medication reconciliation insert your hospital’s name here
Post on 19-Dec-2015
218 views
TRANSCRIPT

Medication Reconciliation
Insert your hospital’s name here
Agenda
Define the problem What is medication reconciliation? CheckPoint measure Things to consider when developing a
process Keys to success

What is the problem? Hospitalized patients who experience an
adverse drug event (ADE) are twice as likely to die as those without an ADE (JAMA 1997; 277:301-306)
The Institute of Medicine has estimated that medication errors account for 7,000 deaths annually (To Error Is Human: building a safer health system, 1997, IOM)
ADEs account for 6.3% of malpractice claims (Arch Intern Med. 2002; 162:2414-2420)
Where is the problem?
Chart reviews revealed that 50% of all medication errors and 20% of adverse drug events are due to poor communication at the interfaces of care (Institute for Healthcare Improvement 2005)
Patient admission to the hospital Patient transfer out of specialty units to
other nursing units Patient discharge from the hospital

Why?
Interfaces lack a process for comparing the patient’s most current list of medications against physician orders for admission, transfer, and discharge

Examples of interface problems Physician admission orders read
“continue home meds” Patients transferring from a critical
care setting to a nursing unit would still have lidocaine drip listed on their medication record
Patients’ discharge orders read “discharge on home meds”

What is Medication Reconciliation?
A process of identifying the most accurate list of medications a patient is taking and using this list to provide correct medications for the patient anywhere within the health care system

How Are Medications Reconciled?
1. Verify: Collect an accurate medication history
2. Clarify: Compare the patients list of current medications – including name, dosage, frequency, and route – against the physician’s orders. Any medication that does not match must be “reconciled” by bringing the discrepancies to the attention of the physician
3. Reconcile: Document the change or why the medication was not ordered to communicate to the healthcare team

When are Medications Reconciled?
Admission The patient’s home medications are
compared to the physician’s admission medication orders
Transfer One Unit to Another Unit The patient’s most current medication
record is compared against the physician's transfer orders
Discharge The patient’s reconciled list of admission
medications is compared against the physician’s discharge orders

Sample High Level Medication Reconciliation Process
Patient Profile H&P/Clinic Note/Outpt Pharmacy
Reconciled Admission Med List
Reconciled Discharge Med List
Admission Orders
Latest MAR
Discharge Orders
Medication Reconciliation is Viewed as a Quality Measure
JCAHO 2005 safety goal IHI 100K Lives Campaign
WI Node 100K Lives Web site Statewide improvement team
(PSW/WHA) CheckPoint Error Prevention Measure It is the right thing to do, but very
challenging to implement

