medicare beneficiary quality improvement project (mbqip) · medicare beneficiary quality...
TRANSCRIPT
MEDICARE BENEFICIARY QUALITYIMPROVEMENT PROJECT (MBQIP)
Began in September 2011
Key quality improvement activity within the Medicare Rural Hospital Flexibility grant program
Goal of MBQIP: to improve quality of care in small rural hospitals
Voluntary program
SCIENCE OF MBQIP
Quality Measurement
Quality Improvement
Improved Patient Outcomes
How Quality Reporting to MBQIP Can Help Your Facility
• Identify opportunities for improvement
• Track progress of improvements
• Gauge how your performance stacks up against other providers
• Demonstrates to your community that your are dedicated to patient safety,
transparency and providing the best possible care
• Positively affect your bottom line – what gets measured, gets managed
Drop the Denominator
• Collecting data has a human impact
• Therefore, it’s best to measure missed opportunities – Not percentages
• Each missed opportunity should be evaluated as to how a new or current
process is performing
SMALL HOSPITAL IMPROVEMENT PROGRAM(SHIP)
To support hospital activities related to patient quality improvement, attaining equipment and/or training to comply with meaningful use of health information technology, ICD-10 standards, and payment bundling.
Hospitals utilize funds to:1) pay for costs related to maintaining accurate prospective payment system
billing and coding such as updating and or implementing ICD-10 hardware/software
2) pay for the costs related to delivery system changes as outlined in the ACA such as value-based purchasing (VBP), accountable care organizations (ACO), and payment bundling.
Participation SHIP Grant Program
SHIP program is very menu driven and hierarchical
1. Signed MBQIP agreement and actively reporting quality measures
2. Working toward ICD-10 implementation and/or Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)
3. Other menu items once 1 and 2 above are met
Medicare Rural Hospital Flexibility Grant Program (Flex)
Three Main Areas:
• Quality Improvement
• Financial and Operational Improvement
• Community Health Needs Assessments

Flex Program
Strongly recommended MBQIP participation in 2013-2014 grant• MBQIP would become intricately involved with Flex• Quality Improvement Organization – Mountain Pacific (Shanelle and
Ericka) actively recruited and provided TA for MBQIP reporting
MBQIP participation mandatory for Flex participation in 2014-2015• Critical Access Hospitals not reporting MBQIP must implement
program• All Critical Access Hospitals must be reporting required MBQIP
measures by August 31, 2015

REPORTING MBQIP MEASURES
Measures reported to QualityNet (CMS Hospital Compare website)
CART tool may be used for extraction and reporting
Measures were implemented in 3 phases:
Phase 1 – Inpatient MeasuresPhase 2 – Outpatient Measures
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)
Phase 3 – Emergency Department Transfer CommunicationPharmacy Review
MBQIP REPORTING MEASURES
Phase 1 Measures
• Pneumonia: CMS Hospital Compare Core Measure (participate in all sub-measures);
PN-3b: Blood Cultures Performed in the Emergency Department Prior to Initial Antibiotic Received in Hospital PN-62: Initial Antibiotic Selection for CAP in Immunocompetent Patient
• Congestive Heart Failure: CMS Hospital Compare Core Measure (participate in all sub-measures)
HF-1: Discharge Instructions HF-2: Evaluation of LVS Function HF-3: ACEI or ARB for LVSD
MBQIP REPORTING MEASURES
Phase 2 Measures Outpatient 1-7: Hospital Compare CMS Measure (all sub-
measures that apply);
OP-1: Median Time to Fibrinolysis in the Emergency Department OP-2: Fibrinolytic Therapy Received Within 30 Minutes of ED Arrival
in the Emergency Department OP-3: Median Time to Transfer to another Facility for Acute Coronary
Intervention in the Emergency Department OP-4: Aspirin at Arrival in the Emergency Department OP-5: Median Time to ECG in the Emergency Department OP-6: Timing of Antibiotic Prophylaxis (Prophylactic Antibiotic
Initiated Within One Hour Prior to Surgical Incision) in Surgery OP-7: Prophylactic Antibiotic Selection for Surgical Patients in
Surgery
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)
MBQIP REPORTING MEASURES
Phase 3 Measures • Pharmacist CPOE/Verification of Medication Orders Within 24 Hours
Numerator: Number of patients whose medication orders are directly entered (CPOE) or verified by a pharmacist within 24 hours.
Denominator: Number of patients with at least one medication in their medication list (entered using CPOE) admitted to a CAH’s inpatient or emergency department during the reporting period.
