medical and non -medical testosterone and steroid hormone … · 2016-11-28 · testosterone and...
TRANSCRIPT
MEDICAL AND NON-MEDICAL TESTOSTERONE AND STEROID HORMONE USAGE AMANDA HO, MD
DISCLOSURES
I have no relevant financial interests to disclose.
LEARNING OBJECTIVES
Explain the different effects of testosterone on men and women.
Compare different steroid hormone testing options.
Describe ways in which testing of hormones differs from testing for other analytes.
Explain the ways in which anabolic steroid usage for athletic performance differs from medical usage of testosterone therapy.
TESTOSTERONE
DEFINITIONS
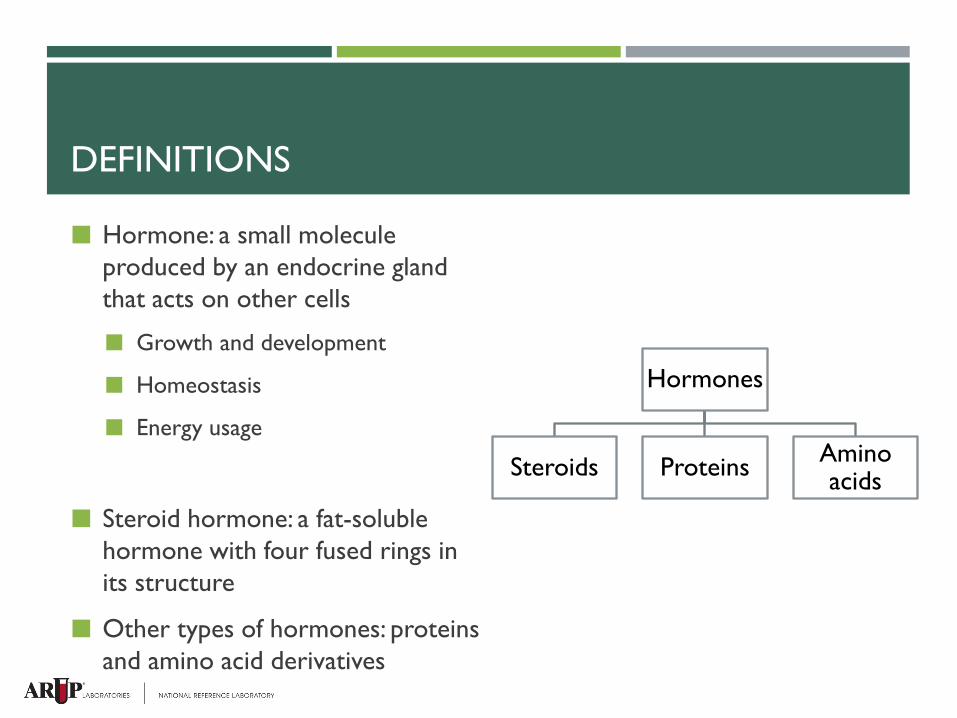
Hormone: a small molecule produced by an endocrine gland that acts on other cells
Growth and development
Homeostasis
Energy usage
Steroid hormone: a fat-soluble hormone with four fused rings in its structure
Other types of hormones: proteins and amino acid derivatives
Hormones
Steroids Proteins Amino acids
STEROID HORMONES
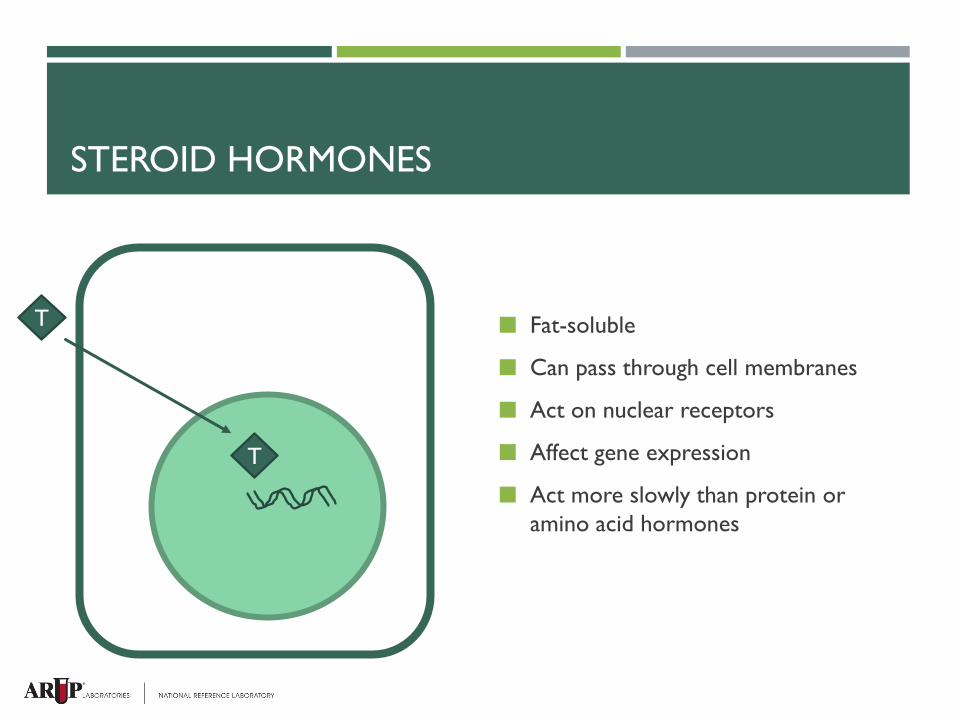
Fat-soluble
Can pass through cell membranes
Act on nuclear receptors
Affect gene expression
Act more slowly than protein or amino acid hormones
T
T
ANDROGENS
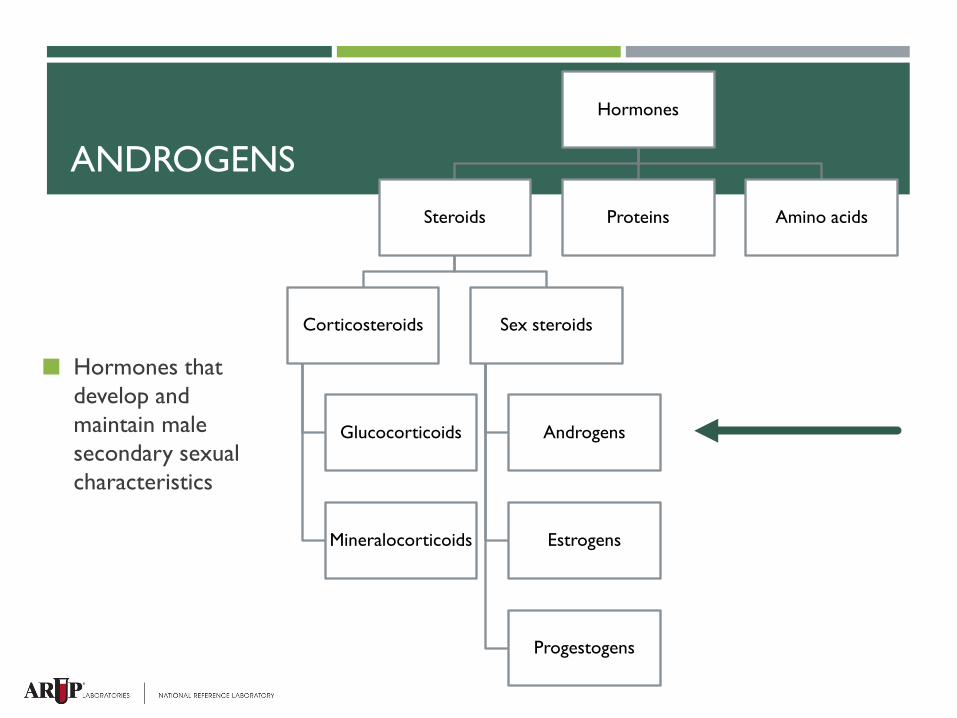
Hormones that develop and maintain male secondary sexual characteristics
