medical devices and the veterans administration
TRANSCRIPT
Medical Devices and the VeteransAdministration
February 1985
NTIS order #PB87-117677

Recommended Citation:Medical Devices and the Veterans Administration—A Technical Memorandum (Washing-ton, DC: U.S. Congress, Office of Technology Assessment, OTA-TM-H-16, February 1985).
Library of Congress Catalog Card Number 85-600509
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402

Preface
This technical memorandum is part of a larger assessment of Federal policies and the medi-cal devices industry, requested by the Senate Committee on Labor and Human Resources. Inits endorsement of the overall assessment, the Senate Committee on Veterans’ Affairs requestedthe Office of Technology Assessment (OTA) to address specifically the activities of the Vet-erans Administration (VA) regarding device development and procurement. The VA is an im-portant provider of medical devices and services for diagnosis, treatment, and rehabilitationof the veteran population.
OTA found that the VA’s current system of medical device-related research, development,evaluation, procurement, and use has a number of weaknesses. Better analytical methods forevaluating and procuring the most appropriate devices at least cost could be applied at variouspoints in technology development and use. In addition, VA research and development, evalua-tion, and procurement could be better integrated. Several new VA programs and committeesmay improve the evaluation and procurement processes and help to integrate the functions, espe-cially the purchase of major new medical technologies.
Valuable guidance was provided by the advisory panel for the OTA assessment on FederalPolicies and the Medical Devices Industry, chaired by Richard R. Nelson, Professor of Econom-ics, Yale University. A large number of persons in the VA and in the medical devices industrywere consulted. John C. Langenbrunner, analyst, is the principal author of this technical memo-..randum. Other key OTA staff involved in its developmentE. Locke, and Jane E. Sisk.
.
JOHN H.Director
were Cynthia P. King, Katherine
GIBBONS
. .Ill

——————
Advisory Panel for Federal Policies and the Medical Devices Industry
Richard R. Nelson, ChairInstitute for Social and Policy Studies, Yale University
New Haven, CT
William F. BallhausInternational Numatics, Inc.Beverly Hills, CA
Ruth FarriseyMassachusetts General HospitalBoston, MA
Peter Barton HuttCovington & BurlingWashington, DC
Alan R. KahnConsultantCincinnati, OH
Grace KraftKidney Foundation of the Upper MidwestCannon Falls, MN
Joyce LashofSchool of Public HealthUniversity of CaliforniaBerkeley, CA
Penn LupovichGroup Health AssociationWashington, DC
Victor McCoyParalyzed Veterans of AmericaWashington, DC
Robert M. MoliterMedical Systems DivisionGeneral Electric Co.Washington, DC
Louise B. RussellThe Brookings InstitutionWashington, DC
Earl J. SaltzgiverForemost Contact Lens Service, Inc.Salt Lake City, UT
Rosemary StevensDepartment of History and Sociology of ScienceUniversity of PennsylvaniaPhiladelphia, PA
Allan R. ThiemeAmigo Sales, Inc.Albuquerque, NM
Eric von HippelSloan SchoolMassachusetts Institute of TechnologyCambridge, MA
Edwin C. WhiteheadTechnicon Corp.Tarrytown, NY

OTA Project Staff: Medical Devices and the Veterans Administration
Roger Herdman, Assistant Director, OTAHealth and Life Sciences Division
Clyde J. Behney, Health Program Manager
Jane E. Sisk, Project Director
Cynthia P. King, Study Director-’
John C. Langenbrunner, Study Director’
Katherine E. Locke, Research Assistant
Ann Covalt, Editor
Virginia Cwalina, Administrative Assistant
Rebecca I. Erickson, P. C./Word Processor Specialist
Brenda L. Miller, P. C./Word Processor SpecialistJennifer Nelson, Secretary3
Principal Contractor
Ralph Bradburd, Williams College
I From December 1983.‘Until November 1983‘Until January 1984.

Glossary of Acronyms
AMVETS—American Veterans of World War II,
BVACIDCTDAVDM&SDODDRGsETIP
FDA
FSSGAOGRECC
HSR&D
Korea, and Vietnam—Blinded Veterans Association—Commercial Item Description—computed tomography—Disabled American Veterans—Department of Medicine and Surgery—Department of Defense—diagnosis-related groups—Experimental Technology Incentives
Program—Food and Drug Administration,
Department of Health and HumanServices
–Federal Supply Schedule—General Accounting Office—Geriatric Research, Education, and
Clinical Centers—Health Services Research and Develop-
ment Service
MEDIPP —Medical District Initiated ProgramPlanning
MR&A —Marketing Research and AnalysisNAS —National Academy of SciencesNMR —nuclear magnetic resonanceNSO —National Service OfficerOTA —Office of Technology AssessmentPSAS —Prosthetics and Sensory Aids ServicePTEC —Prosthetic Technology Evaluation
CommitteePVA —Paralyzed Veterans of AmericaR&D —research and developmentRehabilitation R&D— Rehabilitation Research and
Development ServiceT&E –Testing and Evaluation StaffVA —Veterans AdministrationVAMKC —VA Marketing CenterVAPC —VA Prosthetics CenterVFW —Veterans of Foreign Wars
Statesof the United
vi

Contents
Chapter Page1.
2.
3.
4.
5.
6.
Introduction and Summary . . . . . . . . . . . . . . . . . . . . 3Background and Scope of This Study . . . . . . . . . . . 3Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Veterans and the VA Health Care Delivery System 4Research and Development . . . . . . . . . . . . . . . . . . 5Testing and Evaluation . . . . . . . . . . . . . . . . . . . . . 5Marketing, Procuring, and Supplying Devices . 6Adopting, Using, and Financing Devices . . . . . . 8Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Organization of This Technical Memorandum ... 9
The Veterans Administration and Health Care:An Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Historical Perspective . . . . . . . . . . . . . . . . . . . . . . . . . 13VA Health Care Services . . . . . . . . . . . . . . . . . . . . . . 15
Acute Care Services . . . . . . . . . . . . . . . . . . . . . . . . 15Long-Term Care Services . . . . . . . . . . . . . . . . . . . . 16Ambulatory Care . . . . . . . . . . . . . . . . . . . . . . . . . . 17Other Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
The Veteran Patient Population . . . . . . . . . . . . . . . . 18Veterans’ Service Organizations . . . . . . . . . . . . . . . . 18
Research and Development of Devices . . . . . . . . . . 23Medical Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Research Programs . . . . . . . . . . . . . . . . . . . . . . . . 23Other Medical Research . . . . . . . . . . . . . . . . . . . . . 24
Health Services Research and Development . . . . . . 24Rehabilitation Research and Development . . . . . . . 25
Rehabilitation R&D Centers . . . . . . . . . . . . . . . . . 25Technology Transfer . . . . . . . . . . . . . . . . . . . . . . . . 27
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Testing and Evaluating Devices . . . . . . . . . . . . . . . 33Prototype Devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Commercially Available Devices . . . . . . . . . . . . . . . 35
The VA Prosthetics Center . . . . . . . . . . . . . . . . . . 35Testing and Evaluation Staff, VA Marketing
Center . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Marketing, Procuring, and Supplying Devices . . . 45Prototype Devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Commercially Available Devices . . . . . . . . . . . . . . . 47
Marketing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Procurement and Supply . . . . . . . . . . . . . . . . . . . . 48
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Adopting, Using, and Financing Devices . . . . . . . . 61Veteran Eligibility for Program; and Services . . . .
Income Maintenance . . . . . . . . . . . . . . . . . . . . . . . .Health and Medical Care. . . . . . . . . . . . . . . . . . . .
VA Financing and Resource Allocation . . . . . . . . .Management Initiatives . . . . . . . . . . . . . . . . . . . . .
Adoption and Use of Devices . . . . . . . . . . . . . . . . . .Rehabilitative Devices . . . . . . . . . . . . . . . . . . . . .Medical Equipment and Supplies . . . . . . . . . . . .Social and Political Forces. . . . . . . . . . . . . . . . . . .
Appendix A: Acknowledgments and Health ProgramAdvisory Committee . . . . . . . . . . . . . . . . . . . . . . . . . .
616162636366667071
77
PageAppendix B: Medical Devices and the Veterans
Administration: The Perspective of Veterans’Service Organizations . . . . . . . . . . . . . . . . . . . . . . . . . 80
Appendix C: Veterans Administration Procurementand the Market for Medical Equipment . . . . . . . . . 86
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
List of Tables
Table No. Page1.
2.3.
4.
5.
6.
7.
8.
.
Summary of Rehabilitation Research andDevelopment Projects, Fiscal Year 1983 . . . . . . . . . 26Veterans Administration R& D Budget Overview . 27Selected Device Purchases by the VeteransAdministration Using Federal Supply ScheduleContracts, Fiscal Year 1983 . . . . . . . . . . . . . . . . . . . . 49Veterans Administration Supply Support toOther Federal Facilities, Fiscal Year 1982 . . . . . . . 50Priority Purchasing Sources for VA MedicalCenters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Outlays for Veterans’ Benefits and Services,Fiscal Years 1981-83 . . . . . . . . . . . . . . . . . . . . . . . . . . 63Sample Rehabilitative Devices Distributed toVeterans, Fiscal Year 1982. . . . . . . . . . . . . . . . . . . . . 68VA Controlled Item List for Medical and DentalEquipment, 1982 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
C-1. ‘Sum of Absolute Values of AnnualPercentage Changes in Vendors’ VAMarketing Center X-ray Equipment MarketShares, 1979-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
C-2, Annual VA Marketing Center Procurementof CT Scanning Equipment, 1979-82 . . . . . . . . . . 89
C-3. Annual Percentage Change in VA MarketingCenter Procurement of Nuclear MedicalEquipment, 1979-82 . . . . . . . . . . . . . . . . . . . . . . . . 92
C-4. Changes in Rankings of Four Largest Sellersof Nuclear Medical Equipment Throughthe VA Marketing Center, 1979 -82 . . . . . . . . . . . 92
C-5. Sum of Absolute Values of Year-to-YearPercentage Changes in Vendors’ VA MarketingCenter Nuclear Medical Equipment MarketShares, 1979 -82 . . . . . . . . . . . . . . . . . . . . . . . .......92
List of Figures
Figure No. Page1.
2.
3.4.5.6,
‘The Development and Diffusion of Medical -
Technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Organization Chart of theVeterans Administration, May 1984 . . . . . . . . . . . . 7VA Department of Medicine and Surgery . . . . . . . 14Medical Center Hospital . . . . . . . . . . . . . . . . . . . . . . 16The Innovation Process . . . . . . . . . . . . . . . . . . . . . . . 46Veterans Administration, Department of Medicineand Surgery Medical Districts, 1983 . . . . . . . . . . . . 64
vii

Chapter 1
Introduction and Summary

Chapter 1
Introduction and Summary
BACKGROUND AND SCOPE OF THIS STUDY
Many medical devices have been developed inrecent years, and medical practice has changedaccordingly, lengthening and improving the livesof American people.l In serving its special popula-tion, the Veterans Administration (VA) is one in-creasingly important provider of these sophisti-cated medical devices and services for diagnosis,treatment, and rehabilitation.
This technical memorandum was prepared aspart of OTA’s assessment of Federal Policies andthe Medical Devices Industry, conducted at therequest of the Senate Committee on Labor andHuman Resources, with the endorsement of theSenate Committee on Veterans’ Affairs. Thememorandum responds specifically to the SenateCommittee on Veterans’ Affairs request for infor-mation on the VA’s role in device developmentand procurement.
The VA health care delivery system is now thelargest in the Nation, with 172 medical centers,98 nursing homes, 16 domiciliaries, and 226 out-patient clinics,23 The VA employs the full-timeequivalent of almost 200,000 physicians, dentists,nurses, and administrative and support person-nel. An estimated 30 million veterans are eligible
‘Medical devices encompass an enormous variety of supplies andequipment, from frequently purchased inexpensive items, such asbandages and syringes, to infrequently purchased expensive ones,such as clinical laboratory and imaging equipment. In this studythe definition of a medical device is taken from the 1976 MedicalDevice Amendments to the Food, Drug, and Cosmetic Act (PublicLaw 94-295). They define a medical device as any instrument, appa-ratus, or other similar or related article that is intended to prevent,diagnose, mitigate, or treat disease or to affect the structure or func-tion of the body. Drugs, which achieve their effects through chem-ical action within the body, are separately defined.
‘Many VA medical facilities are actually self-sustaining commu-nities, with a medical center, power plant, restaurant, fire depart-ment, garage, warehouse, movie theater, library, pharmacy, apart-ments, recreation areas, and business offices—with all the needs thatthese facilities require to operate. Medical facility purchases of equip-ment and supplies, therefore, also include items and services thatcannot be strictly classified as medical devices (146).
3The Hospital Corp. of America, a private, “for-profit” hospitalchain, has more facilities, but accounts for revenues only about halfthe size of the VA’s health care delivery budget (32).
for its health care services, and the VA supportsa full range of these services. These same charac-teristics make the VA an excellent setting for eval-uating medical devices and technologies (109,118).
Since the late 1940's the VA has been an impor-tant source of research and development funds,especially for rehabilitative technologies and de-vices. The VA evaluates new equipment for safetyand technical performance. Its Office of Procure-ment and Supply buys many medical devices; itsmedical facilities acquired nearly $1.3 billion inequipment and supplies in fiscal year 1982 alone.4
The VA is also a significant part of the marketfor devices such as prosthetics and wheelchairsthat are designed for disabled people. In addition,other organizations, such as the Department ofDefense, refer to the VA’s supply catalog in mak-ing procurement decisions.
This technical memorandum emphasizes inter-nal VA policies and procedures related to medi-cal devices. It provides information from three dif-ferent perspectives: that of the veteran as aconsumer, that of the device industry as a sup-plier, and that of the VA itself. Topics addressed,for example, include the VA’s effect on privateresearch and development and decisionmakingmore generally.
Research in the biomedical sciences, such asphysiology and anatomy, provides the knowledgeto develop diagnostic, preventive, and therapeu-tic devices. However, much of the basic researchthat leads to these devices is also performed insuch fields as physics, chemistry, and electronics.This situation makes the creation and productionof devices especially complex and difficult to ana-lyze (7).
Nonetheless, several stages of technological de-velopment and diffusion can be identified. Ini-
4Domiciliaries are homes where food, clothing, and necessary med-ical services are provided to ambulatory veterans.
3

——— .
4
tially, the results of basic and applied research are even more costly and lengthy than developing theconsulted in preparing specifications and build- prototype. Following development, facilities foring prototype devices (fig. 1). The next stages, manufacturing the device must be planned andrefining the prototype for marketing and testing constructed, and marketing efforts begun. Finally,its safety, reliability, and performance, may be devices are manufactured, purchased, and used.
Figure 1 .—The Development and Diffusion of Medical Technologies
Extenlof
use
\\
\Innovation
Basic Applied Targeted First Clinical Early Late Acceptedresearch research development human trials adoption adoption practice
Basic research Applied R&D and testing DiffusionSOURCE: Office of Technology Assessment, Development of Medical Technology: Opportunities for Assessment Washlngton, DC US. Government Printing Office, stock
No. 052-003-00217-5, August 1976), as amended.
SUMMARY
Veterans and the VA Health Care with non-service-connected disabilities who areDelivery System unable to obtain or pay for needed medical care
are both eligible for rehabilitative and other com-Among congressionally mandated benefits are prehensive medical services. Several other groups
health care services for eligible veterans. Eligibility of veterans have been declared eligible for VAdetermination is complex but in brief, veterans health care benefits without being unable to pay:with service-connected disabilities and veterans those age 65 and over; Medicaid-eligible veterans;

5
former prisoners of war; veterans exposed todioxin and other defoliants, such as Agent Orange,during the Vietnam War; and veterans exposedto nuclear testing or who served in Hiroshima orNagasaki, Japan, between September 11, 1945,and July 1, 1946. Priorities must be establishedin providing for these groups because VA medi-cal expenditures are limited. Veterans with serv-ice-connected disabilities are accorded top priorityfor medical and rehabilitative care, but approx-imately 80 percent of VA patients have non-service-connected disabilities.
Health benefits are administered by the VA De-partment of Medicine and Surgery, whose respon-sibilities include patient care, research, and edu-cation. Acute care for eligible veterans withmedical, surgical, and psychiatric problems is pro-vided in the VA medical centers, most of whichare affiliated with medical schools. The VA paysfor some care in non-VA hospitals, but usuallyonly for veterans with service-connected disabil-ities. It provides ambulatory care in its outpatientclinics, although it also pays for some private phy-sician visits on a fee-for-service basis. The VA hasan extensive long-term care system, includingnursing homes, domiciliaries, State veterans’homes, hospital-based home care, geriatric daycare, hospice care, and community nursing homecare.
A number of veterans’ service organizationsparticipate in the VA’s delivery of health care. Thelargest of these organizations are The AmericanLegion, the Veterans of Foreign Wars, and theDisabled American Veterans. Nationally, thesegroups attempt to influence legislation. Locally,they support community programs and often havean important influence on VA hospitals. Admin-istrators respond to their inquiries and complaintsand usually try to consult these organizations dur-ing major planning. Several veterans’ service orga-nizations have representatives on national advi-sory bodies to the VA and can influence nationalVA health care policy.
Research and Development
The Federal Government’s role in the researchand development of devices, especially in pros-thetic and disability-related research, dates back
to the 1930s and 1940s. The VA and the Depart-ment of Defense conducted much of the initial re-search on prosthetic devices. Since 1947 the VAhas spent over $30 million on prosthetic deviceresearch alone, while its other research and de-velopment has also grown.
Research and development falls under threeServices: Medical Research, Health Services Re-search and Development, and Rehabilitation Re-search and Development (Rehabilitation R&D).Rehabilitation R&D affects the medical devicesindustry most directly, although the Medical Re-search Service uses major medical equipment andalso clinically evaluates and monitors such devicesas cardiac pacemakers. Rehabilitation R&D con-centrates on prototype devices in three generalareas: prosthetics and amputation (especiallylower limb), spinal cord injury (in developingwheelchairs), and sensory aids (especially for thevisually impaired).
Increased funding for Rehabilitation R&D maybe warranted, especially for the full developmentof devices, since in the past some potentiallyworthwhile prototypes seem to have been aban-doned in early stages. This problem results in partfrom the VA’s lack of structured programs todisseminate information on research and devel-opment. The VA is now addressing this problemof technology transfer through its Office of Tech-nology Transfer and an agreement with the De-partment of Commerce to disseminate informa-tion on promising technologies. VA procurementprocedures have also presented a problem for VAresearch: long delays in obtaining needed researchequipment.
Testing and Evaluation
Once devices are commercially available, theVA may adopt them for use in its facilities or byveteran beneficiaries only after appropriate VAtesting and evaluation. The Prosthetics and Sen-sory Aids Service evaluates rehabilitative devices,and the Office of Procurement and Supply testsand evaluates other types of medical equipment,such as X-ray equipment.
The VA has been active in standards develop-ment and has provided information on its workin this area to other public and private health care

6
delivery groups. Throughout the 1970s, the VAincreasingly used standards in its prosthetics andsensory aids programs. Not only were devicesevaluated, but they were also tested for com-pliance with set standards. Concern grew aboutusing the standards developed for existing tech-nologies to evaluate and purchase new rehabili-tative devices. Newer standards, therefore, haveemphasized performance requirements. This pol-icy has attempted to allow innovation and yet toprovide adequate control for patient safety andwelfare; its success is not yet clear.
The Testing and Evaluation Staff of the VAMarketing Center in Hines, Illinois, tests andevaluates medical devices and systems purchasedby the VA. The staff is part of the Office of Pro-curement and Supply, not part of the Departmentof Medicine and Surgery (fig. 2). Medical devicesare selected for evaluation through requests byVA medical centers, manufacturers, or the VACentral Office, as well as through the Testing andEvaluation Staff itself. Factors affecting selectioninclude potential volume and interest on the partof the VA. Tests are usually consumer researchtests, although sometimes other types of tests areconducted in cooperation with the Medical Re-search Service, the Department of Defense, or out-side private testing laboratories. Evaluations areadvisory and do not obligate VA medical centersto purchase particular products.
Both methodological and organizational prob-lems have been identified in VA testing andevaluation. The VA’s several testing and evalua-tion units may duplicate efforts. In addition, theunits lack control in carrying out experimentalprotocols. New organizational plans may ame-liorate these problems if they are implemented.Comparative evaluations could be good addi-tional sources of information for procurementdecisionmaking.
Marketing, Procuring, andSupplying Devices
The Marketing Research and Analysis Programat the VA Marketing Center is a procurement re-source that gathers and analyzes information onthe range and quality of commercially availableproducts and their compatibility with VA needs.
The size of the VA market allows it to buy medi-cal supplies economically through centralized pro-curement. VA centralized procurement for itsmedical centers and for other Government agen-cies encompasses several programs. There isevidence that centralized VA procurement of somemedical devices, such as catheters, needles, syr-inges, surgical blades, and pacemakers, hasenabled the VA to obtain lower prices than otherpublic and private organizations. VA policies onprocurement have also affected the prices of sev-eral types of major medical equipment (as shownby the study presented in app. C).
Under the terms of the most favored customerclause in VA procurement contracts, suppliers arenot allowed to sell their products under similarcontracts to any private buyer at a price lowerthan that offered the VA. This policy has reducedVA procurement costs, although it may also haveincreased costs to private buyers.
Because of the VA’s brand name justificationrequirement, VA hospitals must justify purchas-ing equipment from other than the least-cost sup-plier on the VA list (e.g., based on service avail-ability). Suppliers are anxious to maintain theirshare of the VA market, and it is likely that theylower prices to be competitive given this re-quirement.
VA contracts with suppliers state that pricesmay not be increased during the contract year,and if they decrease prices, the lower price holdsfor the remainder of the year. This firm fixed priceclause protects the VA from price increases dur-ing a year, but suppliers may charge a higher ini-tial price than they would in the absence of theclause.
By law, the public has access to informationon VA Marketing Center procurement prices formedical equipment. This public disclosure require-ment may result in higher procurement costs fortwo reasons. It reduces the so-called retaliationlag (the time before rival companies learn of pricecuts and reduce their own prices in response).Also, the publicly known VA price may becomeprivate buyers’ target price.
The VA Marketing Center does not make vol-ume commitments, which may result in raisingVA prices for many kinds of equipment. This re-
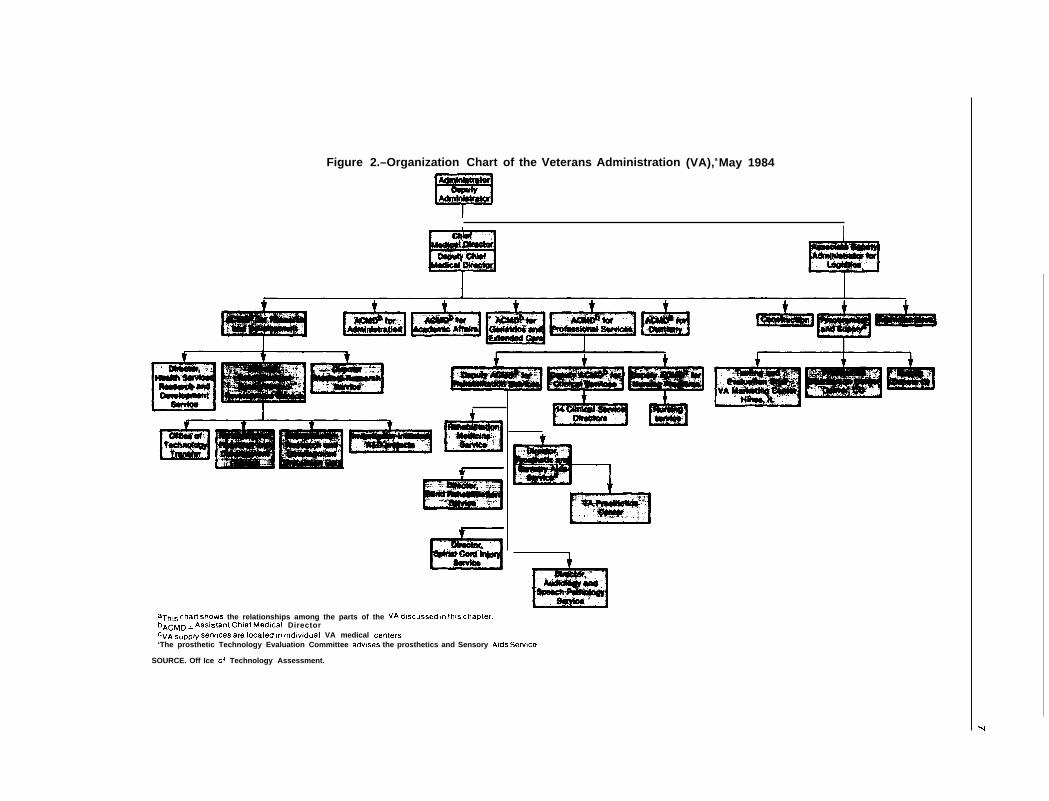
Figure 2.–Organization Chart of the Veterans Administration (VA),a May 1984
I
1
t
aThL~ chart ~h~W~ the relationships among the parts of the VA discussed In this chapter.bACMD = Assl~tant Chief Medical DirectorcvA Supply Sewfces are located In Indiwdual VA medical centers‘The prosthetic Technology Evaluation Committee advises the prosthetics and Sensory Aids se~lce
SOURCE. Off Ice of Technology Assessment.
-1

8
suit depends in some measure on whether theequipment is expensive or inexpensive because ofthe relative transaction costs of contracts, wheresignificant savings may be realized. An unofficialVA policy is to avoid procuring mixed equipmentsystems (components from several manufacturerscombined in systems), to reduce warranty prob-lems. This policy may increase procurement costs,but it may decrease repair costs.
The VA Marketing Center has also encounteredproblems in attempting to ensure product quality,largely because of its increasing use of simplifiedpurchase descriptions in place of more detailedproduct specifications and standards, which arebeing phased out in response to a 1980 Federalpolicy directive. Product quality is likely to im-prove when the VA better integrates all itsinformation-gathering activities (research, devel-opment, testing, evaluation, marketing, etc. ) intopurchasing contract decisions.
Local supply officers are charged with procure-ment for the VA medical centers. The open mar-ket may be used to purchase items not availablefrom centrally managed sources, needed for anemergency, or available at lower prices thanthrough the central Federal Supply Schedule pro-gram managed by the VA. In the early 1960s,open market procurement (i.e., purchases madedirectly by individual VA medical centers) ac-counted for about 10 percent of purchases; thefigure is now about 39 percent. More open mar-ket purchasing permits hospital staff to select man-ufacturers and models that they prefer and,perhaps, to receive orders more quickly. Never-theless, such individual purchases prevent the VAfrom using its potential buying power to gainlower prices through volume purchases.
Adopting, Using, andFinancing Devices
All VA activities relating to medical deviceshave the goal of the adoption and use of good-quality, low-cost medical technologies. Becauseof social and political incentives to overadoptsome medical devices and because of financialconstraints on others, the VA has sporadicallyadopted devices and other technologies, and itsdistribution of resources may not be equitable or
efficient across geographic areas and facilities.More comparative analyses of medical devicesand equipment are needed to ensure better resultsin this regard.
The issue of financing medical devices has in-creased in importance as the population of vet-erans ages and more of them need the assistancesuch devices provide. The high costs of provid-ing unlimited prostheses to veterans, as law re-quires, and the use of high technology in healthcare draw funds from the rest of the VA healthcare activities.
Decisions about adopting and using new med-ical devices would ideally be based on informa-tion about veterans’ needs and the safety, efficacy,and costs of the devices and their alternatives.However, not all needed data are always avail-able, and current VA decisionmaking does notnecessarily consider all the available data. The VAlacks formal processes to decide which VA med-ical centers should adopt new, expensive devicesand to allocate funds among the medical centersfor such purchases.
Because of limited resources, in fiscal year 1981the VA adopted a system of strategic planning,Medical District Initiated Program Planning. Asnew device and equipment requests are madethrough medical district plans, the evaluation oftechnologies could be focused and the adoptionof new technologies could be based on more ac-curate information.
Conclusions
The VA’s current system of medical device-related research, development, evaluation, pro-curement, and use has a number of significantweaknesses. Better analytical methods forevaluating and procuring the most appropriate de-vices at least cost could be applied at variouspoints in technology development and use.
VA research and development, evaluation, andprocurement have often been poorly integrated.The VA’s potential market leverage in procuringdevices, for example, has not been realized instimulating the development of certain devices.Nor have the results of the VA’s own research,development, and evaluation been systematically
9
incorporated in the VA’s procurement and adop-tion decisions.
The VA recently initiated several new programsand committees that may greatly improve theVA’s development and use of medical devices. TheRehabilitation R&D Service’s new EvaluationUnit, which will coordinate and improve thetesting of prototype rehabilitative devices, and theProsthetic Technology Evaluation Committee,which will develop a formal evaluation andcoordination process for commercially availableproducts, are two notable efforts. These improve-ments in evaluation processes may result in more
appropriate adoption and use of medical devicesand other technologies by the VA, and indirectly,by other Government agencies and the privatesector.
A last important sign of the VA’s new direc-tions is the recent formation of a High Technol-ogy Assessment Group to determine future VApolicy on acquiring major new technologies. TheHigh Technology Assessment Group could helpdevelop information for allocating health care re-sources more efficiently and equitably than in thepast.
ORGANIZATION OF THIS TECHNICAL MEMORANDUM
This memorandum groups medical devices intothree general classes: rehabilitative devices (or-thotic and prosthetic devices, such as artificiallimbs), equipment (radiological and laboratorydevices), and supplies (bandages, disposable,etc.). It should be noted, however, that the diver-sity of medical devices defies easy classification.Medical devices include products used for dif-ferent medical purposes (preventive, diagnostic,therapeutic, and rehabilitative) and by differentbranches of medical care (e.g., dentistry, ophthal-mology, orthopedics, and neurology).
Chapter 2 provides the context for discussingpresent VA policies on medical devices and de-scribes briefly the history and characteristics of
the VA health care delivery system. Chapters 3through 6 address the VA’s involvement in re-search and development; testing and evaluation;marketing, procurement, and supply; and financ-ing, adopting, and using devices.
Appendix A acknowledges the valuable assist-ance of the Health Program Advisory Commit-tee and other individuals for their information,advice, and review of drafts. Appendix B reviewsveterans’ service organizations and their perspec-tives on the VA health care delivery system. Ap-pendix C examines VA procurement of eight typesof medical equipment and the effects of VA pur-chasing policies on private manufacturers andbuyers of such medicaI equipment.
25-289 0 - 85 - 2

Chapter 2
The Veterans Administrationand Health Care: An Overview

Chapter 2
The Veterans Administrationand Health Care: An Overview
The Veterans Administration (VA) provides abroad range of services for veterans and their de-pendents. These benefits include compensationpayments for service-related disability or death,pensions based on financial need for totally dis-abled veterans and certain survivors of veteransfor non-service-related disability or death, edu-cation and rehabilitation, home loan guarantees,burial, and–most importantly for this study—free or subsidized hospital, ambulatory, and ex-tended medical care, including nursing home care,to eligible veterans.
VA health care is administered by its Depart-ment of Medicine and Surgery (DM&S), whichhad a budget of $8.1 billion in fiscal year 1983. ’
IThe budget was $6.96 billion in fiscal year 1981 and $7.59 bil-lion in fiscal year 1982. These figures include construction, research,
HISTORICAL PERSPECTIVE
Federal programs for veterans date to the Revo-lutionary War. Until early in this century, how-ever, they were almost exclusively pension pro-grams; what medical and hospital care wasavailable was provided by States or communities.
The VA medical program evolved through aseries of legislative enactments during and afterWorld War I. The war added nearly 5 million peo-ple to the Nation’s veteran population, and newprograms were required to meet their many needs.In 1921 Congress created the U.S. Veterans Bu-reau, which consolidated the functions of severalagencies that had been administering veterans’programs. The veterans’ hospital system was cre-
2Except where noted, this section is adapted from U.S. Congress,Congressional Research Service, Medical Care Programs of the Vet-erans Administration (Report No. 83-99 EPW, Washington, DC,May 16, 1983).
Title 38 of the U.S. Code (sec. 4101) provides thatthe functions of DM&S “. . . shall be those nec-essary for a complete medical and hospital serv-ice, including medical research . . . [and] to carryout a program of training and education of healthservice personnel, acting in cooperation withschools. . . . “ Thus, DM&S has a three-part mis-sion of patient care, research, and education (150).DM&S is administered from the Central Officein Washington, DC, and is headed by a ChiefMedical Director. Specific areas of patient careand program function, such as rehabilitationmedicine, surgery, radiology, and medical re-search, are termed “Services” and are under theCentral Office guidance of Service Directors. Anorganizational chart is shown in figure 3.
and administrative costs, which together account for less than 10percent of all hospital and medical care expenditures (97).
ated in 1922 when 57 Public Health Service hos-pitals were transferred to the Veterans Bureau.The system was constructed rapidly for the manyWorld War I veterans with service-connected in-juries. Within a few years, however, the numberof service-connected cases were no longer suffi-cient to fill available bed space. As a result, in1924 Congress passed legislation expanding eli-gibility for hospitalization benefits to encompassindigent veterans with non-service-connectedhealth needs.
This pattern was repeated after World War II:after the immediate needs of the war’s veteranswere met, the system again had excess capacity
and the process of expanding the scope of medi-cal benefits continued. In recent years most VAhospital patients have been treated for problemsunrelated to military service. Over the years the
13

Figure 3.—VA Department of Medicine and Surgery
.
I I I I 1
SOURCE: U.S. Veterans Administration, Department of Medicine and Surgery, Office of the Chief Medical Director, Washington, DC, Oct. 1, 1982.

15
VA’s medical role has grown in four generaldirections:
m
●
*
●
providing more health care to veterans withnon-service-connected disabilities,providing a greater range of health careservices,training health care personnel and conduct-ing medical research, andproviding some services to certain non-veterans.
Another major development in VA medicalcare after World War II was the affiliation of VAhospitals with medical schools. In the 1920s and1930s the VA hospital system had become some-what isolated from the professional medical com-munity. VA affiliation with medical schools wasviewed as a way to overcome this isolation andimprove the quality of care for veterans. PublicLaw 79-293, which established DM&S within theVA, authorized the affiliation program. On bal-
VA HEALTH CARE
Acute Care Services
SERVICES3
Acute care services are provided mainly in VAhospitals, or medical centers, which are the pri-mary source of medical care for veterans. In fiscalyear 1981 about 1.25 million patients were treatedin VA hospitals, 1.22 million in medical and sur-gical beds and 206,000 in psychiatric bed sections;only about 30,400 were treated in non-VA hos-pitals at VA expense. VA hospital care includesskilled medical and surgical procedures and in-tensive diagnostic and therapeutic services (fig.4). The quality of VA hospital care is generallythought to be enhanced by the affiliations of most
3This section is adapted from U.S. Congress, Congressional BudgetOffice, Veterans Administration Health Care: Planning for 1990(Washington, IX, February 1983).
ance, these affiliations appear to have beenbeneficial to all concerned. The Nation’s veteranshave had better care, and the Nation’s doctorshave been better educated (62).
The VA now provides most of its health careservices in VA hospitals, domiciliaries, nursinghomes, and outpatient clinics. In addition, undercurrent law, the VA may contract for medical carein government or community facilities, but onlyif care either cannot be provided or cannot bemore economically provided in VA facilities. In1981 the VA contracted for nursing home care in2,900 community nursing homes and subsidizedcare on a limited per diem basis at 44 State vet-erans’ homes, including hospitals, nursing homes,and domiciliaries. Noninstitutional care is alsoprovided for veterans through hospital-basedhome care programs, geriatric day care centers,and residential care programs.
VA medical centers with medical, nursing, or den-tal schools.
The number of VA acute care beds has declinedover the last several years. The VA operated anaverage of 82,079 hospital beds during 1981, com-pared to more than 97,OOO beds during 1973.Many changes in the VA system have led to thedecline in total hospital beds, notably a declinein the number of psychiatric hospital beds. Med-ical and surgical beds have also been closedbecause of shorter lengths of stay and shifting pa-tients to outpatient care. Recent legislation re-quires the VA to operate at least 90,000 total hos-pital and nursing home beds (Public Law 97-72)and to have sufficient beds in readiness to sup-port the Department of Defense in times ofdeclared war (Public Law 97-174).