• Outpatient Emergency Department Transfer Communication (Seven Elements) o Pre-Transfer Communication Information o Patient Identification o Vital Signs o Medication-related Information o Practitioner generated information o Nurse generated information o Procedures and tests
Medicare Beneficiary Quality Improvement Project (MBQIP)
Pharmacist CPOE/Verification of Medication Orders within 24 Hours Measure Guide Background: Adverse drug events account for 34.2% of all hospital acquired conditions (Partnership for Patients, 2010). Additionally, each hospital patient can expect to be subjected to, on average, more than one medication error per day (IOM, 2006). The goal of the MBQIP Phase 3 Pharmacist Verification of Medication Orders within 24 hours is to increase the level of pharmacist oversight of the medication administration process at Critical Access Hospitals, resulting in fewer errors, better medication management, and improved patient outcomes. The measure was designed to be non-burdensome, providing a simple numerator/denominator percent value derived from a report generated by the hospital’s order entry software. The Measure: The Pharmacist CPOE/Verification of Medication Orders within 24 Hours Measure consists of a numerator and denominator: Numerator: Number of electronically entered medication orders for an inpatient admitted to a CAH (acute or swing-bed), verified by a pharmacist or directly entered by a pharmacist within 24 hours. Denominator: Total number of electronically entered medication orders for inpatients admitted to a CAH (acute or swing-bed) during the reporting period. Inclusion Criteria: Inpatients admitted to acute care bed, swing bed; observation patients Exclusion Criteria: Outpatients; ED patients Preferred Method: The numerator and denominator are pulled from the Verification Report. Alternate method: The numerator is the number of electronically entered medication orders for an inpatient admitted to a CAH (acute or swing-bed), verified by a pharmacist or directly entered by a pharmacist within 24 hours – based on the pharmacist coverage hours. The denominator would still be reported as the total number of electronically entered medication orders for inpatients admitted to a CAH (acute or swing-bed) during the reporting period.
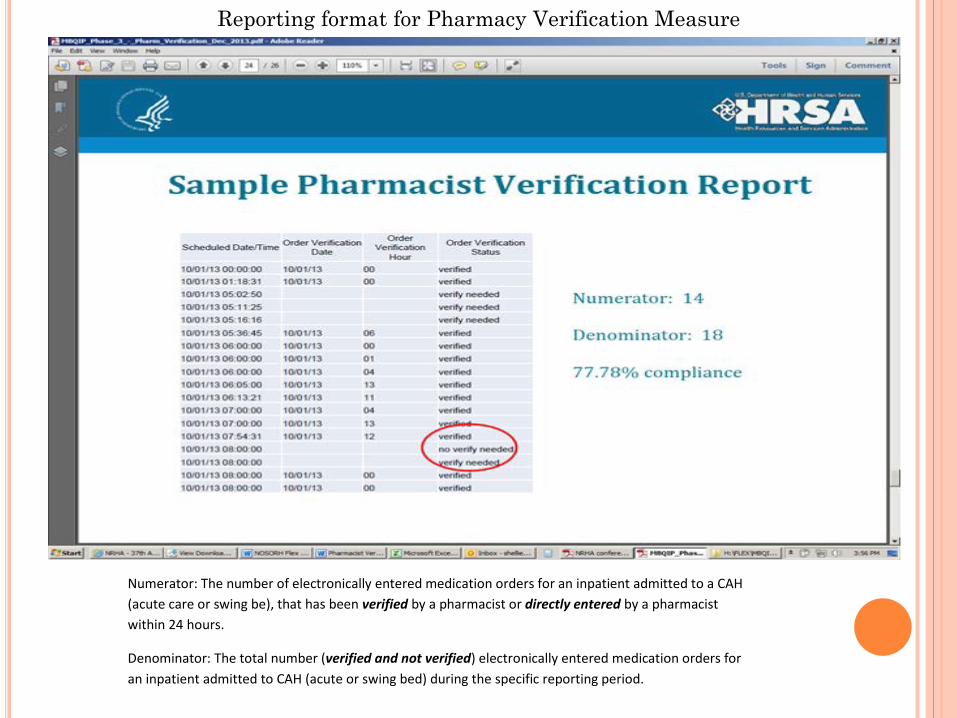
Reporting format for Pharmacy Verification Measure
Numerator: The number of electronically entered medication orders for an inpatient admitted to a CAH (acute care or swing be), that has been verified by a pharmacist or directly entered by a pharmacist within 24 hours.