Hormones
Steroids
Corticosteroids
Glucocorticoids
Mineralocorticoids
Sex steroids
Androgens
Estrogens
Progestogens
Proteins Amino acids
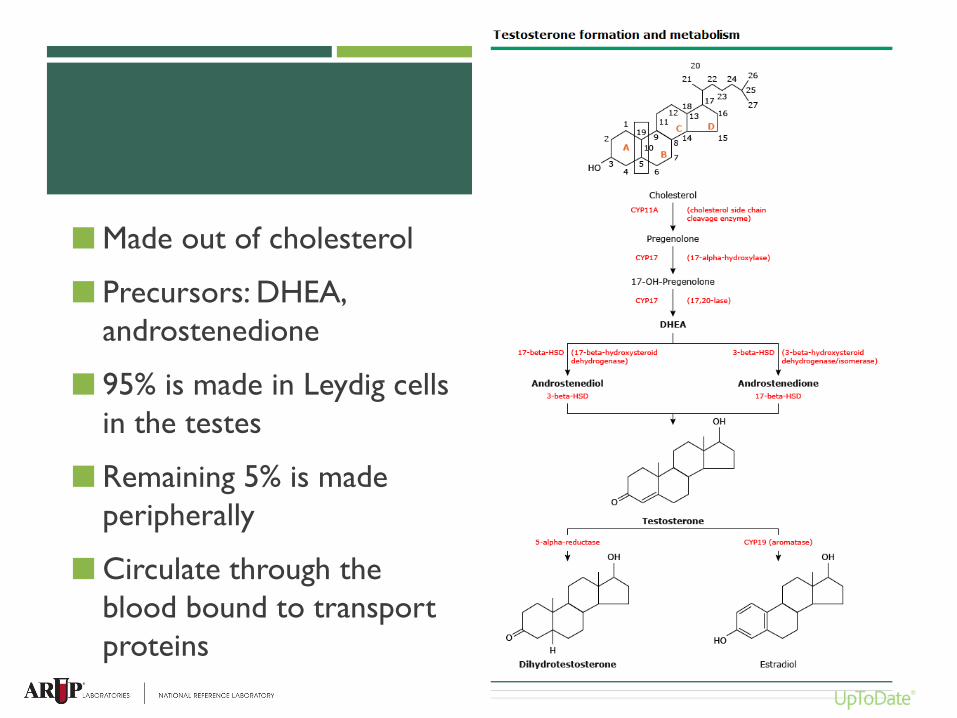
Made out of cholesterol
Precursors: DHEA, androstenedione
95% is made in Leydig cells in the testes
Remaining 5% is made peripherally
Circulate through the blood bound to transport proteins
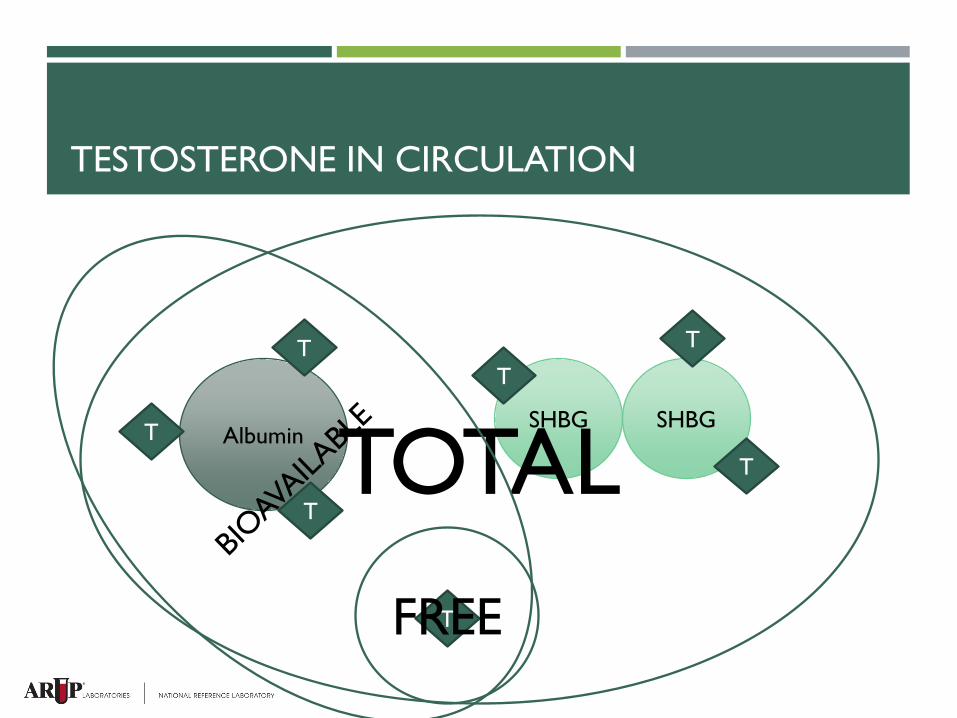
TESTOSTERONE IN CIRCULATION
Albumin SHBG SHBG
T
T
T
T
T
T
T
TOTAL FREE
CONCENTRATIONS - MALE
Three peaks in the male life cycle: 2nd trimester of fetal development
2-3 months of age
Puberty (reaches a plateau) – 300-1080 ng/dL
