Employer Administration Manual 01/09/13 4
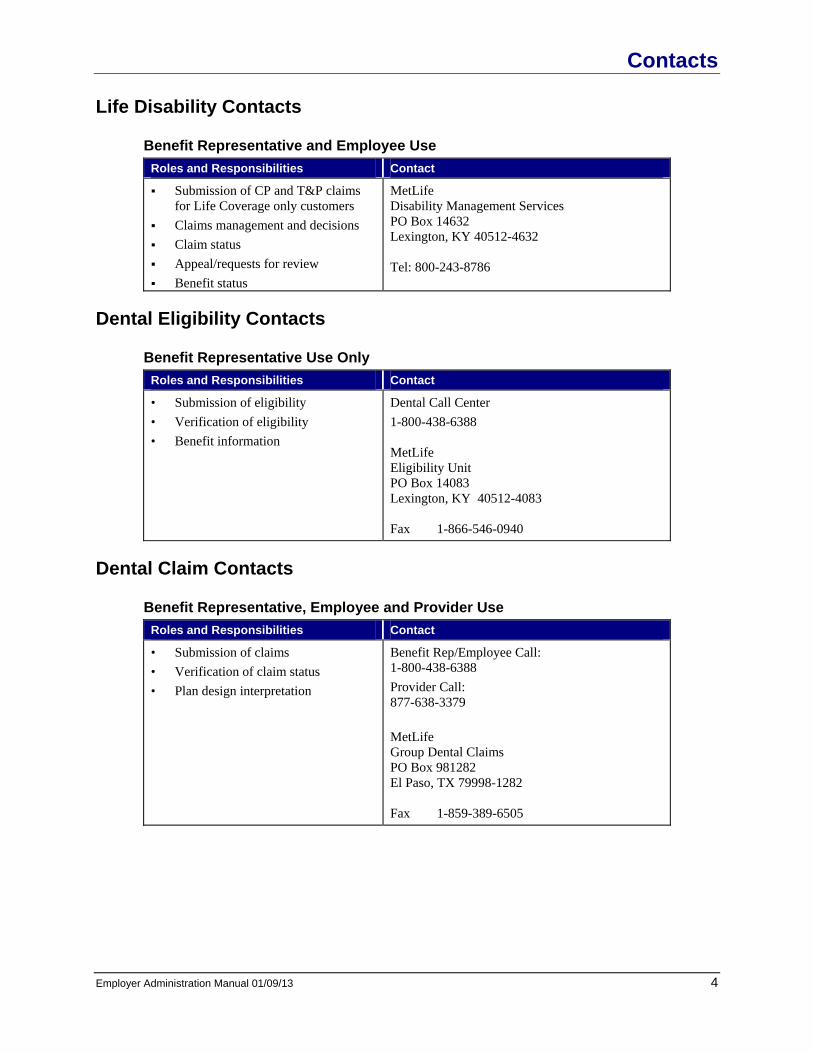
Life Disability Contacts
Benefit Representative and Employee Use Roles and Responsibilities Contact
Submission of CP and T&P claims for Life Coverage only customers
Claims management and decisions Claim status Appeal/requests for review Benefit status
MetLife Disability Management Services PO Box 14632 Lexington, KY 40512-4632 Tel: 800-243-8786
Dental Eligibility Contacts
Benefit Representative Use Only Roles and Responsibilities Contact
• Submission of eligibility • Verification of eligibility • Benefit information
Dental Call Center 1-800-438-6388 MetLife Eligibility Unit PO Box 14083 Lexington, KY 40512-4083 Fax 1-866-546-0940
Dental Claim Contacts
Benefit Representative, Employee and Provider Use Roles and Responsibilities Contact
• Submission of claims • Verification of claim status • Plan design interpretation
Benefit Rep/Employee Call: 1-800-438-6388 Provider Call: 877-638-3379 MetLife Group Dental Claims PO Box 981282 El Paso, TX 79998-1282 Fax 1-859-389-6505

Contacts
Employer Administration Manual 01/09/13 5
Benefit Representative Use Only Roles and Responsibilities Contact
• Directory requests • Locating dentists within the Network • Status of Claim • Status of benefit payment
Dental Customer Service Center 1-888-466-8673
Please note that Personal Health Information may not be shared if the appropriate documentation has not been received by MetLife.
Additional Services Contacts
Benefit Representative and Employee Use Roles and Responsibilities Contact
• Locate a dentist within the Network • Nominate a dentist for the Network
Preferred Dentist Program Tel 1-800-438-6388
Benefit Representative Only Use Roles and Responsibilities Contact
Change in employment planning Retirement planning Financial education Survivor assistance
MetLife Advice Relationship Manager Breanna Tucker Tel: 918-252-8572 Fax: 918-252-8066 Email: [email protected]
• Locate a dentist within the Network • Nominate a dentist for the Network
Preferred Dentist Program Tel 1-800-942-0854

Reporting Structure
Employer Administration Manual 01/09/13 6
Claims Structure Structure - Number - Description
Customer - 113178 - McDowell County Schools
Experience - 113178 - NON-RETRO EXPERIENCE RATED
Group/Report - 113178 - McDowell County Schools
Sub Code/Subdivision - 0001 - ALL EMPLOYEES
Branch - 0001 - ALL EMPLOYEES
Branch - 0002 - ALL COVERED SERVICES
Branch - 0003 - ALL COV SER EXCL SER W/ 12 MONTH WP
Branch - 0004 - ALL COV SER EXCL SER W/ 6 AND 12 MONTH WP
Billing Branches Billing Branch Description
000001 BASIC LIFE All EMPLOYEES
000002 All Employees
000003 All Employees Dental Inurance
CA9999 Cash Branch Insured

Enrollment Procedures
Employer Administration Manual 01/09/13 7
Eligibility Eligibility requirements and effective dates may vary by group and/or type of coverage.
Actively at Work Requirements Actively at work requirements may vary by group and/or type of coverage. Generally, if the Employee is not actively at work on the day coverage would otherwise become effective because of layoff, leave of absence or disability, the coverage becomes effective on the date that the Employee returns to active work. Generally, if the effective date of coverage falls on a day on which the Employee is not scheduled to work or during the Employee's vacation period or weekend, the Employee shall be considered to be actively at work, provided the Employee worked on the last scheduled work day or the day immediately preceding the vacation period.
Deferred Effective Date for Disabled Dependents If a Dependent is disabled as of the effective date of coverage, coverage for that Dependent will not be made effective until the Dependent is no longer disabled and provides satisfactory evidence of good health to MetLife. If a Dependent is confined in a hospital on the effective date of coverage, coverage for that Dependent will not be made effective until the Dependent is no longer hospital confined and provides satisfactory evidence of good health to MetLife.
Handicapped Dependent Children Coverage for Dependent children may be continued beyond the limiting age, as defined in the applicable Certificate, provided the child is physically or mentally incapable of self-sustaining employment on the date the child reaches the limiting age. To continue coverage, all of the following requirements must be met: The child was covered prior to the limiting age The child became handicapped and incapable of self sustaining employment prior to the limiting age
defined in the applicable Certificate The child continues to qualify as a Dependent The child is chiefly dependent upon the Employee for support and maintenance
Guidelines for Continuing Coverage for Handicapped Dependent Children Step Responsibility Description
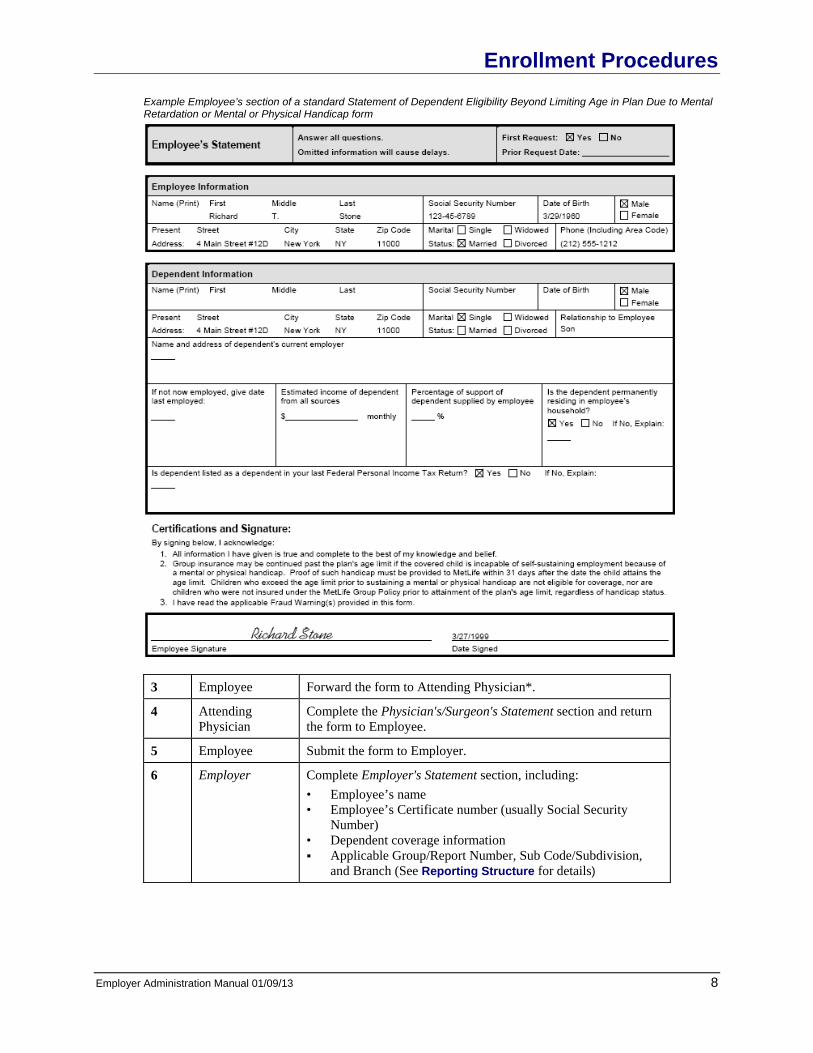
1 Employer Instruct Employee to complete the form, Statement of Dependent Eligibility Beyond Limiting Age in Plan Due to Mental Retardation or Mental or Physical Handicap. See Forms for an unmarked sample.
2 Employee Complete Employee's Statement section, including: Personal information on Employee Personal information on Dependent Dependent's employment and income information
Enrollment Procedures
Employer Administration Manual 01/09/13 8
Example Employee’s section of a standard Statement of Dependent Eligibility Beyond Limiting Age in Plan Due to Mental Retardation or Mental or Physical Handicap form
3 Employee Forward the form to Attending Physician*.
4 Attending Physician
Complete the Physician's/Surgeon's Statement section and return the form to Employee.
5 Employee Submit the form to Employer.
6 Employer Complete Employer's Statement section, including: • Employee’s name • Employee’s Certificate number (usually Social Security
Number) • Dependent coverage information Applicable Group/Report Number, Sub Code/Subdivision,
and Branch (See Reporting Structure for details)