16
Figure 4.—Medical Center Hospital
SOURCE” U S Veterans Administration, VA Organization Manual M-00-1, Change 11, p X-74 (Washington, DC, July 30, 1981)
Long=Term Care Services
The VA provides both institutional and non-institutional long-term care services. Institutionalservices include those of the 101 nursing homeunits associated with VA medical centers andthose provided in community nursing homes,State veterans’ homes, and domiciliaries. Nonin-stitutional care consists of monitoring the healthof patients in their own homes, in congregate(group) homes, and at day care centers. Specialprograms begun in recent years support nonin-stitutional care, such as hospital-based home careand geriatric day care.
VA Nursing Home Care
The VA nursing home units provide the mosthighly skilled and most intensive extended careafter hospitalization, with no time limits. In 1981
the VA operated an average of 8,700 nursinghome beds. Most VA nursing homes are almostfilled: in fiscal year 1982, 54 of 98 VA nursinghomes had occupancy rates above 9S percent.
Community Nursing Homes
The VA also contracts per diem for skilled nurs-ing care at regularly inspected community nurs-ing homes. Over 28,200 veterans were cared forin these homes in 1981. According to the VA, vet-erans are usually placed in such homes when theydo not require the level of care provided in VAnursing homes.
State Veterans’ Homes
State veterans’ homes are facilities establishedby the State for medical and residential care ofveterans. Two VA grant programs support State

veterans’ homes. A per diem program helps theState provide hospital, nursing home, and domi-ciliary care to veterans. Another VA programcontributes to State construction of new domi-ciliary and nursing home facilities and expansionand remodeling of existing facilities. The VA sub-sidized care in State homes for over 24,700 vet-erans in 1981.
VA Domiciliaries
Domiciliaries, the forerunners of the VA pro-grams, date from legislation in 1866 that estab-lished Soldiers’ Homes for disabled veterans. VAdomiciliaries are usually located in the complexof VA medical centers. Veterans placed in domi-ciliaries must be service-disabled or permanentlydisabled and unable to support themselves. Theirhealth often requires some monitoring althoughnot so much as is provided in skilled nursinghomes. In 1981 the VA provided domiciliary carefor over 14,800 persons.
Hospital-Based Home Care
The VA helps patients with residual disabilitiesto remain in their own homes. Patients and theirfamilies are given appropriate instructions inroutine nursing procedures, supervised by ahospital-based treatment team. The team includesa physician, public health nurse, social worker,rehabilitation therapist, and other specialists. Fre-quency of home visits depends on the patient’sneeds and treatment plan. Inpitals served 5,600 patients,minal cancer patients.
Geriatric Day Care
Although several related
1981 teams at 30 hos-one-fifth of them ter-
VA programs are inoperation~the day care program is a new VA proj-ect in which older veterans are helped to returnto their own homes. Under day care programs,veterans continue in rehabilitation at communitycenters or outpatient clinics under VA auspices.
Model programs are in operation at the Chicagoand Boston medical centers and in a communitynear the Loma Linda, California, medical centerin coordination with The American Legion.
Ambulatory Care
The ambulatory care and outpatient clinicalprograms are vital in the VA health care systemas an alternative to hospitalization. The VA oper-ates mental hygiene clinics and day treatmentcenters for psychiatric patients. Clinic services arealso used for care prior to and after hospitaliza-tion. Outpatient clinics also help control chronicconditions, such as arthritis, hypertension, anddiabetes, that are often associated with aging. In1981 more than 15.8 million outpatient medicalvisits were made to VA staff and 2.1 million visitswere made to private physicians funded on a fee-for-service basis by the VA.
Other Services
The VA also operates other outpatient pro-grams to supplement its main hospital and nurs-ing home services. For example, dental care isgiven to eligible veterans and the VA considersit a necessary service for the total care of patientsin acute care or long-term care facilities.
In addition, the VA established Geriatric Re-search, Education, and Clinical Centers (GRECCS)for the growing number of elderly veterans. Thereare currently eight such centers, although 1!5 areauthorized by legislation (Public Law 96-330).GRECCS are located at VA medical centers anduse the research and clinical activities of affiliatedmedical schools. One goal of the program is totrain new geriatric practitioners, teachers, and re-searchers.
The growing aged veteran population is a ma-jor concern of the VA. By 1990 practically allWorld War II veterans, now 12 million persons,

18
will be 65 or older. Although most will be eligi- beds and should have more than 13,000 afterble for free VA health care, only about 2 million 1987. If this number is insufficient, the VA mayare expected to apply for such health care, in- rely on alternative sources such as community oreluding 400,000 service-disabled veterans. The VA State nursing homes.proposes to construct additional nursing home
THE VETERAN PATIENT POPULATION
The VA provides health benefits only to theeligible population. Those eligible are primarilyveterans with service-connected disabilities, thosedischarged from active service because of illnessor injury incurred or aggravated in the line ofduty, former prisoners of war, those exposed toAgent Orange in Vietnam, veterans 65 or older,and veterans unable to pay for their medical care.(Eligibility for VA health care is discussed furtherin ch. 6.) Although seldom required, VA facilitiescan also provide medical care to members of theArmed Forces, dependents or survivors of service-disabled veterans, and other non-veterans forhumane reasons or emergency care.
There are approximately 30 million veterans,of whom 98 percent are male. Forty percent areWorld War II veterans, now in their 50s and 60s.Only a small number of all veterans however, arecurrently served by the VA health care system.About 3 million veterans—10 percent of the vet-eran population —used VA services during 1981.Most veterans use community facilities and serv-ices for medical care, presumably because these
‘This section is adapted from U.S. Congress, Congressional BudgetOffice, Veterans Administration Health Care: Planning for 1990
(Washington, DC, February 1983).
veterans have sufficient public or private healthinsurance or prefer the proximity of non-VA fa-cilities. Veterans receiving VA care have healthinsurance less frequently than those receiving non-VA care.
Most VA services are provided to veterans withservice-connected disabilities or to low-incomeveterans without insurance. In fiscal year 1982,34 percent of the applicants for VA medical carewere service-disabled veterans; such veteransapply for care six times more frequently thanother veterans. Service-disabled veterans are morelikely to need greater medical care, particularlythe specialized care offered by the VA, and havepriority by law.
A significant part of VA health care is givento and requested by the aged. Aged veterans applyfor VA care twice as often as younger veterans,accounting for almost 20 percent of applications.In 1981, 17 percent of veterans aged 65 or olderapplied for medical care at VA facilities, comparedto only 8.5 percent of veterans under 65. In thesame year, the VA funded medical or health ben-efits for over 798,000 veterans 65 or older; one-fourth of patients discharged from VA hospitals—about 236,800—were 65 or older.
VETERANS’ SERVICE ORGANIZATIONSVeterans’ service organizations play a signifi- cluding medical devices. The major organizations
cant role in the VA’s delivery of health care, in- —The American Legion, the Veterans of Foreign
‘This section is adapted from S. C. Farrow, A. D. Kaluzny, and ———..——T. Ricketts, “Proceedings of a Conference on Health Services Re- 5(1/2):1-16, 1981. For further information on veterans’ service orga-search Issues in the Veterans Administration, ” J. Medical Systems nizations, see app. B.

Wars, and the Disabled American Veterans—areall powerful influences both locally, where theyare involved in a variety of activities, such as com-munity programs for youth, and nationally,where they serve their members in the politicalarena. Some organizations represent specificdisabilities, some particular conflicts, and othersethnic and religious affiliations. Thus their inter-est groups sometimes overlap.
Through their local chapters, these organiza-tions significantly influence VA hospitals. Thegroups provide hours of volunteer work offeringsupport and advice to patients and their families,Occasionally, they strongly pressure a hospitaldirector to support a particular policy. Local hos-pitals are sensitive to such pressure and respondto inquiries and complaints. Although veterans’service organizations are not always involved in
planning, they are consulted at times, particularlyabout reducing services or changing bed desig-nations.
Nationally, these organizations attempt to af-fect legislation, notably proposals to reduce serv-ices, although occasionally they lobby for newservices, such as drug treatment centers forVietnam-era veterans.
The opinions of veterans and veterans’ orga-nizations about the VA and medical devices areexamined throughout this study and in detail inappendix B. This chapter has provided a briefoverview of the VA’s health care system and thepopulation it serves. The next four chapters ex-amine VA programs and activities bearing mostdirectly on the development and use of medicaldevices.

Research and Developmentof Devices

Chapter
Research and Development of Devices
Though the Federal Government purchasedmedical devices as long ago as the years follow-ing the Civil War, groundwork for the current sys-tem of device-related research and developmentwas laid in the 1940s by the National Academyof Sciences and the Armed Forces in response tothe postwar needs of veterans. Much initial re-search on prosthetic devices was conducted by theDepartment of Defense (DOD) and the VeteransAdministration (VA). Since 1947 the VA has spentover $3o million on prosthetics research alone.Prosthetics research, along with growing researchin other areas, still continues in the VA system(109).
MEDICAL RESEARCH
The Medical Research Service provides oppor-tunities for clinicians and scientists to study thehealth problems of veterans. During fiscal year1981 approximately 4,100 investigators partici-pated in 5,44o medical research projects conductedat 129 VA health care facilities, including medi-cal centers and independent outpatient clinics(118). Since many VA investigators are health careproviders in VA medical centers, many of thesestudies emphasize the practical care of veteransand the general population (119).
Research Programs
The Merit Review Program is by far the largestprogram within the Medical Research Service, in-volving approximately 2,OOO funded investigators.This research is investigator initiated, as opposedto centrally directed. Although the program sup-ports basic science, it emphasizes clinical research.Approximately 85 percent of all principal in-vestigators in the VA system are physicians whocarry out their research part time, spending mostof their time with veteran patients. Research in-terests arise from daily clinical practice, andresults are applied to patient care. Each in-vestigator pursues his or her own interests, andeach competes against all the others for funding.
VA research and development are now dividedamong three programs or “services”: Medical Re-search, Health Services Research and Develop-ment, and Rehabilitation Research and Devel-opment (Rehabilitation R&D). Only the last, Re-habilitation R&D, is substantially concerned withmedical devices and so is the main focus of thischapter. The other two services are briefly de-scribed, since their programs do affect deviceevaluation and procurement specifically and tech-nology transfer generally, as later chapters report.
High Priority Research focuses on problems ofparticular importance to veterans, whether be-cause of the prevalence or incidence of a condi-tion or because it results from military service,especially from combat (142). Current researchareas are aging, spinal cord injury and tissueregeneration, schizophrenia, alcoholism, AgentOrange, and delayed stress disorders.
The Cooperative Studies Program supportsmulti-center clinical trials within the VA system.The program is administered through the VA Cen-tral Office in Washington, DC, and has one ex-perimental drug unit and four centers to coordi-nate data in different parts of the country.
As of September 1982, 19 studies were in prog-ress, 11 were in active planning, and 12 were infinal analysis (106,142). The largest number oftrials have tested drug therapies, followed by trialsof types of surgery, such as coronary artery by-pass grafts. Although most trials have concernedtreatments, many have also focused on preven-tive health care measures, such as control ofhypertension. The mix of VA clinical trials ismuch like that of the National Institutes of Health(NIH), except that fewer VA trials focus on can-cer treatment.
23

24
Clinical trials follow a well-defined path frominception to publication. Ideas for studies comefrom VA physicians and investigators around thecountry. They are considered by VA panels andoutside advisers, and if judged worthwhile andappropriate for VA research, are planned and car-ried out. Each study is assigned to a coordinat-ing center for help in designing, conducting, andanalyzing the trial (106).
The Cooperative Studies Program enables re-searchers to obtain large enough samples withgeographic diversity to permit valid generaliza-tions—for example, about the relative values ofdifferent treatments or the etiology and naturalhistory of a medical disorder. One Army-VA Co-operative Study revolutionized the treatment oftuberculosis, virtually emptying tuberculosiswards in the early 1950s (142).
Other Medical Research
The VA not only funds research, it is also in-volved in clinical trials funded by others, such as
NIH and pharmaceutical companies (106). TheMedical Research Service maintains a com-puterized data system that encompasses all VAresearch, including that funded by outsidesources.
The VA also supports the retrospective collec-tion and analysis of data on medical proceduresand devices, which, although not intended for re-search can still be used in research. For example,a 1980 VA Inspector General Audit of cardiacpacemaker procurement concluded that the VA’srequisition and monitoring of pacemakers shouldbe more closely controlled (120). Senate hearingslater that year raised concerns about the VA’sability to track pacemaker patients and to iden-tify and protect those affected by recalls. Theseevents prompted the VA to develop a pacemakerregistry and prosthesis profiles for all VA pace-maker patients. The registry is now reviewed peri-odically for both procurement and clinical care,and information is exchanged with other inter-ested Government agencies, such as the Food andDrug Administration, DOD, and NIH (113).
HEALTH SERVICES RESEARCH AND DEVELOPMENT
The Health Services Research and DevelopmentService (HSR&D) develops and supports projectsto evaluate alternative policies and technologiesfor clinical and administrative decisionmaking inVA health care. HSR&D emphasizes managementtools, as in developing an information system forVA clinicians, administrators, researchers, andconsumers (31,119).
Recent broad research priorities focus on careof the aged veteran, VA health care operations,the cost effectiveness of patient care technologies,rehabilitation services, and preventive health care.HSR&D supported 36 investigator-initiated re-search projects at 25 VA medical centers duringfiscal year 1982, In a VA pilot program of preven-tive health care established in response to Public
Law 96-22, subjects of research are schizophrenia,hypertension, psychiatric screening, and dentistry,along with the evaluation of some preventivehealth care services (32,119).
Four regional field programs have recently beenestablished to integrate research with the infor-mation requirements of managers and clinicians.These field programs conduct research, providetechnical assistance to investigators and consulta-tion to administrators and clinicians, educate VAstaff about the uses of health services research,and serve as a systemwide resource in such areasas care of the aged veteran, ambulatory care, andoperational efficiency. In addition, HSR&D ad-dresses information needs of VA Central Officemanagers.

25
REHABILITATION RESEARCH AND
Rehabilitation R&D (formerly RehabilitationEngineering R&D) is the most directly importantVA Service in relation to medical devices. Reha-bilitation R&D was the VA’s response to the needsof disabled people, particularly veterans. TheService evolved from the R&D Division of theProsthetic Service, dating back to 1946, and wasat first mainly an artificial limbs program. In 1973,as a result of increased national focus on rehabil-itation research and engineering needs, Rehabilita-tion R&D was separated from other VA R&D andgiven a mandate to improve the quality of life andfacilitate the independence of physically disabledveterans (109, 127). This mission is to be accom-plished through research, development, and eval-uation of new devices, techniques, and conceptsin rehabilitation. The Rehabilitation Act of 1973(Public Law 93-112), additionally requires Reha-bilitation R&D to cooperate and coordinate activ-ities with the National Institute of HandicappedResearch, Legislation further requires research anddevelopment for automotive adaptive equipment(153).
Rehabilitation R&D primarily develops sophis-ticated, “usable” devices to help individuals. Othergoals include improved rehabilitation methods(e.g., functional electrical stimulation and metho-ds to avoid decubitis uIcers, or bedsores) andtechnology transfer, including increasing theavailability of new devices on the open market.Rehabilitation R&D does not directly furnish orfabricate devices for veterans; rather, prototypedevices are developed and adapted from commer-cially available items purchased from local pri-vate sources (153). Successful models may thenbe produced commercially.
Rehabilitation R&D organizes both intramuraland extramural research and development pro-grams, has established Rehabilitation R&DCenters and research affiliations with engineer-ing schools, and generally attempts to ensure thedissemination and clinical use of new devices,techniques, and concepts (144).
The topics of Rehabilitation R&D range fromtraditional artificial limbs to robotic devices forthe totally paralyzed person (153). Activities are
DEVELOPMENT
concentrated in three areas, representing the mostprevalent service-connected disabilities:
●
●
●
Prosthetics and amputation. RehabilitationR&D emphasizes lower limb prosthetics, in-cluding improved fitting techniques, espe-cially for the elderly. Rehabilitation R&D isnow most heavily committed to this area,which represents about 40 percent of its totalbudget.Spinal cord injury. Rehabilitation R&Ddevotes about 30 percent of its budget to im-proving wheelchairs by improving motor andcontroller efficiency, reducing noise, and de-veloping a fail-safe braking system.Sensory aids. Special emphasis is given toaids for visually impaired people. Studies in-clude those of new sensory aids, people’smobility and orientation needs, and newcommunication and vocational aids. Thisarea represents about 30 percent of theRehabilitation R&D budget (119,152).
Table 1 presents a summary list of Rehabilita-tion R&D projects in fiscal year 1983. Researchpriorities are identified in special meetings, whichinclude representatives from rehabilitation re-search, clinicians, manufacturers, and disabledveterans’ consumer groups. Workshops and sem-inars in fiscal year 1982 focused on hearing im-pairment, prosthetics, and commercializing VAtechnology (152). (For the views of veterans’groups on VA research, see app. B.) Rehabilita-tion R&D has not traditionally supported devicedevelopment for cardiovascular, pulmonary, andrenal disabilities because they have seldom beenservice connected (153). However, such devicesmay receive attention in the Medical ResearchService and be used in VA clinical practice.
Rehabilitation R&D Centers
Three VA Centers perform and support reha-bilitation research and development. The VAProsthetics Center (VAPC) in New York City’ is
‘Within the VA, VAPC has also unofficially been known as theProsthetics Evaluation, Testing, and Information Center, and theRehabilitation Engineering Center.
25-289 0 - 85 - 3

Table 1 .—Summary of Rehabilitation Research andDevelopment Projects, Fiscal Year 1983
Topic
Prosthetics/amputation:Diagnostic procedures. . . . . . . . . . .Surgical procedures . . . . . . . . . . . . .Internal joint/prostheses . . . . . . . . .Gait analysis . . . . . . . . . . . . . . . . . . .Maxillofacial prostheses . . . . . . . . .Prosthetics and orthotics . . . . . . . .
Total . . . . . . . . . . . . . . . . . . . . . . . .
Spinal cord injury:Mobility (including wheelchairs
and automotive adaptiveequipment) . . . . . . . . . . . . . . . . . . .
Manipulative devices (includingcomputer-assisted devicesand environmental controls) . . . .
Surgical procedures . . . . . . . . . . . . .Neuromuscular control (including
functional electrical stimulation,nerve conduction studies, andneural models). . . . . . . . . . . . . . . .
Total . . . . . . . . . . . . . . . . . . . . . . . .
Sensory aids:Blindness and visual impairment . .Deafness and hearing treatment . .Speech impairment. . . . . . . . . . . . . .
Number of projects
49
17518
44
6
25
1023
895
Total . . . . . . . . . . . . . . . . . . . . . . . . 22
Technology dissemination and use:Rehab R&D centers . . . . . . . . . . . . . 2Rehab R&D affiliation . . . . . . . . . . . 2Information dissemination . . . . . . . 6
Total . . . . . . . . . . . . . . . . . . . . . . . . 10SOURCE: Office of Technology Assessment, 1984,
organizationally separate from RehabilitationR&D.2 VAPC was established in 1956 to conductresearch and development in rehabilitation engi-neering, to evaluate commercially available de-vices, to provide customized devices for difficultcases, 3 and to manufacture and distribute ortho-pedic footwear and prosthetic and orthotic de-vices. In the 1950s, VAPC was the basis of a suc-
‘Since this technical memorandum was drafted, the VA has pro-posed a reorganization that would put VAPC, Rehabilitation R&D,and Prosthetics and Sensory Aids Service under one director.
3VAPC represents a merger of the New York Regional Office andthe Prosthetic Testing and Development Laboratory, then part ofthe Research and Development Division of the Prosthetic and Sen-sory Aids Service, to bring research and clinical programs togetherfor the benefit of each. In 1969, VAPC established a program ofsatellite stations to help its engineers and professional personnel workmore closely with patients at the site of hospitalization. Such sta-tions have been established at VA hospitals in Brooklyn, NY, EastOrange, NJ, the Bronx, NY, and Castle Point, NY.
cessful VA intramural research program,developing most of the prosthetic limbs and thefitting techniques used today (127).
A recent audit report (1982) by the VA’s Of-fice of Inspector General, however, disclosed sub-stantial management problems at VAPC over thelast several years and recommended changes inits goals and organization, including the discon-tinuation of its research and development pro-gram (139). The VA hopes to transfer VAPC’SDevelopment Section to the Technology and Per-formance Evaluation Service. Personnel in the Re-search Section were offered reassignment to theEngineering Service at a nearby VA hospital (22).(Other VAPC activities and program changes arediscussed later in this report. )
The other two Rehabilitation R&D Centerswere established only in the last few years andare directly tied to the VA Rehabilitation R&Dprogram. One is in the Palo Alto VA medical cen-ter in California, the other in the Hines, Illinois,VA medical center outside Chicago. Six moreCenters are planned by 1986.
These Centers provide engineering support inVA medical centers where there are existing rela-tionships between VA medical and engineeringcommunities, and they are affiliated with leadingengineering schools, just as VA medical centersare affiliated with medical schools. These affilia-tions bring faculty and students into clinical re-search settings to study the problems of disabledpeople and new procedures and devices in engi-neering. The Centers’ primary goal is to apply ad-vanced technology (e.g., microprocessors) to helpphysically handicapped veterans. The VA viewsthe Centers as natural outcomes of engineeringschool affiliations that successfully produced newrehabilitative devices, techniques, and conceptsin VA clinical settings.
Each Rehabilitation R&D Center is adminis-tered by a director and an assistant director, onea physician and the other a rehabilitative engi-neer, Each Center is staffed with investigators andtechnicians, but receives administrative supportfrom its associated health care facility (144).
The Rehabilitation R&D program is also estab-lishing university-affiliated engineering research

27
programs to help support graduate students andfaculty who undertake rehabilitation engineeringprojects. The program is designed not only to in-terest engineering students in rehabilitation, giventhe critical shortage of trained rehabilitation engi-neering professionals in this country, but also toinfuse new ideas into the Rehabilitation R&D pro-gram through its frequent communication withacademia (19,30,109).
Technology Transfer
Part of the VA’s rehabilitation research pro-gram mandate (38 U.S. C. sec. 4101(c)(2)) is to testprosthetic, orthotic, and orthopedic appliancesand sensory aids, and to disseminate VA resultsand information for the benefit of all disabled per-sons (154).
The VA has traditionally attempted to ensurethe clinical use of new devices, techniques, andconcepts in three major ways:
Ž Through VA investigators who have ap-pointments in affiliated medical or engineer-ing schools and who can communicate the
DISCUSSION
The goals and priorities of VA R&D are diverse,given its extremely broad mandates to address vet-erans’ complex and difficult problems. VA R&Dis especially important for rehabilitative devices,because the markets for many are small and frag-mented. In the past, unless the stages of research,development, and transfer have each been pub-licly funded, market incentives have often been
results of VA research to students and col-leagues.Through peer-reviewed research in the VAintramural program. Because competition forsupport is keen and the review considers thenumber and quality of publications and pres-entations at scientific meetings, there is pres-sure to disseminate information promptly tothe research community, whether in the VAor outside.Through funded Rehabilitation R&D inves-tigator;, two-thirds of whom are involved inpatient care and have direct professional in-terests in physically disabled veterans. Ap-plication of recent results can thus be direct(144).
Rehabilitation R&D also supports the Office ofTechnology Transfer, whose main responsibilityhas been preparing the Journal of RehabilitationR&D (formerly the Bulletin of Prosthetics Re-search). The Office also maintains the ProstheticReference Collection and the Prosthetics Film andAudio-Visual Lending Service for interested re-searchers and clinicians (144).
insufficient to ensure the availability of rehabili-tative devices from private firms (109).
Table 2 summarizes the VA R&D budget. Al-though the commitment to R&D in current dollarshas increased over the past few years (and sub-stantially increased for Rehabilitation R&D infiscal year 1983), the budget is stable or declin-
able 2.—Veterans Administration R&D Budget Overview (thousands of dollars)
Fiscal year
1977 1978 1979 1980 1981 1982 1983Medical research program . . . . . . . . . . . . . . . . . . $101,567 $108,153 $118,016 $122,745 $129,943 $130,842 $141,052
Staffing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4,220 4,367 4,217 4,171 4,171 3,845 4,015Rehabilitation R&D program . . . . . . . . . . . . . . . . 4,419 5,502 7,191 8,085 8,784 7,185 10,001
Staffing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69 90 112 143 (143) 128 250Health services R&D program. . . . . . . . . . . . . . . 3,604 2,996 3,004 3,153 3,083 2,828 3,786
Staffing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45 90 105 104 104 93 120SOURCES” U S. Veterans Administration, Off Ice of Budget and Finance, Cortgressiona/ &dgef Submission (Washington, DC, 1983); R. Nolan, US Veterans Administra-
tion, Office of Budget and Finance, Washington, DC, personal communication, September 1983.

28
ing when inflation is taken into account. Further-more, as a proportion of medical care expendi-tures, funds for R&D have steadily declined forover a decade: In fiscal year 1970, R&D accountedfor 3.4 percent of the total medical care costs, in1982, only 2 percent (144).
Veterans’ service organizations have expressedgreat concern about the effects of relative cutbacksin R&D budgets, especially those for prostheticsand sensory aids.
VAPC has encouraged innovation in the pastby demonstrating that new types of wheelchairswere technologically possible, safe, and most im-portantly, that they had a significant market—the VA (80). The Center’s work with powerwheelchairs in the early 1970s showed they couldbe safely used at speeds greater than a slow walkand on rough terrain, which encouraged manu-facturers to begin making such chairs. VAPCwork on lightweight sports wheelchairs had simi-lar effects. VAPC now focuses on commerciallyavailable devices rather than prototypes, whichmay change the VA’s role in device innovationand development.
Especially given dwindling R&D moneys, theVA peer review and advisory council systems be-come even more important. The Medical ResearchService has a well-developed merit review system,and both HSR&D and Rehabilitation R&D haverestructured and improved their systems withinthe last few years. The Rehabilitation R&D proc-ess, modeled on that of the Medical ResearchService, relies on in-house professionals, Reha-bilitation R&D directors, and a multidisciplinarypanel of non-VA experts to set research prioritiesand review proposals and results (109). Recently,Rehabilitation R&D has also taken steps to in-crease consumer involvement in planning R&D,placing representatives from veterans’ serviceorganizations on its merit review board.
Rehabilitation R&D, the primary focus of VAR&D on medical devices, deserves attention in atleast two other areas. The first concerns Rehabil-itation R&D Centers. Funding has shifted over thelast few years to these Centers and their univer-sity-affiliated programs and away from extramur-al support. A 1981 VA evaluation of the two ex-isting Centers concluded that they were devel-
oping toward a “stable and productive” existence,but noted some achievements were lagging (144).Delays were experienced in selecting Center di-rectors, in completing basic construction and ren-ovation, and in procuring essential computers andoffice supplies. Procurement problems have per-sisted, at least at the Palo Alto Center, which buysrough!y $400,000 in devices annually (not includ-ing office supplies), because the Center must buythrough the Palo Alto VA medical center procure-ment and supply service.
VA medical centers have relatively constantneeds for medical equipment and supplies, but re-search centers, because of the nature of research,can exhibit highly erratic purchasing patterns. Re-search can also require highly sophisticated tech-nology not normally purchased for medical care.Thus, the centralized contracting procedures usedfor medical center procurement may be inade-quate for Rehabilitation R&D. Special contrac-tual procedures can delay projects for a long time.The Palo Alto Center has reported equipment pro-curement lags of up to 18 months (53), longer thanthe duration of some Center projects.
The situation at the Palo Alto Center has beenexacerbated by special VA procurement policiesfor microprocessor equipment. Much of the Cen-ter’s work involves innovative uses of electronicand microprocessor technology. However, untilrecently all VA purchases of such equipment havebeen controlled by the VA’s Central Office ofAutomated Data Processing. Even relatively un-sophisticated circuit board devices costing $100have needed approval not only of the local supplyprocess but also of the Central Office.
Because of medical centers’ increasing needs forautomation, in May 1983 authority was delegatedto the centers to procure all automated data-processing equipment, software, and services witha purchase value of $10,000 or less or a lease costof $300 or less per month (53,122). RehabilitationR&D has additionally designated smoother, moreexpeditious contracting procedures as one of its“special initiatives” beginning in fiscal year 1983(152).
The second issue of interest regarding Rehabil-itation R&D is that of technology transfer. Forseveral years the VA had recognized deficiencies

29
in the use of results from VA-sponsored R&D onrehabilitative devices. Generally, it seems thatconsiderable information on new devices, tech-niques, and concepts had been disseminated, butthere were no structured efforts to transfer tech-nology (109). No system routinely promoted thegreater use of successful prototype devices, whichwere known mainly through their experimentaluse in VA clinical settings (144).
Rehabilitation R&D has established an inter-agency agreement with the Department of Com-merce to identify and develop potential markets
and financing for prototype devices funded anddeveloped through Rehabilitation R&D. The pro-gram’s goal is to develop a better process towardcommercializing VA technologies. In addition, theVA intends to improve its in-house testing andevaluation of prototype devices.
Although still in planning, RehabilitationR&D’s new initiatives in technology transfer area significant step for the VA with regard to med-ical devices. Later chapters further examine theprograms mentioned here, as well as the VA’s rolein technology transfer.

Chapter 4
Testing and Evaluating Devices

Chapter 4
Testing and Evaluating Devices
Testing and evaluation encompass many activ-ities, including requesting, funding, and conduct-ing studies. Techniques for testing medical devicesare equally various, from the informal methodsof individual inventors, developers, and physi-cians to complex clinical trials. No technique isapplicable to every medical device, and in manyinstances simpler methods may be more appro-priate. Often, researchers use a combination oftechniques (7).
Depending on the nature of a device, publicagencies, nonprofit organizations, and privatefirms also use different criteria to evaluate it. Themost common, and perhaps most important, cri-teria used in the early development of health-related products are safety, technical feasibility,and technical performance. Depending on the useor intended market for a device, further test cri-teria may be effectiveness, suitability for desig-
PROTOTYPE DEVICES
Rehabilitation R&D evaluates prototype de-vices and disseminates information, and in bothcases works with the National Institute of Hand-icapped Research. ] As noted earlier, the VA ismandated to test prosthetic, orthotic, and ortho-pedic appliances and sensory aids, and to dissem-inate information on its research for the benefitof all disabled persons (38 U.S. C. sec. 4101).
Still, rehabilitative devices often do not com-plete the transition from research prototypes tocommercially viable products, even though Re-habilitation R&D supports dozens of ongoing de-vice development projects. This discontinuity maybe caused by several separate, but related,obstacles (which are discussed further in ch. 5).One of these obstacles is the lack of unbiased clin-ical evaluations of prototypes’ performances and
‘For discussion of the National Institute of Handicapped Research,see OTA’S report Technology and Handicapped People (109).
nated goals, reliability, cost, cost effectiveness,repairability, convenience, esthetics, consumersatisfaction, patient protection, legal impacts,liability concerns, accessibility, reimbursementstatus, social implications, and ethical concerns(110).
Several Veterans Administration (VA) pro-grams that evaluate innovations have evolvedover the years given the many kinds of decision-making related to medical devices. The Rehabilita-tion R&D Service (Rehabilitation R&D) evaluatesrehabilitative devices still in development. The Of-fice of Procurement and Supply and the Prostheticand Sensory Aids Service, along with other VAmedical, surgical, and rehabilitative service of-fices, evaluate devices that are already commer-cially available but must be approved before theVA can purchase and distribute them.
clinical applications (154). The VA explains thisproblem in a 1981 internal report (144):
The problem is that, after the prototype hasbeen developed, it is necessary to place a num-ber of examples of the developed item into ac-tual use, under conditions in which carefully con-trolled evaluations , . . can be carried out. Only
after these evaluations, and any modificationswhich result from them, is it appropriate to man-ufacture such items for routine placement withveteran patients. In the case of other new healthcare developments (such as the development ofnew drugs) this evaluation phase is funded bythe manufacturer’s capital funds. In the devel-opment of new devices for the disabled, thedeveloper (and/or proposed manufacturer) is fre-quently a very small business which cannot af-ford the capital outlay required to place anumber of prototypes into an evaluation pro-gram . . . The Veterans Administration does notroutinely purchase for its beneficiaries items
33

34
which have not been through testing and evalua-tion.
. . . . the Research and Development budget isnot adequate to provide the capital for purchaseof expensive prototypes to be placed in actualuse by veteran patients under an evaluation pro-tocol. Similarly, it has not been customary to usepatient care funds for this purpose. The only ex-ception has been the purchase, by [the VA Pros-thetics Center] . . . of devices which are put intoevaluation protocols. There is currently no fea-sible alternative in the VA system available forthose instances where, for whatever reason, thepurchase and evaluation of the device by [the VAProsthetics Center2] . . . is inappropriate. Thissituation has led to a number of instances wheredevices have been developed with VA researchand development funds which subsequently nei-ther have been demonstrated to be ineffectualnor have been put into general use by the vet-eran patient.
Expensive prototypes supported by VA R&Dfunding, but never evaluated, include the follow-ing (144):
a wheelchair adapted for use with the ScottVan (a specially equipped van that can bedriven by a person confined to a wheelchairor gurney), with a new system of electroniccontrols;a high-performance wheelchair developed atthe University of California-Berkeley oncontract;a wheelchair control system developed at theJohns Hopkins University Physics Labora-tory on contract;a four-bar linkage knee for above-knee pros-theses developed at the University ofCalifornia-Berkeley on contract; anda standing device for paraplegics developedby Ocean Systems Laboratory in San Diegoon contract.
Recently, Rehabilitation R&D has named itsown evaluation unit to establish and operate a na-tional program with the following goals (154):
. . . . conduct clinical trials (or evaluations) onnew devices, techniques and concepts in reha-bilitation; promote commercialization of re-
2Recall that the VA Prosthetics Center, as noted in ch. 3, primar-ily evaluates commercially available devices rather than prototypes.
search devices evaluated by the program; and di-rect a technical information acquisition anddissemination program, which includes develop-ing educational guidelines and technical manuals[for training programs].
The Rehabilitation R&D Service envisions theunit as a “facilitating and coordinating” center toimprove the “organization and visibility” of theService’s evaluations. Various VA facilities, in-cluding Rehabilitation R&D Centers, the VA Pros-thetics Center (VAPC), and individual medicalcenters, have been involved in testing and evalu-ating new and emerging rehabilitative devicesthrough Service funding (154).
There have been concerns in the past, however,about duplication in testing and evaluating spe-cific rehabilitative devices as they proceed fromdevelopment to marketing and diffusion. For ex-ample, recreational ski equipment for the disabledperson (later commercially produced as Arroyasit-ski equipment) was developed and tested at thePalo Alto Rehabilitation R&D Center and testedat four independent testing and evaluation centers.Still, it could not be purchased for veterans untilVAPC had tested it again (5,6,53).
The Rehabilitation R&D evaluation unit is alsointended to improve prototype testing and evalua-tion themselves through several means:
developing uniform evaluation protocols andreporting procedures,developing criteria for patient or clientselection,designating an appropriate number and thelocations of facilities involved in particularevaluations,preparing and disseminating evaluationresults, andintegrating requirements of the Food andDrug Administration (FDA) and other reg-ulatory agencies.
The unit generally oversees the evaluations per-formed. In simple cases, staff will negotiate ar-rangements. When an evaluation calls for a sub-stantial national or international effort, aworkshop may be held to bring together devel-opers and evaluation professionals to work outarrangements. It is hoped that funding for majorevaluations can be negotiated among all partici-

35
pants who have a stake in a device’s development information on the likelihood of commercial suc-and ultimate commercial success (154). - cess and indications for use, or information on
It is premature to assess the Rehabilitation R&Dchanges that might lead to success. The informa-tion can also lead to more informed decisions
evaluation unit. However, the program is impor-tant insofar as prototype testing and evaluation—
about new research and development for rehabili-tative devices (154).
in the clinic or in the community—can provide
COMMERCIALLY AVAILABLE DEVICES
Any vendor who wishes to sell new medical de-vices, including equipment, supplies and expend-able, and rehabilitative products, may have tosubmit the device for a product demonstration,“bench testing, ” or some other type of testing, toevaluate safety and various other criteria of theVA. New rehabilitative devices have traditionallybeen tested and evaluated by VAPC in New YorkCity, and new equipment and supplies by theTesting and Evaluation Staff (T&E) at the VAMarketing Center in Hines, Illinois.
The VA Prosthetics Center3
VAPC is a unique organization within the VAby virtue of combining programs in clinicalpractice—in prosthetics, orthotics, and technicalaids—and programs in development and evalua-tion for their mutual benefit. New devices canthen be used promptly in the clinic, as part of anevaluation or to study their wider applicability.
VAPC has long stressed in-house evaluation ofcommercial devices. It has been the V A ’ sorganizational focus for nearly all bioengineer-ing and clinical evaluations of commercially avail-able rehabilitative devices and for some hospitalequipment for nearly three decades.4 During itsearly years, evaluations concentrated on limbprostheses in response to the overwhelming needsof World War II veterans. In more recent years,
‘Except where noted, information in this section is based on U.S.\’eterans Administration, Department of Medicine and Surgery, Vet-erans Administration Prosthetic and Sensory Aids Program SinceI+’or/d War 11 (Washington, DC: U.S. Government Printing Office,1978).
‘VAPC’S work has been complemented over the years by someevaluations of contractors, developers, manufacturers, and inven-tors of prototype devices, largely in weighing priorities for its ownR&D.
evaluation has emphasized orthotics and thespinal-cord-injured patient. Evaluations in the1970s emphasized bioengineering directed espe-cially at the stroke patient, the patient with de-veloping vascular insufficiency, and the aged per-son with problems of independence in daily living.
Standards Development
Throughout the 1970s, the VA increasinglyemployed standards in its prosthetic and sensoryaids program. Developing standards requires notonly evaluating devices in drafting the standards,but also compliance testing after the standards areestablished. In theory, compliance testing furthertests the current standard and determines whetherproducts meet the purchaser’s needs. The stand-ards developed reflected desired qualities of pros-thetic and orthotic hardware, orthopedic aids,fitted limbs and braces, and sensory aids. “Speci-fications” of product attributes were included tocontrol devices’ quality, safety, and performance.Such standards were perceived as benefiting bothVA beneficiaries and other disabled people. Oncedeveloped, standards were implemented throughthe VA Office of Procurement and Supply andits contracts with manufacturers and fitters.
VA standards development has required theparticipation of individuals and organizationsboth within and outside the VA. A draft stand-ard of appropriate language can be developedfrom clinical experience with devices and tech-niques and the knowledge and experience of R&Dand evaluation staff. The draft must then beevaluated by those who will work with it: man-ufacturers, prosthetists, orthotists, educationalspecialists, VA supply specialists, and others.Such reviews have also included professional asso-

36
ciations such as the American Society for Testingand Materials, the International Standards Orga-nization, and the Rehabilitation Society of NorthAmerica.
Once a rehabilitative device standard has beenemployed, the VA—through VAPC—performscompliance testing of hardware, sampling themarket and conducting laboratory tests. The VAmakes known the results of such tests to its pro-curement personnel and to manufacturers.5 Whenresults of compliance testing have been negative,the VA has also developed engineering design rec-ommendations.
VAPC has developed standards for lift aids,motor vehicle systems for handicapped people,wheelchairs, knee mechanisms, foot-ankle assem-blies, stump socks, elastic hosiery, crutches, canes,and other related devices. When VAPC has notdeveloped a standard for a device, the VA Of-fice of Procurement and Supply has relied, whenpossible, on other appropriate standards. The re-search and testing of the National Bureau ofStandards (NBS) have been valuable to the VAin evaluation (18,109). NBS has developed devicesto measure slip resistance on walkways, con-ducted performance and reliability tests on hear-ing aids and cardiac pacemakers, developed stand-ards for acrylic bone cements and metals, and ingeneral has helped address technical issues relatedto the needs of disabled individuals.
Veterans’ organizations and others have ex-pressed concern that the VA has used specifica-tions and standards for existing technologies toevaluate and purchase new ones. Thus, emerg-ing devices of unusual design or performance mayhave trouble entering the market, especially thelarge VA market (109). (Small firms may havepronounced difficulties since they have fewer re-sources to address regulations on marketing. )Older standards have been particularly vulnerableto such criticism, because they tend to specifyproduct dimensions and materials.
Newer standards have emphasized, instead,functional or performance requirements, Precise
‘Manufacturers are prohibited by previous policy agreements fromdirectly or indirectly using the results of VA evaluations for adver-tising (18).
materials, fabrication methods, and designfeatures have generally not been specified, Thegoal has been to allow innovation while provid-ing adequate controls for patient safety. At pres-ent, the VA has only four or five general stand-ards for rehabilitative devices; for example, thestandard for wheelchair lift systems covers 21 dif-ferent models and 13 different manufacturers. Yetdespite the VA’s efforts, existing standards maystill bar new technologies.
Shepard and Karen came to this conclusion inthe case of wheelchairs (80). Historically, the VA’sstandards were written with a specific wheelchair,usually an Everest & Jennings model, in mind. TheVA’s evaluations of wheelchairs may have pro-moted safety, but they also functioned in the in-terests of the major manufacturers, As the largestpurchaser of wheelchairs in this country, the VAmight not only overlook new technologies, butpossibly discourage innovation and product im-provement.
In the last few years the VA has replaced moststandards and device specifications with moregeneral Commercial Item Descriptions (CIDS).CIDS are designed to accommodate better the va-riety of privately developed and marketed devices(see ch. 5 for a critical discussion of CIDS) (12).
General Testing and Evaluation
VAPC device testing typically follows severalpreliminary steps (163):
●
●
●
gathering background information, oftenfrom the manufacturer;developing an evaluation protocol that en-compasses any appropriate VA standardsand specifications as well as criteria tovalidate manufacturers’ claims; andhaving the protocol approved by the R&Dcommittees of any local VA medical centersinvolved in the trial.
Standardized protocols are also employed for cer-tain general classes of devices.
Testing protocols range from simple validationassessments to complex clinical evaluations in-volving dozens of VA medical centers or clinics.At the least, rehabilitative devices are tested forsafety, reliability, and the validity of manufac-

37
turers’ claims. New wheelchair products, for ex-ample, are tested for strength, safety, maneuver-ability, and ease of use, although not necessarilyfor durability (18).
Devices can undergo either special laboratorytesting or field testing at VA- medical centers orclinics, or both, Field testing is advantageous inassessing a device’s “usefulness, ” that is, the con-ditions in which a device is most appropriatelyprescribed and used. Field testing also decreasesthe probability of observer bias by relying on alarger and more random group of testers. YetVAPC has not always used field testing becauseof organizational difficulties.
Until fiscal year 1984, neither VAPC staff northe VA Prosthetic and Sensory Aids Service, theprimary users of rehabilitative device evaluations,had authority over researchers, in contrast to thecase of VA testing and evaluation of medicalequipment and supplies (see the later section ofthis chapter on VA Marketing Center testing andevaluation). This absence of authority typicallyresulted in lack of control over experimental pro-tocols and data reporting, and often created aninitial resistance to cooperating in device studies.Group evaluations, which compare similar de-vices, have been attempted but never fully devel-oped (163), since they frequently involve exten-sive field testing.
VA evaluation of commercially available reha-bilitative devices has been the target of com-plaints, especially from veterans’ groups. TheDisabled American Veterans organization hascharacterized the evaluation system as “fraughtwith inefficiencies and communication break-downs” (160). In addition to the Disabled Amer-ican Veterans’ complaints, there have been othercriticisms: that testing priorities are not adequatelyestablished and that there are long delays in eval-uating devices; that clinical prescription criteriamust be more standardized to ensure more con-sistent quality of care; that device needs of vet-erans must be better anticipated; and that devicesshould be evaluated by the FDA (not the VA) forsafety (though by the VA for efficacy and costeffectiveness) (164).
Prosthetics Technology Evaluation Committee
To address concerns about VA evaluations ofcommercially available devices, the Prostheticsand Sensory Aids Service established the Prosthet-ics Technology Evaluation Committee (PTEC)early in 1982. The committee—including repre-sentatives from the Prosthetic and Sensory AidsService, the Office of Procurement and Supply,and Rehabilitation Medicine Services, the VA In-spector General’s Office r and RehabilitationR&D—has developed an evaluation and coordi-nation process for VA products and devices,which is now almost fully operational.
PTEC will be responsible “for assessing andranking the legitimacy and appropriateness ofevaluation proposals and for assessing and ap-proving the results of clinical evaluations” (125).The Prosthetic and Sensory Aids Service estab-lished PTEC primarily because of concern that theVA evaluation process was not sufficiently for-malized. Not only were evaluation effortshampered, but, faced with increasingly expensivedevices and technologies and steady or decliningbudgets, the VA was using its lack of a processto deter supplying expensive prosthetic and sen-sory aids to veterans. b
The PTEC evaluation process probably has twomain strengths: 1) classifying devices into threetypes to determine the testing and evaluation thatdevices will undergo; and 2) coordinating withother parties interested in rehabilitative devices,in the VA delivery system, other Federal agen-cies, independent testing labs, and veterans’groups. (The Paralyzed Veterans of America andthe Disabled American Veterans, for example,both have permanent representatives on this com-mittee. Other veterans’ groups are informed of itsactivities and invited to participate in meetings. )
“L’A policy is to provide blind veterans with all necessary serv-ices and devices to overcome their handicaps and to provide otherd]sabled veterans with devices and technologies deemed nqedicall}’necessary. As in the case of disability compensation and pensions,a ma] or concern to users and policy makers is the cost of co~’eringall available technologies (62, 109 ). This issue is discussed furtherIn ch 6.

