measuring physical fitness of adults in the primary
TRANSCRIPT

MEASURING PHYSICAL FITNESS OF ADULTS�
IN THE PRIMARY CARE SETTING�
By�
BECKY MARSHALL ELDER�
A research project in partial fulfillment of the requirements for the degree of
MASTER OF NURSING�
WASHINGTON STATE UNIVERSITY/ WHITWORTH COLLEGE� Intercollegiate Center for Nursing Education�
August 1999�

ii
To the Faculty ofWashington State University:
The members of the Committee appointed to examine the research project of BECKY MARSHALL ELDER find it satisfactory and recommend that it be accepted.

iii
ACKNOWLEDGEMENT
First and foremost I would like to thank my husband, Scott, for all of his love and
support during the writing of this. Secondly to my parents, for their unending
encouragement and love. To my advisor, Jackie Banasik, thank you for your thoughtful
time and consideration. Thank you to my other committee members, Lorna Schumann
and Ann Hirsch, for their incessant willingness to help.

iv
MEASURING PHYSICAL FITNESS OF ADULTS�
IN THE PRIMARY CARE SETTING�
Abstract�
by Becky Marshall Elder, M.N.� Washington State UniversityIWhitworth College�
August 1999�
Chair: Jacquelyn Banasik
The health benefits of physical activity have been reported in the literature for
many years. Suprisingly, 60% of American adults and 49% of youth (ages 12-21), are
not regularly active. Health care providers are frequently counseling patients regarding
the benefits of regular exercise, yet many are not measuring physical fitness in the office
setting.
Health related physical fitness relates directly to one's health status. Health. care
providers are directly involved with this type of fitness because of its evident correlation
with health promotion and disease prevention. Lack of physical activity and exercise has
been associated with an increase in cardiovascular disease, obesity, and musculoskeletal
problems. Health care providers are in a key position to assess, and measure physical
fitness in adults and ultimately track their progress.
A pre-exercise evaluation needs to be completed prior to customized exercise
prescription. This questionnaire alerts health care providers that further evaluation is
needed prior to instructions for improved fitness. There are five components of health
related physical fitness: body composition, aerobic capacity, muscular strength and
endurance, flexibility, and balance. These components can be objectively assessed in the

v
primary care setting in order to provide tailored exercise prescriptions. As well as having
a motivating effect for individuals, participants can make changes in their exercise habits
and improve their overall fitness. The participant's score is compared with normative
tables, providing information regarding their fitness level. The five components of health
related physical fitness can be measured routinely with improvement noted. The tools
used to measure the components of physical fitness will be discussed as well as
recommendations for use in the primary care setting.

vi
TABLE OF CONTENTS
IIIACKNOWLEDGEMENT
ABSTRACT� IV�
LIST OF TABLES VII�
INTRODUCTION 1�
DEFINITIONS 2�
TOOLS FOR MEASURING FITNESS 3�
QUESTIONNAIRES 4�
PRE-EVALUATION ASSESSMENT 7�
OBJECTIVE MEASUREMENTS OF FITNESS 8�
LITERATURE GAP 20�
RECOMMENDATIONS FOR PRACTICE 20�
CONCLUSION 22�
REFERENCES 23�
APPENDICES�
A. PHYSICAL ACTIVITY READINESS QUESTIONNAIRE 28�
B. PHYSICAL ACTIVITY READINESS EXAMINATION 30�

vii
LIST OF TABLES�
91. Body Mass Index
2. Katch Pulse Recovery Test Standards 11�
3. YMCA 3-Minute Step Test 13�
4. Aerobic Capacity for Women 14�
5. Aerobic Capacity for Men 14�
6. l-RM Bench Press Test 15�
7. Biceps Curls: Upper Body Muscular Endurance for Women 16�
8. Biceps curls: Upper Body Muscular Endurance for Men 16�
9. Partial Curl-Ups for Men and Women 17�
10. Leg Extensions: Lower Body Muscular Endurance for Women 17�
11. Leg Extension: Lower Body Muscular Endurance for Men 17�
12. Sit and Reach Test for Men and Women 19�
13. Balance for Women 19�
14. Balance for Men 20�

1
Measuring Physical Fitness of Adults in the Primary Care Setting
Introduction
The health benefits of physical activity have been reported in the literature for
many years. Surprisingly, 60% of American adults and 49% of youth (ages 12-21), are
not regularly active (President's Council on Physical Fitness and Sports, 1996).
Furthermore, one quarter of the United States adult population is not physically active.
Vigorous physical exercise had been a part of everyday life until the industrial revolution.
Obtaining sufficient exercise in the 1990's is challenging for most people because of
technological advances in the work setting and increasing time constraints. Most families
earn a dual income and have to work outside the home at predominantly sedentary
occupations (Francis, 1987; Bouchard, Shephard, & Stephens, 1993).
Health care providers commonly counsel patients regarding the benefits of regular
exercise, yet many are not routinely measuring physical fitness in the office setting.
Patients are often weighed at their annual check-up, but weight is not a good indicator of
physical fitness. More people are becoming aware of fitness tools and are beginning to
ask their primary care providers to measure their personal fitness. Learning their
personal fitness level may be a primary motivator for some individuals to increase their
physical activity, thus improving their health (Francis, 1987~ Fitness, 1996). A pre
exercise evaluation needs to be completed before providing tailored exercise
prescriptions. This paper examines physical fitness instruments and provides
recommendations for their application in the primary care setting.

