mechanisms of atrial flutter —from macwilliam in 1887 to miyauchi in 2005—
TRANSCRIPT

Mechanisms of Atrial Flutter—From MacWilliam in 1887 to Miyauchi in 2005—
Hrayr S Karagueuzian MD, Peng-Sheng Chen MD, William J Mandel MD
Division of Cardiology, Cedars-Sinai Medical Center, Department of Medicine, David Geffen School of
Medicine at UCLA, Los Angeles, California, USA
(J Arrhythmia 2006; 22: 4–18)
This paper reviews some of the major advancesmade in experimental and clinical studies thatprovided insights into the mechanisms of sustainedand stable atrial flutter in man (AFL).
Early Experimental Findings
John Alexander MacWilliam in 1887 was prob-ably the first to describe the abnormal atrial rhythmknown as atrial flutter. His work opened the way ofcorrelating clinical electrocardiography with theactual visualization of the abnormal beating in thehearts of experimental animals. In his 1887 article inthe Journal of Physiology he described the electri-cally-induced atria arrhythmias this way:
‘‘The application of the current sets the auriclesinto a rapid flutter, the rapidity of which largelydepends upon the excitability of the auricular tissueand the strength of the current employed. Themovements are regular; they seem to consist of aseries of contraction originating in the stimulatedareas and then spreading over the rest of the tissues.The movement does not show any distinct sign ofinco-ordination, it looks like a rapid series ofcontraction waves passing over the auricularwalls.’’1) McWilliam also tested the influence ofvagal stimulation on AFL and found that ‘‘thefluttering movement of the auricles can be checkedor arrested by the influence of the vagus nerve.’’1)
Most interestingly, McWilliam was perhaps the firstto observe an association between cardiac mechan-ical and electrical activity in the maintenance of an
arrhythmia: ‘‘The vagus influence appears to act byweakening the individual contractions [of the atria]to the point of invisibility.’’1)
It was clear from the MacWilliam’s work thatAFL was a rapid (�300 to 400 beats/min) yet aregular rhythm that could be sustained over the atriacausing rapid and regular series of contractions.When Einthoven first introduced the ECG recordingtechnique in man in 1906, he made an actualelectrocardiographic recording of AFL.2) However,it was Sir Thomas Lewis 1909 who recorded a casein a dog of AFL alternating with atrial fibrillation(AF) that he called ‘‘auricular paroxysmal tachycar-dia.’’3) It was only in 1911, that Jolly and Ritchieapplied the term ‘‘auricular flutter’’ to the clinicalarrhythmia in man and described the characteristic‘‘sawtooth waves’’ in the inferior ECG leads.4) Twoyears later, Sir Thomas Lewis established thediagnostic criteria of electrocardiographic of AFLas ‘‘the restless, sawtooth baseline’’5) now known asthe F waves, which today are recognized as theprincipal criterion for the diagnosis of AFL in man.6)
The recognition and the electrocardiographicdescription of this arrhythmia led to intense effortsto determine the mechanism of the AFL that stillcontinues today. It was in 1920 that Lewis and hiscolleagues provided the first mechanistic insight intothe reentrant excitation pattern causing AFL that inmany ways is still valid today. Lewis’ originaldescription of the AFL reads as follows: ‘‘A mainexcitation wave is propagated through the flutteringauricles via a narrow circular pathway embracing
Address for correspondence: Hrayr S Karagueuzian PhD, Sr. Research Scientist, Division of Cardiology, Cedars-Sinai Medical Center,
Professor of Medicine, David Geffen School of Medicine at UCLA. Tel: 310-423-7768 Fax: 310-423-0291
Email: [email protected]
4
J Arrhythmia Vol 22 No 1 2006
Review Article

the two venae cavae; the main wave pursues aunidirectional course and re-enters the originalpathway upon the completion of each circuit.’’7,8)
However, the AFL that Lewis and his colleaguesinduced was short-lived and the number of recordingelectrodes limited, this necessitated much extrapola-tion for the full and complete reconstruction of thereentrant pathway in the atria.
Further insight into the potential mechanisms ofAFL was later provided by the important experi-ments of Brams and Katz in 1932 who have causedsurgical separation of the dog’s right and left atriaand demonstrated that AFL could still be inducedeither in the isolated right or the isolated leftatrium.9) These studies were aimed at determiningif a single and unique right or left atrial focus(reentry or otherwise) was responsible for causingAFL. These authors concluded that: ‘‘Such resultsare obviously incompatible with any theory thatflutter or fibrillation in heart is due to a single focusor a single circus ring sending centrifugal waves intothe other auricles.’’9)
In all of these previous experiments AFL wasinduced by Faradic shocks in otherwise normal atria.AFL induced in this way was short lived. Thisclearly limited investigators because detailed studiesof the arrhythmia requires long periods of stableAFL to allow detailed activation mapping to bemade. This necessitated efforts to develop animalmodels that promote long lasting and stable AFL.Motivated by the desire of maintaining the AFL forlonger duration and better characterization of themechanism and sequence of activation during theAFL, Rosenblueth and Garcia Ramos created asurgical lesion between the SVC and IVC. Theysuggested that the AFL might be sustained by areentrant wavefront around the anatomical obstaclecaused by a surgical lesion. In their originaldescription of the AFL in dogs they observed: ‘‘Upto now the study of flutter has been handicapped bythe rarety of occurrence of long-lasting flutter innormal auricles. Following the simple techniquewhich we have described, flutter episodes mayalways be readily initiated they will usually persistindefinitely and can thus be observed at length; theycan be extinguished at will, if necessary fore thepurposes of the experiment.’’10) These authors alsoshowed that there was no need for the obstacle to beanatomic. They created functional conduction blockbetween the IVC and the SVC by topical applicationof the local anesthetic, cocaine and showed that thecircus movement activation around either the func-tional site of block (local cocaine-induced) or crushinjury (surgical incision) could still induce AFL.10)
They concluded that all that was required to initiateAFL was the presence of conduction block of theactivation front across the crista terminalis, perpen-dicular to the IVC-SVC axis, which could thenpropagate by either clockwise or counterclockwisedirection around the crista causing AFL. Theseauthors also demonstrated that the AFL could beentrained or terminated by electrical pacing and alsocould be terminated by crushing the isthmus over thetricuspid valve (TV) annulus.10) In addition theseauthors presented evidence that a portion of thepathway extended along the crista at the cavaljunction with the right atrial free wall, by showingthat extending the lesion across this region increasedthe flutter cycle length. In other experiments, whenthey made an incision extending from the intercavallesion across the crista all the way to the AV ring,AFL stopped and could not be reinitiated. Finally,these authors showed that the AFL cycle decreasedby the administration of adrenaline and to a lesserextent during vagal stimulation.10) Clearly, the slightacceleration of the flutter rate with vagal stimulation,was an argument against automatic mechanism forthe AFL because vagal activation is known to slowand inhibit all forms of automatic activity. However,the portion of the presumed reentry pathway over theposterior wall of the left atrium was not observed bylater similar experiments by Kimura et al. (1954),Takaysau et al. (1958) and Hayden et al. (1967).These authors demonstrated progressive delay ofactivation times over the left epicardial surface, afinding that does not prove that this activationsequence represents wave propagation in a portion ofthe primary reentrant circuit.11)
The issue of a focal perhaps an automaticmechanism as a cause of AFL was rigorouslypromoted by Prinzmetal and associates in 1950.These authors using high speed cinematography (upto 2,000 frames per second), cathode-ray oscillo-scope and multiple-channel electrocardiography in-sisted that AFL occurs from one ectopic focus anddismissed circus movement reentry as a mechanismof AFL.12) A major cause of this seeming discrep-ancy (focal vs. circus movement) stems from the factthat Prinzmetal and associates used local injection ofaconitine to induce AFL. Aconitine is a drug thatprevents sodium channel inactivation causing repet-itive depolarizations of the kind of early afterdepo-larization-induced triggered activity. According totheir original description: ‘‘When auricular flutter isproduced by applying aconitine locally at the centerof the wall of the right auricle, the contraction wavesare seen to originate at the ectopic focus in aperfectly rhythmic manner, and to spread over the
Karagueuzian HS Mechanisms of atrial flutter
5

auricles in all directions at once. It thus appearsclear that the mechanism of auricular flutter is not acircus movement; for if it were, the contraction wavewould have to pursue a unidirectional path aroundthe cavae. The films show that this is not the case;each contraction wave takes its origin at the ectopicfocus, and, instead of traversing the auricles in asingle direction, actually spreads from the focussimultaneously in all directions. The visual obser-vations disprove the circus movement theory ofauricular flutter and establish the tree nature of theauricular tachycardia.’’12) While it is possible thataconitine-induced AFL may be focal it is howeverunlikely that this AFL model is the clinical counter-part of all forms of AFL in man.
Recent Findings
A case can be made for focal mechanism for sometypes of human AFL as increasing evidence supportsthe idea that the myocardial cells in the atrial venoussystem manifest increased susceptibility to after-potentials and triggered activity. In such cases rapidfocal activity may conceivably cause AFL-likeactivity should triggered activity remain stable andsupported by a single wavefront. The work of Rosenand his associates in 1969 demonstrated that pacingfrom the coronary sinus at rates similar to the AFLrate mimicked AFL in man.13) This isolated findingwas of some interest because of the later demon-stration by Wit and associated14) that the cardiacfibers in the canine coronary sinus may initiatetriggered activity at rates that might drive the atriarapidly simulating clinical AFL. It is thereforepossible that under certain conditions focal activity,such as triggered activity in the coronary sinus,might be a mechanism for at some types of AFL inman.