38
The PTEC process groups devices into threetypes, according to potential risk, innovation, and(importantly) cost. It is like the FDA classifica-tion in determining the kind and extent of evalua-tion by a device’s type. This classification systemis not yet final. It will depend significantly on asurvey of the users (which will also lead toprescription guidelines).
Generally, however, devices in the lowest cat-egory of risk, newness, and cost will seldom besubjected to laboratory testing other than themanufacturers. Additional laboratory testing willconcern only safety. Devices in the middle classwill be laboratory tested, as needed, for com-pliance with existing standards, safety, and valida-tion of manufacturers’ claims. Provided the testresults are positive, products will then undergolimited clinical trials to substantiate laboratoryfindings and to obtain users’ opinions. Only de-vices at the highest level of classification will besubjected to extensive VA lab testing and clinicaltrials (22,50).
PTEC can provide information for variouskinds of decisionmaking, from that of users to thatof policy makers. To the extent possible, PTECwill rely on data from the FDA, independent lab-oratories testing, and others. The amount oftesting information shared by the VA and theFDA has traditionally been negligible, however.Evaluation criteria have generally differed becauseof the VA’s special needs and client population.The VA has also been hesitant for the FDA to useVA data because private device manufacturersmight request free evaluation services from theVA (50).
Testing and Evaluation Staff,VA Marketing Center
At any one time, about 250 devices, rangingfrom hospital-based equipment to supplies and ex-pendable, are being reviewed by the VA Officeof Procurement and Supply as a requisite for pro-curement contracts. The Office’s Testing andEvaluation Staff (T&E), part of the VA Market-ing Center and supply depot in Hines, Illinois, hasprimary responsibility for this aspect of VA de-vice testing.
The T&E was established in February 1976 byadministrative fiat, based on a VA-initiated study,the “McKinsey report.” The study suggested thatthe VA might perform several functions (57):
●
●
●
be a valuable source of information on med-ical devices for other health care providers,centralize and expand existing informationand evaluation activities,support the FDA in ensuring the safety andefficacy of medical devices, andstimulate the development of new or im-proved products for identified needs.
As the McKinsey report was released, the FDAalso entered a memorandum of understandingwith the VA to exchange medical device “experi-ence. ” This agreement would eventually requirea VA clearinghouse for medical device recallsfrom the FDA and hazard reports from VA med-ical centers. Meanwhile, the McKinsey report’srecommendation to stimulate innovation was im-plemented with the help of NBS, which initiatedthe Experimental Technology Incentives Program(ETIP). The VA agreed to participate in marketresearch to promote public or private partnershipsand industry incentives to develop medical de-vices. ETIP, first placed in the VA Central Of-fice, remained dormant for a year. With the estab-lishment of T&E, however, ETIP was transferredto the VA Marketing Center with a grant of$450,000. AS a result of al] these events, T&E hashad responsibility for medical device evaluations,liaison with FDA on recall and hazard alerts, andETIP (134). The ETIP-VA agreement ended in1981, but T&E has continued its market research.
Testing and evaluating VA-purchased medicaldevices is T&E’s central focus. Such medical de-vices are selected for evaluation through requestsby VA medical centers, manufacturers, the VACentral Office, and “in-house” initiatives. Choicesdepend more on volume considerations and theinterest of VA health care facilities than, for ex-ample, cost factors (67).
Once a device is selected for testing and evalua-tion, prospective clinical trials may be carried outunder the auspices of the Medical Research Serv-ice (18) or cooperatively with the Department ofDefense through an agreement with Fort Sam

39
Houston in Texas. Most often, however, testingand evaluation consist of internal consumer re-search to validate manufacturers’ claims with testscarried out at VA medical centers and facilitiesaround the country T&E also has working agree-ments with nearly a dozen private testing labora-tories, for needed laboratory tests, including theEmergency Care Research Institute, Utah Bio-medical Laboratories, Stanford Research Institute,and Underwriters Laboratories. Information isalso shared with some of these laboratories (134).
T&E develops the base protocols, which maybe amended by appropriate medical serviceswithin the VA. Testing sites are also cooperativelyselected, with local VA supply and procurementofficers administering hospital tests (67). As theappropriate VA manual specifies (156), evalua-tions typically take the form of user surveys onmany product features, including compliance withmanufacturers’ claims and industry standards,safety, design, ease of use, durability, cost, andthe products’ advantages and disadvantages com-pared to similar products.
Testing may last from 2 weeks to a full year,but averages 30 to 60 days. Information is thencompiled in a brief description of the product(often derived from manufacturers’ literature) andof survey findings. The Office of Procurement andSupply publishes evaluation results quarterly anddistributes them to VA medical centers, medicaland regional office centers, clinics, and supplydepots and distribution centers, and to procure-ment officers at the VA Marketing Center. Resultsof the evaluations cannot be used by manufac-turers, but they are routinely requested by pri-vate hospitals, nursing homes, and State and localgovernments, and are reprinted by private pub-lications such as Consumer Reports, Hospital Pur-chasing Management, and Health Devices Alert(18,67,147).
Importantly, evaluations are advisory. Theo-retically they are incorporated in national pro-curement contract requirements, but purchases arenot based solely on the evaluations. Purchasingdecisions still rest with individual hospitals,which, on average, purchase from national con-tracts only about 60 percent of the time. Further-more, evaluations stress advantages and dis-
advantages based on a manufacturer’s standardor claim. There are no evaluations of features forwhich manufacturers make no claims. VA regu-lations also prohibit explicitly comparing oneproduct with another. There have been efforts todo group evaluations of some classes of devices.Group evaluations would better control for testingbias and could generate more meaningful infor-mation. Staffing and budgetary restraints, how-ever, have restricted T&E to very few groupevaluations (67).
T&E primarily evaluates standard stock itemsand smaller medical equipment. Decisions to pur-chase expensive devices, for example computedtomography (CT) scanners, involve not onlysupply and procurement staff; they require the ap-proval of special medical equipment committeesin individual medical centers and that of ServiceDirectors in the Central Office.7 Although thereare a few exceptions, Service Directors have tradi-tionally relied only on data generated by the man-ufacturer or on VA “acceptance testing, ” whichprospectively establishes “performance require-ments” (e. g., for reliability, dosages, or perform-ance times), with local interdisciplinary VA teamsassessing devices against the criteria. The Medi-cal Research Service has worked jointly with otherServices in some evaluations. For example, theRadiology Service made purchasing decisionsabout CT scanning with the help of an advisorycommittee including the directors of medicine,surgery, neurosurgery, and neurology. Two re-search projects—one comparing the costs of in-house scanners and those of contracting for scansand another evaluating VA hospitals’ sharing ofCT scanners—also figured in these decisions.
Recently, manufacturers have begun to offerthe VA expensive equipment outright in exchangefor exclusive long-term contracts for disposablethe hardware requires or in exchange for experi-mental data. The VA now lacks a policy on ac-cepting or using such equipment (18).
In fiscal year 1983 T&E began post-marketingsurveillance by surveying all VA purchasers and
‘Expensive medical and dental equipment, generally items above$30,000 and others specified in VA regulations (157), are called “con-trolled items. ” Controlled items are further discussed in ch. 6.

40
users of products previously evaluated. The sur-vey’s goal is to determine performance, quality,and other product characteristics after more pro-longed use. Two dozen items are to be reviewedeach year. Summaries of responses will be pub-lished quarterly along with new product evalua-tions (67,133).
T&E is also concerned with “product assur-ance, ” resolving medical device and product com-plaints and providing staff support for develop-ing specifications, standards, and inspection cri-teria for equipment and supplies bought centrallyand managed by the VA depot system (which isdescribed inch. 5). For example, T&E has devel-oped standards for hospital beds and eyeglassframes, the last jointly with ETIP.
To the extent possible, T&E and, in turn, pro-curement components of the VA have relied onexisting standards and device evaluations, suchas those of the FDA’s National Center for Devicesand Radiological Health in the area of radiationleakage (18). The VA also wants to rely on FDAstandards and testing if the provisions of the 1976Medical Device Amendments on performancestandards are implemented (13). If a device hasbeen on the market for some time, the VA willoften use any evaluations conducted by NBS andthe Department of Defense (18).
The current Administration is also movingtoward voluntary standards as an official policyin all areas. Office of Management and BudgetCircular A-119, currently in effect, describes theuse of voluntary standards for procurement. T&Ehas worked with several voluntary standardsgroups in the past, including the American Societyof Testing and Materials and the National Sanita-tion Foundation. As an alternative to using stand-ards, the VA has increasingly used CIDS, whichare adopted as standards are, but allow a broadermix of devices to be purchased. So far CIDS havehad a much greater impact than standards in thepurchase of medical devices (67), as discussed inthe following chapter.
The VA requires its medical centers to usedepot-stocked items when possible. To ensure usersatisfaction, the VA has a formal system for reg-istering complaints with the VA’s Marketing Cen-
ter, which must promptly resolve these com-plaints.
A 1982 General Accounting Office (GAO) re-port called for this system to be improved (101).Medical centers, it found, were not satisfied withdepot-stocked items and often bought alternativeproducts from other sources without filing a com-plaint. As a result, inferior stock was often notbrought to the Marketing Center’s attention.When complaints were filed, the Marketing Cen-ter often did not take appropriate action, furtherdiscouraging medical centers from reporting com-plaints.
The medical centers use the VA’s Quality Im-provement Report to file complaints about depot-stocked items. During fiscal year 1980, for exam-ple, 478 Quality Improvement Reports were filedon medical supply and equipment items. How-ever, until fiscal year 1982, the marketing and pro-curement officers (“commodity managers”) at theMarketing Center were also responsible for re-sponding to Quality Improvement Reports. GAOfelt that the commodity managers perhaps couldnot evaluate reported problems objectively. Withregard to frequently registered items, GAO foundthat the Marketing Center: 1) did not address themedical centers’ stated problems, 2) did not pro-vide the medical centers with clear resolutions,or 3) provided the medical centers with falseassurances.
In response to the GAO report, the VA trans-ferred responsibility for the quality complaint sys-tem to the Marketing Center’s T&E staff begin-ning in fiscal year 1982 to improve the system’sobjectivity and responsiveness. Transfer to T&Eof the quality complaint system had the additionalbenefits of coordinating evaluations and en-couraging better information exchange with theFDA on medical device problems and experience.All Quality Improvement Reports received byT&E are screened to determine the potential forhazard alerts or product recalls because of riskto the lives or safety of patients and employees.T&E forwards information on hazard alerts to theFDA’s National Center for Devices and Radiologi-cal Health and other divisions of the MarketingCenter, which in turn notify all VA medical fa-cilities.

41
Another function of T&E is developing andmanaging a computerized information storage andretrieval system for consumers. Another out-growth of the VA-ETIP program, this system fa-cilitates the fIow of information among the pur-chasing divisions of the Marketing Center, VAmedical centers, and other Government agencies;
DISCUSSION
This chapter has focused on the VA’s diverseevaluation activities. Generally, VA evaluationsare conducted during the later phases of R&D.Late in the R&D process is generally when infor-mation must be collected for reimbursement,financing, and drug and device regulation (i.e.,for decisions affecting use). This is a good timefor evaluations insofar as information and experi-ence may be available and the device has not yetbeen widely diffused. Evaluations can then affectthe VA’s adoption of devices (109).
The separation of Rehabilitation R&D fromother VA research in 1973 was partly to give morefocus to VA rehabilitation research (109). In turn,this focus helped stimulate the VA to devote moreattention to evaluation, as in establishing theRehabilitation R&D evaluation unit.
At the same time, one veterans’ group has crit-icized the divided responsibility for evaluation.Commercially available devices, especiallyrehabilitative ones, often need refinements beforethe VA can approve them for its use. Accordingto the Disabled American Veterans, in these casesit may not be clear who is responsible forevaluation—Rehabilitation R&D, Prosthetic andSensory Aids Service, or the VA Office of Pro-curement and Supply (160).
Coordinating evaluations has been addressedby forming PTEC. In calling for the involvementof all relevant VA services and in inviting con-sumer groups to participate, the VA appears tobe taking a step toward more systematic evalua-tion of rehabilitative devices. PTEC has the sup-port of such groups as the Paralyzed Veterans ofAmerica and The American Legion (71,82).
provides product, price, and vendor historiesuseful in awarding VA procurement contracts;and contains marketing data useful and availableto private manufacturers. Since larger companiesoften have in-house marketing capabilities the in-formation has been most useful to smaller andemerging companies.
Thousands of rehabilitative devices issue fromthe public, private, and nonprofit sectors. Manyare relatively simple and inexpensive, and othersare costly and complex. Regardless of a device’scost, complexity, or proposed use, it should meetcertain criteria before being widely used, notablythose covering safety, effectiveness, durability,and recommended applications (112). Baselineassessments combine laboratory testing and clin-ical evaluations, Some devices warrant muchbroader assessments. Costs should be explicitlyconsidered in some cases. In others, evaluatingthe devices in the user’s environments may beessential (109).
Both the Rehabilitation R&D evaluation unitand PTEC would seem to embrace these testingneeds. Both programs are new, however, andthere are problems yet to be resolved. PTEC, forexample, needs to expand its field testing activi-ties and to make its testing more national in scope.PTEC’S authority over VA medical facilitiesshould be established internally. The Rehabilita-tion R&D evaluation unit could encourage moretesting and evaluation at Rehabilitation R&DCenters and ensure that its results are valid andcredible to PTEC, to avoid duplication of efforts.Even with these problems, the evaluation unit andPTEC appear to have great potential.
In evaluating medical equipment, supplies, andexpendable, T&E represents a modest but pro-ductive effort, given its small staff. Although notrigorous, its evaluations can provide informationfor purchasing by VA facilities. T&E evaluationsare apparently most often used by smaller, morerural VA facilities. The VA estimates that only
25-289 0 - 85 - 4

42
about 20 percent of its medical centers make pur-chasing decisions based on T&E evaluations. Atthe same time, supply and procurement officersat all VA hospitals use the evaluations as an in-formation resource, including in doing businesswith vendors.
Although T&E evaluation generally does notstudy such features as cost effectiveness, it coulddo so through more group evaluations with mod-est increases in budget and staff. Its publicationsof results and standard setting can have signifi-cant influence because of the VA’s market power.For example, the VA’s requirement that fibrillatingcatheter devices for the heart meet National FireProtection Association Standards led to completeindustry compliance in manufacturing these de-vices, despite the absence of industry consensus(46). VA publication of testing results on hear-ing aids spurred innovation and competitionamong manufacturers (41). (The VA Office ofProcurement and Supply has occasionally been
reluctant to publish its test results, however, be-cause the demographic characteristics of the vet-eran population are not always those of all con-sumers (18). )
It is noteworthy that large private buyers suchas for-profit hospital chains have developedorganizational components similar to T&E. At therecommendation of a private third-party payer,the Hospital Corp. of America recently an-nounced the formation of “product standardiza-tion” committees to evaluate products’ “safety-worthiness, ” failures, and performance, and tomanage product recalls—all tasks of T&E (69).Special evaluation groups may be valuable tolarge medical systems.
T&E’s weakness may lie in not integrating eval-uation information and its market research intothe overall VA marketing, procurement, and sup-ply system. This issue is considered more fully inthe next chapter.

Chapter 5
Marketing, Procuring, andSupplying Devices
Chapter 5
Marketing, Procuring, andSupplying Devices
The Veterans Administration (VA) both pro-motes and purchases medical devices, necessitat-ing different kinds of VA programs. As part ofits commitment to research, development, andevaluation of rehabilitative devices, the VA’sRehabilitation Research and Development Serv-ice (Rehabilitation R&D) works with private orga-nizations in manufacturing and marketing prod-ucts they have developed. The VA MarketingCenter (VAMKC), in the VA Office of Procure-ment and Supply, on the other hand, determines
PROTOTYPE DEVICES
Technology transfer is generally one of themore difficult hurdles in developing and distrib-uting rehabilitative devices. Chapter 3 touched onthe VA’s long absence of structured activities inthis area. No VA system routinely ensures thatsuccessful new prototypes are transferred to clin-ical practice.
There are a number of significant obstacles toprivate industry’s participation in this process aswell
●
●
●
(65,109):
lack of adequate demographic data (or mar-ket statistics) about the technologies disabledpeople need;the commercial vulnerability of some ven-tures because of small, fragmented marketsand high investment costs; andobstacles presented by the patent system, lia-bility insurance requirements, and the third-party payment system.1
‘A further problem, discussed in ch. 4, results from the VA’s be-ing both a large market for many devices and an arbiter of perform-ance and design standards. To a large extent the VA can thus de-termine which technologies enter the market. If the VA usesspecifications and standards developed for existing technologies, itmay impede the emergence of innovative devices.
the VA’s need for commercially available devicesand purchases and supplies these devices.
The VA activities related to prototype rehabil-itative devices, which are discussed here first, bydefinition conclude at the marketing stage. VAactivities related to commercially available devices(rehabilitative devices and equipment and sup-plies), which are described later, encompass mar-keting, procurement, and supply.
Figure 5 illustrates the generally complex dynam-ics and requirements of private sector efforts tobring research ideas, information, and productsto the consumer.
One purpose of the Rehabilitation R&D Cen-ter’s evaluation unit is to address the problemareas of marketing and finance, which it plans todo in at least two ways (154):
●
●
by encouraging device development and in-novation to meet disabled veterans specificneeds, andby helping VA-supported researchers and ap-propriate industry representatives coordinatean interagency program with the Departmentof Commerce for commercializing prototypedevices that the unit evaluates.
The VA Administrator signed an interagencyagreement with the Department of Commerce inMay 1983, and the VA planned to reimburse theDepartment for up to $125,000 in fiscal year 1983for its expertise in marketing and commercializ-ing technology.
The VA is also considering a specific programwith the Department of Commerce like the Na-
45

46
Figure 5. —The Innovation ProcessThe Product life cycle
/ / / . / Research and ///// // / / / / /
Premarketphase
+
I
- - - -
/—
CE: J. E. Muthard, “Putting Rehabilitation Knowledge to Use,” Rehabilitation Monograph No. 11 (Gainesville, FL: University of Florida Rehabilitation ResearchInstitute, 19S0), as cited In (109).
tional Science Foundation’s Small Business In- Another purpose of the evaluation unit is to in-novation Research Program. Funding of up to prove the link between the VA’s R&D and indus-$20,000 would be provided to small businesses to try by several means (154):“demonstrate the_feasibility of a new concept.” -
When feasibility studies have been done, the pro- ●
gram may support a limited number of more sub-stantial proposals to carry new concepts through ●
prototype testing and evaluation. The programwould be directed at established, specific needsof disabled veterans (154).
monitoring the progress of all RehabilitationR&D projects on devices;staying informed of any links RehabilitationR&D projects have with industry, and en-couraging industrial interest where there isnone;

47
developing information on U.S. and foreignindustry that relates to disabled veterans, andaccessing data stored in VA banks and inABLEDATA; 2 andcoordinating the Rehabilitation R&D inter-agency agreement with the Department ofCommerce in market surveys, locating cap-italization funds, and stimulating the com-mercialization of R&D prototype devicesbased on its evaluation program.
The Rehabilitation R&D Center’s evaluationunit can substantially increase, centralize, and im-prove Rehabilitation R&D’s role in marketing andfinancing, though until now efforts have beenpiecemeal. The Rehabilitation R&D Center at PaloAlto, for example, has retained an in-house mar-keting specialist since December 1982. The Palo
2 ABLEDATA is a new computer information system funded bythe National Institute of Handicapped Research as a service of theNational Rehabilitation Information Center based at Catholic Uni-versity, Washington, DC. ABLEDATA combines manufacturers’data and updated information on local availability of products,names of manufacturers, locations of distributors, product descrip-tions, costs, and results of any relevant evaluations. The data bankis accessible to information brokers at locations around the coun-try, and the brokers are accessible to rehabilitation centers, indi-viduals, or anyone who needs the information. The Prosthetic Tech-nology Evaluation Committee (discussed in ch. 4) also plans to shareinformation routinely with ABLEDATA (109).
Alto Center is now working with about 30 com-panies in developing devices.
Nevertheless, the evaluation unit does not nec-essarily solve all problems of technology trans-fer. The Palo Alto group ran into difficulties be-cause of Public Law 96-517, concerning patentrights to inventions developed by nonprofit in-stitutions using Government funds. The VA willnot implement the law for several months, al-though other Federal agencies that fund R&D al-ready have. In the interim, Stanford University(whose engineers work with the VA at Palo Alto)has been unable to file a patent application to pro-tect its intellectual property rights on at least oneprototype device. 3 Instead, Stanford has requestedthat the engineer-inventors participate in VA pat-ent evaluation and application filing and has en-couraged the VA to conduct its investigation ofthe device “with due speed, so that the publica-tion ban will not post before a patent filing deci-sion is made” (53,76).
3A recently named property right distinct from patents, copyrights,trademarks, and trade secrets is “tangible research property.” Forexample, in March 1982 Stanford University developed a specialpolicy on tangible research property to protect its ownership of “tan-gible (or corporeal) items produced in the course of research proj-ects, ” including “biological materials, computer software, comput-er data bases, circuit diagrams, engineering drawings, integratedcircuit chips, prototype devices and equipment, etc. ” (83).
COMMERCIALLY AVAILABLE DEVICES
Marketing
The VA’s Marketing Research and Analysisprogram, developed from the VA-National Bu-reau of Standards Experimental Technology In-centives Program during the late 1970s. It repre-sents a major change in VA procurement inbringing marketing judgment to bear on commer-cial products’ entry into the VA supply systemand is central in developing VA procurementstrategies. Marketing Research and Analysis is pri-marily the responsibility of the Testing and Eval-uation Staff (T&E) of the VAMKC, although eachprocuring division of the VAMKC has a productdevelopment section supporting the program(128).
As a purchaser of devices, the VA attemptsboth to obtain the lowest possible prices in con-tracting and to improve medical care. MarketingResearch and Analysis is a resource for procure-ment by gathering and analyzing information onthe range and quality of available commercialproducts and determining whether they meet VAneeds. This is done through surveys, Quality Im-provement Reports (discussed inch. 4), and othertechniques ranging from informal telephone in-quiries (about products acquired by local medi-cal centers) to comprehensive reviews (of prod-ucts that may improve care VA-wide or effectsubstantial savings) (130). The aim of this prod-

48
uct and market research is to determine the need,demand, and best method of supply for items.Recommendations are then forwarded to procure-ment officers.
This VA program encompasses research inmany areas (130):
●
●
●
●
product research (on products satisfying VAand other users’ needs, product changes re-quired to meet VA needs, product descrip-tions used in commercial transactions, andnew products needed);market analysis (on the number and competi-tiveness of firms, business practices, pricingstructures, distribution practices, restrictionson shelf life and storage);analysis of the commercial market (onacceptability to likely users in light of suchfeatures as reliability and warranty); andanalysis of product support (on warranty andsupport procedures).
Such research originates from the VA CentralOffice, procurement offices at the VAMKC, andT&E.
An obvious priority during the program’s firstyears was to test the hypothesis that because ofits size Federal procurement could significantly in-fluence market innovation by providing an earlymarket for products, thus reducing market entryrisks (52). Results of this test were mixed.
For example, the program authored the Direc-tory of Living Aids for the Disabled Person, hav-ing found that no single printed source of suchinformation existed although there was a corre-sponding demand. Publishing firms were solicitedto determine their interest and the feasibility ofthe endeavor. As an incentive to industry, the VAproposal called for the directory to be publishedonce for distribution to people within the VAhealth care system but allowed the contractor orany other interested parties to use the same datacommercially, with obvious private as well as so-cial benefits. The VA objective, which was re-flected later in the publishers’ bids, was to havebidders recognize the directory’s market poten-tial and publish it at minimal cost to the VA (67).
The program’s projects have not always beenso successful. Another project determined thatsyringe needles should be more readily destroyedfor disposal. Working closely with a small pri-vate firm, the program helped develop such aproduct, but the company eventually went bank-rupt (67).
More recently, the program has focused oncommercially available products. Criticism ofproducts, poor depot sales, and seeming techno-logical breakthroughs are typical subjects of re-search. T&E also frequently relates its testing andevaluation, Quality Improvement Reports, andrecall and hazard alerts to the program’s research(67).
Procurement and Supply4
The VA’s Office of Procurement and Supplysupports the most extensive medical program inthe Federal Government and also provides non-perishable subsistence supplies, medical equip-ment and supplies, drugs, biological, reagents,and chemicals to more than 4,100 installations ofother Government agencies. These services aresupported by nearly 6,800 employees, includingstaff at the Central Office, the VAMKC, threesupply depots, the Prosthetics Distribution Cen-ter, and 172 medical centers.
In fiscal year 1982 the VA’s Office of Procure-ment and Supply spent nearly $1.3 billion on sup-plies and equipment. Two kinds of mechanismssupport this procurement and delivery: the VA’scentral procurement programs, and the local sup-ply activities of medical centers. Generally, cen-tral procurement encompasses all medical equip-ment, supplies, and rehabilitative device items,while local purchases are usually of disposablemedical and dental supplies.
Central Procurement
Several centralized VA procurement programshave been established over the years so that in-
4Except as noted, this section is based on U.S. Veterans Admin-istration, Brief of Office of Procurement and Supply, unpublished(Washington, DC, December 1982) (121).

49
dividual medical centers can obtain supplies andequipment economically, not having to solicit andaward contracts themselves. The VA finances allsupply operations through a revolving supplyfund, charging customers a percentage markupover the item’s purchase price, about 6 percent,to balance the fund (99). The VAMKC providesthese centrally managed supply channels, whichare also available to other Government agencies,such as Public Health Service hospitals, the Bu-reau of Indian Affairs, and Federal correction in-stitutions.
Centralized procurement programs are orga-nized into procurement divisions, each headed bya commodity manager, specializing in differentareas: pharmaceuticals, medical supplies, medi-cal equipment, surgical supplies, and nonperish-able subsistence supplies. These VAMKC pro-grams include a national depot distributionsystem, Federal Supply Schedules (FSS) for itemsthat the General Services Administration assignsto the VA to manage, contracts for direct deliv-ery to medical centers, and decentralized contractsfor direct ordering by medical centers.
VA Supply Depots
During the 1940s, wartime demands and poordistribution systems made it necessary for the VAand the Department of Defense (DOD) to estab-lish depot inventories of hospital stock. Thesedepots have been continuously maintained to thepresent day (34). Under this program, volumepurchases are made at low prices and items aremanaged through three VA supply depots, inSomerville, New Jersey; Hines, Illinois; and Bell,California. A Prosthetics Distribution Center inDenver, Colorado, also serves the approximately200,000 veterans with service-connected dis-abilities.
Medical center supply requests are transmittedto the VA’s Data Processing Center in Austin,Texas, recorded in the automated supply system(the Integrated Procurement, Storage, and Dis-tribution System, or “Log 1“), and then sent tothe appropriate depot to be filled. In fiscal year1982, VA medical centers obtained about $198million in about 650 different supply and equip-ment items (over 95 percent supplies) from the
supply depots. Depot shipments and receipts arealso recorded in Log 1 for the VAMKC’S man-agement of depot stock (100).
Federal Supply Schedules
Under the FSS program, Government agenciescontract with commercial vendors for many sup-plies and services. The schedules allow VA med-ical centers and other agencies to order directlyfrom contractors at preestablished prices. ’ TheVAMKC manages FSS contracts for certain drugs,chemicals, subsistence supplies, and medical sup-plies and equipment (the General Services Admin-istration manages VA FSS contracts for such itemsas furniture and office supplies and equipment)(100). In fiscal year 1982, VA medical centers pur-chased materials worth about $434 millionthrough this program. Table 3 gives a more spe-cific breakdown of FSS purchases for selecteddevices.
Decentralized Contracts and Direct Delivery
The VAMKC also administers decentralizedcontracts for medical centers. These contracts arefor specialized medical equipment, for example,
5 The schedules contain a “buy American differential” clause. Es-sentially, a price differential (percentage) must be applied to a for-eign-made item before placing an order if foreign and domestic prod-ucts are listed under the same special item number in the FSS andboth products satisfy an item requirement (148). This discouragespurchase of the foreign-made item unless the price of the U.S.-madeitem is higher by a certain percentage.
Table 3.—Selected Device Purchases by the VeteransAdministration Using Federal Supply Schedule
Contracts, Fiscal Year 1983a
ExpenditureItems (millions of dollars)
Medical supplies (mainly consumables). . . $120.0Dental supplies and equipment . . . . . . . . . . 17.5Medical supplies and equipment. . . . . . . . . 46.7Pacemakers . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.0Wheelchairs . . . . . . . . . . . . . . . . . . . . . . . . . . 9,6Surgical gloves . . . . . . . . . . . . . . . . . . . . . . . . 1.3Eyeglasses . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.3Medical X-ray film . . . . . . . . . . . . . . . . . . . . . 6,0
aEstimated,
SOURCES: U.S. Veterans Administration, f982Anrwa/ Report (Washington, DC,19S3); U.S. Veterans Administration. Brief of Office of Procurementand Supply, unpublished (Washington, DC, December 1982).

50
electrocardiograph and stress test equipment,sterilizers, pacemakers, and intravenous pumps,which are usually not available through the de-pot or FSS programs. VA medical centers are theprimary users of this program, but other Govern-ment agencies may participate. For direct deliv-eries, the VAMKC not only administers contractsbut also orders for the medical centers. Vendorsthen deliver material to them directly. This pro-gram is used primarily for radiological and nu-clear supplies and equipment (100). In fiscal year1982 these two programs accounted for $158 mil-lion in medical center purchases.
Other Activities
The VAMKC directly procures medical suppliesfor other Government agencies including theAgency for International Development, the Bu-reau of Indian Affairs, DOD, the U.S. Air Forcein the Philippines (CT scanners), the U.S. Armyin Germany, the U.S. Army Medical MaterielAgency (nuclear diagnostic equipment for worldwide distribution), and the U.S. Embassy in Mos-cow. In addition, the VAMKC has processed2,600 individual orders for direct delivery tovarious Army hospitals within the 48 contiguousStates and has provided radiographic equipmentfor U.S. health services in the Virgin Islands. Infiscal year 1982 the total value of this direct pro-curement was $15 million.
The VAMKC also participates in the MedicalShared Procurement Program with DOD, one ofmany Federal interagency agreements for sharingor exchanging materials, facilities and services.b
Commonly used items are procured by one agen-cy to secure the best possible price, while simpli-fying procurement for both the agencies and pri-vate firms. As of July 1983, the total annual dollarvalue of contract awards under the VA-DOD pro-gram was $295 million.
The VA has executed over 200 supply agree-ments with 17 other Federal agencies worth $45.2million per year in exchange for support services.Of the $45.2 million, $33.7 million represents VA
6Agreements have developed pursuant to the Economy Act of June1932, as amended (31 U.S.C. 1535); Public Law 97-258, September1982, as amended; and Public Law 97-332, October 1982.
supply support to other Federal facilities. Table4 shows the source, dollar value, and type of sup-plies provided during fiscal year 1982. The re-maining $11.5 million represents the coordinationor exchange of medical, laboratory, and laundryservices; automatic data-processing systems; re-search and development projects; maintenance offacilities, roads and grounds; and training.
Finally, the VA has established an Office ofSmall and Disadvantaged Business Utilization aspart of a larger Federal program that reservessome procurement for the exclusive bidding ofsmall and minority-owned businesses. The pro-gram was designed to give these businesses equalopportunity to compete for Government contractsand subcontracts (102).
Medical Center Supply Activities
All VA medical centers have similar supply andprocurement characteristics. Generally, each cen-ter has its own supply service that acquires anddistributes supplies and manages center invento-ries. In a few metropolitan areas, centers sharea supply service and warehouse.
The departments within a center, such as die-tetics, engineering, radiology, and pharmacy, or-
71nformation in this section is based on U.S. Congress, GeneralAccounting Office, VA Needs Better Visibility and Control OverMedical Center Purchases, PSAD #81-16, Washington, DC, Dec.12, 1980 (100).
Table 4.—Veterans Administration Supply Supportto Other Federal Facilities, Fiscal Year 1982
costsItems (dollars)From VA depots:
Drugs and medicines . . . . . . . . . . . . . . . . .Other medical supplies . . . . . . . . . . . . . . .General supplies . . . . . . . . . . . . . . . . . . . . .Subsistence supplies . . . . . . . . . . . . . . . . .Equipment . . . . . . . . . . . . . . . . . . . . . . . . . .
Subtotal . . . . . . . . . . . . . . . . . . . . . . . . . .
From f/e/d stations to:Territorial governments . . . . . . . . . . . . . . .Other government agencies . . . . . . . . . . .
Subtotal . . . . . . . . . . . . . . . . . . . . . . . . . .
$8,776,0065,335,163
332,4376,869,817
11,177,690
$32,481,113
$ 371,980803,861
$ 1,175,841
Total . . . . . . . . . . . . . . . . . . . . . . . . . . . $33,656,954SOURCE: U.S. Veterans Administration, Br/ef of Office of Procurement arrd Sup-
p/y, unpublished (Washington, DC, December 1982).

