medicare beneficiary quality improvement program (mbqip) _mbqip... · state logic model — outputs...
TRANSCRIPT
Medicare Beneficiary Quality Improvement Program (MBQIP)
Stephen Njenga, Director of Performance Measurement ComplianceMarch 2018
Housekeeping Handouts Location of restrooms Instead of reimbursing for mileage during the
regional meetings funds were diverted to cover the following offerings that were open to all participating CAHs:Population HealthHigh Reliable Organizations/Culture of SafetyTeamSTEPPSSecondary Data Analysis for CHNA Each hospital was eligible for $3,500
SHIP Deadlines
2017 Grant Period: June 1, 2017 to May 31, 2018 Invoices no later than Thursday, May 31 Award Amount: $8,717
2018 Grant Period: June 1, 2018 to May 31,2019 Not yet awarded Award Amount: $9,000
FLEX Grant Activities
• Patient safety, patient engagement, care transitions, outpatient careQuality
• Financial and operational assessments and actions, revenue cycle management, operational improvement
Financial and Operational
• Identify specific health needs of CAH communities and implement activities
Population Health
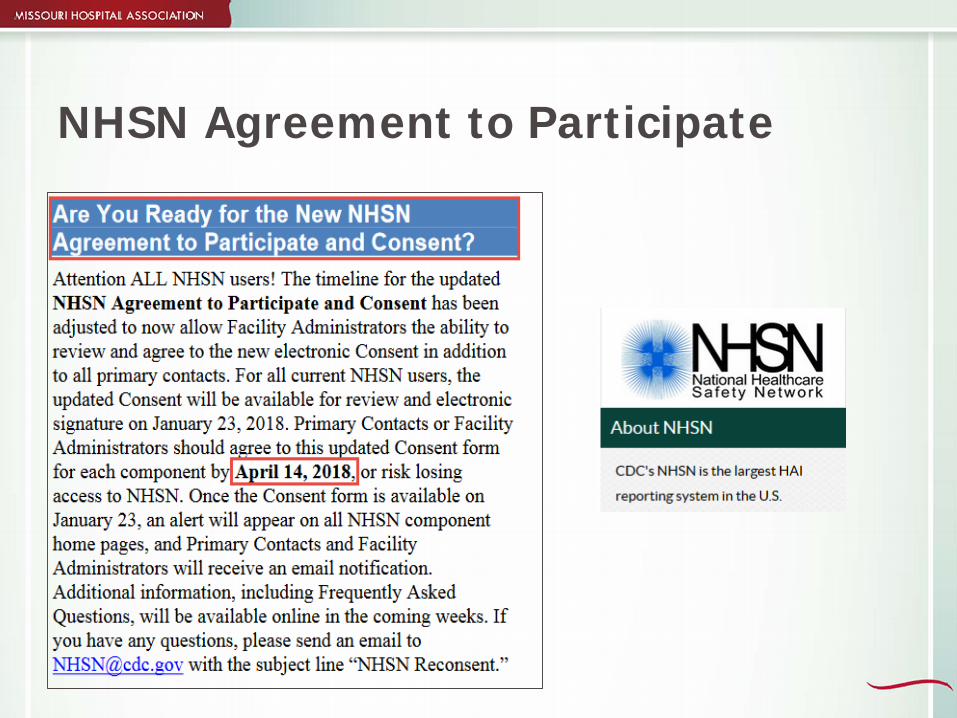
NHSN Agreement to Participate
NHSN Annual Surveys
2017 NHSN survey is due Thursday, March 1Hospitals are always encouraged to submit in
advance to avoid last minute issues. Annual surveys are used for your risk adjustment
for SIR and may change year to year based on your responses. Currently, facilities are using 2016 or 2017 surveys. These surveys will be used to calculate 2016 and 2017
SIRs.
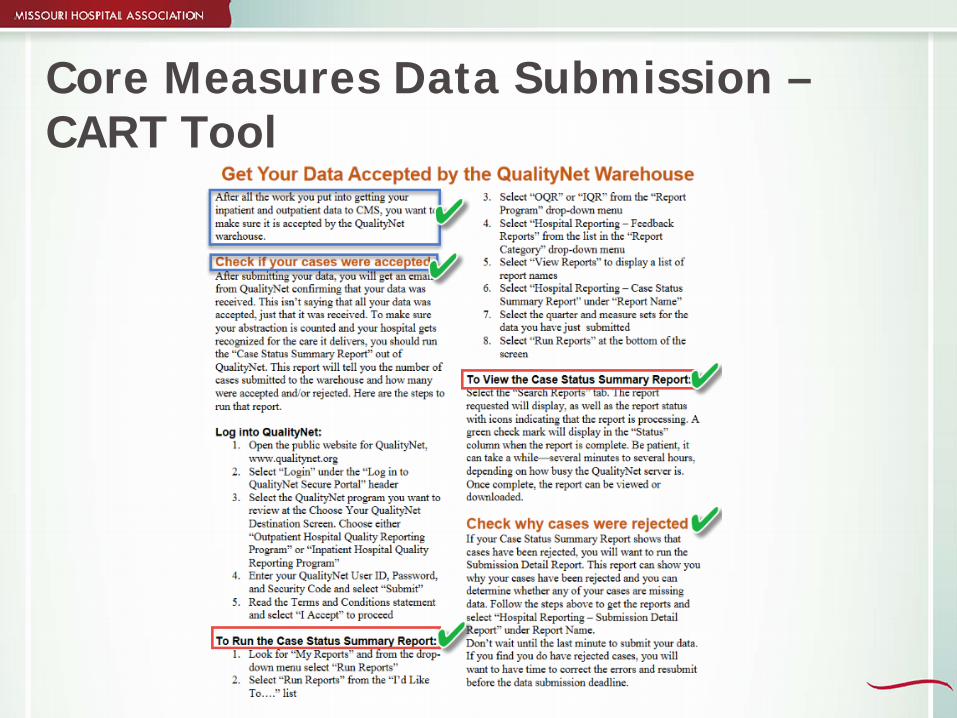
Core Measures Data Submission –CART Tool
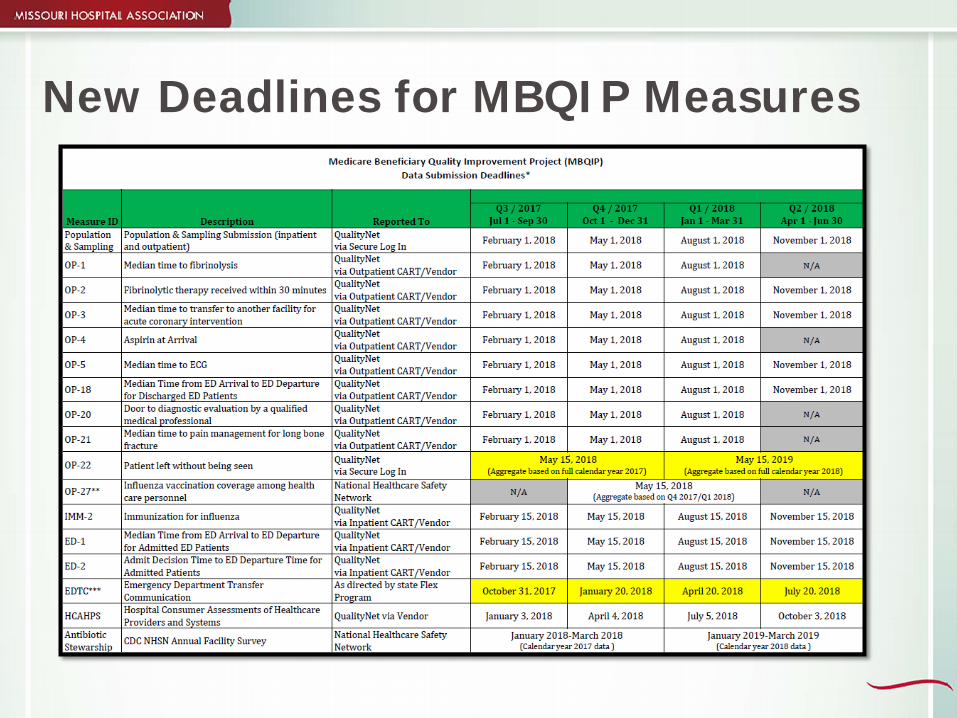
New Deadlines for MBQIP Measures
FLEX Grant Overview
National Logic Model — Inputs
Federal Office of Rural Health Policy
$23 Million
45 States
Resources – toolkits, publications, reports
State Logic Model — Inputs
33 Critical Access Hospitals
Collaboration with DHSS
Resources – toolkits, publications, data

State — Level Core Areas
Quality Improvement (MBQIP)
Operational and Financial Improvement
Population Health Improvement

Program GoalsSh
ort
Term
• Staff understands the program requirements, indicators and strategies
Med
ium
Ter
m • Staff reports measures, adopts projects and best practices
Long
Ter
m • CAHs improve their quality of care, stabilize finances and adjust to changing community needs
Core Area Improvement Activities
CAH Needs Assessments Training and technical assistance Consultations Information sharing Collaboration and networking ROI tracking Scholarships and education reimbursement Data analysis
State Logic Model — Outputs
Quality• Quality Reporting – How many hospitals report? • Quality Improvement – Are hospitals improving the care they provide?
Operational• Operational and financial state measures
• State – standard measures monitored at the state level • Individual – unique measures by hospital
Population Health
• CHNA Compliance – Are all hospitals conducting an assessment that are mandated?
• CHNA Improvement – Are the assessments and action plans making an impact?

Game Changers in Health Care

Changing Landscape in Health Care The Triple Aim To improve health care delivery To improve population health To lower costs — improve efficiencies
– Affordability– Quality/outcomes– Patient experience – Population management

Achieving Triple Aim
Greater efficiencies: Improved access/ outcomes; reduced variability;
reduced costs Characteristics:
– Patient/ family engagement and satisfaction– Measurable results– Implementation, spread and sustainability of evidence-based
best practices– Continuous measurement– Differential rewards: pay for performance and outcomes– Mitigate risk
Performance Improvement
Multiple Opportunities: Clinical
– Consistent implementation of evidence - based practices– Fidelity to recommend models (process measures)– Seamless care transitions
Operational– LEAN Six Sigma — reduce waste, increase efficiency– Throughput improvements– Seamless care transitions
Administrative– Revenue enhancement — coding/billing accuracy– Supply/purchasing management– Seamless care transitions
Quality Improvement Efforts
Convene experts (clinical domain, quality, patient experience) Identify and disseminate best practices (collaboratives) Manage and evaluate programs and grants to transform
care (measure processes, cost, benefit, outcomes) Breakdown/cross silos Work across/share clinical practice
Partner with internal and external stakeholders (Community partners, providers, payers, policymakers)
Payment Rates: decline Quality and Efficiency:
rewarded Readmissions and Low
Quality: penalized Population Health:
important
What to Expect in the Future
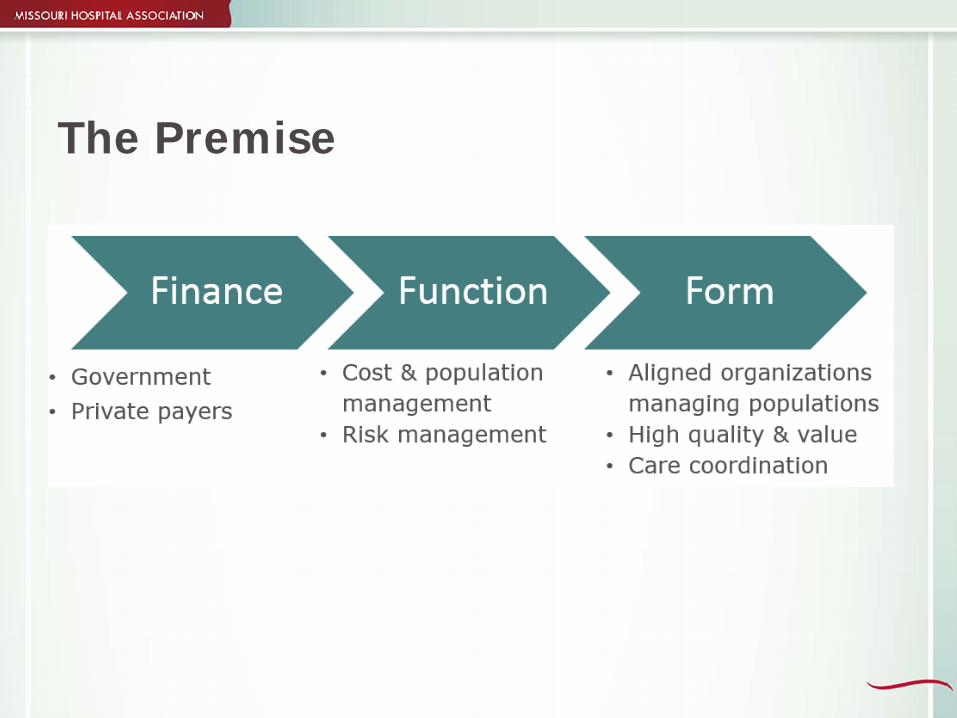
The Premise
Important Considerations for CAHs
Improve/ document efficiency and quality Partner with local primary care providers Improve care coordination and transitions Prepare for population health management Consider participation in an ACO, community
care organization, medical home or other value-based models
To Achieve Value
To achieve excellent performance and success in a value-based system, CAHs must ensure: Leadership alignment Vision and strategy Partnerships, care coordination and community Use of data and information Change-ready adaptable workforce Highly efficient, business-oriented processes Customers, partners and community Staff and culture Efficient processes and operations Information and knowledge Documentation of outcomes and value
Leadership Educate and engage hospital trustees and boards
about the critical role of value-based purchasing and population health Form meaningful partnerships with local
physicians and health care providers Align hospital leaders and managers behind
value and population health
Leadership

