medial collateral ligament - uhealth sports...
TRANSCRIPT

Medial Collateral LigamentEdward Silverman PGY VFebruary 17, 2015

GoalsAnatomyInjuryExamImagingTreatmentNon-operativeOperative
Medial Collateral Ligament

Medial Knee Anatomy Layer I Fascia, Sartorius Layer II Superficial MCL, Posterior oblique
ligament, Medial patellofemoralligament, Semimembranosus attachments
Layer III Knee capsule, Deep MCL
(Warren and Marshall, 1979)

Medial Knee Ligaments Superficial MCL Deep MCL Posterior Oblique Ligament

Superficial MCL Largest structure on the medial side of
the knee One femoral attachment 3.2 mm proximal, 4.8 mm posterior to
medial epicondyle Two tibial attachments Proximal insertion Soft tissue – semimembranosus 12.2 mm distal to joint line Distal insertion Bone – 4.5 - 6 cm distal to joint line Just anterior to posteromedial crest
sMCL primary restraint to valgus stress at 25 deg flex, resists external rotation
Hartshorn et. al. AJSM 2013

Deep MCL Thickened medial joint capsule Meniscofemoral 12.6 mm distal/deep to sMCL
Meniscotibial 3.2 mm distal to joint line Just distal to articular surface
Secondary valgus stablilizer Resists external rotation btw 30-90
degrees

Posterior Oblique Ligament Fibrous extension of distal
semimembranosus Blends with and reinforces post-medial
capsule Previously thought to be part of sMCL rotation and valgus stabilizer btw 0-30
degrees flexion Extension

Medial Knee Anatomy
LaPrade 2009 JBJS Posterior cortex
reference line Line 2 – most posterior
aspect of Blumensaatline POL – Most posterior,
posterior to line 1 sMCL – distal and
posterior to medial epicondyle MPFL – btw adductor
tubercle and medial epicondyle

Injury Valgus stress to a flexed knee External rotation / pivoting injury Blow to anterolateral knee Most commonly injured ligament 0.24 per 1000 (US incidence)
7.3 per 1000 per year (West Point Cadets)

Exam Suspicion based on
mechanism Complete exam – 78% rate of
associated injuries (grade III) Intra-articular effusion –
concern for ACL MCL extra-articular
Valgus stress with knee 30 degrees flexed Grade 1 <5 mm opening Grade 2 5-10 mm opening Grade 3 >10 mm opening
Degree 1st degree – tendernes without
instability 2nd degree – valgus laxity but
firm endpoint 3rd degree – no endpoint

Exam Valgus stress at 0 Posterior oblique ligament If laxity at 0, likely concominant ACL
tear or complete injury to posteromedial capsule
Valgus stress at 30 degrees Long fibers of sMCL
Saphenous nerve neuropraxia Medial meniscus (5% of sMCL
injuries)

Imaging Xray Medial joint space widening (Grade III) Avulsions Stress Xray, physeal injuries Pellegrini-Stieda lesion Chronic, femoral origin

MRI
Best study for diagnosisSite of injury (femoral/tibial
avulsion vs intrasubstance)Associated injuries Medial meniscus (5%) ACL (20%, 52%, 78%)