Enrollment Procedures
Employer Administration Manual 01/09/13 9
Example Employer’s section of a standard Statement of Dependent Eligibility Beyond Limiting Age in Plan Due to Mental Retardation or Mental or Physical Handicap form
7 Employer Submit the completed form to your Account Specialist (Retain a copy for your records).
Mail to:
MetLife Customer Service Center PO Box 2523 Aurora, IL 60507
8 MetLife Notify Employer if child is approved or declined for continued coverage. NOTE: Additional information may be needed before a decision
can be made. Please follow the instructions you receive with the request.
9 Employer Notify Employee if child is approved or declined for continued coverage.
*Attending Physician may also mean Examination Management Services, Inc. (EMSI).
If the child is approved for coverage MetLife will inform the Employer how long coverage will continue. Two months before the end of this period, a new form must be completed that indicates the child's then existing condition and prognosis.
Common-Law Spouses as Dependents A common-law spouse is eligible for coverage as a Dependent, provided a Common-Law Marriage Questionnaire form is received and approved by the Employer. Dependent eligibility as a common-law spouse is based on the following requirements. Generally, a common-law marriage must have been entered into: ♦ In good faith ♦ With the mutual consent of both parties ♦ With a present intent to be married ♦ As a permanent union of the two consenting parties ♦ With both parties having the capacity to marry, that is:
♦ Neither party is married to someone else ♦ Both are of legal age and mental capacity ♦ The parties are not too closely related by blood
In addition, the parties must:

Enrollment Procedures
Employer Administration Manual 01/09/13 10
Live together Hold themselves out to the world as husband and wife
When Dependent coverage for a common-law spouse is requested, the couple must complete and sign a Common-Law Marriage Questionnaire form and submit it to the Employer with the Enrollment Form. The laws on common-law marriage vary from state to state. As of January 9, 2013, a common-law marriage may be entered into in the following states: Alabama Colorado District of Columbia Florida (before 1/1/1968) Georgia (before 1/1/1997) Idaho Indiana (before 1/1/1958) Iowa Kansas Michigan (before 1/1/1957) Mississippi (before 4/5/1956) Montana Nevada (before 3/29/1943) Ohio (before 10/10/1991) Oklahoma Pennsylvania Rhode Island South Carolina South Dakota (before 7/1/1959) Texas Utah
Guidelines for Determining Common-Law Spouse Eligibility Step Responsibility Description
1 Employer Instruct Employee to complete the form, Common-Law Marriage Questionnaire. See Forms for an unmarked sample.
2 Employee and Common-Law Spouse
Complete the form including: Personal information on Employee Personal information on common-law spouse Signatures of Employee and common-law spouse

Enrollment Procedures
Employer Administration Manual 01/09/13 11
Example Employee’s section of a standard Common Law Marriage Questionnaire
3 Employee Submit the completed form to Employer along with required documentation of death, divorce or annulment for each of the parties’ previous marriage(s) if applicable.

Enrollment Procedures
Employer Administration Manual 01/09/13 12
4 Employer Determine eligibility for Dependent group coverage based on the responses to the Common-Law Marriage Questionnaire form. Coverage is available if: Response to item 11 and/or item 12 is a jurisdiction in which
a common-law marriage may be entered Response to items 5 and 9 indicate that both parties were
single at the time the common-law marriage commenced Coverage should be denied if: Response to neither item 11 nor item 12 is one of the
jurisdictions in which a common-law marriage may be entered
Response to items 5 and 9 establish that Employee or purported common-law spouse was married to someone else at the time the common-law marriage began
NOTE: If coverage is denied, Employer should mail the denial letter to Employee.
Example Common-Law Marriage Denial Letter
Dear [Employee Name]: We have reviewed the Common-Law Marriage Questionnaire that was signed and dated by you on ________. Based on your responses to the questionnaire, [it does not appear that you have resided in a state which Common-Law Marriage may be entered into] [and/or] [it appears that you or your purported Common-Law spouse were married to someone else on _____, the date you have indicated your Common-Law Marriage began]. Therefore, we regret to advise you that we are unable to provide you with the dependent group coverage you requested. If you have any questions regarding this matter, please contact your benefits administrator. Sincerely [Employer’s Name] [Date]
5 Employer If Dependent spouse coverage is approved, maintain the form on
file.

Enrollment Procedures
Employer Administration Manual 01/09/13 13
New Enrollments An Employee who is electing, changing or declining coverage for which they are eligible must complete a MetLife Enrollment Form. If an Enrollment Form was completed under a prior carrier, that form is acceptable to MetLife. However, a MetLife Enrollment Form must be used for any new enrollments or changes in coverage on or after the effective date of the applicable MetLife Certificate.
Guidelines for Enrolling Employees Step Responsibility Description
1 Employer Verify that: Employee is eligible Enrollment request is not late (See Late Enrollments in this
section for details)
2 Employer Complete the To Be Completed By The Employer section of the Enrollment Form, including: Group name Applicable Group/Report Number, Sub Code/Subdivision,
and Branch (See Reporting Structure for details) Effective date of coverage Employee job and salary information Reason for Enrollment
Signature of Employer See Forms for an unmarked sample.
Example Employer’s section of a standard Life Enrollment Form
Example Employer’s section of a standard Dental Enrollment Form

Enrollment Procedures
Employer Administration Manual 01/09/13 14
3 Employer Instruct Employee to complete the form.
4 Employee Complete the form, including: Personal information on Employee Request for coverage
Beneficiary designation (See Beneficiary Designation in this section for details)
Sign as appropriate
Example Employee’s section of a standard Life Enrollment Form
Example Employee’s section of a standard Dental Enrollment Form

Enrollment Procedures
Employer Administration Manual 01/09/13 15
5 Employee Retain a copy of the form and the Consumer Privacy Notice for
his or her records.
6 Employee Return the completed form to Employer.
7 Employer Review the form to ensure the following: No missing data Form is authorized (signed and dated) by Employee (and
Dependent if applicable) Beneficiary designation meets all necessary guidelines (See
Beneficiary Designation in this section for details) 8 Employer Notify Employee of confirmation or denial of enrollment for
benefits.
9 Employer File the form with the Employee's records.

Enrollment Procedures
Employer Administration Manual 01/09/13 16
Late Enrollments A late enrollment occurs when an Employee: Has chosen not to enroll himself or herself and/or his or her Dependent(s) for coverage within 31 days of the
eligibility date (See the applicable Certificate for more details) and decides to do so when offered at a later date Reapplies after termination of coverage at the Employee's request Applies for reinstatement upon returning to work after termination of employment, lay-off or leave of absence
and after converting his or her Life Benefits to an individual policy Applies for coverage and was previously eligible for coverage under the prior insurance carrier but did not
enroll
Waiting Period With regard to Dental coverage, a waiting period may be required for late enrollments. See the applicable Certificate for details.

Enrollment Procedures
Employer Administration Manual 01/09/13 17
Processing Coverage Changes This section explains how to process changes in name and Dependent coverage. It also describes processing of cancellation of coverage requested by an Employee, termination of employment, temporary layoff or leave of absence, disability or retirement, and death of an Employee.
Change in Dependent Coverage An Employee may add Dependent coverage without providing proof of good health as long as the request is made within 31 days of one of the following events: Marriage Becoming a parent or legal guardian of a child Loss of spouse's job
If the request is not made within 31 days, the enrollment is considered late. See Late Enrollments in this section for details. Dependent coverage may cancel for any the following reasons: Divorce (There may be exceptions in some states) Death of a Dependent Dependent marries or reaches the limiting age (See the applicable Certificate)
Cancellation of Coverage Requested by an Employee Coverage which requires an Employee contribution will cancel when payments for benefits cease to be made (See the applicable Certificate for details). The Employer must enter the date that benefits end, followed by “Cancelled by Request” on the Employee's Enrollment form next to those coverages being cancelled. If appropriate, indicate the cancellation of coverage on the eligibility data sent to MetLife. The Employer must notify the Employee that restrictions will be imposed if the Employee wishes to rescind the cancellation.
Termination of Employment If Life coverage ends because of termination of employment, terminating Employees must be provided with a conversion notice. The notice describes the Employee's right to convert to an individual policy. States generally require that notification of the right to convert be provided within a specified number of days of the Employee's termination. See Conversion Privilege for details.
Continuation of Group Life Coverage for Minnesota Residents Minnesota law continues coverage for terminated and laid-off Employees for up to 18 months. The law pertains to customers sitused in Minnesota and those sitused outside of Minnesota unless all criteria set forth below are met. The law states: Voluntarily or involuntarily terminated or laid off Employees may continue Group Life coverage for
up to 18 months or the Employee obtains coverage under another Group Life Policy, whichever comes first. An Employee is considered laid off if there is a reduction of hours so that the Employee is no longer eligible for coverage under the Group Life Policy. Continuation of coverage is not extended to Employees discharged for gross misconduct.
The Employer must send a notice by first class mail to the Employee's last known address. The Employee has 60 days to elect continuation of coverage. The 60-day period runs from the later of
the date coverage would otherwise terminate or the date the Employee receives notice of the right to continue coverage.

Enrollment Procedures
Employer Administration Manual 01/09/13 18
If the Employer fails to notify an eligible Employee of the right to continue coverage or fails to remit payment for the continued coverage to the insurer on behalf of the Employee after receipt of the premium from the Employee, the Employer is liable for the Employee's coverage.
The Employee must pay the Employer the cost of the continued coverage. The premium charged to the Employee may not exceed 102 percent of the cost to the Plan.
At the end of the continuation period, an Employee, surviving spouse or Dependent covered under the Plan is entitled to convert the group coverage to an individual policy.
This law does not apply to certificates under a master policy issued outside of Minnesota if all the following criteria are met: The policyholder or certificateholder is not a Minnesota corporation. The policyholder or certificateholder does not have its principal office in Minnesota. The policy or certificate covers less than 25 Minnesota residents. The less than 25 residents must
represent less than 25 percent of all covered persons of the group. If the less than 25 Minnesota residents represent 25 percent or more of the group, the customer is not exempt.
Temporary Layoff or Leave of Absence, Disability, or Retirement Refer to the applicable Certificate for applicable rules. When coverage terminates, enter the date of cancellation on the Employee's Enrollment form.
Death of an Employee All of the deceased Employee's coverages must be cancelled. Enter on the Employee's Enrollment form the date of death, followed by the word "Died." See Guidelines for Processing Claims for instructions on filing death claims.