Denominator: The total number (verified and not verified) electronically entered medication orders for an inpatient admitted to CAH (acute or swing bed) during the specific reporting period.
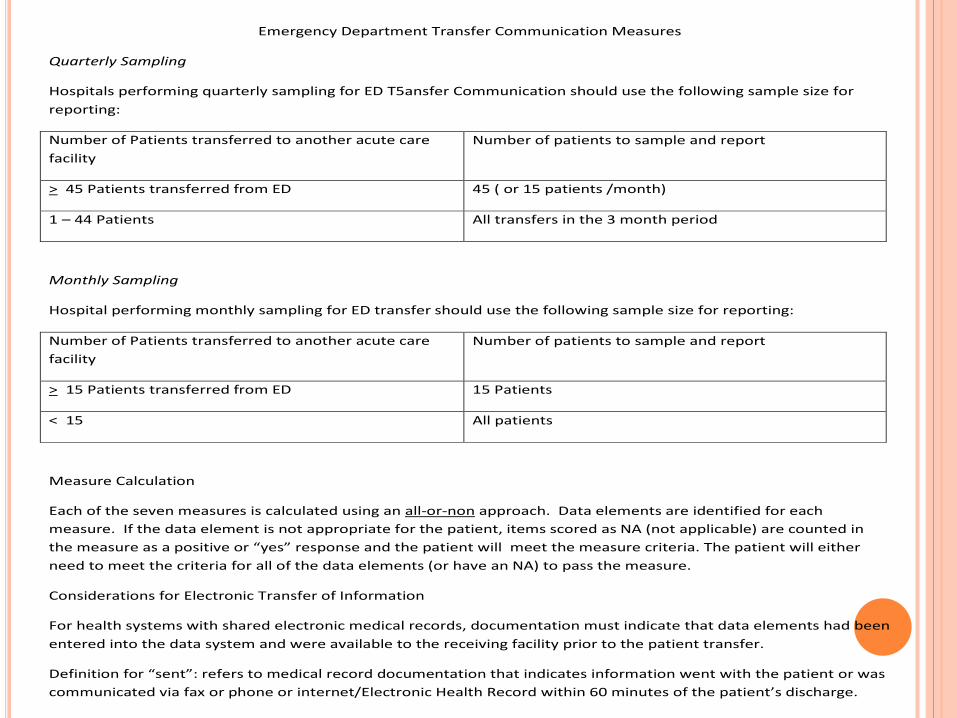
Emergency Department Transfer Communication Measures
Quarterly Sampling
Hospitals performing quarterly sampling for ED T5ansfer Communication should use the following sample size for reporting:
Number of Patients transferred to another acute care facility
Number of patients to sample and report
> 45 Patients transferred from ED 45 ( or 15 patients /month)
1 – 44 Patients All transfers in the 3 month period
Monthly Sampling
Hospital performing monthly sampling for ED transfer should use the following sample size for reporting:
Number of Patients transferred to another acute care facility
Number of patients to sample and report
> 15 Patients transferred from ED 15 Patients
< 15 All patients
Measure Calculation
Each of the seven measures is calculated using an all-or-non approach. Data elements are identified for each measure. If the data element is not appropriate for the patient, items scored as NA (not applicable) are counted in the measure as a positive or “yes” response and the patient will meet the measure criteria. The patient will either need to meet the criteria for all of the data elements (or have an NA) to pass the measure.
Considerations for Electronic Transfer of Information
For health systems with shared electronic medical records, documentation must indicate that data elements had been entered into the data system and were available to the receiving facility prior to the patient transfer.
Definition for “sent”: refers to medical record documentation that indicates information went with the patient or was communicated via fax or phone or internet/Electronic Health Record within 60 minutes of the patient’s discharge.
