measuring antibiotic use in ltcfs
TRANSCRIPT

dason.medicine.duke.edu
MEASURING ANTIBIOTIC USE IN LTCFS
ELIZABETH DODDS ASHLEY, PHARMD, MHS
LIAISON CLINICAL PHARMACIST

Objectives - Compare and contrast advantages and disadvantages to various measures of antimicrobial use
-Describe unique approaches to measuring antibiotic use in long-term care facilities and describe best practices
- Outline key considerations for data validation
- Describe strategies to implement change based on antibiotic consumption data

Measures of Antibiotic Use
What we know from acute care hospitals
3

Top 10 Antibiotics: By Cost

Financial Data
Target audience: Administrators Most common measure of antibiotic use
Must choose between purchases vs. billing data
Pros:
Easily available data
Often tied to institutional goals for stewardship programs
Likely to be a “win” given historical effect of stewardship on this measure
Cons/Limitations:
Must remember to consider changes in contract pricing
Non-administrators less likely to be influenced by results

Top 10 Antibiotics: By Number of Patients
Treated
Defined Daily Dose
Target Audience: Administrators and
Epidemiologists Standardized definition of daily antibiotic dose
Created by the World Health Organization
Correction factor: Total Units (i.e. mg) Drug
DDD Correction Factor
Pros:
Attempts to convert raw purchasing data into utilization data
Allows comparisons with other institutions
Easy to calculate
Cons:
Not everyone agrees with the DDD correction factors
Many use institution-specific correction factors (prescribed daily dose)
Not patient level information
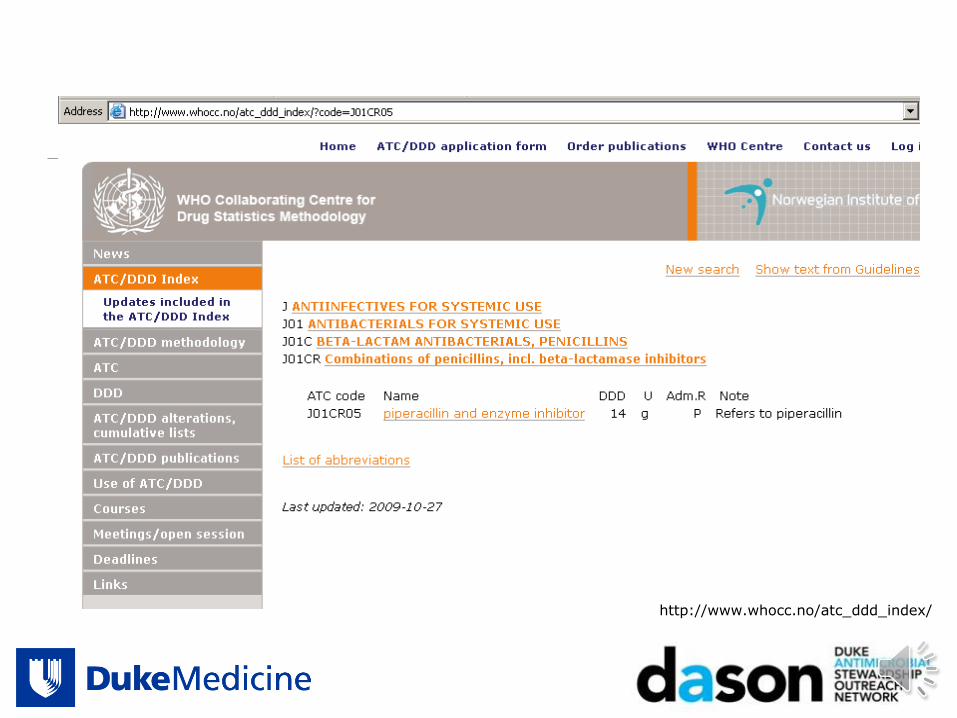
http://www.whocc.no/atc_ddd_index/