Starting around age 40, testosterone levels decline by 0.5-2%/year Decrease in number of Leydig cells
Decrease in the GnRH pulse amplitude
CONCENTRATIONS - FEMALE
9-55 ng/dL
Made in the ovaries and the adrenal glands
No fetal or neonatal peak
Does increase at puberty
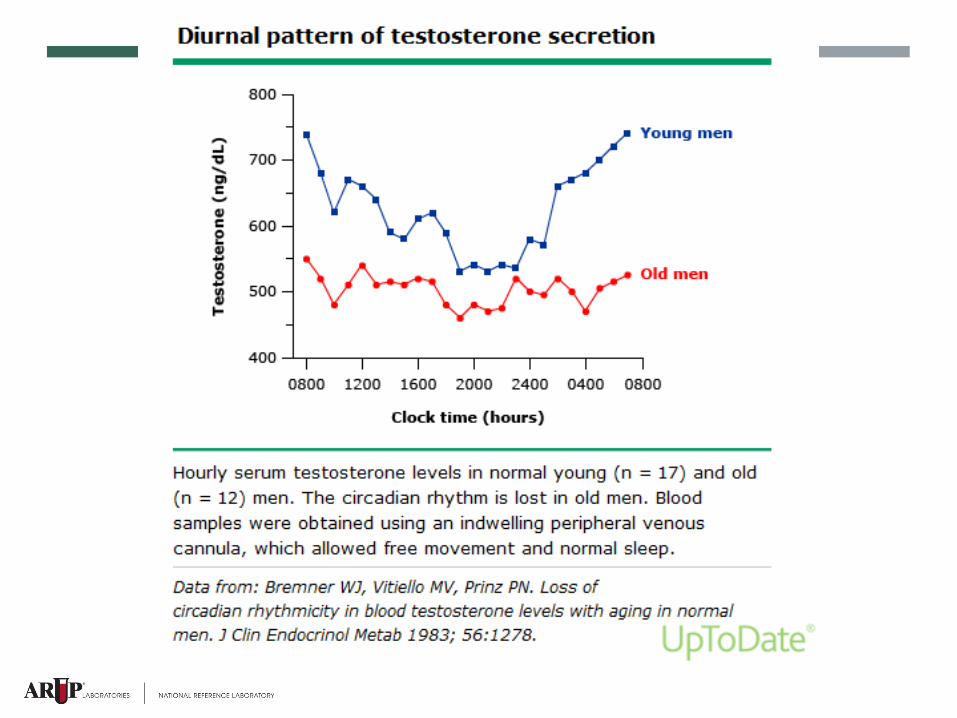
Diurnal variation
Total testosterone peaks slightly before ovulation
Seems to decrease with menopause
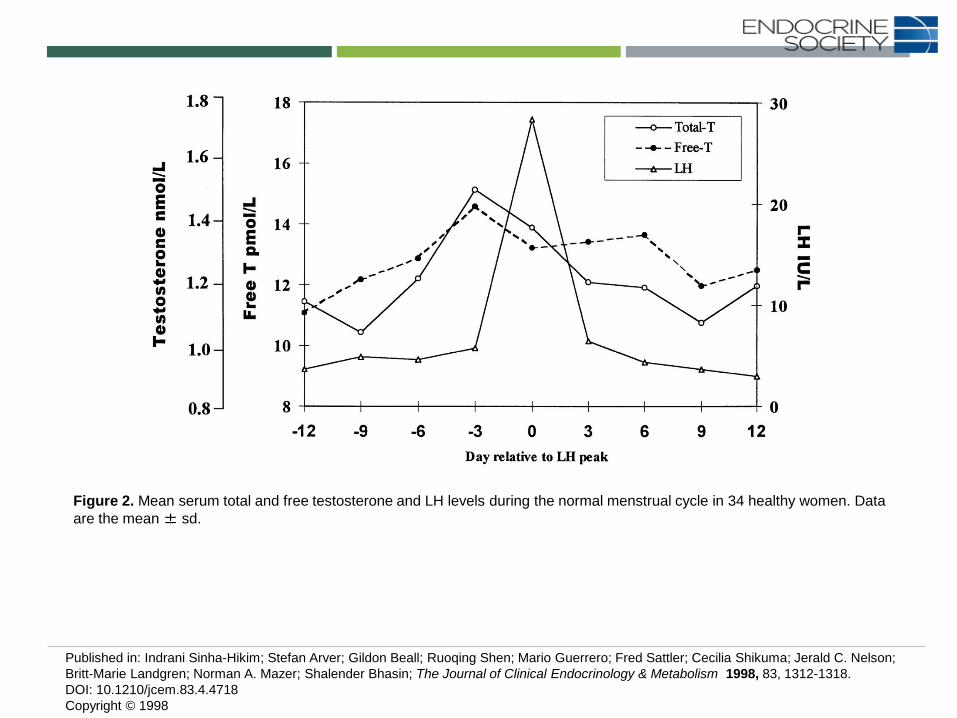
Figure 2. Mean serum total and free testosterone and LH levels during the normal menstrual cycle in 34 healthy women. Data are the mean ± sd.