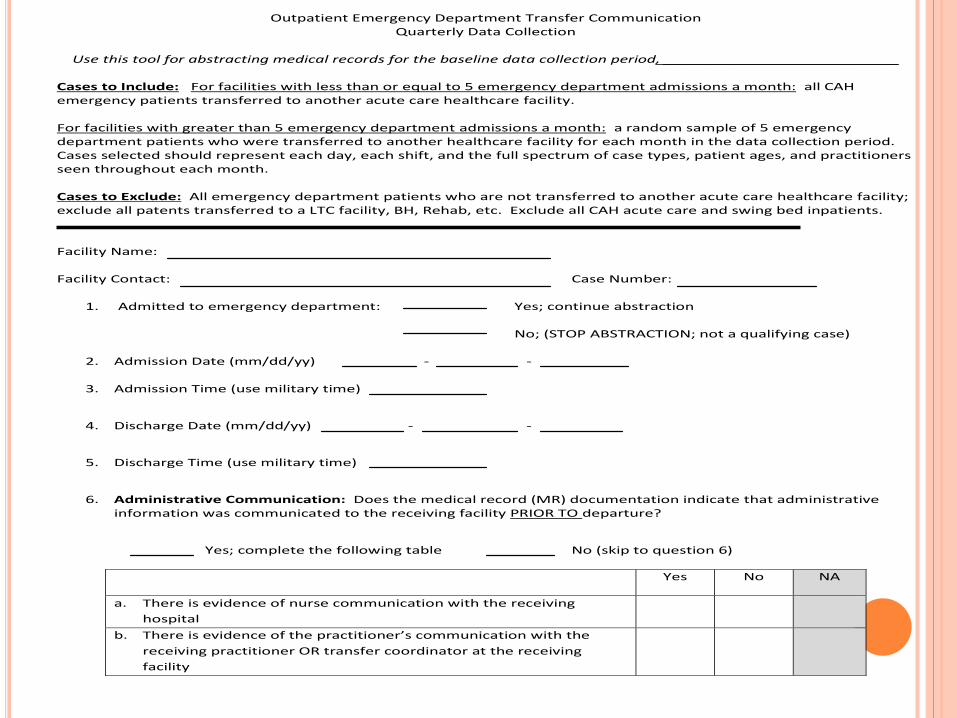
Outpatient Emergency Department Transfer Communication Quarterly Data Collection
Use this tool for abstracting medical records for the baseline data collection period, ___________________________
Cases to Include: For facilities with less than or equal to 5 emergency department admissions a month: all CAH emergency patients transferred to another acute care healthcare facility. For facilities with greater than 5 emergency department admissions a month: a random sample of 5 emergency department patients who were transferred to another healthcare facility for each month in the data collection period. Cases selected should represent each day, each shift, and the full spectrum of case types, patient ages, and practitioners seen throughout each month. Cases to Exclude: All emergency department patients who are not transferred to another acute care healthcare facility; exclude all patents transferred to a LTC facility, BH, Rehab, etc. Exclude all CAH acute care and swing bed inpatients. Facility Name: Facility Contact: Case Number:
1. Admitted to emergency department: Yes; continue abstraction
No; (STOP ABSTRACTION; not a qualifying case)
2. Admission Date (mm/dd/yy) - -
3. Admission Time (use military time)
4. Discharge Date (mm/dd/yy) - -
5. Discharge Time (use military time)
6. Administrative Communication: Does the medical record (MR) documentation indicate that administrative information was communicated to the receiving facility PRIOR TO departure?
Yes; complete the following table No (skip to question 6)
Yes No NA
a. There is evidence of nurse communication with the receiving hospital
b. There is evidence of the practitioner’s communication with the receiving practitioner OR transfer coordinator at the receiving facility
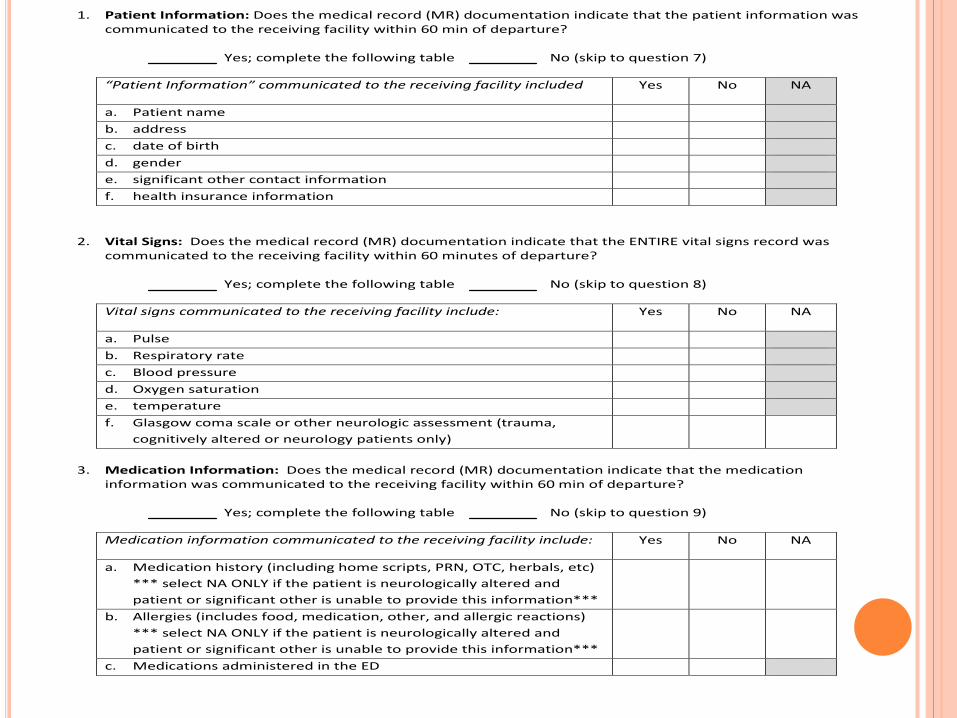
1. Patient Information: Does the medical record (MR) documentation indicate that the patient information was communicated to the receiving facility within 60 min of departure?