Why do the work yourself? ABC Calc
9
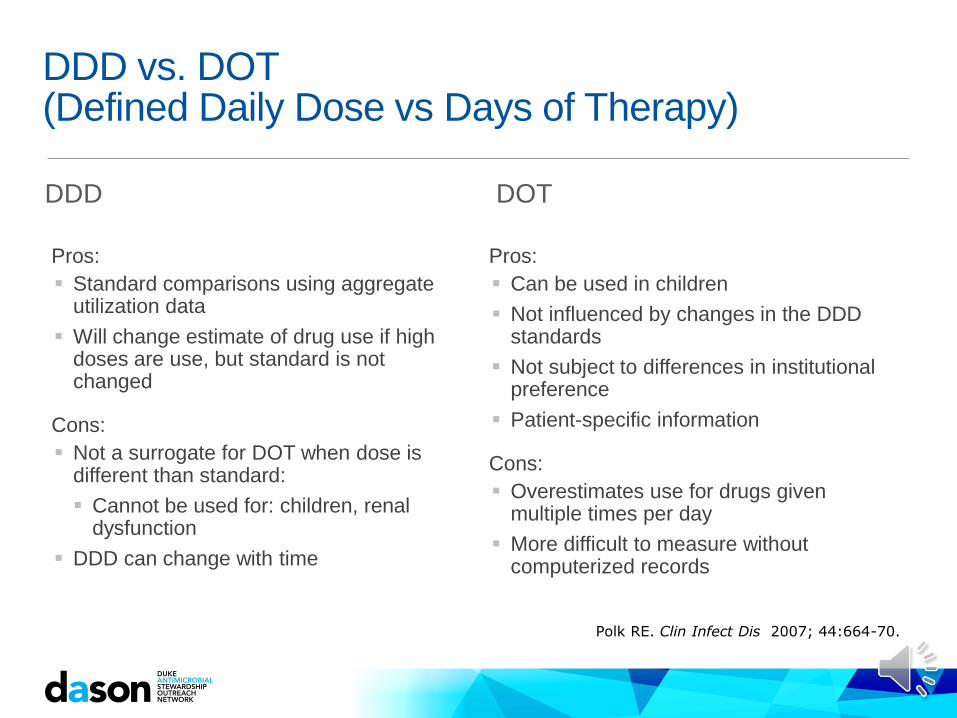
DDD vs. DOT (Defined Daily Dose vs Days of Therapy)
DDD
Pros:
Standard comparisons using aggregate utilization data
Will change estimate of drug use if high doses are use, but standard is not changed
Cons:
Not a surrogate for DOT when dose is different than standard:
Cannot be used for: children, renal dysfunction
DDD can change with time
DOT
Pros:
Can be used in children
Not influenced by changes in the DDD standards
Not subject to differences in institutional preference
Patient-specific information
Cons:
Overestimates use for drugs given multiple times per day
More difficult to measure without computerized records
Polk RE. Clin Infect Dis 2007; 44:664-70.
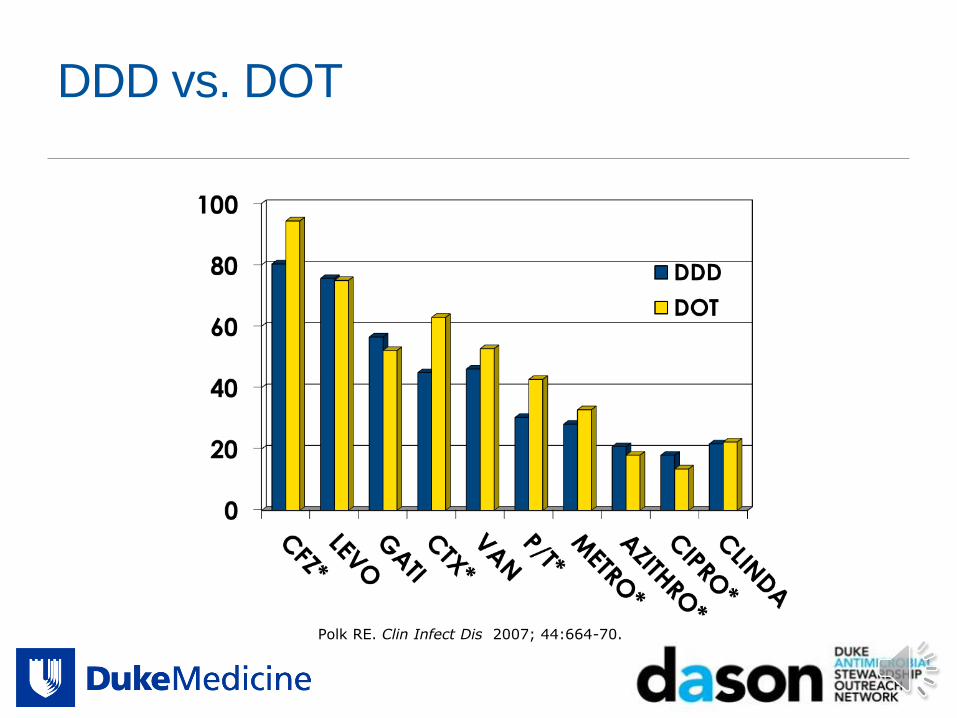
DDD vs. DOT
Polk RE. Clin Infect Dis 2007; 44:664-70.