Strategic Planning
Patients, Partners and Communities
Processes and Operations
Maximize the efficiency of clinical, financial and operation processes Develop effective care coordination teams and
processes, and ensure safe and timely transitions of careMaximize the effectiveness of health information,
social media and telehealth technology
Use Data Effectively
Always Remember that…
The health care market is undergoing transformational change. Leadership awareness/support is critical in helping rural
health providers stay relevant during market transformation. The Performance Excellence Blueprint is a tool to help
rural leaders manage system – wide improvement and navigate change. The framework is flexible and can be used in multiple
ways – a starting point is just reviewing the key success factors and taking a critical look at your organization.
New Reporting Requirements for FY18-21
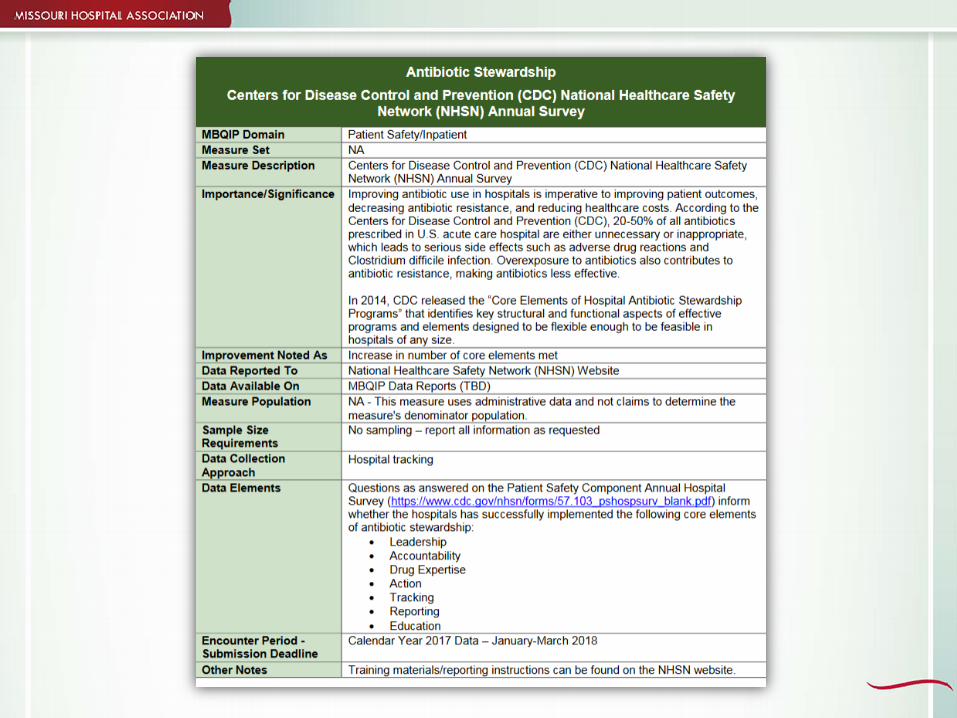
Antibiotic Stewardship - MBQIP
This addition would allow CAHs four years to fully implement an antibiotic stewardship program by FY2021. (September 1, 2018 to August 31, 2022)

Background Information
Former President Obama’s Executive Order and National Strategy (Sept. 2014) PCAST Report to the
President (Sept. 2014) National Action Plan for
Combating Antibiotic-Resistant Bacteria (Mar. 2015)
PCAST-President’s Council of Advisors on Science and Technology
Elements for Antibiotic Stewardship Programs
Leadership Commitment Accountability Drug Expertise Action Tracking Reporting Education
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
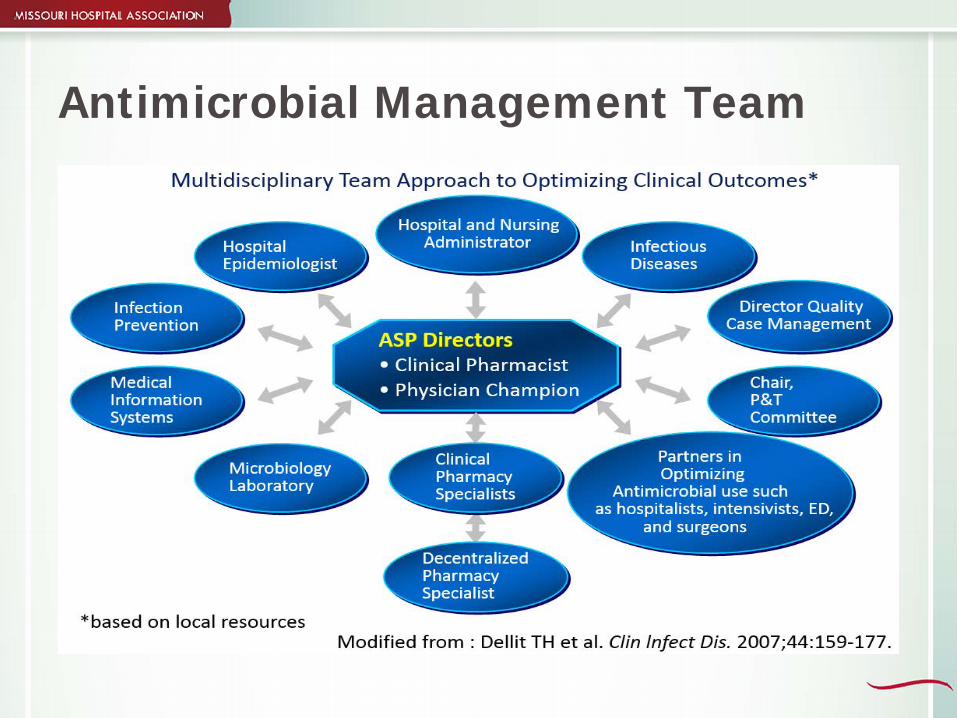
Antimicrobial Management Team
• Selecting physician champion• Complete gap assessment and
action plan as a team• Determine staffing needs to
adequately resource ASP activities
• Create competency/training plan for all disciplines based on current knowledge and involvement
• Invite CEO to ASP team meeting to discuss plan, resources and support
Basic ASP Foundation
• M.D./ PharmD champion• Multidisciplinary team• Gap assessment• Assess staff resources• Competency/training planning• Communication plan for facility • CEO support of ASP — approval
of gap and action plan
Missouri – Antibiotic Stewardship
The state legislature enacted SB579 requiring that by August 28, 2017, each Missouri hospital, excluding mental health facilities, and each ambulatory surgical center, must establish an antimicrobial stewardship program. Hospitals are required to use CDC’s Antimicrobial Use and
Resistance Module when regulations concerning Stage 3 of the Medicare and Medicaid Electronic Health Records Incentive Program take effect. This has been delayed, but hospitals should keep the
program going as they await for the necessary infrastructure to be available for reporting.
Reporting Requirements for ASP
Utilization of the AUR Module specifically requires eMAR and some form of clinical document architecture. The vendor system has to have the service and software
that will allow participating in the AUR pharmacy option through direct reporting. Vendors who have the software and services and are
actively reporting include EPIC, Asolva, MedMinded, Bacter (ICNet), Intelligent Medical Systems (Meditab), RL Solutions, Sentri7, TheraDoc and VigiLanz. Although you may utilize one of these vendors, you may
not have the specific software needed to begin reporting
Measuring Antibiotic Usage
Standardized antimicrobial administration ratio Observed-to-expected/predicted rate Serves as a starting point for antimicrobial use
evaluations by stewardship teams A statistically significant SAAR >1.0 indicates
more antimicrobial use than expected.
Missouri Hospitals IT Survey Results (146 Hospital Responses)
133 have fully implemented the ability to review laboratory results across all units 132 have fully implemented eMAR across all units 105 have fully implemented bar coding or radio
frequency identification for closed-loop medication administration across all units 131 have fully implemented record-preferred
language for communication with providers of care as part of meaningful use