Yes; complete the following table No (skip to question 7)
“Patient Information” communicated to the receiving facility included Yes No NA
a. Patient name b. address c. date of birth d. gender e. significant other contact information f. health insurance information
2. Vital Signs: Does the medical record (MR) documentation indicate that the ENTIRE vital signs record was communicated to the receiving facility within 60 minutes of departure?
Yes; complete the following table No (skip to question 8)
Vital signs communicated to the receiving facility include: Yes No NA
a. Pulse b. Respiratory rate c. Blood pressure d. Oxygen saturation e. temperature f. Glasgow coma scale or other neurologic assessment (trauma,
cognitively altered or neurology patients only)
3. Medication Information: Does the medical record (MR) documentation indicate that the medication
information was communicated to the receiving facility within 60 min of departure?
Yes; complete the following table No (skip to question 9)
Medication information communicated to the receiving facility include: Yes No NA
a. Medication history (including home scripts, PRN, OTC, herbals, etc) *** select NA ONLY if the patient is neurologically altered and patient or significant other is unable to provide this information***
b. Allergies (includes food, medication, other, and allergic reactions) *** select NA ONLY if the patient is neurologically altered and patient or significant other is unable to provide this information***
c. Medications administered in the ED
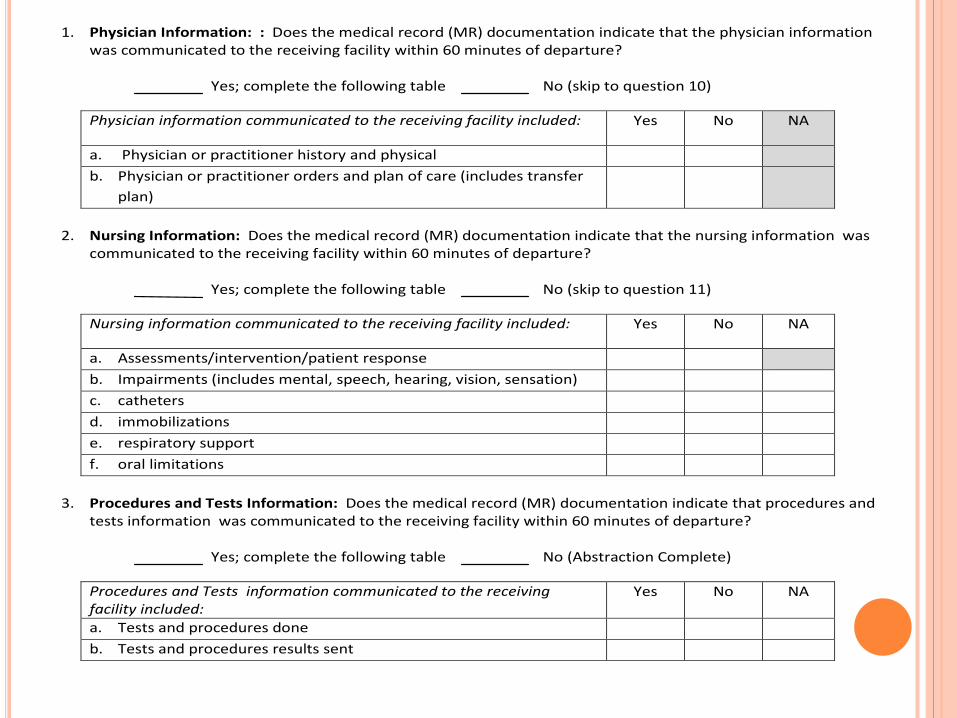
1. Physician Information: : Does the medical record (MR) documentation indicate that the physician information was communicated to the receiving facility within 60 minutes of departure?