DDD vs. DOT (/1,000 Patient Days)
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
DOT
DDD

Time Trends More Useful
University of Rochester Medical Center

Getting to the bottom of the problem….
Measures of antibiotic use are difficult to interpret and compared when examined alone DDD
DOT
Cost
A denominator is needed to standardize measurement of antibiotic use!
14
Numerator Values

Available Denominators for Measuring Antibiotic Use
Admissions: CDC Definition: The aggregate number of patients admitted to the
facility starting on the first day of each month through the end of the calendar month
Patient Days: CDC Definition: A daily count of the number of patients in the patient
care location during a time period. To calculate patient days, for each day of the month, at the same time each day, record the number of patients.
Days Present: CDC Definition: number of patients present in a given location for any
portion of any day
15


Total DOT/1000 PD by Hospital
500
550
600
650
700
750
800
850
900
1Q122Q123Q124Q121Q132Q133Q134Q131Q142Q143Q144Q14
To
tal A
nti
bio
tic D
OT
/1000 P
D
A B C D*
*Carbapenem data not included

Example Benchmark Data

What will we do with standardized data? US Benchmarking Efforts
CDC- Antimicrobial Use and Resistance module
Objective: The primary objective of Antimicrobial Use option is to facilitate risk-adjusted inter- and intra-facility benchmarking of antimicrobial usage. Secondary objective: to evaluate trends of antimicrobial usage over
time at the facility and national levels.
Primary metric: antimicrobial days/ 1000 days present
Data source: electronic MAR (with or without barcode medication administration)
19

Observed to Expected Ratios
Polk R et al. Clin Infect Dis 2011;53:1100-10.

21
http://www.health.sa.gov.au/INFECTIONCONTROL
But what about differences between facilities?
Efforts underway to standardize antibiotic use in acute care hospitals Similar to Standardized Infection Ratio (SIR) for US
Summary measure used to track HAIs
Summary statistic that compares a rate to baseline US experience adjusting for known risk factors
Proposed measure is Standardized Antibiotic Administration Ratio (SAAR)
Compares actual to expected antibiotic use after controlling for facility-level factors
www.qualityforum.org 5/20/15 meeting slides

DOT/1,000 Patient Days January through June 2013
0
20
40
60
80
100
120
140

Knowing Why Helps Too: Ciprofloxacin Top 10 Indications
Hospital A Hospital B
0 2000 4000 6000
Bone/Joint
Empiric - Unclear
Prophy (Surgical)
Empiric - F&N
BSI
Prophy (Non-surg)
SSTI
Other
Intrabdominal
UTI
# of Orders DOT
0 500 1000 1500
Empiric-Unclear
Not Specified
Bone/Joint
BSI
Pneumonia-Other
Other
SSTI
Prophy (Surgical)
Intraabdominal
UTI
# of Orders DOT
2
4

Biggest Lesson we have Learned
25
=

dason.medicine.duke.edu
CAN THIS BE DONE IN LONG TERM CARE FACILITIES?


Sources for Antibiotic Data in Nursing Homes
Purchasing data -Can be difficult for dispensing from a central pharmacy location to
many facilities
Dispensing data Can be difficult with a lot of floor stock
Electronic MAR
Paper and pencil Point prevalence survey
28

Are Additional Metrics Available? Courses/starts per 1,000 resident days
Advantages: easier to measure
Disadvantages: does not tell the whole picture- what about durations and overall exposure
Remember- a single course of chronic UTI prophylaxis is only started once!!!
Benoit SR et al. JAGS 2008;56:2039-44.