8%
37%
20%
10%
25%
0% 10% 20% 30% 40%
Not planning
Discussing & Organizing
Planning & Educating
I mplementation Scheduled
I mplemented
WI Hospital Medication Reconciliation Survey – June 30, 2005
N=57 Wisconsin Hospitals
CheckPoint Scoring
Each hospital that volunteers to publicly report on the medication reconciliation measure will have their score posted to the CheckPoint website with the other Error Prevention measures
The medication reconciliation score will consist of a composite number ranging from 0-100 points
The points are cumulative based on the hospitals response to 4 components
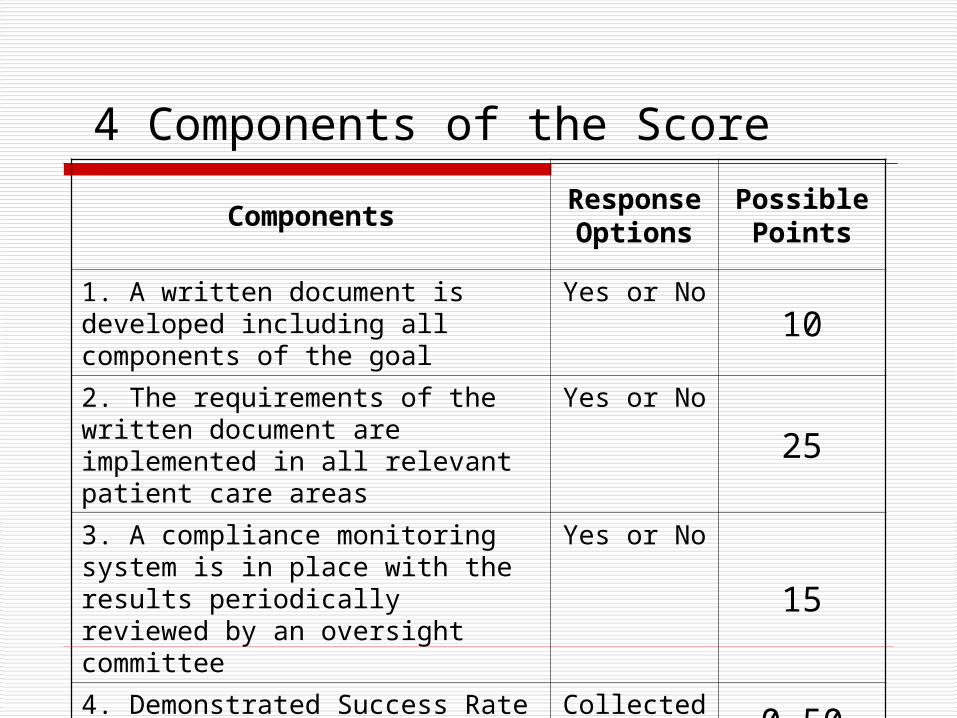
4 Components of the Score
ComponentsRespons
e Options
Possible Points
1. A written document is developed including all components of the goal
Yes or No10
2. The requirements of the written document are implemented in all relevant patient care areas
Yes or No
25
3. A compliance monitoring system is in place with the results periodically reviewed by an oversight committee
Yes or No
15
4. Demonstrated Success Rate (DSR): varies by goal
Collected Rate 0-50

Goal 6 DSR – Medication Reconciliation
Number of cases that have a complete medication reconciliation form in theirmedical record within 48 hours of admission____________________________________ X 100
Total number of cases reviewed
What is a “complete” form?
All fields required by your hospital’s policy are complete on the form Must include medication name, does, frequency,
route and reconciliation status All medications are reconciled with a
Medication order OR Documentation that the medication was not ordered
All required signature are present Must have at least 2 signatures from different
disciplines
What Medications are Included?
All medications on the patients current home medication record should be reconciled Prescription Over-the-counter Homeopathic Vitamins Herbals Nutritional supplements
If your hospital has a policy that excludes OTC, homeopathics, vitamins, herbals, or nutritional supplements from reconciliation, you may consider these medications reconciled
Reconciliation Definitions If a medication is on the patient’s
current home record, but no order is written, it is reconciled if: Documentation that it is not being
ordered Contraindicated for the admitting
condition If the patient is NPO on admission and
no medications are ordered, the case is reconciled

48 Hours
Use the inpatient admission date and time to determine the 48 hour window
Make sure that the date and time the reconciliation was completed is on your reconciliation form
Case Selection
Minimum number is 75 cases in 6 months Inclusion criteria
All patients admitted for inpatient services including admits from the ER and direct admits
Exclusion criteria LOS based on admit date and time of <48 hours Patient unresponsive on admission and you cannot
obtain a medication history from a competent source
Newborn born during that admission

CheckPoint Report
WHA will start reporting the medication reconciliation measure March 15, 2006 as part of the CheckPoint Error Prevention report www.wicheckpoint.org
The data will be updated every 6 months

Optional Internal Measures
Number of reconciled medications Number of medication errors after
reconciliation Number of adverse medication events
related to non reconciliation Number of admissions reconciled
Things to Consider
Admission Sources of information
Patient and family (have patient bring meds?) Physician’s office Patients pharmacy Past medical record Transfer form
Format? What medications are included? Who does it?
Speed and accuracy Discrepancies
What will the process be? Who follows up?
Reconciliation Who does it?

Transfer Compare medication lists before and
after a transfer or procedure Check home meds Who does it?