Missouri Hospitals IT Survey Results(146 Hospital Responses)
117 can automatically generate hospital-specific, meaningful use quality measures by extracting data from EHR without additional manual processes 111 have some level of clinical document
architecture to send clinical/summary of care records
ED Throughput Measures
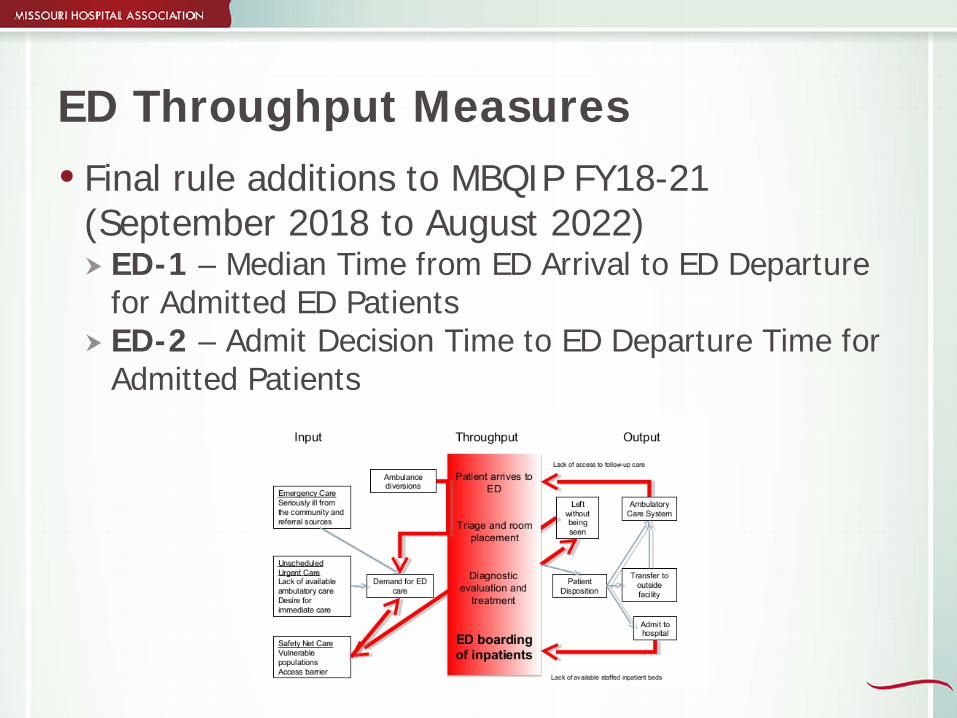
ED Throughput Measures Final rule additions to MBQIP FY18-21
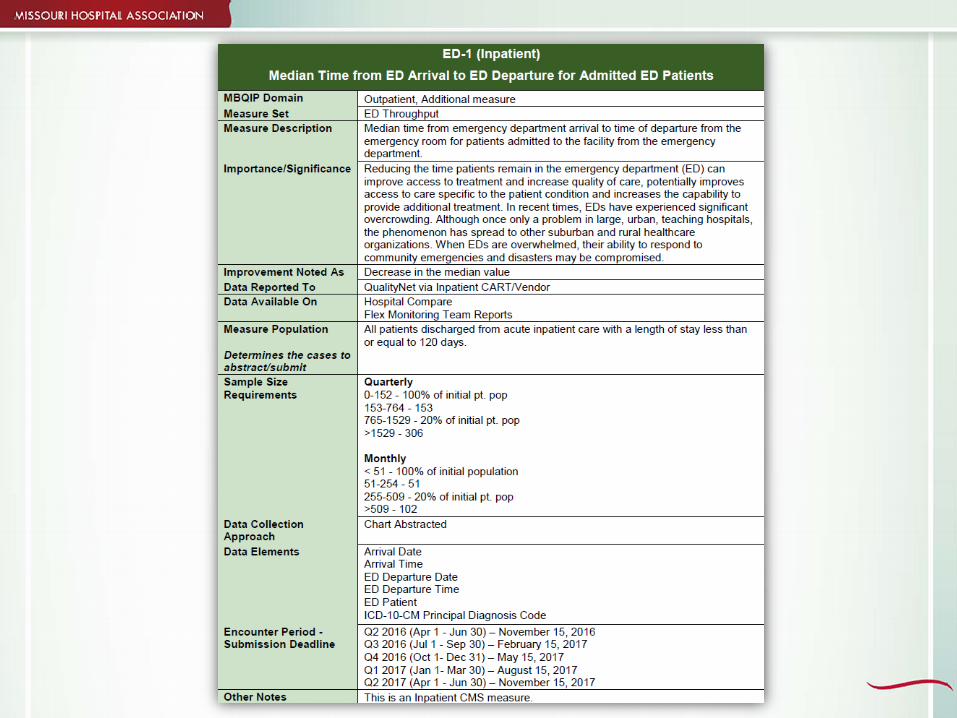
(September 2018 to August 2022) ED-1 – Median Time from ED Arrival to ED Departure
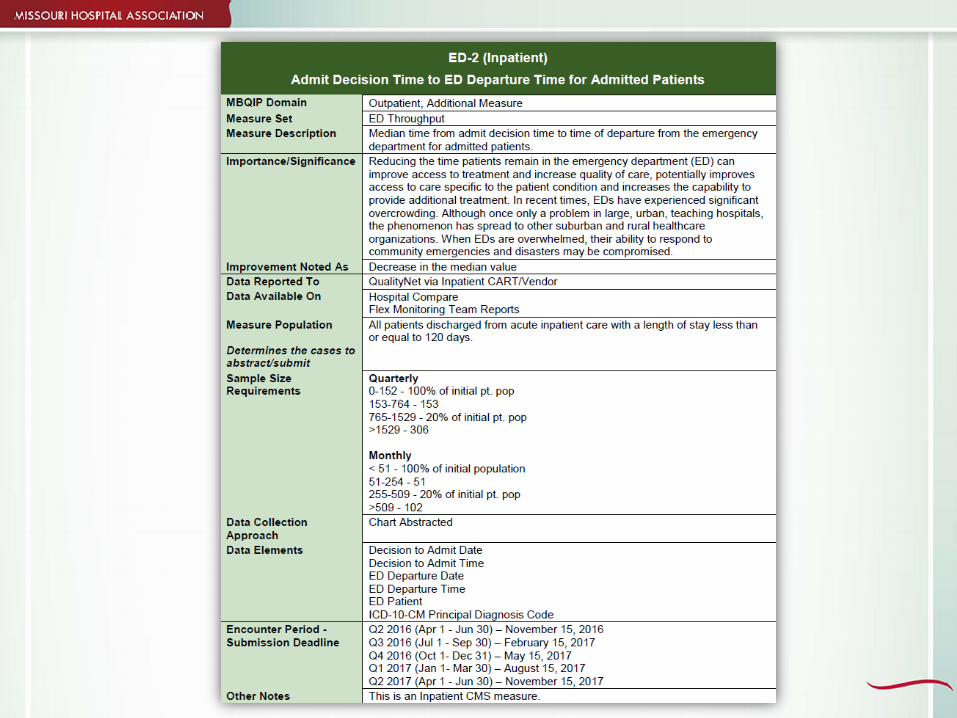
for Admitted ED Patients ED-2 – Admit Decision Time to ED Departure Time for
Admitted Patients

Background Information
The first quarter of required reporting was 3Q17(Submission deadline was February 15, 2018)
CY2016 — 47 persent reported these measures nationallyMissouri’s current reporting rate is 51 perecent. Chart-abstracted and reported to QualityNet on a
quarterly basis Reported using CART tool or approved vendor Patients included in ED-1 and ED-2 measures are
admitted for an inpatient stay from the ED
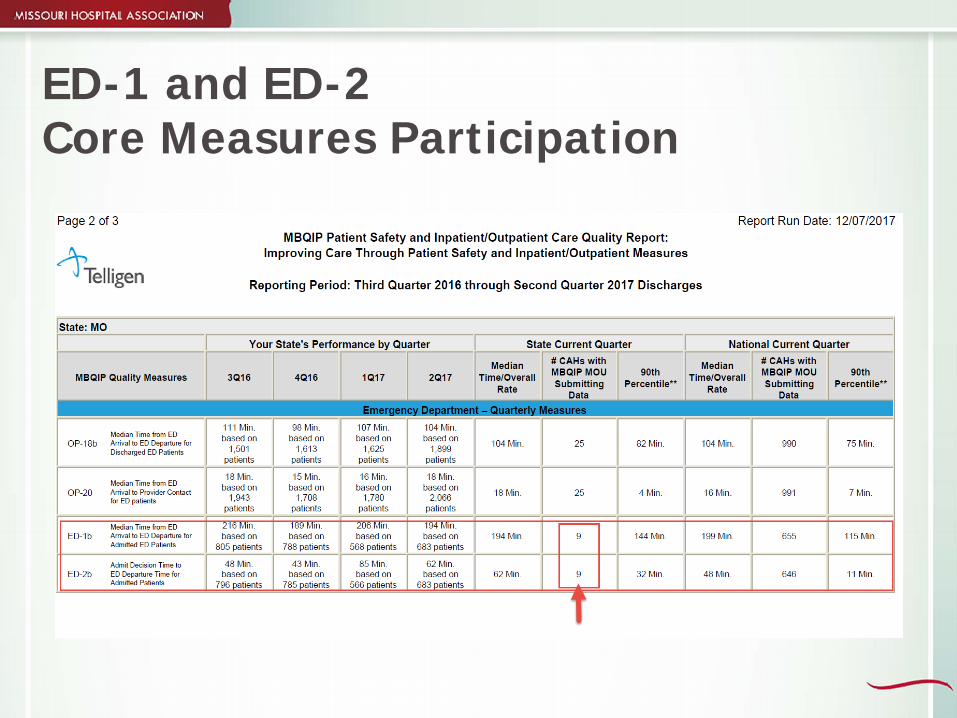
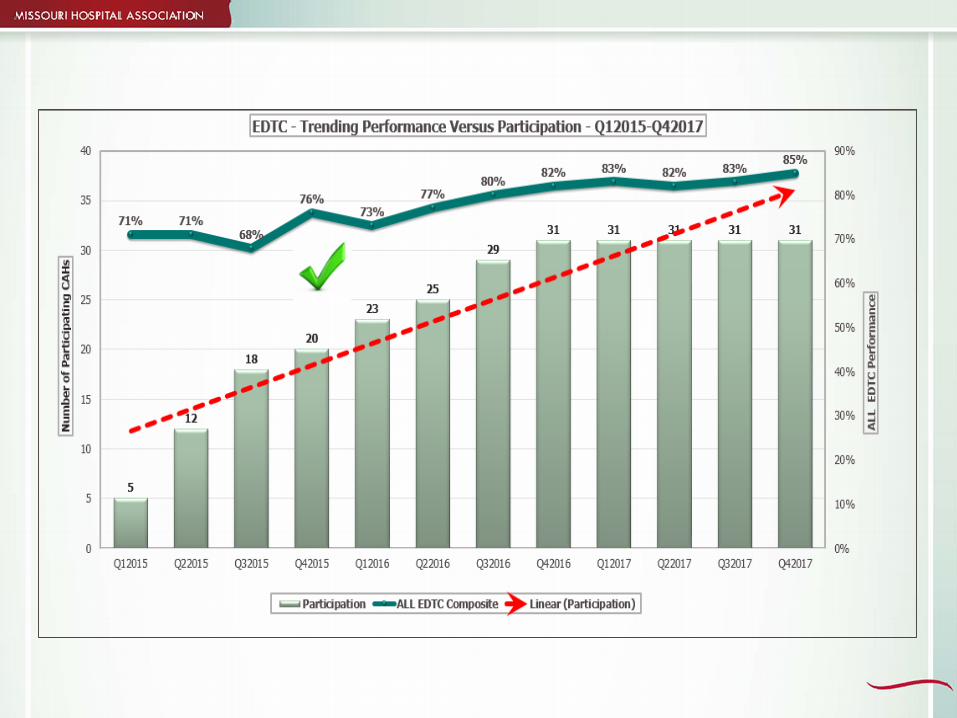
ED-1 and ED-2 Core Measures Participation
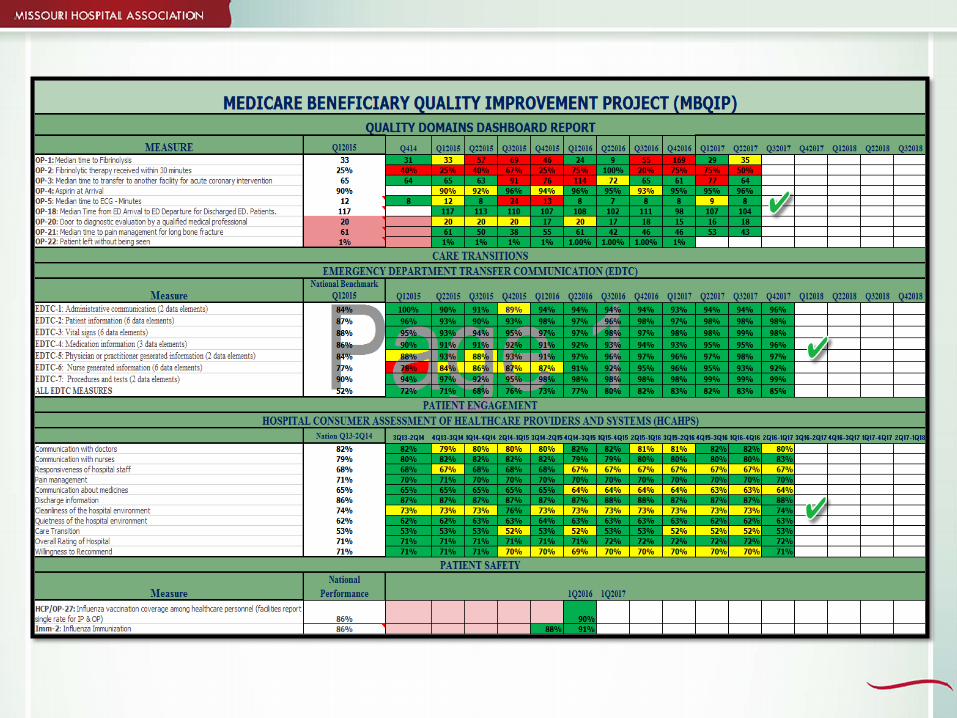
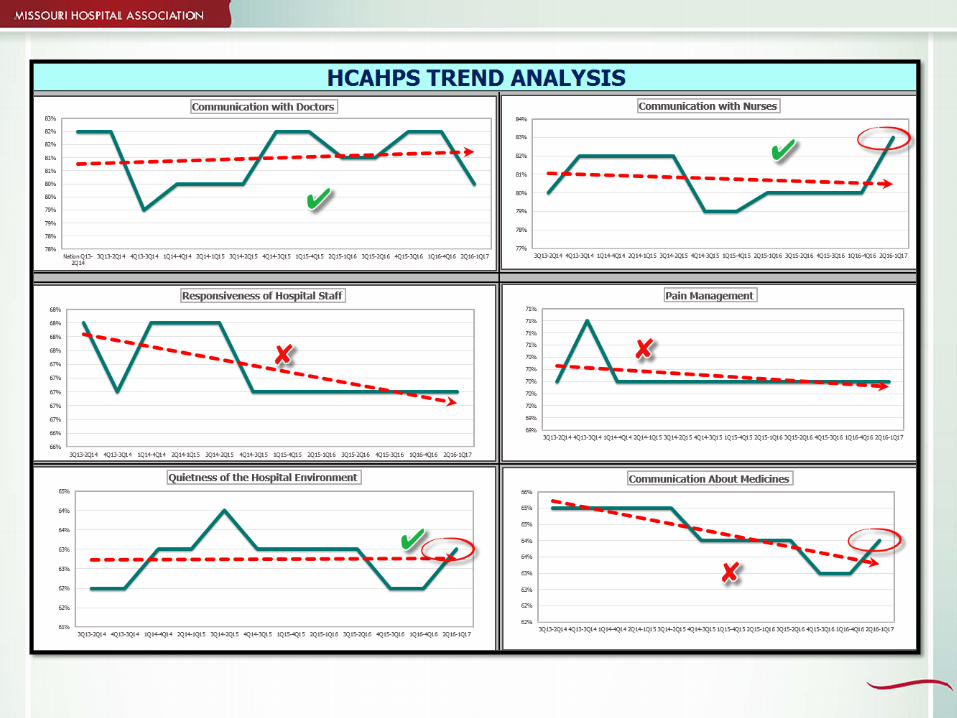
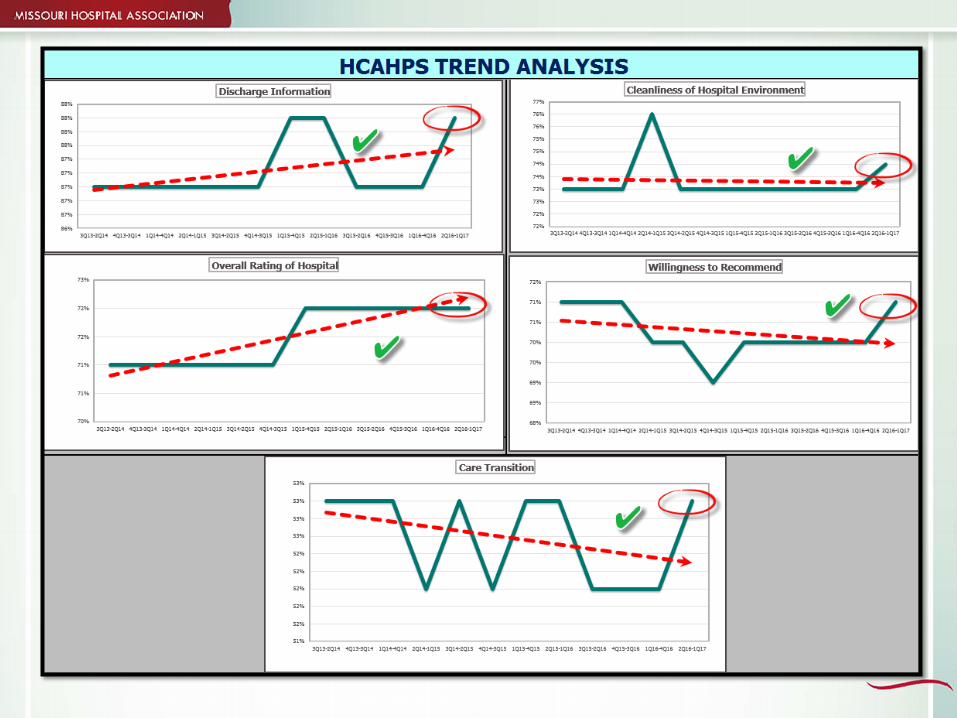
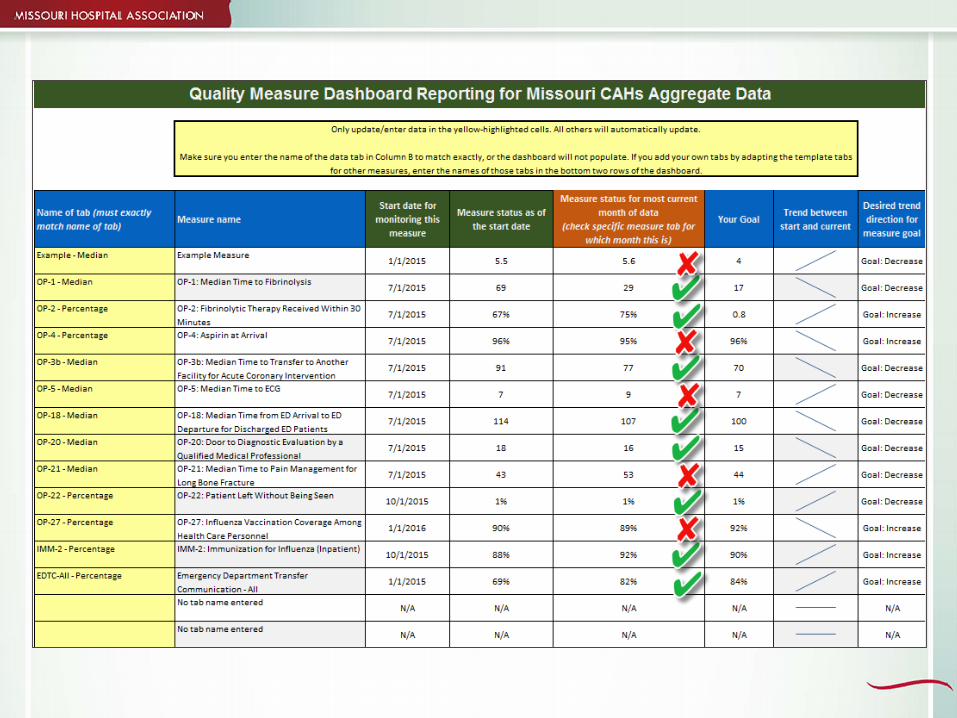
Dashboard Report – All Measures
Hospital Consumer Assessment of Healthcare Providers and
Systems Analytics