Published in: Indrani Sinha-Hikim; Stefan Arver; Gildon Beall; Ruoqing Shen; Mario Guerrero; Fred Sattler; Cecilia Shikuma; Jerald C. Nelson; Britt-Marie Landgren; Norman A. Mazer; Shalender Bhasin; The Journal of Clinical Endocrinology & Metabolism 1998, 83, 1312-1318. DOI: 10.1210/jcem.83.4.4718 Copyright © 1998
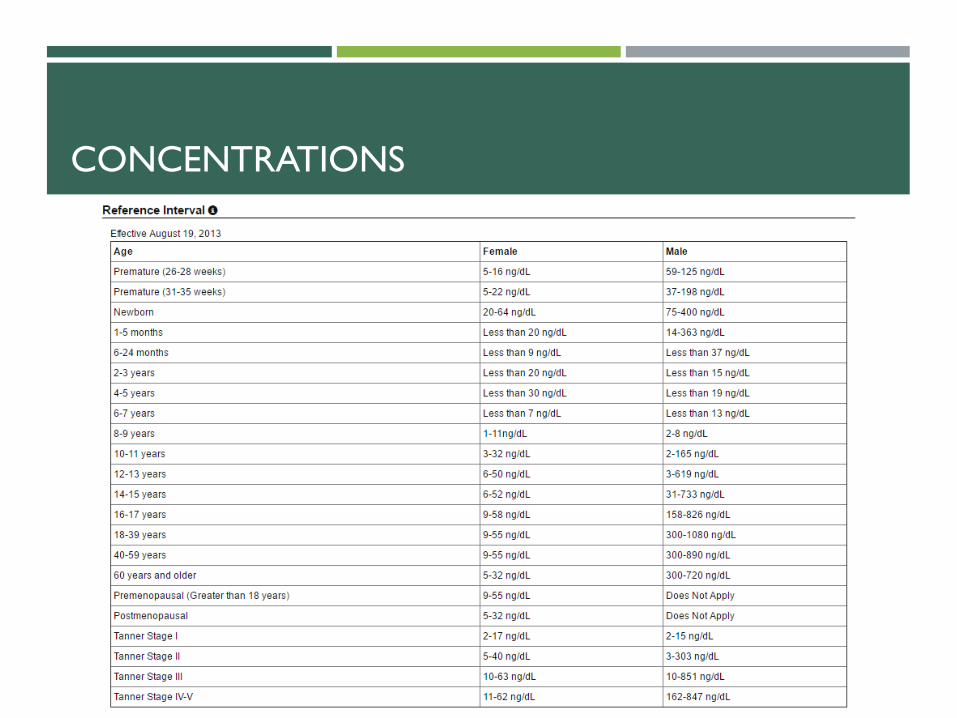
CONCENTRATIONS
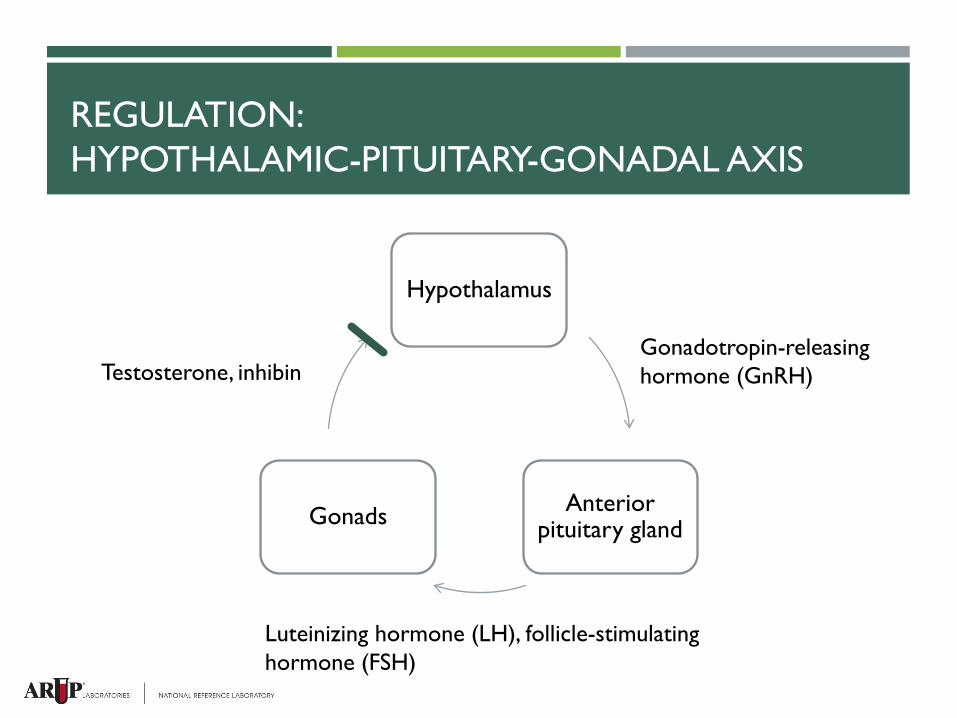
REGULATION: HYPOTHALAMIC-PITUITARY-GONADAL AXIS
Hypothalamus
Anterior pituitary gland Gonads
Gonadotropin-releasing hormone (GnRH)
Luteinizing hormone (LH), follicle-stimulating hormone (FSH)
Testosterone, inhibin
EFFECTS ON THE BODY
Affects cells that are sensitive to androgens
Male sexual characteristics
Acne
Erythropoiesis
Increased lean body mass
Increased energy and libido
HOW WE TEST FOR TESTOSTERONE
CLIENT QUESTION
My patient is receiving testosterone injections.
What test do I order to measure testosterone?
SOME OF THE QUESTIONS THAT NEED TO BE ANSWERED
Man, woman, or child?
Expected levels?
Total, free, or bioavailable?
MEN VS WOMEN AND CHILDREN
Men: 300-1080 ng/dL
Women and children: as low as 1 ng/dL
Electrochemiluminescent immunoassay vs HPLC-MS/MS
Analytical sensitivity:
Immunoassay: 3 ng/dL, but imprecise
HPLC-MS/MS: 1.0 ng/dL
TOTAL, FREE, OR BIOAVAILABLE?