Enrollment Procedures
Employer Administration Manual 01/09/13 19
Beneficiary Designation This section defines Beneficiary, describes common wording used for beneficiary designations, outlines state laws that affect beneficiary designations and offers guidelines for designating or changing a Beneficiary. This section also describes how payments are made to the Beneficiary.
Choosing a Beneficiary The Beneficiary is the person(s) or trust that is designated to receive the Life Benefits upon the death of the Insured.
Examples of Common Beneficiary Designations The following table, Common Beneficiary Designations, shows examples of common beneficiary designations. Note that each example includes the name of the Beneficiary and his or her relationship to the Insured. If there is more than one Beneficiary, the wording specifies the proportionate distribution. To facilitate claim processing, designations should include the beneficiary’s name, address, date of birth, relationship to the insured, and percentage. A beneficiary’s Social Security number is helpful, but not required.
Common Beneficiary Designations Type of Beneficiary Example
Insured's Estate Estate
One Beneficiary Jane Doe, relationship: spouse
Two Beneficiaries in equal shares Peter Doe: relationship: parent, and Ann Doe, relationship: parent, in equal shares
Two Beneficiaries in unequal shares 75% to Peter Doe, relationship: parent, and 25% to Ann Doe, relationship: mother
One primary and one contingent Beneficiary
Primary Beneficiary: Jane Doe, relationship: spouse
Contingent Beneficiary: Thomas Doe, relationship: child
Charity The University of Chicago Capital Fund. Include address of development office
Trust A.B.C. Trust Company of Chicago, Illinois
Michael W. Jones Trustee, under Trust Agreement dated (insert date). Include TIN and contact information for trustee
Impermissible Designations The Employee may not designate the following as a Beneficiary: His or her Employer A guardian for minors An individual in the capacity of administrator of his or her estate A funeral home, if the Employee resides in any of the following states: Georgia, Illinois, Michigan,
New York, South Dakota, or Tennessee. If the Employee resides outside these states, a funeral home may be named a beneficiary.

Enrollment Procedures
Employer Administration Manual 01/09/13 20
Designations to Avoid The Employee should not name an organization or endowment unless it is a legal entity (i.e., has a legal existence as a corporation, trust or other entity).
Designating or Changing a Beneficiary A new Employee should name his or her Beneficiary(ies) on the Enrollment Form when he or she enrolls for Life Benefits. If an Enrollment Form is not necessary, a Beneficiary Designation form should be completed and kept with the Employee’s files. The process used for the initial designation of a Beneficiary is the same as that used for changes to that designation.
Guidelines for Designating or Changing a Beneficiary Step Responsibility Description
1 Employer Instruct Employee to complete the appropriate Beneficiary Designation form. See Forms for unmarked samples.
2 Employee Complete the Beneficiary Designation form in duplicate, including: Group Policy Number Employee’s Social Security Number Primary Beneficiary designation and personal information, if
applicable Contingent Beneficiary designation and personal information,
if applicable Trustee designation, including title of the agreement and date
it was executed, if applicable Personal information on Employee (or owner if assigned) Signature of Employee (or owner if assigned)

Enrollment Procedures
Employer Administration Manual 01/09/13 21
Example Employee’s section of a standard Beneficiary Designation form
3 Employee Return the form to Employer.
4 Employer Verify the following: Form is signed and dated by Employee Designation is legible (If not legible, ask Employee to
complete a new form) Beneficiary’s name is listed in full Beneficiary’s relationship to Employee is listed. If not related
to Employee, the relationship shown should be “non-relative”
No erasures or use of other correction methods
5 Employer Return one copy to Employee to attach to his or her Certificate.
6 Employer File the other copy with the Employee’s records.

Enrollment Procedures
Employer Administration Manual 01/09/13 22
Allocation of Payment Payment will be made to the Beneficiary as indicated on the Enrollment and/or Beneficiary Designation form with the following exceptions:
If the Designated Beneficiary Is Payment Will Be Made To
Estate of Insured Administrator or executor of deceased's estate
A minor TCA or court appointed Guardian of Person and Property of the minor's Estate
An incompetent Beneficiary Guardian or other appointed representation of incompetent Beneficiary
In these situations, court appointments are generally necessary. A court certificate showing the appointment should be submitted. However, the submission of proof of death should not be delayed. If any material is omitted, give the full facts for the omission.

Sending Enrollment Data to MetLife
Employer Administration Manual 01/09/13 23
MetLife's Unified Inforce System (UIS or Inforce) maintains complete records on your Employees' and their Dependents' eligibility status for certain coverages provided under your Plan. MetLife uses these records to determine eligibility for your Benefit Plan when Employees submit their claims for payment. For that reason, it is critical that you send enrollment information to MetLife as quickly as possible. MetLife provides you with options for sending enrollment data so that updates reflect the most recent information.
Updating through MetLink® MetLink® is a web-based system that allows you to update enrollment changes through a secure Internet connection. For more information, contact your Account Specialist.

Billing
Employer Administration Manual 01/09/13 24
Self Billing through MetLink® Electronic self billing through MetLink® features: Online, real-time access to all billing and payment information over a secure Internet connection Recordkeeping structure and reporting format that can eliminate the need for separate spreadsheets Central reporting location for consolidating data from satellite or remote offices Electronic history of billing that helps in budget planning and forecasting

Billing
Employer Administration Manual 01/09/13 25
The following benefit and premium calculation examples are based on some of MetLife’s standard plan designs. If your company’s plan design is not noted below, please contact your Account Manager for instructions on calculating benefit and premium amounts.
Basic Life and AD&D Life Insurance rates for Basic Life are generally based on each $1,000 of benefit. Premiums are paid to MetLife based on the volume of coverage for all employees.
Flat Benefit Amount Every employee receives the same benefit amount, subject to the age reduction schedule. Example: All Employees receive a flat $20,000.
Multiple of Salary Benefit Amount Employees receive different life insurance benefit amounts depending on their annual salary. For example, if the plan is 2 X salary, each employee’s benefit would equal 2 times his salary, usually rounded to the next higher or nearest $1,000.
Salary Class Benefit Amount Employees receive different life insurance benefit amounts determined by their salary class. For example, all hourly employees are eligible for a flat benefit of $20,000 while all salaried employees are eligible for a multiple of salary benefit of 2 X salary to a maximum of $250,000.
To calculate you need to know:
− The definition of each salary class (e.g. class 1 = clerical, class 2 = assembly line, etc. or class 1 = hourly, class 2 = salaried)
− The flat insurance benefit amount or the salary multiplier for each salary class − The salary class of the employee ♦ The example below shows the ABC Company who has a “Salary Multiple Benefit Amount” in the amount of
2X salary. The benefit is subject to a maximum benefit of $250,000 and the reduction schedule states benefits reduce to 35% at age 65 and 50% at age 70 (reduced amounts are based on the benefit at the time.) Benefits are rounded to the next higher $1,000.
Date Of
Birth Annual Salary
Basic Life/AD&D
Benefit
Calculation
1/1/55 $54,400 $109,000 $54,400 x 2 = $108,800 12/1/62 $45,000 $90,000 $45,000 x 2 = $90,000 8/5/65 $200,000 $250,000 $200,000 x 2 = $400,000 however, as this exceeds the
maximum, benefit is reduced to $250,000 3/17/30 $100,000 $100,000 $100,000 x 2 = $200,000 however, as employee is
age 71, benefit is reduced by 50% of original benefit of $100,000
7/1/56 $75,230 $151,000 $75,230 x 2 = $150,460 $700,000 The total amount of Basic Life and AD&D.
The bill line for the above example would look as follows: Experience
Number Billing Branch
Billing Coverage and Description
Ins Co Use Only
No. of Lives Insurance / Benefit
Rate Per
Premium per coverage
0101011 000001 Basic Life P01 00 5 700,000 $0.12/$1,000 $84.00

Billing
Employer Administration Manual 01/09/13 26
Optional Life Life Insurance rates for Optional Life are generally based on each $1,000 of benefit. Premiums are paid to MetLife based on the volume of coverage for all employees. Optional Life is standardly sold with step rates, allowing different rates for defined age groups. The age groups are typically 5 years (example: 30 – 34), and usually start with the first age group being participants less than 30.
Incremental Benefit Amount Employees can choose coverage in increments. For example, a plan could be increments of $10,000 to a maximum of $200,000. Employees can choose any increment of $10,000 up to the maximum.
Multiple of Salary Benefit Amount Employees receive different life insurance benefit amounts depending on their annual salary. For example, most multiple of salary plans will offer a 1 – 3, 4, or 5 times salary option up to a defined maximum. Employees can choose the level of coverage that they want. Example: The ABC Company’s schedule is in increments of $10,000 to a maximum of $500,000 and the plan is step-rated. The bill would appear as follows: Experience
Number Billing Branch
Billing Coverage and Description
Ins Co Use Only
No. of Lives Insurance / Benefit
Rate Per
Premium per coverage
0101011 000001 Optl <30 P02 00 6 120,000 $0.05/$1,000 $6.00 Optl 30 – 34 P02 01 1 20,000 $0.07/$1,000 $1.40 Optl 35 – 39 P02 02 3 230,000 $0.09/$1,000 $20.70 Optl 40 – 44 P02 03 $0.12/$1,000 Optl 45 – 49 P02 04 6 170,000 $0.17/$1,000 $28.90 Optl 50 – 54 P02 05 2 90,000 $0.23/$1,000 $20.70 Total $77.70

Billing
Employer Administration Manual 01/09/13 27
Dependent Life Dependent Life plans can vary. Some employers may offer an employer paid benefit in which the spouse receives a flat $10,000 and each child receives $5,000. Many employee paid plans will offer the spouse increments of $10,000 to choose from to a defined maximum while the child coverage may be increments of $2,000 to a maximum amount, or even a flat benefit of $10,000. Dependent Life calculations can vary as well. Dependent Life can be calculated on a step rate basis (for spouses only), on a per employee basis (spouse or children), or on a per $1,000 basis (spouse or children). Child rates typically are on a per employee basis and the employee pays one rate regardless of the number of children covered. For example, if the per employee rate is $1.25 and the employee has 5 children, the employee will still only pay $1.25. Example: The ABC company has both an employer paid and an employee paid Dependent Life plan. The employer paid plan offers $10,000 per spouse and $2,000 per child on a per employee basis. The employee paid plan offers spouses increments of $10,000 to a $100,000 maximum on a per $1,000 basis and a flat $10,000 per child on a per employee basis. Experience
Number Billing Branch
Billing Coverage and Description
Ins Co Use Only
No. of Lives Insurance / Benefit
Rate Per
Premium per coverage
0101011 000001 Depl – ER Paid B02 00 230 $2.80/EE $644.00 Depl – Spouse B02 01 123 3,460.000 $0.08/$1,000 $276.80 Depl – Child B02 02 155 $1.75/EE $271.25 Total $1192.05

Billing
Employer Administration Manual 01/09/13 28
Dental Typically, the premium for Dental coverage is calculated on a “per employee” basis. This simply means that for each tier of coverage (Employee Only, Employee +1, Family, etc.), a count is made of the number of employees that fall into each of those tiers. The exception to this would be for a self-funded or ASO Dental group. These groups usually have a premium which is calculated on a per employee only basis. It does not matter how many employees have single or family or dependent coverage. A count would be taken of all employees that have dental coverage, regardless of the dependent coverage they may have, and that number is multiplied by the ASO fee that has been assigned to this customer. In the 3-tier example below, 155 employees have chosen coverage for themselves only, 79 have chosen coverage for themselves plus one dependent (spouse or child), and 129 have chosen family coverage.
3 Tier Coverage Experience
Number Billing Branch
Billing Coverage and Description
Ins Co Use Only
No. of Lives Insurance / Benefit
Rate Per
Premium per coverage
0101011 000001 Dental – EE Only P01 00 155 $19.93/EE $3,089.150101011 000001 Dental – EE + 1 P02 00 79 $41.46/EE $3,275.340101011 000001 Dental – Family P03 00 129 $63.13/EE $8,143.77 In the following 2-tier example, 265 employees have chosen coverage for themselves only and 192 employees have chosen family coverage
2 Tier Coverage Experience
Number Billing Branch
Billing Coverage and Description
Ins Co Use Only
No. of Lives Insurance / Benefit
Rate Per
Premium per coverage
0101011 000001 Dental – EE Only P01 00 265 $21.25/EE $5,631.250101011 000001 Dental – Family P02 00 192 $59.02/EE $11,331.84

