medication administration policy
TRANSCRIPT
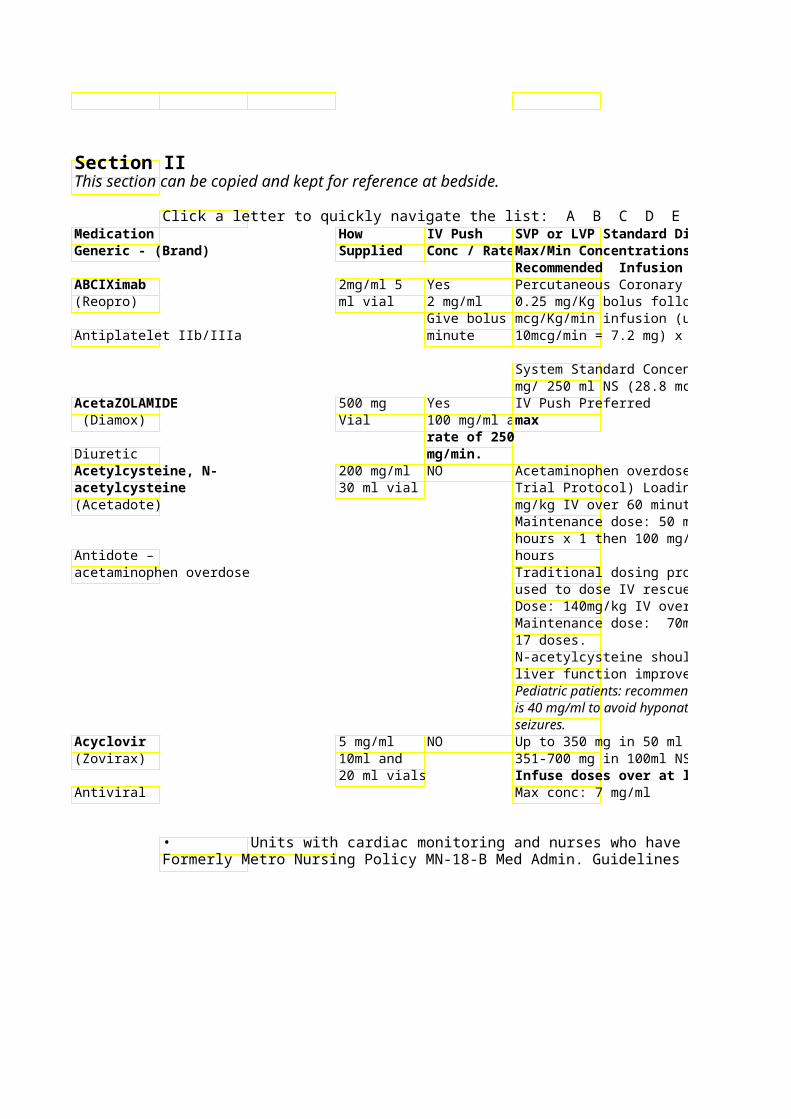
Section IIThis section can be copied and kept for reference at bedside.
Click a letter to quickly navigate the list: A B C D E F G H I J K L M N O P Q R S T U V W X Y Z Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / RateMax/Min Concentrations
Recommended Infusion Time ABCIXimab 2mg/ml 5 Yes Percutaneous Coronary Intervention: (Reopro) ml vial 2 mg/ml 0.25 mg/Kg bolus followed by 0.125
Give bolus omcg/Kg/min infusion (up to max Antiplatelet IIb/IIIa minute 10mcg/min = 7.2 mg) x 12 hours
System Standard Concentration: 7.2 mg/ 250 ml NS (28.8 mcg/ml)
AcetaZOLAMIDE 500 mg Yes IV Push Preferred (Diamox) Vial 100 mg/ml amax
rate of 250 Diuretic mg/min.Acetylcysteine, N- 200 mg/ml NO Acetaminophen overdose: (Prescott acetylcysteine 30 ml vial Trial Protocol) Loading dose: 150 (Acetadote) mg/kg IV over 60 minutes
Maintenance dose: 50 mg/kg IV over 4 hours x 1 then 100 mg/kg IV over 16
Antidote – hours acetaminophen overdose Traditional dosing protocol may be
used to dose IV rescue – Loading Dose: 140mg/kg IV over 60minutes; Maintenance dose: 70mg/kg IV Q4h x 17 doses. N-acetylcysteine should continue until liver function improves!! Pediatric patients: recommended conc is 40 mg/ml to avoid hyponatremia and seizures.
Acyclovir 5 mg/ml NO Up to 350 mg in 50 ml NS or D5W (Zovirax) 10ml and 351-700 mg in 100ml NS or D5W
20 ml vials Infuse doses over at least 60 min. Antiviral Max conc: 7 mg/ml
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Click a letter to quickly navigate the list: A B C D E F G H I J K L M N O P Q R S T U V W X Y Z SVP or LVP Standard Diluent Precautions / Comments Stability / Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Percutaneous Coronary Intervention: Preprinted order set available Do not shake solution or 0.25 mg/Kg bolus followed by 0.125 transport via tube system. mcg/Kg/min infusion (up to max Monitor Hgb/Hct, platelets, PT, PTT 10mcg/min = 7.2 mg) x 12 hours 6 hours after admin and 24 hrs afterAdminister in separate IV line
administration System Standard Concentration: 7.2 0.22 micron filter must be used mg/ 250 ml NS (28.8 mcg/ml) in preparation!!
** Verify dose to be given. Discard vial after drawing up correct dose. **Reconstitutesterile
water only.May cause thrombophlebitis
Acetaminophen overdose: (Prescott Caution with use in patients with Trial Protocol) Loading dose: 150 asthma and/or history of Administer in separate IV line mg/kg IV over 60 minutes bronchospasm Maintenance dose: 50 mg/kg IV over 4 Solution may turn hours x 1 then 100 mg/kg IV over 16 Common adverse effects: rash, pink/lavender in color – still ok
urticaria and pruritus to use Traditional dosing protocol may be used to dose IV rescue – Loading Urticaria and pruritus may be treated Dose: 140mg/kg IV over 60minutes; with antihistamine (i.e. Maintenance dose: 70mg/kg IV Q4h x diphenhydramine) with physician
order. N-acetylcysteine should continue until liver function improves!! Pediatric patients: recommended conc is 40 mg/ml to avoid hyponatremia and
Up to 350 mg in 50 ml NS or D5W Renal tubular damage with infusionsDo NOT refrigerate – 351-700 mg in 100ml NS or D5W <60min. precipitate may form. Infuse doses over at least 60 min. Phlebitis if conc.>7mg/ml
Dose reduction recommended for CrCl < 50 ml/min
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Do not shake solution or transport via tube system.
Administer in separate IV line
0.22 micron filter must be used
Administer in separate IV line
pink/lavender in color – still ok
1
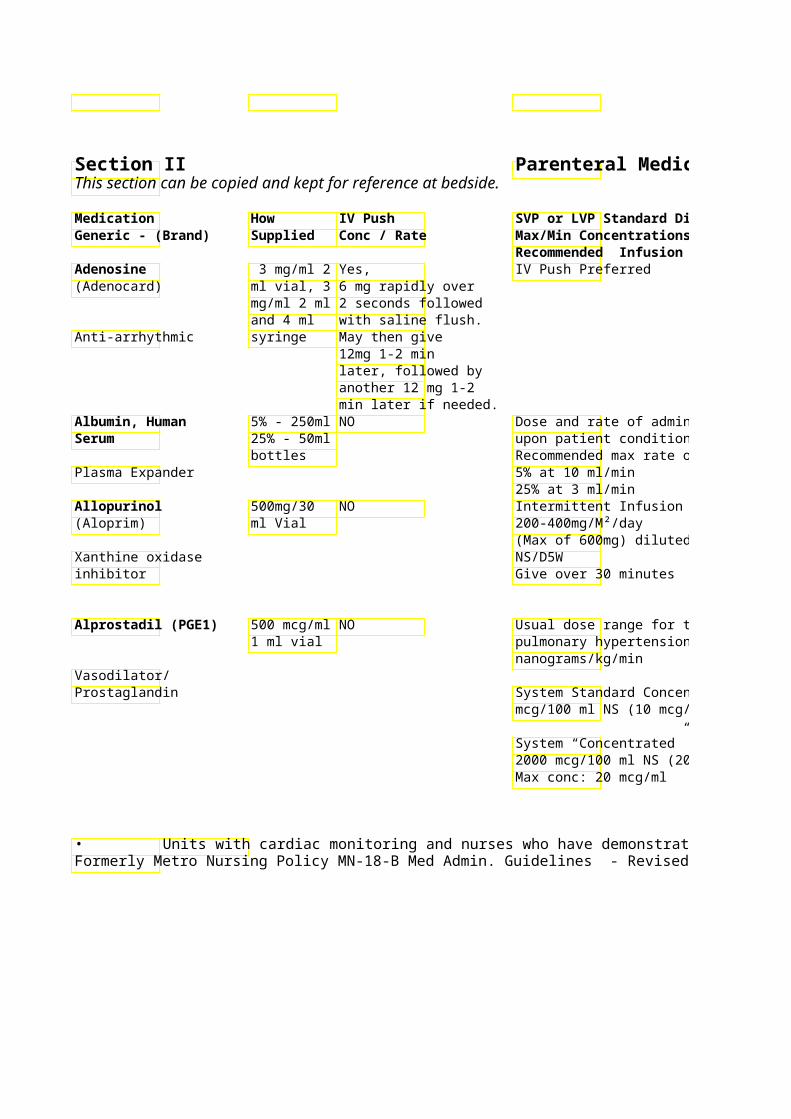
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Adenosine 3 mg/ml 2 Yes, IV Push Preferred (Adenocard) ml vial, 3 6 mg rapidly over
mg/ml 2 ml 2 seconds followed and 4 ml with saline flush.
Anti-arrhythmic syringe May then give 12mg 1-2 min later, followed by another 12 mg 1-2 min later if needed.
Albumin, Human 5% - 250ml NO Dose and rate of adminisSerum 25% - 50ml upon patient condition.
bottles Recommended max rate of infusion: Plasma Expander 5% at 10 ml/min
25% at 3 ml/min Allopurinol 500mg/30 NO Intermittent Infusion – (Aloprim) ml Vial 200-400mg/M²/day
(Max of 600mg) diluted Xanthine oxidase NS/D5W inhibitor Give over 30 minutes
Alprostadil (PGE1) 500 mcg/ml NO Usual dose range for tre1 ml vial pulmonary hypertension:
nanograms/kg/min Vasodilator/ Prostaglandin System Standard Concent
mcg/100 ml NS (10 mcg/
System “Concentrated” Concentration: 2000 mcg/100 ml NS (20Max conc: 20 mcg/ml
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
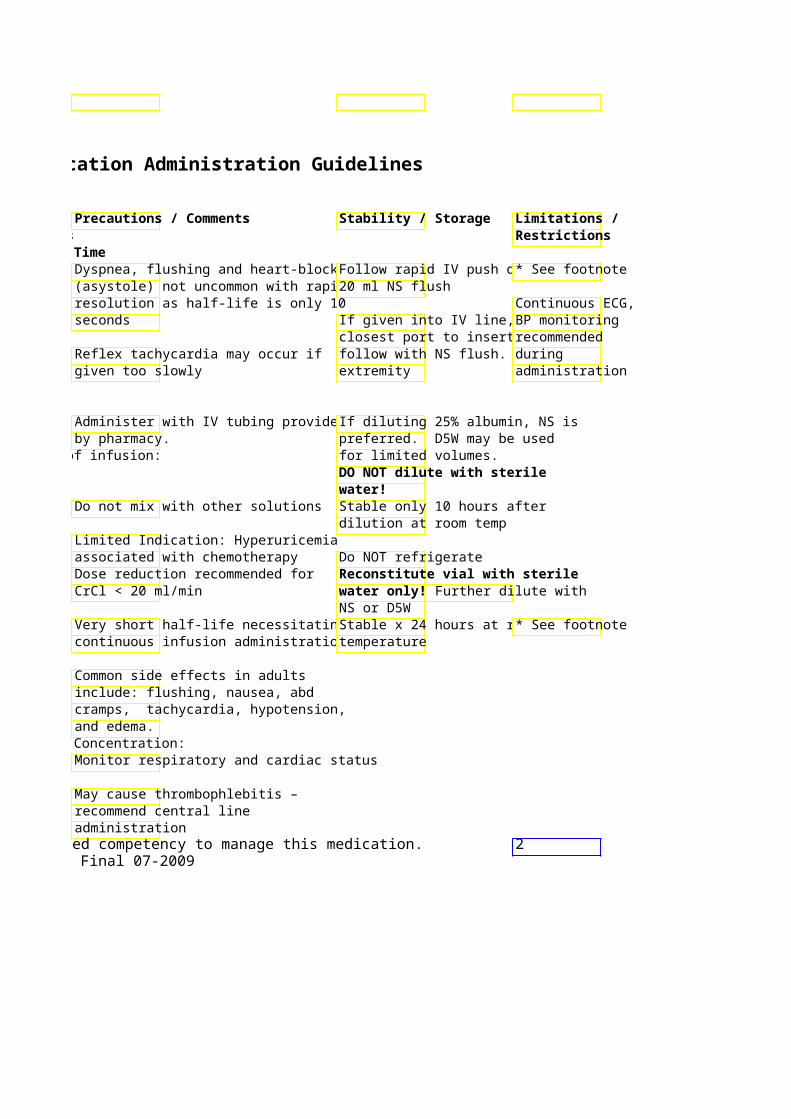
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Dyspnea, flushing and heart-block Follow rapid IV push dos* See footnote (asystole) not uncommon with rapid 20 ml NS flush resolution as half-life is only 10 Continuous ECG, seconds If given into IV line, use BP monitoring
closest port to insertion recommended Reflex tachycardia may occur if follow with NS flush. Ele during given too slowly extremity administration
Administer with IV tubing provided If diluting 25% albumin, NS is by pharmacy. preferred. D5W may be used
Recommended max rate of infusion: for limited volumes. DO NOT dilute with sterile water!
Do not mix with other solutions Stable only 10 hours after dilution at room temp
Limited Indication: Hyperuricemia associated with chemotherapy Do NOT refrigerate Dose reduction recommended for Reconstitute vial with sterile CrCl < 20 ml/min water only Further dilute with
NS or D5W Very short half-life necessitating Stable x 24 hours at roo * See footnote continuous infusion administration temperature
Common side effects in adults include: flushing, nausea, abd cramps, tachycardia, hypotension, and edema.
System “Concentrated” Concentration: Monitor respiratory and cardiac status
May cause thrombophlebitis – recommend central line administration
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 2Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
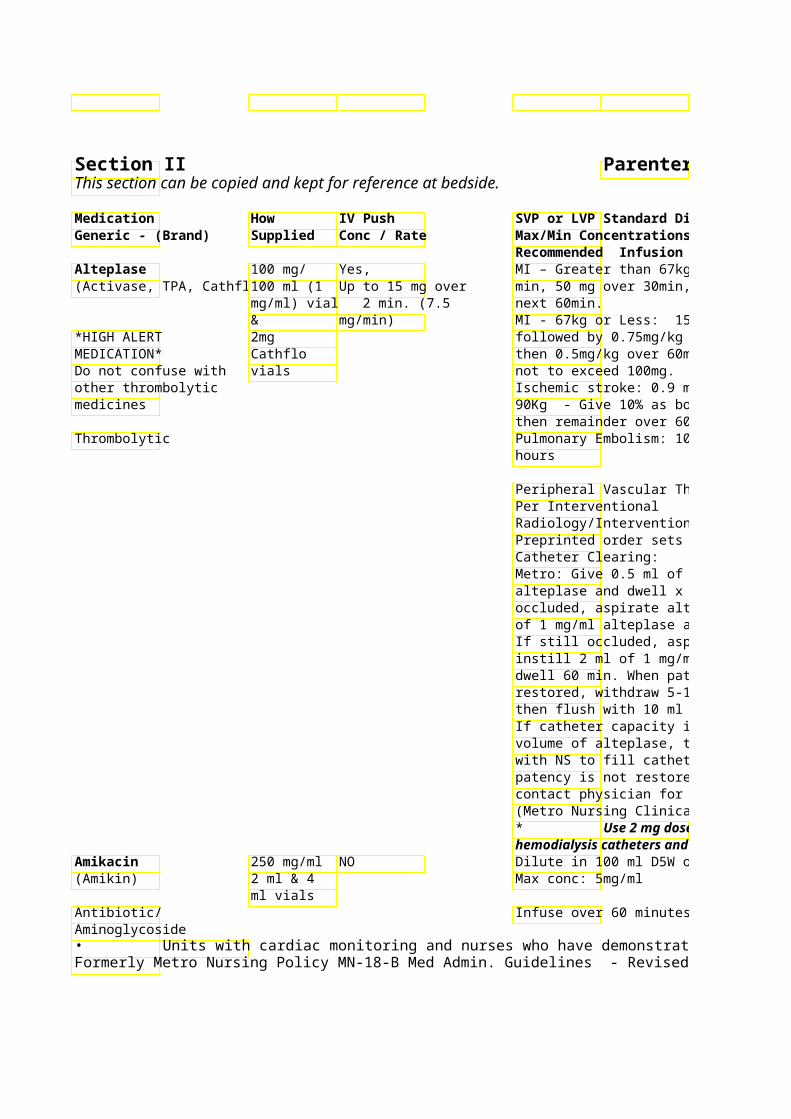
Recommended Infusion Time Alteplase 100 mg/ Yes, MI – Greater than 67kg:(Activase, TPA, Cathflo) 100 ml (1 Up to 15 mg over min, 50 mg over 30min,
mg/ml) vial 2 min. (7.5 next 60min. & mg/min) MI - 67kg or Less: 15mg
*HIGH ALERT 2mg followed by 0.75mg/kg oMEDICATION* Cathflo then 0.5mg/kg over 60miDo not confuse with vials not to exceed 100mg. other thrombolytic Ischemic stroke: 0.9 mgmedicines 90Kg - Give 10% as bolus over 1min,
then remainder over 60mThrombolytic Pulmonary Embolism: 10
hours
Peripheral Vascular ThroPer Interventional Radiology/InterventionalPreprinted order sets avaCatheter Clearing: Metro: Give 0.5 ml of 1 mg/ml alteplase and dwell x 60 min. If still occluded, aspirate alteplase, instill 1 ml of 1 mg/ml alteplase and dwell 60 min. If still occluded, aspirate alteplase, instill 2 ml of 1 mg/ml alteplase and dwell 60 min. When patency is restored, withdraw 5-10 ml and discard then flush with 10 ml NS. If catheter capacity is greater than volume of alteplase, then follow dose with NS to fill catheter volume. If patency is not restored after 2 ml dose, contact physician for further orders. (Metro Nursing Clinical Policy MN-11) * Use 2 mg dose initially for hemodialysis catheter
Amikacin 250 mg/ml NO Dilute in 100 ml D5W or (Amikin) 2 ml & 4 Max conc: 5mg/ml
ml vials Antibiotic/ Infuse over 60 minutes Aminoglycoside • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
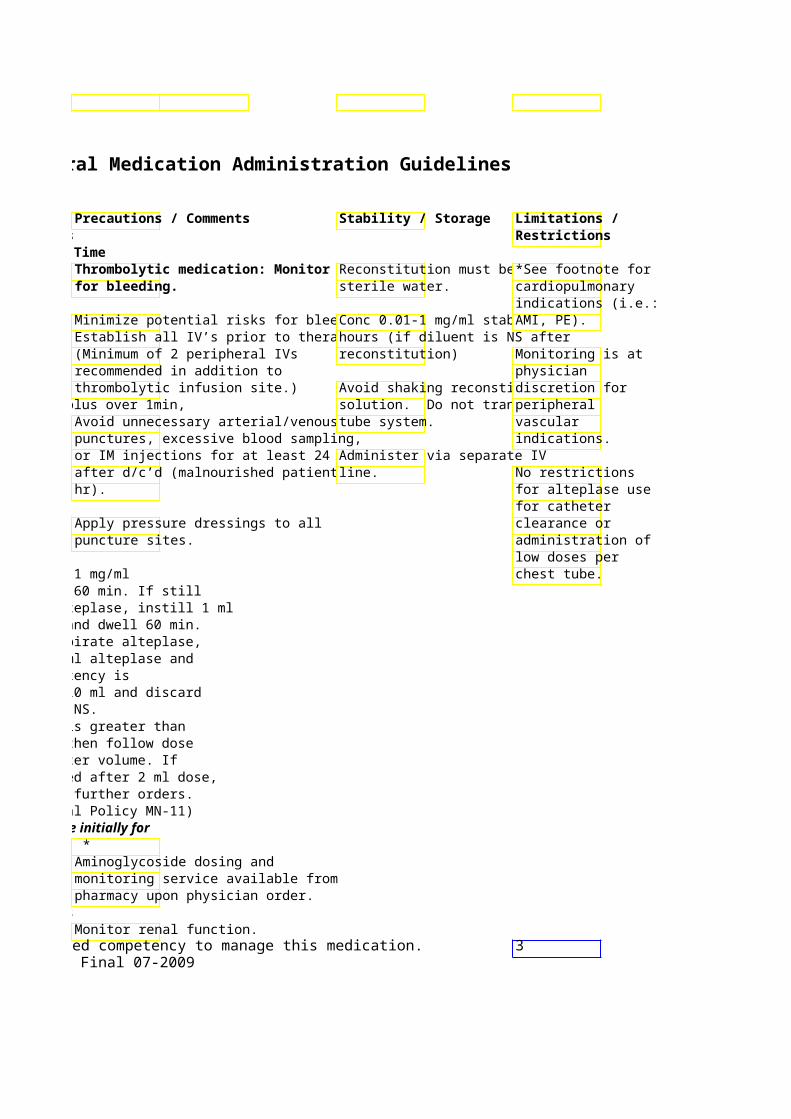
Thrombolytic medication: MonitoReconstitution must be w*See footnote for for bleeding. sterile water. cardiopulmonary
indications (i.e.: Minimize potential risks for bleeding:Conc 0.01-1 mg/ml stablAMI, PE). Establish all IV’s prior to therapy. hours (if diluent is NS after (Minimum of 2 peripheral IVs reconstitution) Monitoring is at recommended in addition to physician thrombolytic infusion site.) Avoid shaking reconstitudiscretion for
90Kg - Give 10% as bolus over 1min, solution. Do not transpoperipheral Avoid unnecessary arterial/venous tube system. vascular punctures, excessive blood sampling, indications. or IM injections for at least 24 hr Administer via separate IV after d/c’d (malnourished patients 4 line. No restrictions hr). for alteplase use
for catheter Apply pressure dressings to all clearance or puncture sites. administration of
low doses per Metro: Give 0.5 ml of 1 mg/ml chest tube. alteplase and dwell x 60 min. If still occluded, aspirate alteplase, instill 1 ml of 1 mg/ml alteplase and dwell 60 min. If still occluded, aspirate alteplase, instill 2 ml of 1 mg/ml alteplase and dwell 60 min. When patency is restored, withdraw 5-10 ml and discard then flush with 10 ml NS. If catheter capacity is greater than volume of alteplase, then follow dose with NS to fill catheter volume. If patency is not restored after 2 ml dose, contact physician for further orders. (Metro Nursing Clinical Policy MN-11)
Use 2 mg dose initially for *Aminoglycoside dosing and monitoring service available from pharmacy upon physician order.
Monitor renal function. Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 3
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
MedicationHow IV Push SVP or LVP Standard Diluent Generic - ( Supplied Conc / Rate Max/Min Concentrations
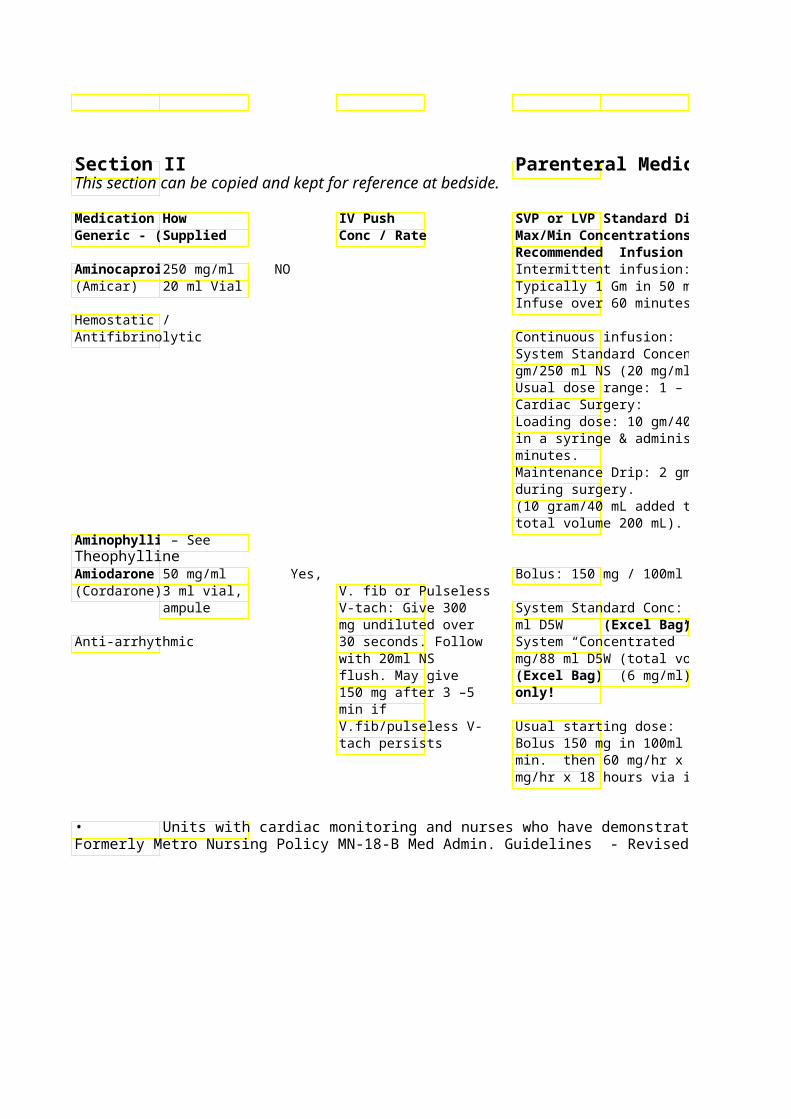
Recommended Infusion Time Aminocapro250 mg/ml NO Intermittent infusion: (Amicar) 20 ml Vial Typically 1 Gm in 50 ml NS/D5W
Infuse over 60 minutes. Hemostatic / Antifibrinolytic Continuous infusion:
System Standard Concentration: 5 gm/250 ml NS (20 mg/ml) Usual dose range: 1 – 1.25 Gm/hr Cardiac Surgery: Loading dose: 10 gm/40 mL drawn up in a syringe & administered IV over 20 minutes. Maintenance Drip: 2 gm/hr (40mL/hr) during surgery. (10 gram/40 mL added to 150mL NS; total volume 200 mL).
Aminophyll – See Theophylline Amiodaron50 mg/ml Yes, Bolus: 150 mg / 100ml D5W (PVC) (Cordarone)3 ml vial, V. fib or Pulseless
ampule V-tach: Give 300 System Standard Conc: 450 mg / 250 mg undiluted over ml D5W (Excel Bag)
Anti-arrhythmic 30 seconds. Follow System “Concentrated” conc: 600 with 20ml NS mg/88 ml D5W (total volume 100 ml)flush. May give (Excel Bag (6 mg/ml) 150 mg after 3 –5 only! min if V.fib/pulseless V- Usual starting dose: tach persists Bolus 150 mg in 100ml D5W over 10
min. then 60 mg/hr x 6 hours then 3mg/hr x 18 hours via infusion.
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Max/Min Concentrations Recommended Infusion Time
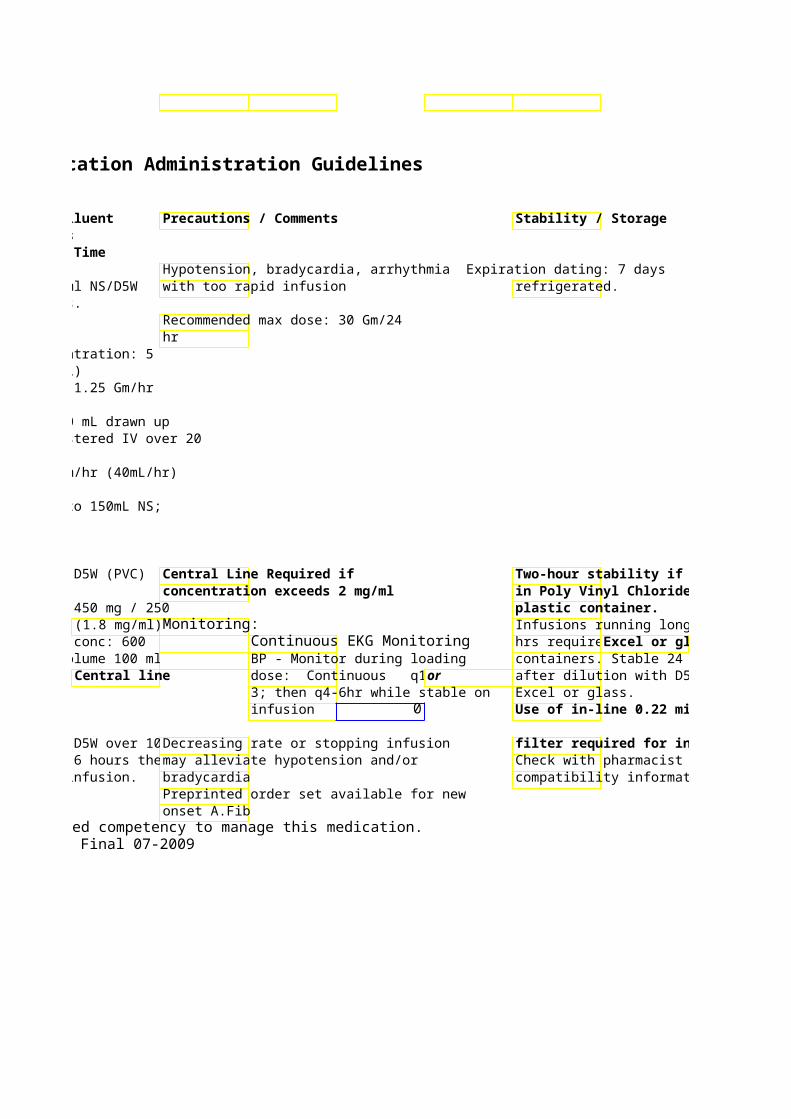
Hypotension, bradycardia, arrhythmia Expiration dating: 7 days Typically 1 Gm in 50 ml NS/D5W with too rapid infusion refrigerated. Infuse over 60 minutes.
Recommended max dose: 30 Gm/24 hr
System Standard Concentration: 5 gm/250 ml NS (20 mg/ml) Usual dose range: 1 – 1.25 Gm/hr
Loading dose: 10 gm/40 mL drawn up in a syringe & administered IV over 20
Maintenance Drip: 2 gm/hr (40mL/hr)
(10 gram/40 mL added to 150mL NS;
Bolus: 150 mg / 100ml D5W (PVC) Central Line Required if Two-hour stability if concentration exceeds 2 mg/ml in Poly Vinyl Chloride (PVC)
System Standard Conc: 450 mg / 250 plastic container. (1.8 mg/ml) Monitoring: Infusions running longer than 2
System “Concentrated” conc: 600 Continuous EKG Monitoring hrs require Excel or glassmg/88 ml D5W (total volume 100 ml) BP - Monitor during loading containers. Stable 24 hours
Central line dose: Continuous q15 or after dilution with D5W in 3; then q4-6hr while stable on Excel or glass. infusion 0 Use of in-line 0.22 micron
Bolus 150 mg in 100ml D5W over 10Decreasing rate or stopping infusion filter required for infusions. min. then 60 mg/hr x 6 hours then 3may alleviate hypotension and/or Check with pharmacist for mg/hr x 18 hours via infusion. bradycardia compatibility information.
Preprinted order set available for new onset A.Fib
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
* See footnote in Poly Vinyl Chloride (PVC)
Infusions running longer than 2 Excel or glass
containers. Stable 24 hours after dilution with D5W in
Use of in-line 0.22 micron
filter required for infusions. Check with pharmacist for compatibility information.
4
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Amphotericin B 50 mg and NO Optional Test dose: 0.1 mg/kg up to 1 (Fungizone) 100 mg mg in 50 ml
vials min
Anti-fungal Doses < 25 mg/250 ml 26-50 mg/500 ml Infuse over 3 hours
Amphotericin B Lipid 100 mg vial NO 3 - 5mg / Kg / Day typical dose Complex (Abelcet) Dilute with D5W
concentration of 2 mg / ml. Anti-fungal Infuse over 2 hours
Amphotericin B 50 mg Vial NO 3 – 5 mg/Kg/Day typical dose Liposomal Dilute with D5W(AmBisome) concentration of 1-2 mg/ml
Infuse over 2 hours Anti-fungal
Ampicillin 0.5, 1 & 2 NO Up to 1 Gm 50ml NS Gm Vial 2Gm 100ml NS
Antibiotic/ Beta-lactam Infuse dose over 30 min • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication.

Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Max/Min Concentrations Recommended Infusion Time Optional Test dose: 0.1 mg/kg up to 1 Test Dose no longer considered Use
D5W . Infuse ove necessary & no longer recommended. Protect from light.
Monitoring: VS q15 min x 1 hr then Do NOT filter D5W q 1 hr for at least 1 hr post-infusion. D5W
Administer any pre-medications 30 Amphotericin may cause renal minutes prior to starting daily wasting of K , Mg , HCO
infusion – Premeds must be per and Na Daily monitoring
physician order. recommended. Recommended pre-medications: Supplementation may be Acetaminophen 500-1000 mg PO or required. 650 mg PR ; Diphenhydramine 25-50 mg PO/IV ; Hydrocortisone 25-50 mg IV (use only in pt history of severe rigors) Sodium loading recommended to prevent nephrotoxicity. 500 ml NS before and after infusion. Lower volume (i.e. 250 ml) may be consider in pt with cardiac compromise or develop HTN during NS infusion.
3 - 5mg / Kg / Day typical dose Monitor VS q15 min x 1 hr then q 1 Use to final hr for at least 1 hr post-infusion.
concentration of 2 mg / ml. Gently agitate solution prior to Administer any pre-medications 30 beginning infusion and every 2 minutes prior to starting daily hours. infusion See Amphotericin B for Stable 6 hr at room temp – recommended pre-meds.
3 – 5 mg/Kg/Day typical dose Monitor VS q15 min x 1 hr then q 1 Use to final hr for at least 1 hr post-infusion.
concentration of 1-2 mg/ml Gently agitate solution prior to Administer any pre-medications 30 beginning infusion and every 2 minutes prior to starting daily hours. infusion Stable 6 hrs after dilution at See Amphotericin B for room temp recommended pre-meds. Penicillin derivative – check allergies
Infuse dose over 30 min Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication.

Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Stability / Storage Limitations / Restrictions
D5W only
Protect from light. Do NOT filter
Amphotericin may cause renal wasting of K , Mg , HCO + 2
3 -+
and Na Daily monitoring recommended. Supplementation may be
D5W only
Gently agitate solution prior to beginning infusion and every 2
Stable 6 hr at room temp –
D5W only
Gently agitate solution prior to beginning infusion and every 2
Stable 6 hrs after dilution at room temp
5
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Ampicillin / Sulbacta 1.5 & 3 Gm Not advised <1.5 Gm/50 ml NS (Unasyn) Vial 1.6 to 3 Gm/100 ml NS
(2/3 amp, Infuse dose over 30 minutes Antibiotic/ Beta-lactam 01/03/13
sulbactam) Anidulafungin 50 mg vial Not advised Intermittent infusion: (Eraxis) 50 mg in 100 ml NS or
100 mg in 250 ml NS orAntifungal 200 mg in 500 ml NS or
MAX infusion rate 1.1 mg/minute Anticoagulant Citrate 500 ml NO Dextrose – A bags Not for intravenous (ACD-A) administration. Do NOT infuse
directly into patient. *HIGH ALERT MEDICATION* Continuous infusion with Continuous
Renal Replacement Therapy (CRRT) Anticoagulant and Plasmapheresis
Used as anticoagulant for the machines – not effective as anticoagulant for patient.
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Penicillin derivative – check allergies
Infuse dose over 30 minutes Dose reduction recommended for CrCl < 30 ml/min Histamine-mediated symptoms Reconstitute vials with (rash, urticaria, flushing, prurituaccompanying diluent only dyspnea, and hypotension) possible – infrequent when infusion rate < 1.1 mg/min
MAX infusion rate 1.1 mg/minute May cause hypocalcemia
Not for intravenous administration. Do NOT infuse directly into patient.
Continuous infusion with Continuous Renal Replacement Therapy (CRRT)
Used as anticoagulant for the machines – not effective as anticoagulant for
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 6Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
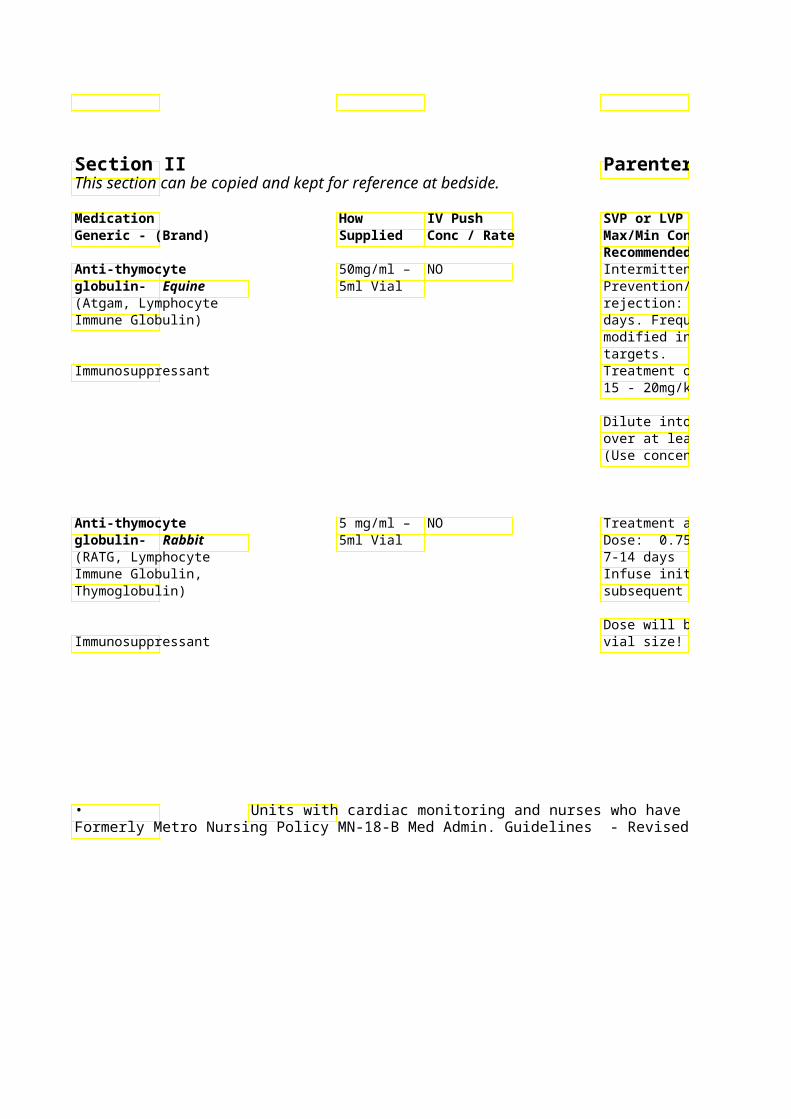
Recommended Infusion Time Anti-thymocyte 50mg/ml – NO Intermittent Infusion – globulin- Equine 5ml Vial Prevention/treatment tra(Atgam, Lymphocyte rejection: 5-15 mg/kg daily for 7-14 Immune Globulin) days. Frequency and dur
modified in response to targets.
Immunosuppressant Treatment of aplastic an15 - 20mg/kg daily for 5
Dilute into 250-1000ml over at least 4 hours (Use concentrations of 4
Anti-thymocyte 5 mg/ml – NO Treatment acute rejectioglobulin- Rabbit 5ml Vial Dose: 0.75mg/kg - 1.5 m(RATG, Lymphocyte 7-14 days Immune Globulin, Infuse initial infusion ovThymoglobulin) subsequent infusions ove
Dose will be rounded to Immunosuppressant vial size!
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
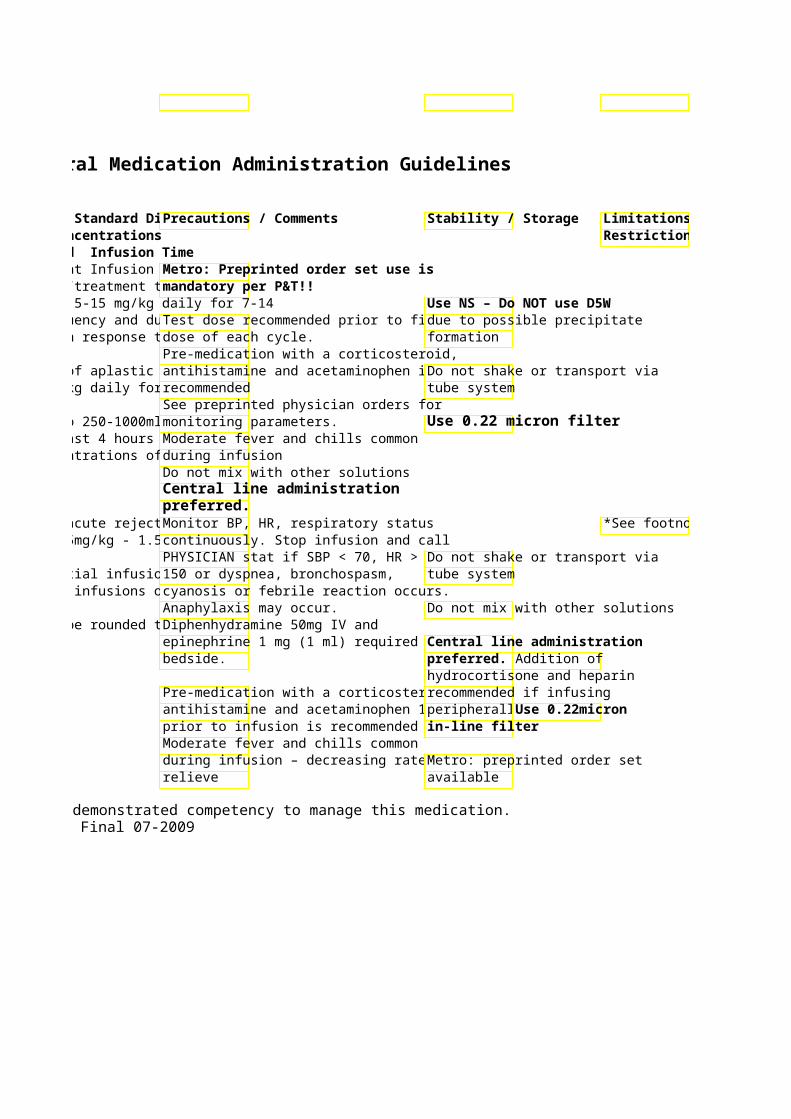
SVP or LVP Standard DPrecautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Intermittent Infusion – Metro: Preprinted order set use is Prevention/treatment tramandatory per P&T!! rejection: 5-15 mg/kg daily for 7-14 Use NS – Do NOT use D5Wdays. Frequency and durTest dose recommended prior to firstdue to possible precipitate modified in response to dose of each cycle. formation
Pre-medication with a corticosteroid, Treatment of aplastic anantihistamine and acetaminophen is Do not shake or transport via 15 - 20mg/kg daily for 5 recommended tube system
See preprinted physician orders for Dilute into 250-1000ml monitoring parameters. Use 0.22 micron filterover at least 4 hours Moderate fever and chills common (Use concentrations of 4during infusion
Do not mix with other solutions Central line administration preferred.
Treatment acute rejectioMonitor BP, HR, respiratory status *See footnote Dose: 0.75mg/kg - 1.5 mcontinuously. Stop infusion and call
PHYSICIAN stat if SBP < 70, HR > Do not shake or transport via Infuse initial infusion ov 150 or dyspnea, bronchospasm, tube system subsequent infusions ovecyanosis or febrile reaction occurs.
Anaphylaxis may occur. Do not mix with other solutions Dose will be rounded to Diphenhydramine 50mg IV and
epinephrine 1 mg (1 ml) required at Central line administration bedside. preferred. Addition of
hydrocortisone and heparin Pre-medication with a corticosteroid,recommended if infusing antihistamine and acetaminophen 1 peripherally.Use 0.22micron prior to infusion is recommended in-line filter Moderate fever and chills common during infusion – decreasing rate maMetro: preprinted order set relieve available
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
*See footnote
7
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
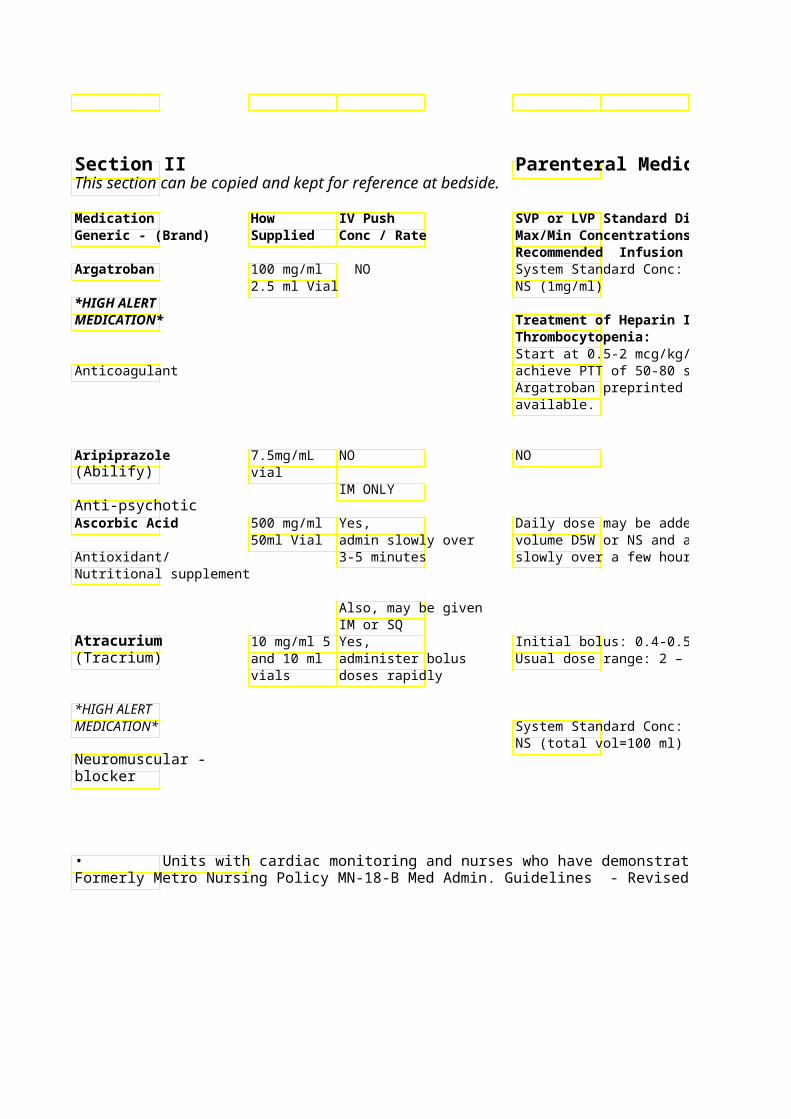
Recommended Infusion Time Argatroban 100 mg/ml NO System Standard Conc:
2.5 ml Vial NS (1mg/ml) *HIGH ALERT MEDICATION* Treatment of Heparin
Thrombocytopenia:Start at 0.5-2 mcg/kg/min
Anticoagulant achieve PTT of 50-80 seArgatroban preprinted oravailable.
Aripiprazole 7.5mg/mL NO NO (Abilify) vial
IM ONLY Anti-psychotic Ascorbic Acid 500 mg/ml Yes, Daily dose may be adde
50ml Vial admin slowly over volume D5W or NS and aAntioxidant/ 3-5 minutes slowly over a few hours Nutritional supplement
Also, may be given IM or SQ
Atracurium 10 mg/ml 5 Yes, Initial bolus: 0.4-0.5 mg/(Tracrium) and 10 ml administer bolus Usual dose range: 2 – 2
vials doses rapidly
*HIGH ALERT MEDICATION* System Standard Conc:
NS (total vol=100 ml) (5 mg/ml) Neuromuscular -blocker
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
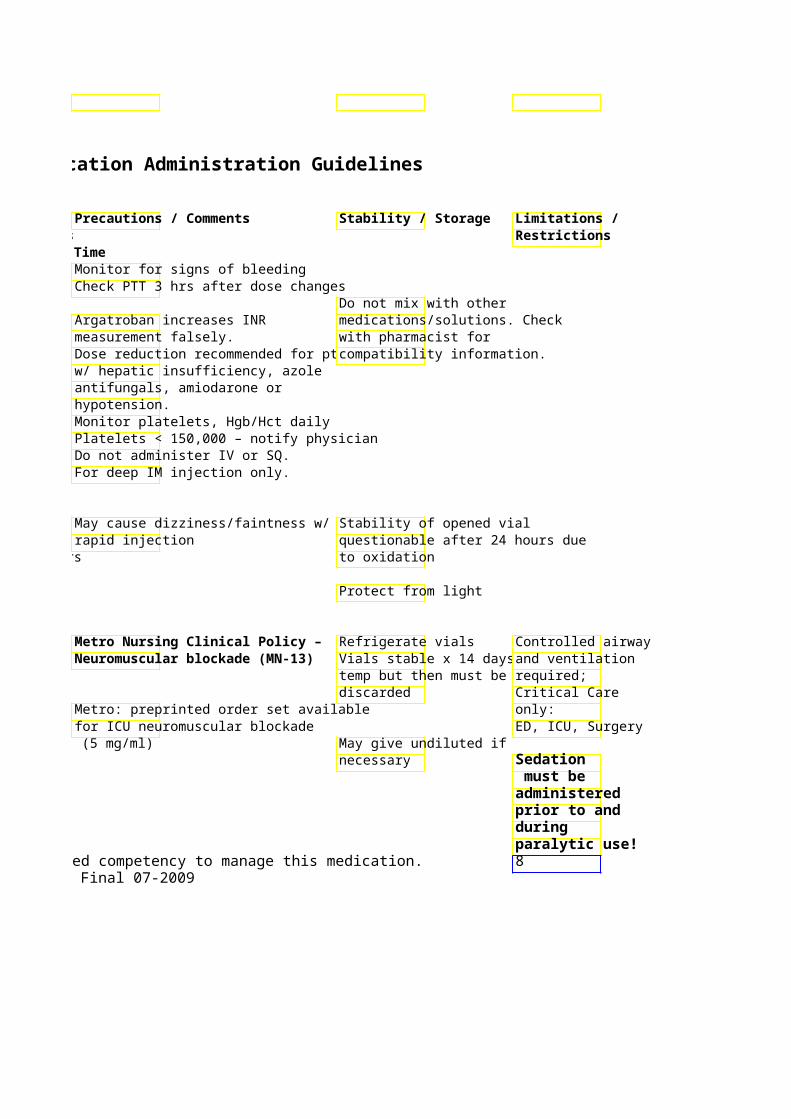
Monitor for signs of bleeding Check PTT 3 hrs after dose changes
Do not mix with other Argatroban increases INR medications/solutions. Check measurement falsely. with pharmacist for Dose reduction recommended for pt compatibility information. w/ hepatic insufficiency, azole antifungals, amiodarone or hypotension. Monitor platelets, Hgb/Hct daily Platelets < 150,000 – notify physician Do not administer IV or SQ. For deep IM injection only.
May cause dizziness/faintness w/ Stability of opened vial rapid injection questionable after 24 hours due
slowly over a few hours to oxidation
Protect from light
Metro Nursing Clinical Policy – Refrigerate vials Controlled airway Neuromuscular blockade (MN-13Vials stable x 14 days a and ventilation
temp but then must be required; discarded Critical Care
Metro: preprinted order set available only: for ICU neuromuscular blockade ED, ICU, Surgery
NS (total vol=100 ml) (5 mg/ml) May give undiluted if necessary Sedation
must be administered prior to and during paralytic use!
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 8Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
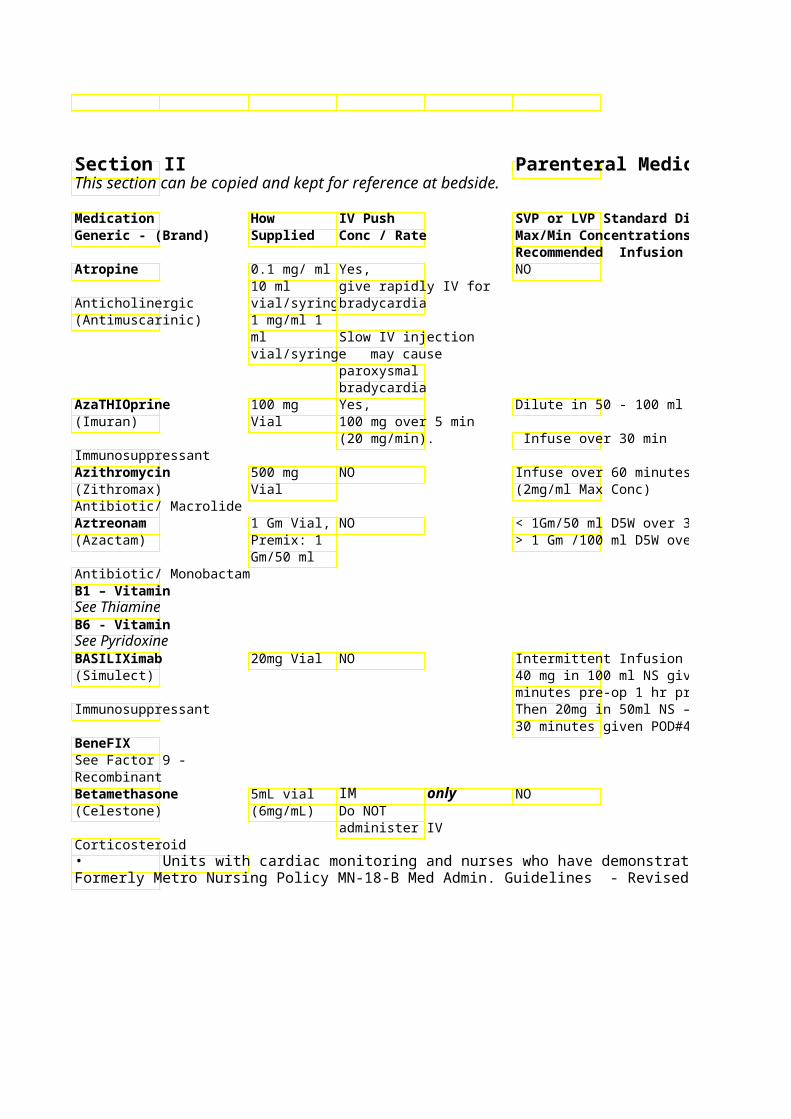
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Atropine 0.1 mg/ ml Yes, NO
10 ml give rapidly IV for Anticholinergic vial/syringe bradycardia (Antimuscarinic) 1 mg/ml 1
ml Slow IV injection vial/syringe may cause
paroxysmal bradycardia
AzaTHIOprine 100 mg Yes, Dilute in 50 - 100 ml NS (Imuran) Vial 100 mg over 5 min
(20 mg/min). Infuse over 30 min Immunosuppressant Azithromycin 500 mg NO Infuse over 60 minutes (Zithromax) Vial (2mg/ml Max Conc) Antibiotic/ Macrolide Aztreonam 1 Gm Vial, NO < 1Gm/50 ml D5W over (Azactam) Premix: 1 > 1 Gm /100 ml D5W ove
Gm/50 ml Antibiotic/ Monobactam B1 – Vitamin See Thiamine B6 - Vitamin See Pyridoxine BASILIXimab 20mg Vial NO Intermittent Infusion – T(Simulect) 40 mg in 100 ml NS give
minutes pre-op 1 hr priorImmunosuppressant Then 20mg in 50ml NS – infuse over
30 minutes given POD#4. BeneFIX See Factor 9 - RecombinantBetamethasone 5mL vial IM only NO (Celestone) (6mg/mL) Do NOT
administer IV Corticosteroid • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
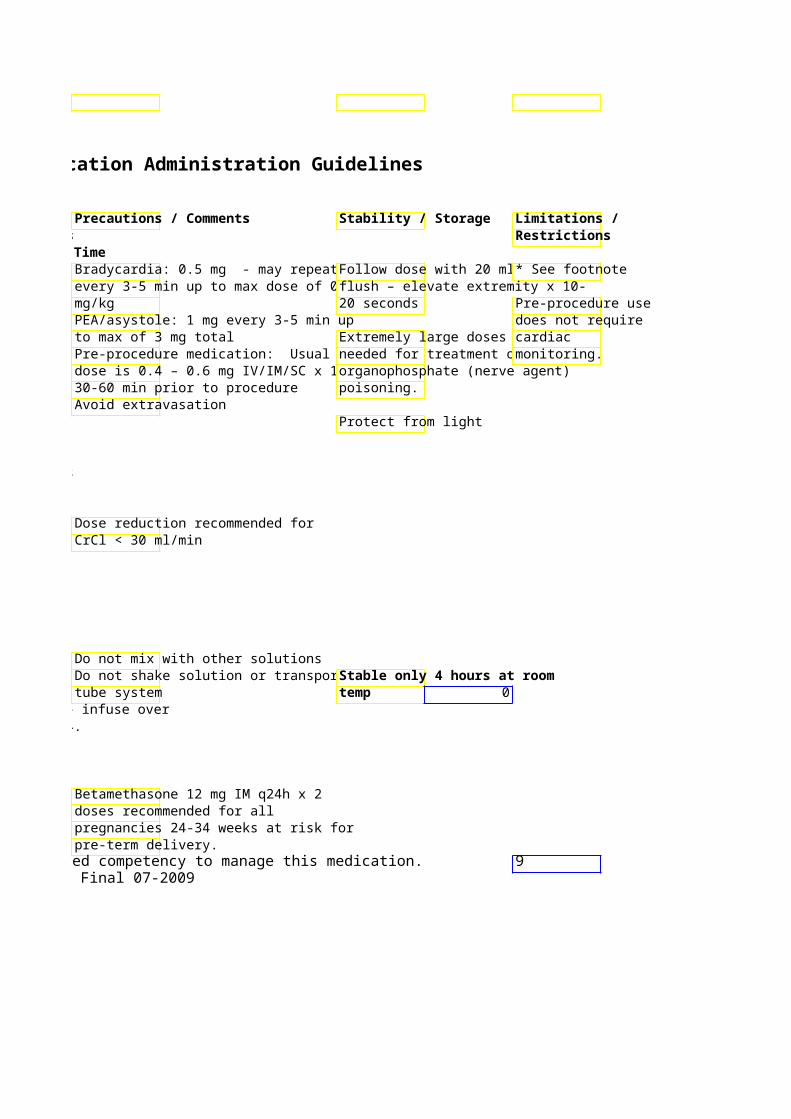
Bradycardia: 0.5 mg - may repeat Follow dose with 20 ml * See footnote every 3-5 min up to max dose of 0.0flush – elevate extremity x 10-mg/kg 20 seconds Pre-procedure use PEA/asystole: 1 mg every 3-5 min up does not require to max of 3 mg total Extremely large doses mcardiac Pre-procedure medication: Usual needed for treatment of monitoring. dose is 0.4 – 0.6 mg IV/IM/SC x 1, organophosphate (nerve agent) 30-60 min prior to procedure poisoning. Avoid extravasation
Protect from light
Dose reduction recommended for CrCl < 30 ml/min
Do not mix with other solutions Do not shake solution or transport viStable only 4 hours at room tube system temp 0
Then 20mg in 50ml NS – infuse over 30 minutes given POD#4.
Betamethasone 12 mg IM q24h x 2 doses recommended for all pregnancies 24-34 weeks at risk for pre-term delivery.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 9Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
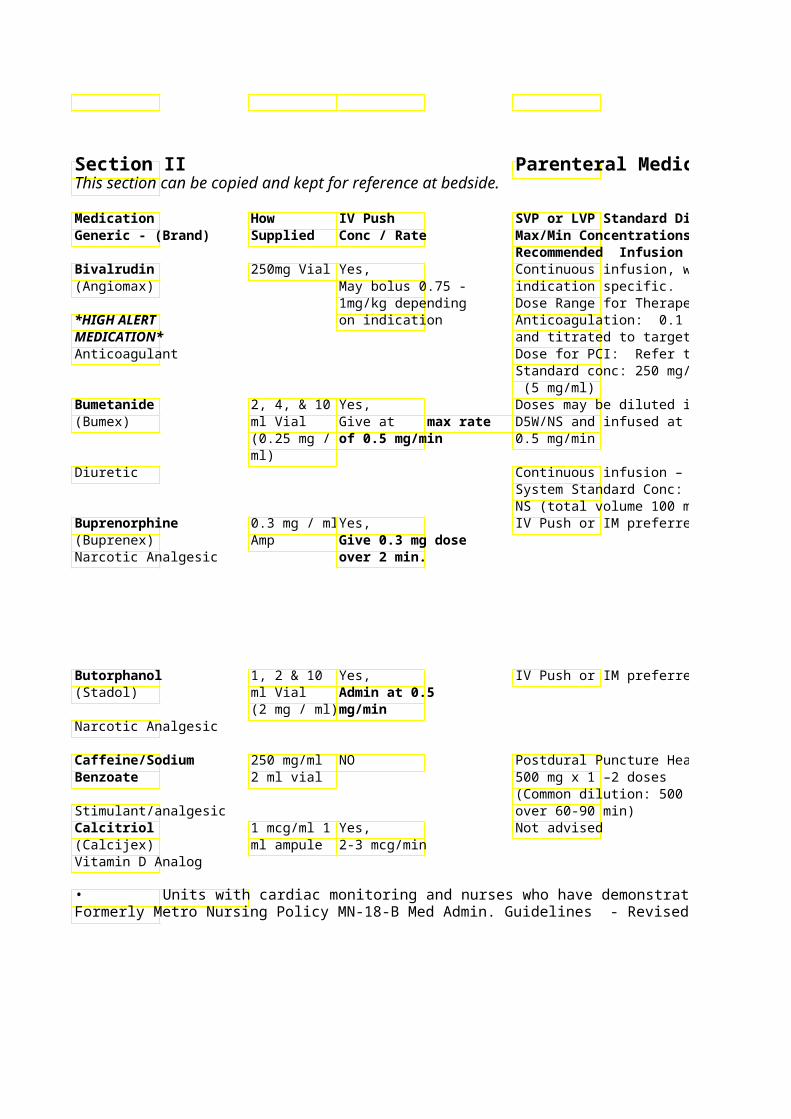
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Bivalrudin 250mg Vial Yes, Continuous infusion, we(Angiomax) May bolus 0.75 - indication specific.
