medical comorbidities and their impact on … comorbidities that affect wound...tissue integrity....
TRANSCRIPT
MEDICAL COMORBIDITIES AND THEIR
IMPACT ON WOUND HEALING
Lee C. Ruotsi, MD, CWS, UHM
Wound Care is Only Part of the Story…
Success Depends on How
You Manage the Rest of the Patient’s Problems
2
3
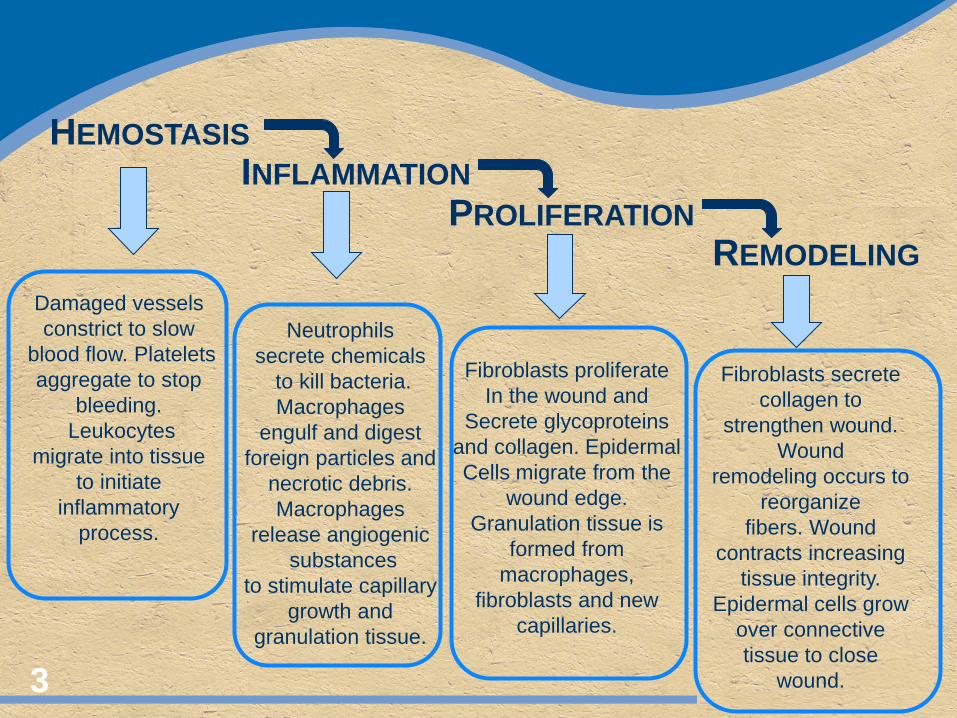
HEMOSTASIS INFLAMMATION
PROLIFERATION REMODELING
Damaged vessels constrict to slow
blood flow. Platelets aggregate to stop
bleeding. Leukocytes
migrate into tissue to initiate
inflammatory process.
Neutrophils secrete chemicals
to kill bacteria. Macrophages
engulf and digest foreign particles and
necrotic debris. Macrophages
release angiogenic substances
to stimulate capillary growth and
granulation tissue.
Fibroblasts proliferate In the wound and
Secrete glycoproteins and collagen. Epidermal Cells migrate from the
wound edge. Granulation tissue is
formed from macrophages,
fibroblasts and new capillaries.
Fibroblasts secrete collagen to
strengthen wound. Wound
remodeling occurs to reorganize
fibers. Wound contracts increasing
tissue integrity. Epidermal cells grow
over connective tissue to close
wound.
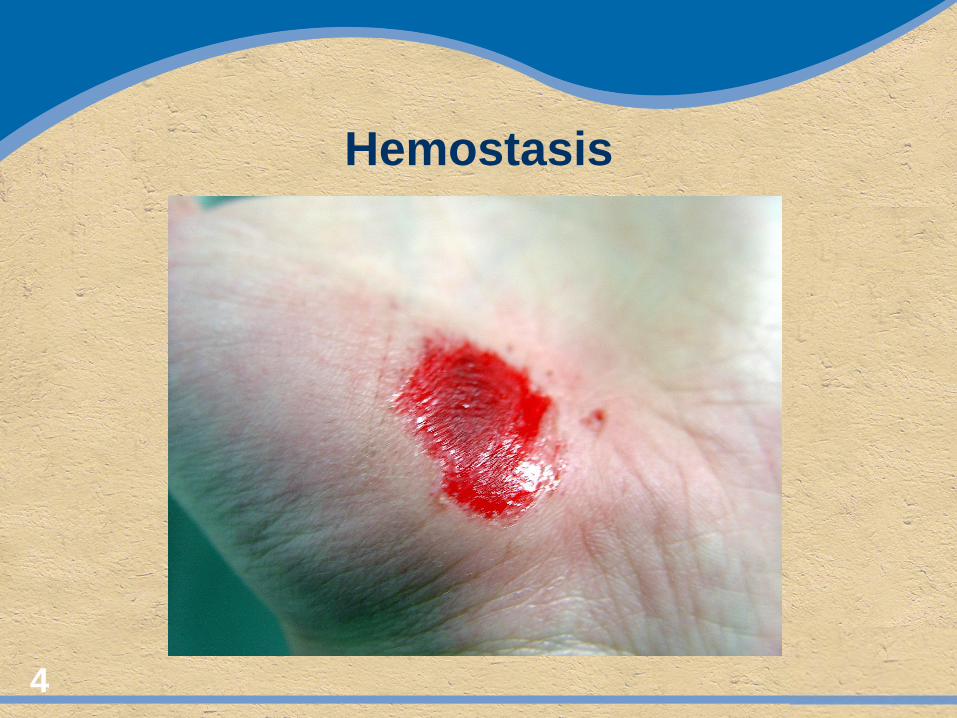
Hemostasis
4
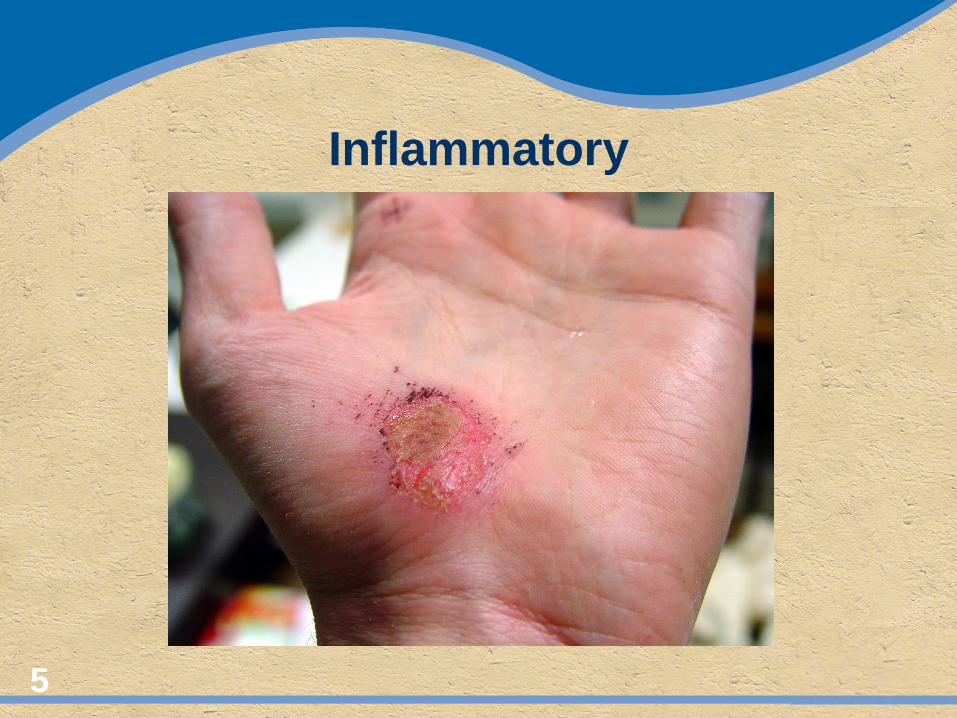
Inflammatory
5
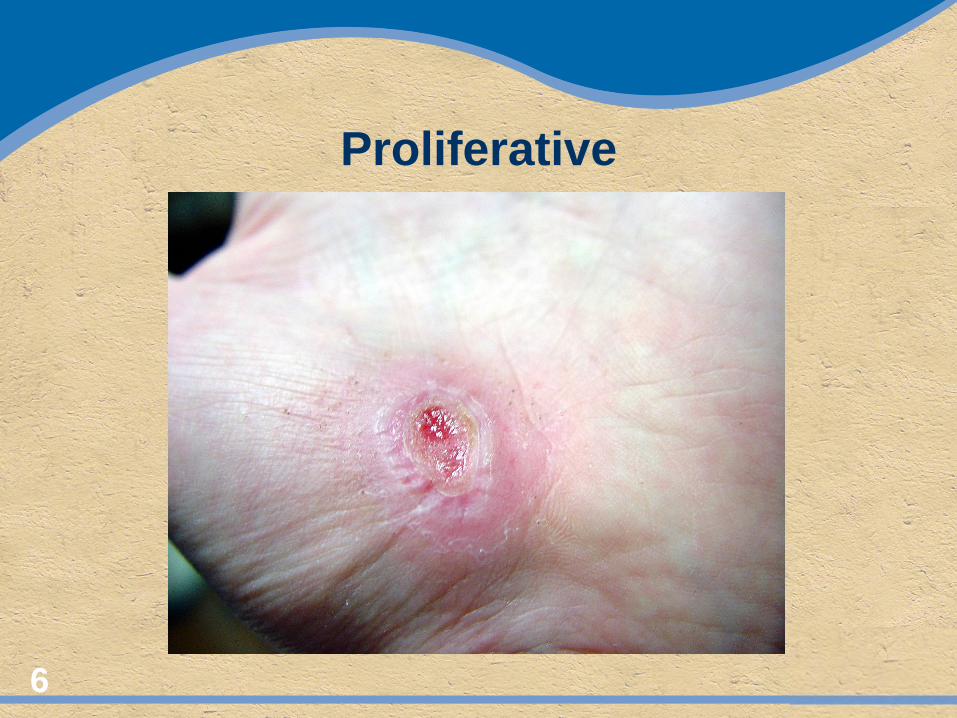
Proliferative
6
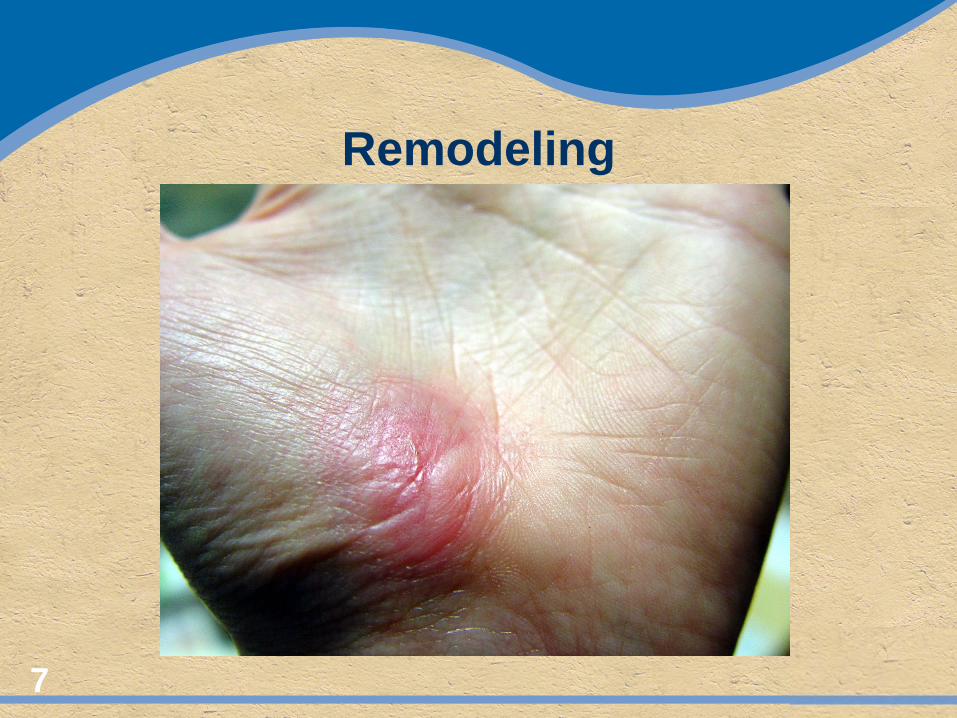
Remodeling
7
Abnormal Wound Healing Failure to progress through normal orderly
stages of wound healing in a timely fashion Chronicity has been defined by failure to
progress to closure over a 90 day period.
