medicare hospital reimbursement university of michigan health system presented by thomas marks...
Post on 22-Dec-2015
225 views
TRANSCRIPT
Medicare Hospital Reimbursement
University of Michigan
Health Systempresented by Thomas Marks
Director, Hospital Accounting&Reimbursement
Medicare Payment Systems
Institutional• Hospital inpatient
– medical/surgical
– psychiatric
– rehabilitation
– long-term, childrens, cancer
• Hospital outpatient
• Skilled nursing facility
• Hospice
• Ambulatory surgery center
Other Providers• Physician
• Clinical laboratory
• Physical/speech/occ therapy
• End stage renal dialysis
• Ambulance (ground and air)
• Durable medical equipment
• Home infusion
• Home health agency

Topics to Cover
• Brief historical perspective
• Medicare inpatient PPS– DRGs - Disproportionate share
– Area wage adjustments - Direct GME
– Indirect medical education - Organ acquisition
• Medicare outpatient PPS– APCs, structure and payment rules
– HOPD status
• Settlements
• Medicare policy issues
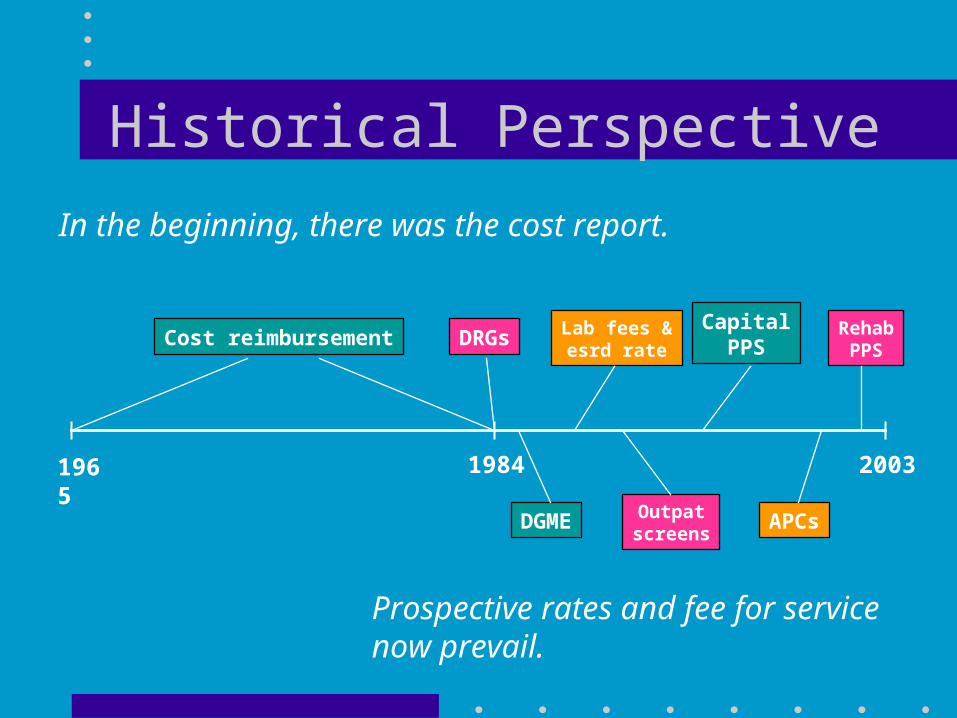
Historical Perspective
1965 1984 2003
DRGs
In the beginning, there was the cost report.
DGME
Lab fees &esrd rate
Outpatscreens
APCs
CapitalPPS
RehabPPS
Cost reimbursement
Prospective rates and fee for service now prevail.