Are Additional Metrics Available?
30
Number (or percentage) of patients receiving antimicrobials
Advantages:
This number can help target education.
Disadvantages:
This can still underestimate
key prescribing practices.
Myelotte JM and Neff M. AJIC 2003;18-25.
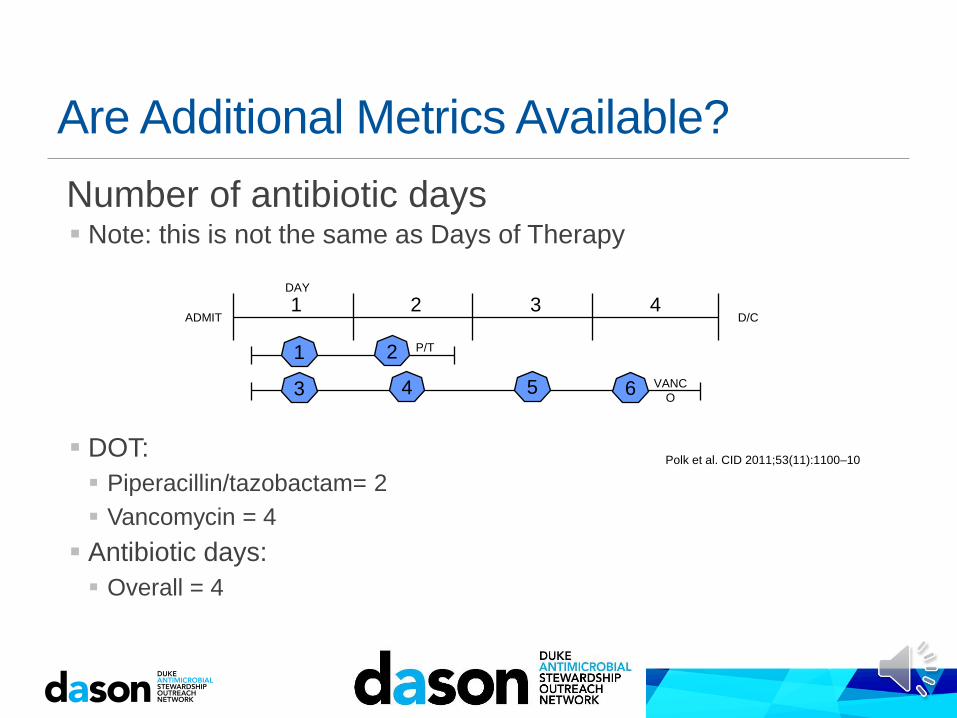
Are Additional Metrics Available?
Number of antibiotic days Note: this is not the same as Days of Therapy
DOT:
Piperacillin/tazobactam= 2
Vancomycin = 4
Antibiotic days:
Overall = 4
ADMIT D/C 4 3 1 2
P/T
VANC
O
Polk et al. CID 2011;53(11):1100–10
1
3 4
2
5 6
DAY
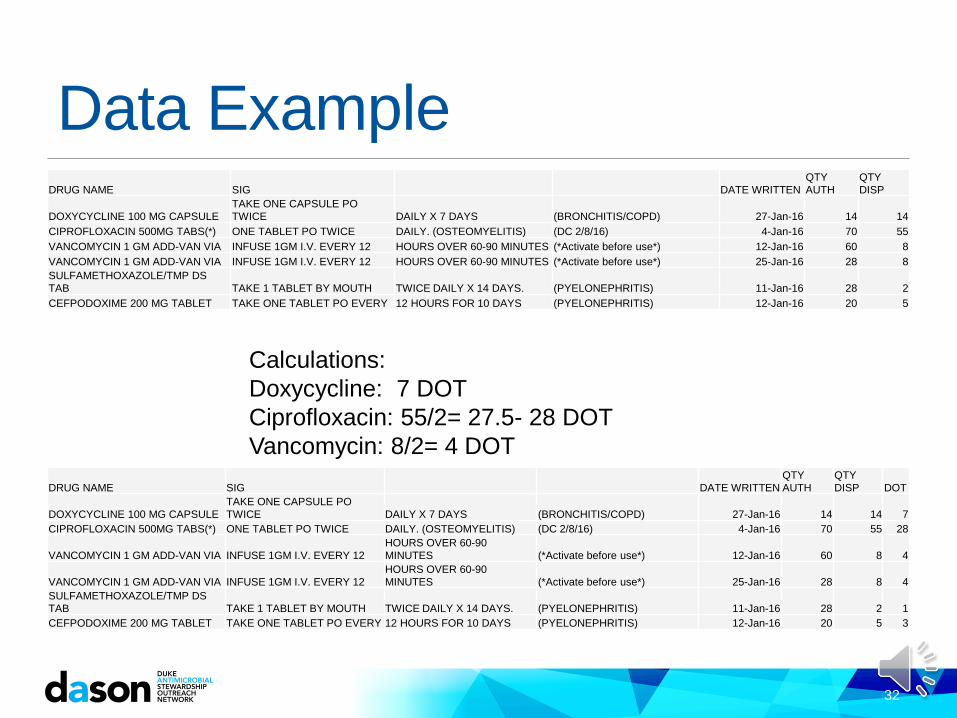
Data Example DRUG NAME SIG DATE WRITTEN
QTY
AUTH QTY
DISP
DOXYCYCLINE 100 MG CAPSULE TAKE ONE CAPSULE PO
TWICE DAILY X 7 DAYS (BRONCHITIS/COPD) 27-Jan-16 14 14
CIPROFLOXACIN 500MG TABS(*) ONE TABLET PO TWICE DAILY. (OSTEOMYELITIS) (DC 2/8/16) 4-Jan-16 70 55
VANCOMYCIN 1 GM ADD-VAN VIA INFUSE 1GM I.V. EVERY 12 HOURS OVER 60-90 MINUTES (*Activate before use*) 12-Jan-16 60 8
VANCOMYCIN 1 GM ADD-VAN VIA INFUSE 1GM I.V. EVERY 12 HOURS OVER 60-90 MINUTES (*Activate before use*) 25-Jan-16 28 8
