medical simulation 3.0
TRANSCRIPT

Medical Simulation 3.0: Improving Patient Safety and Healthcare Delivery Transformation
Yue Dong, M.D.

Disclosures
• The views and opinions are expressed in following presentations are presenters’ own, not representative of Mayo Clinic, Society of Simulation of Healthcare(SSH), Healthcare Systems Modeling and Simulation Affinity Group (HSMSAG)
• Faculty and organizing committee do not endorse or recommend any specific products or services mentioned on this presentation.
• Faculty and organizing committee do not have any personal financial interest related to the presentation.

©2011 MFMER | 3123886-3

Mayo Clinic Core Value :
Quality (Outcome + Safety + Service)
Value =Cost per over time
Smoldt RK, Cortese DA. Pay-for-performance or pay for value? Mayo Clinic Proceedings 2007;82:210-3
“The needs of the patient come first.”

Surgical never events and contribution human factors
Mayo Clinicroughly 1 in every 22,000 procedures
National Practitioner Data Bank1 in every 12,000 procedure
Thiels CA, et al. Surgery 2015 May 29 http://www.ncbi.nlm.nih.gov/pubmed/26032826

Minnesota Adverse Events 2015
©2011 MFMER | 3123886-6

Rates of All Harms, Preventable Harms, and High-Severity Harms per 1000 Patient-Days, Identified by Internal and External Reviewers, According to Year
Landrigan CP et al. N Engl J Med 2010;363:2124-2134
Rates of All Harms, Preventable Harms, and High-Severity Harms per 1000 Patient-Days, Identified by Internal and External Reviewers, According to Year
Landrigan CP et al. N Engl J Med 2010;363:2124-2134

Healthcare systems safety • 400,000 Americans
die each year as a result of medical errors. (3rd after heart disease and cancer)
• $765 billon (35%) US healthcare cost is wasted each year
• US annual healthcare cost more than $ 3 trillion (16% GDP)
James JT. Journal of Patient Safety 2013;9:122-128; CDC.gov; http://resources.iom.edu/widgets/vsrt/healthcare-waste.html


ICU as Systems of Systems
Adopted from: Network medicine--from obesity to the "disease". Barabási AL., N Engl J Med. 2007 Jul 26;357(4):404-7.
SHOCKDIC AKI
ALI
Physician RTPharmacist
Nurse
Time
Bas
elin
e
Patie
nt O
utco
me,
Pr
ovid
er S
atis
fact
ions

Learning Healthcare Systems• Significant changes in the health
care delivery system, changes largely concerned with organization• quality improvement• operational efficiency• error reduction and patient safety
IOM. The Learning Healthcare System: Workshop Summary. Washington, DC: The National Academies Press; 2007.

“Blue Highways” on the NIH Roadmap
Practice-basedresearch
Phase 3 and 4 clinicaltrialsObservational studiesSurvey research
Basic scienceresearch
Preclinical studiesAnimal research
Human clinicalresearch
Controlledobservational studiesPhase 3 clinical trials
T1Case series
Phase 1 and 2clinical trials
Clinical practice
Delivery of recommendedcare to right pt at right timeIdentification of new clinicalquestions and gaps in care
T2
Translationto humans
T2Guideline
developmentMeta-analyses
Systematicreviews
Translationto patients
T3Dissemination
researchImplementation
research
Translationto practice
Westfall JM et al: JAMA 297:403, 2007
Bench Bedside Practice

The Science of Healthcare Delivery
• Understanding disease biology
• Finding effective therapies
•Therapies delivered effectively

2011, Health IT and Patient Safety: Building Safer Systems for BetterCare, Committee on Patient Safety and Health Information Technology; Institute of Medicine

What is simulation? • Simulation is the imitation or
representation of one act or system by another.
• Healthcare simulations have four main purposes – education, assessment, research, and health systems integration to facilitate patient safety…

©2011 MFMER | 3123886-16
Society for Simulation in Healthcare

SSH Membership Continuing Growth
17
2005 2006 2007 2008 2009 2010 2011 2012 20130
500
1000
1500
2000
2500
3000
3500
180
539
1205
15201702
1850
2438
2925 2918

History of medical simulation
1026宋代针灸铜人1969SimOneDr. Abrahamson

Simulation 1.0
Education Assessment
Systems Integration
Research
Simulation

Mayo Clinic Multidisciplinary Simulation Center

Ultrasound guided central line insertion

Precourse- literature review Precourse exam (Online)
Cadaver lab (Procedural Skills Lab) (1 hour)
Ultrasound hands-on station (1 hour)
Gown/Gloving/Universal Precautions(1 hour)
Certification Station (following with feed back)
Briefing
Expe
rienc
eDebriefing
Lear
ning
goa
l driv
en
Central Line Workshop
Courtesy of William Dunn, MD