Historical Perspective (continued)
• What remains as cost-reimbursed: – inpatient psychiatric (although subject to a cap)
– organ acquisition
• “Cost” is still important in Medicare policy– All payment systems are benchmarked to cost in the aggregate
– Some payment systems provide extensive payment differentiation based on cost differences
– Cost data is used to set weights and rates for prospective payments
Inpatient Payment• DRG-based payment = adjusted rate x DRG relative weight
– Operating and capital components are separate but similar
– Psych and rehab units are excluded
• Adjusters: – area wage index
– indirect medical education (IME)
– disproportionate share (DSH)
• Additional payments:– outliers
– direct graduate medical education (GME)
– organ acquisition
– bad debts
UMHHC 2002 PPS Revenue
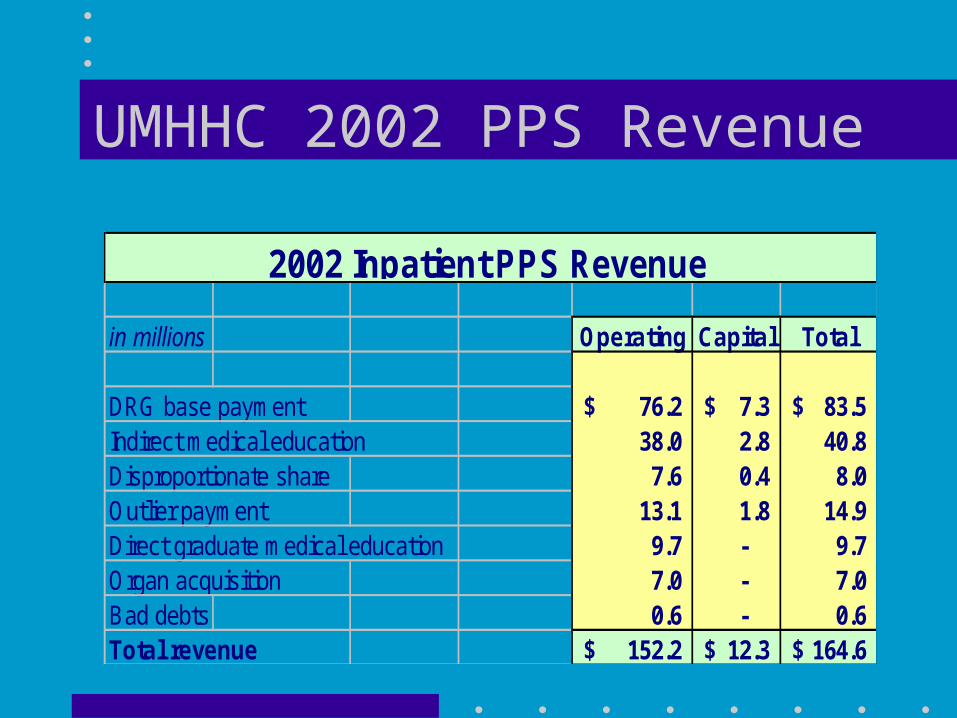
in millions Operating Capital Total
DRG base payment 76.2$ 7.3$ 83.5$ Indirect medical education 38.0 2.8 40.8 Disproportionate share 7.6 0.4 8.0 Outlier payment 13.1 1.8 14.9 Direct graduate medical education 9.7 - 9.7 Organ acquisition 7.0 - 7.0 Bad debts 0.6 - 0.6 Total revenue 152.2$ 12.3$ 164.6$
2002 Inpatient PPS Revenue
PPS Payment Differences
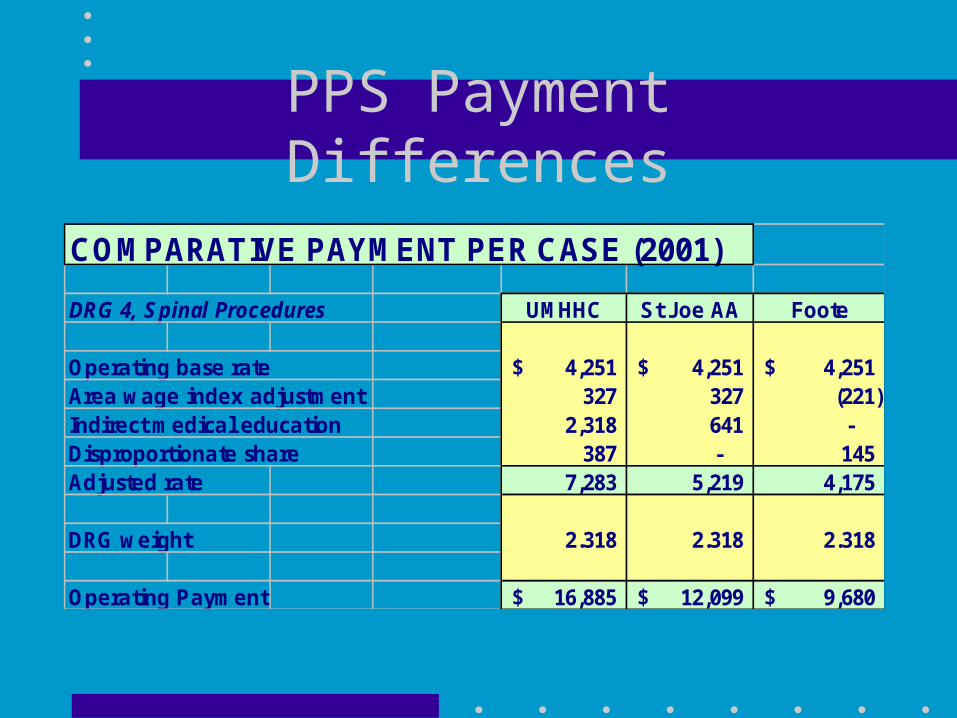
COMPARATIVE PAYMENT PER CASE (2001)
DRG 4, Spinal Procedures UMHHC St Joe AA Foote
Operating base rate 4,251$ 4,251$ 4,251$ Area wage index adjustment 327 327 (221) Indirect medical education 2,318 641 - Disproportionate share 387 - 145 Adjusted rate 7,283 5,219 4,175