1mg/kg depending Dose Range for Therapeutic *HIGH ALERT on indication Anticoagulation: 0.1 – MEDICATION* and titrated to target PTTAnticoagulant Dose for PCI: Refer to or
Standard conc: 250 mg/ (5 mg/ml)
Bumetanide 2, 4, & 10 Yes, Doses may be diluted in(Bumex) ml Vial Give at max rate D5W/NS and infused at m
(0.25 mg / of 0.5 mg/min 0.5 mg/min ml)
Diuretic Continuous infusion – System Standard Conc: 10 mg/ 60 ml NS (total volume 100 ml) (0.1 mg/ml)
Buprenorphine 0.3 mg / ml Yes, IV Push or IM preferred (Buprenex) Amp Give 0.3 mg dose Narcotic Analgesic over 2 min.
Butorphanol 1, 2 & 10 Yes, IV Push or IM preferred (Stadol) ml Vial Admin at 0.5
(2 mg / ml) mg/min Narcotic Analgesic
Caffeine/Sodium 250 mg/ml NO Postdural Puncture HeadBenzoate 2 ml vial 500 mg x 1 –2 doses
(Common dilution: 500 mg/L. Given Stimulant/analgesic over 60-90 min) Calcitriol 1 mcg/ml 1 Yes, Not advised (Calcijex) ml ampule 2-3 mcg/min Vitamin D Analog
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Dose reduction recommended for CRCL < 30 ml/min
Dose Range for Therapeutic Bleeding risk PTT & ACT affected by bivalrudin Pre-printed order sets for Cath Lab PCI & Therapeutic Anticoagulation in Heparin Allergic Patients High doses have been associated with muscle stiffness and tenderness
Monitor BP/ fluid status
System Standard Conc: 10 mg/ 60 ml NS (total volume 100 ml) (0.1 mg/ml)
Monitor for excess sedation, cardiovascular and respiratory status ** NOTE: Reversal may require higher doses of naloxone** **After naloxone administration - monitor for risk of recurrent respiratory depression. ** May cause withdrawal in opioid / methadone dependent patients. Monitor for excess sedation, cardiovascular and respiratory status
May cause withdrawal in opioid / methadone dependent patients. Monitor BP/HR – may cause Do NOT refrigerate * See footnote hypertension/tachycardia
(Common dilution: 500 mg/L. Given
Used in the treatment of Discard ampule after use. hypocalcemia/secondary hyperparathyroidism in chronic renalStable 8 hr in syringe failure patients.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 10Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
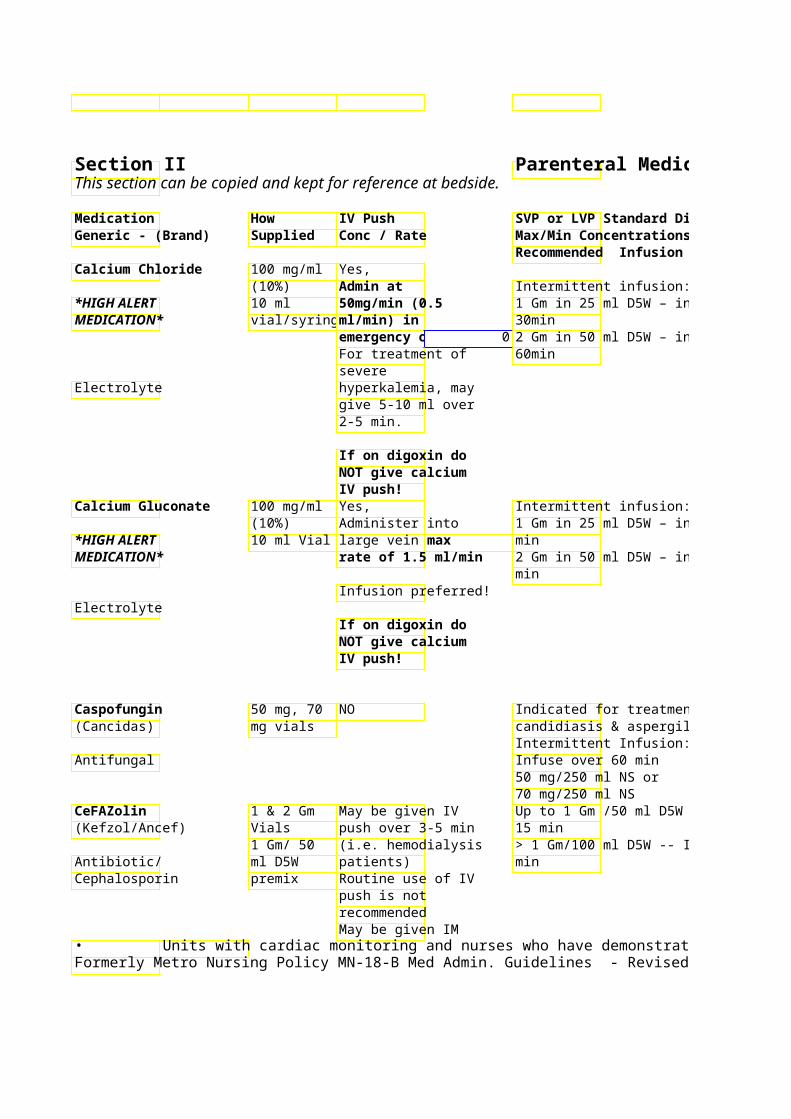
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Calcium Chloride 100 mg/ml Yes,
(10%) Admin at Intermittent infusion: *HIGH ALERT 10 ml 50mg/min (0.5 1 Gm in 25 ml D5W – infuse over MEDICATION* vial/syringe ml/min) in 30min
emergency 0 2 Gm in 50 ml D5W – infuse over For treatment of 60min severe
Electrolyte hyperkalemia, may give 5-10 ml over 2-5 min.
If on digoxin do NOT give calcium IV push!
Calcium Gluconate 100 mg/ml Yes, Intermittent infusion: (10%) Administer into 1 Gm in 25 ml D5W – infuse over 15
*HIGH ALERT 10 ml Vial large vein atmax min MEDICATION* rate of 1.5 ml/min 2 Gm in 50 ml D5W – infuse over 30
min Infusion preferred!
Electrolyte If on digoxin do NOT give calcium IV push!
Caspofungin 50 mg, 70 NO Indicated for treatment of invasive (Cancidas) mg vials candidiasis & aspergillosis
Intermittent Infusion: Antifungal Infuse over 60 min
50 mg/250 ml NS or 70 mg/250 ml NS
CeFAZolin 1 & 2 Gm May be given IV Up to 1 Gm /50 ml D5W -- Infuse ove(Kefzol/Ancef) Vials push over 3-5 min 15 min
1 Gm/ 50 (i.e. hemodialysis > 1 Gm/100 ml D5W -- Infuse over 3Antibiotic/ ml D5W patients) min Cephalosporin premix Routine use of IV
push is not recommended May be given IM
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
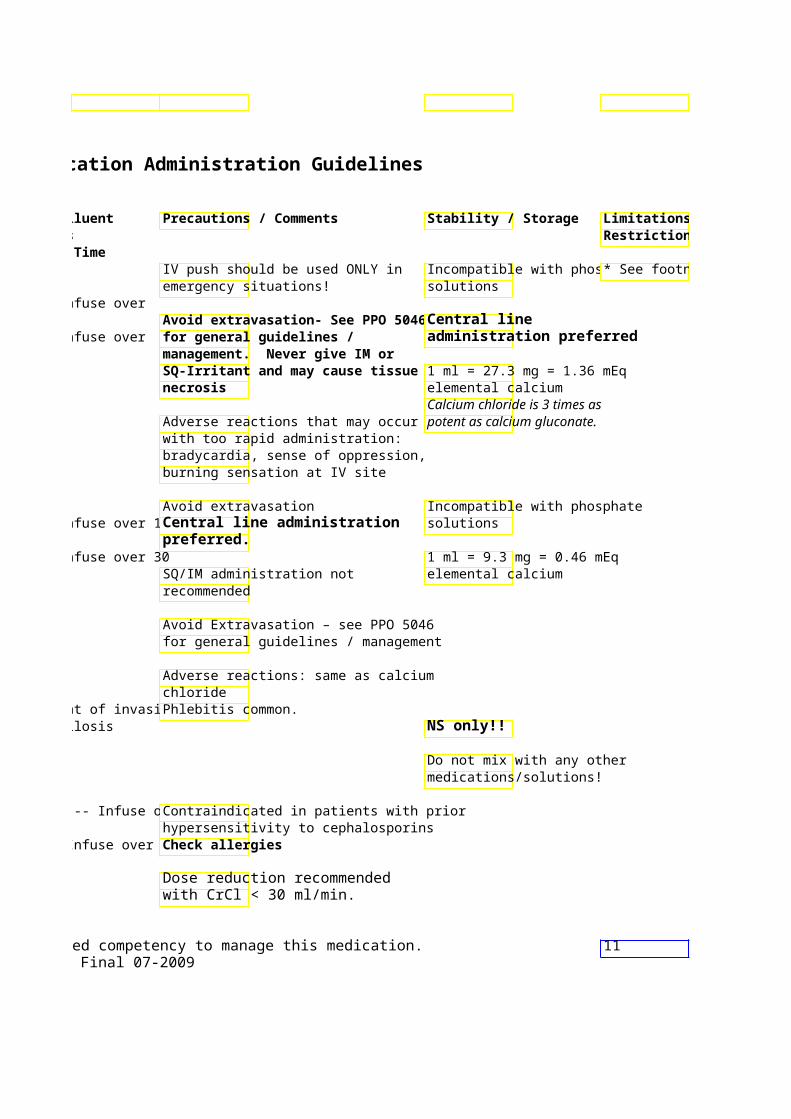
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
IV push should be used ONLY in Incompatible with phosp* See footnote emergency situations! solutions
1 Gm in 25 ml D5W – infuse over Avoid extravasation- See PPO 50Central line
2 Gm in 50 ml D5W – infuse over for general guidelines / administration preferred management. Never give IM or SQ-Irritant and may cause tissue1 ml = 27.3 mg = 1.36 mEq necrosis elemental calcium
Calcium chloride is 3 times as Adverse reactions that may occur potent as calcium gluconate. with too rapid administration: bradycardia, sense of oppression, burning sensation at IV site
Avoid extravasation Incompatible with phosphate 1 Gm in 25 ml D5W – infuse over 15 Central line administration solutions
preferred. 2 Gm in 50 ml D5W – infuse over 30 1 ml = 9.3 mg = 0.46 mEq
SQ/IM administration not elemental calcium recommended
Avoid Extravasation – see PPO 5046 for general guidelines / management
Adverse reactions: same as calcium chloride
Indicated for treatment of invasive Phlebitis common. candidiasis & aspergillosis NS only!!
Do not mix with any other medications/solutions!
Up to 1 Gm /50 ml D5W -- Infuse oveContraindicated in patients with prior hypersensitivity to cephalosporins
> 1 Gm/100 ml D5W -- Infuse over 3Check allergies
Dose reduction recommended with CrCl < 30 ml/min.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 11Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
* See footnote
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
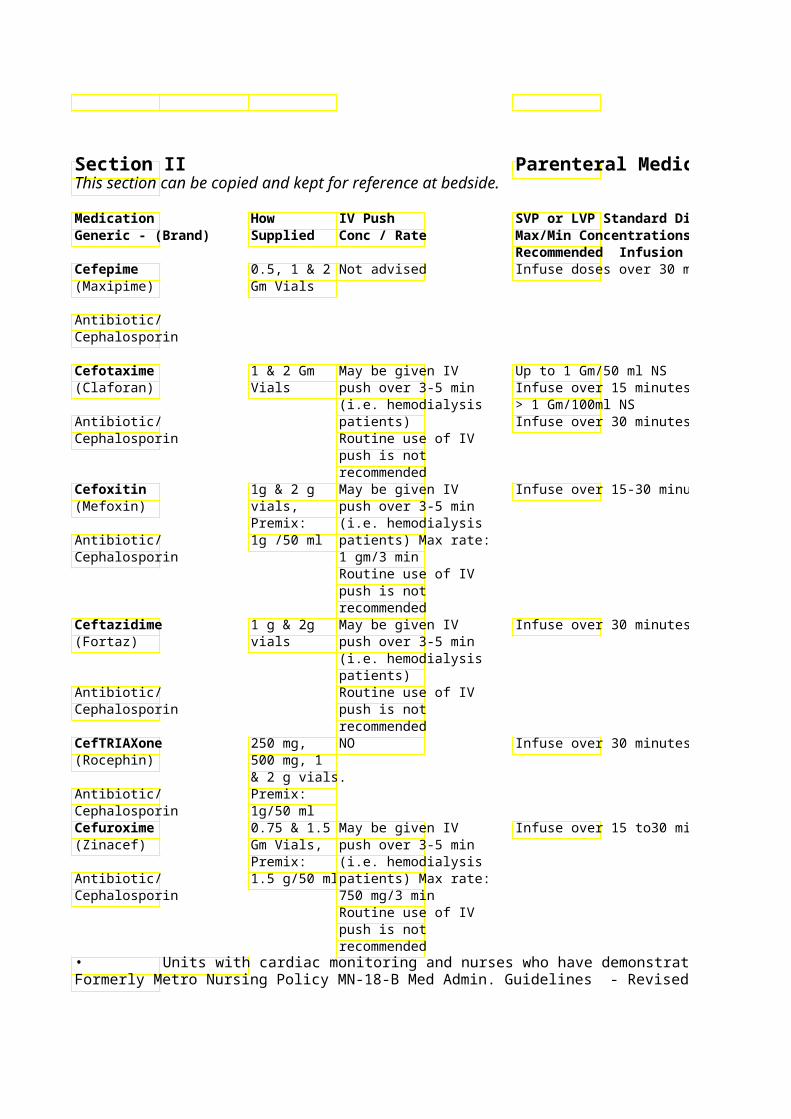
Recommended Infusion Time Cefepime 0.5, 1 & 2 Not advised Infuse doses over 30 mi(Maxipime) Gm Vials
Antibiotic/ Cephalosporin
Cefotaxime 1 & 2 Gm May be given IV Up to 1 Gm/50 ml NS (Claforan) Vials push over 3-5 min Infuse over 15 minutes
(i.e. hemodialysis > 1 Gm/100ml NS Antibiotic/ patients) Infuse over 30 minutes Cephalosporin Routine use of IV
push is not recommended
Cefoxitin 1g & 2 g May be given IV Infuse over 15-30 minut(Mefoxin) vials, push over 3-5 min
Premix: (i.e. hemodialysis Antibiotic/ 1g /50 ml patients) Max rate: Cephalosporin 1 gm/3 min
Routine use of IV push is not recommended
Ceftazidime 1 g & 2g May be given IV Infuse over 30 minutes (Fortaz) vials push over 3-5 min
(i.e. hemodialysis patients)
Antibiotic/ Routine use of IV Cephalosporin push is not
recommended CefTRIAXone 250 mg, NO Infuse over 30 minutes (Rocephin) 500 mg, 1
& 2 g vials. Antibiotic/ Premix: Cephalosporin 1g/50 ml Cefuroxime 0.75 & 1.5 May be given IV Infuse over 15 to30 min(Zinacef) Gm Vials, push over 3-5 min
Premix: (i.e. hemodialysis Antibiotic/ 1.5 g/50 ml patients) Max rate: Cephalosporin 750 mg/3 min
Routine use of IV push is not recommended
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies
Dose reduction recommended with CrCl < 60 ml/min Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies
Dose reduction recommended with CrCl < 50ml/min.
Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies
Dose reduction recommended with CrCl < 50 ml/min.
Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies
Dose reduction recommended with CrCl < 50 ml/min.
Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies Do NOT co-administer with IV calcium products. Contraindicated in patients with prior hypersensitivity to cephalosporins Check allergies
Dose reduction recommended with CrCl < 20 ml/min.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 12Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
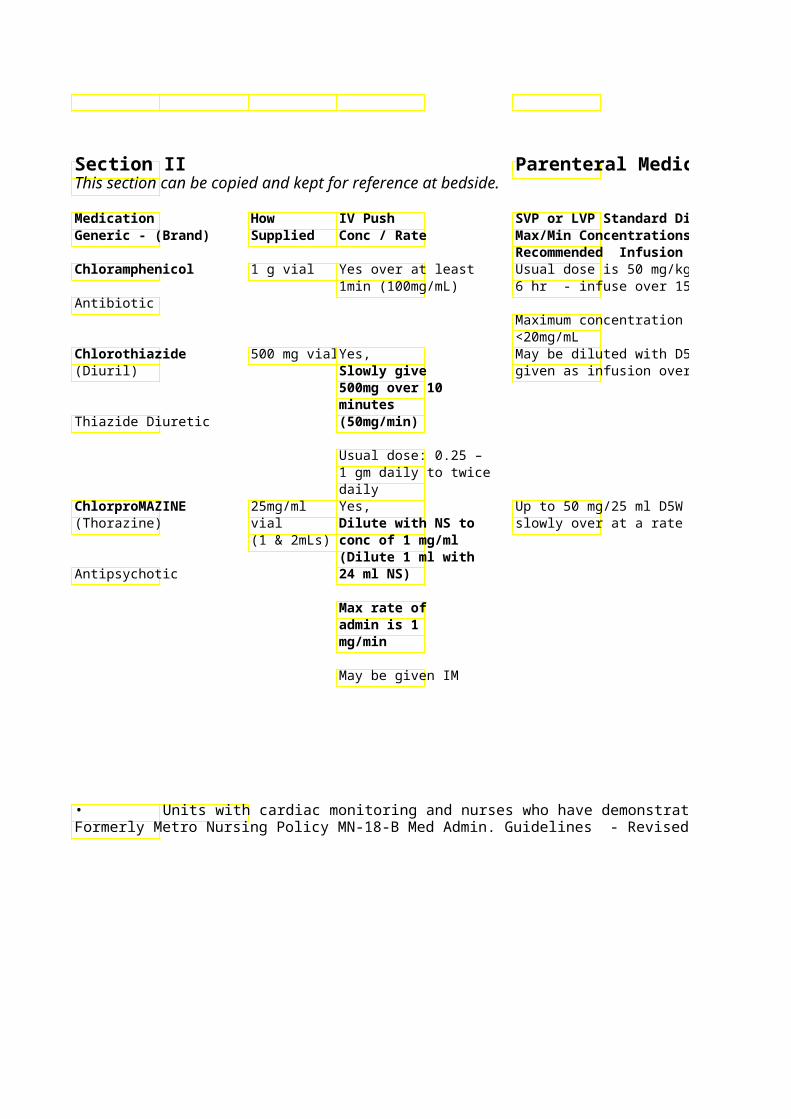
Recommended Infusion Time Chloramphenicol 1 g vial Yes over at least Usual dose is 50 mg/kg/
1min (100mg/mL) 6 hr - infuse over 15-30Antibiotic
Maximum concentration fo<20mg/mL
Chlorothiazide 500 mg vial Yes, May be diluted with D5W(Diuril) Slowly give given as infusion over 1
500mg over 10 minutes
Thiazide Diuretic (50mg/min)
Usual dose: 0.25 – 1 gm daily to twice daily
ChlorproMAZINE 25mg/ml Yes, Up to 50 mg/25 ml D5W (Thorazine) vial Dilute with NS to slowly over at a rate of
(1 & 2mLs) conc of 1 mg/ml (Dilute 1 ml with
Antipsychotic 24 ml NS)
Max rate of admin is 1 mg/min
May be given IM
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
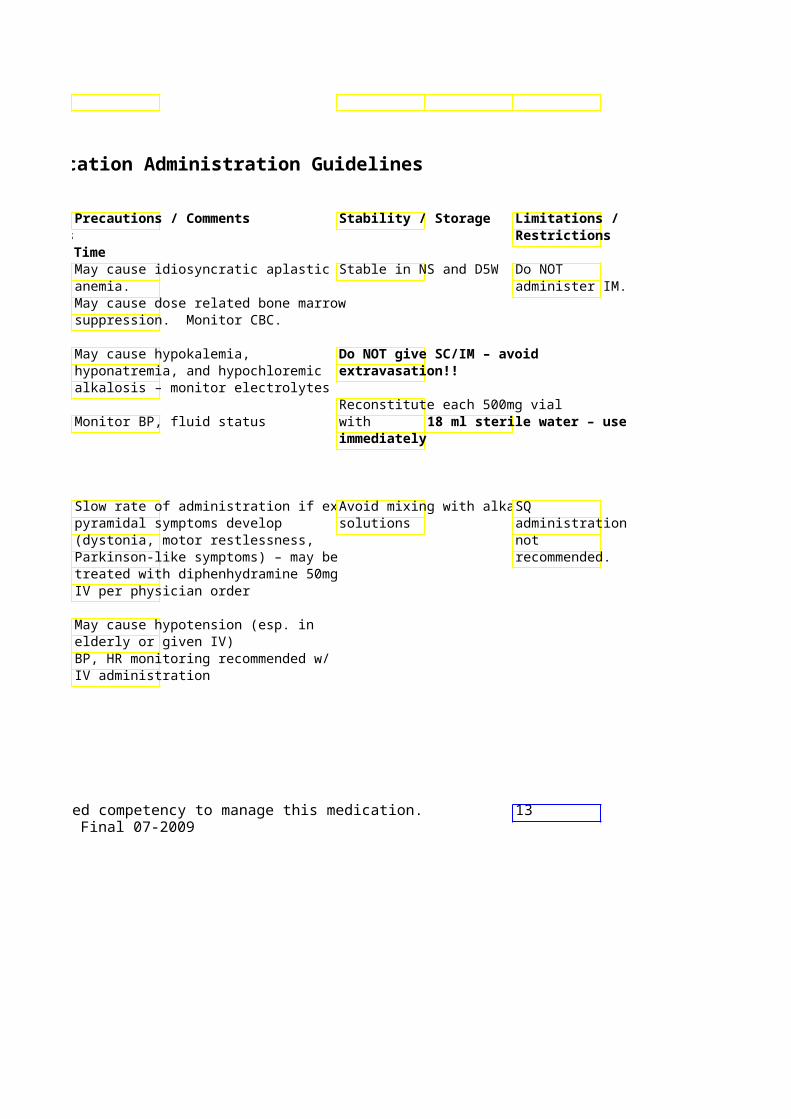
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
May cause idiosyncratic aplastic Stable in NS and D5W Do NOT anemia. administer IM. May cause dose related bone marrow suppression. Monitor CBC.
May cause hypokalemia, Do NOT give SC/IM – avoid hyponatremia, and hypochloremic extravasation!! alkalosis – monitor electrolytes
Reconstitute each 500mg vial Monitor BP, fluid status with 18 ml sterile water – use
immediately
Slow rate of administration if extra- Avoid mixing with alkali SQ pyramidal symptoms develop solutions administration (dystonia, motor restlessness, not Parkinson-like symptoms) – may be recommended. treated with diphenhydramine 50mg IV per physician order
May cause hypotension (esp. in elderly or given IV) BP, HR monitoring recommended w/ IV administration
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 13Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
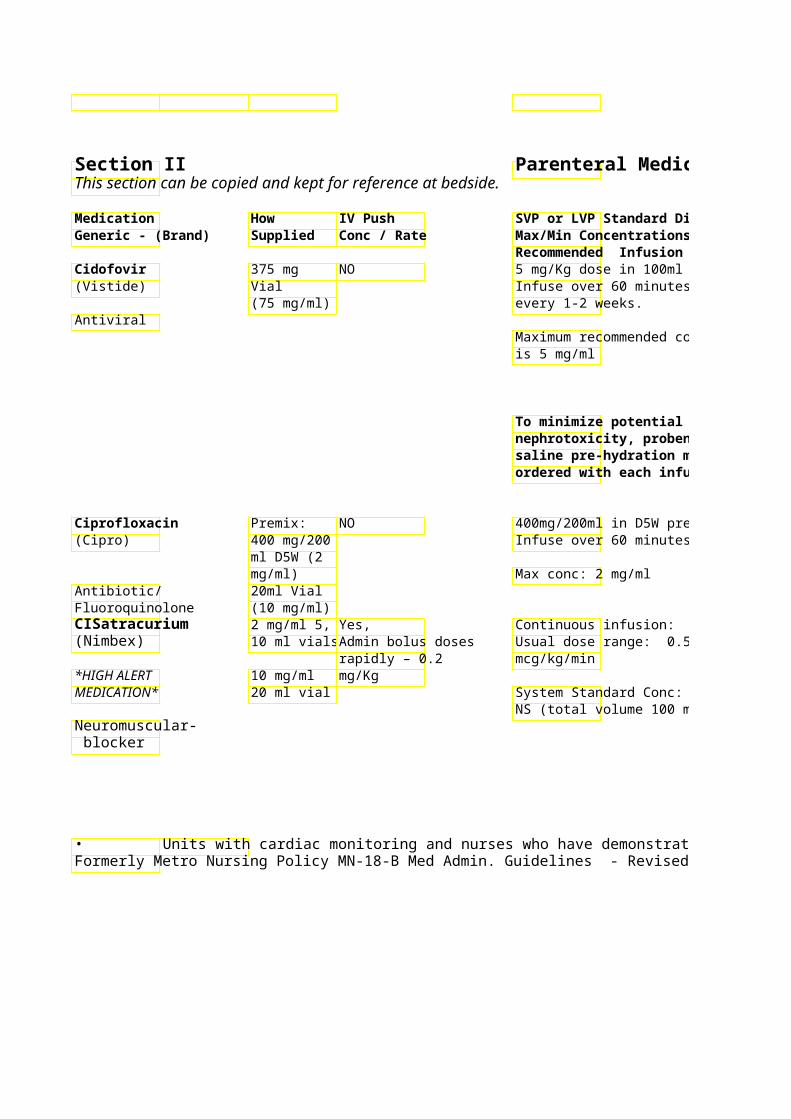
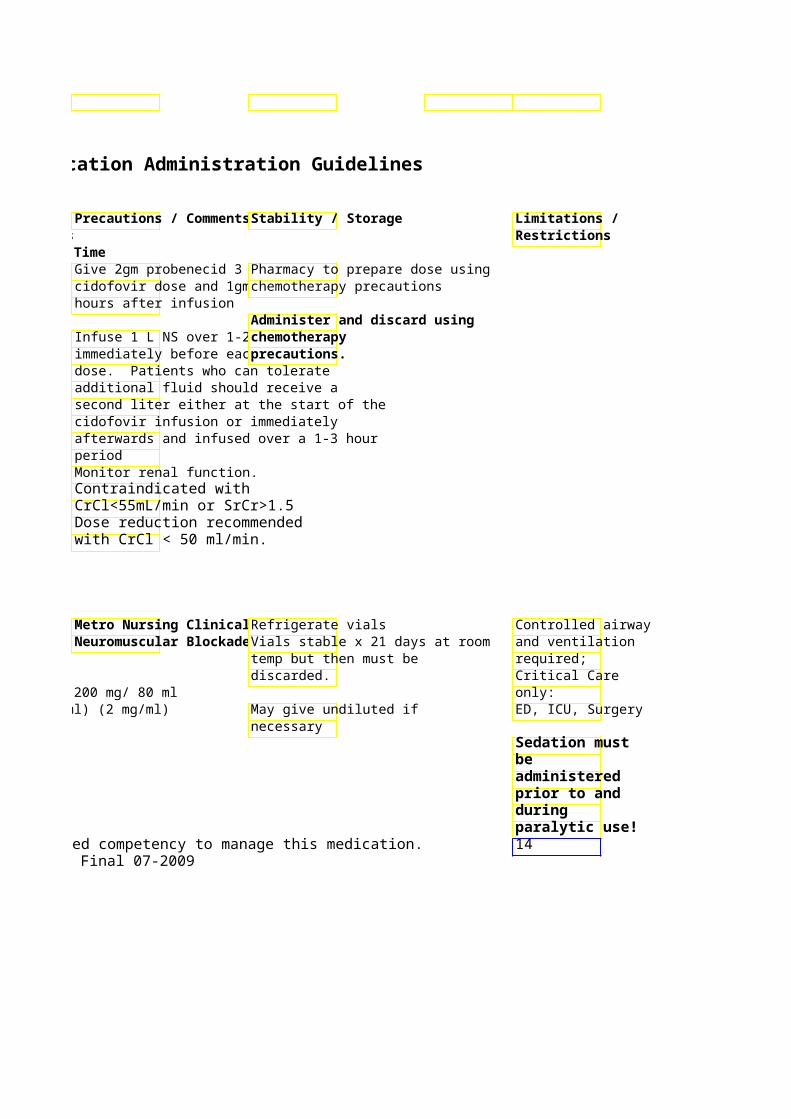
Recommended Infusion Time Cidofovir 375 mg NO 5 mg/Kg dose in 100ml N(Vistide) Vial Infuse over 60 minutes
(75 mg/ml) every 1-2 weeks. Antiviral
Maximum recommended cis 5 mg/ml
To minimize potentialnephrotoxicity, probesaline pre-hydration ordered with each inf
Ciprofloxacin Premix: NO 400mg/200ml in D5W pr(Cipro) 400 mg/200 Infuse over 60 minutes
ml D5W (2 mg/ml) Max conc: 2 mg/ml
Antibiotic/ 20ml Vial Fluoroquinolone (10 mg/ml) CISatracurium 2 mg/ml 5, Yes, Continuous infusion: (Nimbex) 10 ml vials Admin bolus doses Usual dose range: 0.5 –
rapidly – 0.2 mcg/kg/min *HIGH ALERT 10 mg/ml mg/Kg MEDICATION* 20 ml vial System Standard Conc: 200 mg/ 80 ml
NS (total volume 100 ml) (2 mg/ml) Neuromuscular- blocker
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Give 2gm probenecid 3 hPharmacy to prepare dose using cidofovir dose and 1gm achemotherapy precautions hours after infusion
Administer and discard using Infuse 1 L NS over 1-2 h chemotherapy immediately before each precautions.dose. Patients who can tolerate additional fluid should receive a second liter either at the start of the cidofovir infusion or immediately afterwards and infused over a 1-3 hour period Monitor renal function. Contraindicated with CrCl<55mL/min or SrCr>1.5 Dose reduction recommended with CrCl < 50 ml/min.
Metro Nursing Clinical Refrigerate vials Controlled airway Neuromuscular BlockaVials stable x 21 days at room and ventilation
temp but then must be required; discarded. Critical Care
System Standard Conc: 200 mg/ 80 ml only: NS (total volume 100 ml) (2 mg/ml) May give undiluted if ED, ICU, Surgery
necessary Sedation must be administered prior to and during paralytic use!
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 14Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
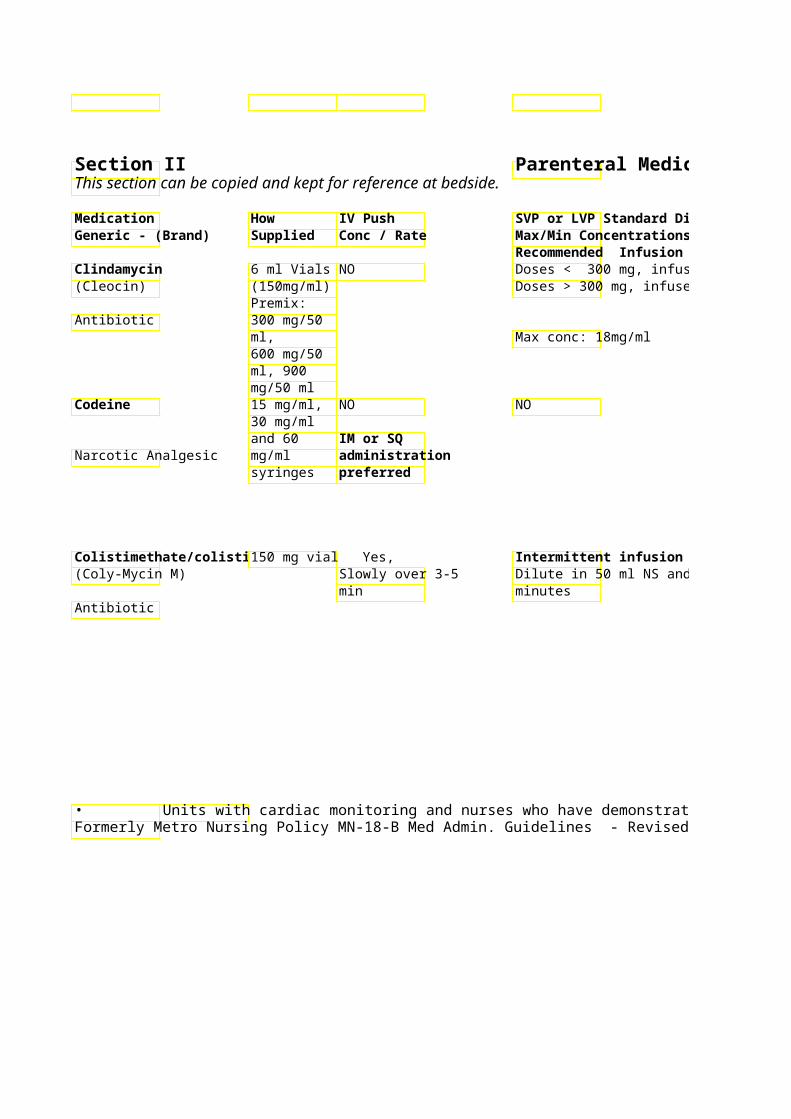
Recommended Infusion Time Clindamycin 6 ml Vials NO Doses < 300 mg, infuse(Cleocin) (150mg/ml) Doses > 300 mg, infuse
Premix: Antibiotic 300 mg/50
ml, Max conc: 18mg/ml 600 mg/50 ml, 900 mg/50 ml
Codeine 15 mg/ml, NO NO 30 mg/ml and 60 IM or SQ
Narcotic Analgesic mg/ml administration syringes preferred
Colistimethate/colisti 150 mg vial Yes, Intermittent infusion (Coly-Mycin M) Slowly over 3-5 Dilute in 50 ml NS and i
min minutes Antibiotic
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
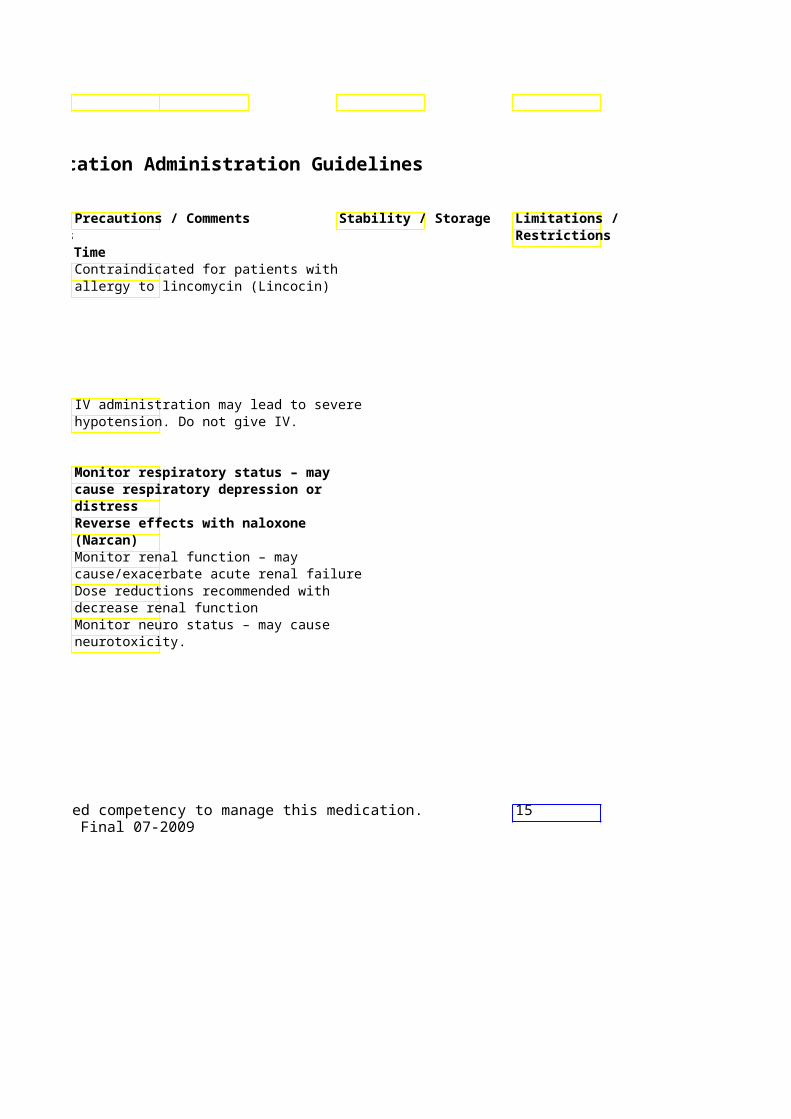
Contraindicated for patients with allergy to lincomycin (Lincocin)
IV administration may lead to severe hypotension. Do not give IV.
Monitor respiratory status – may cause respiratory depression or distress Reverse effects with naloxone (Narcan) Monitor renal function – may cause/exacerbate acute renal failure Dose reductions recommended with decrease renal function Monitor neuro status – may cause neurotoxicity.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 15Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
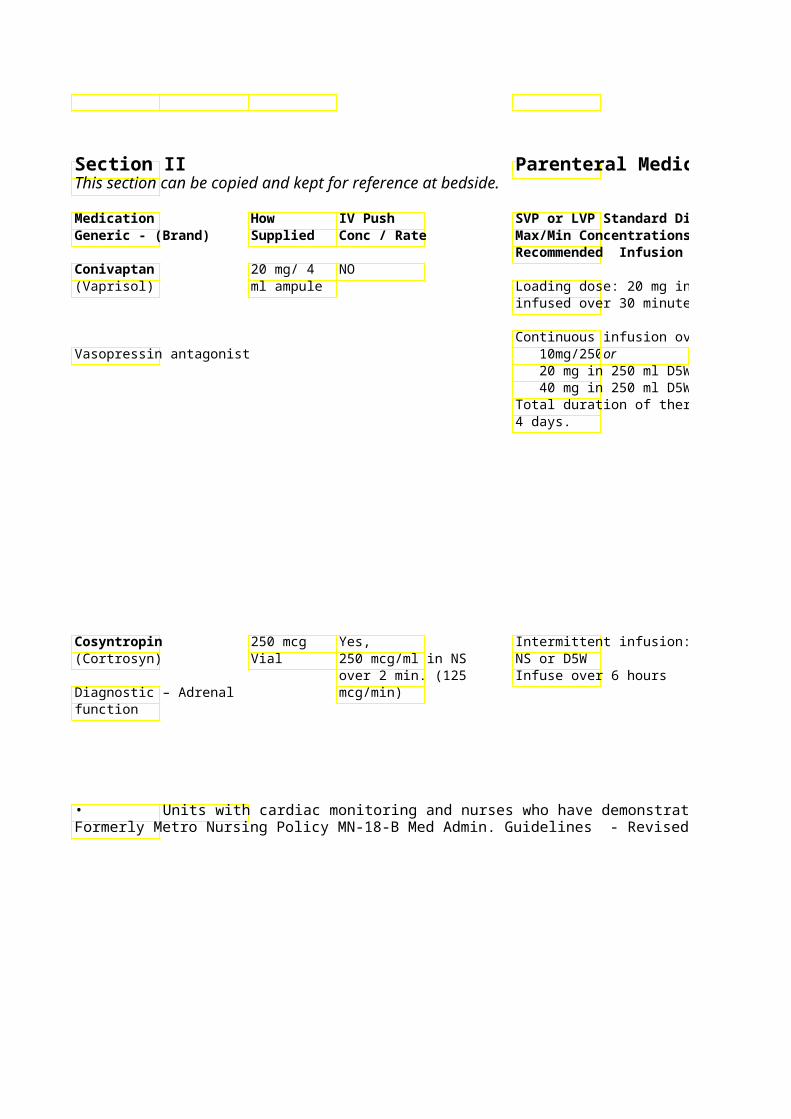
Recommended Infusion Time Conivaptan 20 mg/ 4 NO (Vaprisol) ml ampule Loading dose: 20 mg in 100 ml D5W
infused over 30 minutes
Continuous infusion over 24hours: Vasopressin antagonist 10mg/250or
20 mg in 250 ml D5W 40 mg in 250 ml D5W Total duration of therapy not to exc4 days.
Cosyntropin 250 mcg Yes, Intermittent infusion: 250mcg/250 m(Cortrosyn) Vial 250 mcg/ml in NS NS or D5W
over 2 min. (125 Infuse over 6 hours Diagnostic – Adrenal mcg/min) function
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Loading dose: 20 mg in 100 ml D5WIndicated for the treatment of infused over 30 minutes euvolemic symptomatic
hyponatremia Dilute with D5W only! Continuous infusion over 24hours:
Overly rapid correction Infuse via separate line. or (>8-12 mEq/L/24 hrs) may result in
40 mg in 250 ml D5W serious sequelae. Protect ampule from light. Total duration of therapy not to exc VASCULAR IRRITANT!
Peripheral infusion site must be rotated every 24 hours – infuse via large vein only! Serial serum sodium levels (recommended every 6 hours) required with physician call back parameters (minimum: Call physician if increase in serum sodium > 8 mEq in 24 hours or If levels and call back parameters not included in original order, physician must be contacted for order per Metro P&T
Intermittent infusion: 250mcg/250 m250 mcg = 25mg corticotropin (ACTH) Infusion stable 12 hr
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 16Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time CycloSPORINE 50 mg Amp NO (Sandimmune) (10 mg/ ml) Intermittent Infusion – typically q 12
hr For doses < 12.5 mg, give over 60 min For doses > 12.5 mg, Infuse over minimum of 2 hours. Concentration must be 0.4 – 2 mg/ml
Continuous infusion – Change bag daily at 1800 System Standard Conc: 250 mg/250 ml NS System “Concentrated” Conc: 250 mg/
Immunosuppressant 100 ml NS Cytomegalovirus 1 Gm and NO Usual Dose: 50-150mg/kg – doses up (CMV) Immune 2.5 Gm to 400mg/kg for severe CMV infection Globulin (CytoGam) Vials
Initial Dose: 15 mg/kg/hr - May increase to 30 mg/kg/hr if no adverse reactions after 30 min. - May increase to max rate of 60 mg/kg/hr if no adverse reactions after a subsequent 30 min. Do NOT exceed 60 mg/Kg/hr!! Max volume = 75 ml/hr Subsequent Doses: 15 mg/kg/hr for 15 min, then 30 mg/kg/hr for 15 min, then 60 mg/kg/hr if no adverse reactions Do NOT exceed 60 mg/kg/hr!!
CMVIG/ IgG antibody to Max volume = 75 ml/hr. CMV
Daclizumab 5mg/ml – NO Intermittent Infusion – (Zenapax) 5ml vial 1mg/Kg diluted into 50ml NS.
Infuse over 15 minutes via peripheral or central line.
Immunosuppressant
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / CommenStability / Storage Max/Min Concentrations Recommended Infusion Time
Due to the risk of anaphylaxis, patients Intermittent Infusion – typically q 12 receiving cyclosporine IV should be
under continuous observaUse admin set provided by For doses < 12.5 mg, give over 60 min least the first 30 minute pharmacy (Non PVC tubing) For doses > 12.5 mg, Infuse over start of the infusion and at frequent minimum of 2 hours. intervals durEpinephrinProtect ampule from light Concentration must be 0.4 – 2 mg/ml st
be available (UBC) during 1 30 minutes
Continuous infusion – Change bag daily at 1800 IV dose = 0.33 x PO dose System Standard Conc: 250 mg/250 ml
(Excel) (1 mg/ml) System “Concentrated” Conc: 250 mg/ Monitor cyclosporine trough
(Excel) (2.5 mg/ml)concentrations. Usual Dose: 50-150mg/kg – doses up Monitor vital signs befo Start infusion within 6 hr of to 400mg/kg for severe CMV infection through, after infusion entering vial. Complete
change in rate. infusion within 12 hr of Initial Dose: 15 mg/kg/hr entering vial. - May increase to 30 mg/kg/hr if no Potential adverse reactions: flushing, adverse reactions after 30 min. chills, muscle cramps, b Administer through IV line - May increase to max rate of 60 fever, nausea, vomiting,with in-line 15micron filter. mg/kg/hr if no adverse reactions after a decreased blood pressure. subsequent 30 min. Do NOT exceed 60 Administer using a separate IV mg/Kg/hr!! Max volume = 75 ml/hr If patient develops minorline. May be \"piggybacked\" Subsequent Doses: 15 mg/kg/hr for 15 (nausea, back pain, flushinto pre-existing line of NS or min, then 30 mg/kg/hr for 15 min, then IV rate or temporarily in D5W, however CMV-IG should 60 mg/kg/hr if no adverse reactions infusion. not be diluted more than 50%. Do NOT exceed 60 mg/kg/hr!! Max volume = 75 ml/hr. If anaphylaxis or hypotension
occurs, discontinue the infusion and contact the physician.
Intermittent Infusion – 5 doses define standard Stable 24 hours after dilution 1mg/Kg diluted into 50ml NS. therapy. First dose beforefrigerated Infuse over 15 minutes via peripheral and subsequent doses 14Stable 4 hr at room temp or central line.
Do not mix with other solutions Do not shake solution or transport via tube system
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Use admin set provided by pharmacy (Non PVC tubing)
Protect ampule from light
Start infusion within 6 hr of entering vial. Complete
Administer through IV line with in-line 15micron filter.
Administer using a separate IV line. May be \"piggybacked\" into pre-existing line of NS or D5W, however CMV-IG should not be diluted more than 50%.
Stable 24 hours after dilution
Stable 4 hr at room temp
Do not mix with other solutions Do not shake solution or transport via tube system
17
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / RateMax/Min Concentrations
Recommended Infusion Time Dalfopristin / 500mg Vial NO Usual dose: Quinupristin 7.5mg/Kg (in 250 ml D5W) q 8-12 hr(Synercid)
Infuse over 60 minutes
Concentrated solution in 100ml D5W – pain, burning, itch – further dilute Antibiotic central line administration only
Dalteparin Pre-filled NO Not advised. (Fragmin) syringes,
multi-dose SC Anticoagulant/ Low vial administration molecular weight heparin only! Do NOT
give IM Dantrolene 20 mg Vial Yes, Malignant Hyperthermia (MH)(Dantrium) Rapid admin Prevention: 2.5 mg/Kg infused over
advised for60 minutes 1.25 hours prior to Malignant treatment oanesthesia. Hyperthermia Hotline Malignant (for contact with MH Hyperthermia Treatmentexpert) (MH) given rapidly. Repeat dose every 5 1-800-MH-HYPER min until symptoms subside or (1-800-644-9737) 10mg/Kg (recommended upper
limit) has been reached (subsequent doses may be given as needed!)
Then continue 1 mg/kg every 4-8 hr for 24 – 48 hrs.
Muscle relaxant DAPTOmycin 250 mg, NO Dilute in 100 ml NS – (Cubicin) 500 mg vial Infuse over 30 min
Usual dose: 4-6 mg/kg IV q24h
Antibiotic Max concentration: 20mg/mL
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Restrictions
Flush IV lines before and after 7.5mg/Kg (in 250 ml D5W) q 8-12 hradmin with D5W only, avoid Do not shake
NS
Infusion site reactions common – Concentrated solution in 100ml D5W – pain, burning, itch – further dilute
doses (500-750mL) if these occur Arthralgia & myalgia common SC administration only! Do NOT See syringe for manufacturer give IM expiration date
Malignant Hyperthermia (MH)Staff in areas where stored toDilute with STERILE : 2.5 mg/Kg infused overperiodically check expiration WATER onl– 60 ml per 20
date on vials to insure use of mg = 0.33 mg/ml. date medication when neededPrepare immediately before
administration. Six-hour : 2.5 mg/KgAvoid extravasation – central line stability at room temp.
given rapidly. Repeat dose every 5 administration preferred. Do not ** Powder in vials may take withhold care if no central access available!! several minutes to dissolve
limit) has been reached (subsequent ** doses may be given as needed!) Monitor urine output
Then continue 1 mg/kg every 4-8 hr Call Code 4 and/or pharmacy for assistance if treating MH
Dose reduction recommended for CrC** Not compatible in < 30: q48 hr dextrose !!
Usual dose: 4-6 mg/kg IV q24h May cause elevated CPK levels – Stable 12 hr at room temp/48 monitor for myopathy hrs refrigerated
Max concentration: 20mg/mL Check with pharmacist for compatibilities
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 18Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Darbepoetin alfa Vials: Yes, Not necessary (Arenesp) 25 mcg/ml SQ or IV bolus
40 mcg/ml Red cell stimulating 60 mcg/ml hormone 100 mcg/ml
200 mcg/ml
Deferoxamine 500 mg, NO Dose varies with indicati(Desferal) 2000 mg Acute Iron Overload: IM
Vials IM administration unless pt in shock. Repreferred is 1000 mg then 500 mg
doses. Subsequent dosesMay be given SC Max dose = 6 Gm/24 hr.
If given via IV infusion:mg/kg/hr for first 1000rate of 125 mg/hr for su
Iron Chelating agent Desmopressin 1 ml Vial Yes, Usual Dose: 0.3 mcg/kg (DDAVP) (4 mcg/ml) for treatment of given over 15-30 min
diabetes insipidus To stabilize hemostasis before surgery Hormone – Vasopressin – may give 2-4 administer 30min prior tanalog mcg/d Give max Children < 10 kg, -dilute
rate of 4 mcg/min May be given subcutaneously
Dexamethasone 4 mg/ml 1, Yes, IV Push preferred. (Decadron) 5, 25 and IV Push preferred
30 ml vials – all doses oDoses may be diluted inCorticosteroid 24 mg/ml 5 min. IM injection used in OB
ml vial q12h x 4 doses recommended as alternative to betamethasone for all pregnancies 24-34 weeks at risk for pre-term delivery.
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor for injection site pain, Do not shake product orRestricted to headache, arthralgias, and myalgias.transport via tube syste Outpatient Hemoglobin <10 in chemotherapy- administration induced anemia. Refrigerate only. Hemoglobin < 12 mg/dl in chronic Check kidney disease / other indications. hemoglobin prior
to administration. Notify physician prn for dose reduction or interruption based on most recent hemoglobin.
Flushing, hypotension and shock havReconstitute with STERILE been reported with IV administrationWATER then dilute with NS slow infusion rate if this occurs. Chronic Iron Overload: 500 – 1000 mg daily IM 2000 mg IV with each unit of Protect from light transfused blood – administered separately. Max rate = 15 mg/kg/hr.Do NOT Refrigerate Max dose = 6 Gm/24 hr no matter amount of blood transfused. Dilute in 500 ml or 1000 ml NS Monitor HR and BP during infusion Refrigerate vial and for 60 minutes after.
To stabilize hemostasis before surgery Stable 12 hr after diluted When used to manage diabetes refrigerated insipidus, monitoring of urine output every 8 hr recommended May cause hyponatremia – monitor Na+ Doses > 10 mg may be ordered as intermittent IV infusion Pt may complain about perianal itching/tingling with doses > 10 mg
q12h x 4 doses recommended as alternative to betamethasone for all pregnancies 24-34 weeks at risk for
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 19Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
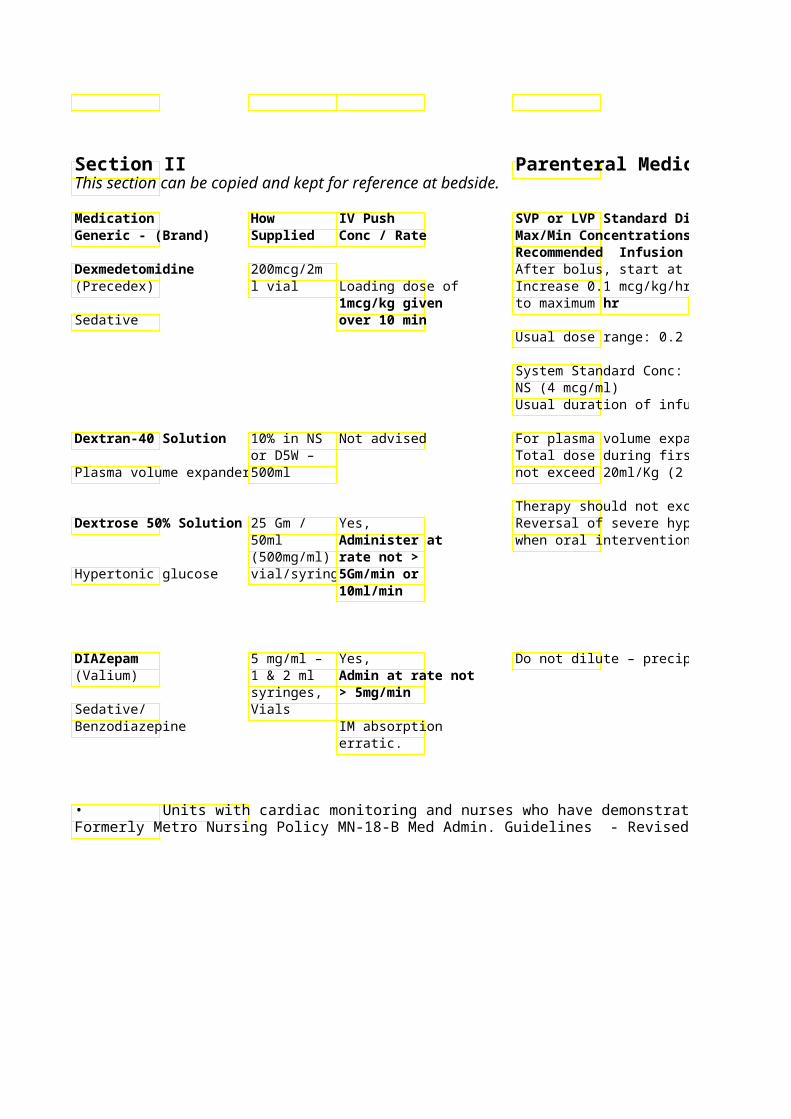
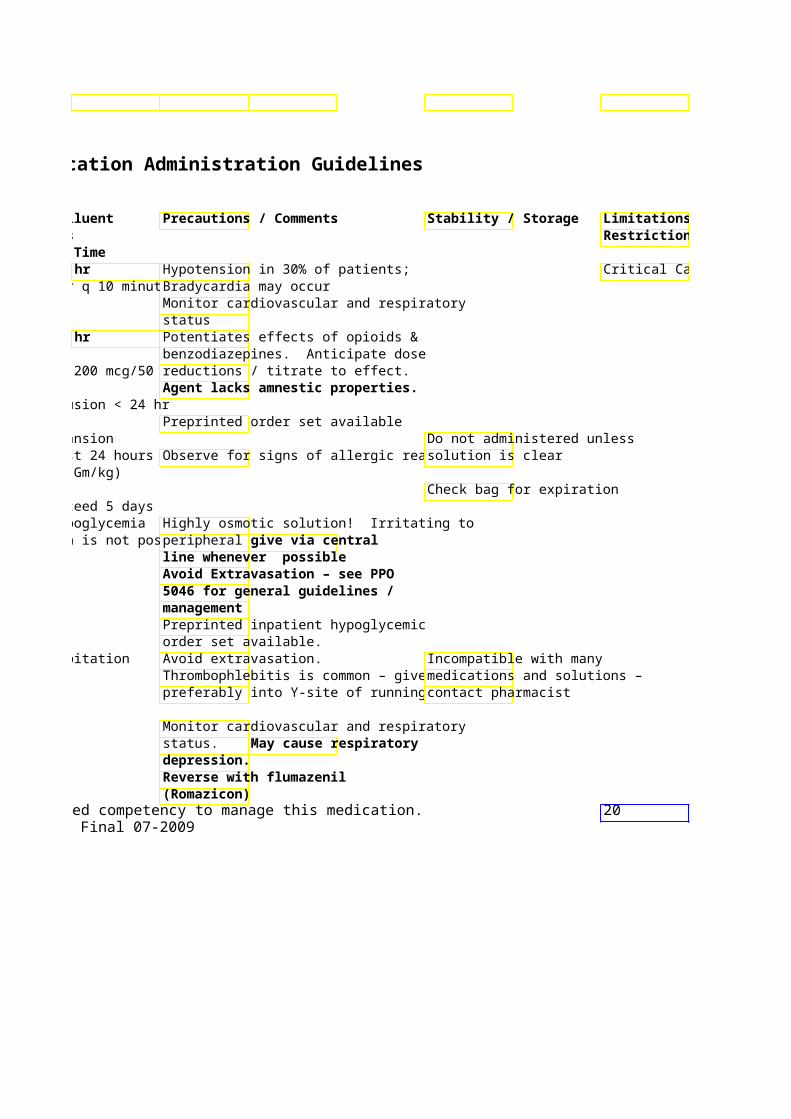
Recommended Infusion Time Dexmedetomidine 200mcg/2m After bolus, start at 0.4(Precedex) l vial Loading dose of Increase 0.1 mcg/kg/hr q 10 minutes
1mcg/kg given to maximum hrSedative over 10 min
Usual dose range: 0.2 –
System Standard Conc: 200 mcg/50 NS (4 mcg/ml) Usual duration of infusion < 24 hr
Dextran-40 Solution 10% in NS Not advised For plasma volume expansion or D5W – Total dose during first 24 hours shou
Plasma volume expander500ml not exceed 20ml/Kg (2 Gm/kg)
Therapy should not exceed 5 days Dextrose 50% Solutio25 Gm / Yes, Reversal of severe hypoglycemia
50ml Administer at when oral intervention is not possible(500mg/ml) rate not >
Hypertonic glucose vial/syringe 5Gm/min or 10ml/min
DIAZepam 5 mg/ml – Yes, Do not dilute – precipitation (Valium) 1 & 2 ml Admin at rate not
syringes, > 5mg/min Sedative/ Vials Benzodiazepine IM absorption
erratic.
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
hr Hypotension in 30% of patients; Critical Care only Increase 0.1 mcg/kg/hr q 10 minutesBradycardia may occur
Monitor cardiovascular and respiratory status
hr Potentiates effects of opioids & benzodiazepines. Anticipate dose
System Standard Conc: 200 mcg/50 reductions / titrate to effect. Agent lacks amnestic properties.
Usual duration of infusion < 24 hr Preprinted order set available
For plasma volume expansion Do not administered unless Total dose during first 24 hours shouObserve for signs of allergic reactionsolution is clear not exceed 20ml/Kg (2 Gm/kg)
Check bag for expiration Therapy should not exceed 5 days Reversal of severe hypoglycemia Highly osmotic solution! Irritating to when oral intervention is not possibleperipheral vegive via central
line whenever possible Avoid Extravasation – see PPO 5046 for general guidelines / management Preprinted inpatient hypoglycemic order set available.
Do not dilute – precipitation Avoid extravasation. Incompatible with many Thrombophlebitis is common – give medications and solutions – preferably into Y-site of running IV. contact pharmacist
Monitor cardiovascular and respiratory status. May cause respiratory depression. Reverse with flumazenil (Romazicon)
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 20Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Critical Care only
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
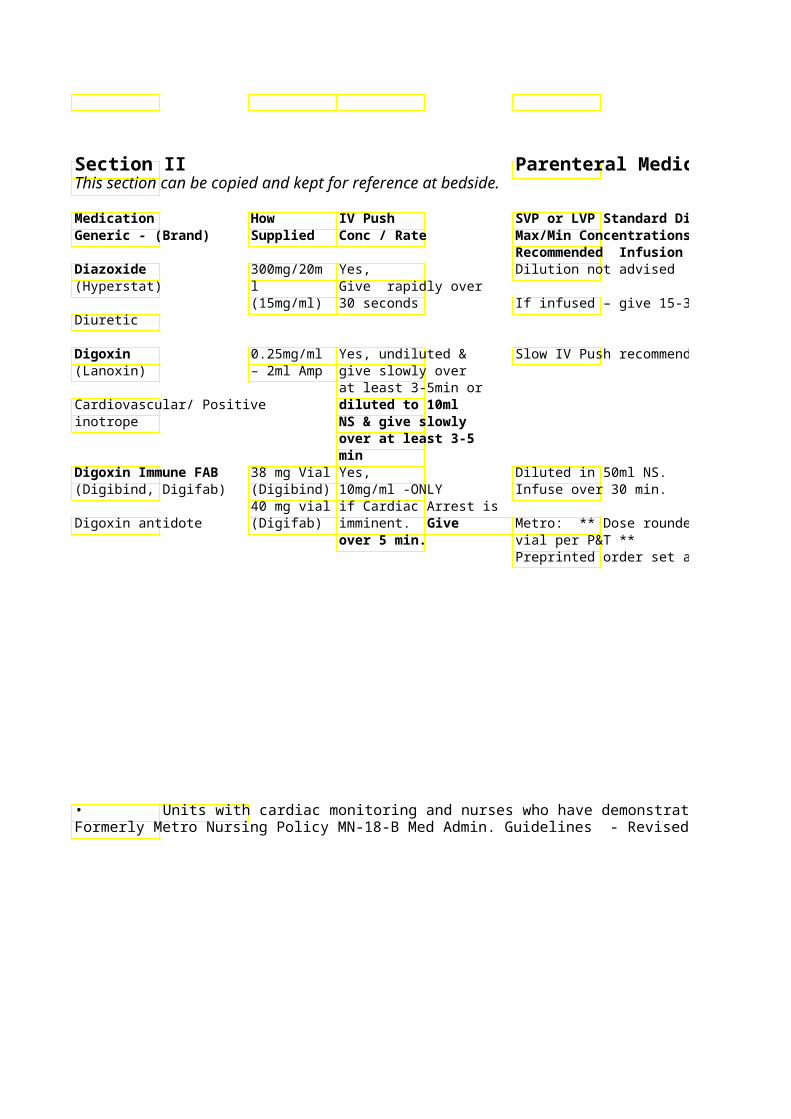
Recommended Infusion Time Diazoxide 300mg/20mYes, Dilution not advised (Hyperstat) l Give rapidly over
(15mg/ml) 30 seconds If infused – give 15-30 mg/min Diuretic
Digoxin 0.25mg/ml Yes, undiluted & Slow IV Push recommen(Lanoxin) – 2ml Amp give slowly over
at least 3-5min or Cardiovascular/ Positive diluted to 10ml inotrope NS & give slowly
over at least 3-5 min
Digoxin Immune FAB 38 mg Vial Yes, Diluted in 50ml NS. (Digibind, Digifab) (Digibind) 10mg/ml -ONLY Infuse over 30 min.
40 mg vial if Cardiac Arrest is Digoxin antidote (Digifab) imminent. Give Metro: ** Dose rounded
over 5 min. vial per P&T ** Preprinted order set avai
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Avoid extravasation Use Central Line Do not mix with other IV* See footnote if available. medications.
