medicaladministration fsa/hra administration care
TRANSCRIPT

MEDICAL ADMINISTRATIONFSA/HRA ADMINISTRATIONCARE MANAGEMENTSTOP LOSSTHE HEALTH CARE PARTNERSHIP
DATE
FORM H: Quest ionnai re
Pro ject Number: 16-01-07
DRAFT

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 1

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 2
I. SCOPE OF SERVICES1 . 1 M E D I C A L A D M I N I S T R A T I O N
· Onshore (U.S.) administration of claims processing, member services, provider services and all aspects ofmedical administration
· Benefit determination, coordination of benefits and appeals (including external review)· Managed care network services· Provider contractual negotiations, including pay for performance· Custom network development, maintenance and operation· Full claims fiduciary· Acceptance of electronic eligibility file from district or its third party designate· Health care medical management services· Disease management services· Transplant benefit management services including transplant access program (Transplant
Centers of Excellence Network)· Specialty resource centers – Cancer, Neonatal, Reproductive resource services, Kidney resource,
Maternity, and outline others as applicable· Enhanced clinical review/hi-tech radiology· Claim recovery services (overpayments and adjustment services due to coordination of benefits,
retroactive termination, audits [hospital, DRG, high cost drugs], duplicate bills and contractcompliance)
· Escheat services· Subrogation services· 24/7 nurseline resource center· Claim abuse and fraud management services· Assistance with general plan administration· Claim accounting, draft reconciliation and provider 1099 reporting· Claim systems production and development· Account Management Services:
o On-site supporto Enrollment meeting supporto Enrollment kitso Administration of account structure (premium and claims accounts for reporting purposes)o Administration of employer site to review billing, enrollment and claimso ID card productiono Administration of alternate ID’so Electronic eligibility processing both manual and tape processingo Ability for employer or designated third party to make online eligibility updateso Underwriting services (including projections and reserve estimates)o Customer reporting system administrationo Access to customized ad-hoc reporting and provision of ad-hoc hours bank

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 3
o Claims processing, medical claim review, coordination of benefitso Access to member services toll free 800# as well as member portal to access claim
status, eligibility, plan features, physician/facility look up, transparency tools and onlinehealth information, including web based & mobile
o Preparation and communication of annual accounting package· Production of Summary Plan Descriptions and Summary of Benefits & Coverage (SBC’s)· Shared services and facility Reasonable & Customary R&C) payment schedules – out of network
contractual discount negotiation services – or carve out of such services· Administration of a fee schedule based on Medicare allowable for out-of-network claims· Administration of online participant website, enabling access to online providers, member claims,
member explanation of benefits (EOBs), personal health records· Development of customized explanation of benefits (EOBs)· Access to stop loss management services, including reporting to a third party vendor, if selected· Billing and eligibility services· Billing reconciliation services· Administration, including payout if applicable, of plan performance guarantees· Administration of allowances including but not limited to communication, MWBE, investment
dollars, audits· Plan sponsor reporting, including quarterly “stop light” dashboard as well as annual reporting· Plan sponsor banking services (self-funded only)· Run out administration services· Plan audit services, including internal audits and cooperation with external audits· SOC 1/ SSAE administration audit reports· Wellness incentive support and administration· Medicare secondary payer reporting· Provider network management reporting (including premium designation)· Predictive modeling services· Mental health network management services· Precertification, utilization review and case management services· Large claims review support· Integration of pharmacy third party claims data to support benefit accumulators as well as
predictive modeling· Access to online discount program· Reporting to designated data warehouse· Implementation and ongoing support of single sign on (SSO)· Compliance with current and evolving legislation including but not limited to, the Patient Protection
and Affordable Care Act, HIPAA, GINA, Mental Health Parity, ERISA
1 . 2 F S A / H R A A D M I N I S T R A T I O NF S A A D M I N I S T R A T I O N
· Section 125 Flex plan administration

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 4
· Creation of FSA plan documents· Record keeping for FSA transaction and overall plan sponsor accounting· Administration of plan reimbursements to plan participants (claims processing)· Employer plan sponsor reporting including banking, transactions etc.· Administration of forfeited funds· Administration of plan audits· Administration of member communication materials· Administration of plan compliance and plan sponsor legislative updates· Administration of plan overpayments· Administration of non-discrimination testing· Administration and distribution of FSA debit cards· Establishment of employer sponsored plan asset accounts· Administration of plan set up, web enrollment maintenance, administration of deposits· Administration and support of non-discrimination testing
HRA ADMINISTRATION
· Record keeping for HRA transaction and overall plan sponsor accounting· Administration of fund allocation and health incentives· Administration of plan reimbursements to plan participants (claims processing and order of
reimbursement account, i.e. HRA, FSA.)· Employer plan sponsor reporting including available funds, transactions etc.· Administration of plan audits, and cooperation with third party audits· Administration of member communication materials· Administration of plan compliance and plan sponsor legislative updates· Administration of plan overpayments· Creation of HRA plan document· Administration of plan set up, including rollover to next plan year
1 . 3 C A R E M A N A G E M E N TFor the purposes of this RFP “Care Management “includes Disease Management (DM), CustomCare Management (CCM), and Case Management. Disease Management services consists ofinteractive communication between an individual and a health professional or expert systemthrough various modalities (e.g., telephonic, email, online, face-to-face, etc.), to address individualswith chronic conditions, typically those who are moderate to low chronically ill. Conditionsaddressed might include (but are not limited to) asthma, COPD, CHF, CAD, depression, diabetes,maternity, obesity, etc. Custom Care Management is defined as a customized program thatproactively outreaches and manages the highest risk/cost patients. Expertise in conditions such ascancer care, neonatology, maternal health, renal disease & behavioral/mental health are useful.Includes a dedicated nurse for employees, addresses gaps in care, consists of an integratedmedical team, has extended phone hours and measurable referrals and/or warm transfers to othervendor partners. CCM utilizes evidence based best practices in counseling and support. Casemanagement is the process of assessment, planning, facilitation, care coordination, evaluation,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 5
and advocacy for options and services to meet an individual’s health needs, promoting cost-effective treatments and quality outcomes.
1 . 4 S T O P L O S S· Administration of individual excess risk benefit level (specific stop loss/ISL) which includes all
services as outlined in the Summary Plan Description· Reimbursement of stop loss triggers above the ISL level· Tracking and payment of individual/specific stop loss claims· Administration of aggregate stop loss factors (ASL) inclusive of the same benefits as listed in the
first bullet· Administration of annual aggregate attachment point and tracking· Underwriting services for annual renewal of stop loss and factors· Payment of ISL and/or ASL stop loss claims· Clinical evaluation of large claimants· Option to include prescription drug benefits in both specific (individual) and aggregate stop loss
coverage· Development of policy that outlines coverage and premiums in effect during any given policy year

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 6
II. INTRODUCTION TO QUESTIONNAIRE
2 . 1 E X P L A N A T I O N T O P R O P O S E R SAny Proposer who desires an explanation or interpretation of the RFP and its related documents, or whodiscovers any discrepancies or omissions in the RFP or related documents, shall notify the designatedHISD Project Manager in writing. Each notification must make specific reference to the applicable sectionof the RFP (e.g., Section, Page Number, and quote from RFP document) to be considered by HISD. HISDreserves the right to reject any request that does not conform to these instructions. Oral explanations orinstructions provided will not be binding. Any information given to a Proposer concerning the RFP may befurnished in writing promptly to all other potential Proposers as an addendum to the RFP, if thatinformation is necessary in submitting offers, or if the lack of it would be prejudicial to any otherProposers.
All communications regarding this RFP must be coordinated through the HISD Project Manager named inSection 1.1.4/1.1.5 – Instruction Submission Requirements and Procedures. Failure to do so may result indisqualification of the Proposer from further consideration.
AddendaThe only method by which any requirement of this RFP may be modified is by written addendum issuedby the Procurement Services Department. All addenda will be posted on the HISD ProcurementServices’s Proposal Solicitations Download website. For more information go to www.houstonisd.org andfind the link under Community > Do Business with HISD > Bid Opportunitieshttp://www.houstonisd.org/Page/68148.
If an addendum to the proposal document is a result of a pre-proposal conference, the District will post theaddendum, within a reasonable time, following the conference to the HISD Proposal SolicitationsDownload website. The District is not responsible if a Proposer does not receive the proposal revision intime to include the information with the proposal submission. Proposals may not be considered if they donot include written information additionally requested in addenda that may be issued regarding the project.If a Proposer does not have access to the internet, a copy of the addenda may be secured in theProcurement Services Department. The department is located in the Hattie Mae White EducationalSupport Center, 4400 West 18th Street, Level 2NE, Houston, Texas 77092. Department business hoursare 8 AM to 5 PM Central Time, Monday – Friday (excluding District holidays).
Copies of any Addenda will be cross posted on ProposalTech.
ExceptionsIf any exceptions are taken to any portion of this RFP, the Proposer must clearly indicate the exceptiontaken and include a full explanation as a separate attachment to the proposal. The failure to identifyexceptions or proposed changes will constitute acceptance by the Proposer of the RFP as proposed bythe District. The District reserves the right to reject a proposal containing exceptions, additions,qualifications, or conditions.
Information to Be Requested from ProposerTo achieve a uniform review process and obtain the maximum degree of comparability, it is required thatproposals be organized in the manner specified.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 7
The table below provides a listing of all parts of this RFP. You will need to ensure that you received eachof these parts to confirm that your proposal is complete and meets all submission requirements.
Proposers must submit one copy of FORM H: Questionnaire, and any referenced supplementalmaterial online through ProposalTech. Failure to include supplemental material, where requestedwithin the questionnaire, could negatively impact your score.
Each proposer must submit hardcopies/binders including their questionnaire and supplementalmaterial along with the other required attachments to the addresses listed in Section 2.3. Form Hquestions must be submitted electronically through Proposal Tech (www.proposaltech.com). Paperonly copies of the RFP questionnaire will not be accepted.
If electronic submissions are password protected, please provide the password for access inbound proposal marked “ORIGINAL”, on the inside cover. Please respond to requests forinformation by submitting your responses in a binder with tabs labeled as indicated in thefollowing table. A demonstration of how to use Proposal Tech will be presented at the Pre-proposal Conference on February 15, 2016; 1-3pm, Hattie Mae White Educational Support CenterRoom 2E26, 4400 West 18th Street, Houston, Texas 77092. Should you need further support onthe Proposal Tech software during the RFP process, please contact Proposal Tech support [email protected] or 877-211-8316 option 4 for the support team.
Please see the table below for a list of items and their required submission format:Description Exhibit
(Letters)Census Data AClaims Data BDisruption Request CGeo Access Request DCurrent Fees E
(HISD, AISD, KISD)Top 25 Conditions F
(HISD, AISD, KISD)Plan Designs G
(HISD, AISD, KISD)Stop Loss Designs H
(HISD, AISD)HISD HIPAA Business Associate Agreement I
Description Proposer’s Order ofDocuments
Submission Mode
Title Page - Transmittal Letter & Executive SummaryTable of Contents Tab 1 Paper Copy ONLYProposal Submission Forms (HISD FORMS A-G) Tab 2
Company Information Form A Paper Copy ONLYMWBE Attachment Form B Paper Copy ONLYAddendum for Agreement Funded by US Federal Grant Form C Paper Copy ONLYPricing and Service Affirmation Form D Paper Copy ONLYException Form Form E Paper Copy ONLYPrice Schedule Form F Electronic submission via
Proposal TechSupplier Relations Form G Paper Copy ONLY
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 8
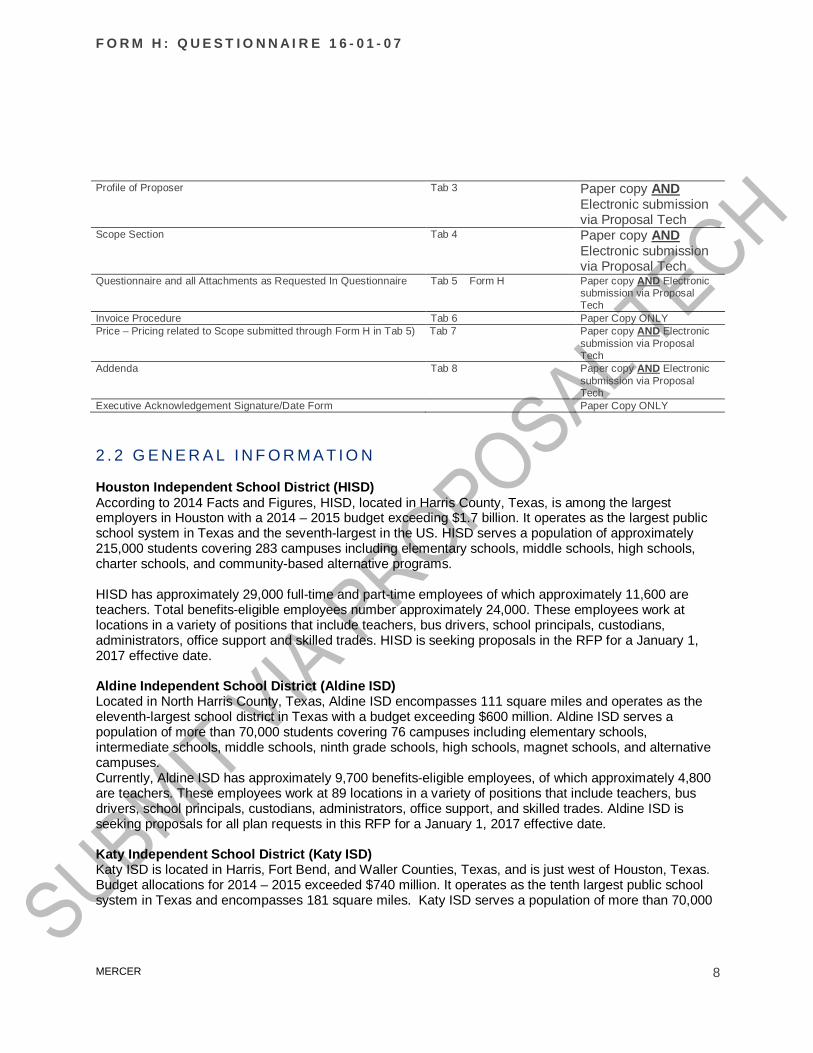
Profile of Proposer Tab 3 Paper copy ANDElectronic submissionvia Proposal Tech
Scope Section Tab 4 Paper copy ANDElectronic submissionvia Proposal Tech
Questionnaire and all Attachments as Requested In Questionnaire Tab 5 Form H Paper copy AND Electronicsubmission via ProposalTech
Invoice Procedure Tab 6 Paper Copy ONLYPrice – Pricing related to Scope submitted through Form H in Tab 5) Tab 7 Paper copy AND Electronic
submission via ProposalTech
Addenda Tab 8 Paper copy AND Electronicsubmission via ProposalTech
Executive Acknowledgement Signature/Date Form Paper Copy ONLY
2 . 2 G E N E R A L I N F O R M A T I O N
Houston Independent School District (HISD)According to 2014 Facts and Figures, HISD, located in Harris County, Texas, is among the largestemployers in Houston with a 2014 – 2015 budget exceeding $1.7 billion. It operates as the largest publicschool system in Texas and the seventh-largest in the US. HISD serves a population of approximately215,000 students covering 283 campuses including elementary schools, middle schools, high schools,charter schools, and community-based alternative programs.
HISD has approximately 29,000 full-time and part-time employees of which approximately 11,600 areteachers. Total benefits-eligible employees number approximately 24,000. These employees work atlocations in a variety of positions that include teachers, bus drivers, school principals, custodians,administrators, office support and skilled trades. HISD is seeking proposals in the RFP for a January 1,2017 effective date.
Aldine Independent School District (Aldine ISD)Located in North Harris County, Texas, Aldine ISD encompasses 111 square miles and operates as theeleventh-largest school district in Texas with a budget exceeding $600 million. Aldine ISD serves apopulation of more than 70,000 students covering 76 campuses including elementary schools,intermediate schools, middle schools, ninth grade schools, high schools, magnet schools, and alternativecampuses.Currently, Aldine ISD has approximately 9,700 benefits-eligible employees, of which approximately 4,800are teachers. These employees work at 89 locations in a variety of positions that include teachers, busdrivers, school principals, custodians, administrators, office support, and skilled trades. Aldine ISD isseeking proposals for all plan requests in this RFP for a January 1, 2017 effective date.
Katy Independent School District (Katy ISD)Katy ISD is located in Harris, Fort Bend, and Waller Counties, Texas, and is just west of Houston, Texas.Budget allocations for 2014 – 2015 exceeded $740 million. It operates as the tenth largest public schoolsystem in Texas and encompasses 181 square miles. Katy ISD serves a population of more than 70,000
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 9
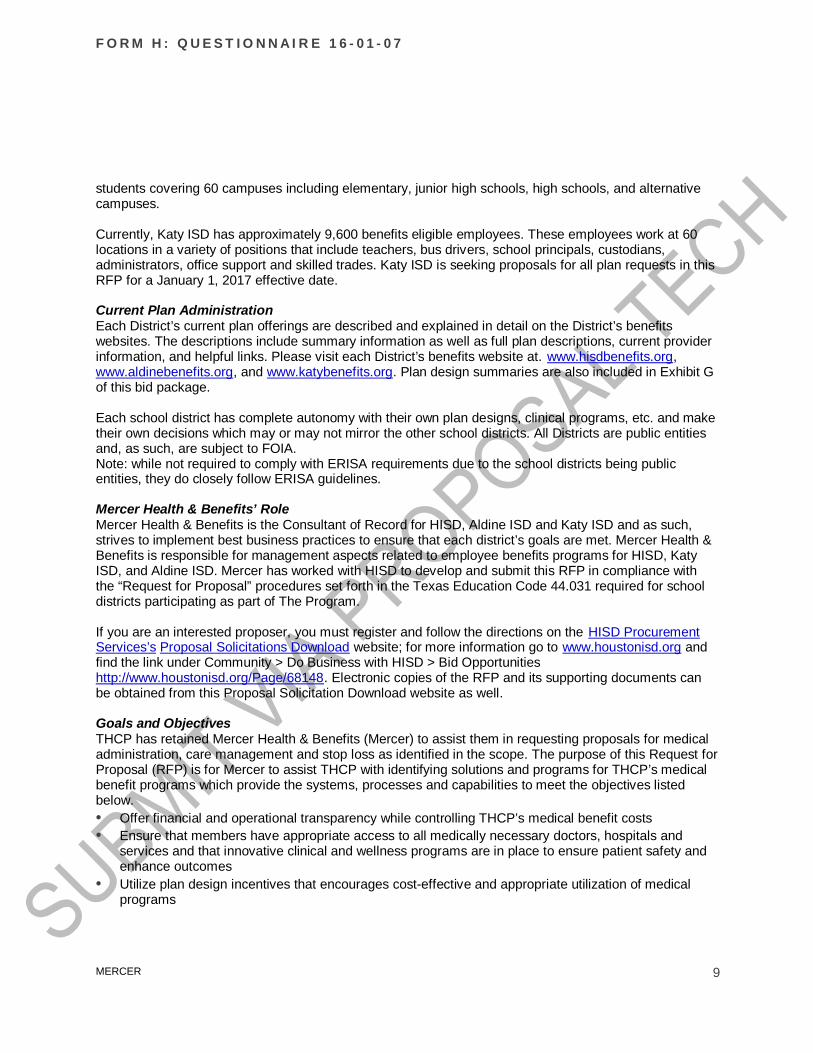
students covering 60 campuses including elementary, junior high schools, high schools, and alternativecampuses.
Currently, Katy ISD has approximately 9,600 benefits eligible employees. These employees work at 60locations in a variety of positions that include teachers, bus drivers, school principals, custodians,administrators, office support and skilled trades. Katy ISD is seeking proposals for all plan requests in thisRFP for a January 1, 2017 effective date.
Current Plan AdministrationEach District’s current plan offerings are described and explained in detail on the District’s benefitswebsites. The descriptions include summary information as well as full plan descriptions, current providerinformation, and helpful links. Please visit each District’s benefits website at. www.hisdbenefits.org,www.aldinebenefits.org, and www.katybenefits.org. Plan design summaries are also included in Exhibit Gof this bid package.
Each school district has complete autonomy with their own plan designs, clinical programs, etc. and maketheir own decisions which may or may not mirror the other school districts. All Districts are public entitiesand, as such, are subject to FOIA.Note: while not required to comply with ERISA requirements due to the school districts being publicentities, they do closely follow ERISA guidelines.
Mercer Health & Benefits’ RoleMercer Health & Benefits is the Consultant of Record for HISD, Aldine ISD and Katy ISD and as such,strives to implement best business practices to ensure that each district’s goals are met. Mercer Health &Benefits is responsible for management aspects related to employee benefits programs for HISD, KatyISD, and Aldine ISD. Mercer has worked with HISD to develop and submit this RFP in compliance withthe “Request for Proposal” procedures set forth in the Texas Education Code 44.031 required for schooldistricts participating as part of The Program.
If you are an interested proposer, you must register and follow the directions on the HISD ProcurementServices’s Proposal Solicitations Download website; for more information go to www.houstonisd.org andfind the link under Community > Do Business with HISD > Bid Opportunitieshttp://www.houstonisd.org/Page/68148. Electronic copies of the RFP and its supporting documents canbe obtained from this Proposal Solicitation Download website as well.
Goals and ObjectivesTHCP has retained Mercer Health & Benefits (Mercer) to assist them in requesting proposals for medicaladministration, care management and stop loss as identified in the scope. The purpose of this Request forProposal (RFP) is for Mercer to assist THCP with identifying solutions and programs for THCP’s medicalbenefit programs which provide the systems, processes and capabilities to meet the objectives listedbelow.• Offer financial and operational transparency while controlling THCP’s medical benefit costs• Ensure that members have appropriate access to all medically necessary doctors, hospitals and
services and that innovative clinical and wellness programs are in place to ensure patient safety andenhance outcomes
• Utilize plan design incentives that encourages cost-effective and appropriate utilization of medicalprograms