Billing
Employer Administration Manual 01/09/13 29
Late Payments Payments are due on the first of each month. If MetLife does not receive payment within the contractual grace period, customized lapse letters and account balance summaries generate automatically. The following chart details the sequence of lapse letters and under which circumstance they are sent:
Letter Premium not received by
Reminder Letter The end of Grace Period
Warning Letter 30 days after the end of Grace Period
Cancellation Letter 60 days after the end of Grace Period
Results of Late Premium and Invoices If MetLife receives your premium payment more than 60 days after the due date, the premiums paid appear in the month they were received for reporting purposes. MetLife applies monies received to the oldest due and unpaid balance. If MetLife receives your invoice more than 60 days after the due date, a system generated estimate is entered until an actual invoice has been received and processed. Any difference between the system generated estimate and the actual bill will be reflected in the current month. This will affect year-end financial reports.
Cancelled Coverage If payment has not been received within 90 days of the due date, cancellation of coverage under a Group Insurance Policy will occur. Since MetLife is responsible for processing claims incurred prior to the cancellation date, you are responsible for premium payments until the cancellation date. Additional amounts may become payable based upon other contractual terms or arrangements. If Employees contribute to the cost of this insurance and you continue to collect contributions beyond the date of cancellation, you may become liable for the benefits.
Reinstatement Rules Reinstatement may occur without a gap in coverage once within a 12-month period. MetLife considers reinstatement only if you pay the premium due by the end of the reinstatement period. MetLife may hold claims incurred after the cancellation date until the reinstatement period is over. If MetLife reinstates you, the claims will be processed.
Rehire Rules If a former employee is rehired within 6 months, MetLife will bring them back at the same amount of coverage, without medical evidence of insurability (MEOI), even if it exceeds the guarantee issue (GI) amount. Still within the 6 months they may apply for additional coverage but they must provide MEOI. After 6 months a rehire would be treated as a New Hire and follow the guidelines under the New Enrollment section. These individuals would have to provide MEOI for any coverage in excess of the GI amount.

Billing
Employer Administration Manual 01/09/13 30
Lockboxes Lockbox Check Conversion is the changing of a paper check into an electronic check. The check becomes an Electronic Funds Transfer (EFT) and is processed through the Automated Clearing House (ACH). The ACH is the federally regulated electronic payment network used by 95% of US financial institutions. MetLife uses Lockbox Check Conversion to electronically convert a check received at the lock box (point of receipt) and to process the payment through the Automated Clearing House (ACH) network. In an effort to receive payment from customers as quickly as possible, lockboxes are located close to where payment is originated. Setting up our lockboxes with one bank (Mellon), near the point of origination, and funneling payment to one Demand Deposit Account (DDA) reduces the mail float time. MetLife currently has six lockboxes: two each in Los Angeles, CA; Chicago, IL; and Pittsburgh, PA. There are two lockboxes, designated “A” and “B,” in each of the three cities listed above. • Customers using our standard invoices will remit invoices and payments to the “A” lockbox. • Customers using non-standard invoices will remit their invoices and payments to the “B” lockbox. Mellon Bank will process the “A” lockbox invoices while the Remittance Processing Center in Tampa will process the “B” lockbox invoices.
Lockbox Addresses
Type “A” Type “B” Los Angeles (LA): Los Angeles (LB): Dept LA21296 Dept LA21203 Pasadena, CA 91185-1296 Pasadena, CA 91185-1203 Chicago (CA): Chicago (CB): Dept CH10579 Dept CH10261 Palatine, IL 60055-0579 Palatine, IL 60055-0261 Pittsburgh (PA): Pittsburgh (PB): P.O. Box 360229 P.O. Box 360905 Pittsburgh, PA 15251-6229 Pittsburgh, PA 15251-6905
FedEx Lockbox Mellon Financial Services Dept. CH10579 5505 North Cumberland, Suite 301 Chicago, IL 60656 Phone: 773-763-5631
All FedEx should go to the Chicago address above…regardless of point of origination.

Billing
Employer Administration Manual 01/09/13 31
Lockbox Assignments by State/Region Lockbox addresses are assigned to a customer based on from where payment is coming --not the situs location. • Find the state/region from which payment is being sent. The Lockbox city is the city to where payments should
be sent. Be sure to use the appropriate Lockbox Envelope.
State/Region Lockbox City State/Region Lockbox City Alabama ............. Chicago IL Montana ............... Los Angeles CA Alaska ................ Los Angeles CA Nebraska .............. Chicago IL American Samoa. Los Angeles CA Nevada ........... Los Angeles CA Arizona ............... Los Angeles CA New Hampshire .... Pittsburgh PA Arkansas ............ Chicago IL New Jersey .......... Pittsburgh PA California ............ Los Angeles CA New Mexico ......... Los Angeles CA Colorado ............ Los Angeles CA New York ............. Pittsburgh PA Connecticut ........ Pittsburgh PA North Carolina ...... Pittsburgh PA Cuba .................. Pittsburgh PA North Dakota ........ Chicago IL Delaware ............ Pittsburgh PA N. Mariana Island . Los Angeles CA Dist of Columbia.. Pittsburgh PA Ohio ..................... Chicago IL Florida ................ Pittsburgh PA Oklahoma ............ Los Angeles CA Georgia .............. Pittsburgh PA Oregon ................ Los Angeles CA Guam ................. Los Angeles CA Pennsylvania ....... Pittsburgh PA Hawaii ................ Los Angeles CA Philippine Islands . Los Angeles CA Idaho .................. Los Angeles CA Puerto Rico .......... Pittsburgh PA Illinois ................. Chicago IL Rhode Island ........ Pittsburgh PA Indiana ............... Chicago IL South Carolina Pittsburgh PA Iowa ................... Chicago IL South Dakota ....... Chicago IL Kansas ............... Chicago IL Tennessee ........... Pittsburgh PA Kentucky ............ Chicago IL Texas ................... Los Angeles CA Labrador ............. Los Angeles CA Utah ..................... Los Angeles CA Louisiana ............ Chicago IL Vermont ............... Pittsburgh PA Maine ................. Pittsburgh PA Virgin Islands ....... Pittsburgh PA Maryland ............ Pittsburgh PA Virginia ................ Pittsburgh PA Massachusetts ... Pittsburgh PA Washington .......... Los Angeles CA Michigan ............ Chicago IL West Virginia ...... Chicago IL Minnesota .......... Chicago IL Wisconsin ............ Chicago IL Mississippi ......... Pittsburgh PA Wyoming .............. Los Angeles CA Missouri ............. Chicago IL

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 32
Life Claims
Life Claims Insurance benefits are generally payable under a properly documented claim when: An Employee dies either while insured or within 31 days following termination of insurance due to
termination of employment A covered Dependent of an insured Employee dies while the insured Employee is active or within 31
days after insurance has been discontinued due to termination of employment
Step Responsibility Description
1 Employer When an Employee or a covered Dependent dies, verify the Employee’s or covered Dependent’s: Eligibility as defined in the applicable Certificate Participation in the applicable Plan
2 Employer Complete Employer's Statement section of the Life Insurance Claim Form including: Personal information on Employee.
If a Dependent claim, personal information on Dependent Applicable Group/Report Number, Sub Code/Subdivision and
Branch (See Reporting Structure for details) Amount(s) of Life Benefits and whether reduced by:
- A reduction formula - An Accelerated Benefits payment Last day worked
See Forms for an unmarked sample.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 33
Example Employer’s section of a standard Life Insurance Claim Form

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 34
Example Employer’s section of a standard Life Insurance Claim Form for a Dependent

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 35
Example Employer’s section of a standard Life Insurance Claim Form for a Trust

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 36
3 Employer Send the following to Beneficiary: • Claimant's Statement section of claim form • Important Message to Group Life Benefits Beneficiaries form,
if Employee had not elected a Mode of Settlement prior to his or her death
See Forms for an unmarked sample.
4 Beneficiary Complete: Claimant's Statement section, including:
- Personal information on Beneficiary - Personal information on Deceased
Important Message to Group Life Benefits Beneficiaries form (if applicable)

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 37
Example Beneficiary’s section of a standard Life Insurance Claim Form