If infused – give 15-30 mg/min Protect from light. Do not administer IM/SQ Darkened solutions should not
be used. Check apical pulse prior to administration. If heart rate is less than 50 BPM or otherwise specified – HOLD dose & call physician
Monitor vital signs & ECG *See footnote Monitor for hypokalemia – obtain Use reconstituted product serial potassium levels especially immediately. during the hours after administration
Use administration set provided Digoxin serum level assay not by pharmacy which includes accurate after digibind. Pharmacy 0.22 micron filter will notify lab pt has received digoxin immune FAB
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 21Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
* See footnote
*See footnote
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Dihydroergotamine 1mg/ml – Yes, Continuous infusion may(DHE) 1ml amp Give at max rate status migranosis
of 1mg/min Antimigraine/ Ergot alkaloid May be given IM
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Total IV dose should not exceed 2 Protect ampule from light mg/day (3mg/day if continuous infusion). Total weekly dose should not exceed 6 mg (20mg over 7 days if continuous infusion). Monitor HR and BP. Contact physician immediately (and stop infusion if continuous infusion) if chest pain develops. Contact physician immediately if numbness/tingling of extremeties, nausea/vomiting unrelieved by antiemetics, leg cramping, or coldness of skin develops. Contraindicated in patients with hypersensitivity to ergot alkaloids – ergotamine. Contraindicated if ergotamine or triptan used within past 24 hours Contraindicated with multiple drug classes (i.e. MAO-Inhibitors, potent inhibitors of 3A4). Contraindicated in patients with ischemic heart disease.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 22Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
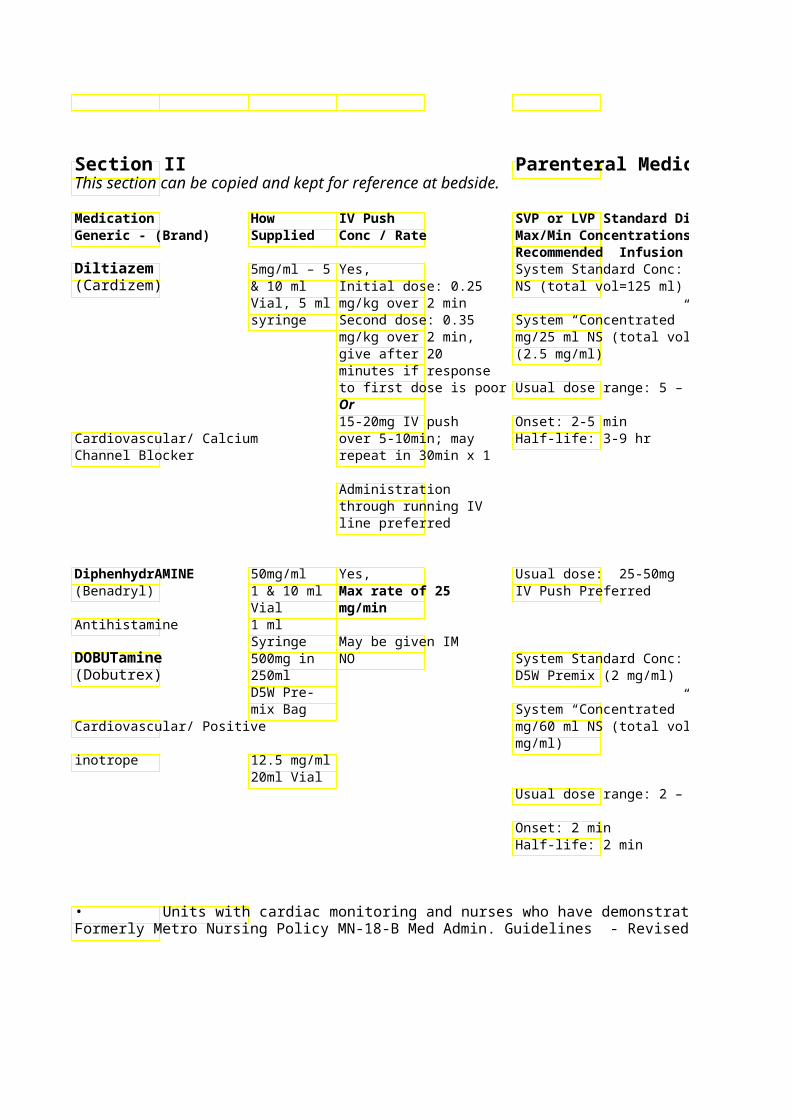
Recommended Infusion Time Diltiazem 5mg/ml – 5 Yes, System Standard Conc: (Cardizem) & 10 ml Initial dose: 0.25 NS (total vol=125 ml)
Vial, 5 ml mg/kg over 2 min syringe Second dose: 0.35 System “Concentrated”
mg/kg over 2 min, mg/25 ml NS (total volume 50 ml) give after 20 (2.5 mg/ml) minutes if response to first dose is poor Usual dose range: 5 – 15Or 15-20mg IV push Onset: 2-5 min
Cardiovascular/ Calcium over 5-10min; may Half-life: 3-9 hr Channel Blocker repeat in 30min x 1
Administration through running IV line preferred
DiphenhydrAMINE 50mg/ml Yes, Usual dose: 25-50mg (Benadryl) 1 & 10 ml Max rate of 25 IV Push Preferred
Vial mg/min Antihistamine 1 ml
Syringe May be given IM DOBUTamine 500mg in NO System Standard Conc: (Dobutrex) 250ml D5W Premix (2 mg/ml)
D5W Pre-mix Bag System “Concentrated” c
Cardiovascular/ Positive mg/60 ml NS (total volumg/ml)
inotrope 12.5 mg/ml 20ml Vial
Usual dose range: 2 – 2
Onset: 2 min Half-life: 2 min
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
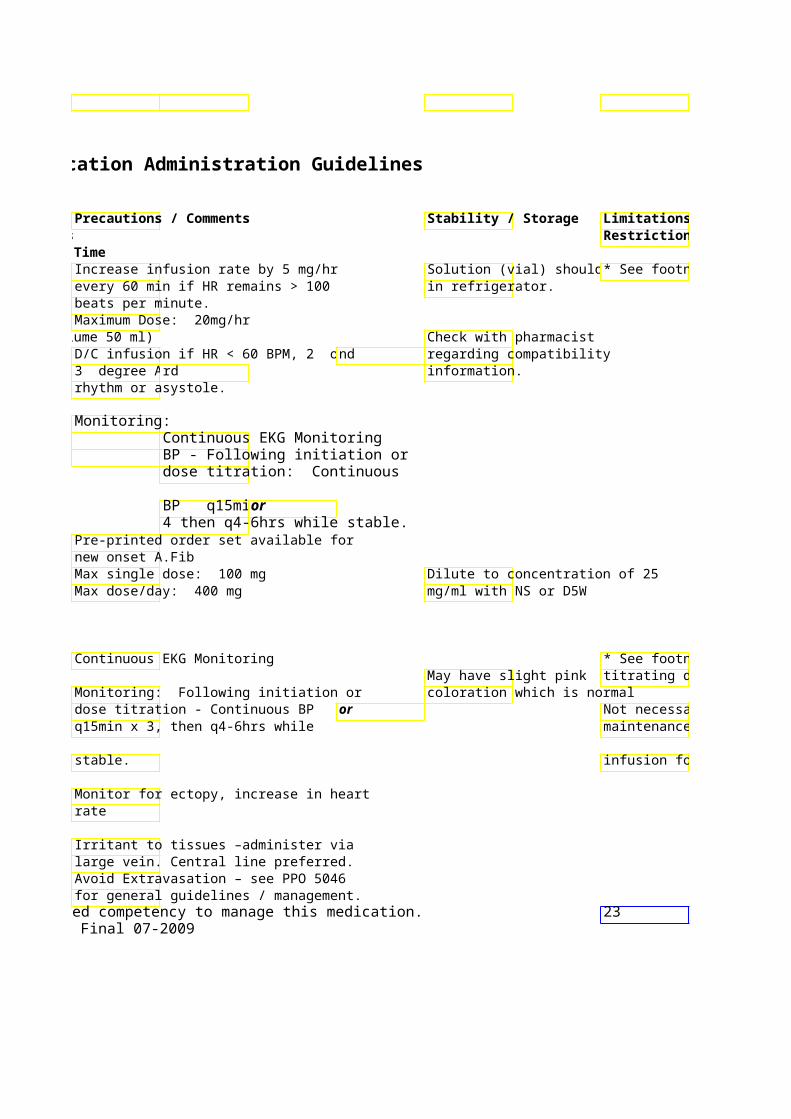
Increase infusion rate by 5 mg/hr Solution (vial) should be* See footnote every 60 min if HR remains > 100 in refrigerator. beats per minute. Maximum Dose: 20mg/hr
mg/25 ml NS (total volume 50 ml) Check with pharmacist D/C infusion if HR < 60 BPM, 2 or nd regarding compatibility 3 degree AVrd information. rhythm or asystole.
Monitoring: Continuous EKG Monitoring BP - Following initiation or dose titration: Continuous
BP q15minor4 then q4-6hrs while stable.
Pre-printed order set available for new onset A.Fib Max single dose: 100 mg Dilute to concentration of 25 Max dose/day: 400 mg mg/ml with NS or D5W
Continuous EKG Monitoring * See footnote if May have slight pink titrating dose.
Monitoring: Following initiation or coloration which is normal dose titration - Continuous BP or Not necessary for q15min x 3, then q4-6hrs while maintenance
stable. infusion for CHF
Monitor for ectopy, increase in heart rate
Irritant to tissues –administer via large vein. Central line preferred. Avoid Extravasation – see PPO 5046 for general guidelines / management.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 23Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
* See footnote
* See footnote if titrating dose.
Not necessary for maintenance
infusion for CHF
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
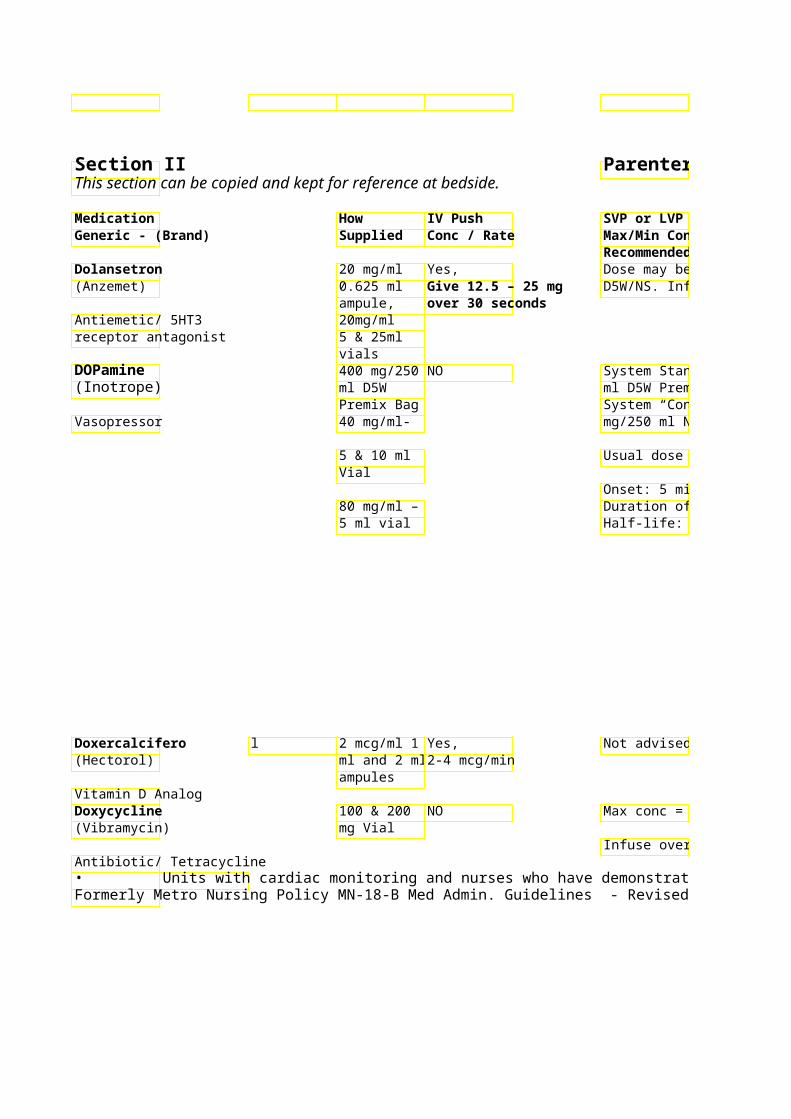
Recommended Infusion Time Dolansetron 20 mg/ml Yes, Dose may be diluted in (Anzemet) 0.625 ml Give 12.5 – 25 mg D5W/NS. Infuse over 15 min
ampule, over 30 seconds Antiemetic/ 5HT3 20mg/ml receptor antagonist 5 & 25ml
vials DOPamine 400 mg/250NO System Standard Conc: (Inotrope) ml D5W ml D5W Premix (1.6 mg/
Premix Bag System “Concentrated” Vasopressor 40 mg/ml- mg/250 ml NS (3.2 mg/m
5 & 10 ml Usual dose range is 2 – 20 mcg/kg/min Vial
Onset: 5 min 80 mg/ml – Duration of action: 10 m5 ml vial Half-life: 2 min
Doxercalcifero l 2 mcg/ml 1 Yes, Not advised (Hectorol) ml and 2 ml 2-4 mcg/min
ampules Vitamin D Analog Doxycycline 100 & 200 NO Max conc = 1 mg/ml (Vibramycin) mg Vial
Infuse over minimum of 60 min Antibiotic/ Tetracycline • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard DPrecautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Dose may be diluted in May cause QT prolongatiDo not mix with other Non-formulary. D5W/NS. Infuse over 15 min medications. Autosubstitution
to ondansetron
System Standard Conc: Monitoring - Following initiation * See footnote ml D5W Premix (1.6 mg/or dose titration: Con Consult pharmacist for System “Concentrated” or q15min x 3compatibility information. Central Line mg/250 ml NS (3.2 mg/mq4-6h while stable. Avoid infiltration – Administration
Phentolamine (Regitine) Usual dose range is 2 – 20 mcg/kg/min intradermally Required unless
order obtained Onset: 5 min Dopaminergic effects: /subcutaneously from physician Duration of action: 10 m < 5 mcg/kg/min recommended for for peripheral Half-life: 2 min Beta effects (Improved Cmanagement administration!!
Output): 2-10 mcg/Kg/min Midline access is Alpha > Beta Effects Avoid Extravasation – see not = to a (Vasoconstriction): PPO 5046 for general central line. > 10-15 mcg/Kg/min guidelines / management Check IV site
every 30 Central Line Administration minutes while Required unless order obtained dopamine is from physician for peripheral administered administration!! peripherally.Check IV site every 30 minutes while dopamine is administered peripherally.
Not advised Used in the treatment o Protect from light hyperparathyroidism in chronic renal failure patients. Discard ampule after use.
Max conc = 1 mg/ml Avoid extravasation -Irri Stable 12 hr at room temp or tissues 72 hr refrigerated
Infuse over minimum of 60 min Protect from light
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 24Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Limitations / Restrictions
Non-formulary. Autosubstitution to ondansetron
* See footnote
Central Line Administration
Required unless order obtained from physician for peripheral administration!! Midline access is not = to a central line. Check IV site every 30 minutes while dopamine is administered peripherally.
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
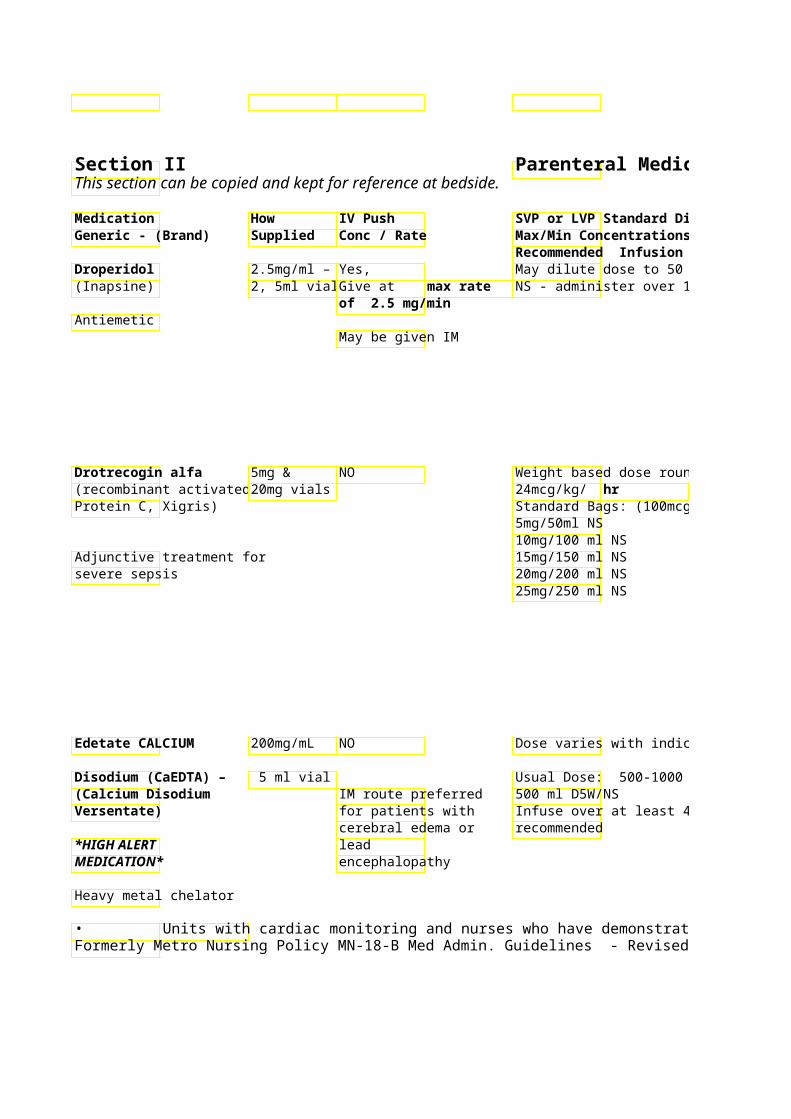
Recommended Infusion Time Droperidol 2.5mg/ml – Yes, May dilute dose to 50 ml in D5W or (Inapsine) 2, 5ml vials Give at max rate NS - administer over 15 min
of 2.5 mg/min Antiemetic
May be given IM
Drotrecogin alfa 5mg & NO Weight based dose rounding – (recombinant activated 20mg vials 24mcg/kg/ hr Protein C, Xigris) Standard Bags: (100mcg/ml)
5mg/50ml NS 10mg/100 ml NS
Adjunctive treatment for 15mg/150 ml NS severe sepsis 20mg/200 ml NS
25mg/250 ml NS
Edetate CALCIUM 200mg/mL NO Dose varies with indication.
Disodium (CaEDTA) – 5 ml vial Usual Dose: 500-1000 mg/m /day in(Calcium Disodium IM route preferred 500 ml D5W/NS Versentate) for patients with Infuse over at least 4 hrs – 8-12 hrs
cerebral edema or recommended *HIGH ALERT lead MEDICATION* encephalopathy
Heavy metal chelator
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
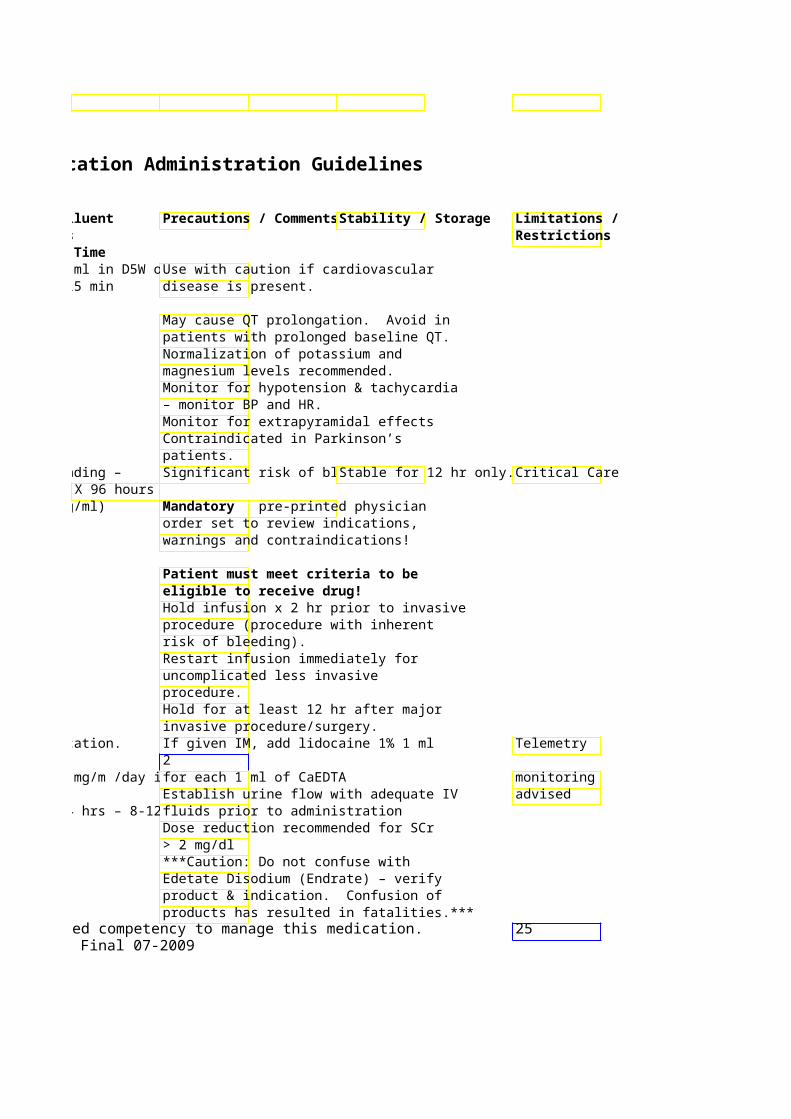
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time May dilute dose to 50 ml in D5W or Use with caution if cardiovascular NS - administer over 15 min disease is present.
May cause QT prolongation. Avoid in patients with prolonged baseline QT. Normalization of potassium and magnesium levels recommended. Monitor for hypotension & tachycardia – monitor BP and HR. Monitor for extrapyramidal effects Contraindicated in Parkinson’s patients.
Weight based dose rounding – Significant risk of bleedi Stable for 12 hr only. Critical Care X 96 hours
Standard Bags: (100mcg/ml) Mandatory pre-printed physician order set to review indications, warnings and contraindications!
Patient must meet criteria to be eligible to receive drug! Hold infusion x 2 hr prior to invasive procedure (procedure with inherent risk of bleeding). Restart infusion immediately for uncomplicated less invasive procedure. Hold for at least 12 hr after major invasive procedure/surgery.
Dose varies with indication. If given IM, add lidocaine 1% 1 ml Telemetry 2
Usual Dose: 500-1000 mg/m /day infor each 1 ml of CaEDTA monitoring Establish urine flow with adequate IV advised
Infuse over at least 4 hrs – 8-12 hrs fluids prior to administration Dose reduction recommended for SCr > 2 mg/dl ***Caution: Do not confuse with Edetate Disodium (Endrate) – verify product & indication. Confusion of products has resulted in fatalities.***
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 25Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
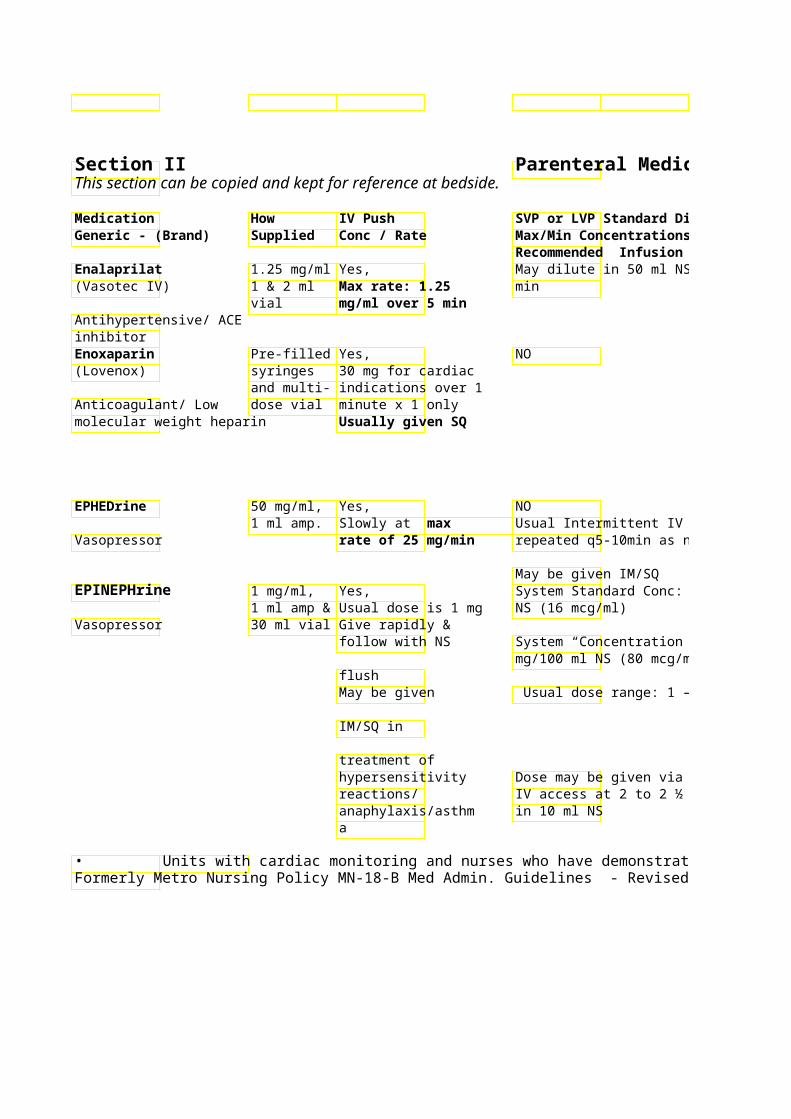
Recommended Infusion Time Enalaprilat 1.25 mg/ml Yes, May dilute in 50 ml NS –(Vasotec IV) 1 & 2 ml Max rate: 1.25 min
vial mg/ml over 5 min Antihypertensive/ ACE inhibitor Enoxaparin Pre-filled Yes, NO (Lovenox) syringes 30 mg for cardiac
and multi- indications over 1 Anticoagulant/ Low dose vial minute x 1 only molecular weight heparin Usually given SQ
EPHEDrine 50 mg/ml, Yes, NO 1 ml amp. Slowly at max Usual Intermittent IV do
Vasopressor rate of 25 mg/min repeated q5-10min as needed
May be given IM/SQ EPINEPHrine 1 mg/ml, Yes, System Standard Conc:
1 ml amp & Usual dose is 1 mg NS (16 mcg/ml) Vasopressor 30 ml vial Give rapidly &
follow with NS System “Concentration” Conc: 8 mg/100 ml NS (80 mcg/m
flush May be given Usual dose range: 1 –
IM/SQ in
treatment of hypersensitivity Dose may be given via ETreactions/ IV access at 2 to 2 ½ x Ianaphylaxis/asthm in 10 ml NS a
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
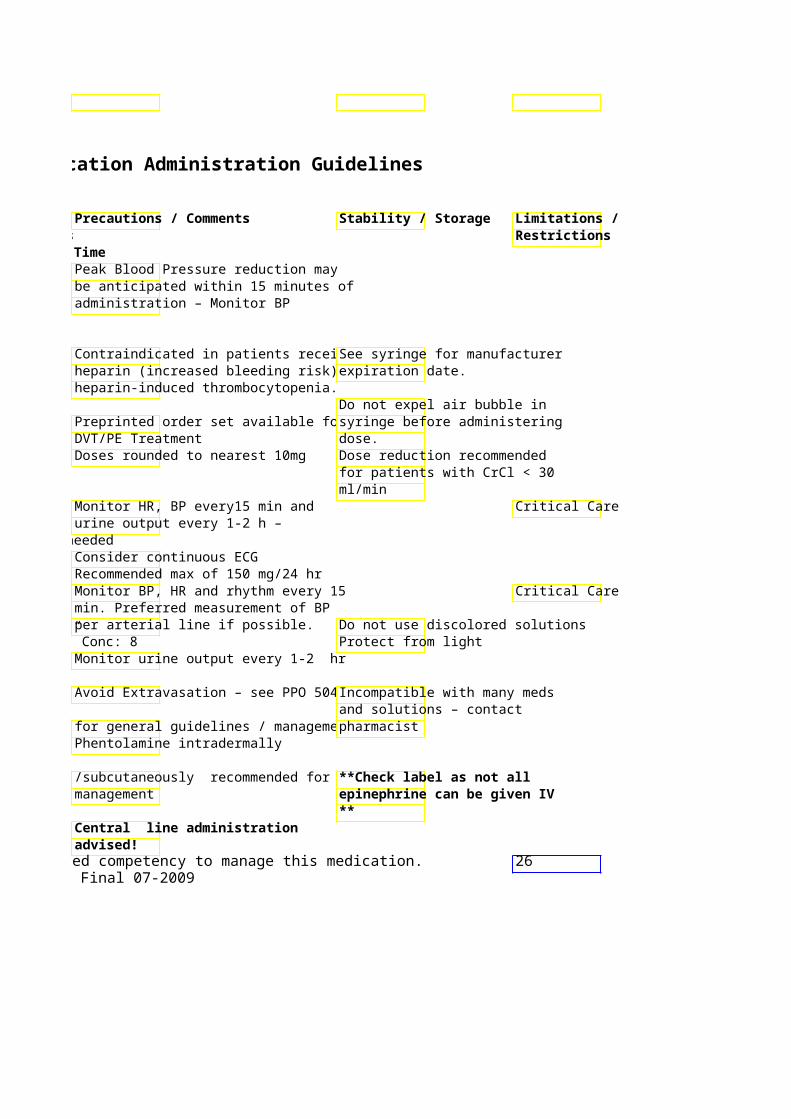
Peak Blood Pressure reduction may be anticipated within 15 minutes of administration – Monitor BP
Contraindicated in patients receivingSee syringe for manufacturer heparin (increased bleeding risk) an expiration date. heparin-induced thrombocytopenia.
Do not expel air bubble in Preprinted order set available for syringe before administering DVT/PE Treatment dose. Doses rounded to nearest 10mg Dose reduction recommended
for patients with CrCl < 30 ml/min
Monitor HR, BP every15 min and Critical Care urine output every 1-2 h –
repeated q5-10min as needed Consider continuous ECG Recommended max of 150 mg/24 hr Monitor BP, HR and rhythm every 15 Critical Care min. Preferred measurement of BP per arterial line if possible. Do not use discolored solutions
System “Concentration” Conc: 8 Protect from light Monitor urine output every 1-2 hr
Avoid Extravasation – see PPO 5046 Incompatible with many meds and solutions – contact
for general guidelines / managementpharmacist Phentolamine intradermally
/subcutaneously recommended for **Check label as not all management epinephrine can be given IV
** Central line administration advised!
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 26Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Epoprostenol 0.5 and 1.5 NO Continuous infusion requ(Flolan) mg vials Upon admission, patient
for converted from home infVasodilator/ reconstituti to hospital IV infusion pump. Prostaglandin on
Usual starting dose is 2Kg/min. Titrate per physician orders.
**Metro: preprinted oavailable – use advise
Eptifibatide 2mg/ml – Yes, Continuous Infusion – (Integrelin) 10ml Vial 180mcg/Kg bolus Acute Coronary Syndrom
for loading over 1-2 minutes. 0.5 - 2 mcg/Kg/min (max 15 mg/hr) Antiplatelet IIb/IIIa doses & ACS – x 1
0.75mg/ml PTCA - Repeat System Standard Conc: 100ml Vial bolus in 10 min Premix (0.75 mg/ml) for maintenance infusions
Ertapenem 1 Gm vial NO 1 Gm/50 ml NS (INVanz) Infuse over 30 min
May be given IM Antibiotic/ Carbapenem
Erythromycin 500 & NO Up to 500 mg in 100ml 1000mg 501 - 1000 mg in 250ml
Antibiotic/ Macrolide vials (Max Concentration = 500mg/100ml NS) Infuse all doses over 60
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
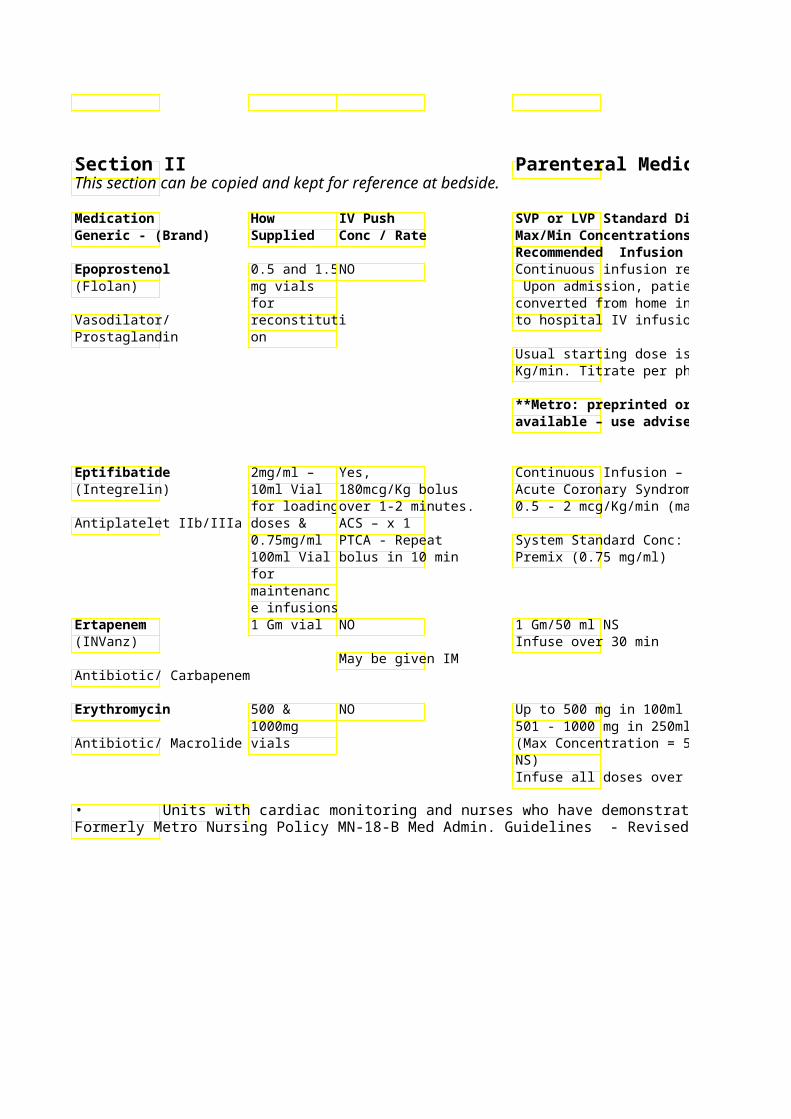
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Avoid interruptions of infusion Dilute only with * See footnote ( half-life = 6 min) – loss of dis manufacturer-supplied control could lead to death diluent!
to hospital IV infusion pump. Monitor for hypotension, flushing, headache, N/V, anxiety & chest pain.Protect from light
Kg/min. Titrate per physician orders. A “Flolan Dosing Weight” is ** Metro: Bag must be established and used throughout thechanged every 8 hr even if patient’s therapy. The “Flolan Dosingbag not empty **Weight” should be used when calculating infusion rate. Pre-printed order set available for ACS/PTCA Compatible with heparin
0.5 - 2 mcg/Kg/min (max 15 mg/hr) Monitor for bleeding. Use vented set to administer Recommended to decrease infusion undiluted eptifibatiderate to 1 mcg/kg/min for pt with SrCr 2 –4 mg/dl
Caution with PCN allergycheck Stable 6 hr at room tempRestricted allergies hr refrigerated – use wit indications per
after removal from refri P&T Dose reduction recommended for CrCl < 30 ml/min Stable in NS only! Slow infusion rate if vein irritation Stable 24 hours refrigerated, 8 occurs hours at room temp after
(Max Concentration = 500mg/100ml dilution Avoid Extravasation – see PPO 5046 for general guidelines / management
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 27Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
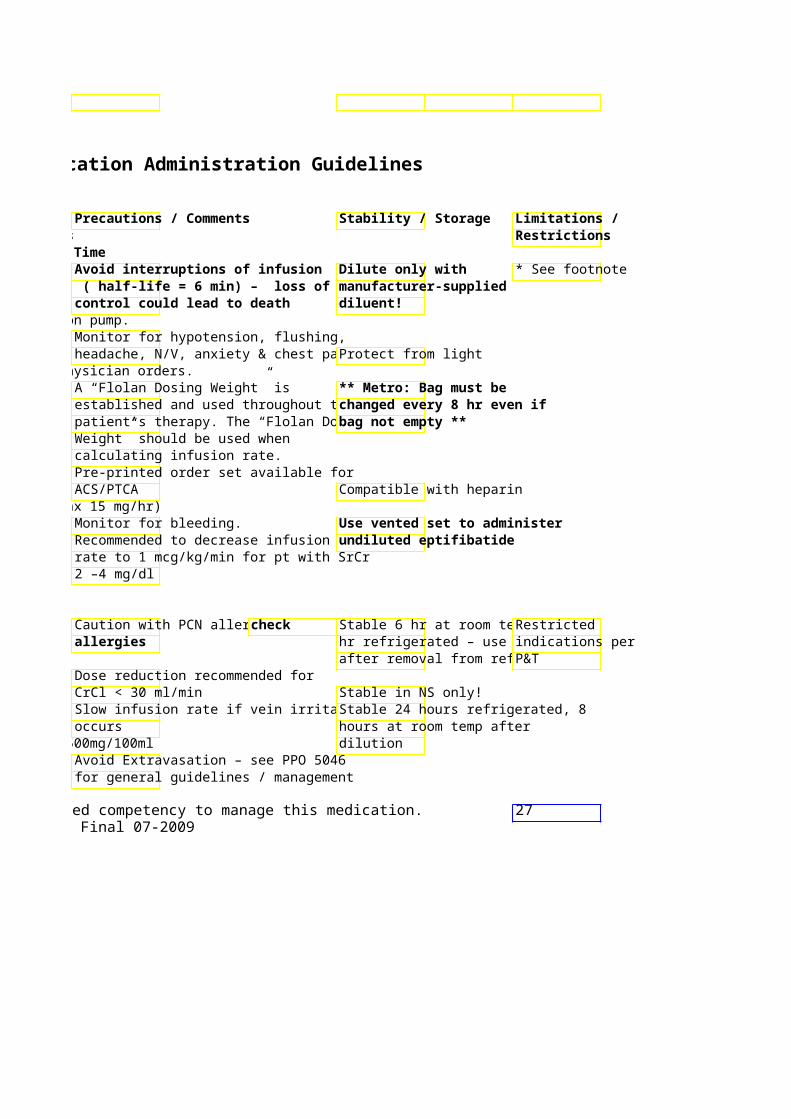
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Erythropoietin, 2,3,4,10, 20Yes Dilution not advised epoetin alfa & 40 Give SQ or IV (Epogen, Procrit) thousand Push over 30-60 Chronic Renal Failure: Recommended
units/ml seconds initial dose: 50 – 100 univials 3 times per week. SQ m
Red cell stimulating 20000 administered weekly hormone unit/2 ml
Multi-dose vial
Esmolol 10mg/ml Yes, System Standard Conc: (Brevibloc) 10 ml Vial IV push loading NS Premix (10mg/ml)
doses (500 Cardiovascular/ Beta- Premix: 2.5 mcg/Kg) over 60 System “Concentrated” Conc:
2000mg/100 ml NS (20 mg/ml) Blocker Gm/250 ml seconds Central Line Only
Dose range: 50 – 200 m(Titrate in 50 mcg/Kg/min increments every 5 min to desired r
Onset: immediate Peak response: 5 min Duration: 10-30 min Half-life: 9 min
Esomeprazole 20 mg, 40 Yes, System Standard Concent(Nexium IV) mg vials 5 ml over 3 mg/ 250 ml NS (0.32 mg
minutes Usual dose for GI bleeds: 80 mg (in
Proton Pump Inhibitor Reconstitute vial 100ml NS) bolus over 30 minutes then with 5 ml NS 8 mg/hr continuous infusion
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
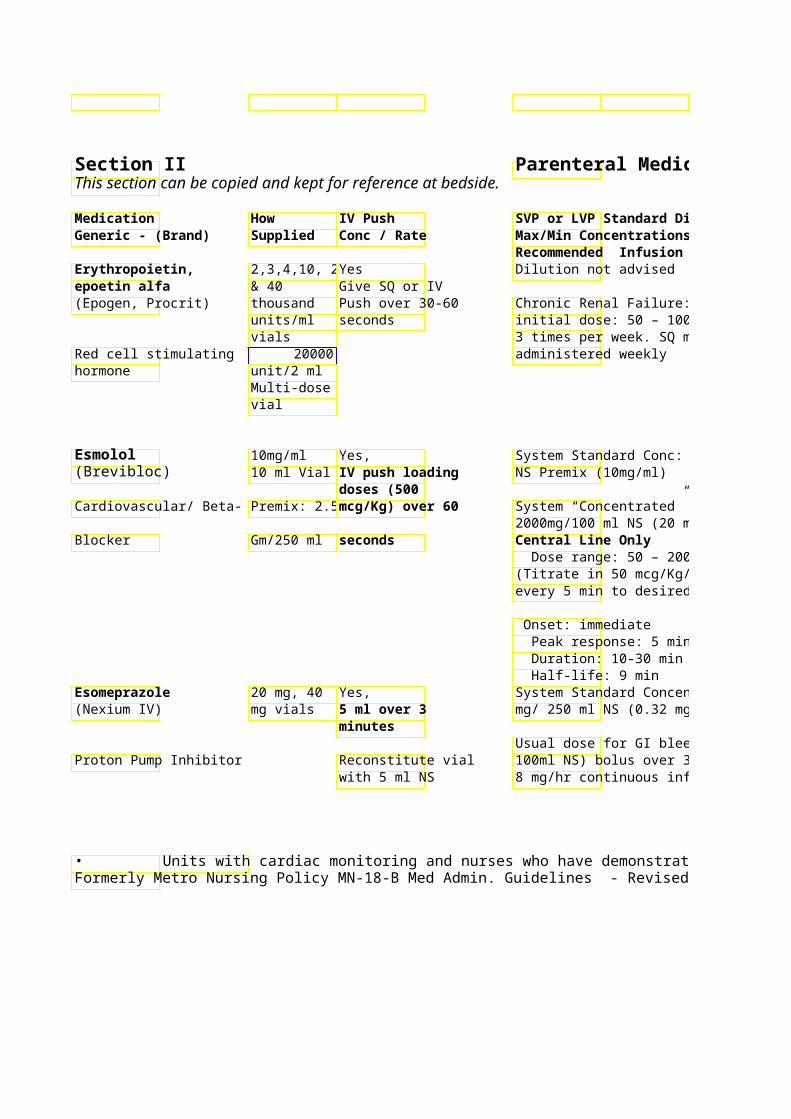
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor for hypertension, fever, Do not shake product orCheck headache, arthralgias & nausea transport via tube syste hemoglobin prior
Chronic Renal Failure: Recommended to administration. Goal: Refrigerate vials See EMAR for Hemoglobin <10 in chemotherapy- Hold parameters. induced anemia. Notify physician Hemoglobin < 12 mg/dl in chronic prn for dose kidney disease / other indications. reduction or
interruption based on most recent hemoglobin.
Monitor BP and Heart Rate/Rhythm Telemetry / every 5-15 min during dose initiation Critical Care and titration. Advised
System “Concentrated” Conc: * See footnote 2000mg/100 ml NS (20 mg/ml)
Doses > 200 mcg/kg/min do not have increased benefits
(Titrate in 50 mcg/Kg/min increments nd rdContraindications: 2 /3 degree AV block, sinus bradycardia, cardiogenic shock
Continuous infusion duration should Reconstitute vial with 5 ml NS. not exceed 72 hr Use within 1 hour of
reconstitution. Usual dose for GI bleeds: 80 mg (in 100ml NS) bolus over 30 minutes then Diluted solution stable for 12 8 mg/hr continuous infusion hours (NS)
Do not administer with other medications/fluids – check with pharmacist for compatibility information
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 28Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
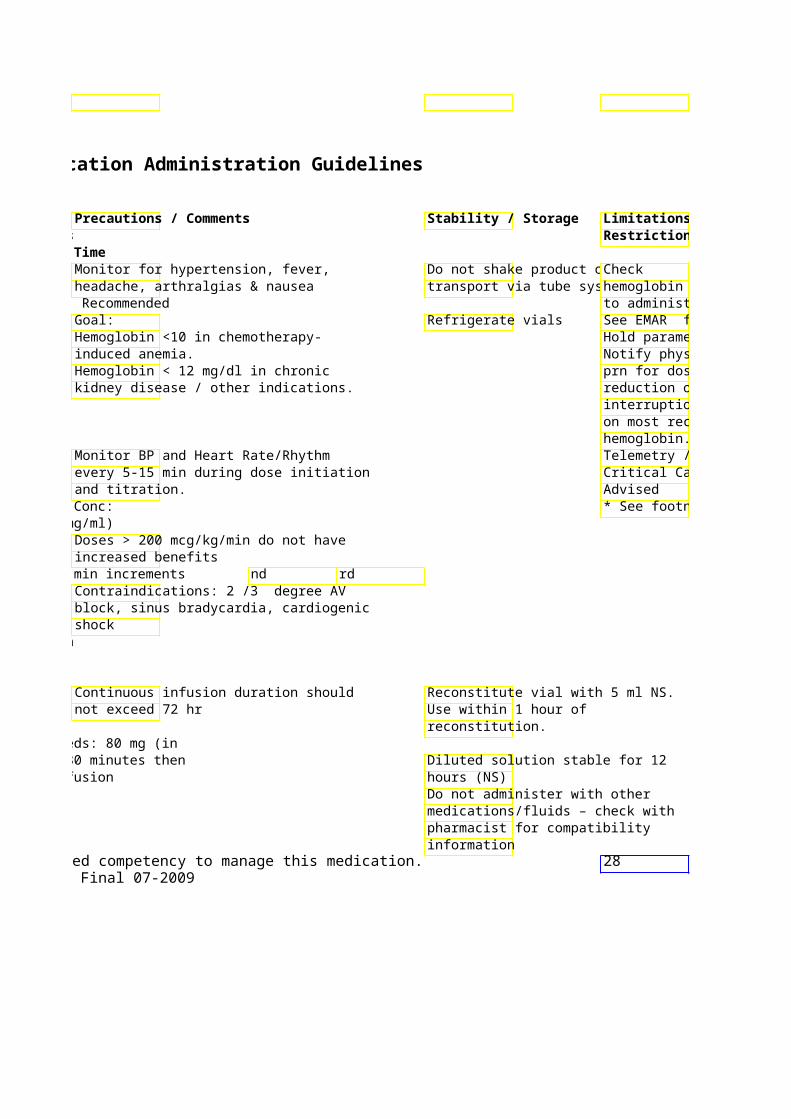
Limitations / Restrictions
hemoglobin prior to administration. See EMAR for Hold parameters. Notify physician prn for dose reduction or interruption based on most recent hemoglobin. Telemetry / Critical Care
* See footnote
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Estrogens, Conjugate25 mg vial Yes, Not advised (Premarin IV) 5mg/min at
5 mg/ml conc. Usual intermittent dose -slow IV push Hormone - Estrogen Abnormal uterine bleedi
Uremic bleeding: 0.6mg
Ethacrynic acid 50 mg Vial Yes, Slow IV push recommen(Edecrin) Give over > 3 min
Max of 100 mg Diuretic per single dose
Etidronate Disodium 50mg/ml – NO Usual dose for treatment(Didronel IV) 6ml Amp hypercalcemia: 7.5 mg/K
(300mg) days Inhibitor of bone Diluted in 250ml NS – inmetabolism minimum of 2 hours
(3 mg/ml max concentrat
Etomidate 2 mg/ml Yes NO 10 ml vial, 0.3 mg/Kg over
**HIGH ALERT 20 ml 15-60 seconds MEDICATION** vial/syringe
Sedative
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
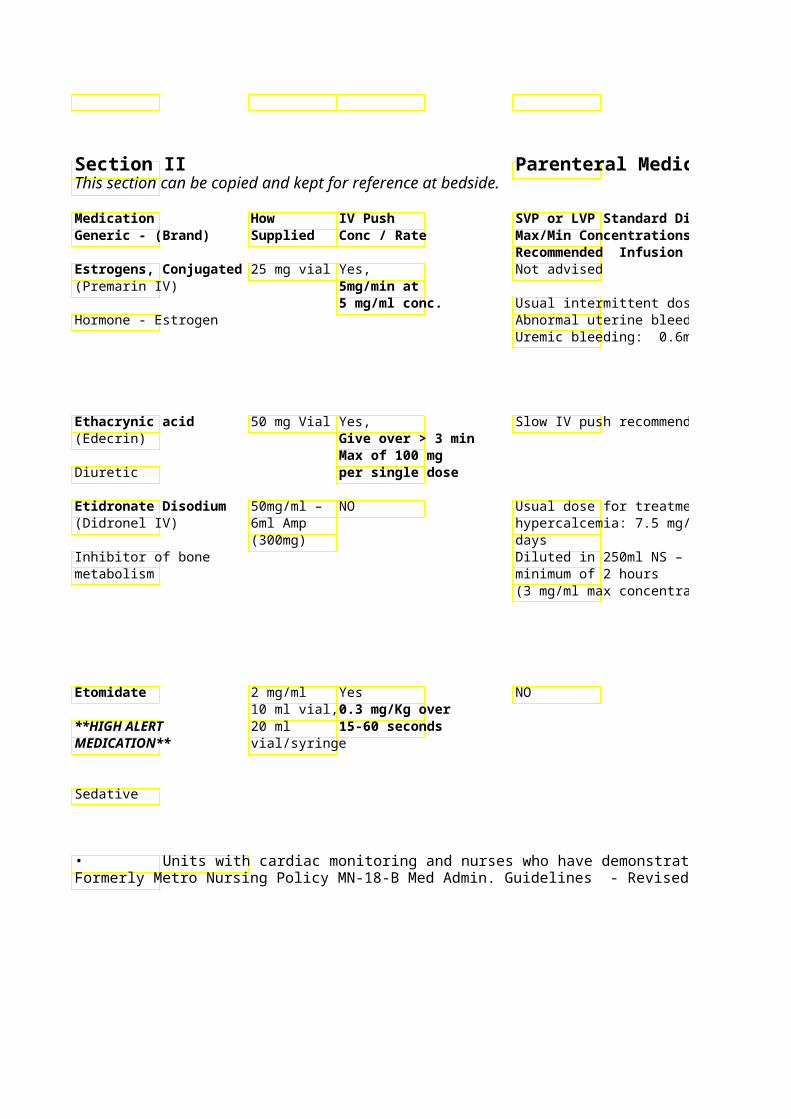
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Slow rate of administration if Refrigerate before and body/facial flushing occurs following reconstitution.
Usual intermittent dose -slow IV push Do not use darkened solution. Used for treatment of abnormal uterine bleeding. Also used for Do not shake vial!! uremic bleeding. Do not mix with other
solutions/medications ** Verify dose to be given. Discard vial after drawing up correct dose. ** Slow rate of administration if vein irritation occurs and/or consider different IV site
No IM/SC administration! Temporary taste loss not uncommon following IV etididronate
Adequate hydration recommended prior to administration Too rapid administration may lead to renal insufficiency Dose decrease recommended in pt with SrCr 2.5 – 4.9 mg/dl. Not recommended in pt with SrCr > 5 mg/dl Monitor BP, HR and RR Critical Care
Pain at injection site common Transient myoclonic movement/seizure-like activity may occur.
Nausea/vomiting common Etomidate has no analgesic properties.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 29Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Exenatide Pre-filled No NO (Byetta) syringes
SC **HIGH ALERT administration MEDICATION** ONLY
Incretin mimetic/adjunctive therapy for diabetes Factor VIIa - 1mg, 2mg Yes, give over 2Usual single dose: 15 - Recombinant & 5 mg min (Novoseven) vials Continuous infusion may be done –do
Reconstitute with NOT further dilute FactorBlood factor diluent provided to into running IV line
final concentration of 1mg/mL
Factor 8 – Human Vials – size Yes – Slow IV VonWillebrand Disease ( Humate-P ) varies push at rate not to
based on exceed 4mL/min Usual Dose: 40-80 IU/kg*dose; for major bleeds or invasive
pooled procedures, continue wiplasma
doses of 25-30 IU/kg Q8- 12h source
Infusions: Use diluent & fprovided with product. No additional (inline) filtration or dilut
recommended. Factor 8 – 250, 500, Yes - Slow IV Hemophilia A – Usual Dose:Recombinant 1000,2000 push over 5-10min IU/kg initial dose; for ma(Helixate) units/vial invasive procedures, con
IU/kg repeated Q12h
Factor 9 – 250, 500, Yes - Slow IV Hemophilia B – Usual Dose:Recombinant 1000,2000 push over 5min IU/kg to achieve a target(BeneFIX) units/vial of 70-80%; Repeat dose
intervals at a dose of 40
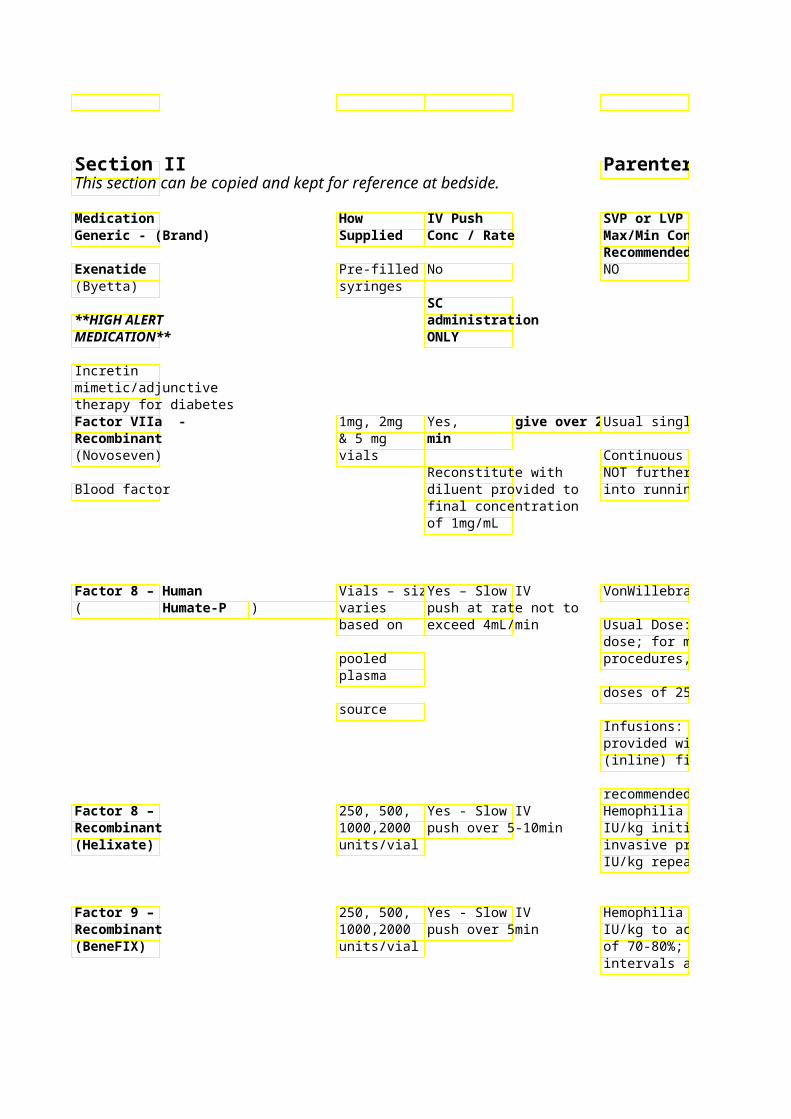
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
SVP or LVP Standard DPrecautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Not for use in Type 1 diabetics or for Non-formulary. the treatment of diabetic ketoacidosiRefrigerate Patient may use
Do NOT mix with insulown supply if Common side effect: nausea deemed necessary
& appropriate by prescriber.
Usual single dose: 15 - Monitor Coagulation profile, PTT/PT Vial stable at room temperature Hgb/Hct, platelets for 2 years prior to
Continuous infusion may be done –do reconstitution. NOT further dilute FactorMay increase risk of thrombotic into running IV line events Once reconstituted -
administer within 3 hours. Non-emergent indications: Confirm final coagulation results and Factor VIIa order with prescriber prior to administration.
VonWillebrand Disease ***Caution: Product is labeled in Use diluent provided Factor 8 uni and von Willebrand
Usual Dose: 40-80 IU/kg*factor:Ristocetin Cofactor (VWF:RCo)Stability: 24hrs room temp or dose; for major bleeds or invasive procedures, continue wi units. In VWD disease dose is basedrefrigerated
VWF:RCo content. *** doses of 25-30 IU/kg Q8- 12h
Product is NOT typically used for Infusions: Use diluent & fHemophilia A provided with product. No additional (inline) filtration or dilut **Use higher dose for patients with
type 2 and 3 VWD recommended. Hemophilia A – Usual Dose:Multiple products in Hemophilia A Use diluent provided IU/kg initial dose; for maavailable – this may be used as a Stability: 3hrs – invasive procedures, con“universal product” for urgent Stability may be extended on a IU/kg repeated Q12h reconstitution. Life-threatening case-by-case basis –
bleeds/ Major surgery: Target Factorconcentrations / dilutions must 8 levels of 80-100%. be considered.
Hemophilia B – Usual Dose:Decreased Factor 9 recovery requireUse diluent provided IU/kg to achieve a targethigher relative dose to achieve targeStability: 3hrs of 70-80%; Repeat doseFactor 9 levels. Stability may be extended on a intervals at a dose of 40Dose = Target level x Pt wt x 1.3 case-by-case basis. –
concentrations / dilutions must be considered.
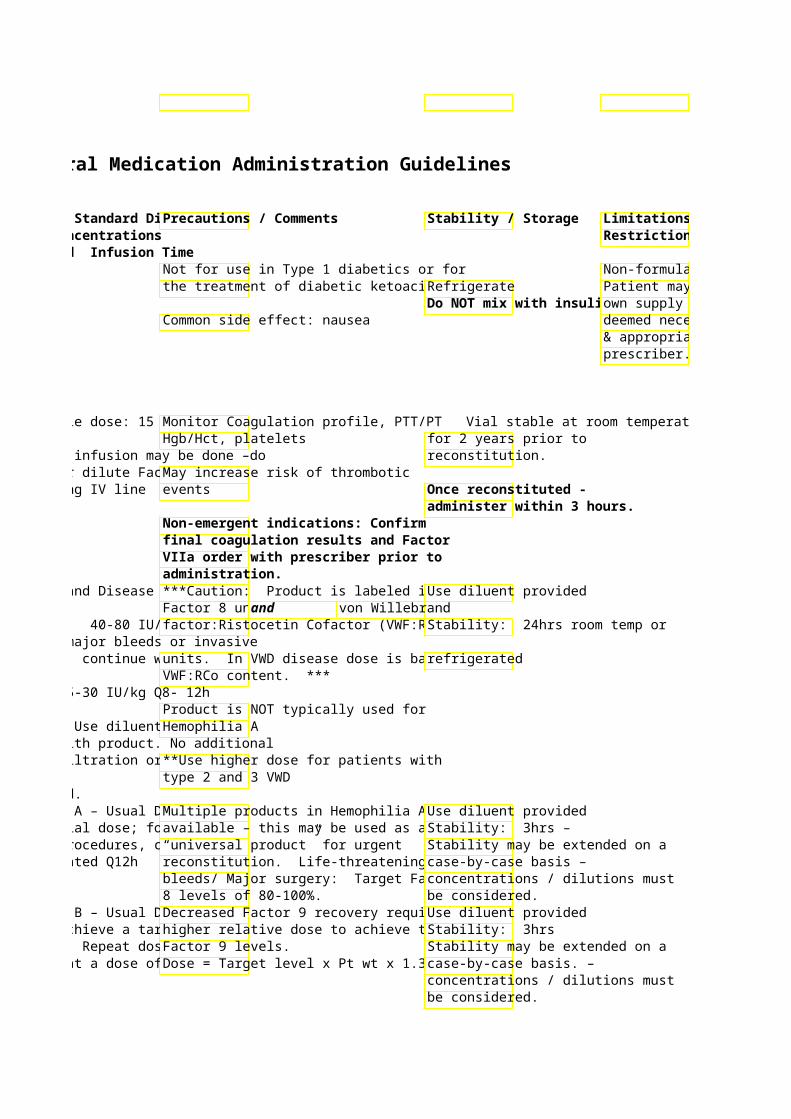
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 30Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Limitations / Restrictions
Non-formulary. Patient may use own supply if deemed necessary & appropriate by prescriber.
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Factor 9 Complex – Vial sizes Yes – 5-10mL/min Warfarin reversal in lifeHuman vary based Do not exceed bleeds – Usual dose: (Profilnine SD) on pooled 10mL/min – rates 50 units/kg or 4,000 unit
plasma in excess of this Doses may be repeated source may result in response (total dose ran
vasomotor 100units/kg) reactions.