SULFAMETHOXAZOLE/TMP DS
TAB TAKE 1 TABLET BY MOUTH TWICE DAILY X 14 DAYS. (PYELONEPHRITIS) 11-Jan-16 28 2
CEFPODOXIME 200 MG TABLET TAKE ONE TABLET PO EVERY 12 HOURS FOR 10 DAYS (PYELONEPHRITIS) 12-Jan-16 20 5
32
Calculations:
Doxycycline: 7 DOT
Ciprofloxacin: 55/2= 27.5- 28 DOT
Vancomycin: 8/2= 4 DOT
DRUG NAME SIG DATE WRITTEN QTY
AUTH QTY
DISP DOT
DOXYCYCLINE 100 MG CAPSULE TAKE ONE CAPSULE PO
TWICE DAILY X 7 DAYS (BRONCHITIS/COPD) 27-Jan-16 14 14 7
CIPROFLOXACIN 500MG TABS(*) ONE TABLET PO TWICE DAILY. (OSTEOMYELITIS) (DC 2/8/16) 4-Jan-16 70 55 28
VANCOMYCIN 1 GM ADD-VAN VIA INFUSE 1GM I.V. EVERY 12 HOURS OVER 60-90
MINUTES (*Activate before use*) 12-Jan-16 60 8 4
VANCOMYCIN 1 GM ADD-VAN VIA INFUSE 1GM I.V. EVERY 12 HOURS OVER 60-90
MINUTES (*Activate before use*) 25-Jan-16 28 8 4
SULFAMETHOXAZOLE/TMP DS
TAB TAKE 1 TABLET BY MOUTH TWICE DAILY X 14 DAYS. (PYELONEPHRITIS) 11-Jan-16 28 2 1
CEFPODOXIME 200 MG TABLET TAKE ONE TABLET PO EVERY 12 HOURS FOR 10 DAYS (PYELONEPHRITIS) 12-Jan-16 20 5 3