Clinical competence
Met
ric a
sses
smen
t
Time
Traditional training
Safety standard
Simulation-based training
Simulation-based objective assessment Discern Clinical Proficiency in Central Line Placement, Dong, et. al, CHEST 2010

©2011 MFMER | 3123886-24

©2011 MFMER | slide-25
WHO Global Priorities for Patient Safety Research
Bates DW, et al. Global priorities for patient safety research. BMJ 2009;338:b1775

ED Trauma Team Training
©2011 MFMER | 3123886-26

Learning Objective
Faculty Development
Curriculum
Facility and Technology
Assessment
Debriefing
Simulation based education
Learners

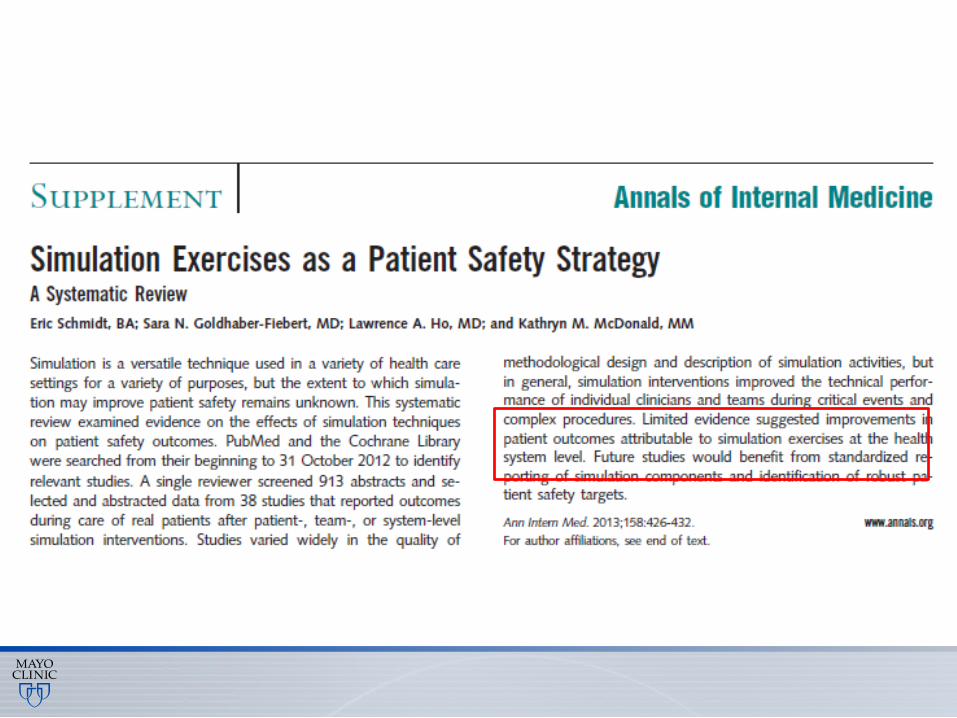
Key questions for SBT? • Does the simulation-based education work• How does simulation compare with other
instructional approaches? • Why are some simulation interventions better
than others (and how can we improve them all)?
• Is simulation-based education worth its costs?
David Cook, The literature on healthcare simulation education: What does It show ? http://webmm.ahrq.gov/perspective.aspx?perspectiveID=138#ref8


ROI of Simulation based training
• Approximately 9.95 CRBSIs were prevented among MICU patients with CVCs / year
• Cost of CRBSI were $82,000 in 2008 dollars and 14 additional hospital days (including 12 MICU days).
• Cost of the simulation-based education $112,000.
• 7 to 1 rate of ROI
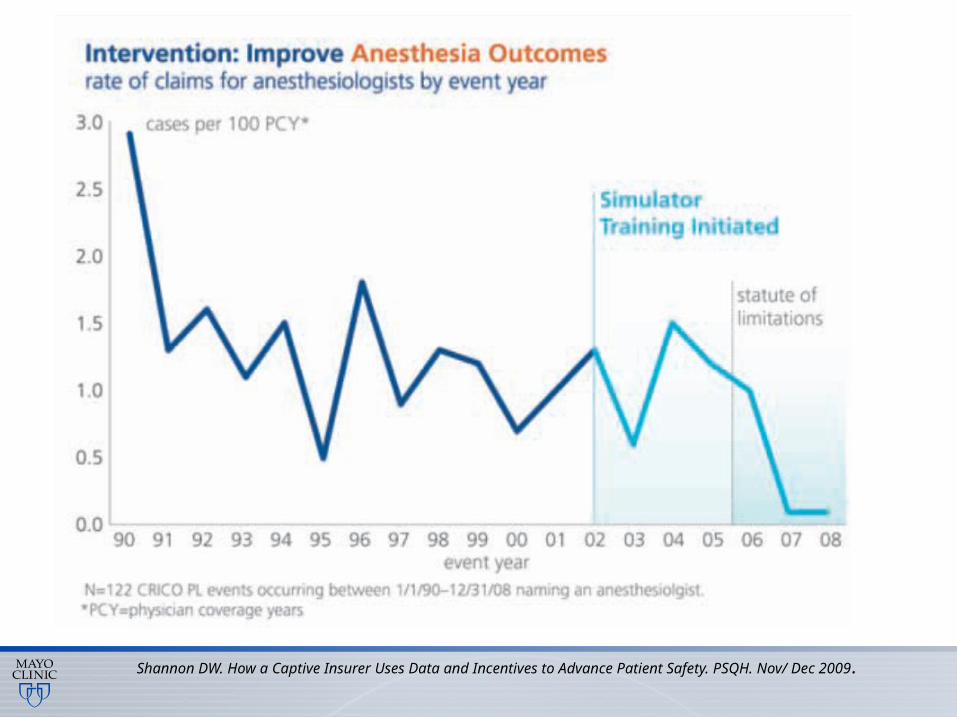
Shannon DW. How a Captive Insurer Uses Data and Incentives to Advance Patient Safety. PSQH. Nov/ Dec 2009.