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 10
• Provide members with a better understanding of the true costs of medical care borne/incurred on theirbehalf
• Leverage new approaches to managing THCP medical utilization and cost trends and provide qualitydecision support to its benefits group
• Coordinate with other THCP providers (pharmacy benefit manager, Condition Management firms,etc.) on health improvement and patient education initiatives
• Ease the administrative burden and complexity of the program while maintaining program quality,breadth, and cost effectiveness
Current StateEach district’s self-funded medical plans are currently administered by Aetna. Each District offers similarconsumer-directed health plan options and less similar EPO, PPO, and POS options. Aetna also currentlyadministers the district’s Flexible Spending and Health Reimbursement Accounts. The self-fundedprescription drug plans are administered by Express Scripts, and feature a number of utilizationmanagement programs, and similar plan designs which vary by District. Aetna currently providesNurseline and Maternity care services. Viverae is currently providing lifestyle and condition managementfor Aldine ISD and Katy ISD. All 3 Districts provide employees with a health portal powered by Viveraewhich contains consumer engagement tools, informational resources, and single sign on access for mostproviders who require authentication. HISD currently maintains two (2) on-site clinics with servicesprovided by Concentra. More detail on each program is available on each District’s website atwww.hisdbenefits.org, www.aldinebenefits.org, or www.katybenefits.org.
Current THCP Vendor PartnersAldine ISD HISD Katy ISD
Medical Aetna Aetna AetnaPBM Express Scripts Express Scripts Express ScriptsStop Loss Aetna Aetna N/AHealth Advocacy Aetna Aetna AetnaCase management Aetna Aetna Aetna24 Hour Nurseline Aetna Aetna AetnaEAP Not offered Aetna ValueOptions (Beacon Health)Health Assessment Viverae Viverae ViveraeWeb portal Viverae Viverae ViveraeLifestyle managementprograms (online & telephonic)
Viverae Not offered Viverae
Condition Management Viverae Not offered ViveraeIncentive Administration Viverae Viverae ViveraeOn-site clinics Not offered Concentra Not offeredExpert Medical Consultation Best Doctors Advance Medical Not offered
RFP ProcessThe RFP process will provide you approximately three (4) weeks to complete your proposal. Mercer willassist the districts in evaluating the proposals based on District criteria and priorities and presentsummary results to the Districts and their insurance committee members (varies by District). The Districtswill determine finalists and may or may not invite finalists in for finalist interviews. The Districts may ormay not desire site visits with any or all of the finalists. Administration and committee recommendationswill be presented to the Boards of Education for contract awards. It is preferred for contract drafts to benegotiated prior to the Board approval.
Please keep the following in mind as you develop your proposal.
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 11
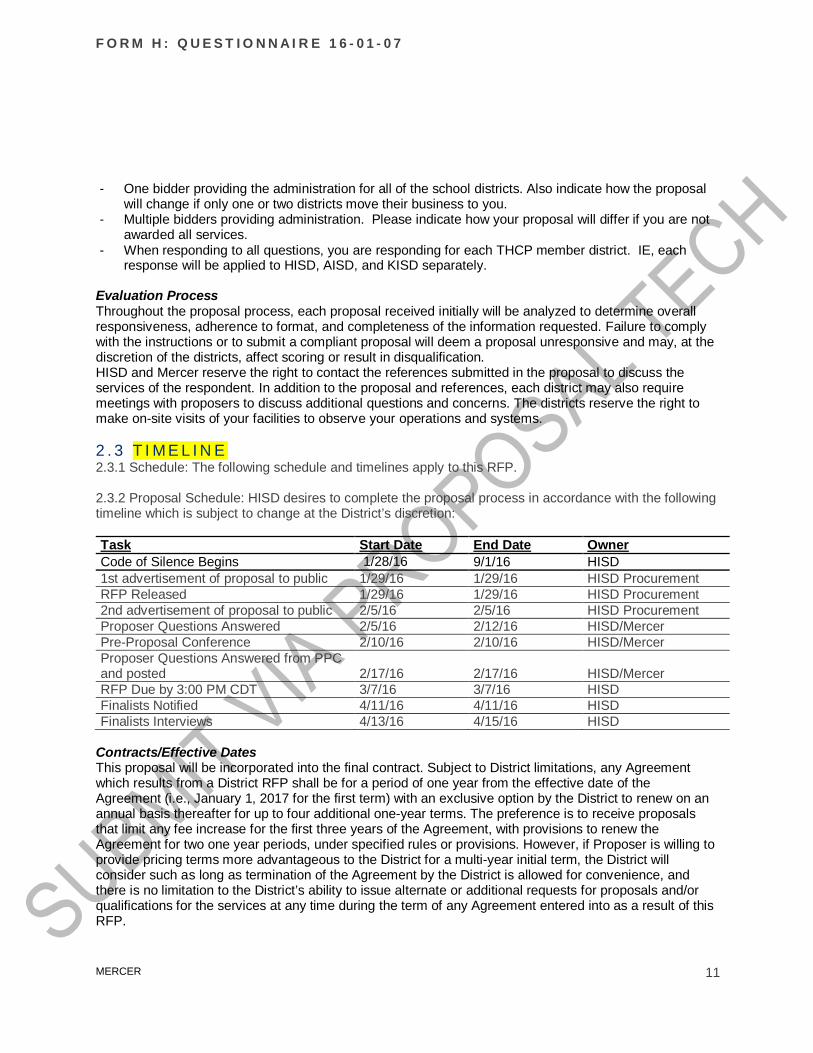
- One bidder providing the administration for all of the school districts. Also indicate how the proposalwill change if only one or two districts move their business to you.
- Multiple bidders providing administration. Please indicate how your proposal will differ if you are notawarded all services.
- When responding to all questions, you are responding for each THCP member district. IE, eachresponse will be applied to HISD, AISD, and KISD separately.
Evaluation ProcessThroughout the proposal process, each proposal received initially will be analyzed to determine overallresponsiveness, adherence to format, and completeness of the information requested. Failure to complywith the instructions or to submit a compliant proposal will deem a proposal unresponsive and may, at thediscretion of the districts, affect scoring or result in disqualification.HISD and Mercer reserve the right to contact the references submitted in the proposal to discuss theservices of the respondent. In addition to the proposal and references, each district may also requiremeetings with proposers to discuss additional questions and concerns. The districts reserve the right tomake on-site visits of your facilities to observe your operations and systems.
2 . 3 T I M E L I N E2.3.1 Schedule: The following schedule and timelines apply to this RFP.
2.3.2 Proposal Schedule: HISD desires to complete the proposal process in accordance with the followingtimeline which is subject to change at the District’s discretion:
Task Start Date End Date OwnerCode of Silence Begins 1/28/16 9/1/16 HISD1st advertisement of proposal to public 1/29/16 1/29/16 HISD ProcurementRFP Released 1/29/16 1/29/16 HISD Procurement2nd advertisement of proposal to public 2/5/16 2/5/16 HISD ProcurementProposer Questions Answered 2/5/16 2/12/16 HISD/MercerPre-Proposal Conference 2/10/16 2/10/16 HISD/MercerProposer Questions Answered from PPCand posted 2/17/16 2/17/16 HISD/MercerRFP Due by 3:00 PM CDT 3/7/16 3/7/16 HISDFinalists Notified 4/11/16 4/11/16 HISDFinalists Interviews 4/13/16 4/15/16 HISD
Contracts/Effective DatesThis proposal will be incorporated into the final contract. Subject to District limitations, any Agreementwhich results from a District RFP shall be for a period of one year from the effective date of theAgreement (i.e., January 1, 2017 for the first term) with an exclusive option by the District to renew on anannual basis thereafter for up to four additional one-year terms. The preference is to receive proposalsthat limit any fee increase for the first three years of the Agreement, with provisions to renew theAgreement for two one year periods, under specified rules or provisions. However, if Proposer is willing toprovide pricing terms more advantageous to the District for a multi-year initial term, the District willconsider such as long as termination of the Agreement by the District is allowed for convenience, andthere is no limitation to the District’s ability to issue alternate or additional requests for proposals and/orqualifications for the services at any time during the term of any Agreement entered into as a result of thisRFP.
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 12
At the District’s option, there may be an additional 90-day transitional period added to the term at the endof the Agreement. The Agreement prices, terms and conditions are to remain in effect during thetransitional period.Any change in rates will occur on January 1 and will need to be documented. Written notification of apremium/fee change will be presented to HISD at least 10 months prior to the anniversary date for HISD’sconsideration.
Mercer CompensationMercer will be performing the RFP evaluation in order to provide recommendations and advise eachdistrict. Mercer is compensated on a fee-for-service basis by the districts. Please delete any and allconsultant/advisor compensation from your quoted premiums/fees. Should any embedded compensationbe included that cannot be removed, it should be clearly disclosed as part of your proposal.
Best and finalTHCP reserves the right to return to the top candidates to request a best and final proposal based on oneor more components of the initial proposal; however, this does not guarantee that you will be given anyopportunity to adjust your submitted proposal. HISD reserves the right to negotiate certain terms andconditions relative to the contract. All finalist(s) are advised that HISD will require submission of M/WBEparticipation compliance documentation.
2 . 4 I N S T R U C T I O N S2.4.1 General InstructionsYour response should include sufficient information for full analysis of each strategy or solution you areproposing. Include a full description of how the solution or strategy works, the supporting network ofproviders, network access fees, other program fees, any IT development costs, file feeds, etc.), potentialsavings (including information on how the potential savings projections were derived), savingsguarantees. Understand that THCP employers will negotiate collectively but will contract individually withthe service provider;- Provide responses to the individual Districts and Mercer as instructed;- Conform to the rule that there are to be no calls to HISD, KISD, AISD or Mercer. All
information/questions are to be sent as instructed within this RFP. Failure to comply can result indisqualification; and
- Submit questions as instructed within this RFP. Any information given to one prospective Proposerwill be furnished to all if such information is necessary to Proposer in submitting their proposal or ifthe lack of such information would be prejudicial to an uninformed Proposer.
ExhibitsExhibit A - CensusExhibit B – Claims DataExhibit C – Disruption RequestExhibit D – Geo Access RequestExhibit E – Current FeesExhibit F – Top 25 ConditionsExhibit G – Plan DesignsExhibit H – Stop Loss ProvisionsExhibit I – HISD HIPAA Business Associate Agreement

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 13
Exhibit J – Current Integration Status
Proposal Submission ProcessAll proposers are to complete all sections of the RFP for which they are proposing to provide services.The omission of any section should be clearly outlined in the cover letter of their proposal along with briefexplanation as to why your organization is not submitting responses for a particular section.
In addition to the provisions set forth in Section 1.5 (HISD’s RFP / Submission of Proposals), you mustsubmit one signed original, one electronic copy (ProposalTech), and one hard copy with an electroniccopy included of your proposal to the following: Deyen Greene-Evans Houston Independent School District Board Services - Room 1C03 Hattie Mae White Education Support Center 4400 West 18th Street Houston, Texas 77092-8501
You must submit one signed original, one electronic copy (ProposalTech), and four hard copies (whichalso include an electronic copy of your full submission) of your proposal to the following:
Ms. Keena Sims-Bradley Director of Benefits Aldine Independent School District 15010 Aldine Westfield Road Houston, Texas 77032
You must submit one signed original, one electronic copy (ProposalTech), and one hard copy (which alsoincludes an electronic copy of your full submission) of your proposal to the following:
Mr. Lance Naumann Katy Independent School District Insurance/Risk Management Office 6301 South Stadium Lane Katy, TX 77494
Each proposal shall be in a sealed envelope plainly marked “SEALED PROPOSAL” – Benefits Manager:Request for Proposals to include the company name and address of Proposer. Each original proposalshall be marked “ORIGINAL” to be distinguished from the copies. If electronic copies are passwordprotected, provide the password in the front cover of each proposal binder marked “ORIGINAL”.
PROPOSALS MUST BE SUBMITTED PRIOR TO 3:00 PM CDT ON FRIDAY, March 7, 2016 ASDIRECTED ABOVE. NO ORAL, TELEGRAPHIC, TELEPHONIC, OR FACSIMILE PROPOSALS WILLBE CONSIDERED.For hand-delivered proposals, it will be the sole responsibility of the proposer to have its proposalenvelope date and time stamped before the deadline. Proposal envelopes received after March 7, 2016,3:00 PM CDT deadline will neither be date/time stamped or accepted.
Notice of delaysWhen the Proposer encounters difficulty which delays or threatens to delay timely performance (including

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 14
actual or potential labor disputes), the proposer shall immediately give notice thereof in writing to eachmember of HISD, stating all relevant information with respect thereto. Such notice shall not in any wayconstitute a basis for an extension of the delivery or performance schedule or be construed as a waiver byHISD of any right or remedies to which it is entitled by law or pursuant to provisions herein. Failure to givesuch notice, however, may be grounds for denial of any request for an extension of the delivery orperformance schedule because of such delay.
Force majeureProposer shall not be liable for delay in delivery or performance or for failure to give notice of delay whensuch delay is due to factors beyond its control, including, but not limited to, fires, strikes, explosions,governmental regulations, court orders or decrees, or acts of nature such as flood, wind, earthquake,tornado, or hurricane. If the proposer is unable to perform any of its obligations as a result of forcemajeure, the proposer shall immediately give written notice to HISD of the date of inception of the forcemajeure condition and the extent to which it will impact performance.
Questions from ProposersAll responses to the RFP must be prepared in accordance with the proposal format set forth herein inaddition to the provisions set forth in Section 1 (HISD’s RFP / Instructions, Submission Requirements andProcedures).
Proposers may make written inquiries concerning this RFP to obtain clarification of the requirements.Inquiries must be submitted no later than 5:00 PM CDT on February 10, 2016. Inquiries should besubmitted to the following via email: Deyen Greene-Evans Procurement Department Houston Independent School District Fax: (713) 556-6641 Email to: [email protected]
Questions received by this deadline, and corresponding answers, will be provided by issuance of writtenaddenda.All proposers are expected to carefully examine the RFP documents. Any ambiguities or inconsistenciesshould be brought to the attention of the individual identified above. It is believed that all informationnecessary to complete a response is included in this RFP. It is the responsibility of the proposer to obtainclarification of any information contained herein that is not fully understood either through the writtenquestion process or at the pre-proposal conference.
Description of proposed itemsIn Section 1.2 (HISD’s RFP / Notice for RFP / Instructions Submission Requirements and Procedure),detailed listings of proposal items have been provided.
QuestionnairesThe questionnaires will verify the proposer’s ability and willingness to meet various requirements andexpectations about the services that you will provide to this district under this contract. It will verify specificaspects of the services you will perform. Failure to respond affirmatively to all confirmations does notdisqualify a vendor.
Confidentiality Statement

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 15
You are required to sign an HISD Confidentiality Statement which can be obtained through HISDProcurement Services’s Proposal Solicitations Download website; for more information go towww.houstonisd.org and find the link under Community > Do Business with HISD > Bid Opportunitieshttp://www.houstonisd.org/Page/68148. This form must be completed and returned to procurement priorto the release of any data.
Responding to the RFPTo respond to this RFP, you are required to have a personal computer with internet access, MS Office(Microsoft Word and Excel), and respond via the methods mentioned above. You will access the RFPfrom ProposalTech using the link on HISD’s website: http://www.houstonisd.org/Page/68148.Your intent to bid will be confirmed through ProposalTech. If you decline to bid, please include yourreasoning.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 16
III. QUOTED LINE OF COVERAGEPlease check the box(es) below for the line(s) of coverage you intend to bid. Note, all respondents willbe required to provide responses to all questions in Section IV – General Questions. If aquestion is not applicable to the line of coverage in which you are bidding, please mark thequestion No, and provide a response as to why in the explanation.
o Medical Administrationo FSA/HRA Administrationo Care Managemento Stop Loss

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 17
IV. GENERAL QUESTIONNAIREYou are required to respond to all questions in this section, even if you do not bid for all lines of coveragelisted requested in this questionnaire. When responding to all questions, you are responding for eachTHCP member district. IE, each response will be applied to HISD, AISD, and KISD separately.
4 . 1 G E N E R A L I N F O R M A T I O NAll proposers must complete this general portion of the RFP.
Responses1. What is the legal name of your organization as it should appear on the contract?
2. Until what date is your proposal valid (must be January 1, 2017 or later)?
3. With the exception of insured risks, will you extend similar proposal terms and conditions to other publicentity clients who may join THCP?
4. What is your company’s financial rating according to the following:• Standard & Poor's• Moody's• A.M. Best
5. Will you act in accordance with the documents and instruments governing our clients’ plans and complywith all applicable state and federal laws and regulations including, but not limited to, the following?Please respond to the following:• Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985 (Select)• Employee Retirement Income Security Act (ERISA) of 1974 (instructive only; THCP plans are not
subject to ERISA)(Select)
• Health Insurance Portability and Accountability Act (HIPAA) of 1996 (and all subsequentamendments, including the HITECH act, including the nondiscrimination, special enrollment,coverage certification, privacy, security, Electronic Data Interchange (EDI), and other HIPAArequirements
(Select)
• Mental Health Parity Act of 1996 (Select)• Newborns and Mothers? Health Protection Act of 1996 (Select)• The Women’s Health and Cancer Rights Act of 1998 (Select)
6. To the extent applicable, are you now and will you remain duly licensed and in full compliance with allfederal and state statutory administrative requirements?
(Select)
7. You have provided a redlined contract for the Districts review as Attachment S4: A – Sample Contract.You agree that the terms and conditions in this sample will be acceptable to your organization in theagreement reached with the District(s). You have included the requirements in Section 2 in your samplecontract.
(Select)
8. You will agree to carry insurance with responsible insurance carriers acceptable to each district and withminimum limits of liability coverage as stated below, for each district, against claims for damages causedby bodily injury, including death, to employees, and claims for property damage.· You shall furnish certificates of insurance to the districts indicating compliance with the coverage
listed in chart below.· This insurance should be maintained in full force and effect throughout the duration of the Service
Agreement. In the event that it is not commercially feasible to maintain insurance the periodrequired by the Agreement, you shall supply the districts with equivalent assurance to the requiredinsurance, acceptable to the districts.
· The districts shall be named as an additional insured on the automobile and commercial generalliability policy. The districts shall be named as an alternate employer on the workers’ compensationpolicy. A waiver of subrogation shall be issued in favor of the districts in the workers’compoensation, automobile and commercial general liability policies.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 18
· You shall provide the districts with original certificates of insurance, acceptable to the districts.Insofar as allowed by law, such certificates shall indicate an agreement by each carrier not to cancelcoverage without providing a minimum of thirty (30) days prior written notice
· In the event there is a deductible on any policy, you shall provide evidence the satisfaction of thedistrict, upon the district’s request, that it is able to satisfy the deductible.
Type of coverage Minimum Limitsa. Workers’ Compensation and Employer’s
LiabilityStatutory$100,000 per accident
b. Automobile Liability:Bodily Injury & Property Damage for allowned, non-owned vehicles and hiredvehicles
$1,000,000 Combined Single Limit
c. Commercial General Liability $1,000,000 Combined Single Limitd. Professional Liability $5,000,000 per person/per incidente. Cyber/Privacy/Security Insurance
Covering unauthorized release or Acess topersonally identifiable information
$5,000,000 per incident
Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
10. Your organization currently has more than three employer clients who have more than 10,000employees with programs in place for more than two years.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
11. You agree that THCP reserves the right to retain third party contractor(s) (DesignatedAgent(s)) to receive claims/utilization information and/or data (Data) from Supplier and storethe data on HISD's behalf.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
12. THCP shall put in place policies and procedures to protect the confidentiality of the Dataconsistent with HIPAA (and all applicable amendments) requirements. You agree that you willbe required to do the same, including the execution of a Business Associate Agreement whereapplicable.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
13. All file layouts will be according to Health Insurance Portability and Accountability Act (HIPAA)standard Electronic Data Interchange (EDI) 834 format, no additional fees will be applied fordata manipulation for inbound/outbound files.
Single, Radio group.1: Agree,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 19
2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
14. Bidder currently meets HIPAA safe harbor requirements.Single, Radio group.1: Agree,2: Disagree, please explain: [ 500 words ]
15. Do you encrypt PHI according to National Institute of Standards and Technology (NIST)guidelines?Single, Radio group.1: Yes,2: No, please explain: [ 50 words ]
16. Do you agree to the template Business Associate Agreement (BAA) as provided as Exhibit I –HISD HIPAA Business Associate Agreement .1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
17. THCP shall have the annual right to evaluate key pricing terms (e.g. administrative and clinicalprogram fees) and all other terms with a financial impact (e.g., service performance guarantees,trend management guarantees) to ensure that pricing remains competitive in the marketplacethroughout the contract term.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
18. Subcontractor disclosure: Agent, subsidiary, affiliate, and vendor agree to disclose allsubcontractor relationships that will be used in the performance of services for THCP. Duringthe contract period, vendor will notify HISD at least 90 days in advance of any changes to theprovision of services by agent, subsidiary, an affiliate, or to its subcontracted relationships. Thisshould include any off-shore or domestic subcontracted relationships for member, physician,pharmacist, or other support. THCP will have the right to approve or reject any subcontractor oragent change.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
19. You agree not to pay brokerage/agent fees, including overrides.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
20. If you disagree to question 19, confirm that these fees can be broken out from your pricing as a separateline item.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 20
3: Disagree (explain): [ Unlimited ]
4 . 2 C O M P A N Y - S P E C I F I C I N F O R M A T I O NGeneral information questionnaire Response1. What is the name of your organization?2. What is the name of your parent organization?3. Please provide the following information about your company:
• Address• City• State• ZIP code• Telephone number
• Fax number
• General e-mail address• Web address
• Internal identification code for this offering
4. Provide the contact information of the individual authorized to answer questions related to the proposal:
• Name
• Title
• Address
• Phone Number
• Fax Number
• Email Address
5. How many years have you been in business, specifically for theservices you are proposing on?
6. Please provide references for three current accounts comparable in size to THCP in Houston. Public sector clients arepreferred:Client 1
• Length of relationship years
• Number of participating employees employees
• Services provided
• Contact name
• Contact phone number
Client 2
• Length of relationship years
• Number of participating employees employees
• Services provided
• Contact name
• Contact phone number
Client 3
• Length of relationship years
• Number of participating employees employees