2
Definitions
Despite the increased interest in physical fitness, a universally accepted definition
of "physical activity" or "physical fitness" does not exist (Bouchard et aI., 1993). These
terms need to be clearly defined in order to allow for accurate assessment of individual
fitness levels. The following definition of physical activity is used, " ... any bodily
movement produced by skeletal muscles that results in energy expenditure" (Caspersen,
Powell, & Christenson, 1985, p. 126). Normally, energy expenditure is measured in
kilocalories. In contrast, physical fitness is the ability to carry out daily tasks; which can
be measured with specific tests. "Physical fitness is a set of attributes that people have or
achieve that relates to the ability to perform physical activity" (Caspersen et aI., 1985, p.
126). Physical fitness is categorized into performance-related fitness and health-related
fitness (Bouchard et aI., 1993). Performance related fitness has a minimal relationship to
health. It is the ability of an individual to perform in a test or a sports competition. In
contrast, health promotion and disease prevention are concerned with health-related
fitness. Health-related fitness refers to the components of fitness that are affected by
habitual physical activity and relate directly to one's health status. The components of
health-related fitness include body composition, aerobic capacity, muscular strength and
endurance, flexibility, and balance (Brown, & Miller, 1998; Caspersen et aI., 1985;
President's Council, 1996).
Physical fitness is a complex behavior difficult to measure subjectively yet can be
measured objectively. Various instruments exist to measure physical fitness. These
instruments evolved over the years because of the strong evidence suggesting physical
activity improves health (Francis, 1987). Barriers to measuring physical fitness include:

3
safety, effectiveness, cost of equipment, time constraints, feasibility, and acceptability by
the patient. The variety of measurement tools and the different aspects of fitness that are
measured compound the difficulty of assessing physical fitness. For example, some
instruments measure aerobic capacity, muscular strength, endurance, flexibility and
balance. Others, like questionnaires, classify activities, looking at habitual energy of
everyday or strenuous activities. Many of these tests are appropriate for young and
middle-aged persons but are less relevant for the elderly. A questionnaire that is both
useful and useable in the primary care setting for the adult population as well as the
elderly needs to be developed.
Tools for Measuring Fitness
Physical fitness measurement tools have been utilized in three different arenas:
the laboratory setting, epidemiological studies, and individual-assessment. Tests in these
areas measure the components of physical fitness separately with different mechanisms
or machines (Caspersen et aI., 1985).
Instruments used in the laboratory setting include treadmill or cycle ergometer,
underwater weighing, cable tensiometer, isokinetic tests, and Leighton flexometer
(Caspersen et aI., 1985). These instruments help measure the components of physical
fitness. The fitness literature contains an exhaustive number of different measurement
tools, with no consensus among fitness leaders of a "gold standard." These tools are
expensive, require expert technicians, and are too cumbersome for use in the primary care
setting.
Tests used in epidemiological studies include: calorimetry, job classification,
measures based on self-report, physiologic markers, direct monitoring of behavior,

4
mechanical and electronic monitors, and dietary measures (Caspersen et aI., 1985).
These tests have many drawbacks for use outside of epidemiological studies because of
the need for equipment, specially trained personnel, time constraints, and cost. Further
epidemiological studies need to be completed in order to develop standards for health
policy in relation to instruments that measure physical fitness.
Individual assessment tests can realistically be used in the primary care setting to
measure the attributes ofphysical fitness. The YMCA, Fitness and Amateur Sport in
Canada, and the American Association ofHealth, Physical Education, Recreation and
Dance have developed physical fitness testing batteries that are reliable, valid, and have
national norms. These batteries measure the components of physical fitness; body
composition, aerobic capacity, muscular strength, endurance, flexibility, and balance
(Nieman, 1990).
Questionnaires
Questionnaires have been used in epidemiological research, to predict health
status, to describe physical activity, and for exercise prescription and monitoring
(Ransdell & McMillen, 1997). Self-reporting instruments ask people to classify their
level of physical activity_ An inverse relationship exists between the volume of
information obtained and the cost and time required for these self-reports (Haskell et aI.,
1992). Three types of physical activity questionnaires exist: recall, global self
assessment, and quantitative history (Ransdell & McMillen, 1997).
Recall questionnaires have been used to obtain personal records of physical
activity over an extended period. Participants can keep track of precise details about their
physical activity or general estimates of their usual activity. Little time is needed and it is

5
relatively simple to complete. This requires recalling details of past activities but
requires less effort than completing logs or diaries (president's Council, 1996). Recall
questionnaires are used when a specific estimated numerical value is needed for the level
of physical activity. " ... physical activity level is calculated as ''unitless interval scores"
(from 1 to 25 points) or as kcal'day or kcal'wk" (Ransdell & McMillen, 1997, p. 183).
Comparative standards are available for this type of questionnaire because it has been
used frequently (Ransdell & McMillen, 1997). The hindrance of recall questionnaires is
the inability to adequately quantify activity, distinguish between light, moderate, or
seasonal activity. Like the other self-report methods, it is subject to bias based on
memory recall (Ransdell & McMillen, 1997).
Global self-assessment questionnaires are based on recalling information. This
tool is easy to use because it rates physical activity relative to other people's activity
levels. Simple questions are asked regarding the level of physical activity. The test is
frequently used to classify individuals as active or sedentary (Ransdell & McMillen,
1997). Global self-assessments have a good rate of repeatability, reasonable validity, and
can be scored to assess the components of physical fitness (Bouchard et aI., 1993). Only
a specific level of activity or seasonal activity may be reported, and this questionnaire
deals only with high intensity activity, which is problematic. Global self-assessments
yield ratings of inactive, moderately active, or very active (Hensley, Ainsworth, &
Ansorge, 1993). Individuals are able to complete this global self-assessment in one to
two minutes.
The third data collection instrument is the quantitative history questionnaire. This
tool measures physical activity from a specific period of time. For example, activity is
6
obtained from last summer, over the past year, or a lifetime (Ransdell & McMillen,
1997). Categories for selection include much more active, about as active, or much less
active. The questions can trigger certain lifetime events that may help with long-term
memory of activity levels, thus providing detailed information that can reflect specific
seasonal activities (Hensley et aI., 1993). The time it takes to determine this information
may not be cost effective, and the accuracy of self-reporting is based on the memory of
the respondent (Ransdell & McMillen, 1997).
Questionnaires that have been developed for the general population regardless of
age, are inaccurate when used with the elderly (Washburn, Smith, Jette, & Janney, 1993).
For example, content is not sensitive enough to present the kinds of activity engaged in
by an older population, and the size of print may be too small making questions difficult
to read (Ransdell & McMillen, 1997).
Research studies that have reviewed questionnaires have not concurred about the
most effective one to use (Halfmann, Keller, & Allison, 1997; Jacobs, Ainsworth,
Hartman & Leon, 1993). For example, Knapsik, Jones, Reynolds, & Staab (1992)
developed a global self-assessed physical fitness questionnaire. Their study was the first
to examine the relationship between subjective and objective measures ofaerobic fitness.
The variables that were measured subjectively and objectively were aerobic capacity,
muscular strength, endurance, and flexibility. Their results showed that a simple self...
rating from physically active populations could categorize their fitness level. The
categories that were used were labeled as below average, average, above average, and
excellent (Knapsik, et aI., 1992). However, one limitation of their study was that their
subjects were very physically active and may have been more aware of their fitness levels