51
der through the center’s supply service. The sup-ply service is required to fill requisitionsappropriately and promptly, ensuring that ven-dor competition is adequate and prices are rea-sonable. Expendable supplies received by a med-ical center are either stocked in the center’swarehouse (posted) or delivered directly to the ap-propriate department (unposted).
The VA’s automated supply system providesinformation for medical centers, as well as theVAMKC, to use in procurement. The medicalcenters contribute data on their stock orders, re-ceipts, and distribution, and use Log 1 to man-age local stock, whereas the VAMKC uses thisinformation not only to manage depot stock butto identify posted items with central managementpotential. Log 1 has files on three types of medi-cal center procurements: expendable posted and un-posted supplies and nonexpendables (equipment).
As described above, the VAMKC centrallymanages items commonly used by VA medicalcenters and provides several centrally managedsupply channels, but it purchases very littledirectly for the centers. The VAMKC mainly se-lects items based on medical center usage, on theassumption that it can obtain lower prices andmore reliable sources than individual medical cen-ters can. VA priorities for sources of medical cen-ter supplies are listed in table 5.
To ensure proper supply channels are selected,the VA requires that the medical centers’ supplyservices review each purchase request. The openmarket may be used to purchase items not avail-
Table 5.—Priority Purchasing
able from centrally managed (so-called manda-tory) sources, when they are needed for an emer-gency or are available at lower prices thanthrough FSS.
The VA’s Impact on Product Quality
An important responsibility of the VAMKC isensuring product quality. This responsibility hasproved difficult to fulfill. In fiscal year 1980 theVAMKC began using Commercial Item Descrip-tions (CIDS) in place of more detailed productspecifications and standards to purchase medicalsupplies and equipment, in response to a new Fed-eral procurement policy to “purchase commercialproducts and use commercial distribution sys-tems” whenever possible (117).8 CIDS and pur-chase descriptions (the latter used only for smallor special purchases) are simplified product de-scriptions of the functional or performance char-acteristics of commercial products acceptable forGovernment use (115). These descriptions are stillto ensure that items purchased are satisfactory.
A 1982 General Accounting Office (GAO)study found that the VA had applied the new pol-icy improperly (101). The VA’s purchase descrip-tions were only one or two sentences long and
8VA specifications were detailed documents, typically coveringdesign, materials, workmanship, and other product features; sam-pling, testing, and inspecting procedures to be used; packaging andmarketing requirements; and other measures to determine whethera product qualified for purchase. Specifications are not to be con-fused with standards, which typically include only a product descrip-tion and performance requirements. However, specifications oftenincorporated standards (12).
Sources for VA Medical Centers
VA priority Approximate annual purchases PercentageSupply channel ranking (millions of dollars) of total
VA excess . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 N Ab N Ab
VA supply depots . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 $197.9 15.3’YoOther government excess . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 0.4Federal prisons and correctional institutions, blind-made
—
and severely handicapped products . . . . . . . . . . . . . . . . . . . . . 4 1.0 1General Services Administration stock . . . . . . . . . . . . . . . . . . . . 5 34<1 2.7VA decentralized contracts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 41.4Federal Supply Schedule contracts . . . . . . . . . . . . . . . . . . . . . . . 7 434.4 3;:;Open market purchases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 498.2 38.5Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . None 86.0 6.6aFiscal year 1982.bNot available.SOURCE: U.S. Veterans Administration, Brief of Office of Procurement and Supply, unpublished (Washington, DC, December 1982).

52
contained little specific information. In addition,GAO concluded that in developing purchase de-scriptions, the VAMKC marketing divisions didnot communicate with users and suppliers. As aresult, the VA purchased many medical items thatwere either unneeded or inferior.
GAO also found other problems in the newCID system. Before using CIDS, the VA had reliedon three elements for quality control:
●
●
●
the marketing division, through its specifica-tions, standards, and qualified products lists;the depot inspectors, through inspectionsupon delivery; andindividual medical centers, through profes-sional opinions and assessments. - -
When the VA stopped using detailed specifica-tions, it also discontinued this three-elementquality assurance program, believing that the pro-gram was based on using detailed specificationsand was therefore no longer applicable. As a re-sult of this change, however, quality standardswere not consistently established in purchasingdevices, and inspection programs were no longerdependable. Again, GAO found that stockeditems were frequently poor or inappropriate. Sur-gical instruments had defects, such as cracks, pits,or rough edges, that could prevent sterilization.Some did not close properly or failed to meet VAtest standards. Other items had missing or bro-ken parts and misaligned components. Finally,when medical centers received these defectiveitems, their complaints were often ignored.
In response to the GAO study, the VA reinsti-tuted some of its traditional measures for qualityassurance:
●
●
●
reestablishing a qualified products list for sur-gical instruments,developing inspection criteria for depot itemsto supplement purchase descriptions, andtransferring responsibility for quality com-plaints from the purchasing divisions to T&Eto improve objectivity and responsiveness (asdiscussed at length in ch. 4).
The VA has now taken a further step throughan interagency agreement with the Food and DrugAdministration (FDA). As of March 1982 the FDAassumed certain quality assurance responsibilities
for VA medical device contracts, including depotstock inspection and investigating the manufac-turing practices of potential contractors (116).
There is still concern, however, that CIDS andpurchase descriptions will contribute to the lowerquality of VA medical equipment and supplies.Surgical instruments, for example, have drawncomplaints from VA medical centers, and for thesame defects (67,79).
The issue of quality has also arisen regardinghospital beds. VA testing and evaluation led tothe recommendation that beds be purchased withspecific safety controls for repositioning, and thisrecommendation was incorporated in earlier prod-uct specifications. VA marketing research alsofound that certain positioning features significant-ly increased cost, yet that VA hospitals rarely usedthese features. Neither of these findings, however,has been consistently applied in VA centralizedpurchasing contracts using CIDS. Instead, moreexpensive beds and beds with fewer safety featureshave often been purchased because of poor prod-uct descriptions (67,79).
Nevertheless, such problems do not demand areturn to the old specifications. The VA, veterans’service organizations, and private manufacturersand vendors agree that device specifications wereoften too rigid, stifling innovation given the sizeof the VA market. One private firm made woodencanes considered obsolete by every other purchas-er, yet it maintained a profitable operation for sev-eral years because of the VA’s outdated specifica-tions. Bradburd also found that VA specificationsfor medical equipment were often written by con-sidering a particular manufacturer’s product, put-ting other manufacturers at a serious disadvan-tage (14) (see app. C). Other VA specificationswere simply unenforced given the range of sup-pliers (12,54,67).
The VA, then, has tried to strike a balance inusing CIDS, writing device product descriptionsboth to maximize the number of potential sup-pliers and to prevent an influx of inferior items.Commodity managers, who are responsible forboth contracts and developing CIDS, now workclosely with T&E to incorporate device evalua-tions and market research into product descrip-tions (12).

53
However, despite the attempted cooperation ofT&E and purchasing divisions, problems may stillarise because their individual goals of quality andefficiency may conflict. Purchasing divisions arecharged to contain VA costs as well as to see thatsupplies are available. Also, factors other thanprice and availability (e.g., product reliability andperformance), while taken into account, are moredifficult to quantify in purchasing.
The VA’s Impact on Product Cost
The impact of the VA’s procurement system onproduct cost depends on supply conditions, thetype of procurement (centralized or decentral-ized), and VA contract procedures and policies.Many industries believe that the VA and otherGovernment agencies obtain the best buy (44).Becker and his colleagues found the “overridingpremise” in selling to Government agencies is thatthey expect low prices. However, industries stillcan benefit (9):
Government orders are sought by most man-ufacturers that would be unacceptable and un-profitable if normal accounting practices werefollowed. The manufacturer generally sells atthese reduced prices based on the premise thatthis is “incremental” or add-on business. . . .With smaller margins than would otherwise berealized . . . the manufacturer may . . . increasemanufacturing . . . utilization of otherwiseunused production time and facilities.
The VAMKC decides to manage an item cen-trally based on several factors: usage, need, cus-tomer service, and cost.9 Certain minimum cri-teria must additionally be met:
●
●
●
●
●
$15,000 in potential sales for new items,an estimated savings of at least 15 percentfor supplying an item through depot stock,annual sales of at least $10,000 to retain anitem supplied through depot stock,the use of an item by at least 10 percent ofall VA hospitals to retain an existing methodof supply, anda realized savings of at least 5 percent on anycentralized contract.
‘Once a decision has been made to procure an item centrally, con-tracts are developed through either a formal bid or negotiation, de-pending on need, demand, and number of manufacturers (12).
These criteria have probably contributed to effi-ciency and savings in VA centralized procurement.
There is also some empirical evidence thatVAMKC policies result in lower product costs.A recent study by IMS America, Ltd., under con-tract to the VA, concluded that the VA is a “mostfavored customer,” even compared to large insti-tutional buyers (44). The study compared theprices of selected items for the VA and the Hos-pital Corp. of America, including catheter needles,syringes, surgical tape, surgical blades, and com-mon pharmaceuticals. The study found that theVA consistently obtained the best buy and con-cluded that the results probably would have beenthe same had another sample of products beencompared. “The size of the VA as a buyer aloneclearly places the VA at an advantage, ” the re-port observed (44).
VA centralized procurement has also comparedfavorably with other Federal procurement. A re-cent survey of 25 hospitals in 10 States by the In-spector General of the Department of Health andHuman Services found that the price of cardiacpacemakers was about 17 percent higher for Medi-care than for the VA (120).
Two studies have criticized the VAMKC’S man-agement of the depot system. The 1982 GAO re-port and the 1983 President’s Private Sector Sur-vey on Cost Control found that VA inventorymanagement techniques increased costs (34).10 TheVA is now simplifying and automating its order-ing and storage systems.
OTA examined the likely effects of VA policieson the costs of procuring nine types of major med-ical equipment: X-ray equipment, computerizedtomography (CT) seamers, digital imaging equip-ment, nuclear diagnostic equipment, nuclear mag-netic resonance (NMR) and positron emission to-mography (PET) scanners, ultrasound diagnosticequipment, patient monitoring equipment, elec-tro-encephalogram (EEG) and electrocardiogram(ECG) equipment, and hemodialysis equipment(this study is presented in app. C). The studyfocused on how the VA affects and is affected by
l’JThe President’s Private Sector Survey on Cost Control furtherrecommended the complete dismantling of the VA depot systembased on its own cost-accounting analysis. Analysis of this issue,however, is beyond the scope of this report.

54
market conditions, and especially on how VAprocurement policies affect the prices and prod-ucts manufacturers offer to the VA. Five officialcontract procedures and one unofficial VA poli-cy were examined for their effects on equipmentcosts: 1) brand name justification, 2) the firm fixedprice clause, 3) public disclosure requirements, 4)no volume commitment, 5) the most favored cus-tomer clause, and 6) the unofficial reluctance toprocure mixed equipment systems.
Analysis of the likely effects of these policiesindicated that they have different, perhaps con-flicting results on procurement prices:
● Brand Name Justification. —When a VA hos-pital is authorized to buy equipment, theVAMKC forwards to the hospital a list ofsuppliers on contract whose equipment meetsthe requirements of the purchase order,ranked by order of cost. The hospital is re-quired to buy from the least-cost supplierunless it can justify purchasing from a dif-ferent source (e.g., because of service avail-ability). This requirement is called brandname justification. Because suppliers are anx-ious to maintain their share of the VAMKCmarket, the requirement almost certainlyresults in lower prices.
● Firm Fixed Price Clause. —Under the termsof a VAMKC contract, suppliers cannot in-crease prices during the contract year. Fur-thermore, if they lower the price at any timeduring the year, the lower price holds for theremainder of the contract year. The firmfixed price clause may or may not result inlower procurement costs. Suppliers offer tem-porary price discounts in the private marketto promote their products. Normally, pro-motional offers would probably be extendedto the VAMKC as well, but because of thefirm fixed price clause, suppliers are reluc-tant to make them. Even the requirement thatprices not be increased during a contract yearhas indeterminate effects on procurementcosts. Although the requirement does pro-tect those who buy~ through the VAMKCfrom price increases, suppliers may chargea higher price at the start to ensure a profit.
●
●
Altogether, it is extremely difficult to deter-mine the net effect of the firm fixed priceclause.Public Disclosure Requirements.—By law,the public has access to VAMKC procure-ment prices for medical equipment. Boththeoretical and empirical evidence supportthe view that this results in higher procure-ment costs for the VAMKC. First, a firm’sbenefits from cutting its price are in part afunction of the so-called retaliation lag, thelength of time before rivals learn of the pricecut and cut their own prices in response. Pricedisclosure requirements reduce the retaliationlag, and therefore discourage price cutting inthe VAMKC market. Because other buyersof medical equipment also have access to theprice data, the VAMKC price may serve asthe other buyer’s target in pricing negotia-tions, which can also inhibit price cutting inthe VAMKC market. Suppliers of X-ray, nu-clear medical, patient monitoring, and hemo-dialysis equipment have stated that prices of-fered to the VAMKC are higher because ofthe contract disclosure requirement. Somesuppliers said the disclosure requirement didnot affect pricing in their markets becausepricing information was widely availablefrom other sources.No Volume Commitment. —Having a con-tract with the VAMKC does not imply anycontractual volume commitment in procure-ment. For most equipment categories (otherthan X-ray and nuclear diagnostic equip-ment), the absence of a volume commitmentis a major factor in pricing. There are twolikely reasons why volume commitmentwould be unimportant in some industries,but very important in others. First, whenequipment is purchased from stock and isfairly standardized, a volume commitmentcan reduce manufacturing costs that can bepassed on to the buyer, but not when theequipment is custom made. Second, the ef-fects of volume commitment seem to dependon whether equipment is expensive or inex-pensive. When equipment is inexpensive, thecosts of preparing contracts and marketing

55
●
●
are higher relative to the purchase price ofthe equipment. In this situation, the cost sav-ings that come with volume commitment aremore significant. Some suppliers indicatedthat they might lower prices by 5 to 10 per-cent in exchange for a volume commitment.One supplier in the ultrasound market statedthat a group purchase of even 15 to 20 unitswould suffice for a larger price discount thanis now offered.Most Favored Customer Clause .—Under theterms of a VAMKC contract, suppliers areprohibited from selling their equipment undera “like contract” to any private buyer at aprice lower than that offered the VAMKC.If a lower price is offered to a private buyer,this price must be given to the VAMKC forthe rest of the contract year. This stipulationhelps ensure that the VAMKC’S clients ben-efit from vendor competition in the privatemarket. Although the strictness with whichthe most favored customer clause is inter-preted varies from one equipment categoryto the next, it almost certainly reducesVAMKC equipment procurement costs. Themost favored customer clause can also havea powerful impact on private buyers. In a fewmarkets, private buyers are offered lowerprices than the VAMKC when they makecontractual volume commitments, on thegrounds that these are not “like contracts. ”The effect of the clause is obviously less inthese markets. However, in cases of no vol-ume commitment, the most favored customerclause may have the effect of increasing pricesthat private buyers must pay for medicalequipment, especially for X-ray, nucleardiagnostic, ultrasound, patient monitoringequipment, and CT scanning devices.Reluctance to Procure Mixed Systems.—Although there is apparently no formal re-quirement to this effect, VAMKC personnelare reluctant in practice to purchase mixedmedical equipment systems, those in whichitems of different companies are intercon-nected. The most important reason for thisis the difficulty of assigning financial respon-sibility for repairs under warranty, in addi-tion to that of determining responsibility foractually making the interconnection. Unfor-
tunately, this VA policy may practicallyeliminate many smaller companies from theprocurement process, causing higher initialprocurement costs.
Perhaps the greatest effects on VA product costsare the result of its generally decentralized pro-curement. Many purchasing decisions are madeby individual VA facilities, not by the VAMKC.
Two decades ago, VA medical centers neededto make few purchases on the open market, only10 percent of their supplies. When the militarydraft ended, it was hard to keep physicians in theArmed Forces, partly because they could not ob-tain the medical instruments and supplies that theypreferred. For this reason, VA and DOD hospi-tal physicians were allowed to purchase moreitems through the open market (34), the purchas-ing arrangement that now accounts for $498 mil-lion, or 38 percent, of VA medical center suppliesand equipment (table 5).
A 1980 GAO report on VA medical center pur-chasing analyzed the large proportion of openmarket purchases (100). GAO concluded that theVA was paying too much as a result of the fol-lowing:
●
●
●
●
●
The VA had not standardized many commonitems. Medical centers were therefore inde-pendently purchasing many different prod-ucts for basic needs, which increased pur-chasing costs.The VA lacked sufficient visibility over med-ical center purchases to address central pro-curement issues effectively, and needed animproved information system.Medical centers failed to use the VA’s “man-datory” supply sources, even though com-mon items were available at lower cost fromthese sources.Competitive bids, although required by Fed-eral procurement regulations for purchasesabove $500, were not often obtained, pro-viding little assurance that reasonable priceswere paid.Neighboring VA medical centers independ-ently obtained common supplies, failing toshare product and vendor information andpurchasing and contracting experience.

56
The VA generally agreed with GAO’s conclu-sions, and the Central Office tightened controlover some aspects of local purchasing by in-stituting quarterly reports on medical centers’ pur-chases from other than mandatory sources. Med-ical centers have complained, however, that theirpurchasing patterns have often stemmed fromproblems with the VAMKC, for example, theproblems of product quality discussed earlier inthis chapter. The VAMKC also delayed from 3to 6 months in sending mandatory source listingsto the medical centers, though apparently at leastin part because of the change to a newly integratedsystem of Federal stock numbers .11 Because ofsuch delays, items may be centrally managed, butmedical centers are unaware of it when orderingsupplies and equipment. These delays also weak-ened the control sought by the Central Office ininitiating quarterly reports (43,51).
In other areas, there has been little or no re-sponse to the 1980 GAO report. Neither the Cen-
I IThe VA Cataloging operations are centralized at the VA supplydepot in Hines, Illinois. Data on items entering the supply systemand on changes in existing items are submitted by medical centersand central procurement programs to the Cataloging Division tobe cataloged in the Federal Catalog System. Cataloged data are thensubmitted to the Defense Logistics Services Center in Battle Creek,Michigan, for national stock number assignment. The national stocknumber identifies an item through all phases of logistics by all Fed-eral agencies. A VA master computer file of all repetitively procureditems contains the national stock numbers and relevant descriptiveand management data for all supply transactions involving theseitems. User catalogs are produced and regularly updated for cen-trally and noncentrally managed items. Additionally, nonexpendableitems are cataloged for property accountability. The major prob-lem in cataloging is eliminating duplicate stock numbers for identi-cal items. The VA-DOD Shared Procurement Program is coordi-nating the cataloging of all new medical items and reviewing thosealready cataloged to eliminate duplication. The VA also participatesin the Federal Supply Management Council Working Group for Cat-aloging Systems in developing Government-wide cataloging policiesand practices for improved supply management. On Nov. 1, 1982,the VA became the cataloging agent and manager for civil agenciesof Federal Supply Group 65, Medical, Dental, and Veterinary Equip-ment and Supplies (121).
DISCUSSION
tral Office nor neighboring VA medical centershave further consolidated purchases or sharedproduct or vendor information. Such coordina-tion has been achieved by VA medical centers onoccasion, but only rarely and by coincidence; forexample, buyers from VA medical centers inWashington, DC, Baltimore, Maryland, Martins-burg, West Virginia, and Perry Point, Maryland,came together for a few years to buy plated mediafor clinical laboratories. One factor inhibiting con-solidated buying is the relative lack of automateddata management systems for supply officers atlocal medical centers, providing little opportu-nity to share contract and purchase experience(18,43,51).
More recently, the President’s Private SectorSurvey on Cost Control criticized the open mar-ket purchasing by VA medical centers, and calledfor more central purchasing to achieve the priceadvantages of buying standard items in quantity.The report commends the recent VA-DOD sharedprocurement efforts, but suggests that VA (andDOD) management provide more routine, de-tailed reports highlighting the number or valueof items purchased on the open market locally thatmight be more economically purchased under na-tionally negotiated contracts. With better devel-oped information systems for supply managementand by “aggressively seeking out commonly pur-chased items to be included in contract negotia-tions, ” VA hospitals could expect to attain the fol-lowing (34):
. . . a level of local purchases that approximatesthe 15 to 25 percent rate experienced by privatesector hospital management firms. This levelshould be given to local hospital personnel as amanagement objective. These personnel haveperformed well toward other goals and it is rea-sonable to believe that they can also achievethese goals. This method has worked well in theprivate sector hospital chains.
With regard to marketing, purchasing, and sup- have been accomplished in various ways. Ideally,plying medical products, the VA has three gen- they should also be attained together. At leasteral goals: product innovation, product quality, with respect to commercially available devices,and low product cost. Individually, these goals however, the VA’s organization and decisionmak-

57
ing have at times exacerbated the inherent ten-sion among these goals.
Available evidence indicates that the VA’s cen-tralized procurement programs, through variouscontract and distribution mechanisms, have oftenensured low prices for their medical centers’ equip-ment and supplies. Manufacturers also generallyexpress a positive view toward the VAMKC proc-ess. The VA is perceived as “progressive” in itspurchasing, and VA central procurement staff aregenerally viewed by device manufacturers asknowledgeable and fair (see app. C).
Nevertheless, the VA’s procurement of medi-cal equipment can be improved. For example, theVAMKC could consider making contractual vol-ume commitments, in particular, for patient mon-itoring, EEG, ECG, hemodialysis, and ultrasoundequipment. Even if the VA practice of decentral-ized purchasing continues for these types of equip-ment, enough VA hospitals may want a givensupplier’s product to warrant a volume commit-ment that would ensure a greater discount.
The VAMKC might also alter contract disclo-sure requirements so that contract price informa-tion is not accessible until 6 months after the be-ginning of a contract year. This policy wouldprovide virtually all the protection of publicdisclosure requirements but could increase thewillingness of manufacturers to discount theirproducts.
Last, the VAMKC should explicitly recognizethat the purchase price of major medical equip-ment often amounts to a small fraction of annualoperating costs. Perhaps the major complaint ofdevice manufacturers is that the VA considers pur-chase price only—not total operating costs—indetermining its suppliers (see app. C for analysis).
Lower equipment and supply costs of course,must not be obtained by sacrificing product qual-ity. The VA has implemented new quality assur-ance policies over the last few years, attemptedto improve the objectivity and responsiveness ofits quality complaint system, and established a
special agreement with the FDA to obtain its ex-pertise in quality assurance. Even so, there mustbe closer monitoring of the VA’s use of specifica-tions, purchase descriptions, and CIDS to ensurequality control.
The VA has adopted over 60 CIDS for medicalsupplies and expendable alone, and is in the proc-ess of adopting some 90 more (12). These docu-ments have influenced the purchase of medical de-vices and will continue to.
Given its use of purchase descriptions andCIDS, the VA should consider the merits of com-parative evaluations. These would more explicitlyidentify device alternatives for VA customers.Comparative evaluations could also identify, andperhaps evaluate, positive and negative featuresof the different devices. Product quality features(e.g., safety, durability, and performance) couldthen be considered along with cost in makingchoices about devices.
The potentially most useful comparative meth-od now is cost-effectiveness analysis. In consid-ering both economic and clinical information, thismethod integrates concerns about costs with thoseabout quality. In a cost-effectiveness analysis, anoutcome is specified (e. g., a patient’s functionalstatus) and the costs of alternative means toachieve it (e.g., using devices) are compared .12
Although cost-effectiveness analyses and similaranalytic techniques have certain methodologicalweaknesses, they can still illuminate issues andsynthesize relevant data. Comparative analysesare neither simple nor necessary for every typeof device. Yet they can improve decisions and pur-chasing contracts, depending on the VA’s use ofthem. More generally, integrating all the VA’s in-formation in purchasing seems as promising as itdoes challenging.
IZFor more discussion on cost-effectiveness analysis, wx U.S. Con-gress, Office of Technology Assessment, The Implications of Cost-Ef-fectiveness AnaJysis of Medical Technology, GPO stock No. 052-003-0076 (Washington, DC: U.S. Government Printing Office, 1980)(107),
25-289 0 - 85 - 5

58
Increased procurement through centralized con- the VA’s being a larger buyer of medical supplies ~tracts would promote the VA’s leverage in the are at least two important ones: 1) greater pricemarket because the size of its market would grow. discounts, and 2) the encouragement of device in-The large number of medical centers’ open mar- novation by providing a larger early market forket purchases now reduces the VA’s advantages new products (52,128).as a large buyer. Among the possible benefits of

Chapter 6
Adopting, Using, andFinancing Devices

Chapter 6
Adopting, Using, and Financing Devices.
The desired result of all the activities directedtoward medical devices is the appropriate adop-tion and use of these devices. In examining thecapacity of the Veterans Administration (VA) tomeet veterans’ needs for such devices, it is thusnecessary to look at the VA system of adoptingand using devices, including selecting, providing,and paying for them. Issues of resource alloca-tion must also be considered in examining thissystem.
Veterans adopt and use medical devices, de-pending primarily, though not entirely, on the VAprograms and services for which veterans are eligi-ble. Through these programs and services, vet-erans receive devices directly, have them financed,and learn about them (109). I
IThe issue of eligibility becomes particularly important since, ac-cording to VA estimates, 58 percent of VA patients are at or belowthe poverty line. Data compiled by the National Center for HealthStatistics from 1971 to 1974 show that the lower a hospitalized vet-eran’s income, the more likely he is to be treated in a VA ratherthan non-VA hospital. In 1980 the VA estimated that veterans dis-
The VA makes available an enormous range ofmedical devices, including, for example, over 300sensory aids for the blind (13). During fiscal year1982, the VA provided over $81 million in pros-thetic services. Each year it provides commerciallyavailable prosthetic devices and services to about1 million disabled veterans (118). In addition, itprovides a range of devices through routine pa-tient care services.
Since adopting and using medical devices de-pends to a great degree both on veteran eligibilityand VA budgeting and financing, these topics arediscussed first. More specific policies and issuesaffecting adoption and use of devices—rehabili-tative devices and medical equipment and sup-plies—are then examined. Finally, more explicitapproaches that consider device adoption in lightof resource allocation are addressed.
charged from VA hospitals were five times more likely to have an-nual incomes under $4,000 (26 percent) than over $10,000 (5 per-cent) (96).
VETERAN ELIGIBILITY FOR PROGRAMS AND SERVICES2
Many VA programs serve veterans’ needs, in-cluding those for: 1) income maintenance, 2) med-ical care, 3) social services, 4) educational serv-ices, 5) vocational rehabilitation and independentliving, and 6) housing assistance. VA programsvary not only in purpose, but in origin, eligibilitycriteria, and ways of providing services (e.g.,through funding only, funding and referral toservices, or direct provision of services), and infinancing and administration.
The greatest expenditures for medical devicesare made through income maintenance and relatedtransfer payments and medical care programs.
‘Except as noted, this discussion is based on an earlier OTA re-port Technology and Handicapped People (109).
Income Maintenance
The VA administers a major income mainte-nance program through compensation for service-connected disabilities and pensions for non-serv-ice-connected disabilities. The VA estimated thatin fiscal year 1983, an estimated $10.2 billionwould be spent for 2.6 million veterans throughthe compensation program, and $4.0 billion for1.8 million veterans through the pension program.
The amount veterans are compensated for serv-ice-connected disabilities depends on how muchtheir disabilities affect their earning capacity incivilian occupations. Additional compensation isprovided for dependents. To be eligible, a veteranmust have contracted a disease, suffered a non-misconduct injury, or aggravated an existing dis-ease or injury in the line of duty, during war or
61
25-289 0 - 85 - 6

62
peacetime. Proof of disability is based on servicemedical records. Service connection may begranted by presumption if a veteran develops oneof several chronic diseases within 1 year of dis-charge from service, tuberculosis or Hansen’s dis-ease within 3 years, or multiple sclerosis within7 years. Once service connection is established,the VA assigns a percentage to the disability froman established “Schedule for Rating Disabilities”(111). Eligibility is thus based on medical criteriaand proof of service. Vocational factors were con-sidered only in developing the “Schedule for Rat-ing Disabilities. ” An individual does not have toprove the inability to earn an income or to sup-port himself or herself with unearned income.
Pensions for non-service-connected disabilitiesprovide incomes to totally and permanently dis-abled veterans and their dependents whose incomeis below an established standard. To be eligible,veterans must have served at least 90 days, in-cluding at least 1 day of wartime, must be medi-cally determined to be disabled, and must havepersonal resources and income below a legislatedamount. At age 65, veterans are considered dis-abled regardless of their physical condition or in-come. Disabled survivors of veterans may alsoreceive benefits if they meet the income test (95).Eligible veterans receive VA cash payments (withthe amount determined by statute), medical andsocial services, and housing and education benefits.
Erlanger and colleagues note that although thedistinction between service- and non-service-con-nected disabilities has always been made in dis-cussing veterans’ benefits, the legitimacy of all vet-erans’ pressure for benefits has never been seri-ously questioned, as was observed in the 1980hearings on the Veterans’ Disability Compensa-tion and Survivors’ Benefits Amendments (111).Veterans’ disability programs have always beenseparate from civilian programs, with better ben-efits and less strict eligibility requirements. Themajor concern of policymakers has been the costof providing all eligible disabled veterans with allnecessary services (26).
Income maintenance programs are importantfor disabled veterans not only for income, but alsofor supplemental benefits and referrals to otherservices. Both device and service technologies areprovided under supplemental benefits, while the
income itself allows recipients to purchase devicesnot covered by supplemental benefits. Incomemaintenance from both compensation and pen-sion programs are funded from general revenues.
Health and Medical Care
Chapter 2 described the VA’s comprehensivemedical and rehabilitative services for veteranswith service-connected disabilities and for thosewith non-service-connected disabilities unable topay for medical care. These services are federallyfunded. Priority for medical and rehabilitativecare is given to veterans with service-connecteddisabilities, an estimated 3 million people. Vet-erans with non-service-connected disabilities maybe admitted to VA hospitals if they are unableto pay for hospital care elsewhere and if beds areavailable.3 Approximately 80 percent of VA pa-tients are veterans without service-connected dis-abilities (114).
VA health and medical benefits include pre-hospitalization, hospitalization and posthospital-ization care, prosthetic and medical devices, nurs-ing home and domiciliary care, devices, transpor-tation services, outpatient services, and prescribeddrugs. Unlike coverage under Medicare and Med-icaid, all technologies and devices suited to an eli-gible veteran’s circumstances and needs are madeavailable. The VA provides blind veterans withnecessary services and devices to overcome theirhandicap and provides other disabled veteranswith technologies and devices deemed medicallynecessary. A growing concern of VA users andpolicymakers is the cost of covering all availabletechnologies and devices. There are now fundingrestrictions for some medical care for veteranswithout service-connected disabilities; for exam-ple, a foster home program is available to suchveterans only when they can pay its cost (109).
3The “inability to pay” requirement does not apply to veterans:1) 65 or older, 2) receiving VA pensions, 3) eligible for Medicaid,4) rated service-connected disabled, or 5) considered former prisonersof war. It also does not apply to those requesting medical servicesin connection with exposure to dioxin or other toxic substances inherbicides or defoliants (e.g., Agent Orange) used for military pur-poses in Vietnam Aug. 5, 1964, through May 7, 1975, in connec-tion with exposure to ionizing radiation from detonated nuclear de-vices as a result of participation in the testing of such a device, orin the U.S. occupation of Hiroshima and Nagasaki between Sept.11, 1945, and July 1, 1946 (96).

63
VA FINANCING AND RESOURCE ALLOCATION
Table 6 shows outlays for veterans’ benefits andservices by functional categories for fiscal years1981 through 1983. Approximately 70 percent ofthe VA budget represents entitlement programs,such as the pension and compensation programs.Spending for these programs is “uncontrollable”in that Congress must modify existing law bychanging the eligibility criteria in order to affectspending. The remaining 30 percent of the VAbudget goes to discretionary programs, primar-ily medical care. Spending for discretionary pro-grams can generally be changed through the ap-propriations process (96).
Veterans who seek VA medical care, then, areserved within the limits of VA resources and leg-islated priorities (94). Under a limited and con-trolled budget, the VA health care system plansfor 1 and 5 years ahead. Alternative plans are pre-pared, ranging from a 5 percent cut in the pres-ent budget to an increase in real terms. Once Con-gress fixes the appropriation, the budget is thenset for the following fiscal year. A reduced ap-propriation, of course, requires a correspondingreduction in staff or services.
Once its appropriation is set, the VA health caresystem is characterized by highly decentralizedplanning and financial management. The VA hasregional and functional health care market areas
Table 6.—Outlays for Veterans’ Benefits and Services,Fiscal Years 1981-83
Outlays by fiscal year(millions of dollars)
1981 1982 1983Items (actual) (estimated) (estimated)
Income security $12,909 $14,070 $14,843Education, training, and
rehabilitation. . . . . . . . 2,254 1,883 1,557Hospital and medical
care . . . . . . . . . . . . . . . 6,965 7,594 8,108Housing . . . . . . . . . . . . . . 201 –68 –863Other benefits and
services . . . . . . . . . . . . 662 680 741Offsetting receipts. . . . . – 3 – 3 – 3
Total outlays . . . . . . $22,988 $24,155 $24,383SOURCE Budget of the United States Government for Fiscal Year 1963, pp. 5-166,
as reported by U.S. Congress, Congressional Research Service, MedicalCare F70grarns of the Veterans Adrnirristration, Report No. 63-99 EPW(Washington, DC, May 16, 1983).
and has assigned fiscal and budgetary authorityto the regional consortia of its medical centers.
Regional allocations are prospectively budgetedby the Central Office. There are now 28 subdivi-sions known as “Veterans Administration Medi-cal Districts” (fig. 6). Each medical district typi-cally represents 4 to 10 VA medical centers thatall offer primary and secondary care and someaccess to tertiary care. This “regionalization” inmedical district budgeting is intended to help co-ordinate services provided by all members of thedistrict, to avoid unnecessary duplication and toencourage new services only where they are re-quired by large populations (16).
The formula used in resource allocation givessome weight to outpatient visits but more to bedoccupancy. A new system for budgeting inpatientcare based on diagnosis-related groups (DRGs) isbeing introduced (see the corresponding sectionbelow). In the future, the formula maybe changedto reflect the size of the veteran population, ad-justed for age (29,59).
Management Initiatives
Several health care management initiatives havebeen taken in recent years through both legislativemandate and administrative fiat. These initiativesaffect the VA’s allocation of resources and adop-tion and use of devices, particularly equipment.
Facility Planning
Each VA medical center annually prepares aconstruction and facility improvement plan cov-ering the next 5 years. This plan, which is re-viewed and approved by the Central Office, pro-poses construction according to program andservice plans.
Each year, the VA develops and submits toCongress a 5-year comprehensive medical facil-ity construction plan for VA projects requiringover $2 million. The plan submitted in June 1982,covering fiscal years 1983 through 1987, identified252 projects with a total estimated cost of $5.4billion (119).

64
Figure 6.—Veterans Administration, Department of Medicine and Surgery Medical Districts, 1983
SOURCE: U.S. Veterans Administration, as reprinted in U.S. Congress, Congressional Budget Office, Human Resources and Community Development Division, VeteransAdrrrlnk?tration Health Care: Planning for f9W (Washington, DC, Februa~ 1983).
Construction needs for projects costing less than$2 million are also identified from the medical cen-ter facility plans. For fiscal years 1983 through1987, such projects numbered more than 1,400,with an estimated total cost of $850.4 million. Infiscal year 1982 the VA began emphasizing thesesmaller projects and proposed an increase for itsfiscal year 1983 budget for this purpose (119).
Medical Equipment Reporting System
Not surprisingly, the VA’s medical equipmentinventory has increased in both quantity and com-plexity over the years. To manage all this medi-cal equipment, the VA has developed an interac-tive computer-based Medical Equipment Report-ing System to help both VA medical centers andthe Central Office maintain and access equipmenthistories, identify important performance trends,track mandated corrective actions, and establish
a data base for utilization review and resourceplanning. Each VA medical center will eventuallyhave access to both local and systemwide experi-ences and trends (119).
Health Resources Sharing
Public Law 97-174, the VA-Department of De-fense Health Resources Sharing and EmergencyOperations Act, was intended to promote costsavings while providing veterans and the militarymore comprehensive services. The two agenciesplan several joint efforts (121):
● Establishing a VA-Department of DefenseHealth Care Resources Sharing Committeeto review policies and practices and to rec-ommend changes. Monitoring the acquisitionof major equipment and the locations of newfacilities will be part of the committee’sresponsibilities.