DRG weight 2.318 2.318 2.318
Operating Payment 16,885$ 12,099$ 9,680$
DRG Payments
• DRG structure– Currently 528 DRGs, intended to be groupings of clinically-similar
diagnoses and procedures
– Medical DRGs - generally based on principal diagnosis
– Surgical DRGs - generally based on principal procedure
– Complications/commorbidities and patient age may also be factors
• DRG Relative Weights– Average cost of cases in a DRG compared to average cost for all cases
– Cost derived from charges on Medicare claims
– Generally, a three-year lag between claims data (used to set weights) and payment dates
DRG Payments - Weights
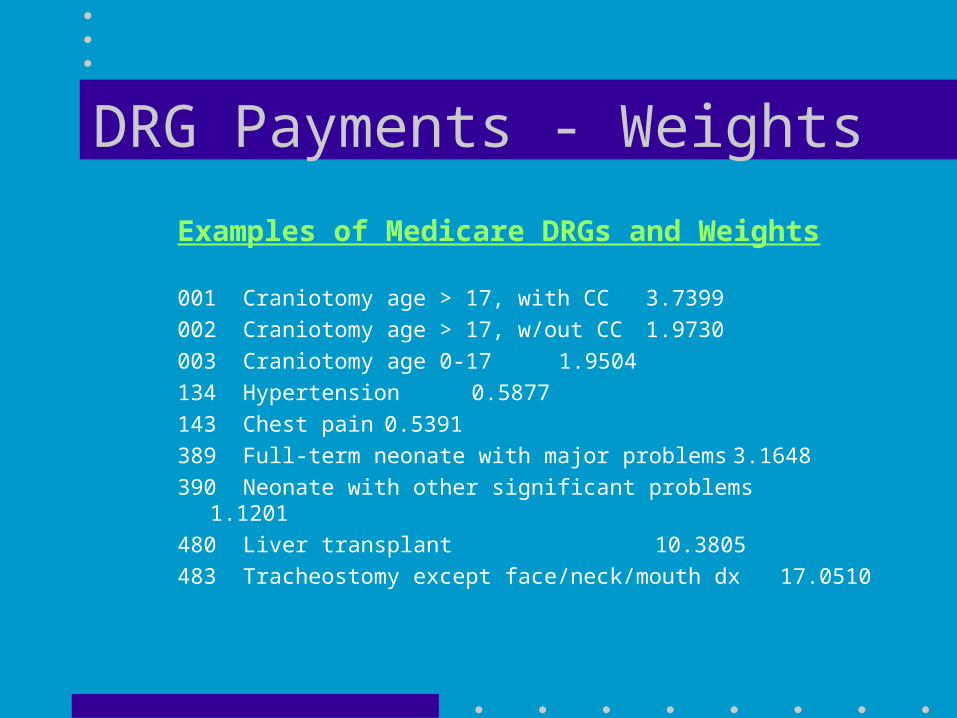
Examples of Medicare DRGs and Weights
001 Craniotomy age > 17, with CC 3.7399
002 Craniotomy age > 17, w/out CC 1.9730
003 Craniotomy age 0-17 1.9504
134 Hypertension 0.5877
143 Chest pain 0.5391
389 Full-term neonate with major problems 3.1648
390 Neonate with other significant problems 1.1201
480 Liver transplant 10.3805
483 Tracheostomy except face/neck/mouth dx 17.0510
DRG Payments - Documentation
• All inpatient cases coded by Medical Information Systems
• Cannot code what is not in the medical record
• Importance of documentation– All procedures must be defined
– Existence of complications
– Existence of commorbidities
• Several initiatives are underway to improve documentation
Area Wage Index• What does it pay for?