The mechanism of AFL in humans was studiedmore extensively by Puech and his collaborators in1970 at Montpelier Clinic in France. Using esoph-ageal and atrial endocardial activation mapping withmultipolar (ten) electrode catheters, this pioneeringstudy, reporting experience on 55 patients over a 15year period (1955 to 1970) provided much insightinto the mechanisms of AFL in man.15) Theseauthors defined AFL as an atrial rhythm at ratesranging between 230 beat/min to 330 beat/min(atrial cycle lengths of 260ms to 180ms) andassociated with 2:1 or higher degrees of AV block.15)
These authors first dismissed Prinzmetal’s focaltheory of AFL as being of an ‘‘extremely simplisticcharacter’’ and asserted with their mapping data thatthe most commonly occurring AFL in man resulted
from a reentrant waves of excitation in the rightatrium that rotated counterclockwise along the cristaterminalis.15) These authors also found the lesscommon form of AFL (only one case) in whomthe rotation of the reentrant wavefronts was clock-wise.15) The occurrence of AFL with a focalmechanisms or reentry located in the left atriumwas rather a rare phenomenon in Puech’s report.15)
Attempts to terminate AFL with pacing failed in thehands of these French investigators, perhaps due tothe application of relatively low current strengths ofstimulation.16) Pacing at rates faster than the AFLrate converted the AFL to AF in few cases withsubsequent (minutes to hours later) resumption of theoriginal AFL.15) With the report of Puech andassociates it became clear that macro-reentry in theright atrium is a common mechanism of AFL in man.More thorough endocardial mapping of human type1 atrial flutter was carried by Feld and associates.17)
These authors using catheter ablation technique,endocardial mapping and entrainment pace mappingduring AFL (mean cycle length of 253� 39msec)determined the critical site for the maintenance ofAFL in order to ablate it and cure the arrhythmia.The critical site of the reentry circuit consisted of anarea of slow conduction, and the exit site from thearea of slow conduction. These authors found acounterclockwise reentrant wave during the AFLthat originated just inferior or posterior to thecoronary sinus ostium, proceeded superiorly in theatrial septum to the right atrial free wall, theninferiorly toward the tricuspid annulus and finallymedially between the inferior vena cava and thetricuspid annulus, where low-amplitude fragmentedelectrical activity was noted. Entrainment pacemapping from this area produced an exact P wavematch to atrial flutter on 12-lead ECG with a long(greater than 40msec) stimulus-to-P interval indi-cated slow conduction, whereas pacing just inferioror posterior to the coronary sinus ostium produced anexact P wave match with a short stimulus-to-Pinterval (less than 40msec), presumably identifyingthe exit site from the area of slow conduction.Radiofrequency ablation of this critical site termi-nated and prevented the reinduction of AFL in 70 percent of the patients. Sites where ablation wassuccessful, were located just inferior or posterior tothe coronary sinus ostium and were characterized bydiscrete electrograms with activation times of �20 to�50msec before P wave onset and exact entrain-ment pace maps with a stimulus-to-P interval of 20to 40msec, consistent with the exit site from the areaof slow conduction.17) These authors concluded thatradiofrequency energy applied to a critical area in
J Arrhythmia Vol 22 No 1 2006
6

AFL reentrant circuit, inferior or posterior to thecoronary sinus ostium, terminates and preventsarrhythmia reinduction.17) Similar findings were alsoobserved by Cosio and associates18) who have shownthat radiofrequency ablation of the inferior venacava-tricuspid valve isthmus was an effective pro-cedure in terminating and preventing reinduction ofin common AFL in humans.
The Era of Computerized Mapping
Since the 1980s when computer-assisted cardiacmapping technology became available and whennewer animal models of AFL were developed,detailed analysis and greater insight of AFL mech-anism became possible. A prelude to AFL studiesusing a large number of electrodes was first made byBoineau and associates in a dog with spontaneousand inducible AFL resembling typical and atypicalhuman AFL. Using up to 96 epicardial atrial bipolarelectrodes these authors not only mapped thesequence of activation during AFL but also con-structed maps of refractory period distribution of themapped atrium. These studies concluded that AFLwas caused by a circus conduction pattern on the freewall of the right atrium and was the result of a‘‘nonuniform bimodal refractory state of the atriumthat simultaneously exerted a blocking effect whilepermitting conduction and complex shaping of theunblocked wave, which was routed back to the itssite of origin.’’19) These authors further concludedthat for AFL to occur three interacting factors werenecessary: first, an ectopic atrial beat, second,nonuniform distribution of atrial refractory periodscharacterized by a bimodal distribution with closeproximity of the regions of longest and shortestrefractory periods, and three, slow conduction of thewave initiated by the ectopic atrial beat.19) Accord-ing to these authors, the paroxysmal nature of theAFL was related to the changing nature of atrialrefractoriness (dynamic heterogeneity) and atrialectopic activity which in these authors words ‘‘areextremely labile and influenced by multiple secon-dary factors and tertiary factors’’ like the ‘‘auto-nomic nervous system’’ and ‘‘a particular distribu-tion of the refractory field.’’19) Bioineau later refinedhis assessment of AFL mechanism and gave a primalrole to the tricuspid annulus in the reentry by stating:‘‘The tricuspid annulus forms an integral anteriorcomponent of the circular reentrant surface.’’20)
The study by Hoffman’s group at ColumbiaUniversity of the circular movement during lesion-based stable AFL, confirmed some of Boineau’sfindings, i.e., the role of the anterior tricuspid
annulus as a component of the reentry circuit.However, perhaps most importantly their study casta whole new way of interpreting the mechanism andthe primary location of reentrant activation byintroducing the phenomenon of outward secondaryspread of excitation from a primary focus or ‘‘rotor’’a term later coined by Winfree.21) In this respectFrame et al. in a series of elegant Y-lesion basedexperiments, originally introduced by Resebluethand Garcia Ramos, have shown both in intact heartsand in isolated tricuspid ring preparations in vitrothat the induced AFL was caused by a reentrantimpulse that circulated around the tricuspid valveorifice in either a clockwise or counter-clockwisedirection.11,22) The Y-shaped lesion in the Frame at alstudies was caused by one incision made betweenthe cava and the second lesion, connected to the first,extended intro a portion of the free wall of the rightatrium.22) These authors found no discrete segmentof markedly slow conduction in the reentrant circuitaround the ring and cutting a portion of the ringterminated the rhythm and prevented its reinduction.Most interestingly the reentry, albeit at slower rate,was also induced in atrial tissue surrounding thetricuspid orifice when this structure was isolated andsuperfused in vitro.11) This study introduced a newconcept of the pattern of reentrant excitation,originally described in chemical reactions by Win-free.23) According to this dynamic scenario rotationaround a relatively small core (functional or ana-tomical) sends an outwardly propagating wave thatenvelops a larger body of atrial tissue giving theimpression of a larger (primary) reentrant circuitthan the actual primary size of the reentry (seeFigure 1). This scenario is also depicted schemati-cally based on our own observations on reentry inventricular tissue around a core of functional blockwhich is remarkably similar to Frame’s ring tissuereentry around a core of anatomical block (Figure 2).A variant of Frame’s model was introduced Feld etal.24) who have shown that a single linear incisionbetween the IVC and SVC (‘‘crush injury’’) couldcause circus movement activation around the obsta-cle created between the cavae causing AFL in the insitu canine hearts. These authors did not suggestreentry to be sustained around the tricuspid ring aswas suggested by Frame et al. A possible explan-ation of the difference between these two studies, assuggested by Frame et al., may result from the abilityof the Y-shaped lesion to provide a ‘‘protectivebarrier’’ for the impulse to travel around the ring,which these authors insisted was the primaryanatomical obstacle around which the wave circu-lated. The ‘‘secondary’’ lesions caused by the Y-
Karagueuzian HS Mechanisms of atrial flutter
7
incision served, according to these authors, as pureprotective barriers to prevent short-circuiting and/orpremature interruption of the reentrant activa-tion.11,22)
A new model of canine AFL was developed in1986 by Waldo and associates using the method ofpostpericardiotomy pericarditis.25) Using sterile tech-niques, the pericardium was opened by way of aright thoracotomy, the atrial surfaces were gener-ously dusted with talcum powder and a single layerof gauze was placed on the free left and right atrialwalls. The dogs were allowed to recover and AFLwas readily induced in this model in the conscious,nonsedated state. These authors using 372 unipolarelectrodes arranged in 186 bipolar pairs concludedthat AFL was caused by a reentrant excitation thatalways included a septal component, did not alwaysrequire a right atrial free wall reentrant circuit andwas associated with a line of functional conductionblock in the right atrial free wall.16,26) The tricuspidring annulus was not the primary site of rotationduring AFL in Waldo’s model. These authors furthershowed that that a positive flutter wave in ECG leadII (counterclockwise circus movement) was associ-ated with early activation of the Bachmann’s bundleregion compared with the posteroinferior left atriumand a negative flutter was associated with the earlyactivation of the posteroinferior left atrium com-
pared with Bachmann’s bundle and activation of aconsiderable portion of the left atrium in aninferosuperior direction (clockwise circus move-ment).27) The studies of Waldo’s group on sterilepericarditis and that of Boineau’s in a dog withnaturally occurring AFL emphasized that myocardialdiscontinuity between the caval orifices and slowconduction form together the principal obstaclearound which the flutter wave circulates and wereconsidered by these investigators to play a decisiverole in the maintenance of AFL.