Simulation 1.0
©2011 MFMER | 3123886-32
Education Assessment
Systems Integration
Research
Simulation

©2011 MFMER | 3123886-33
Five steps to develop checklists for evaluating clinical performance: An integrative approach 。 Schmutz J, Eppich WJ, Hoffmann F, Heimberg E, Manser T. Academic Medicine. 2014 Jan;89(7):996-1005

Central Line Procedure Checklist
Simulation-based objective assessment Discern Clinical Proficiency in Central Line Placement, Dong, et. al, CHEST 2010

©2011 MFMER | slide-35
Simulation-based objective assessment Discern Clinical Proficiency in Central Line Placement, Dong, et. al, CHEST 2010

Short-term and Long-term Impact of the Central Line Workshop on Resident Clinical Performance During Simulated Central Line Placement 。 Laack, Dong, et al. Simulation in Healthcare 9 (4), 228-233

“Medicine used to be simple, ineffective and relatively safe. Now it is complex, effective and potentially dangerous” Sir Cyril Chantler

Information overload
2012, IOM, Discussion Paper1: The Clinical Trials Enterprise in the United States: A Call for Disruptive Innovation

The Complexities of Physician Supply and Demand: Projections Through 2025. 2008 AAMC http://www.aamc.org/workforce
“ Simply educating and training more physicians will not be enough to address theseshortages. Complex changes such as improving efficiency, reconfiguring the way some services are delivered and making better use of our physicians will also be needed.”

Simulation 2.0
©2011 MFMER | 3123886-41
Education Assessment
Systems Integration
Research
Simulation

Human Factor Research• Using simulation as a tool to study human
performance variation under different “stress conditions” (fatigue, cognition, workload, etc.)
• conduct usability testing of devices instrument and processes

The effect of drug concentration expression on epinephrine dosing errors: a randomized trial
Wheeler DW, Carter JJ, Murray LJ, Degnan BA, Dunling CP, Salvador R, et al.. Ann Intern Med 2008;148:11-4.
(1 mg in 1 mL) (1 mL of a 1:1000 solution)

Arriaga AF, Bader AM, Wong JM, et al. Simulation-based trial of surgical-crisis checklists. N Engl J Med 2013;368:246-253

Ahmed, et al. Critical Care Medicine, 39(7) 1626-1634
The effect of two different electronic health record user interfaces on intensive care provider task load, errors of cognition, and performance

Simulation 3.0
©2011 MFMER | 3123886-46
Education Assessment
Systems Integration
Research
Simulation

Dr. Lucian Leape Dr. Donald M. Berwick
Transforming healthcare: a safety imperative
L Leape, D Berwick, C Clancy, et al. Qual Saf Health Care 2009; 18:424-428


A technical systems grow in complexity and connectedness, inevitably will lead to accidents with catastrophic potential
• the degree of system complexity
• tight coupling of processes, • and the inability of a single
individual or small group of individuals to manage all the potential interactions
• Stochastic escalation
©2011 MFMER | 3123886-49
Perrow, C. Living with high-risk technologies. Princeton University Press: John Wiley and Sons Ltd; New Jersey: 1999.

What is system integration ?

Caffezo, et al rom discovery to design, Human factor in healthcare, 2012


Modeling Complexity (Rouse, 2007)
“ Starting with this model of the enterprise, the overarching strategy should focus on increasing complexity where it can be managed best and decreasing complexity for end users.”