65
Publishing guidelines based on the commit-tee’s recommendations, which must not ad-versely affect the range of services, qualityof care, or established priorities of eitheragency.Authorizing interagency sharing agreementsamong all medical facilities for referrals, withreimbursement to the facility delivering care.
The VA is first determining services that canbe shared, to permit direct reimbursement. Shar-ing will primarily be locally initiated, but a fewprograms will be developed in the VA’s CentralOffice and the Pentagon.
The VA’s authority to share specialized medi-cal resources was first established in 1966 (in Pub-lic Law 89-785) to permit VA medical centers toshare underutilized, specialized, scarce, and costlyresources with other medical centers, communityhospitals, Federal and State hospitals, clinics, andblood and organ banks, so as to eliminate duplica-tion. The law similarly permits the VA to usecommunity resources for veterans. Shared re-sources have included computed tomography(CT) scanners, electron microscopy studies, spe-cialized laboratory procedures, nuclear medicineservices, radiation therapy, cardiac catheteriza-tion, open heart surgery, dialysis, ultrasound, andmammography (119).
Medical District Initiated Program Planning
Perhaps the VA’s most important step for theadoption and use of devices has been Medical Dis-trict Initiated Program Planning (MEDIPP), begunin 1981. MEDIPP is a long-range “strategic plan-ning system” giving greater responsibility for re-source allocation to the VA’s 28 medical districts(136).
MEDIPP evolved to respond to two seeminglyincompatible conditions: the short-range demandfor more (and different) services and long-rangedeclining demand, both a function of the agingveteran population. As the many veterans ofWorld War II and the Korean conflict enter their60s and 70S, their health care needs will increase.Yet, as these veterans die, the demand for serv-ices will drop sharply, especially if no major mil-itary conflict brings large numbers of veterans intothe system (123).
From 1970 through 1979 VA medical care ap-propriations tripled, from roughly $1.7 billion to$5.3 billion. Cost consciousness increased corre-spondingly toward the end of the decade. Since1977 the VA has faced stable or declining healthcare budgets (adjusted for inflation). Given thegeneral political concern about VA spending andthe changing demographics of the veteran popula-tion, the VA has recognized that past planningand management approaches are no longer fea-sible. MEDIPP is intended to provide the basisfor planning and managing the VA’s changinghealth care delivery needs (59,123).
Since the VA will certainly have to discontinuesome services or facilities, organizational and con-stituency understanding and acceptance may besignificant hurdles for MEDIPP’s success. For thisreason, MEDIPP will involve administrative andclinical personnel at several levels within the VADepartment of Medicine and Surgery.
MEDIPP begins its work each year on Novem-ber 1 when the VA’s Chief Medical Director pub-lishes a list of the general issues, objectives, andgoals for the immediate and long-range future ofthe Department of Medicine and Surgery pro-grams. This report is used by each VA medicaldistrict, which appoints a district planning boardand staff to develop a district plan. District plansreflect demographic analysis, a workload forecast,and a review of local resources submitted by theVA facilities within its jurisdiction. District plansare reviewed by district and regional administra-tors and councils, and when approved, submittedto the VA Central Office (119,136).
In MEDIPP’s first year, 28 medical district planswere submitted to the Central Office on Novem-ber 1, 1982, covering fiscal years 1985 through1990. More than 400 administrative and clinicalpersonnel helped prepare the plans, along withthe representatives from veterans’ service orga-nizations who served on medical district planningboards, advisory committees, and task forces.These initial district plans will provide the basisfor developing a national strategy that identifiesprogram directions of the Department of Medi-cine and Surgery, trends in veterans’ health careneeds, and the types and sizes of facilities and mixof health care services required to meet these needs(119).

.
66
An initial problem in MEDIPP has been devel-oping adequate program standards and criteriatoward formulating VA district plans and nationalpolicies. Like health planning laws and programs(e.g., certificate-of-need requirements) that reg-ulate private health care investments, MEDIPPmust set quantitative and other standards for spe-cific technologies, such as general hospital beds,open heart surgery, cardiac catheterization, andend-stage renal disease services. The VA is alsonow developing case-mix workload and generalstaffing guidelines for new planning standards(7,59).
The promise of MEDIPP is in providing the VAan initial framework for rational planning in anera of dwindling health care resources. Its signifi-cance in relation to devices mostly concerns equip-ment. District plans will propose the creation, ex-pansion, or dismantling of services, specifyingrequirements for construction, staffing, and newequipment. The implications of the plans for med-ical supplies will probably be vague. Likewise,changes in the adoption and use of prosthetic de-vices will be identified through MEDIPP only inthe case of new rehabilitative services. However,MEDIPP could identify and monitor the need anddemand for various types of major medical equip-ment. MEDIPP could then be used not only inplanning, but also to track the adoption and useof major equipment. Requests and proposals fordevice equipment could then be considered in lightof their cost effectiveness in delivering care. Tosome extent, VA-initiated research has already be-gun to explore these possibilities, as discussedbelow.
ADOPTION AND USE OF DEVICES
Eligibility and payment for services obviouslyaffect the adoption and use of devices. The deci-sion of whether to include a device in a specificservice or to provide a device to an individual indelivering care is also assumed to have a majorinfluence on adoption and use.
Individuals’ circumstances and needs have tra-ditionally been identified at the clinical level,within the relationship of patient and provider.
Diagnosis-Related Groups
Another new process that may affect medicaldevice adoption and use is setting VA inpatientbudgets using DRGs (28). Although the VA hasbudgeted prospectively because of the congres-sional appropriations process, the use of a case-mix measure such as DRGs is intended to distrib-ute funds more rationally among medical centersthan have previous arrangements. DRGs classifypatients by principal diagnosis, surgical proce-dure, age, presence or absence of significant co-morbidities or complications, and other relevant cri-teria. The new Medicare prospective payment sys-tem for hospitals is also based on DRGs. The VAbudgeting system and the Medicare payment sys-tem use similar mathematical models to assign pa-tients to DRGs and to allocate resources amongDRGs.
Data sources for the VA system include all VAdischarge abstracts, costs by different service cat-egories (medical, surgical, psychiatric), the cur-rent model of 470 DRGs used by Medicare, andthe New Jersey Reimbursement Schedule. Sincethe VA has no patient-based method of assign-ing costs, the VA used New Jersey cost data toassign relative DRG weights to the VA discharges,and these weights were used for allocation deci-sions (27).
DRGs will also be used in VA utilization re-view and quality assurance programs (27). Capi-tal purchases are excluded from the DRG rate, andhospitals do not keep surpluses. Thus, DRG budg-eting will affect the use of devices more than theirpurchase, which will be affected more byMEDIPP.
VA medical, surgical, and rehabilitative serviceshave been relied on to determine need, developrationales for specific devices, and request pro-curement formally through the VA Office of Pro-curement and Supply (13).
Rehabilitative Devices
After World War II, VA rehabilitation serviceswere concerned primarily with treating a fairly

67
large group of young war-injured veterans. TheVA’s rigorous pursuit of this mission, accordingto a 1977 National Academy of Sciences (NAS)report, led to its world leadership in the clinicaluse of devices and techniques for aiding physi-cally handicapped people (62).
Today more than 80 percent of those treatedthrough the VA’s rehabilitative services have non-service-connected disabilities, with many suffer-ing from the chronic diseases associated withaging. The postwar period has also seen rapidgrowth in medical knowledge and technology, in-cluding substantial changes in treatment ap-proaches in rehabilitation (62).
The VA provides rehabilitative devices througha number of special services and programs.
Rehabilitation Medicine
All VA hospitals have rehabilitation medicineservices, but only 52 have rehabilitation medicinebed sections. The VA rehabilitation programsvary in size, type, and organizational arrangement(62,119). For example, there is a cardiopulmonaryrehabilitation program at the VA medical centerin Wood, Wisconsin, and driver training pro-grams for the handicapped at several other med-ical centers. In fiscal year 1982, the VA beganusing an additional teaching vehicle (the MED-VAN Mark IX system) for severely disabled vet-erans, such as quadriplegics, at two VA medicalcenters. Six independent living centers were estab-lished in 1981 at VA medical centers to eliminatethe barriers that limit veterans in community liv-ing, including barriers that are physical, psycho-logical, social, and environmental. More than 25VA medical centers are also involved in rehabilita-tion programs focusing on the aging veteran (119).
Spinal Cord Injury Centers
There are now 19 VA Spinal Cord Injury Cen-ters across the country. They provide initial care,rehabilitation, and long-term care for about 7,200patients. In addition, there are about 31,000 year-ly outpatient visits of those with spinal cord in-juries. Home care programs for these patients re-corded 14,600 visits in fiscal year 1982. Manyspecial services must be provided to the spinal-cord-injured patient, from medical and rehabilita-
tion care to adjustment counseling. Urodynamiclaboratories have been established recently forSpinal Cord Injury Centers to provide intensiverehabilitation and sustaining care. Urodynamiclaboratories are essential for evaluating theneurogenic bladder, and proper diagnosis oftenpermits patients to be catheter-free and avoidurinary tract infections (119,145).
Blind Rehabilitation
In the Blind Rehabilitation Program, servicesare provided by the six VA Blind RehabilitationCenters and Clinics, and by 75 Visual ImpairmentService Teams located at VA medical centers.
The Blind Rehabilitation Centers give trainingin orientation and mobility, communication,manual skills, and activities of daily living, alongwith evaluating vision and prescribing aids suchas electronic reading and travel aids. The BlindRehabilitation Centers also provide counseling topatients and their families, physical recondition-ing, and recreation, and they conduct research onblindness and rehabilitation, prosthetics, and sen-sory aids for blind people.
The Visual Impairment Service Teams focus onoutpatient treatment, annually reviewing thehealth profiles, living circumstances, social adjust-ment, and personal needs of blind people. Theseteams include staff physicians, social workers, andother VA medical center personnel.
The VA also has a Vision Impairment Centerto Optimize Remaining Sight. Currently there isonly one such center, at the VA medical centerin Kansas City, Missouri, under the Hospital Op-tometry Section of the Eye Clinic (141).
Audiology and Speech Pathology
During fiscal year 1982, the VA issued approx-imately 34, 000 hearing aids to eligible veteransthroughout the Nation. The procedure for obtain-ing a hearing aid from the VA is straightforward.The eligible veteran applies for a hearing aid atthe nearest VA facility, and is given orological andaudiological examinations. During 1982 morethan 574,000 patient visits were reported by the98 VA audiology and speech pathology programs.Additionally, a program offering services by com-

68
puter is being pilot tested in the southeastern re-gion of the country (119,127).
Prosthetics
By regulation, the prosthetic shops (“OrthoticLaboratories”) of VA hospitals may make onlytemporary prostheses. Definitive prostheses mustbe obtained from commercial vendors under con-tract to the VA.
Definitive prostheses are obtained through aprosthetics representative, a veteran with a serv-ice-connected disability who is the purchasingagent for all prostheses, from eyeglasses to mo-torized wheelchairs. The 96 prosthetics represent-atives at some 80 VA facilities dispense more than$84 million per year in devices in initial and re-peat prescriptions (62). Table 7 gives a sample ofrehabilitative devices distributed to veterans infiscal year 1982.
Clearly, the prosthetics representative is cen-tral in the adoption process. Representatives mustbe thoroughly familiar with all VA-authorizedprosthetic, orthotic, and sensory aid devices, andother rehabilitative equipment. Representativesmust also know fitting techniques, eligibility re-quirements, and device sources. They are respon-sible for educating the clinical and managementstaff at their hospitals about the prosthetics pro-gram. Finally, they must submit administrativereports and work with contracting prostheticssuppliers (159).
Prosthetics representatives serve as counselorsfor veterans who need prostheses. Clinic teamsof physicians, physical or occupational therapists,
Table 7.—Sample Rehabllitative Devices Distributedto Veterans, Fiscal Year 1982
ValueItem Number of devices (dollars)
Aids for the blind. . . 15,156 $ 512,352Artificial limbs . . . . . 10,598 10,171,840Braces . . . . . . . . . . . . 36,308 2,336,293Corset belts . . . . . . . 20,641 236,884Eyeglasses . . . . . . . . 101,286 3,419,484Hearing aids . . . . . . . 32,252 243,625Shoes. . . . . . . . . . . . . 29,597 704,740Wheelchairs . . . . . . . 30,981 10,055,721SOURCE: U.S. Veterans Administration, VA Annual Report IWZ (Waahlngton, DC,
19s3).
prosthetists, and prosthetics representatives meetwith the veteran to decide which, if any, pros-thesis should be prescribed. They choose fromamong the devices approved by the Prosthetic andSensory Aids Service (PSAS) of the VA. PSASmakes its decisions through its Prosthetic Tech-nology Evaluation Committee on the basis of eval-uative research conducted by the VA or other in-vestigators. In some cases, clinic staff mayrecommend a prosthesis that has not yet beenevaluated. PSAS is asked to rule on these casesindividually (88). When it determines that newcommercially available devices are needed, PSASwill formulate the technical specifications for thedevices, and negotiate service contracts with pri-vate manufacturers directly or through profession-al associations, such as the American Orthoticsand Prosthetics Association (13,24).
PSAS also directs the national VA prostheticsprogram, including the VA Prosthetics Center (seechs. 3 and 4); 20 Prosthetic Treatment Centers,which provide specialized services for a region;53 Orthotic Laboratories, which fabricate and fittemporary limbs; 11 Restoration Clinics, con-cerned with artificial eyes, facial and body restora-tions, cosmetic hands, plastic ear inserts, and simi-lar items; and prosthetic activities within VAmedical centers and outpatient clinics (143).
Past Problems
Prosthetics representatives specifically and theVA prosthetics program generally have been thefocus of criticisms over the last several years. The1977 NAS study of the VA concluded that the VAtook much longer to obtain prosthetic devicesthan did private hospitals. In addition, the studyquestioned the prosthetics representatives’ refill-ing device prescriptions that did not require amedical recertification of need (62). A 1979 VAprogram evaluation concurred with the NAS re-port, concluding that some prosthetic services forpatients were too slow, and also noted that theprogram’s efficiency and effectiveness were dimin-ished by other factors (143). One was the reduc-tion in the Central Office staff for PSAS fromeight in 1973 to four in 1979. The report stated:“Liberalizing legislation has had the effect of in-creasing Prosthetic and Sensory Aid workload,yet program staffing was decreased. . . .Present

69
staffing of the service would appear inadequate. ”To minimize increased workload and decreasedstaffing, various VA Central Office functions wereassigned to selected field facilities. In several cases,no authority was delegated and no official trans-fer documents addressed these significant oper-ating changes (2,143). The VA report furtherfound no evidence of major program planning inthe PSAS Central Office.
The NAS evaluation also concluded that theVA chain of command, in which prosthetics fieldpersonnel report directly to hospital directors,resulted in lack of direction to prosthetics repre-sentatives in the field (62):
There is a lack of sufficient communication be-tween VA Central Office program officials and[VA medical center] prosthetic representatives.Most problems in this area are due to a lack ofupward communications. Upward communica-tions must pass through [VA medical center]Operations to get to Prosthetic and Sensory AidsService.
Recent Policy Changes
Since the VA’s internal evaluation of PSAS, thelatter’s Central Office staff was increased fromfour to eight persons and began to address someof the problems of the prosthetics program. Tospeed prosthetics procurement, for example, VAmedical centers have been allowed since 1981 todirectly purchase (through decentralized con-tracts) new, commercially available prosthetic ororthotic appliances and repairs for other prosthe-tic appliances costing up to $300 (2,118). Otherefforts begun in 1982 were comprehensive train-ing programs for new prosthetics representativesand other prosthetics personnel, revised contract-ing procedures for artificial limbs, a more system-atic evaluation program (see ch. 4), a newsletter,and revisions of outdated training and specifica-tion manuals, many dating to the 1950s. In addi-tion, the VA is now discussing reorganization thatwould put Rehabilitation R&D, PSAS, and theVA Prosthetics Center in one administrative struc-ture (13).
Veterans’ groups, such as Disabled AmericanVeterans and Paralyzed Veterans of America,have supported recent PSAS policy changes, butfeel many more are needed (2,39). Because of
PSAS’S very large field staff, veterans’ groups areconcerned that Central Office policy changes willbe delayed (159). (App. B further discusses theconcerns of veterans’ organizations. ) There arestill many reports of disabled veterans’ being pro-vided inappropriate devices, because of either thepractices of prosthetics representatives or CentralOffice policies. For example, wheelchairs procuredby VA medical centers for hospital transportationare often distributed to veterans as prescriptionchairs. Such chairs have often not met veterans’needs and have not proved durable outside hos-pitals.
Future Issues
Perhaps the major PSAS issue that the VA mustaddress over the next few years is the prostheticsbudget and related fiscal practices. The PSASbudget has tripled in 8 years to $84 million andhas been projected to reach $500 million annuallyin 4 to 5 years (24). One reason for the steep risein costs has been the increased purchase of sophis-ticated technology for handicapped people. An-other reason is the increasing population of vet-erans whose mobility and senses are affected byaging (119). Probably the most significant forcebehind the escalation, however, is that provid-ing prosthetics to veterans is unlimited by law (38U.S.C. sec. 5023):
The Administrator may procure prosthetic ap-pliances and necessary services required in thefitting, supplying, and training and use of pros-thetic appliances by purchase, manufacture, con-tract, or in other such manner as the Adminis-trator may determine to be proper, withoutregard to any other provisions of the law.
Because the prosthetics budget receives no sep-arate congressional appropriation, funds for pros-thetics are drawn from the VA’s annual appropria-tion for medical care, which is fixed prospectively.As a result, the prosthetics budget has drained re-sources from other parts of the health care budg-et as prosthetics costs have expanded.
The unconstrained prosthetics budget has alsocontributed to undesirable administrative prac-tices within the VA. Because PSAS handles a highvolume of devices, and because of the generalavailability of prosthetic devices, other VA reha-bilitative services (Blind Rehabilitation, Spinal

70
—
Cord Injury Centers, etc.) have come to use PSASas a purchasing clearinghouse for their own sup-plies and devices. PSAS therefore orders such sup-plies as pacemakers and kidney dialysis machines,which have very little to do with the functionsof prosthetics representatives. Although this han-dling of supply functions has helped hold downthe personnel requirements of other rehabilitativeservices, it has of course placed fiscal and admin-istrative burdens on PSAS (24,160).
The VA has tried to constrain prosthetics coststhrough somewhat paradoxical fiscal practices.Although PSAS directs national VA prostheticspolicies, it has little control or advisory functionover the program’s budget outside the Central Of-fice. PSAS participates in the Central Office’s ini-tial distribution of funding to medical districts.The distribution of funds within the medical dis-tricts, however, is the responsibility of the medi-cal district directors, and that within medical cen-ters is the responsibility of the medical centerdirectors. All medical districts and medical centersare semiautonomous, so that prosthetics servicesreceive whatever budget allotment their medicalcenter director determines. Poor communicationbetween the PSAS Central Office and prostheticsrepresentatives about budget needs has sometimesresulted from the separation of program andbudget lines of authority (143). The proposedadministrative realignment mentioned earliershould ameliorate this situation.
VA policymakers are examining several waysto resolve the increasing budgetary and fiscalproblems in providing prosthetic devices. One ap-proach is to have Congress appropriate a pros-thetics budget separate from other health carefunding. A second would limit devices to veteranswith service-connected disabilities, now a minor-ity of the disabled veterans served by the VA. Athird approach is to assess more thoroughly theimpact of the range of rehabilitative devices onthe health and well-being of the individual veter-an and on VA costs. The third approach wouldallow the VA to plan resource allocations morerationally. The VA has already implemented thisapproach to some extent through the ProstheticsTechnology Evaluation Committee, as discussedin chapter 4. This committee makes decisionsabout rehabilitative device adoption and use in
the context of general VA health care goals. Simi-lar approaches can be taken in acquiring and usingother devices, as discussed below.
Medical Equipment and Supplies
Although the VA centrally plans its general pol-icy, daily planning, administration, and deliveryof health care is carried out by VA medical facil-ities. The VA Service Directors in the Central Of-fice issue performance guidelines and routinelymonitor the utilization and quality of all programunits, but have very little authority over medicalcenters’ decisions about device adoption and use.As noted above, budgets are allocated regionally,and medical equipment and supplies are pur-chased by local supply officers. The VA providesits central Testing and Evaluation Staff, but itsrole is advisory. The main Central Office influ-ence over routine device purchase and use isthrough establishing testing standards, evaluatingand centralizing contracting in light of thosestandards, and establishing purchasing sourcepriorities for VA facilities. The determining fac-tors for many device purchases are found withinindividual VA health care facilities (38,62). Phy-sician freedom in choosing medical devices, forexample, has been at least an implicit VA policysince the early 1960s.
Controlled Item Acquisition
A clear exception to this purchasing pattern ex-ists with equipment and supplies that the VA Cen-tral Office regulates as “controlled items. ” Thecontrolled medical device items (listed in table 8)are generally relatively costly equipment, requir-ing an initial investment of $5,000 or more. Theymay also require substantial outlays for facilityspace, staffing, disposable, and maintenance (157).Controlled item acquisition can be regarded asanalogous to certificate-of-need requirements (84).
Acquisition of medical and dental equipmenton the VA’s controlled item list may be initiatedeither locally or through a Service Director in theCentral Office. In the first case, VA medical fa-cilities often rely on Major Medical EquipmentCommittees, a cross-section of medical center staffand clinicians, to determine medical need. Whenit is warranted, the committee will request that

71
Table 8.—VA Controlled Item List for Medicaland Dentai Equipment, 1982
—Cost threshold
Equipment type (dollars)
Cardiac defibrillation . . . . . . . . . . . . . . . . . .Physiological monitoring . . . . . . . . . . . . . .C!inicai laboratory equipment and
instrumentation . . . . . . . . . . . . . . . . . . . . .Electroencephalograph . . . . . . . . . . . . . . .Gastric hypothermia . . . . . . . . . . . . . . . . . . .Electron microscope for use in clinical
laboratory . . . . . . . . . . . . . . . . . . . . . . . . . .X-ray apparatus . . . . . . . . . . . . . . . . . . . . , . .Nuclear medicine . . . . . . . . . . . . . . . . . . . . .Ultrasonic unit, diagnostic . . . . . . . . . . . . .X-ray film processor, automatic or
manual e. . . . . . . . . . . . . . . . . . . . . . . . . . . .Dental cabinet, modular or unitizede . . . . .Dental operating chair . . . . . . . . . . . . . . . .Dental operating unite . . . . . . . . . . . . . . . . .High velocity oral evacuation unite . . . . . .Dental operating Iighte. . . . . . . . . . . . . . . . .Automatic dental X-ray film processor . .Dental X-ray apparatus . . . . . . . . . . . . . . . .Acupuncture equipment and needlese f
. . .Neurosurgical subcutaneous
stimulator . . . . . . . . . . . . . . . . . . . . . . . . .Surgical laser, including accessories . . .Cardiac pacemaker surveillance
equipment. . . . . . . . . . . . . . . . . . . . . . . . .—
$4,500(b)
30,000’7,500
10,000
(b)(b)
5,000d5,000
(b)1,200(b)(b)(b)(b)
1,0002,500(b)
(b)(b)
(b)NOTE: If a device’s purchase price exceeds the “cost threshold,” the purchase
must be specially reviewed.aconstant display of electrocardiographic curve, temperature, respiration, and
blood pressure.bNo cost threshold.cper Item or where combined cost components total $~,~ or more.dper item or Items costing this amount in a single purchase.eEXCept when acquired from a VA supply depot, a VA decentralized schedule,
the VA Marketing Center, or a Federal Supply Schedule contract.f Restricted to research in the Surgical SerVICe.
SOURCE: U.S. Veterans Administration, VA Marrua/, subchapter E, change 155(Washington, DC, Oct. 14, 19S2).
an additional evaluation be performed on site inthe medical center. Evaluations may also be con-ducted in conjunction with the VA’s Medical Re-search Service, as was the case for CT scanners.The committees generally meet as needed to con-sider equipment standards and safety, to resolveproblems involved in acquisition and use, and todevelop and recommend policy (140).
Service Directors in the Central Office approveor disapprove controlled item acquisitions basedon more or less explicit criteria of program needs,experimental or commercial status, and the sup-port provided to other VA facilities and districts.Often, specific standards of productivity or uti-lization are developed in advance and dissemi-nated to medical facilities.
Service Directors also seek to ensure that re-sources are available for pIanned or authorizedprogram growth. If funding is not availablethrough a facilities budget allotment, equipmentmay be reimbursed through a special fund main-tained by the Chief Medical Director’s office. Thisfund is used to allocate moneys, as they becomeavailable during the year, toward unfunded VAneeds, although no explicit criteria are used inmaking these supplemental allocations (62).
When device acquisition has been part of abroader effort to initiate so-called specialized med-ical services (e. g., renal transplantation or openheart surgery), the VA’s Chief Medical Directorhas in the past also established ad hoc advisorygroups. These groups have been composed of VAand non-VA physicians with expertise in the par-ticular program specialties, who, through regularmeetings, and sometimes site visits, provide qual-ity overviews of the programs.
For example, the shift toward purchasing CTscanners, rather than contracting for CT services,was justified in a 1978 VA report by the SpecialCentral Office Advisory Group for ComputerizedTomography Units (155). The report found thatthe cost of performing a CT examination on VA-owned scanners was only about 60 percent of thecost of the same examination obtained under con-tract from a civilian institution, which led to theVA’s policy of purchasing CT equipment when-ever possible (108).
Social and Political Forces
As this chapter has shown, the VA has oftendeveloped well-defined procedures, conductedanalyses, and presented technical criteria forequipment acquisition within its facilities. How-ever, these facts should not obscure the politicaland social factors in VA device adoption and use.Regardless of the VA’s planning, medical schoolpreferences and politics have considerably influ-enced the VA system.
Thompson, for example, has argued that theVA’s desire to be associated with medical schoolshas shaped hospital construction decisions farmore than other concerns, such as promoting vet-erans’ access to medical care (91). To ensure the

72
quality of their personnel and foster medical pro-fessionalism, VA administrators have wished tolocate facilities near medical schools and havesought to make their institutions hospitable placesfor teaching and research. Medical schools havesuccessfully encouraged VA hospitals to seek thelatest equipment and specialized facilities. The1977 NAS study noted a proliferation of variousspecial care units, for example, nearly 70 cardiaccatheterization units (62). Each VA hospitalseemed to want its own specialized resources, inpart to satisfy its medical school affiliates, eventhough these resources were frequently underused.
Two other factors have also affected resourceallocation, namely, the VA’s voluntary relation-ships with regional and State health planningagencies and the absence of effective utilizationreview. Under Public Law 93-641, the NationalHealth Planning and Resources Development Actof 1974, the VA was given voting membership onState health coordinating councils and on regionalhealth systems agencies .4 A VA hospital was sup-posed to submit an application to the health sys-tems agency for new construction or equipment.The agency made a recommendation to the VACentral Office, which could approve or dis-approve without regulatory constraint and did nothave to explain its action. NAS recommended thatthe VA become part of the general health careplanning process established for communities andregions (62).
The absence of effective utilization review is asecond possible reason for inefficient resource al-location. VA hospitals have not been under theProfessional Standards Review Organization(PSRO) program, the peer utilization review forMedicare and Medicaid. The VA moved, some-what slowly, to establish a VA Health Services
4The main reasons for this legislation were to establish mecha-nisms for developing national health planning policy and to aug-ment areawide and State planning for health services, manpower,and facilities, in order to curtail the rise in health care expenditures,improve access to care, and ensure quality of care, A non-VA hos-pital needed to apply for approval of substantial construction andexpensive equipment to the local or areawide health systems agency,which made a recommendation to the State planning agency. TheState agency approved the recommendation or reversed it with anexplanation; the applicant could appeal. Final approval or denialof an application was made by the Secretary of Health and HumanServices.
Review Organization for quality assessment andutilization review. As part of this initiative,Thompson (90) notes that the VA may haveadopted some of the shortcomings of the PSROprogram, such as deriving standards for hospi-tals in peer groups by examining treatment proc-esses, which would identify outlier hospitals butwould not pinpoint excesses committed by all fa-cilities in a peer group.
Other social and political forces have con-strained the VA’s adoption and use of devices. Forexample, the VA’s attempts to increase its CTscanners were criticized in a General AccountingOffice report (98) and opposed by Congress in thelate 1970s. When, in 1978, the VA moved to pur-chase 13 new scanners to supplement its existing24, congressional resistance prompted the VA towithdraw the request. Furthermore, the Office ofManagement and Budget placed considerablepressure on the VA to reduce hospital beds. TheVA reduced them, as a result, from about 121,000in 1964 to fewer than 90,000 in 1980 (91). (Re-cent legislation [Public Law 97-174] requires theVA to operate at least 98,000 beds.)
Generally, the social and political pressures onthe VA to overadopt devices in some areas of careand to constrain expenditures in others have anadditional important implication. The VA’s re-sources may be adequate for its functions, butmay not be distributed equitably or efficientlyamong geographic areas, types of facilities, orfunctions within and across hospitals. The VA’soften sporadic adoption and use of devices andother technologies and patterns of care seem toprovide ample evidence of this. The VA has dem-onstrated international leadership in such areasas cardiac care and radioisotopes. Yet in 1983fewer than one-third of VA hospitals had CTscanners (40), and the 1977 NAS study found evi-dence of maldistribution of equipment, basic andspecialized services, staff, and beds (62).
NAS also found that some of this poor distri-bution could be attributed to the VA Central Of-fice and its Service Directors, because some im-portant allocation decisions seemed to rest moreon judgment than on explicit criteria. Recent evi-dence suggests that the VA has not restructuredits allocation process to address this problem.

73
The VA recently decided to purchase a nuclearmagnetic resonance (NMR) unit, which is one ofthe newest advances in medical imaging and diag-nosis, and which some experts believe may assumemany of the present functions of the CT scanner.As the clinical potential of this new scanning tech-nique becomes better understood, many VA med-ical centers may want to procure their own units.NMR is an expensive technology, however, cost-ing $1 million or more for the machine alone andnecessitating facility modifications that may costan additional $1 million (84). Because of its cost,policymakers have urged a thorough assessmentof its health benefits before widely using it.
The VA Central Office decided to purchase anNMR unit early in 1983. On the recommendationof the Director of Nuclear Medicine, the ChiefMedical Director chose to place this unit at theSt. Louis VA Medical Center. This particular VAfacility was chosen because it represented, in theService Director’s judgment, the best mix of sup-port equipment, staff, and physical location (81).
The decision to place the NMR unit at the St.Louis VA medical center may have been correct,but the NMR decision process has been questionedby observers both within the VA and elsewhere.Explicit criteria for choosing a location were neverdeveloped, nor was an expert advisory groupformed, nor were protocols developed for an ob-jective evaluation of VA needs.
Early in the adoption process, the VA MedicalResearch Service proposed a strategy to introduceNMR into the VA system: a solicitation of all in-terested VA medical centers to submit proposalsfor an NMR center. These proposals would beevaluated by an ad hoc advisory committee, andtheir recommendations forwarded to the ChiefMedical Director for review and action. Impor-tantly, the review would include studies of the costeffectiveness of NMR compared to more conven-tional imaging devices (35).
The proposed strategy, however, was not ini-tially considered by the office of the Chief Medi-cal Director. Only in November 1983, after thefirst NMR unit was being placed in St. Louis, didthe office of the Chief Medical Director begin toimplement such a strategy. The VA’s apparentlack of system in decisions about new technology
raises serious concerns about VA resource alloca-tion. Because of NMR’s clinical potential and be-cause of its high costs, NMR is an important testof VA policy. At this time, though, it would ap-pear that the VA has not developed a wise poli-cy for acquiring major medical devices, such asNMR.
Future Acquisition Issues
The VA must continually confront issues aboutmany new devices and other technologies such asNIvIR, assess their need, demand, and relative val-ue, and make decisions about their purchase anduse. This chapter has discussed the VA’s currentrelated policies and programs. There is some evi-dence, however, that VA methods of acquiringdevices and other technologies may be in tran-sition.
An internal VA study examined the relation-ship between technology needs and MEDIPP (15).An earlier section of this chapter examinedMEDIPP as a framework for VA planning anddiscussed its usefulness in identifying VA needsfor major medical equipment. In MEDIPP’s firstyear, ending in November 1982, 28 district planswere analyzed, and two significant findingsemerged regarding device adoption and use. Thefirst was that, in addition to traditional routingrequests, VA districts are unexpectedly usingMEDIPP to request the purchase of controlleditem equipment. There were specific requests forover 40 major equipment items, including sevenCT and six NMR scanners, six cardiac catheteriza-tion items, two computerized electrocardiographydevices, and digital subtraction angiographyequipment. Some districts requested major equip-ment items through both traditional Central Of-fice channels and MEDIPP. Other districts madeno major equipment requests through MEDIPP.
The second finding was that MEDIPP identifiedabout 50 VA-wide issues for future health caredelivery. Of those 50, the acquisition of devices(and the larger issue of medical technology) wasamong the four considered most important.5 VAadministrators and planners believed that both
‘The other issues were (in order) bed levels, geriatric care, anddata validity (good recordkeeping).

74
immediate and secondary impacts of technologyacquisition are crucial in planning and resourceallocation.
The findings from the first MEDIPP cycle con-firm the potential utility of MEDIPP, not only inplanning but also in tracking major equipmentadoption and use. As new equipment requests aremade through medical district plans, a good eval-uation program could guide technologies’ diffu-sion within the VA (15).
One evaluation that might be effective is tech-nology assessment, or comprehensive technologyassessment, as it is sometimes called. This formof policy analysis provides information on the ef-fects of a device or other technology, includingsocial, ethical, political, economic, and technicaleffects. Technology assessment uses various meth-ods and draws on many disciplines. It takes sev-eral important factors into account: 1) unintendedand unanticipated impacts of technological appli-
cations; 2) indirect effects; and 3) the distributionof costs, benefits, and other effects among all in-terested parties.
Technology assessment has not been used veryextensively in the VA health care system. In June1983, however, the Chief Medical Director of theVA formed a High Technology AssessmentGroup, which will “determine what course the VAshould follow with respect to acquisition of ma-jor new technology in the future” (84). As the VAfaces changing health care delivery needs and sta-ble or declining health care budgets, some ana-lytical method is needed to address more compre-hensively the many factors involved in adoptingand using costly equipment. Appropriate evalua-tion methods are probably needed for severalkinds of VA users, from technicians to Service Di-rectors. Such an effort might be very useful to theVA in allocating health care resources more effi-ciently and equitably.
Appendixes

Appendix Am —Acknowledgments andHealth Program Advisory Committee
In addition to the advisory panel, this technical memorandum has benefited from the advice and reviewof experts in rehabilitation, veterans’ affairs, and health policy. The staff would like to express its appreciationto the following people for their valuable guidance. -
L. W. Ashton, General Electric Medical Systems,Washington, DC
Peter W. Axelson, Veterans Administration, PaloAlto, CA
H. V. Tino Ballenca, Mennen Medical, Inc.,Buffalo, NY
Chester G. Bazel, Veterans Administration,Washington, DC
Taylor Benson, Marquette Electronics, Marquette,WI
Henry Bergman, Public Citizen Health ResearchGroup, Washington, DC
Steve Bialys, Veterans Administration, Hines, ILJay C. Bisgood, Department of Defense,
Washington, DCRonald A. Blackwood, Honeywell Medical
Electronics, Pleasantville, NYHal Booker, Veterans Administration, Washington,
DCJack Breslar, Veterans Administration,
Washington, DCErnest M. Burgess, Prosthetics Research Study,
Seattle, WAGene D. Burton, Hospital Corp. of America,
Nashville, TNWilliam T. Butler, Baylor College of Medicine,
Houston, TXRichard Cole, Extracorporeal Co., King of Prussia,
PAClyde C. Cook, Veterans Administration,
Washington, DCFrank Coombs, Veterans Administration,
Washington, DCJohn A. D. Cooper, Association of American
Medical Colleges, Washington, DCWarren B. Cozzens, Marquette Electronics, Inc.,
Marquette, WIMarco Cucinella, Spacelabs, Inc., Chatsworth, CAJack Cumming, Xonics Corp., Chicago, ILDonald Custis, Veterans Administration,
Washington, DCRoger D. Daniro, General Services Administration,
Washington, DCRichard diMonda, American Hospital Association,
Chicago, IL
Fred Downs, Veterans Administration,Washington, DC
Frank B. Engel, CGR Corp., Baltimore, MDCarlton C. Evans, Veterans Administration,
Washington, DCElbert O. Garner, Hospital Corp. of America,
Nashville, TNMargaret Giannini, Veterans Administration,
Washington, DCPeter G. Goldschmidt, Veterans Administration,
Washington, DCDavid German, Disabled American Veterans,
Washington, DCRichard J. Greene, Veterans Administration,
Washington, DCRobert Hart, Technicare Corp., Solon, OHVince Hlinovsky, Paralyzed Veterans of America,
Washington, DCJessie Holder, Veterans Administration, Hines, ILRalf Hotchkiss, Washington, DCC. Richard Hullihen, Picker International, Solon,
OHHenry Humphreys, Veterans Administration,
Washington, DCFrederico Juarbe, Veterans of Foreign Wars of the
United States, Washington, DCRichard Kaiser, Veterans Administration, Hines, ILW. B. King, Philips Medical Systems, Inc.,
Springfield, VARodney S. Kirk, The American Legion,
Washington, DCThomas Kodl, Veterans Administration, Hines, ILBarbara Kolledge, Veterans Administration, New
York, NYKenneth Kreitner, Veterans Administration, Palo
Alto, CALawrence Liefer, Veterans Administration, Palo
Alto, CAJames Lykins, Veterans Administration, Hines, ILGabriel Manasse, Veterans Administration,
Tucson, AZAlIan C. Martin, Technicare Ultrasound, Rolling
Meadows, ILVernon McKenzie, Department of Defense,
Washington, DC
77
25-289 0 - 85 - 7

78
Matthew F. McNulty, Jr., The Medical Center,Georgetown University, Washington, DC
L. L. Mitchell, General Services Administration,Washington, DC
Frank A. Morrone, Jr., Veterans Administration,Washington, DC
Lyle Mussman, Advanced TechnologyLaboratories, Bellevue, WA
Robert Nolan, Veterans Administration,Washington, DC
Foster Palmer, Veterans Administration, Hines, ILDavid J. Passamaneck, AMVETS, Washington,
DCLynn Phillips, Paralyzed Veterans of America,
Washington, DCAlbert Press, Cobe Laboratories, Denver, COBarbara J. Pryor, Washington, DCEdward M. Pugh, Picker International, Falls
Church, VARichard M. Ryan, Jr., Medical Advisory Group
International, Winchester, MA
Sam Serritelli, Veterans Administration, Hines, ILJames Smith, Veterans Administration,
Washington, DCJohn F. Sommer, Jr., The American Legion,
Washington, DCJohn Stuart, Veterans Administration, Hines, ILFred Stuvek, Jr., Siemens Medical Systems, Inc.,
Iselin, NJWilliam Sullivan, Diasonics, Milpitas, CAMark Tauscher, Hewlett-Packard Co., Rockville,
MDWilliam W. Thompson, Blinded Veterans
Association, Washington, DCRobert Teidt, Mennen Medical, Inc., Buffalo, NYNoel Woosley, AMVETS, Washington, DCDonald Wright, Veterans Administration, New
York, NYDennis Wyant, Veterans Administration,
Washington, DC
HEALTH PROGRAM ADVISORY COMMITTEE
Sidney S. Lee, Committee ChairPresident, Milbank Memorial Fund
New York, NY
Stuart H. A1tman*DeanFlorence Heller SchoolBrandeis UniversityWaltham, MAH. David BantaDeputy DirectorPan American Health OrganizationWashington, DCCarroll L. Estes**ChairDepartment of Social and Behavioral SciencesSchool of NursingUniversity of California, San FranciscoSan Francisco, CARashi FeinProfessorDepartment of Social Medicine and Health PolicyHarvard Medical SchoolBoston, MA
“Until April 1983.● *Until March 1984.
Harvey V, FinebergDeanSchool of Public HealthHarvard UniversityBoston, MAMelvin A. Glasser***DirectorHealth Security Action CouncilCommittee for National Health InsuranceWashington, DCPatricia KingProfessorGeorgetown Law CenterWashington, DCJoyce C. LashofDeanSchool of Public HealthUniversity of California, BerkeleyBerkeley, CA
——● **Until October 1983.
79
Alexander LeafProfessor of MedicineHarvard Medical SchoolMassachusetts General HospitalBoston, MAMargaret Mahoney*PresidentThe Commonwealth FundNew York,NYFrederick MostellerProfessor and ChairDepartment of Health Po!icy and ManagementSchool of Public HealthHarvard UniversityBoston, MANorton NelsonProfessorDepartment of Environmental MedicineNew York University Medical SchoolNew York, NYRobert OseasohnAssociate DeanUniversity of Texas, San AntonioSan Antonio, TXNora PioreSenior AdvisorThe Commonwealth FundNew York, NYMitchell Rabkin**PresidentBeth Israel HospitalBoston, MA
Dorothy P. RiceRegents LecturerDepartment of Social and Behavioral SciencesSchool of NursingUniversity of California, San FranciscoSan Francisco, CARichard K. RiegelmanAssociate ProfessorGeorge Washington UniversitySchool of MedicineWashington, DCWalter L. RobbVice President and General ManagerMedical Systems OperationsGeneral Electric Co.Milwaukee, WIFrederick C. RobbinsPresidentInstitute of MedicineWashington, DCRosemary StevensProfessorDepartment of History and Sociology of ScienceUniversity of PennsylvaniaPhiladelphia, PA
● Until August 1983.● *Until April 1983.