7
than the average person. Further testing of self-ratings of the fitness components to
determine if this simple questionnaire is applicable to the general population is
warranted.
Hopkins and Walker (1988) recommend the Stanford seven-day recall as the best
self-reporting instrument. The authors cite reliability, validity, and ease ofuse, as the
major advantages of this questionnaire. One disadvantage, however, is it favors those
involved in organized athletics. In contrast, a different seven-day recall was reported as
part of the Five-City Project (Sallis, et a!., 1985). The activities that were classified
included occupational and leisure and were classified based on their known energy costs.
Additional strengths of this questionnaire are that it can be administered in a relatively
short amount of time at very little cost, and can determine changes in activity patterns.
The scale was tested on 2,113 males and females, with reliable and valid statistical
outcomes (Sallis et a!., 1985). These are just a few examples of questionnaires
mentioned in the literature. Further investigation into standardizing questionnaires needs
to be done in order for effective use in the primary care setting.
Pre-evaluation Assessment
Before completing a health related fitness test battery, a pre-evaluation tool
should be completed. The British Columbia Department ofHealth, in conjunction with
the Multidisciplinary Advisory Board on Exercise (MABE), developed the Physical
Activity Readiness Questionnaire (PAR-Q) (Appendix A). The PAR-Q directs potentially
high-risk adults, or those needing special consideration, to seek medical advice prior to
starting or increasing their present fitness level. The PAR-Q involves seven questions
that are self-administered and conclude with a plan of action either to seek medical

8
advice, start a graduated exercise program, or postpone any physical activity (Chisholm,
Collis, Kulak, Davenport, & Gruber, 1975). Those identified as needing medical
clearance are encouraged to get their exercise prescriptions by their primary care
providers. The disadvantage of the original PAR-Q was that it screened out a substantial
number of elderly people. The revised PAR-Q alleviates this concern. With the new
revision, the number of participants screened out has been significantly reduced
(Shephard, Thomas, & Weller, 1991). MABE also developed guidelines for primary care
providers to determine what type or level of physical activity should be undertaken.
These guidelines (Physical Activity Readiness Examination (PAR-X)) (Appendix B) can
be used to complement the PAR-Q (Chisholm, et aI., 1975). Patients with known or
suspected activity limitations, or those in need of rehabilitation, should be referred to
exercise physiologists and rehabilitation specialists for specific evaluation.
Objective Measurements ofFitness
Instead of using self-reporting techniques in the primary care setting, objective
tests can be used to measure the five components of physical fitness. The first
component, body composition, can be measured in a variety ofways. Some fitness
experts recommend measuring skinfold sites for an overview of body composition. A
three-site skinfold test for men includes chest, abdomen, and thigh. For women the test
includes triceps, suprailiac, and thigh measurements. The accuracy and reliability of
using these measurements depend upon the tester, use of calipers, and the location of
measurement sites (Nieman, 1994). For most populations, body composition can be
estimated by using body height and weight and then calculating a body mass index (BMI
= body mass in kilograms, divided by height in meters squared) (President's Council,

9
1996). Basically, the BMI identifies whether a person is overweight based on the height
in relation to the weight (National Center for Health Statistics, 1997). A "healthy" BMI
range is between 20 and 25. Above 25-29 is considered moderately overweight while
over 29 is deemed obese. Morbid obesity is a BMI greater than 40 (Kenney, 1995).
Inordinate weight for height has been associated with an increased incidence of
hypertension, impaired glucose tolerance, and hypertriglyceridemia (Bouchard et al.,
1993). Table 1 provides a guide for individual weight based on height. The numbers
across the top signify the body mass index with height noted along the left vertical
column. BMI's do not make allowances for bone structure or gender. Women tend to
have less muscle and bone so they will usually fall at the lower end of the "healthy"
range of the BMI. Men are generally taller, have more muscle, and bone usually fall
within the higher ranges.
Table 1�
Body Mass Index
BMI 19 20 21 22 23 24 25 26 27 28 30�
4'10" 91 96 100 105 110 115 119 124 129 134 143� 4'11' 94 99 104 109 114 119 124 128 133 138 148� 5' 97 102 107 112 118 123 128 133 138 143 153� 5'1" 100 106 111 116 122 127 132 137 143 148 158� 5'2' 104 109 115 120 126 131 136 142 147 153 164� 5'3" 107 113 118 124 130 135 141 146 152 158 169� 5'4" 110 116 122 128 134 140 145 151 157 163 174� 5'5" 114 120 126 132 138 144 150 156 162 168 180� 5'6" 118 124 130 136 142 148 155 161 167 173 186� 5'7" 121 127 134 140 146 153 159 166 172 178 191� 5'8" 125 131 138 144 151 158 164 171 177 184 197� 5'9" 128 135 142 149 155 162 169 176 182 189 203� 5'10" 132 139 146 153 160 167 174 181 188 195 207� 5'11' 136 143 150 157 165 172 179 186 193 200 215� 6'0" 140 147 154 162 169 177 184 191 199 206 221�

10
Secondly, aerobic capacity is determined by measuring the body's maximal rate
of oxygen consumption. It is also known as cardio-respiratory fitness, cardiac endurance,
and aerobic power. Nieman defines aerobic capacity as ''the ability to continue or persist
in strenuous tasks involving large muscle groups for extended periods of time" (1994, p.
571). Aerobic capacity is considered the most important component of health-related
physical fitness by fitness leaders (Neiman, 1994).
A widely accepted and accurate method of assessing aerobic capacity is
measuring maximal oxygen consumption (V02 max). A treadmill or cycle ergometer is
used for accurate measurement in epidemiological studies (Stevens & Sykes, 1996).
"V02 max is most accurately determined by measuring expired air composition and
respiratory volume during maximal exertion" (President's Council, 1996, p. 34).
Expensive equipment, trained technicians, and acceptability and willingness of the
participant to exercise until exhaustion are all required. Henceforth, indirect ways of
estimating V02 max have been developed that require the participant to exercise less
strenuously. Aerobic capacity may be difficult to measure in the elderly population due to
cardiovascular disease and musculoskeletal problems (Kallinen, Suominen, Vuolteenaho,
& A1e~ 1998).
The step test can be utilized safely and effectively in the primary care setting to
estimate aerobic capacity. One of the earliest reported step tests was the Harvard Step
Test (Francis, 1987). Fitness was determined with an index score after participants
stepped up and down on a bench for a particular amount of time. Heart rate was
monitored after completing the steps. One limitation of this particular step test is short
statured people's inability to step as easily as their taller counterparts. It has been