Chronicity may also be defined by wound characteristics
8 Mustoe TA, O'Shaughnessy K, Kloeters O. Chronic wound pathogenesis and current treatment strategies: a unifying hypothesis. J Plast Reconstr Surg. 2006;117:35-41
The Chronic Wound
Has failed to proceed through and orderly and timely process to produce anatomical and functional integrity, or proceeded through the repair process without establishing a sustained anatomic and functional result.
Robson MC, Barbul A. Guidelines for the best care of chronic wounds.
Wound Repair and Regeneration. Volume 14, Issue 6, pp 647 – 648, Nov 2006
9
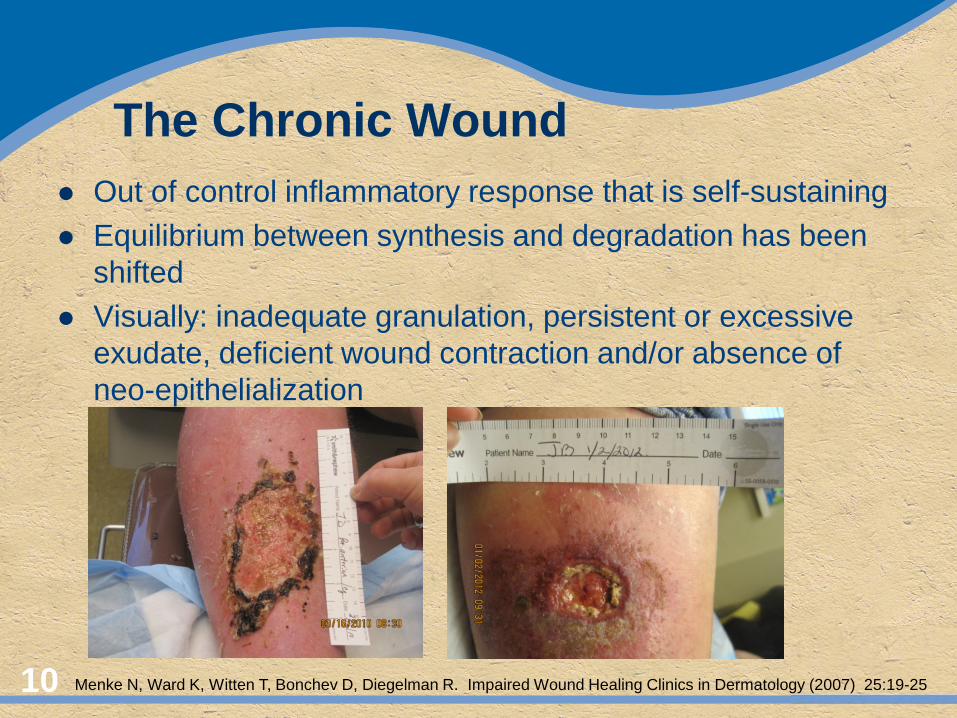
The Chronic Wound Out of control inflammatory response that is self-sustaining Equilibrium between synthesis and degradation has been
shifted Visually: inadequate granulation, persistent or excessive
exudate, deficient wound contraction and/or absence of neo-epithelialization
10 Menke N, Ward K, Witten T, Bonchev D, Diegelman R. Impaired Wound Healing Clinics in Dermatology (2007) 25:19-25
“A chronic wound is an acute wound with an impediment”
T.K Hunt, M.D.
“The impediment may be the treating physician”
Harriett Hopf, M.D.
11
12
Systemic Co-morbidities
Vasculitis Rheumatoid disease Lupus (SLE) Scleroderma Wegener’s Granulomatosis Polyarteritis Nodosa
Diabetes Polycythemia Vera Renal failure Chemotherapy Radiation Pyoderma
Gangrenosum
13
Good H&P
HPI – Wounding PMH PSH Past wounding hx Etiology Location Treatment Response
Meds Family hx ROS Thorough exam Skin Wounding Vascular supply Infection 14
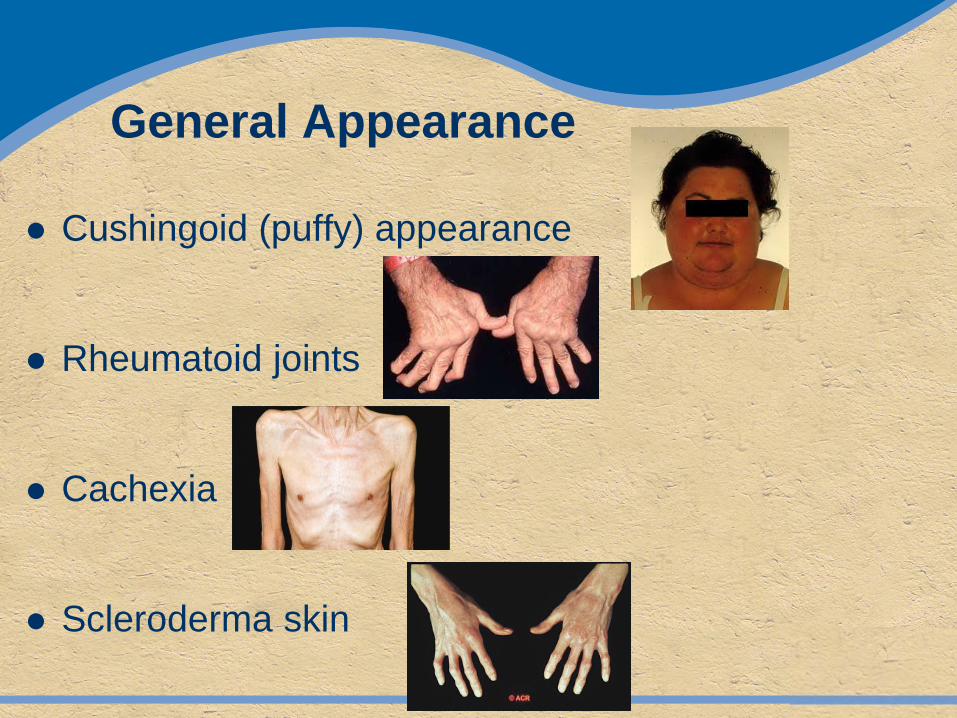
General Appearance
Cushingoid (puffy) appearance
Rheumatoid joints
Cachexia
Scleroderma skin
General Appearance
Abnormal affect and behavior
Focal neurologic deficit
Tobacco
17
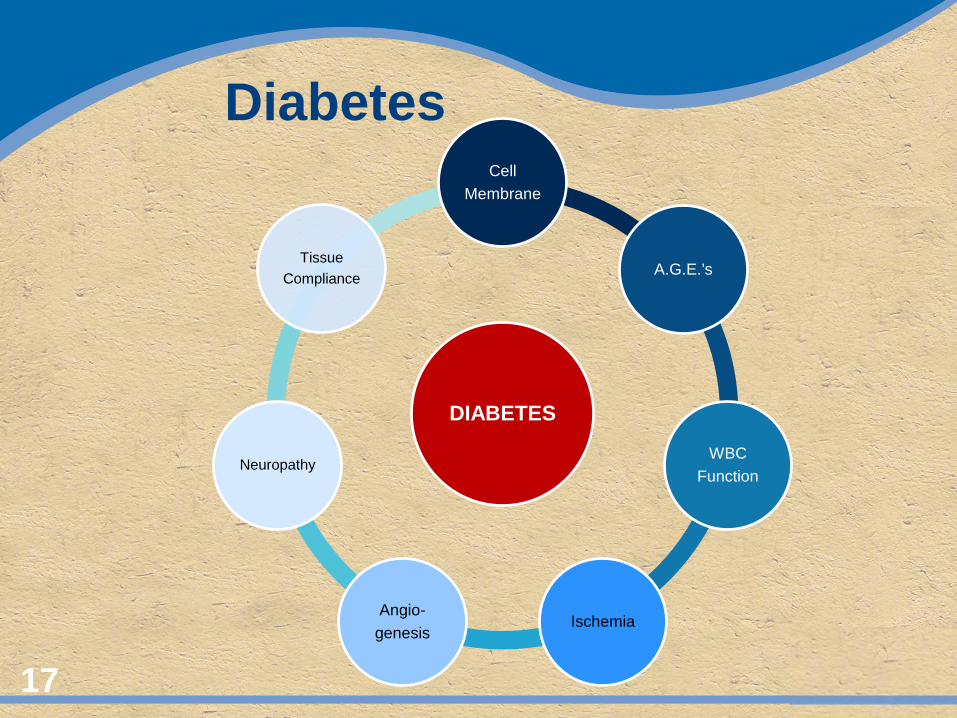
DIABETES
Cell Membrane
A.G.E.’s
WBC Function