– Differences in cost of living (wage levels) impact cost per case
• Methodology: – Each hospital reports wage, benefit and worked hour data annually
– Average compensation per hour computed for each metro area
– Each metro area assigned an Area Wage Index value
– Labor portion of DRG rate (about 71%) is adjusted
• Examples:Ann Arbor 1.1103 New York 1.4414
Grand Rapids 0.9548 Hattiesburg MS 0.7441
Indirect Medical Education (IME)
• Why does it exist?– Teaching hospitals have higher costs
– IME is intended to level the playing field
– Statistical correlation between teaching intensity and cost per case
– Ratio of residents to beds is used to measure teaching intensity
• What does it pay for?– Patient severity and complexity not adequately addressed by DRGs
– New technology and standby capacity
– Inefficiencies, as residents provide much of the care
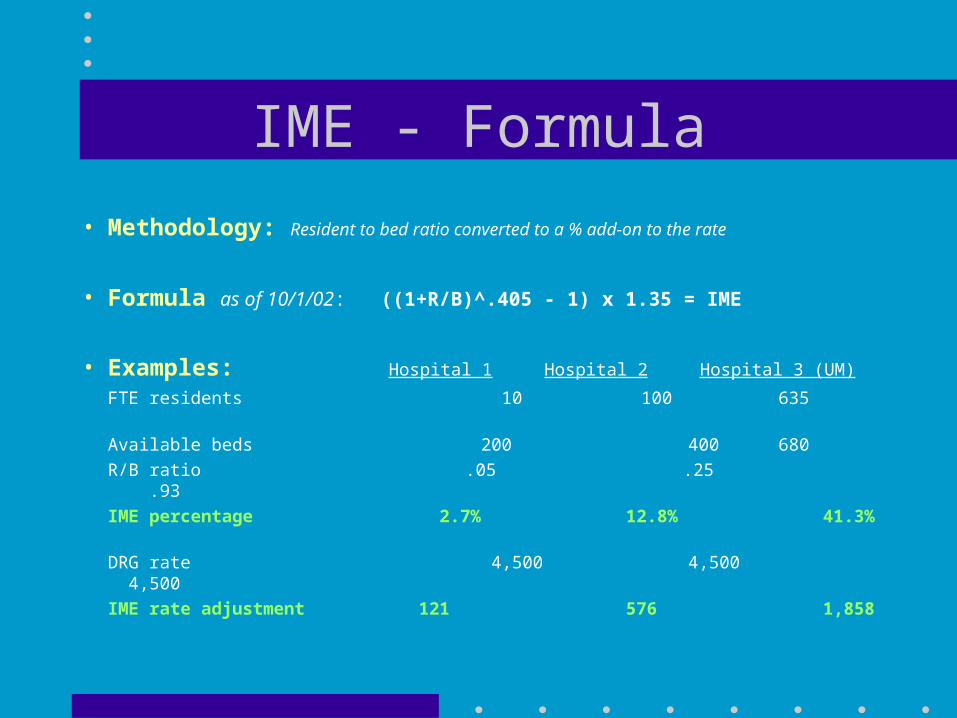
IME - Formula
• Methodology: Resident to bed ratio converted to a % add-on to the rate
• Formula as of 10/1/02: ((1+R/B)^.405 - 1) x 1.35 = IME
• Examples: Hospital 1 Hospital 2 Hospital 3 (UM)
FTE residents 10 100 635
Available beds 200 400 680
R/B ratio .05 .25 .93
IME percentage 2.7% 12.8% 41.3%
DRG rate 4,500 4,500 4,500
IME rate adjustment 121 576 1,858
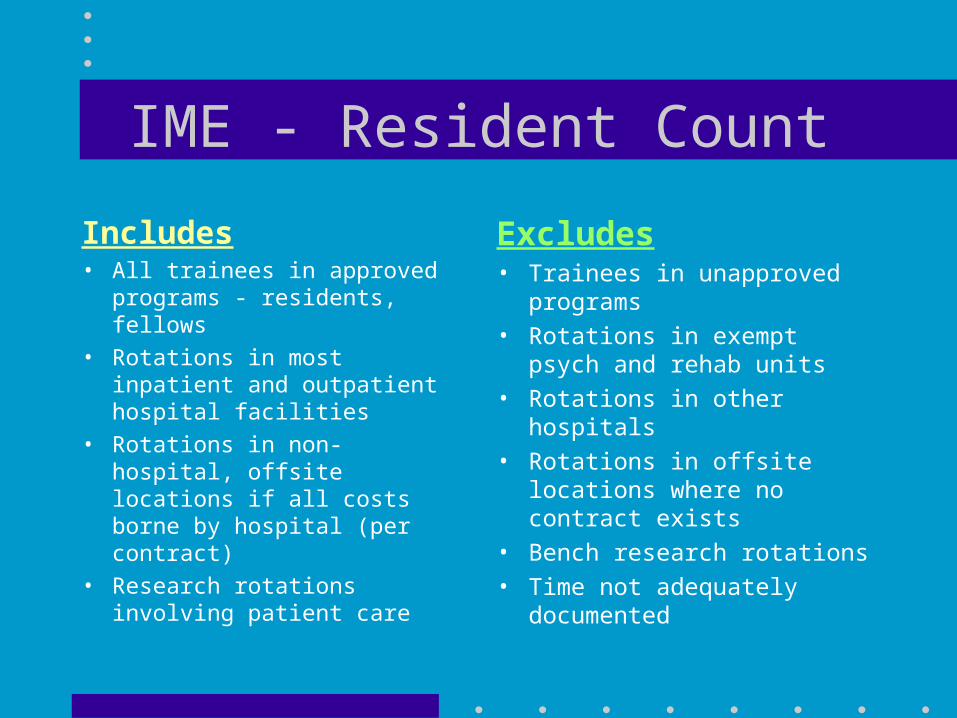
IME - Resident Count
Includes• All trainees in approved
programs - residents, fellows