11
modified over the years and now has a variety of variations with the principle remaining
the same.
There are single step tests and multistage step tests. Francis (1987) recommends
using the single step test in an office setting. It provides a quick measurement of aerobic
capacity, requires little equipment, and has an index score on which to base fitness. One
such test was developed by Katch (as cited in Francis, 1987) for middle aged adults. The
Katch Pulse Recovery Test requires a 12-inch bench and a stopwatch. The participant
steps 24 times onto the bench over three minutes. Five seconds after completing the test~
heart rate is counted for one minute. Normative data for this test includes classifying the
person's fitness according to heart rate recovery, as seen in Table 2. The step can be
raised to 16 inches for a sufficient steady state heart rate greater than 120 but less than
170 beats per minute. Fit individuals needing a greater challenge can increase the
stepping frequency for fitness assessment (Francis, 1987).
Table 2
Katch Pulse Recoyery Test Standards
Fitness Classification 60 Second Recovery Pulse Rate Excellent 71-78 Very good 79-83 Average 84-99 Below Average 100-107 Poor 108-118 (From ''Fitness Assessment Using Step Tests," by K.T. Francis, 1987, Comprehensive Therapy, 13(4), p. 38. Copyright 1987 by K.T. Francis. Reprinted with permission.)
The multistage step test can be considered if cardiovascular disease is suspected.
This test provides a gradual increase in work rate and stops activity before exhaustion is
reached. An example of a multistage step test reported by Siconolbi, Garber, Lasater, and
Carleton (as cited in Francis, 1987) can be used in the office setting. This test involves a

12
portable 10-inch step. The participant steps in three stages, stepping up 17, 26, and 34
times per minute. Heart rate response is obtained during the last 30 seconds of each stage
before starting the next level. The predicted maximum heart rate is 220 minus age. The
measured rate should not exceed 65% of the predicted maximum during the test (Francis,
1987). One-minute intervals separate the stages. Participants can advance to the next
stage by meeting specific criteria outlined in the test.
The Chester Step Test (as cited in Stevens & Sykes, 1996) measures aerobic
capacity using a 12-inch bench. Participants start out at a slow pace (15 steps per minute)
and increase there pace every two minutes to 20, 25, 30, and 35 steps per minute. The
heart rate is monitored continuously throughout the test. The test is complete once the
heart rate achieves 80% of the nlaximal heart rate (220 minus age). A graphical chart is
used to visualize predicted aerobic capacity. There is no gender bias in this test and a
moderate level of exertion is reached. One drawback is obese patients are required to
maintain their balance by nlanaging their body weight while performing the step test.
The 3-minute step test developed by the YMCA is ideal for a health related fitness
battery. The equipment needed is minimal making it cost effective. The equipment
needed includes 12-inch bench, metronome, and a stethoscope. The participant is not
allowed to practice because heart rate will be affected. The participant steps onto the
bench, at 24 steps per minute, for three minutes. After completing the exercise, heart rate
is counted with a stethoscope for one full minute, with the participant seated (Golding,
Myers, & Sinning, 1989). This post-exercise heart rate is the qualitative rating of fitness
and is compared to the norms in Table 3.

13
Table 3�
YMCA 3-Minute Step Test Post Exercise I-Minute Heart Rate <beats/min>
Age 18-25 26-35 36-45 46-55� Gender M F M F M F M F�
(M = male, F = female; From Fitness and Sports Medicine (p. 502), by D.C. Nieman,� 1990, Palo Alto, CA: Bull Publishing Company. Copyright 1989 by the YMCA of the�
Excellent 70-78 72-83 73-79 72-86 72-81 74-87 78-84 76-93� Good 80-88 88-97 83-88 91-97 86-94 93-101 89-96 96-102� Above average 91-97 100-106 91-97 103-110 98-102 104-109 99-103 106-113� Average 101-104 110-116 101-106 112-118 105-111 111-117 109-115 117-120� Below average 107-114 118-124 109-116 121-127 113-118 120-127 118-121 121-126� Poor 118-126 128-137 119-126 129-135 120-128 130-138 124-130 127-133� Very poor 131-164 141-155 130-164 141-154 132-168 143-152 135-158 138-152�
USA. Permission requested.)�
YMCA 3-Mioute SteD Test Post Exercise I-Minute Heart Rate <beats/min>
Age 56-65 >65� Gender M F M F� Excellent 72-82 74-92 72-86 73-86�
(M = male, F = female; From Fitness and Sports Medicine (p. 502), by D.C. Nieman,� 1990, Palo Alto, CA: Bull Publishing Company. Copyright 1989 by the YMCA of the�
Good 89-97 97-103 89-95 93-100� Above average 98-101 106-111 97-102 104-114� Average 105-111 113-117 104-113 117-121� Below average 113-118 119-127 114-119 123-127� Poor 122-128 129-136 122-128 129-134� Very poor 131-150 142-151 133-152 135-151�
USA. Permission requested.)�
Another test for aerobic capacity is called the one-mile walk test. The participant,
after warming up and stretching, walks one mile as fast as possible. The participant
monitors progress with a stopwatch. The results are compared to norms for age and sex.
Grouped by age ranges, the participant's score falls into categories of poor, fair, average,
good and excellent. Minutes and seconds are found in tables 4 and 5 (Fitness, 1996).
This tool can be used for self-assessment of physical fitness outside of the primary care
setting.