Famotidine 10mg/ml – Yes, IV Push preferred (Pepcid) 2 & 4 ml 10mg/ml – give Intermittent infusion:
Vial over 1 min 20mg/50 ml NS – infuse over 15 min H2 Receptor Antagonist
Dilute with 5-10 ml NS or D5W
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
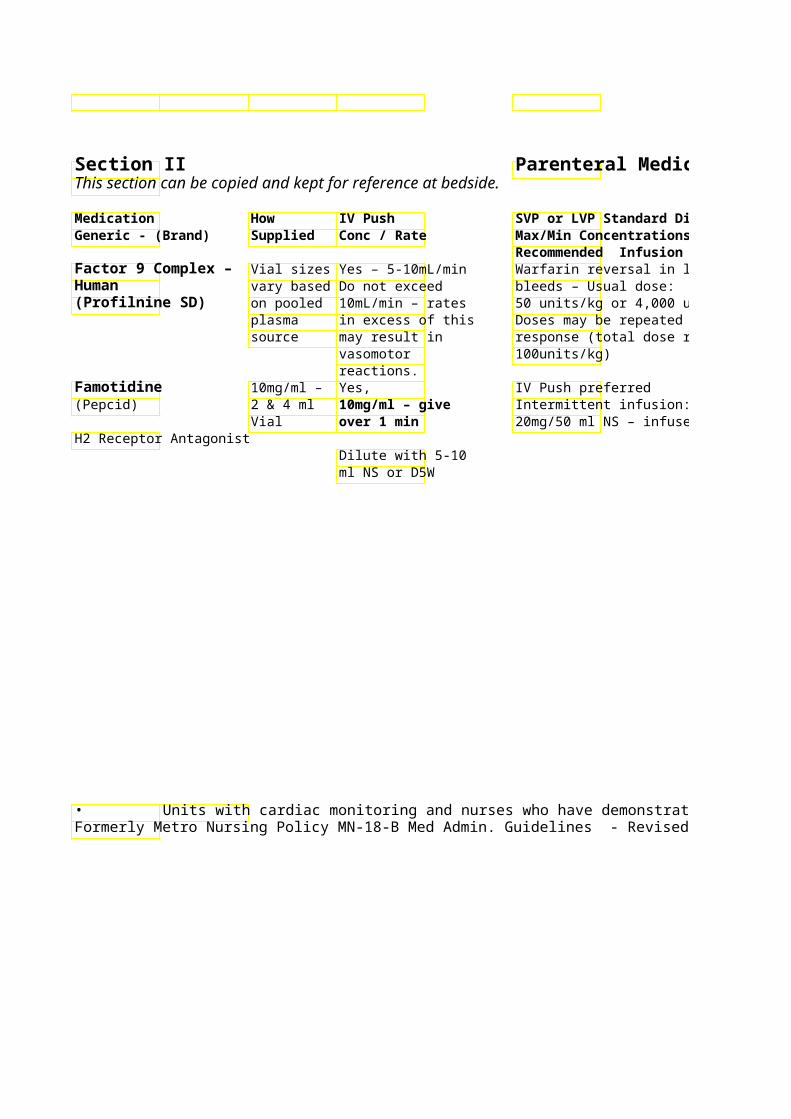
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Product FDA approved for Use diluent provided (SW) Hemophilia B. Contains Factors II, VII, IX, X – In life-threatening bleeds: coadministration with vitamin K & additional source of factor 7 (FFP or NovoSeven) is recommended. Dose reduction recommended for pt with CrCl < 50 ml/min
20mg/50 ml NS – infuse over 15 min
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 31Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
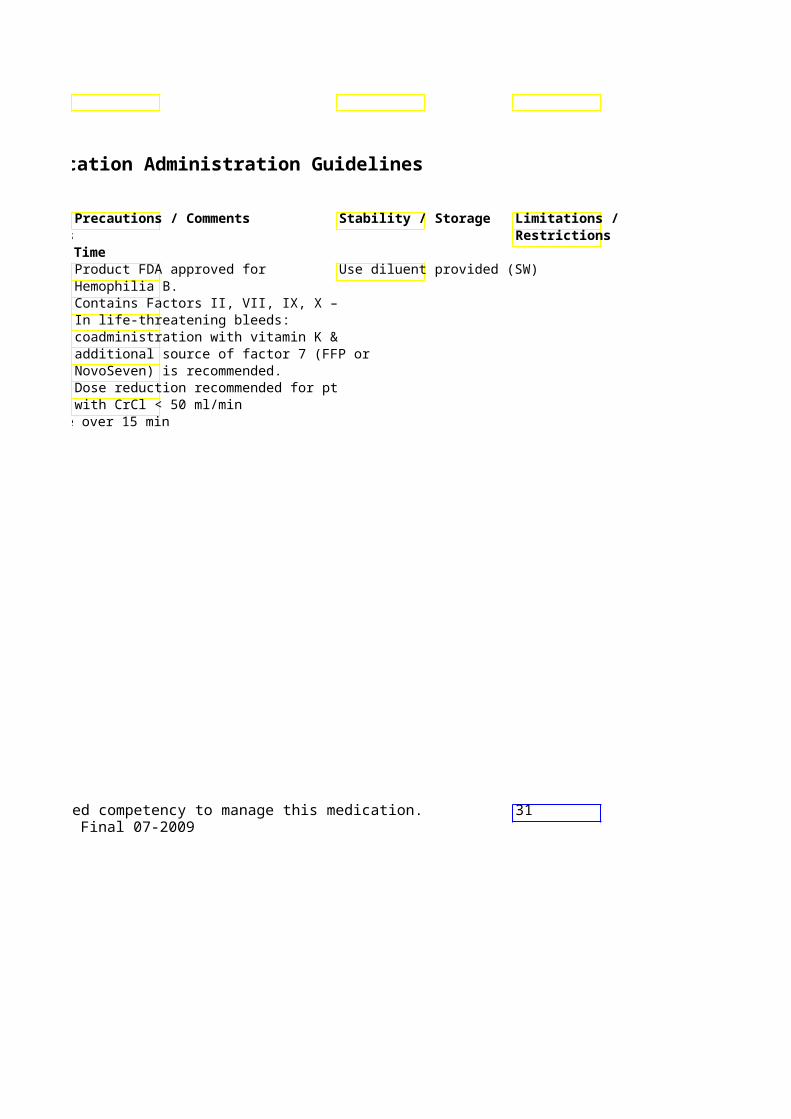
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Fat Emulsion 20% Yes Start continuous intra(Intralipid, Liposyn) 500 ml 1.5 mL/kg IV at 0.25 mL/kg/min upon
bag bolus over 1 of first IV bolus. Local anesthetic minute (for toxicity suspected local Increase infusion to 0.5 mL/kg/min throughout fat emul
anesthetic if adequate circulationtoxicity); restored/BP declines after second consider bolus. repeating bolus up to two more Continue lipid infusiontimes q 3-5 hemodynamic stabilityminutes if recovery may take longer than an adequate hour. circulation not restored A total cumulative dos
mL/kg has been reco
Fenoldopam 10 mg/ml – NO Continuous infusion re(Corlopam) 5ml Amp Begin at 0.05 mcg/Kg/min
up by 0.05mcg/Kg/min eAntihypertensive minutes to desired effec
Usual dose range: 0.05 – 1.6 mcg/Kg/min
System Standard Conc: NS (40 mcg/ml) System “Concentrated” mg/100 ml NS (100 mcg/
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
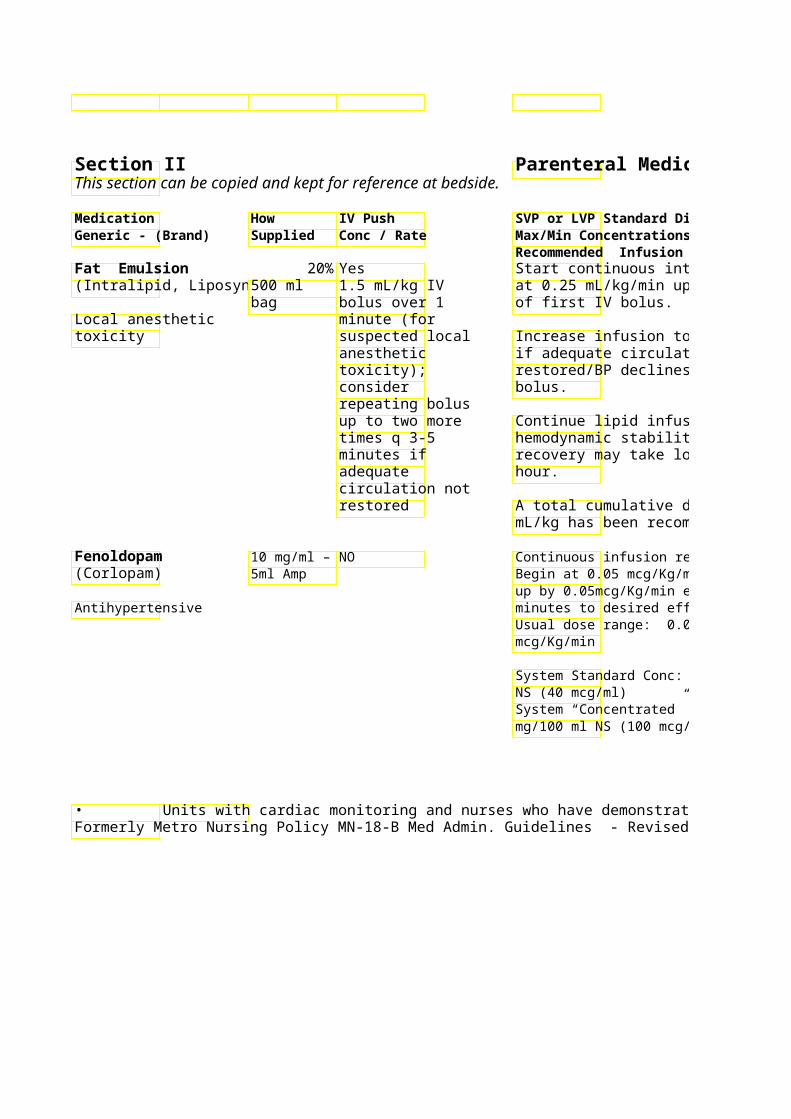
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Do not use propofol as lipid Stored at room temperature. None source.
Recommended storage in ACLS must be continued L&D, OR, and other areas
Increase infusion to 0.5 mL/kg/min throughout fat emulwith high volume use of administration! local anesthetics.
restored/BP declines after second Achieving continuous infusion rate > 1200 ml/hr (0.25 mL/kg/hr for a 80 kg patient) may require infusion via multiple lines.
recovery may take longer than an ** No standard dosing has been established – contact Poison Control and/or see www.lipidrescue.org for further information **Monitor BP (preferably via arterial Critical Care line if possible), HR q 15 min during Incompatible with many dose initiation and titration. medications/solutions – contact Half-life = 5 min. Effects quickly pharmacist
Usual dose range: 0.05 – 1.6 reversed with D/C of drip Doses > 1.5 mcg/kg/min rarely required
Tachycardia may occur if drug started at rate > 0.1 mcg/kg/min or if titrated too quickly
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 32Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
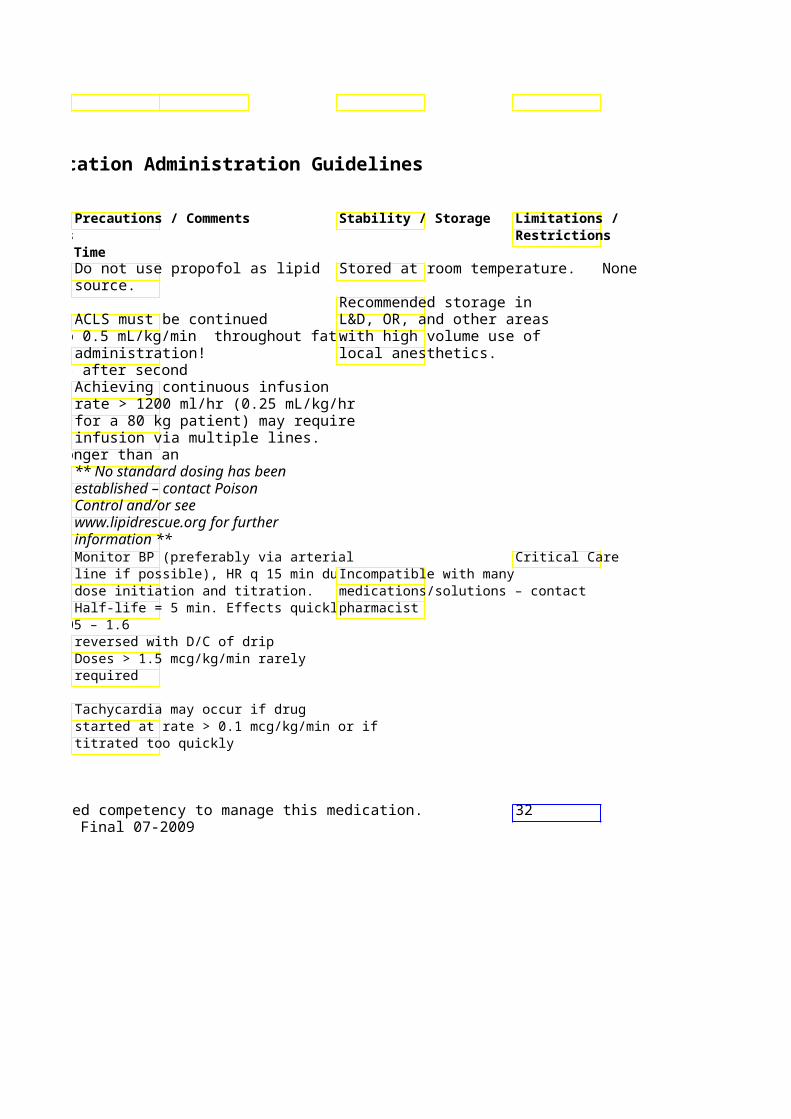
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time FentaNYL 50 mcg/ml Yes, Continuous infusion or PCA (Sublimaze) – various Slowly over 3 – 5 recommended
sized minutes **HIGH ALERT amps/vials Bolus dose range: 10–30 mcgMEDICATION** Continuous IV dose range: 20 – 60
mcgNarcotic analgesic
System Standard Conc for continuouinfusion: 1250 mcg/250 ml NS Premi(5 mcg/ml) System “Concentrated “ Conc: 1000 mcg/ 100 ml NS (10 mcg/ml)
Ferrous Gluconate Amps Yes, Intermittent infusion: Complex 62.5mg/5 Max 12.5mg/min 62.5 mg – 125 mg/100 ml NS (Ferrlecit) ml Infuse over 30 - 60 min
Give 62.5 mg over Iron Supplement 5 min Doses greater than 125 mg require
Give 125 mg over dilution 10 min IV push not Max dose per Metro P&T = 250 mg
recommended for doses > 125 mg
Filgrastim 300mcg/ 1 SQ preferred Intermittent infusion: (Neupogen) ml 300mcg/18ml D5W
480mcg/1.6 480mcg/25ml D5W White cell stimulating ml Vials Infuse over 30 min hormone Fluconazole Premix NO Intermittent administration (Diflucan) 200mg/200 recommended
ml & Infuse at max rate of 200 mg/hour Antifungal 400mg/400
ml • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
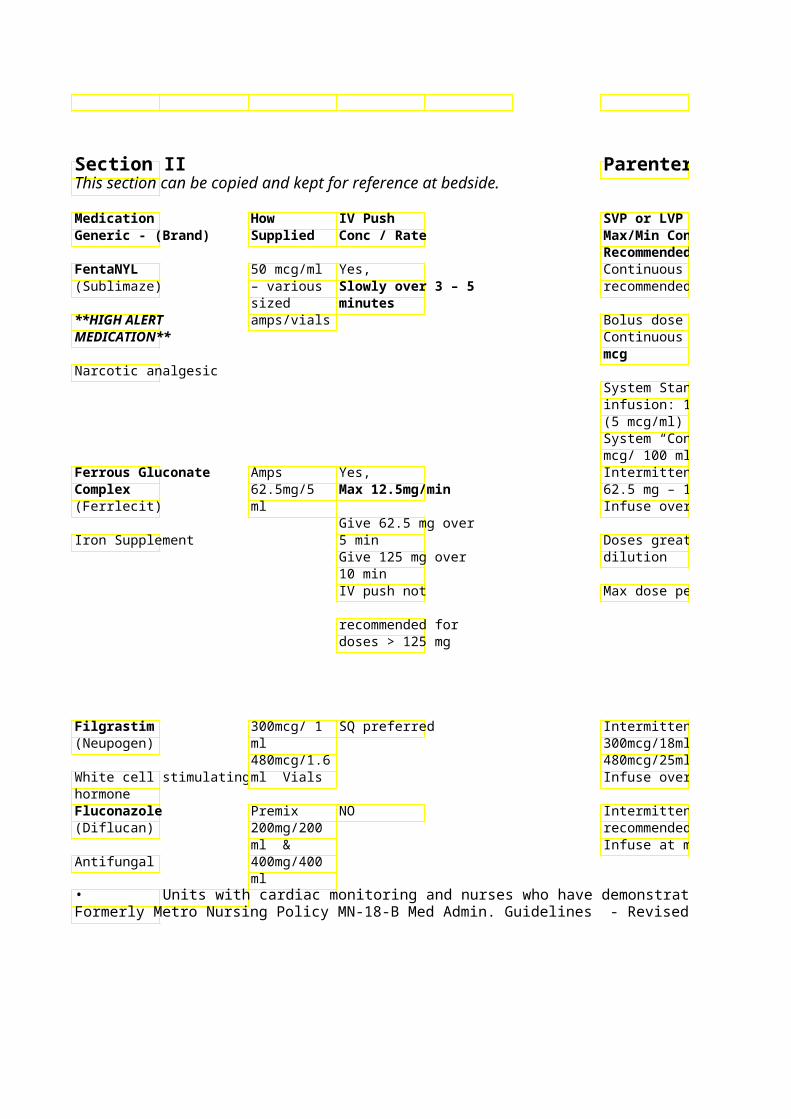
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Max/Min Concentrations Recommended Infusion Time Continuous infusion or PCA Monitor BP, RR recommended
Too rapid administration Bolus dose range: 10–30 mcg may cause respiratory Continuous IV dose range: 20 – 60 depression/distress
/hr Reverse effect with naloxone
System Standard Conc for continuou(Narcan) infusion: 1250 mcg/250 ml NS PremiOptimal dose determined by patient (5 mcg/ml) response System “Concentrated “ Conc: 1000 mcg/ 100 ml NS (10 mcg/ml) Intermittent infusion: Test dose not necessary 62.5 mg – 125 mg/100 ml NS Unopened ampules good until Infuse over 30 - 60 min Monitor vital signs (BP) includin expiration dating from
orthostatic BP – manufacturer Doses greater than 125 mg require
Metro: For Outpatient Admin - Doses < 250 mg – monitor patient
Max dose per Metro P&T = 250 mg for 1 hour post-infusion per P&T Doses of 250 mg – monitor patient for 2 hours post- infusion per P&T
May cause hypotensio or hypertension, chest, back or groin pain. Symptoms typically resolve 1-2 hours after infusion completed.
Intermittent infusion: Refrigerate 300mcg/18ml D5W 480mcg/25ml D5W Do not shake product or Infuse over 30 min transport via tube system
Dilute in D5W only!! Intermittent administration recommended Dose reduction recommended for Infuse at max rate of 200 mg/hour CrCl < 50 ml/min
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
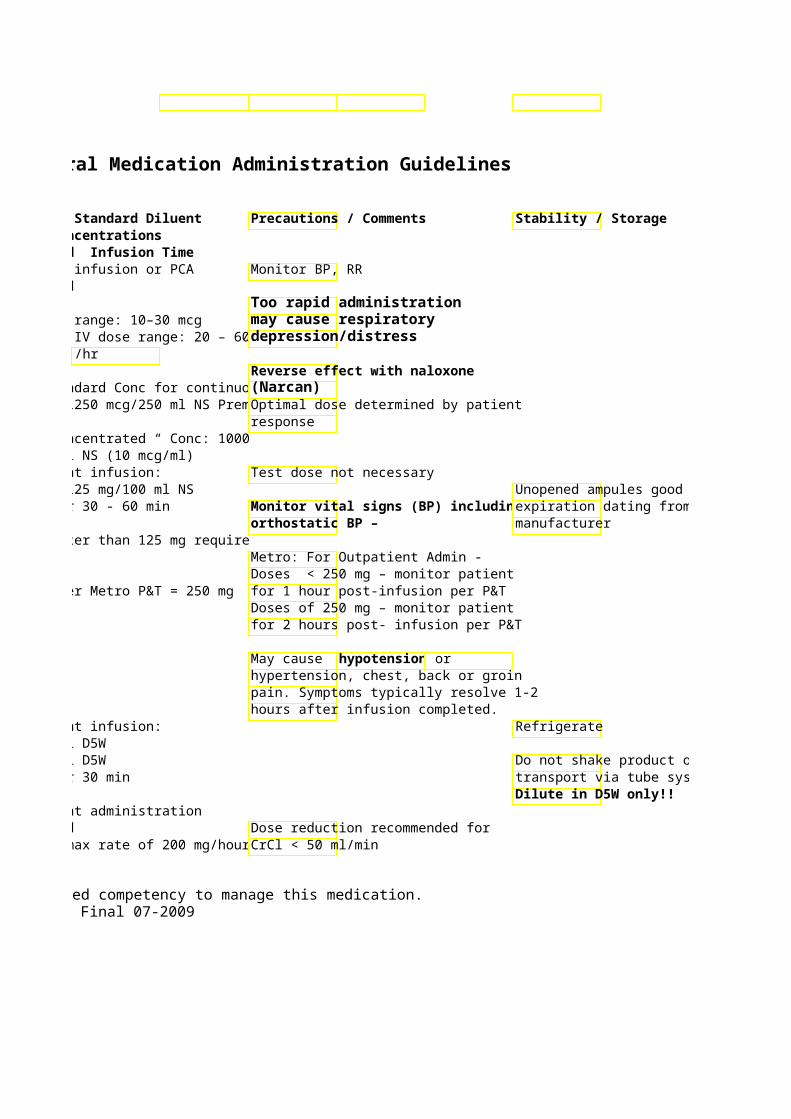
Limitations / Restrictions
Metro: If PCA ordered, mandatory order set must be used
Unopened ampules good until
Metro: max dose per infusion is 250 mg per P&T
Do not shake product or transport via tube system
33
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Flumazenil 5 & 10 ml Yes, To reverse benzodia(Romazicon) vial 0.1 Give rapidly over (BZD) effe – intermittent
mg/ml 15-30 seconds administration recomme**HIGH ALERT preferably into IV repeated every 60 secMEDICATION** large vein with of 3mg/hr.
running IV **Reversal Agent** Titrate to response usingBenzodiazepine doses. Most patients res
doses between 1 & 3 mg (BZD) antagonist Folic Acid 5mg/ml – Yes, Common component in “
10 ml vial Give over 1-2 min Vitamin/Nutritional May dilute with NS or Dsupplement May be given SQ, administered continuousl
IM peripheral or central line
Fomepizole 1Gm/ml – NO Intermittent Infusion – (Antizol) 1.5 ml vials 15mg/Kg load then 10mg
12h x 4 then 15mg/Kg evEthylene glycol and serum ethylene glycol <20mg/dL and / Methanol Antidote or resolution of acidosis
Dilute with 100ml NS and30 minutes
Fondaparinux Pre-filled NO (Arixtra) syringes
Administer SC Anticoagulant only! Do NOT
give IM!
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Irritant, avoid infiltration – intermittent
Elim half-life = 60 min – much less Monitor BP, HR, RR than typical BZD’s and re-sedation following initial respois& not unusualMay unmask BZD controlled seizures or precipitate BZD withdrawal in
doses between 1 & 3 mg chronic BZD users. Dilution recommended for > 5 mg Protect from light
Methanol Poisoning: Cofactor in elimination - Higher dose folic acid (50-75mg) administered q4h x 24h or until resolution of acidosis. Solution may solidify at temps Monitor ethylene < 77°F, run under warm water or hold glycol or in hands to liquify methanol serum
serum ethylene glycol <20mg/dL and / Dialyzable – dosing interconcentrations Monitor for signs of allergic reaction should be increased to every 4 shortness of breath, rash, hives, andhr during hemodialysis pruritus. Do not wait for results of methanol/ethylene glycol blood levels to initiate therapy. Administer SC only! Do NOT giveSee syringe for manufacturer IM! expiration date.
Contraindicated per manufacturer inDo not expel air bubble in patients w/ CrCl < 30 ml/min or bodysyringe before administering weight < 50 kg dose.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 34Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / RateMax/Min Concentrations
Recommended Infusion Time Foscarnet 24 mg/ml NO Peripheral Line: Must be diluted to 1(Foscavir) in 250 and mg/ml with NS or D5W
500ml Antiviral bottles Central line: May be given undiluted.
Induction Dose: rate not to exceed 1 mg/kg/min (minimum of 1 hour) every 8 hours. Maintenance Dose: 90-120 mg/kg/dagiven over 2 hours
Fosphenytoin 50 mg/ml Yes May dilute to 50 or 100ml with NS. (Cerebyx) 2 & 10 ml Dilute to tot Infuse not rate not faster than
vial 10mL (or ma150mg/min Anticonvulsant concentration of
25mg/mL) aRate reduction to 75 mg/min administer recommended in elderly and pt with rate of 150 coronary heart disease.
May be given IM undiluted
Furosemide 10mg/ml Yes, Dilute doses 100-200 mg with (Lasix) vial and Doses < 10NS/D5W and administered no faster
pre-filled may be givthan 10 mg/min. Doses > 200 mg must Diuretic syringes push at mabe diluted and given no faster than 4
of mg/min. 10 mg/min
Continuous infusion usual dose range 1 – 20 mg/hr. Higher doses may be been used in kidney failure. System Standard Conc: 250mg/250ml NS (1 mg/ml) System “Concentrated” Conc: 250 mg/100ml NS (total volume 125 ml) (2 mg/ml)
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Restrictions
Adequate hydration is recommended May administer prior to and during treatment to Do NOT refrigerate undilundiluted through minimize renal toxicity solution central line only!
Central line: May be given undiluted. Dose reduction recommended in pt Incompatible with many with decrease CrCl medications and solutions,
check with pharmacist May cause thrombophlebitis
Prodrug of phenytoin - preferred product for IV/ IM administration. Refrigerate vials
Automatically substituted for phenytoin.
recommended in elderly and pt with Monitor BP/HR/RR during infusion and 30-60 min after.
Flushed feeling with IV admin. not uncommon - pruritus – commonly near groin area Do not use furosemide solutions that are yellow in color
than 10 mg/min. Doses > 200 mg must Do NOT refrigerate - may IV furosemide = 50% PO dose crystallize with refrigeration
Monitor urine output/fluid status, BP Continuous infusion usual dose range 1 – 20 mg/hr. Higher doses may be
System Standard Conc: 250mg/250ml
mg/100ml NS (total volume 125 ml) (2
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 35Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVPPrecautions / Comments Generic - (Brand) Supplied Conc / RateMax/Min Concentrations
Recommended Infusion Time Ganciclovir 500mg vial NO Dilute dose Irritant - monitor for phlebitis and (Cytovene) Reconstitut Infuse over infusion site pain
e with 10ml Antiviral NS to Final concenDose reduction recommended for Cr
10mg/ml not recommended for 50mg/ml peripheral aCl < 70 ml/min
Gentamicin 10mg/ml NO Dilute all d Aminoglycoside dosing and and D5w monitoring service available from
Antibiotic/ 40mg/ml in ** May be giInfuse over pharmacy upon physician order. Aminoglycoside 2 & 20ml undiluted
vials & intrathecallyExtended intMonitor renal function. premixed using preserinfuse over 60min minibags in free product ** various doses
Glucagon 1 mg Vial Yes, Continuous iForms precipitate when mixed with 1mg/ml ovetreatment ofchloride solutions, NO
Hormone, seconds beta-blockerwith sterile water or D5W Antihypoglycemic Agent May also be range: 1 – Tx of hypoglycemia: usually awakens
IM or SQ pt within 15 min Granisetron 1mg/ml Yes, IV Push prefGive dose 30 minutes prior to (Kytril) Vial Undiluted ovIntermittent chemotherapy to prevent
seconds Antiemetic/ 5HT3 ml NS or D5Wnausea/vomiting. receptor antagonist Haloperidol 5mg/ml Yes, Prefer inter Use with caution if cardiovascular (Haldol) Vial and Give at max rate disease is present.
syringe of 5mg/minTitrate dose to desired effect Antipsychotic/ Use only the May cause QT prolongation. Anxiolytic lactate salt of Normalization of potassium and
haloperidol for IV magnesium levels recommended. Push – NOT Monitor for hypotension and/or Decanoate salt symptoms of angina. Also, monitor for
extrapyramidal effects May be given IM
Will NOT cause respiratory depression. Contraindicated in Parkinson’s patients
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
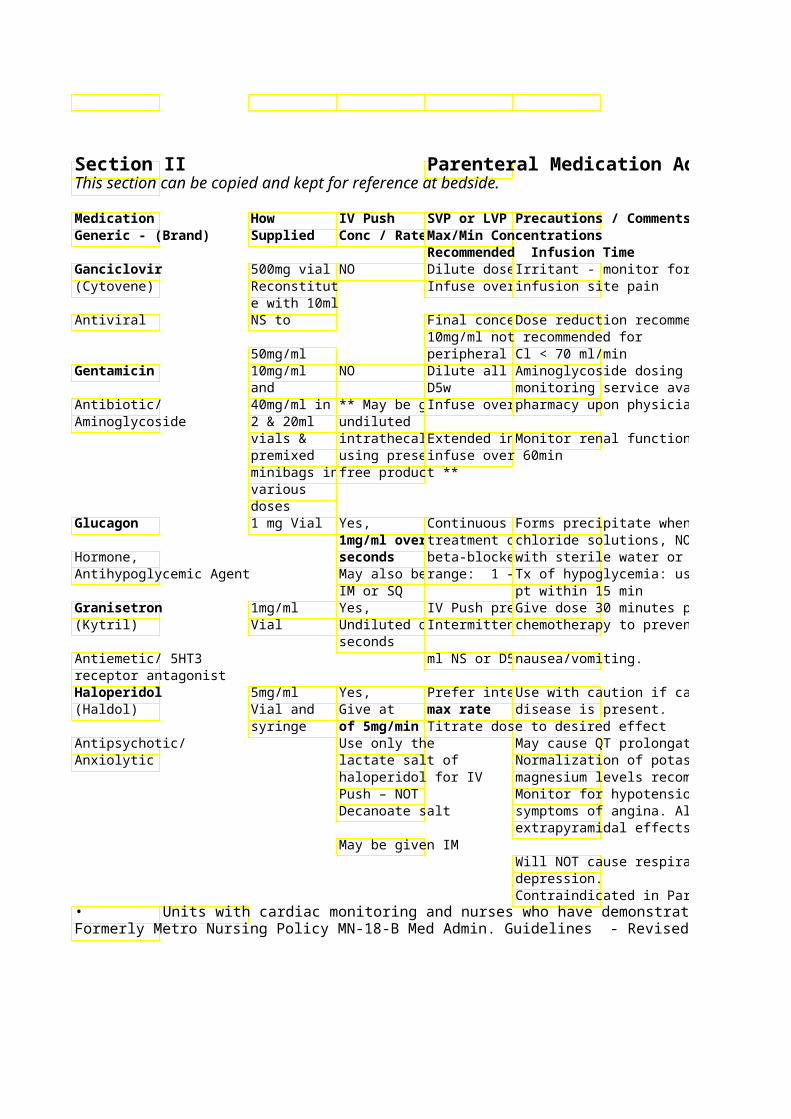
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Limitations / Restrictions
Irritant - monitor for phlebitis and Use chemotherapy precautions for preparation,
Dose reduction recommended for Cr administration & disposal
Aminoglycoside dosing and monitoring service available from pharmacy upon physician order.
Forms precipitate when mixed with Use immediately after NS – Dilute reconstitution.
with sterile water or D5W Tx of hypoglycemia: usually awakens
Give dose 30 minutes prior to chemotherapy to prevent
Use with caution if cardiovascular Recommended to flush line with at least 2 ml NS before and after med admin
May cause QT prolongation. Normalization of potassium and magnesium levels recommended. Monitor for hypotension and/or symptoms of angina. Also, monitor for extrapyramidal effects
Will NOT cause respiratory
Contraindicated in Parkinson’s patients Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 36
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Helixate See Factor 8 - Recombinant Heparin Various Yes, Continuous infusion –
concentra- All doses Standard conc: 25000 un**HIGH ALERT tions vials administered over MEDICATION** and 10-20 seconds, D5W premix (50 units/ml
syringes undiluted
Recheck concentratioPremix See specific weight-baseof vial/bag before administering dose! bag: Do NOT give IM!! protocols (PPOs) for Cardiac
50 units/ml Indications and for Treatment of 500 ml DVT/PE
Anticoagulant Hetastarch 6% solution NO Intravenous infusion pref(Hespan) in 500ml exceed 1500ml/24 hours
NS Plasma expander
Humate-P See Factor 8 - Human HydrALAZINE 20mg/ml Yes, Intermittent or continuo(Apresoline) Vials Give undiluted at a recommended Antihypertensive max rate of Exception – OB uses con
5mg/mininfusions 50 mg/500 ml D5W or fluphysician
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
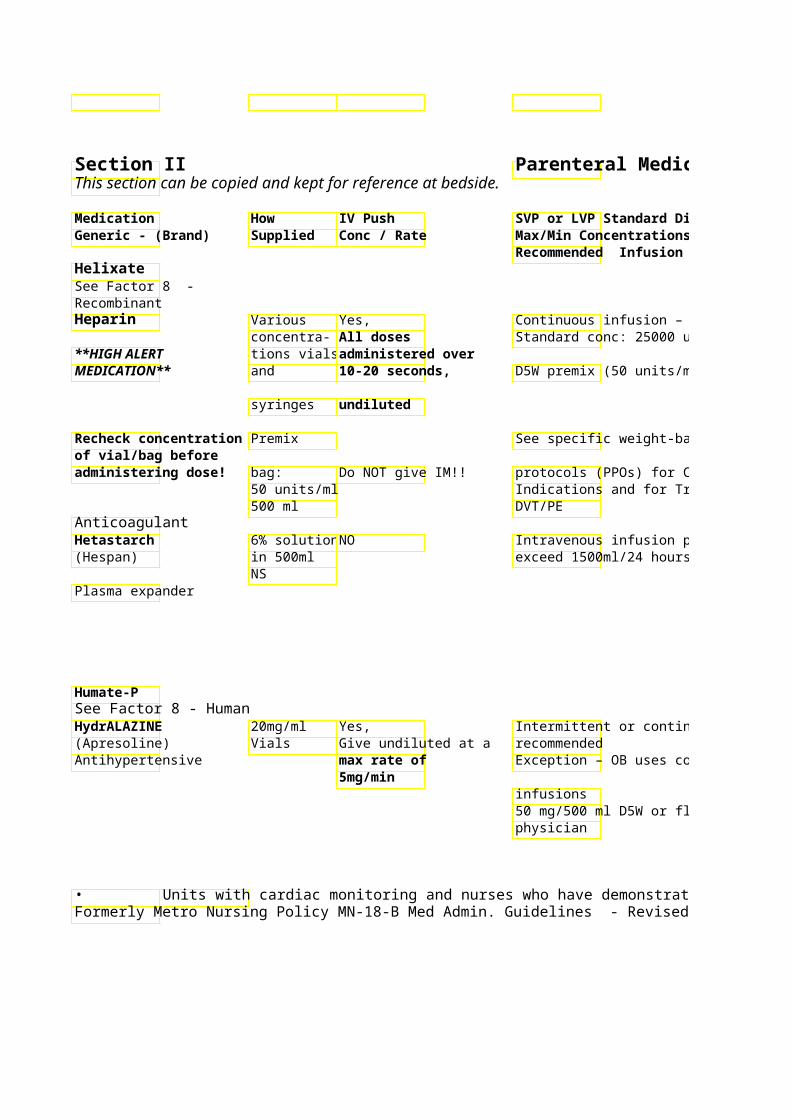
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor platelets – may cause Per manufacturer on vialRecheck thrombocytopenia with any dose (evsyringes concentration
catheter flushing!) Multi-dose vials expire of vial/bag before
Monitor for signs of bleeding from initial opening. administering
Monitor PTT 6 hours after any dose dose!change or per orders
protocols (PPOs) for Cardiac Indications and for Treatment of
Rare allergic reactions to hetastarch have been reported. Monitor for hypersensitivity reactions.
Monitor for plasma volume overload – (dyspnea, fluid in lungs, rapid increase in blood pressure) Dose reduction recommended for severe renal insufficiency
Monitor for reflex tachycardia after Incompatible with many each dose. Monitor BP every 5 min medications and solutions, until stabile. check with pharmacist
Maximal reduction in blood pressure seen 15-80 min after doses given
Metro: See MWH-19-MAT: Women’s Health Policy & Procedures – Hydralazine: Continuous Infusion
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 37Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
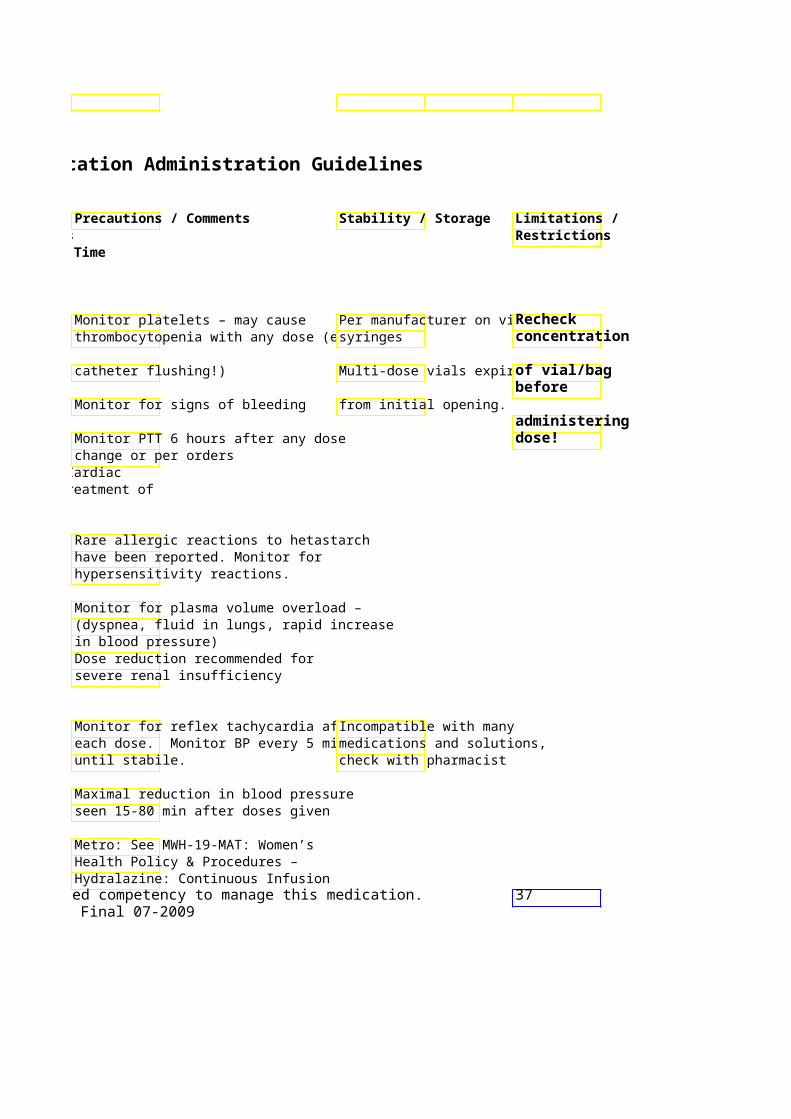
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Hydrocortisone Various Yes, IV Push preferred. May d
vial sizes Give undiluted 50ml in NS or D5W and gCorticosteroid 100mg/2ml doses over 30 –60 several minutes.
250mg/2ml seconds500mg/4ml 1000mg/8ml
HYDROmorphone 2, 4, or Yes, Continuous infusion: (Dilaudid) 10mg/ml Give dose slowly
Vials and over 2-3 min or System Standard Conc: *HIGH ALERT syringes max rate of 0.5 NS (0.2 mg/ml) MEDICATION* mg/min System “Concentrated”
100 ml NS (0.5 mg/ml) Narcotic analgesic
Hydroxocobalamin 1 kit = 2 x NO 2.5 gm reconstituted wit(Cyanokit) 2.5 gm infuse over 7.5 minutes –
vials total of 5 gm
Antidote – cyanide poisoning 2nd 5 gm dose may be g
minutes to 2 hours depending on severity/clinical response for total dose of 10 gm
HydrOXYzine 25 & NO Intermittent Infusion – N(Vistaril) 50mg/ml Preferred!
Vials & IM preferred Antihistamine Syringes
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
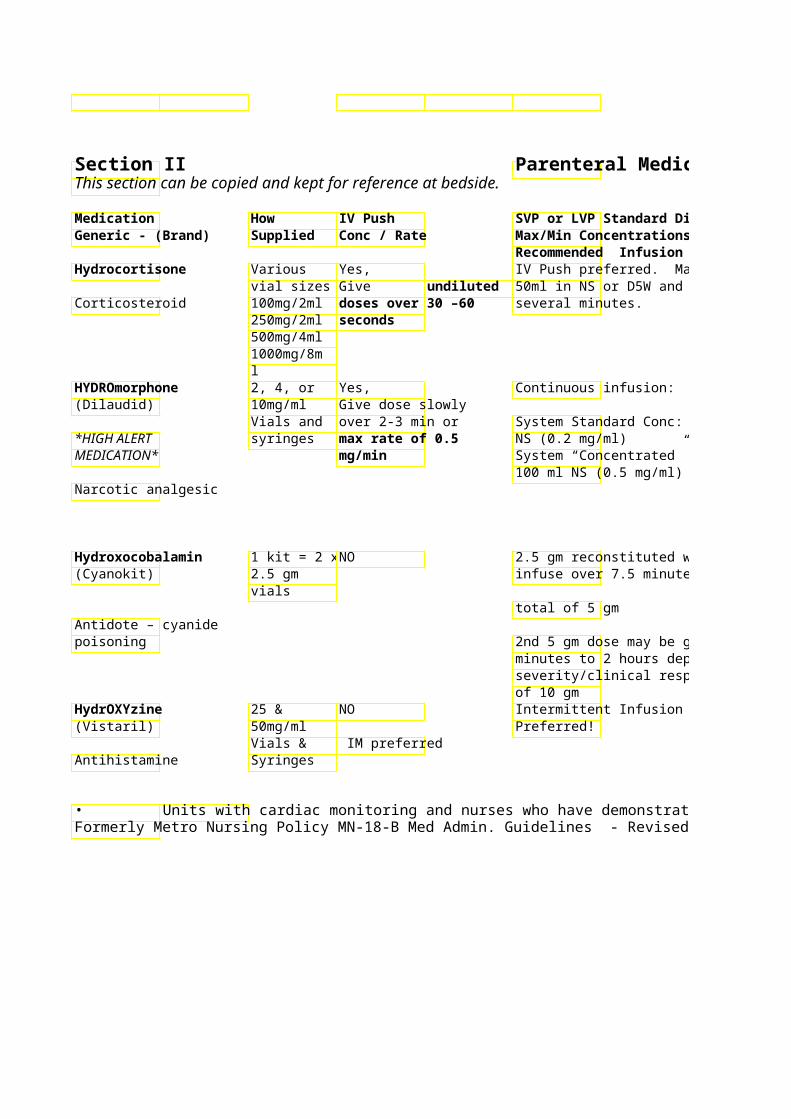
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Local infusion related adverse effectCheck vial/syringe for are rare. expiration date.
Intrathecal administration: use preservative-free ONLY!!
Reverse effects with naloxone Very Potent opioid analgesic.
(Narcan) High doses (IV >1mg or IM > Monitor RR, HR, BP 2mg) in opioid naïve patMetro: If PCA Give lower doses to elderly, debilitatmust be verified with ordered, or patients on additional CNS prescriber. mandatory PCA depressants order set must be
IV dose = 1/3 to 1/5 POused Hydromorphone 1.5 mg IV = Morphine 10 mg IV Urine and skin will turn red May cause hypertension Stable 6 hours
Allergic reactions including anaphylaxis, pruritus, rash may occur
minutes to 2 hours depending on severity/clinical response for total dose
May interfere with various lab tests Hypotension, phlebitis and hemolysis reported following IV administration Intra-arterial administration has resulted in endarteritis, thrombosis and gangrene. Do NOT give IV-push
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 38Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
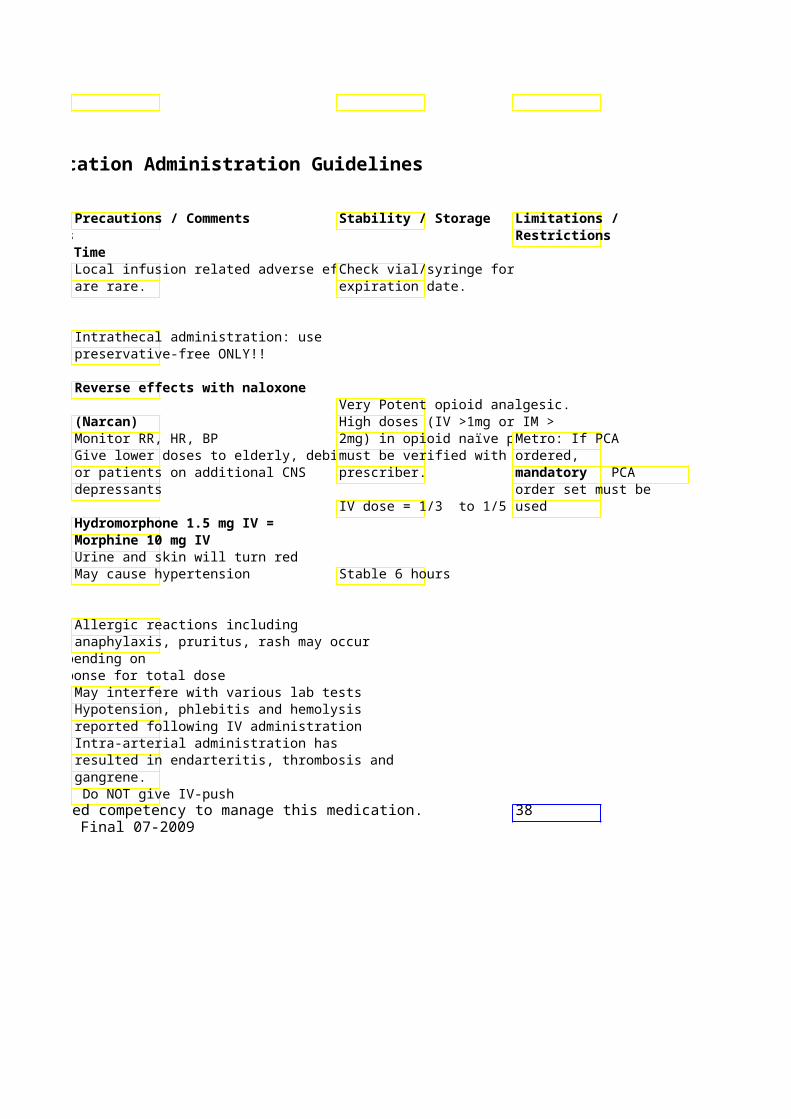
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Ibutilide 1mg/10ml NO 1 mg/50 ml NS (Corvert) Infused over 10 min
Stop infusion when afib/aAnti-arrhythmic terminated
If < 60kg dose @ 0.01mMay repeat same dose 10completion of initial dosconverted
Preprinted order set avai
Imipenem/Cilastatin 500mg Vial NO < 500mg/10 0(Primaxin)
30 minutes Antibiotic/ Carbapenem > 500 mg/250ml NS. Inf
minutes
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
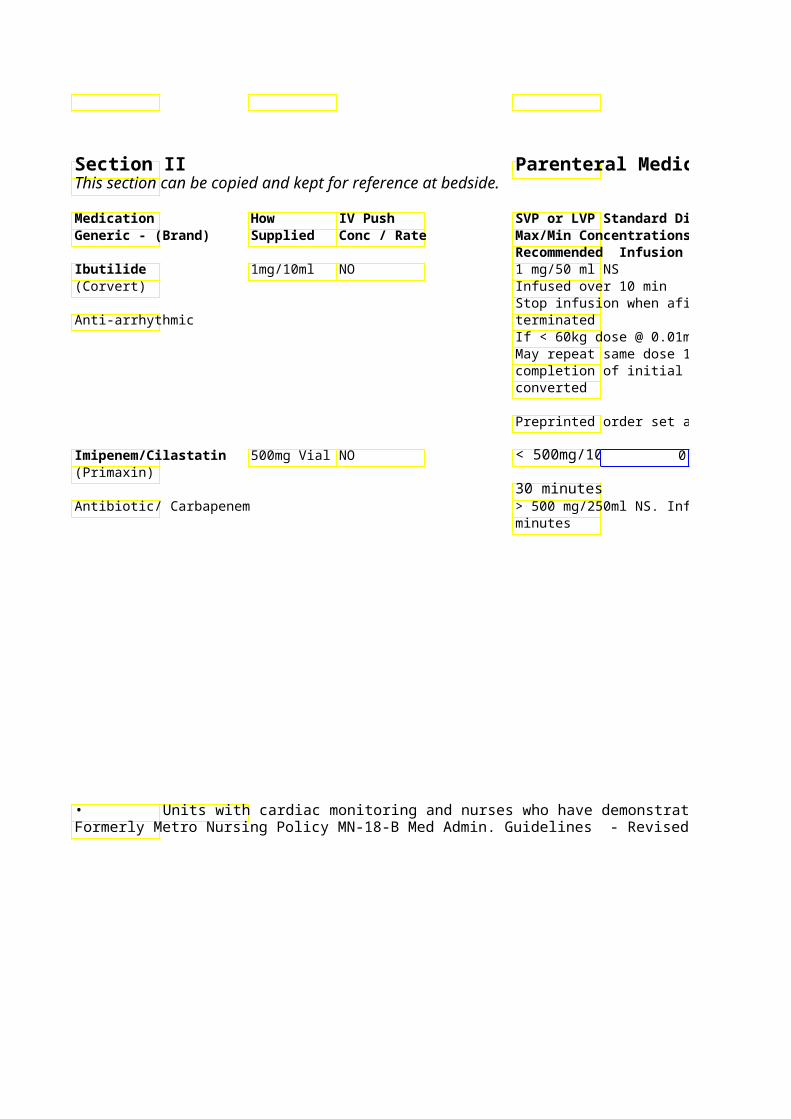
Parenteral Medication Administration Guidelines
Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Continuous cardiac monitoring * See footnote recommended for at least 4 hours bedside monitor after completion of infusion. & defibrillator
recommended Monitor for increased QT interval prolongation and ventricular arrhythmia potential
Check potassium and magnesium levels: should be within normal limits at time of infusion Reduce rate of infusion if
nausea/vomiting occur Caution with penicillin allergyCheck allergies Dose reduction recommended for CrCl < 70 ml/min
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 39Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Immune Globulin Various Not advised Standard IVIG (CarimuIntravenous (IVIG) strengths & contains sucrose
brands Initial Dose -Carimune:
Immune modulator 3% solution recommende
previously untreated patiFirst dose dispensed as solution – usually 6g dose– after first bag – remainprovided as 6% solution. may be further concentrneeded. Initial Rate -Carimune 3Initiate at 30-60mL/hr x tolerated may increase rate every 15-
30minutes to a maximum oSubsequent Doses – (Ca
12% Solutions): After 1st dose of 3% solution, subsequent infusions (be administered at a higconcentration and higher increasing q15-30 min). maximum rate of 2 mg/k
Sucrose-free IVIG 10%
Initial Dose-Gammagard Initiate at 15-30mL/hr atolerated every 30min 5mL/kg/hr (Gammagard)2.4mL/kg/hr (Privigen), r
Subsequent Doses: Highbe possible for Privigenindication & tolerabilitypharmacist).
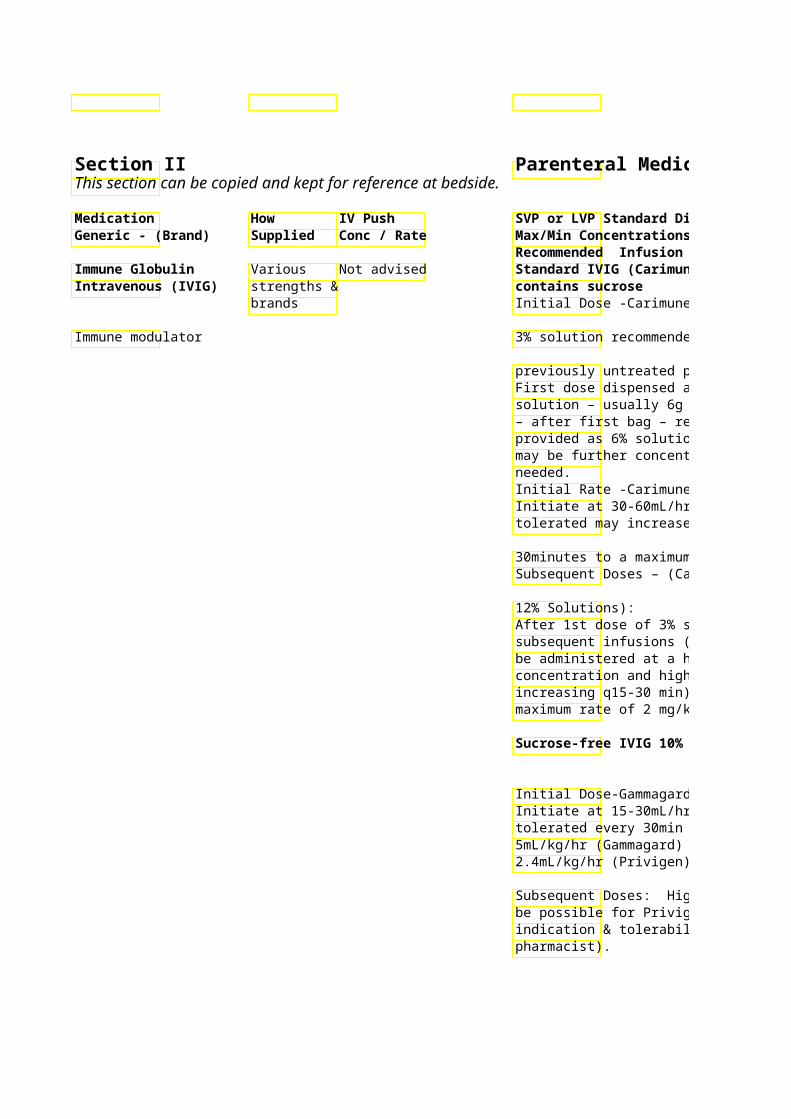
• Units with cardiac monitoring and nurses who have demonstratedFormerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Fin

Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitoring Unless clinically - Monitor BP every 15 minutes for first Filter not required for:indicated (i.e. IgA hour of every infusion, then every 30Carimune, Privigen or deficiency) - 60 min. for duration of the initial Gammagard. infusion. Monitor Blood Pressure requests for
specific brands every 30-60 min. during subsequentGammagard S/D requirescannot be infusions if the patient has a history – use provided administration intolerance to IVIG. set that includes 15 mic accommodated. Decrease rate or stop infusion iffilter. If administration s Indication patient experiences adverse provided, contact pharmrequired with all reactions. filter! orders. Consider premedication with Pharmacists will acetaminophen +/- diphenhydramineReconstitute Carimune viprovide ordered Refer to IVIG PPO with sterile water dose as 3%, 6% or
tolerated may increase rate every 15-12% solution
symptoms of anaphylaxis and have (Carimune) or a epinephrine available to treat. 10% solution
(Gammagard, - Monitor renal function Privigen).
After 1st dose of 3% solution, Adverse reactions include Pharmacist will hypotension, headache, fatigue, change round dose down in pulse, flushing, tightness in chest, to nearest vial (3, chills, fever, dizziness, 5, 6 or 10g) nausea/vomiting, backache, leg depending on cramps, uticaria, and diaphoresis availability within Standard (Sucrose-containing) IVIG 90% of calculated
dose. is appropriate for most patients; however, IVIG has been associated with renal dysfunction, ARF, osmotic nephrosis, and death. Patients predisposed to ARF include patients with: 1) any degree of pre-existing renal insufficiency, 2) diabetes mellitus, 3) age > 65, 4) volume depletion, 5) sepsis, 6) paraproteinemia, 7) pts receiving known nephrotoxic drugs In these patients, IVIG should be administered at the minimum concentration and the minimum
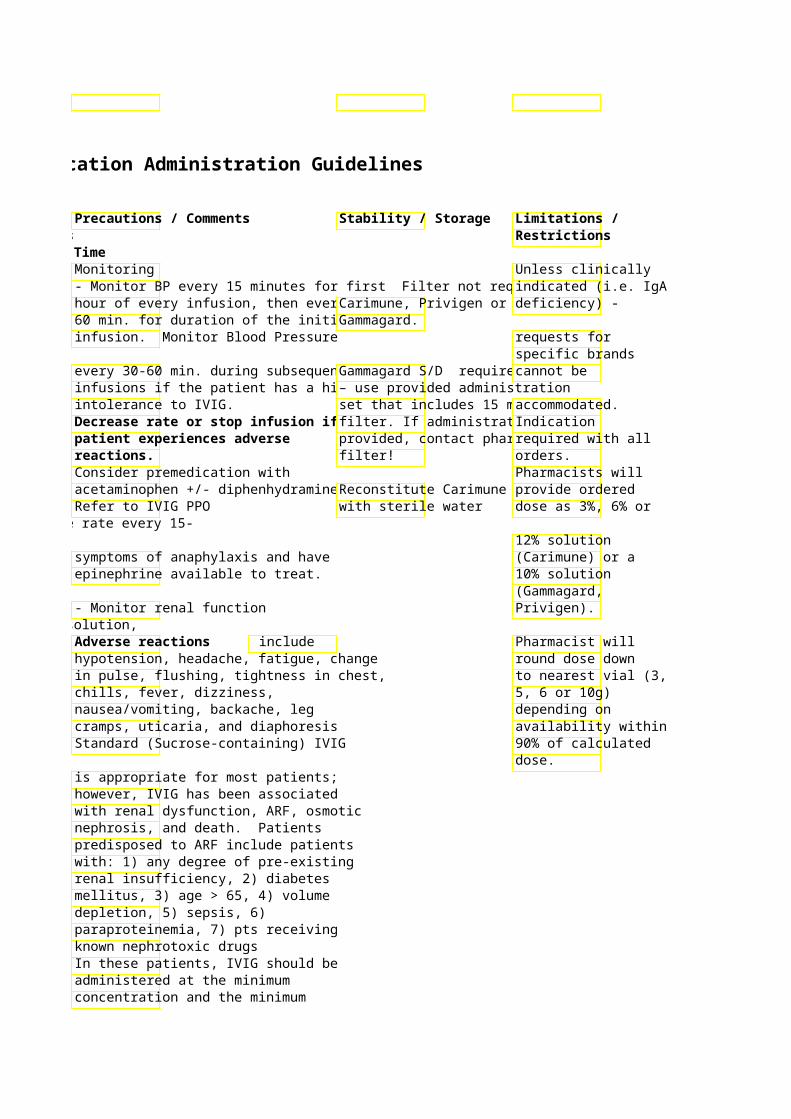
infusion rate that is practical. Sucrose-free IVIG may also be 40considered.

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Inamrinone 20 ml amp Yes Loading dose 0.75 mg/K(Inocor) (5 mg/ml) May give formerly – amrinone undiluted via Usual dose range: 5-10
central line or Standard conc: 400 mg/running IV. Give (total vol=330 ml) (1.2
Cardiovascular/ Positive over 2-3 min. “Concentrated” conc: 500 mg/100 ml
inotrope NS (total vol=200 ml) (2
Maximum Concentration = undiluted (5 mg/ml)
Indomethacin 1mg Vial Yes, Not advised (Indocin) Give 0.1 – 0.25
mg/Kg dose over Anti-inflammatory/ 5-10 seconds NSAID
InFLIXimab 100 mg NO Infuse slowly over 2 hou(Remicade) Vial
Recommended Doses: Monoclonal antibody Crohn’s: 5 mg/Kg
Rheumatoid Arthritis: 3
Concentration should be 0.4 - 4mg/ml
Insulin- Human 100 Regular Insulin System Standard ConcentRegular units/ml 10 used for IV route. 150 Units/150ml NS (1 unAlso see Section III ml vial Give all doses over
15-30 seconds *HIGH ALERT MEDICATION*
Recheck insulin name Also administered and dose before SQ – see section administering! IV of guidelines Antidiabetic • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Dose-related thrombocytopenia Dilute with NS only * See footnote occurs in 2-3% within 48-72 hr after initiation. Reverses within one week Incompatible with many upon d/c of med. medications/solutions – check Monitor BP, HR every 15 min with pharmacist
“Concentrated” conc: 500 mg/100 ml Total cumulative dose should not exceed 10 mg/kg
Maximum Concentration = undiluted
For closure of Patent Ductus ArteriosPrepare solution just prioNeonatal in premature infants between 500 & administration Intensive Care 1750 Gram Weight.
Do not dilute with agents See labeling for age specific dosing containing benzyl alcohol. Use Course of therapy involves 3 doses preservative-free sterile water 24 hours apart or NS only! Monitor for allergic symptoms – Administer within 3 hrs of shortness of breath, rash, hives, andpreparation pruritus.