• Rotations in most inpatient and outpatient hospital facilities
• Rotations in non-hospital, offsite locations if all costs borne by hospital (per contract)
• Research rotations involving patient care
Excludes• Trainees in unapproved
programs
• Rotations in exempt psych and rehab units
• Rotations in other hospitals
• Rotations in offsite locations where no contract exists
• Bench research rotations
• Time not adequately documented
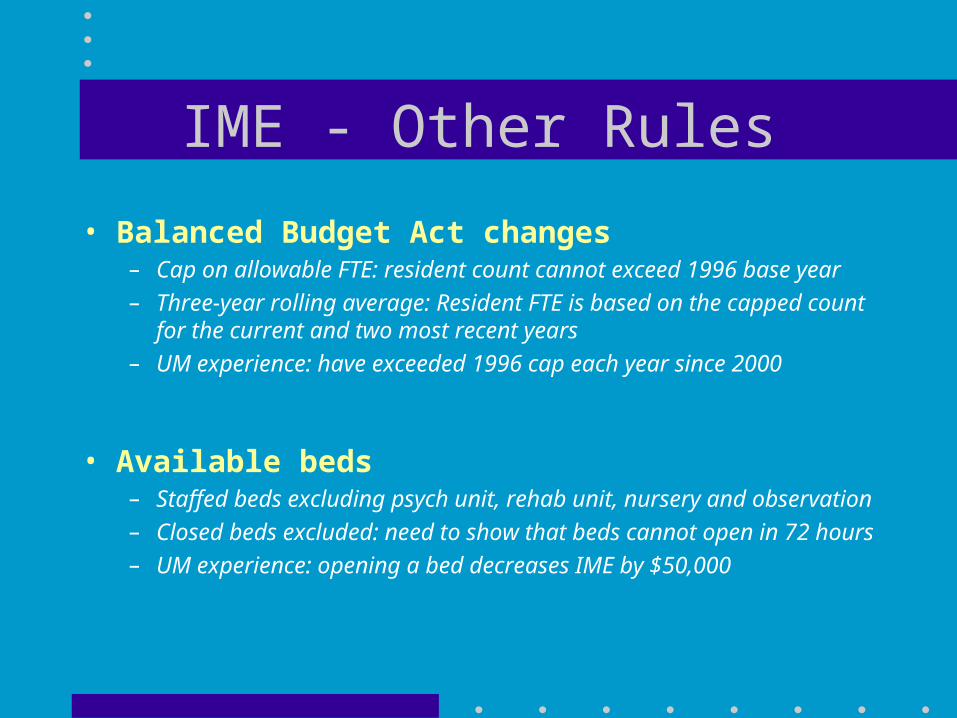
IME - Other Rules
• Balanced Budget Act changes– Cap on allowable FTE: resident count cannot exceed 1996 base year
– Three-year rolling average: Resident FTE is based on the capped count for the current and two most recent years
– UM experience: have exceeded 1996 cap each year since 2000
• Available beds– Staffed beds excluding psych unit, rehab unit, nursery and observation
– Closed beds excluded: need to show that beds cannot open in 72 hours
– UM experience: opening a bed decreases IME by $50,000
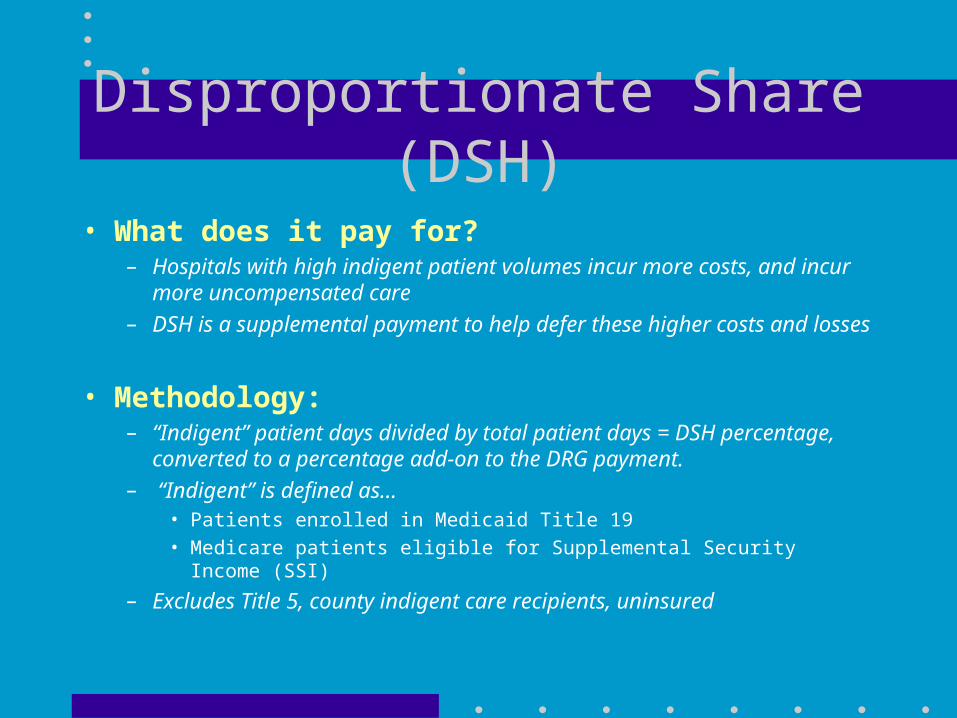
Disproportionate Share (DSH)
• What does it pay for?– Hospitals with high indigent patient volumes incur more costs, and incur
more uncompensated care– DSH is a supplemental payment to help defer these higher costs and losses
• Methodology: – “Indigent” patient days divided by total patient days = DSH percentage,
converted to a percentage add-on to the DRG payment. – “Indigent” is defined as...