14
Table 4
Aerobic Capacity for Women
AGE 40-49 50-59 60-69 70-79 Excellent <14:12 <14:42 <15:06 <18:18 Good 14:12-15:06 14:42-15:36 15:06-16:18 18:18-20:00 Average 15:06-16:06 15:36-17:00 16:18-17:30 20:00-21 :48 Fair 16:06-17:30 17:00-18:06 17:30-19:12 21 :48-24:06 Poor >17:30 >18:06 >19:12 >24:06 (Measured in minutes:seconds; From "Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Table 5
Aerobic Capacity for Men
AGE 40-49 50-59 60-69 70-79 Excellent <12:54 <13:24 <14:06 <15:06 Good 12:54-14:00 13:24-14:24 14:06-15:12 15:06-15:48 Average 14:00-14:42 14:24-15:12 15:12-16:18 15:48-18:48 Fair 14:42-15:30 15:12-16:30 16:18-17:18 18:48-20:18 Poor >15:30 >16:30 >17:18 >20:18 (Measured in minutes: seconds; From ''Fitness. Measuring Fitness over 40," 1996, University of Califomia at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
The third component of fitness, muscular strength and endurance includes
measures of muscular strength, agility, and coordination. "Muscular strength is the
maximum force or tension level that can be produced by a muscle group" (Heyward,
1991, p. 12). Grip strength is frequently used because of the availability of national
norms, simplicity, and low cost. However, fitness leaders argue just one test is not
sufficient to measure muscular strength (Kenney, 1995). For a comprehensive
assessment, more than one muscle group must be tested. Suggested assessment includes
the upper and lower body. Standard tests include grip strength, and bench pressing using
free weights (president's Council, 1996). The simplest measure of muscular strength is
15
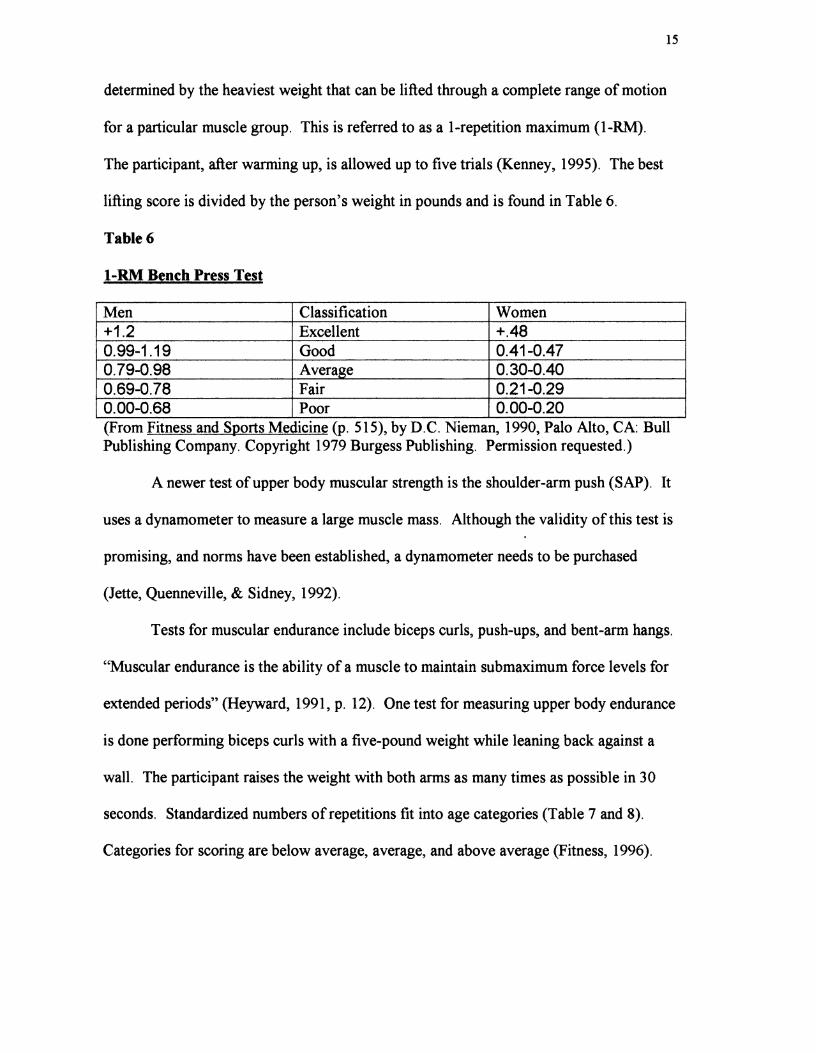
determined by the heaviest weight that can be lifted through a complete range of motion
for a particular muscle group. This is referred to as a I-repetition maximum (I-RM).
The participant, after warming up, is allowed up to five trials (Kenney, 1995). The best
lifting score is divided by the person's weight in pounds and is found in Table 6.
Table 6
l-RM Bench Press Test
Men Classification Women +1.2 Excellent +.48 0.99-1.19 Good 0.41-0.47 0.79-0.98 Average 0.30-0.40 0.69-0.78 Fair 0.21-0.29 0.00-0.68 Poor 0.00-0.20 (From Fitness and Sports Medicine (p. 515), by D.C. Nieman, 1990, Palo Alto, CA: Bull Publishing Company. Copyright 1979 Burgess Publishing. Permission requested.)
A newer test of upper body muscular strength is the shoulder-arm push (SAP). It
uses a dynamometer to measure a large muscle mass. Although the validity of this test is
promising, and norms have been established, a dynamometer needs to be purchased
(Jette, Quenneville, & Sidney, 1992).
Tests for muscular endurance include biceps curls, push-ups, and bent-arm hangs.
"Muscular endurance is the ability of a muscle to maintain submaximum force levels for
extended periods" (Heyward, 1991, p. 12). One test for measuring upper body endurance
is done performing biceps curls with a five-pound weight while leaning back against a
wall. The participant raises the weight with both arms as many times as possible in 30
seconds. Standardized numbers of repetitions fit into age categories (Table 7 and 8).
Categories for scoring are below average, average, and above average (Fitness, 1996).