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 21
General information questionnaire Response• Services provided
• Contact name
• Contact phone number
7. How many clients do you currently have?
What is the average size?
How many clients over 20,000 employees do you have?
8. Is your principal place of business located in Texas? (Select)If not, do you employ at least 500 employees in Texas? (Select)
9. Has your company published any outcome or ROI studiesspecific to the Houston metropolitan area for clients with a peremployee per year (PEPY) cost at or below the district PEPY? Ifyes, please attach articles as a PDF file as Attachment S4: B –Outcome/ROI studies and/or cite online location(s) or webaddress where the publication can be found..
(Select)
10. Follow up to Q. 10, If yourorganization has not produced anypublished studies specific to the Houston metropolitan area,provide specific case studies to support your ability to impactPEPY of a client in similar size and PEPY costs to the districts.As Attachment S4 – B.
11. Please list any third-party organizations who will participate in the execution of the services you will provide to THCP underthis proposal (name, nature of relationship, year partnership began, contract time period, performance guarantees).
Partner
Partner
Partner
Partner
Partner
Partner
Partner
Partner
Partner
12. Are you accredited? If yes, which organization(s) are yourprograms accredited through?
(Select)
13. Have you received any awards of excellence over the past 5years? Which ones and when?
(Select)
14. Does your organization have a regular product release schedule?If yes, what is the frequency of regular releases? What is theprocess for mid-release updates?
(Select)
15. Do you provide marketing/promotion services to members? If yes,what services are typically included and what are the costs forthose services?
(Select)
16. Are you able to track the effectiveness of thesemarketing/promotional services (e.g., hits on website)?
17. How do you keep users engaged in your programming?
18. Will you agree to add one or more school districts as part of youruser advisory group? Please describe your user advisory groupand the role the District representative would play.
(Select)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 22
General information questionnaire Response19. What type of data will you need from THCP to implement the
proposed products/services? How often will THCP need to supplyyou with data and in what format? How should this data bedelivered?
20. Detail your organization’s standard approach to measuringprogram success.
4 . 3 A C C O U N T M A N A G E M E N T
Account ManagementMinimum Requirement
Agree,Agree with exception,
or Disagree Evidence/supporting detail1. Vendor will provide the following key staff positions:
Executive Sponsor must be a designatedsenior executive that has decision makingauthority and overall responsibility for theprograms and services provided as part ofthe overall, integrated Program.
<Choose One>
Account Manager with a minimum of fiveyears experience working with theprograms you are proposing foremployers with more than 20,000 eligibleemployees. This should be a dedicatedposition.
<Choose One>
Implementation Manager with a minimumof five years experience implementing theprograms you are proposing on andservices for employers with more than20,000 eligible employees. This will be adedicated position working with theAccount Manager in a lead role on allimplementation activities. This includesbecoming an active member of theoverall, integrated Program team. Also,this person is responsible for the staffingand oversight of implementation sub-group activity.
<Choose One>
Subject Matter Experts are designatedexperts to actively engage in, andpossibly lead, sub-group teams duringimplementation and the ongoingmanagement of the program, includingbut not limited to• IT/IS and Web Portal• Data analytics and reporting• Legal and compliance• Data and operational integration• Clinical• Communications• Measurement and evaluation
<Choose One>
Designated implementation teamfrom initial project launch datethrough 90 days following theeffective date.
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 23
Account ManagementMinimum Requirement
Agree,Agree with exception,
or Disagree Evidence/supporting detail2. Please provide an implementation project
plan as Attachment S4: C –Implementation Project Plan.
Account ManagementImplementation/Supplemental Response3. Please describe your account/relationship management structure
including client resources, change management, issue resolution andstrategic planning resources. Please provide bios for the team membersyou are assigning to the THCP account, including those indicated inquestion 1 above and any others who will be on the team as AttachmentS4: D – Biographies
4. Who is the proposed medical director? How does this individual plug intothe district’s program to ensure that decisions are consistent with theplan benefits?
5. What are the hours and days of availability for your account team?
6. How many other accounts would the account team be assigned to? Interms of THCP’s size, where would THCP rank among these otheraccounts?
7. Please confirm that your organization is willing to replace any teammember from the team servicing the THCP project if that team memberis not meeting the needs of the Districts.
(Select)
8. Describe your proposed approach for communicating (i.e., conferencecalls, meetings) with THCP:• During the implementation phase of this project• Ongoing, after implementation, through year one• On any changes in project definition, scope, and/or requirements
9. Please provide a detailed project plan (as Attachment S4: E – ProjectPlan) that describes your suggested transition/rollout plan for each of theservices included in this RFP. What role does your client typically playduring the implementation process? Please be specific about the type ofresources you will need from THCP and the amount of time requiredfrom those resources throughout the implementation.
10. Please describe how you transition from the implementation team to theongoing administration team.
11. All deliverables should be delivered to client in anelectronic format 5 business days in advance ofpresentation to the client.
<Choose One>
4 . 4 I N T E G R A T I O N S E R V I C E STHCP seeks to deliver a comprehensive Program that presents a seamless experience to members.Today, the program includes a comprehensive array of best practice products and services, delivered bymultiple vendor partners. Each vendor-partner is expected to respectfully collaborate with all partiesinvolved in the development of the integrated Program, while offering subject matter expertise to ensure

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 24
an optimal Program design. We anticipate the need to this kind of collaboration and integration tocontinue.
Integration responsibilities will expand as THCP rolls out other health and wellness initiatives. Examplesof additional areas that will be integrated over time may include: wellness programs, care managementprograms, pharmacy benefit managers, EAP and behavioral health services, work/life programs, fitnessfacilities on-site health and wellness clinics, disability and Workers Compensation plans.
In addition, it is the stated desire of the THCP Districts to simplify many of the integration efforts that aregoing on today, making the vendor management experience for the Districts simpler and morestreamlined. Please provide details around any services you are willing to offer that would accomplish thisstated goal along with the cost of providing such services. Tell us who your vendor partners would be insuch an endeavor, the structure of your relationship, and how the integration will benefit the Districts.Attach your proposal for these services as Attachment S4: F – Integration Services
All Vendor-partners will be required to collaborate with THCP for effective management of the overallProgram and to deliver an excellent experience to the member.
Integration services questionnaire Response1. Define how your organization approaches supporting seamless
programs and services when there are other third party vendorsinvolved.
2. Provide your point-of-view on the service of integration plays inconsumerism, behavior change and engagement and how the serviceyou are offering THCP drives that point-of-view into your serviceoffering.
3. Actively participate in the development of the business rules for:process flows, data exchange, cross-referrals, co-management andcase conferences to support Program delivery.
4. Provide your proposal for service integration as Attachment S4: E –Integration Services
(Select)
5. Enhance IT systems to support integration, including the followingspecifications:
Utilize a sophisticated technology platform that supports anddocuments all of the activities that pertain to the services you areproposing.
<Choose One>
Offer a level of integration within your organization or with strategicpartners to allow shared information and/or shared IT platforms. Forexample, allow access and/or capability for other vendor partners tosee certain areas of your IT platforms.
<Choose One>
Have a system platform capable of tracking member call activity fromfirst point of contact to call resolution (e.g., process, issue categoriesand resolution detail), within the integrator's areas of responsibilityand for calls triaged to outside Vendor partners.
<Choose One>
Provide detailed reporting around members referred inbound andoutbound. This reporting should not only be of members appropriatefor transfer, but the net number of transfers that actually occurred.
<Choose One>
Use data near or real-time data when received to perform delivery ofrespective programs and services.
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 25
Integration services questionnaire ResponseHave a system platform with the capability to refer to other programsand provide system messaging to facilitate awareness of other THCPhealth initiatives.
<Choose One>
Use technology to communicate with members and providers (e.g.,IVR, e-mail, Internet).
<Choose One>
Have a web-based system capable of: (a) consolidating informationinto user-friendly online format, (b) providing access to memberservice representatives internal to integrator and (c) assisting Vendorpartners in member navigation and promotion of programs andresources.
<Choose One>
6. Conduct training programs for Account and Operations staff in orderto assure successful delivery of programs based on THCP integrationspecifications.
<Choose One>
7. Provide and/or develop system access to other vendor-partners forTHCP-specific data elements.
<Choose One>
8. Refer members to appropriate programs as defined by businessrules.
<Choose One>
9. Support co-management of members participating in multipleprograms as defined by business rules.
<Choose One>
10. Support the established processes for communication andcollaboration regarding services and member contacts.
<Choose One>
11. Will you be able to accommodate Single Sign On (SSO) with THCPmember’s employee health information and benefit portal? Whatsecurity protocols will you support once the SSO exchange hasoccurred and the THCP member has successfully transferred to yoursite?
<Choose One>
12. Please describe in detail your integration experience in support of thefollowing activities. Address in your responses the following:• Years of experience• Clients serviced in each capacity• Role in supporting each of the following to deliver a seamless,
integrated Program for the client and their members:‒ Account Management‒ Program and service business rules and process flows‒ Technology to support business rules and process flows‒ Communications‒ Incentives‒ Data aggregation, predictive modeling, data exchange‒ Program tracking, reporting, measurement and evaluation‒ Master Contractor for all programs and services across the
health continuumOne of multiple vendors that have a key role in delivering one or moreproducts and services as part of an overall Program
13. We have provided as a part of this RFP as Exhibit J – CurrentIntegration of the Districts’ programs. Please confirm that you areable to provide at least this level of service. If you agree and are ableto provide more integration, please indicate the additional integrationyou can provide in the evidence/supporting details portion of theresponse.
<Choose One>
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 26
4 . 5 C O M M U N I C A T I O N S
Communications questionnaire
Agree,Agree withexception, orDisagree Evidence/supporting detail
1. Provide resources to support the development of anintegrated communication platform meeting THCP’sgraphical and content criteria to ensure alignment andintegration of messages/advice across all programs andservices to ensure consistency, limit confusion andfacilitate optimal the member experience.
<Choose One>
2. Provide materials that support the development andimplementation of a comprehensive communication andengagement strategy to maximize awareness,understanding and engagement in programs andservices.
<Choose One>
3. Provide consultative services as needed fordevelopment of promotional materials that are program-specific, as well as joint promotion efforts (e.g.,newsletters, posters, blast emails, on-site events) topromote the overall program throughout the program’slongevity.
<Choose One>
4. Integrate and coordinate communications to ensureconsistency and alignment between print and onlinecontent.
<Choose One>
5. Obtain THCP Communications’ review and approval ofall communications pieces (letters, flyers and inserts)before they are sent to THCP members.
<Choose One>
6. Produce material on THCP’s timetable; recognizing thatoccasionally that will be on short notice.
<Choose One>
7. With THCP Communications’ approval, promoteservices through multiple modes of communication(e.g., paper, web-based, telephonic, posters,management debriefings, etc.) and technology.
<Choose One>
8. Please confirm that you will provide SPD documentsbased on your knowledge of the plans for 2016 for theirreview, revision and adoption. Provide a timeline fordocument preparation, review, revisions and approvalthat will ensure delivery of an approved document in Q4of 2016 – Prior to the plan effective date of January 1,2017. You can view the current plan documents on theindividual District benefits websites (see Section 4.1.2).This is for the medical and FSA/HRA plans. Pleasenote, THCP Districts offer non-ERISA plans, and arenot required to provide SPDs, however have opted toprovide documents that mirror ERISA requireddocuments. Plan documents should be provided forreview in Q4 of each year thereafter.
<Choose One>
Communications questionnaire Response

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 27
Communications questionnaire Response9. Provide three URL and user name/passwords for demonstration
purposes for any online resources you are proposing.
10. Discuss your organization’s ability to coordinate, produce andimplement an on-going communication campaign to promoteprograms and services. Be sure to address how you will workwith THCP members’ current communication and/or humanresources teams to develop this campaign and the level ofcustomization included in your THCP quote.
11. Please specify to what degree THCP will be able to customizeprinted program promotion and educational materials. What is anacceptable timetable for allowed customization?
12. Please specify to what degree THCP will be able to customizethe look and content of your website dedicated to THCPmembers. Please be specific about number of pages THCP canhave your firm change or build, which portion of pages arecustomizable, your willingness to rename your site or accept a re-direct and your ability to take deep links. What is an acceptabletimetable for allowed customization?
13. Are you willing to provide a communications budget to be used atthe District’s discretion to support the services provided under thisagreement? If so, state how much the financial offer portion ofyour proposal
(Select)
14. If members want to receive paper notifications from you (i.e.,EOB, HRA report, etc.) what if the process for them to tell youthat? Do they have to opt out of electronic notifications or is paperassumed?
4 . 6 U N I Q U E I D E N T I F I E R S
Unique Identifiers Response1. Please identify how you protect the storage and access of personally identifiable
information (PII) or personal health information (PHI).
2. Describe how long PII/PHI is stored after a member terminates from coverage.
3. Describe your processes for destruction of PII/PHI.
4. Provide on who, outside of your organization, data is transmitted to (i.esubcontractors).
5. Describe your ability to accept and use a unique identifier (other than SSN) foridentification and accumulation purposes, keeping in mind that accumulation andtransmittal of data may be required to/from multiple vendors.
4 . 7 H E A L T H C A R E R E F O R M
4.7.1 Eligibility and Enrollment
4.7.1.1 Please confirm that you will follow each district’s definition of eligible employee.• Single, Radio group.
1: Agree,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 28
2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.2 Please confirm that if a member district decides to determine eligibility by defining full-timeemployee using the lookback measurement method in Treas. Reg. 54.4980H-3(d), you willsupport a definition of eligible employee using the lookback measurement method.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.3 Please confirm that you will support an eligibility definition based on any permissiblemeasurement/administrative/stability periods permitted by Treas. Reg. 54-4980H-3(d) thatClient selects. If there is a minimum administrative period that you need, please identify thatperiod.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.4 What support are you able to provide to each member district if it decides to use thelookback measurement period to determine the full-time status of any of its employees?500 words
4.7.1.5 If you are unable to track employee hours of rehired employees, please confirm that you willprocess rehires as instructed by THCP.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.6 Please confirm that if a member district decides to determine eligibility by defining full-timeemployee using the monthly method in Treas. Reg. 54.4980H-3(c), you will support andadminister a definition of eligible employee using the monthly method. If there are anylimitations on a district’s use of that method, please identify those limitations.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.7 What support are you able to provide to THCP if it decides to use the monthly method todetermine the full-time status of any of its employees.
500 words
4.7.1.8 Please confirm that you will follow each district’s definition of a covered dependent, should amember district decide to cover a broader or narrower group of children than those within thedefinition of “child” under Section 152(f)(1) of the Internal Revenue Code.Single, Radio group.1: Agree,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 29
2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.9 Please confirm that you will follow each district’s definition of covered grandchildren, should a memberdistrict decide to cover grandchildren as dependents.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.1.10 Describe the process how you determine a disabled dependent. How will current disabled dependentsbe transferred to your system and flagged? How often do you require re-certification? How is ittransmitted back to the client for flagging in the system of record so overage disabled dependents arenot dropped off the plan?500 words
4.7.2 Employer shared responsibility penalties
4.7.2.1 Please confirm that you will administer the plan so as to support THCP’s effort to at all timesprovide a plan with 60% minimum value, as described in Code Section 36B(c)(2)(C)(ii), asinterpreted by applicable guidance.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.2.2 Please confirm that you will calculate the minimum value of each district’s benefit plans underCode Section 36B(c)(2)(C)(ii), using one of the methods that have been identified byregulators and selected by the district. If yes, please identify the method you will be using todetermine minimum value. If not, confirm that you will provide each district with whateverinformation it needs to calculate the minimum value of coverage.
• Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.2.3 Please confirm that the minimum value of the plan under Code Section 36B(c)(2)(C)(ii) will beconfirmed using the MV calculator released by HHS.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.2.4 Please confirm that you will provide THCP with whatever information it needs to calculate theaffordability of coverage.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 30
4.7.2.5 Please confirm that you will assist each district in the event that it has to appeal any CodeSection 4890H shared responsibility penalty that may be assessed against Client based uponcoverage during the plan year, and please confirm that you will provide such assistance so asto permit Client to meet all applicable deadlines and other requirements of the appealsprocess as they may be set forth by regulators.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3 Health plan mandates
4.7.3.1 Preventive Services4.7.3.1.1 Confirm that you will cover preventive services in accordance with Section 2713 of the Public
Health Service Act (PHSA), as amended by the Affordable Care Act, and to the full extentrequired by all agency regulations and guidance, including but not limited to the FAQ XVIII,Q/A 1, issued Jan. 9, 2014, and FAQ XXIX, Q/A-1 – Q/A-10, issued Oct. 23, 2015.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.1.2 Confirm that you will amend your list of preventive services to comply with any forthcomingguidance about what preventive services must be covered by non-grandfathered planswithout cost sharing. For future guidance that clarifies existing preventive services rules,how long will it take your organization to begin administering preventive service claimsaccording to that future guidance?Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.1.3 Will you be preparing communications describing any change to the covered preventiveservices? What will those communications be, and how will they be distributed?Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2 Cost sharing limits4.7.3.2.1 Confirm that you will administer the plan so as to comply with the cost sharing limits
applicable to large employer plans pursuant to Section 2707(b) of the PHSA and Section1302(c) of the ACA, including but not limited to the rules related to embedded out-of-pocketmaximums, as described in FAQ XXVI, issued May 26, 2015.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 31
4.7.3.2.2 Confirm that you will track all in-network out-of-pocket expenses to determine when amember has reached the out-of-pocket maximum.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2.3 Confirm that you will count only in-network out-of-pocket expenses towards the annual out-of-pocket maximum.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2.4 If you are not able to count only in-network out-of-pocket expenses towards the annual out-of-pocket maximum, please identify the expenses that are counted towards the annual out-of-pocket maximum and describe how the out-of-pocket maximum is calculated.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2.5 Confirm that you are able to track out-of-pocket costs for in-network essential health benefits(EHBs) separately from other out-of-pocket costs.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2.6 If you are not able to track only out-of-pocket costs for in-network essential health benefits(EHBs) separately from other out-of-pocket costs, please identify the expenses that will beincluded in the out-of-pocket costs for in-network benefits.500 words
4.7.3.2.7 Confirm that your organization will be able to coordinate with vendors of any carved-outbenefit (example: pharmacy benefits) that may be retained by Client to administer the annuallimitation on out-of-pocket expenses. If there are any limitations on your ability to do this,please identify those limitations (example: coordination limited to certain vendors only).Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.2.8 Can you administer the cost sharing limits if the out-of-pocket maximum is split among themedical coverage and any carved out benefit (other than mental health/behavioral benefits)?If there are any limits to your ability to administer the benefits with cost sharing limits split inthe manner permitted by FAQ XVIII, Q/A 3, issued Jan. 9, 2014.Single, Radio group.1: Yes,2: No (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 32
4.7.3.2.9 Confirm that you will be excluding spending for non-covered services from the cost sharinglimits, as permitted by FAQ XVIII, Q/A5, issued Jan. 9, 2014.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.3 Annual dollar limits on Essential Health Benefits (EHBs)4.7.3.3.1 Confirm that you will make a reasonable determination as to which benefits are considered
EHBs, and administer the plan so as to remove all annual dollar limits on those benefits asrequired by Section 2711 of the PHSA.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.3.2 Confirm that you will continue to revise your definition of EHBs to comply with any newguidance that may be issued, and that you will alert Client as to those revisions and prepare acommunication to participants if necessary.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.4 Clinical trials4.7.3.4.1 Confirm that you will make a good faith, reasonable effort to comply with the coverage
mandates for clinical trials in accordance with Section 2709 of the PHSA, in accordance withFAQ XIV, Q/A 3 (issued Apr. 23, 2013). Confirm that you will comply with any future guidance(whether regulatory or subregulatory) that is issued concerning the implementation of thecoverage mandate for clinical trial coverage.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.5 Provider nondiscrimination4.7.3.5.1 Confirm that you will make a good faith, reasonable effort to comply with Section 2706 of the
PHSA, which prohibits discrimination against health care providers, in accordance with FAQXIV, Q/A 2 (issued Apr. 23, 2013). .Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.5.2 Confirm that you will comply with any future guidance (whether regulatory or subregulatory)that is issued concerning the prohibition of discrimination against health care providers.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 33
Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.6 Elimination of preexisting condition limitations4.7.3.6.1 Confirm that you will comply with the prohibition on preexisting condition exclusions for all
participants, as set forth in Section 2704 of the PHSA.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.6.2 Confirm that you will comply with any future guidance that is issued concerning theimplementation of the prohibition on preexisting condition exclusions for all participants.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.7 Elimination of excessive waiting periods4.7.3.7.1 Confirm that you will comply with the restrictions on waiting periods, as set forth in Section
2708 of the PHSA, the final rule published Feb. 24, 2014 (79 FR 10296), and any futureapplicable guidance (whether regulatory or subregulatory).Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.7.2 Confirm that you can administer the plan according to any waiting period Client selects that iscompliant with the final rules identified in the previous question.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.8 Excepted benefits4.7.3.8.1 Confirm that you will not require exhaustion of any Employee Assistance Plan benefits before
paying medical claims.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.3.8.2 Confirm that you will not require any other integration or “gatekeeper” interaction with theEmployee Assistance Plan.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 34
4.7.3.8.3 Are any health reimbursement accounts (HRAs) that you administer integrated with the majormedical coverage as required by IRS Notice 2013-54?Single, Radio group.1: Yes,2: No (explain): [ Unlimited ]
4.7.4 Ongoing reporting and Disclosure4.7.4.1 Confirm that you will provide THCP with any information required to meet its reporting
obligations under the Affordable Care Act.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.2 Confirm that you will support THCP’s compliance with the W-2 reporting requirement for thecost of employees’ health coverage, in accordance with applicable IRS guidance, for exampleby providing information upon request.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.3 Confirm that you will prepare new uniform summaries of benefit coverage (SBCs) that complywith applicable government regulations in advance of open enrollment.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.4 Confirm that you will provide the new SBCs.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.5 Confirm that you will work with Client in the weeks following delivery of the draft SBC to revisethe SBC as may be necessary.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.6 If you are not going to prepare new uniform Summaries of Benefit Coverage (SBCs), confirmthat you will support each district as necessary in the preparation of its SBCs. Confirm thatyou will review and confirm the accuracy of the SBC as prepared by each district, and identifyhow much time you will need for this process. SBCs must be finalized prior to OpenEnrollment for posting and distribution.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 35
4.7.4.7 Confirm that you will be responsible for distribution of the SBC during open enrollment, and ifso, what information you will require from each district and when. If not, describe what yourrole will be in meeting the distribution obligations for the SBC.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.8 Confirm that you will be responsible for maintaining the SBC and providing it to any new hireor special enrollee throughout the year. Please let THCP know what information you need toaccomplish this task, and how that information should be provided.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.9 Confirm that you will be responsible for providing the SBC notice to a participant within sevenbusiness days of the participant’s request.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.10 Confirm that you will reissue the SBCs (or provide some other notice of the change as maycomply with the final rules) at least 60 days in advance of any mid-year change to the SBCcontent.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.11 Confirm that you will complete all necessary state and local filings wherever possible underapplicable laws and regulations, and where not possible, you will provide assistance to eachdistrict as needed. Confirm that you will notify THCP where you will not be conducting aspecific filing.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.4.12 Confirm that you will be preparing and distributing a communication to participants describingall changes (to plan design, benefits, etc.) to the plan, in such a manner as to satisfy therequirements of a Summary of Material Modification under ERISA (or a Summary of MaterialReduction in benefits, if applicable).Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 36
4.7.5 Reporting/disclosure obligation under IRS Code Sections 6055 and 60564.7.5.1 Confirm that you will support THCP with the reporting required by Code Section 6055.
Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.5.2 Is there any assistance that you intend to provide to employers with respect to the CodeSection 6055 reporting? If yes, describe.Unlimited words
4.7.5.3 Confirm that you will support THCP in submitting its IRS filing under Code Sections 6056.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.5.4 Is there any assistance that you intend to provide to employers with respect to the CodeSection 6056 reporting? If yes, describe.Unlimited words
4.7.5.5 Confirm that you will comply with any additional guidance (whether regulatory orsubregulatory) concerning the reporting obligations under Sections 6055 and 6056.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.5.6 Will you be making the reasonable efforts to obtain the necessary taxpayer ID numbers(TINs) for all covered individuals described in the preamble to Treas. Reg. Section 1.6055? Ifnot, what assistance, if any, can you provide to THCP in its efforts to obtain the necessaryTINs?Unlimited words
4.7.5.7 Will you provide any assistance to employers who want to electronically furnish the reportingpursuant to Sections 6055/6056? If yes, will you be handling the acquisition and tracking ofparticipant consents? Will you require any assistance from THCP?Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.6 Fees4.7.6.1 Patient-Centered Outcomes Research Institute (PCORI) fee4.7.6.1.1 Confirm that you will handle the calculation of the PCORI fee for THCP, including calculating
the number of covered lives according to applicable regulations. If not, confirm that you willsupport THCP by providing whatever data and assistance is needed for THCP to calculatethe PCORI fee.Single, Radio group.1: Agree,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 37
2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.6.1.2 Confirm that you will support THCP by providing whatever data and assistance is needed forTHCP to pay the PCORI fee via a Form 720.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.6.1.3 Please confirm that you will comply with any future guidance (whether regulatory orsubregulatory) concerning collection of these fees.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.7 Compliance4.7.6.1.4 Will you act in accordance with the documents and instruments governing our clients plans
and comply with all applicable state and federal laws and regulations including, but not limitedto, the following: HIPAA of 1996 (including HITECH and all other amendments), including thenondiscrimination, special enrollment, coverage certification, privacy, security, EDI, and otherHIPAA requirements.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]
4.7.6.1.5 Please describe your process to stay up-to-date on legislative changes that may affectprogramming and operations of your service:500 words.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 38
V. MEDICAL QUESTIONNAIREThe Districts’ current medical programs are built on a base of consumer directed health plans with healthreimbursement accounts. The current program provides tiered benefits for specialist and hospital servicesin an EPO environment. Each District also offers at least one plan option that makes use of a singlehospital system, which today is Memorial-Hermann. The plans are supplemented with a number ofutilization management and care management services including maternity management, radiologymanagement, a “gaps in care” program (Med Query) provided by Aetna. The Districts are interested inlearning what programs, services and products you have that will allow them to build on what they have inplace today to make it work “better, faster, and cheaper.”
The Districts are interested in a self-insured program that offers savings guarantees. It is very important tothe Districts to have certainty in their contracting process. Please pay careful consideration to the caveatsand limitations on your pricing, with the knowledge that certainty in “the deal” is preferred.
5 . 1 M E D I C A L S T R A T E G YPlease tell us about any quality enhancement and efficiency improvement efforts you are proposing forthe Districts. Include a full description of how the solution or strategy works, the supporting network ofproviders, all costs for each program component (ASO fees, network access fees, other program fees,any IT development costs, etc), potential savings (including information on how the potential savingsprojections were derived), savings guarantees, credit your underwriters will guarantee for each strategyimplemented toward stop loss terms as attachments under Tab 6. Please label your attachments asAttachment S5: A - Strategic Initiatives – “1”, “2”, etc., as labeled in the table below. Be succinct, yetthorough. If you would recommend grouping or coupling solutions or strategies, please note that in yourresponse.
5.1.1. Strategic InitiativesStrategy Yes/No1. Accountable Care Organizations Please select2. Patient Centered Medical Homes Please select3. Network Options (including tiering) Please select4. Centers of Excellence Please select5. Utilization management/Case Management Please select6. Value Based Design Please select7. Medical Tourism Please select8. Re-Admission Reduction Please selectOthers: Please list here and indicate the names of each.9. Please select10. Please select11. Please select12. Please select13. Please select
5 . 2 M E D I C A L A D M I N I S T R A T I O N5.2.1. Compliance/Legal
Compliance/legal questions Response Evidence/supporting detail
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 39
Compliance/legal questions Response Evidence/supporting detail1. Will you agree to be the “named claims fiduciary”
regarding review of claims and appeals of adversebenefit determinations? The fiduciary responsibility willinclude discretionary authority to determine entitlementto plan benefits as determined by the plan documentsfor each claim received and to construe the terms of theplan. The claims fiduciary has no other fiduciaryresponsibility under the plan other than the claimsappeal process.
(Select)
2. In discharging your responsibilities, will you agree to the following:• Act in accordance with the documents and
instruments governing the plan, and any applicablefederal or state law
(Select)
• Be the “appropriate named fiduciary” for thepurpose of providing a participant who has anadverse benefit determination with a full and fairreview of the decision denying the claim. Yourdecision on appeal of the adverse benefitdetermination shall be the final review for the plan
(Select)
• Have sole and complete discretionary authority todetermine eligibility for benefits, to construe theterms of the THCP plans, to make factualdeterminations, and to determine the validity ofcharges submitted for reimbursement under theplan. You shall be deemed to have properlyexercised such authority unless you have abusedyour discretion hereunder by acting arbitrarily andcapriciously
(Select)
• Notwithstanding the foregoing, THCP shall be theadministrator of the plan, and shall have sole andcomplete discretionary authority to determinequestions relating to the eligibility of employeesand dependents for participation in the plan,including determination of who is a participant.Nothing in the contract shall limit the ability ofTHCP to amend or terminate the plan
(Select)
3. Will you agree to protect THCP and its plan participants from incurring liability for payment of any fees which are your legalobligation including, but not limited to, the following?• Sufficient insolvency and liability insurance (Select)• A contractual arrangement with medical providers
affiliated with you that prohibit such providers fromholding any participant liable for payment of anyfees which are your obligation
(Select)
• Other protection from liability for participants asprovided by applicable state or federal laws
(Select)
4. Will you provide the plan with detailed reporting on yourmanagement of individual rights in a mutually agreedupon format upon request?
(Select)
5. If claims are paid in error by you as the claimsadministrator, will you agree to be responsible for youractions by reimbursing the amounts paid in error to thedistricts?
(Select)
5.2.2. Member SatisfactionMember satisfaction questions Response Evidence/supporting detail