Do NOT shake or transport Premedication with acetaminophen solution through pneumatic and diphenhydramine recommendedtube system
Concentration should be 0.4 - 4mg/ml Preprinted order sets available Use administration set provided
by pharmacy (contains 1.2 micron filter)
Waste 10-20 ml of diluted solution Recheck through the administration set to Vials are stable x 28 dayinsulin name saturate binding sites in IV tubing first use refrigerated or and dose before connection to infusion pump. temp before Preprinted order sets available for administering!
insulin infusions in ICU patients, Adult Surgical/Medical Patients, and DKA/Hyperosmolar Nonketotic Coma Patients Monitor blood glucose
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 41Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
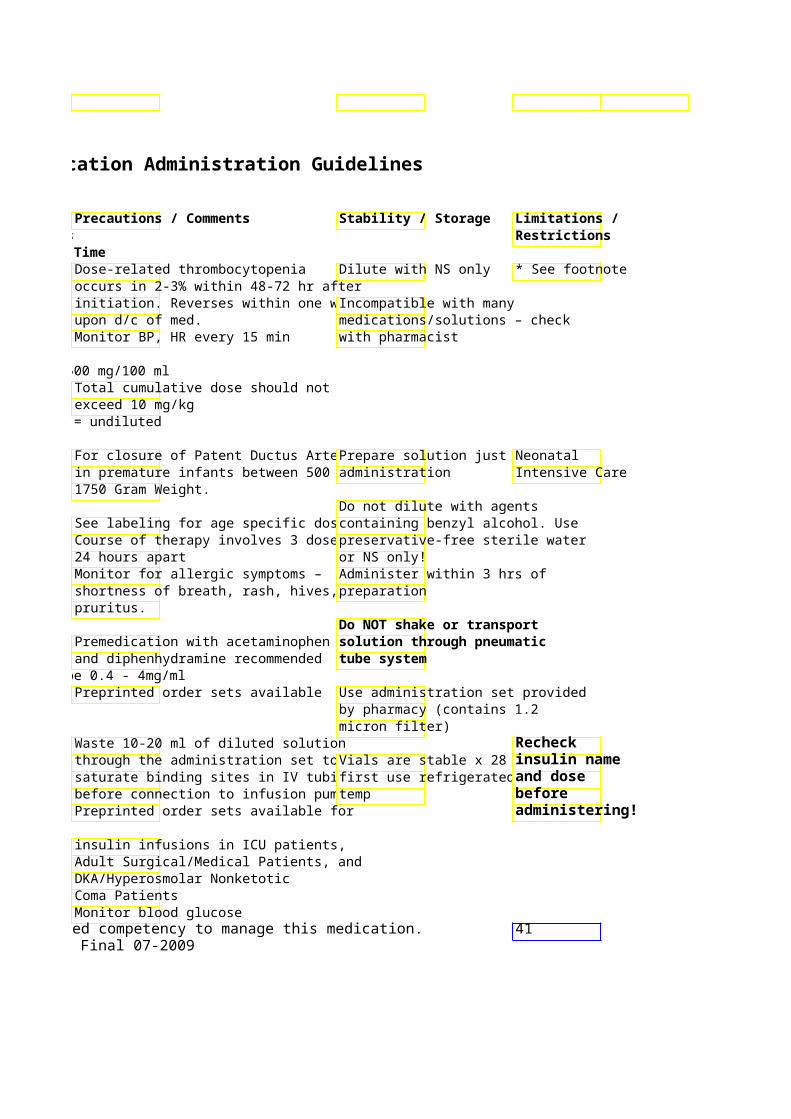
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Iron Dextran 50 mg/ml- Yes, Dose > 200mg = Total Dose Infusion(INFed) 2ml Vial Doses up to 200mg (TDI) - dilute into 250-500 ml NS Max
at max rate oconc = 50 mg/ml Iron supplement mg/min
Infuse over 2-6 hours
May be given IM – IV infusion preferred over IM due to local complications and unpredictable absorption with IM admin
Iron Sucrose Complex20mg/ml – Yes, (Venofer ) 5ml Undiluted up to 50 mg IV in 50 ml NS over 15 min
vial 200mg at max 100 mg IV in 50 ml NS over 30 min rate of 20mg/min 200 mg IV in 50 ml NS over 60 min
Iron supplement 300 mg IV in 100 ml over 2 hours
Maximum Dose per P&T: 300 mg – no more frequently than once weekly
Isoniazid 100 mg / Yes, Dilution not advised.(Nydrazid®) ml Vial – Administer
10ml undiluted & slowly Antimicrobial over 5 minutes
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
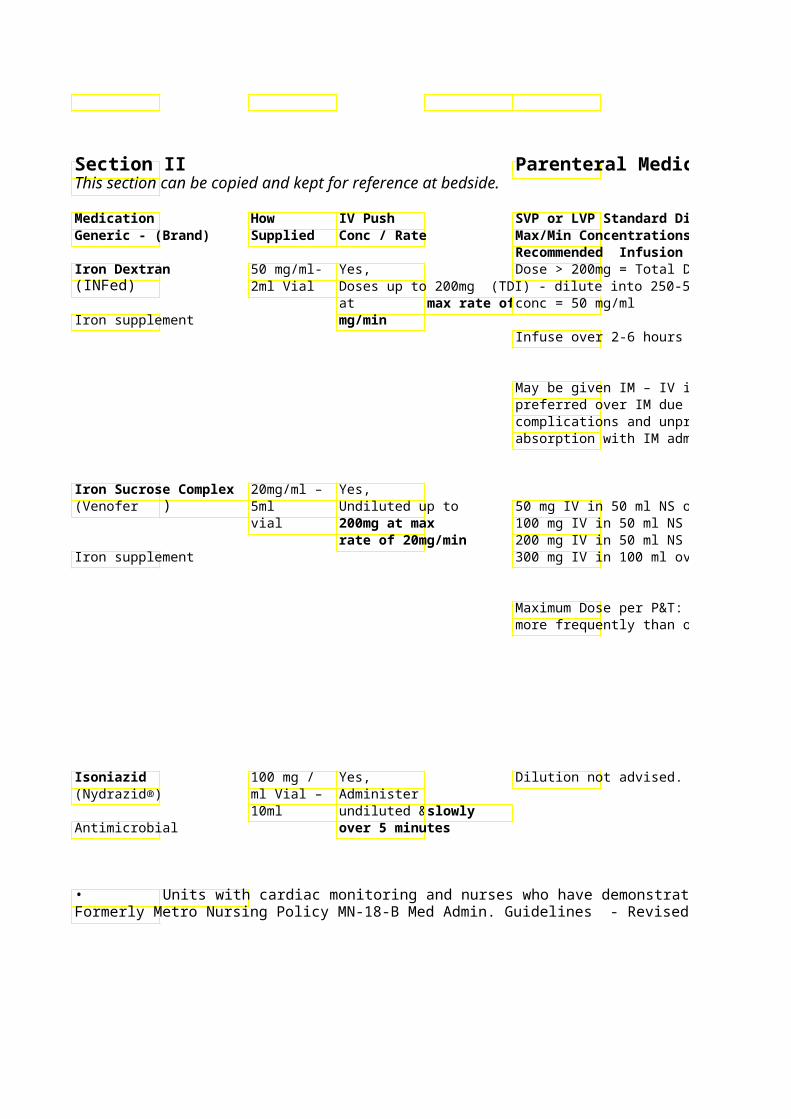
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Dose > 200mg = Total Dose Infusion25 mg test dose IV-Push over 30 Use NS – D5W has increased
Doses up to 200mg (TDI) - dilute into 250-500 ml NS Max seconds to 5 min recommended incidence of phlebitis/pain at before each total dose infusion injection site Observe and monitor BP and HR every 15 min for 60 minutes after teLean body weight (or ideal dose before implementing infusion body weight) not actual body
weight should be used in May be given IM – IV infusion Have the following readily available calculating dose preferred over IM due to local during infusion: diphenhydramine 50 complications and unpredictable mg IV, epinephrine 1:1000 (1 mg/ml)Incompatible with many absorption with IM admin and hydrocortisone 100mg/2ml medications/solutions, check
Anaphylactoid/Hypotensive reactionswith pharmacist possible. Hypotensive reactions may be
50 mg IV in 50 ml NS over 15 min possible 100 mg IV in 50 ml NS over 30 min 200 mg IV in 50 ml NS over 60 min Test dose not necessary. 300 mg IV in 100 ml over 2 hours
Monitor vital signs (BP) including orthostatic BP –
Maximum Dose per P&T: 300 mg – no more frequently than once weekly Metro: For Outpatients -
Doses < 100 mg – monitor patient for 1 hour post-infusion per P&T Doses 200-300 mg – monitor patient for 2 hours post- infusion per P&TMay cause hypotensio or hypertension, chest, back or groin pain. Symptoms typically resolve 1-2 hours after infusion completed. Solution may cause local irritation Solution may crystallize at low Slow rate if tingling sensation room temperature. reported in extremities
Warm slowly to re-dissolve Oral administration preferred. May be given IM via ventrogluteal site due to volume per dose.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 42Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
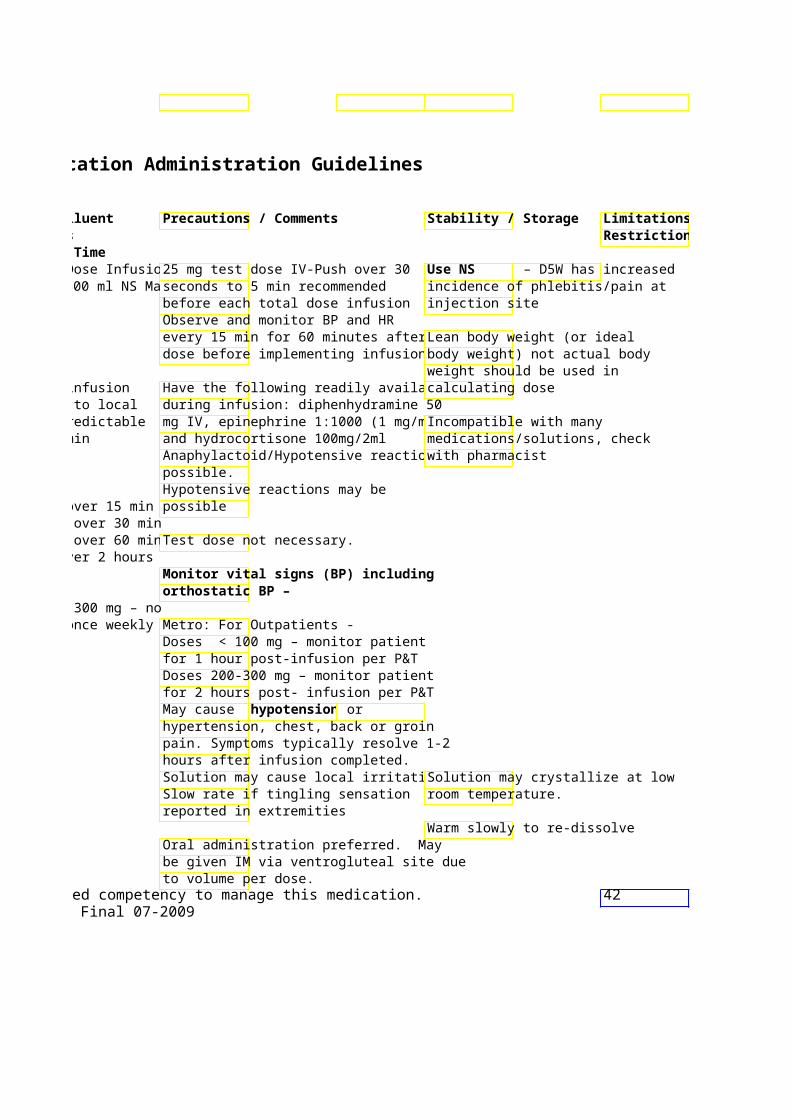
Limitations / Restrictions
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Isoproterenol 0.2 mg / ml NO System Standard Conc: (Isuprel ) ® 5 ml amp NS (4 mcg/ml)
System “Concentrated” Cardiovascular/ mg/250 ml NS (8 mcg/mlChronotrope
Usual dose range: 1-10Decrease/temporarily stoHR > 110. Doses sufficieHR > 130, may induce vearrhythmias or angina.
K – Vitamin K – See Phytonadione Ketamine 10 mg/ml Yes, Usual dose for sedation:
20 ml vial; Slowly over 2-3 IV 50 mg/ml min (conc max Continuous infusions ma
Analgesic- 10 ml vial; 50mg/ml) during surgery as generalsedative/anesthetic Infusion may be used as
analgesic for refractory May also be given syndromes IM
Infusion: Dilute dose infinal concentration of 1(max: 2 mg/mL)
** Oxygen via nasal cannula at minimum w/continuous poximetry/ECG monitorinrecommended while sed
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
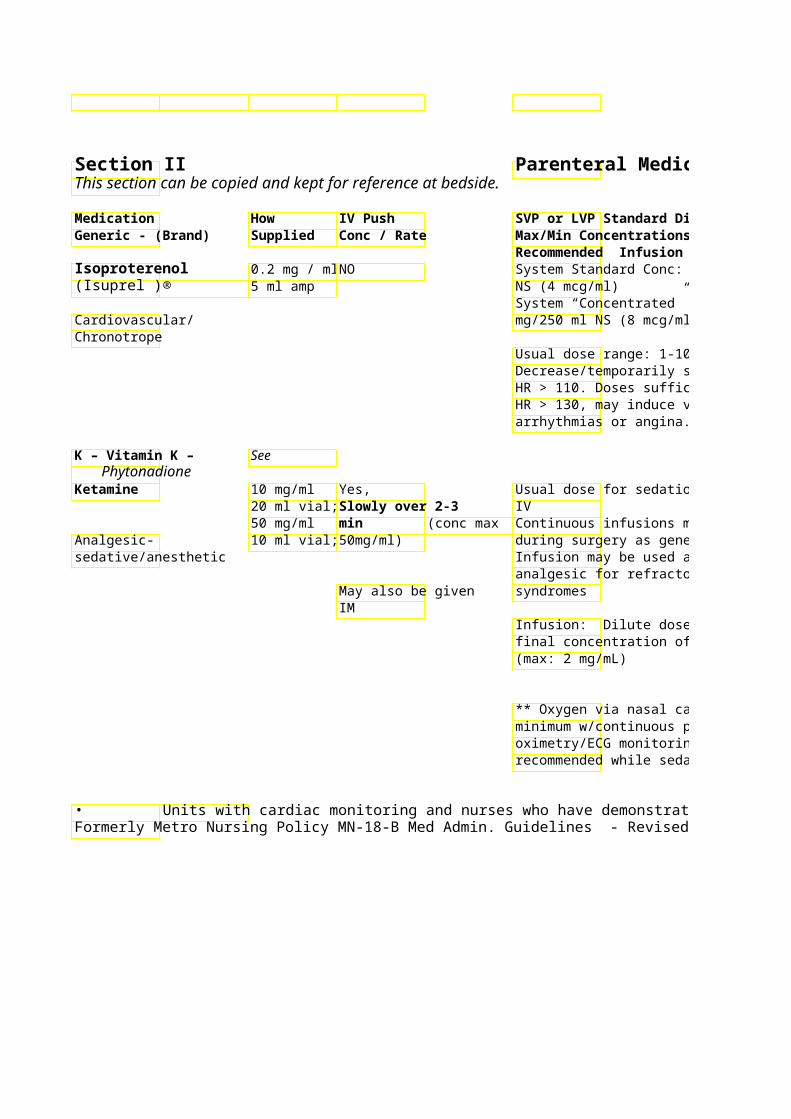
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor ECG continuously; BP and Incompatible with many * See footnote HR every 15 min meds/solutions – check with Monitor urine output every 1-2 hr pharmacist May cause PVC’s
Cardiac transplant patients have little or no response to Atropine. Isoproterenol is considered first line drug for treatment of severe bradycardia in heart transplant patients
Monitor RR, BP, HR and mental Protect from light Critical Care & status. prescriber May cause – experienced * respiratory depression with high w/administratiodoses or too rapid injection n * cardiovascular stimulation (HTN, tachycardia) * hypersalivation / excessive secretions - may be managed with atropine/glycopyrolate. *Emergence phenomenon (vivid dreams, hallucinations, delirium, confusion)
** Oxygen via nasal cannula at Benzodiazepines (eg. midazolam) may decrease/alleviate CV stimulation and emergence phenomenon
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 43Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
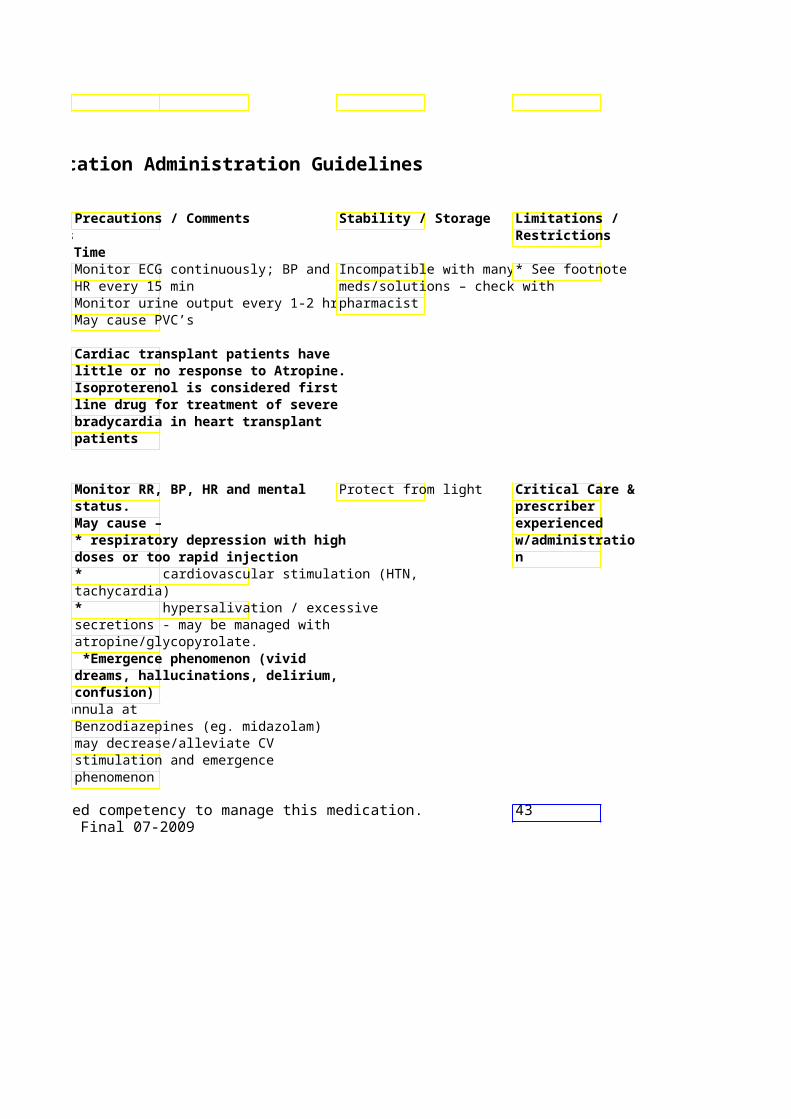
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Ketorolac 15 mg & 30 Yes, Give IV - push (Toradol) mg per ml Give over 15-30
syringe & seconds Analgesic/ Anti- vial inflammatory/ NSAID
Labetalol 5 mg/ml 4 Yes, Continuous infusion: Initi(Trandate, Normodyne) ml syringe, Give 10 mg over2 mg/min titrate to desir
20 ml vial minutes System Standard Conc: Antihypertensive 250 mg/150 ml NS (total vol 200 ml)
(1.25 mg/ml)
System “Concentrated” 300 mg/40 ml NS (total v(3mg/ml) Undiluted 5mg/ml = max conc
Lacosamide 10mg/mL NO Dilute all doses in 100m(Vimpat) single dose administer over 30min
20mL vial Anti-seizure Lansoprazole 30 mg vial NO 30 mg in 50 ml NS (Prevacid) Infuse over 30 min
Proton Pump Inhibitor
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
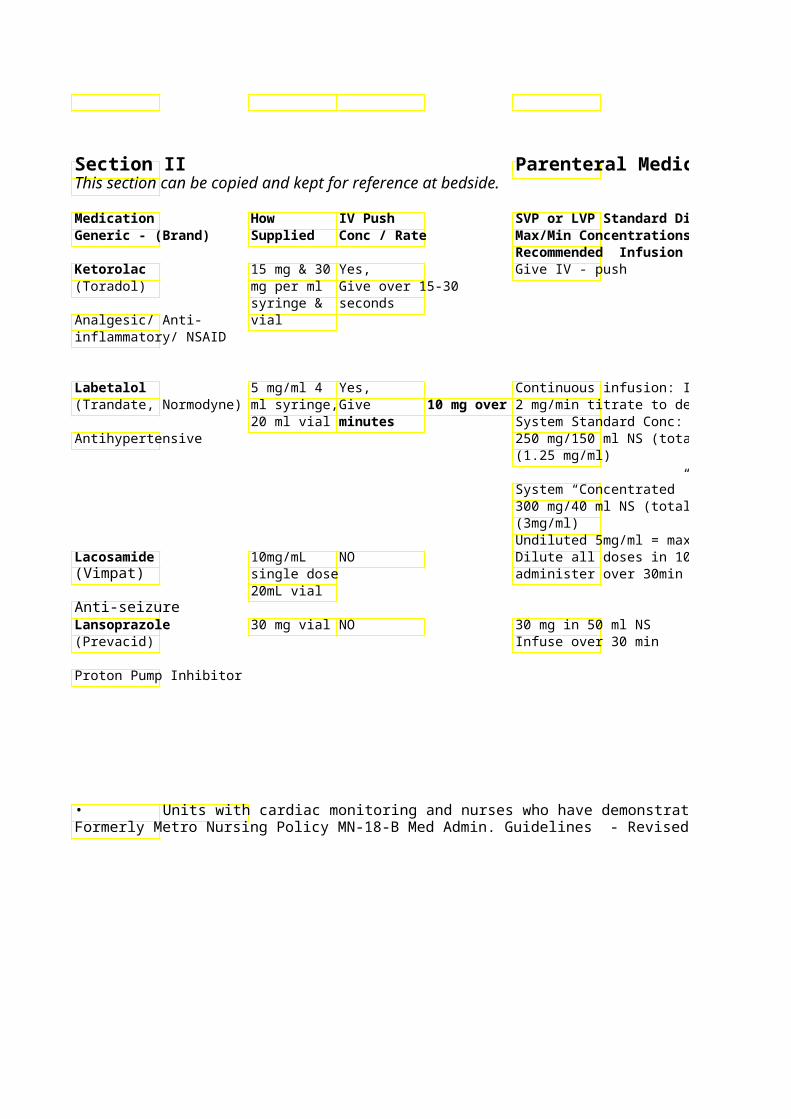
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Recommended max dose is 120 Pain with injection common-slow mg/day infusion if this occurs Recommended max dose for
CrCl < 50 ml/min or age > 65 NSAID – check allergies y.o. is 60 mg/day
Max recommended length of therapy is 5 days
Maximum anti-hypertensive effect * Continuous apparent approximately 5 min after infusion - see each dose NOT compatible with alkfootnote
250 mg/150 ml NS (total vol 200 ml) solutions such as furosemide Titrate to desired BP parameters (Lasix) – check with Intermittent doses
pharmacist for compatibil- monitor VS. May cause orthostatic hypotension. May cause Administer to pt while in supine hypotension and position if possible. bradycardia
Undiluted 5mg/ml = max conc IV dose = PO dose IV doses mixed in 0.9% NaCl
are stable for 24 hours at room temperature.
IV dose = PO dose Vial must be reconstituted with Sterile Water and further diluted within 1 hr
In-line filter must be used! Do not administer with other medications/fluids – check with pharmacist for compatibility information
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 44Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
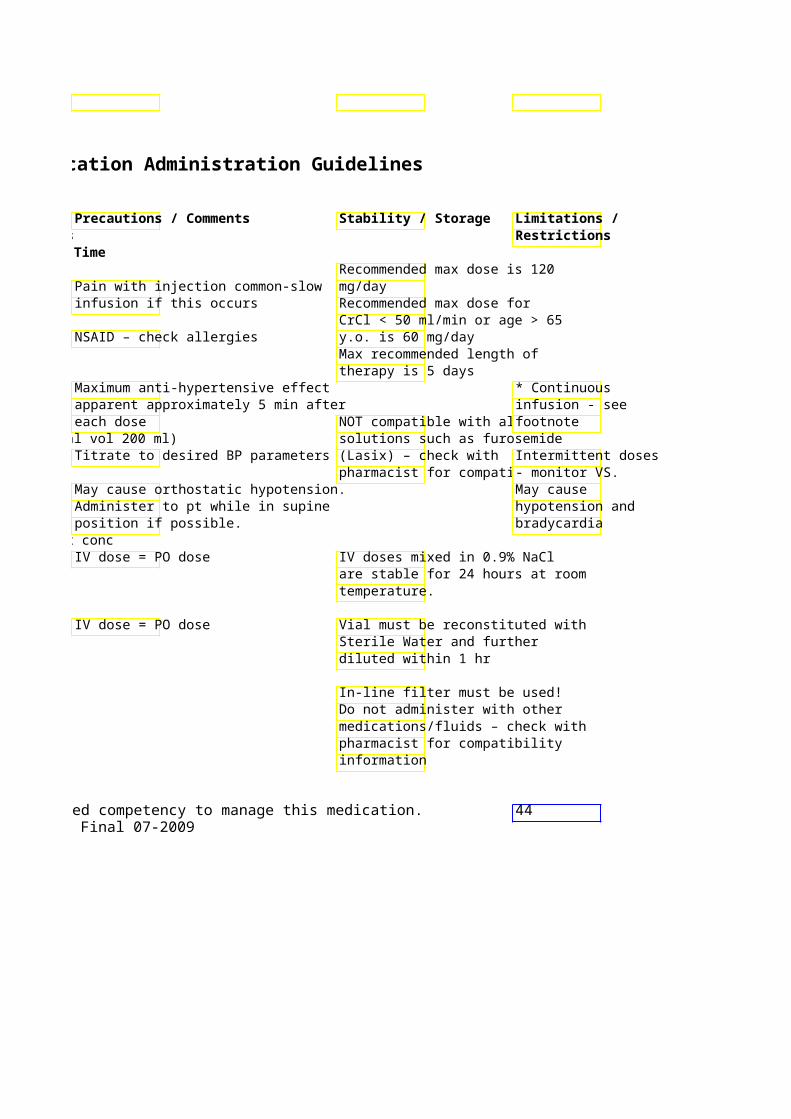
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Lepirudin 5 mg/ml 10 Yes, Maintenance infusion: 0(Refludan) ml vial Loading dose (0.4 titrate to target aPTT
mg/kg – max 44 *HIGH ALERT mg)*: IV Push System Standard Conc: MEDICATION* over 30 seconds NS (0.5 mg/ml)
Anticoagulant Preprinted order set avai
Levetiracetam 500 mg/5 NO Dilute in 100 ml NS and (Keppra) ml vial minutes
Anticonvulsant
Levofloxacin 25mg/ml NO Infuse 250 and 500 mg d(Levaquin) Vial. min
Premix: Antibiotic/ 500mg/100 Infuse 750 mg dose over 90 min Fluoroquinolone ml Levocarnitine 200 mg/ml Yes, May be given as intermit(Carnitor) 2.5 ml Give over 2-3 min – diluted to conc of 0.5 to 8 mg/ml in
ampule NS or LR Nutritional supplement/Amino acid
Levothyroxine 200 mcg/5 Yes, Slow IV push recommen(Levothroid, Synthroid) ml Give over 2 min
vial Hormone - thyroid
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
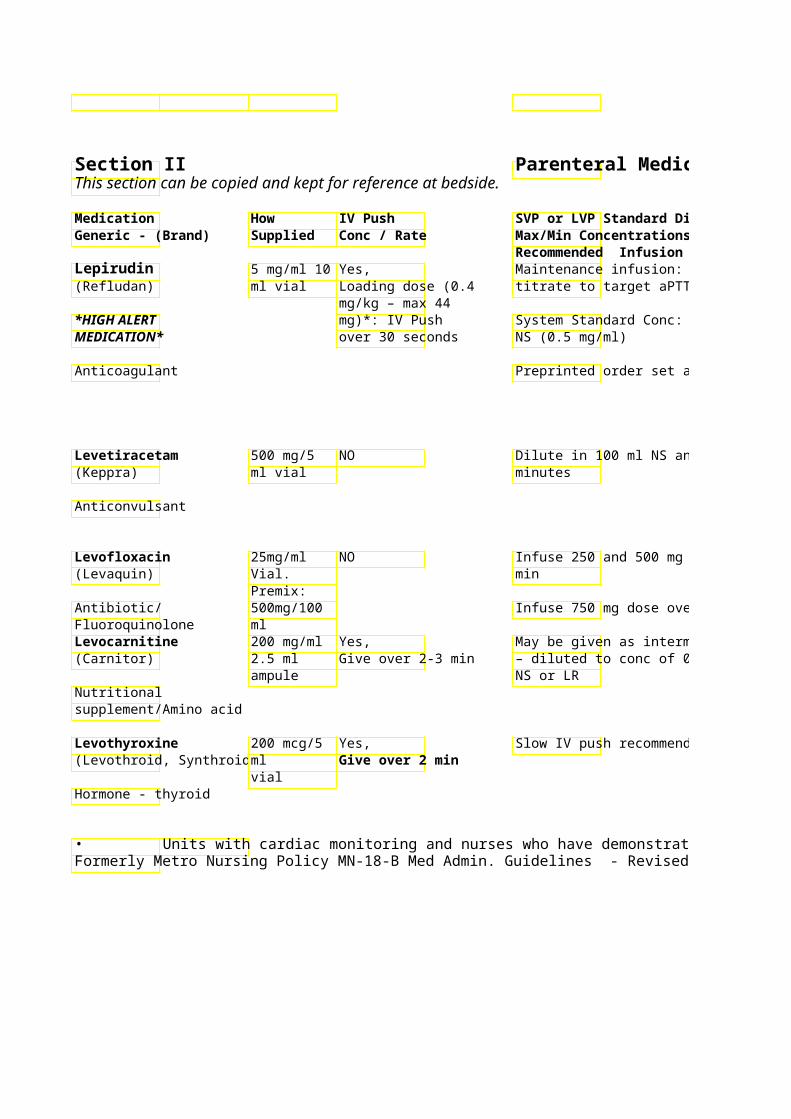
Parenteral Medication Administration Guidelines
Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Anticoagulant for use in patients with heparin associated thrombocytopenia
Monitor for signs of bleeding! Monitor therapy with aPTT (1.5-2.5 x baseline) 4 hours after beginning drip or change in the rate of a continuous infusion *Adjust dose if CrCl < 60 ml/min, SrCr > 1.5, or if pt has received thrombolytic Double check drug name
Store at room temperature IV Dose = PO Dose Dose reduction for patieCompatible with NS, D5W, < 50 ml/min recommendLR, lorazepam, diazepam and
valproate Dose reduction for patients with CrCl < 50 ml/min recommended
Infuse 750 mg dose over 90 min
May cause HTN – monitoDiscard ampule immediately – diluted to conc of 0.5 to 8 mg/ml in after use
May cause N/V – slow rate of infusion Use NS or LR – NOT D5W
May cause hypercalcemia ** Verify dose to be giveUse immediately after vial after drawing up correconstitution
Use NS only to reconstitute IV dose = 50% of PO dose
Do not combine with other solutions
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 45Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
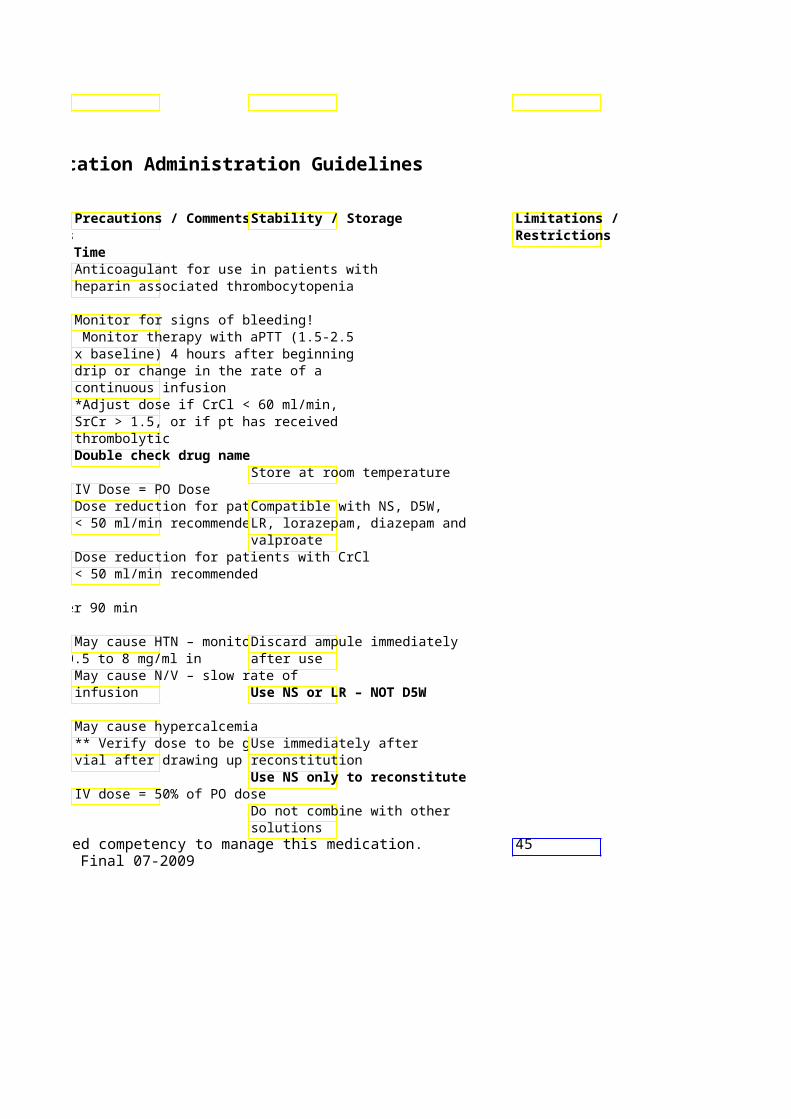
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Lidocaine 100mg Yes, Continuous infusion requ
Syringes, 50-100mg over 2 maintain anti-arrhythmic effect Anti-arrhythmic 2Gm/500ml minutes at max
Premix rate of 50mg/min Usual dose range: 1 – 4System Standard Conc: ml D5W Premix (4 mg/ml
** Do not use in WPW syndrome System “Concentrated”
mg/ 100 ml NS (total volume 200ml) ** (10 mg/ml)
Can be given via ET tubeIV dose
Linezolid Premix: NO Max conc: 2 mg/ml (Zyvox) 400mg/
200ml NS, Administer dose over 60Antimicrobial 600mg/
300ml NS Premix bags
LORazepam 2 & 4 Yes, Continuous infusion (Ativan) mg/ml Dilute with equal System Standard Conc:
syringe / volume NS-Give D5W Excel or glass bottleSedative/ Vial at max rate of 2 volume 100 ml) (1 mg/ml) Benzodiazepine mg/min
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
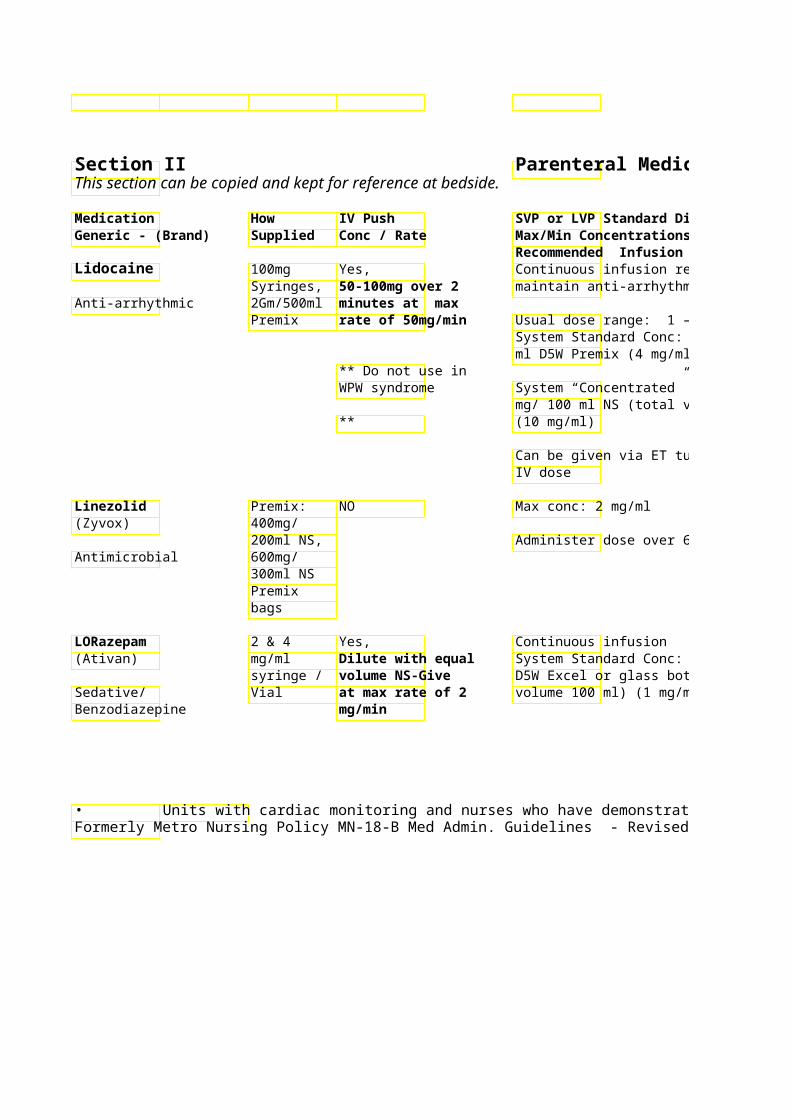
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Continuous EKG Monitoring * See footnote maintain anti-arrhythmic effect
Do NOT exceed 300 mg/hour or 4 Continuous ECG monitoring. mg/min Cardiac signs of toxicity: Widening Therapeutic serum lidocaine of QRS, bradycardia, increasing levels: 1.5 to 5 PVCs, hypotension, heart block Toxic levels: > 5 Non-cardiac signs of toxicity:
mg/ 100 ml NS (total volume 200ml) numbness of lips, tongue and face; tremors; paresthesias; diploplia; mental status changes, nausea/vomiting; confusion; slurred speech Weak MAO inhibitor – verify patient Compatible with NS, D5 Low tyramine on low tyramine diet (in addition to LR restriction (in ordered diet) addition to Low tyramine diet to continue x 3 Incompatible with ceftri ordered diet) days after d/c of medication. Avoid co-administration with meds Normally may exhibit a yellow that may increase risk of serotonin color syndrome (i.e. SSRIs, SNRIs, TCAs) Monitor respiratory and Critical Care for cardiovascular status Vials stable 60 days at continuous May cause respiratory depressiotemp infusion
volume 100 ml) (1 mg/ml) Observe for crystals (maContinuous
Reverse with flumazenil micron in-line filter). infusion may be (Romazicon) given
unmonitored if used for comfort care/hospice pt
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 46Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
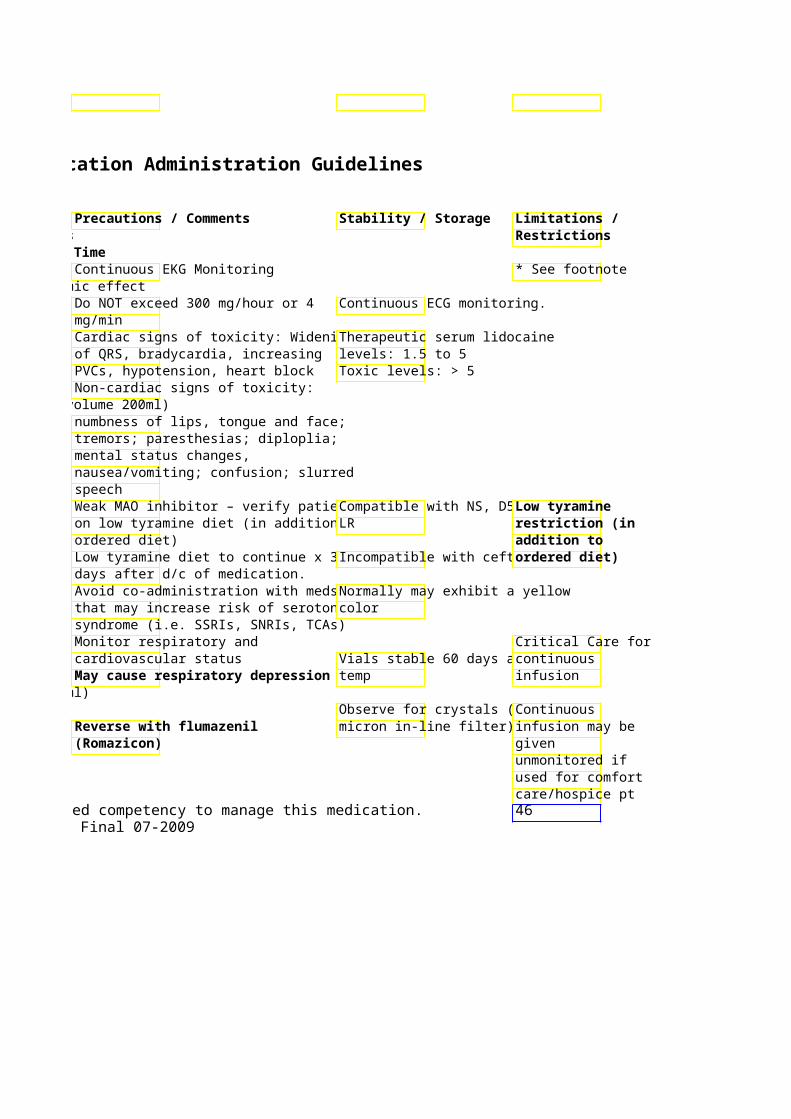
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Magnesium Vials: 4 Yes, Intermittent infusion: Magnesium
mEq/ml – Bolus dose only supplementation - 1 – 2 Gm over 30 *HIGH ALERT multiple for Torsades de min MEDICATION* vial sizes Pointes
Premix Dilute with 10 ml Pre-eclampsia/eclampsia: Usual boluElectrolyte bags: NS/D5W for 1 gm dose is 4 grams given over 20-30
1 Gm/100 dose; 20 ml minutes ml, 2 NS/D5W for 2 gm Pre-term labor: Usual bolus dose is 6Gm/50 ml, dose. Give at max grams given over 20-30 minutes 4Gm/100 rate of 1Gm/minml, 6 Gm/ Continuous Infusion: 1- 4 Gm/hr 50 ml & 20 gm/50 ml System Standard Conc: 20 grams/ 5Premix ml Sterile Water Premix (40 mg/ml)
Mannitol Vial 25%- Yes, Intermittent Infusion: (Osmitrol) (12.5Gm/5 12.5 Gm/50 ml Infuse over 30-60 min
0ml) over 5 min orOsmotic diuretic Premix: 1g/kg over no less
20% (100 than 10 min 12.5 gm = 62.5 ml of 20%, 50 ml 25% Gm/500 25 gm = 125 ml of 20%, 100 ml 25%ml) 50 gm = 250 ml 20%, 200 ml 25% 10% (50 Gm/ 500 Metro: Infusion bags from pharmacy ml) contain extra volume for priming of
tubing and filter. Meperidine 25,50,75 & Yes, Continuous infusion NOT advised (Demerol) 100 mg/ml Dilute dose to
syringe, 10ml with NS and PCA administration recommended *HIGH ALERT 50 mg/ml give at max rate MEDICATION* vial of 10 mg per
minute System Standard Conc: 250 mg/ 250ml NS (1 mg/ml)
Narcotic analgesic System “Concentrated” Conc: 250 mg/ 100 ml NS (2.5 mg/ml)
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
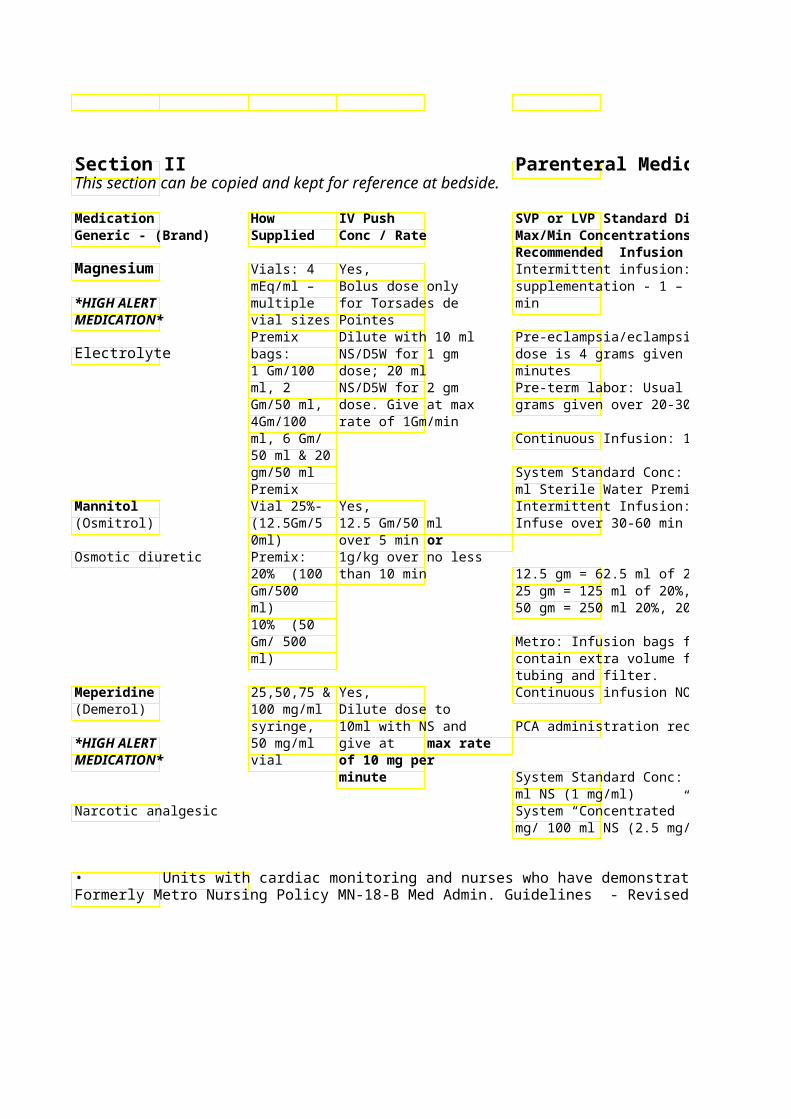
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Intermittent infusion: Magnesium 1 Gm = 8.12 mEq Mg. **Metro OB: supplementation - 1 – 2 Gm over 30 Mandatory use of
Metro OB: Assess DTR, respirations, order set for IV signs and symptoms of Mg toxicity infusion
Pre-eclampsia/eclampsia: Usual bolu(muscle weakness, ECG changes, dose is 4 grams given over 20-30 hypotension, sedation, confusion),
I&Os. Obtain Mg levels as order by Pre-term labor: Usual bolus dose is 6physician grams given over 20-30 minutes May cause respiratory/cardiovascular
collapse Continuous Infusion: 1- 4 Gm/hr
Antidote for Mg toxicity: calcium System Standard Conc: 20 grams/ 5 gluconate ml Sterile Water Premix (40 mg/ml)
Use 0.22 micron in-line filter Do not refrigerate!!
Inspect vials/bags for crystals prior to administration
12.5 gm = 62.5 ml of 20%, 50 ml 25% 25 gm = 125 ml of 20%, 100 ml 25%Hypertonic solutions – monitor 50 gm = 250 ml 20%, 200 ml 25% venous site for irritation.
Avoid Extravasation – see PPO 5046 Metro: Infusion bags from pharmacy for general guidelines / management contain extra volume for priming of Common hold parameters: Na+ > 145
or Serum Osmolarity > 310 Continuous infusion NOT advised Not recommended for patients 6PCA: Check syringe for
years or older nor patients with expiration date Metro: If PCA PCA administration recommended poor renal function 0 ordered,
mandatoryMonitor for delirium, or other CNS set must be used
System Standard Conc: 250 mg/ 250toxicity Monitor respiratory status – may
System “Concentrated” Conc: 250 cause respiratory depression or mg/ 100 ml NS (2.5 mg/ml) distress
Reverse respiratory depression with naloxone (Narcan)
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 47Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
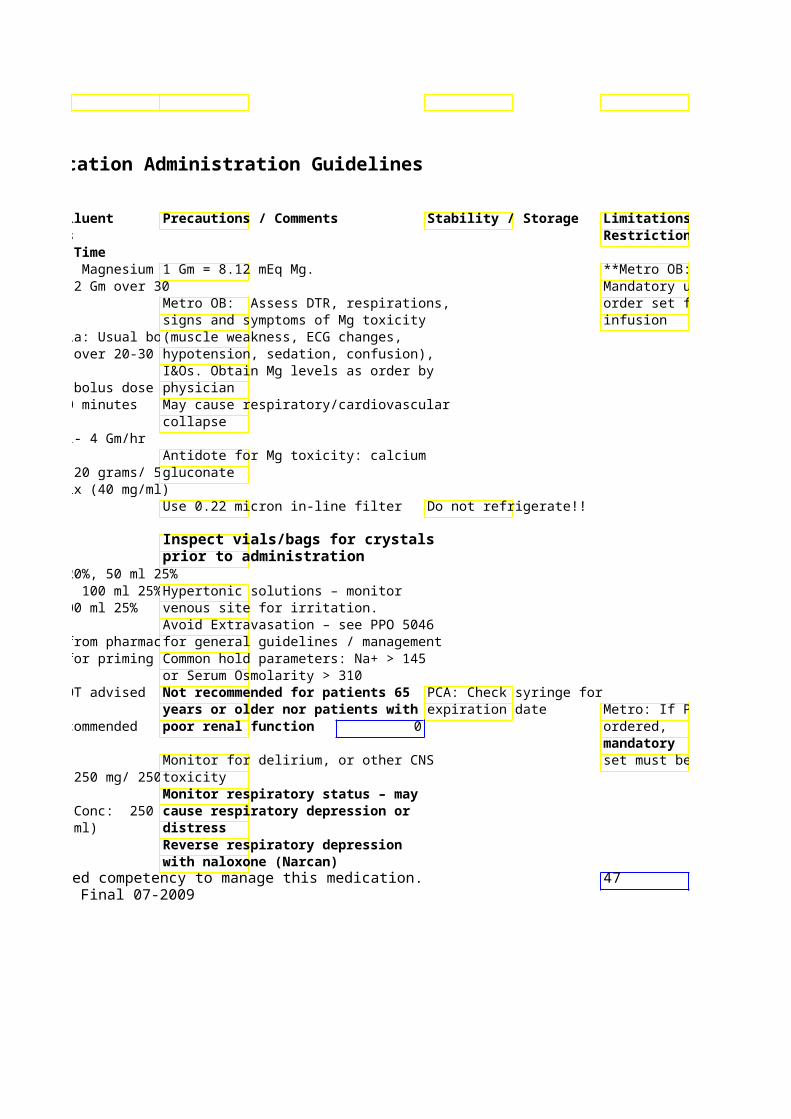
Limitations / Restrictions
**Metro OB: Mandatory use of order set for IV
Metro: If PCA
order set must be used

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Meropenem 500 mg & 1 May be given IV Intermittent Infusion – U(Merrem) Gm vials push over 3-5 min 500mg/50mL –1g/100mL
(i.e. hemodialysis 30min Antibiotic/ Carbapenem patients)
Routine use of IV Extended infusions overpush is not be used for treatment of recommended pathogens.
Methyldopate 50mg/ml – NO Intermittent Infusion (Aldomet IV) 5 & 10ml Up to 250mg in 50ml D5
Vial 30min Antihypertensive 251-500mg in 100ml D5
60min Methylene Blue 1% Yes, Continuous infusion:
Solution 1-2 mg/kg Methemoglobinemia: (co(10mg/mL) SLOWLY over 3- methemoglobin to hemog1 ml 5 min 0.1 – 0.15 mg/kg/hr amp/vial 10 ml Metro: Preprinted order set amp/vial available for treatmen
shock/refractory hypoLoading dose 2mg/kg inover 30min followed by infusion of 0.5-2mg/kg/hr
System Standard Conc: 500 mg/ 50 ml NS (total volume 100 ml
Thiazone dye
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
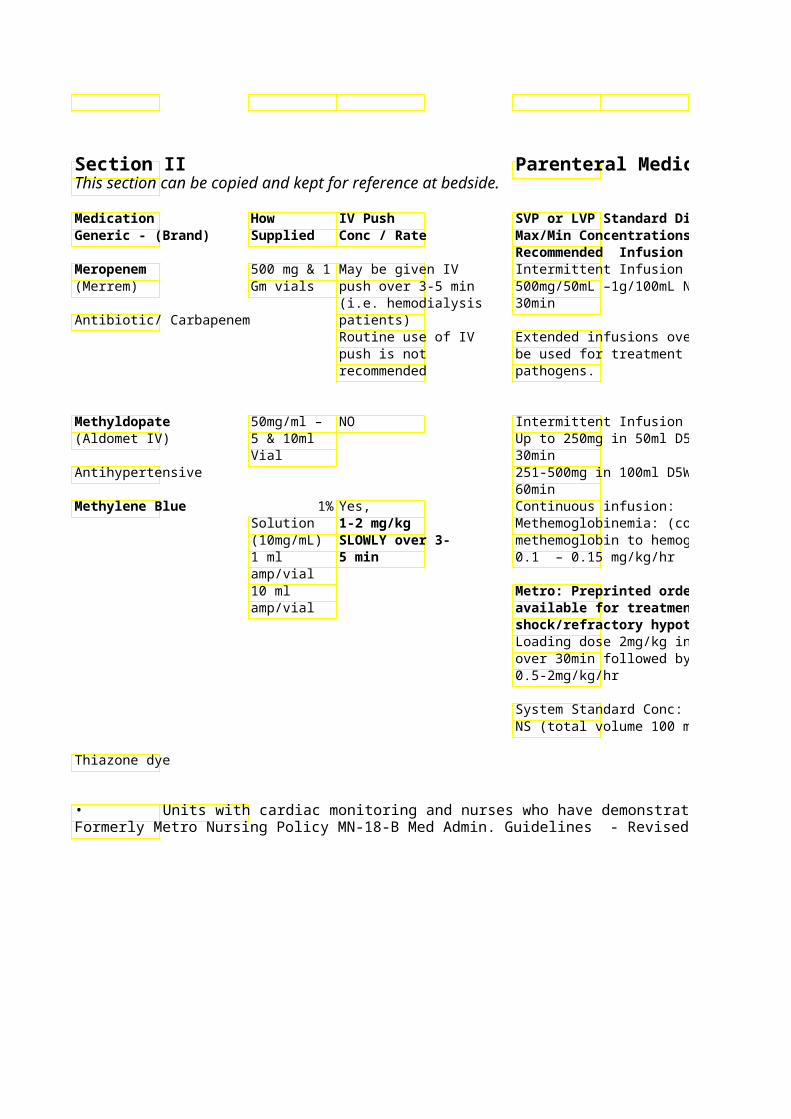
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor for allergic reaction-rash, Stable 24 hr after dilution with hives, and shortness of breath, NS refrigerated pruritus.
Stable only 4 hr after dilution Caution with penicillin allergy with D5W refrigerated Check allergies!
Dose reduction recommended in pts w/ CrCl < 50 ml/min Monitor BP / Orthostasis Uncommon anecdotal reports of paradoxical pressor response with IV methyldopate-blood pressure may increase Urine and feces may turn blue-greenIncompatible with many * See footnote Skin discoloration may also occur. medications/solutions – contact Avoid extravasation – may cause pharmacist necrotic abscesses
Use only NS for dilution Metro: Preprinted order set
Total doses > 7 mg/kg may cause dyspnea, cyanosis, dysrhythmias, hypotension, CNS depression
over 30min followed by infusion of Use with caution in pts w/ severe renal insufficiency or G-6-PD deficiency
System Standard Conc: 500 mg/ 50 ml Administer via Central Line only!Pulse Ox reading may be artificially low during IV administration
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 48Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
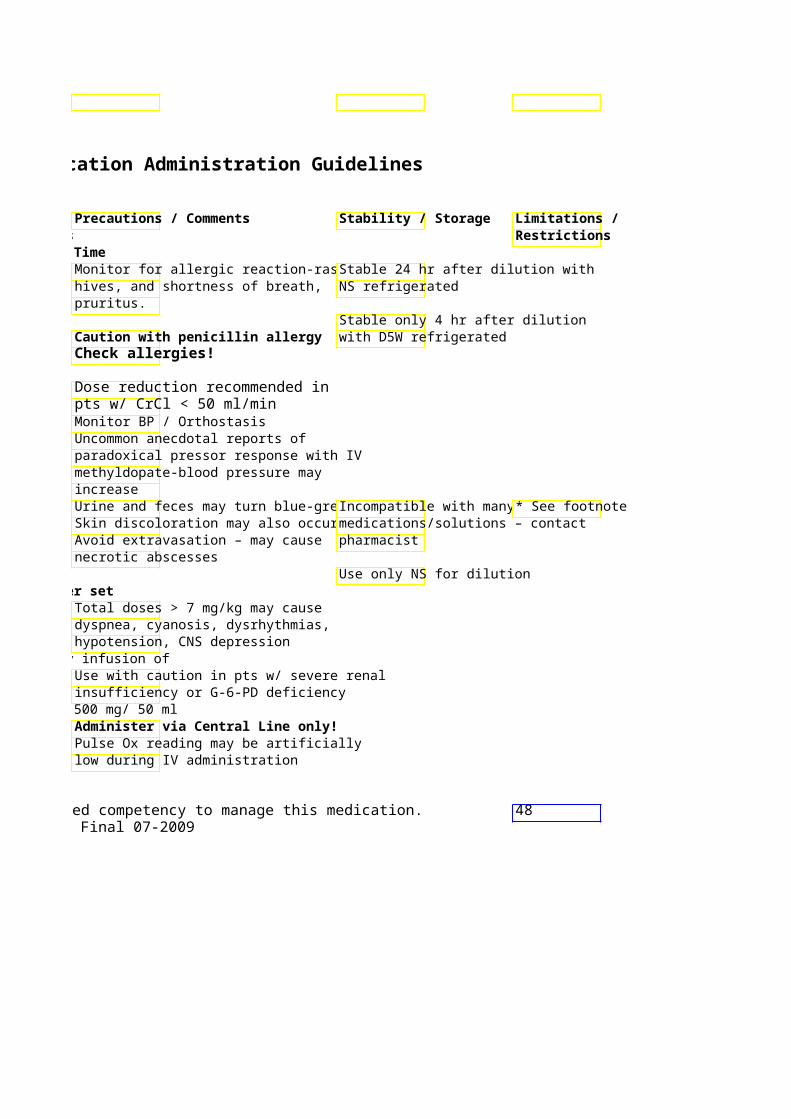
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Methylergonovine 0.2 mg/ml NO Usual dose: 0.2 mg IM q4 hr (Methergine) 1 ml amp Give IM only
0.2 mg over 1 min Uterine Stimulant
Methylnatrexone 12mg / NO Not recommended. (Relistor) 0.6ml vial
SQ Intermittent SQ administration ONLY. Opioid Antagonist administration
ONLY MethylPREDNISolone 40, 125 & Yes – IV Push preferred method of (Solu-Medrol) 500mg at max rate oadministration
Vial, 1&2 mg/min Intermittent Infusion Gm Vial 100-250mg in 50ml NS – give over 1
Corticosteroid min > 250mg in at least 50ml NS – give over 60 min
MetoCLOPramide 5mg/ml in Yes, Intermittent Infusion (Reglan) 2,10, 20 & Give at 5 mg/min Doses > 10mg, dilute in 50 ml. Infus
30 ml Vial over 15 min Prokinetic/antiemetic
MetoPROLOL 1mg/ml – Yes, IV-push preferred (Lopressor) 5ml Give at max rate
Syringe & of 5mg/min Acute myocardial infarction: Cardiovascular/Beta Amp 5 mg IVP every 5 minutes x 3 Blocker • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
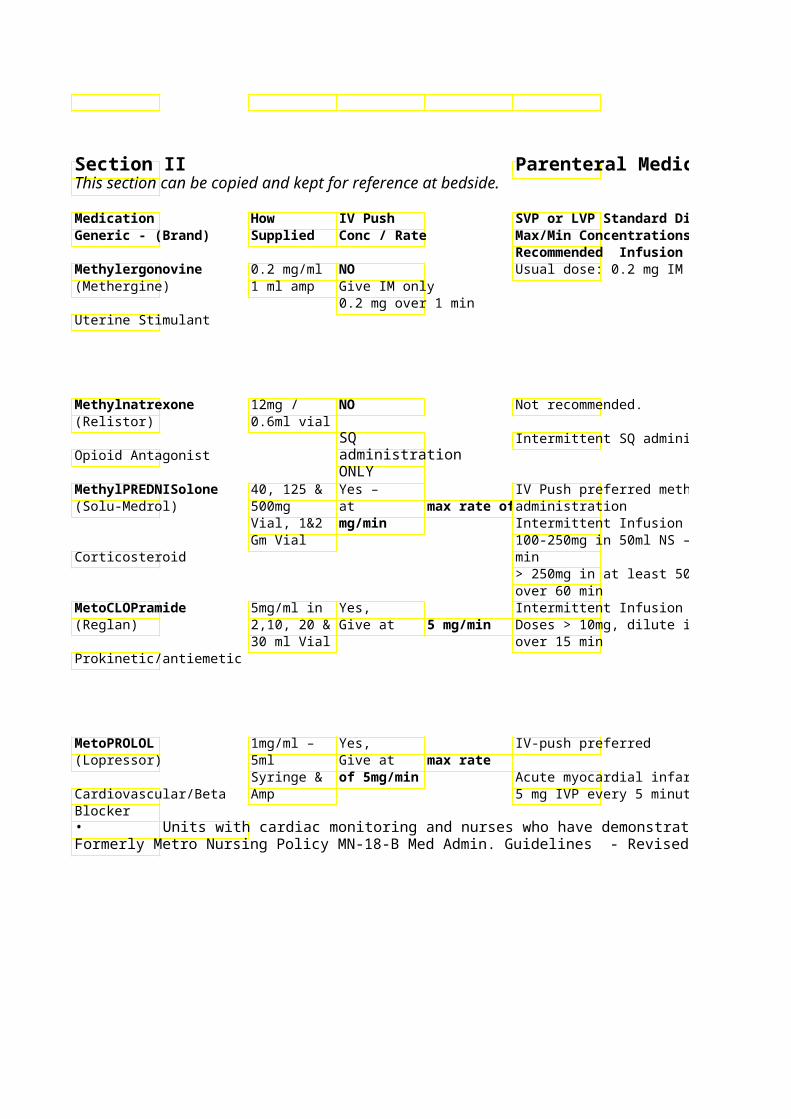
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Usual dose: 0.2 mg IM q4 hr Monitor BP – do not administer if BP Discard discolored solutions
> 140/90
Do NOT give via IV administration due to increased risk of HTN and CVA. Intravenous administration in severe, life-threatening situations ONLY. Usual dose q48h – SQ in upper arm, Store at room temperature. abdomen or thigh only.