The functional reentrant excitation in atrial tissuefirst described by Allessie et al. known as the‘‘leading circle’’28,29) is in line with subsequentdevelopments and elucidation of the mechanism offunctional reentry that became also known as‘‘rotor’’21) or ‘‘spiral wave.’’30) We found that func-tional reentry in atrial tissue is also consistent withthe spiral wave mechanism of excitation with anexcitable but non-excited core.31) The spiral waveonce induced is often unstable and moves from onesite to another (meandering)32) with a tendency toanchor to an anatomical obstacles of suitable size(i.e., equal or greater than 10mm diameter).33)
Smaller sized obstacles were ineffective in causingstable spiral attachment.33) In this respect it ispossible that in the Frame et al. studies a reentrantwavefront could have be induced in the first place
A B
TOTO
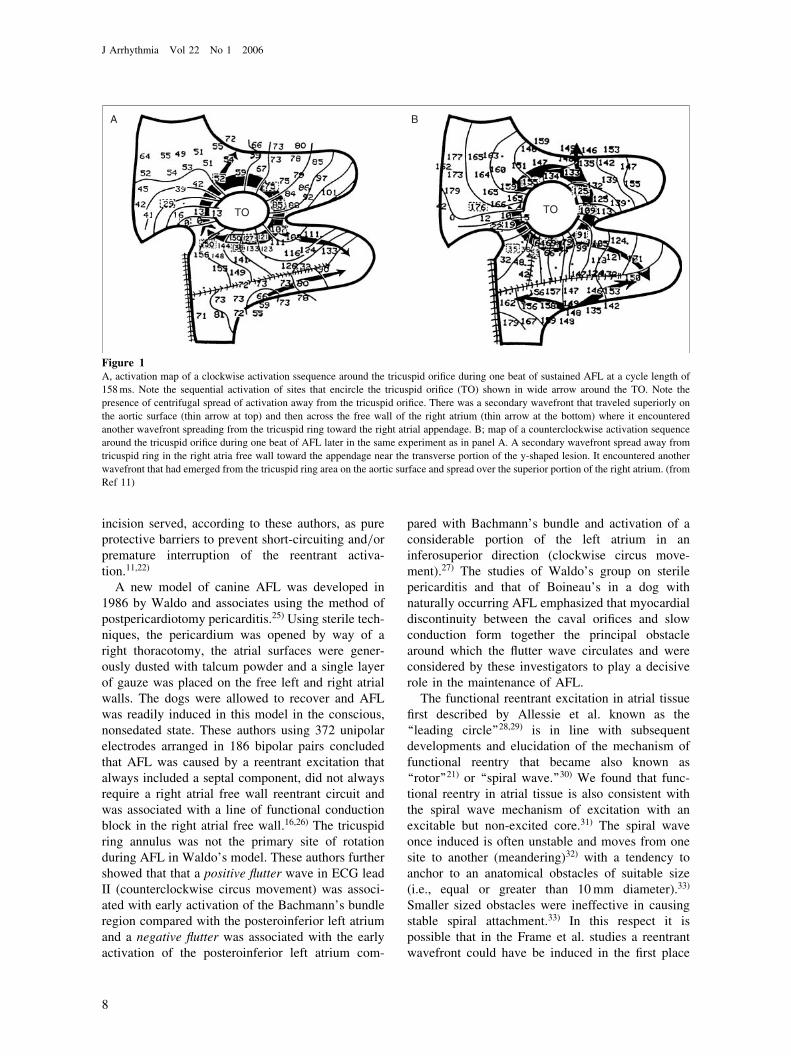
Figure 1A, activation map of a clockwise activation ssequence around the tricuspid orifice during one beat of sustained AFL at a cycle length of
158ms. Note the sequential activation of sites that encircle the tricuspid orifice (TO) shown in wide arrow around the TO. Note the
presence of centrifugal spread of activation away from the tricuspid orifice. There was a secondary wavefront that traveled superiorly on
the aortic surface (thin arrow at top) and then across the free wall of the right atrium (thin arrow at the bottom) where it encountered
another wavefront spreading from the tricuspid ring toward the right atrial appendage. B; map of a counterclockwise activation sequence
around the tricuspid orifice during one beat of AFL later in the same experiment as in panel A. A secondary wavefront spread away from
tricuspid ring in the right atria free wall toward the appendage near the transverse portion of the y-shaped lesion. It encountered another
wavefront that had emerged from the tricuspid ring area on the aortic surface and spread over the superior portion of the right atrium. (from
Ref 11)
J Arrhythmia Vol 22 No 1 2006
8
during programmed stimulation and that such aspiral could have anchored around the tricuspid ring,that is typically larger than 10mm in diameter,11)
causing stable spiral attachment rotation around thering. When this happened an outward spread of thefront from the ring took place giving the impressionof a larger macroreentrant circuit. Consequently, it islikely, at least during some of the episode that theAFL model induced in the Y-lesion configurationmay cause AFL by reentry around the ring as theprimary site of the reentry. Most importantly how-
ever and with much clinical impact, whether fullrotation occurs around the ring or it occurs fullyaround the crista, both of these circuits have acommon atrial anatomical path located between theIVC and the tricuspid ring, the right atrial isthmus.This isthmus is a critical part of the AFL reentrycircuit regardless of the primary location of thereentry (ring vs. crista) as its disruption is associatedwith termination of AFL and inability to reinitiate it.In the Y-shaped lesion model of canine AFL, asuggested counterpart of the common AFL in man34)
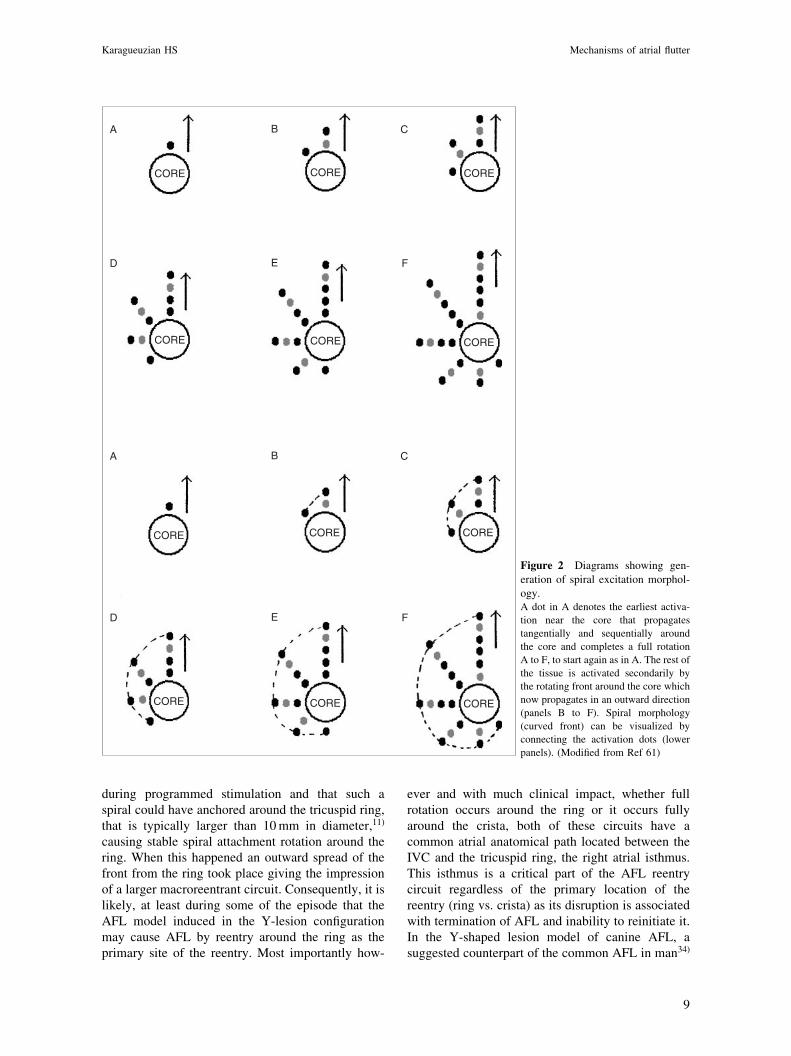
Figure 2 Diagrams showing gen-
eration of spiral excitation morphol-ogy.A dot in A denotes the earliest activa-
tion near the core that propagates
tangentially and sequentially around
the core and completes a full rotation
A to F, to start again as in A. The rest of
the tissue is activated secondarily by
the rotating front around the core which
now propagates in an outward direction
(panels B to F). Spiral morphology
(curved front) can be visualized by
connecting the activation dots (lower
panels). (Modified from Ref 61)
CORE CORE CORE
CORECORECORE
CORE CORE CORE
CORECORECORE
A B C
A B C
D E F
D E F
Karagueuzian HS Mechanisms of atrial flutter
9

interruption of the anterior portion of the ring(isthmus) caused termination of the AFL.34)
Boyden introduced a different model of AFLassociated with chronic right atrial enlargement,atrial hypertrophy and increased interstitial atrialfibrosis. These structural abnormalities were inducedby surgically creating tricuspid regurgitation andbanding of the pulmonary artery in the doghearts.35,36) Using 192 pairs of recording electrodesthe total endocardial activation of both atria duringelectrically-induced AFL were determined. Reen-trant pattern of activation, in either clockwise orcounterclockwise pattern were demonstrated duringepisodes of induced stable AFL. An area of func-tional block was found to be necessary as anessential component of reentry in this canine modelof inducible AFL with structurally remodeledhearts.36)
Miyauchi Canine Model of AFL
While most if not all previous experimental AFLrelied on surgically creating lesions in order toinduce stable, long lasting AFL, much of themechanisms of AFL in man, perhaps with theexception of AFL in some post-op patients, isfunctionally based and often does not involveanatomical lesions. We recently developed a newmodel of AFL37) that resembles the common type ofAFL in man without causing surgical lesions. In thismodel, using high resolution electrode mappingtechnique in the in situ hearts we discovered thatthe ‘‘natural’’ evolution of chronic ventricular my-ocardial infarction and chronic nicotine administra-tion promotes intense right atrial interstitial fibrosis.This leads to flattening of the atrial electricalrestitution curve which leads to stable and sustainedreentry around the crista terminalis causing AFL andoften requiring electrical shock for termination.Because of the great similarity of AFL in this modelto human AFL, both in terms of mechanism andresponse to pacing and catheter-based RF ablation ofthe right atrial isthmus, we will describe this modelin some detail.