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 38
5
5 Beneficiary Submit the following to Employer or MetLife: Completed Claimant's Statement
Certified copy of the Death Certificate bearing raised or colored seal indicating cause and manner of death (If death occurs in foreign country, the beneficiary/informant must request a Report of the Death of an American Citizen Abroad form from the US Consulate. This document is necessary to confirm the local magistrate's death certificate)
Completed Election of Mode of Settlement form (if applicable)
6 Employer Submit the following: • Completed claim form (Retain a copy for your records) • Certified copy of the Death Certificate • All forms filed on the deceased's Life Insurance:
- Employee's Enrollment Form - Beneficiary Designation form(s) - Election of Mode of Settlement form if completed by
employee - Statement of Health forms.
- If a Dependent spouse claim and if applicable, a copy of the Common-Law Marriage Questionnaire form
Mail to:
Metropolitan Life Insurance Company Group Life Claims PO Box 6100 Scranton, PA 18505-6100 NOTE: If there are multiple Beneficiaries, it is not necessary to
wait until all Beneficiaries' claim forms are returned before submitting the necessary forms to MetLife.
7 Employer If claim is for a Dependent: If the deceased Dependent is the only Dependent of
Employee, cancel all Dependent Benefits. If the deceased Dependent was included in the Beneficiary
designation, advise Employee to designate a new Beneficiary.
8 MetLife Process claim. NOTE: MetLife may request additional information.
9 MetLife Forward notification of a claim payment or a claim denial to Beneficiary with a copy to Employer.
When MetLife Processes Claims Normally, MetLife processes claims within ten (10) working days of receipt of: Completed claim form Certified Death Certificate showing cause and manner of death All forms filed on the deceased's Life Insurance
For Life claims, employers may provide Employer’s Statement, Enrollment Form, and Beneficiary Designation information via MetLink Life Claims in lieu of paper forms. If you have questions regarding this process, please contact your Account Manager.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 39
If the claim is not processed within ten (10) working days, contact the MetLife Group Life Claims Office at 1-800-638-6420 for a status update.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 40
Life Disability and Long Term Disability Single Claim (Process for customers who have waiver & LTD paper claims)
Continued Protection Premium Waiver (PW), also known as Continued Protection (CP), provides continuation of group life coverage without further premium payment for Employees meeting the contractual definition of disability. Coverage continues according to the plan provisions, even if the Customer cancels or moves the policy.
Step Responsibility Description
1 Employer When an Employee becomes totally disabled: Continue to submit premium on Employee's behalf until the
earliest of the claim approval / denial or until the Employee is no longer an active Employee.
If the Employee is no longer an active Employee, or if premium will not be remitted: Instruct Employee to convert to a personal policy (see
Conversion Privilege for details) to avoid losing coverage in case the CP claim is denied
2 Employer Verify the Employee’s: Eligibility as defined in the applicable Certificate Participation in the applicable Plan
3 Employer Complete the Employer Statement section of the Group Life Insurance Statement of Review form. Please refer to the MetLife Premium Waiver Claims Submission Checklist for instructions on completing the Employer Statement.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 41
MetLife Premium Waiver Claim Submission Checklist
RE: Insured: S.S. No.: Please check that the requested documents are enclosed to enable us to process this claim. Failure to supply these necessary documents will delay the processing of the claim. Employer's Statement All areas are completed, including, but not limited to:
The type of coverage and dollar amount. Coding (Report Number, Sub Code, and Branch Number) Salary information Date insurance amount last changed
Job Description attached. Employer statement is signed by authorized representative. The hand-written, typed, or
stamped signature of the employer representative on a cover letter is also acceptable. If applying for Supplemental/Optional Life, two years of enrollment history are required for elected
coverage. The enrollment should apply to the year of the employee’s date lasted worked in addition to the year prior. Original or legible fax or copy of the enrollment forms or evidence of enrollment. (No enrollment form is necessary when the coverage is employer-paid, and all employees receive a set amount, such as $50,000 or one times pay.) For optional/contributory coverages, original or legible fax or copy of enrollment forms or evidence of enrollment for current period and for the prior two years if Medical Evidence of Insurability (MEOI) could apply.
Supplemental/Optional Life enrollment information is always needed, even if a disability claim is filed
with MetLife Disability. Employee’s Statement completed by the insured.
If the Employee’s Statement is not included, please be sure to have the form provided to the Insured/Employee.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 42
Key Elements of the Employer Statement
Type of Claim Submission
• Continued Protection (Waiver of Premium) – CP
Disability coverage approved after satisfying a waiting period of a number of months, which is specified in the contract. Once an employee is approved for CP, premiums are waived, and MetLife is liable for the disabled employee’s death benefit (even after the contract terminates). Fully Insured Benefits.
• Continued Life Insurance (Premium Pay) – CI A coverage under which a disabled employee may be covered for a period of time provided premiums are paid.
• Total and Permanent Disability - T&P A disability that will presumably last for the Insured's lifetime and which prevents the individual from engaging in any occupation for which he or she is reasonably suited by education or experience.
Section 1 - Employer’s Demographic Information
Section 2 - Employees Demographic Information
Important Notes:
• Please remember to attach the job description • The salary area should reflect the salary used for the calculation base for the Life coverage in effect on the
employee’s last day worked.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 43
• Number of hours worked per week is based on the number of hours worked per week by the employee prior to the date last worked.
Section 3 - Coverage Information
Important Notes:
• Date lasted worked is the date the employee was last performing the duties of their job. If the employee's date lasted worked fell within the effective dates with MetLife and was prior to their termination date, they are eligible for a Life Waiver review.
• Why did employee cease work on that date? Employer’s version of why the Employee stopped working on the date provided above
• Coverage - Only submit the coverage’s where MetLife administers the Life coverage and is applicable to the type of claim being submitted for review.
• Report, Sub Code, and Branch, also known as the MetLife Structure, which is the identifying group of numbers that makes each customer and its locations unique from other customers and from other locations within the customer.
• If applying for Supplemental/Optional Life, two years of enrollment history are required for elected coverage. Original or legible fax or copy of enrollment forms or evidence of enrollment for current period and for the prior two years if Medical Evidence of Insurability (MEOI) could apply. Supplemental/Optional Life enrollment information is always needed, even if a disability claim is filed with MetLife Disability.
Employer’s Signature

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 44
• Employer statement must be signed by an authorized representative. The hand-written, typed, or stamped signature of the employer representative on a cover letter is also acceptable.
4 Employer Send the claim form to Employee (retain a copy for your records).
5 Employee Complete the Employee Statement section, including: Personal information on Employee Personal information on Attending Physician
Example Employee’s section of a Group Life Insurance Statement of Review form
6 Employee Forward the claim form to Attending Physician.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 45
7 Attending Physician
Complete the Attending Physician's Statement of Disability section and return the completed claim form to Employee.
8 Employee Submit the completed claim form to Metropolitan Life Insurance Company PO Box 14632 Lexington, KY 40512-4632
9 Employer Notify MetLife if Employee returns to active work or if Employee retires (if applicable to your plan).
10 Employer If an eligible Employee dies before the submission of proof of disability and within one year of termination of employment, send full facts with the completed claim form to: Metropolitan Life Insurance Company Group Life Claims PO Box 6100 Scranton, PA 18505
11 MetLife Issue the approval, denial or termination notice and return it to the Employer and Employee.
12 MetLife Correspond directly with Employee periodically as set forth in the applicable Certificate to determine that he or she continues to be totally disabled.
13 Employer As of the date of approval, make no further premium remittances on Employee's behalf.
14 Employer If Employee dies, follow the procedures in Life Claims.
When MetLife Receives Claims Documentation Normally, MetLife acknowledges receipt of claims documentation within ten (10) working days If you have any questions, please contact the MetLife Waiver Claims Office at 1-800-300-4296 for a status update.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 46
Accelerated Benefits Option (ABO) Claims Under the ABO provision, an insured Employee or a covered Dependent spouse may apply for a percentage of his or her Group Life coverage as defined in the applicable Certificate. Accelerated Benefits are paid in a lump sum check or in three monthly installments. The amount of any Accelerated Benefits paid to the insured Employee or a covered Dependent spouse reduces the Life Benefits payable to the Beneficiary and the amount of Life Benefits available for the insured Employee or a covered Dependent spouse to convert.
Step Responsibility Description
1 Employer When an Employee or a covered Dependent spouse is diagnosed as having a terminal illness, verify the Employee’s or covered Dependent spouse’s: Eligibility as defined in the applicable Certificate Participation in the applicable Plan
2 Employer Select the applicable claim form: Accelerated Benefits Claim Form
See Forms for an unmarked sample.
3 Employer Send the claim form to Employee.
4 Employee Complete the Claimant’s Statement section, including: Personal information on Employee
If a Dependent spouse claim, personal information on Dependent spouse
Amount(s) of Life Benefits

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 47
Example Employee’s section of a standard Accelerated Benefits Claim Form
5 Employee Forward the claim form to Attending Physician.
6 Attending Physician
Complete the Statement of Attending Physician section and return the claim form to Employee.
7 Employee Submit the completed Claimant’s Statement section and Statement of Attending Physician section to Employer.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 48
8 Employer Complete the Employer’s Statement section, including: Personal information on Employee
If a Dependent spouse claim, personal information on Dependent spouse
Applicable Group/Report Number, Sub Code/Subdivision and Branch (See Reporting Structure for details)
Amount(s) of Life Benefits and whether reduced by: - A reduction formula Last day worked
Example Employer’s section of a standard Accelerated Benefits Claim Form

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 49
9 Employer Submit the following: • Completed claim form (Retain a copy for your records) • All forms filed on the Employee's Life Insurance:
- A copy of the Employee's Enrollment Form - A copy of all Statement of Health forms
- If a Dependent spouse claim and if applicable, a copy of the Common-Law Marriage Questionnaire form
Mail to:
MetLife Group Life Claims PO Box 6068 Utica, NY 13504-6068
10 MetLife Process claim. NOTE: MetLife may request additional information.
11 MetLife Forward notification of a claim payment or a claim denial to Beneficiary with a copy to Employer.
12 Employer Reduce Life Insurance inforce on the Invoice form by the amount of the ABO payment once the ABO is approved.
13 Employer When Employee or a covered Dependent spouse dies, follow the procedures in Life Claims. NOTE: Make sure that the amount of the Life Benefits inforce
shown in the Employer's Statement of Life Insurance Claim Form has been reduced by the amount of any Accelerated Benefits paid to the Insured.
When MetLife Processes Claims Normally, MetLife processes claims within ten (10) working days of receipt of: Completed claim form All forms filed on the Employee's Life Insurance
For ABO claims, employers may provide Employer’s Statement, Enrollment Form, and Beneficiary Designation information via MetLink Life Claims in lieu of paper forms. If you have questions regarding this process, please contact your Account Manager. If the claim is not processed within ten (10) working days, contact the MetLife Group Life Claims Office at 1-800-638-6420 for a status update.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 50
Dental Claims The purpose of Dental Care Benefits is to encourage the prevention, early detection and correction of dental problems by providing benefits for oral examinations, cleanings and x-rays, and for the treatment of disease, accidents and/or injuries. Benefits are payable for covered dental services performed or prescribed by a dentist while coverage is in effect. The applicable Certificate provides specific information on your benefit Plan and level of payment. MetLife's Dental Care Benefits plans allow Employees to obtain dental care services from either a participating provider or a non-participating provider.
Participating Providers A participating dentist is a general dentist or specialist who has agreed to accept negotiated fees as payment in full for covered services provided to plan members. Employees can find a participating Network provider by:
• Obtaining provider listings, including maps and driving directions, on the Internet at www.metlife.com/mybenefits
• Calling 1-800-438-6388 8 a.m. to 11 p.m. (EST), Monday - Friday to receive an updated directory of Participating Dentists (printed in English or Spanish) by mail
Pre-Treatment Estimates MetLife suggests that Employees request a pre-treatment estimate if the cost of dental work is expected to exceed a pre-determined amount. See the applicable Certificate to determine the amount at which a pre-treatment estimate is suggested. MetLife reviews the pre-treatment submission and provides both the dentist and patient with an estimate of the benefits. To avoid misunderstandings about benefits, MetLife recommends that the Employee request the pre-treatment estimate before services are rendered. The estimate is not a guarantee of the final benefit payable.
Full-Time Student Verification Process If the claim form indicates the dependent is a full-time student, this information is entered into the claim system and the dental claim processes normally. If the claim form does not indicate the dependent is a full-time student, the dental claim is denied. A request is sent to the employee asking for the student status information. The following narrative is sent out on the Explanation Of Benefits (EOB) to the dentist and the employee: IN ORDER TO DETERMINE PLAN BENEFITS ON THIS CLAIM, THE FOLLOWING INFORMATION IS NEEDED IN WRITING: 1. IS PATIENT A FULL-TIME STUDENT? __________________ 2. NAME AND LOCATION OF STUDENT'S SCHOOL. ________________ 3. IS PATIENT TOTALLY DISABLED? ___________________ 4. IS PATIENT TOTALLY DEPENDENT ON EMPLOYEE FOR SUPPORT? ________________ RECEIPT OF THIS INFORMATION COMBINED WITH PLAN LIMITATIONS WILL DETERMINE THE PATIENT'S ELIGIBILITY FOR BENEFITS. The Employee completes the applicable questions and returns the EOB form to MetLife. MetLife will re-process the claim based on the additional information submitted by the employee.