0
100
200
300
400
500
600
700
800
1 2 3 4 5
DD
D/1
0,0
00 r
es
ide
nt
da
ys
Antibiotic Use by Nursing Home
Based on Aggregate Purchasing Data
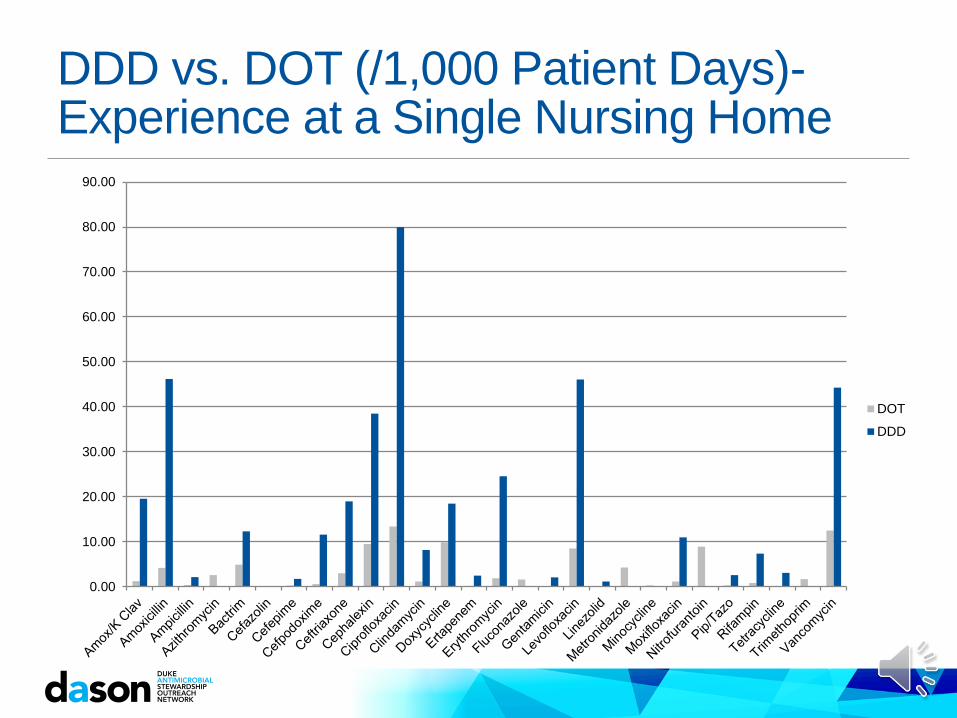
DDD vs. DOT (/1,000 Patient Days)- Experience at a Single Nursing Home
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
DOT
DDD
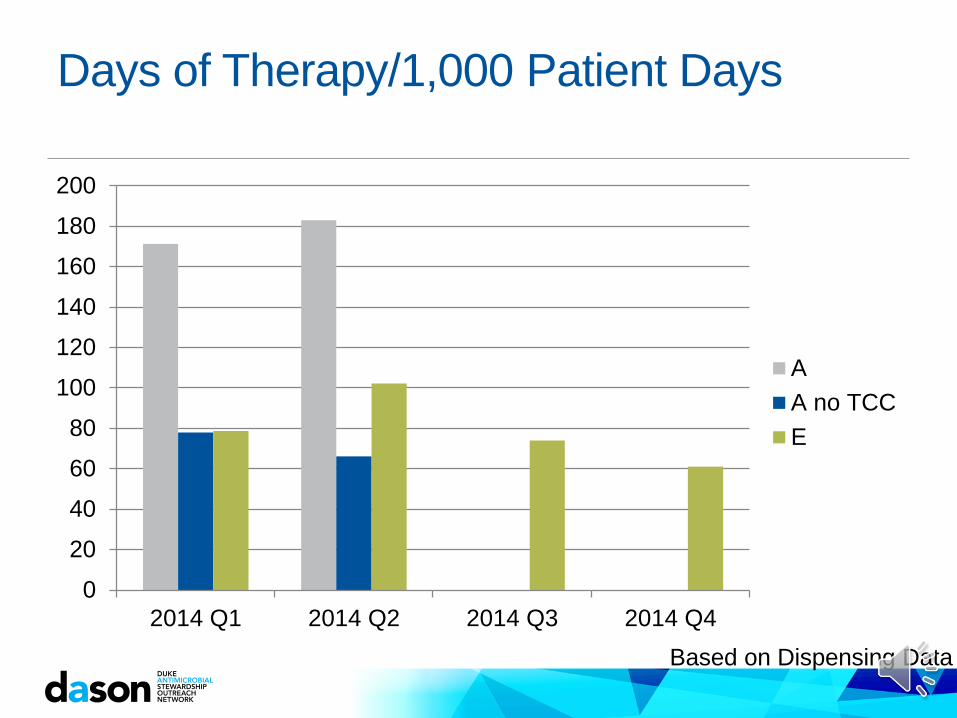
Days of Therapy/1,000 Patient Days
0
20
40
60