The Rational of the Model
Epidemiological studies have shown that smokingpromotes myocardial infarction and is a major causeof chronic obstructive pulmonary disease (COPD) inthe U.S.38) COPD is shown to be an independentpredictor of AFL.39) Since nicotine is a majorconstituent of tobacco smoke and an agent thoughtto be the culprit of cardiac arrhythmias40) we testedthe hypothesis that the combined presence of chronic
myocardial infarction (MI) and nicotine promotesAFL in intact canine hearts.37) MI was created byligating the left anterior descending coronary arteryjust distal to the first diagonal branch as described byMiyauchi et al.41) In the second group after creatingan MI, mini osmotic pumps were implanted s.q. tocontinuously deliver 5mg/kg/day of nicotine for aone month period. This dose of nicotine correspondsto the daily intake of nicotine by heavy smokers.42,43)
In the third group, thoracotomy was performed andtwo nicotine loaded pumps implanted s.q. with noMI and finally a fourth group received no surgeryand no nicotine.
AFL Characteristics
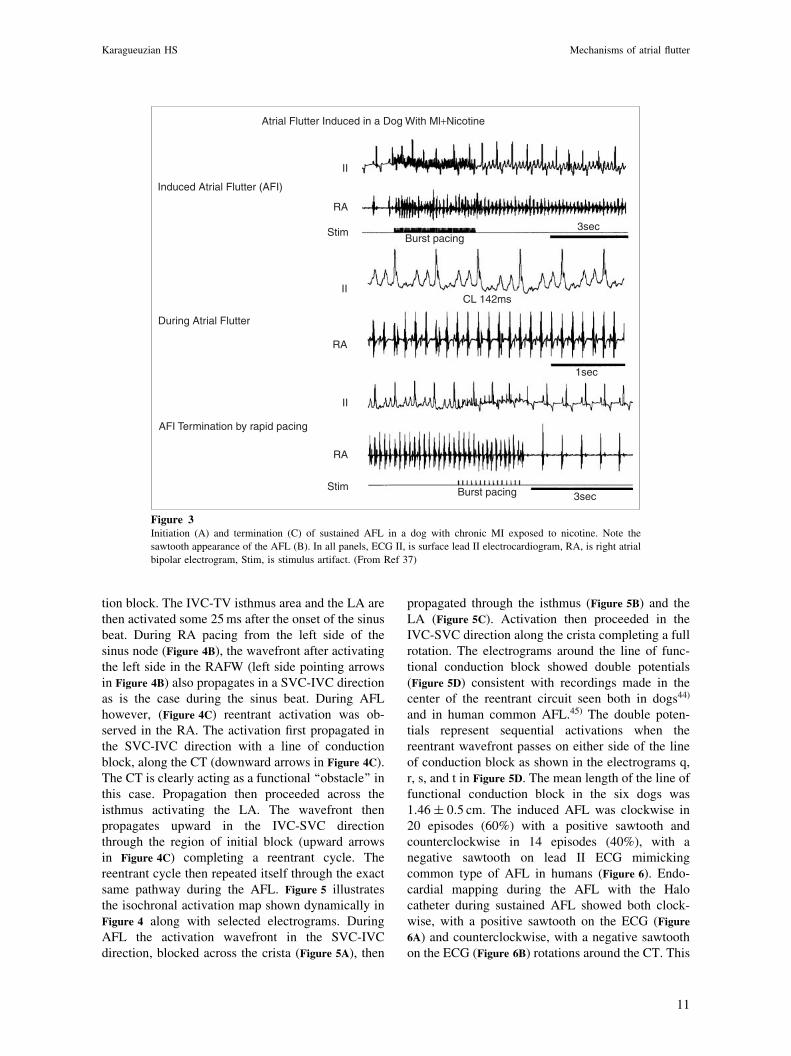
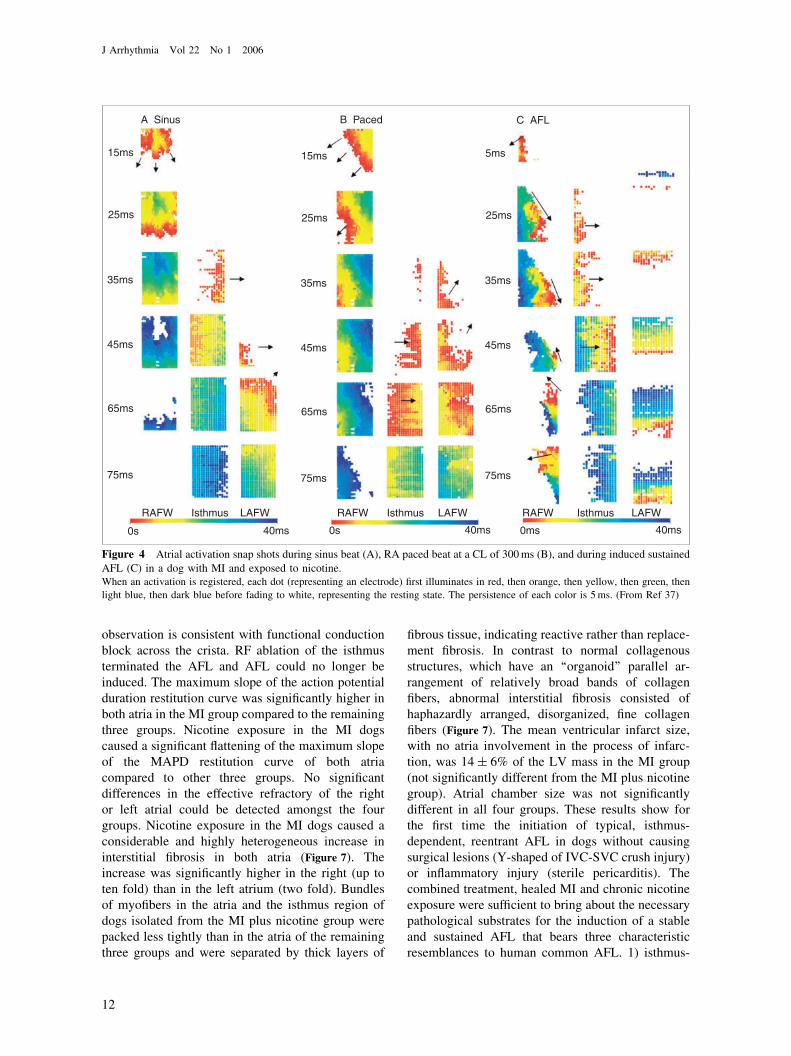
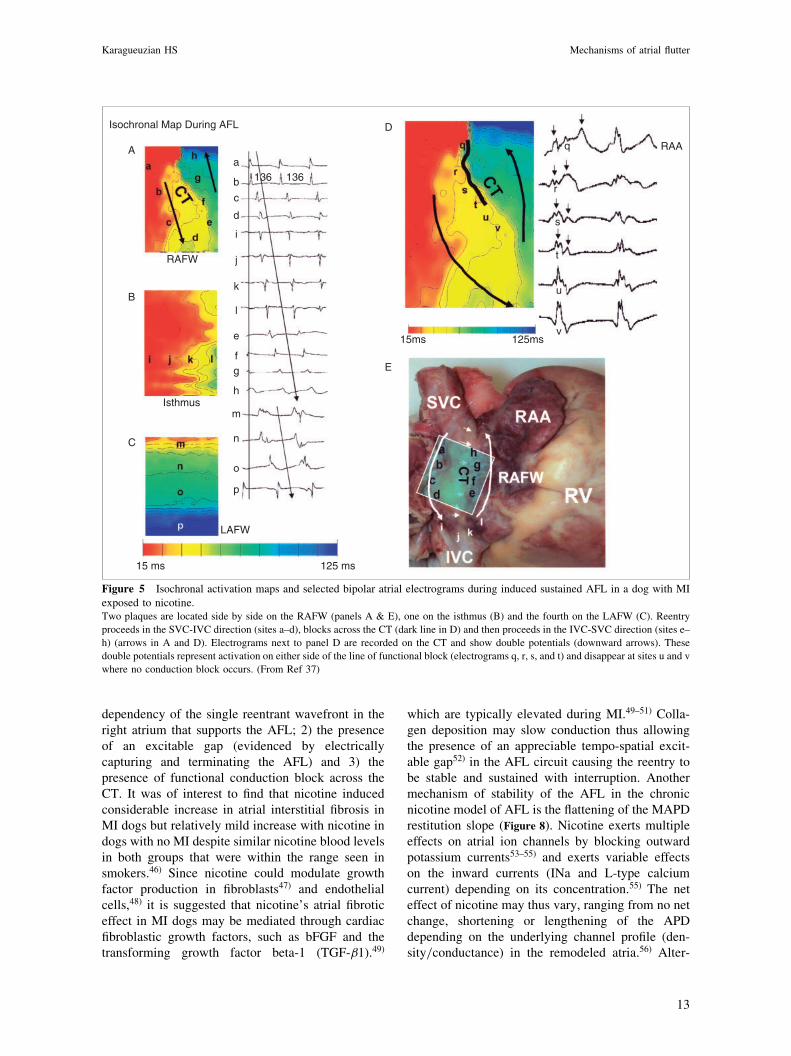
Vulnerability to AFL was tested by programmedelectrical stimulation and the resultant arrhythmiawas mapped epicardially using 1,792 bipolar elec-trodes distributed over four plaques (1.5 by 2.7 cm)with a spatial resolution of 1-mm.41) The plaqueswere placed on both atrial epicardial surfaces. Twoplaques were sutured side by side on the right atrialfree wall (RAFW) and the crista terminalis (CT)region. The third was sutured on the LA free wall(LAFW) and the fourth, in the isthmus areaencompassing the inferior vena cava (IVC) and thetricuspid annulus (TA). We also did simultaneousepicardial (1,792 electrodes) and endocardial (Halocatheter with 20 electrodes) mapping during ablationof the AFL with radiofrequency energy (30W for30–60 s). Atrial monophasic action potentials andelectrical restitution curves were constructed usingthe dynamic pacing protocol.37,41) The results haveshown that either burst or atrial pacing at CLs of200–150ms induces sustained AFL at a mean CL of134� 10ms in the MI dogs exposed to chronicnicotine administration (Figure 3). The induced AFLhad the characteristic sawtooth appearance on ECGlead II (Figure 3). The AFL lasted for more than30min requiring electrical cardioversion for termi-nation. Pacing the atria at CLs shorter (114� 9ms)than the CL of the AFL however could alsoterminate the AFL (Figure 3). Ability to prematurelycapture the AFL with subsequent termination indi-cates the presence of an excitable gap in the AFLcircuit. No AFL could be induced in any of the dogsin the remaining 3 groups. Figure 4 shows thedynamic atrial activation pattern: 1) during sinusrhythm, 2) during atrial pacing and 3) during aninduced sustained AFL in a dog with MI andexposed to chronic nicotine adminstration. Duringsinus rhythm (Figure 4A), the activation propagatesfrom the upper towards the lower RA and fullyactivates the entire RA without undergoing conduc-
J Arrhythmia Vol 22 No 1 2006
10
tion block. The IVC-TV isthmus area and the LA arethen activated some 25ms after the onset of the sinusbeat. During RA pacing from the left side of thesinus node (Figure 4B), the wavefront after activatingthe left side in the RAFW (left side pointing arrowsin Figure 4B) also propagates in a SVC-IVC directionas is the case during the sinus beat. During AFLhowever, (Figure 4C) reentrant activation was ob-served in the RA. The activation first propagated inthe SVC-IVC direction with a line of conductionblock, along the CT (downward arrows in Figure 4C).The CT is clearly acting as a functional ‘‘obstacle’’ inthis case. Propagation then proceeded across theisthmus activating the LA. The wavefront thenpropagates upward in the IVC-SVC directionthrough the region of initial block (upward arrowsin Figure 4C) completing a reentrant cycle. Thereentrant cycle then repeated itself through the exactsame pathway during the AFL. Figure 5 illustratesthe isochronal activation map shown dynamically inFigure 4 along with selected electrograms. DuringAFL the activation wavefront in the SVC-IVCdirection, blocked across the crista (Figure 5A), then
propagated through the isthmus (Figure 5B) and theLA (Figure 5C). Activation then proceeded in theIVC-SVC direction along the crista completing a fullrotation. The electrograms around the line of func-tional conduction block showed double potentials(Figure 5D) consistent with recordings made in thecenter of the reentrant circuit seen both in dogs44)