Ischemia Angio-
genesis
Neuropathy
Tissue Compliance
Diabetes
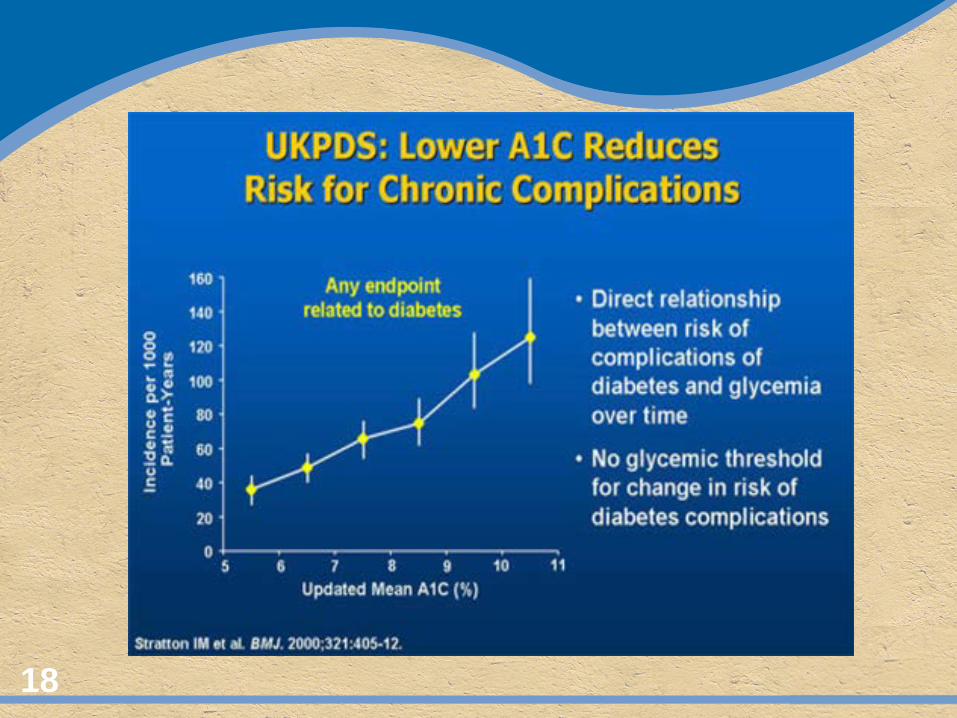
18
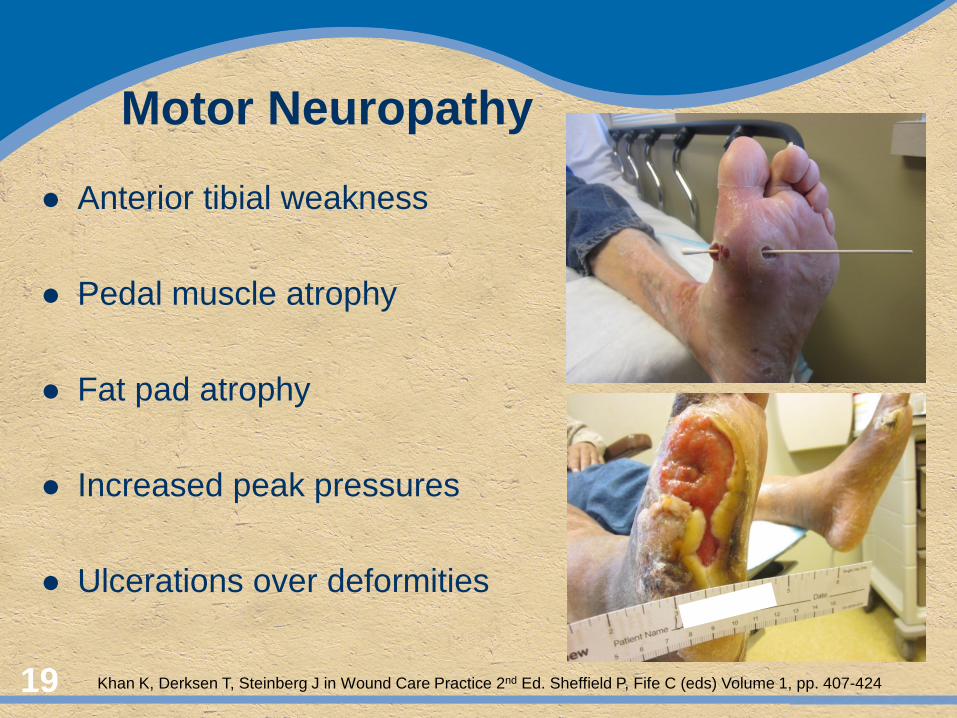
Motor Neuropathy
Anterior tibial weakness
Pedal muscle atrophy
Fat pad atrophy
Increased peak pressures
Ulcerations over deformities
19 Khan K, Derksen T, Steinberg J in Wound Care Practice 2nd Ed. Sheffield P, Fife C (eds) Volume 1, pp. 407-424
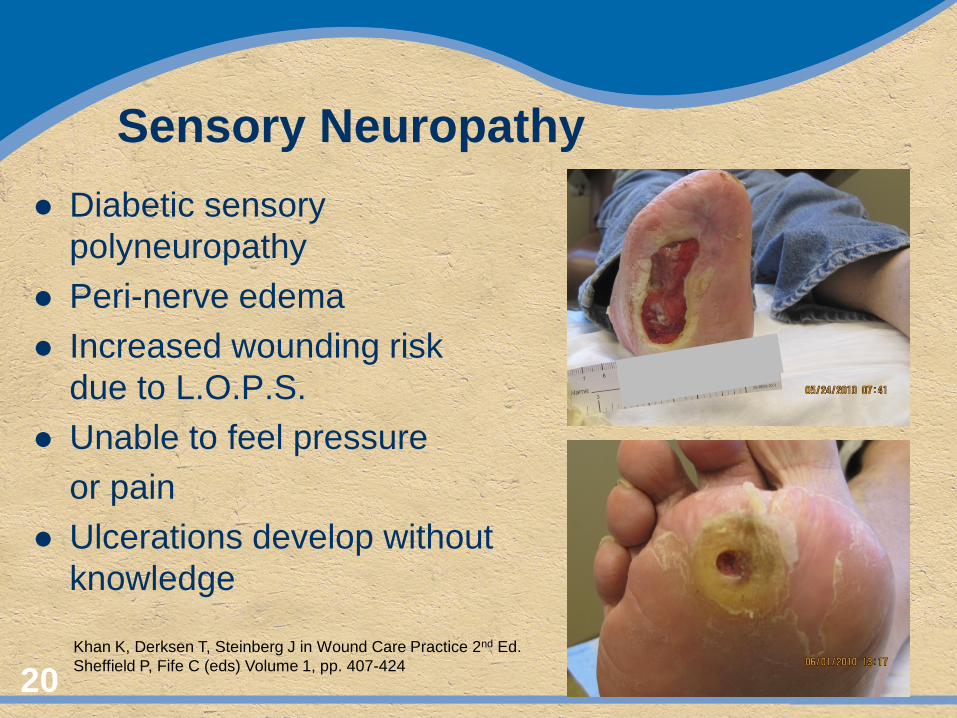
Sensory Neuropathy Diabetic sensory
polyneuropathy Peri-nerve edema Increased wounding risk
due to L.O.P.S. Unable to feel pressure or pain Ulcerations develop without
knowledge
20 Khan K, Derksen T, Steinberg J in Wound Care Practice 2nd Ed. Sheffield P, Fife C (eds) Volume 1, pp. 407-424
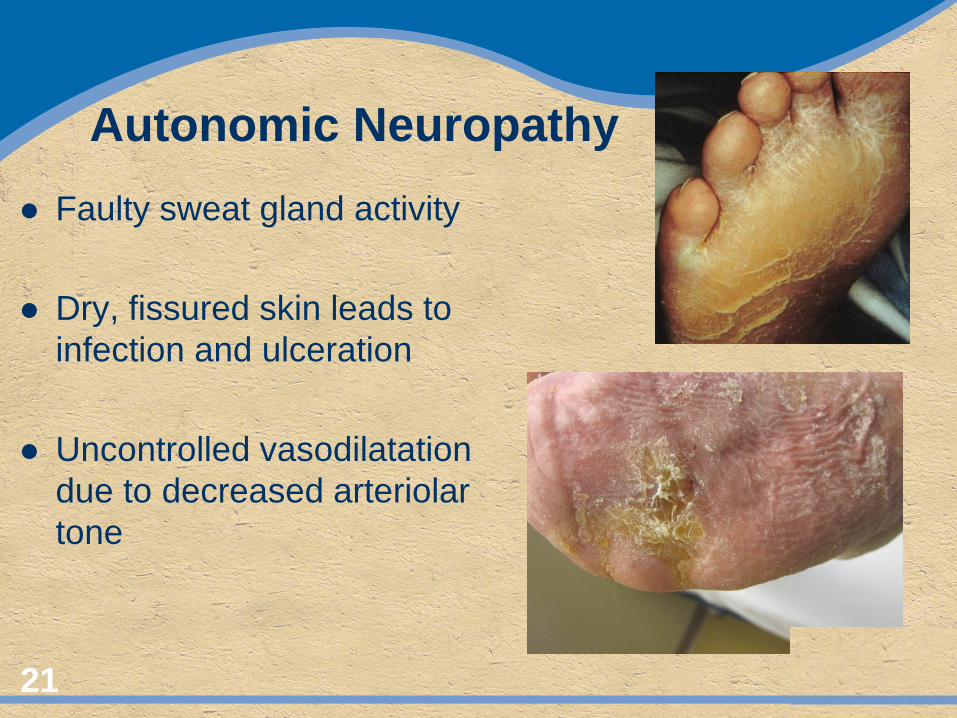
Autonomic Neuropathy Faulty sweat gland activity Dry, fissured skin leads to
infection and ulceration Uncontrolled vasodilatation
due to decreased arteriolar tone
21
Autoimmune Disorders
Rheumatoid Arthritis Crohns Disease Pernicious Anemia Ulcerative Colitis Antiphospholipid Syn. Graves Disease Wegener’s
Granulomatosis 22
Psoriasis Systemic Lupus Polymyositis Dermatomyositis Ankylosing
Spondylitis Sjogren’s Syndrome Autoimmune
Hemolytic anemia
Autoimmune Mechanism Protective component of immune system mounts
attack on normal structures 75% women of childbearing age Auto-antibodies generated against normal body
structures or abnormal materials deposited on normal structures
Auto-antibodies may be continuously, intermittently or transiently produced, determining temporal nature of process
23 Smith AP. Etiology of the problem wound. In: Sheffield PJ, Fife CE. (eds) Wound Care Practice 2nd edition, Volume 1. Best Publishing Co. 3 - 50
Rheumatoid Disease Systemic autoimmune disorder of unknown etiology
Leg ulcerations in 8 – 9% of patients
Ulcer is smooth, irregularly shaped and painful