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 40
Member satisfaction questions Response Evidence/supporting detail1. Will you provide a single identification (ID) card for
medical and pharmacy claims even if pharmacy iscarved-out to another vendor? If yes, what informationwill you provide on the card?
(Select)
2. Is language on the ID card customizable? If yes, towhat extent can it be customized? Are there anyadditional fees for customization?
(Select)
3. Will you agree that all customer servicesrepresentatives are required to complete training relatedto THCP’s plans before being allowed to work on theTHCP accounts?
(Select)
4. Please answer the following questions with regards toyour customer service call center you propose forTHCP:• Are your claims processing and customer service
functions performed by the same group?
(Select)
5. Will you provide a dedicated customer service unit?• If No, describe how the unit would be assigned
(Select)
6. How many customer service representatives are therein the unit?
7. What hours will your call center be open?8. What languages will the customer service
representatives in this unit speak?9. Will you match inquiries/complaints to the treating
physician?(Select)
10. Will calls be tracked and reported electronically by the following?• Employer group (Select)• Individual member (Select)• Physician/physician group (Select)
11. Will your customer service representatives stay on theline to assure successful call transfer?
(Select)
12. What percentage of customer service calls aremonitored for quality assurance purposes?
13. What percentage of customer service calls arerecorded?
14. Where is your claims/customer service unit located? Isthere any portion that is offshored? If so, please detail.Would you consider processing all services onshore? Ifso, is there an additional cost? Please detail.
15. Will you update your online directories at least weekly toreflect accurate provider listings?
(Select)
16. Describe how your organization’s service units, i.e.claims, member services, provider relations, worktogether.a. Are services units under the same or separate
reporting structure? Provide a flowchart showinghow these units work together as Attachment S5:B– Service Units Flow Chart
b. Describe how training occurs for these units.c. How are the service units monitored to ensure
consistent message to providers, members, andclients?
5.2.3. NetworksNetworks questions Response Evidence/supporting detail1. Do any of your plans listed below require referral to a specialist by a primary care physician?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 41
Networks questions Response Evidence/supporting detailEPO (Select)PPO (Select)Consumer directed (Select)
2. Are there any physician groups (with more than 6providers) in your network that will expire in the next sixmonths?
(Select)
If yes, please list the top five provider groups (ordered by the number of utilizing members; the most members being group 1)Are you expecting any recontracting difficulties?Name Recontracting difficulties?• (Select)• (Select)• (Select)• (Select)• (Select)
3. Describe member notification process for upcomingprovider terminations.
4. Are there any major facilities (hospitals) in your networkup for recontracting within the next two years OR arethere any major facilities in your network that haverequested (or you expect to request) contractamendments?• If Yes, If yes, please list.
(Select)
5. Do you currently rent any networks in the HoustonMSA?
(Select)
If yes, please list the rental networks:•••
6. What capabilities do you have to control out-of-networkphysician and facility costs?
7. Are you able to accommodate a different plan design foran individual provider?
(Select)
8. If you are a Houston-based (not national) program, doyou have a solution for out of area dependents andCOBRA participants living outside the Houston MSA?Please explain. Include information on administrativedetails, discounts provided, and other cost andadministrative considerations.
(Select)
9. What do you use to measure the quality and efficiencyof providers in the network? How do you measureproviders referring outside of the network?
10. Describe how you would quantify the performance of anarrow or tiered network vs performance of broadernetwork from a unit cost perspective.
11. Out-of-Network OON Performance.a. What do you expect the OON utilization % to be?
Please specify separately for each district basedon their current plan designs.
b. What fees are associated with OON reduction(shared savings)?
c. Will you be able to administer OON at a flat % ofMedicare instead of shared savings? How will thisimpact the administrative fees?
12. Mental Health/Substance Abused. Describe the breadth and depth of your MH/SA
networke. What percentage of providers are currently
accepting new patients?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 42
Networks questions Response Evidence/supporting detailf. What percentage of providers are currently working
with state/governmental referrals only?g. How does organization monitor autism spectrum
disorder to determine appropriateness of care?
5.2.4. GeoAccess RequestGeoAccess request questions Response Evidence/supporting detail1. What date was your GeoAccess database last
updated? (mm/dd/yyyy)2. On what basis do you determine GeoAccess – straight
line (i.e. how the crow flies) or actual driving distance?.3. Referencing your response to question 2, can your
standard capabilities be modified. If so, please explain.
5.2.5. General CapabilitiesGeneral capabilities questions Response1. Describe in detail your capabilities for utilization
review/management.2. Describe in detail your capabilities for case
management.3. Describe in detail your capabilities for health
reimbursement account administration4. Will you provide a Data specialist who will spend at
least 500 hours per year on analysis of THCP claimsand meet our data request needs at no additional cost?
(Select)
5. Please describe any innovative technologies youincorporate to improve your service (i.e. SMSmessaging, live chat communications, etc…)
6. Are custom network provider directories available viamobile applications?
(Select)
7. Describe in detail your capabilities of PersonalizedHealth Record (PHR) for members. Can members useit not only to store claims history, but transfer to specificproviders? Is there an auto notification process for X-Ray, MRI, lab results, etc.?
(Select)
5.2.6. Client ServicesPlan administration questions Response Evidence/supporting detail1. Will you provide a fully-dedicated on-site customer
service representative who has remote access to yourclaim system, to assist members, keeps an activeissues log, access to claims details and medicalrecords to assist in claims audit and the daily checkregisters, conducts team review calls and isresponsible for reporting back to THCP any issues andexperiences for each ISD?
(Select)
• If yes, do you agree to provide a dedicated on siterepresentative to HISD specifically, and anadditional on site representative to the otherTHCP member districts if requested?
• If yes, are there any additional charges or fees forthis service?
(Select)
• If yes, the on-site representative must be anemployee of your organization, not a contractor.
(Select)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 43
Plan administration questions Response Evidence/supporting detail• You agree to allow the district(s) final approval
with regards to the designated on siterepresentative.
2. Will you provide an assigned medical clinician who isresponsible for maintaining a high claimantclaims/conditions/activities list for monthly or semi-monthly high claimant meetings at District locations?• If yes, are there any additional charges or fees for
this support?
(Select)
3. Will you provide an assigned case manager who isfamiliar with THCP claims to participate in the meetingsdescribed in #2 directly above?• If yes, are there any additional charges or fees for
this support?
(Select)
4. Do you agree to provide allowances for each of thefollowing items listed below? Please note that fundsmust be provided separately for each district.· Pre and/or post implementation audit (Select)· Ongoing audit (Select)· Investment dollars (Select)· Communications (Select)· M/WBE (Select)
5. THCP currently provides on-site flu vaccine where theprovider comes to each district’s school sites toadminister the vaccines.· Do you contract with providers for this program?
If yes, please provide the name of the providers.Otherwise, what type of relationship you havewith the providers who can provide similarprogram?
(Select)
· Can you offer these programs for the districtsseparately, depending on each district’s needs?
(Select)
· If allowances are offered to each district, can thepart of the allowances be used for the flu vaccineprogram?
(Select)
· Can you provide a brochure detailing yourorganization’s offering for on-site flu vaccineprograms, including provider name(s), claimsprocessing, utilization, etc. as Attachment S5:C -Flu Vaccine Program?
(Select)
6. Assume all responsibility and liability for theperformance of the stop loss according to the terms ofyour contract with THCP regardless of yourrelationship/contract with the third-party vendor andguarantee reimbursement of claims processed abovethe stop loss level?
(Select)
7. Your organization has experience in coordinating andexchanging data with data warehouse vendors, healthmanagement vendors, and on-site clinics to promotehealth improvement initiatives.
<Choose One>
8. Do you have a procedure in place for handlingdisclosure issues?
(Select)
9. Will you take responsibility for the following? (First-tier and appeals process and providing resolution to appeals in thefollowing)• Medically necessary issues (non-emergent) (Select)• Life threatening conditions and/or continued
hospital stays (expedited appeals)(Select)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 44
Plan administration questions Response Evidence/supporting detail• Complaints and appeals (non-emergent) including
quality of care, quality of service andadministrative services
(Select)
10. Will you take responsibility for the following? (Second-tier and appeals process and providing resolution to appeals in thefollowing)• Medically necessary issues (non-emergent) (Select)• Life threatening conditions and/or continued
hospital stays (expedited appeals)(Select)
• Complaints and appeals (non-emergent) includingquality of care, quality of service andadministrative services
(Select)
• Are there any costs associated with externalappeals? Please detail.
(Select)
11. What has been your ability for other Houston clients tomaintain a PEPY at or better than the current THCPPEPY? Provide case studies as Attachment S5: D –Plan Performance Case Studies to demonstrate howand why you have been able to mitigate trends.
12. Can you produce and deliver customized electronicEOBs?• If yes, are there any associated charges or fees?
(Select)
13. Are you willing to commit in delivering final SummaryPlan Description documents prior to 1/1? Will youagree to offer Performance Guarantee to support thiscommitment?
14. Will you allow Mercer to perform the following types of audits?• Pre-effective date audit of eligibility (Select)• Pre-effective date audit of claims processing (Select)• Pre-effective date audit of plan design set-up (Select)• Post-effective date audit of eligibility (Select)• Post-effective date audit of claims processing (Select)• Post-effective date audit of plan design set-up (Select)
15. Will you agree to a self-billed method of collectingpremiums/fees from our clients?
(Select)
16. How will your organization assist THCP with MedicareSecondary Payer (MSP) claims? Who will provide theassistance? Will they work with prior carriers to resolveMSP issues? Are there any limitations to suchassistance? Is there a price for this service?
17. For Coordination of Benefits, what methodology do youuse when determining which plan is primary? What isthe effectiveness against industry standards? How doyou process overpayment or underpayment ofbenefits? Describe how you inquire documentation todetermine benefit payments.
18. Do you continue to provide services after contracttermination? Please respond to each of the questionsbelow:
(Select)
· Will you continue to process run-out claimsfor claims incurred prior to termination date?If so, how long are you willing to processrun-out claims? Please provide anyadditional costs associated to this service inyour financial proposal
(Select)
· Are there any additional charges associatedto processing of run-out claims? Pleaseprovided all additional charges inAttachment S5: E – Medical Financials
(Select)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 45
Plan administration questions Response Evidence/supporting detail· Will you continue to support any claims
issues?(Select)
· Will you continue to assist with MedicareSecondary Payor issues that may arise?Please provide all costs related to thisservice in Attachment S5: E – MedicalFinancials
(Select)
19. Subrogation and Reimbursement· What methodology do you use in
determining identification and recovery ofpayments?
· What is the typical percentage of paymentrecovery?
· Are there any fees associated with thisservice?
(Select)
· Describe the process in reporting back to theclient, including frequency and timing.
Reporting questions Response Evidence/supporting detail1. Will you provide the following monthly financial reports within ten calendar days after the end of the month to THCP and
Mercer?Claims liability/cost• If No, how many days after the end of the month
will it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Retention and network access fees• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Number of claims• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Paid claims broken down as: Capitation, if applicable.• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Paid claims broken down as: Fee-for-service claims• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Paid claims broken down as: Paid check listing (if ASO)• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Paid claims broken down as: Outstanding checks (ifASO)• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)Paid claims broken down as: Daily and weekly fundtransfers(if ASO)• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 46
Reporting questions Response Evidence/supporting detailPaid claims broken down as: Adjustments includingvoids and stop-payments (if ASO)• If No, how many days after the end of the month
would it be available?
(Select)
• If No, are there any associated charges or fees? (Select)2. Will you provide claims and utilization reports within 30 calendar days after the end of the quarter to THCP and Mercer
including the following information?Per member per month (PMPM) comparisons• If yes, are there any associated charges or fees?
(Select)
Age/sex demographics• If yes, are there any associated charges or fees?
(Select)
Employee/dependent status• If yes, are there any associated charges or fees?
(Select)
Types of services rendered• If yes, are there any associated charges or fees?
(Select)
Use of services• If yes, are there any associated charges or fees?
(Select)
Who provided the services?• If yes, are there any associated charges or fees?
(Select)
Frequency the services are used• If yes, are there any associated charges or fees?
(Select)
Case management services and results• If yes, are there any associated charges or fees?
(Select)
Reporting questions Response3.
In what format will you report the following? OverpaymentsCollectionpercentages
Collectiontimeline
Reasons foroverpayment
E-mail (Select) (Select) (Select) (Select)Letter (Select) (Select) (Select) (Select)File (Select) (Select) (Select) (Select)FTP site (Select) (Select) (Select) (Select)Don't do it (Select) (Select) (Select) (Select)Charges or fees (Select) (Select) (Select) (Select)E-mail (Select) (Select) (Select) (Select)
Reporting questions Response Evidence/supporting detail4. Can you report projected savings from patient
migration? Are there any costs associated with newpatient testings?
(Select)
5. Will you agree to deliver annual accounting reports toTHCP within 90 calendar days from the end of thepolicy period?
(Select)
6. Will you agree to provide online access to claims reports including, but not limited to, the following?Paid claims (Select)Eligibility (Select)Total claims by claimant (Select)Number of claims (Select)Type of service (Select)
7. Describe the breadth of on-line reporting available toconsultant and THCP directly into your reportingsystems. Can custom reports also be created andsaved in that system for our retrieval as updates areavailable?
8. Describe the training you will provide to enable ouraccessing your reporting system, and which reports canbe run by clients, THCP members, consultant, etc.
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 47
Reporting questions Response Evidence/supporting detail9. Do you agree to report to THCP’s selected data
warehouse monthly at no additional charge? Do youhave any limitations with the data transmission to thedata warehouse?
(Select)
10. Do you agree to provide access to daily check register? (Select)
11. For reports that cannot be run through your system,how many hours will you provide to run these reports?Are there any associated charges or fees?
12. The THCP member disctricts are requesting a quarterly“stop light” dashboard on plan performance. Pleaseattach as Attachment S5: G – Sample Stop Light Reportwhat your version of this stop light report would looklike.
13. Network performance. Detail reporting on how yourhigh performance, or a customized hybrid network,would be evaluated against the overall broad network.Please provide sample reporting as Attachment S5: H -Sample High Performance Network Report.
a
Payments questions Response Evidence/supporting detail14. Will you notify each District within THCP individually of the following?
• A large claim ($50K or more in charges) uponsubmission
(Select)
• A potential large claim ($50K or more in expectedcharges) upon a trigger diagnosis admission
(Select)
15. What is the process for reviewing large claimpayments? What authority does the claim processorhave to approve claims payments?
16. Will you process all medical claims in one location? (Select)17. Describe your banking arrangements for claims
payment purposes (ASO only).18. Describe your preferred banking arrangements for
payment of fees or premiums
5.2.7. System CapabilitiesSystem capabilities questions Response Evidence/supporting detail1. Do you have experience interfacing with carve-out
vendors (e.g., prescription drug, mental health,Condition Management, on-site clinics)?
(Select)
2. Will you accept data from carve out vendors at noadditional charge? Please detail.
3. Will you allow eligibility updates to be completed via theWeb by THCP?
(Select)
5.2.8. High Performance NetworksHigh Performance Networks Response1. Please describe any plan design limitations when
implementing a High Performance Network. Does yourorganization have recommended plan designs tomaximize savings opportunities? Please respond withrespect to HDHP designs.
2. On average, what percentage of providers in your broadnetwork receives high performance designations?Please provide responses specific to specialty andregion (North, South, East, West, NE, NW, SE, SWHouston).