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 51
MetLife will only request full-time student status once per school year period which is considered as September through August of the calendar year. If there is at least one claim in the patient's history during the school year period, then subsequent claims for the same patient within the same school year will not require the full-time student information to be included on the subsequent claims.
Guidelines for Dental Claims Submission Step Responsibility Description
1 Employer Forward the Dental Expense Claim Form to Employee. See Forms for an unmarked sample.
2 Employee Complete the To Be Completed By The Employee section and give it to Provider.
Example Employee’s section of a standard Dental Expense Claim Form
If the charges are more than the Pre-Determined Amount
3 Provider Before treatment starts: Complete the remainder of the claim form Check the Pre-Treatment Estimate box
4 Provider Before treatment starts, submit: Completed claim form Appropriate x-rays
Mail to:
MetLife Dental Claims PO Box 981282 El Paso, TX 79998-1282 NOTE: If Provider does not submit the claim form, it is the
Employee's responsibility to do so.
5 MetLife Send to Employee and Provider an Explanation of Benefits (EOB) that shows the amount the Dental Plan will pay.
6 Provider After treatment, resubmit the EOB stating the date of treatment.
Mail to:
MetLife Dental Claims PO Box 981282 El Paso, TX 79998-1282

Guidelines for Claims Submission
Employer Administration Manual 01/09/13 52
7 MetLife Process claim. NOTE: MetLife may request additional information.
8 MetLife Forward notification of a claim payment or a claim denial to the Employee and Provider.
If the charges are less than the Pre-Determined Amount
3 Provider After treatment: Complete the remainder of the claim form Check the Statement of Actual Services box
4 Provider Mail the claim to: MetLife Dental Claims PO Box 981282 El Paso, TX 79998-1282 NOTE: If Provider does not submit the claim form, it is the
Employee's responsibility to do so.
5 MetLife Process claim. NOTE: MetLife may request additional information.
6 MetLife Forward notification of a claim payment or a claim denial to the Employee and Provider.
When MetLife Processes Claims Normally, MetLife processes claims within ten (10) working days after receipt of the completed claim form. If the claim is not processed within ten (10) working days, contact the MetLife Group Dental Claims Office at 1-800-438-6388 or check www.metlife.com/mybenefits for a status update. Please note that Personal Health Information may not be shared if the appropriate documentation has not been received by MetLife.

Absolute Assignments
Employer Administration Manual 01/09/13 53
Overview If your Group Policy permits assignments as a gift, an Employee may assign the rights to his or her Group Life Insurance. If your Group Policy does not permit assignments as a gift, an Employee may assign the rights to his or her Group Life Insurance provided that an Officer of your Company executes the waiver and consent to the assignment that is included on the gift assignment form. MetLife honors viatical assignments if your Group Policy permits assignments as a gift. If your Group Policy does not permit assignments as a gift, MetLife will honor a viatical assignment only if an Officer of your Company executes the waiver and consent to the assignment that is included on the viatical assignment form. However, MetLife must accept a viatical assignment from a viator residing in California even if your Group Policy does not permit assignments. California law mandates that a viatical assignment be permitted even if the Life Insurance Policy under which the benefits are being assigned otherwise prohibits assignments. This California law applies only to the viatical assignment being requested by the Insured. It does not apply to any subsequent viatical assignments of the Insured’s Life Insurance coverage by subsequent owners. The Employee must understand that assigning their benefits means loss of all ownership and control over the assigned benefits.
General Information about Assignments This section contains information about assignments under plans that prohibit assignments. The section also defines key terms, explains what is assignable and describes common reasons for making assignments.
Plans that Contain a Prohibition Against Assignments If your Plan prohibits assignments, an assignment (of assignable coverages only) can be made as an exception using a form containing “Waivers and Consents” language as described above. When allowing assignments as exceptions, you should have clear, written decision-making procedures to determine when assignments will be allowed. Your legal counsel should review the procedures to ensure that they are not discriminatory. These procedures should be followed for all assignment requests.
Assignors and Assignees The assignor (the Insured) is the party transferring ownership of the coverage to the assignee. The assignee is usually the Insured's spouse, child(ren) or trustee of a trust established by the Insured. For viatical assignments, the assignee is a viatical settlement provider. Once an assignment is completed, the assignee is the owner of the coverage and would become the assignor for any future assignments. The following table defines assignors and assignees in more detail.
Assignment Terms and Descriptions
Term Description
Assignor An individual or entity that absolutely assigns all right, title, interest and incidents of ownership of an Insured's coverage. For a viatical assignment, the assignor is referred to as a viator.
Viator In general, a viator is an assignor who is a terminally or chronically ill insured who absolutely assigns to a viatical settlement provider all right, title, interest and incidents of ownership of his or her coverage. A viator is a type of assignor.

Absolute Assignments
Employer Administration Manual 01/09/13 54
Assignee An individual or entity to whom a transfer of all right, title, interest and incidents of ownership of an Insured's coverage is made. For a viatical assignment, the assignee is referred to as a “viatical settlement provider.” For a viatical reassignment, the assignee may be an individual, entity or another viatical settlement provider.
Viatical Settlement Provider
The person, or entity, that pays a viator a discounted amount of the insurance benefit.
Assignable Coverage Most contracts limit assignments to Employee insurance because only a benefit “on your own account” is assignable. For example, Dependent Life is not assignable because the coverage purchased by the Employee is insurance on the life of the Employee's Dependent, or “on the account of a Dependent.” Continued Protection Life Disability Benefits are assignable. Group Term Life Insurance may not be assigned as collateral for a loan or to secure payment for services, such as for future funeral expenses.
Rights over which Assignor Loses Control When an assignor assigns coverage, he or she transfers the rights to: Designate and change Beneficiaries and contingent Beneficiaries Elect or revise an optional mode of settlement for the assigned coverage Convert the assigned coverage to an individual policy Port the assigned coverage Make any application or election with respect to the assigned coverage, when and if the Employee would
otherwise be eligible to make it Receive any increase in the amount of insurance Make required Employee contributions if the Plan calls for Employee contributions Reassign the coverage
Following an assignment, all rights that the assignor otherwise could exercise now belong to the assignee. Once an assignment is made, the assignee is the owner of the Insured's coverage. For any future assignments, the owner is the assignor. The following sections explain an assignee's rights in more detail.
Designate and Change Beneficiaries and Contingent Beneficiaries When the assignor assigns his or her coverage, he or she surrenders the right to designate Beneficiaries. The assignee now has the right to change the beneficiary designation and is free to name anyone as Beneficiary other than the Insured's Employer. The assignee is not required to designate a Beneficiary at the time an assignment is made. However, unless and until the assignee designates a new Beneficiary, any existing beneficiary designation on file at the time the assignment is made will remain on record and the Life Insurance proceeds will be paid accordingly upon receipt of a properly supported claim.

Absolute Assignments
Employer Administration Manual 01/09/13 55
Elect or Revise an Optional Mode of Settlement for the Assigned Coverage The assignee has the right to elect or revise optional mode(s) of settlement of the proceeds (if the Group Policy allows this option) of the assigned coverage. Requests for election of settlement options by assignees are infrequent. If the previous owner elected an optional mode of settlement, the assignee must complete a Revocation of an Optional Mode of Settlement form.
Convert the Assigned Coverage to an Individual Policy The assignee has the right to convert (when the coverage(s) has a conversion option) the assigned coverage to an individual policy under the same conditions that apply to the original owner. See Conversion Privilege for details. When a conversion event occurs for an Insured, check for any assignments made for the Insured's coverage to determine who should receive the conversion notice. If the Insured has assigned his or her coverage, give the conversion notice to the assignee (not to the Insured).
Make Any Application or Election with Respect to the Assigned Coverage Once the assignment has been made, the assignor can no longer make any applications or elections that would affect the assigned coverage. Examples that would affect the assigned coverage are: Re-enrollment Increasing or decreasing the coverage amount Canceling the coverage
Receive Any Increase in the Amount of Insurance If the coverage increases for any reason, the assignee is entitled to that increase, not the assignor. However, when an assignor partially assigns the coverage, the amount of any increase is distributed among the owners in proportion to their ownership share.
Make Required Employee Contributions Assignees become responsible for any required Employee contributions for the assigned coverage(s). To avoid a coverage lapse, Employee contributions must be paid. The assignee can continue the Employee contributions as follows: Have the Employee contribution continue to be deducted from the Employee's salary. Have the Employee contribution continue to be deducted from the Employee's salary and reimburse the
Employee for the deducted contribution. Arrange an alternate payment method, with the Employer, for making the Employee contribution. If
arrangements for an alternate payment method are made, MetLife should still receive the payment from the Employer. MetLife will not accept direct payment from an assignee. MetLife does not require notification of, or arrange for, alternate payment methods.
Implications for Viatical Assignments Due to the nature of viatical assignments, once the viator receives the proceeds of a viatical settlement, he/she may no longer have an interest in keeping his or her coverage in force. On the other hand, the viatical settlement provider wants to protect its investment. Because the viator may have no concerns about coverage lapse, viatical settlement providers often reimburse the Employee for their contributions or arrange for alternate payment methods with the Employer. Viatical settlement providers take control of the payments to protect against coverage lapse.

Absolute Assignments
Employer Administration Manual 01/09/13 56
Reassign the Coverage As owner, the assignee of a gift or viatical assignment may choose to make an assignment to another person or entity, including a trustee under a trust agreement. Any future assignment requires the assignee to complete the assignment process as the assignor. NOTE: The standard gift and viatical assignment forms must be used for both assignment and
reassignments.

Absolute Assignments
Employer Administration Manual 01/09/13 57
Processing the Request The following procedures describe the steps that the assignor and assignee take to request: Assignment to an individual Assignment to a trust Assignment to a viatical settlement provider
This section then describes review and follow-up procedures that apply to all assignments and those that apply when the assignment is accepted and unacceptable.
Guidelines for Processing Assignments Step Responsibility Description
1 Assignor Request the applicable form from Employer: • Gift Absolute Assignment to Individual
• Gift Absolute Assignment to Trustee Absolute Assignment Pursuant to a Viatical Settlement See Forms for unmarked samples.
NOTE: If the Assignor resides in a Community Property Jurisdiction and the assignment is to someone other than the Assignor's spouse, the Assignor and the Assignor's spouse should complete the Spouse Waiver for Assignment of Group Life Benefits section on the assignment form.
2 Assignor Complete areas applicable to Assignor on the form.
3 Assignor Provide the form to Assignee for completion.
4 Assignee Complete areas applicable to Assignee on the form.
5 Assignee If an individual assignment, complete the Contingent Beneficiary section with the Assignee's estate as the contingent Beneficiary.

Absolute Assignments
Employer Administration Manual 01/09/13 58
Example Assignor’s and Assignee’s section of a standard Gift Absolute Assignment to Individual form
6 Assignee If an individual assignment exists and the Assignee wants to designate someone other than his or her estate as the contingent Beneficiary, the Assignee must complete the form, Beneficiary Designation By Owner. See Forms for an unmarked sample.