and in human common AFL.45) The double poten-tials represent sequential activations when thereentrant wavefront passes on either side of the lineof conduction block as shown in the electrograms q,r, s, and t in Figure 5D. The mean length of the line offunctional conduction block in the six dogs was1:46� 0:5 cm. The induced AFL was clockwise in20 episodes (60%) with a positive sawtooth andcounterclockwise in 14 episodes (40%), with anegative sawtooth on lead II ECG mimickingcommon type of AFL in humans (Figure 6). Endo-cardial mapping during the AFL with the Halocatheter during sustained AFL showed both clock-wise, with a positive sawtooth on the ECG (Figure6A) and counterclockwise, with a negative sawtoothon the ECG (Figure 6B) rotations around the CT. This
Atrial Flutter Induced in a Dog With Ml+Nicotine
II
RA
II
RA
Stim
II
RA
Stim
Induced Atrial Flutter (AFI)
During Atrial Flutter
AFI Termination by rapid pacing
Burst pacing
Burst pacing
3sec
3sec
1sec
CL 142ms
Figure 3Initiation (A) and termination (C) of sustained AFL in a dog with chronic MI exposed to nicotine. Note the
sawtooth appearance of the AFL (B). In all panels, ECG II, is surface lead II electrocardiogram, RA, is right atrial
bipolar electrogram, Stim, is stimulus artifact. (From Ref 37)
Karagueuzian HS Mechanisms of atrial flutter
11
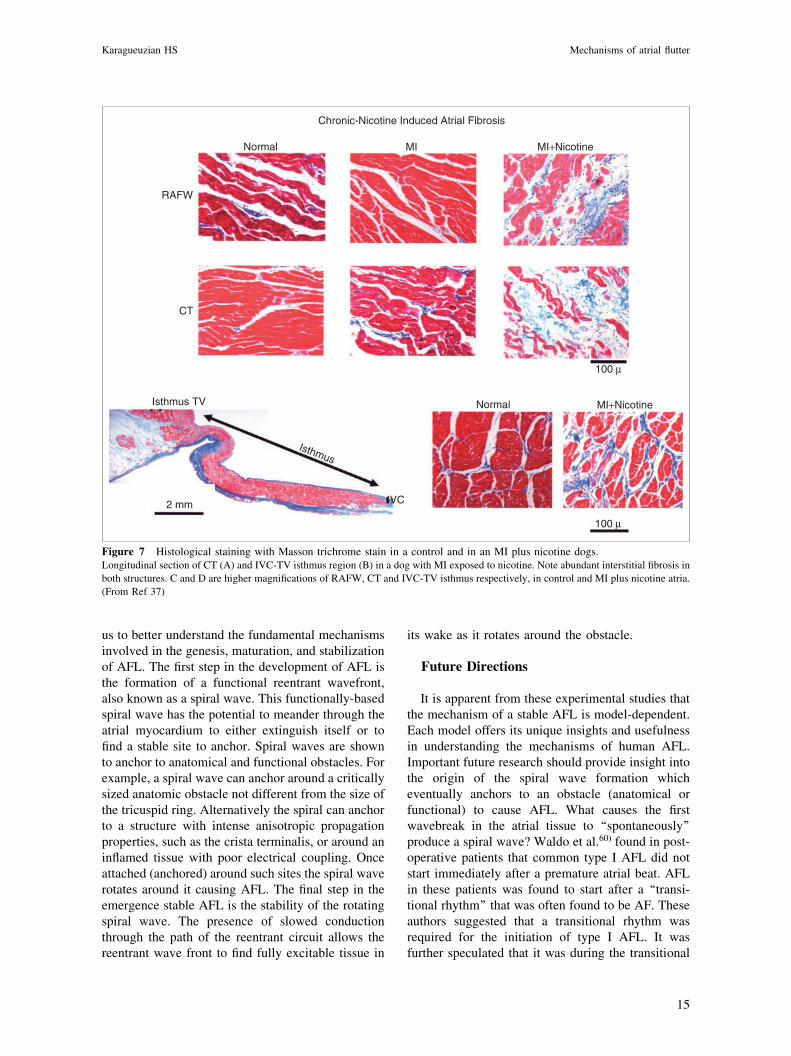
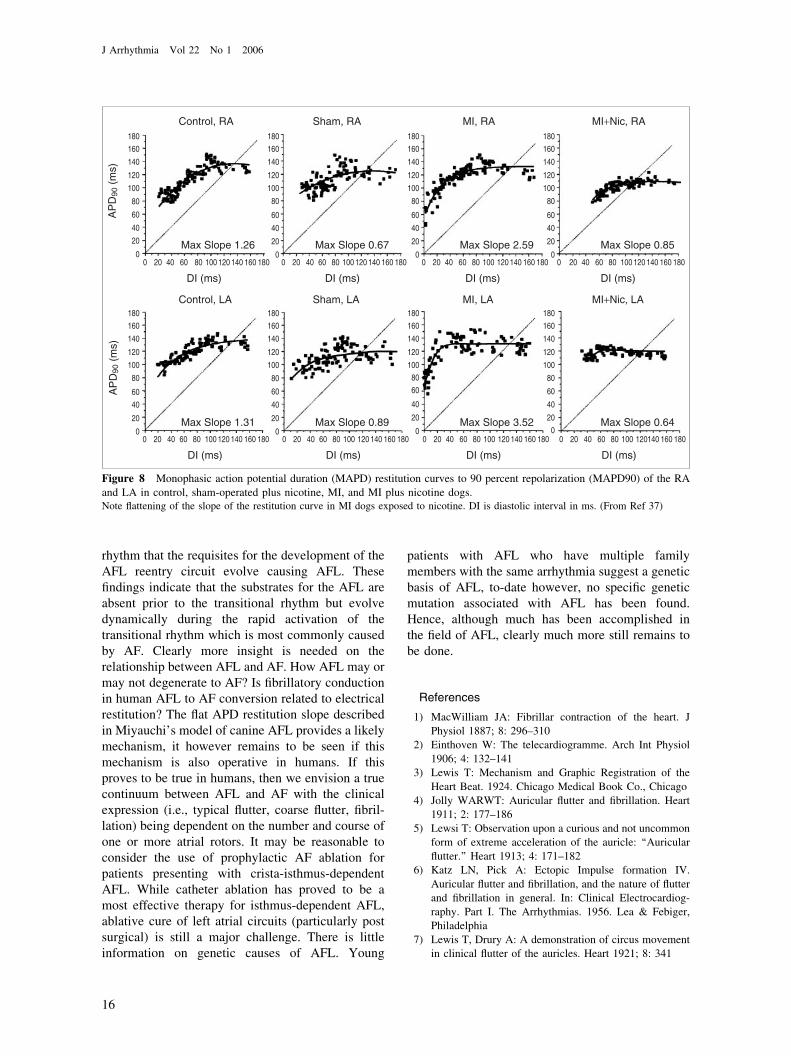
observation is consistent with functional conductionblock across the crista. RF ablation of the isthmusterminated the AFL and AFL could no longer beinduced. The maximum slope of the action potentialduration restitution curve was significantly higher inboth atria in the MI group compared to the remainingthree groups. Nicotine exposure in the MI dogscaused a significant flattening of the maximum slopeof the MAPD restitution curve of both atriacompared to other three groups. No significantdifferences in the effective refractory of the rightor left atrial could be detected amongst the fourgroups. Nicotine exposure in the MI dogs caused aconsiderable and highly heterogeneous increase ininterstitial fibrosis in both atria (Figure 7). Theincrease was significantly higher in the right (up toten fold) than in the left atrium (two fold). Bundlesof myofibers in the atria and the isthmus region ofdogs isolated from the MI plus nicotine group werepacked less tightly than in the atria of the remainingthree groups and were separated by thick layers of
fibrous tissue, indicating reactive rather than replace-ment fibrosis. In contrast to normal collagenousstructures, which have an ‘‘organoid’’ parallel ar-rangement of relatively broad bands of collagenfibers, abnormal interstitial fibrosis consisted ofhaphazardly arranged, disorganized, fine collagenfibers (Figure 7). The mean ventricular infarct size,with no atria involvement in the process of infarc-tion, was 14� 6% of the LV mass in the MI group(not significantly different from the MI plus nicotinegroup). Atrial chamber size was not significantlydifferent in all four groups. These results show forthe first time the initiation of typical, isthmus-dependent, reentrant AFL in dogs without causingsurgical lesions (Y-shaped of IVC-SVC crush injury)or inflammatory injury (sterile pericarditis). Thecombined treatment, healed MI and chronic nicotineexposure were sufficient to bring about the necessarypathological substrates for the induction of a stableand sustained AFL that bears three characteristicresemblances to human common AFL. 1) isthmus-
A Sinus B Paced C AFL
15ms
25ms
35ms
45ms
65ms
75ms
15ms
25ms
35ms
45ms
65ms
75ms
5ms
25ms
35ms
45ms
65ms
75ms
0s 40ms 0s 40ms 0ms 40ms
RAFW LAFWIsthmus RAFW LAFWIsthmus RAFW LAFWIsthmus
Figure 4 Atrial activation snap shots during sinus beat (A), RA paced beat at a CL of 300ms (B), and during induced sustained
AFL (C) in a dog with MI and exposed to nicotine.When an activation is registered, each dot (representing an electrode) first illuminates in red, then orange, then yellow, then green, then
light blue, then dark blue before fading to white, representing the resting state. The persistence of each color is 5ms. (From Ref 37)
J Arrhythmia Vol 22 No 1 2006
12
dependency of the single reentrant wavefront in theright atrium that supports the AFL; 2) the presenceof an excitable gap (evidenced by electricallycapturing and terminating the AFL) and 3) thepresence of functional conduction block across theCT. It was of interest to find that nicotine inducedconsiderable increase in atrial interstitial fibrosis inMI dogs but relatively mild increase with nicotine indogs with no MI despite similar nicotine blood levelsin both groups that were within the range seen insmokers.46) Since nicotine could modulate growthfactor production in fibroblasts47) and endothelialcells,48) it is suggested that nicotine’s atrial fibroticeffect in MI dogs may be mediated through cardiacfibroblastic growth factors, such as bFGF and thetransforming growth factor beta-1 (TGF-�1).49)