Yes; complete the following table No (skip to question 10)
Physician information communicated to the receiving facility included: Yes No NA
a. Physician or practitioner history and physical b. Physician or practitioner orders and plan of care (includes transfer
plan)
2. Nursing Information: Does the medical record (MR) documentation indicate that the nursing information was
communicated to the receiving facility within 60 minutes of departure?
Yes; complete the following table No (skip to question 11)
Nursing information communicated to the receiving facility included: Yes No NA
a. Assessments/intervention/patient response b. Impairments (includes mental, speech, hearing, vision, sensation) c. catheters d. immobilizations e. respiratory support f. oral limitations
3. Procedures and Tests Information: Does the medical record (MR) documentation indicate that procedures and
tests information was communicated to the receiving facility within 60 minutes of departure?
Yes; complete the following table No (Abstraction Complete)
Procedures and Tests information communicated to the receiving facility included:
Yes No NA
a. Tests and procedures done b. Tests and procedures results sent
• Congestive Heart Failure: CMS Hospital Compare Core Measure o HF-1: Discharge Instructions (Retired by CMS 12/31/2013, can still upload into
CART until further notice) o HF-2: Evaluation of LVS Function (Retired by CMS 01/01/2015, can still upload
into CART until further notice) o HF-3: ACEI or ARB for LVSD (Retired by CMS 01/01/2015, can still upload into
CART until further notice) • Pneumonia: CMS Hospital Compare Core Measure
o PN-3b: Blood Cultures Performed in the Emergency Department Prior to Initial Antibiotic Received in Hospital (Retired by CMS 12/31/2013, but can still upload into CART until further notice)
o PN-6b: Initial Antibiotic Selection for CAP in Immunocompetent Patient (Retired by CMS 01/01/2015, can still upload into CART until further notice)
CMS Retired Measures – Still MBQIP Active
• OP-4: Aspirin at Arrival in the Emergency Department (Retired by CMS 01/01/2015, can still upload into CART until further notice)
• OP-5: Median Time to ECG in the Emergency Department • OP-6: Timing of Antibiotic Prophylaxis (Prophylactic Antibiotic Initiated Within One
Hour Prior to Surgical Incision) in Surgery(Retired by CMS 01/01/2015, can still upload into CART until further notice)
• OP-7: Prophylactic Antibiotic Selection for Surgical Patients in Surgery (Retired by CMS 01/01/2015, can still upload into CART until further notice)
CMS Names VIQR National Support Contractor
The Centers for Medicare & Medicaid Services (CMS) has announced that FMQAI/HSAG has been named the Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach and Education National Support Contractor.
Submit all questions regarding the Hospital IQR Program to the contractor via the Hospital Inpatient Quality Reporting Questions and Answers tool or by phone, toll-free, at (844) 472-4477 or (866) 800-8765 weekdays from 8 a.m. to 8 p.m. Eastern Time (5 a.m. to 5 p.m. Pacific Time).
The Centers for Medicare & Medicaid Services (CMS) has designated HSAG as the Hospital OQR Program Support Contractor. HSAG provides technical support and feedback to assist hospitals with quality data reporting.
Submit all questions about the Hospital OQR Program to HSAG at Hospital Outpatient —Questions/Answers or by calling, toll-free, (866) 800-8756 weekdays from 7 a.m. to 6 p.m. Eastern Time.