Felty’s Syndrome; Combination of RA,
splenomegaly, granulocytopenia and leg ulcers
JB Shah. Approach to Commonly Misdiagnosed Wounds and Unusual Leg Ulcers. In: Sheffield PJ, Fife CE (eds) Wound Care Practice 2nd Edition Volume 1. Best Publishing Co. Pp. 581 - 601 24
Rheumatoid Disease
Systemic Treatment: High dose steroids, cyclophosphamide, Dapsone, disease modifying agents
Wound treatment: Standard wound care, bioengineered skin, growth factors
25
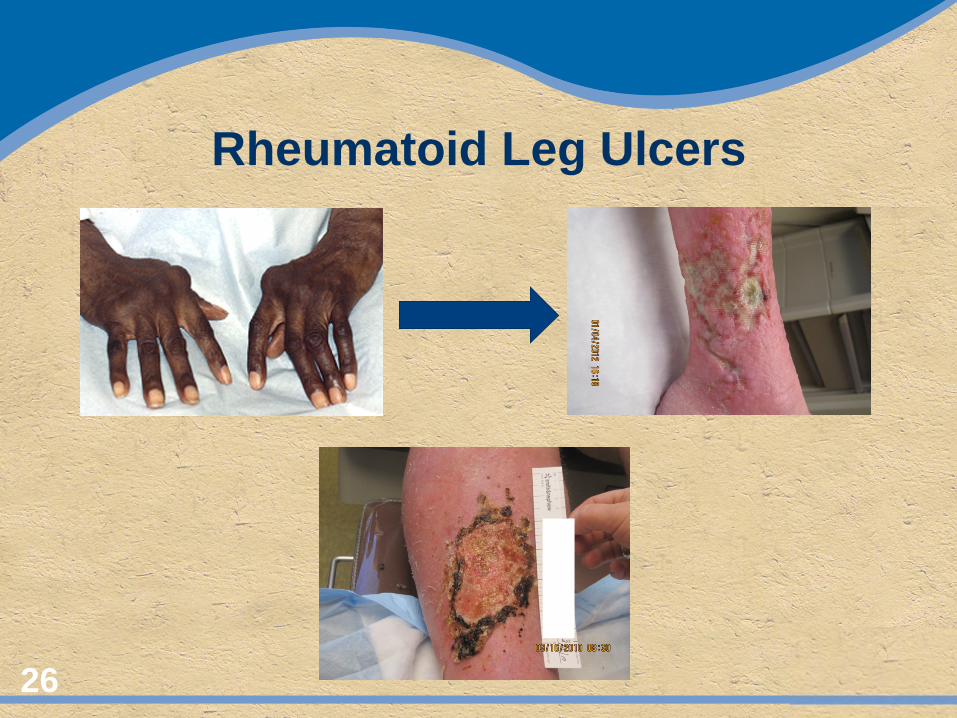
Rheumatoid Leg Ulcers
26
Systemic Lupus (SLE) Systemic autoimmune disease of unknown etiology Well defined margins with purulent wound bed and
varying granulation Surrounding skin normal or erythematous with atrophie
blanche Leg ulcer prevalence approx. 2% Commonly in pre-tibial areas and painful Treatment challenging – systemic and intra-lesional
steroids and topical retinoic acid
27 JB Shah. Approach to Commonly Misdiagnosed Wounds and Unusual Leg Ulcers. In: Sheffield PJ, Fife CE (eds) Wound Care Practice 2nd Edition Volume 1. Best Publishing Co. Pp. 581 - 601
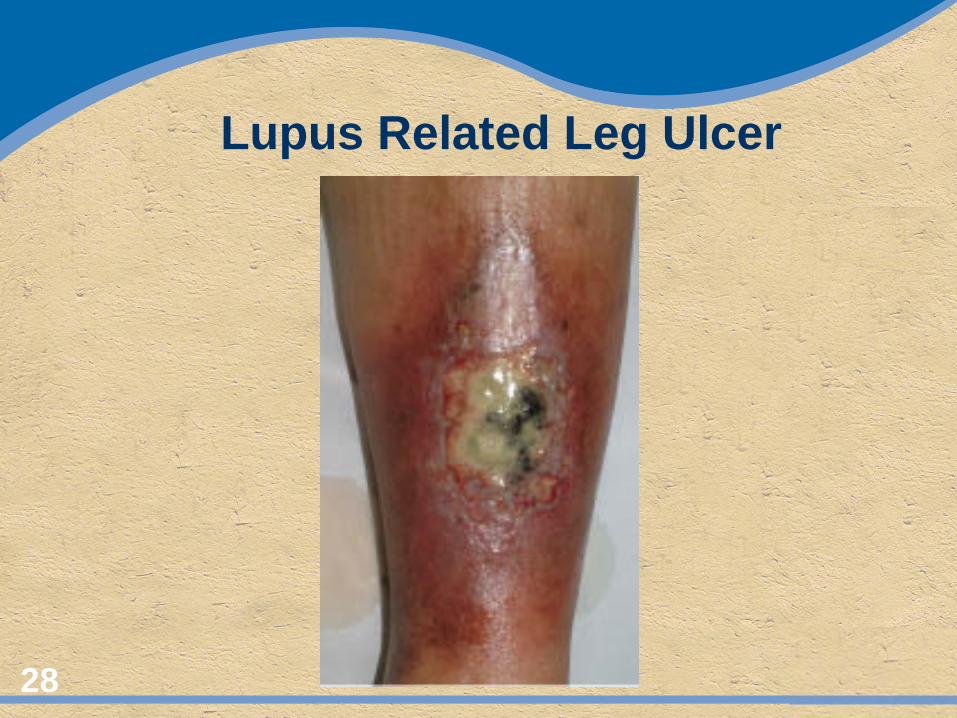
Lupus Related Leg Ulcer
28
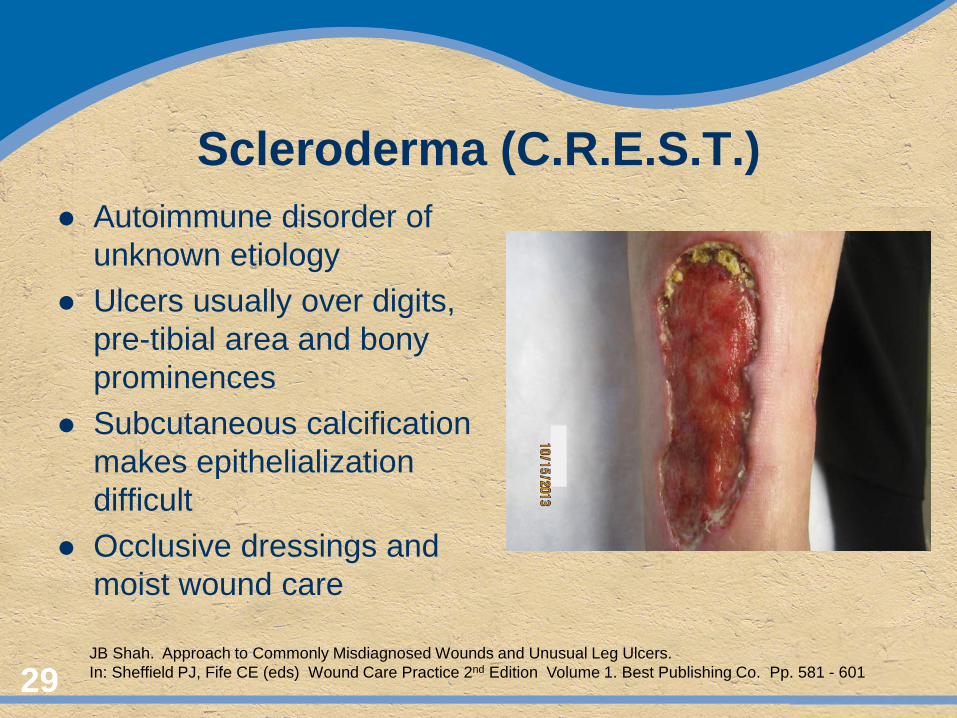
Scleroderma (C.R.E.S.T.) Autoimmune disorder of
unknown etiology Ulcers usually over digits,
pre-tibial area and bony prominences
Subcutaneous calcification makes epithelialization difficult
Occlusive dressings and moist wound care
29 JB Shah. Approach to Commonly Misdiagnosed Wounds and Unusual Leg Ulcers. In: Sheffield PJ, Fife CE (eds) Wound Care Practice 2nd Edition Volume 1. Best Publishing Co. Pp. 581 - 601
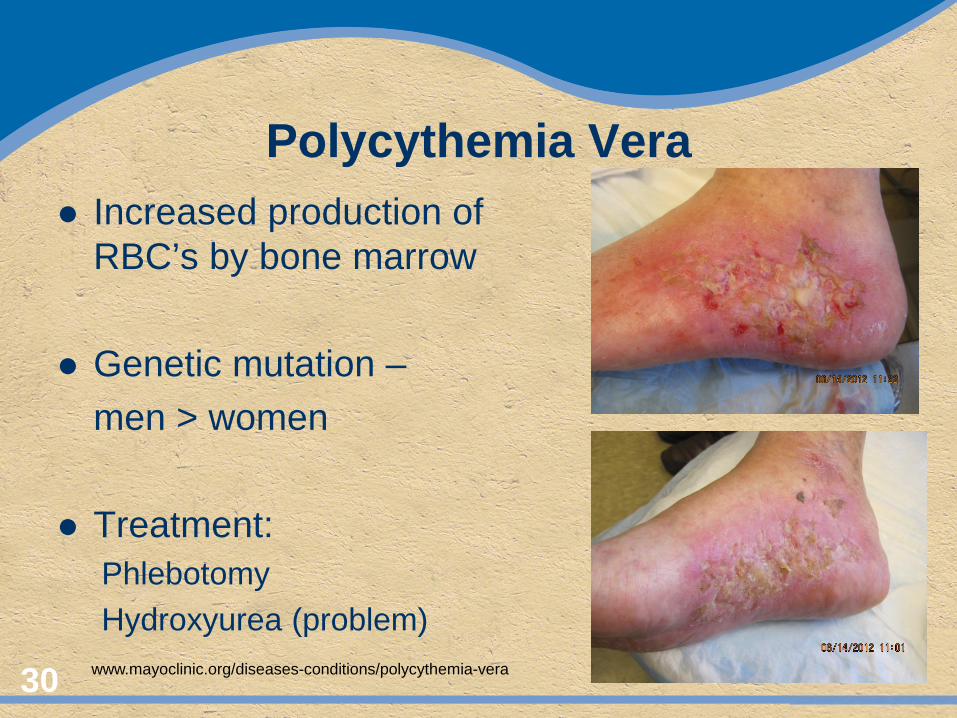
Polycythemia Vera Increased production of
RBC’s by bone marrow Genetic mutation – men > women Treatment: Phlebotomy Hydroxyurea (problem)
30 www.mayoclinic.org/diseases-conditions/polycythemia-vera
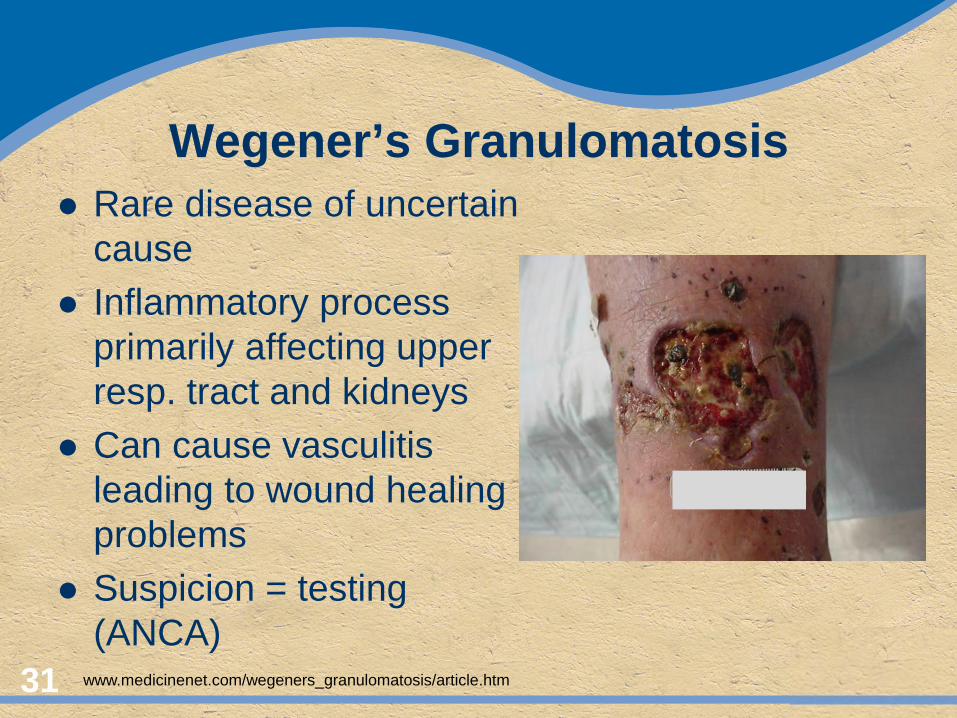