— — —
Appendix B.— Medical Devices andthe Veterans Administration: The Perspective
of Veterans’ Service Organizations
There have been veterans’ service organizations inthis country since before the Declaration of Independ-ence. The first, the Society of the Cincinnati, wasformed during the Revolutionary War. Today thereis no accurate record of all the veterans’ organizationsin this country (89). They range from small groups inisolated areas to large organizations that play a rolein forming national policy. Most of the organizationsperform two kinds of services for veterans. They helpindividual veterans obtain Federal benefits and serv-ices and provide their own services to veterans. Fortheir members as a group, they represent veterans’ con-cerns before legislative bodies.l
The six veterans’ organizations discussed here areactive nationally. They all work closely with the Vet-erans Administration (VA) while providing services,monitoring the VA’s activities, and suggesting im-provements in VA operations. OTA conducted an in-formal survey of these organizations’ relationshipswith the VA by talking with their representatives.Views were sought on the VA’s responsiveness to vet-erans’ health care needs and the strengths and weak-nesses of current VA programs, particularly with re-gard to prosthetics and rehabilitative devices. Each ofthe six organizations consulted is briefly describedalong with their viewpoints, with emphasis on prob-lem areas and suggested improvements, Note that theseorganizations represent only one perspective on theissues. Their views should be considered keeping inmind that they are consumers of VA health care andtherefore not impartial observers.
Paralyzed Veterans of America
The Paralyzed Veterans of America (PVA) is a na-tional, nonprofit service organization for paralyzedveterans, founded in 1946 and chartered by Congressin 1971. 2 With 11,000 members and 36 chaptersthroughout the United States, Puerto Rico, and Mex-ico, PVA is the largest advocate for 25,000 paralyzedAmerican veterans. Although membership is limitedto veterans who have spinal cord injury or disease and
‘It is estimated that betweens million and 5 million, out of almost 30 mil-lion, veterans in the United States belong to veterans’ organizations. It is dif-ficult to establish a more precise figure because many, and in fact, probablymost veterans who do belong to an organization belong to more than one (i’o).
2A congressional charter essentially lends prestige to an organization; thereare no legal benefits of a congressional charter.
an honorable discharge (injury may or may not haveoccurred during military service), PVA also works asan advocate for the other 175,000 nonveteran para-lyzed Americans, as well as all U.S. veterans (71).PVA’S emphasis is on improved medical treatment andrehabilitation for all those with spinal cord injuries.
PVA was involved in the VA establishment of SpinalCord Injury Centers in the late 1940s to treat spinalcord injuries and diseases. There are now 19 SpinalCord Injury Centers across the country, with PVA rep-resentatives in each (39).
PVA is also concerned with meeting the posthospi-talization needs of both paralyzed veterans and otherparalyzed Americans, including accessible housing,specialized transportation, high-quality education, andprosthetic aids for more independent living. PVA’Sactivities are organized around four major programs,for national service, advocacy, legislation, and re-search.
The national service program operates 46 regionalservice offices, corresponding to regional facilities ofthe VA, staffed by national service officers trained toadvise veterans and their dependents on their needs,legal benefits, health care (including prosthetics, medi-cation, and rehabilitation), education, housing, andother VA benefits. National service officers also mon-itor the activities of the VA medical centers in theirjurisdictions, including the appearance, condition, andmaintenance of the facility; the adequacy and avail-ability of medical equipment; personnel training, reten-tion, and levels; prosthetic availability, fitting, and dis-tribution policies; outpatient treatment and admissionprocedures; and the hospital administration’s long-range plans and goals (68).
PVA’S advocacy program is committed to eliminat-ing barriers to disabled people in housing, transpor-tation, employment, education, and rehabilitation.The advocacy department has represented PVA’S posi-tions on numerous committees, both public and pri-vate, and has participated in several lawsuits, as afriend of the court and as a litigant.
The PVA legislative program considers how changesin laws affect disabled veterans and other handicappedpersons and encourages the Government to protectand expand veterans’ benefits. PVA monitors and ad-vocates legislation both federally and locally, andtestifies at legislative and administrative hearings.
The PVA research program explores ways to im-prove the care, treatment, and rehabilitation of spinal-
80

81
cord-injured people and promotes the search for a curefor spinal cord injury. PVA is the largest private sup-porter of central nervous system research in the UnitedStates (68). Through the Technology and ResearchFoundation,. established in 1975, PVA awards researchgrants and fellowships for research related to spinalcord injury, including basic and applied medical re-search and research on rehabilitation methods andaids. PVA itself conducts demographic and statisticalstudies to clarify problems related to spinal cord in-juries (71).
Disabled American Veterans
After World War I, some disabled veterans formedlocal self-help groups that eventually became theDisabled American Veterans (DAV), a national non-profit association established in 1920 and chartered byCongress in 1932. The founders of DAV worked withother organizations toward the legislation for a cen-tral Government agency to handle veterans’ affairs—the Veterans Bureau, forerunner of today’s VeteransAdministration, DAV now has 818,000 members anda nationwide network of service programs, in addi-tion to a Vietnam veterans outreach program, a na-tional legislative program, and a national employmentprogram.3 DAV places special emphasis on meetingthe needs of Vietnam veterans. Approximately 25 per-cent of DAV’S members are veterans of the VietnamWar period and Vietnam veterans represent 95 per-cent of the professional staff, both at DAV’S nationalheadquarters and in the field.
DAV’S national service program operates much thesame as does PVA’S corresponding program, with ap-proximately 250 national service officers in 68 officesacross the United States, who provide free counselingand claims representation for disabled veterans andtheir families. In addition, since 1973 DAV has sentField Service Units to rural and suburban areas to serveveterans and families living too far from DAV offices.All DAV national service officers are disabled veteranswith service-connected, wartime disabilities who func-tion as attorneys-in-fact, representing veterans beforethe Veterans Administration, the Social SecurityAdministration, the Labor Department, and other Fed-eral and State agencies. They provide counseling ondisability benefits, rehabilitation programs, and otheravailable services, and help in preparing claims andassembling evidence to support claims.
DAV also provides a Disaster Fund (for disabled vet-erans needing help because of natural disasters), an
Emergency Relief Fund (for disabled veterans facingfinancial emergencies), and a Scholarship Fund (forchildren of needy disabled veterans). These programsare available only to veterans with service-connecteddisabilities, although one need not be a DAV memberto apply.
DAV’S national legislative program monitors andadvocates legislation affecting benefits for disabled vet-erans and their families, including disability compen-sation, health care, employment, vocational rehabili-tation, and death benefits. DAV also advocates archi-tecture designed for handicapped people. Like PVA’Sadvocacy and legislative programs, this DAV programis active at local, State, and national levels.
Through its national employment program, DAVhelps disabled veterans find jobs, supports local em-ployment programs, helps employers and local gov-ernment officials place disabled veterans in jobs andjob programs, and files job discrimination complaintson behalf of disabled veterans. DAV works closelywith the National Alliance of Business, the President’sCommittee on Employment of the Handicapped, andother private and public organizations concerned withcreating equal employment opportunities for handi-capped people.
Veterans of Foreign Wars of theUnited States
The Veterans of Foreign Wars of the United States(VFW) is the Nation’s oldest existing veterans’ serviceorganization, and one of its largest. It originated fromthe veterans’ groups formed in the early 1900s by vet-erans of the Spanish American War, the Philippine In-surrection of 1899, and the China Relief Expedition of1900. Several of these early groups eventually bandedtogether to form a new organization, which in 1914became the VFW.4 Since 1914, the VFW has workedfor compensation, pension, hospital, and bonus ben-efits for World War I veterans; the GI Bill of Rightsfor veterans of World War 11, Korea, and Vietnam;and other major laws providing benefits to veterans.
The VFW now has nearly 2 million members; in thepast 15 years membership has increased by more than250,000. Membership in the VFW is open to any U.S.citizen who has served honorably in any overseasengagement for which a campaign medal or ribbonwas awarded by the U.S. Government. The VFW hasnearly 10,000 posts (local chapters), in the UnitedStates, Germany, Thailand, Korea, Japan, France, andother countries (45).
‘To qualify for membership in DAV, an honorably discharged veteran musthave a disability incurred in wartime military service or under conditionssimilar to war (23).
4The VFW, however, recognizes its founding year as 1899, when the firstof the organizations that would become the VFW was formed.

82
VFW operates a nationwide service network likethose of PVA and DAV to aid all veterans and theirfamilies (regardless of whether they are VFW mem-bers) in filing claims for benefits. It also promotes leg-islation for veterans’ rights and benefits and nationalsecurity, and sponsors community activities, includingprograms aimed at stimulating patriotism and an ap-preciation of national heritage.
The American Legion
The American Legion is the largest veterans’ orga-nization in the United States. It was born at a caucusof the first American Expeditionary Force in 1919 inParis, with the goal of building an association of vet-erans “whose primary devotion was to God and Coun-try” (89). The American Legion now has about 2.5 mil-lion members, of whom about 25 percent are Vietnamveterans. s Its Auxiliary boasts an additional 1 millionmembers (89). The American Legion has seven pro-grams that have remained essentially unchanged sincethe organization’s beginnings. The programs are forveterans’ affairs and rehabilitation, children andyouth, Americanism, national security, foreign rela-tions, legislation, and economics.
The American Legion’s main concern has alwaysbeen the “welfare of veterans and their families.” Itsprograms for veterans’ affairs and rehabilitation,children and youth, and economics are all intendedto serve veterans and their families in various ways. b
Its other programs—except for those of the LegislativeDivision,7 which promotes issues of interest to theorganization (including veterans’ rights and bene-fits)—do not directly benefit veterans. Rather, theyfurther the organization’s ideals of patriotism and goodcitizenship, and advocate its views on national secu-rity and foreign policy.
Through its veterans’ affairs and rehabilitation pro-gram, The American Legion operates a nationwide net-work of 16,000 service officers who provide help inpreparing and filing claims for VA benefits (like theservice networks of other veterans’ organizations).This program also offers advice and representation incases before the VA’s Board of Veterans Appeals and
‘Any honorably discharged veteran who served in World War I (Apr. 6,1917, to Nov. II, 1918), World War 11 (Dec. 7, 1941, to Dec. 31, 1946), theKorean War (June 25, 1950, to Jan. 31, 1955) or the Vietnam War (Dec. 22,1%1, to May 7, 1975) is eligible for membership in The American Legion.
6Although the objectives of the program for children and youth have grownto include improved social and economic conditions for all children, theoriginal purpose of this program was to ensure the well-being of the chih-lrenof deceased and disabled veterans.
The Legislative Division is the lobbying arm of The American Legion. Al-though other issues also get vigorous support from this division, legislationfor veterans’ benefits specifically and the economic well-being of veteransgenerally is given priority attention.
the Department of Defense Boards for discharge re-view, and in correcting military records. These serv-ices are provided free, regardless of whether the vet-eran is a member of The American Legion. In addition,the program employs six field representatives whoregularly conduct onsite visits in the VA’s 172-hospitalsystem, much like PVA’S hospital monitoring (82).
American Veterans of World War 11,Korea, and Vietnam
The American Veterans of World War II, Korea,and Vietnam (AMVETS) was founded in 1944 andchartered by Congress in 1947. Although AMVETSwas originally formed for veterans of World War 11,in 1966 its charter was amended to include veteransof the Korean War and Vietnam. AMVETS now hasabout 200,000 members, of whom about a third areVietnam veterans.8
AMVETS’ goals and services are very similar tothose of The American Legion and the VFW. As a serv-ice organization, AMVETS’ primary commitment isto serving veterans and their families. Its service of-ficers are stationed at VA regional offices and medi-cal facilities in every State. These service officers aretrained professionals who offer counseling and repre-sentation to all veterans and help them obtain thebenefits to which they are entitled, including compen-sation, education, employment, hospitalization, andrehabilitation (162). AMVETS also participates in theVA’s Voluntary Service Program (as do some otherveterans’ organizations), whose volunteer workersprovide services for hospitalized veterans.
AMVETS also provides many community servicessuch as drug abuse education programs, voter registra-tion drives, programs to promote safe driving habits,and a college scholarship program for needy children.Some of AMVETS’ community service projects arealso intended to encourage patriotism, such as the Na-tional Americanism Essay Project it sponsors, and theAMVETS Memorial Carillons in national cemeteriesand at historic sites throughout the United States.
Blinded Veterans Association
The Blinded Veterans Association (BVA) is a non-profit organization founded in 1945 by a group of vet-
5Membership in AMVETS is open to any honorably discharged Americanveteran who actively served in the Armed Forces between Sept. 16, 1940,and May 7, 1975. Those who entered the service for the first time on or afterMay 8, 197s, are not now eligible for AMVET membership, but legislationis pending to open AMVETS membership to all honorably discharged vet-erans who served in the Armed Forces from May 7, 197s, to an indefinitefuture date.

83
erans blinded in World War II. BVA was incorporatedin 1947 and in 1958 was granted a congressional char-ter. Almost 5,000 of the nearly 50,000 blind veteransin this country belong to BVA.9 Some of these blindveterans also have other disabilities such as a hearingloss or missing limbs.
BVA operates much like the other veterans’ organi-zations by providing help to individuals through a na-tionwide service network and by representing the in-terests of blind veterans in promoting legislation. BVAhas two major service programs, the Field Service Pro-gram and the Outreach Employment Program. Bothare provided under contracts with the Federal Gov-ernment: the Field Service Program under contractwith the VA and the Outreach Employment Programunder contract with the Department of Labor. Thereare 37 BVA regional groups that provide help at Stateand local levels.
BVA’S Field Service Program is unique in that blindveterans are actually sought out by the field represent-atives and offered help. BVA obtains the names ofblind veterans from the VA and hospital records andthrough word of mouth. A field representative thenvisits the veteran and encourages him or her to seekwhatever assistance is appropriate. The programemploys 10 field representatives, all blind veteransthemselves, who help blind veterans in obtaining ben-efits, including disability compensation or pension, re-habilitation and vocational training, and prostheticequipment and training in its use. The representativesalso counsel the veteran’s family and help them to takeadvantage of existing community programs. This pro-gram serves as an adjunct to the VA’s 76 Visual Im-pairment Service Teams at VA medical centers, whoare responsible for reaching as many blind veteransas possible to provide them physical examinations andrehabilitation (91).
The Outreach Employment Program makes use ofregional employment representatives who help blindveterans by finding prospective employers, providingadvice on resumes and job applications, keeping theveterans informed of potential job opportunities, andoffering counseling in cases of job discrimination. Theprogram also tries to convince employers, throughpublic service advertising and directly, to hire blindveterans.
Observations on the VeteransAdministration Health CareDelivery System
The veterans’ service organizations interviewed forthis appendix believe that the Veterans Administrationis doing a more than adequate job of tending to thehealth care needs of veterans in the United States.Some problems were noted, although in many casesefforts are already being made to alleviate them. Com-ments on specific VA departments follow.
Rehabilitation Research and Development Service
The VA’s Rehabilitation Research and DevelopmentService (Rehabilitation R&D) is primarily responsiblefor the research, development, and evaluation of newdevices, techniques, and concepts in rehabilitation.’”Such activities generally focus on the three most prev-alent service-connected disabilities of veterans: pros-thetic aids for amputees, especially lower-limb pros-thetics (which represents about 40 percent of theService’s budget); aids for veterans with spinal cordinjuries, with special emphasis on wheelchairs (repre-senting about 30 percent of the budget); and sensoryaids, including aids for the visually impaired (repre-senting about 30 percent of the budget)(5). Althoughthe dollar amount allocated to Rehabilitation R&Drose 40 percent from fiscal year 1982 to fiscal year 1983(a $2.9-million increase), this Service receives only 6.4percent of the VA research and development budget(see table 2 in ch.3).
PVA, DAV, and BVA all feel that greater fundingshould be provided for research sponsored byRehabilitation R&D. However, they disagree on whichareas should be emphasized. PVA would like to seemore R&D conducted on aids for spinal-cord-injuredveterans, DAV on prosthetics, and BVA on sensoryaids for the blind (33,39,161).
All the organizations noted that positive changeshave been made in the last few years, such as increasedfunding for Rehabilitation R&D and greater partici-pation of veterans’ organizations in setting researchpriorities. The VA recently held three informal sessionsto discuss research priorities in upper- and lower-limbprosthetics, speech pathology, audiology and aids forhearing-impaired veterans, and functional electricalstimulation. Nearly 50 people from across the coun-
‘Membership in BVA is open to all veterans with service-connected blind-ness. Blinded veterans with non-service-connected blindness are eligible forassociate membership.
1ORehabilitation R&D and other VA programs for research and develop-ment are discussed in ch. 3 of this technical memorandum. The testing andevaluation of devices is carried out by the VA Prosthetics Center in New YorkCity and the VA Marketing Center in Hines, Illinois (see also ch. 4).

84
try participated in each session, including experts inthe relevant fields, VA representatives, physicians, de-vice manufacturers, and representatives of all the ma-jor veterans’ organizations.
PVA, DAV, BVA, AMVETS, and The AmericanLegion are also represented on the VA RehabilitationR&D merit review panel, which recommends researchpriorities and reviews research proposals and results.
Prosthetics and Sensory Aids Service
The Prosthetics and Sensory Aids Service (PSAS)is generally responsible for providing eligible veteranswith the prosthetic and rehabilitative devices and sen-sory aids that they need for independent living. PSASis also involved with the research, development,testing, and evaluation of commercial devices, as wellas procurement and supply. Veterans’ organizationscommended the VA for increasing the size of PSASstaff, for recognizing the need for training VA fieldrepresentatives and developing a comprehensive train-ing program, and for encouraging more involvementwith veterans’ organizations. Some of these initiativeshave already produced results, others will require moretime.
Several veterans’ organizations noted that some ofthe information available on benefits is not accurate.Inadequate training of field representatives is not themain reason for this, however, but rather that thePSAS Program Operating Manual requires much revi-sion. The manual, which describes the process of is-suing devices, including eligibility requirements andverification of eligibility, has not been revised since1956. The field representatives’ reliance on an incom-plete and outdated manual resulted in the inconsistentapplication of national policy and arbitrariness in therepresentatives’ interpretation of rules. The manual isnow being revised, with help from all major veterans’organizations.
The most frequent complaint about PSAS concernsthe long delays in providing prosthetic and rehabili-tative devices to veterans. All the organizations inter-viewed gave examples of unacceptable delays betweenthe order and actual delivery of devices. For example,a cane was delivered only after several months anda custom-designed wheelchair only after a year. Longdelays for repairs were also noted, such as hearing aidand eyeglass repairs that took up to 5 weeks. Thesedelays are primarily attributed to the fact that allorders must go through the Office of Procurement andSupply’s Prosthetics Distribution Center in Denver,Colorado,
It is possible that a decentralized distribution sys-tem would be more effective. The VA considers it morecost effective to stock large quantities of devices at one
center. However, a complete analysis should take intoaccount inventory costs, the costs of paperwork in-volved in placing orders, and the time that disabledveterans spend without devices essential to their every-day activities. The veterans’ organizations suggestedthat PSAS have greater flexibility to contract with localsuppliers in distributing devices. The VA Office of In-spector General audited the Prosthetics DistributionCenter in 1983 (138) and made recommendations toimprove the efficiency and economy of the distribu-tion and repair functions of the Prosthetics Distribu-tion Center. However, the recommended changes mustbe negotiated with the Department of Medicine andSurgery before taking action.
The VA Prosthetics Center
The VA Prosthetics Center (VAPC) has been widelyviewed by veterans’ groups as having serious organiza-tional problems, largely because of its autonomy .11VAPC now has direct line authority through PSAS,which could help solve some of these problems.VAPC’S original goals were to conduct research anddevelopment in rehabilitation engineering, to evaluateand test commercially available assistive devices, toprovide direct patient care for difficult prosthetic andorthopedic cases (i. e., customized devices), and tomanufacture and distribute orthopedic footwear andprosthetic and orthotic devices. These are still VAPC’Sresponsibilities, with the exception of R&D, but therehave been problems with VAPC’S providing direct pa-tient care.
VAPC Special Clinic Teams were intended to pro-vide expert fitting and construction of prostheses forthe most difficult prosthetic cases.lz People from acrossthe Nation were to be sent to VAPC when they neededspecial treatment. According to DAV, however, thisprogram has not been successfully implemented. In ad-dition, plans to introduce five additional Special ClinicTeams in other hospitals across the country have beenlate in implementation. These additional teams wereto be trained and in place by October 1984. Instead,as of November 1984, seven teams have been iden-tified, but the teams are not complete and more train-ing is needed, The new target date is March 1985 (13).
The Chief Medical Director proposed that VAPC’Sspecial patient care services be moved in January 1983from present facilities in New York City to theManhattan VA Medical Center, on the expectationthat a hospital setting would be more conducive to di-rect patient care. DAV has questioned the proposed
IIVApC is dixusxd in chs, 3 and a.]zSPwial C]inic Teams are discussed in ch. B.

85
location on the grounds that it may not be accessibleto handicapped veterans. The proposal to move VAPCis still being discussed and Congress must be notifiedprior to any action (13,164).
Along with other VA departments, VAPC has alsobeen involved with setting standards and evaluatingcommercially available devices. Prosthetic aids, wheel-chairs, and aids for blind and hearing-impaired vet-erans are all produced mostly by private manufac-turers and provided to the VA through contracts.Many commercially manufactured devices are evalu-ated to ensure that they meet VA standards prior tothe VA’s adopting them for use. PVA and DAV in-dicated, however, that some new products are con-strained by the VA’s more specific standards.
As far as the VA’s evaluation is concerned, PVA,DAV, and 13VA all mentioned that inefficiencies in thesystem result in delays, and that the device needs ofveterans are not always met because of inconsistentand restrictive policies and standards. PSAS initiatedthe Prosthetic Technology Evaluation Committee inearly 1982 to address problems in VA evaluations, 13PVA and DAV have permanent representatives on thiscommittee, which is responsible “for assessing andranking the legitimacy and appropriateness of evalua-tion proposals and for assessing and approving theresults of clinical evaluations. ” Other veterans’ orga-nizations are kept informed of the committee’s activi-ties and invited to participate in its meetings. All theorganizations feel that the committee is a first step inthe right direction, that improvements are already evi-dent, and that further progress will take time, but canbe expected.
Summary and Conclusions
Although the veterans’ organizations discussed herehave different eligibility requirements, different degrees
IJThe prosthetics Techno]on Evaluation Committee is discussed in ch. Q.
of involvement in political issues, and different pro-grams for veterans, all of the organizations emphasizethe needs of their particular members, and these needsare often those of all veterans.
The delivery of high-quality rehabilitation servicesand medical care, including prosthetic and rehabili-tative devices, is a main concern of these organizations.All have representatives in place at some, if not all,VA medical facilities. These representatives functionlike consumer representatives for the VA, determin-ing the needs of veterans, assessing their eligibility forVA benefits, and helping them obtain the benefits. Inaddition, representatives of some organizations mon-itor the activities of VA health care facilities to pro-mote high-quality care.
Since veterans’ service organizations are so closelyinvolved in the VA’s delivery of health care, both asparticipants and observers, their perceptions of VAprograms are valuable. These organizations generallyfeel that they have an excellent working relationshipwith the VA. Although there are still problems, theview of these organizations seems to be that the VAis increasing efforts to involve veterans’ groups in plan-ning and policy decisions and to respond to the groups’concerns. All these organizations meet regularly withthe VA, and some have representatives on various VApanels. In addition, informal meetings are held be-tween veterans’ organizations and the VA as issuesarise.
Not surprisingly, these organizations would like tosee greater Federal allotments to the VA, as well asgreater VA allotments to the programs serving theirmembers. Another consensus view is that there arelong delays in providing and repairing prosthetic andrehabilitative devices. Although a certain amount ofprocedure and delay has been expected because of thesize of the VA bureaucracy, improvements could bemade, Through cooperation and discussion betweenthe VA and veterans’ service organizations, progressis being made to improve these services as fundspermit.

Appendix C.— Veterans Administration Procurementand the Market for Medical Equipmentl
This appendix describes and analyzes the ways thatVeterans Administration (VA) procurement of medi-cal equipment affects and is affected by conditions ofdemand and supply in the markets for X-ray equip-ment, computed tomography (CT) scanning equip-ment, digital imaging equipment, nuclear diagnosticequipment, nuclear magnetic resonance (NMR) andpositron emission tomography (PET) scanning devices,ultrasound diagnostic equipment, patient monitoringand electroencephalograph (EEG) and electrocardi-ography (ECG) equipment, and hemodialysis equip-ment. The discussion encompasses the ways procure-ment policies of the VA affect the prices and productsthat are offered and the practices of private buyers.Manufacturers’ comments on VA procurement are alsosummarized.
This study is based on data available through theVA Marketing Center (VAMKC) about its procure-ment. Although important national market structuredata exist, most are available only in the form of 4-digit SIC codes, which are too broad a classificationfor the analysis here. 2 In fact, all types of equipmentexamined in this study fall within a single 4-digit SICcode, SIC 3693, electromedical and electrotherapeuticsequipment.
Some Bureau of Census data are available in thefiner 5-digit and 7-digit codes, but they suffer from sev-eral problems: First, data are withheld at these levelsbecause of Bureau requirements to maintain confiden-tiality of individual firms’ data; second, some impor-tant structural data are not reported at all at theselevels of analysis; and third, there begin to be severeproblems in the data reliability of plants that producemany products.
Private proprietary sources of data are not boundby the same confidentiality requirements as the Bu-reau of the Census, but they tend to be incomplete andare frequently inconsistent (3).
Because of VAMKC contractual reporting require-ments, however, the characteristics of specific equip-ment markets can be reconstructed, including infor-mation on product market concentration, marketshares of individual firms, and market share in-stability. (When findings are reported here, care hasbeen taken to ensure their confidentiality.) In addition,
IBased on a paper prepared for OTA by Ralph Bradburd (14).‘SIC codes are Standard Industrial Classification codes, which are used
by the Bureau of the Census of the Department of Commerce to classify prod-ucts for the Census of Manufactures, which provides the most comprehen-sive statistics on medical device industries (see IOS).
data gleaned from interviews with manufacturers’ rep-resentatives have been analyzed along with VAMKCdata for a fuller interpretation.
Diagnostic X= Ray Equipment
X-rays are a highly penetrating form of elec-tromagnetic radiation of much higher frequency thanvisible light. They are generated in evacuated glassbulbs called X-ray tubes that contain two electrodes,an anode and a cathode. High voltage applied betweenthe two electrodes causes electrons to flow from thecathode to the anode, and X-rays are produced as theelectrons strike the anode. Since substances vary intheir opacity to X-rays, X-rays that have passedthrough a body can provide information on its inter-nal structure (63). In standard radiography, X-rays thathave passed through the body strike a sensitivephotographic film, and the resulting picture reflects thestructures through which the X-rays have passed. Aconventional radiograph is effectively a shadowgraph,a projection of the X-ray absorption of a three-dimensional body onto a two-dimensional detector.(Standard X-rays are also called “projection X-rays.”)In fluoroscope, the detector is a fluorescent screenrather than photographic film. In modern fluoroscope,X-rays are detected by a phosphor surface next to thesurface of a photoemitter, to intensify the image. Thefinal image can be viewed directly or camera recorded.
Conventional radiography provides excellent spatialresolution but rather poor contrast resolution. In otherwords, objects of different opacity to X-rays than sur-rounding material are quite distinct in X-ray images,but it is difficult to discern even a large target objectif its opacity to X-rays does not differ significantlyfrom that of surrounding material. As a result, exceptin regions of low absorption, namely the chest, breast,and extremities, conventional radiography is unsuitedfor characterizing soft-tissue detail (75).
General Demand Characteristics
Supplies v. Equipment Costs.—Annual expenditureson X-ray film and other supplies depend on how muchX-ray equipment is used. In a large hospital, the an-nual cost of supplies can easily be as great as the pur-chase price of the equipment (21,25). X-ray film, filmdevelopment chemicals, and other supplies are typi-cally purchased independently of X-ray equipment.
Equipment Purchase Price. -X-ray equipment variesgreatly in price depending on its characteristics. A sim-
86

87
ple unit may cost as little as $30,000, while the equip-ment for a fully appointed procedures room may costwell over $1 million. Peripheral equipment is also re-quired, such as developing rooms, viewing equipment,and cabinets for storing X-ray photographs.
Servicing and Technical Support.—The need fortechnical support and servicing of X-ray equipment in-creases with its complexity. Sophisticated X-ray equip-ment may require up to 8 weeks for installation andcalibration (21). For annual service contracts, manu-facturers quoted costs ranging from 5 to 14 percentof equipment purchase costs. Servicing costs and“downtime” of equipment are both important con-siderations in purchasing, and service availability cansupport a VA hospital’s “brand name justification” forpurchasing equipment (which is explained below).
The VA Market: Demand and Supply
VA Demand.—VA X-ray equipment purchases arechanneled through the VAMKC’S Radiological andNuclear Equipment and Supplies Division. TheVAMKC negotiates annual contracts with vendors,and when VA medical centers (or other units that pur-chase through the VAMKC) are authorized to pur-chase X-ray equipment, the VAMKC places the order,arranges for direct delivery to the medical center, andadministers the contract (40).
X-ray equipment accounts for more direct deliverymedical equipment capital expenditures than any othersingle equipment category, and represents a substan-tial annual budget item. As a proportion of medicalequipment expenditures, those for X-ray equipmenthave been falling, representing 71 percent of total med-ical equipment expenditures other than through theFederal Supply Schedule (FSS) in 1979, 69.6 percentin 1980, 50.2 percent in 1981, and 46.9 percent in1982. 3 Yet the corresponding absolute dollar amountin 1982, over $59 million, was larger than that in anyof the previous 3 years (131,132).
The VAMKC manages direct delivery purchases ofX-ray equipment for a number of Government agen-cies other than the VA, including the Public HealthService. Even so, the VA accounted for 91.3 percentof VAMKC’S total direct delivery X-ray equipment ex-penditures in 1979, 78.2 percent in 1980, and 73.8 per-cent in 1981 (131).
VA Demand Relative to the National Market.—TheVAMKC appears to be a significant part of the na-
3The FSS program is administered by the Office of Federal Supply and Serv-ices of the General Services Administration. VAMKC is the commodity man-ager for this program’s Group 65, Medical, Dental, and Veterinary Equip-ment and Supplies. VAMKC establishes contracts with manufacturers of thisequipment under the policy guidance and procurement regulations of the Gen-eral Services Administration. (This arrangement is discussed further in ch. 5.)
tional market for X-ray equipment. The VAMKC re-quires that vendors disclose total annual sales of theequipment covered in their annual contracts. Althoughincomplete, the data made available to OTA by theVAMKC indicate that it purchases roughly 5 to 10 per-cent of the X-ray equipment of companies on annualcontract. Companies apparently vary in the propor-tion of the X-ray equipment sales they make throughthe VAMKC, for one company below 5 percent, foranother over 10 percent (132). For many, but not allcompanies, the VA is either their largest or one of theirlargest customers (4,21,25,48,86).
VAMKC Demand Variability .-Total expendituresfor X-ray equipment orders processed by the VAMKCare highly variable. From 1979 to 1980, they fell by35.6 percent, and from 1980 to 1981, they fell an ad-ditional 37.2 percent. Finally, from 1981 to 1982, theyrose by 297.6 percent. The variability of VA demandfor X-ray equipment was somewhat greater than thatof other agencies that purchase through the VAMKC.VA purchases fell by 44.9 percent from 1979 to 1980,and by 40.8 percent from 1980 to 1981 (131). (Avail-able data do not permit the calculation of the cor-responding 1981-82 percentage change. ) Such demandvariability is high compared with most American in-dustries (93). Its effect on the market will be discussedbelow.
Suppliers to the VA Market.—Many major manu-facturers of X-ray equipment have had VAMKC an-nual contracts in the past 3 years, including (in alpha-betical order) CGR Corp., General Electric Co.,General X-ray, H. G. Fischer, Orthopedic Equipment,Philips Medical Systems, Picker International, Ray-theon, Siemens Corp., and Xonics Medical Systems.However, this VAMKC market is relatively concen-trated: Four firms accounted for almost 95 percent ofsales to the VA in 1982 (132). In addition, if vendorsare ranked by sales volume for 1979 through 1982, thesame four firms are always found at the top, with nonemoving by more than one rank (131,132).
Taken alone, these data might indicate lack of com-petition in the market. However, further data analy-sis shows that, although rankings by market sharehave not changed much, the market shares themselveshave. In measuring market share changes, the great-est possible sum of the absolute values is 200. This isthe value resulting should the market change handscompletely, with every firm with any sales in the firstperiod having none in the second and other firms en-tirely capturing the market. Table C-1 shows the sig-nificant annual changes in market shares during thesample period.
There are several possible explanations of theobserved volatility in market shares. One is that the

88
Table C-l.—Sum of Absolute Values of AnnualPercentage Changes in Vendors’ VA Marketing Center
X-ray Equipment Market Shares, 1979-82
1979-80 1980-81 1981-82
Sum of absolute values. . . . . . 26.4 45.8 29.3As a percentage of maximum
possible value (200) ... , . . . 13.2 22.9 14.6SOURCES: U.S. Veterans Administration, Marketing Center, Radiological and
Nuclear Equipment and Supplies Division, unpublished data, Hines,IL, 1983; and U.S. Veterans Administration, Marketing Center, Radi-ological and Nuciear Equipment and Supplies Division, unpublishedinformation from vendors’ 1982 contracts, Hines, IL, 1983.
individual buyers of X-ray equipment prefer particu-lar companies’ products, and it happens that the pur-chase cycles of these buyers alternate to produce theobserved shifts. Although the data do not permit a testof this hypothesis, it seems unlikely. An alternative,and more likely, explanation is that the firms ag-gressively compete with each other in price or prod-uct performance, with the lead in either or both ofthese dimensions, and hence the market share, chang-ing hands from year to year.
CT Scanning Devices
CT scanners area form of X-ray equipment. As instandard radiography, X-rays are generated anddetected, and the attenuation of the X-rays as they passthrough the body provides information about thestructures through which they have passed.
In CT scanning, the X-ray beam is passed througha collimator (a device for producing a beam of paral-lel rays of light or other radiation) that forms the beaminto a thin fan in a plane perpendicular to the long axisof the body. On the other side of the body is an arrayof X-ray detectors. Each of these detectors producesa charge signal proportional to the X-ray energy it ab-sorbs. Signal strength is a function of the attenuationof the X-ray along the path between the detector ele-ment and the X-ray source.
To produce a cross-sectional image, depth informa-tion is obtained by rotating the source and detectorarray around the body axis while taking projectionsof the same section from several hundred differentangles. The data from each projection are “digitized”and processed. A series or “stack” of contiguous CTimages contains all the data necessary for construct-ing a variety of quasi-three-dimensional forms (75).
CT scanning devices help overcome two limitationsof standard X-ray equipment. First, they allow thediagnostician to obtain a view of a cross-section of thebody, as opposed to a projection that provides onlyinformation on the total accumulated attenuation ofthe X-ray beam as it passes from one side of the body
to the other. A tumor or lesion directly behind a boneas the body is viewed may not be detectable in a stand-ard X-ray. Also, standard X-ray equipment usuallycannot determine the depth of a tumor or lesion, buta cross-sectional view can. In addition, because thedetector absorption data are digitized and can be proc-essed, greater contrast resolution is possible (as ex-plained in the discussion of image data processorsbelow). CT scanners are extremely important in de-tecting tumors, in determining the optimal path for ra-diation therapy, and in other uses.
General Demand Characteristics
Supplies v. Equipment Costs.—Accurate data arenot available on the annual costs of supplies for CTscanners. However, because these scanners are muchmore expensive than standard X-ray equipment, andbecause they use digital image recording rather thanexpensive X-ray film, the cost of their supplies shouldbe smaller relative to equipment costs compared withstandard X-ray equipment.
Equipment Purchase Price.—The list price of a CTscanning device generally varies between $600,000 and$1,500,000 depending on its manufacturer and char-acteristics. These prices have begun to fall as the mar-ket has matured and the cost of data-processing com-ponents has fallen (40).
Servicing and Technical Support.—CT scanners areextremely sophisticated equipment and, to performproperly, must be very finely adjusted. (The VA hiresan outside consultant, a physicist, to inspect installedCT scanners.) As a result, both technical support andservicing are extremely important. One vendor quoteda price of $85,000 for the annual service contract ona CT scanner with a list price of about $1 million, orabout 8.5 percent of the equipment’s purchase price(4,25,42,86).
The VA Market: Demand and Supply
VA Demand.—CT scanning devices are purchasedthrough the VAMKC, rather than through the usualFSS, decentralized contracts, or direct delivery pro-grams (all described in ch. 5). Purchases of CT scan-ners must be approved by the VA Central Office inWashington, DC. The Central Office has ranked VAhospitals by their need for CT scanners. Funds for thescanners are budgeted in the VA Central Office andare provided centrally, not as usual through hospitalfunds. Purchases are delayed until a sufficient num-ber are possible, so a group purchase can be made withsignificant savings. The VAMKC then requests bidsfor equipment meeting its specifications.