• Patients enrolled in Medicaid Title 19
• Medicare patients eligible for Supplemental Security Income (SSI)
– Excludes Title 5, county indigent care recipients, uninsured
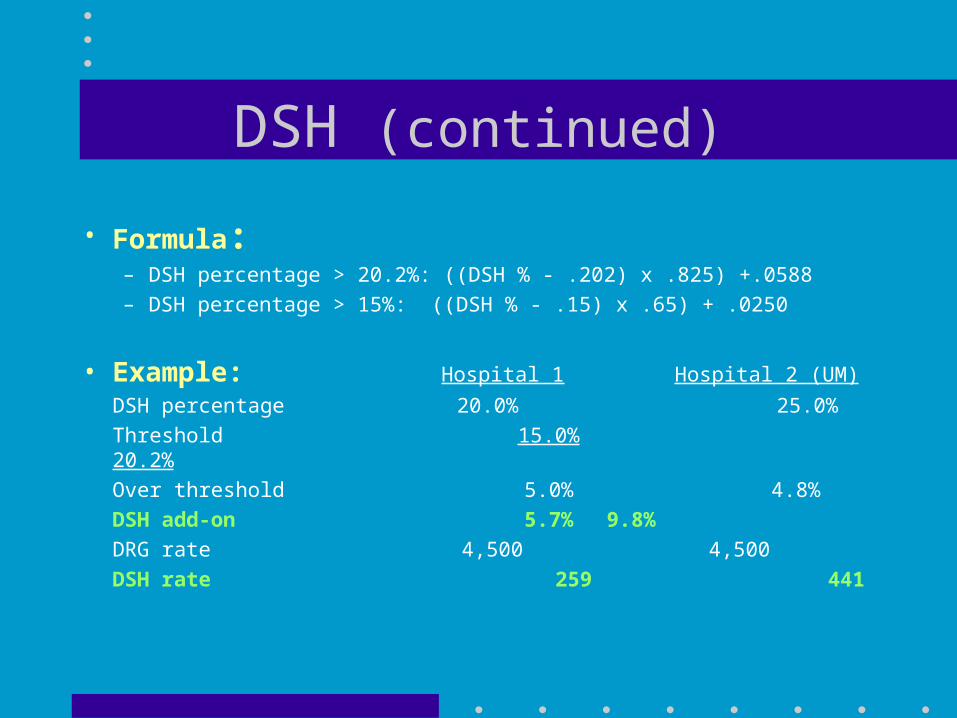
DSH (continued)
• Formula:– DSH percentage > 20.2%: ((DSH % - .202) x .825) +.0588
– DSH percentage > 15%: ((DSH % - .15) x .65) + .0250
• Example: Hospital 1 Hospital 2 (UM)
DSH percentage 20.0% 25.0%
Threshold 15.0% 20.2%
Over threshold 5.0% 4.8%
DSH add-on 5.7% 9.8%
DRG rate 4,500 4,500
DSH rate 259 441
Outlier Payments• What does it pay for?
– Individual cases may have very high costs
– Outlier payment provides partial recovery of costs not covered by DRG
• Methodology:– Charges converted to cost using hospital’s cost-to-charge ratio (CCR)
– Cost is compared to a threshold: DRG payment + fixed threshold
– Cost > threshold is reimbursed 80%
• Example: – Charges=$150,000, CCR=0.50, DRG pymt=$10,000, threshold=$33,560– Cost: $75,000 (150,000 charges x 0.50 ccr)
– Threshold: $43,560 (10,000 drg payment + 33,560 threshold)
– Outlier payment: (75,000-43,560) x 80% = $25,152
– Total payment for this case: DRG (10,000)+outlier (25,152) = $35,152
Direct GME
• What does it pay for?– Direct GME is intended to cover the direct costs of approved residency
programs: • resident salaries and benefits
• faculty supervision and teaching
• other direct costs and overhead allocable to GME
• Methodology: hospitals receive a fixed amount per resident FTE, multiplied by Medicare % of patient days– Fixed amount is hospital specific, based on 1985 cost per resident
– Medicare % of patient days includes days for patients enrolled in Medicare managed care plans
Direct GME (continued)• FTE Count: Same as IME except...