Wegener’s Granulomatosis Rare disease of uncertain
cause Inflammatory process
primarily affecting upper resp. tract and kidneys
Can cause vasculitis leading to wound healing problems
Suspicion = testing (ANCA)
31
www.medicinenet.com/wegeners_granulomatosis/article.htm
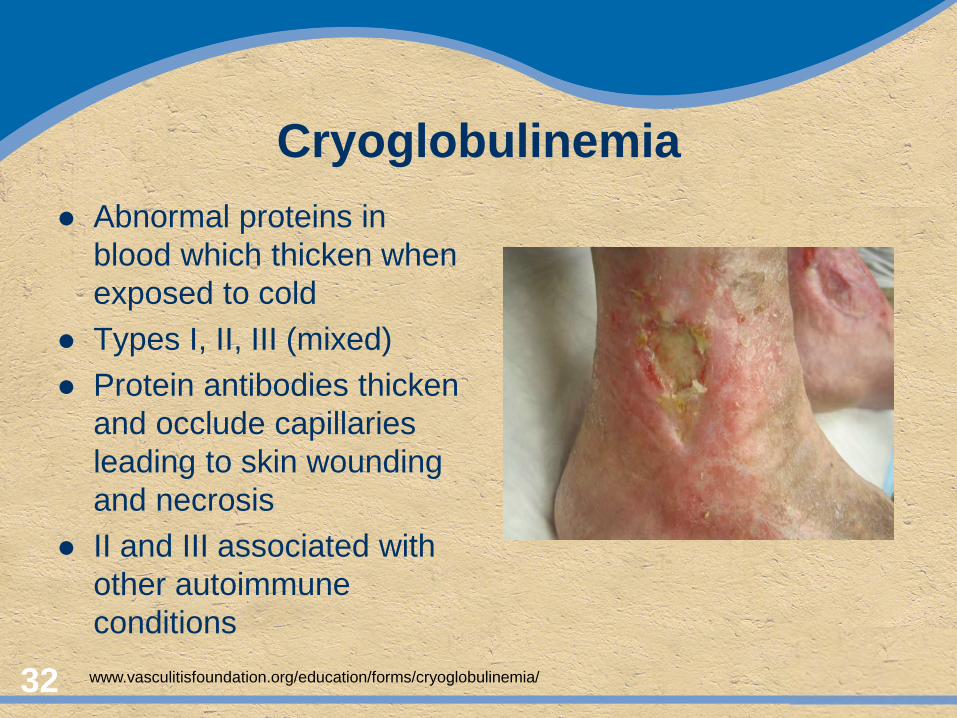
Cryoglobulinemia Abnormal proteins in
blood which thicken when exposed to cold
Types I, II, III (mixed) Protein antibodies thicken
and occlude capillaries leading to skin wounding and necrosis
II and III associated with other autoimmune conditions
32 www.vasculitisfoundation.org/education/forms/cryoglobulinemia/
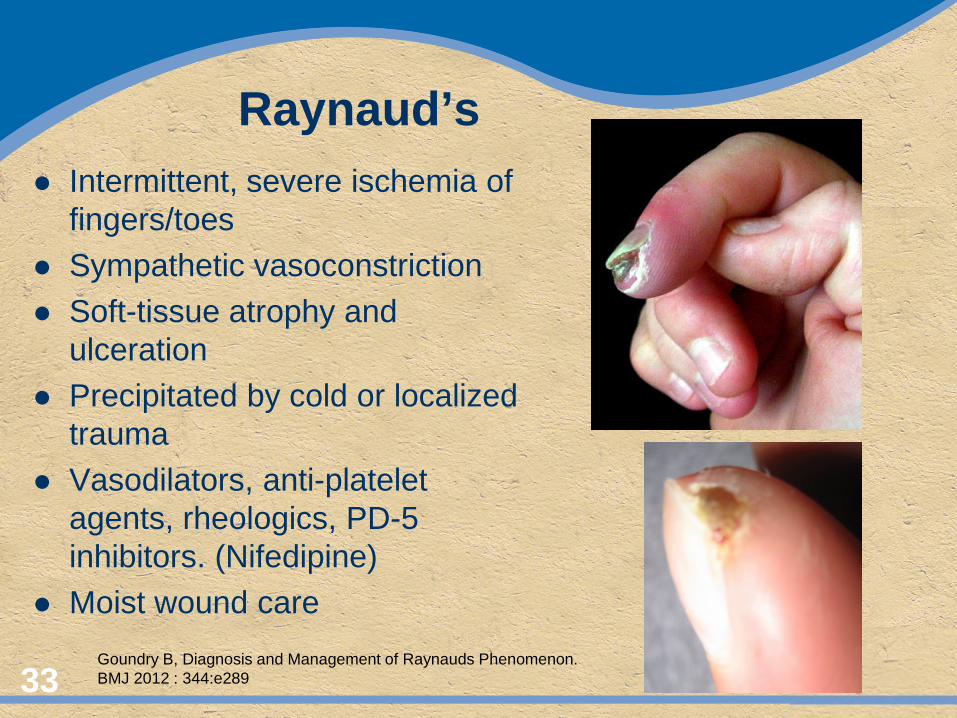
Raynaud’s Intermittent, severe ischemia of
fingers/toes Sympathetic vasoconstriction Soft-tissue atrophy and
ulceration Precipitated by cold or localized
trauma Vasodilators, anti-platelet
agents, rheologics, PD-5 inhibitors. (Nifedipine)
Moist wound care 33
Goundry B, Diagnosis and Management of Raynauds Phenomenon. BMJ 2012 : 344:e289
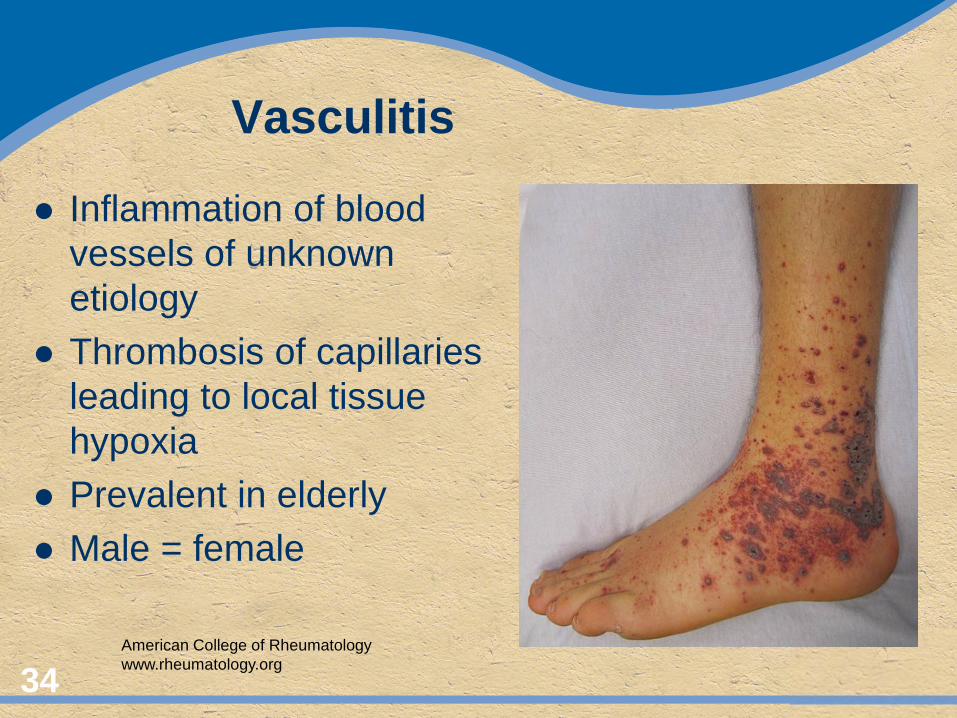
Vasculitis
Inflammation of blood vessels of unknown etiology
Thrombosis of capillaries leading to local tissue hypoxia
Prevalent in elderly Male = female
34 American College of Rheumatology www.rheumatology.org
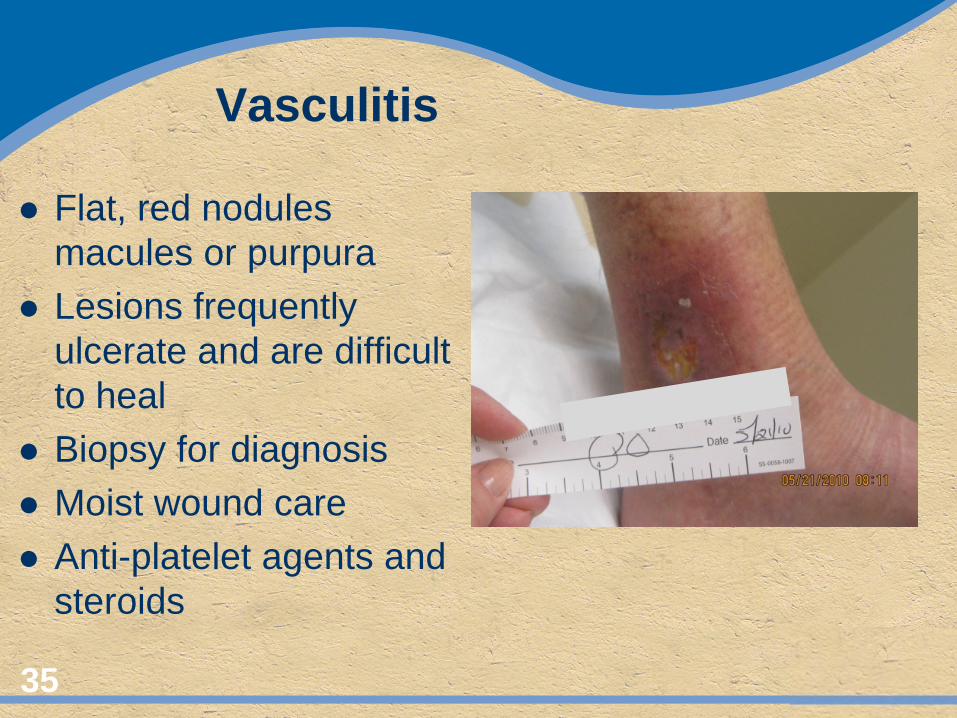
Vasculitis
Flat, red nodules macules or purpura
Lesions frequently ulcerate and are difficult to heal
Biopsy for diagnosis Moist wound care Anti-platelet agents and
steroids
35
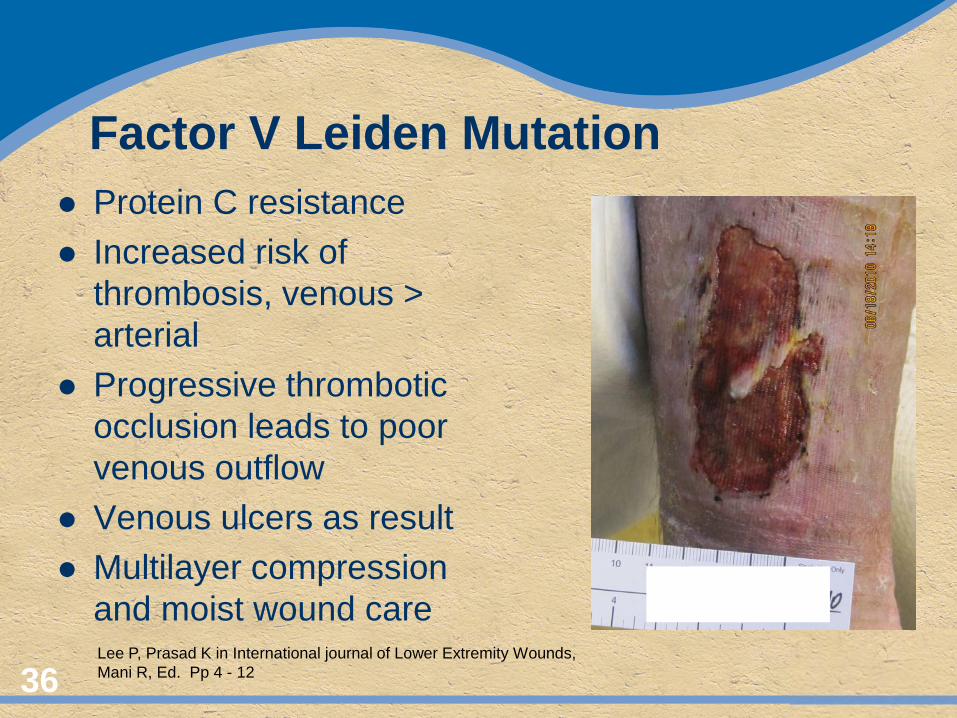
Factor V Leiden Mutation Protein C resistance Increased risk of
thrombosis, venous > arterial
Progressive thrombotic occlusion leads to poor venous outflow
Venous ulcers as result Multilayer compression
and moist wound care
36
Lee P, Prasad K in International journal of Lower Extremity Wounds, Mani R, Ed. Pp 4 - 12