89
In 1982 the VAMKC requested a bid for purchaseof 23 CT scanners, 21 for VA hospitals and 2 for theAir Force. The list price for the equipment of the win-ning bidder was $1,359,000 per unit; the VAMKC pro-cured the equipment at $917,730 per unit. An addi-tional $4.4 million worth of CT scanners were boughtin the same year from another company. In 1983, theVAMKC purchased 24 CT scanners through similarbidding. In that year, the list price for the equipmentpurchased was $1,383,500 per unit; the VAMKC pro-cured the equipment at $829,950 per unit (40).
CT scanners have accounted for a growing propor-tion of VAMKC-procured equipment costs. In 1979CT scanners represented 6.1 percent of non-FSS equip-ment expenditures; in 1980, 13.1 percent; and in 1981,28.2 percent. In 1982 CT scanners accounted for 20.2percent of total non-FSS equipment procurement, asomewhat smaller percentage than the year before, buta higher total dollar commitment, $25,512,122 com-pared to $8,386,270. Since 1980 CT scanners have ac-counted for more VAMKC procurement dollars thanany other category of equipment except X-ray equip-ment, with most of this CT equipment going to VAhospitals (table C-2). In 1983 VAMKC procurementof CT scanners totaled $19,918,800 (40,132).
VA Demand Relative to the National Market.—Asmentioned above, CT scanners have not been pur-chased through the usual VAMKC annual contracts.As a result, there is much less information to estimatethe relative importance of VA procurement in the na-tional market. According to a representative ofSiemens, the CT market is now about 600 units peryear (for all manufacturers), down from 750 per yeara few years ago (86). If this number is accurate,VAMKC procurement probably does not account formore than 4 to 5 percent of total national expenditureson CT equipment.
In this market, the VAMKC may also not be somemanufacturers’ largest account. Nonetheless, the totaldollar volume of VAMKC CT procurement—almost$20 million–may be high enough for VAMKC’S pro-
Table C-2.—Annual VA Marketing Center Procurementof CT Scanning Equipment, 1979.82
1979 1980 1981 1982
Total annual CTprocurement byVAMKC ($ millions) . . . $3.2 $4.5 $8.4 $25.5
VA proportion of totalVAMKC procurement . . 100°/0 20.70/o 88.40/o N.A.
SOURCES: U.S. Veterans Administration, Marketing Center, Radiological andNuclear Equipment and Supplies Division, unpublished data, Hines,IL, 1983; and U.S. Veterans Administration, Marketing Center, Radi.ological and Nuclear Equipment and Supplies Division, unpublishedinformation from vendors’ 1982 contracts, Hines, IL, 1983.
curement practices to influence manufacturers’ behav-ior, if not as much as in other markets.
VAMKC Demand Variability .—VAMKC procure-ment of CT scanning devices has fluctuated from yearto year, but much of this fluctuation seems moreappropriately characterized as growth rather than de-mand instability, certainly in the period from 1979 to1982. 111 any case, given that VAMKC procurementis a small fraction of the national market, a drop inVAMKC orders, such as available data indicated forfiscal year 1983 (from 25 to 24 scanners), is unlikelyto have an impact on manufacturers.
Suppliers to the VA Market.—A number of majorcompanies produce CT scanning equipment, includingCGR, General Electric Co., Picker International, andSiemens. Since 1979 the VAMKC has purchased CTequipment from General Electric, Pfizer, and PickerInternational (Pfizer has since left the CT market) andsome equipment from Technicare, a subsidiary ofJohnson & Johnson, for use with CT equipment. In1982 a number of companies responded to theVAMKC request for technical proposals to supply CTequipment. Only two of those companies’ proposalsmet the necessary technical specifications. Those twocompanies were then issued an invitation for bid. Ofthe two companies that received an invitation for bid,only one company’s product passed the testing forspecifications, and that company received the contract.(There was a second round of bidding in 1982, withdifferent specification requirements, to replace five CTunits purchased in 1979. ) In 1983 three companies sub-mitted technical proposals that met specification re-quirements; those three companies received an invita-tion for bid. One of the three companies’ products didnot pass testing, and the contract was given to thelower of the two remaining bids. Thus, in both 1982and 1983, one firm received either all or most of theorders (40).
It is difficult to say whether the number of poten-tial CT equipment suppliers to the VA market will in-crease or decrease in the next few years. As the mar-ket matures, it is likely that some firms now active willexit the market. On the other hand, it is likely thatthe equipment of more of the firms remaining will meetVAMKC specifications. Thus, it is hard to predictwhether competition in the VA market will increaseor decrease.
Digital Image Processing Equipment
Digital image processing is a technology that recon-structs and enhances images based on data stored elec-tronically in digital form, The system is perhaps bestexplained by comparing it with the technologies it is

replacing. In traditional projection radiography, forexample, the X-rays passing through the subject strikean X-ray sensitive photographic film. The chemicalson the film are exposed (i. e., darkened) at particularlocations depending on the attenuation of X-ray beamsas they pass through the subject on their way fromtheir source to the film. In a digitized projection X-ray system, the photographic film is replaced by a gridof electronic detectors that transmit their data on X-ray exposure to a computer, where the data are re-corded in digital form. These recorded data can thenbe processed in a variety of ways and used in recon-structing images. (The familiar computer-printed pic-tures of the Mona Lisa and Snoopy are examples ofimage production from digital data, though these com-puter programs are vastly less sophisticated than thoseused in medical imaging. )
In digital fluoroscope, a photoemitter is connectedto an image-intensifying system, which creates a videosignal that is digitized, stored, and processed. A televi-sion monitor driven by a digital display controller thenconverts the processed information into displayedbrightness (75).
Digital image processing offers a number of impor-tant advantages over standard radiographic andfluoroscopic techniques and is being applied to ultra-sound techniques as well. Notably, this processing canvary the brightness and contrast of a picture so adiagnostician can focus on particular features. As men-tioned in the discussion of X-ray equipment, contrastresolution is a problem in standard radiographic tech-niques, Because the film must record a wide range ofX-ray attenuation occurring between the source andthe detector, it is often difficult if not impossible todistinguish two objects similarly opaque to X-rays inan X-ray photograph. The advantage of digital imageprocessing is that signals representing a narrow rangeof X-ray attenuation can be processed to obtain highcontrast. This enhancement is like that of a medicalthermometer compared to an outdoor thermometer.The outdoor thermometer must record temperaturesanywhere from –30O to over 100° F, a very widerange; a medical thermometer can be more sensitivesince it only covers a range from 94° to 108° F, Simi-larly, one may adapt a digital image to focus on a nar-row range more sensitively.
There are other advantages of digital image proc-essing as well. It can also be used for edge enhance-ment and to increase the clarity of the X-ray image.Its greater sensitivity makes possible less X-ray ex-posure, and the time diagnosis takes is also reducedby eliminating the time-consuming step of film devel-opment.
One of the most important medical applications ofdigital image processing is in angiography (103). Inangiography, a catheter is threaded through a vein orartery until properly positioned and a dye that isopaque to X-rays is injected. Subsequent X-rays of theinjected region highlight the blood vessel passages, re-vealing arterial blockages, constrictions, and othersigns of atherosclerotic disease. Angiography requiresminor surgery, however, and is not without risk; anaverage of 2 in 1,000 patients die from complications(77).
Digital image processing substantially reduces therisks of angiocardiography and arteriography. In ei-ther procedure, dyes injected into the bloodstreambegin to diffuse through the bloodstream, and usingstandard X-ray techniques this meant that dye had tobe injected very close to the location of interest, re-quiring invasive surgery. Digital image processing,however, can enhance the information about the flowof dye. The new techniques can sense far loweramounts of dye than standard equipment, whichallows the dye to be injected in peripheral veins. Veryrevealing images of interior structures can be createdusing digital subtraction. First, an X-ray image of anarea is taken before injecting the dye and the patternobtained is stored on computer disks or tapes. Thenthe dye, usually iodine, is injected, and as the dyepasses through the area’s arteries, a television moni-tor displays a pattern representing the difference, pointfor point, between the images before and after injec-tion. In this way, a much less cluttered picture is cre-ated (58).
Another important advantage of digital image proc-essing is that its operating costs are much lower thanthose of standard radiography. It does not require ex-pensive X-ray film, the annual costs of which can beas great as the capital cost of standard radiographicequipment. Also, because images are stored on suchmedia as magnetic tape or disks in very little space,the large storage facilities now required are no longerneeded (25,37). In addition, the diagnostician can re-trieve stored X-rays almost instantly from a computerterminal.
Because of the enormous and rapidly growing ad-vantages of digital imaging, the markets for radio-graphic and fluoroscopic equipment are now unstable.One manufacturer’s representative predicted that theentire imaging market could be captured by digital im-aging within 5 years (25).
The VA Market: Demand and Supply
VA Demand.—In discussing VA demand for digi-tal image processing equipment, it is necessary to dis-tinguish between such equipment that is an integral

91
part of an X-ray system and that called “digital add-on” equipment, which is appended to an existing sys-tem to “digitize” it. It is difficult to determine the ex-tent of total VAMKC procurement of digital imageprocessing equipment from available VAMKC docu-ments. The available documents indicate that in 1982the VA purchased $342,261 worth of digital radiog-raphy equipment and $438,900 worth of digital fluor-oscope equipment, for a total of $781,161, or justslightly more than 0.6 percent of the total VAMKCnon-FSS expenditures for medical equipment. How-ever, an unknown part of the expenditures for “X-rayequipment” may actually represent such imagingequipment purchased as part of a system (132). In thisdiscussion we will focus on VAMKC procurement ofdigital “add-on” equipment.
The Problem of Mixed Systems.—Perhaps the mostimportant feature of the market for digital add-onequipment is the problem of putting together the prod-ucts of different companies into a coherent system.VAMKC procurement personnel and manufacturers’representatives indicate their concern about assigningresponsibility for equipment breakdowns, particularlyduring the warranty period. They fear that when a sys-tem does not function properly, each of the companieswill place the blame on a component produced by theothers. In addition, there is the problem of coordinat-ing the delivery of mixed systems, and especially, ofdetermining which manufacturer is responsible forconnecting the components. Finally, there are theissues of service costs and the larger discounts typicallyoffered when the VAMKC purchases an entire systemfrom one manufacturer (40).
As a result of these complications, the VAMKCstrongly prefers to purchase complete X-ray systemsrather than purchase their components from differentmanufacturers. When the VAMKC does purchase dig-ital add-on equipment, it prefers to purchase thisequipment from the same manufacturer that producedthe system (40). This preference probably reduces thenumber of vendors to the VA market, which may in-crease the costs of the digital add-on equipment. Avail-able documentation does not indicate if the impact ofthis preference is significant, and if it is, whether ornot the above-mentioned difficulties with mixed sys-tems still make the preference for avoiding mixed sys-tems the most cost-effective strategy.
Suppliers to the VA Market. -There are probably30 or 40 manufacturers of digital image processingequipment today (37). However, many of them pro-duce only add-on equipment, and thus, for the rea-sons discussed above, may have some difficulty sell-ing their products through VAMKC. In 1982 theVAMKC purchased digital image processing equip-ment from only two companies (132).
Nuclear Diagnostic Equipment
In diagnostic nuclear medicine, pharmaceuticalstagged with a gamma-ray-emitting isotope are ad-ministered to a patient. The steady-state or dynamicdistribution of the isotope in the body is then deter-mined by an imaging system. The most common im-aging system is the “gamma camera, ” which producesa projection image. It is also possible to combine cross-sectional techniques and isotope imaging in emissioncomputed tomography, in which one or many gammacameras rotate around the patient and collect and storedata for many projection images. Techniques like thoseused in CT are then used to create cross-sectionalimages.
Diagnostic nuclear medicine has a number of medi-cal uses. It requires only a low radiation dose and isparticularly suited to the study of cardiac dynamicsand to whole-body imaging, which can determine theextent of certain diseases (75). Nuclear medical equip-ment is commonly used in diagnosing thyroid dysfunc-tion, using a radioisotope of iodine as the tracer.
The VA Market: Supply and Demand
VA Demand.—The VA and several other agenciespurchase nuclear medical equipment through the di-rect delivery program of the VAMKC’S Radiologicaland Nuclear Equipment and Supplies Division. Nucle-ar medical equipment accounts for a variable but sig-nificant part of total annual VAMKC medical equip-ment procurement expenditures. In 1979 it accountedfor 19 percent of total non-FSS equipment expendi-tures; in 1980, 12.5 percent; in 1981, 18.1 percent; andin 1982, 6.6 percent. Total expenditures for nuclearmedical equipment were $10 million in 1979, $4.3 mil-lion in 1980, $5.4 million in 1981, and $8.3 miIlion in1982 (131,132).
The VAMKC manages direct delivery purchases ofnuclear diagnostic equipment for a number of agen-cies, including the VA, Public Health Service, Army,Navy, Air Force, and other Government agencies. Itappears that the VA is not always the largest buyerof nuclear medical equipment through the VAMKC,In 1979 the VA accounted for 81.2 percent of total ex-penditures on nuclear medical equipment; by 1980 itaccounted for only 49 percent of the expenditures,though it was still the largest buyer; and in 1981 theVA accounted for only 32.4 percent of expenditures,buying less than the Army (131). There is no break-down of equipment purchases by agency in 1982 or1983.
VAMKC Procurement Relative to the National Mar-ket.—VAMKC procurement of nuclear medical equip-ment accounts for a moderately significant part of the

92
national market. In 1982 VAMKC procurement to-taled about $8.3 million. Based on the data that nu-clear medical equipment vendors must provide theVAMKC, it would appear that VAMKC procurementin that year accounted for approximately 7 percent ofthese vendors’ nuclear medical equipment sales (witha range from about 5 to 10 percent) (132),
VAMKC Demand Variability .—VAMKC procure-ment of nuclear medical equipment has fluctuated fromyear to year (see table C-3). The variability of nuclearmedical equipment expenditures is not as great as thosefor X-ray equipment, but it is significant.
Suppliers to the VA Market.—Companies withVAMKC annual contracts in the past 3 years include(in alphabetical order) Elscint, Inc.; General ElectricCo.; MEDX, Inc.; Picker International; Raytheon;Siemens; Technicare; and Toshiba Medical Systems,All major manufacturers appear to have an annualcontract with the VAMKC.
It is difficult to assess the competitiveness of the nu-clear medical equipment market. The four firms withthe largest market shares in 1982 accounted for almost95 percent of VAMKC procurement, and the patternis similar in earlier years for which data are available.With such high market concentration, the firms arelikely to recognize their mutual dependence, and vig-orous price rivalry would not be expected.
However, other factors operating in the nuclearmedical equipment market suggest that this simplestructural measure may underestimate true competi-tiveness. First, in this market there is very rapid tech-nological change. In such situations, firms tend to com-pete very vigorously in both product development andpricing (78). Second, there have been notable changesin the rankings of the top four firms in the VAMKCmarket (table C-4).
Not only have the rankings of the firms shifted, butas table C-5 shows, so have their market shares. (Ifthe firms were quite close to each other in marketshares, there could be significant movement in thefirms’ rankings without significant shifts in marketshares. ) Again, the greatest possible sum of the abso-lute values of market share changes is 200. The data
Table C-3.—Annual Percentage Change inVA Marketing Center Procurement ofNuclear Medical Equipment, 1979-82
1979-80 1980-81 1981-82
Total. . . . . . . . . . . . . . . . . . . -57.50/0 +25.9Y0 +54.80/0VA only . . . . . . . . . . . . . . . . -74.3°/0 –16.7°/0 N.A.SOURCE: U.S. Veterans Administration, Marketing Center, Radiological and
Nuclear Equipment and Suppiies Division, unpublished data, Hines,IL, 1983; and U.S. Veterans Administration, Marketing Center,Radiological and Nuclear Equipment and Supplies Dlvlsion, unpub-lished information from vendors’ 1982 contracts, Hines, IL, 1983.
Table C.4.—Changes in Rankings of Four LargestSellers of Nuclear Medical Equipment Through the
VA Marketing Center, 1979-82
1979 1980 1981 1982A B B D
A D A~ C A CD D C B
NOTE: The firm with the largest 1979 VA market share is identified as Firm A, thatwith the second largest 1979 market share Firm B, etc.
SOURCES: U.S. Veterans Administration, Marketing Center, Radiological andNuclear Equipment and Supplies Division, unpublished data, Hines,IL, 1983; and U.S. Veterans Administration, Marketing Center,Radiological and Nuclear Equipment and Supplies Division, un-published information from vendors’ 1982 contracts, Hines, IL, 1983.
Table C.5.—Sum of Absolute Values of Year-to-YearPercentage Changes in Vendors’ VA Marketing CenterNuclear Medical Equipment Market Shares, 1979.82
1979-80 1980-81 1981-82Sum of absolute values. . . . . . 14.1 40.5 35.4As a percent of maximum
possible value (200) . . . . . . . 7.0% 20.30/o 17.7%SOURCES: U.S. Veterans Administration, Marketing Cater, Radiological and
Nuclear Equipment and supplies Division, unpublisheci data. Hines.IL, 1983; and U.S. Veterans Administration, Marketing ‘Cente~:Radiological and Nuclear Equipment and Supplies Division, unpub-lished information from vendors’ 1982 contracts, Hines, IL, 1983,
in table C-S suggest that firms are competing with eachother for market share, although, as discussed in thesection on X-ray equipment, other explanations arepossible.
The market concentration and market share datapoint to opposite conclusions about competition in thismarket. It is impossible, given available data, to assesspricing rivalry in the VAMKC nuclear medical equip-ment market. However, though it may be difficult toassess the static efficiency of this market, the pace oftechnological change and improvement in product per-formance are consistent with high dynamic efficiency.
NMR Devices
NMR, or as it is also known, magnetic resonanceimaging (MRI), is based on the principle that infor-mation can be gathered on the composition of tissuethrough its response to powerful magnetic fields. Thebasic tool of NMR is an immense and extremelypowerful doughnut-shaped magnet that can enclose thepatient’s entire body. When subjected to magneticfields, hydrogen nuclei within the patient’s body alignthemselves in parallel ranks, spinning like tops, andwobbling or “processing,” as tops do, around their axesof spin. The patient is then irradiated with a short elec-tromagnetic pulse, which pushes the spinning nuclei

93
over on their sides. When the pulse subsides, the nucleireturn to their positions, reradiating in the processsome of the energy they had absorbed. Sensitivereceivers pick up this electromagnetic echo. The in-formation about the tissue comes from the timing andintensity of the signal, which depend on the amountof fat or water in a tissue and the type of motion ofthe nuclei. Computers then analyze the signals anddisplay a cross-sectional image of the area studied (1).The techniques used for developing a cross-sectionalimage are essentially the same as those used in CTscanners, through digital data processing.
The advantage of NMR is that, unlike CT scanners,NMR does not expose the patient to X-rays. NMR mayprove useful in diagnosing cancer and in detectingbrain abnormalities and possibly heart damage (56).
Demand and Supply
NMR (or MRI) devices have only recently receivedapproval of the Food and Drug Administration (FDA),and thus are only beginning to be sold commercially.Their cost is expected to be roughly that of CT scan-ning devices (56) or perhaps higher (86). Accordingto a recent estimate, by August 1984, 93 NMR unitswere installed within the United States (84). It is widelybelieved that NMR’s potential market is extremelylarge. One manufacturer’s representative estimatedthat the NMR national market maybe as large as $250million to $300 million a year within 2 or 3 years (42).Given the size of the potential market for NMR de-vices, a number of manufacturers have entered thefield, including General Electric, Philips, Picker, andTechnicare.
Through fiscal year 1983 only one NMR device hadbeen procured through the VAMKC, one for a clini-cal evaluation. This procurement is unlikely to affectthe market significantly. Performance specificationswere drawn up for the purchase, but they were basedon those of available products, and so should not haveaffected product development (40).
Because NMR’s use in medicine is so new and hasso recently received FDA approval for clinical use, themarket is in its youth. However, NMR will likely havea significant market within a few years. It would clear-ly be in the public interest for the VAMKC to beginplanning its NMR procurement policies.
PET Devices
PET is another technique for cross-sectional imag-ing. It is unique in producing images of chemical activ-ity within the body, such as local metabolism. In PET,positron-emitting isotopes of biologically significantatoms—e.g., oxygen, nitrogen, or carbon—are pro-
duced using a cyclotron. These isotopes are then at-tached, or “tagged,” to a physiologically active mate-rial, such as glucose, and administered to the patient.Finally, a scanner determines the postinjection distri-bution of the isotope, the information being processedlike that in a CT scan to produce a two-dimensionalimage. The image is significant because the distribu-tion of the isotope reflects the distribution, and there-fore the utilization, of the metabolize (75).
Demand and Supply
PET has attracted attention in the popular press forits potential in diagnosing metabolic disorders, brainabnormalities, and cancer. It would appear to be a wayof observing abnormalities in body chemistry, withgreat medical potential.
At present, however, there does not appear to bea significant market developing for PET scanners. Inpart, this probably reflects the expense of PET, per-haps $1 million for the PET scanner itself and as muchas another $2.5 million for a cyclotron to produce theradioactive isotopes (1).
The VA has purchased two PET scanning devicesand apparently has no immediate plans to purchasemore, so VAMKC procurement practices have mostlikely not affected whatever market this product has.It is uncertain whether a market for PET will developlater, but at the moment PET does not appear to bean important issue for procurement planners.
Ultrasound Diagnostic Equipment
Ultrasound is generally defined as vibrations be-tween 20 kHz and 30 MHz. The sound frequencies usedfor most diagnostic purposes range from 1 to 12 MHz.Such ultrahigh frequencies are produced by piezoelec-tric transducers that convert electrical energy to vibra-tory mechanical energy (sound). After a short soundburst, the transducer circuitry is switched to act as areceiver for returning sound or echoes, and for eachpulse of sound emitted the reflectivity of tissue alongthe line of sound transmission is measured. The return-ing echo is converted to an electrical signal that is proc-essed and stored in digital form.
In traditional ultrasound the echoes are displayedon an oscilloscope, with the intensity of each echo rep-resented by a correspondingly bright spot on thescreen. The position of the echo is displayed in the X-Y plane depending on the position of the transducerand the transit time of the acoustic pulse. In more mod-ern ultrasound equipment, the digitized informationcan be processed with digital image processing to ob-tain a better picture of the target object. Moving thesound beam through the tissues by moving the trans-
2 5 - 2 8 9 0 - 8 5 - 8

94
ducer is termed scanning. Using scanning techniques,a series of parallel or orthogonal tomograms, whichare images of a slice or plane, can be assembled intoa three-dimensional image of an organ.
Ultrasound is extremely useful in diagnosing heartdisease and in detecting abnormalities of the liver,kidneys, gallbladder, and lymph nodes in the abdomen(72). It also has the very important attraction ofemploying nonionizing radiation at low power levels;no harmful effects have been found in humans inalmost 30 years of clinical application (72). However,ultrasound has limitations. It requires a soft-tissue pathbetween the transducer and the region of study; in-tervening bone, air, or dense fat attenuates and distortsthe sound (60,72). In addition, ultrasound cannot ef-fectively penetrate deep into tissue (about 22 cm is nowthe practical limit) and thus cannot effectively analyzeproblems in blood vessels or other parts deep withinthe body (77).
General Demand Characteristics
Supplies v. Equipment Costs.—Ultrasound equip-ment is relatively inexpensive to operate. Costs of sup-plies and expendable are modest, perhaps at most one-fifth or one-sixth of the equipment’s purchase price,according to one industry source (60).
Equipment Purchase Price.—Ultrasound equipmentvaries substantially in price depending on a system’scapabilities. A system typically costs between $40,000and $120,000, in the middle range for the diagnosticmedical equipment discussed here.
Servicing and Technical Support.—Servicing andtechnical support are important to the proper function-ing of ultrasound equipment. Manufacturers will fre-quently provide training in these areas to customers’personnel, and service availability is one of the im-portant factors affecting VA procurement of ultra-sound equipment (60,85).
The VA Market: Demand and Supply
VA Demand. -Ultrasound equipment has been pur-chased through the VAMKC’S direct delivery programsince April 1983. Prior to that it was purchasedthrough decentralized contracts. From March 1, 1980,to February 1981, such ultrasound procurement totaled$6.84 million; from March 1,1982, to March 31,1983,VAMKC procurement of ultrasound equipment to-taled about $11.5 million; in 1983 it is expected to beabout $5 million (85).
Differences in contract, fiscal, and calendar yearsmake it impossible to calculate the proportion of non-FSS medical equipment expenditures accounted for byultrasound equipment. The $11.5 million spent on
ultrasound equipment in the 1982 contract year isequal to about 9 percent of total VAMKC direct de-livery equipment procurement costs in the 1982 Gov-ernment fiscal year. The 1980 contract year ultrasoundprocurement of $6.84 million is equal to about 20 per-cent of 1980 fiscal year direct delivery equipment pro-curement costs, although it was not included in thedirect delivery program at the time. The figure for 1983is likely to be much smaller, perhaps 5 to 10 percent(85,131,132). Exact data are not available, but accord-ing to the VAMKC contract specialist for ultrasound,the VA accounts for about 60 percent of total VAMKCprocurement of ultrasound equipment, with the Army,Air Force, and Public Health Service accounting formost of the rest (85).
VA Demand Relative to the National Market.-TheVA accounts for a very small proportion of the na-tional demand for ultrasound equipment. Severalsources estimated that national sales of ultrasoundequipment in 1982 were about $400 million (60,74).Assuming VA procurement to be 60 percent ofVAMKC procurement, VA expenditures represent noteven 2 percent of the national market; VAMKC pro-curement altogether was probably not more than 3percent. National sales of ultrasound equipment areexpected to be less in 1983 than in 1982, about $285million. However, VAMKC ultrasound procurementis expected to fall even more, to about $5 million, orless than 2 percent of the market. Although VAMKCprocurement may account for a larger proportion ofsome vendors’ sales than this, no vendor indicated onits annual contract that VAMKC procurement ac-counted for more than 5 percent of the company’sultrasound equipment sales (85).
VAMKC Demand Variability .-VAMKC ultra-sound procurement expenditures vary substantiallyfrom year to year. The decline from contract year 1982to contract year 1983, for example, is expected to begreater than 55 percent. More than half the manufac-turers’ representatives interviewed indicated thatVAMKC demand variability is greater than that ofmost private customers (55,60,74,87).
Suppliers to the VA Market. -The capital require-ments to enter the ultrasound market are smaller thanfor many other kinds of diagnostic medical equipment,and many small companies have entered the marketin recent years. This is reflected in the VAMKC mar-ket, where more than 15 companies will have annualcontracts this year (85).
Although some companies do specialize in particu-lar ultrasound applications (abdominal, cardiac, etc. )there appears to be substantial competition in the mar-ket. In contrast to the VAMKC’S procurement of otherkinds of medical equipment discussed here, its procure-

95
ment of ultrasound equipment is very evenly distrib-uted among the vendors on contract. The four ven-dors with the largest shares of the VAMKC marketaccounted for only slightly more than half of theVAMKC market in 1982; sales of the vendors rankedseventh and eighth totaled almost as much as thoseof the vendor with the largest share; and even the low-ranked vendors accounted for significant shares of theVAMKC market (85). Consistent with this low mar-ket concentration, the relative ease of entry into themarket, and the industry’s very rapid technologicalchange, the ultrasound equipment market was de-scribed by the VAMKC contract specialist as “fiercelycompetitive” (85).
Electromedical Equipment
The 5-digit SIC category Electromedical Equipment(SIC Code 36932) includes a wide variety of diagnos-tic, therapeutic, and patient monitoring equipment. Inthis discussion, VA procurement of electrocardiograph(ECG), electroencephalograph (EEG), and patientmonitoring equipment is examined.
In electrocardiography, electrodes attached to thechest and extremities measure changes in the electri-cal potential of the body’s surface, which are associ-ated with the electrical activity accompanying the ac-tion of the heart. Thus, such measurements can detectheart abnormalities. In electroencephalograph, elec-trodes attached just under the scalp detect electricalactivity in the brain. EEG recordings are used indiagnosing epilepsy, stroke, tumors, and other brainabnormalities. ECG and EEG recordings were origi-nally made on paper rolls (63), but digital recordingtechniques are replacing the old recordings, so thatECG and EEG equipment can easily be used in patientmonitoring as well as diagnosis.
Patient monitoring equipment is used to monitor pa-rameters reflecting a patient’s medical condition, suchas blood pressure, pulse, brainwave activity, tempera-ture, and respiration. Modern patient monitoringequipment is based on semiconductor chip technology,and often incorporates microcomputer components.Patient monitoring equipment varies in complexity andcost, from stand-alone units that monitor one or a fewfunctions for a single patient to central station systemsthat can monitor a wide range of physiological indi-cators for a very large number of patients and transmitthe data for display to a single location, such as anurses’ station (20).
General Demand Characteristics
Equipment Purchase Price.—Stand-alone EEG,ECG, and patient monitoring units range from $2,000
to $16,000, while systems can cost anywhere from$20,000 to several hundred thousand dollars depend-ing on their size and complexity (20).
Servicing and Technical Support .—According to anindustry source, most EEG, ECG, and patient monitor-ing equipment does not require much servicing, andthe annual cost of a full-service contract is about 5 to10 percent of the equipment’s purchase price.
The VA Market: Demand and Supply
VA Demand .-Patient monitoring systems are pur-chased through the VAMKC direct delivery program;stand-alone monitoring units and EEG and ECG equip-ment are purchased through the FSS program.
In July 1982 the responsibility for procurement ofpatient monitoring systems was transferred within theVAMKC. Unfortunately, the procurement data werenot similarly transferred, and it was not possible toconstruct a historical series for this kind of equipment.In addition, according to VAMKC personnel, FSS pro-curement data for stand-alone EEG, ECG, and patientmonitoring equipment are also not readily availablefor 1981 and 1982 (49).
FSS procurement of such stand-alone equipmentduring the first three quarters of the 1983 contract year(beginning August 1982) totaled $4.6 million (49).Assuming that this figure can be extrapolated for theyear (multiplying it by four-thirds), annual FSS pro-curement during the contract year should be about$6.2 million.
In fiscal year 1982 (beginning October 1981),VAMKC procurement of patient monitoring systemsunder the direct delivery program totaled $12.2 mil-lion, which suggests that expenditures for such systemsare about twice those for stand-alone equipment. Inthe same year, procurement of patient monitoring sys-tems represented close to 10 percent of total equipmentprocurement under the direct delivery system (132).The lack of data makes it impossible to calculate cor-responding figures for earlier years.
VAMKC Procurement Relative to the National Mar-ket.—According to one industry source, the nationalmarket for patient monitoring systems is about $220million, and that for stand-alone EEG, ECG, and pa-tient monitoring units about $100 million (20). If theVAMKC figures of $6 million for stand-alone equip-ment purchases and $12 million for monitoring sys-tem purchases are in fact representative, then VAMKCprocurement accounts for about 5 to 6 percent of na-tional sales for both categories of equipment, Becausethe data are incomplete, and because VAMKC pro-curement of other medical equipment varies greatlyfrom year to year, it is best to consider these estimatesas rough ones.

Suppliers to the VA Market.—Although a numberof firms produce patient monitoring equipment, theVAMKC market is dominated by a few large firms.In fiscal year 1982, the four firms with the largestshares of VAMKC direct delivery procurement ac-counted for close to 95 percent of such procurement,and a single firm accounted for much of the 95 per-cent (132). The national market for patient monitor-ing equipment is also highly concentrated. Some com-panies appear to have a much higher share of theVAMKC direct delivery market than they do of thenational market, while for other companies the reverseis true. Based on information in 1982 annual contracts,one vendor’s share of the direct delivery market wasonly 7 percent of its share of the national market, whileanother vendor’s direct delivery market share wasalmost seven times as large as its nationaI marketshare. This is a puzzling phenomenon, and to under-stand it would require a closer investigation than ispossible here; however, since it may reflect somepositive or negative feature of procurement rather thanchance, it may warrant further study.4 It was not pos-sible, given available date, to calculate the market con-centration of the FSS patient monitoring equipmentmarket.
Despite the apparent market concentration and theexistence of a dominant firm, Hewlett-Packard, boththe VAMKC and industry sources characterized thefirms in the patient monitoring equipment market asvery competitive (20,47,49,92).
Hemodialysis Equipment
Dialysis is the transfer of solute (a dissolved sub-stance) across a semipermeable membrane. Hemodial-ysis, through “artificial kidney” machines, is dialysisto purify the blood of people whose kidneys have part-ly or completely ceased to function. In such machines,blood is circulated on one side of a semipermeablemembrane while a special dialysis fluid is circulatedon the other. The dialysis solution must closely matchthe chemical composition of the blood. Metabolicwaste products, such as urea and creatinine, diffusethrough the membrane into the dialysis fluid and arediscarded, while substances needed by the body (e.g.,sodium chloride) are prevented from diffusing by in-cluding the same substances in the dialysis fluid (63).
‘One possible explanation is that VA hospitals are generally larger,university-affiliated hospitals. Certain vendors do better in this select mar-ket than they do elsewhere (10).
The VA Market: Demand and Supply
VA Demand. -Manufacturers contract with the FSSdivision of the VAMKC to provide hemodialysisequipment and supplies to Government agencies atspecified prices. These prices, along with product de-scriptions, provide the supply schedules that VA hos-pitals and other Government agencies use to orderequipment and supplies directly. Most schedules areso-called multiple award schedules, specifying severaldifferent vendors’ versions of an item so that buyerscan choose among them. Multiple award schedules aregoverned by a most favored customer clause (describedlater below). Less frequently, the FSS program awardscontracts through competitive bidding and makes asingle award (47).
The VA spends a relatively modest sum on hemo-dialysis equipment relative to its expenditures onhemodialysis disposable and supplies. One manufac-turer estimated that in the national market equipmentcosts are onlys to 8 percent of total dialysis costs, withdisposable, consumables and personnel costs account-ing for the remainder (17).
According to the FSS Solicitation for Offers for1984, estimated expenditures for hemodialysis equip-ment for 1984, which are based on actual 1983 expend-itures, are slightly under $650,000 (129), or about one-half of 1 percent of total annual VAMKC equipmentprocurement expenditures. This figure seems unreal-istically low. At approximately $7,000 per machine(the price quoted by two manufacturers), the VAwould have purchased only 93 machines. However,the VA now has about 1,900 machines in use, and theaverage machine is replaced afters years; this impliesa 20-percent turnover rate (17) and thus that the VAshould be buying about 400 machines annually. In esti-mates of the VA’s importance in the national market,it will be assumed that a normal annual procurementis between 10 and 20 percent of stock or 200 to 400hemodialysis machines per year. If this is the case, thenannual expenditures on hemodialysis equipment arebetween 1 and 2 percent of total annual medical equip-ment procurement.
VA Demand Relative to the National Market.—There are approximately 25,000 hemodialysis ma-chines in use in the United States today; of these, about1,900, or 7.6 percent, are in use in VA installations.
The market for new machines is a function of de-preciation and obsolescence of existing equipment andthe growth of new facilities. More than one manufac-turer estimated that the size of the national market wasabout 4,000 to 5,000 machines per year at an averageunit price of between $7, 000 and $8,000, or between$28 million and $40 million (17,73). If FSS procure-ment of hemodialysis equipment is roughly propor-

97
tional to its share of dialysis equipment now in use,then it should account for about 7 to 8 percent of thenational market. It is probably safe to say that FSSprocurement represents between 5 and 10 percent ofthe national market.
Suppliers to the VA Market .—The national marketfor hemodialysis equipment is highly concentrated; thethree largest companies account for about 90 percentof total market sales, and only five firms account forvirtually all the national sales. Data are not availableto calculate manufacturers’ market shares of theVAMKC FSS market, but sales in this market appearas highly concentrated as in the national market(17,73,135).
Analysis and Implications for Policy
The Importance of VA Procurement inthe National Market
The VA’s proportion of the national market formedical equipment, considered in isolation, is amisleading measure of the market leverage that the VAexerts. VA procurement is channeled through theVAMKC, which also acts as contract negotiator andadministrator for the Public Health Service, the armedservices, and other Government agencies. The com-bined procurement of all these groups, then, deter-mines the buying power of the VA. As a result, therest of this discussion will consider all VAMKC pro-curement, rather than its procurement for the VAalone.
VAMKC procurement accounts for a significant, butnot overwhelming, proportion of the national marketfor most types of equipment examined in this appen-dix; in some of the markets, the VA proportion is verymodest. Based on data in VAMKC annual contracts,VAMKC procurement accounts for 5 to 10 percent ofthe national markets for X-ray, nuclear diagnostic, andhemodialysis equipment, about 5 percent of the na-tional market for EEG, ECG, and patient monitoringequipment, 3 percent of the national market for CTscanning equipment, and 1 to 2 percent of the ultra-sound equipment market. The VAMKC share of thenational market for digital image processing equipmentis uncertain, but most likely is very small (40,131,132).Thus, although the dollar amounts of VAMKC pro-curement may be significant, and vendors are certainlyanxious to maintain their VAMKC market share,VAMKC procurement does not dominate any marketexamined here.
Conditions of Supply
Numerous structural characteristics of the marketcan be said to shape observed market outcomes (78),but only a few of the most important will be discussedhere.
Barriers to Entry
For some of the equipment categories examined, par-ticularly CT scanners and radiographic and nucleardiagnostic systems, the capital requirements of themarket appear to preclude the entry of small firms.The servicing and technical support of some productsare so important that the firms that cannot offer well-organized nationwide support suffer a severe dis-advantage.
Of course, all these markets are not entirely closedto small firms. There is enormous technological changeoccurring in almost all the markets examined, muchof it in computer applications to diagnostic medicine,and in software rather than hardware. In such mar-kets, a small firm can succeed if it finds a niche. (Onthe basis of reports of mergers and acquisitions, theresult of that success is often being purchased at anattractive price by a larger firm in the medical equip-ment market. )
Market Concentration
Market concentration, the proportion of salesaccounted for by the largest sellers in a particular mar-ket, is quite high in almost all the medical equipmentmarkets examined here. In the VAMKC markets forX-ray, nuclear diagnostic, patient monitoring, andhemodialysis equipment, the four largest firms in eachclass accounted for 90 to 95 percent of procurementexpenditures within their classes. Procurement of CTscanners has been based on competitive bids, and thesame firm won the contract in both major bids. Onlyin the market for ultrasound equipment are VAMKCprocurement expenditures spread more evenly over alarge number of companies, Generally, such high mar-ket concentration is associated with a lack of highpricing rivalry, but it is not clear that this is the casefor the industries examined here.
Market Share Instability
High market concentration can sometimes be amisleading indicator of firms’ conduct in the market.In both the X-ray and nuclear diagnostic equipmentVAMKC markets, market share instability suggeststhat rivalry among the firms is greater than would bepredicted on the basis of market concentration.