Absolute Assignments
Employer Administration Manual 01/09/13 59
Example Assignee’s section of a standard Beneficiary Designation By Owner form
7 Assignee If there is an Optional Mode of Settlement form on file and Assignee wants to revoke the mode of settlement, complete a Revocation of an Optional Mode of Settlement form. See Forms for an unmarked sample.
8 Assignee If there is an Optional Mode of Settlement form on file and Assignee wants to request a new optional mode of settlement, complete an Election of Mode of Settlement form. See Forms for an unmarked sample.
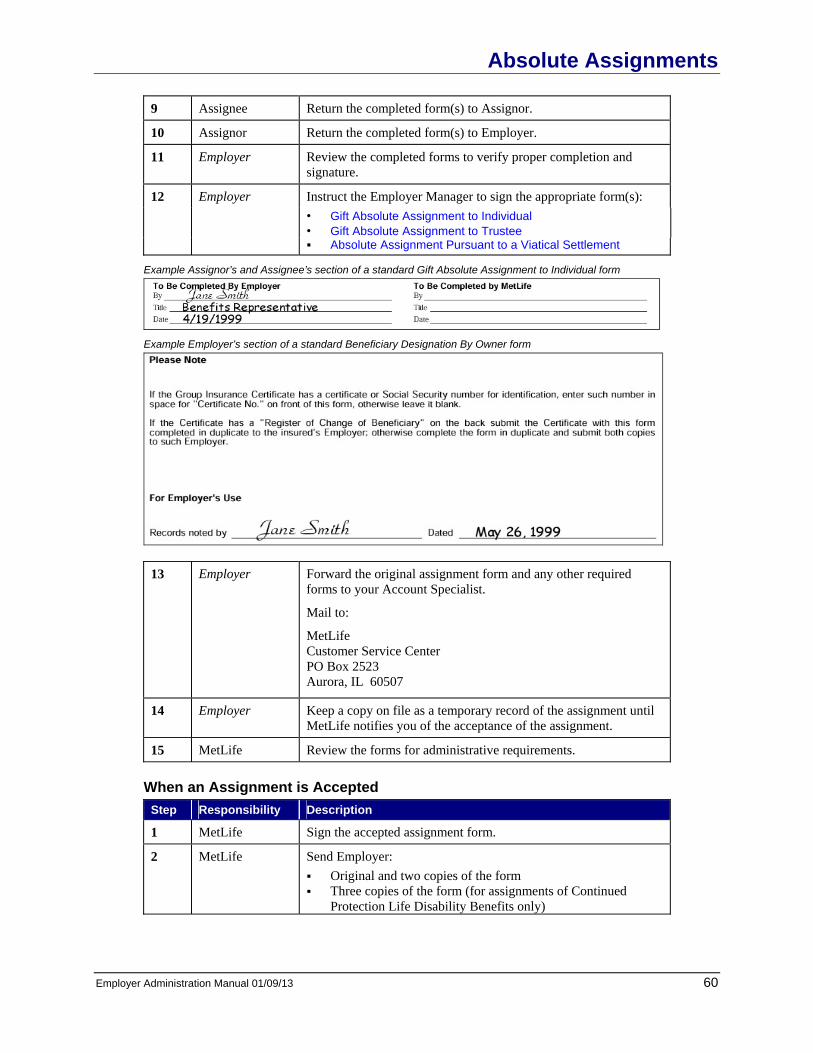
Absolute Assignments
Employer Administration Manual 01/09/13 60
9 Assignee Return the completed form(s) to Assignor.
10 Assignor Return the completed form(s) to Employer.
11 Employer Review the completed forms to verify proper completion and signature.
12 Employer Instruct the Employer Manager to sign the appropriate form(s): • Gift Absolute Assignment to Individual
• Gift Absolute Assignment to Trustee Absolute Assignment Pursuant to a Viatical Settlement
Example Assignor’s and Assignee’s section of a standard Gift Absolute Assignment to Individual form
Example Employer’s section of a standard Beneficiary Designation By Owner form
13 Employer Forward the original assignment form and any other required forms to your Account Specialist.
Mail to:
MetLife Customer Service Center PO Box 2523 Aurora, IL 60507
14 Employer Keep a copy on file as a temporary record of the assignment until MetLife notifies you of the acceptance of the assignment.
15 MetLife Review the forms for administrative requirements.
When an Assignment is Accepted Step Responsibility Description
1 MetLife Sign the accepted assignment form.
2 MetLife Send Employer: Original and two copies of the form Three copies of the form (for assignments of Continued
Protection Life Disability Benefits only)

Absolute Assignments
Employer Administration Manual 01/09/13 61
3 Employer Send Assignor: A letter notifying that the assignment is complete Two copies of the completed assignment form
NOTE: One copy of each form goes to Assignee and to Assignor as evidence of the assignment and for a record of the transaction.
4 Employer Attach the original assignment form to the Employee's Enrollment Form and note “Assignment Made” on the Enrollment Form.
When an Assignment is Unacceptable Step Responsibility Description
1 MetLife Notify Employer that the assignment form is unacceptable in its current state.
2 Employer Notify Assignor that the assignment has been rejected.
3 Employer Provide new forms to Assignor if needed.
4 Employer If Assignor wishes to resubmit the request, forms must be resubmitted to MetLife.
Procedures Following the Assignment
Beneficiary Designation by the Assignee The assignee is not required to designate a Beneficiary at the time an assignment is made. However, unless and until the assignee designates a new Beneficiary, any existing beneficiary designation on file at the time the assignment is made will remain on record and the Life Insurance proceeds will be paid accordingly upon receipt of a properly supported claim.
Conversion When events give rise to a conversion privilege, the Employer must give the conversion notice directly to the assignee (not to the Employee).
Portability When events give rise to portability eligibility, the Employer must give the portable term election form directly to the assignee (not to the Employee).
Death of the Assignee The Employer must notify MetLife of the death of an assignee. The new owner of the previously assigned coverage(s) must be established. The terms of the assignment document itself will determine who becomes the next owner. For example, if the assignee left a will which has been admitted to probate, it will be necessary to send your Account Specialist a copy of the probated will and a copy of those documents evidencing appointment of an executor. If the assignee left his or her entire estate to the Insured by will, the executor could generally transfer ownership of the insurance back to the Insured.
Certificate Rider If it becomes necessary to issue a Certificate Rider to insured Employees, the rider should be given to the insured Employee to be delivered to the assignee for attachment to the Certificate.

Absolute Assignments
Employer Administration Manual 01/09/13 62
Additional Information
Community Property Jurisdictions Certain states are community property jurisdictions and may have restrictions regarding assignments. As of January 9, 2013, the following are community property states: Arizona California Idaho Louisiana Nevada New Mexico Puerto Rico Texas Washington Wisconsin
The assignor completes the Spouse Waiver for Assignment of Group Life Benefits section on the assignment form if he or she resides in a community property jurisdiction. The assignor should consult with his or her attorney about questions that involve community property laws.
Valuation for Purposes of Federal Gift Taxation When an assignor makes an assignment of his or her Group Life Insurance, the assignment may trigger federal and tax gift law liability. The assignor must consent his or her own tax advisor with respect to any gift tax questions. MetLife only determines the value of assigned Group term coverage for the month in which the assignment is made when it prepares such valuation on IRS Form 712, Part II. The assignor, with the advice of his or her tax advisor, must determine the value of any additional gifts with respect to Group Life Insurance for federal or state gift tax purposes after the month in which the gift was made.
Collateral Assignments Assignments are not permitted as collateral security, or for value.
Partial Assignments An assignor may assign all or any combination of assignable coverages. The assignor may also assign any dollar amount or percentage of his or her assignable coverage(s). Partial assignments must be noted on the coverage signature line on the assignment form next to the assignor's signature. The exact dollar amount or percentage should be written out. Percentages or exact dollar amounts are acceptable for gift assignments. We strongly suggest percentages not be used for viatical assignments. If a percentage is used when a viatical assignment is involved, the Insured's intended Beneficiary could stand to lose additional benefits if the Insured's coverage amount changes.
Multiple Assignees Assignments to more than one individual/entity may create additional administrative and legal problems. However, MetLife does accept multiple assignees for gift and viatical assignments. If the assignment form indicates multiple assignees and a flat dollar amount or percentage is not allocated to each assignee, MetLife assumes equal amounts of the assigned coverage(s) are being assigned to each assignee.

Absolute Assignments
Employer Administration Manual 01/09/13 63
Accelerated Benefits Option (ABO) If an Insured has ABO, but has already assigned the coverage, neither the Insured nor the assignee can exercise the ABO option. If an Insured has ABO and has not assigned the coverage, the Insured can exercise his or her ABO option. The Insured may assign all or any part of the remaining benefit (after the ABO has been approved).
Assignments Made to Minors MetLife will accept a valid assignment to a minor. However, a minor's legal incapacity to act can create difficulties. When an assignor indicates that he or she intends to assign to a minor, MetLife recommends that the assignor consult an attorney.
Multiple Beneficiaries for Assignments Only MetLife accepts multiple Beneficiaries. The assignee should provide each Beneficiary's name, address, date of birth, and designated amount. We recommend all multiple designations be expressed as percentages. If no amount is designated to each Beneficiary, MetLife assumes equal amounts to each Beneficiary.

Conversion Privilege
Employer Administration Manual 01/09/13 64
Overview The Group Policy provides for the conversion of Group Life Benefits to an individual life policy when Group Life Benefits end or in some states when such benefits reduce. An Employee who wishes to convert any of his or her Life coverages must apply for the individual policy during the period in which coverage may be converted. The Employee also must pay the full premium costs of the coverage. The individual policy is issued without evidence of insurability and becomes effective on the 32nd following termination or reduction of Group Life Benefits as discussed in Period of Conversion Privilege. Employees who are going to work for another Employer may not be interested in converting their policies because they will be covered under their new Employer's benefit plans. However, an Employee who is not going to work immediately for another Employer or whose new Employer's benefit plan has a waiting period may wish to purchase an individual life insurance policy. Employees in either scenario must be offered conversion. An Employee also may apply to convert his or her Life Insurance or Dependent Life Insurance (if applicable) to an individual policy when his or her Life Insurance is canceled or when a Dependent spouse or child attains the limiting age. Dependent child or spouse coverage may also be converted when the dependent ceases to meet the eligibility requirements, such as upon divorce or active military service.
Coverage Ends Due To Termination If coverage ends because of termination of employment or termination of membership in a covered class, the individual policy may provide benefits in an amount equal to, but not in excess of, the amount of Group Life Benefits that ended. If Life coverage terminates for any other reason, refer to the applicable Certificate for specific issues.
Coverage Ends Due To Retirement An Employee whose Group Life Benefits end at retirement is eligible to convert up to the full amount of Life Benefits inforce on the date the Employee retires.
Coverage Ends Due To Termination of Group Policy or Amendment of Group Policy to Eliminate a Class If coverage ends because the group policy is terminated without a successor carrier, or amended to end Group Life Benefits on an entire class, such as eliminating retiree coverage, different conversion rules apply. Affected individuals may convert the lesser of the amount of Group Life Benefits lost or $10,000. The application period and procedures are unchanged. Voluntary cancellation of group coverage at the request of the insured, or cancellation for failure to pay required contributions does not trigger a conversion privilege.
Application Period for Life Conversion
Termination of Life Insurance Life conversion is generally governed by the law of the state where the Group Policy is issued. Persons who are eligible to convert must generally apply for a conversion policy as follows: If the notice is given within 15 days from the date when the Group Life Benefits end, the person
generally has 31 days from the date benefits ended to convert. If the notice is given more than 15 days from the date when the Group Life Benefits end, the person
generally has 15 days from the date the conversion notice is given to apply for a conversion policy. This extended application period is subject to an overall limit of 91 days from the date benefits ended.