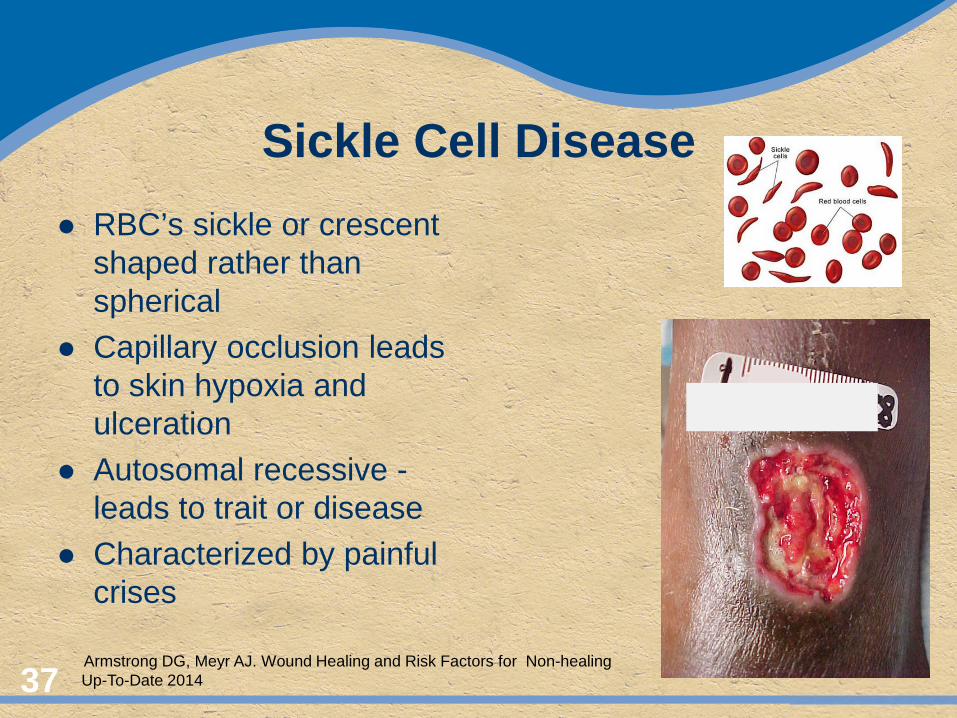
Sickle Cell Disease RBC’s sickle or crescent
shaped rather than spherical
Capillary occlusion leads to skin hypoxia and ulceration
Autosomal recessive - leads to trait or disease
Characterized by painful crises
37
Armstrong DG, Meyr AJ. Wound Healing and Risk Factors for Non-healing Up-To-Date 2014
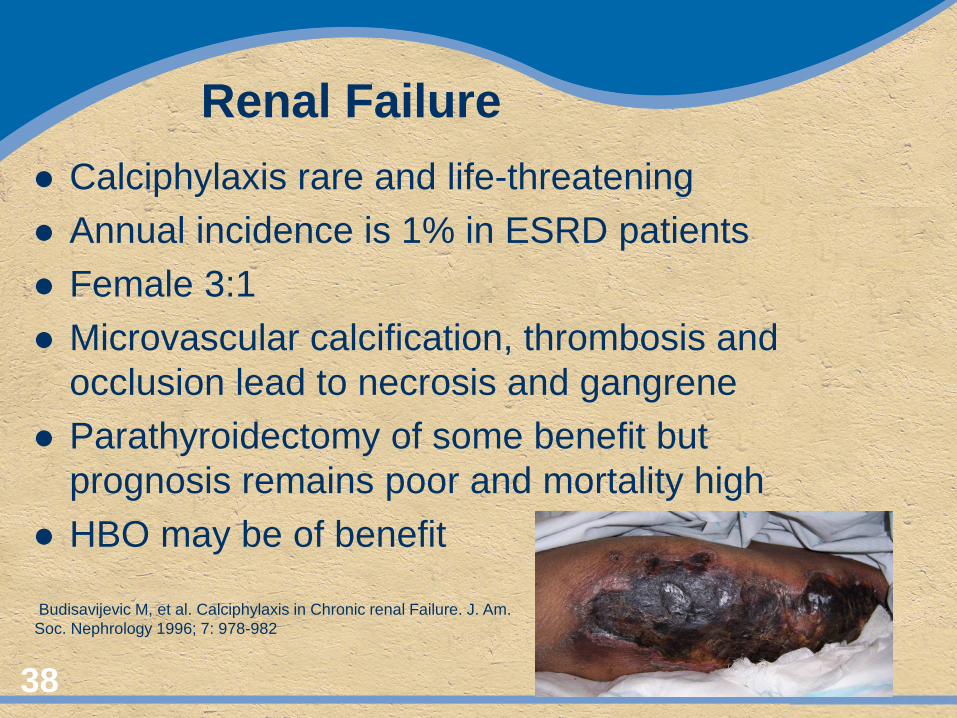
Renal Failure Calciphylaxis rare and life-threatening Annual incidence is 1% in ESRD patients Female 3:1 Microvascular calcification, thrombosis and
occlusion lead to necrosis and gangrene Parathyroidectomy of some benefit but
prognosis remains poor and mortality high HBO may be of benefit
38
Budisavijevic M, et al. Calciphylaxis in Chronic renal Failure. J. Am. Soc. Nephrology 1996; 7: 978-982
Protein Energy Malnutrition Insidious onset. May be rapid. Elderly and lower socioeconomic groups at risk Good food is more expensive than bad food Hyperglycemia delays wound healing Multiple supplements and interventions Early diagnosis important Prealbumin and Transferrin good markers Nutrition/dietary consultation
39 Possinger C. Nutrition & Wound Care – From Treatment to Prevention. Catholic Medical Partners (CMP) IPA April, 2014
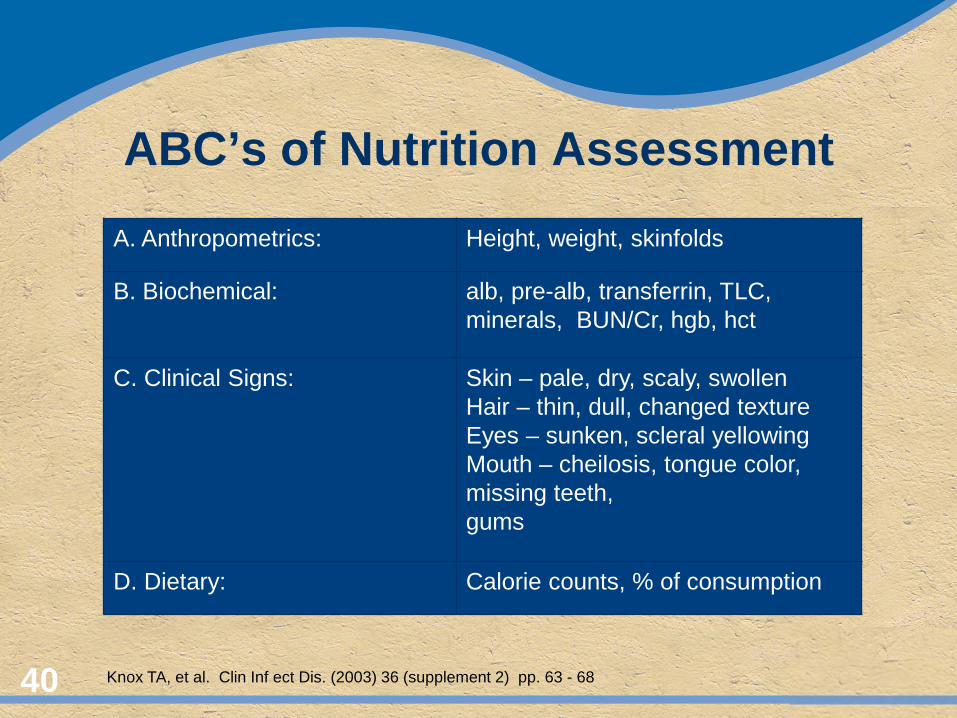
ABC’s of Nutrition Assessment
40
A. Anthropometrics: Height, weight, skinfolds
B. Biochemical: alb, pre-alb, transferrin, TLC, minerals, BUN/Cr, hgb, hct
C. Clinical Signs: Skin – pale, dry, scaly, swollen Hair – thin, dull, changed texture Eyes – sunken, scleral yellowing Mouth – cheilosis, tongue color, missing teeth, gums
D. Dietary: Calorie counts, % of consumption
Knox TA, et al. Clin Inf ect Dis. (2003) 36 (supplement 2) pp. 63 - 68
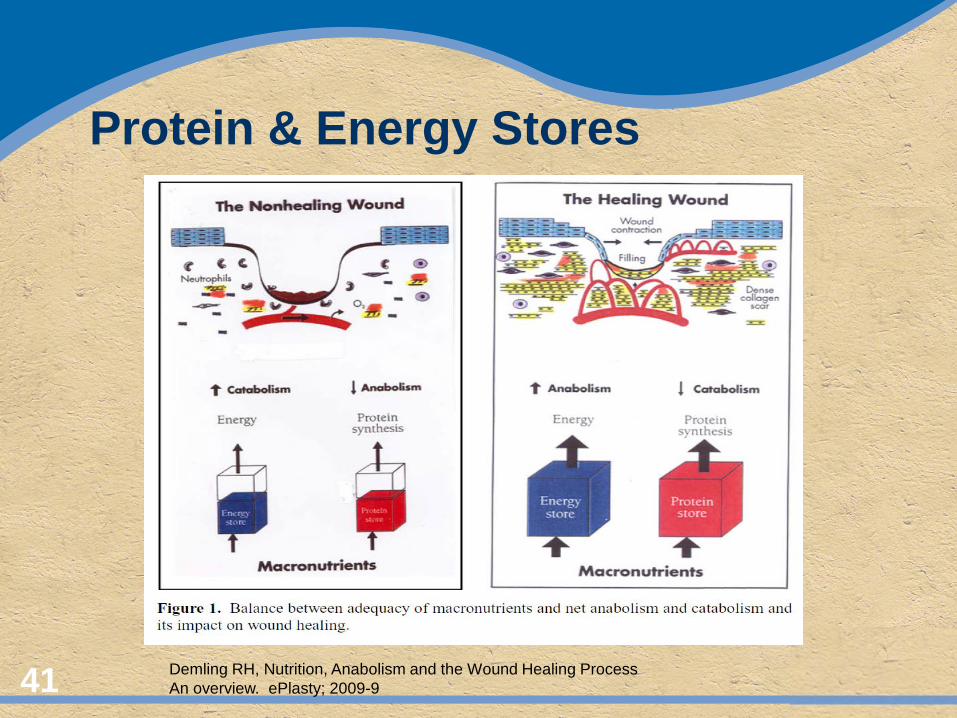
Protein & Energy Stores
41 Demling RH, Nutrition, Anabolism and the Wound Healing Process An overview. ePlasty; 2009-9