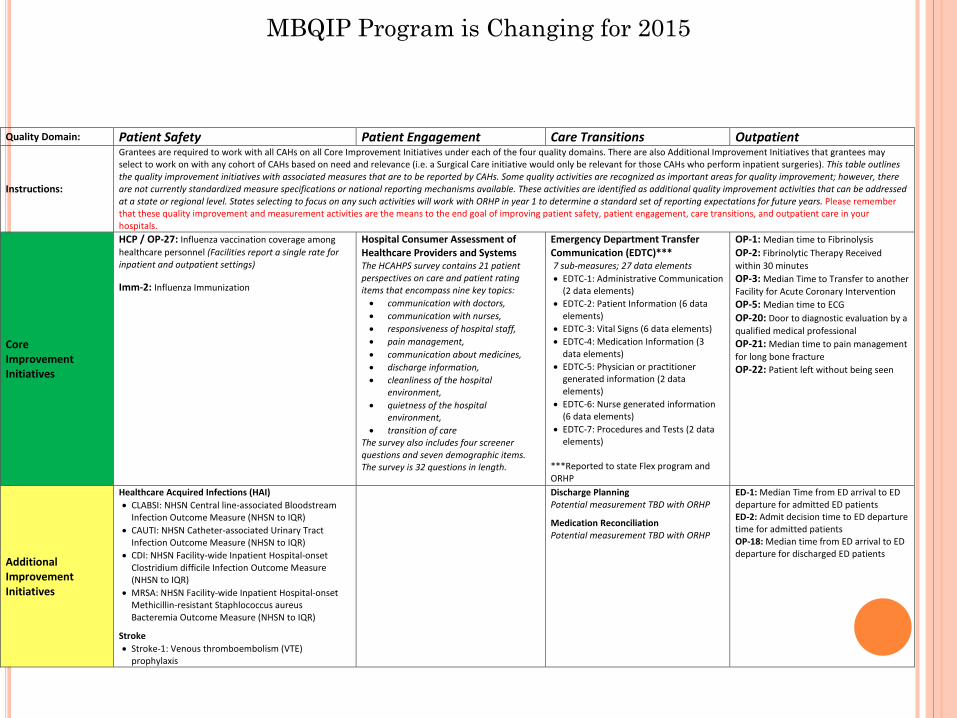
Quality Domain: Patient Safety Patient Engagement Care Transitions Outpatient
Instructions:
Grantees are required to work with all CAHs on all Core Improvement Initiatives under each of the four quality domains. There are also Additional Improvement Initiatives that grantees may select to work on with any cohort of CAHs based on need and relevance (i.e. a Surgical Care initiative would only be relevant for those CAHs who perform inpatient surgeries). This table outlines the quality improvement initiatives with associated measures that are to be reported by CAHs. Some quality activities are recognized as important areas for quality improvement; however, there are not currently standardized measure specifications or national reporting mechanisms available. These activities are identified as additional quality improvement activities that can be addressed at a state or regional level. States selecting to focus on any such activities will work with ORHP in year 1 to determine a standard set of reporting expectations for future years. Please remember that these quality improvement and measurement activities are the means to the end goal of improving patient safety, patient engagement, care transitions, and outpatient care in your hospitals.
Core Improvement Initiatives
HCP / OP-27: Influenza vaccination coverage among healthcare personnel (Facilities report a single rate for inpatient and outpatient settings) Imm-2: Influenza Immunization
Hospital Consumer Assessment of Healthcare Providers and Systems The HCAHPS survey contains 21 patient perspectives on care and patient rating items that encompass nine key topics: • communication with doctors, • communication with nurses, • responsiveness of hospital staff, • pain management, • communication about medicines, • discharge information, • cleanliness of the hospital
environment, • quietness of the hospital
environment, • transition of care
The survey also includes four screener questions and seven demographic items. The survey is 32 questions in length.
Emergency Department Transfer Communication (EDTC)*** 7 sub-measures; 27 data elements • EDTC-1: Administrative Communication
(2 data elements) • EDTC-2: Patient Information (6 data
elements) • EDTC-3: Vital Signs (6 data elements) • EDTC-4: Medication Information (3
data elements) • EDTC-5: Physician or practitioner
generated information (2 data elements)
• EDTC-6: Nurse generated information (6 data elements)
• EDTC-7: Procedures and Tests (2 data elements)
***Reported to state Flex program and ORHP
OP-1: Median time to Fibrinolysis OP-2: Fibrinolytic Therapy Received within 30 minutes OP-3: Median Time to Transfer to another Facility for Acute Coronary Intervention OP-5: Median time to ECG OP-20: Door to diagnostic evaluation by a qualified medical professional OP-21: Median time to pain management for long bone fracture OP-22: Patient left without being seen