MCL Healing Extra-articular, good blood supply Hemorrhage, inflammation, repair, remodeling Repair with type 1 collagen Grade III with gapping – ↑ type 3 collagen Creighton et. al. ‘05
Immobilization hinders the healing,↓ load to failure Thornton et. al. ‘05
Adjuvants Ultrasound, PRP, Stem cells etc. Promising early results Pending publication UM Sports!
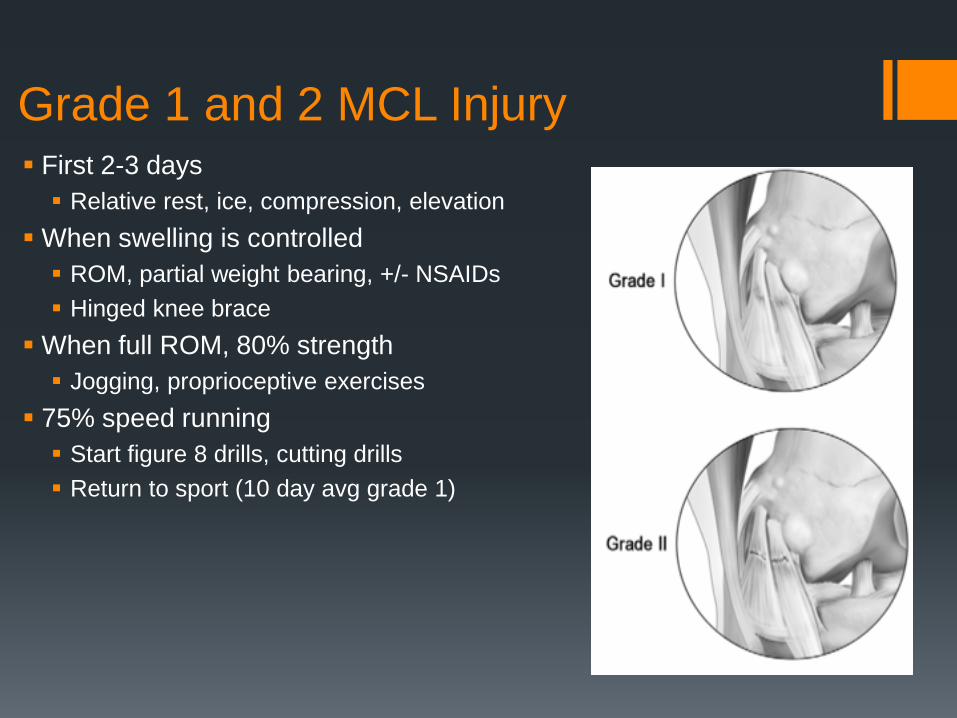
Grade 1 and 2 MCL Injury First 2-3 days Relative rest, ice, compression, elevation
When swelling is controlled ROM, partial weight bearing, +/- NSAIDs Hinged knee brace
When full ROM, 80% strength Jogging, proprioceptive exercises
75% speed running Start figure 8 drills, cutting drills Return to sport (10 day avg grade 1)

Grade 3 MCL Injuries 80% incidence of concomitant ligament
injuries Need to treat according to other injuries Isolated MCL Early repair vs late reconstruction Based on location of tear
Giannotti et. al. 2006

7.3 per 1000 per year (West Point Cadets) 73% grade 1, 27% grade 2/3 All non-operatively treated Grade 1 – lost 13.5 days, High grade – lost
29 days

Surgical Indications Persistent instability preventing normal activities or return to
sport Failed Non-operative treatment
Multi-ligamentous knee injuries MCL management Early primary repair vs non-operative management Bony avulsions – ORIF Reconstruct cruciates, non-op MCL
Tibial sided avulsions

Tibial avulsion
Taketomi et. al. Knee 2013
Stener like lesion• Tibial side avulsions• Rare, associated with
ACL tear• 9/12 type 2 or 3, poor
healing potential • Stener like lesion• Early repair

2011 CORR Italy 36 patients, chronic valgus laxity
(combined ACL) Medial reefing Reefing of medial capsule from
epicondyle Anterodistally, distally and
posterodistally Decreased laxity and improved
functional scores postop

2005 AJSM Japan Autograft hamstring Good results in small
case series n=24 Aim for anatomic
reconstruction of sMCL

2014 China Double bundle
reconstruction technique sMCL and POL
Better restoration of rotational stability Don’t sacrifice medial
hamstrings Dynamic stability

Prophylactic Bracing 1990 AJSM USMA West Point 1396 cadets Intramural, tackle football. RCT, Prophylactic brace vs no brace Decreased # of MCL injuries, significant
difference for defensive players.
1994 Big Ten Study Nonsignificant trend towards decreased
MCL injuries in braced linemen Similar nonsignificant increase in injury
rate for brace skill players Very low risk at baseline
2003 AAOS position statement “Prophylactic knee braces may provide
limited protection against injuries to the MCL in football players. Scientific studies have not demonstrated similar protection to other knee ligaments, menisci, or articular cartilage.”

Summary Non-operative treatment Surgery Reserved for valgus instability, failed non-operative tx Tibial side avulsions Associated with Multiligamentous injury