80
100
120
140
160
180
200
2014 Q1 2014 Q2 2014 Q3 2014 Q4
A
A no TCC
E
Based on Dispensing Data
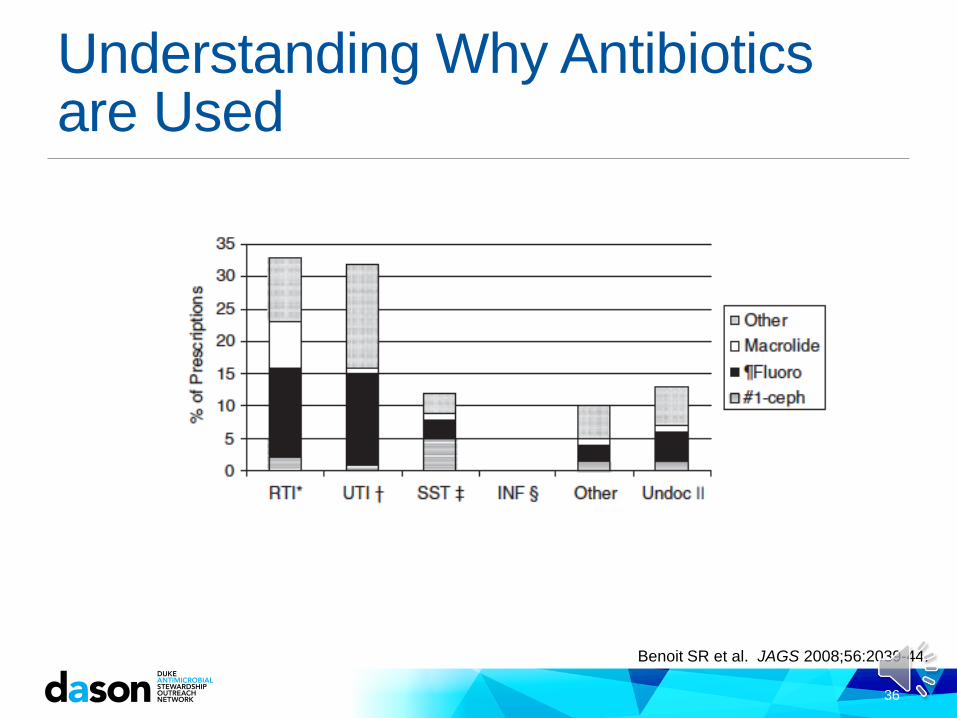
Understanding Why Antibiotics are Used
36
Benoit SR et al. JAGS 2008;56:2039-44.
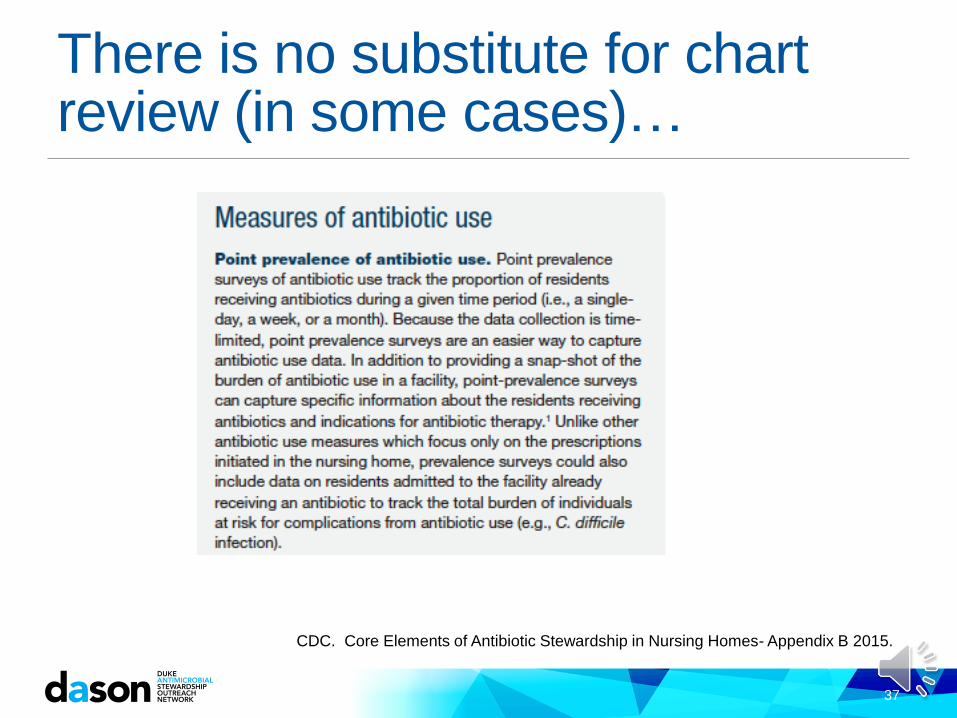
There is no substitute for chart review (in some cases)…
37
CDC. Core Elements of Antibiotic Stewardship in Nursing Homes- Appendix B 2015.