Additional Improvement Initiatives
Healthcare Acquired Infections (HAI) • CLABSI: NHSN Central line-associated Bloodstream
Infection Outcome Measure (NHSN to IQR) • CAUTI: NHSN Catheter-associated Urinary Tract
Infection Outcome Measure (NHSN to IQR) • CDI: NHSN Facility-wide Inpatient Hospital-onset
Clostridium difficile Infection Outcome Measure (NHSN to IQR)
• MRSA: NHSN Facility-wide Inpatient Hospital-onset Methicillin-resistant Staphlococcus aureus Bacteremia Outcome Measure (NHSN to IQR)
Stroke • Stroke-1: Venous thromboembolism (VTE)
prophylaxis
Discharge Planning Potential measurement TBD with ORHP
Medication Reconciliation Potential measurement TBD with ORHP
ED-1: Median Time from ED arrival to ED departure for admitted ED patients ED-2: Admit decision time to ED departure time for admitted patients OP-18: Median time from ED arrival to ED departure for discharged ED patients
MBQIP Program is Changing for 2015
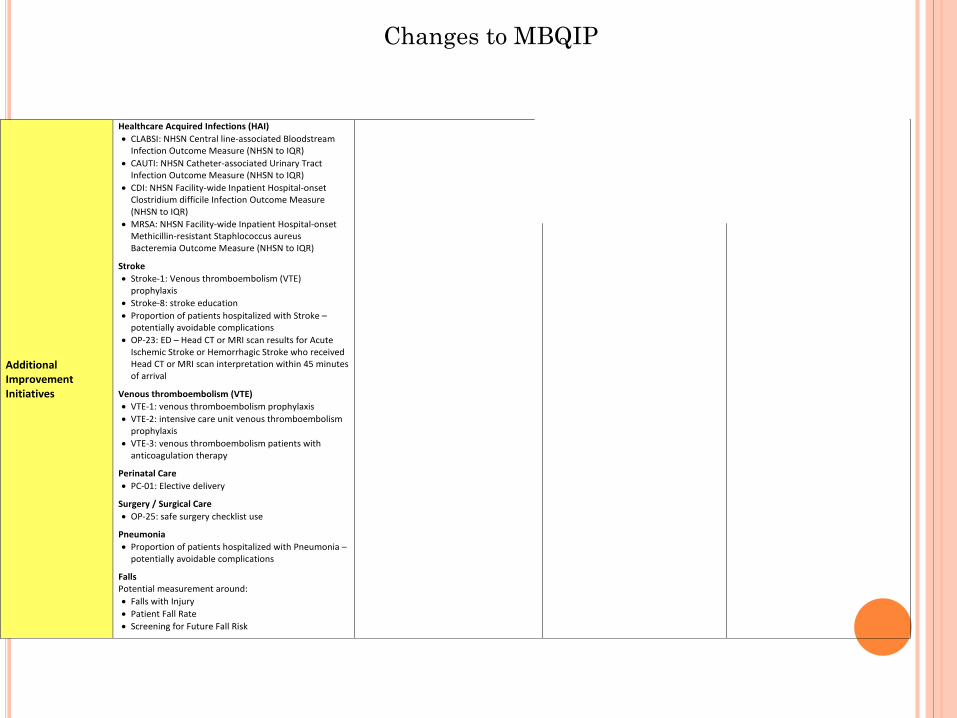
Additional Improvement Initiatives
Healthcare Acquired Infections (HAI) • CLABSI: NHSN Central line-associated Bloodstream
Infection Outcome Measure (NHSN to IQR) • CAUTI: NHSN Catheter-associated Urinary Tract
Infection Outcome Measure (NHSN to IQR) • CDI: NHSN Facility-wide Inpatient Hospital-onset
Clostridium difficile Infection Outcome Measure (NHSN to IQR)
• MRSA: NHSN Facility-wide Inpatient Hospital-onset Methicillin-resistant Staphlococcus aureus Bacteremia Outcome Measure (NHSN to IQR)
Stroke • Stroke-1: Venous thromboembolism (VTE)
prophylaxis • Stroke-8: stroke education • Proportion of patients hospitalized with Stroke –
potentially avoidable complications • OP-23: ED – Head CT or MRI scan results for Acute
Ischemic Stroke or Hemorrhagic Stroke who received Head CT or MRI scan interpretation within 45 minutes of arrival
Venous thromboembolism (VTE) • VTE-1: venous thromboembolism prophylaxis • VTE-2: intensive care unit venous thromboembolism
prophylaxis • VTE-3: venous thromboembolism patients with
anticoagulation therapy
Perinatal Care • PC-01: Elective delivery
Surgery / Surgical Care • OP-25: safe surgery checklist use
Pneumonia • Proportion of patients hospitalized with Pneumonia –
potentially avoidable complications
Falls Potential measurement around: • Falls with Injury • Patient Fall Rate • Screening for Future Fall Risk
Discharge Planning Potential measurement TBD with ORHP
Medication Reconciliation Potential measurement TBD with ORHP
ED-1: Median Time from ED arrival to ED departure for admitted ED patients ED-2: Admit decision time to ED departure time for admitted patients OP-18: Median time from ED arrival to ED departure for discharged ED patients
Changes to MBQIP