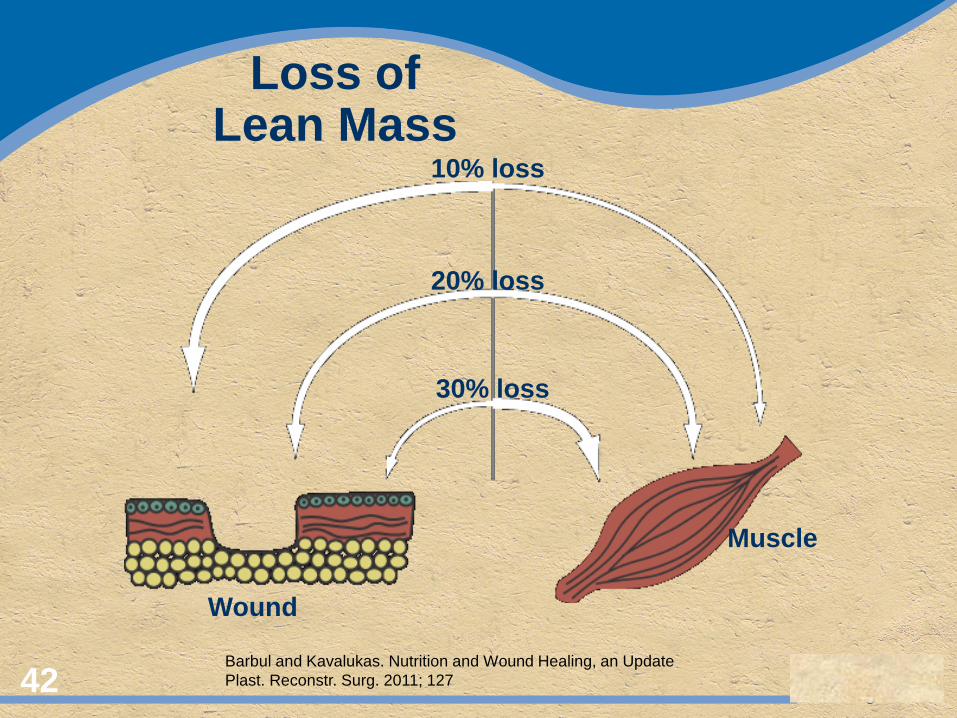
Loss of Lean Mass
42 Barbul and Kavalukas. Nutrition and Wound Healing, an Update Plast. Reconstr. Surg. 2011; 127
10% loss
20% loss
30% loss
Wound
Muscle
Aging ↑ Life expectancy Skin is largest organ we have Thinning of dermis and basement membrane ↓ density of vascularity and nerves ↓ amount of collagen and ability to produce
collagen Multiple comorbidities
43 Cheung C, Older Adults and Ulcers. Chronic Wounds in the Geriatric Population Advances in Skin and Wound Care. January 2010, Vol. 23, No. 1 pp 39-44
Aging
↓ Growth factors ↓ Epithelialization ↓ Angiogenic activity ↑ Multiple meds ↓ mobility and ↑ falls ↑ in mood disorders ↓ percentage of closed
wounds in elderly by 25% as compared to younger population
44 Cheung C, Older Adults and Ulcers. Chronic Wounds in the Geriatric Population Advances in Skin and Wound Care. January 2010, Vol. 23, No. 1 pp 39-44

45
3/28/13
8/26/13
Medications
46
Systemic Steroids NSAIDS Methotrexate Heparin Hydroxyurea Amlodipline/Nifedipine Warfarin Select chemotherapeutics Povidone
Smith RG. Podiatry Management August 2008 www.podiatrym.com
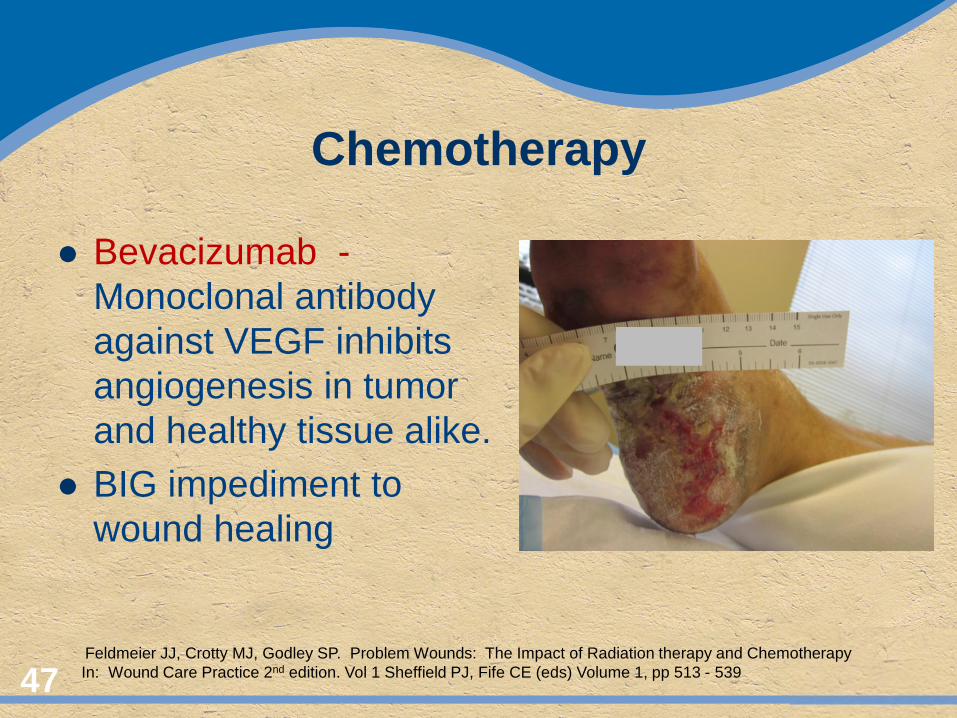
Chemotherapy
Bevacizumab - Monoclonal antibody against VEGF inhibits angiogenesis in tumor and healthy tissue alike.
BIG impediment to wound healing
47
Feldmeier JJ, Crotty MJ, Godley SP. Problem Wounds: The Impact of Radiation therapy and Chemotherapy In: Wound Care Practice 2nd edition. Vol 1 Sheffield PJ, Fife CE (eds) Volume 1, pp 513 - 539
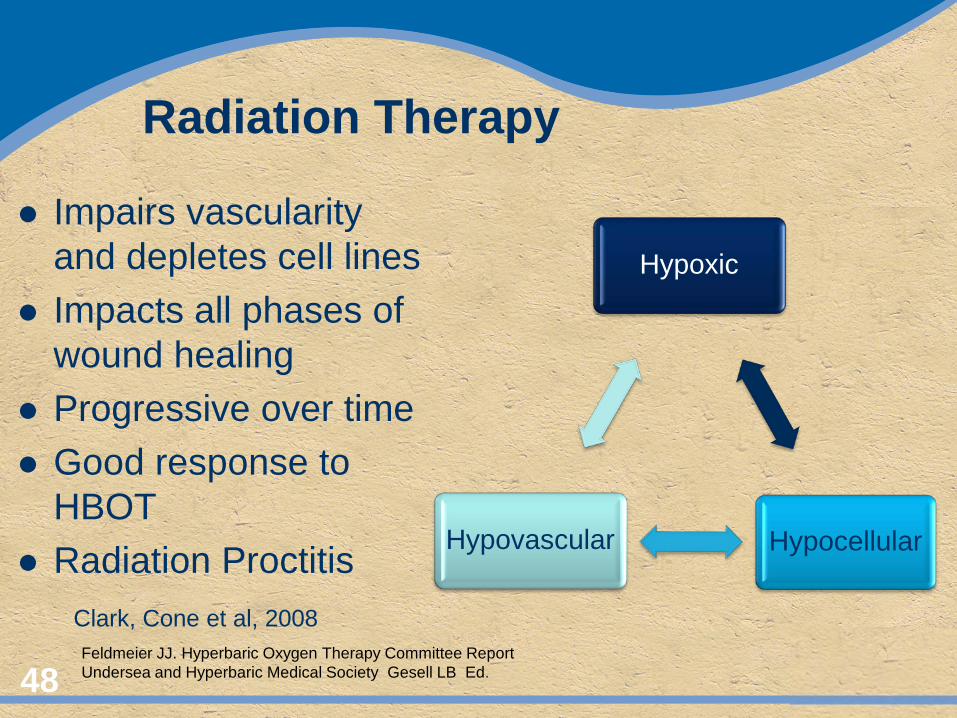
Radiation Therapy
Impairs vascularity and depletes cell lines
Impacts all phases of wound healing
Progressive over time Good response to
HBOT Radiation Proctitis
48
Clark, Cone et al, 2008 Feldmeier JJ. Hyperbaric Oxygen Therapy Committee Report Undersea and Hyperbaric Medical Society Gesell LB Ed.