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 48
High Performance Networks Response3. What kind of turnovers by specialty does your
organization experience? How are employees notified incase of a change?
4. Please describe the methodology for identifying highperforming providers. Do both hospitals and physiciansreceive high performance designations? If physiciansdo, are PCPs and specialists included? If applicable,please specify which specialties are included. Also,include minimum number of episodes/observationsrequired per provider and scoring requirements. Howare providers who do not have the minimum number ofepisodes/observations handled?
5. Are incentives provided to physicians who are HighPerformance providers (monetary or otherwise)?• If yes, how will these be charged back to THCP?
6. Is efficiency measured on an episodic basis as part ofnetwork selection? Is quality measured as part ofnetwork selection? If yes, please describe the qualitymeasures used in detail.
7. Is quality and efficiency rating information available onthe employee portal? Please describe the employeeinterface and provide sample screen shots. If not,describe your organization’s plans to make thisinformation available in the future. Please specify whatis currently available and what will be available in thefuture.
8. How frequently is your HPN assessed?9. Can you provide THCP notice of provider changes to
the HPN by the first of August of each year changes aremade?
10. How do you manage disruption and continuity of carewhen you do regular maintenance of your HPN?
11. Please provide any employee communications you haveavailable to describe the HPN to employees (asAttachment S5: F – HPN EE Communications).
(Select)
5.2.9. CostsCost questions Response Evidence/supporting detail1. Please provide your financial proposal as Attachment
S5: E – Medical Financials.xls. Please ensure proposedfinancials are provided separately for Houston, Aldine,and Katy.
(Confirm)
2. Please provide the following medical trend information:Fully insured book of business HMO CHDP PPO
20132014Projected 2015
3. Provide the following medical loss ratio information:Fully insured book of business HMO CHDP PPO
20132014Projected 2015
4. For out-of-network claims, please describe your R&Cfee profile• How often is it updated? (Select One)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 49
Cost questions Response Evidence/supporting detail5. THCP (HISD only) currently utilizes a custom out-of-
network fee schedule that is based on a percentage ofMedicare reimbursements. Will you allow each District(including HISD and any district which may join THCPin the future) to choose the percentile and basis of R&Cthat is administered?
(Select)
6. Do you have a shared savings program for out-of-network claims? Please provide detailed costsassociated with shared savings and expected OON %of claims.
7. Please detail your reporting around out-of-networkclaims and your shared savings programs. Monthly,quarterly, annually? Please provide sample reporting.
8. Will you allow the districts to opt out of your sharedsavings program at no additional charge?
5 . 3 M E D I C A L A D M I N I S T R A T I O N P E R F O R M A N C E G U A R A N T E E S5.3.1 General Requirements
Item Requirement Agree / Disagree Comments1. If you self-report performance results and if there is an audit
which shows less favorable results, then the audit resultsprevail.
2. Performance guarantees should be applied on a pass/failbasis, that is, if the PG is met or exceeded, it is passed. If theresults fall below the PG standard, the vendor is considered tohave failed that measurement.
3. Claim quality, turnaround time and customer serviceperformance guarantees will be based on quarterly results;penalties paid annually based on quarterly results
4. Total fees at risk for eligibility, claims, customer service, andaccount management performance measurements will be noless than 20% of ASO fees
5. Performance results should be client-specific versus book ofbusiness or site level.
6. Performance results will be report to the hundredth place (2decimal places).
5.3.2 Eligibility Requirements (Total at Risk: 4%)Item Requirement Agree / Disagree Comments
1 Annual Enrollment ID Card Production and Distribution: IDcards will be produced and mailed to plan participants within 10business days of receiving the enrollment eligibility file (2%)
2 Ongoing ID Card Production and Distribution: 95% of IDcards will be mailed within 5 business days and 100% ID cardsmailed within 7 business days of notification of change inbenefit, new member coverage and valid family status change(1%)
3 Eligibility Updates: 98% of eligibility updates will be processed

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 50
within 4 business days of receipt of data and 100% of eligibilityupdates will be processed within 5 business days of receipt ofcomplete and accurate data (1%)
5.3.3 Account Management Requirements (Total at Risk: 2%)Item Requirement Agree / Disagree Comments
1 Overall Account Management: Services provided by theaccount management staff or service center staff during theguarantee period will be measured at an average evaluationscore of 3.75 or higher (2%)Requires use of evaluation tool using as rating scale of 1through 5 (1 is the lowest; 5 the highest)
5.3.4 Claims Requirements (Total at Risk: 8%)Item Requirement Agree / Disagree Comments
1 Financial payment accuracy: 99.30% or higher (2%)Measures the percentage of paid dollars process accurately -total paid minus absolute value of over and underpaymentsdivided by total paid dollars
2 Payment incidence accuracy: 98.00% or higher (2%)Measures the percentage of claims processed without apayment error – total number of claims (pays and no pays) thatwere processed without a payment error divided by total numberof claims processed
3 Claims processing accuracy: 97.00% of higher (1%)Measures the percentage of claims processed without any typeof error (payment or non-payment) – total number of claim thatwere processed without an error of any type divided by the totalnumber of claims processed
4 Claims turnaround time (14 calendar days): 94% (1%)Measures the percentage of all claims processed within aspecified number of calendar days
5 Claims turnaround time (30 calendar days): 99% (2%)Measures the percentage of all claims processed within aspecified number of calendar days
5.3.5 Customer Service Requirements (Total at Risk: 5%)Item Requirement Agree / Disagree Comments
1 Telephone service factor (TSF): 85% of calls answered within30 seconds (2%)Measures the percentage of all member calls answered within30 seconds or less
2 Average speed of answer: < or = 1% (1%)Measures the average speed of answer for all member calls
3 Call Quality: 97.5% or better (2%)Measures the average vendor internal call quality score during

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 51
the reporting period
5.3.6 Member Satisfaction Requirements (Total at Risk: 1%)Item Requirement Agree / Disagree Comments
1 Annual Member Satisfaction Survey: >85% (1%)Measures plan member satisfaction with a vendor’s claimsprocessing and customer service performance. Members maybe asked “Overall, how satisfied are you with the way weadminister your medical health insurance plan?” If less than85% pf the respondents are satisfied overall, the PG will bedeemed to have been failed. Satisfied may be defined ascompletely satisfied, very satisfied, or somewhat satisfied.
2 Net Promoter Score (NPS): Report only measurementThe NPS score is calculated by subtracting the percentage ofcustomers who are Detractors from the percentage ofcustomers who are Promoters. The percentage of Passive is notfactored into the results equation.The NPS score is derived based on a direct question, e.g., “Ona scale of 1 to 10, how likely is it that you would recommend ourcompany/service to a friend or colleague.” Scoring is often on ascale of 0 to 10, and scores are categorized as follows:· Promoters (score 9 to 10) – are loyal enthusiasts who will
refer to others· Passives (score 7 to 8) – are satisfied but unenthusiastic
customers· Detractors (score 0 to 6) – are unhappy customers who
can damage a firm’s brand and impeded growth throughnegative word-of-mouth
5 . 4 M E D I C A L A D M I N I S T R A T I O N F E E E X H I B I TTo be included

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 52
VI. FSA/HRA QUESTIONNAIRE6 . 1 F L E X I B L E S P E N D I N G A C C O U N T ( F S A )All 3 Districts offer full service medical and dependent care flexible spending accounts.
GeneralFSA – General questions Response1. How long has your organization provided FSA (including Health
and Dependent Care throughout this questionnaire) administrativeservices? (Be specific if outsourced or in-sourced.)
2. What is the average size participant group for which you provideFSA services?
3. Please list the services included in your initial set-up fee.4. Please list the services included in your ongoing maintenance fee.5. Please list the services included in your claims processing fee.6. Is there a minimum group size (of participants) required for
maintenance fees to be waived?<Choose One>
• If yes, what is the minimum number?7. Are there any other fees for FSA administration not included
above?<Choose One>
• If yes, please list them all. Include information about anyexpenses that are not a part of your stated fees.
8. Confirm that your services include administration of allreimbursements allowed under FSA regulations.
<Choose One>
9. Please describe any innovative technologies you incorporate toimprove your service (i.e. SMS messaging, live chatcommunications, etc…)
Operations/claim administrationOperations/claims administration questions Response1. Describe your claims processing procedures.2. Do you require a minimum payroll deduction? <Choose One>3. Can you mail reimbursement checks directly to employees’
homes?<Choose One>
4. Can employees elect to have funds direct deposited? <Choose One>5. What methods of submission does your organization accept claims
forms (e.g., online, Smartphone, fax, mail)?6. What percentage of claims submissions are submitted via:
Online?Smartphone?Email?Fax?Mail?Other?
0.00%0.00%0.00%0.00%0.00%0.00%
7. What is the average turnaround time from receipt of areimbursement request to check issuance?
8. What is the average turnaround time from receipt of areimbursement request to direct deposit?Are you willing to guarantee turnaround on your time? <Choose One>
9. How are the unsubstantiated payments handled? Describe yourprocess of notifying members and clients.
10. Can communications relating to unsubstantiated claims becustomized by the client?
<Choose One>
11. What 1099/W-2 support is available for unsubstantiated claims?12. What is the $ amount threshold for requiring claims substantiation?
Can the client request a different amount?13. At what points debit cards are turned off? Is it modifiable by the
client?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 53
GeneralFSA – General questions Response14. What is the reconciliation process for forfeitures? When does this
occur and at what point is the money returned to the district?15. What format do you provide account statements to participants
(e.g., e-mail, secure website, mail)?16. How frequently and when do you provide account statements to
participants?• How frequently and when do you provide account statements
to the client?17. Do you have a designated toll-free number for customer service
(claim and account balance inquiries, fax submissions)?<Choose One>
• What are the operating hours of the FSA customer servicedepartment?
18. Are your forms able to be completed online? <Choose One>19. What processes do you have in place to ensure that there is no
"double dipping" between the consumer plans' associated accountand the FSA account?
20. Do you have the ability to provide automatic reimbursement, alsoknown as streamlined claims or auto-substantiation (i.e.,employees would not need to complete a separate FSA claim form)for claims through the health plan?
<Choose One>
• If yes, describe your process.• Must employees opt in each year? <Choose One>• If yes, do you have any concerns with coordinating claims files
between medical, dental, vision or Rx carriers?• Please list any vendors with whom you currently streamline
claims.• Do you have a standard format that must be used, or do you
have flexibility to take another carrier’s format instead?• Is there an additional fee to use another carrier’s layout?
21. What are the access methods available to participants and theemployer's staff (e.g., Web, IVR, CSR)?
22. Describe your claims review and appeal processes.23. Describe your process for handling elections which exceed federal
limits.24. Describe your process for administering forfeitures.25. Provide systems diagram and flowchart as Attachment S6: A –
FSA Systems.<Choose One>
26. Describe your ability to provide a limited purpose FSA. Include anylimitations.
27. How do you manage both a limited and full-benefit FSA when bothare being offered by the same employer?
28. You agree that incumbent will process run-out (until filing deadlinein 2017 for 2016 plan year).
<Choose One>
29. Will you allow the plan sponsor to audit your records annually? <Choose One>Banking/fundingBanking/funding questions Response1. Describe your banking arrangement for the FSA.2. What are the minimum deposit requirements?3. Describe for us all timelines associated with banking and payment
of fees.4. How would you interface with the employer’s payroll/HRIS system
regarding enrollment changes and corresponding deductionchanges due to family status changes?
5. What procedures are used to reconcile the employer's payrolldeduction information?• How frequently is this done?
6. Whose check stock will be used for reimbursement checks?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 54
GeneralFSA – General questions Response7. Describe how banking information is updated.8. Under your standard arrangement, are checks cut bi-weekly,
monthly, etc.?ReportingReporting questions Response1. Describe the online capabilities available to participants and to HR.2. Do you provide employees with online access to current balance
information?<Choose One>
3. Do you have online reporting that supports viewing of the lowestlevel of detail? (i.e., summary by type of transaction/services atmember-specific level)
<Choose One>
• In what format (PDF, Excel, Word) are reports available?• Does the client have the ability to manipulate (i.e., sort) report
data?<Choose One>
• How often is report data updated (e.g., real time, daily,weekly, monthly)?
4. Can the employer or its designee make changes to participants’eligibility/elections online?
<Choose One>
5. Do you perform discrimination testing without additional charges? <Choose One>If no, please list in fees.
Debit cardDebit card questions Response1. Do you offer 'debit cards' or a similar product for participants to
withdraw funds from their account?<Choose One>
• If yes, please describe capabilities and any requirements indetail. Specifically, do you require the client to pre-fund for theDebit?
• Is there an additional cost for debit cards?2. If a participant uses the debit card for a copay, is a receipt
required?<Choose One>
3. Describe your debit card claim substantiation process and whensubstantiation is required.
4. Describe your process for crediting/refunding for over chargeswhen a debit card if used at the point of service?
CommuterCommuter questions Response1. Is your commuter program 100% compliant? <Choose One>2. How do you define and implement the “readily available” guidelines
as defined under Section 132(f)(3)? List the markets that areimpacted by this regulation and explain the administration process.
3. Describe your ability to provide transit and parking options coveringall fifty US states. Do you cover more than just the majormetropolitan areas?
4. Please confirm that the following services are offered:• Commuter transit pass ordering <Choose One>• Direct pay parking arrangements (specify which providers) <Choose One>• Online parking reimbursement feature for out of pocket
expenses<Choose One>
• Online ordering capabilities <Choose One>• Transit passes mailed to employees homes <Choose One>• Optional debit card to load commuter passes <Choose One>
5. Do you have a partner vendor that is used to fulfill transit passorders?
<Choose One>
6. Describe quality assurance measures that are in place to assurepasses are delivered on a timely basis.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 55
CommuterCommuter questions Response7. Describe fulfillment process from beginning to end. Be sure to
describe the participant experience.8. Describe the process for handling transit passes that exceed the
current IRS monthly limits.9. Has your company worked with transportation business partners
(e.g., transit pass suppliers) in the past?<Choose One>
10. Explain your process for administering various parking/commutingcombinations.
11. Describe your process for interfacing with vanpool companies, bothpublic and private.
12. Do you support annual transit passes? <Choose One>• Which metro areas?
13. Do you offer vouchers in addition to transit passes? Indicate themethods available for distribution of vouchers.• Do you have the ability to mail vouchers to a single employer
location for distribution?• How do you handle vouchers that may be lost in the mail or
misplaced?14. Do you allow reimbursements of cash expenditures? <Choose One>
• Is this reimbursement limited to situations where participantshave just begun to participate in the plan?
<Choose One>
15. Describe your process for keeping up-to-date on transit fares andmedia; transit companies, both private and public; and vanpoolcompanies, both private and public.
16. How do you stay current with IRS requirements for both commutingand parking?• How do you communicate these changes to clients and their
employees?17. Is there a monthly deadline for changing elections? <Choose One>
• Are there a maximum number of changes that can be madeannually?
<Choose One>
─ If yes, indicate options for the frequency of employeecommuter elections (i.e., monthly, quarterly, annually).
18. Does your system send e-mail reminders and confirmations toemployees?
<Choose One>
19. What account information is available to employees on thewebsite?• Through an IVR system?
OtherOther questions Response1. If the plan is terminated, what run-out services do you provide?
• What are the associated costs?2. How many current members are enrolled in your health, dependent
and limited purpose FSA programs? Please provide information oneach for the past three years.
3. Will your organization provide participants with a year-endoutstanding balance report separately identifying any amountsforfeited for each FSA account?
<Choose One>
4. Will your organization provide participants with separate notificationat the end of each submission regarding transactions requiringsubstantiation (at no additional cost)?
<Choose One>
6 . 2 H E A L T H R E I M B U R S E M E N T A R R A N G E M E N T ( H R A )Client services – reporting

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 56
HRA – Client services – reporting questions Response1. What is the frequency an employee receives an account
statement?Choose one
2. How do you provide account statements (e.g., online, e-mail,secured website, paper)?
3. Can you provide utilization reporting? If so, how frequent can thistype of reporting be provided? Will there be any additional chargesassociated with this service?
(Select)
4. If offered both HRA and FSA, can the client designate which fundscan be used first?
System capabilitiesHRA – Systems capabilities questions Response1. Can a portion of a single HRA account be designated for specific use
by percentage?(Select)
• If yes, is a separate account supported or required for thefollowing:
(Select)
2. Can a portion of a single HRA account be designated for specific useby fixed dollar amount?
(Select)
• If yes, is a separate account supported or required for thefollowing:
(Select)
3. Can the employer specify the list of eligible expenses? (Select)• If yes, is a separate account supported or required for the
following:(Select)
4. Can the list of eligible expenses differ from the “insurance” plan? (Select)• If yes, is a separate account supported or required for the
following:(Select)
5. Can you administer post-deductible HRAs? (Select)• If yes, is a separate account supported or required for the
following:(Select)
6. Are accounts member-specific? (Select)• If yes, is a separate account supported or required for the
following:(Select)
7. Are accounts employee-specific? (Select)• If yes, is a separate account supported or required for the
following:(Select)
8. Can contribution amounts vary by employee salary? (Select)• If yes, is a separate account supported or required for the
following:(Select)
9. Can contribution amounts vary between singles and families? (Select)• If yes, is a separate account supported or required for the
following:(Select)
10. Are accounts that vary by employee compliance with healthmaintenance or health status supported?
(Select)
• If yes, is a separate account supported or required for thefollowing:
(Select)
11. Are members able to accumulate/carry over fund balances year-to-year?
<Choose One>
12. Can each plan sponsor organization indicate payment orderpreference (e.g., FSA versus HRA)?
<Choose One>
13. Can you administer separate and distinct eligible charges for HRAand FSA?
<Choose One>
14. Can you provide standalone HRAs for the following:• Current use by active employees? <Choose One>
• Future/deferred use for retiree medical? <Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 57
System capabilitiesHRA – Systems capabilities questions Response15. Can you administer HRAs by:
• Member-specific accounts established and maintained by yourorganization? <Choose One>
• Member-specific accounts established and maintained byanother vendor?
<Choose One>
• Employer-specific accounts that are established and maintainedby your organization?
<Choose One>
• Employer-specific accounts that are established and maintainedby another vendor?
<Choose One>
• Individual member accounts not established, althoughtransaction and balance information is stored at the memberlevel?
<Choose One>
• Detailed transaction and balance information for each membermaintained where the employer holds actual funds?
<Choose One>
• Other, please specify: <Choose One>16. Does the employer have to pass account contributions to you? <Choose One>
• How do you administer the funding of claims payments?17. What are your transactional rules/limitations for HRAs?18. Can you limit expenses as defined by IRC Section 213(d)? <Choose One>19. Are there investment options for HRA balances? <Choose One>
• If yes, who is responsible for providing these services?20. Are stored-value debit cards with HRA dollars offered? <Choose One>
• If yes, is this a required element of the plandesign/administration?
• If yes, are there any additional costs or fees?• Can the debit card be used as the member ID card for the
“insurance plan”?<Choose One>
21. Can you administer the HRA without administering the insuranceportion of a CDH plan?
<Choose One>
• If yes, is this a required element of the plandesign/administration?
22. Do you coordinate the HRA with other vendors if the followingcoverages are carved-out?• Pharmacy <Choose One>• Behavioral health <Choose One>• FSA <Choose One>
23. Will you receive eligibility files/data from other vendors? <Choose One>• What is your standard frequency?• If a client required a different data transfer frequency, would
there be any associated charges or fees?<Choose One>
24. Do you currently pay providers directly from an HRA? <Choose One>• If yes, is this a required element of the plan
design/administration?• If no, is this functionality planned for the future?
─ If yes, please provide the targeted release date.25. Can participants elect to have automatic reimbursement or elective
reimbursement?<Choose One>
26. If the HRA pays providers directly, please describe the preferredmethod/process for collecting funds that are the member’sresponsibility (due to insufficient HRA funds) but are not collected atthe time of service.• Does this method differ for medical services and prescription
drugs?<Choose One>
27. Do you have the capabilities for preventing double reimbursement(i.e., HRA and FSA) in the event of duplicate coverage?
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 58
System capabilitiesHRA – Systems capabilities questions Response28. What are the supported approaches for HRAs in each of the
following events?• Adding coverage for family members (moving up in tiers)
─ Leave HRA and insurance deductibles static for theremainder of the plan year
─ Prorate HRA and insurance deductible weekly─ Prorate HRA and insurance deductible monthly─ Prorate HRA and insurance deductible quarterly─ Prorate HRA and insurance deductible semi-annually─ Other (please specify)
• Removing coverage for family members (moving down in tiers)─ Leave HRA and insurance deductibles static for the
remainder of the plan year
─ Prorate HRA and insurance deductible weekly─ Prorate HRA and insurance deductible monthly─ Prorate HRA and insurance deductible quarterly─ Prorate HRA and insurance deductible semi-annually─ Other (please specify)
• Separation─ Both employee and spouse retain entire accumulated HRA
balance (if spouse elects COBRA)─ Employee and spouse divide accumulated HRA balance
evenly (if spouse elects COBRA)─ Employee and spouse divide accumulated HRA balance
based on coverage tier selected post-separation[employee + child(ren) retains more than employee only]
─ Other (please specify)• New Hire
─ Prorate HRA and insurance deductible weekly
─ Prorate HRA and insurance deductible monthly─ Prorate HRA and insurance deductible quarterly─ Prorate HRA and insurance deductible semi-annually─ Other (please specify)
• Changing plans to non-HRA-based plan─ Employee forfeits HRA balance─ Employee retains HRA balance─ Other (please specify)
• Changing plans to HRA-based plan─ Employee forfeits HRA balance
─ Employee retains HRA balance─ Other (please specify)
• Leaving the company and returning (at a later date)─ Employee forfeits HRA balance
─ Employee retains HRA balance─ Other (please specify)
• Retiring from the company (pre-65)─ Employee forfeits HRA balance
─ Employee retains HRA balance─ Other (please specify)