HCAHPS
Standardized survey tool to measure patient’s perception of quality of care by physicians and hospital staff during hospital stayWhy? Consumers – provide information helpful in choosing a
hospital Hospitals – offer incentives to improve quality of care
How? A way to compare hospitals Provides meaningful data for improvement efforts
HCAHPS
HCAHPS
The epicenter of these experiences for patients is generally focused on the patient room and five different types of human interactions during the patient stay When the patient is alone in the room When the patient and a visitor are together in the room When the patient and nurse interact in the room When the patient and physician interact in the room When the patient and support services interact in the room These different human interactions create the paradigm for
defining the patient experience … the people, the process and the place. These three interactions need to work well collaboratively in
order to yield a satisfactory patient experience and quality HCAHPS scores.
HCAHPS
People — the physical space of the patient room can contribute to engaging the caregiver by providing plenty of natural light, giving caregivers adequate space to work, and planning spaces that combine multiple functions. Process — Lean design principles should be used to
improve the caregiver’s workflow and limit the number of value-wasted movements. By making their job more efficient, they can save energy and leverage opportunities for rest and respite. Place — The physical space needs to be quiet and clean.
Using easy-to-clean flooring materials and designing patient rooms to limit room-to-room and corridor-to-room noise transfer enables the space to address typical areas for satisfaction shortfalls.
What Works?
Improving patient experience involves the following: Front-line staff need to be involved with creating the
experience. Focus on two to three interventions that are done with
excellence and consistency. The focus MUST be on creating a healing experience
for the patient. Create a process for continuous accountability and staff
recognition.
Intention - Connection - Action
1. Intention What is my intention going into the patient’s room?
2. Connect Build a relationship with the patient before doing
anything to them.
3. Action After I’m clear about my intention and I have
connected with the patient, only then do I carry out any tasks of the job such as checking vitals, administering medications, or even their diagnosis and treatment
Use Five Ps to Anticipate Needs
Pain Potty Positioning Personal needs Patient Priority
Decrease falls and call lights Use language that suggests what they might need,
rather than just asking if they have a need.
Making Five Ps Proactive
Typical question: Do you need to use the restroom?
Proactive language: “I’m about to give you pain medication which might
make you sleepy. Would you like me to help you to the restroom first so that you won’t have to get back up?”
“I know you are used to getting up on your own, but since you are connected to an IV, let me go ahead and help you to the bathroom while I am here so that I can make sure you are safe.”
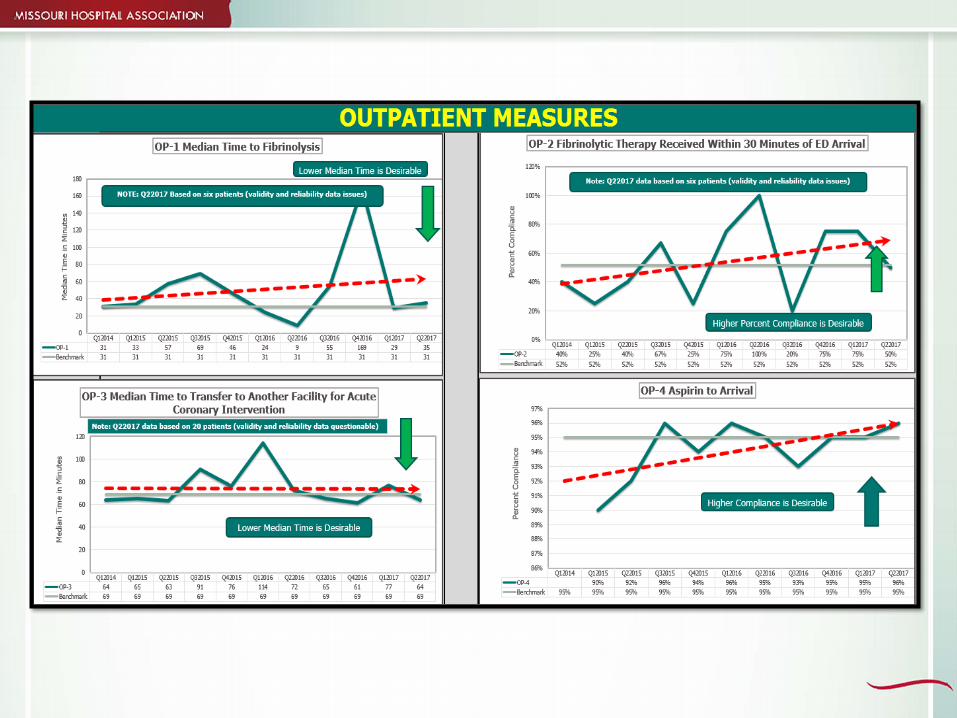
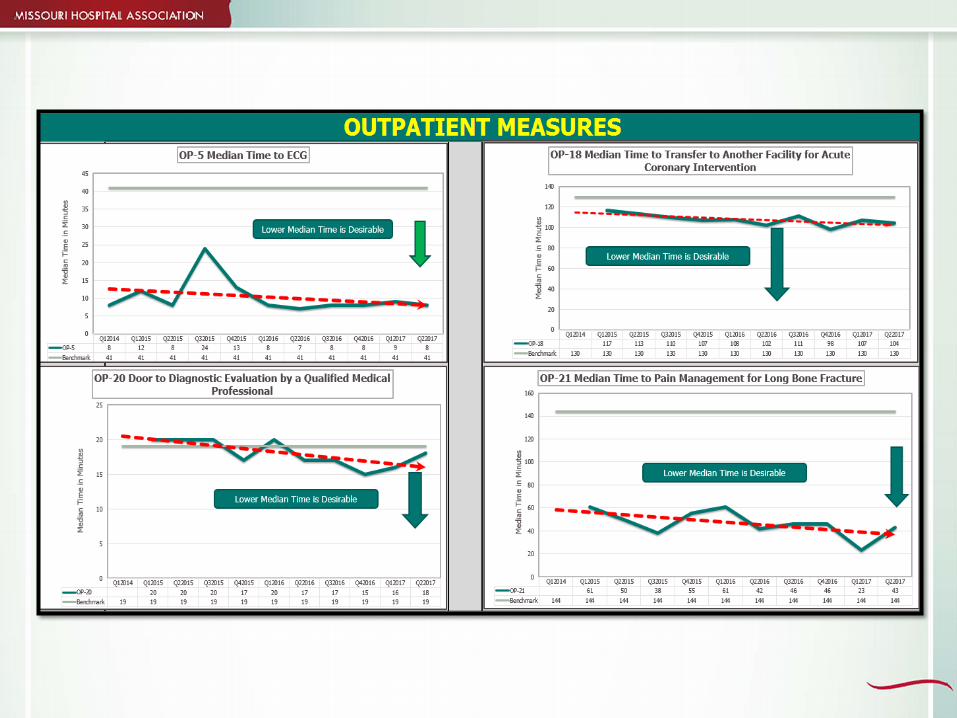
Outpatient Measures Analytics
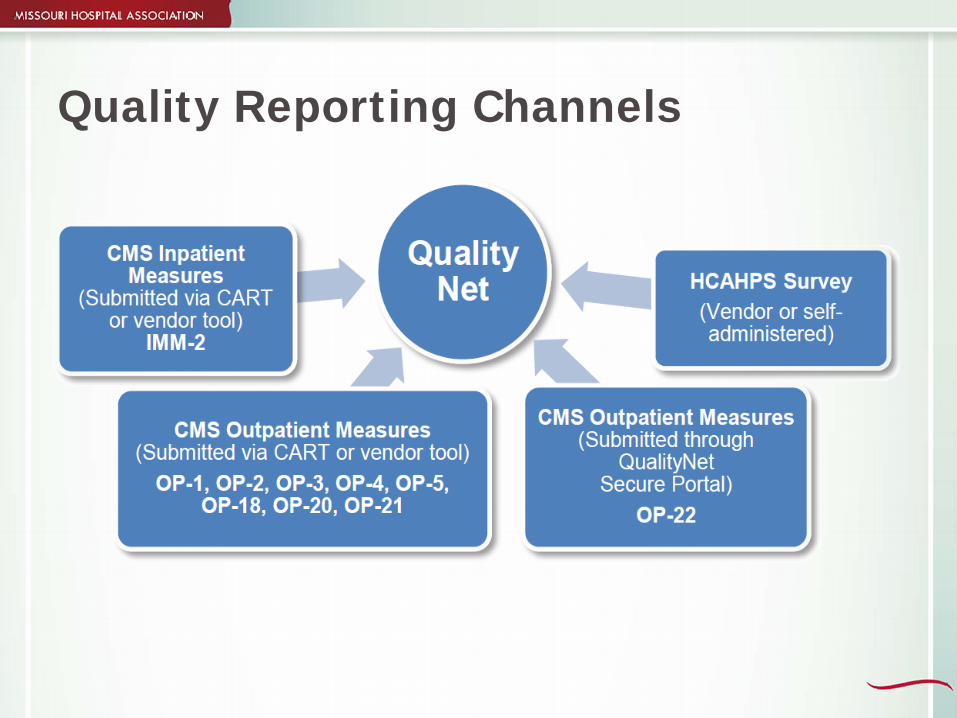
Quality Reporting Channels