Intermittent SQ administration ONLY. Once drawn up in a syringe Frequency not to exceed Q24h dose is stable at room
temperature for 24hours IV Push preferred method of Acute Spinal Cord Injury : Critical Care
Continuous Infusion -- Usual dose: Reconstitute vials with strecommended for 30 mg/kg bolus over 15 min then 5.4water only. May further dcontinuous
100-250mg in 50ml NS – give over 1mg/kg/hr x 23 (or 48) hours with NS. infusion
> 250mg in at least 50ml NS – give ** Depo-Medrol must be given IM – not IV ** Slow rate if extra-pyramidal symptoms Contraindicated
Doses > 10mg, dilute in 50 ml. Infus(dystonia, motor restlessness, in patients with parkinson-like symptoms) occur Parkinson’s Reverse EPS with diphenhydramine disease. (Benadryl) 50mg IV per physician order Contraindicated in Parkinson’s patients. Monitor HR and BP Administer undiluted * See footnote
Acute myocardial infarction: 5 mg IVP every 5 minutes x 3
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 49Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
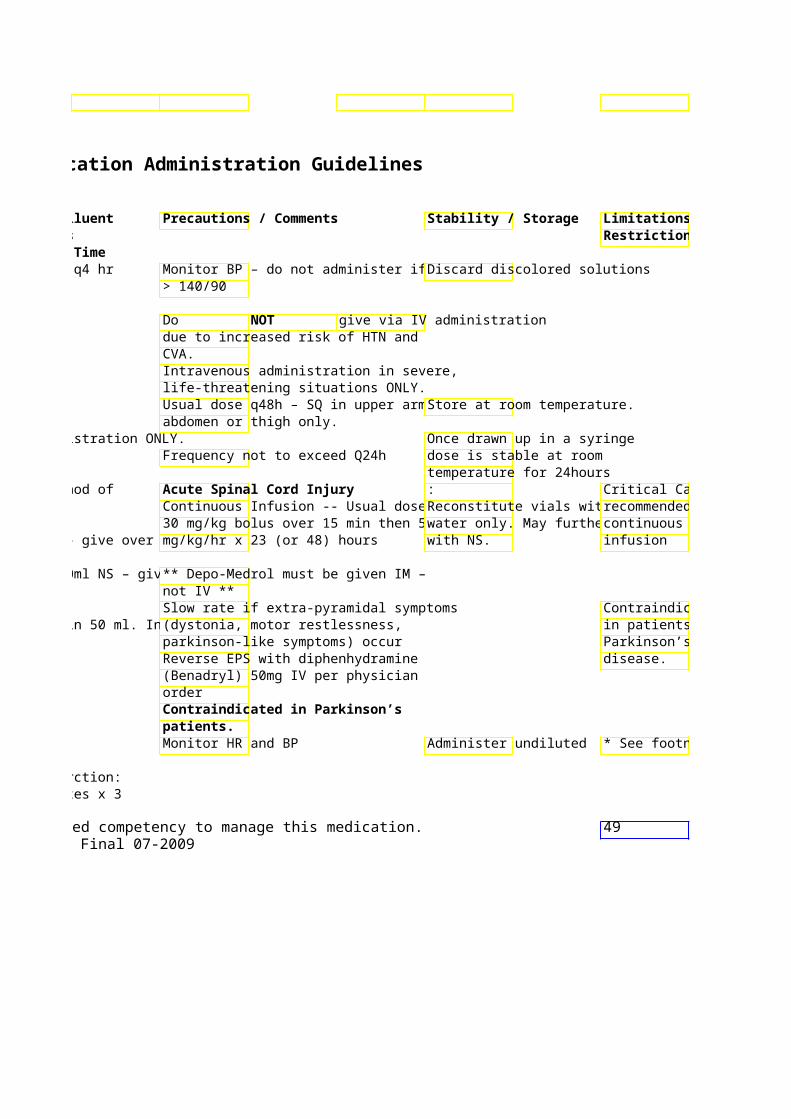
Limitations / Restrictions
Critical Care recommended for continuous
Contraindicated in patients with Parkinson’s
* See footnote
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time MetroNIDAZOLE 500 mg NO Infuse over 60min (Flagyl) Vial,
Premix: 500 mg/100
Antibiotic ml
Micafungin 50 mg, 100 NO For treatment of candidemia, invasiv(Mycamine) mg vials candidiasis, aspergillus infections
Intermittent infusion: 50-150 mg in Antifungal 100 ml NS or D5W infused over 60
minutes MIDAZolam 1 & 5 Yes, Continuous infusion: (Versed) mg/ml 1 – 2.5 mg doses Usual dose range: 0.5 – 10 mg/hr
Vial & over 2 – 3 Syringes minutes. Titrate System Standard Conc: 50 mg/ 100
Sedative/ SLOWLY NS (0.5 mg/ml) Benzodiazepine
Milrinone 200 Yes, Continuous Infusion: (Primacor) mcg/ml- Loading dose 50 Usual dose range: 0.25 – 1
100ml mcg/Kg over 10 mcg/kg/min – titrate to response Premix, minutes
Cardiovascular/ Positive 10 & 20 ml System Standard Conc: 20mg/100 mlD5W Premix (200 mcg/ml)
inotrope vial 1 mg/ml System “Concentrated” Conc: 20
mg/30 ml NS (total volume 50 ml) (400 mcg/ml) Half-life: 1-3 hr
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
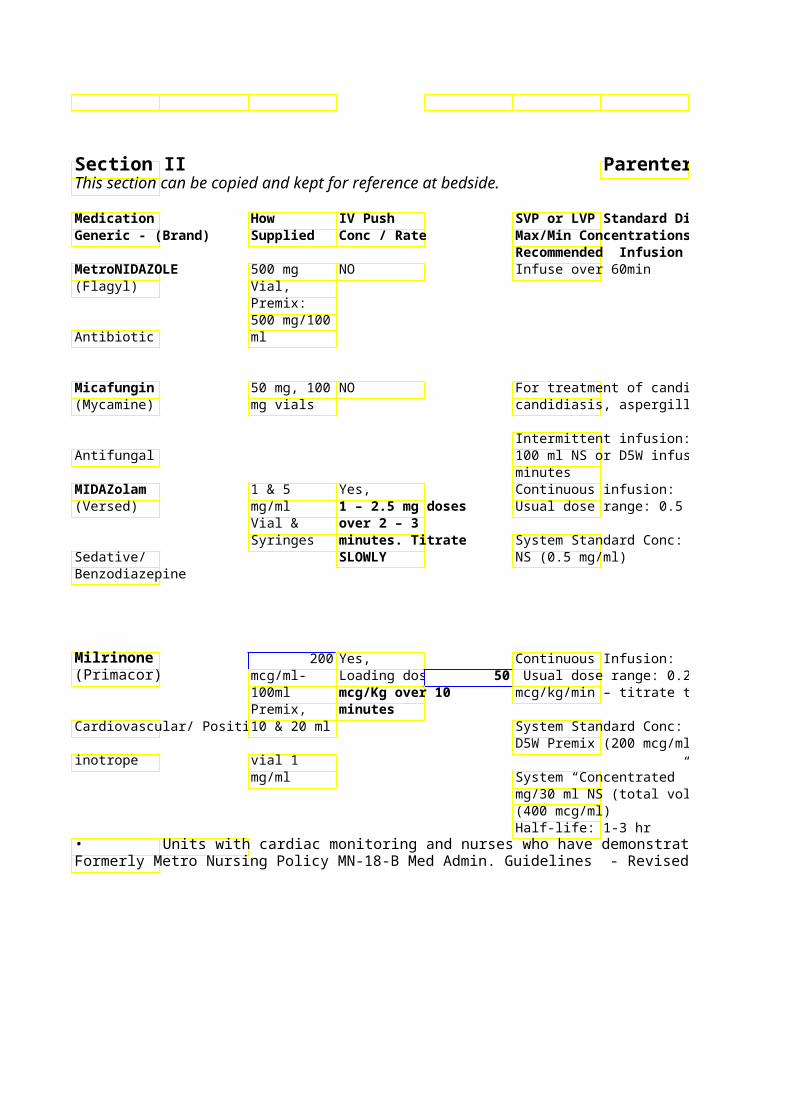
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Incompatible with many meds and May form crystals if solutions – check with pharmacist refrigerated, warm to room
temperature to re-dissolve
Avoid ETOH use during treatment and 72 hours post due to possible disulfiram like reaction
For treatment of candidemia, invasivNo dose adjustments required in Dilute vials prior to candidiasis, aspergillus infections renal/hepatic dysfunction reconstitution with NS (without
bacteriostatic agent) Intermittent infusion: 50-150 mg in 100 ml NS or D5W infused over 60
Titrate doses slowly especially in the *See footnote Usual dose range: 0.5 – 10 mg/hr elderly
Monitor respiratory and Critical Care for System Standard Conc: 50 mg/ 100 cardiovascular status continuous
infusion Rapid and/or frequent administration may cause respiratory depression Reverse effects with flumazenil (Romazecon) Dose reduction recommended for * See footnote
Usual dose range: 0.25 – 1 decreased renal function Incompatible with many meds mcg/kg/min – titrate to response – check with pharmacist
Monitoring: System Standard Conc: 20mg/100 ml Continuous EKG Monitoring D5W Premix (200 mcg/ml)
Following initiation or dose System “Concentrated” Conc: 20 titration: ormg/30 ml NS (total volume 50 ml) q15min x 3, then q1h x 4
then q4h x 2 then q4-6 hours while stable.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 50Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
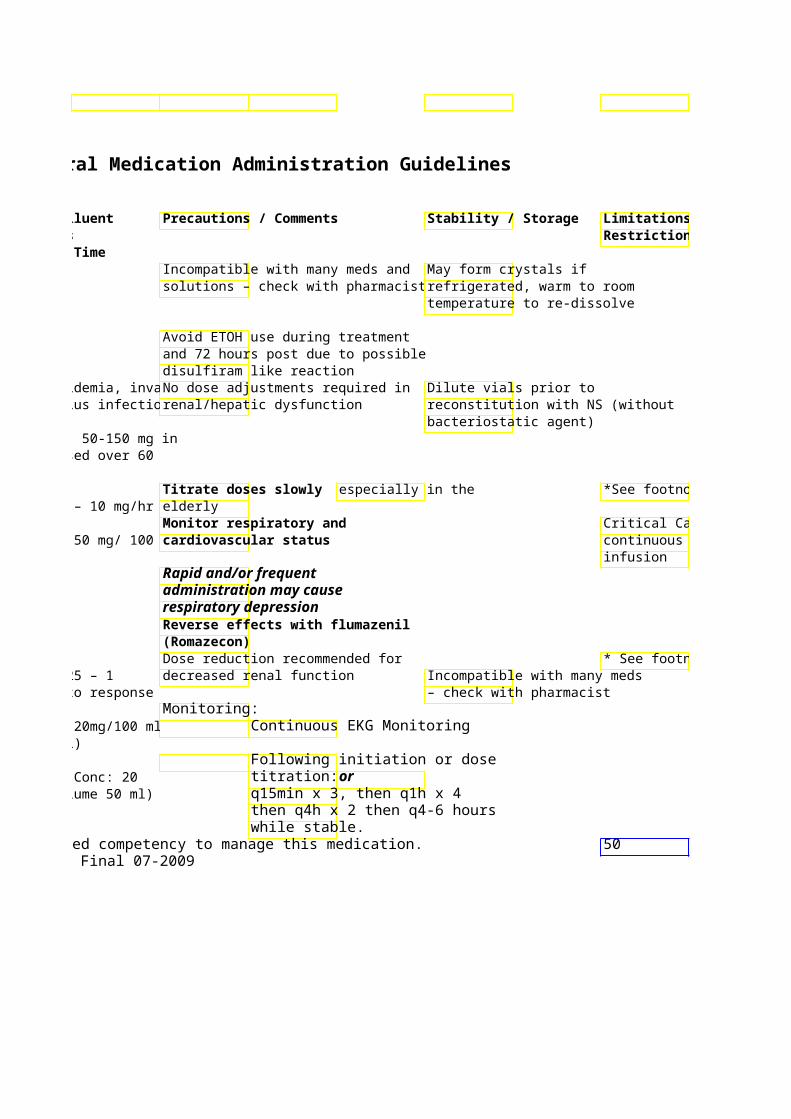
Limitations / Restrictions
*See footnote
Critical Care for continuous
* See footnote
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Morphine Various Yes, Continuous Infusion –
concentra- at max rate of 1 *HIGH ALERT tions, vials mg/min System Standard Conc: 50mg/250ml MEDICATION* & syringes. NS (0.2 mg/ml)
System “Concentrated” 50mg/100ml NS (0.5 mg/
Narcotic analgesic
Chronic pain managemedose is effective dose
Moxifloxacin 400 mg/250NO Infuse over 60 min (Avelox) ml
Premix Antibiotic/ Fluoroquinolone Multivitamin MVI-12 NO Common component of banana bag.
(adult) 10 Vitamin/ Nutritional ml vial Manufacturer recommsupplement minimum volume for infusions of
500 ml.Muromonab CD3 1 mg/ml – Yes, NO (Orthoclone OKT3) 5 ml Amp 5 mg over 60
seconds
Immunosuppressant
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
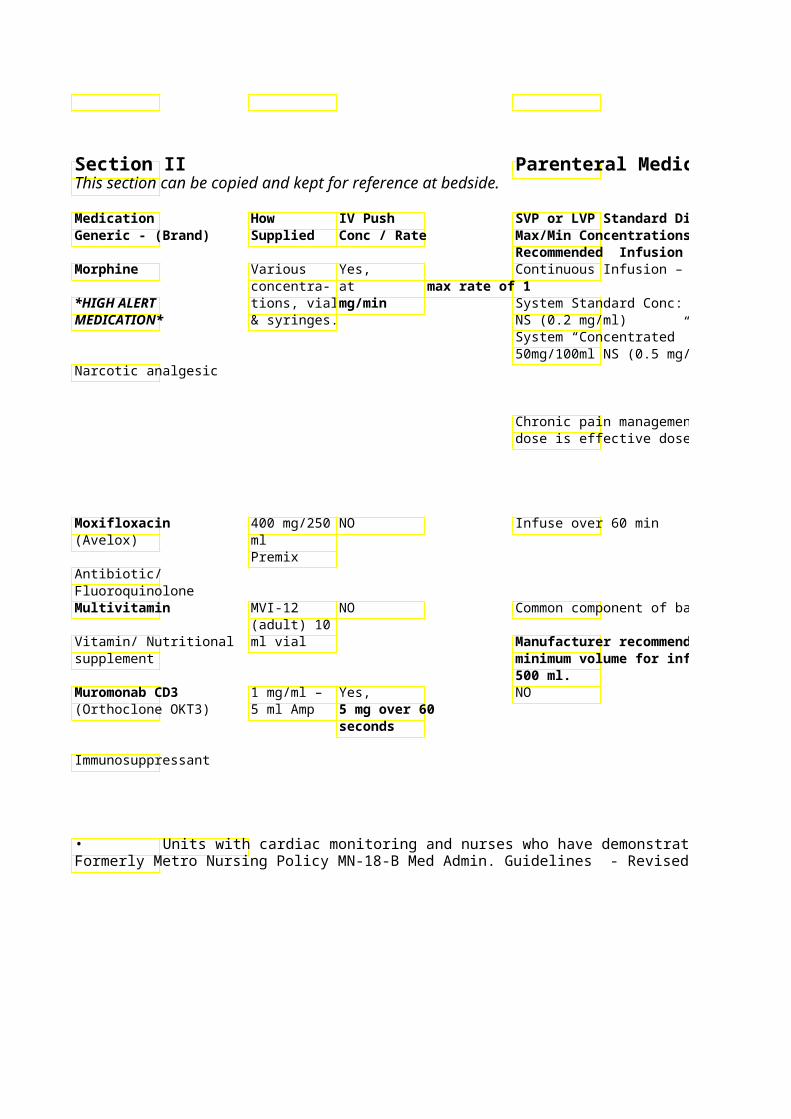
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Max/Min Concentrations Recommended Infusion Time
Hierarchy of effects ? analgesia PCA: Check syringe for ? sedation ? respiratory depression expiration date
System Standard Conc: 50mg/250ml Monitor respiratory and cardiovascular status – may cause respiratory depression/distress
Titrate to dose that relieves pain without excessive sedation – avoid abrupt dose changes Lower doses advised in elderly, debilitated or in patients receiving other CNS depressants Reverse effects with naloxone (Narcan)
Common component of banana bag.
Common component of TPN. minimum volume for infusions of
Pre-dose corticosteroid, antihistamine and acetaminophen recommended
Do not mix with other Be aware of potential for cytokine solutions/medications release syndrome (CRS) & acute hypersensitivity (allergy) reactions with initial doses Dose is 5 mg IV daily x 10-14 days in adults
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
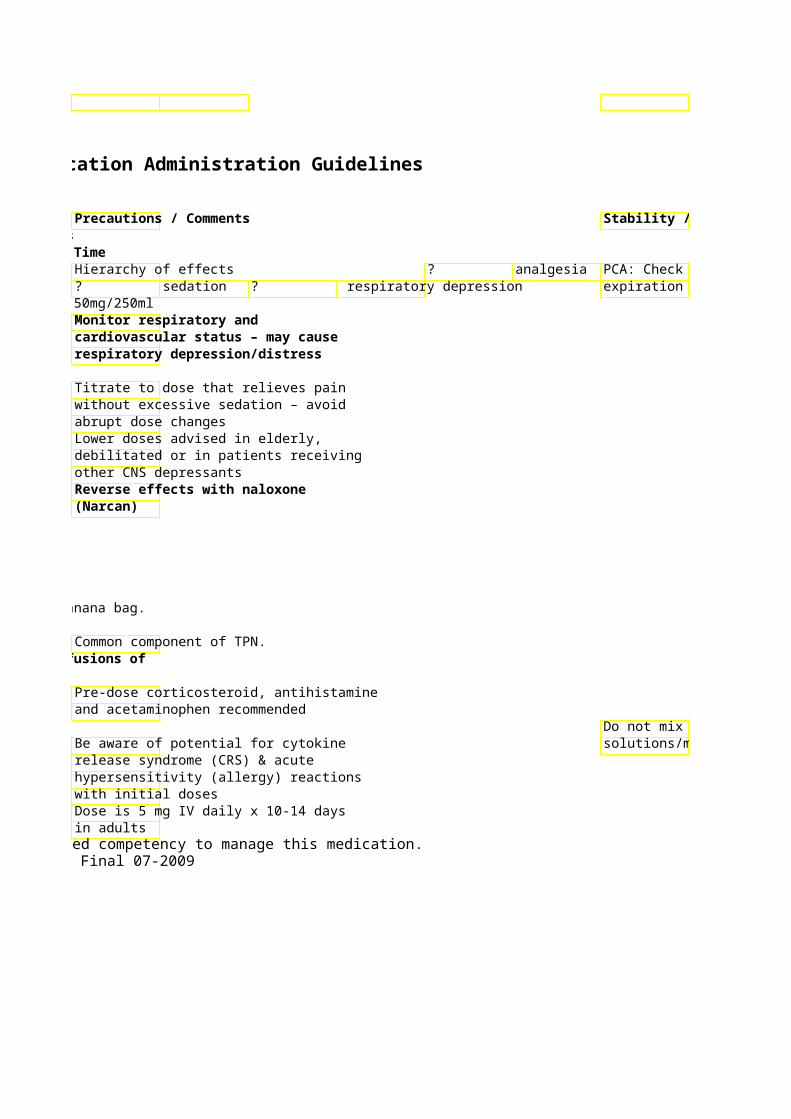
Stability / Storage Limitations / Restrictions
PCA: Check syringe for expiration date
Metro: If PCA ordered, mandatory order set must be used
* See footnote
Do not mix with other solutions/medications
51
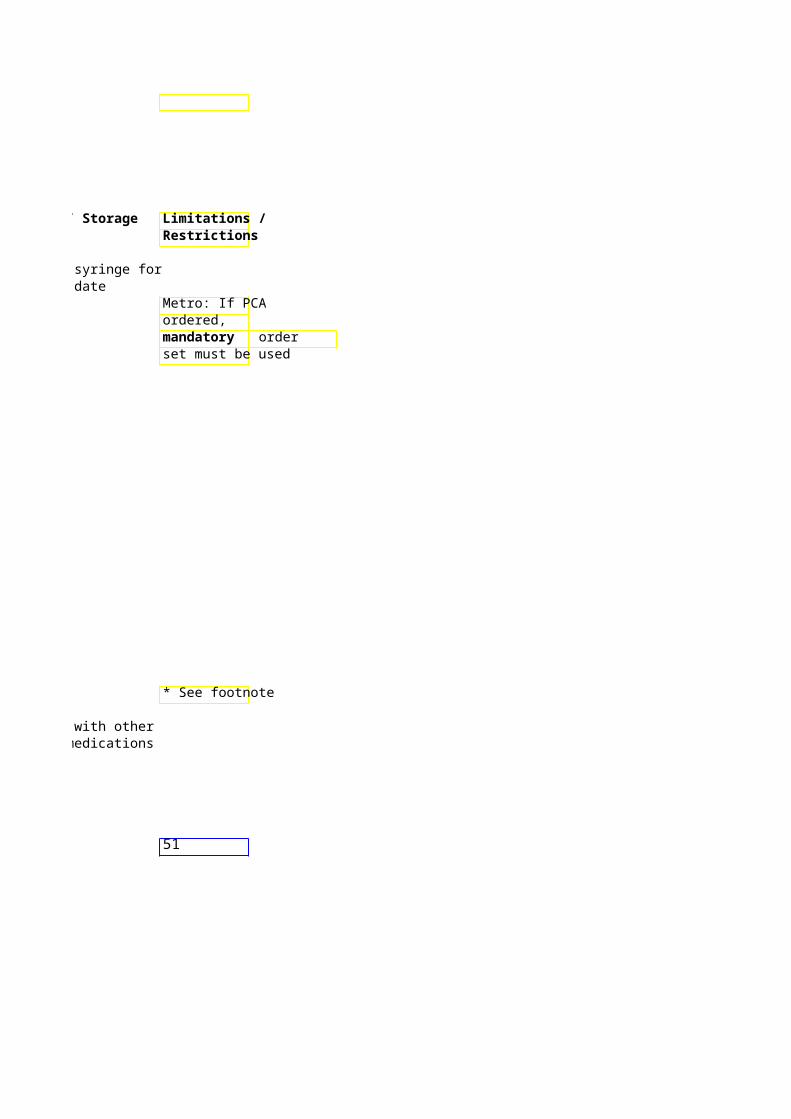
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Mycophenolate mofeti500mg Vial NO Infuse over 2 hours (CellCept)
Immunosuppressant
Nafcillin 1 & 2 Gm NO Intermittent Infusion (Nafcil) Vials < 2 Gm give over 30min
2 Gm/100 > 2 Gm give over 60min ml Premix
Antibiotic/ Penicillin
Nalbuphine 10mg/ml – Yes, Not Advised – Give IV Push (Nubain) 10ml Vial at max rate of 1
20mg/ml – mg/min10ml Vial
Narcotic Analgesic
NaLOXone 0.4 & Yes, Not advised – Give IV Push (Narcan) 1 mg/ml, 0.1 – 0.4 mg over
various size 1 minute Continuous infusion for epidural REVERSAL AGENT syringes & May repeat IV associated pruritis
vials doses at 2-3 min System Standard Conc: 1 mg/250ml Narcotic Antagonist/ intervals or per NS (4mcg/mL)
order System “Concentrated” Conc: 2 Reversal agent for mg/100 ml NS (20mcg/mL) Narcotics• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
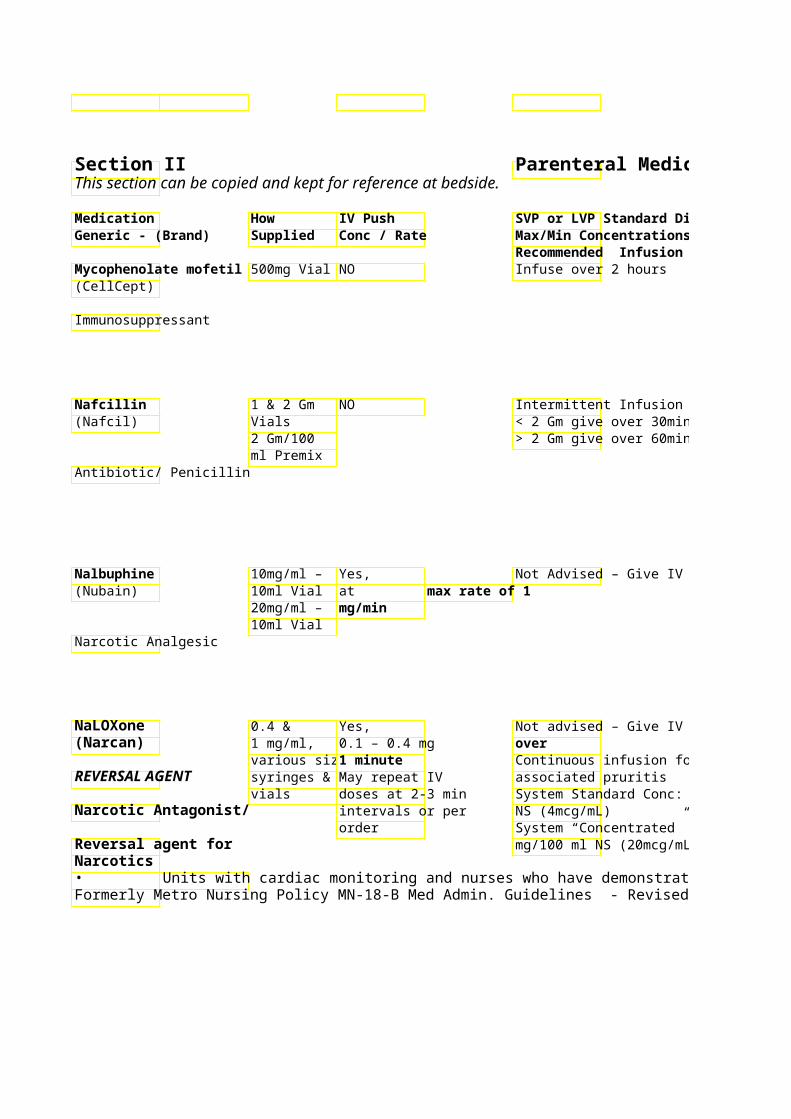
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Each 500mg vial reconstituted with Do not mix with other 14ml D5W solutions/medications Final concentration of solution should be 6 mg/ml Avoid direct contact with solution. If this occurs, thoroughly wash exposed area with soap and water –teratogen. Penicillin -
< 2 Gm give over 30min allergies > 2 Gm give over 60min
Avoid Extravasation – see PPO 5046 for general guidelines / management Tissue damage reported with infiltration – prefer central line administration if available Slow rate or further dilute if phlebitis occurs
Not Advised – Give IV Push 10 mg Nalbuphine = 10 mg IV Morphine
Monitor respiratory status – may cause respiratory depression Reverse with naloxone (Narcan) May cause withdrawal in opioid dependent patients.
Not advised – Give IV Push Used for reversal of narcotic agents Onset of action within 2 min
Continuous infusion for epidural If no response after 10 mg given,
System Standard Conc: 1 mg/250ml question narcotic overdose
System “Concentrated” Conc: 2 Reversal of opiod depression may mg/100 ml NS (20mcg/mL) cause nausea/vomiting, sweating,
tremulous, tachycardia, and HTN. Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 52
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
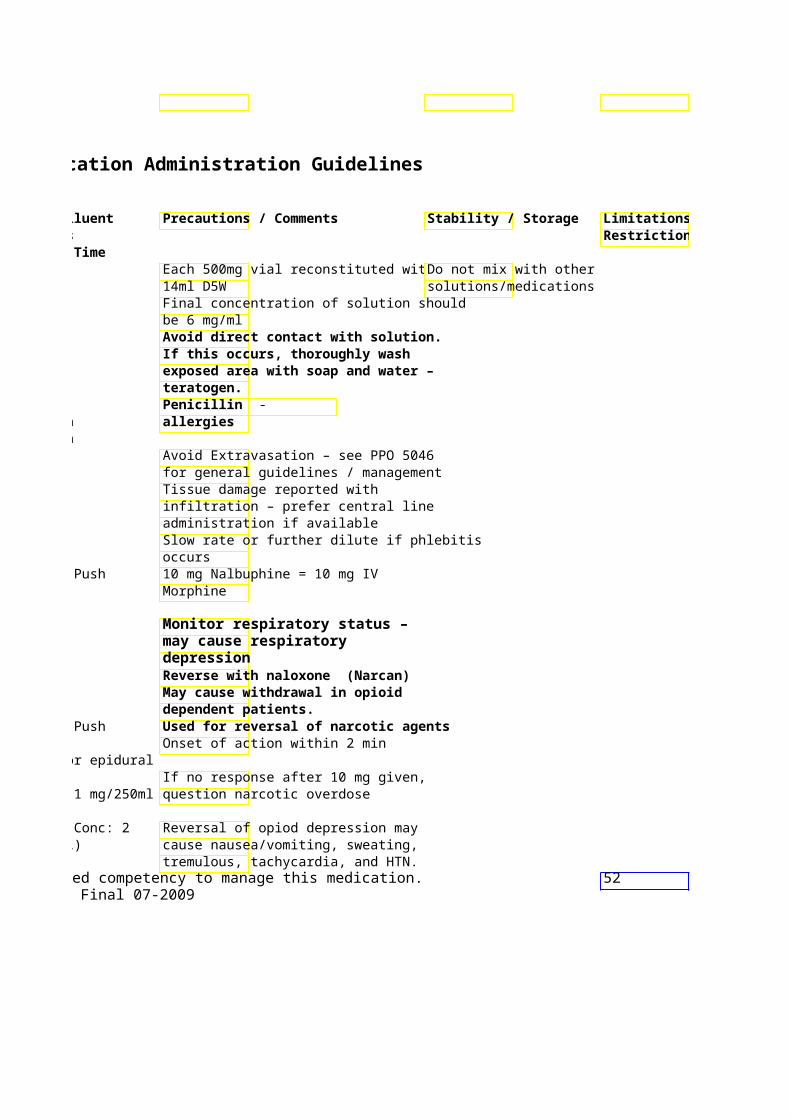
Limitations / Restrictions
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time NATALizumab 300mg/15 NO Intermittent infusion: 3(Tysabri) ml vial ml NS. Infuse over 1 hou
Monoclonal antibody for Multiple Sclerosis & Crohns Disease
Neostigmine 1 mg/ml = Yes, NO (Prostigmin) 1:1000 – 10 0.5 – 2 mg. Give
ml vial SLOWLY 0.5 mg/ml
Anticholinesterase = May give IM 1:2000 – 1 ml amp/vial 0.25 mg/ml Usual max/total = 1:4000 – dose is 5 mg 1 ml amp
Nesiritide 1.5 mg vial Bolus dose: 2 Continuous infusion: Usu(Natrecor) mcg/kg IV push 0.01 mcg/kg/min. Drip m
over 1 minute. increased by 0.01 mcg/kBolus not always needed to maximum dose of 0.03
Cardiovascular/ given. mcg/kg/min. Vasodilator
System Standard Conc: NS (6 mcg/ml)
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
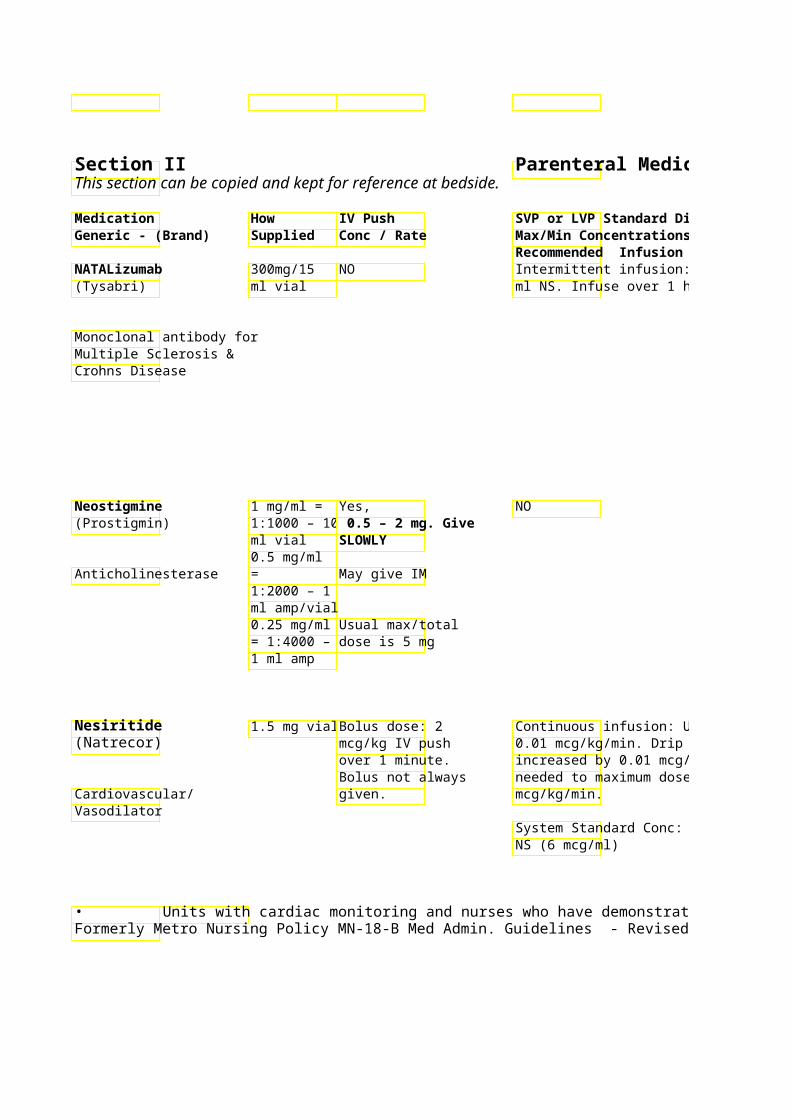
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Restrictions in administration apply –Vials: Refrigerate and prMust be only patient, physician, in fusion center from light administered in and pharmacy must be registered with FDA registered FDA. USE NS ONLY! outpatient
infusion areas – Preprinted order set available for Stable 8 hours after dilu check with site administration in ASLMC refrigerated. Warm to r (i.e. ASLMC – CND and ASLMC ATC. temp prior to infusion. CND/ATC only;
no inpatient May cause infusion-related/ Do NOT shake. Do NOT areas) hypersensitivity reactions. Monitor transport via tube system. patient during and x 1 hour post-infusion. Emergency preprinted order set available. Antidote for non-depolarizing *See footnote neuromuscular blockade (see Precautions/
Comments) Metro: For Acute Colonic Pseudo-Obstruction (Ogilvie’s Syndrome): Per P&T --Bedside telemetry/RN presence required during administration. Give over 10 min. Patients must remain in monitored bed 4-6 hours after administration. Use with caution in renal dysfunction. Decrease dose for CrCl < 50mL/min Monitoring parameters and IV Flush tubing with approx* See footnote incompatibilities available on pre- ml prior to connecting to printed order set patient and prior to bolus if
needed to maximum dose of 0.03 ordered. For initiation or dose titration, Incompatible with heparin, monitor BP every 15 min x 4, every 30 min x 2, every 1hr x 2 hr then insulin, furosemide, every 4 hr. Hold for BP < 90. bumetanide, enalaprilat, and
hydralazine. Consult pharmacist for compatibility information.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 53Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
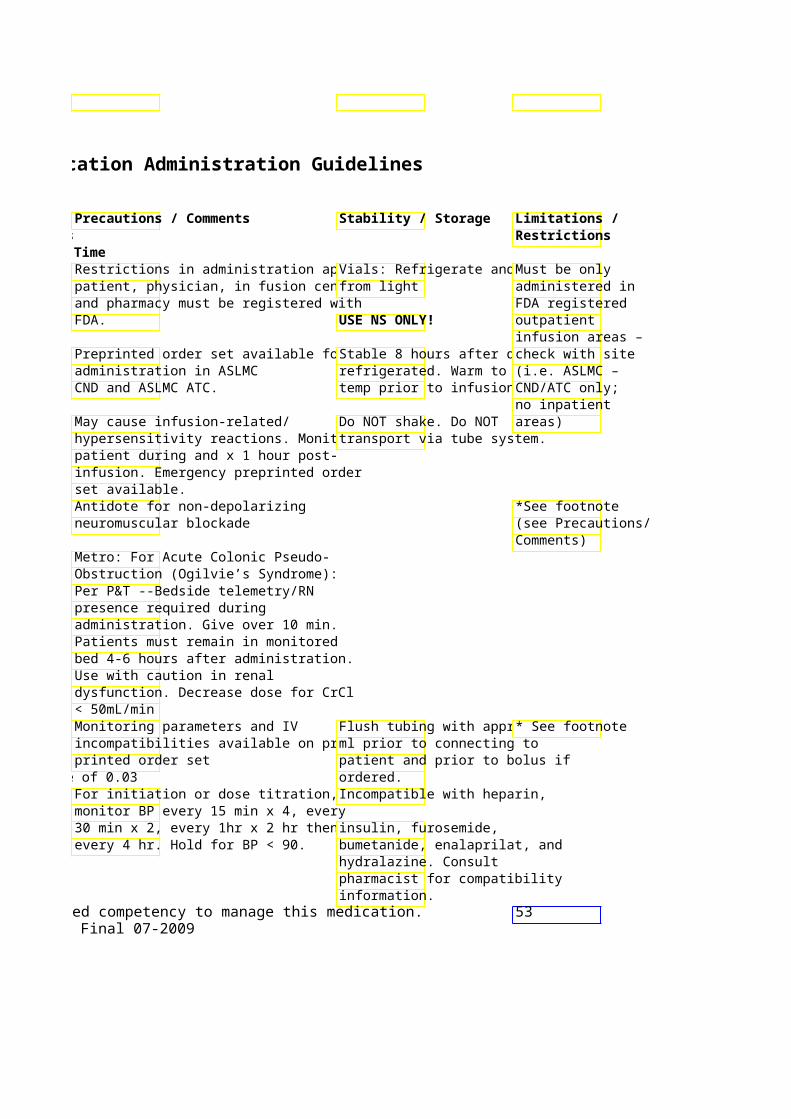
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time NiCARdipine 2.5mg/ml – NO Continuous Infusion (Cardene) 10ml Amp System Standard Conc:
NS (0.1mg/ml) Cardiovascular/ Calcium Channel Blocker System “Concentrated”
mg/80 ml NS (total vol 100 ml) (0.5 mg/ml)
Usual dose range: 2.5 – Recommended titration: Initiate at 2.5-5mg/hr & increase infusimg/hr Q15min until at B15 mg/hr). Once desiredreached, reduce to mainmg/hr.
NitroGLYcerin Vial NO Continuous Infusion – Ini(Tridil) 50mg/10ml mcg/min then titrate by
Premix increments q5min to desCardiovascular/ 50mg/500m Usual dose: 10-200 mcgVasodilator l &
50mg/250m System Standard Conc: l D5W Premix (glass bottl
mcg/ml) System “Concentrated” mg/250 ml NS (glass bottmcg/ml)
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
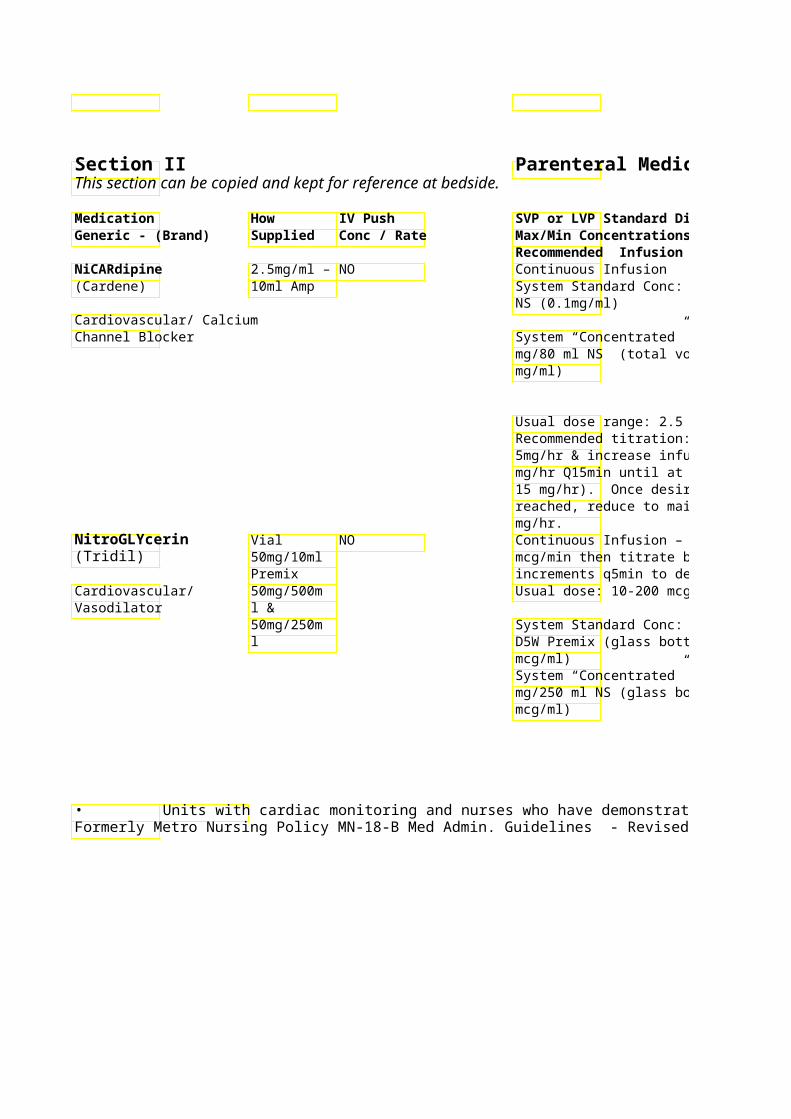
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Rate >3mg/hr: Continuous BP & Critical Care – EKG Monitoring See footnote*
Central line access advised! Rate 1-3mg/hr: Continuous BP & HR vitals or Manufacturer recommends
mg/80 ml NS (total vol 100 ml) (0.5 q4-6h while stable. changing IV site every 12
hours if run peripherally Normally solution light yellow in color
Recommended titration: Initiate at 2.5-Incompatible with Lactated Ringers or bicarbonate solutions – contact pharmacist for compatibility information
Monitoring - For initiation or dose Glass container only * See footnote titration: Continuous BPor Use vented set q5min x 3, then q15min x 3, then Q4-6hr while stable. Check with pharmacist
regarding compatibility Side effects include: hypotension, information. HA (common), tachycardia ** If IV tubing changes are needed, monitor pt every 15 min x 1 hr for possible NTG-retitration. IV tubing sets must be changed every 72 hr. **
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 54Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
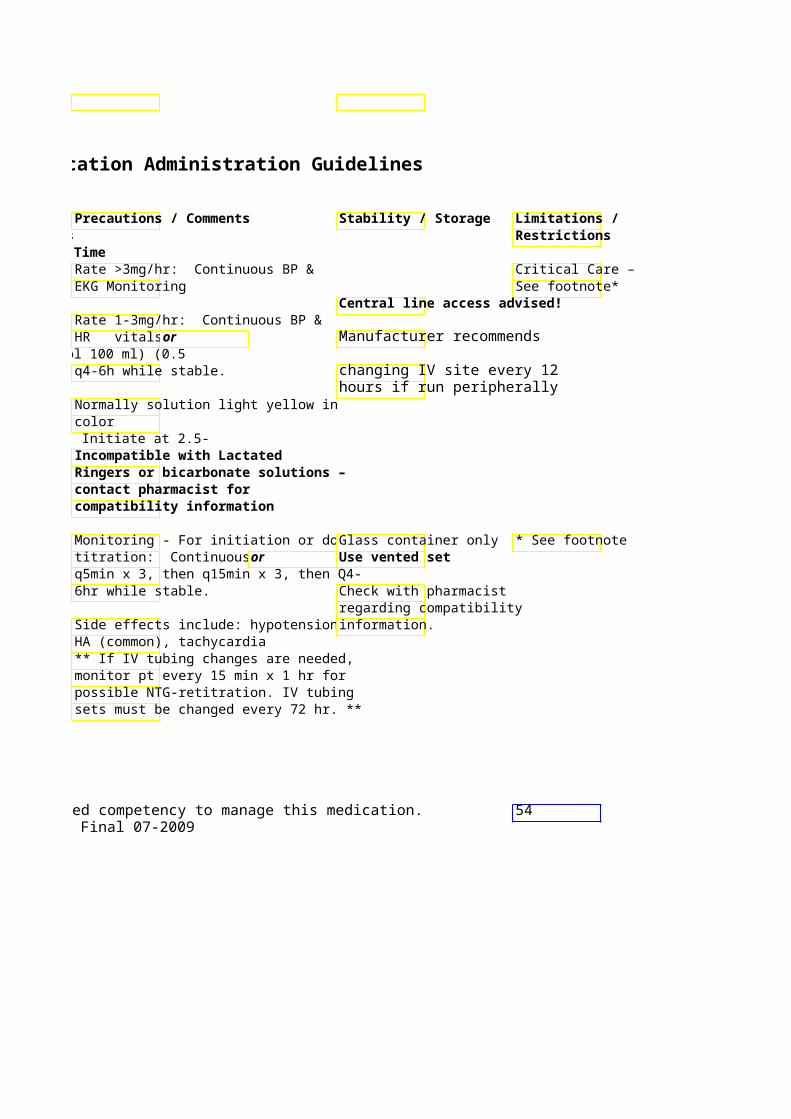
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time NitroPRUSSide 50mg/2 ml NO Continuous Infusion: (Nipride) vial Usual dose range: 0.5 –
mcg/Kg/min Cardiovascular/ System Standard = 50 mVasodilator (200mcg/ml)
System “Concentrated” mg/100 ml NS (500mcg/
Onset: 30-60 sec Peak effect: 1-2 min Duration: 1-10 min Half-life: 3-4 min
Tachyphylaxis has been particularly with doses mcg/kg/min – d/c drug imoccurs!!
Norepinephrine 1 mg/ml- NO Continuous Infusion: (Levophed) 4 ml amp Usual dose range: 2 – 12 mcg/min
Vasopressor System Standard Conc: NS (16 mcg/ml)
System “Concentrated” mg/250 ml NS (32 mcg/ml)
Onset: immediate Duration: 1-2 min
Octreotide 0.05 mg/ml Yes, Intermittent Infusion – (SandoSTATIN) 1 ml, 0.1 Give dose over 3 Dilute with 50ml NS – Infuse over 15
mg/ml 1 minutes minutes ml, 0.5
Hormone - Somatostatinmg/ml 1 ml May be given SQ Continuous IV/Subcutaneous Infusion ampules; System Standard Conc: 500 mcg/250 0.2 mg/ml ml NS (2 mcg/ml) 5 ml, 1 System “Concentrated” Conc: 1000 mg/ml 5 ml mcg/100 ml NS (10 mcg/ml) vials
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
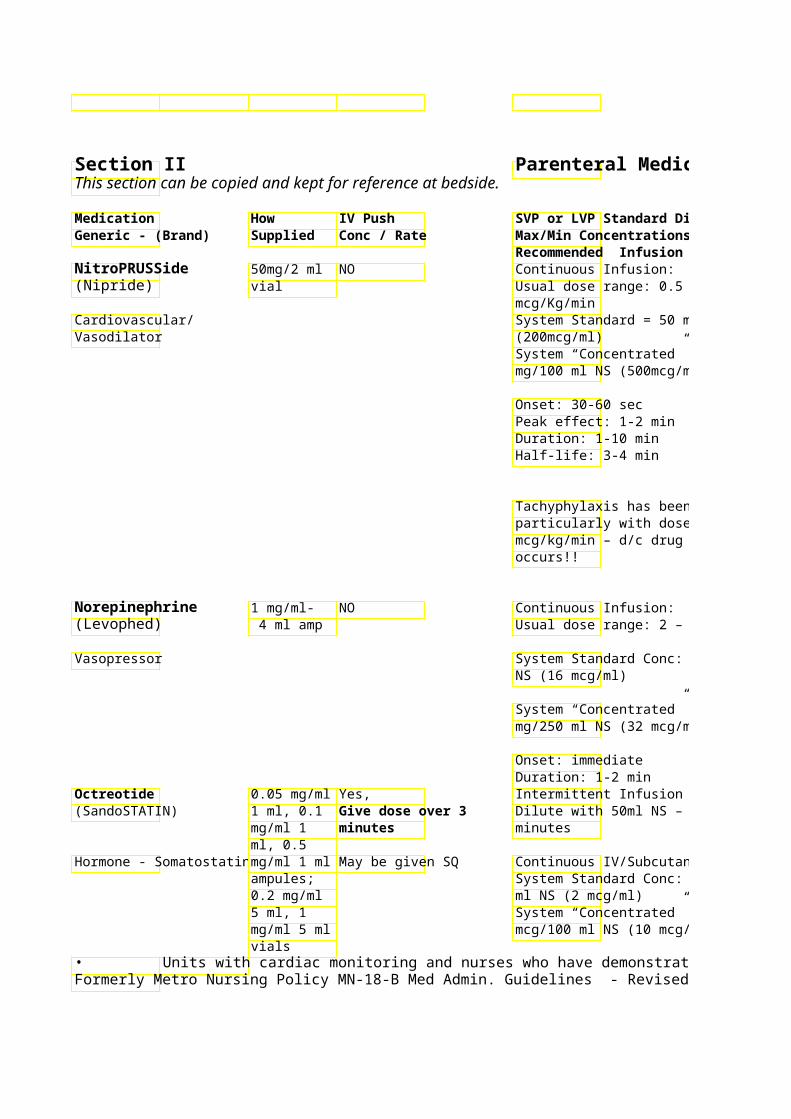
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor BP (via arterial line if Protect from light Critical Care possible) and HR every 15 min Sodium thiosulfate 500mg Monitor urine output every 1-2 hr may be added to each Excessive infusion may produce nitroprusside infusion bag to cyanide toxicity. Monitor for signs decrease cyanide formation. and symptoms of cyanide toxicity: Addition is recommended mental status changes, dyspnea, HA,when nitroprusside dose is N/V, ataxia, absent reflexes, distant > 2 mcg/kg/min for more than heart sounds, widely dilated pupils, one hour or for infusion shallow breathing, and coma. duration > 72 hr Increased risk of cyanide toxicity in pt with renal dysfunction or hepatic insufficiency. ** Do not run infusion at 10
mcg/kg/min for longer than 5-May need to check thiocyanate 10 min – if this high of dose (renally cleared metabolite) levels. needed, call physician for S/sx thiocyanate toxicity: fatigue, alternative** muscle weakness, tinnitus, confusion, psychosis, hallucinations, nystagmus, coma Central Line Advised! Critical Care
Usual dose range: 2 – 12 mcg/min Avoid infiltration – Phentolamine Check with pharmacist (Regitine) SQ recommended for regarding compatibility management of infiltration
information ( PPO 5046)
mg/250 ml NS (32 mcg/ml) Monitor BP, HR every 5-15 min
Monitor urine output every 1-2 hr Refrigerate undiluted product
Dilute with 50ml NS – Infuse over 15 Multi-dose vial stable 14 days refrigerated after initial use
Continuous IV/Subcutaneous Infusion System Standard Conc: 500 mcg/250
System “Concentrated” Conc: 1000 mcg/100 ml NS (10 mcg/ml)
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 55Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
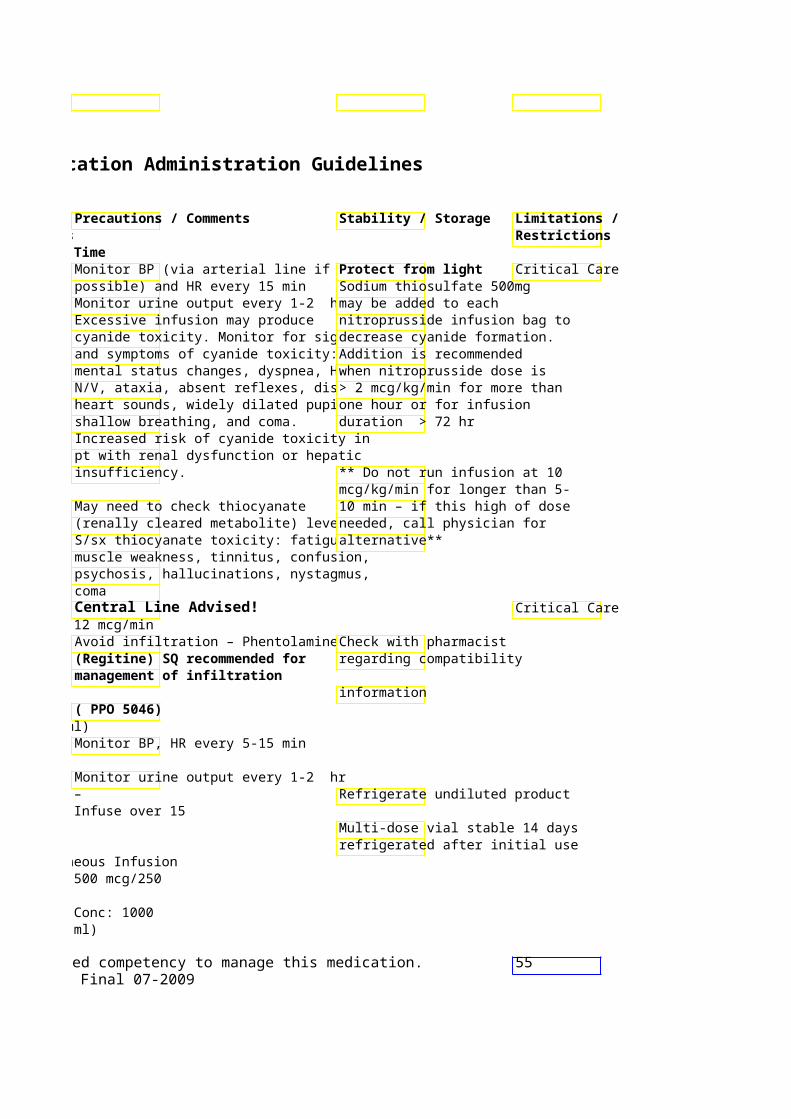
Section IIThis section can be copied and kept for reference at bedside.
Medication How IV Push Generic - (Brand) Supplied Conc / Rate
Ondansetron 2mg/ml – 2 Yes, (Zofran) & 20ml 4 mg over 1-2
Vials min for post-op Antiemetic/ 5HT3 nausea/vomiting receptor antagonist
Oxytocin 10 units/ml NO (Pitocin) 1 ml
syringe/vial
*HIGH ALERT MEDICATION*
Hormone – Uterine stimulant
Pamidronate 30 mg/10 NO (Aredia) ml and 90
mg/10 ml vials
Bisphosphonate
Pancuronium 1 mg/ml 10 Yes, (Pavulon) ml vial, 0.1 mg/Kg bolus
2 mg/ml 2 given rapidly *HIGH ALERT ml and 5 ml MEDICATION* vials/
syringes Neuromuscular blocker
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
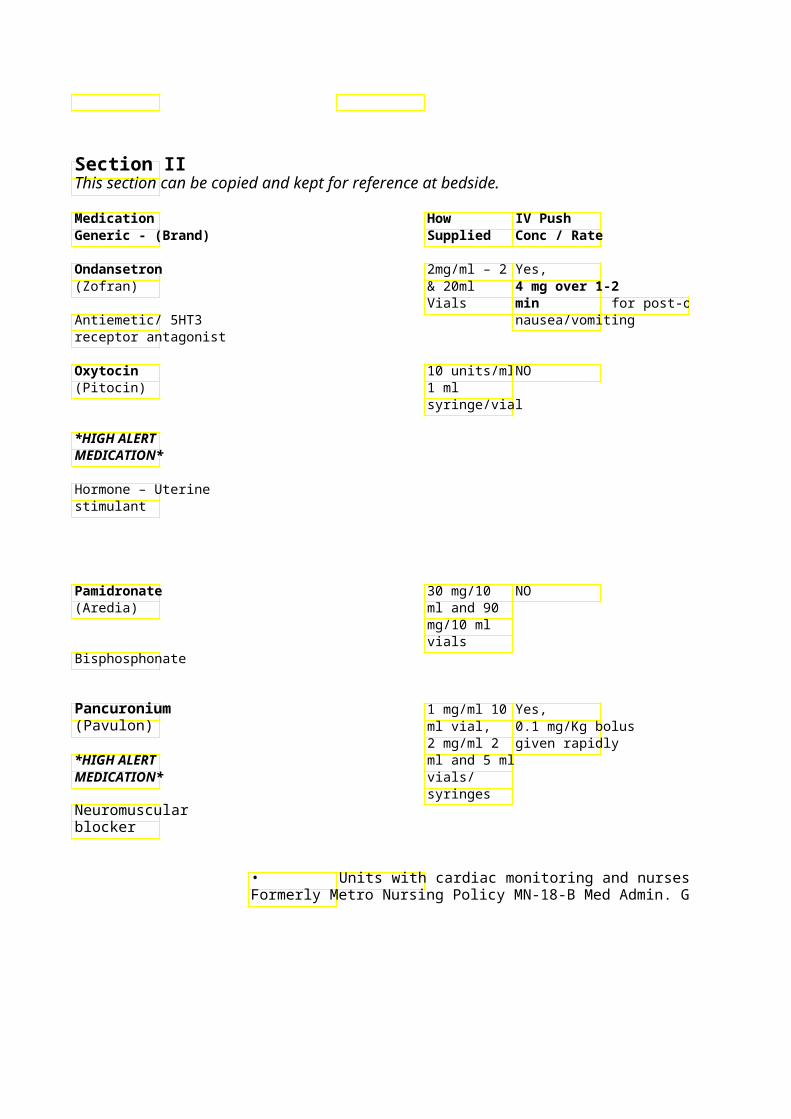
Parenteral Medication Administration Guidelines
SVP or LVP Standard DPrecautionStability / Storage Max/Min Concentrations Recommended Infusion Time Intermittent Infusion – Recommended max dose is 32 8, 12, 16, 20 or 24 mg i mg/day Infuse over 15 minutes
Flat dose response from 1-4mg. Continuous infusion: Max of 32mg/day Continuous Infusion – Metro: See MWH-11-MAT: Induction of labor: 1-2 miWomen’s Health Policy and increase by 1-2 milli-uni Procedures – Maternal for Oxytocin: minutes as needed Induction and Augmentation of Labor
System Standard Conc: 2Metro: Pre-printed order set available ml NS (0.02 units/ml) for Labor Induction/Stimulation
System “Concentrated” See site specific administration policy units/ 1000 ml NS (0.04 units/ml)
Monitor VS – may cause Postpartum Hemorrhage: hypotension, hypertension, titrated to absence of h bradycardia Infuse over 3 to 24 hr Renal function should be assessed
prior to each dose
Dose should not exceed 90 mg May cause HTN and bone pain Infusion site reactions possible – slow infusion rate if occurs
Continuous Infusion – Refer to ClStore undiluted product (vial) System Standard Conc: on Neuromunder refrigeration NS (total volume 100 ml)(i.e MN13)
Refer to Preprinted order sets available for ICU neuromuscular blockade
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
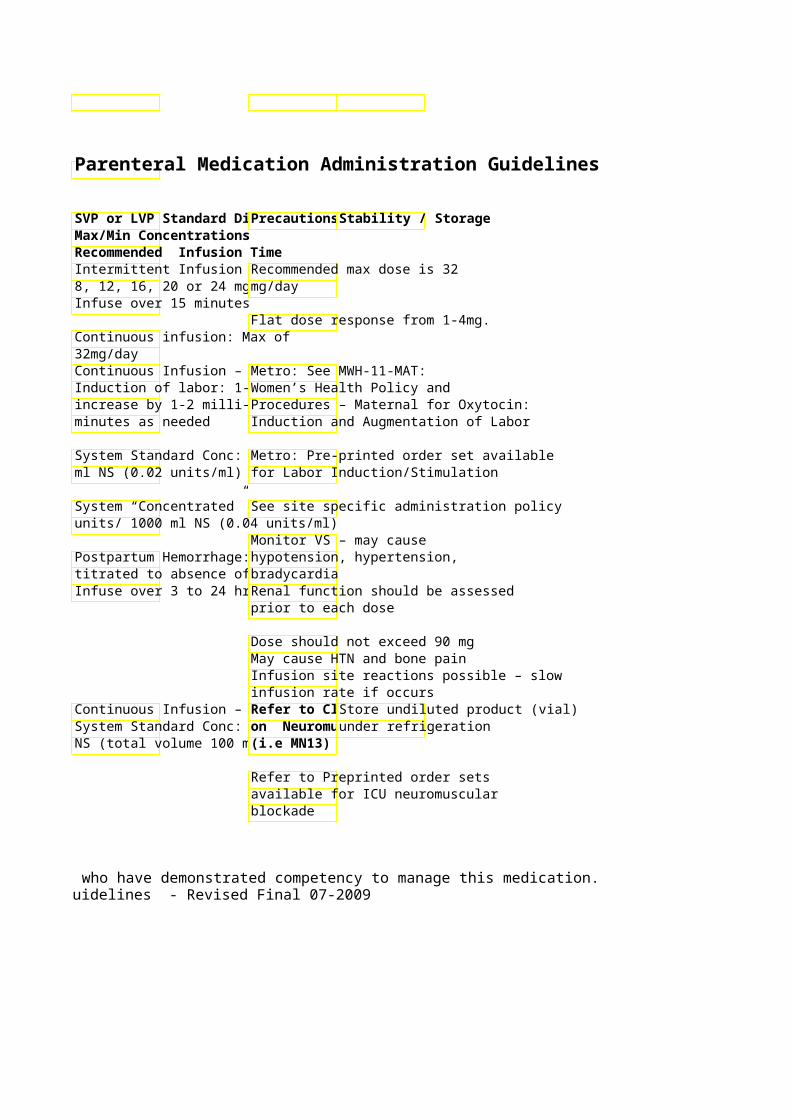
Limitations / Restrictions
Controlled airway and ventilation required; Critical Care only
Sedation must be administered prior to and during paralytic use! 56
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Pantoprazole 40mg Yes, Continuous infusion: (Protonix) /10ml vials 40–80mg over
2min System Standard Conc: 80 mg/ 500 ml NS (0.16 mg/ml)
Proton Pump Inhibitor Dilute 40 mg vial System “Concentrated” Conc: 80 mg/ with 10 ml NS 100 ml NS (0.8 mg/ml)
Parenteral Nutrition----------- No (PN)
Paricalcitrol 2 mcg/ml 1 Yes – IV push preferred (Zemplar) ml, 5 mcg/min
5 mcg/ml 1 Vitamin D Analog ml
vials • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
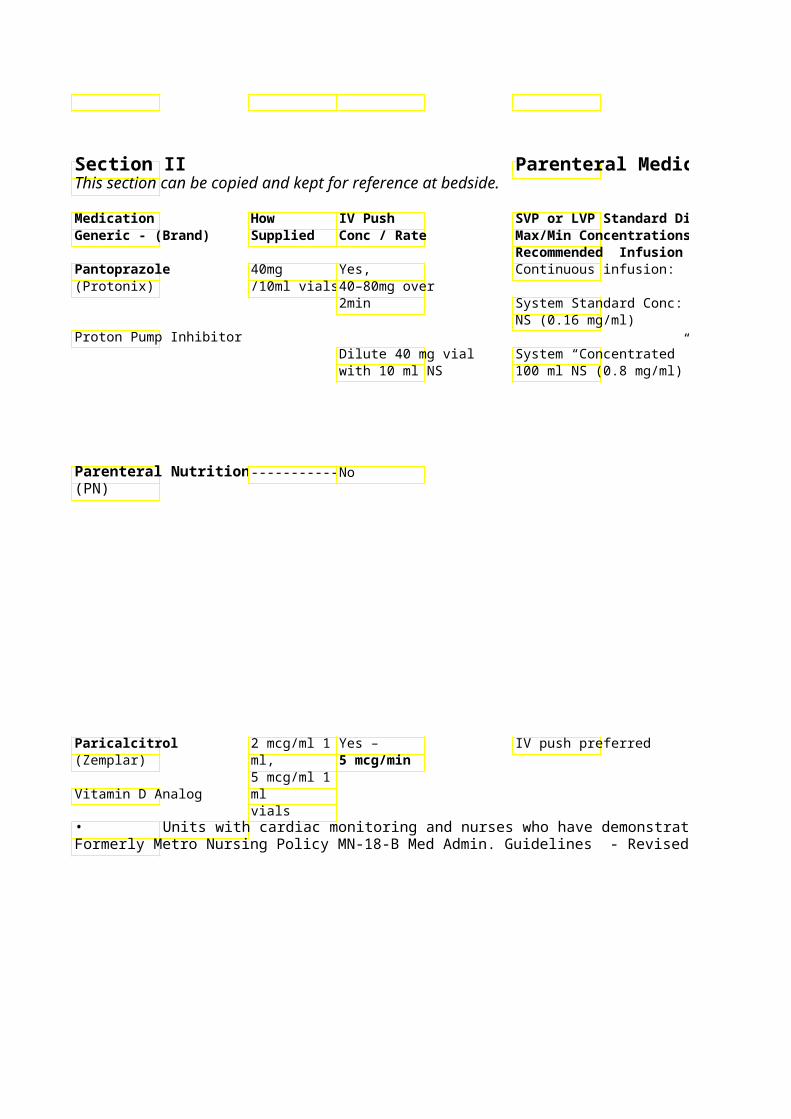
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Continuous infusion duration should Vial: stable at room not exceed 72 hr temperature or refrigeration 24
System Standard Conc: 80 mg/ 500 ml hrs after reconstitution. Run separately!! Do not infuse with any other medication !! Intermittent / Continuous
System “Concentrated” Conc: 80 mg/ Infusion (40mg-80mg/100mL): Check with pharmacist for possible Stable for 24hrs room temp. compatible medications.
Infusion (80mg/500mL NS): Stable for 12hrs at room temp. Filtration not required during preparation or administration.