Most Common Indication for Antibiotic Use In Nursing Homes
0 50 100 150 200 250 300
UTI
Cellulitis
Pneumonia
Bone/joint infection
Thrush
C. diff
Wound infection
Intra-abdominal
Based on Dispensing Data
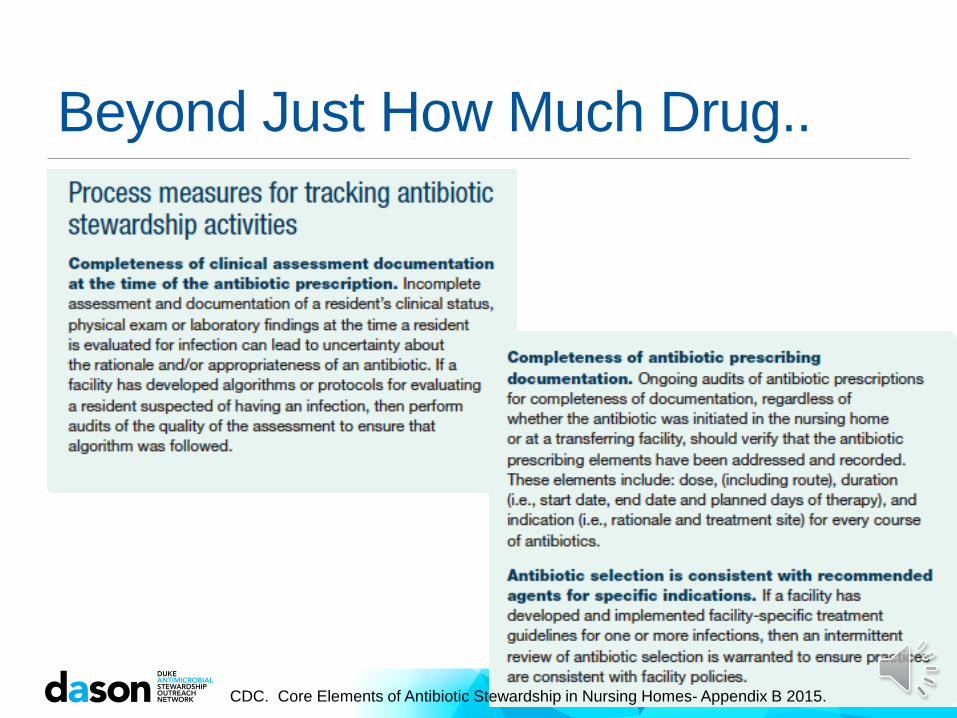
Beyond Just How Much Drug..
CDC. Core Elements of Antibiotic Stewardship in Nursing Homes- Appendix B 2015.


41 CDC. Core Elements of Antibiotic Stewardship in Nursing Homes- Appendix B 2015.

Do we know our target?
Less is better:
42
Daneman N et al. JAMA Internal Medicine 2015;175:1331-9.
Making the Data Actionable Data alone will not answer all the questions, but is allows more refined reviews Who?- Who is writing for the antibiotics?
What?- What is the most frequently used antibiotic?
Where?- Are there units that tend to use the most antibiotics?
When?- Are there times when antibiotics are most likely to be prescribed?
Why? - What is the most common reason antibiotics are used?
From there Conversations become more productive
Guidelines for use can be created with provider input
Remember- always ask why- the reasons behind the use might not be what you had guessed!

44