16
Table 7
Biceps Curls: Upper Body Muscular Endurance for Women
Age 40-49 50-59 60-69 70-79 Above average >27 >25 >22 >21 Average 21-27 20-25 19-22 18-21 Below average <21 <20 <19 <18 (Number of repetitions; From ''Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Table 8
Biceps Curls: Upper-Body Muscular Endurance for Men
AGE 40-49 50-59 60-69 70-79 Above average >34 >33 >31 >28 Average 30-34 29-33 26-31 24-28 Below average <30 <29 <26 <24 (Number of repetitions; From "Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Other muscular endurance tests include push-ups for upper body endurance,
partial curl-ups for abdominal or trunk muscle endurance, and leg extensions for lower
body endurance. Males perform the traditional push-up and females use the knee-
supported position. The partial curl-up is preferred as a safer test than a full sit-up, with
the feet unsupported and knees bent. Individuals curl up in a controlled manner with
their hands outstretched reaching for the patella (Jette et aI., 1992). The partial curl-up is
performed at a rate of20 repetitions per minute, using a metronome (Sidney & Jette,
1990). The partial curl-up eliminates hyperextension of the lower back and has been
recommended in the Canadian national fitness program (Niema~ 1994). As noted in
Table 9, abdominal endurance decreases with increasing age (Sidney & Jette, 1990).

17
Table 9
Partial Curl-Ups for Men and Women
Age 20-29 30-39 40-49 50-59 60-69 Sex F M F M F M F M F M Excellent >30 >42 >30 >34 >25 >30 >17 >26 >20 Above average 24-30 31-42 21-30 27-34 19-25 22-30 11-17 20-26 14-20 Average 20-23 22-30 16-20 21-26 11-18 16-20 6-10 14-19 7-13 Below average 12-19 20-21 9-15 15-20 3-10 10-16 1-5 6-13 1-6 Poor <12 <20 <9 <15 <3 <10 0 <6 0 (F = females, M = males; normative values for females 60-69 are not available. From "The Partial Curl-up to Assess Abdominal Endurance: Age and Sex Standards," by K. Sidney and M. Jette, 1990, Sports Training, Medicine and Rehabilitation, 2, p. 52. Copyright 1990 Harwood Academic Publishers GmbH. Permission requested.)
Leg extensions are performed to measure lower body endurance. The participant
sits on the edge of a table with a 10 pound weight attached to the ankle, raising the leg as
many times in 30 seconds as possible without locking the knee. Tables 10 and 11 show
the fitness categories (Fitness, 1996).
Table 10
Leg Extensions; Lower Body Muscular Endurance for Women
AGE 40-49 50-59 60-69 70-79 Above average >27 >27 >25 >25 Average 24-27 23-27 22-25 23-25 Below average <24 <23 <22 <23 (Number of repetitions; From ''Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Table 11
Leg Extensions: Lower Body Muscular Endurance for Men
AGE 40-49 50-59 60-69 70-79 Above average >31 >30 >29 >30 Average 27-31 27-30 25-29 25-30 Below average <27 <27 <25 <25

18
(Number of repetitions; From "Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Flexibility is the fourth measure of fitness. It involves the movement of a joint
freely through an entire range of motion (Heyward, 1991). General flexibility is believed
to be significant for health, especially as individuals age, in order to maintain
independence (Bouchard et aI., 1993). Low back pain is common among adult men and
women due to their lack of flexibility (Pollock & Wilmore1990). No single measure
provides an individual's overall flexibility because measurement is specific to the joint
being measured (President's Council, 1996). Flexibility testing has been limited to the sit
and reach test which measures lower back and hamstring flexibility. Flexibility is
difficult to measure objectively or reliably (Fitness, 1996). The Canadian Standardized
Test ofFitness uses a simple field test called the Sit and Reach Test. The participant sits
down with legs outstretched on the floor. The feet are placed up against a board with a
yardstick attached. The 26-centimeter mark on the yardstick is placed at the point where
the feet contact the board. The participant then reaches as far down the yardstick as
possible. Knees are fully extended and no bouncing is permitted (Pollock & Wilmore,
1990). The score is read in centimeters after holding the position for one-second (Table
12). The length of the upper and lower limbs affect the maximal reach tests and may be
unsafe for some people to perform (Bouchard et aI., 1993). Jette et aI., (1992) question
the importance of flexibility in general fitness assessment. They argue data does not
demonstrate improved flexibility is a health benefit. Further research in this area is
needed to support their claim, as many fitness leaders deem flexibility an important
element ofhealth related physical fitness.

19
Table 12
Sit and Reach Test for Men and Women <centimeters)
Age (years) 20-29 30-39 40-49 50-59 60-69 Gender M F M F M F M F M F Excellent >40 >41 >38 >41 >35 >38 >35 >39 >33 >35 Above average 34-39 37-40 33-37 36-40 29-34 34-37 28-34 33-38 25-32 31-34 Average 30-33 33-36 28-32 32-35 24-28 30-33 24-27 30-32 20-24 27-30 Below average 25-29 28-32 23-27 27-31 18-23 25-29 16-23 25-29 15-19 23-26 Poor <24 <27 <22 <26 <17 <24 <15 <24 <14 <23 (M = males, F = females; From Exercise in Health and Disease (p. 684), by M.L. Pollock and J.H. Wilmore, 1990, Philadelphia, PA: W.B. Saunders Company. Copyright 1986 Fitness Canada, Government of Canada. Permission requested.)
Lastly, balance is measured as a component of physical fitness. Balance as a
component of health-related physical fitness is under debate. Some sources site it as a
component ofperformance-related physical fitness, while others deem it important to
one's health. Gait assessment for balance, agility, and coordination is especially
meaningful in the elderly population. Older persons are more prone to loss ofbalance
and falls (President's Council, 1996). Tests for measuring balance have been limited to
balance stands and walking on a narrow line. The participants stand on their dominant
leg, with their eyes open for up to 30 seconds. Their scores are (found in Table 13 or 14)
based on their ages and the number of seconds balance is maintained (Fitness, 1996).
Minimal time is needed for this balance assessment. It can easily be incorporated into the
routine neurological examination performed by health care providers.
Table 13
Balance for Women
AGE 40-49 50-59 60-69 70-79 Above average >15.5 >8.7 >4.5 >2.6 Average 7.2-15.5 3.7-8.7 2.5-4.5 1.5-2.6 Below average <7.1 <3.1 <2.4 <1.4