– Bench research, and rotations in psych and rehab units are included– Residents beyond initial residency period are counted at 50% (fellows)
Subject to 1996 cap
Based on three-year rolling average
• UM Experience, FY2002:– Resident FTE, unadjusted 748 FTE– Impact of initial residency period limit -108 FTE– Resident FTE, adjusted 630 FTE– Capped, three-year rolling average 603 FTE– Medicare payment per adjusted FTE $20,282 – Medicare cost per adjusted FTE $34,943

Organ Acquisition Cost• What does it pay for?
– Covers all organ procurement activities:• purchases from organ procurement agency
• excision from live donors and cadavers
• transportation, preservation
• administrative support
– Also covers pre-transplant evaluations of prospective recipients/donors• clinic visits, tissue typing, diagnostic testing
• Methodology - cost reimbursement:– Medicare cost report used to determine cost for each organ type– Medicare pays its share of total cost based on ratio of Medicare usable
organs / total usable organs
• UM results: average reimbursement > $40,000 per organ
PPS-Exempt Units• Psychiatric exempt unit
– cost reimbursed subject to a per-discharge limit
– limit = 75th percentile cost per discharge
• Rehabilitation exempt unit– through 2002: cost subject to per-discharge limit
– beginning FY2003: prospective payment system• DRG-like groups called case-mix groups (CMGs)
• 100 CMGs in total, four levels of severity for each CMG
• Assignment based on...
– impairment category (stroke, spinal cord injury, head trauma, etc)
– functional scores (motor skills, cognitive skills)
– patient age
• Adjustments for Area Wage differences, DSH (no IME)
• Additional payment for outlier cases

Outpatient Reimbursement
UMHS MEDICARE OUTPATIENT (Millions)
Charges Payments
Outpatient prospective payment (APCs) 80.4$ 42.4$ Clinical laboratory 11.7 2.7 Physical, speech, occupational therapy 3.5 1.9 Renal dialysis 2.0 0.3 Air ambulance 1.3 0.9
98.9$ 48.2$
Outpatient PPS• Ambulatory Payment Classifications (APCs)
– Began effective 8/1/2000
– Prior to 2000, cost reimbursed with adjustments
• Major differences from DRGs
– measuring the payable encounter• inpatient: a single payment for each admission
• outpatient: multiple payments possible for each visit
– assigning the encounter to a payment group• inpatient: principal diagnosis
• outpatient: procedure codes
Outpatient PPS (continued)
• Current APC structure - number of APCssignificant procedures 217
other payable procedures 118
ancillary tests 41
visits 8
drugs and devices 174
• Excluded from APCs, paid under separate fee scheduleclinical laboratory
rehab therapy
renal dialysis
orthotics and prosthetics

Outpatient PPS (continued)
• Payment– Each APC assigned a relative weight
– CMS sets a national conversion factor, adjusted for area wage index
– Adjusted conversion factor x weight = payment
– Outlier payments may be available (not lucrative)
– No provision for IME, DSH
• Packaged services (bundling) - not separately paid– most drugs and devices
– medical supplies
– anesthesia, recovery
– observation, with some exceptions
– procedures deemed to be incidental (ex: pulse oximetry)
Outpatient PPS (continued)
Examples - APC Rates mid-level clinic visit $53.88
high-level ER visit 241.37
cataract procedure w/ IOL 1,236.48
level I endoscopy, upper airway 51.18
level III endoscopy, upper airway 177.79
electrocardiogram 20.47
level I plain film except teeth 42.56
CT scan with contrast material 250.53
chemotherapy by infusion 200.42
level 1 radiation therapy 87.82
cochlear implant 20,442.02
Outpatient PPS (continued)
• Special payment rules– surgical discounting: if more than one procedure is performed during a
visit, the most expensive procedure paid 100%, others paid 50%
– drugs:• in initial years of APCs, cancer drugs and several other higher-cost drugs were
paid separately
• beginning on 1/1/03, many cancer drugs are now packaged into the infusion payment and the payment for higher-cost drugs was reduced
– devices:• the OPPS legislation provided that expensive devices receiving FDA approval
within three years would be paid separately.