Discharge Review 3 lists
Current meds Home Meds Discharge orders
Document format Who does it?
Patient Education Address hospital formulary changes Who gets the discharge medication list? Encourage patient to maintain a accurate medication
list over time

Team effort, but who does what?
Physician Best knowledge of patient Decision maker/write the orders
Nurse Best access to patient and family Frequently does the admission history Frequently does the discharge education
Pharmacist Best knowledge of drugs and formulary Limited patient and family access Hosp/community pharmacy interface Transfer reconciliation

Patient Real decision maker Variable motivation factors that need to be
included Need tools to keep track of medications
Administration Realize the gravity and challenges of the process Prioritize clinical resources Culture of patient safety
Keys to Successful Implementation
1) Teamwork!2) Commitment to improve by nurses,
pharmacists, physicians, and administration3) Baseline and ongoing data collection to track
progress4) Policies and procedures to govern the process5) Well designed and communicated processes
a) Thorough evaluation of existing processes including a high level flowchart of the existing process to determine where problems exist
b) Flowchart new process to assure new problems not created and to use as a communication tool

6) Create/adopt forms to document reconciliation at admission, transfer and discharge
a) May have one or many forms b) Forms may be paper, electronic, or a combination of
botha) Remember to review computer systems to
determine if there are links to existing information that could be utilize
7) Educate staff to assure that everyone understands and can use the new process consistently
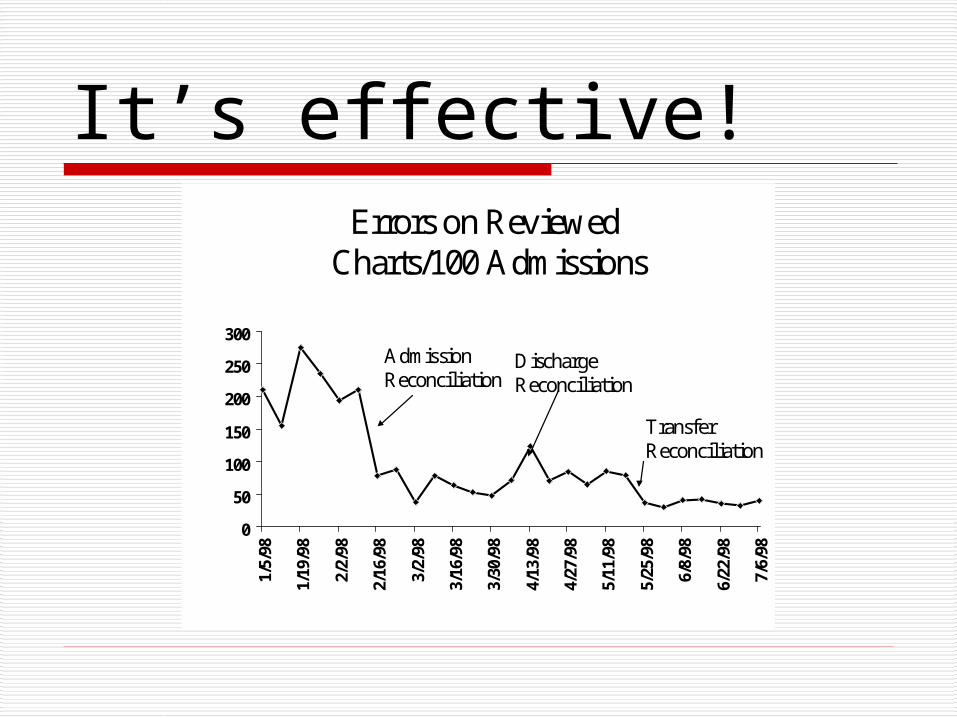
It’s effective!Errors on Reviewed
Charts/100 Admissions
0
50
100
150
200
250
300
1/5/98
1/19/98
2/2/98
2/16/98
3/2/98
3/16/98
3/30/98
4/13/98
4/27/98
5/11/98
5/25/98
6/8/98
6/22/98
7/6/98
AdmissionReconciliation
DischargeReconciliation
TransferReconciliation