Hypoxic
Hypocellular Hypovascular
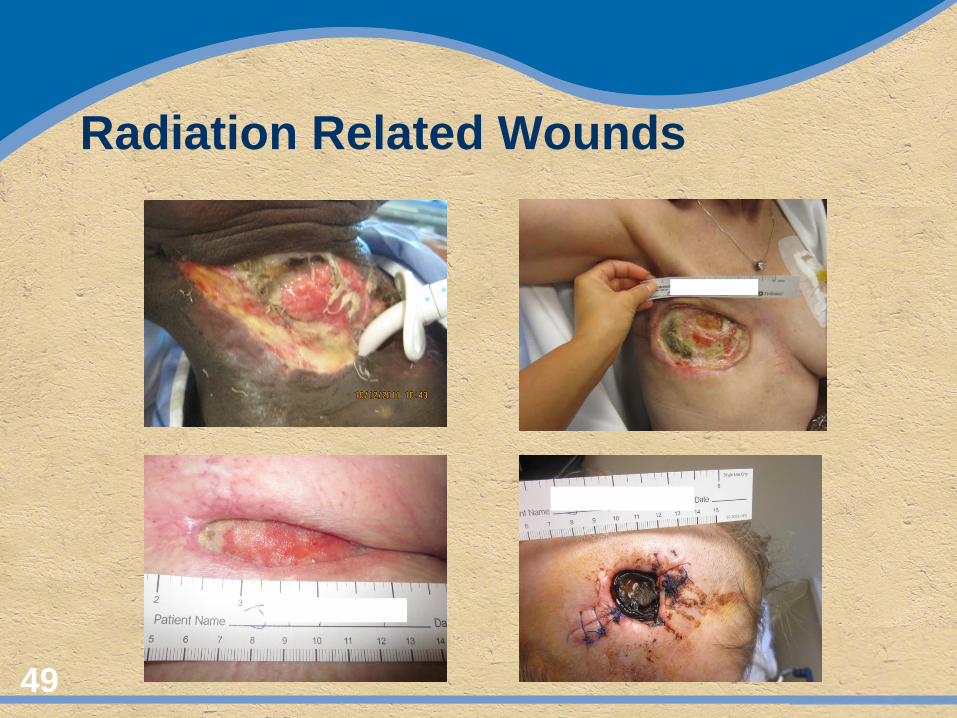
Radiation Related Wounds
49
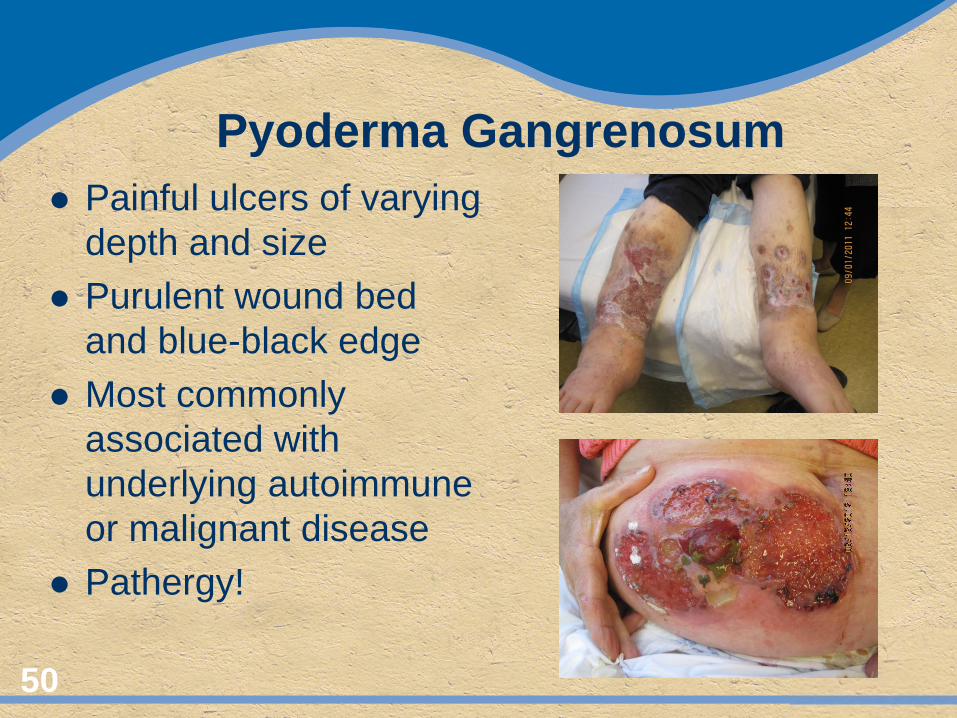
Pyoderma Gangrenosum Painful ulcers of varying
depth and size Purulent wound bed
and blue-black edge Most commonly
associated with underlying autoimmune or malignant disease
Pathergy!
50
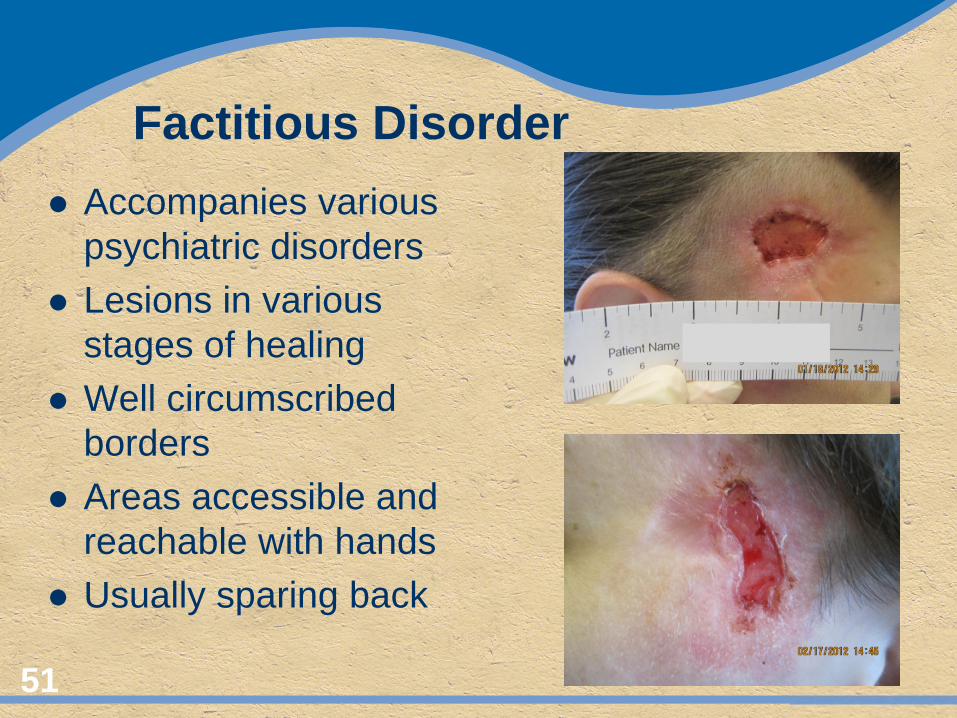
Factitious Disorder Accompanies various
psychiatric disorders Lesions in various
stages of healing Well circumscribed
borders Areas accessible and
reachable with hands Usually sparing back
51
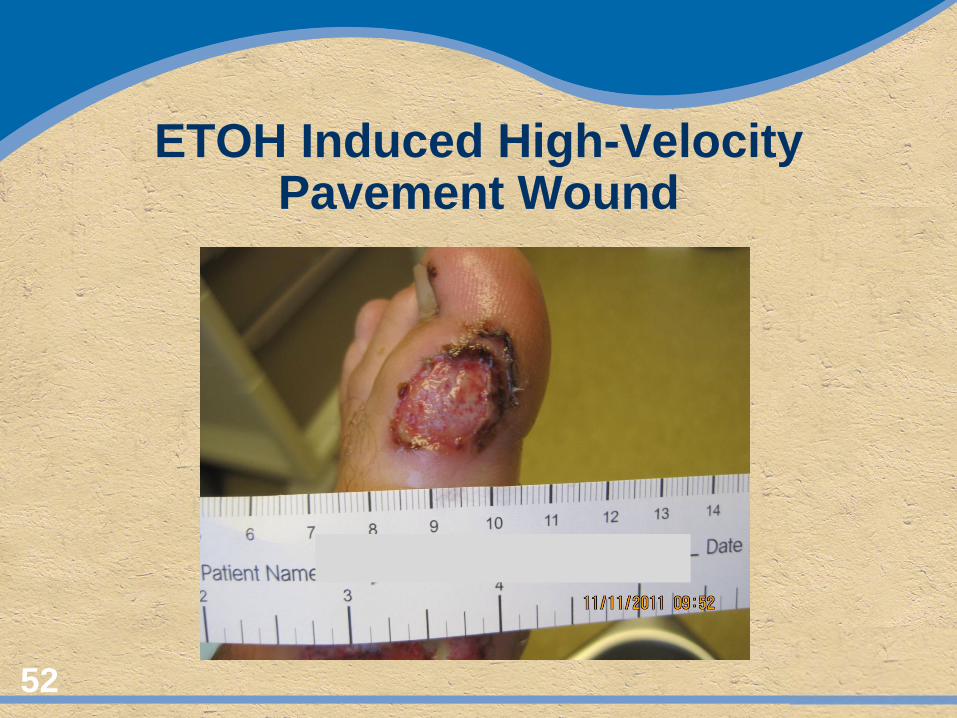
ETOH Induced High-Velocity Pavement Wound
52
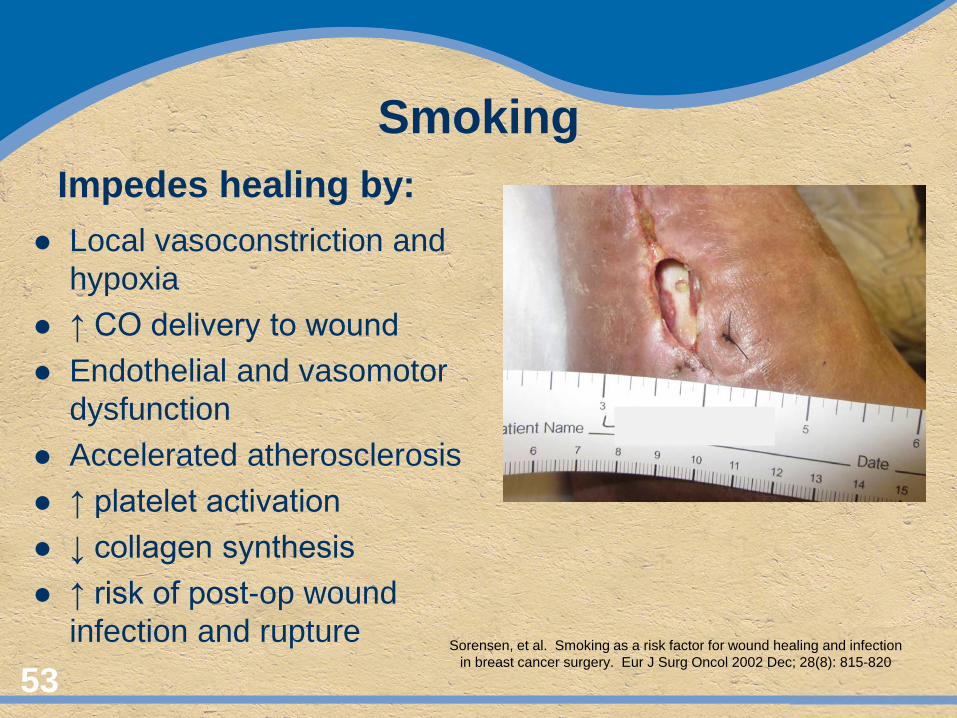
Smoking Impedes healing by:
Local vasoconstriction and hypoxia
↑ CO delivery to wound Endothelial and vasomotor
dysfunction Accelerated atherosclerosis ↑ platelet activation ↓ collagen synthesis ↑ risk of post-op wound
infection and rupture
53
Sorensen, et al. Smoking as a risk factor for wound healing and infection in breast cancer surgery. Eur J Surg Oncol 2002 Dec; 28(8): 815-820

54
Summary
Careful H&P History of prior wounding Lifestyle and mobility questions Nutritional assessment Wound characteristics Prior treatment; successes and failures
Pay attention: When all else fails – take a history!
55