Total: measures all testosterone
Free
Bound to SHBG
Bound to albumin
Free: unbound, dissolved in blood
Either calculated or measured directly with equilibrium dialysis
Bioavailable: free + albumin-bound
Calculated
MEASURING SHBG
Quantitative electrochemiluminescent immunoassay
Helps to determine free vs bound testosterone
Many conditions may affect SHBG and thus affect total testosterone
FACTORS AFFECTING SHBG
Decrease
Obesity
Hypothyroidism
Diabetes
Glucocorticoids and progestins
Androgenic steroids
Increase
Aging
Liver disease
Hyperthyroidism
HIV
Estrogens
Anti-seizure medications
PITFALLS OF STEROID HORMONE TESTING
Present in small amounts
Bound to carrier molecules
Diurnal variation
TESTING CONSIDERATIONS
Gender and age
Expected levels – in concordance with patient’s gender and age?
Need more information than a total level?
MEDICAL TESTOSTERONE THERAPY
ACCORDING TO THE FDA…
Testosterone replacement therapy should only be given to men with confirmed low levels of testosterone and symptoms of testosterone deficiency
SYMPTOMS OF ANDROGEN DEFICIENCY
Nonspecific
Decreased energy
Depression
Anemia
Reduced muscle bulk and strength
Diminished performance
Specific
Decreased libido
Loss of body hair
Low bone mineral density or low-trauma fracture
Hot flushes
Infertility
Small testicular size
HYPOGONADISM
Primary
Disease of the testes
High GnRH, FSH, LH
Acquired or congenital
Secondary
Disease of the hypothalamus or pituitary
Low GnRH, FSH, LH
Acquired or congenital
AGE-RELATED DECREASE IN TESTOSTERONE
Remember, testosterone decreases by 0.5-2%/year
Only problematic when symptomatic
Many names:
Testosterone deficiency syndrome (TDS)
Late-onset hypogonadism (LOH)
(Partial) androgen deficiency of the aging male ((P)ADAM)
Goal: to improve signs and symptoms of deficiency
LAB DIAGNOSIS
Endocrine Society Clinical Practice Guideline (Bhasin S et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010 Jun;95(6):2536-59.):
Don’t screen everybody
Measure morning testosterone levels twice
If borderline low, consider testing free or SHBG
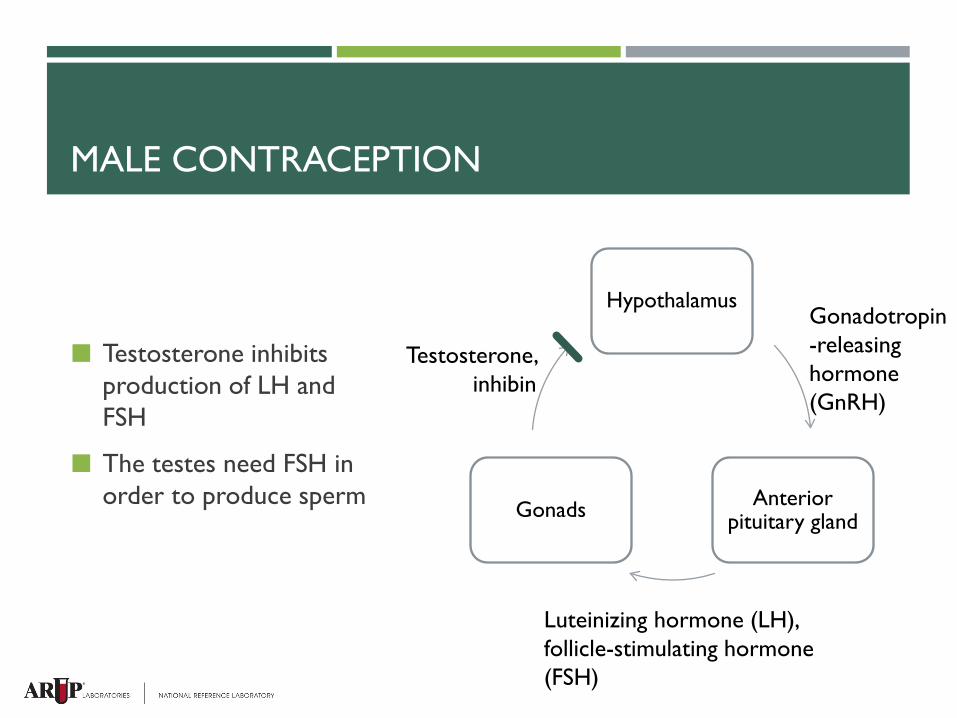
MALE CONTRACEPTION
Testosterone inhibits production of LH and FSH
The testes need FSH in order to produce sperm
Hypothalamus
Anterior pituitary gland Gonads
Gonadotropin-releasing hormone (GnRH)
Luteinizing hormone (LH), follicle-stimulating hormone (FSH)
Testosterone, inhibin
FEMALE TO MALE TRANSITION
Hormone therapy is one part of the overall gender transition in transgender patients
Two goals of hormone therapy in transitioning from female to male: Suppress native (female) hormones
Induce and maintain male secondary sexual characteristics
FEMALE TO MALE TRANSITION: EFFECTS OF TESTOSTERONE ADMINISTRATION
What changes
Facial hair growth
Deepening of the voice
Increase in lean body mass
Acne
Increased libido
Breast changes
Susceptibility to male pattern baldness