Importance of Documentation
Communicates to others what was done Facilitates patient care Supports data collection Reflects quality of decision - making Justifies legal defense Supports regulatory compliance Supports fair payment /reimbursement
Documentation is Important
ED physician and nursing documentation in some cases is weak or missing. The documentation does not fully support patient care, correct coding and accurate charging. Examples: Length of laceration is not always documented. IV start and stop time is often not documented. Critical care nursing time is not documented. Physicians’ charts are not always complete. Documentation does not always comply with payer and
regulatory guidelines.

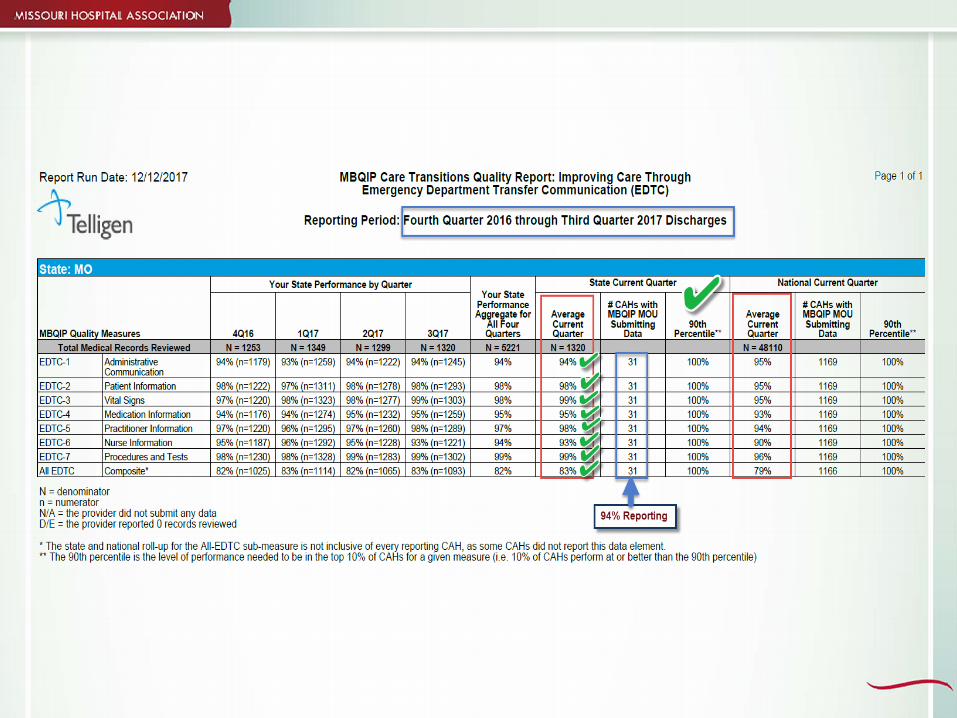
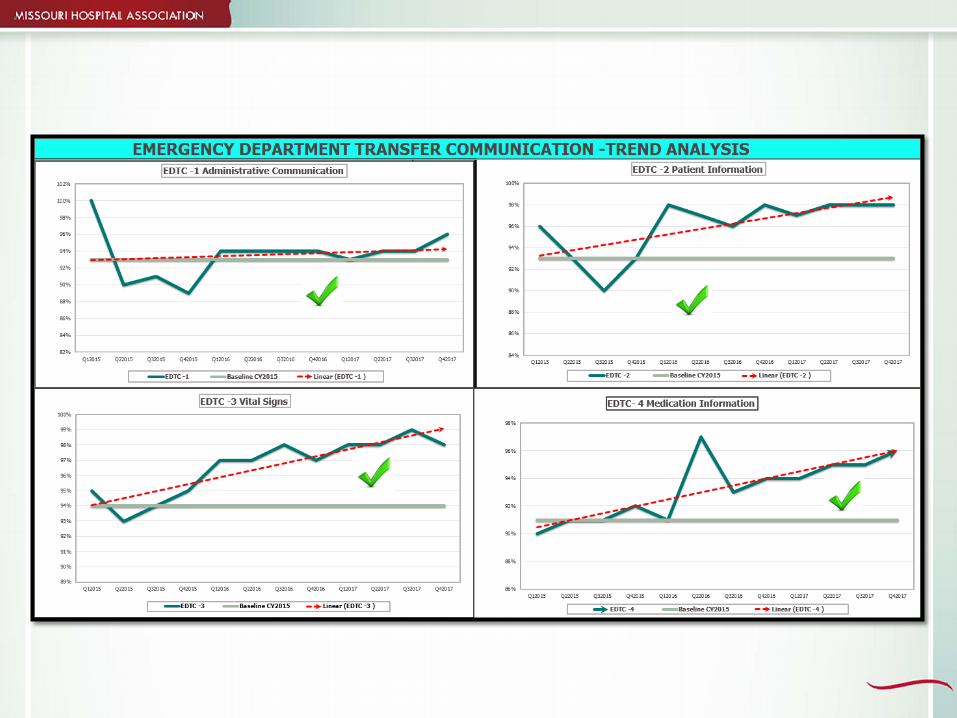
Emergency Department Transfer Communication Analytics
Quality Reporting Process
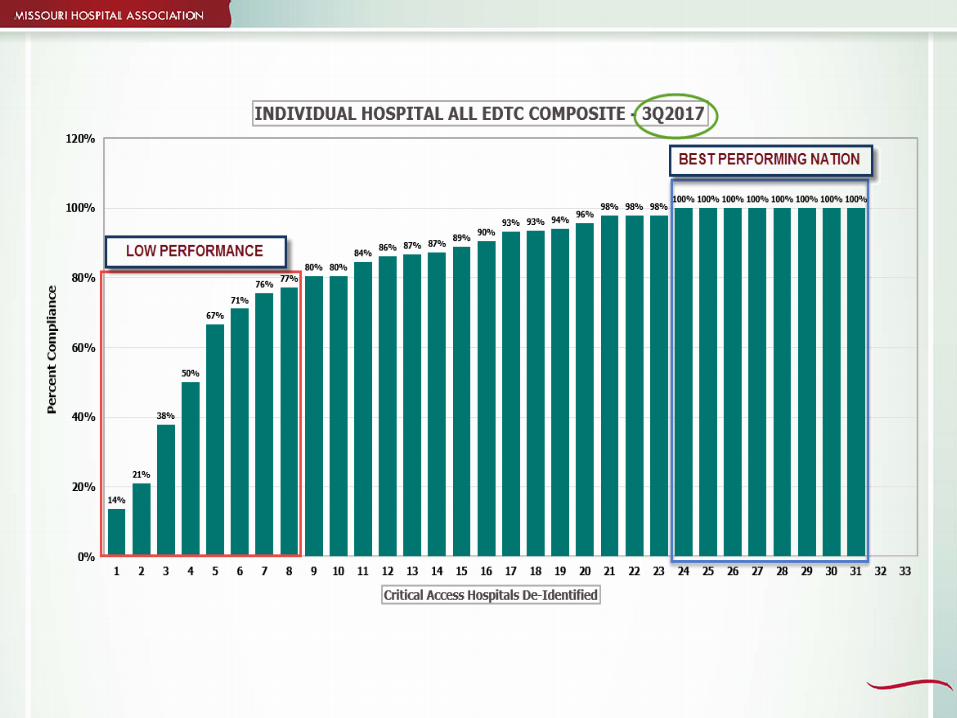
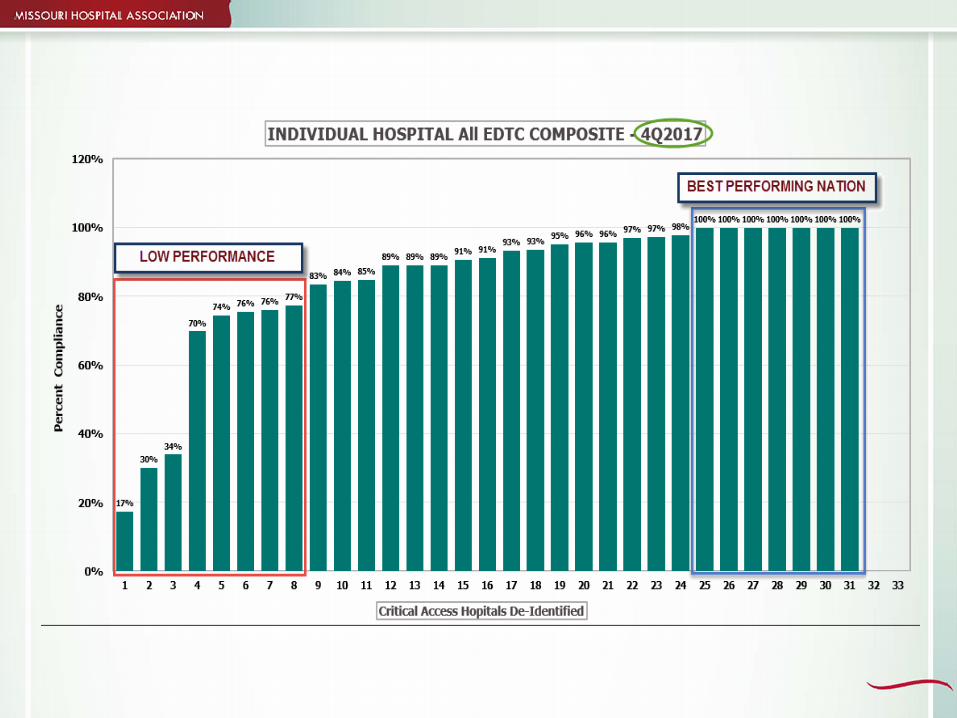