Route of administration:Central lineDo not administer any
If no central line acce , confirm wi medications/solutions/blood pharmacist that osmolality (< 900 products etc. with PN. If millimoles) is appropriate for alternative IV access is a peripheral administration.
problem, contact the pharmacist for compatibility
PN which includes lipids: change information. tubing every 24 hours. Use 1.2 micron filter for PN with lipids. PN with no lipids: change tubing every 96 hours. Use 0.22 micron filter for PN without lipids. Avoid Extravasation – see PPO 5046 for general guidelines / management Used in the prevention and treatmenDiscard vial after use. of secondary hyperparathyroidism in chronic renal failure patients.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 57Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
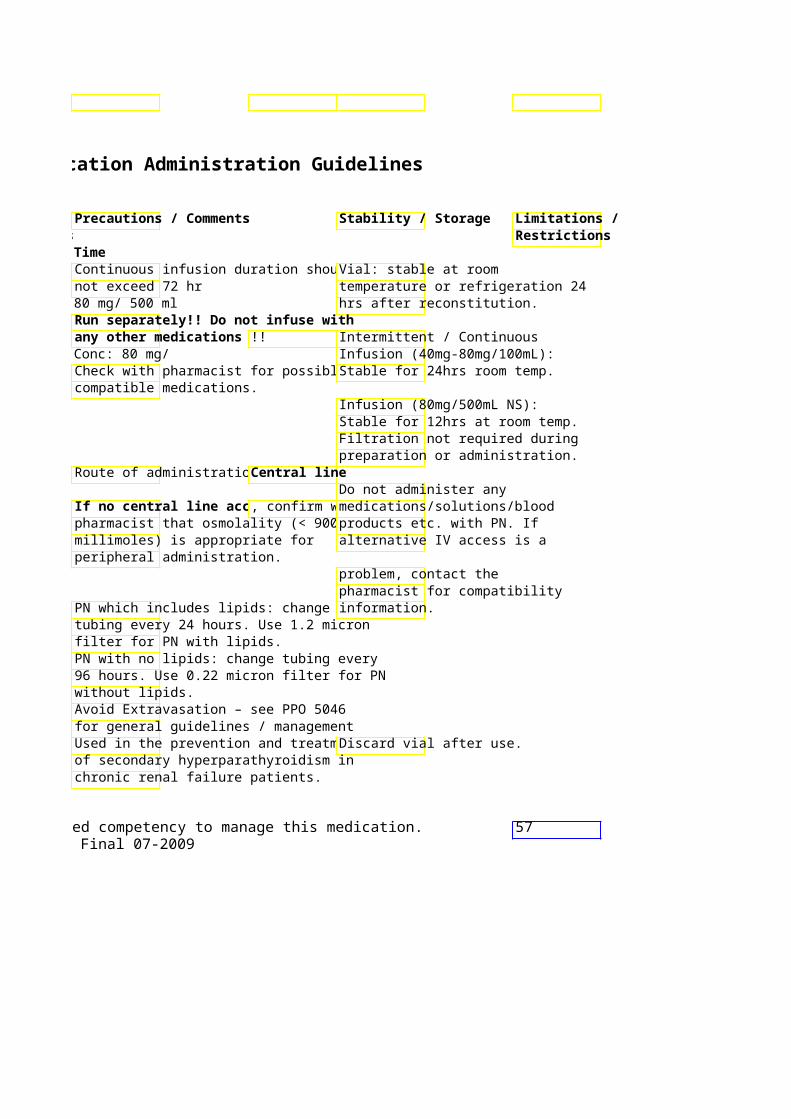
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / RateMax/Min Concentrations
Recommended Infusion Time Pegfilgrastim 6mg/0.6ml NO Give only SQ!! (Neulasta) syringe Give 6 mg SQ as
a 1 time dose onlyWhite cell stimulating hormone Penicillin G 1,5,10 & 20 NO Intermittent Infusion – (sodium or potassium Million Up to 3 Million Units/50 ml NS. Infusesalt) Unit Vials over 30 minutes
Premix: 3 3.1 - 5 Million Units/100 ml NS. Million Infuse over 60 minutes
Antibiotic/ Penicillin Unit/50ml container
Pentamidine 300mg vial NO Intermittent Infusion – (Pentam) 4 mg/Kg diluted into 250ml D5W –
over 60 minutes
Antiprotozoal
Nebulized product also available.
Pentazocine 30 mg/ml 1 Yes, Not recommended (Talwin) ml syringe Max rate of 5
and amp, mg/min 30 mg/ml
Narcotic Analgesic 10 ml vial
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
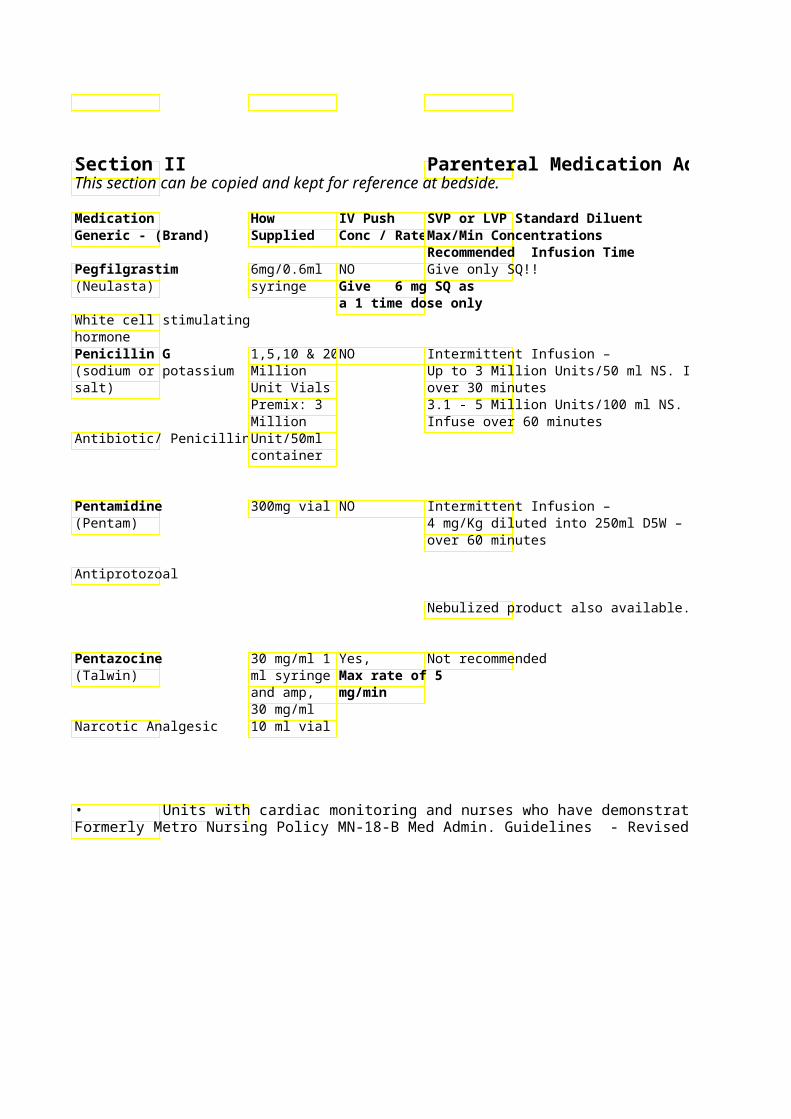
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Restrictions
Long acting filgrastim Refrigerate May cause bone pain
Do not shake product or transport via tube system
Penicillin allergy precautions – Check allergies
Avoid rapid infusions – seizures may result Dose reduction recommended for CrCl < 50 ml/min Watch K+ -- 1 million units PCN G contains 1.7 mEq K+ Monitor BP every 15 min during 60 min infusion
Do NOT refrigerate – Administer in supine position crystallization may occur Monitor blood glucose daily during therapy-hypoglycemia common Daily BUN/SCr, and LFTs recommended Metallic taste noted to be common Recommended max dose is 360 Pentazocine 30 mg = Morphine mg/24 hr 10 mg IV
Monitor respiratory status – may cause respiratory depression Reverse with naloxone (Narcan)
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 58Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
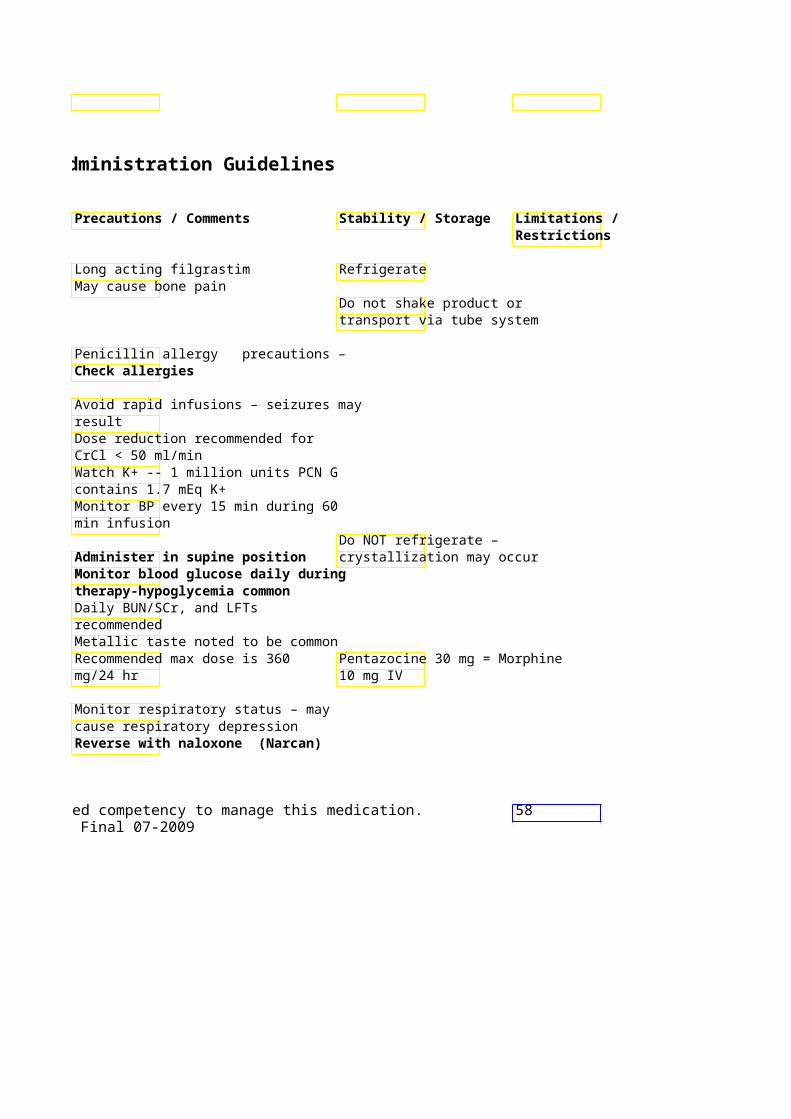
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time PENTobarbital 50mg/ml – Yes, (Nembutal) 1 ml Give slowly at System Standard Conc:
syringe, 20 max rate of 50 ml NS (total volume 250 & 50 ml mg/min mg/ml) Vials
*HIGH ALERT Metro: Preprinted order sMEDICATION* for Barbiturate Coma for
Refer to ICP protocol (Sedative/ Barbiturate Loading /Bolus Doses:
over 15-60min, respectivContinuous Infusion: Init1.5mg/kg/hr.
Perphenazine 5 mg/ml 1 Yes – but only use (Trilafon) ml amp IV if absolutely
necessary Dilute 5 mg w/ 9
Antipsychotic Agent ml NS and give 0.5 mg/min IM administration recommended
PHENObarbital 60 mg/ml 1 Yes, Intermittent Infusion: (Luminal) ml, 130 Give slowly at Loading dose: 15mg/kg i
mg/ml 1 ml max rate of 60 Infuse over 15-30 minutes syringes mg/min
Anticonvulsant/ Maintenance doses: 1-Sedative/ Barbiturate (divided doses) may be g
push
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
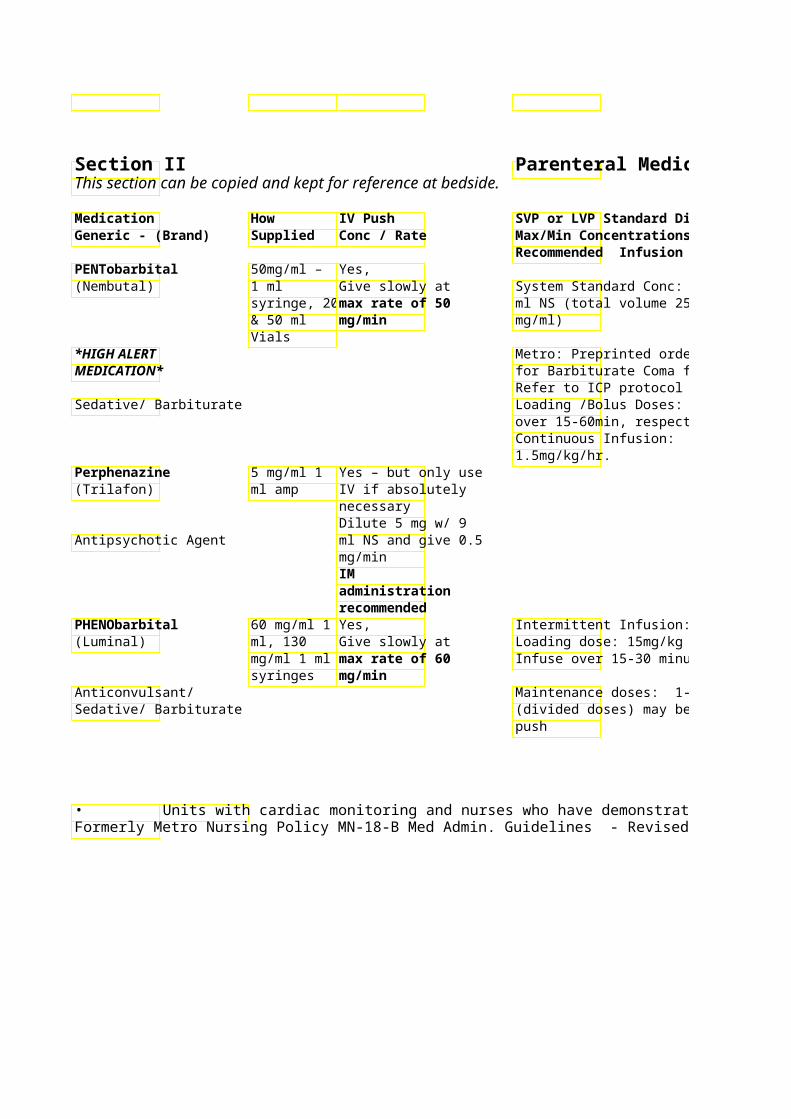
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Undiluted solution is alkaline – avoidIncompatible with most Controlled infiltration. Central line medications/solutions – airway and administration preferred. with pharmacist ventilation
required – With IV administration Use 0.22 micron filter with monitor respiration & cardiac infusion Critical care function continuously only! Monitor pentobarbital levels. Goal levels: Hyponotic/sedation: 1–5 mcg/ml Coma: 10-50 mcg/ml
Usual dose is 1 mg every 2-3 min Recommended max dose is 5 mg
May cause contact dermatitis; Extrapyramidal symptoms (ie. Dystonia rxn) possible
Postural hypotension may occur – monitor BP Undiluted solution is very alkaline – *See footnote avoid infiltration
Infuse over 15-30 minutes Incompatible with most Critical Care for Monitor BP, HR, RR medications/solutions – continuous With continuous IV administratiowith pharmacist infusions monitor respiration & cardiac function continuously Too rapid administration may cause respiratory distress and hypotension
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 59Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
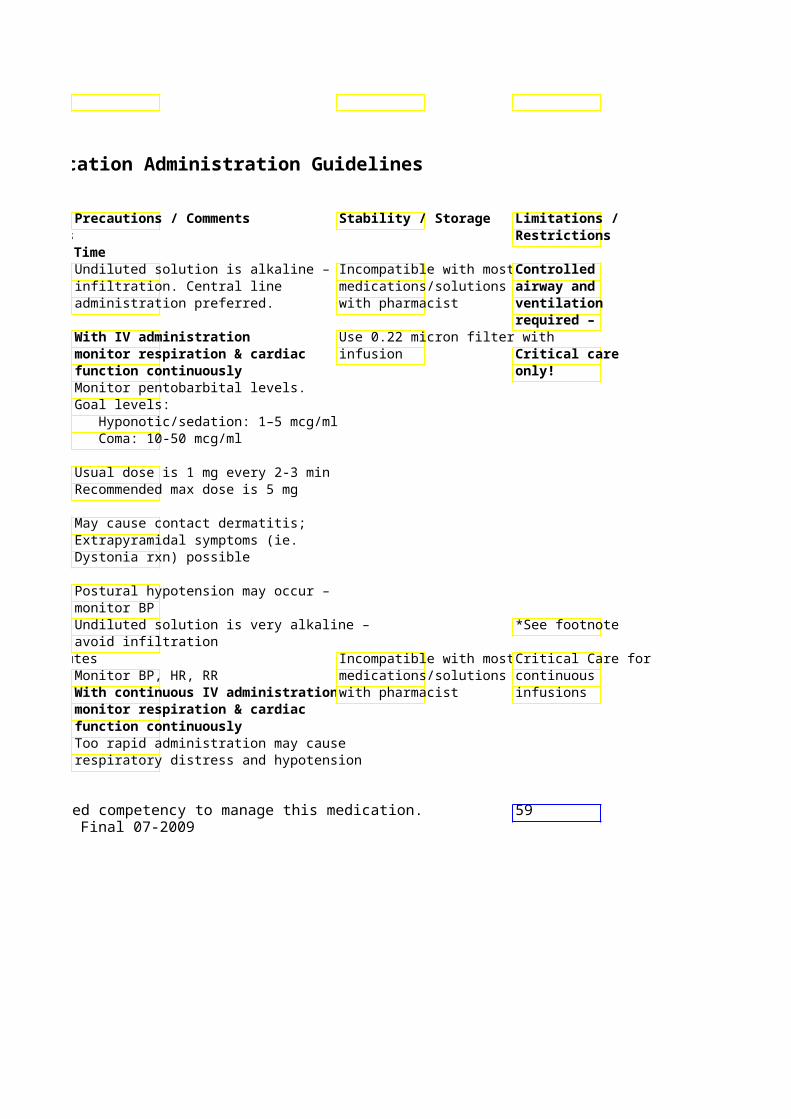
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Phentolamine 5mg/ml – Yes, SQ administration preferred (Regitine) 1ml Vial 5mg/10ml NS
Give over 30 Administer within 12 hr of seconds extravasation
Vasodilator SQ administration preferred
Phenylephrine 10 mg/ml – Yes, rarely. Continuous Infusion (Neosynephrine) 1 & 5ml 0.1-0.5 mg given System Standard Conc: 50 mg/250 m
Vial over at least 1 NS (200 mcg/ml) Vasopressor min System “Concentrated” Conc: 50 mg
Prep: add 1 ml of 100 ml NS (0.5 mg/ml) phenylephrine 10 Usual dose range: 40-60 mcg/min is mg/ml to 100 ml usually adequate NS – final conc 0.1 mg/ml
PhenyTOIN 50 mg / ml Yes, Dilute with only(Dilantin) 2ml M ax rate of between 2 & 10 mg/ml.
Syringe & mg/min 2 or 5ml
Anticonvulsant vial Rate of 25 mg/min Recommended loading dose: 15-20 mg/kg
recommended in elderly or presence Recommended maintenance dose: 5of coronary artery mg/kg/day disease.
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
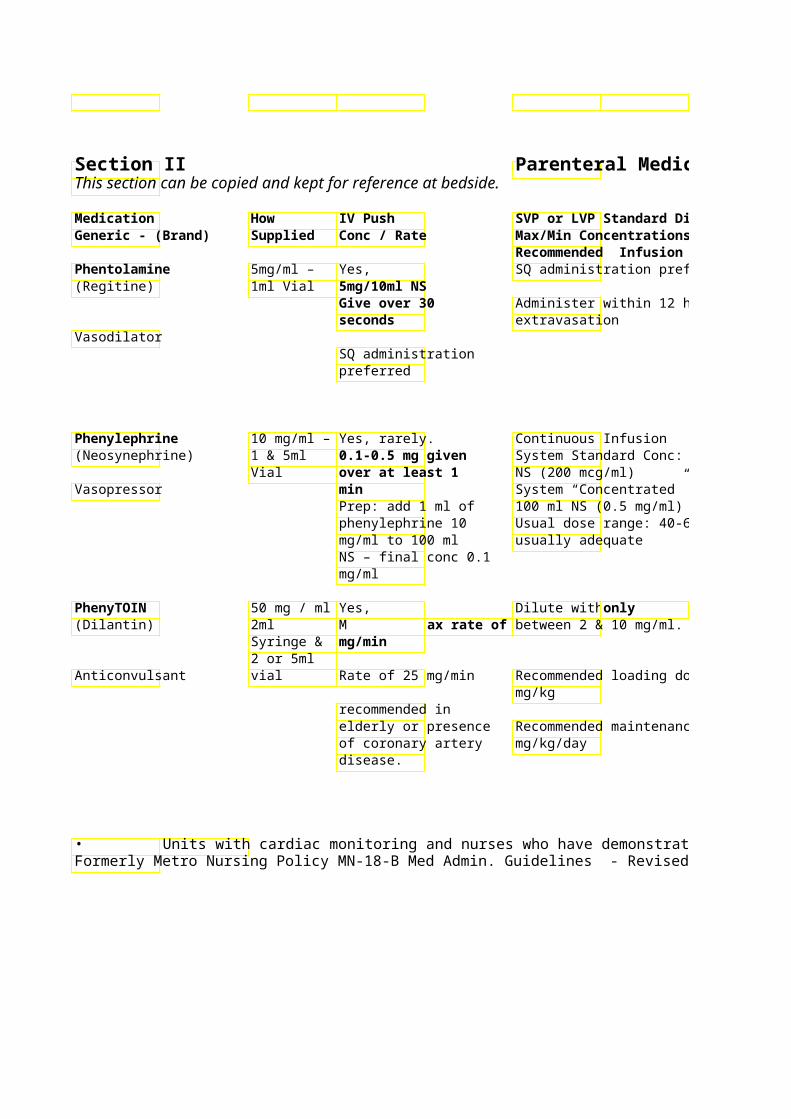
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time SQ administration preferred Antidote for peripheral ischemiaUse reconstituted solution
due to dopamine, dobutamine, immediately Administer within 12 hr of norepinephrine, metaraminol,
epinephrine , phenylephrine. See PPO 5046
SQ admin: dilute to 0.5-1 mg/ml and inject 0.5 ml in multiple sites to cover extravasation area (doses up to 50 mg have been used) Avoid infiltration – Phentolamine Critical Care
System Standard Conc: 50 mg/250 m(Regitine) SQ recommended for management oPPO
System “Concentrated” Conc: 50 mg5046 for general extravasation guidelines / management
Usual dose range: 40-60 mcg/min is Monitor BP, HR every 15 min Monitor urine output every 1-2 hr
Central line advised! NS to a conMonitor BP Administer immediately after
between 2 & 10 mg/ml. dilution. Stable only 4 hr. Central line administration required for doses > 300mg. Fosphenytoin Use in-line filter (0.22 micron)
Recommended loading dose: 15-20 may be given peripherally. Flush IV line with 10 ml NS
Watch for crystal formation. before and after dose Recommended maintenance dose: 5Alkaline solution – local burning administered
upon administration is common – slow infusion if occurs Avoid Extravasation – see PPO 5046 for general guidelines / management Fosphenytoin is preferred – refer to fosphenytoin entry.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 60Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
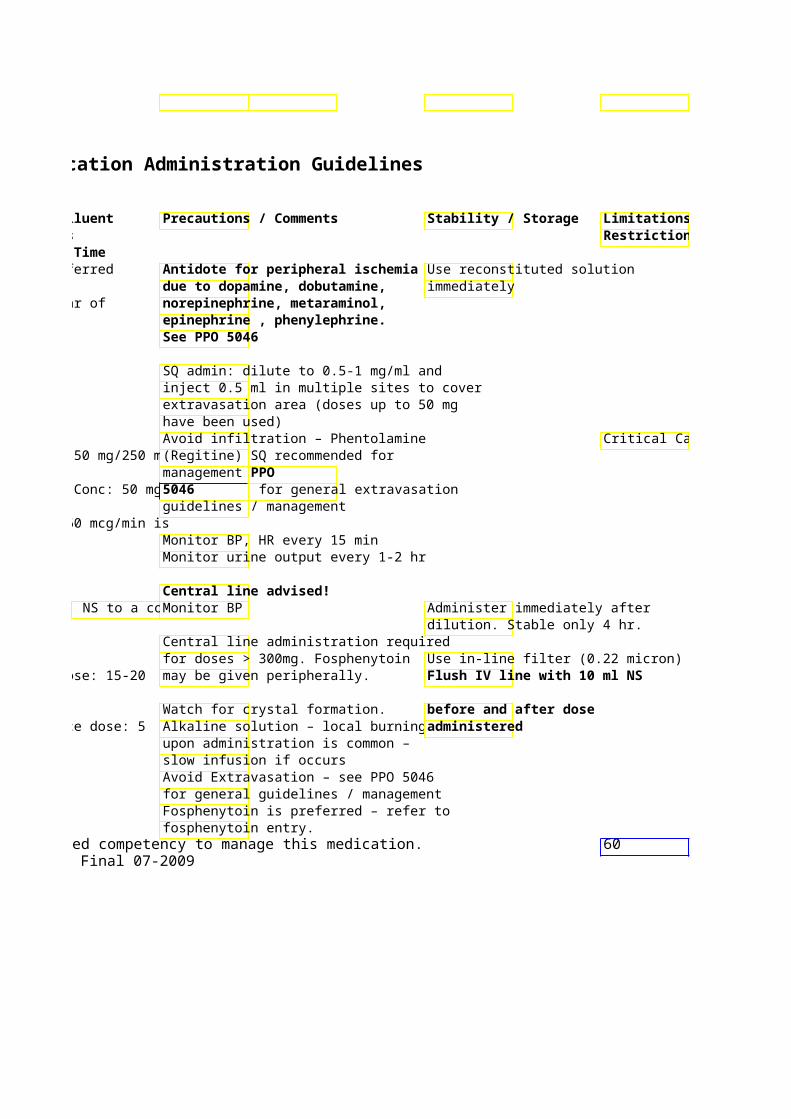
Limitations / Restrictions
Critical Care
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Phosphate – Potassiu 5 & 10 ml NO Infuse slowly as dilute solutions or Sodium Salts Vial Recommended infusion rates:
3 mMol 5 mMol Phos/100 ml D5W over 1 hr *HIGH ALERT (Millimoles 10 mMol Phos/150 ml D5W over 2 hrMEDICATION* ) Phosphate 15 mMol Phos/250 ml D5W over 3 hr
& 4.4 mEq 20 mMol Phos/250 ml D5W over 4 hrElectrolyte K or 4 mEq 30 mMol Phos/250 ml D5W over 6 hr
Na per ml Physostigmine 1mg/ml – Yes, NO (Antilirium) 2ml Amp at max rate of
1mg/minCholinergic
Phytonadione 1 mg/0.5 NO Intermittent infusion- Usual Dose: (Vitamin K – ml amp/ 5-10mg/50 ml NS over 30-60minutesAquamephyton) syringe respectively.
10 mg/ml Vitamin/ Reversal of amp May be administered over 15min in
50mg/5 ml emergency reversal (ICH). Anticoagulation vial
Piperacillin 2, 3, and 4 NO Dilute in 100 ml NS/D5W and infuse (Pipracil) gm vials IM administration over minimum of 30 minutes
recommended Antibiotic/Penicillin
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
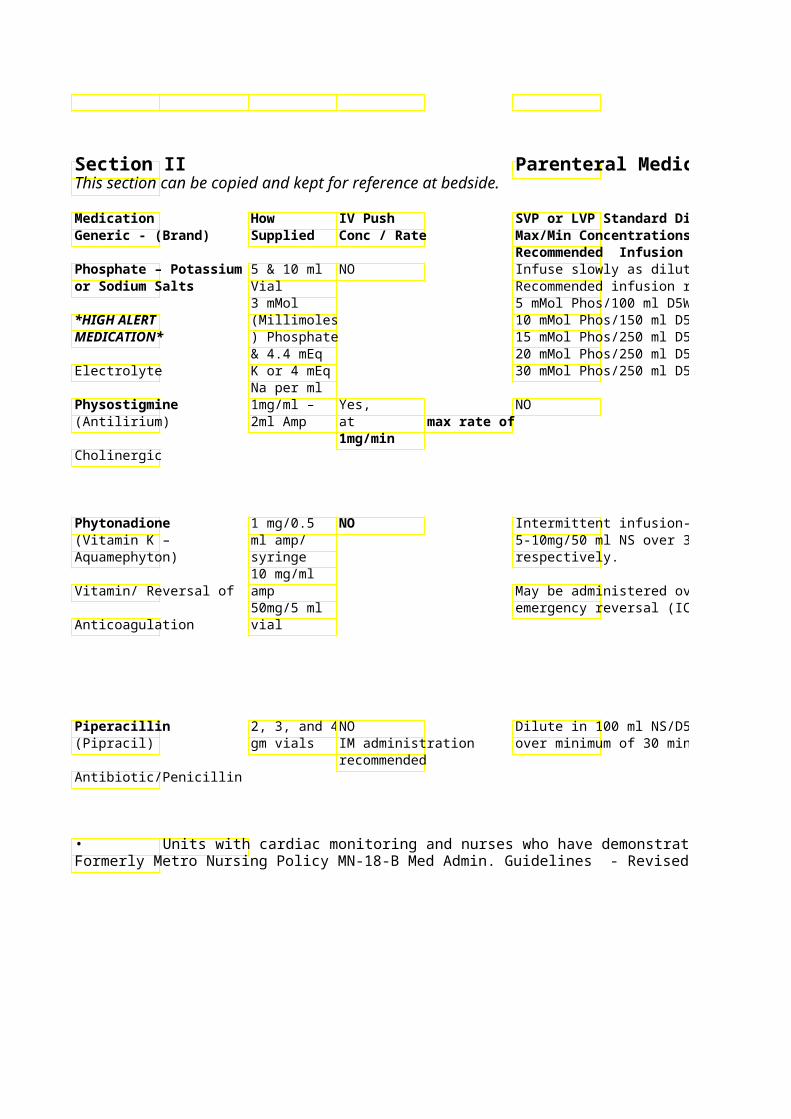
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Infuse slowly as dilute solutions Lower dose recommended with Not compatible with calcium Recommended infusion rates: concomitant hyper-calcemia solutions 5 mMol Phos/100 ml D5W over 1 hr 10 mMol Phos/150 ml D5W over 2 hrRecommended dose range is 0.08 – 15 mMol Phos/250 ml D5W over 3 hr0.24 mMol/Kg 20 mMol Phos/250 ml D5W over 4 hrSodium Phosphate or Potassium 30 mMol Phos/250 ml D5W over 6 hrPhosphate should always be ordered
in millimoles (mMol) For reversal of anti-cholinergic Too rapid administrat*See footnote toxicity may cause bradycardiDo not confuse
respiratory distress with Recommended max dose is 4 mg in pyridostigmine. 30 min
Atropine readily available (UBC)
Intermittent infusion- Usual Dose: Severe anaphylactoid reactions haveUse immediately after dilIV route 5-10mg/50 ml NS over 30-60minutesoccurred – usually during / immediate restricted to
following infusions. Fatal reactions Protect from light. Critical Care, have been reported. OR & ED
May be administered over 15min in Monitor closely for signs of administration. emergency reversal (ICH).
flushing, weakness, tachycardia, Outside of these SOB, abdominal pain, and areas: physician hypotension; discontinue infusion. administration Consider fluids, diphenhydramine, only. epinephrine, corticosteroids & supportive therapy.
Dilute in 100 ml NS/D5W and infuse Penicillin derivative – Check over minimum of 30 minutes allergies
Slow infusion rate if vein irritation occurs Dose reduction recommended for CrCl < 40 ml/min
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 61Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
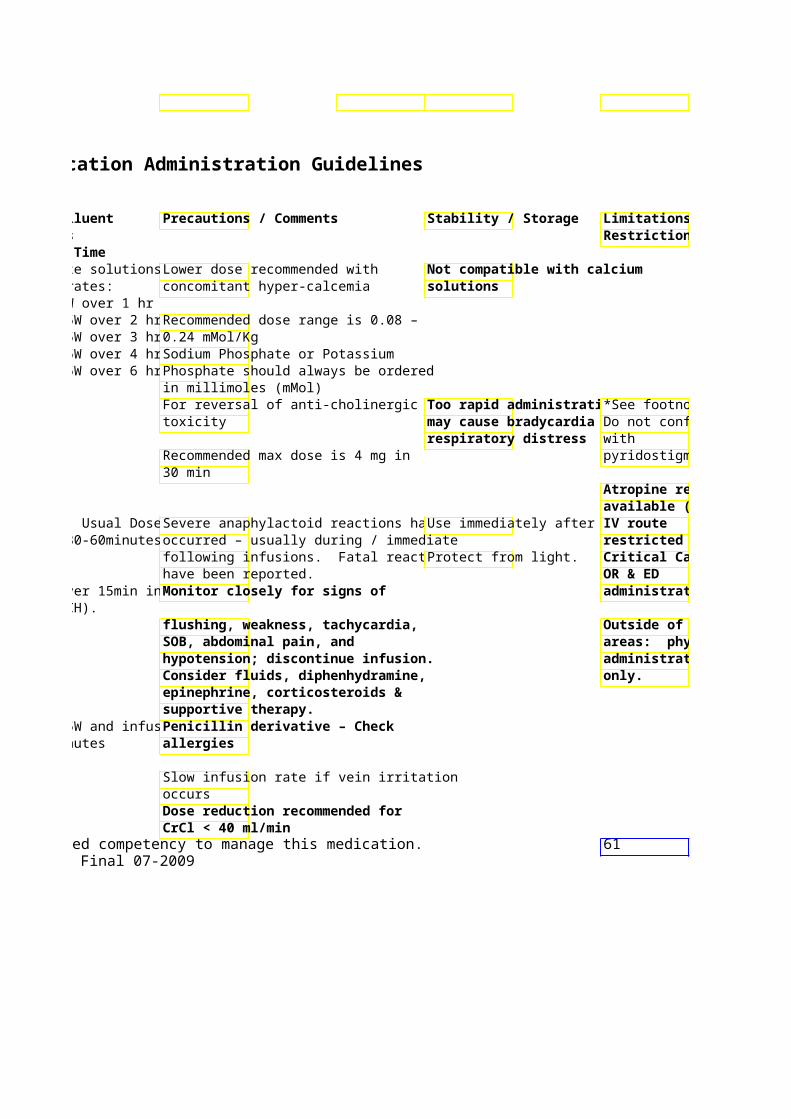
Limitations / Restrictions
*See footnote Do not confuse
pyridostigmine.
Atropine readily available (UBC)
restricted to Critical Care,
administration.
Outside of these areas: physician administration
Section IIThis section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Piperacillin/Tazo- 2/0.25, NO Infuse over minimum of bactam (Zosyn) 3/0.375 &
4/0.5 Gm Vial and
Antibiotic/ Penicillin Premix
2/0.25 in 50 ml, 3/0.375 in 50 ml, 4/0.5 in 100 ml
Potassium Chloride Vials – NEVER GIVE Maximum concentration:2mEq/ml IV PUSH!! •
*HIGH ALERT Premix MEDICATION* bags: •
10mEq/ 50 & 100ml,
Electrolyte 20mEq /50 • & 100ml Administration rate:
•
•
•
Pramlintide No, Not advised (Symlin)
SC *HIGH ALERT administration
MEDICATION* only!
Synthetic analog of
amylin/ adjunct
treatment of diabetes • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication.
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
SVP or LVP Standard DPrecautions / Comments Stability / Storage Max/Min Concentrations Recommended Infusion Time Infuse over minimum of Penicillin derivative – Check
allergies
Slow infusion rate if vein irritation occurs
Dose reduction recommended for CrCl < 40 ml/min Extended infusions over 3 -4 hours may be used for treatment of resistant pathogens.
Maximum concentration:Avoid extravasation – see PPO 5046 Slowing potassium infusiIntermittentfor general guidelines / management. increasing maintenance fline: 20 mEq/100 ml rate, or increasing SVP Intermittent infusion, central line: may reduce stinging if 20 mEq/50 ml encountered with peripheral
administration. If these LVP/IV fluids: 80 mEq/L measures fail, lidocaine 10-50
Administration rate: mg may be added for peripheral administration upon MD order.
Usual: 10 mEq/hr (20 mEq/hr for Greater than 100 mg/day not 20 mEq/50 ml) recommended. Max admin rate without telemetry: 20 mEq/hr Max. admin rate with telemetry: 40 mEq/hr (exceeding 40mEq/hr for severe, life-threatening, symptomatic hypokalemia requires cardiac monitoring & physician presence)
Not advised Used as adjunct to mealtime insulin in Type I & Type 2 DM. Do NOT mix with insul
Can cause severe hypoglycemia when Unopened vials: used with insulin – monitor for s/sx of refrigerate/protect from l
hypoglycemia See vial for expiration daCaution: Product labeled in mg/mL.
Opened vials: Discard afDosed in mcg . Administered using daysinsulin syringes labeled in units.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication.
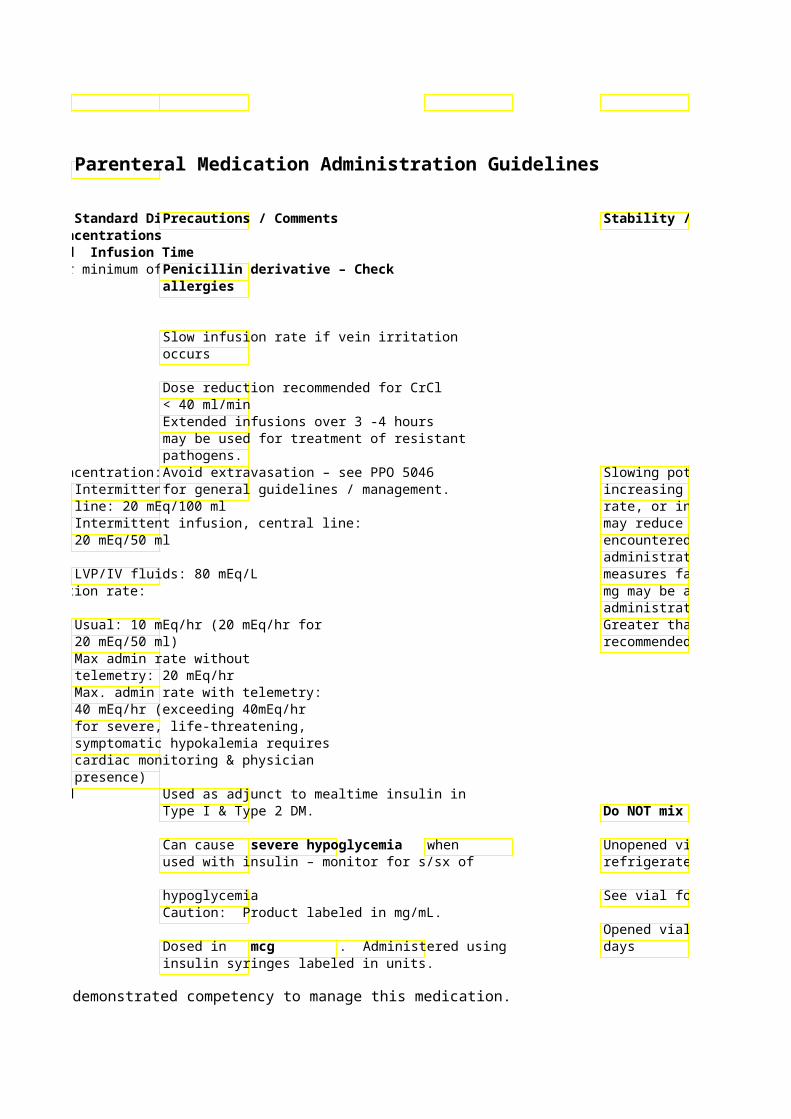
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Stability / Storage Limitations / Restrictions
Slowing potassium infusi* See footnote if increasing maintenance frate of infusion rate, or increasing SVP exceeds may reduce stinging if 20mEq/Hr encountered with peripheral administration. If these measures fail, lidocaine 10-50 mg may be added for peripheral administration upon MD order. Greater than 100 mg/day not recommended.
Metro: Do NOT mix with insulPramlintide will
NOT be Unopened vials: dispensed for refrigerate/protect from linpatients per
See vial for expiration daP&T. See Metro Pharmaceutical
Opened vials: Discard afServices P&P 3.55 (06/06)
62
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Procainamide 100 mg/ml Yes, Continuous Infusion: (Pronestyl) 10 ml vials Diluted to Usual dose range: 2 – 6
20mg/ml and give 500 mg/ml at 20-50 mg/mSystem Standard Conc: 1 Gm/250 ml
Cardiovascular/ Anti- 2 ml vials Up to total dose of NS (4mg/ml) arrhythmic for IM 1 Gm System “Concentrated”
injections Gm/100 ml NS (10 mg/ml
Prochlorperazine 5mg/ml, Yes, 5 mg per Intermittent Infusion – (Compazine) syringes minute maximum 10mg in 50ml NS over 15min
and Vials rate
Antiemetic
Profilnine SD See Factor 9 Complex - Human Promethazine 25 & Yes, Not advised – IM Preferr(Phenergan) 50mg/ml - max of 25 mg/min
Vials For IV admin: Antihistamine/ Dilute to 10-20 ml antiemetic with NS and admin
via running IV line
IM Preferred
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
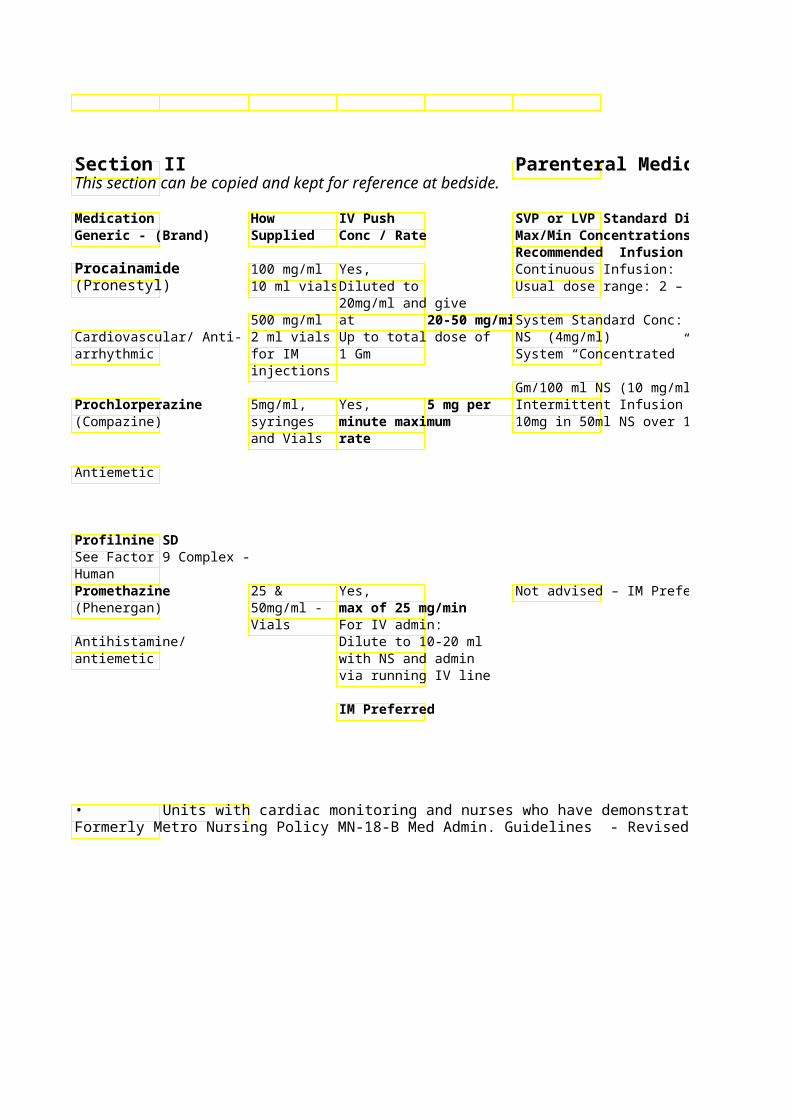
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor BP every 2-3 min during * See footnote loading dose then every 15 min untilCheck with pharmacist stable during initial infusion. regarding compatibility
System Standard Conc: 1 Gm/250 ml information. Continuous ECG monitoring. Elimination half-life extended in renal
failure. Do not exceed 40 mg in 24 hours Protect diluted soluti Contraindicated
10mg in 50ml NS over 15min light in patients with Slow rate if extra-pyramidal symptoms Parkinson’s (dystonia, motor restlessness, disease parkinson-like symptoms) occur Monitor for hypotension – recommend patient lay down or sit for 30 min after dose
Monitor for hypotension, tachycardia. Metro: Promethazine
Avoid extravasation --Apply warm injection is not compresses for 20-30 minutes 4-6 available due to times a day for 1-2 days. safety concerns Extravasation – see PPO 5046 for including general guidelines / management extravasation.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 63Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
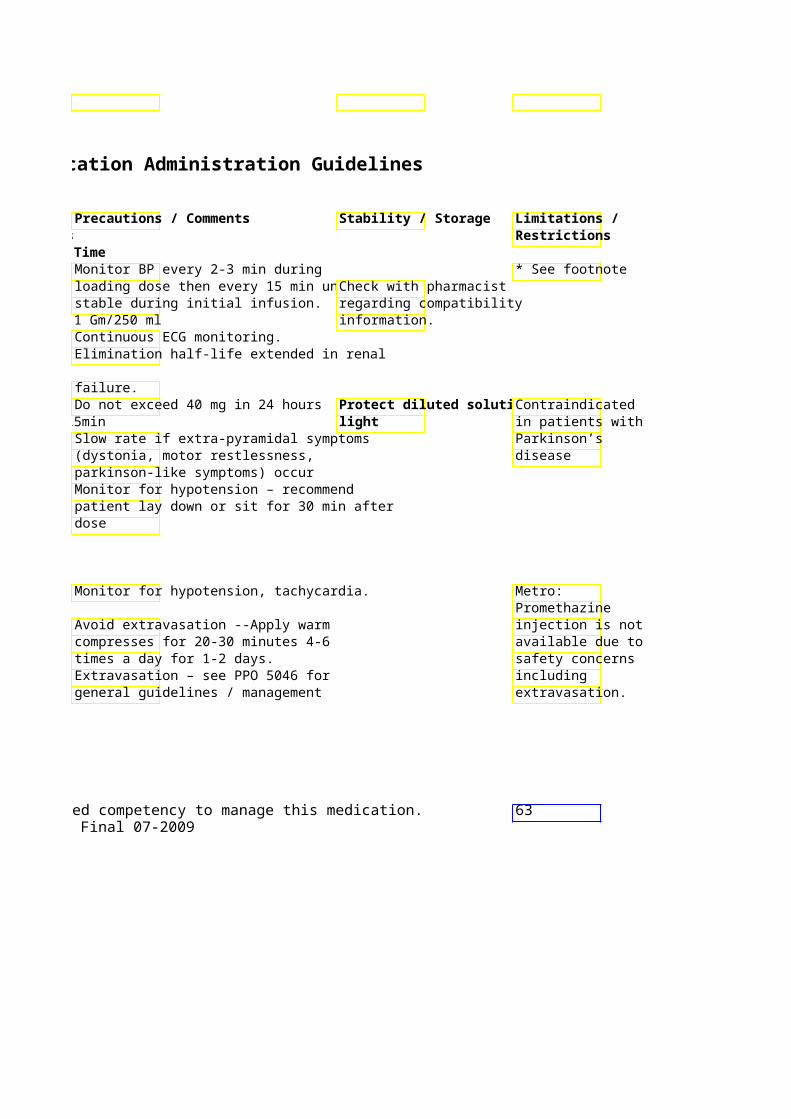
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Propofol 10mg/ml – Yes, Continuous Infusion – IC(Diprivan) 20ml Amp, Give slowly over 5mcg/kg/min with additi
50 & 3-5 min. mcg/kg/min increments every 5 *HIGH ALERT 100ml minutes to sedation leveMEDICATION* bottles – fat
emulsion Usual dose range: 5-50 Sedative
System Standard Conc: ml Premix (10 mg/ml)
Propranolol 1mg/ml – Yes, NO (Inderal) vial 0.5mg then
1mg/min every 5-10 min to max of
Cardiovascular/ Beta- 0.1mg/Kg Blocker
Max rate: 1 mg/min
Protamine 10mg/ml – Yes, NO 5 and 25ml 10mg/ml given
Heparin antagonist Vials over 1-3 minutes. Max dose: 50mg in any 10 minute period
Pyridostigmine 5 mg/ml 2 Yes NO (Mestinon) ml amp, 5 Max rate of 5
mg/ml 5 ml mg/min Cholinergic vial
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
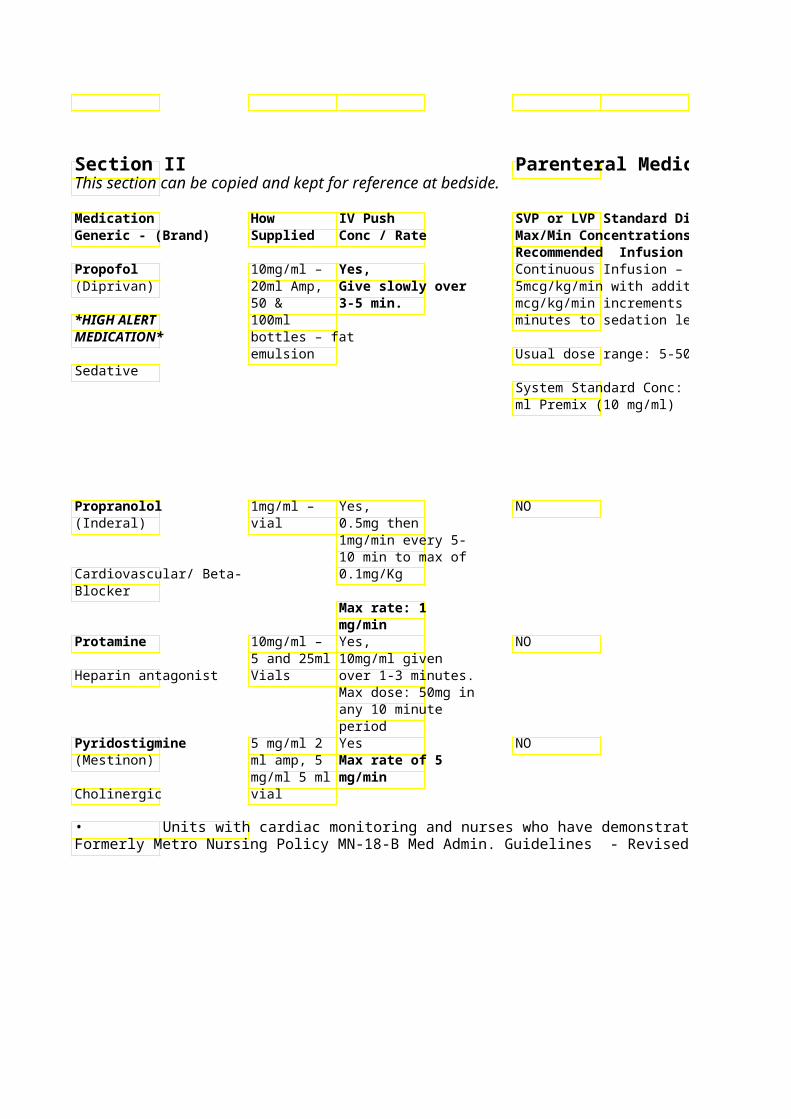
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Do not mix with other solutions Discard unused solutionsCritical Care for infuse if emulsion appears separ12 hours continuous
mcg/kg/min increments every 5 infusion; Propofol contains 1.1 Kcal/ ml Change tubing everIV push mode
hours limited to areas Monitor closely for hypotension, that can provide bradycardia, and respiratory Do not filter respiratory depression monitoring and
prompt For infusions > 72 hours, intubation recommend checking triglycerides Avoid Extravasation – see PPO 5046 for general guidelines / management BP every 5 min during titration, thenMay dilute w/ 10 ml D5W* See footnote 15min until stable give undiluted Monitor Heart Rate-bedside monitor + defibrillator
IV maintenance dose may be given every 4 hrs
Monitor for hypotension & bradycardia
1 mg protamine for approx 100 units USP Heparin
Used in pt with myasthenia gravis Incompatible with many Monitored bed medications/solutions – recommended.
May be used to reverse effects of nowith pharmacist Do not confuse depolarizing neuromuscular blockers. with Other agents preferred. physostigmine.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 64Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
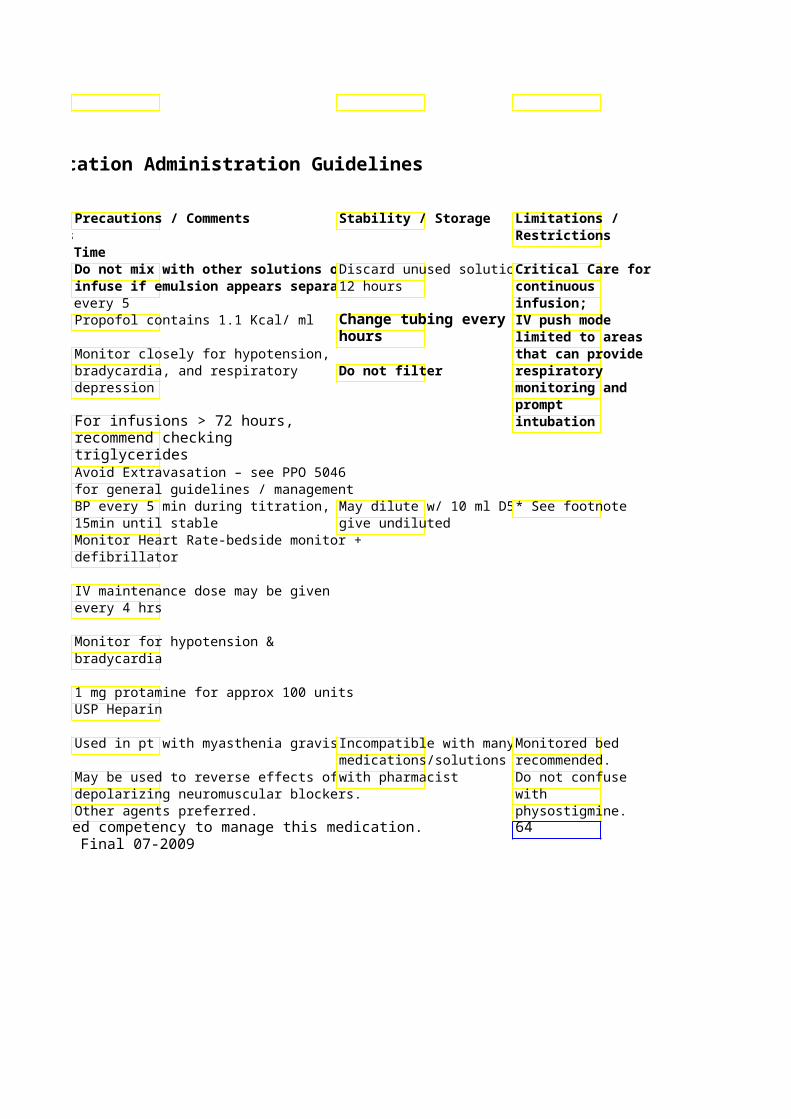
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Pyridoxine 100mg/ml Yes, Intermittent Infusion – (Vitamin B-6) in 10 & 50 – 100 mg/min 5 Gm in 50ml NS over 3
30ml vials 50-100mg in 50mL NS oVitamin/ Nutritional Supplement
Ranitidine 25mg/ml – Yes, Slow IV-Push preferred (Zantac) vial and Dilute 50mg dose
syringe up to 5ml with NS Continuous Infusion: H Receptor 2 and give over 2-3 System Standard Conc: 150mg/250ml Antagonist minutes NS (0.6 mg/ml) Remifentanil Powder for Yes, over 30-60 Slow IV push or via cont(Ultiva) Injection: seconds by infusion
1mg,2mg, Anesthesia or with *HIGH ALERT 5mg vials continuous airway Continuous Infusion: MEDICATION* support System Standard Conc: 2mg/100mL Narcotic Analgesic (20mcg/mL). Dose range 0.025-
2mcg/kg/min Reteplase 1 unit/ml Yes, May be used for treatme(r-PA, Retevase) 10 ml vial For AMI: Peripheral Arterial Occlu
10 units over 2 min . Repeat 10
*HIGH ALERT units after 30 min MEDICATION* Do not confuse with Flush with other thrombolytic minimum of 30-50 medicines. ml NS or D5W
Thrombolytic
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
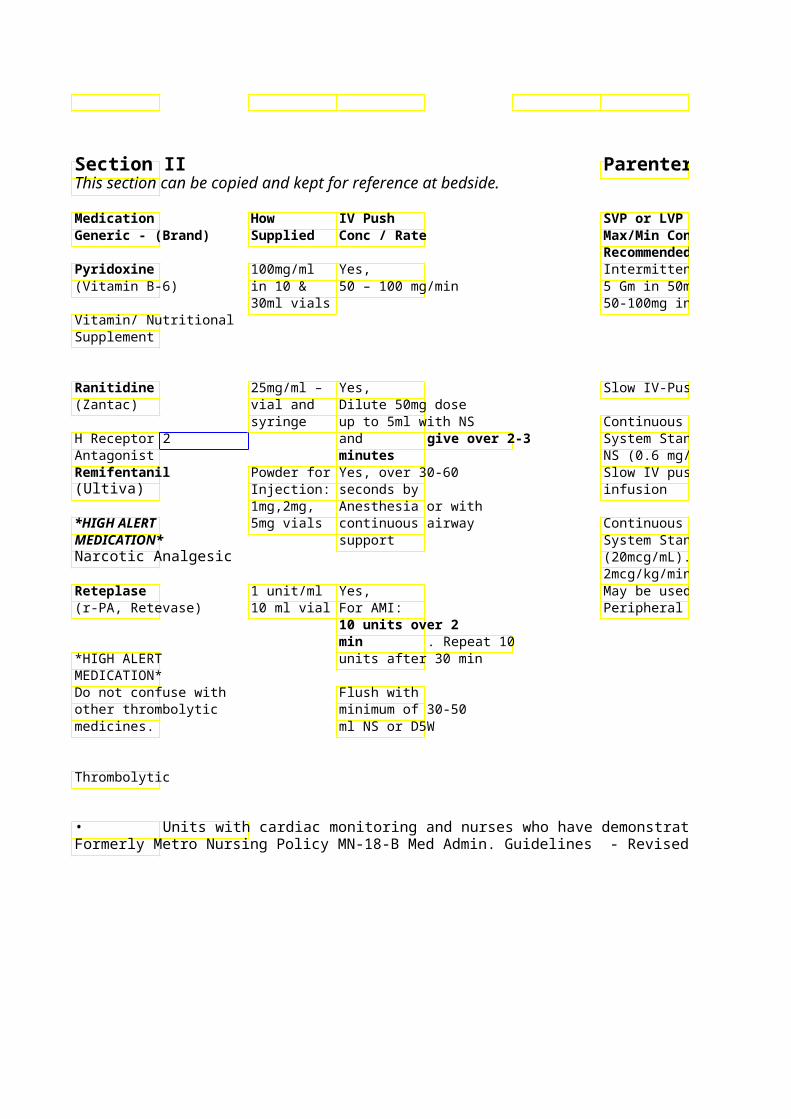
Parenteral Medication Administration Guidelines
SVP or LVP Standard DPrecautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time Intermittent Infusion – Antidote: Isoniazid poisoning or 5 Gm in 50ml NS over 3 overdose - Give equivalent amounts of 50-100mg in 50mL NS opyridoxine as ingested Isoniazid.
Antidote: Ethylene glycol toxicity – administer 50-100mg q6h until ethylene glycol levels undetectable / resolution of acidosis
Slow IV-Push preferred
Continuous Infusion: System Standard Conc: 150mg/250ml NS (0.6 mg/ml) Slow IV push or via cont Risk of apnea / respiratory depression. Anesthesia /
Anesthesia Consult Only
Continuous Infusion: System Standard Conc: 2mg/100mL (20mcg/mL). Dose range 0.025-2mcg/kg/min May be used for treatmeThrombolytic medication: Monitor Do not shake or transpor*See footnote for Peripheral Arterial Occlufor bleeding. tube system. cardiopulmonary
Minimize potential risks for bleeding: indications (ie: Establish all IV’s prior to therapy. Incompatible with hepariAMI, PE). (Minimum of 2 peripheral IVs Check compatibilities with recommended in addition to pharmacist Monitoring is at thrombolytic infusion site.) physician Avoid unnecessary arterial/venous Do not mix with any discretion for punctures, excessive blood samplingmeds/solutions. peripheral and IM injections for at least 24 hr vascular after d/c’d (malnourished patients 48 indications. hr). Apply pressure dressings to all puncture sites.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 65Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Limitations / Restrictions
Anesthesia / Anesthesia Consult Only
*See footnote for cardiopulmonary indications (ie:
Monitoring is at
discretion for
indications.
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time RifAMPIN 600mg Vial NO Intermittent Infusion – (Rifamycin) for Up to 600mg diluted in
Injection or NS over 30 minutes
Antibiotic
Rocuronium 10mg/ml – Yes, Continuous Infusion: (Zemuron) 5ml Vial intubation dose 0.6 Usual dose range: 5-20
mg/Kg rapidly *HIGH ALERT MEDICATION*
Neuromuscular blocker
Sargramostim 500mcg/ml NO Intermittent infusion: 25(GM-CSF – Leukine) vial over 2 hours
Colony Stimulating Factor Sodium Bicarbonate 8.4% Yes,
solution 50 mEq (50 ml) 1mEq/ml & over 1-2 minutes Sodium bicarbonate may be added to
Electrolyte syringe IV fluids – check with phNeonatal: Neonates: avoid compatibility/stability i
4.2% admin of 10 solution 0.5 ml/min mEq/ml 10 or greater ml syringe
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
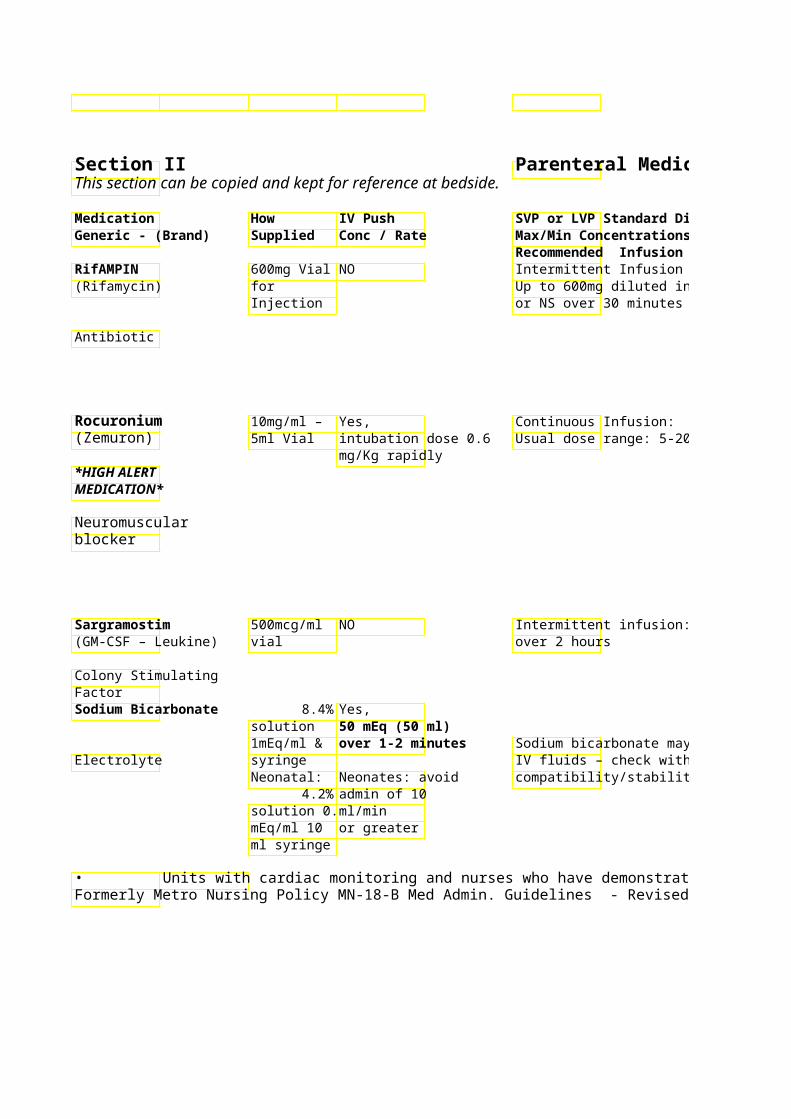
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
May cause a reddish-orange discoloration of urine, saliva, teaProtect from light sweat and stool Permanent discoloration of soft Expires 4 hours after contact lenses may occur. preparation. Avoid infiltration = local irritation and inflammation. If this occurs, the infusion should be discontinued and started at another site. Refer to Nursing Clinical PoliciesRefrigerate vials. Unope Controlled airway on Neuromuscular Blockade (i.e.vial stable at room tempand ventilation MN-13) days but then must be required;
discarded. Critical Care only: ED, ICU, Surgery
Sedation must be administered prior to and during paralytic use!