Conversion Privilege
Employer Administration Manual 01/09/13 65
For example, if notice is provided 80 days following termination of Group Life Benefits, the application period will end on day 91, or 11 days from the date of notice.
If the group policy is sitused in New York, if the notice is given more than 15 days but less than 90 days from the date when the Group Life Benefits end, the person has 45 days from the date the conversion notice is given to apply for a conversion policy. However, if no notice is given, the maximum conversion period in New York is 91 days from the date of termination.
If the group policy is sitused in California, if the notice is given more than 15 days from the date Group Life Benefits end, the person has 25 days to convert. In no event will this period extend beyond 91 days.
The specific provisions governing conversion rights vary among states. Please contact your Account Specialist for details.
Conversion Variations for New Hampshire Residents When the Group Policy is cancelled or amended to end the Life Benefits of a covered class, persons eligible to convert must apply for a conversion policy within the following timelines: If the notice is given within 15 days from the date when the Group Life Benefits end, the person has 31
days within which to convert. If the notice is given more than 15 days from the date when the Group Life Benefits end, the person
has 15 days from the date the conversion notice is given to apply for a conversion policy.
Reduction of Life Insurance Persons who are eligible to convert the amount of any Group Life Benefits reduction(s) must apply for a conversion within the application period as measured from the date Life Benefits are reduced.
Guidelines for Completing Conversion Forms Step Responsibility Description
1 Employer Immediately upon termination or reduction of Group Life Benefits for Employee and/or covered Dependent, complete Part A and Part B of the Conversion of Group Life Benefits to an Individual Policy form. See Forms for an unmarked sample. NOTE: The conversion application request may be delayed if
pertinent information is omitted.

Conversion Privilege
Employer Administration Manual 01/09/13 66
Example Employer’s section of a standard Conversion of Group Life Benefits to an Individual Policy form
2 Employer Distribute the completed form as follows: Give or mail the original of the completed form to the person
eligible to convert Fax one copy to MetLife Advice Resource Center at 1-888-
422-4272. It is not necessary to send a copy to the MetLife administrative contact.
3 Person eligible to convert
Contact MetLife’s Advice Resource Center to begin the application process. Phone 1-877-ASK-MET7 (1-877-275-6387) Email [email protected]

Annual Census Request
Employer Administration Manual 01/09/13 67
67
MetLife evaluates performance of each group plan once a year. These evaluations may or may not result in rate changes. We review covered lives and demographic information, and therefore require updated census. Your Account Specialist will be sending you a request for census at least once a year. You should expect to receive it around 60 days prior to your renewal notification date and we ask that it be sent to us within 30 days of our request. We will ask for information on each employee eligible for the Life coverage that you have with us. The requested data will include specific information on each employee such as date of birth, gender, salary, occupation, as well as plan information such as level of benefits and participation. Most employers submit the data to us in Microsoft Excel or a text format. If you have different system requirements, please work with your Account Specialist. MetLife is committed to providing World Class Customer Service. When you receive the census request, prompt attention to this matter will enable us to continue to provide you with the best possible service at competitive prices.

Additional Services
Employer Administration Manual 1/9/2013 68
Preferred Dentist Program MetLife’s network was designed to help your employees get easy access to the care they need and lower their out-of-pocket costs.
Finding a Network Dentist Employees can find a participating Network provider by: Obtaining provider listings, including maps and driving directions, on the Internet at
www.metlife.com/mybenefits Calling 1-800-438-6388 8 a.m. to 11 p.m. (EST), Monday - Friday to receive an updated directory of
Participating Dentists (printed in English or Spanish) by mail
Nominating a Dentist to Join the Network Employees can nominate a dentist to join MetLife’s Network by having their dentist:
Write MetLife
Dental Program Management 501 US Highway 22 – Area 3N Bridgewater, NJ 08807
Email [email protected]
Other Issues Regarding Network Dentists Employees can call the customer service number 1-800-438-6388
WillsCenter.com
Available With All Coverages WillsCenter.com is an on-line will preparation document generation service available to all McDowell County Schools [active full-time employees/retirees], regardless of coverage and at no additional cost. This website is maintained by SmartLegalForms, Inc., a national provider of up-to-date and state compliant estate documents. This important life planning service allows a McDowell County Schools [employee/retiree] and/or their spouse to answer a state specific questionnaire to generate a will, living will, power of attorney or HIPAA authorization form. Documents can be saved on-line and revised at a later time. In addition, reference materials are available to assist in answering any questions. Note that the service does not include any attorney services or legal advice. Keep in mind that a will is an important document to have because it helps to secure your family’s financial future by documenting important decisions about the distribution of your assets and who cares for your children in the event of your death. This is a secure and viable alternative if you are unable to have an attorney prepare these documents. There is no cost to the [employee] to access this website or to generate any of the documents. In addition, there is no need for McDowell County Schools to provide eligibility information.
The WillsCenter.com service includes: 1. Access to a secure on-line service from the privacy of your own home. 2. Guidelines for preparing and updating an [employee] and spouse’s will, living will, power of attorney
and HIPAA authorization form. 3. Retention of documents while the account is active. 4. A self-help on-line library of valuable information.

Additional Services
Employer Administration Manual 1/9/2013 69
5. Excellent on-line and telephone customer support.
Access to this service is easy…. [Employees] simply access the following link: www.willscenter.com
• Customer Support Toll-Free Phone: 1-888-861-1089
• Customer Service: Monday - Friday: 9:00 AM - 5:00 PM Saturday: 9:00 AM - 12:00 Noon
Communications to [Employees] McDowell County Schools can communicate the value of this benefit with easy to understand employee communications created by MetLife. We have an array of communications such as the Employee Flyer which can be distributed in a paper format by you or posted on McDowell County Schools’s Intranet. Voicemail and E-mail announcements and Newsletter copy is also available for your use. Contact your MetLife Representative for samples. WillsCenter.com is a document service provided by SmartLegalForms, Inc., an affiliate of Epoq Group, Ltd. SmartLegalForms, Inc. is not affiliated with MetLife and the WillsCenter.com service is separate and apart from any insurance or service provided by MetLife. The WillsCenter.com service does not provide access to an attorney, does not provide legal advice, and may not be suitable for your specific needs. Please consult with your financial, legal, and tax advisors for advice with respect to such matters.

Reports
Employer Administration Manual 01/09/13 70
Listed below are standard reports MetLife offers to Employers. For assistance with any report, contact your Account Specialist.
Eligibility Listing (1-line edit report) The Eligibility Listing shows who is listed in MetLife’s United Inforce System (UIS) as having coverage. This report will be provided once annually to aid in your reconciliation. Any additional Eligibility Listings may incur a charge. Contact your Account Specialist for details.
Sample Eligibility Listing (1-line edit report)
0123456 XYZ COMPANY EMPLOYEE LAST NAME FIRST NAME COV START STOP GROUP SUB BRANCH STATUS MEMS CANC NUMBER DATE DATE NUMBER COV REASON 123456789 ANDREWS VINCENT D 09/08/97 0123456 0001 0001 A 1 234567890 CARTER JEFF D 02/15/00 0123456 0001 0001 A 8 345678901 JONES NICOLE D 06/24/96 0123456 0001 0001 A 4 456789012 MARTINEZ GEORGE D 03/13/79 0123456 0001 0001 A 1 567890123 MILLER JENNIFER D 06/27/00 0123456 0001 0001 A 1 987654321 NELSON JANINE D 10/20/95 0123456 0001 0001 A 1 876543210 SMITH JOHN D 05/01/98 0123456 0001 0001 A 4 765432109 PHILLIPS ERIC D 08/08/92 0123456 0001 0001 A 8 654321098 THOMPSON ANN D 12/06/88 0123456 0001 0001 A 1 543210987 WASHINGTON KEVIN D 11/19/98 0123456 0001 0001 A 4

Forms
Employer Administration Manual 01/09/13 71
This section contains the names and numbers of all forms mentioned in this manual. Addresses for forms that you mail are given here as well. For your convenience, a reference sample of each form is included at the end of this section.
How to Order To order any of the forms listed in this section, please contact your Account Specialist.

Forms
Employer Administration Manual 01/09/13 To order copies of forms, please contact your Account Specialist 72
Section Sub Section Form Name Form Number Send to Enrollment Procedures
New Enrollments Enrollment for Group Insurance Benefits GEF09-1
Maintained by Employer
Enrollment Procedures
Handicapped Dependent Children
Statement of Dependent Eligibility Beyond Limiting Age in Plan Due to Mental Retardation or Mental or Physical Handicap
MM2287-LAP Sandra Hollahan Account Specialist MetLife Customer Service Center PO Box 2523 Aurora, IL 60507
Enrollment Procedures
Spouses as Dependents
Common-Law Marriage Questionnaire JY0654 Maintained by Employer
Enrollment Procedures
Beneficiary Designation
Beneficiary Designation JY6004
MM6327
Maintained by Employer
Guidelines for Claims Submission
Life Claims Life Insurance Claim Statement DC-TCA5(xDTP)
Metropolitan Life Insurance Company Group Life Claims PO Box 6100 Scranton, PA 18505-6100
Guidelines for Claims Submission
Accelerated Benefits Option (ABO) Claims
Accelerated Benefits Claim Form
ABO-PAM+BEL-6 MetLife Group Life Claims PO Box 6068 Utica, NY 13504-6068
Guidelines for Claims Submission
Dental Claims Dental Expense Claim Form JY0333 MetLife Group Dental Claims PO Box 981282 El Paso, TX 79998-1282
Absolute Assignments
Absolute Assignments
Gift Absolute Assignment to Individual G1205
Maintained by Employer
Absolute Assignments
Absolute Assignments
Gift Absolute Assignment to Trustee G1205-T
Maintained by Employer
Absolute Assignments
Absolute Assignments
Absolute Assignment Pursuant to a Viatical Settlement
G1205-V-TERM
Maintained by Employer
Absolute Assignments
Absolute Assignments
Beneficiary Designation by Owner G10481-OWNER
Maintained by Employer

Forms
Employer Administration Manual 01/09/13 To order copies of forms, please contact your Account Specialist 73
Section Sub Section Form Name Form Number Send to Absolute Assignments
Absolute Assignments
Important Notice to Assignee G10667
Maintained by Employer
Conversion Privilege
Conversion Privilege
Conversion of Group Life Benefits to an Individual Policy
G685 The original to the person eligible to convert One copy to: MetLife Advice Resource Center Fax 1-888-422-4272 Email [email protected]
Guidelines for Claims Submission
New Mexico Domestic Abuse Short Form Notice
New Mexico Domestic Abuse Short Form Notice
EINFODISC-NM MetLife Consumer Affairs Attn: Betty Webb 500 Schoolhouse Road Johnstown, PA 15904