Spotlight Hospital

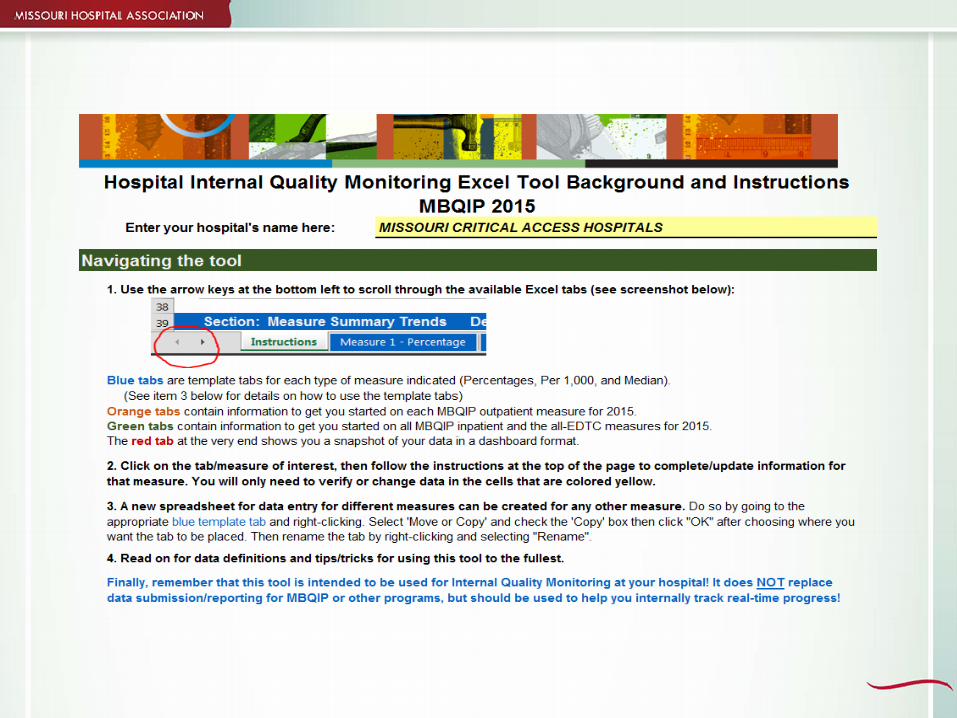
Internal Quality Monitoring Tool
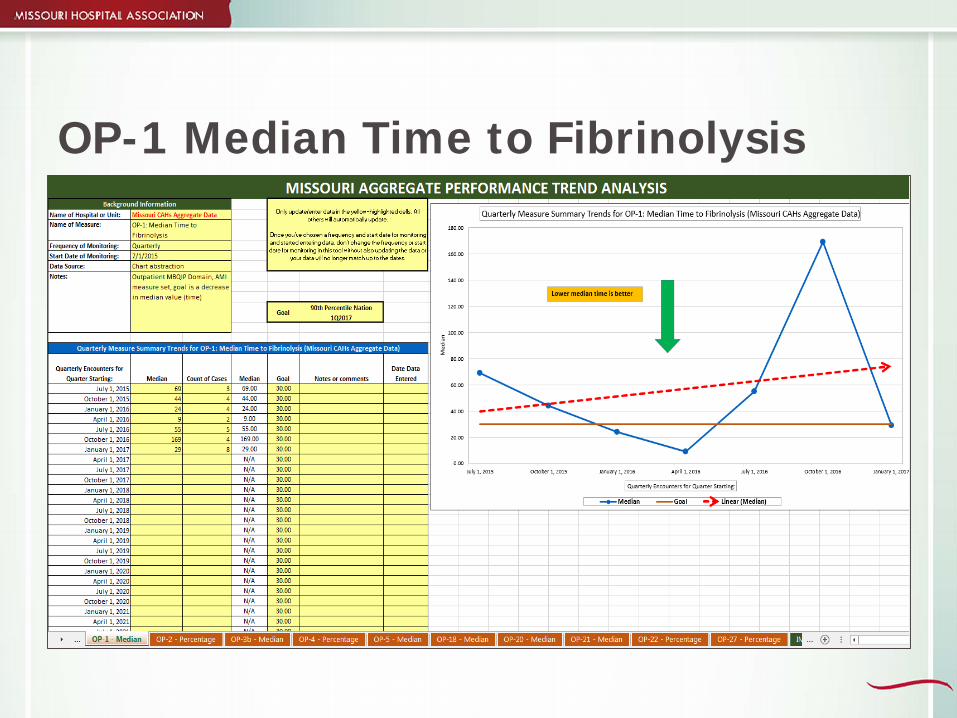
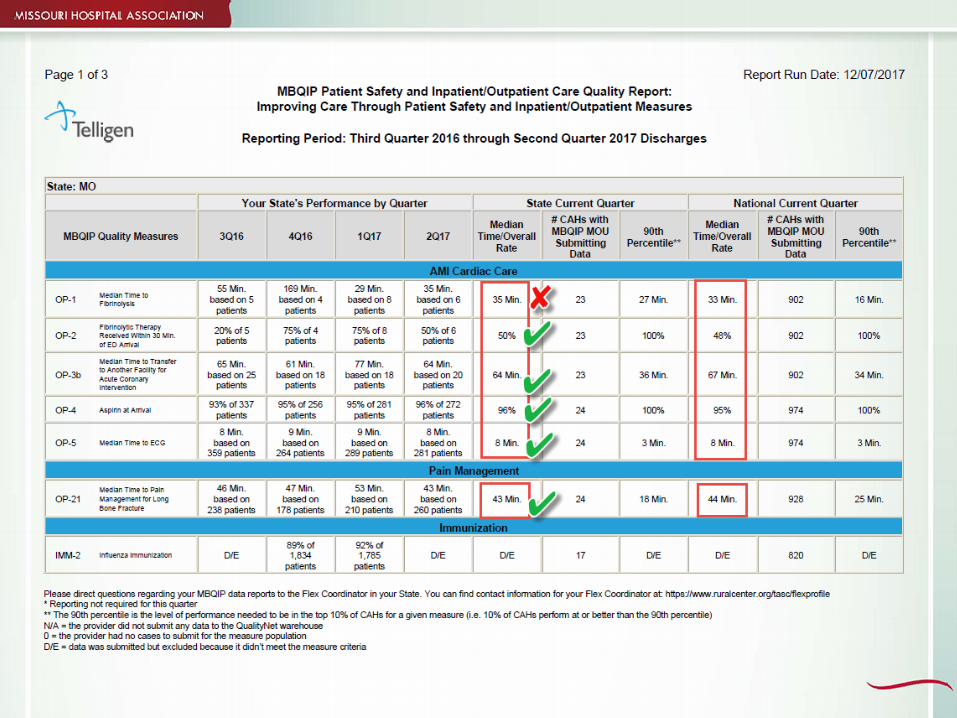
OP-1 Median Time to Fibrinolysis
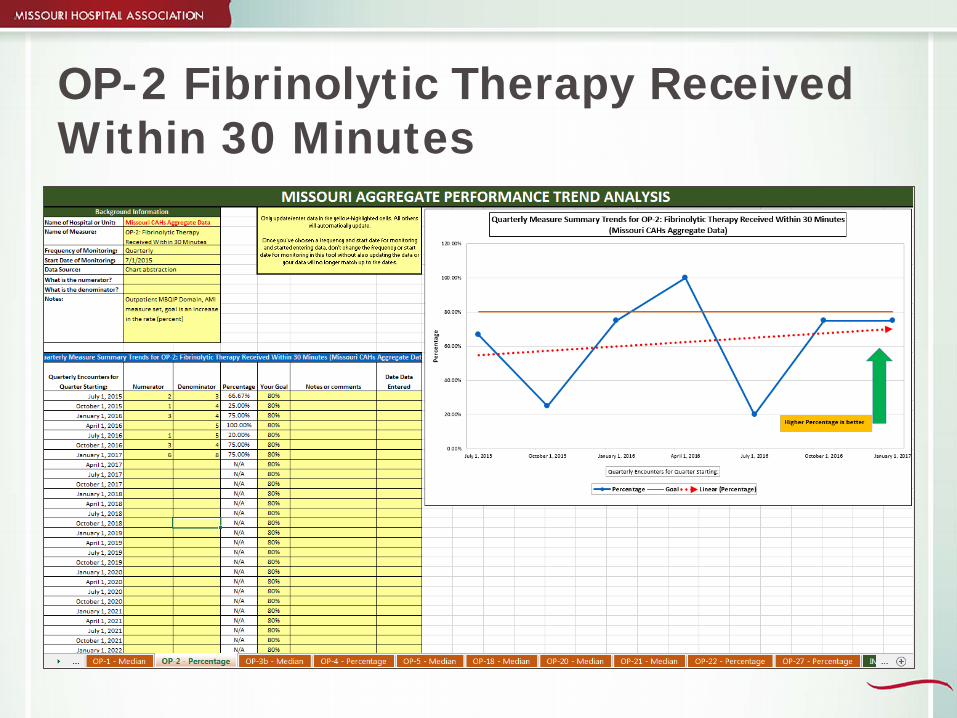
OP-2 Fibrinolytic Therapy Received Within 30 Minutes
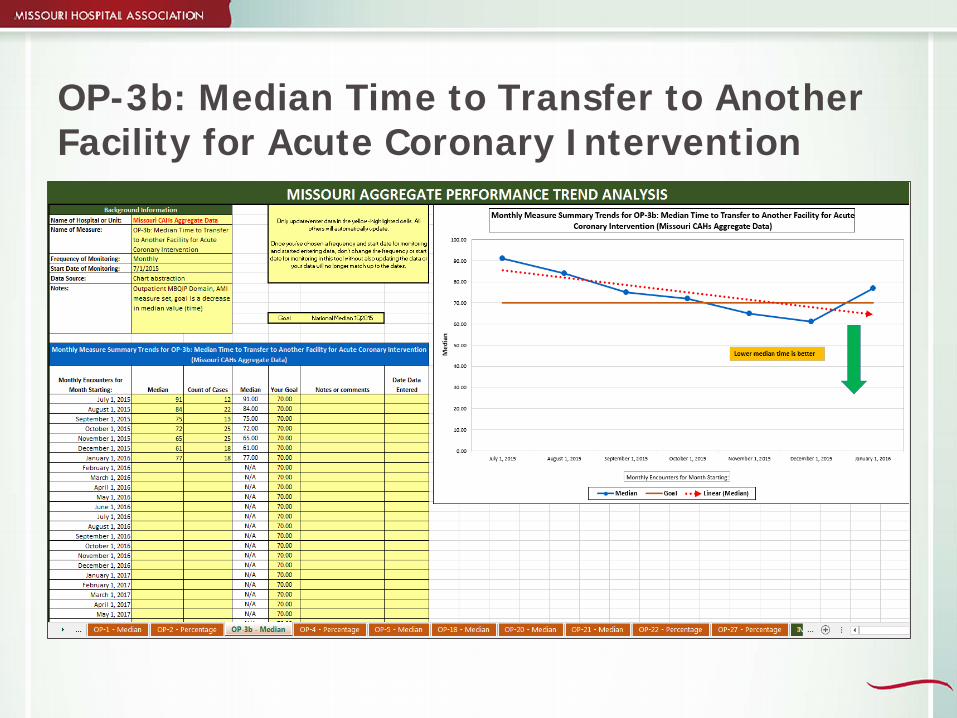
OP-3b: Median Time to Transfer to Another Facility for Acute Coronary Intervention
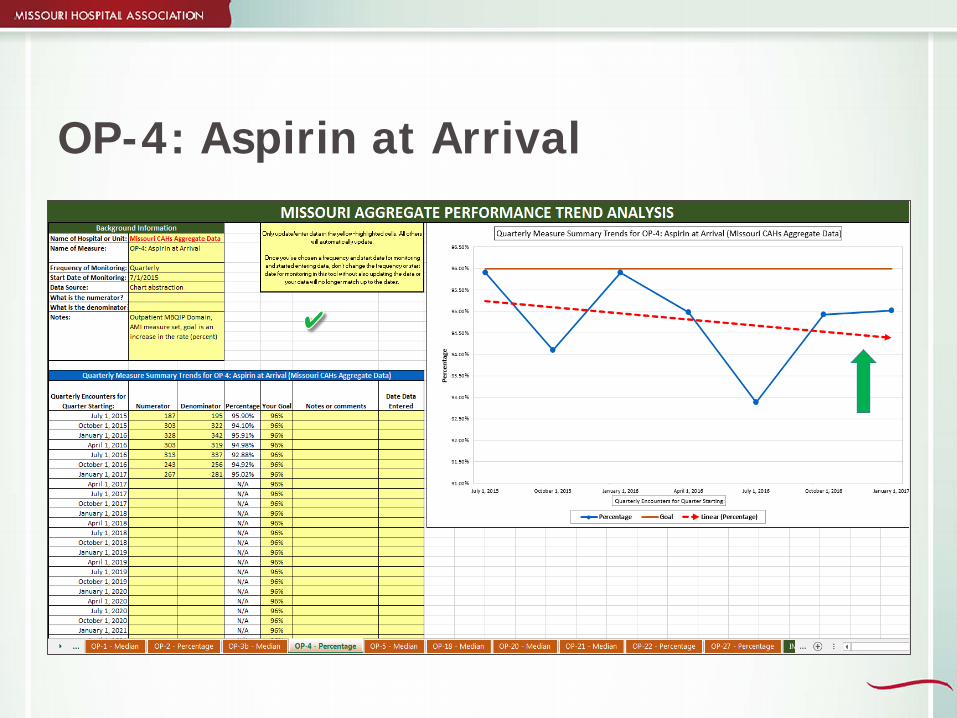
OP-4: Aspirin at Arrival
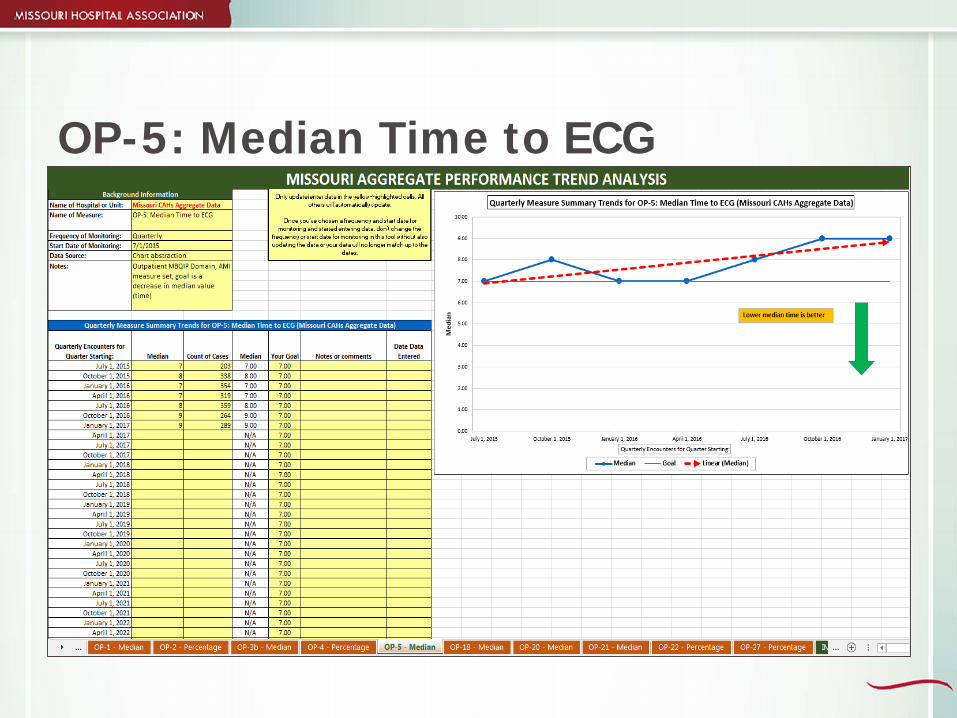
OP-5: Median Time to ECG
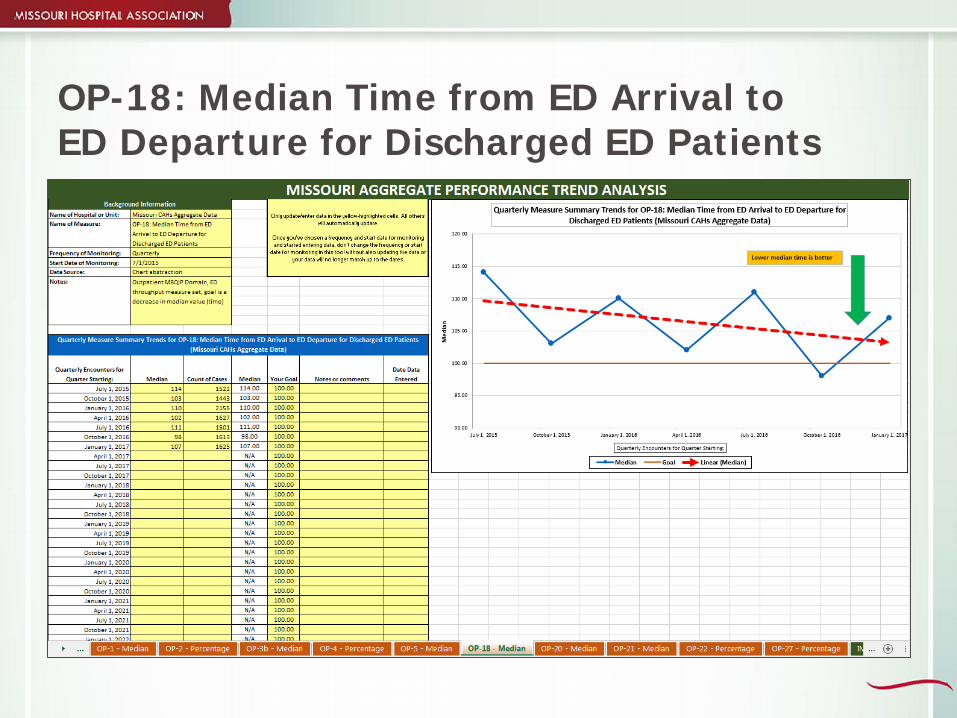
OP-18: Median Time from ED Arrival to ED Departure for Discharged ED Patients
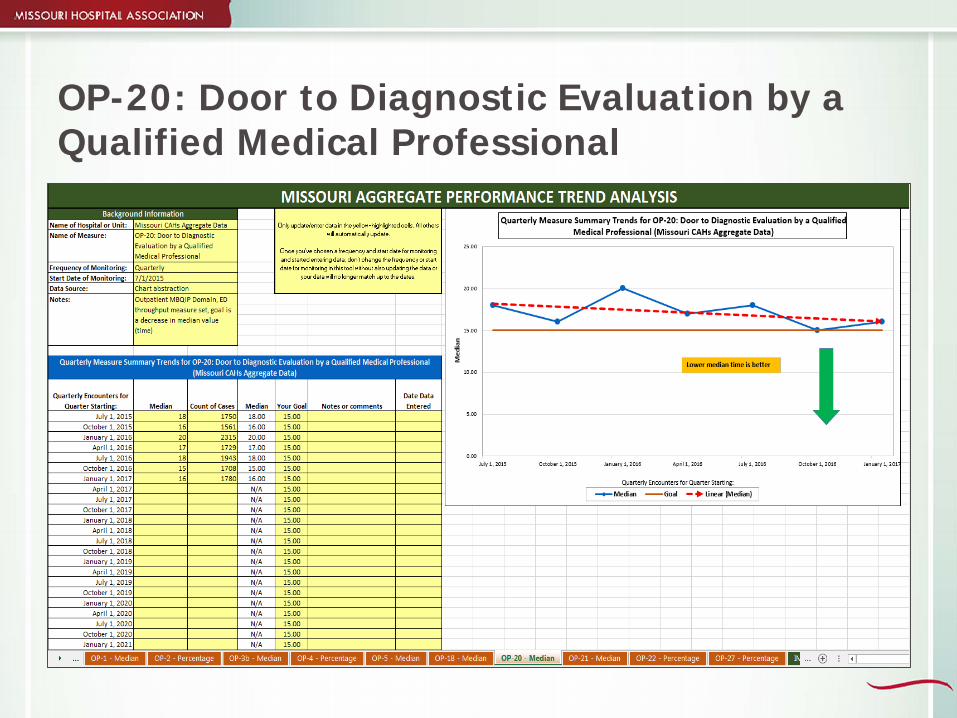
OP-20: Door to Diagnostic Evaluation by a Qualified Medical Professional
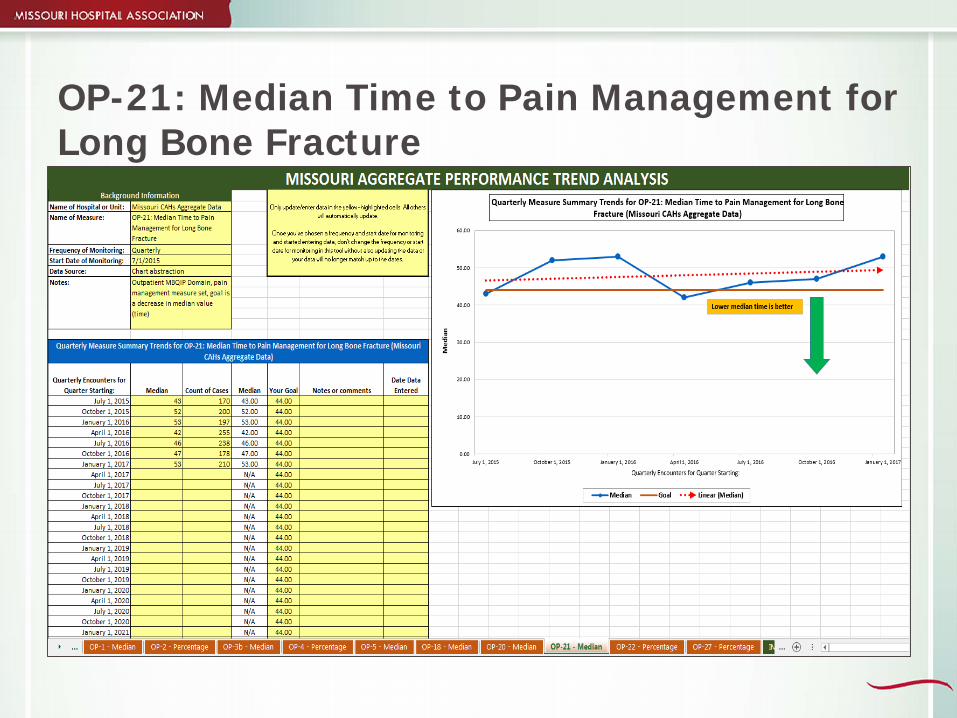