20
(Measured in seconds~ From "Fitness. Measuring Fitness over 40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Table 14
Balance for Men
AGE 40-49 50-59 60-69 70-79 Above average >14.8 >6.7 >4.0 >3.3 Average 4.1-14.7 3.2-6.7 2.5-4.0 1.5-2.6 Below average <4.0 <3.1 <2.4 <1.7 (Measured in seconds; From "Fitness. Measuring Fitness over .40," 1996, University of California at Berkley Wellness Letter, 12(7), p. 6. Copyright 1996 by Health Letter Associates. Permission requested.)
Literature Gap
The generalization of the findings cited in many studies with regard to fitness
assessment are limited due to the lack of random assignment, use of control groups, and
other methodological flaws (Lee, 1991). Most physical activity research has been
completed using male subjects, with an emphasis on the younger population. This limits
the extrapolation of the findings to both the elderly and women (Lee, 1991). A gap in the
literature exists in terms of follow-up studies measuring people's fitness levels across a
continuum to see if maintenance or improvement in fitness is sustained.
Bouchard, Shephard, & Stephens (1993) state most adults do not need fitness
tests. Instead, they recommend exercise prescriptions for the five components of health-
related fitness and information on how to reach minimal to desirable levels of fitness.
Pollock & Wilmore (1990) disagree and state that physical fitness test batteries are
important. They recommend a follow-up fitness evaluation after three to six months and
again after a year of training under regular circumstances.
Recommendations for Practice

21
There is no clear consensus in the literature for measuring physical fitness nor is
there a gold standard for the type of measurement instrument. However, certain health
related fitness test batteries can be modified to use in the primary care setting. Minimal
time and expense are needed to prepare a test battery. For example, health care providers
or other ancillary staff can measure the five components of fitness separately to estimate
total physical fitness for health. First, a pre-assessment questionnaire is completed,
specifically the revised PAR-Q (Appendix A). A positive response to the PAR-Q
indicates that a medical examination is warranted and the PAR-X (Appendix B) can be
utilized for that exam. Once a participant is cleared for fitness testing, informed consent
is obtained. Then a baseline blood pressure, heart rate, height, and weight are recorded.
Height and weight are used in calculating body mass index, an indicator ofbody
composition (found in Table 1). Using the YMCA's three-minute step test, the second
component, aerobic capacity, can be measured (Table 3). The third component, muscular
strength is tested using the bench press for upper body muscular strength (Table 6), and
the leg press for lower body muscular strength. Bicep curls can be utilized to measure
upper body muscular endurance (Table 7 and 8), partial curl-ups to test abdominal
musculature (Table 9), and leg extensions for measuring lower body muscular endurance
(Table 10 and 11). Flexibility, the fourth component, is tested and scored using the
Canadian Standardized Test ofFitness sit and reach test found in Table 12. Finally,
balance is measured by standing on one leg, with scores found in Table 13 or 14. Those
that are tested, and given medical clearance, are given individualized prescriptions for
exercise involving the five components of fitness.

22
Conclusion
The relationship between physical fitness and health is well documented (Haskell
et aI, 1985). Blair et a1. (1989), found that there was a strong and consistent inverse
correlation between physical fitness and mortality in men and women. Lack of physical
activity and exercise has been associated with an increased risk of cardiovascular disease,
obesity, and musculoskeletal problems (Heyward, 1991). People who engage in regular
physical activity reduce their risk of chronic disease and have improved energy (Nieman,
1994). Physical fitness can be measured in a multitude ofways. However, safety, cost of
equipment, time constraints, and practicality in terms of patient acceptability must be
taken into consideration before choosing a health related fitness test battery.
Health care providers are in a key position to assess, and measure physical fitness
in adults and ultimately track their progress. The assessment of each ofthe five
components ofhealth related physical fitness helps in developing a tailored exercise
prescription with specific exercises applied to the development of each component. After
obtaining a baseline measurement, adults are able to set realistic goals and then work
toward attaining these goals by routinely measuring their personal fitness. Measurement
of such goals can be ascertained in the primary care setting with improvement noted. As
well as having a motivating effect for individuals, participants can make changes in their
exercise habits and improve their overall fitness and health.

23
References
Blair, S.N., Kohl, H.W., Paffenbarger, R.S., Clark, D.G., Cooper, K.H., &
Gibbon, L.W. (1989). Physical fitness and all-cause mortality. Journal of the American
Medical Association, 262(17), 2395-2401.
Bouchard, C., Shephard, R.I., & Stephens, T. (Eds.) (1993). Physical Activity,
Fitness, and Health. Champaign, IL: Human Kinetics Publishers.
Brown, D.A. & Miller, W.C. (1998). Normative data for strength and flexibility
of women throughout life. Journal of Applied Physiology, 78, 77-82.
Caspersen, C.T., Powell, K.E., & Christenson, G.M. (1985). Physical activity,
exercise, and physical fitness: Definition and distribution for health-related research.
Public Health Research, 100(2), 126-130.
Chisholm, D.M., Collis, M.L., Kulak, L.L., Davenport, W., & Gruber, N. (1975).
Physical activity readiness. B.C. Medical Journal. 17(11), 375-378.
Fitness. Measuring fitness over 40. (1996). University of California at Berkeley
Wellness Letter, 12(7), 6.
Francis, K.T. (1987). Fitness assessment using step tests. Comprehensive
Therapy, 13(4), 36-41.
Golding, L.A., Myers, C.R., & Sinning, W.E. (Eds.). (1989). V's Way To
Physical Fitness (3rd ed.). Champaign, IL: Human Kinetics Publishers, Inc.
Halfmann, P.L., Keller, C. & Allison, M. (1997). Pragmatic assessment of
physical activity. Nurse Practitioner Forum, 8(4), 160-165.
Haskell, W.L., Leon, A.S., Caspersen, C.J., Froelicher, V.F., Hagberg, J.M.,
Harlan, W., Holloszy, J.M., Regensteiner, J.G., Thompson, P.O., Washburn, R.A. &