which are typically elevated during MI.49–51) Colla-gen deposition may slow conduction thus allowingthe presence of an appreciable tempo-spatial excit-able gap52) in the AFL circuit causing the reentry tobe stable and sustained with interruption. Anothermechanism of stability of the AFL in the chronicnicotine model of AFL is the flattening of the MAPDrestitution slope (Figure 8). Nicotine exerts multipleeffects on atrial ion channels by blocking outwardpotassium currents53–55) and exerts variable effectson the inward currents (INa and L-type calciumcurrent) depending on its concentration.55) The neteffect of nicotine may thus vary, ranging from no netchange, shortening or lengthening of the APDdepending on the underlying channel profile (den-sity/conductance) in the remodeled atria.56) Alter-
Isochronal Map During AFL
A
D
E
B
C
RAFW
LAFW
Isthmus
15 ms 125 ms
15ms 125ms
136 136a
b
c
d
j
k
l
e
fg
h
m
n
o
p
i
RAAq
r
s
t
u
v
Figure 5 Isochronal activation maps and selected bipolar atrial electrograms during induced sustained AFL in a dog with MIexposed to nicotine.Two plaques are located side by side on the RAFW (panels A & E), one on the isthmus (B) and the fourth on the LAFW (C). Reentry
proceeds in the SVC-IVC direction (sites a–d), blocks across the CT (dark line in D) and then proceeds in the IVC-SVC direction (sites e–
h) (arrows in A and D). Electrograms next to panel D are recorded on the CT and show double potentials (downward arrows). These
double potentials represent activation on either side of the line of functional block (electrograms q, r, s, and t) and disappear at sites u and v
where no conduction block occurs. (From Ref 37)
Karagueuzian HS Mechanisms of atrial flutter
13

natively, nicotine’s flattening effect of the MAPDrestitution may not result from direct ion channeleffect but rather from the inability of the highlyfibrotic right atrial tissue (increased stiffness) todistend (i.e., stretch) at short diastolic intervals.Decreased stretch may decrease APD shortening andthus prevent attainment of ultra short diastolicintervals causing a flat electrical restitution curve.57)
The absence of atrial fibrosis in the MI group forexample, permits stretch to develop during rapidpacing causing shortening of the APD and thus theattainment of ultra short diastolic intervals. Cardiactissue with a flat electrical restitution curve does notundergo wavebreak58) while the partial electricaluncoupling caused by the considerable increase inright atrial fibrosis promotes slow conduction59) thatincreases the excitable gap interval during the flutter.The coexistence of these two electrophysiologicalproperties, uncoupling due to fibrosis and flatteningof the restitution curve are of considerable impor-
tance in the formation of stable reentry and providenovel insight into the pathogenesis of a stable AFLwithout its conversion to AF. The nicotine model ofAFL might provide insight into the mechanisms andperhaps the pathogenesis of human AFL, as inter-stitial fibrosis and flattening of APD restitution curvemay develop in a broad spectrum of diseases,including smoking, heart failure, myocardial infarc-tion, and cardiac hypertrophy. To the extent that thismodel may be representative of human AFL, thecombined development of increased atrial fibrosisand flattened atrial electrical restitution curve mightbe important etiological factors in the pathogenesisof common AFL in man that afflicts some 200,000patients every year in the US.39)
Summary and Concluding Remarks
The experimental insights and the availability ofincreasing and informative human data on AFL led
A
B
Clockwise AFL
Counterclockwise AFL
RAA1
2
3
4
5
67
8
9
5 6
7
8
9
10
CS
RAA
1
2
3
4
1
2
3
4
5
6
78
9
10
10
CS
CS
136 136
100ms
100ms
140 140
CTa
bc
de
f
gh
IVC
1
2
3
4
10
CS
CT
a
b
cd
e
f
gh
IVC
Isthmus
Halo catheter
Isthmus
Halo catheter
II
RAA
II
RAA
1 sec
1 sec
TA
Figure 6 Endocardial mapping during AFL in a dog with MI and nicotine using a Halo catheter positioned around the CT.Panel A, is a clockwise reentrant AFL at a CL of 136ms and a positive sawtooth pattern on ECG lead II. B, is during AFL with
counterclockwise reentry in the same dog showing negative sawtooth pattern on ECG lead II. Next to each set of electrograms (1 to 10) a
schematic diagram shows the locations of the Halo electrodes. CS is coronary sinus and RAA is right atrial appendage bipolar electrogram.