• Initially, there were hundreds of these devices, now a handful
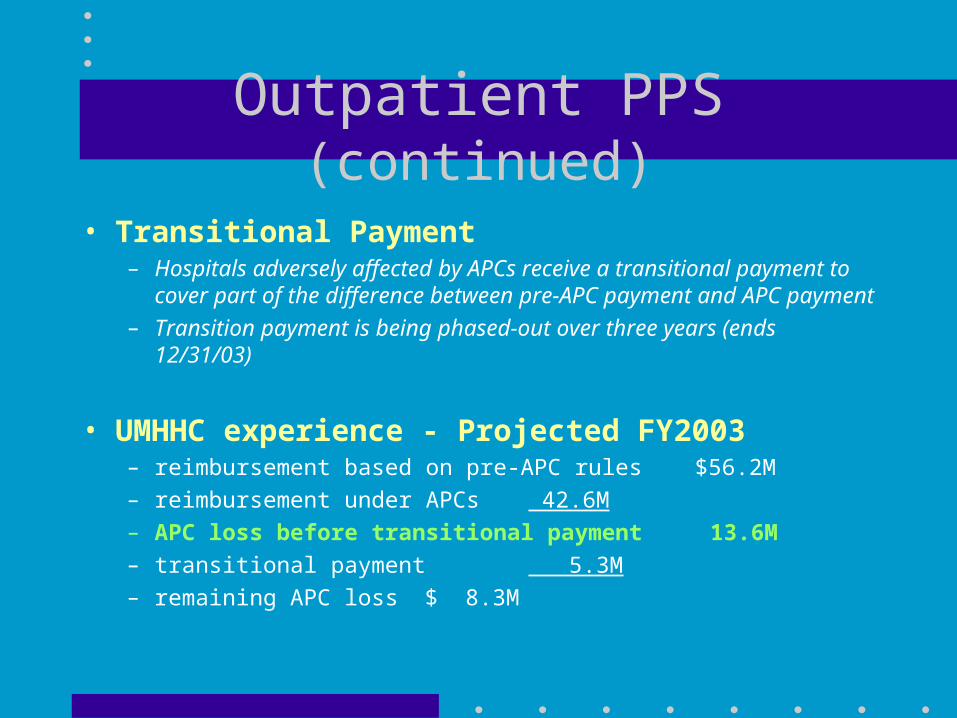
Outpatient PPS (continued)
• Transitional Payment– Hospitals adversely affected by APCs receive a transitional payment to
cover part of the difference between pre-APC payment and APC payment
– Transition payment is being phased-out over three years (ends 12/31/03)
• UMHHC experience - Projected FY2003– reimbursement based on pre-APC rules $56.2M
– reimbursement under APCs 42.6M
– APC loss before transitional payment 13.6M
– transitional payment 5.3M
– remaining APC loss $ 8.3M
HOPD Status• To qualify for APCs, sites must be designated as hospital-
based outpatient departments (HOPD)
• Criteria and requirements for HOPD status: – Must be under common ownership and control
– Integrated financial operations, clinical services, medical records, admin
– Medical staff at site have privileges at the hospital
– Must hold itself out to the public as part of the hospital
– Cannot be more than 35 miles from the main campus
– Must meet federal EMTALA, anti-dumping, non-discrimination rules
• All but a handful of UMHS sites are HOPD

Other Outpatient
• Clinical laboratory - Medicare fee schedule
• Rehab therapy - Medicare fee schedule
• Renal dialysis - composite rate per visit
• Common features– no differentiation between hospital based and independents
– no differentiation based on teaching status or other factors
Settlements
• Many elements of hospital reimbursement are based on aggregate data covering the full fiscal year– Resident counts for IME and Direct GME
– Medicaid-eligible patient days for DSH
– Cost data for organ acquisition and outpatient transitional payment
A retrospective settlement is required
• Hospitals receive cash via biweekly interim payments
• Settled to “actual” after year-end
Settlements (continued)
• Settlement Process and typical timeline– Hospital year-end 6/30/02
– Cost report submitted 11/30/02
– Tentative settlement by intermediary 3/31/03
– Audit by intermediary and final settlement 9/30/04
– Appeal filed by hospital if necessary 3/31/05
– Appeal settled if possible 9/30/06
– Legal proceedings if necessary ???
Medicare Policy-Broad Issues
• How large can Medicare grow?– current federal deficits
– cost trend in health care
– aging of the population
• Competing priorities - distributing federal dollars– prescription drug benefit
– funding for the uninsured and underinsured
– between provider types - hospital vs physician vs home health vs ...
– within the hospital line:• urban vs rural
• teaching vs non-teaching
Medicare Policy-UM Issues
• Concerns– GME funding, especially IME (IME rates are “inherently too high”)
– Pressure to eliminate rate differentiation
• HOPD versus freestanding counterparts
• Disparities between hospitals
– Area wage adjustment and occupational mix
• Opportunities– Inpatient severity of illness adjustments
– IME-type adjustment for outpatient
– Rebasing GME caps on resident FTEs
– Additional payment for new technology
Resources
• HHC Reimbursement– Department number: 647-3321
– Director: Tom Marks, 6-7990 ([email protected])
• Centers for Medicare and Medicaid Services (CMS)– Website: http://cms.hhs.gov
– Provider data: http://cms.hhs.gov/providers/• recent regulations
• statistics
• public use files
– Other data: links to beneficiary and coverage information, publications by the Agency, Medicare manuals, research, statistics and more
Questions ???