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 59
System capabilitiesHRA – Systems capabilities questions Response
• Retiring from the company (post-65)─ Employee forfeits HRA balance
─ Employee retains HRA balance─ Other (please specify)
• Death of employee─ HRA balance forfeited─ Other covered members retain HRA balance only if they
elect COBRA─ Other covered members retain HRA balance regardless of
continued insurance coverage─ Other (please specify)
29. How long can you retain an HRA once the participant hasterminated?
30. Describe your various claims payment processes by type (EFT,check, etc.) from receipt to processing to posting through payment.
31. Describe the workflow related to exchanging data with a health planto administer an integrated HDHP/ HSA. Please show what data issent to whom and when and how the data that you collect isreflected in your systems.• Who tracks the data flow and how long does each step take?
32. For claims that are not reimbursed via a streamlined process or adebit card, what documentation must accompany each claim forreimbursement?• Will participants be able to submit reimbursement requests by
fax?<Choose One>
• Will participants be able to submit reimbursement requestselectronically?
<Choose One>
• Describe the process of how claims can be submitted.33. Please detail how you administer mid-year changes to an HRA.
• How do you calculate the new reimbursable maximum and/ormaintain separate reimbursable maximums?
34. Who conducts quality reviews for reimbursement accuracy?• Are quality reviews performed pre- or post-disbursement?• How often are audits performed?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 60
VII. CARE MANAGEMENT QUESTIONNAIRE7 . 1 C A R E M A N A G E M E N T
For the purposes of this RFP, Care Management encompasses 3 types of programs: DiseaseManagement, Custom Care Management, and Case Management.1) Disease Management - Services consist of interactive communication between an individual and a
health professional or expert system through various modalities (e.g., telephonic, email, online, face-to-face, etc.), to address individuals with chronic conditions, typically those who are moderate to lowchronically ill. Conditions address might include conditions such as, but not limited to: asthma, COPD,CHF, CAD, depression, diabetes, maternity, obesity, etc.
2) Custom Care Management – A customized program to proactively outreach and manage the highestrisk/cost patients. Expertise in conditions such as cancer care, neonatology, maternal health, renaldisease & behavioral/mental health are useful. Includes a dedicated nurse for employees, addressgaps in care, consist of an integrated medical team, has extended phone hours and measurablereferrals and/or warm transfers to other vendor partners. Utilizes evidence based best practices incounseling and support.
3) Case Management – the process of assessment, planning, facilitation, care coordination, evaluation,and advocacy for options and services to meet an individual’s health needs, promoting cost-effectivetreatments and quality outcomes.
A service that identifies members with potentially catastrophic illnesses, high cost claims andhospitalizations and actively coordinating their care in an effort to reduce expenses and improve themedical care they receive.
7 . 2 G E N E R A L Q U E S T I O N S7.2.1 Define what services are subject to pre-authorization. Please outline the pre-authorization
program for these services and supply details on how the program works.2000 words
7.2.2 Describe the process of moving members out of an inpatient setting into a less costly home healthcare setting, if appropriate. Is this directed by the physician, or is your organization involved inreviewing clinical notes?
2000 words
7.2.3 Do you have customizable solutions for the plan sponsor and the family?1: Yes,2: No3: Yes, with Deviations
7 . 3 H E AL T H A S S E S S M E N T7.3.1 Please provide a description of your health assessment and wellness offerings that are
standard/included in pricing. (Please DO NOT provide details around your wellness buy-upoptions)
500 words
7.3.2 Do you agree that these services may be deactivated without any penalty:AgreeAgree, with exception

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 61
Disagree
7 . 4 D I S E A S E M A N A G E M E N T7.4.1 What is the branded name that you have given your Disease Management Service?
Unlimited
7.4.2 Briefly state the value proposition.Unlimited.
7.4.3 Indicate the year in which you fully offered this service.Unlimited.
7.4.4 What is you standard implementation timeframe for this service from kick-off to programlaunch date?Single, Pull-down list.1: 30 Days,2: 60 Days,3: 90 Days,4: 120 Days,5: 180 Days
7.4.5 How does this service integrate with other services offered by your organization?Unlimited.
7.4.6 Is this service offered as a stand-alone product?1: Yes,2: No3: Yes, with Deviations
7.4.7 What types of programs are offered to the participant? Indicate if they are sold bundled togetheror on a stand-alone basis for employer purchase and state the program names as they are presentedto the participant. Enter “Not Applicable” as needed.
Program Type Program Name Purchase Package
Arthritis Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Asthma Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Autoimmune disorders Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Cancer Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Chronic Obstructive Pulmonary Disease (COPD) Unlimited. Single, Pull-down list.
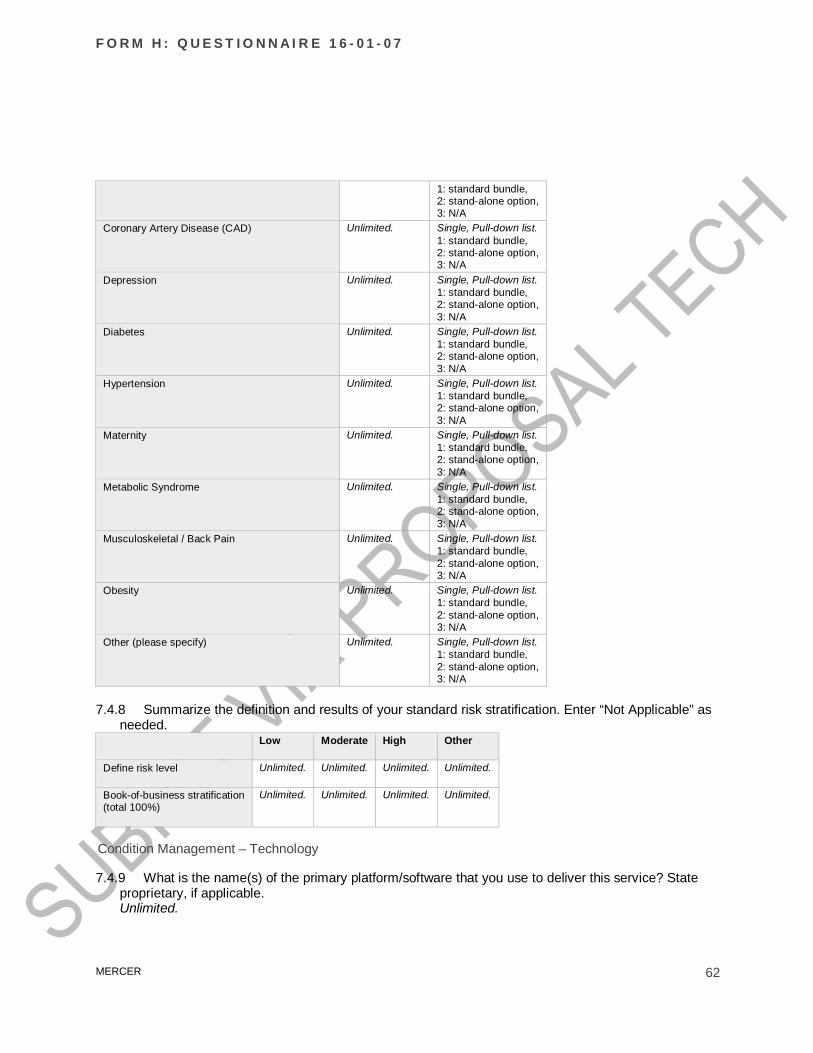
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 62
1: standard bundle,2: stand-alone option,3: N/A
Coronary Artery Disease (CAD) Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Depression Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Diabetes Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Hypertension Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Maternity Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Metabolic Syndrome Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Musculoskeletal / Back Pain Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Obesity Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
Other (please specify) Unlimited. Single, Pull-down list.1: standard bundle,2: stand-alone option,3: N/A
7.4.8 Summarize the definition and results of your standard risk stratification. Enter “Not Applicable” asneeded.
Low Moderate High Other
Define risk level Unlimited. Unlimited. Unlimited. Unlimited.
Book-of-business stratification(total 100%)
Unlimited. Unlimited. Unlimited. Unlimited.
Condition Management – Technology
7.4.9 What is the name(s) of the primary platform/software that you use to deliver this service? Stateproprietary, if applicable.Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 63
7.4.10 If you do re-stratify for identified programs, how often?Unlimited.
7.4.11 Does your system automatically adjust the risk/acuity level of an individual upon receipt of claimsdata on an ongoing basis?Single, Radio group.1: Yes,2: No
7.4.12 If your system automatically adjusts risk/acuity levels, how are the clinical managers made awareof changes to individuals that they may be assigned to working with?Unlimited.
7.4.13 What predictive modeling tools that enable you to predict, assess and monitor readiness tochange?Unlimited.
7.4.14 Describe the tool that you have to monitor migration of individuals and/or cohorts within anemployer's population and how it is used in the delivery of services.Unlimited.
7.4.15 Describe the tool(s) that you use to assess readiness to change and how it is used in the deliveryof services.Unlimited.
7.4.16 Can coach/clinicians view the participant's activity on goals and trackers that may be available onyour portal?Single, Radio group.1: Yes,2: No
7.4.17 How often do you update your identification/stratification methodology?Unlimited.
7.4.18 Indicate how the program is delivered (mail/phone/email/onsite/etc.) to the participant by risklevel.
Program Type Low Moderate High Other
Arthritis Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 64
8: N/A 8: N/A 8: N/A 8: N/AAsthma Multi, Checkboxes.
1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Autoimmunedisorders
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Cancer Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Chronic ObstructivePulmonary Disease(COPD)
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 65
directionalcommunication betweenorganization andindividual),8: N/A
directionalcommunication betweenorganization andindividual),8: N/A
directionalcommunication betweenorganization andindividual),8: N/A
directionalcommunication betweenorganization andindividual),8: N/A
Coronary ArteryDisease (CAD)
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Depression Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Diabetes Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Hypertension Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one on
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one on
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one on
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one on

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 66
one),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
one),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
one),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
one),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Maternity Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
MetabolicSyndrome
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Musculoskeletal /Back Pain
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Obesity Multi, Checkboxes.1: Phone-based,2: Email,
Multi, Checkboxes.1: Phone-based,2: Email,
Multi, Checkboxes.1: Phone-based,2: Email,
Multi, Checkboxes.1: Phone-based,2: Email,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 67
3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Other (pleasespecify)
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
Multi, Checkboxes.1: Phone-based,2: Email,3: Mobile (SMS),4: Web-based method(other than email),5: In person (one onone),6: On site groupclasses,7: Paper-based (bi-directionalcommunication betweenorganization andindividual),8: N/A
7.4.19 Are participants assigned a primary coach/clinician with whom they work on an ongoing basis?Single, Radio group.1: Yes,2: No
7.4.20 What is your organization's hierarchy for clinical management services? Unlimited.
7.4.21 If a participant has co-morbid conditions, please outline your hierarchy to determine coachingpriority.Unlimited.
7.4.22 Describe any promotion tactics that are specific to engaging members in Disease Managementprograms.Unlimited.
7.4.23 How does your financial model work (e.g., Per Employee Per Month (PEPM), Per Participant,etc.)?Unlimited.
7 . 5 C U S T O M C A R E M A N A G E M E N T ( O V E R V I E W )For the purposes of this RFP, Custom Care Management is a customized program to proactively outreachand manage the highest risk/cost patients. Expertise in conditions such as cancer care, neonatology,
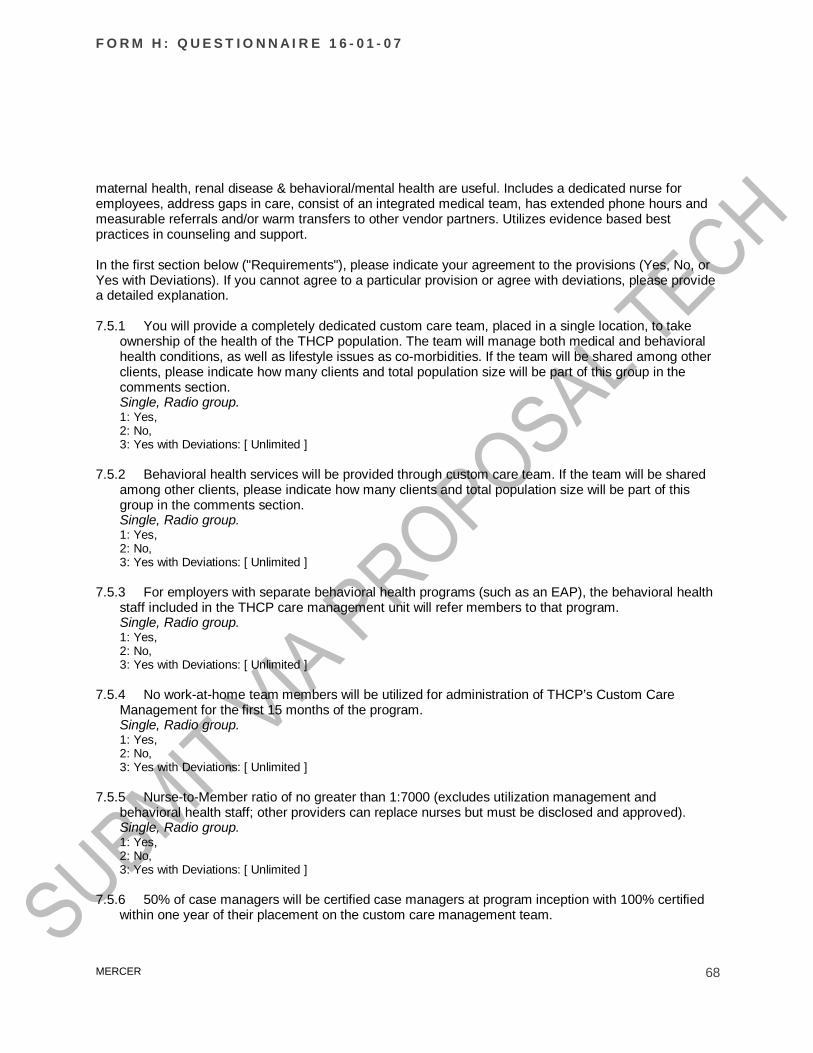
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 68
maternal health, renal disease & behavioral/mental health are useful. Includes a dedicated nurse foremployees, address gaps in care, consist of an integrated medical team, has extended phone hours andmeasurable referrals and/or warm transfers to other vendor partners. Utilizes evidence based bestpractices in counseling and support.
In the first section below ("Requirements"), please indicate your agreement to the provisions (Yes, No, orYes with Deviations). If you cannot agree to a particular provision or agree with deviations, please providea detailed explanation.
7.5.1 You will provide a completely dedicated custom care team, placed in a single location, to takeownership of the health of the THCP population. The team will manage both medical and behavioralhealth conditions, as well as lifestyle issues as co-morbidities. If the team will be shared among otherclients, please indicate how many clients and total population size will be part of this group in thecomments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.2 Behavioral health services will be provided through custom care team. If the team will be sharedamong other clients, please indicate how many clients and total population size will be part of thisgroup in the comments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.3 For employers with separate behavioral health programs (such as an EAP), the behavioral healthstaff included in the THCP care management unit will refer members to that program.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.4 No work-at-home team members will be utilized for administration of THCP’s Custom CareManagement for the first 15 months of the program.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.5 Nurse-to-Member ratio of no greater than 1:7000 (excludes utilization management andbehavioral health staff; other providers can replace nurses but must be disclosed and approved).Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.6 50% of case managers will be certified case managers at program inception with 100% certifiedwithin one year of their placement on the custom care management team.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 69
Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.7 Custom care team will be available Monday through Friday from 6 AM until 8 PM Central Timeand will operate from 8 AM until 3 PM Central Time on weekends.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.8 Describe in detail your capabilities for utilization review/management. [unlimited]
7.5.9 Utilization Management: You will provide pre-authorization for:Response Yes with
Deviationsa. Elective inpatient admissions. Single, Radio group.
1: Yes,2: No,3: Yes with Deviations (explainin next column)
Unlimited.Nothingrequired
b. Mutually agreed upon list of outpatientprocedures
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explainin next column)
Unlimited.Nothingrequired
c. Mutually agreed upon list of radiology/imagingservices
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explainin next column)
Unlimited.Nothingrequired
d. Chemotherapy administered in outpatient centeror physician's office
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explainin next column)
Unlimited.Nothingrequired
e. Specialty drugs administered through themedical plan
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explainin next column)
Unlimited.Nothingrequired
7.5.10 You will perform a post-discharge plan and follow-up call within 48 hours by the custom care teamfor every discharge.Single, Radio group.1: Yes,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 70
2: No,3: Yes with Deviations: [ Unlimited ]
7.5.11 There will be no “gold-carding” of facilities excusing them from the utilization managementprocess.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.12 This team will also be responsible for the traditional functions of:Response Yes with
Deviationsa. Case management Single, Radio group.
1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
b. Complex case management Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
c. Pre and post discharge phone calls Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
d. High acuity condition management (all conditionsexcept transplant)
Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
e. Treatment decision support Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
f. Gaps-in-care follow-up Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
g. Answering nurseline calls during regular custom caremanagement team hours
Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 71
h. Behavioral health case management Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
i. Coordination with all internally and externally providedprograms by THCP employers to their members
Single, Radio group.1: Yes,2: No,3: Yes with Deviations(explain in next column)
Unlimited.Nothingrequired
7.5.13 Nurses or other professionals on the custom care team will have specific expertise in cancer care,neonatology, maternal health, renal disease, rehabilitative medicine and mental health.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.14 You will staff at least one dedicated social worker.If the team will be shared among other clients, please indicate how many clients and total populationsize will be part of this group in the comments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.15 All nurses will have some training in the basics of lifestyle management including nutrition,smoking cessation and exercise physiology so they can support co-morbid lifestyle issues in membersthey are managing.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.16 You will staff a full-time nurse manager who has ultimate responsibility for the management of theoverall population and who is responsible to make sure the right people are being managed at theright time by the right resource. If the team member will be shared among other clients, pleaseindicate how many clients and total population size will be part of this group in the comments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.17 You will staff a full-time nurse in charge of training the custom care team and the continualmonitoring of team performance and continuous skill improvement. In addition, this individual ischarged with making sure that at time of unit opening, 50% of case managers are certified casemanagers at program inception with 100% certified within one year of their placement on the customcare management team.Single, Radio group.1: Yes,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 72
2: No,3: Yes with Deviations: [ Unlimited ]
7.5.18 You will staff a team leader for every eight nurse case managers, who serves as a mentor to theteam, identifies issues, reviews complex cases, assures proper use of other team resources, andassures that the caseload assigned to his/her team is being managed in the best way possible. Theteam leaders will report to the nurse manager.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.19 You will staff a dedicated medical director, who shares responsibility with the nurse manager forthe management of the overall health of the THCP population. The dedicated medical directoroversees the work of other medical directors on THCP cases and will spend at least 50% of his/hertime in direct consultation with treating physicians.If the team member will be shared among other clients, please indicate how many clients and totalpopulation size will be part of this group in the comments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.20 You will staff a designated pharmacist, who will provide consultation to the custom care team andwho will review the cases of all patients taking more than six medications on an ongoing basis. If theteam member will be shared among other clients, please indicate how many clients and totalpopulation size will be part of this group in the comments section.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.21 You will provide a dedicated Behavioral Health team leader.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.22 If the team member will be shared among other clients, please indicate how many clients andtotal population size will be part of this group.
Unlimited
7.5.23 Behavioral health members of the team will provide intake for mental health referrals, bothinpatient and outpatient, including helping a member find the right mental health provider, a conciergeservice to help members make appointments with mental health providers, and providing generalinformation about the behavioral health benefit.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 73
7.5.24 Behavioral health team members will also provide consultation to the rest of the team on casesthat may have a behavioral health component.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.25 For members with primary behavioral health needs, the behavioral health specialists on the teamwill provide comprehensive management, including concurrent review, discharge planning, casemanagement, and short-term supportive interventions. (Note: This may be transferred to anothervendor should an individual employer choose this option). If yes, please describe this process.Single, Radio group.1: Yes, Comments2: No,3: Yes with Deviations: [ Unlimited ]
7.5.26 For members with complex medical problems, they will be managed in a proactive, ongoingfashion, in a longitudinal manner, which includes not having case management continually turned onand off with each admission.Single, Radio group.If yes, please describe this process.1: Yes, comments2: No,3: Yes with Deviations: [ Unlimited ]
7.5.27 The custom care team will reach out to members at designated times, including but not limited to:Response Yes with
Deviationsa. Calls to schedule elective admissions (exceptpregnancy)
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
b. Post-discharge calls to the entire population Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
c. All members who are identified as likely to be admittedor have high costs (through predictive modeling)
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 74
d. All members with chronic conditions identified ashaving gaps in their care or having an emergency roomvisit or admission due to that condition
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
e. All members with a mental health related emergencyroom visit
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
f. All members with cancer Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
g. All members identified with chronic kidney disease oron dialysis
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
h. All members being evaluated for possible organtransplantation
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
i. All members identified with a gap-in-care until the gap isclosed (contact not necessarily telephonic)
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
j. All members on disability (except pregnancy), who arenot already being managed
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 75
k. All members incurring greater than $50,000 in medicalcosts
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
l. All members receiving a specialty medication SHOULDWE DEFINE BY COST?
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
m. Any member identified with a condition that qualifiesfor treatment decision support
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
n. All members who call into nurseline after hours willreceive a follow up call from the custom care team
Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
o. All members being evaluated for hospice Single, Radiogroup.1: Yes,2: No,3: Yes with Deviations(explain in nextcolumn)
Unlimited.Nothingrequired
The custom care team will take inbound calls in the following situations:Response Yes with
Deviationsa. Any member that wants to discuss a medical issue Single, Radio
group.1: Yes,2: No,3: Yes withDeviations (explainin next column)
Unlimited.Nothingrequired
b. Warm transfers from the customer service team formembers who meet any of the criteria for an outreach call
Single, Radiogroup.1: Yes,
Unlimited.Nothing