Do not filter solution Concentrations less than Use only NS to dilute 10mcg/mL require albumin
0.1% added to solution to Monitor BP – syncope may occur prevent adsorption. especially after 1 dosstDo not mix with other medications – Check with pharmacist
Sodium bicarbonate may be added to Neonates: Flush w/ 10-20 ml NS before after administration
Avoid extravasation!! Central line administration advised when ever possible. (See PPO 5046)
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 66Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Sodium Chloride 3%500 ml bag Not advised
Rate and infusion duratio*HIGH ALERT MEDICATION*
Hypertonic solution
Sodium citrate, 4% 500 ml NO NOT to be infusebags intravenously.
Anticoagulant StreptoMYCIN 1g vial NO Intermittent IV Infusion
(powder) 500-1000mg in 100mL NAntimicrobial 60min
May administer via deep
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
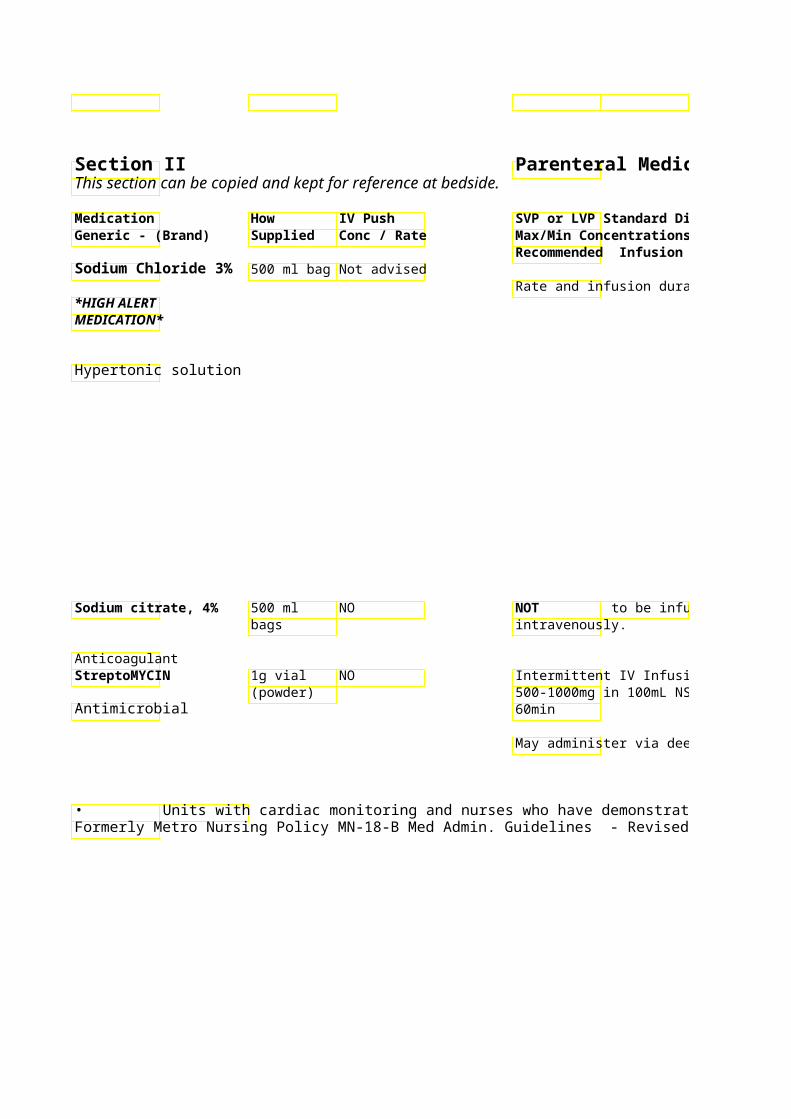
Parenteral Medication Administration Guidelines
Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Hypertonic (3%) saline i Do not mix with any physiologic and is only i medications/solutions. Contact Metro: neurosurgica+ pharmacist for compatibility Mandatory PPO with severe (Na < 120) information. with serial symptomatic hyponatremia. sodium levels
(minimum q 4 Chronic Hyponatremia: hr) and Risk associated with rapCentral line administration and mandatory call correction (greater thCritical Care admission parameters 0.5mEq/L/hr or 8 mEq/advised. (minimum order
+includes osmotic demyelination and to call if Na permanent neurologic damage. correction
exceeds 8 Periodically hypertonic saline is used mEq/24 hr) – if at low rates for short periods of times not included in s/p urological surgeries, etc. – the original order, limitations/restrictions need not apply physician must in such instances. be contacted per
P&T. May be used as an alternative to capping with heparin (ex. PICC lines, Mahukar lines, etc.)
Dose adjustment in elderly / reduced renal function.
Monitor hearing, renal function & serum concentrations as indicated.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 67Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Mandatory PPO with serial sodium levels (minimum q 4
mandatory call parameters (minimum order
to call if Na correction exceeds 8 mEq/24 hr) – if not included in original order, physician must be contacted per

Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Succinylcholine 20mg/ml Yes, Other medications prefe
10ml Vial prior to intubation continuous infusions *HIGH ALERT 0.6mg/kg slowly MEDICATION* over 30 seconds Contraindicated in patients with
personal or family hmalignant hyperthe
Neuromuscular history of skeletal blocker myopathy!!
Tacrolimus 5mg/ml – NO Continuous Infusion – (Prograf) 1ml Amp Usual dose: 0.05 – 0.1
Standard conc: 5 mg/25(Excel) (20 mcg/ml)
Immunosuppressant Intermittent infusion (q14 hr Conc must be 0.004 – 0.02 mg/ml
Tenecteplase 50mg vial Yes, Acute Coronary Syndrom(Tnkase) Weight based Myocardial Infarction:
bolus dosing (15 - Preprinted order set avai50mg depending
*HIGH ALERT on weight) Give Peripheral Vascular ThroMEDICATION* dose over 5 Per Interventional RadiolDo not confuse with seconds into Preprinted order set avaiother thrombolytic running NS line medicines.
Thrombolytic
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Refer to Nursing Clinical Policies Refrigerate Controlled airway Neuromuscular Blockade and ventilation (i.e. MN-13) required;
Contraindicated in patients with Critical Care Too rapid administration may cause only: bradycardia ED, ICU, May cause hyperkalemia – increased Surgery. risk with use in patients with burns, Sedation must severe trauma, stroke, spinal cord be administered injury, muscular dystrophy, multiple prior to and sclerosis, tetanus, Parkinson’s disease. during paralytic
use! May cause rhabdomyolysis *NOTE: Sublingual administration preferred due to risk of allergic reaction with IV product* Use admin set provided by
pharmacy Monitor for allergic reaction especially during initial 30 minu IV = ¼ PO Dose of first infusion – anaphylaxis
Conc must be 0.004 – 0.02 mg/ml Monitor for hyperkalemia, hyperglycemia and elevated BP Monitor trough tacrolimus levelsThrombolytic medication: Monitor *See footnote for for bleeding. cardiopulmonary Minimize potential risks for bleeding:May precipitate in IV lines indications (ie: Establish all IV’s prior to therapy. with D5W. Flush line with NS AMI, PE). (Minimum of 2 peripheral IVs before and after recommended in addition to administering. Monitoring is at thrombolytic infusion site.) physician Avoid unnecessary arterial/venous Do not mix with other discretion for punctures, excessive blood samplingmedications/solutions. peripheral and IM injections for at least 24 hr vascular after d/c’d (malnourished patients 48 indications. hr). Apply pressure dressings to all puncture sites.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 68Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
Limitations / Restrictions
Controlled airway and ventilation
Critical Care
Sedation must be administered prior to and during paralytic
*See footnote for cardiopulmonary indications (ie:
Monitoring is at
discretion for
indications.
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Terbutaline 1 mg/ml NO Continuous infusion: Used(Brethine) ampule SQ administration pre-term labor contractio
preferred – 0.25 Sympathomimetic mg SQ x 1, may Titrate to contractions
repeat x 1 after 15- absence of contractions 30 min. Max dose of 0.5 mg in 4 hr Uterine relaxation: 0.25recommended. – given IV push
Theophylline Premix NO Intermittent Infusion – bags: 5mg/kg theophylline loa800mg/500 30 min
Bronchodilator ml Continuous Infusion – 0.4mg/Kg/hr theophylline System Standard Conc:Premix (1.6 mg/ml)
Thiamine 100mg/ml Yes, A common component in(Vitamin B-1) – 2ml vial Administer via bag” – 1000 ml bag.
large vein over at least 3 min with May also be given as int
Vitamin/ Nutritional running IV fluids. infusion: 100 mg/50 ml D5W. Infuse supplement Also may be given over 15 – 30 min.
IM Thiopental 400 mg & Yes, (Pentothal) 500 mg Over 10-15
syringes seconds Sedative/ Barbiturate
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
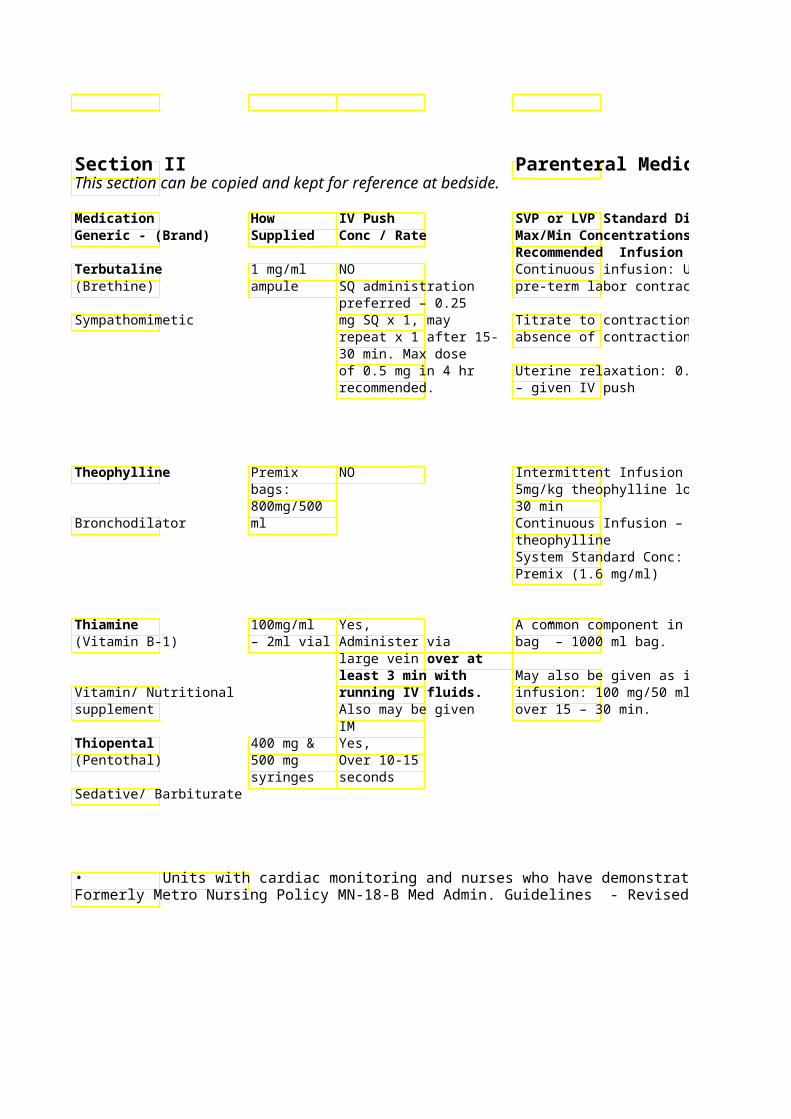
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Monitor for s/sx pulmonary edema in * See footnote pt on continuous infusion Protect ampule from light
Monitor HR (maternal and fetal), BP, ECG, I&Os
See site specific administration policy
Metro: See MWH-17-MAT: Women’s Health Policies & Procedures – Terbutaline sulfate: Administration for Tocolysis Theophylline serum level monitoring is recommended periodically during IV infusion
Continuous Infusion – 0.4mg/Kg/hr Monitor HR, BP (Note: Aminophylline is 80% theophylline: 500mg aminophylline = 400mg theophylline)** Verify dose to be given. Discard vial after drawing up correct dose. **
Pain at IV site noted at times. infusion: 100 mg/50 ml D5W. Infuse
Avoid infiltration – may treat Controlled airway affected area with lidocaine 1% and ventilation Central line administration preferred required –
Monitor respiration & cardiac Critical care function continuously only! Contraindicated in patient with porphyria
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 69Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
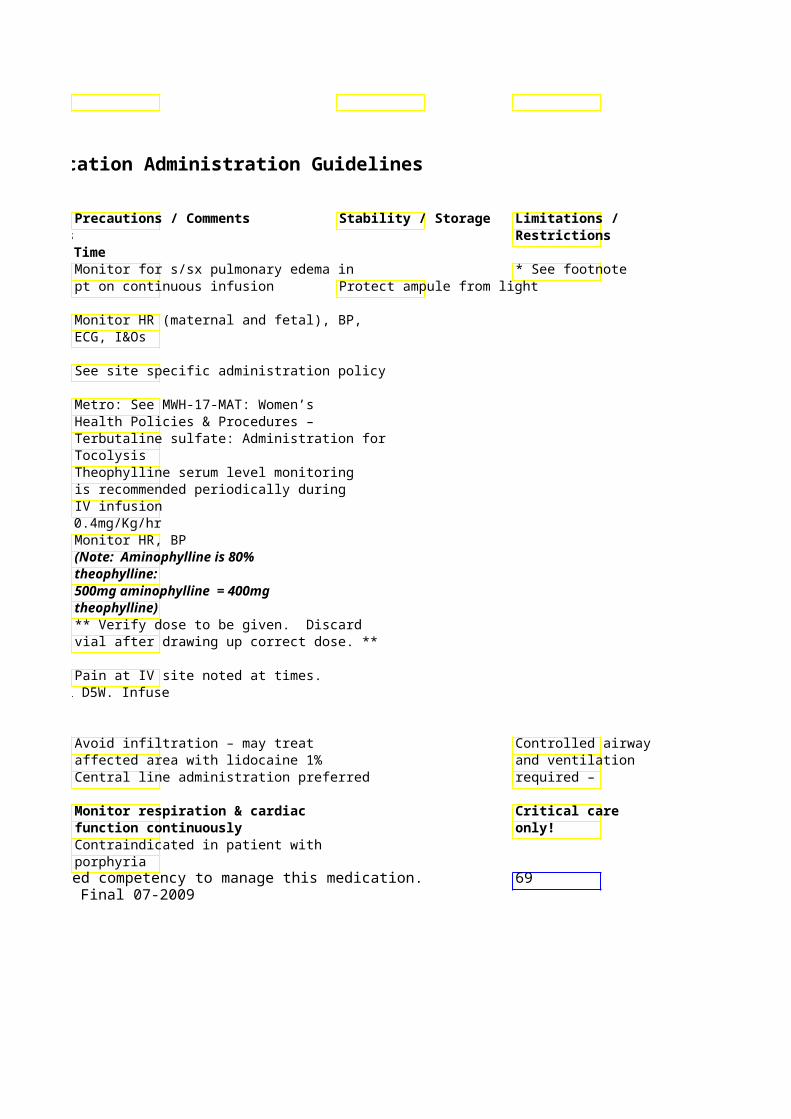
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Tigecycline 50 mg/5 ml NO Intermittent infusion: (Tygacil) vial 100 mg in 100 ml D5W o
mg in 100 ml D5W or NS. Infuse over Antibiotic 30-60 minutes
Max conc = 1 mg/ml
Tirofiban 12.5 mg/ml Yes, Continuous Infusion – (Aggrastat) 50 ml vial, 25 mcg/Kg over 3 PTCA: 0.15mcg/Kg/min
minutes in PTCA Unstable Angina: 0.4 mcg/Kg/min x 12.5mg/250 30min then 0.1 mcg/Kg/
Antiplatelet IIb/IIIa ml premix bag Standard Conc: 12.5mg/250ml NS
(50mcg/ml)
Tobramycin 10mg/ml & NO Intermittent Infusion – (Nebcin) 40mg/ml – All doses diluted into 50
Vial or D5W and infused overAntibiotic/ minutes Aminoglycoside Torsemide 10mg/ml – Yes, May be given as continuo(Demadex) 2 & 5ml Max 5 mg/min
Amps System Standard Conc: 100 mg/100 ml Loop Diuretic NS (1 mg/ml) Tranexamic acid 100mg/ml NO IV infusion during cardia(Cyclokapron) – 10ml Refer to PPO as needed.
Amps Antifibrinolytic • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
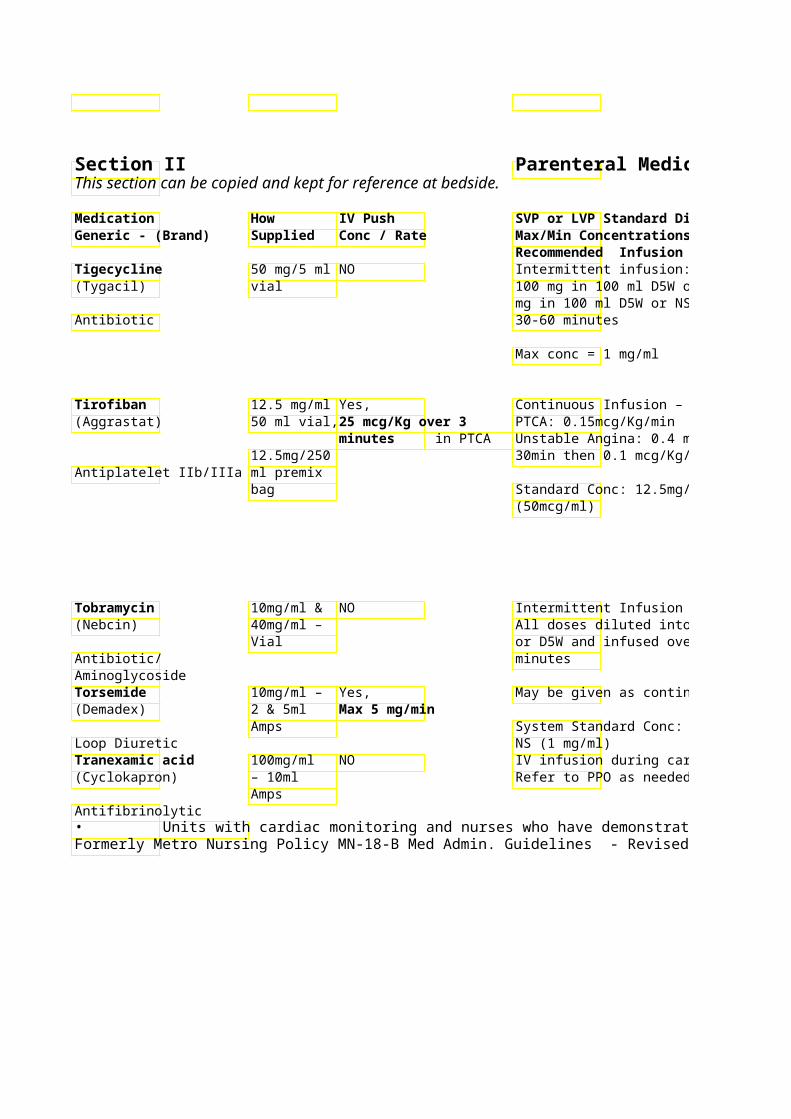
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Dose reduction needed for patients wDiluted solution is hepatic impairment yellow/orange in color
mg in 100 ml D5W or NS. Infuse over Stable 6 hrs at room temp/ 24 hrs refrigerated after dilution
Contact pharmacist for compatibility information
Pre-printed orders for unstable angina or PTCA applications are available
Unstable Angina: 0.4 mcg/Kg/min x Monitor for signs of bleeding!! Monitor VS every 15 min
Standard Conc: 12.5mg/250ml NS Dose reduction to 0.05mcg/kg/min recommended for pt with CrCl < 30ml/min Monitor APTT, Hgb/Hct, PT/INR, and platelets daily while receiving tirofiban Aminoglycoside dosing and monitoring service available from pharmacy upon physician order.
Monitor renal function. Recommended max single dose is 200 mg
System Standard Conc: 100 mg/100 ml
Do not mix with penicillin Refer to PPO as needed.
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 70Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
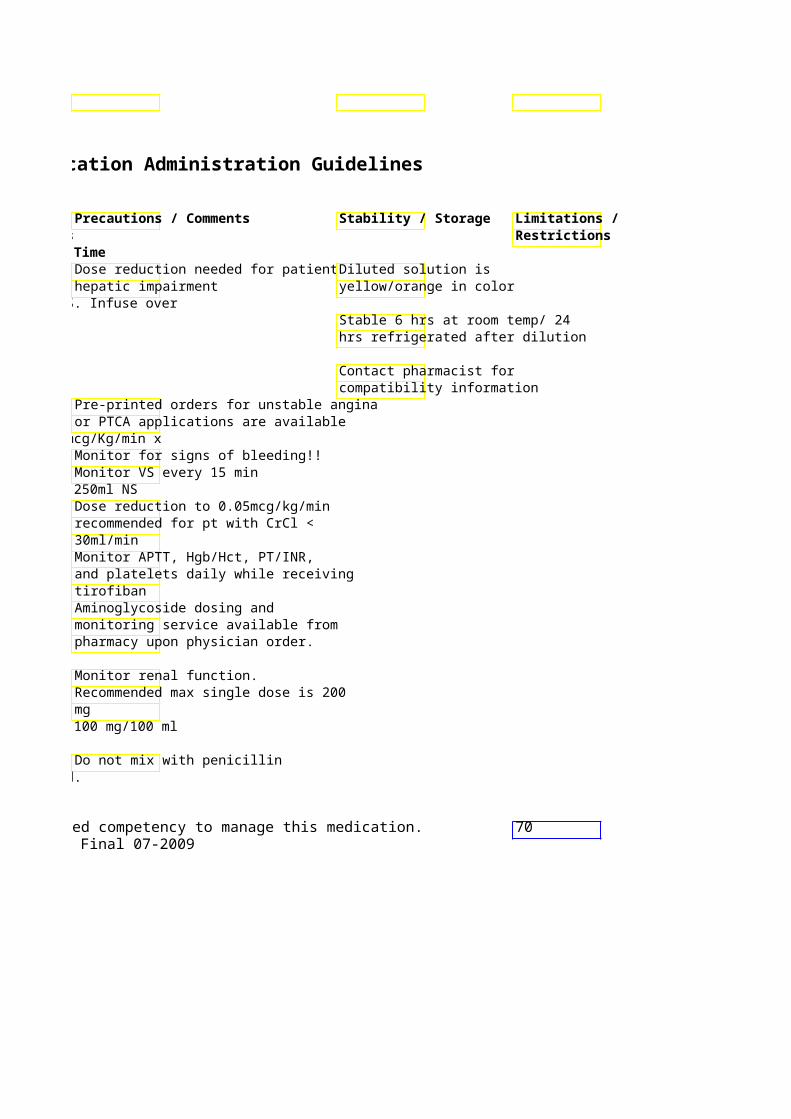
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Treprostinil 1, 2.5, 5, NO Subcutaneous or intr(Remodulin) and 10 continuous infusion
mg/ml 20 ml vials
Cardiovascular/ *** Metro: Use of prVasodilator order set advised **
Trimethoprim & 80mg TMP NO Intermittent Infusion – Sulfamethoxazole + 400mg PCP (Pneumocystis Carini(Cotrimoxazole) SMX per Pneumonia): 15-20mg/kg(Bactrim, Septra) 5ml vial doses (q 6h)
Each 80mg (5ml) TMP dil100ml D5W
Antibiotic/ Sulfonamide Infuse dose over 90min Urokinase 250000 Varying doses Varying continuous infus(Abbokinase) unit vial depending on depending on indication
indication – external reference or phconsult external reference or System Standard Conc: 1
*HIGH ALERT pharmacist. units/250 ml NS (4000 un
MEDICATION* Give over 10 min
Thrombolytic
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
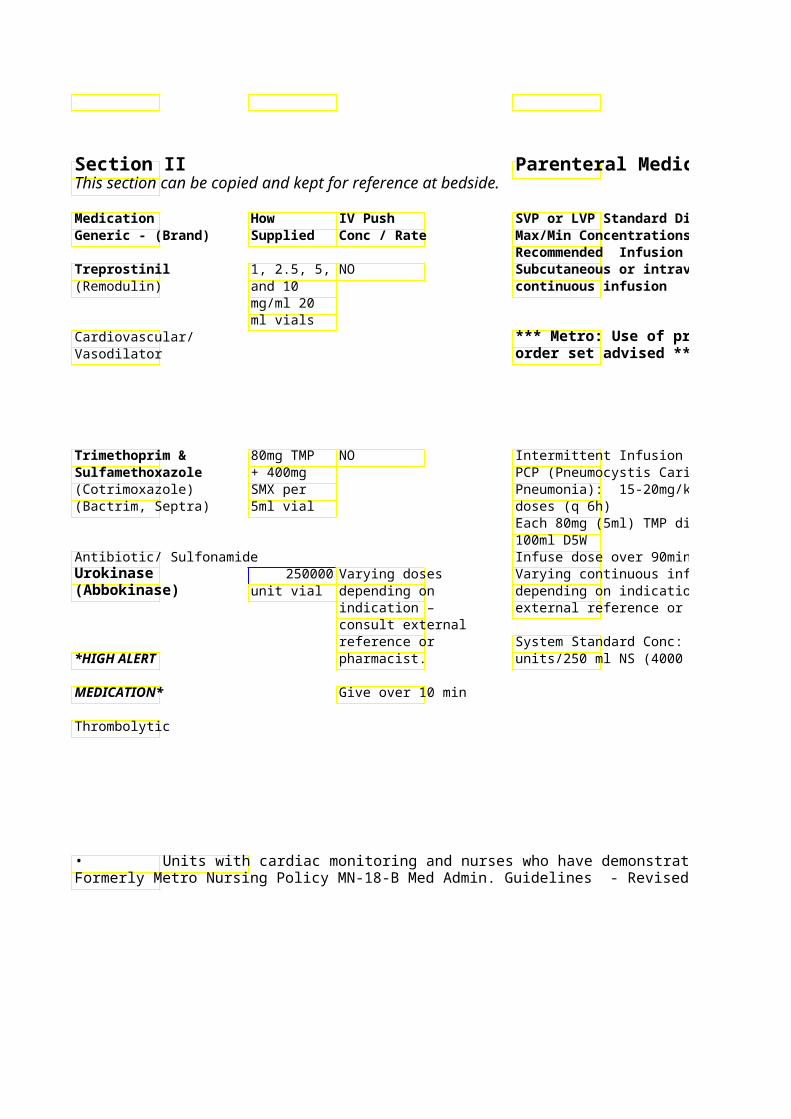
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Avoid infusion interruptions SC: Stable 28* See footnote – loss of disease control could lead use if refrigerated; 14 days at to death room temp
SC administration: Only use Monitor for hypotension, flushing, syringe pump provided by headache, N/V, anxiety & chest pain 0 home health care agency. A “Remodulin Dosing Weight” is IV: 1 mg in 100ml NS stable established and used throughout the 48 hr at room temp. patient’s therapy. The “Remodulin Dosing Weight” should be used when calculating infusion rate. Flush line before and after Sulfa Cotrimoxazole with D5W 5 ml in 100 derivative – Do not mix with any other Stable 4 houcheck
medications/solutions – contact 5 ml in 75 allergies!! pharmacist Stable 2 hours
Infuse dose over 90min Thrombolytic medication: Monitor Critical Care for for signs of bleeding. continuous Minimize potential risks for bleeding: infusion Establish all IV’s prior to therapy. (Minimum of 2 peripheral IVs Monitoring is at recommended in addition to physician
discretion for thrombolytic infusion site.) peripheral Avoid unnecessary arterial/venous punctures, excessive blood sampling, vascular
indications. and IM injections for at least 24 hr after d/c’d (malnourished patients 48 hr). Apply pressure dressings to all puncture sites. Thrombin time elevated
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 71Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
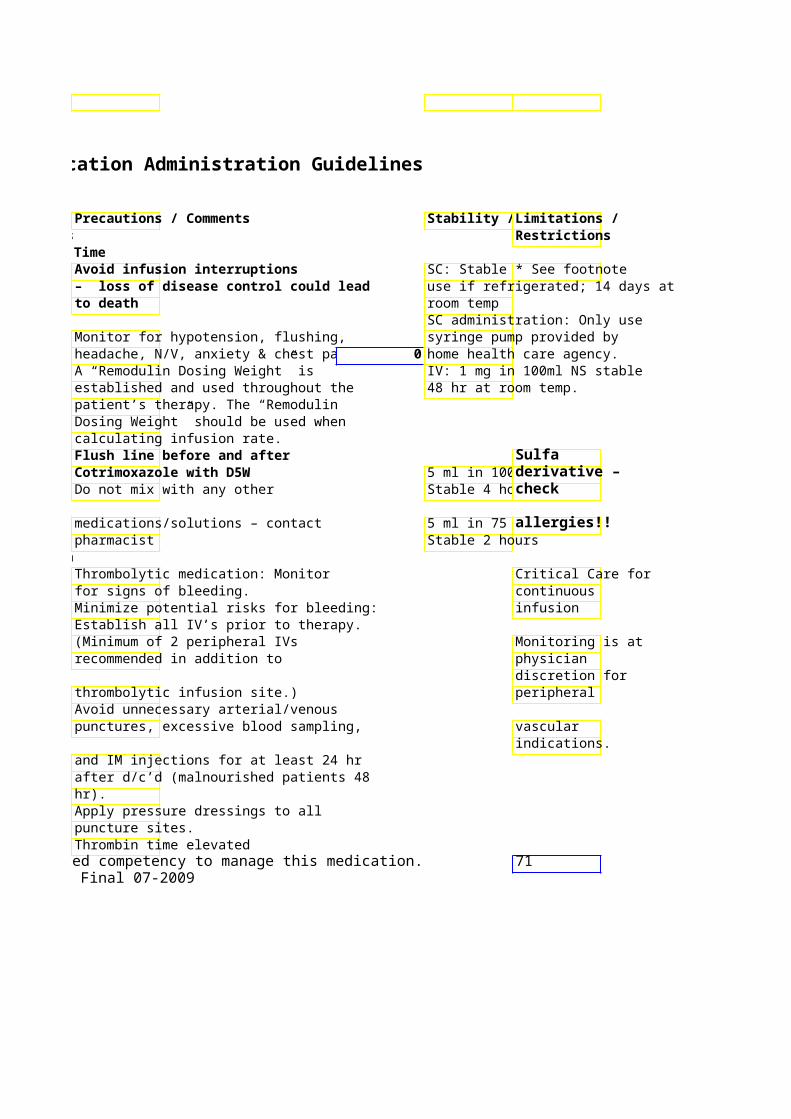
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard Diluent Generic - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Valproate Sodium 100mg/ml NO Intermittent Infusion – (Depacon) – 5ml vial Loading dose: 15 mg/Kg in 50-100 m
NS or D5W over 10-15 minutes Anticonvulsant Maintenance dose: 2-5 mg/kg q6-8h in
50-100 ml NS or D5W Infusion rate may be up to 3 mg/kg/min (total dose </= 15 mg/kg)
Vancomycin 500mg & NO Intermittent Infusion – 1Gm vial, <500mg in 100ml NS/D5W
Antibiotic/Glycopeptide Premix > 500 mg in 250ml NS/D5W bag: 500mg Infuse doses < 500 over 60 minutes /100ml
Infuse doses < 1 gm over 90 minuteInfuse doses > 1 gm over 120 minut
Vasopressin 20 units/ml Yes, Continuous Infusion – (Pitressin) –1 & 10ml For persistent Usual dose range:
vial VF/pulseless VT 0.2-1.0 units/min (GI bleeds) Hormone or asystole/PEA 0.02- 0.1 units/min (Shock)
40 units IV push x 1 – after flush System Standard Conc: 100 Units/
100ml NS (1 unit/ml) 10 ml NS
Vecuronium 10 & 20 mg Yes, Continuous Infusion: (Norcuron) vials intubation dose 0.1 Usual dose range: 1-2 mcg/Kg/min
(powder) mg/Kg rapidly *HIGH ALERT System Standard Conc: 50 mg/50 ml MEDICATION* NS (total vol=100 ml) (0.5 mg/ml)
Neuromuscular blocker
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
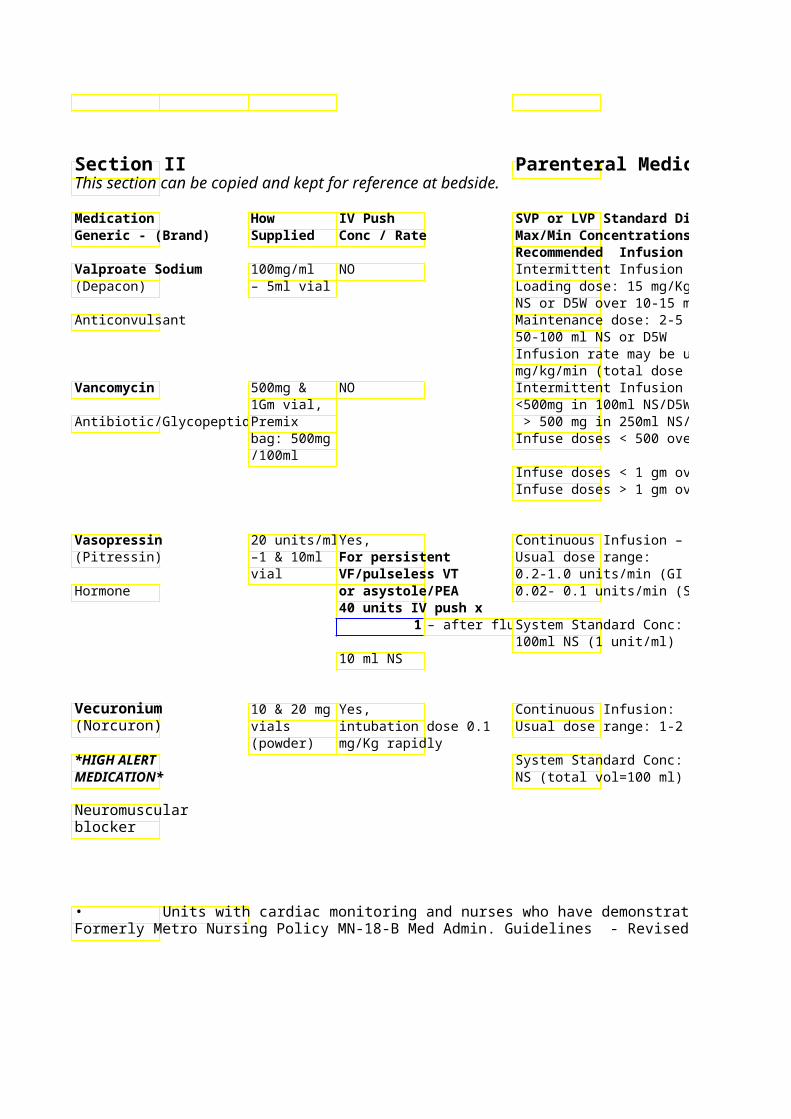
Parenteral Medication Administration Guidelines
SVP or LVP Standard Diluent Precautions / CommenStability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Dosing and monitoring service Loading dose: 15 mg/Kg in 50-100 mavailable from pharmacy per NS or D5W over 10-15 minutes physician order. Maintenance dose: 2-5 mg/kg q6-8h in
Infusion rate may be up to 3 mg/kg/min (total dose </= 15 mg/kg)
Slow rate of infusion if hypotension or <500mg in 100ml NS/D5W flushing occur > 500 mg in 250ml NS/D5W Avoid extravasation – Refer to PPO Infuse doses < 500 over 60 minutes 5046
Infuse doses < 1 gm over 90 minuteAminoglycoside dosing and Infuse doses > 1 gm over 120 minutmonitoring service available from
pharmacy upon physician order. Monitor renal function. Avoid extravasation/infiltration – Critical Care central line advised.
0.2-1.0 units/min (GI bleeds) 0.02- 0.1 units/min (Shock) Monitor BP, HR every 15 min
Monitor urine output every 1-2 hrSystem Standard Conc: 100 Units/ Monitor fluid and electrolyte status
Bradycardia and hypertension are early signs of toxicity Refer to Nursing Clinical Policies Controlled airway
Usual dose range: 1-2 mcg/Kg/min on Neuromuscular Blockade and ventilation (i.e. MN-13) required;
System Standard Conc: 50 mg/50 ml Critical Care NS (total vol=100 ml) (0.5 mg/ml) Preprinted order set available for ICU only:
neuromuscular blockade ED, ICU, Surgery. Sedation must be administered prior to and during paralytic use!
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 72Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
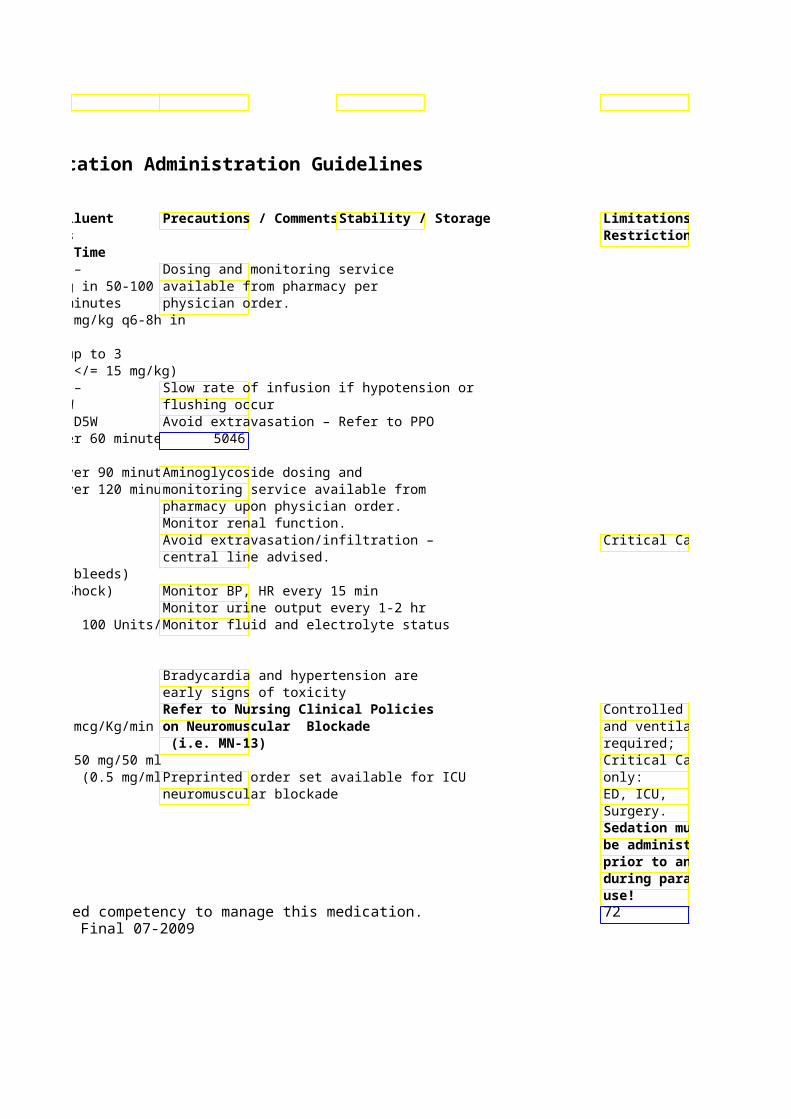
Limitations / Restrictions
Critical Care
Controlled airway and ventilation
Critical Care
Sedation must be administered prior to and during paralytic
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Verapamil 2.5mg/ml – Yes, Continuous Infusion: (Isoptin) 2 & 4ml 5-10 mg over 2 Usual dose range: 5-20
vial minutes (max rate Standard conc: 125 mg/150 ml NS Cardiovascular/ Calcium of 5 mg/min) (total vol=200 ml) (0.6Channel Blocker Slower in elderly “Concentrated” conc: 1
patients – max rate NS (total vol=100 ml) (of 2 mg/min
Vitamin K –See PhytonadioneVoriconazole 10 mg/ml NO Recommended dose: 6 mg(Vfend) 20 ml vial 12 hr x 2 doses then 4 m
12 hr Antifungal
Dilute in 250 ml NS Infuse over 2 hr
Refer to preprinted o2627) for dose, indications & contraindications
Warfarin 5 mg vial Yes, NO (Coumadin) Give dose over 1-
2 minutes Anticoagulant
IM administration NOT advised!
• Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009

Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Not compatible with bicarbonate * See footnote solutions
Standard conc: 125 mg/150 ml NS Avoid mixing with other medications/solutions – check with pharmacist
IV formulation contraindicated in pt with CrCl < 50 ml/min. PO formulation not contraindicated in pt with renal insufficiency nor is any dose reduction recommended Dose reduction recommended in pt with hepatic insufficiency/drug-drug interactions
2627) for dose, indications & Transient visual disturbances may occur ** Verify dose to be given. Discard Use only sterile water for vial after drawing up correct dose. **reconstitution
Once reconstituted, use within Monitor INR 4 hours
Keep vial in carton until use Do NOT refrigerate
Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 73Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
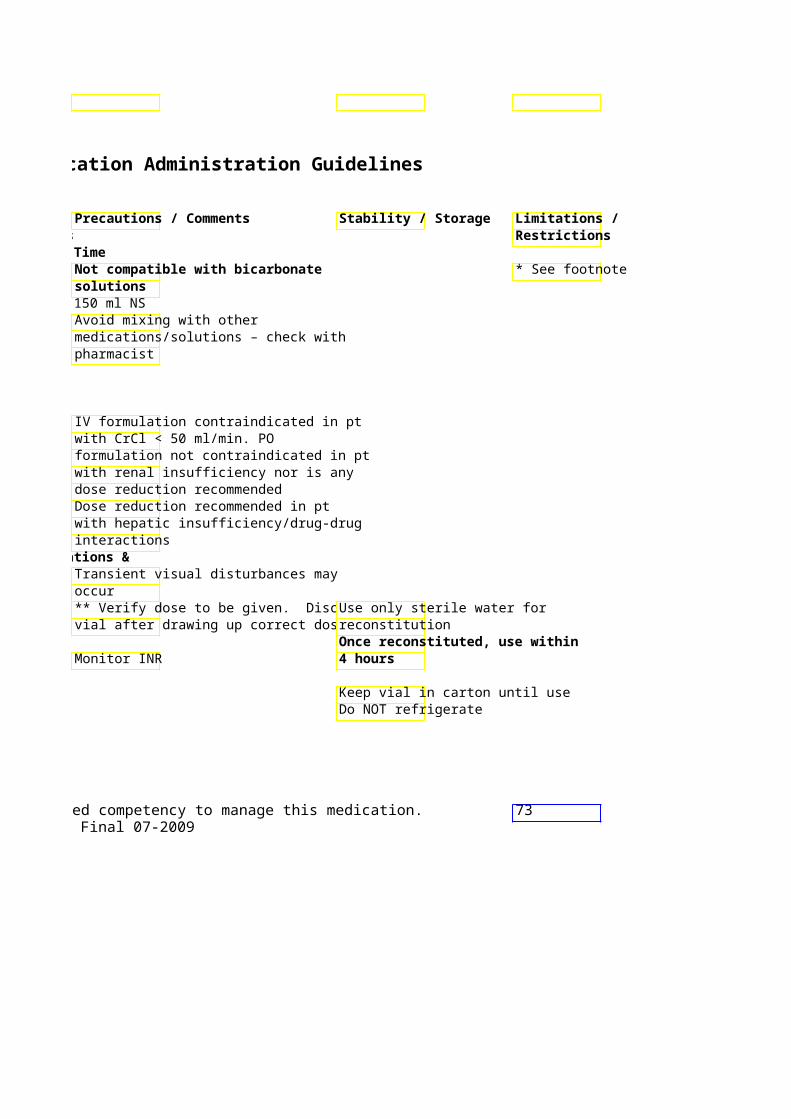
Section II Parenteral Medication Administration Guidelines This section can be copied and kept for reference at bedside.
Medication How IV Push SVP or LVP Standard DGeneric - (Brand) Supplied Conc / Rate Max/Min Concentrations
Recommended Infusion Time Ziconotide intrathecal100 mcg/ml Indicated for the managinfusion 1 & 5 ml Intrathecal severe chronic pain in (Prialt) vials, 25 administration intrathecal therapy is w
mcg/ml 20 only!! who are intolerant of or *HIGH ALERT ml vial other treatments. MEDICATION* due to intrathecal administration!!
Non-opioid analgesic
Zidovudine 10 mg/ml NO Intermittent infusion: 20 ml vial Infuse over 30-60 min
Antiviral L&D: 2mg/kg IV bolus ofollowed by 1mg/kg/hr IVuntil cord clamped, then PO regimen for infant(s).
Zoledronic Acid 4 mg vial NO Hypercalcemia / Bone Me(Zometa / Reclast) 5mg 4 mg/100ml NS or D5W o
premixed minimum of 15 minutes solution Repeat prn usually ever
Bisphosphonate but no more than once per week
Paget’s Disease / Osteop5mg/100mL premixed solminimum of 15minutes once yearly.
Doses given over < 15 mincrease risk of renal tox
Reference: Aurora Health Care - Department of Pharmacy Services – March 2009 • Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
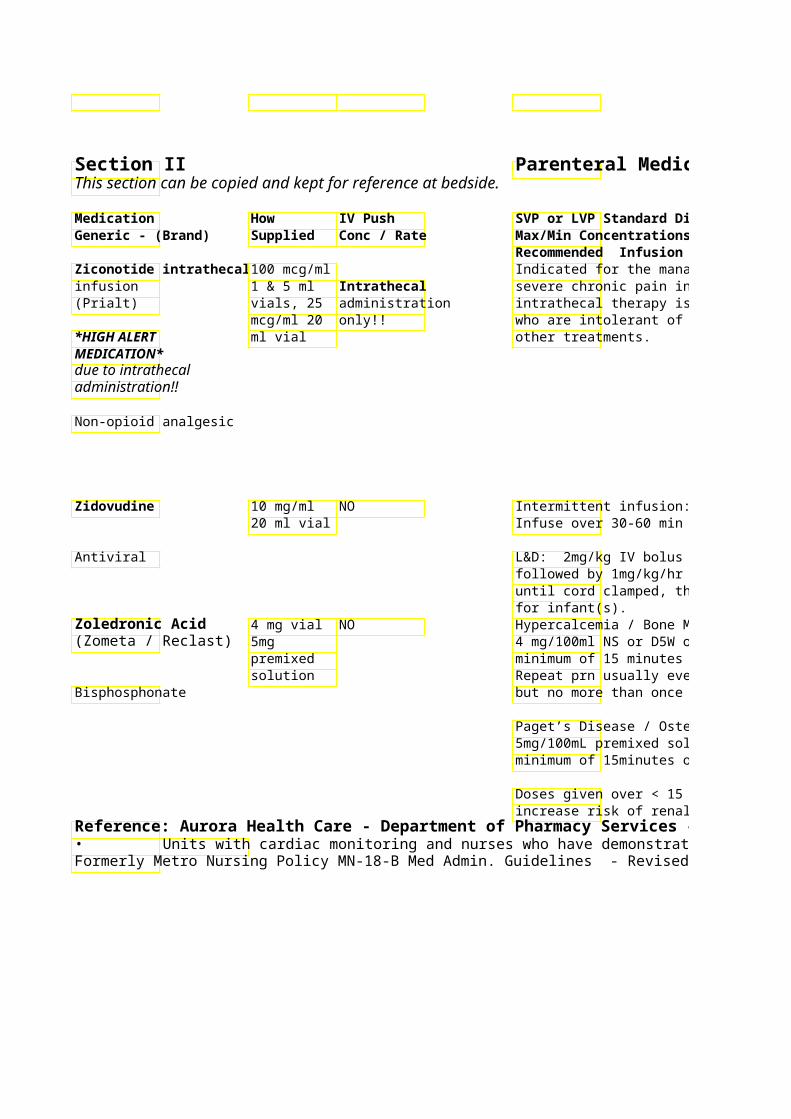
Parenteral Medication Administration Guidelines
Precautions / Comments Stability / Storage Limitations / Max/Min Concentrations Restrictions Recommended Infusion Time
Approved only for use in Medtronic Refrigerate SynchroMed EL, SynchroMed II Infusion Systems and Simms Deltec Dilute only with preservative CADD Micro External Microinfusion free NS Device and Catheter.
Expiration once placed in infusion Protect from light pump: Initial fill: 25 mcg/ml undiluted = 14 days Refill of pump: 25 mcg/ml & 100 mcg/ml undiluted = 60 days 100 mcg/ml diluted = 40 days May cause anemia or neutropenia Stable after dilution:
8 hr at room temp 24 hr refrigerated
100 mg PO zidovudine every 4 hr = 1 mg/kg IV every 4 hr Vial: Protect from light
until cord clamped, then PO regimen Do not mix with other medications/solutions
Assess baseline renal function, serum Restricted to calcium and vitamin D levels prior to outpatient use. administration. Monitor renal function (I/O, SCr) Mandatory
but no more than once per week System-wide Dose reduction recommended for orders required patients with CrCl < 60 ml/min. for use. Not recommended if CrCl <30ml/min
minimum of 15minutes once yearly. Hypotension in 10% of patients Bone pain common Mild fever and flu-like symptoms
Reference: Aurora Health Care - Department of Pharmacy Services – March 2009 Units with cardiac monitoring and nurses who have demonstrated competency to manage this medication. 74
Formerly Metro Nursing Policy MN-18-B Med Admin. Guidelines - Revised Final 07-2009
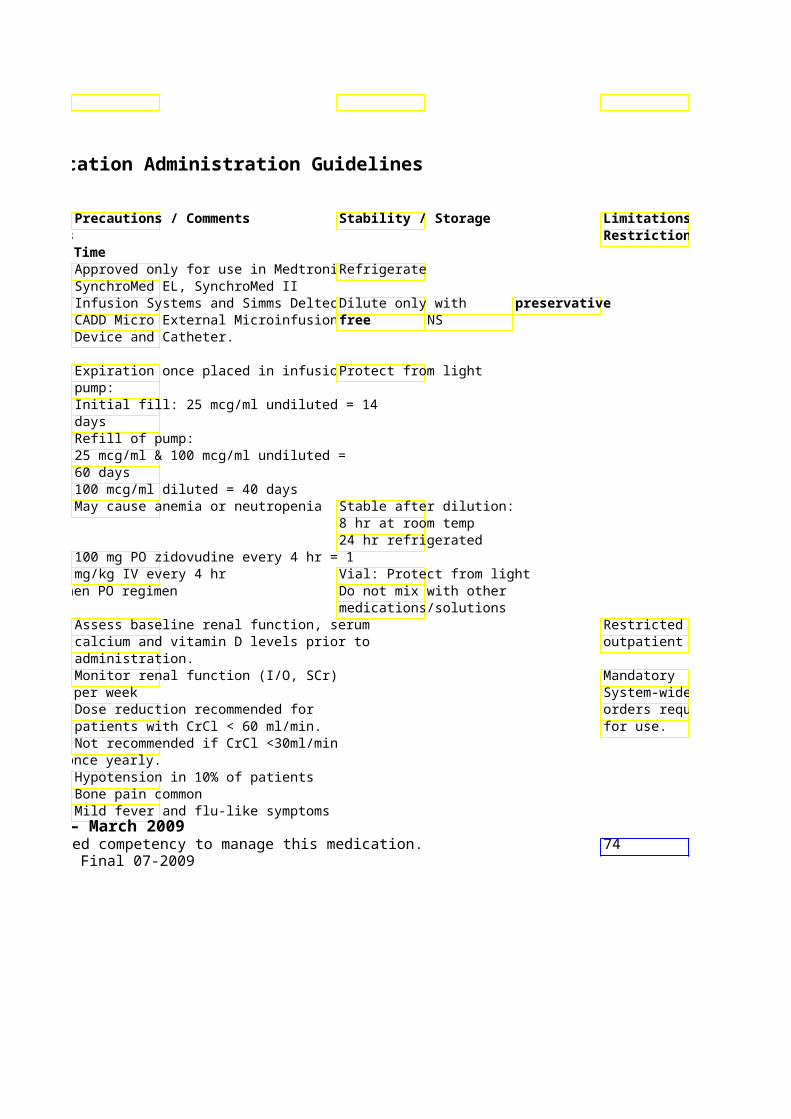
Limitations / Restrictions
Restricted to outpatient use.
System-wide orders required
Insulin & Parenteral Antiglycemic Agents Aurora Hospitals
Rapid-Acting Insulin Apidra; Insulin Glulisine Onset: 5 minutes Duration: 2-4 hours May be mixed with Novolin N (NPH) only 1 unit Apidra 1 unit regular human i?Give within 15 minutes before a meal or within 20 minutes after starting a meal In hospital: administer only when meal tray available Therapeutically equivalent to insulin aspart / lispro. Note: peak & duration extended in T2DM Rapid-Acting Insulin
Novolog; Insulin Aspart * Onset: 5-15 minutes Duration: 3-5 hoursMay be mixed with Novolin N (NPH) Therapeutically equivalent to Lispro (Humalog) In hospital: administer only when meal tray available
Short-Acting Insulin Novolin R; Regular Insulin * Onset: 30-60 minutes Duration: 5-8 hoursMay be mixed with: Novolin N (NPH) Therapeutically equivalent to Humulin R
Intermediate-Acting Insulin Novolin N; NPH Insulin *Onset: 2-4 hours Duration: 14-18 hours May be mixed with Novolog and Novolin R Therapeutically equivalent to Humulin N
Long-Acting Insulin Lantus; Insulin Glargine* Onset: 1.5-2 hours Duration: 20-24 hours
Can not be mixed with any other insulins Administered once daily in most patients.
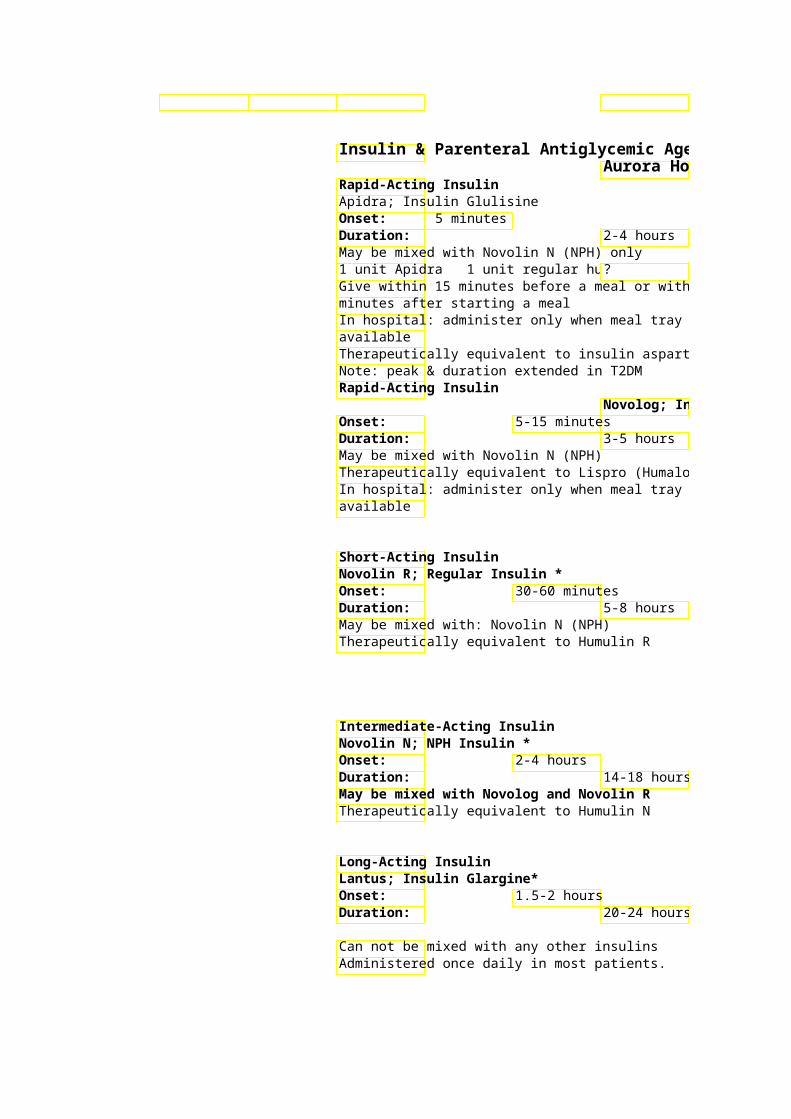
Insulin & Parenteral Antiglycemic Agents Aurora Hospitals
Give within 15 minutes before a meal or within 20
Therapeutically equivalent to insulin aspart / lispro.
Novolog; Insulin Aspart *
14-18 hours May be mixed with Novolog and Novolin R
20-24 hours
Long-Acting Insulin ®
Levemir ; Insulin Detemir * Onset: 3-14 hours Duration:Can not be mixed with any other insulins Administered once or twice daily
Insulin Aspart Mix Novolog Mix 70/30
Onset: More rapid than regular insulin mixes - administer with meals Peak effect:Duration:Administered once or twice daily. Do not mix with other insulin products. Shake prior to use – must appear uniformly white & cloudy. Premixed 70/30 Insulin Novolin 70/30 * Onset: 30-60 minutes Duration: Premixed with 70% NPH and 30% Regular Cannot be mixed with any other insulin
Parenteral Antigylcemic Agents – These are ®Symlin ; Pramlintide Amylin Analog - augments effects of insulin and
reduces prandial insulin requirements by 50% Should not be started in hospitalized patients due
Do not mix with insulin products. ®Byetta ; Exenatide Glucagon-like Peptide-1 Analog (GLP-1) used in Type 2 DM Peak response: 2 3 hours Duration: up to 5 hours Hold if NPO.
Insulin Product Ordered Insulin Glulisine (Apidra) Insulin Lispro (Humalog) Humulin 50/50 Humalog (Lispro Mix) 75/25 Humalog (Lispro Mix) 50/50

Novolin 70/30 Note: Formulary Substitutions as of April 2009. Contact your pharmacist with questions regarding substitutions as necessary

6-24 hours
More rapid than regular insulin mixes -
1-4hours up to 24hours
Do not mix with other insulin products. Shake prior
30-60 minutes 14-18 hours
not Insulin Products
Amylin Analog - augments effects of insulin and Do likely to skip a meal/not eat enough,
? hypoglycemic, or has gastroparesis Should not be started in hospitalized patients due Give SQ immediately prior or within 15 min
to high risk of nausea, vomiting, & beforehypoglycemia. meals.
only, as an alternative to insulin-
Formulary Insulins & Antiglycemics are indicated with an asterix (*).
AHC Formulary Substitution Equivalent number of units of Insulin Aspart (Novolog)Equivalent number of units of Insulin Aspart (Novolog)
50% of the ordered doseNPH and 50% of ordered dose as Equivalent number of uniInsulin Aspart Mix 70/30 (Novolog Mix 70/30)
50% of the ordered doseNPH and 50% of the ordered dose as
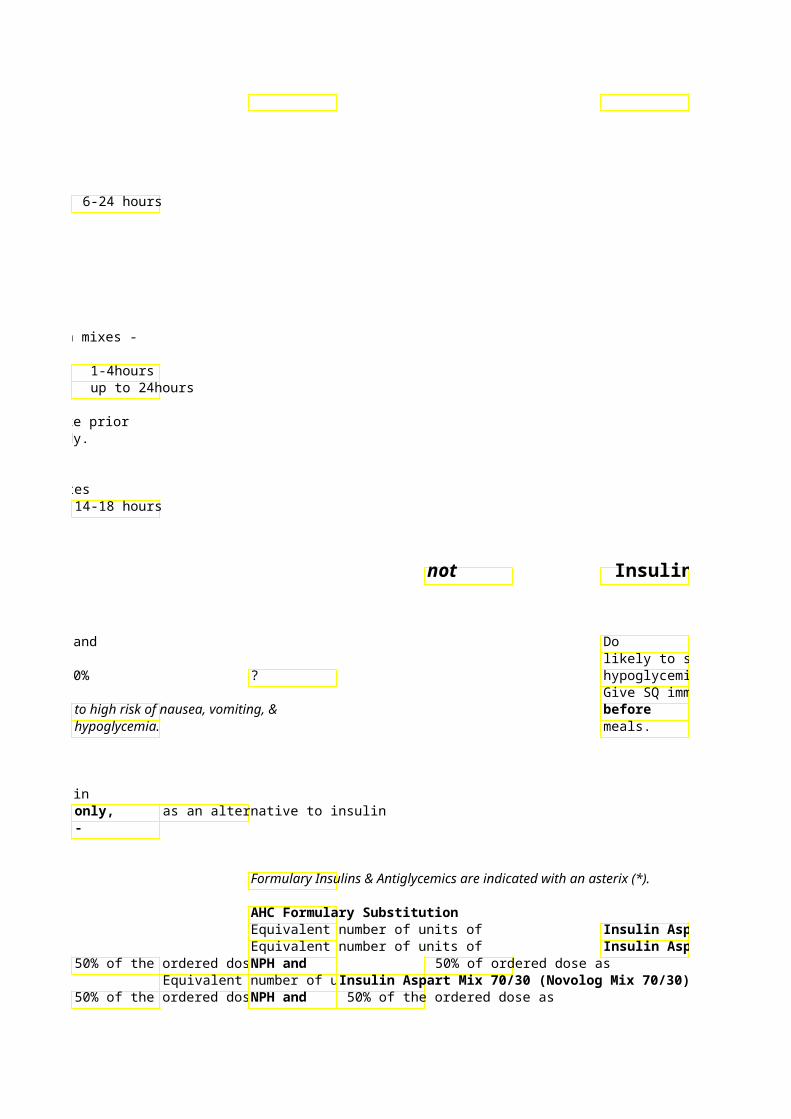
Equivalent number of uniInsulin Aspart Mix 70/30 (Novolog Mix 70/30)Note: Formulary Substitutions as of April 2009. Contact your pharmacist with questions regarding substitutions as necessary
Insulin Products
not use pramlintide if the patient is NPO, likely to skip a meal/not eat enough, hypoglycemic, or has gastroparesis Give SQ immediately prior or within 15 min
each major meal, do not give after
Twice daily SQ injection, before breakfastand supper.
Dose anytimbefore meals.
Formulary Insulins & Antiglycemics are indicated with an asterix (*).
Insulin Aspart (Novolog)Insulin Aspart (Novolog)
Insulin Aspart (Novolog)Insulin Aspart Mix 70/30 (Novolog Mix 70/30)
Insulin Aspart (Novolog)

Insulin Aspart Mix 70/30 (Novolog Mix 70/30)0