Adjust structure and process to eliminate or minimize risks of health care-associated injury, before they have an adverse event-impact on the outcomes of care
Donabedian. Evaluating of Medical Care. The Milbank Memorial Fund Quarterly, Vol. 44, No. 3, Pt. 2, 1966 (pp. 166–203)

Systems Engineering Initiative for Patient Safety (SEIPS) Work system design for patient safety: the SEIPS model.Carayon P, et al . Qual Saf Health Care. 2006 Dec;15 Suppl 1:i50-8. Review.

Simulation, modeling and Analysis, Law and Kelton, 2000

Robert Pool, Science, Vol. 256, No. 5053 (Apr. 3, 1992)
“ Computation has become a ‘third branch’ of science, alongside theory and experiment”


McDonnell , G. (July, 2007).Workshop on Multiscale Modeling using AnyLogic 6 with Health Examples at International System Dynamics Society Conference. Boston, MA
Simulation Application in Healthcare

Operation Research using DES (Discrete Event Simulation)
1. Formulate the research question2. Define the operational process (workflow)3. Collect date to fit distribution4. Construct and validate the model5. Run experiment
©2011 MFMER | 3123886-60


Crit Care Med 2007 Vol. 35, No. 11
Critical Importance of Timing

Spain Study
Ferrer R, et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008;299(19):2294-2303.

Research Methodology
Baseline Process
Identify Causes of Delay
Process Modeling
Suggestions for Improvement
Measure ImpactSensitivity Analysis
Statistical Analysis
Root Cause Analysis &FMEA
Discrete-EventSimulation
ANOVADesign of Experiment
User Requirement and Scope

Workflow analysis by providers

Data Collection• Time frame
• Dec 2007 to June 2009• Sample size:
• 600 sepsis patients• Source of data
• Sepsis QI Project (Courtesy of Dr. Afessa)• EMR: ICU Datamart• Direct observations: CVC, fluid infusion, etc.• Expert opinions: MD, RN, RT, Pharmacist, et al• Administration database
• Obstacles with data• Uncompleted dataset• Care process variation

Fellow ResidentConsultant PharmacistBedside RN
Sepsis Recongnition
Antibiotics/Source Control
Fluid Resuscitation
Central Venous Catheterization
Vesopressor Administration
Inotrope Administration
Transfusion
Patient
Sep
sis
Res
usci
tatio
n G
oal R
each
ed
Simulation Modeling of Healthcare Delivery During Sepsis Resuscitation
Dong Y, et al. Optimization of healthcare delivery during sepsis resuscitation by simulation and modeling. Simulation in Healthcare 2010;5:423.

Accelerated T&X
CVC Efficiency
ScVO2
Monitors
No CXR DelayEarly Recognition
ResuscitationRecognition
Sepsis Care Optimization by Discrete Event Simulation (S-CODES)

Model ValidationEmpirical
DataModel Data
% Variance
Duration (months) 18 18 0%Total Sepsis Patients
597 600 0.5%
Average number of patients/day
2.4 2.7 -1.3 %
Average Cycle Time (min)
382 418 9.4 %

Sepsis Resuscitation Time Reduction by Different OptionsClinical Data
Sepsis Resusiation Time Reducation by Different Options
29.16 26.81
7.81
137.92
16.11
55.94
0.00
30.00
60.00
90.00
120.00
150.00
Opt 1 - Early Recog Opt 2 - Quick CVC Opt 3 - No X-Ray Opt 4 - PreType/Cross
Opt 5 - ScVO2Monitors
Opt 6 - All
Tim
e (m
in)
DES study in clinical practices
• Analyze & Visualize patient flow (Batarseh 2014)
• Optimize unit bed capacity (Zhu 2012)
• Forecast near-future operation status (Hoot 2009)
• Study interaction between providers (Lim 2013)
• Evaluate ED/EMS interaction (Stahl 2003)
• Decrease inpatient boarding (Levin 2008)
©2011 MFMER | 3123886-71


Recent Major Reports
• Executive Office of the President President’s Council of Advisors on Science and Technology: Report To The President Better Health Care And Lower Costs: Accelerating Improvement Through Systems Engineering (May 2014)
• National Science Foundation: Operations Research - A Catalyst for Engineering Grand Challenges (May 2014) • The ASQ Healthcare Division Marshall Plan: "Put Me In The Game, Coach! ” (The Quality Management Forum, Winter 2014)

Simulation to improve quality and safety
Constructive
Virtual
Live
Training
Assessment
Research and Integration
Patient
Healthcare Providers
Healthcare Systems
©2011 MFMER | 3123886-76


Learning from others

Summary• Quality and patient safety are the
driver for value based healthcare delivery
• Use more simulation to • Improve provider and team skills • Improve systems performance

From Mayo Clinic Center for Innovation

Healthcare Systems Modeling & Simulation Affinity Group
goo.gl/PRIkog
goo.gl/0r5mOs
http://www.ssih.org/Interest-Groups/Healthcare-Systems-Modeling-Simulation
goo.gl/7QuuQd