OP-21: Median Time to Pain Management for Long Bone Fracture
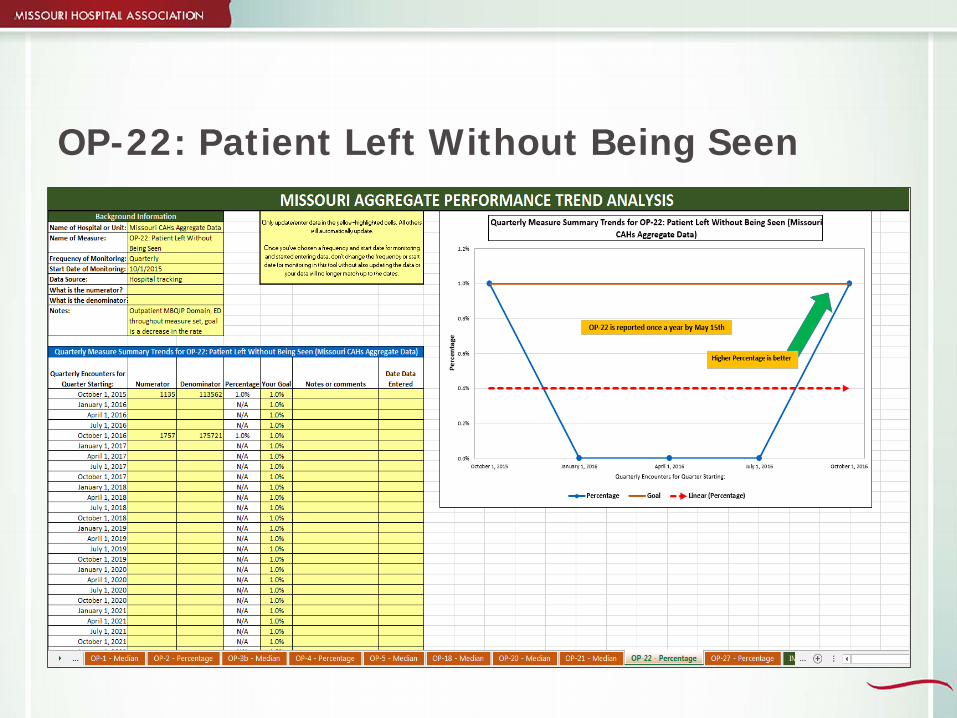
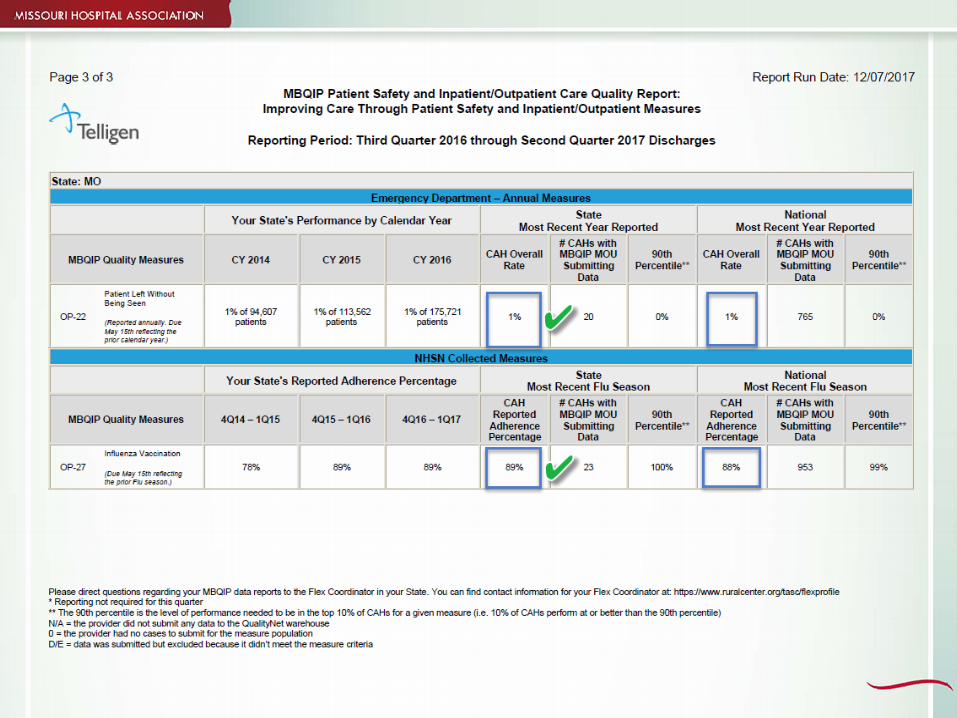
OP-22: Patient Left Without Being Seen
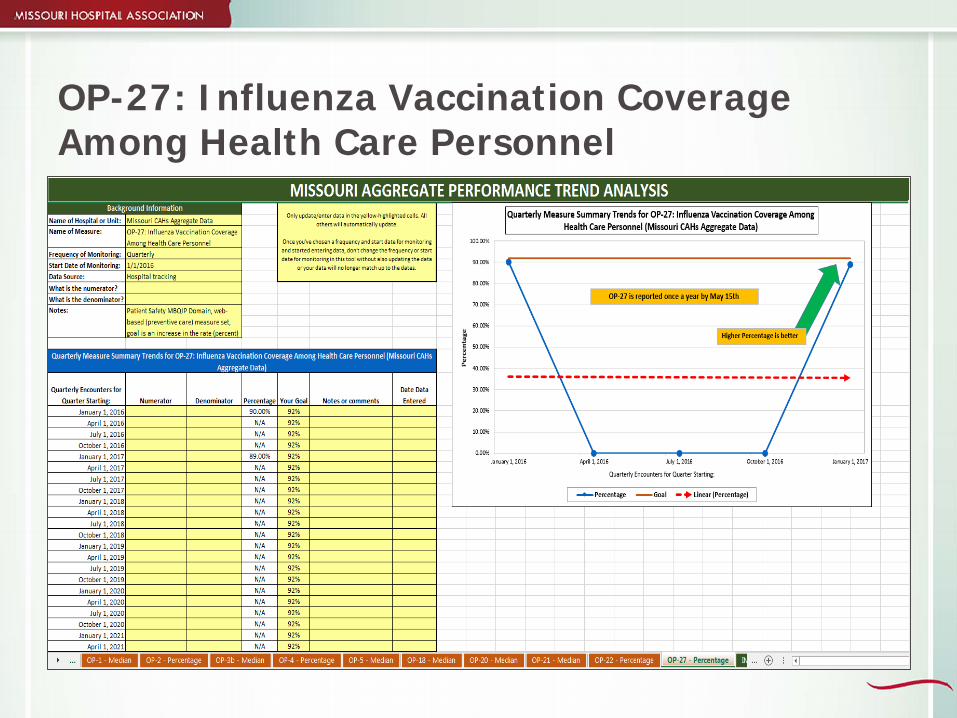
OP-27: Influenza Vaccination Coverage Among Health Care Personnel
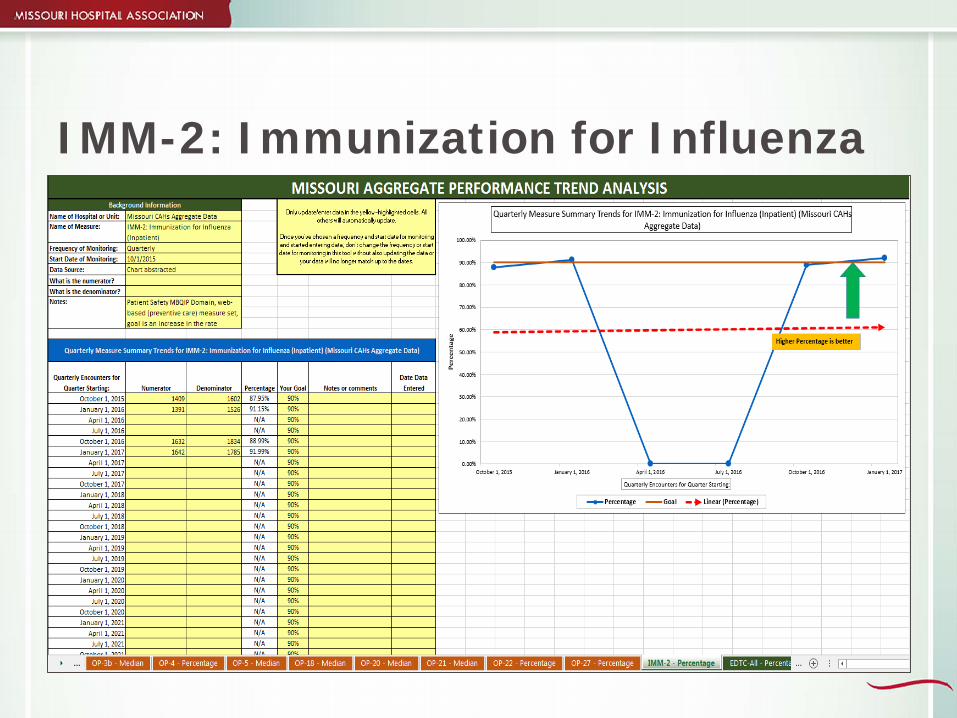
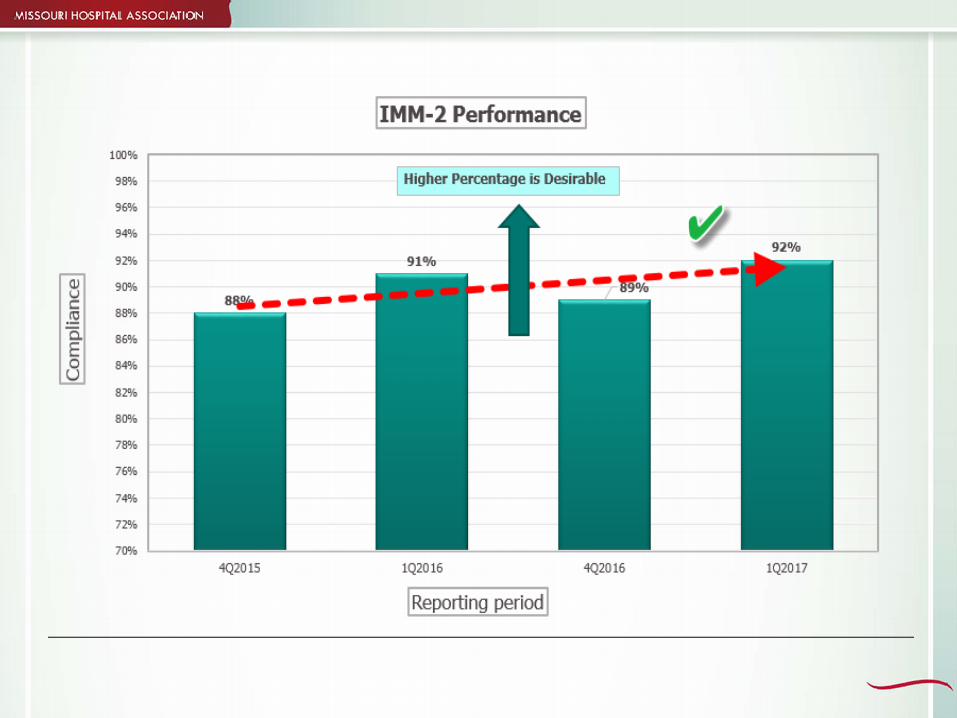
IMM-2: Immunization for Influenza
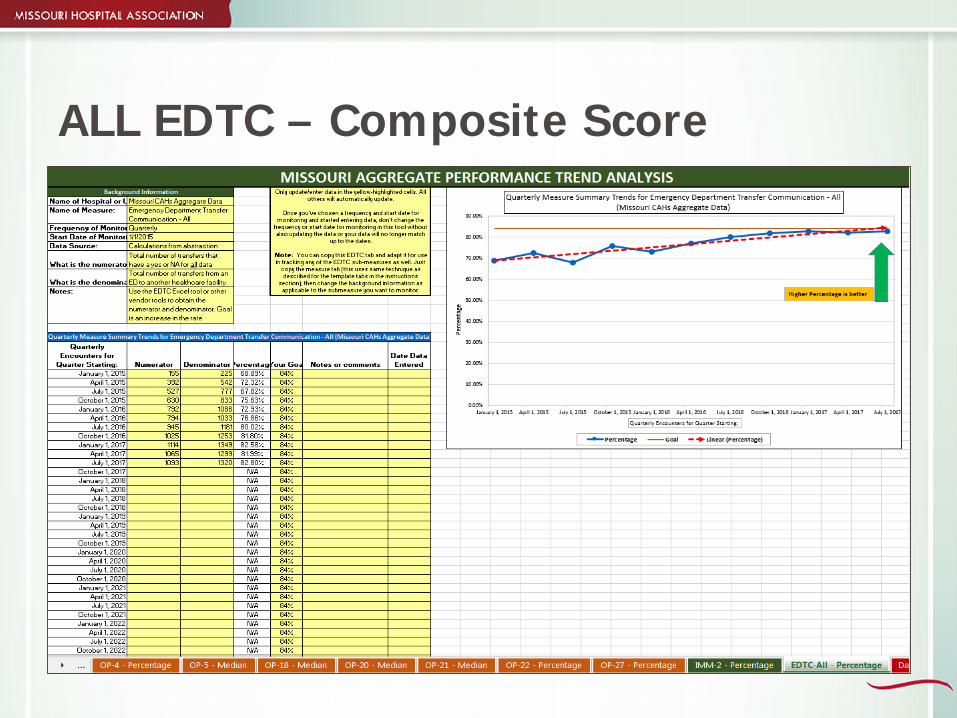
ALL EDTC – Composite Score
Food for Thought“Even if you’re on the right track,
you’ll get run over if you just sit there.”-Will Rogers
Resources

Care Learning
Online program Orientation FLEX program overview Quality reporting and improvement Financial and operational excellence Population health management
Cost is covered by FLEX program

Resources HCAHPS http://www.hcahpsonline.org/home.aspx MBQIP Measures Fact Sheets
http://web.mhanet.com/SQI/mbqip/MBQIP-Measures-Fact-Sheets-Final_2015-11-10.pdf Federal Office of Rural Health Policy
http://www.hrsa.gov/ruralhealth/ FLEX Monitoring Team http://www.flexmonitoring.org/ QualityNet https://www.qualitynet.org/ CDC Antibiotic Stewardship Program
https://www.cdc.gov/getsmart/healthcare/pdfs/core-elements.pdf#page=14
References
MHA http://web.mhanet.com/mbqip.aspxMHA https://web.mhanet.com/chna.aspx QualityNet https://www.qualitynet.org Hospital Compare
https://www.medicare.gov/hospitalcompare/search.html National Rural Health Resource Center
https://www.ruralcenter.org/tasc/mbqip


Stephen Njenga, MPH, MHA, CPHQ, CPPSDirector of Performance Measurement Compliance
Missouri Hospital [email protected]
573/893-3700, ext. 1325