(From Ref 37)
J Arrhythmia Vol 22 No 1 2006
14
us to better understand the fundamental mechanismsinvolved in the genesis, maturation, and stabilizationof AFL. The first step in the development of AFL isthe formation of a functional reentrant wavefront,also known as a spiral wave. This functionally-basedspiral wave has the potential to meander through theatrial myocardium to either extinguish itself or tofind a stable site to anchor. Spiral waves are shownto anchor to anatomical and functional obstacles. Forexample, a spiral wave can anchor around a criticallysized anatomic obstacle not different from the size ofthe tricuspid ring. Alternatively the spiral can anchorto a structure with intense anisotropic propagationproperties, such as the crista terminalis, or around aninflamed tissue with poor electrical coupling. Onceattached (anchored) around such sites the spiral waverotates around it causing AFL. The final step in theemergence stable AFL is the stability of the rotatingspiral wave. The presence of slowed conductionthrough the path of the reentrant circuit allows thereentrant wave front to find fully excitable tissue in
its wake as it rotates around the obstacle.
Future Directions
It is apparent from these experimental studies thatthe mechanism of a stable AFL is model-dependent.Each model offers its unique insights and usefulnessin understanding the mechanisms of human AFL.Important future research should provide insight intothe origin of the spiral wave formation whicheventually anchors to an obstacle (anatomical orfunctional) to cause AFL. What causes the firstwavebreak in the atrial tissue to ‘‘spontaneously’’produce a spiral wave? Waldo et al.60) found in post-operative patients that common type I AFL did notstart immediately after a premature atrial beat. AFLin these patients was found to start after a ‘‘transi-tional rhythm’’ that was often found to be AF. Theseauthors suggested that a transitional rhythm wasrequired for the initiation of type I AFL. It wasfurther speculated that it was during the transitional
Chronic-Nicotine Induced Atrial Fibrosis
Normal MI MI+Nicotine
RAFW
CT
Isthmus TV
IVC
Isthmus
2 mm
Normal MI+Nicotine
100 μ
100 μ
Figure 7 Histological staining with Masson trichrome stain in a control and in an MI plus nicotine dogs.Longitudinal section of CT (A) and IVC-TV isthmus region (B) in a dog with MI exposed to nicotine. Note abundant interstitial fibrosis in
both structures. C and D are higher magnifications of RAFW, CT and IVC-TV isthmus respectively, in control and MI plus nicotine atria.
(From Ref 37)
Karagueuzian HS Mechanisms of atrial flutter
15
rhythm that the requisites for the development of theAFL reentry circuit evolve causing AFL. Thesefindings indicate that the substrates for the AFL areabsent prior to the transitional rhythm but evolvedynamically during the rapid activation of thetransitional rhythm which is most commonly causedby AF. Clearly more insight is needed on therelationship between AFL and AF. How AFL may ormay not degenerate to AF? Is fibrillatory conductionin human AFL to AF conversion related to electricalrestitution? The flat APD restitution slope describedin Miyauchi’s model of canine AFL provides a likelymechanism, it however remains to be seen if thismechanism is also operative in humans. If thisproves to be true in humans, then we envision a truecontinuum between AFL and AF with the clinicalexpression (i.e., typical flutter, coarse flutter, fibril-lation) being dependent on the number and course ofone or more atrial rotors. It may be reasonable toconsider the use of prophylactic AF ablation forpatients presenting with crista-isthmus-dependentAFL. While catheter ablation has proved to be amost effective therapy for isthmus-dependent AFL,ablative cure of left atrial circuits (particularly postsurgical) is still a major challenge. There is littleinformation on genetic causes of AFL. Young
patients with AFL who have multiple familymembers with the same arrhythmia suggest a geneticbasis of AFL, to-date however, no specific geneticmutation associated with AFL has been found.Hence, although much has been accomplished inthe field of AFL, clearly much more still remains tobe done.
References
1) MacWilliam JA: Fibrillar contraction of the heart. J
Physiol 1887; 8: 296–3102) Einthoven W: The telecardiogramme. Arch Int Physiol
1906; 4: 132–1413) Lewis T: Mechanism and Graphic Registration of the
Heart Beat. 1924. Chicago Medical Book Co., Chicago
4) Jolly WARWT: Auricular flutter and fibrillation. Heart1911; 2: 177–186
5) Lewsi T: Observation upon a curious and not uncommonform of extreme acceleration of the auricle: ‘‘Auricular
flutter.’’ Heart 1913; 4: 171–1826) Katz LN, Pick A: Ectopic Impulse formation IV.
Auricular flutter and fibrillation, and the nature of flutterand fibrillation in general. In: Clinical Electrocardiog-
raphy. Part I. The Arrhythmias. 1956. Lea & Febiger,Philadelphia
7) Lewis T, Drury A: A demonstration of circus movementin clinical flutter of the auricles. Heart 1921; 8: 341
180
160
140
120
100
AP
D90
(m
s)
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
AP
D90
(m
s)
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
180
160
140
120
100
80
60
40
20
180160140120100806040200
0
DI (ms)
Control, RA
Max Slope 1.26
Sham, RA
Max Slope 0.67
MI, RA
Max Slope 2.59
MI+Nic, RA
Max Slope 0.85
Control, LA
Max Slope 1.31
Sham, LA
Max Slope 0.89
MI, LA
Max Slope 3.52
MI+Nic, LA
Max Slope 0.64
Figure 8 Monophasic action potential duration (MAPD) restitution curves to 90 percent repolarization (MAPD90) of the RA
and LA in control, sham-operated plus nicotine, MI, and MI plus nicotine dogs.Note flattening of the slope of the restitution curve in MI dogs exposed to nicotine. DI is diastolic interval in ms. (From Ref 37)
J Arrhythmia Vol 22 No 1 2006
16
8) Lewis T: The nature of auricular flutter. In: Mechanismsand graphic registration of the heart beat. Lewis T, ed.
1924. Chicago Medical Book Co., Chicago9) Brams WA, Katz LN: The nature of experimental flutter
and fibrillation of the heart. Am Heart J 1931; 7: 249–261
10) Rosenblueth A, Ramos JG: Studies of flutter and
fibrillation. II. The influence of artificial obstacles onexperimental auricular flutter. Am Heart J 1947; 33:
677–68411) Frame LH, Page RL, Boyden PA, Fenoglio JJJ, Hoffman
BF: Circus movement in the canine atrium around thetricuspid ring during experimental atrial flutter and
during reentry in vitro. Circulation 1987; 76: 1155–117512) Prinzmetal M, Corday E, Brill IC, Sellers AL, Oblath
RW, Flieg WA, Kruger HE: Mechanism of the auriculararrhythmias. Circulation 1950; 1: 241–245
13) Rosen K, Lau S, Damato D: Simulation of atrial flutterby rapid coronary sinus pacing. Am Heart J 1969; 78:
635–64414) Wit AL, Cranefield PF: Triggered and automatic activity
in the canine coronary sinus. Circ Res 1977; 41: 434–44515) Puech P, Latour H, Groleau R: Le flutter et ses limites.
Arch Mal Coeur 1970; 61: 116–14416) Waldo AL: The interrelationship between atrial fibrilla-
tion and atrial flutter. Prog Cardiovasc Dis 2005; 48: 41–56
17) Feld GK, Fleck RP, Chen P-S, Boyce K, Bahnson TD,Stein JB, Calisi CM, Ibarra M: Radiofrequency catheter
ablation for the treatment of human type 1 atrial flutter.Identification of a critical zone in the reentrant circuit by
endocardial mapping techniques. Circulation 1992; 86:1233–1240
18) Cosı́o FG, Gil ML, Goicolea A, Arribas F, Barroso JL:Radiofrequency ablation of the inferior vena cava-
tricuspid valve isthmus in common atrial flutter. Am JCardiol 1993; 71: 705–709
19) Boineau JP, Schuessler RB, Mooney CR, Miller CB,Wylds AC, Hudson RD, Brockus CW: Natural and
evoked atrial flutter due to circus movement in dogs.
Role of abnormal atrial pathways, slow conduction,nonuniform refractory period distribution and premature
beats. Am J Cardiol 1980; 45: 1167–118120) Boineau JP: Atrial flutter: a synthesis of concepts.
Circulation 1985; 72: 249–25721) Winfree AT: Rotors in normal ventricular myocardium.