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 76
2: No,3: Yes withDeviations (explainin next column)
required
c. Nurseline calls during the hours the team is operating Single, Radiogroup.1: Yes,2: No,3: Yes withDeviations (explainin next column)
Unlimited.Nothingrequired
d. Behavioral health team members will intake mental healthreferrals, both inpatient and outpatient.
Single, Radiogroup.1: Yes,2: No,3: Yes withDeviations (explainin next column)
Unlimited.Nothingrequired
e. Behavioral health team members will help a member findthe right mental health provider, make appointments withmental health providers, and provide general informationabout the behavioral health benefit.
Single, Radiogroup.1: Yes,2: No,3: Yes withDeviations (explainin next column)
Unlimited.Nothingrequired
7.5.28 Describe any promotion tactics that are specific to engaging members in Custom CareManagement programs.Unlimited.
7.5.29 The custom care team will support the use of high quality providers and centers ofexcellence/PCMH, and they will help members find the best provider for their condition.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.30 You will support the Continuous Quality Improvement Process for the care management program.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.31 The custom care team will interact with members through multiple communication channels,including:
Response Yes with Deviationsa. Telephonic Single, Radio group.
1: Yes,2: No,3: Yes with Deviations (explain in next column)
Unlimited.Nothing required
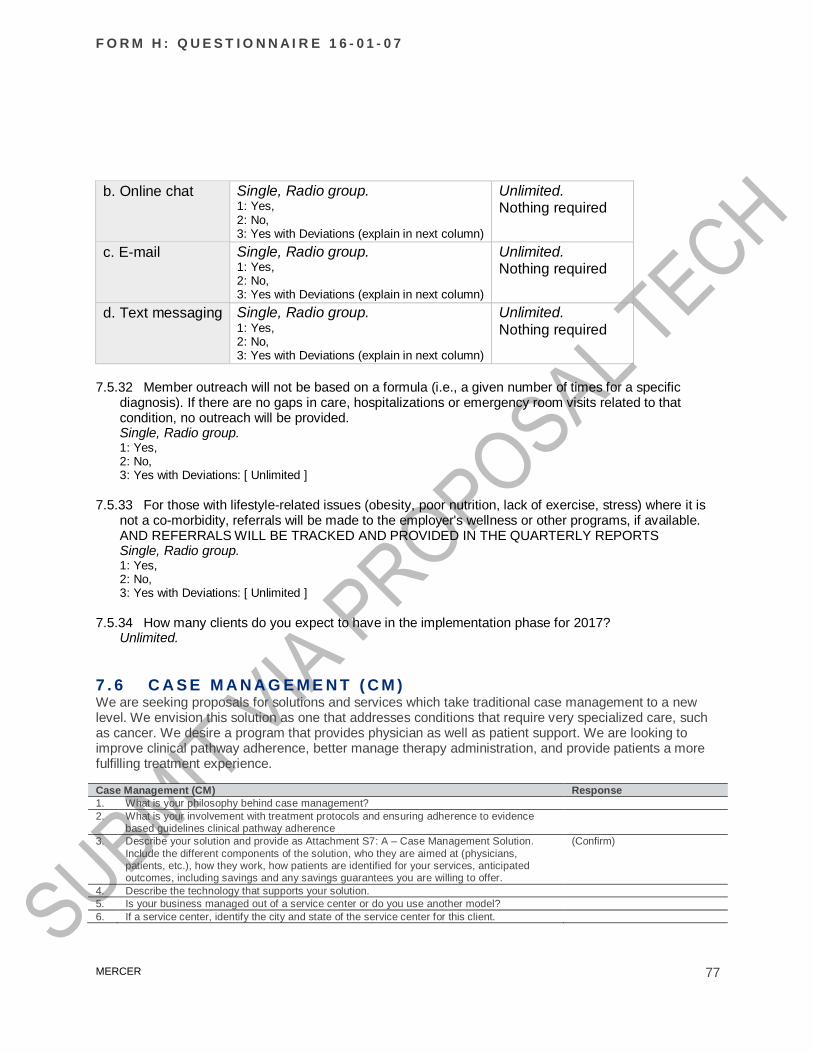
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 77
b. Online chat Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in next column)
Unlimited.Nothing required
c. E-mail Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in next column)
Unlimited.Nothing required
d. Text messaging Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in next column)
Unlimited.Nothing required
7.5.32 Member outreach will not be based on a formula (i.e., a given number of times for a specificdiagnosis). If there are no gaps in care, hospitalizations or emergency room visits related to thatcondition, no outreach will be provided.Single, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.33 For those with lifestyle-related issues (obesity, poor nutrition, lack of exercise, stress) where it isnot a co-morbidity, referrals will be made to the employer's wellness or other programs, if available.AND REFERRALS WILL BE TRACKED AND PROVIDED IN THE QUARTERLY REPORTSSingle, Radio group.1: Yes,2: No,3: Yes with Deviations: [ Unlimited ]
7.5.34 How many clients do you expect to have in the implementation phase for 2017?Unlimited.
7 . 6 C A S E M A N A G E M E N T ( C M )We are seeking proposals for solutions and services which take traditional case management to a newlevel. We envision this solution as one that addresses conditions that require very specialized care, suchas cancer. We desire a program that provides physician as well as patient support. We are looking toimprove clinical pathway adherence, better manage therapy administration, and provide patients a morefulfilling treatment experience.
Case Management (CM) Response1. What is your philosophy behind case management?2. What is your involvement with treatment protocols and ensuring adherence to evidence
based guidelines clinical pathway adherence3. Describe your solution and provide as Attachment S7: A – Case Management Solution.
Include the different components of the solution, who they are aimed at (physicians,patients, etc.), how they work, how patients are identified for your services, anticipatedoutcomes, including savings and any savings guarantees you are willing to offer.
(Confirm)
4. Describe the technology that supports your solution.5. Is your business managed out of a service center or do you use another model?6. If a service center, identify the city and state of the service center for this client.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 78
Case Management (CM) Response7. If another model, please describe.8. Identify which of the following are included in the scope of your specialty CM program:
CancerNeonatal Intensive Care Unit (NICU)Chronic Renal Disease/ESRD Other (provide specifics)
Explanation9. What are the qualifications of the clinical personnel who would service the District
accounts?10. How would you integrate with the other health and wellness programs that THCP offers?11. Is your methodology of case management remote or in-hospital? What is engagement %
for remote vs in-hospital? Provide a guide for a member through an inpatient experience asAttachment S7: B – Case Management Member Guide.
12. What type of outreach can members expect? What type of assistance can be provided fortheir family? Provide data to support additional level of support and engagement asAttachment S7: C – Case Management Member Support
7 . 7 E N G A G E M E N T7.7.1 Provide your definition of member “participation” and “engagement” in Disease Management or
Custom Care Management (i.e., when is a member counted as a “participant” or “engaged” in yourreporting).
Unlimited.
7.7.2 Provide an overview of the process that the coach/clinician uses to help the participant set initialgoals?
Unlimited.
7.7.3 Are goals modified at all during the duration of the coaching intervention?Single, Radio group.1: Yes,2: No
7.7.4 Are members in all acuity levels eligible for nurse/telephonic interventions?Single, Radio group.1: Yes,2: No, Explain: [ Unlimited ]
7.7.5 Does the frequency of coaching calls vary by acuity level?Single, Radio group.1: Yes,2: No
7.7.6 Do participants ever migrate to a lower acuity level (graduate) from the Condition Managementprogram?Single, Radio group.1: Yes,2: No
7.7.7 If yes, do you have a set criteria to determine if a participant is eligible to migrate to a lower acuitylevel?Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 79
7.7.8 Who determines this criteria?Unlimited.
7.7.9 Do nurses have the ability to migrate participants to a lower acuity level?Single, Radio group.1: Yes,2: No
7.7.10 If No, does the medical director have the ability to migrate participants to a lower acuity level?Unlimited.
7.7.11 Can coaches/clinicians change the set frequency of coaching interventions per member?Single, Radio group.1: Yes,2: No
7.7.12 If frequency of coaching interventions is changed, is it based on achievement of participant goals?Unlimited.
7.7.13 Has your organization established any practices to manage a member's health once they aredischarged from a hospital and are finishing up case management?Single, Radio group.1: Yes,2: No
7.7.14 How does your organization minimize false positives and ensure that outreach is appropriate?Unlimited.
7.7.15 Does your organization have a set criteria to determine the appropriate number of calls aparticipant should be engaged in based on their acuity level?Single, Radio group.1: Yes,2: No
7.7.16 Indicate the modalities through which participants can communicate with their coach/clinician:Multi, Checkboxes.1: Phone,2: Secure email,3: Instant chat via portal,4: Text messaging,5: Other
7.7.17 Your organization has experience in coordinating and exchanging data with data warehousevendors, health management vendors, and on-site clinics to promote health improvement initiatives.Single, Radio group.1: Agree,2: Agree with exception (explain): [ Unlimited ] ,3: Disagree (explain): [ Unlimited ]

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 80
7.7.18 Please describe any innovative technologies you incorporate to improve your service (i.e. SMSmessaging, live chat communications, etc…)500 words.
7 . 8 R e p o r t i n g a n d R e s u l t s7.8.1 Describe the standard reports provided for your Disease Management service. Enter “None”, “Not
Applicable” or “Not Available” as needed.Report Name Description Frequency Time between close of reporting period and delivery to client
1 Unlimited. Unlimited. Unlimited. Unlimited.
2 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
3 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
4 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
5 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
6 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7.8.2 Describe the standard reports provided for your Custom Care Management service. Enter “None”,“Not Applicable” or “Not Available” as needed.Report Type Standard/Custom/
Not AvailableFrequency Time between close of
reporting period anddelivery to client
1 General MemberReports
Single, Radio group.1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
2 Care management Linereports (Call centerperformance)
Single, Radio group.1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
3 Provider Reports Single, Radio group.1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
4 Complaint Reports Single, Radio group.1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
5 Utilization Reports Single, Radio group.1: Standard,2: Custom,
Unlimited. Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 81
3:Not available: [ Unlimited ]6 Staffing Reports Single, Radio group.
1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
7 Annual Reports Single, Radio group.1: Standard,2: Custom,3:Not available: [ Unlimited ]
Unlimited. Unlimited.
7.8.3 Describe the standard reports provided for your Case Management service. Enter “None”, “NotApplicable” or “Not Available” as needed.Report Name Description Frequency Time between close of reporting period and delivery to client
1 Unlimited. Unlimited. Unlimited. Unlimited.
2 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
3 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
4 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
5 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
6 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7.8.4 What key metrics are used to measure the success of this service?Metric Frequency
Coaching Program (phone / e-coaching)
Identified candidates for programs (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Identified candidates by risk stratification level (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Identified candidates attempted but unable to reach (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Tracks types of reasons for unable to reach (# and %) Multi, Checkboxes.1: Online report access,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 82
2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Enrolled participants by risk stratification level (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Enrolled participants by condition / program (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Enrolled participants who have voluntarily dropped out (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Track types of reasons for participants dropping out (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Average volume of emails exchanged (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Average volume of coaching calls completed (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Participant progress through telephonic coaching program (# and %) Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Participant completion of phone-based programs by program type Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Mail-based Program
Participant enrollment within your mail-based programs by program type Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,
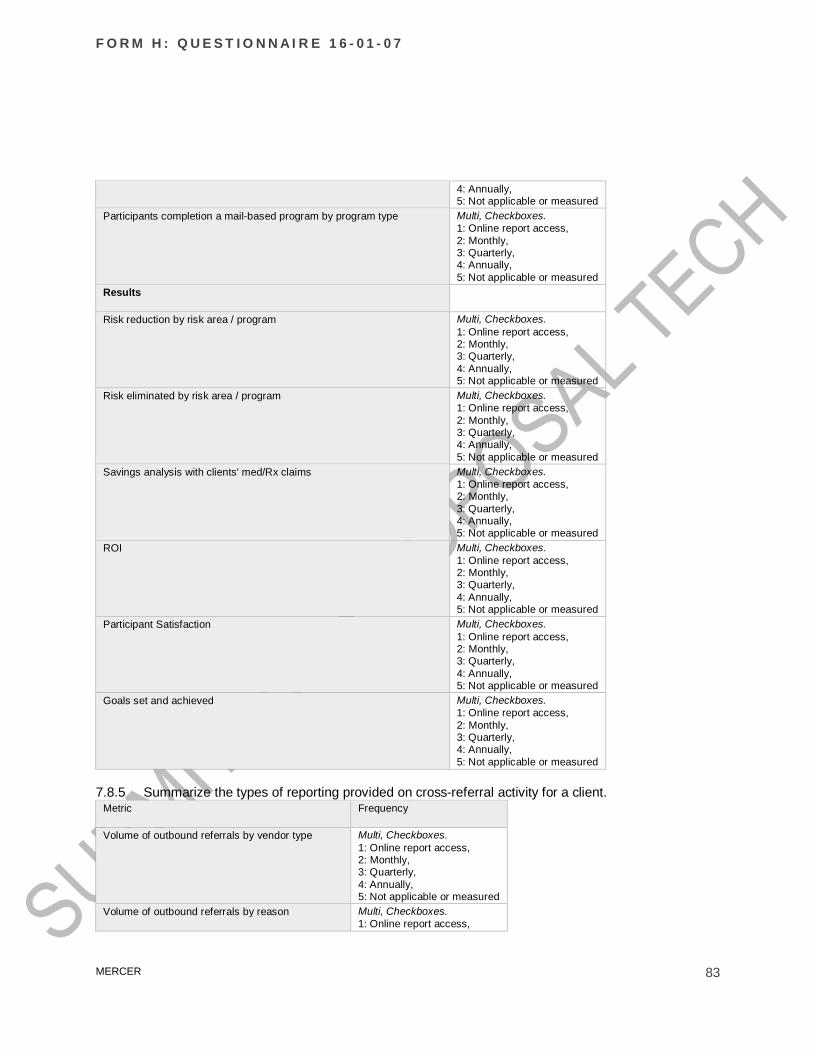
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 83
4: Annually,5: Not applicable or measured
Participants completion a mail-based program by program type Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Results
Risk reduction by risk area / program Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Risk eliminated by risk area / program Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Savings analysis with clients' med/Rx claims Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
ROI Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Participant Satisfaction Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Goals set and achieved Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
7.8.5 Summarize the types of reporting provided on cross-referral activity for a client.Metric Frequency
Volume of outbound referrals by vendor type Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of outbound referrals by reason Multi, Checkboxes.1: Online report access,

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 84
2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of outbound referrals by method of transfer Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of inbound referrals by vendor type Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of inbound referrals by reason Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of inbound referrals by method of transfer Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
Volume of successful program enrollments Multi, Checkboxes.1: Online report access,2: Monthly,3: Quarterly,4: Annually,5: Not applicable or measured
7.8.6 For cross referral reporting, is there a limit to the types of vendors that are included in thestandard reporting?Unlimited.
7.8.7 Summarize the ROI methodology used in your standard reporting.Unlimited.
7.8.8 Describe any cohort analysis reports that you deliver within your standard reporting package. Forexample, tracking a group of program participants over more than one reporting cycles.Unlimited.
7.8.9 List recently peer-reviewed articles on results (e.g. participation, outcomes) of this service thatyour organization has published in a peer-reviewed periodical. Enter “None” or “Not Applicable” asneeded. Provide data to support additional level of support and engagement as Attachment S7: D –Published Works
Title Date PublicationUnlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 85
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
To the month.Nothing required
Unlimited.Nothing required
7.8.10 Please detail your BOB participation levels for clients who incentivize participation in DiseaseManagement or Custom Care Management, and those who do not incentivize participation.Unlimited
7.8.11 Provide identification and participation rates on your total BOB by program. Enter “0” if none, notapplicable or available.
Health Risk Identified Eligibles(% BOB population)
Coaching Participants(% BOB population)
Arthritis Percent. Percent.Asthma Percent. Percent.Autoimmune disorders Percent. Percent.Cancer Percent. Percent.Chronic Obstructive Pulmonary Disease (COPD) Percent. Percent.Coronary Artery Disease (CAD) Percent. Percent.Depression Percent. Percent.Diabetes Percent. Percent.Maternity Percent. Percent.Metabolic Syndrome Percent. Percent.Musculoskeletal / Back Pain Percent. Percent.Obesity Percent. Percent.Other (please specify) Percent.
Nothing requiredPercent.Nothing required
7.8.12 Provide risk reduction rates by program for the last calendar year. Enter “0” if none, not applicableor available.
Health Risk 2013 BOB At-Risk (% BOBpopulation)
2014 BOB At-Risk (% BOBpopulation)
Define At-Risk
Arthritis Percent. Percent. Unlimited.Asthma Percent. Percent. Unlimited.Autoimmune disorders Percent. Percent. Unlimited.Cancer Percent. Percent. Unlimited.Chronic Obstructive PulmonaryDisease (COPD)
Percent. Percent. Unlimited.
Coronary Artery Disease (CAD) Percent. Percent. Unlimited.Depression Percent. Percent. Unlimited.Diabetes Percent. Percent. Unlimited.Hypertension Percent. Percent. Unlimited.Maternity Percent. Percent. Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 86
Metabolic Syndrome Percent. Percent. Unlimited.Musculoskeletal / Back Pain Percent. Percent. Unlimited.Obesity Percent. Percent. Unlimited.Other (please specify) Percent.
Nothing requiredPercent.Nothing required
Unlimited.Nothingrequired
7.8.13 What is your book-of-business average number of minutes for first coaching call duration?Unlimited.
7.8.14 What is your book-of-business average number of minutes for the second coaching call duration?Unlimited.
7.8.15 Please confirm your ability to carve out the following services:Service Yes/No/Not Applicable Cost (PEPM)Utilization ManagementPre-admission supportPost-discharge supportEpisodic Care CoordinationCase ManagementChronic Condition Management
7 . 9 S T A F F A N D Q U A L I T Y A S S U R A N C E C A R E M A N A G E M E N T –7.9.1 Describe the staff that is responsible for development and maintenance of the operations of your
care management services.Unlimited.
7.9.2 Describe the process that is established to make ongoing enhancements to the operations of yourcare management services.Unlimited.
7.9.3 Does your organization offer flexible and/or extended call center hours?Unlimited.
7.9.4 Please select all of the languages accommodated through your call center and clinical staffMulti, Checkboxes.1: French,2: Spanish,3: Arabic,4: Mandarin,5: Russian,6: Portuguese,7: German,8: Cantonese,9: Other (list): [ 500 words ]
7.9.5 Provide your business hours of operation. (Central Standard Time). Enter “Not Applicable” asneeded.
Business Unit Monday through FridayFrom
Monday throughFriday
SaturdayFrom
SaturdayTo
SundayFrom
SundayTo

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 87
To
Clinical Resources Unlimited. Unlimited. Unlimited. Unlimited. Unlimited. Unlimited.Customer ServiceCenter
Unlimited. Unlimited. Unlimited. Unlimited. Unlimited. Unlimited.
Unlimited Unlimited. Unlimited. Unlimited. Unlimited. Unlimited. Unlimited.Unlimited Unlimited. Unlimited. Unlimited. Unlimited. Unlimited. Unlimited.
7.9.6 How do you handle coverage during non-business work hours?Unlimited.
7.9.7 Provide details about the size, turnover rate, education and experience of the staff who deliverthis service.
Type of StaffMember
Totalnumberof FTEs(current)
2014turnoverrate
Requiredminimumlevel ofeducation
Predominantlevel ofeducation
SpecialtyCertificationsand CCM/DMTrainings
Requiredminimumnumber ofyears relativeexperience
Averagenumber ofyearsrelativeexperience
CustomerService
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
EnrollmentSpecialists
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
ConditionManagement -non-nurse
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
ConditionManagement -RN
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
ConditionManagement -BSN
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
ConditionManagement -MD
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
ConditionManagement -Pharmacist
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
DedicatedMedicalDirector
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
Social Worker Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
BehavioralHealthClinician
Integer.Nothingrequired
Percent.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothingrequired
Unlimited.Nothing required
Integer.Nothingrequired
Integer.Nothingrequired
Other Integer.Nothing
Percent.Nothing
Unlimited.Nothing
Unlimited.Nothing
Unlimited.Nothing required
Integer.Nothing
Integer.Nothing