98
Summary of Competitive Conditions
Although the medical equipment markets examinedin this appendix certainly do not conform to the pic-ture of perfectly competitive markets, the volatility ofmarket shares and the very rapid pace of technologi-cal change suggest that these markets still functioncompetitively. In a few cases, rivalry may be basedmore on product performance than price. Two of theVAMKC markets, for ultrasound diagnostic and pa-tient monitoring equipment (the first of which is highlyconcentrated and the second not), were both describedby VAMKC personnel as extremely competitive (49).
The Impact of VAMKC Procurement onVendor Pricing
The impact of VAMKC procurement on market out-come depends not only on supply conditions and thelevel of VAMKC procurement, but also on the proce-dures and policies that govern VAMKC procurement,the most important of which are analyzed below.
Brand Name Justification .-When a VA hospital isauthorized to buy equipment, the VAMKC forwardsto the hospital a list of suppliers on contract whoseequipment meets the specifications of the purchase or-der, ranked by order of cost. By regulation, the hos-pital is required to buy from the least-cost supplierunless it can justify purchasing from a different source(e.g., service availability). This requirement is calledbrand name justification. Because suppliers are anx-ious to maintain their share of the VAMKC market,the requirement almost certainly lowers prices.
Firm Fixed Price Clause.—Under the terms of aVAMKC contract, suppliers cannot increase pricesduring the contract year. Furthermore, if they lowerthe price at any time during the year, the lower priceholds for the remainder of the year. The firm fixedprice clause may or may not result in lower procure-ment costs. Suppliers offer temporary price discountsin the private market to promote their products. Nor-mally, promotional offers would probably be extendedto the VAMKC as well, but because of the firm fixedprice clause, suppliers are reluctant to make them.Even the requirement that prices not be increased dur-ing a contract year has indeterminate effects on pro-curement costs. While the requirement does protectthose who buy through the VAMKC from price in-creases, suppliers may charge a higher price at the startto ensure a profit. Altogether, it is extremely difficultto determine the net effect of the firm fixed price clause.
Public Disclosure Requirements. -By law, the pub-lic has access to VAMKC procurement prices for med-ical equipment. Both theoretical and empiricalevidence support the view that this results in higher
procurement costs for the VAMKC. First, a firm’sbenefits from cutting its price are in part a functionof the so-called retaliation lag, the length of time beforerivals learn of the price cut and cut their own pricesin response. Price disclosure requirements reduce theretaliation lag, and therefore discourage price cuttingin the VAMKC market. Because other buyers of med-ical equipment also have access to the price data, theVAMKC price may be the private buyer’s target inpricing negotiations, which can also inhibit price cut-ting in the VAMKC market. Finally, suppliers of X-ray, nuclear medical, patient monitoring, and hemo-dialysis equipment have stated that the prices offeredto the VAMKC are higher because of the contractdisclosure requirement. Some suppliers said thedisclosure requirement did not affect pricing in theirmarkets, for the reason that pricing information waswidely available from other sources.
No Volume Commitment.—Having a contract withthe VAMKC does not imply any contractual volumecommitment in procurement. For two equipment cat-egories, X-ray equipment and nuclear diagnostic equipment, volume commitment does not appear to be animportant consideration. For the other equipment cat-egories examined here, volume is a major influence onpricing.
There are two likely reasons why volume commit-ment would be unimportant in some industries andvery important in others. First, when equipment is pur-chased from stock, and is fairly standardized, a vol-ume commitment can reduce manufacturing costs thatcan be passed on to the buyer, but not when the equip-ment is custom made. Second, the effects of volumecommitments seem to depend on whether equipmentis expensive or inexpensive. When equipment is inex-pensive, the costs of preparing contracts and market-ing are higher relative to the purchase price of theequipment. In this situation, the savings that comewith volume commitment are more significant. Somesuppliers indicated that they might lower their pricesby 5 to 10 percent in exchange for a volume commit-ment. One supplier in the ultrasound market, statedthat a purchase of even IS to 20 units would sufficefor a larger price discount than is now offered theVAMKC.
Most Favored Customer Clause. -Under the termsof a VAMKC contract, suppliers are prohibited fromselling their equipment under a “like contract” to anyprivate buyer at a price lower than that offered theVAMKC. If a lower price is offered to a private buyer,this price must be given to the VAMKC for the restof the contract year. This stipulation helps ensure thatthe VAMKC’S clients benefit from any vendor com-petition in the private market,

99
Although the strictness with which the most favoredcustomer clause is interpreted varies from one equip-ment category to the next, it almost certainly reducesVAMKC equipment procurement costs. In a few mar-kets, private buyers are offered lower prices than theVAMKC when they make contractual volume com-mitments, on the grounds that these are not “like con-tracts, ” and the effect of the clause is obviously lessin those markets. The most favored customer clausecan greatly influence private buyers, as discussedbelow.
Informal Procedures. -VAMKC personnel said theywere reluctant in practice to purchase mixed medicalequipment systems, those in which items of differentmanufacturers are interconnected. The most impor-tant reason for this is the difficulty of assigning finan-cial responsibility for repairs under warranty, in ad-dition to that of determining responsibility for actuallymaking the interconnections. Unfortunately, this VApolicy may practically eliminate many smaller com-panies in procurement, causing higher initial procure-ment costs. The reluctance to purchase mixed systemsis based on experience, but the value of this policyshould be reviewed periodically.
The Impact of VAMKC Procurement onVendor R&D
In contrast to prosthetic devices, which veteransmay have special needs for and the VA has activelydeveloped and procures with great leverage, the cate-gories of medical equipment examined here are onesthat the VA and VAMKC affect relatively little. Ofthe various VAMKC procurement mechanisms thatcould influence vendors’ research and product devel-opment, only three seem to exert any significant im-pact, and of the three, one type is rather indirect.
Specifications. -The VAMKC can and does influ-ence product development through specifications.These are often developed from industry standards orbased on the characteristics of products already on themarket. To maintain their share of the VAMKC mar-ket, firms must produce equipment that satisfies thespecifications, and some vendors in the markets forX-ray equipment, nuclear diagnostic equipment, CTscanning devices, and patient monitoring equipmentstated that they altered their products to meet the re-quirements (though most of these equipment modifica-tions are incremental changes in performance, not fun-damental improvements in product design). Differentmanufacturers’ products have different strengths. It isa great advantage for a manufacturer to have VAMKCequipment specifications “written to its own machine, ”as discussed below.
Product Evaluations.—The VAMKC’S Testing andEvaluation Staff evaluates some medical equipmentand supply items and makes the results available tothe public. According to the director of this program,these results are heavily used (66). It is impossible toquantify the effect of this program on manufacturers’development activities, though no doubt there is some.
Indirect Effects.—Within the limitations determinedby its shares of the various medical equipment mar-kets, VAMKC procurement can encourage manufac-turers’ R&D to the extent that it embraces new tech-nologies. For the most part, vendors characterizedVAMKC procurement as moderately progressive inthis regard. The VAMKC has a policy of not purchas-ing equipment that is not commercially available andalready in clinical use. Thus, VAMKC procurementis not “state of the art” in most instances. However,the fact that most VA installations do attempt to haveup-to-date equipment probably has some small posi-tive impact on the profitability, and therefore the ex-tent, of manufacturers’ R&D.
Effects of VAMKC Procurement onPrivate Buyers
VAMKC procurement practices may affect privatebuyers of medical equipment in several ways. Themost important of these are its information on prod-uct evaluations and prices, and the most favored cus-tomer clause.
Product Evaluation Information.—As mentionedabove, the product evaluation information producedby the VAMKC’S Testing and Evaluation Staff is ex-tensively used. It must be assumed that the availabil-ity of such information leads to better informed med-ical equipment procurement by private buyers.
Availability of Price Information.—There is clearevidence that the price information available fromVAMKC annual contracts and bids has sometimes in-fluenced private buyers of medical equipment. A pro-curement director for a large, private, centrally man-aged hospital group stated that in one case, he “insistedon a better deal because the VA got a better deal. ” Atthe very least, the VAMKC price may be the targetfor private buyers of medical equipment.
Most Favored Customer Clause. -In contrast to theeffects of available product evaluation and price in-formation, the most favored customer clause increasesthe prices that private buyers must pay for medicalequipment. Interviews with both vendors and buyersindicated that the clause affects prices of X-ray, nu-clear diagnostic, ultrasonic, patient monitoring, andCT scanning equipment. One private buyer indicatedthat the most favored customer clause was a “major

100
problem” for him. Even when vendors offer lowerprices to buyers who make volume commitments, theeffect of the VAMKC is still felt.
The most favored customer clause limits price dis-counting in the private market. For this reason, al-though the stipulation may lower VAMKC procure-ment expenditures, it may actually raise Federal healthcare expenditures through its effect on the equipmentand supply costs of private providers of health care.The Federal Government’s role in financing health careextends far beyond the agencies that procure medicalequipment and supplies through the VAMKC, and ifthe most favored customer clause increases equipmentcosts for private buyers who are reimbursed on thebasis of costs, it could increase rather than decreasetotal Federal health care expenditures.
Manufacturers’ Views ofVAMKC Procurement
Manufacturers generally demonstrate a positiveview of VAMKC procurement. Other than the fail-ure to make volume commitments, which was dis-cussed “above, only three issues were identified asclearly problematic: contract documentation require-ments, the delay in processing procurement orders,and the problem of “tailored specifications. ”
Contract Documentation Requirements. -Contractdocumentation was the major complaint of many ven-dors, especially those of less expensive products, forwhom documentation costs are more significant rela-tive to equipment purchase prices. Documentationmay also be a greater source of dissatisfaction amongsmaller firms because larger firms are more likely to
have employees specializing in Government accounts.Several manufacturers suggested that the VAMKCmaintain a central computer file for contract documen-tation and simply have vendors update the file whennecessary, rather than supply full documentationrepeatedly.
Delay in Processing Orders.—The time required forthe VAMKC to process orders was a major source ofirritation for some manufacturers. Apparently, the de-lays are important only for firms that normally selltheir equipment from stock. When manufacturers pro-duce equipment to order, the order typically becomespart of the order backlog (unless the market is ex-tremely slack). In this situation, the time necessary forprocessing the order is absorbed easily and does notcause problems. When equipment is sold from stock,however, the order can usually be filled immediately,and, as a result, the bureaucratic delay is a major ir-ritation. It is not clear what can be done to alleviatethis problem, except perhaps to computerize the pro-curement process more.
Tailored Specifications. -As mentioned above, dif-ferent manufacturers’ products tend to have differentareas of strength. When equipment specifications arewritten to the specifications of a particular manufac-turer’s product, essentially as “tailored specifications, ”other manufacturers are at a distinct disadvantage inthe VAMKC market. A number of manufacturersfrom a variety of equipment markets complained ofthis problem, suggesting that it warrants greater at-tention from VAMKC personnel. If specification re-quirements can be prepared with attention to their im-pact on the number of vendors able to compete,procurement costs may be reduced without significantsacrifice in quality of care.

References

References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12,
13(
14<
15.
16.
Adler, J., and Witherspoon, D., “New Looks In-side the Body, ” Newsweek, Aug. 16, 1982: 56-59.“An Overview of the VA Prosthetics Researchand Development Program, ” DA V Magazine24(3):8-9, March 1982.Arthur Young & Co,, “A Profile of the MedicalTechnology Industry and Governmental Pol-icies,” June 30, 1981, Appendix A: 11,35.Ashton, L., Manager for Government MedicalAccounts, General Electric Medical, Washington,DC, personal communication, Aug. 11, 1983.Axelson, P., Consultant, Washington, DC, per-sonal communication, May 1983. Axelson, P., U.S. Veterans Administration Re-habilitation Research and Development Center,Palo Alto, CA, personal communication, July1983.Banta, H. D., Behney, C. J., and Willems, J. S.,Toward Rational Technology in Medicine,Springer series on Health Care and Society, vol.5 (New York: Springer Publishing Co., 1981).Bazel, C. G., Program Analyst, U.S. VeteransAdministration, Rehabilitation R&D Program,Washington, DC, personal communication, Oct.24, 1983.Becker, R., Lehn, R., Zarlango, P., and Kruger,D., “Hospitals and Government Agencies, ” inPrinciples of Pharmaceutical Marketing (3d ed.),Mickey Smith (cd. ) (Philadelphia: Lea & Fabiger,1983), at 301-340.Bellanca, T., Vice President, Mennen Medical,Buffalo, NY, personal communication, August1983.Benson, T., Marquette Electronics, Marquette,WI, personal communication, Aug. 15, 1983.Bialys, S., U.S. Veterans Administration, Hines,IL, personal communication, May 1983.Booker, H., U.S. Veterans Administration,Washington, DC, personal communications, No-vember 1982, April 1984, and November 1984.Bradburd, R., Veterans Administration Procure-ment and the Market for Medical Equipment,background paper prepared for the Office ofTechnology Assessment, U.S. Congress, Wash-ington, DC, 1983.Breslar, J., U.S. Veterans Administration, Wash-ington, DC, personal communications, May andJune 1983.Chase, J. D., Chief Medical Director, letter to theNational Academy of Sciences, in U.S. Congress,Senate Committee on Veterans’ Affairs, “Vet-erans Administration’s Response to the Study of
17.
18.
19.
20.
21.
22.
23.
24,
25.
26.
27.
28.
29.
30.
31.
Health Care for American Veterans,” a reportprepared by the Veterans Administration (Wash-ington, DC: U.S. Government Printing Office,Sept. 22, 1977).Cole, D., Product Manager for HemodialysisEquipment, Extracorporeal Co., King of Prussia,PA, personal communication, Oct. 11, 1983.Cook, C., U.S. Veterans Administration, Wash-ington, DC, personal communication, December1982.Coombs, F., U.S. Veterans Administration, Wash-ington, DC, personal communication, January1983.Cucinella, M., Director of National Accounts,Spacelabs, Inc., Chatsworth, CA, personal com-munication, Sept. 28, 1983.Cumming, J., National Accounts, Xonics Corp.,Chicago, IL, personal communication, August1983.Custis, D., U.S. Veterans Administration, Wash-ington, DC, personal communication, Novem-ber 1983.Disabled American Veterans, “Background Infor-mation on the DAV . . . “ news release, Wash-ington, DC, August 1982.Downs, F., U.S. Veterans Administration, Wash-ington, DC, personal communication, Novem-ber 1982 and June 1983.Engel, F., National Accounts, CGR Corp.,Baltimore, MD, personal communication, Aug.15, 1983.Erlangel, H. S., et al., Institute for Research onPoverty, University of Wisconsin, Madison, WI,“Disability Policy: The Parts and the Whole, ” un-published paper, August 1979.Evans, C. C., Holden, F., and Speight, J., “ADRG Based Resource Allocation System for theVeterans Administration,” Allocation Develop-ment Service, U.S. Veterans Administration, un-published paper, 1983.Evans, C. C., U.S. Veterans Administration,Allocation Development Service, Washington,DC, personal communication, March 1984.Farrow, S. C., Kaluzny, A. D., and Ricketts, T.,“Proceedings of a Conference on Health ServicesResearch Issues in the Veterans Administration,”J. Medical Systems 5(1/2):1-16, 1981.Giannini, M., U.S. Veterans Administration,Washington, DC, personal communication, No-vember 1982.Goldschmidt, P. G., “Health Services Researchand Development in the Veterans Administra-
103

104
32.
33.
34.
35.
36.
37,
38.
39.
40.
41.
42.
43.
44.
45.
46.
tion, ” paper presented at the ll0th AnnualMeeting of the American Public Health Associa-tion, Montreal, Quebec, Canada, Nov. 17, 1982.Goldschmidt, P. G., U.S. Veterans Administra-tion, Washington, DC, personal communication,January 1983.German, D., Administrative Assistant, DisabledAmerican Veterans, Washington, DC, personalcommunications, June 16, 1983, and Nov. 1,1983.Grace Commission, President’s Private SectorSurvey on Cost Control: Task Force Report onthe Veterans Administration, draft, Washington,DC, May 17, 1983.Greene, R., U.S. Veterans Administration, Med-ical Research Service, “A Veterans Administra-tion Nuclear Magnetic Resonance Center, ”memorandum to ACOS for Research and Devel-opment, U.S. Veterans Administration, Washing-ton, DC, 1983.Greene, R., U.S. Veterans Administration, Wash-ington, DC, personal communication, June 1983.Hart, R., Director of Government and Regula-tory Affairs, Technicare Corp., Cleveland, OH,personal communication, October 1983.Hartley, K., and Hutton, J., The Economics ofthe U.K. Medical Equipment Market, Universityof York, England, unpublished, October 1982.Hlinovsky, V., Assistant to the National ServiceDirector, Paralyzed Veterans of America, Wash-ington, DC, personal communication, June I5,1983.Holder, J., Division Chief, Radiological and Nu-clear Equipment and Supplies Division, VAMKC,Hines, IL, personal communication, Aug. 31,1983.Hotchkiss, R., Consultant, Washington, DC, per-sonal communication, December 1982.Hullihen, C. R., National Accounts, Picker In-ternational, Cleveland, OH, personal communi-cation, September 1983.Humphreys, H., U.S. Veterans AdministrationMedical Center, Washington, DC, personal com-munication, June 1983.IMS America, Ltd., Veterans AdministrationPrice Analysis of Hospital Supply and Phar-maceutical Products, Order No. TE-Q1-83,Rockville, MD, May 5, 1983.Juarbe, F., Director, National Veterans Service,Veterans of Foreign Wars of the United States,Washington, DC, personal communication, Oct.24, 1983.Kahn, A., Applied Electronic Consultants, Inc.,Washington, DC, personal communication, Oc-tober 1982.
4 7
48.
49.
50
51
52
53
54
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
Kaiser, R., Advisory Contracts Specialist, FSSDivision, VAMKC, Hines, IL, personal commu-nication, Aug. 31, 1983.King, W., Manager for Government Business,Philips Medical Systems, Inc., Springfield, VA,personal communication, Aug. 15, 1983.Kodl, T, Contracting Officer, FSS Division,VAMKC, Hines, IL, personal communication,Oct. 11, 1983.Kolledge, B., U.S. Veterans Administration Re-habilitation Engineering Center, New York, NY,personal communication, June 1983.Kreitner, K., U.S. Veterans Administration Med-ical Center, Palo Alto, CA, personal communi-cation, July 1983.Lewis, J., “National Science and Technology Pol-icy: Its Impact on Technological Change, ” Re-search Management (20):13-16, January 1977.Liefer, L., U.S. Veterans Administration Reha-bilitation Research and Development Center,Palo Alto, CA, personal communication, July1983.Lykins, J., U.S. Veterans Administration, Mar-keting Center, Hines, IL, personal communica-tion, May 1983.Martin, A., National Accounts, Technicare Ultra-sound, Rolling Meadows, IL, personal commu-nication, October 1983.Marx, J. L., “NMR Opens a New Window Intothe Body, ” Science 210(4467):302-305, Oct. 17,1980.McKinsey & Co., Serving as a National Resourcefor Evaluating Hospital Supplies and Equipment:Teams Progress Report to the Chief Medical Di-rector, Hines, IL, Mar. 20, 1974.Miller, J. A., “Cell-e-vision,” Science News119(15):234-238, Apr. 11, 1981.Morrone, F., U.S. Veterans Administration,Health System Planning Service, Washington,DC, personal communication, June 1983.Mussman, L., National Accounts Manager, Ad-vanced Technology Laboratories, Bellevue, WA,personal communication, Oct. 12, 1983.Muthard, J. E., “Putting Rehabilitation Knowl-edge to Use, ” Rehabilitation Monograph No. 11(Gainesville, FL: University of Florida Rehabilita-tion Research Institute, 1980), as cited in (109).National Academy of Sciences, Health Care forAmerican Veterans, prepared for the Committeeon Veterans Affairs, U.S. House of Representa-tives, Committee Print No. 36 (Washington, DC:U.S. Government Printing Office, 1977).The New Columbia Encyclopedia (New York:Columbia University Press, 1975).Nolan, R., U.S. Veterans Administration, Office

105
65.
66.
67.
68<
69.
70.
71,
72.
73,
74.
75.
76.
77.
78.
79.
80.
81.
of Budget and Finance, Washington, DC, person-al communication, September 1983.Over, A. M., Jr., et al., “A Model of the Demandfor Durable Medical Equipment, ” submitted tothe Health Care Financing Administration, De-partment of Health, Education, and Welfare,March 1980.Palmer, F., Chief, Testing and Evaluation Divi-sion, VAMKC, Hines, IL, personal communica-tion, Aug. 31, 1983.Palmer, F., U.S. Veterans Administration Mar-keting Center, Hines, IL, personal communica-tion, May 1983.Paralyzed Veterans of America, “Paralyzed Vet-erans of America Annual Report, 1981 -1982,”Washington, DC, 1982.Parthenon Insurance Co., “Product Standardiza-tion, ” unpublished report, June 1983.Passamaneck, D. J., National Legislative Direc-tor, AMVETS, Washington, DC, personal com-munication, Oct. 24, 1983.Phillips, L., National Research Director, Para-lyzed Veterans of America, Washington, DC,personal communication, June 3, 1983.Popp, R. L., and Macovski, A., “Ultrasonic Diag-nostic Instruments, ” Science 210(4467): 268-272,Oct. 17, 1980.Press, A., National Accounts, Cobe Laboratories,Denver, CO, personal communications, August,September, and October 1983.Pugh, E., Manager of Government Sales, PickerInternational, Falls Church, VA, personal com-munication, Oct. 12, 1983.Redington, R. W., and Berninger, W., “MedicalImaging Systems,” Physics Today 34(8):36-44,August 1981.Reimers, J., Stanford University, Palo Alto, CA,letter to Dr. Frank Ebaugh, Chief of Staff, Vet-erans Administration Medical Center, Palo Alto,CA, June 29, 1983.Roloff, J., “Sounding Out 3-D Interiors” ScienceNews 123(20):314-319, May 14, 1983.Scherer, F. M., Industrial Market Structure andEconomic Performance, 2d ed. (Chicago, IL:Rand McNally Publishing Co., 1980).Serritelli, S., U.S. Veterans Administration Mar-keting Center, Hines, IL, personal communica-tion, May 1983.Shepard, D. S., and Karen, S. L., The Marketfor Wheelchairs: Innovations and Federal Policy(Health Technology Case Study 30), OTA-HCS-30 (Washington, DC: U.S. Congress, Office ofTechnology Assessment, November 1984).Smith, J., U.S. Veterans Administration, Wash-ington, DC, personal communication, May 1983.
82.
83<
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
Sommer, J. F., Jr., Deputy Director, NationalVeterans Affairs and Rehabilitation Commission,The American Legion, Washington, DC, personalcommunication, July 16, 1983.Stanford University, “Policy on Tangible Re-search Property, ” memo from the Vice Provostand Dean of Graduate Studies and Research tomembers of the Academic Council and membersof the Academic Staff-Research, Mar. 16, 1982.Steinberg, E., and Cohen, A. B., Nuclear Mag-netic Resonance Imaging Technology: A Clini-cal, Industrial and Policy Analysis (Health Tech-nology Case Study 27), OTA-HCS-27 (Washing-ton, DC: U.S. Congress, Office of TechnologyAssessment, September 1984).Stuart, J., Contracting Officer, Radiological andNuclear Equipment and Supplies Division,VAMKC, Hines, IL, personal communication,October 1983.Stuvek, F., National Accounts, Siemens Corp.,Iselin, NJ, personal communication, Sept. 29,1983.Sullivan, B., Director of Federal and CorporateBusiness Division, Diasonics, Milpitas, CA, per-sonal communication, Oct. 12, 1983.Tanenbaum, S. J., The Boston Elbow (HealthTechnology Case Study 29), OTA-HCS-29 (Wash-ington, DC: U.S. Congress, Office of Technolo-gy Assessment, November 1984).The American Legion, “The American Legion:Service to the Community, State and Nation, ”pamphlet, Washington, DC, September 1981.Thompson, F. J., Health Policy and theBureaucracy: Politics and Implementation (Cam-bridge, MA: Massachusetts Institute of Technol-ogy Press, 1981).Thompson, W. W., National Field Service Direc-tor, Blinded Veterans Association, Washington,DC, personal communication, Oct. 18, 1983.Tiedt, R., Manager of Sales Administration,Mennen Medical, Buffalo, NY, personal commu-nication, Sept. 28, 1983.U.S. Bureau of Labor Statistics, Time Series Datafor U.S. Input Output Industries, BLS bulletinNo. 2018 (Washington, DC: U.S. GovernmentPrinting Office, 1979).U.S. Congress, Congressional Budget Office,Human Resources and Community DevelopmentDivision, Veterans Administration Health Care;Planning for 1990 (Washington, DC, February1983).U.S. Congress, Congressional Research Service,Cash and Non-Cash Benefits for Persons WithLimited Income: Eligibility Rules, Recipient, andExpenditure Data, FY1977-79, Report No. 81-44

106
96.
97.
98.
9 9
100.
101.
102.
103.
104.
105
106.
107.
EPW, Washington, DC, Feb. 12, 1981.U.S. Congress, Congressional Research Service,Medical Care Programs of the Veterans Admin-istration, Report No. 83-99 EPW, Washington,DC, May 16, 1983.U.S. Congress, Congressional Research Service,Veterans Administration 1983 Budget, Issue BriefNo. IB82013, Washington, DC, Nov. 18, 1982.U.S. Congress, General Accounting Office, Com-puted Tomographic Scanners: Opportunity forCoordinated Federal Planning Before SubstantialAcquisitions, Report No. HRD-78-41, Washing-ton, DC, Jan. 30, 1978.U.S. Congress, General Accounting Office, Fed-eral Government Still Striving to Establish SingleDrug Procurement System, Report No. HRD-80-59, Washington, DC, June 30, 1980.U.S. Congress, General Accounting Office, VANeeds Better Visibility Over Medical Center Pur-chases, Report No. PSAD 81-16, Washington,DC, Dec. 12, 1980.U.S. Congress, General Accounting Office, Hu-man Resources Division, “VA Needs to ImproveIts Quality Assurance Program for Medical Sup-ply and Equipment Items,” (PLRD-82-44) unpub-lished memorandum report, Washington, DC,Feb. 23, 1982.U.S. Congress, Office of Technology Assessment,Commercial Biotechnology: An InternationalAnalysis, OTA-BA-218 (Washington, DC: U.S.Government Printing Office, January 1984).U.S. Congress, Office of Technology Assessment,The Cost Effectiveness of Digital SubtractionAngiography in the Diagnosis of Cerebrovascu-lar Disease (Washington, DC: U.S. GovernmentPrinting Office, in press).U.S. Congress, Office of Technology Assessment,Development of Medical Technology: Opportu-nities for Assessment, GPO stock No. 052-003-00217-5 (Washington, DC: U.S. GovernmentPrinting Office, August 1976, as amended).U.S. Congress, Office of Technology Assessment,Federal Policies and the Medical Devices Indus-try, OTA-H-230 (Washington, DC: U.S. Govern-ment Printing Office, October 1984).U.S. Congress, Office of Technology Assessment,The Impact of Randomized Clinical Trials onHealth Policy and Medical Practice—BackgroundPaper, OTA-BP-H-22 (Washington, DC: U.S.Government Printing Office, August 1983).U.S. Congress, Office of Technology Assessment,The Implications of Cost-Effectiveness Analysisof Medical Technology, OTA-H-126 (Washing-ton, DC: U.S. Government Printing Office, Aug-ust 1980).
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
U.S. Congress, Office of Technology Assessment,Policy Implications of the Computed Tomogra-phy (CT) Scanner: An Update—Background Pa-per, GPO stock No. 052-003-00793-2 (Washing-ton, DC: U.S. Government Printing Office,1981).U.S. Congress, Office of Technology Assessment,Technology and Handicapped People, GPO stockNo. 052-003-00874-2 (Washington, DC: U.S.Government Printing Office, 1982).U.S. Congress, Office of Technology Assessment,Technology Transfer at the National Institutes ofHealth—A Technical Memorandum, GPO stockNo. 052-003-00869-6 (Washington, DC: U.S.Government Printing Office, 1982).U.S. Congress, Senate Committee on VeteransAffairs, “Veterans’ Disability Compensation andSurvivors’ Benefit Amendments of 1980, ” hear-ing held on June 17, 1980 (Washington, DC: U.S.Government Printing Office, 1980).U.S. Department of Health, Education, and Wel-fare, Office of Human Development Services, Re-habilitation Services Administration, and the Vet-erans Administration, Rehabilitation Engineering:A Plan for Continued Progress (Charlottesville,VA: Rehabilitation Engineering Center, Univer-sity of Virginia, 1978).U.S. Department of Health and Human Services,Rahmoeller, G. A., Director, Division of Cardio-vascular Devices, Bureau of Medical Devices,Food and Drug Administration, “Memorandumon Pacemaker Registry Meeting, ” Washington,DC, Apr. 29, 1981.U.S. Department of Health and Human Services,Office of Health Research, Statistics, and Tech-nology, National Center for Health Statistics, Di-vision of Health Interview Statistics, “Health CareCoverage Under Private Health Insurance, Medi-care, Medicaid, and Military or Veterans Admin-istration Health Benefits: United States, 1978, ”Advance Data, No. 71, DHHS publication No.(PHS) 81-1250, Hyattsville, MD, June 29, 1981.U.S. General Services Administration, FederalStandardization Handbook, Report No. FPMR101-29, Washington, DC, December 1981,U.S. Interagency Agreement between the Veter-ans Administration and the Food and Drug Ad-ministration, #IGA V101(91)P-82OO5, Washing-ton, DC, March 1982.U.S. Office of Management and Budget, Officeof Federal Procurement Policy, A Guide for theAcquisition and Distribution of CommercialProducts, pamphlet No. 2, Washington, DC,April 1980.

107
118.
119.
120.
121
122,
123.
124.
125.
126.
127.
128.
129.
130.
131.
U.S. Veterans Administration, 2981 Annual Re-port, Washington, DC, 1982.U.S. Veterans Administration, 2982 Annual Re-port, Washington, DC, 1983.U.S. Veterans Administration, Assistant Inspec-tor General for Auditing, “Report of Audit: Pro-curement and Monitoring of Pacemakers, ” Proj-ect No. 101A-79-42, Feb. 13, 1980.U.S. Veterans Administration, Brief of Office ofProcurement and Supply, unpublished, Washing-ton, DC, December 1982.U.S. Veterans Administration, Department ofMedicine and Surgery, Chief Medical Director’sLetter on “Medical Center ADP Planning andProcurement Package,” #10A3D, Washington,DC, May 1983.U.S. Veterans Administration, Department ofMedicine and Surgery, “Chief Medical Director’sPreface to Strategic Outlook, ” draft 5, version 2,Washington, DC, May 11, 1983.U.S. Veterans Administration, Department ofMedicine and Surgery, letter to Honorable AlanK. Simpson, Chairman, Senate Committee onVeterans Affairs, concerning the VA Rehabilita-tion Engineering Center, Washington, DC, May12, 1983.U.S. Veterans Administration, Department ofMedicine and Surgery, Minutes of the ProstheticTechnology Evaluation Committee Meeting,Washington, DC, Feb. 26, 1983.U.S. Veterans Administration, Department ofMedicine and Surgery, Office of the Chief Medi-cal Director, “Department of Medicine and Sur-gery Organization—Oct. 1, 1982, ” Washington,DC, Oct. 1, 1982.U.S. Veterans Administration, Department ofMedicine and Surgery, Prosthetic and SensoryAids Service, Veterans Administration Prostheticand Sensory Aids Program Since World War II(Washington, DC: U.S. Government Printing Of-fice, 1977).U.S. Veterans Administration, Marketing Cen-ter, “Experimental Technology and Incentive Pro-gram in the Veterans Administration: 1975-1981,”unpublished internal document, Hines, IL, 1982.U.S. Veterans .4dministration, Marketing Cen-ter, Federal Supply Schedule Solicitation for Of-fers for 1984, document #M4-Q-38-83, Hines, IL,1983.U.S. Veterans Administration, Marketing Cen-ter, Office of the Director, “Procedural GuidelineNumber 11,” Hines, IL, May 9, 1983.U.S. Veterans Administration, Marketing Cen-ter, Radiological and Nuclear Equipment and
132,
133,
134.
135,
136.
137,
138,
139,
140<
141,
142.
143.
144.
145,
Supplies Division, unpublished data, Hines, IL,1983,U.S. Veterans Administration, Marketing Cen-ter, Radiological and Nuclear Equipment andSupplies Division, unpublished information fromvendors’ 1982 contracts, Hines, IL, 1983.U.S. Veterans Administration, Marketing Cen-ter, sample memorandum on “1 Year Follow-upEvaluation on Product, ” Hines, IL, no date.U.S. Veterans Administration, Marketing Cen-ter, “Testing and Evaluation Staff: OrientationBriefing for the Director, ” Hines, IL, December1979.U.S. Veterans Administration, Marketing Cen-ter, vendors’ responses to the Federal SupplySchedule Solicitation for Offers for 1984, docu-ment #M4-Q-38-83, Hines, IL, 1983.U.S. Veterans Administration, Medical DistrictInitiated Program Planning: Guidance for thePreparation of Medical District Plans, vol. 1,Washington, DC, June 1983.U.S. Veterans Administration, Office of Budgetand Finance, Congressional Budget Submission,Washington, DC, 1983.U.S. Veterans Administration, Office of Inspec-tor GeneraI, “Audit of Prosthetics DistributionCenter, Denver, Colo., ” Report No. 3R5-A22-052, Washington, DC, Mar. 16, 1983.U.S. Veterans Administration, Office of inspec-tor General, Office of Audit, Report of Audit:VA Rehabilitation Engineering Center, NewYork, N. Y., project No. lR2-007, unpublished,Washington, DC, Feb. 25, 1982.U.S. Veterans Administration, Office of Planningand Program Evaluation, The Automobile andAdaptive Equipment Program: A Program Eval-uation, Washington, DC, 1981.U.S. Veterans Administration, Office of Planningand Program Evaluation, Blind RehabilitationProgram Evaluation, Washington, DC, February1982.U.S. Veterans Administration, Office of Planningand Program Evaluation, Medical Research Pro-gram Evacuation, Washington, DC, Aug. 24,1981.U.S. Veterans Administration, Office of Planningand Program Evaluation, Prosthetic TreatmentProgram Evaluation, November 1979.U.S. Veterans Administration, Office of Planningand Program Evaluation, Rehabilitative Engineer~ing Research and Development Program Evalua-tion, Washington, DC, August 1981.U.S. Veterans Administration, Office of Planningand Program Evaluation, Spinal Cord Injury Pro-
108
146.
147.
148.
149.
150,
151,
152.
153.
154.
gram Evaluation, Washington, DC, July 1979.U.S. Veterans Administration, Office of Procure-ment and Supply, Could You Use a MultibillionDollar Customer?: VA Invites You to SubmitYour Product or Service, Information BulletinNo. 90-4, Washington, DC, June 1982.U.S. Veterans Administration, Office of Procure-ment and Supply, “Evaluation of New Products, ”Washington, DC, Jan. 13, 1983.U.S. Veterans Administration, Office of Procure-ment and Supply, “Multiple Award Federal Sup-ply Schedule: 65 II F,” Washington, DC, Sept.3, 1982.U.S. Veterans Administration, Prosthetic andSensory Aids Service, unpublished internal docu-ment, 1983.U.S. Veterans Administration, Rehabilitation Re-search and Development Service, “Agency Brief-ing Package 1981, ” unpublished, 1981.U.S. Veterans Administration, Rehabilitation Re-search and Development Service, “Annual Report1982, ” unpublished, 1982.U.S. Veterans Administration, Rehabilitation Re-search and Development Service, “Briefing for theAdministrator Designee, ” unpublished, 1982.U.S. Veterans Administration, Rehabilitation Re-search and Development Service, “Briefing for theService Director Designee, ” unpublished, 1981.U.S. Veterans Administration, Rehabilitation Re-search and Development Service, “Developmentand Evaluation Program, ” Washington, DC,1983.
0
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
U.S. Veterans Administration, Special CentralOffice Advisory Group, A Report on the Evalua-tion of Computerized Tomography (CT) UnitsWithin the Veterans Administration Hospitals,Washington, DC, 1978.U.S. Veterans Administration, VA Manual MP-2, Chapter E, Change 64, “Initiation of Field Test-ing,” Washington, DC, Apr. 1, 1971.U.S. Veterans Administration, VA Manual MP-2, Subchapter E, Change 155, Subpart 108-26.51—Requisitions to Central Office, Washington, DC,Oct. 14, 1982.U.S. Veterans Administration, VA OrganizationManual M-00-1, Change 11, p. X-74, Washing-ton, DC, July 30, 1981.“VA Prosthetics . . . A Lack of Training, ” DA VMagazine 24(5):8-9, May 1982.“VA Prosthetics . . . Some Recommendations, ”DAV Magazine 24(8):8-9, August 1982.Vale, S. A., Acting Executive Director, BlindedVeterans Association, Washington, DC, personalcommunication, July 12, 1983.Woosley, N., National Service Director,AMVETS, Washington, DC, personal commu-nication, July 16, 1983.Wright, D., U.S. Veterans Administration, Re-habilitation Engineering Center, New York, NY,personal communication, June 1983.Wyant, D., Prosthetics and Sensory Aids Serv-ice, U.S. Veterans Administration, Washington,DC, personal communication, October 1982,May 1983, and October 1983.
INFORMATION CENTER
OFFICE OF TECHNOLOGY ASSESSMENT