Proc Kon Ned Akad V Wetensch 1990; 93: 513–53622) Frame LH, Page RL, Hoffman BF: Atrial reentry around
an anatomic barrier with a partially refractory excitablegap. A canine model of atrial flutter. Circ Res 1986; 58:
495–51123) Winfree AT: Spiral waves of chemical activity. Science
1972; 175: 634–63624) Feld GK, Shahandeh-Rad F: Activation patterns in
experimental canine atrial flutter produced by right atrialcrush injury. J Am Coll Cardiol 1992; 20: 441–451
25) Page PL, Plumb VJ, Okumura K, Waldo AL: A newanimal model of atrial flutter. J Am Coll Cardiol 1986; 8:
872–87926) Uno K, Kumagai K, Khrestian CM, Waldo AL: New
insights regarding the atrial flutter reentrant circuit:
studies in the canine sterile pericarditis model. Circu-lation 1999; 100: 1354–1360
27) Okumura K, Plumb VJ, Page PL, Waldo AL: Atrialactivation sequence during atrial flutter in the canine
pericarditis model and its effects on the polarity of theflutter wave in the electrocardiogram. J Am Coll Cardiol
1991; 17: 509–518
28) Allessie MA, Bonke FIM, Schopman FJG: Circusmovement in rabbit atrial muscle as a mechanism of
tachycardia. Circ Res 1973; 33: 54–6229) Allessie MA, Bonke FI, Schopman FJ: Circus movement
in rabbit atrial muscle as a mechanism of tachycardia. III.The ‘‘leading circle’’ concept: a new model of circus
movement in cardiac tissue without the involvement ofan anatomical obstacle. Circ Res 1977; 41: 9–18
30) Pertsov AM, Davidenko JM, Salomonsz R, Baxter WT,Jalife J: Spiral waves of excitation underlie reentrant
activity in isolated cardiac muscle. Circ Res 1993; 72:631–650
31) Ikeda T, Uchida T, Hough D, Lee JJ, Fishbein MC,Mandel WJ, Chen P-S, Karagueuzian HS: Mechanism of
spontaneous termination of functional reentry in isolatedcanine right atrium: Evidence for the presence of an
excitable but nonexcited core. Circulation 1996; 94:1962–1973
32) Ikeda T, Wu T-J, Uchida T, Hough D, Fishbein MC,Mandel WJ, Chen P-S, Karagueuzian HS: Meandering
and Unstable reentrant wave fronts induced by acetyl-choline in isolated canine right atrium. Am J Physiol
1997; 273: H356–H37033) Ikeda T, Yashima M, Uchida T, Hough D, Fishbein MC,
Mandel WJ, Chen P-S, Karagueuzian HS: Attachment ofmeandering reentrant wave fronts to anatomic obstacles
in the atrium. Role of the obstacle size. Circ Res 1997;81: 753–764
34) Tabuchi T, Okumura K, Matsunaga T, Tsunoda R,Jougasaki M, Yasue H: Linear ablation of the isthmus
between the inferior vena cava and tricuspid annulus forthe treatment of atrial flutter. A study in the canine atrial
flutter model. Circulation 1995; 92: 1312–1319
35) Boyden PA, Hoffman BF: The effects on atrial electro-physiology and structure of surgically induced right atrial
enlargement in dogs. Circ Res 1981; 49: 1319–133136) Boyden PA: Activation sequence during atrial flutter in
dogs with surgically induced right atrial enlargement: I.Observations during sustained rhythms. Circ Res 1988;
62: 596–60837) Miyauchi M, Qu Z, Miyauchi Y, Zhou SM, Pak H,
Mandel WJ, Fishbein MC, Chen P-S, Karagueuzian HS:Chronic nicotine in hearts with healed ventricular
myocardial infarction promotes atrial flutter that resem-bles typical human atrial flutter. Am J Physiol 2005; 288:
H2878–H288638) Department of Health, Education and Welfare. Smoking
and Health: A Report of the Surgeon General. 1979.Washington, DC. Ref Type: Report
39) Vidaillet H, Granada JF, Chyou PH, Maassen K, OrtizM, Pulido JN, Sharma P, Smith PN, Hayes J: A
population-based study of mortality among patients withatrial fibrillation or flutter. Am J Med 2002; 113: 365–
370
Karagueuzian HS Mechanisms of atrial flutter
17

40) Benowitz NL: Drug therapy. Pharmacologic aspects ofcigarette smoking and nicotine addiction. N Engl J Med
1988; 319: 1318–133041) Miyauchi Y, Zhou S, Okuyama Y, Miyauchi M, Hayashi
H, Hamabe A, Fishbein MC, Mandel WJ, Chen LS, ChenPS, Karagueuzian HS: Altered atrial electrical restitution
and heterogeneous sympathetic hyperinnervation in
hearts with chronic left ventricular myocardial infarc-tion: implications for atrial fibrillation. Circulation 2003;
108: 360–36642) Sekhon HS, Keller JA, Proskocil BJ, Martin EL, Spindel
ER: Maternal nicotine exposure upregulates collagengene expression in fetal monkey lung. Association with
alpha7 nicotinic acetylcholine receptors. Am J RespirCell Mol Biol 2002; 26: 31–41
43) Sekhon HS, Jia Y, Raab R, Kuryatov A, Pankow JF,Whitsett JA, Lindstrom J, Spindel ER: Prenatal nicotine
increases pulmonary alpha7 nicotinic receptor expressionand alters fetal lung development in monkeys. J Clin
Invest 1999; 103: 637–64744) Feld GK, Shahandeh-Rad F: Mechanism of double
potentials recorded during sustained atrial flutter in thecanine right atrial crush-injury model. Circulation 1992;
86: 628–64145) Olshansky B, Okumura K, Henthorn RW, Waldo AL:
Characterization of double potentials in human atrialflutter: studies during transient entrainment. J Am Coll
Cardiol 1990; 15: 833–84146) Henningfield JE, Stapleton JM, Benowitz NL, Grayson
RF, London ED: Higher levels of nicotine in arterial thanin venous blood after cigarette smoking. Drug and
Alcohol Dependence 1993; 33: 23–2947) Manabe I, Shindo T, Nagai R: Gene expression in
fibroblasts and fibrosis: involvement in cardiac hyper-trophy. Circ Res 2002; 91: 1103–1113
48) Lamers JM, Hartog JM, Verdouw PD, Hulsmann WC:Dietary fatty acids and myocardial function. Basic Res
Cardiol 1987; 82 Suppl 1: 209–22149) Kang JX, Leaf A: Prevention of fatal cardiac arrhythmias
by polyunsaturated fatty acids. Am J Clin Nutr 2000; 71:
202S–207S50) Lee WL, Chen JW, Ting CT, Lin SJ, Wang PH: Changes
of the insulin-like growth factor I system during acutemyocardial infarction: implications on left ventricular
remodeling. J Clin Endocrinol Metab 1999; 84: 1575–1581
51) Gillis AM, Keashly R, Watson PA, Mathison HJ, Parsons
HG: Influence of dietary fat on the pharmacodynamics ofpropafenone in isolated, perfused rabbit hearts. Circu-
lation 1992; 85: 1501–150952) Peters NS, Coromilas J, Hanna MS, Josephson ME,
Costeas C, Wit AL: Characteristics of the temporal andspatial excitable gap in anisotropic reentrant circuits
causing sustained ventricular tachycardia. Circ Res 1998;
82: 279–29353) Wang HZ, Shi H, Liao SJ, Wang Z: Inactivation gating
determines nicotine blockade of human HERG channels.Am J Physiol 1999; 277: H1081–H1088
54) Wang H, Shi H, Zhang L, Pourrier M, Yang B, Nattel S,Wang Z: Nicotine is a potent blocker of the cardiac A-
type K(+) channels. Effects on cloned Kv4.3 channelsand native transient outward current. Circulation 2000;
102: 1165–117155) Satoh H: Modulation by nicotine of the ionic currents in
guinea pig ventricular cardiomyocytes. Relatively highersensitivity to IKr and IKl. Vascul Pharmacol 2002; 39:
55–6156) Yashima M, Ohara T, Cao J-M, Kim Y-H, Fishbein MC,
Mandel WJ, Chen P-S, Karagueuzian HS: Nicotineincreases ventricular vulnerability to fibrillation in hearts
with healed myocardial infarction. Am J Physiol HeartCirc Physiol 2000; 278: H2124–H2133
57) Bode F, Sachs F, Franz MR: Tarantula peptide inhibitsatrial fibrillation. Nature 2001; 409: 35–36
58) Garfinkel A, Kim Y-H, Voroshilovsky O, Qu Z, Kil JR,Lee M-H, Karagueuzian HS, Weiss JN, Chen P-S:
Preventing ventricular fibrillation by flattening cardiacrestitution. Proc Natl Acad Sci U S A 2000; 97: 6061–
606659) Ohara T, Qu Z, Lee M-H, Ohara K, Omichi C, Mandel
WJ, Chen P-S, Karagueuzian HS: Increased vulnerabilityto inducible atrial fibrillation caused by partial cellular
uncoupling with heptanol. Am J Physiol Heart CircPhysiol 2002; 283: H1116–H1122
60) Waldo AL, Cooper TB: Spontaneous onset of type Iatrial flutter in patients. J Am Coll Cardiol 1996; 28:
707–712
61) Kamjoo K, Uchida T, Ikeda T, Fishbein MC, GarfinkelA, Weiss JN, Karagueuzian HS, Chen P-S: The impor-
tance of location and timing of electrical stimuli interminating sustained functional reentry in isolated swine
ventricular tissues—evidence in support of a smallreentrant circuit. Circulation 1997; 96: 2048–2060
J Arrhythmia Vol 22 No 1 2006
18