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 88
required required required required required required
7.9.8 Is your business managed out of a service center? If no, please explain your model.1: Yes,2: No [Unlimited]
7.9.9 What size employer groups would be considered for a dedicated and designated coaching team?Unlimited.
7.9.10 What is the minimum number of lives to open the unit as described in the RFP?
Service # of lives required for a dedicated unitDisease management integerCustom Care Management integerCase Management integer
7.9.11 Is there a maximum number of lives you can accommodate in 2017?Single, Radio group.1: Yes, how many? [ Unlimited ],2: No
7.9.12 Where are your coaching call center(s) located (City/State/Country)?Unlimited.
7.9.13 What percentage of your coaches/clinicians work remotely from home offices?Percent.
7.9.14 What is the average number of employer groups/clients assigned to a coach/clinician?Unlimited.
7.9.15 What is the ratio of coaches/clinicians to managers?Unlimited.
7.9.16 What is the average ratio of coaches/clinicians to eligible members?Unlimited.
7.9.17 If applicable, explain your philosophy on coach case mix as it relates to participant risk level andcoach specialty.Unlimited.
7.9.18 If applicable, explain your philosophy on coach case mix as it relates to participant risk level andcoach seniority.Unlimited.
7.9.19 What is the average total number of open cases / number of participants that a coach/clinicianworks with at any given time?Unlimited.
7.9.20 Do you monitor participant retention by individual coach/clinician?
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 89
Single, Radio group.1: Yes,2: No
7.9.21 Do you have an operational resource that is dedicated to integration work (i.e. coach or teamleader)?Single, Radio group.1: Yes,2: No
7.9.22 How do you differentiate levels of seniority amongst your coaching staff?Unlimited.
7.9.23 What percentage of your coaching staff is considered senior?Percent.
7.9.24 How frequently do managers review individual coach/clinician case loads throughout the year?Unlimited.
7.9.25 Do you tape coaching calls or record coaching interactions (e.g., record screen interactions)?Single, Radio group.1: Yes (voice recording only),2: Yes (both voice recording and computer screen interaction/screen capture),3: No
7.9.26 How long are call recordings retained?Unlimited.
7.9.27 How many taped calls are audited per coach/clinician per month?Decimal.
7.9.28 Are calls monitored for all coaches/clinicians?Single, Radio group.1: Yes,2: No
7.9.29 How frequently are audited calls reviewed with individual coaches/clinicians?Unlimited.
7.9.30 Are all callers informed that calls are being recorded?Single, Radio group.1: Yes,2: No
7.9.31 How often does the management team meet to review cases and discuss quality improvementpractices?Unlimited.
7.9.32 Explain your approach to training new coaches/clinicians.Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 90
7.9.33 Explain your approach to ongoing training and development for the coaching staffUnlimited.
7.9.34 What percentage of your coaches/clinicians working with participants with a chronic conditionhave an nursing background?Percent.
7.9.35 Does your Medical Director conduct clinical case reviews on at least a monthly basis?Single, Radio group.1: Yes,2: No3: Yes, with deviations
7.9.36 Are these cases reviewed at least on a monthly basis?Single, Radio group.1: Yes,2: No
7.9.37 How often do you conduct grand rounds?Unlimited.
7.9.38 What metrics are in place to measure clinical quality?Unlimited.
7.9.39 Which of the following are included within the clinical platform as checkpoints forcoaches/clinicians to ensure:
Multi, Checkboxes.1: Members are seeing the appropriate providers,2: Member aware of alternative treatments,3: Member utilizing the best facility for their condition in area,4: Treatment plan followed is in line with best practice guidelines
7.9.40 Do you agree to allow and fund third-party audits of your clinical services?Agree\Agree with exceptionDisagree
7 . 1 0 E N R O L L M E N T
7.10.1 Please complete the following tables regarding your assessment of Acuity LevelsAcuity Level Definition Methods and Timing Used to Initially Enroll ParticipantsLowModerateHigh

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 91
Acuity LevelAverage Lengthof Program
Average Number of OutboundCoaching Calls/Program
Rationale forNumber of Calls
LowModerateHigh
7.10.2 Describe the process by which individuals are stratified into risk levels and/or determined to beeligible for this service.
Unlimited.
7.10.3 Does your identification and stratification process begin within 3 business days after receivingdata (i.e., medical, Rx, etc.) files?
Single, Radio group.1: Yes,2: No
7.10.4 If identification and stratification doesn't begin within 3 business days of receiving data, whendoes it begin?
Unlimited.
7.10.5 Do you begin the enrollment process within 3 business days after identification and stratification iscomplete?
Single, Radio group.1: Yes,2: No
7.10.6 If the enrollment process doesn't start within 3 business days after identification and stratificationis complete, after how many days does it start?
Decimal.
7.10.7 Does your organization have any plans to change the identification and stratificationmethodology?
Single, Radio group.1: Yes,2: No
7.10.8 Do you proactively outreach to members identified for elective surgeries or procedures? And if so,what is the timing of outreach? Is it live or IVR?
Single, Radio group.1: Yes, explain: [ Unlimited ] ,2: No
7.10.9 What modalities do you use to conduct outreach to individuals eligible to enroll in theseprograms? Enter “Not Applicable” as needed.
Low Moderate High Other
Email contact - # sent Unlimited. Unlimited. Unlimited. Unlimited.
Email contact - frequency Unlimited. Unlimited. Unlimited. Unlimited.
IVR contact - # sent Unlimited. Unlimited. Unlimited. Unlimited.
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 92
IVR contact - frequency Unlimited. Unlimited. Unlimited. Unlimited.
Phone contact - #calls made Unlimited. Unlimited. Unlimited. Unlimited.
Phone contact - frequency Unlimited. Unlimited. Unlimited. Unlimited.
Home mailing contact - # sent Unlimited. Unlimited. Unlimited. Unlimited.
Home mailing contact - frequency Unlimited. Unlimited. Unlimited. Unlimited.
Text message contact - # sent Unlimited. Unlimited. Unlimited. Unlimited.
Text message contact - frequency Unlimited. Unlimited. Unlimited. Unlimited.
7.10.10 Do you have a standard process for members to opt-out if they do not wish to be contacted?Single, Radio group.1: Yes,2: No
7 . 1 1 S E R V I C E I N T E G R A T I O N7.11.1 List which types of data are taken in for analysis and the preferred frequency of data intake. Enter
“Not Applicable” as needed.Data Analyzed for eligibility /
outreachAnalyzed for stratificationapplication
Preferred frequency ofintake
Health Assessment Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Lab/screening values Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Medical claims Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Rx claims Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Behavioral healthclaims
Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Disability claims Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
Other Yes/No.Nothing required
Yes/No.Nothing required
Unlimited.Nothing required
7.11.2 Has your organization implemented clinical staff real-time access to member pharmacy data (todetermine medication compliance)? How many clients do you have this implemented currently?Describe how the data is used by the clinical staff. (Please note this question is not about your abilityto set up real-time access but actual experience with clients).
Unlimited.
7.11.3 What is your practice for data collection and use of participation data from a third-party lifestylemanagement program?

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 93
Unlimited.
7.11.4 Relative to integration with other clinical care management programs, indicate which of thefollowing data is collected/analyzed prior to outreach for Condition Management:
Multi, Checkboxes.1: Pre-certification for inpatient admission,2: Inpatient admission,3: Persistent high cost claimant status,4: ER visit,5: Diagnosis of cancer, Chronic Kidney Disease (CKD),,6: Gap in care status,7: Evaluation for hospice,8: Medication Adherence
7.11.5 You will provide integration with an employer's other internal and external programs. For eachprogram, workflows for data sharing and coordination will be developed, and you will use warmtransfers whenever possible. Interfaces include, but are not limited to:
Response Yes withDeviations
a. Customer service Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
b. Pharmacy Benefit Manager Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
c. EAP vendor Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
d. Disability vendor Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
e. Workers' compensation vendor Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
f. Worksite-based wellnessinitiatives
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 94
g. On-site/Nearsite clinics Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
h. Data warehouses Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
i. Expert medical opinioncompanies
Single, Radio group.1: Yes,2: No,3: Yes with Deviations (explain in nextcolumn)
Unlimited.Nothing required
7.11.6 Explain your approach to integration with Lifestyle Management programs, both if they are offeredinternally by your organization or if a client partners with another vendor to provide LM services. Besure to address how the appropriate program enrollment is determined and how multiple outreachcalls are avoided.
Unlimited.
Summarize your practices related to relevant integration of this service with other health managementpartners' services.Unlimited.
7.11.7 Briefly summarize your experience integrating with a disability vendor into your ConditionManagement programs.
Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 95
7 . 1 2 C A R E M A N A G E M E N T P G S A N D P R I C I N G7.12.1 Performance Guarantees: Custom Care ManagementFlagged: Client SpecificCare Management – Reporting and ResultsProvide your organization's performance standards for your Condition Management service. Enter “None”,“Not Available” or “Not Applicable” as needed.
Performance Standard Target BOB Average BOB Best
1 Unlimited. Unlimited. Unlimited. Unlimited.
2 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
3 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
4 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
5 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
6 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7 Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
Unlimited.Nothing required
7.12.2 What is the total percent of fees at risk you are willing to offer?Percent.
7.12.3 Are you willing to offer this performance guarantee around Implementation — Fully go live on themutually agreed upon launch date, not less than 90 days following client decision: 2% fees at risk.
Unlimited.
7.12.4 Are you willing to offer this performance guarantee around these 3 elements of Satisfaction:Satisfaction — Employer/client satisfaction with account management — satisfied or highly satisfied (ona 5 point scale, 4 is satisfied. Survey questions will be provided by Mercer and administered via a Mercerclient survey): 1% fees at risk.Satisfaction — Employer/client satisfaction with program operations — 90% satisfied or highly satisfied(on a 5 point scale, 4 is satisfied. Survey questions will be provided by Mercer and be administered via aMercer client survey): 1% fees at risk.Satisfaction — Participant satisfaction — 90% moderately satisfied or better (on a 5 point scale, 3 ismoderately satisfied. Survey questions will be provided by Mercer but may be administered via vendorstandard process): 1% fees at risk in Y1 and 2% fees at risk in Y2 and Y3.Unlimited.
7.12.5 Are you willing to offer this performance guarantee around Reporting — Data required forstandard Mercer dashboard will be provided within 30 days of the close of each quarter: 1% of fees atrisk.
Unlimited.
7.12.6 Are you willing to offer this performance guarantee around Technology — 99.5% websiteavailability other than scheduled and communicated down time. All scheduled down time must becommunicated to client 72 hours in advance of down time and to participants 48 hours in advance ofdown time: 2% fees at risk.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 96
Unlimited.
7.12.7 Please provide your standard performance guarantees including those based on chronic conditionimprovements, as attachment S7: E- Performance Guarantees for Care Management.
Unlimited.
7.12.8 Are you willing to offer performance guarantees around financial savings.• If so, how much of your fees at risk will you offer for such a guarantee?
Unlimited.
7.12.9 What is your standard methodology for measuring savings?Unlimited.
7.12.10 Please provide your organization's experience calculating savings using an individual-level,multivariate savings methodology.
Unlimited.
7.12.11 Please complete the following table:Response
Are you willing to put any performance guarantees around engagement levels? • Ifso, please describe what those specific metrics are. • Are you willing to put anyperformance guarantees around risk stratication improvement? • If so, pleasedescribe what those specific metrics are.
Unlimited.
• performance guarantee Recruitment — 100% of identified are reached out towithin 30 days. First call, email, or postal mailing attempted within 30 days of HAcompletion (for clients who purchase services with an outreach component): 2%fees at risk.
Unlimited.
• performance guarantee Participation — 30% or more of members targeted foroutreach, with valid contact information (defined as name, complete contactaddress, and at least one valid telephone number), will agree to participate.Members will complete at least one coaching call or live coaching interaction onlineor in person and schedule their second — to be evaluated based on participantsenrolled in the year being assessed, but reviewed quarterly; for online modules,identified participants will enroll and begin an online module (for clients thatpurchase coaching services or online health education modules): 1% fees at risk.
Unlimited.
• performance guarantee Engagement — A minimum of 30% of participants willcomplete a minimum of three coaching calls. Members will complete three coachingcalls or live coaching interaction online or in person — to be evaluated based onparticipants enrolled in the year being assessed, but reviewed quarterly; for onlinemodules, identified participants will complete the module and pass the testing orgraduation requirement (for clients that purchase coaching services or online healtheducation modules): 1% fees at risk.
Unlimited.
• performance guarantee Health Improvement in Y2 and Y3 — There will be atleast an average of 2% net reduction year over year in the total number of peoplewith greater than 2 risks: 1% fees at risk.
Unlimited.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 97
7.12.12 What is your PEPM cost for Care Management Coaching (inbound and outbound)?Unlimited.
7.12.13 What is your per participant cost for Care Management Coaching (inbound and outbound)?Unlimited.
Custom Care Management Pricing GridFlagged: Client Specific
7.12.14 Please complete the following pricing grid for onsite clinic management.Pricing Details: Y1 Y2 Y3 Details
Contract LengthNA NA NA
Fixed Staffing Costs: Please detailDollars. Dollars. Dollars. Unlimited.
Admin Fees: Please detailDollars. Dollars. Dollars. Unlimited.
Ad Hoc reporting Fees NA NA NAUnlimited.
Implementation Fees: Please detail Dollars. NA NA Unlimited
Operational Costs: Please detail Dollars. Dollars. Dollars. Unlimited
PPPM Dollars. Dollars. Dollars. Unlimited
Eligibility File Integration Fees Dollars. Dollars. Dollars. Unlimited
Technology Fees Dollars. Dollars. Dollars. Unlimited
Training fees Dollars. Dollars. Dollars. Unlimited
Inbound file feed fees Dollars. Dollars. Dollars. UnlimitedOutbound file feed fees Dollars. Dollars. Dollars. UnlimitedOther Fees: Dollars. Dollars. Dollars. Unlimited

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 98
VIII. STOP LOSS QUESTIONNAIRE
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
1. Your proposal is subject to and isconsistent with the Mercernational stop loss agreementcurrently in place with Mercer, ifapplicable.
<Choose One>
2. Specific and aggregate stop losscoverage applies to all medicalexpenses, including all mentalhealth and substance abuseclaims, covered under the self-insured plan(s) (excluding Rxclaims). All benefits paid underthe benefit plan must accumulateto specific stop loss limits withoutany limitations or exclusions. Thespecific stop loss lifetimemaximum must be consistent withthe underlying medical plan(s).
<Choose One>
3. Specific and aggregate stop losscoverage applies to all eligiblemembers as defined by themedical plan.
<Choose One>
4. You will accept the claimadministrator’s interpretation asto what is an eligible expenseunder the medical plan.
<Choose One>
5. The actively-at-work requirementand dependent non-confinementrules must be waived for alleligible members as of theireffective date of coverage.
<Choose One>
6. Pre-existing condition limitationsare waived.
<Choose One>
7. No new lasers at renewal, unlessrequested by or on behalf of theemployer.
<Choose One>
8. Quotes are on a firm basis for aJanuary 1, 2017 effective dateand guaranteed for 12 months(Premium only not attachmentpoints).
<Choose One>
9. You agree to set your AggregateAttachment Point at 115% of theclaims.
<Choose One>
10. You agree to set your MinimumAggregate Attachment Point atthe appropriate level of theexpected Aggregate AttachmentPoint in accordance with yourcompliance with the MercerNational Agreement,
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 99
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
11. Notice of the final change inexcess risk premium must beprovided by 90 days beforerenewal date of each year.Coverage must be binding nolater than 60 days. The newpremium will not be effective untilthe following policy anniversary.
<Choose One>
12. Written notice must be providedat least 60 days before youterminate the contract.
<Choose One>
13. If necessary, you may revisepremiums at a time other than theanniversary date only if specificevents occur. These events areas follows:• The number of covered
employees changes bymore than 15%
• There are significantchanges in the underlyingplans that would materiallyalter your risk.
<Choose One>
14. You or your insurer, if a separateorganization, must be rated A, A+or A++ by A.M. Best or anequivalent rating bureau.
<Choose One>
15. THCP retains the right toterminate the contract at any timewith 30 days written notice.
<Choose One>
16. A copy of your marked up versionof HISD’s contract has beenincluded in your proposal asAttachment S8: A – Sample StopLoss Contract.
<Choose One>
17. An assigned account managerwill support THCP’s benefit staff
<Choose One>
18. Your disclosure form will notcontain wording which requiresknowledge of any individual whomay have a condition that mightresult in a claim level at 50% orabove the requested stop losscoverage threshold (or similarlanguage).
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 100
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
19. If you require a disclosurestatement, the employer will fillthe information out to the best oftheir knowledge. In the event aclaim occurs which should havebeen on the disclosure statementbased upon information the planadministrator had but of whichTHCP had no knowledge, thestop loss insurer must treat thisas a legitimate claim andreimburse THCP without applyingany benefit reduction and/orcontractual modifications.
<Choose One>
20. Claims administrator(s) must beapproved by your firm.
<Choose One>
21. Please provide your definition ofa paid claim.
<Choose One>
22. Define clearly the terms andconditions of your contract asthey apply to contract termination.
<Choose One>
23. Describe how you will treatongoing claims as of theinception date of a contract.
<Choose One>
24. You agree not to limit coveragefor large, ongoing claim cases atrenewal.
<Choose One>
25. You will allow a claim audit by thepolicyholder and/or third party?
<Choose One>
26. Describe your case managementcapabilities to monitor/managepotentially high dollar cases.
<Choose One>
27. As the stop loss carrier, youprovide underwriting/claimservice in-house (if disagreeprovide the name of the thirdparty).
<Choose One>
28. Describe your renewal ratingprocess.
<Choose One>
29. Describe your credibility formula. <Choose One>30. Please list third party
administrators you haveassessed as acceptable.
<Choose One>
31. What is your procedure forapproving a claims administratorthat you have never worked with?
<Choose One>
32. List your standard contract’s setof general exclusions andlimitations.
<Choose One>
33. Describe your definition ofexperimental and investigationalprocedures.
<Choose One>
34. What is the maximum timeallowed for submission of validclaims?
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 101
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
35. If THCP selects a contract with“run-in” coverage (e.g. 24/12) arethere any limitations associatedwith the “run-in” claims.
<Choose One>
36. Provide a brief description or listof data needed to process aspecific claim reimbursement.
<Choose One>
For claims exceeding the specific stop loss level, please address the following six items:37. From start to finish, overall claim
data collection to paymentprocedure
<Choose One>
38. Timing parameters for all partiesinvolved, including the client, andyour review to paymentturnaround time
<Choose One>
39. Interaction with the claimsadministrator
<Choose One>
40. Interaction with the utilizationreview firm
<Choose One>
41. Interaction with large casemanagement service
<Choose One>
42. Auditing of stop loss claims <Choose One>Please indicate if each of the following six items impact the aggregate calculation and to what extent.43. Claims incurred by individuals
lasered under the individual stoploss contract
<Choose One>
44. Claims exceeding the individualspecific stop loss level or acertain threshold if no individualstop loss is in place.
<Choose One>
45. Capitation payments and fees <Choose One>46. Fiduciary claim exceptions to the
SPD<Choose One>
47. State health surcharges <Choose One>48. Other reductions, if any. <Choose One>Please address the following five items that are associated with a client receiving an aggregate claim reimbursement.49. When must you be notified that
the aggregate limit has beenexceeded
<Choose One>
50. Timing of reimbursement onceyou are notified the aggregatelimit has been exceeded
<Choose One>
51. Information/data required <Choose One>52. Procedures for handling
reimbursement request<Choose One>
53. Timing process from datacollection to payment
<Choose One>
54. Does the aggregate stop losscoverage cover all provisionsoutlined in the Plan Documentwithout exception?
<Choose One>
55. How credible is the client’sexperience for this proposal?
<Choose One>
56. How credible is the client’sexperience for renewal?
<Choose One>

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 102
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
57. You will provide a multi-year rateor rate increase guarantee (Ifagree, please describe).
<Choose One>
58. Your proposed offering allowsyou to load premium rates for“known” risks.
<Choose One>
59. Are you willing to accept a largeclaims data feed on a quarterlybasis?
<Choose One>
60. What claims and eligibility data isneeded and what timingrequirements do you place on thedisclosure of this information (e.g.50%, 100% notification)? Pleasebe specific in your response.
<Choose One>
61. Is there a maximum annual dollaramount that will be reimbursed ifthe aggregate attachment point isexceeded?
<Choose One>
62. Are the terms of the aggregateStop Loss coverage consistentwith the specific stop losscoverage? Clarify all differences.
<Choose One>
63. Aldine ISD’s current stop losspolicy covers prescription drugclaims for only one individual dueto savings in acquisition cost onmedications ordinarily providedunder the medical plan (see largeclaims in Exhibit B – Claims Data(AISD).xlsx). Confirm that you willcover this individual’s pharmacyclaims.
<Choose One>
64. Confirm that you can provide a nolaser quote for Aldine ISDincluding this individual.
<Choose One>
65. If you are also quoting as themedical administrator pleaseprovide the current allowedmedical charge equivalent for thedrug Soliris (NDC:25682000101).
<Choose One>
66. Are you willing to provideseparate quotes for:· Medical only· Medical/Rx
<Choose One>
67. If the answer to Question 66 isyes, please be sure and providethe financial proposal for bothmedical only and medical/rx forboth HISD and Aldine ISD.

F O R M H : Q U E S T I O N N A I R E 1 6 - 0 1 - 0 7
MERCER 103
Stop Loss Questionnaire
Agree,Agree withexception,
Disagree, N/AException/supporting detail/description orcommentary
68. Can you provide a one page StopLoss report on plan performanceon a quarterly basis? Attach asample of this report asAttachement S5:E – Sample StopLoss Report
<Choose One>

M E R C E R ( U S ) I N C .500 Dallas Street; Suite 1500Houston, TX 77002+1 713 276 2100www.mercer.com