Cessation of menstruation
What stays the same
Female bone structure
Shorter height
Broader hips
Breast fat mass
Genitalia
FORMULATIONS
Oral?
Almost completely metabolized in first pass
Intramuscular injection
Gel, cream, or patch
Intradermal implant
Nasal spray
Buccal patch
MONITORING RECOMMENDATIONS
Endocrine Society Clinical Practice Guideline (Bhasin S et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010 Jun;95(6):2536-59.):
Measure serum testosterone 3-6 months after starting supplementation and then annually
Goal is to achieve a total serum testosterone level in the middle of the normal range for a young, healthy adult male (300-1000 ng/dL)
ADVERSE EFFECTS
May increase risk of cardiovascular disease
May worsen symptoms of BPH
May increase risk of prostate cancer
Probably increases hematocrit
Acne
Gynecomastia
Suppression of spermatogenesis
NON-MEDICAL TESTOSTERONE USAGE
ANABOLIC STEROIDS
ANDROGENIC ANABOLIC STEROIDS
Hormones that have the same biological effects as testosterone
We’ve discussed the androgenic (masculinizing) effects of testosterone
Also anabolic (muscle-building) effects
Synthetic hormones designed to have more anabolic than androgenic effects
DO THEY WORK?
Hard to determine, because often used in supratherapeutic doses
Lean body mass increase of 2-5kg
Increase in circumference of shoulders, neck, upper arms
Increase in muscle strength
ADVERSE EFFECTS
Hard to determine, because often used in supratherapeutic doses
Suppression of HPG axis Decreased sperm production and testicular atrophy
Increased aggression and hostility
Acne
Gynecomastia
REGULATION
Over 630 sports agencies follow the guidelines of the World Anti-Doping Agency (WADA) International Olympics Committee (IOC)
Major US sports leagues have their own policies
WADA DOCUMENTS
Prohibited Substances
Int’l Standard for Therapeutic Use Exemptions
Int’l Standard for Protection of Privacy
Int’l Standard for Testing and Investigation
Int’l Standard for Laboratories
BANNED AAS
Exogenous AAS, and other substances with a similar chemical structure or similar biological effect(s).
Endogenous AAS, when administered exogenously, and their metabolites and isomers.
MEASURING ANABOLIC STEROIDS
Tests available to measure many different anabolic steroids in the urine
Testosterone to epitestosterone ratio
Testosterone to LH ratio
Creatinine
Masking agents
IN SUMMARY
Testosterone is present in both men and women and exerts similar masculinizing effects on both
Choosing a lab test to measure testosterone depends on the demographics of the patient and expected levels
Steroid hormone levels change throughout the day and throughout the lifespan
FDA recommends administration to a small group
There are many possible side effects of exogenous administration
Positive and negative effects of anabolic steroids are difficult to measure
THANK YOU!