24
Wilson, P.W. (1992). Cardiovascular benefits and assessment of physical activity and
physical fitness in adults. Journal of the American Medical Association, 24(6), 8201
S220.
Haskell, W.L., Montoye, H.J., Orenstein, D. (1985). Physical activity and
exercise to achieve health-related physical fitness components. Public Health Reports,
100(2), 202-211.
Hensley, L.D., Ainsworth, B.E., & Ansorge, C.J. (1993). Assessment of physical
activity- Professional accountability in promoting active lifestyles. Journal ofPhysical
Education, Recreation and Dance, 64(1), 56-64.
Heyward, V. H. (1991). Advanced Fitness Assessment & Exercise Prescription.
(2nd ed.). Champaign, IL: Human Kinetics Books.
Hopkins, W.G. & Walker, N.P. (1988). The meaning of "physical fitness."
Preventive Medicine, 17, 764-773.
Jacobs, D.R., Ainsworth, B.E., Hartman, T.L. & Leon, A.S. (1993). A
simultaneous evaluation of 10 commonly used physical activity questionnaires. Medicine
and Science in Sports and exercise, 25(1), 81-91.
Jette, M., Quenneville, J., & Sidney, K. (1992). Fitness testing and counseling in
health promotion. Canadian Journal of Sports Science, 17(5), 194-198.
Kallinen, M., Suominen, H., Vuolteenaho, O. & Alen, M. (1998). Effort
tolerance in elderly women with different physical activity backgrounds. Medicine &
Science in Sports & Exercise, 30(1), 170-176.
Kenney, W.L. (Ed.). (1995). ACSM's Guidelines for Exercise Testing and
Prescription. (5th ed.). Baltimore, MD: A Waverly Company.

25
Knapsik, J.J., Jones, B.H., Reynolds, K.L., & Staab, J.S. (1992). Validity of self
assesses physical fitness. American Journal ofPreventive Medicine, 8(6), 367-372.
Lee, C. (1991). Women and aerobic exercise: Directions for research
development. Annals ofBehavioral Medicine, 13, 133-140.
National Center for Health Statistics. (1997). Healthy People 2000 Review, 1997.
Hyattsville, Maryland: Public Health Service.
Nieman, D.C. (1990). Fitness and Sports Medicine. Palo Alto, CA: Bull
Publishing Company.
Nieman, D.C. (1994). The exercise test as a component of the total fitness
evaluation. Primary Care, 21(3), 569-587.
Pollock, M.L. & Wilmore, J.H. (1990). Exercise In Health and Disease. (2nd ed.).
Philadelphia, PA: W.B. Saunders Company.
President's Council on Physical Fitness and Sports (1996). Physical activity and
health: A report to the Surgeon General. Washington D.C.: U.S. Department ofHealth
and Human Services.
Ransdell, L.B., & McMillen, B. (1997). Uses and limitations of physical activity
questionnaires in health education. Journal ofHealth Education, 28(3), 182-186.
Sallis, J.F., Haskell, W.L., Wood, P.D., Fortmann, S.P., Rogers, T., Blair, S.B. &
Paffenbarger, R.S. (1985). Physical activity assessment methodology in the five-city
project. American Journal ofEpidemiology, 121(1), 91-106.
Shephard, R.J., Thomas, S., Weller, I. (1991). The Canadian home fitness test.
Sports Medicine, 11(6), 358-366.

26
Sidney, K., & Jette, M. (1990). The partial curl-up to assess abdominal
endurance: Age and sex standards. Sports Training, Medicine and Rehabilitation, 2, 47
56.
Stevens, N. & Sykes, K. (1996). Aerobic fitness testing: An update. Occupational
Health, 48(12), 436-438.
Washburn, R.A., Smith, K.W., Jette, A.M. & Janney, C.A. (1993). The physical
activity scale for the elderly (PASE): Development and evaluation, 46(2), 153-162.

27
APPENDIX A
PHYSICAL ACTIVITY READINESS QUESTIONNAIRE

--------------------------------
30 Physical Activity ADDRESS�
_ Readiness� Examination~~. ~ BIRTHDATE SEX TELEPHONE
Par·X is the medical complement to Par.Q. the Physical Activity S.L No. MEDICAL No, Readiness QuestionNire. PI_ refer to "Guide To Use" below.
. ~:':i'F ACnVlTY LEVEL~, ACnVlTYINTERESTS No Yes Comments I Additional History L M H o Recreation 0 Sports
Heart Trouble 0 01'1� Job 0 0 0 o Fitness Program , , .
C!lest Pain 0 0� Leisure 0 0 0 o Other;Z Fitness Program
;l� Dizziness 0 0 o Regular ,;J Blood Pressure 0 0 o Sporadic• ';5 Musculoskeletal 0 0� o None
Other reason j 0 0� Over 65 Years 0 0�;1
'lId;cations (relevantl 0 0
YSI~§~~ Wt. _Ht.� BP
Cardiovascular� 0 ECGCl
0 Respiratory 0� Exercise Test
~ •:0 Musculoskeletal 0� X·Ray 0 Hemoglobin 0 Urinalysis
I
0 Other 0 Other
o Based upon a current review of health status. _
o ________________ is considered suitable for: o o o Unrestricted ActivitY
o Progressive Exercise Program
o with no restrictions/special exercises
o with avoidance of� _Most adults are able to readily participate in physical activity and fitness programs.�
PAR·Q by itself is adequate for the majority of adults. However. some may require�
J medical evaluation and specific advice (exercise prescription!.�
o with addition of� _
PAR·X is an exercise·specific checklist for clinical use for persons with positive
responses to PAR·Q or when further evaluation is otherwise warranted. In addition. o Only a medically supervised exercise program until furtherPAR·X can serve as a permanent record. Its use is self explanatory.
medical clearance
o Physiotherapy
FOllowing evaluation. generally a PLAN is devised for the patient by the examining� Special Concerns lif anyl:�physician. To assist in this. three additional sections are provided:
•� PHYSICAL ACTIVITY RECOMMENDATIONS (overleaf) with selected�
advice and pointers for most adults who are suited to participate in any�
activity and/or a progressive exercise conditioning program.� ________________ M.D.
•� PHYSICAL ACTIVITY PRESCRIPTIONS (PAR x overleaf) is a chart·type
checklist� of conditions requiring special medical consideration and management. _______________ 19 _
•� PHYSICAL ACTIVITY READINESS form (to right) is an optional tear·off tab (D~t")
for verifying clearance. restrictions. etc.• or for making a referral.
Further Information:
o Attached
o To Be Forwarded '''A·a. PAR-X and PAR" were dey. loped by th' 8rltl$t\ Colum~i. D.~rtm.nt of Health. They wert�
eor,Cl!OtUilliZf'd and critIqued by the Multtdisciplin...-y AdYlsory BOilrd on EXlfciselMABEL Translaflon,� o Available Upon RequestrtorOdUCtion and use of tich in its .ntirety is .ncouraQed.