medicine reconciliation - disabilities fife files/nhs/the nhs fife... · reviewer nhs fife joint...
TRANSCRIPT

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 1 of 12 Review Due:
MEDICINE RECONCILIATION
DOCUMENT CONTROL POLICY NO F6-9
Policy Manual/System NHS FIFE JOINT CODE OF PRACTICE: MEDICINES
Author J Bate, B Wilkie, M Paterson, A Kilpatrick
Version No: 1.0
Reviewer NHS Fife Joint COPM Review Group
Implementation Date
Status Draft Last Review Date January 2014
Authorised By: Medical Director Next Review Date
Associate Nurse Director NHS Fife
Director of Pharmacy
NHS Fife acknowledges and agrees with the importance of regular and timely review of policy statements and aims to review policies within the timescales set out. New policies will be subject to a review date of no more than 1 year from the date of first issue. Reviewed policies will have a review date set that is relevant to the content (advised by the author) but will be no longer than 3 years. If a policy is past its review date then the content will remain extant until such time as the policy review is complete and the new version published. NHS Fife are currently working toward the merge of both Community Health Partnership and Operational Division policies to create one NHS Fife Code of Practice Medicines. During this merge there may be a risk of discrepancies in the numbering throughout documents and advise Code of Practice Medicines users to take care if cross-referencing. 1. FUNCTION
To establish a standardised process of obtaining and documenting an up-to-date and
accurate medication list for a patient that has been compared with the most recently available information with any discrepancies, changes, deletions or additions resulting in a complete list of medications accurately communicated. This policy applies at all key transition points e.g. admission, transfer and discharge and aids in providing a seamless transition of care across the boundaries
2. LOCATION
All areas in which medicines are prescribed and/or administered across NHS Fife 3. RESPONSIBILITY
3.1 This policy applies to all healthcare professionals who are responsible for undertaking
medicines reconciliation at the key transition points of admission, including pre-assessment, transfer between wards and discharge.
Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 2 of 12 Review Due:
3.2 Medical Staff
Obtain and document on the medicines reconciliation form, an accurate medication list using at least two vital sources (if available). See 4.2 for further guidance
Document a plan for each medicine on the medicines reconciliation form by completing the continue, withhold and stop boxes
Prescribe medicines accurately onto the medicine chart
Undertake medicines reconciliation on discharge and record this on the immediate discharge and prescription form.
3.3 Pharmacy
Clinical Pharmacy staff will check that medicines reconciliation is undertaken on admission, transfer and discharge and work with the multidisciplinary team to resolve any issues
Assist with informal referrals from medical and nursing staff of more complex patients or where there is inadequate information to obtain an accurate medication history
Dispense necessary medicines prescribed on the immediate discharge and prescription form
There may be areas where pharmacy staff undertake medicines reconciliation on the admission document
3.4 Nursing
Highlight to medical staff if there are medicines that a patient normally takes at home that are not prescribed on the medicine kardex.
Nurse practitioners will undertake medicines reconciliation on the admission document
Check the correct medicine, dose and frequency are supplied to the patient from the immediate discharge and prescription form
File the appropriate copy of the immediate discharge and prescription form in the patient’s notes.
4. OPERATIONAL SYSTEM
4.1 Medicines Reconciliation on Admission 4.1.1 This task must be undertaken by the admitting doctor or advanced nurse
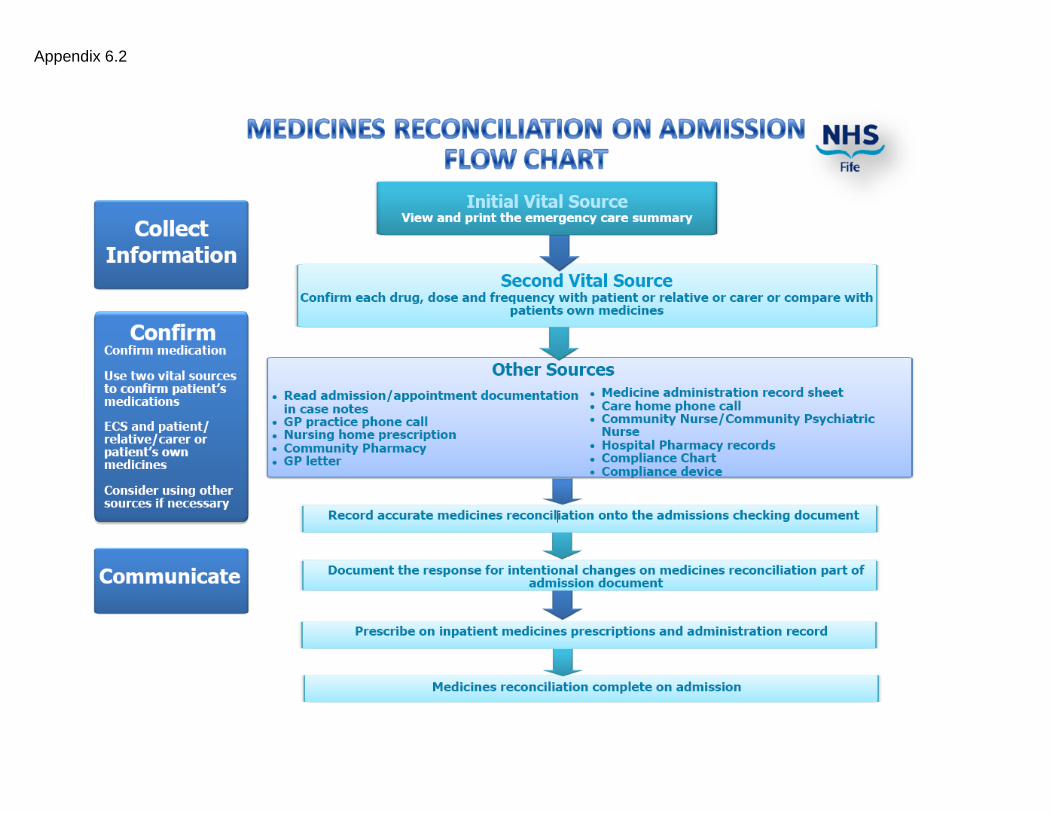
practitioner to any healthcare setting 4.2 Collect medicine list using at least two vital sources (if available)
a) Emergency Care Summary (ECS) b) Patient or carer c) Patient’s own medicines.

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 3 of 12 Review Due:
Other sources that may be used to obtain an accurate medication history include:
GP letter
GP practice printout
Medicine Administration Record Sheet (MAR)
GP repeat slip
Phone call with GP or practice pharmacist
Community pharmacy
Care home phone call
Case notes / previous discharge prescription
Community Nurse e.g. Community Psychiatric Nurse (CPN), District Nurse
Day Hospitals
Anticoagulation clinics
Hospital pharmacy records e.g. anti-TNF medicines, psychiatric medicines
Compliance chart / device
Outpatient letters. This list is not exhaustive.
4.2.1 Registered practitioners must use their clinical judgement to determine what sources are appropriate to obtain an accurate medicine list for each individual patient.
4.3 The “collected” medicine list must be confirmed with the patient / carer
Discuss each individual medicine, dose and frequency with the patient or carer (where possible)
Use the patient’s own medicines (where possible) to verify the information on the electronic medication list to confirm the final list of medicines
Check that the patient is not receiving medicines from sources other than GP e.g. antipsychotic clinics, infectious diseases unit, homecare companies, sexual health clinics, non-medical prescribing clinics, haematology clinics, community pharmacy over the counter medicines or herbal medicines.

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 4 of 12 Review Due:
4.3.1 Medicines that require special attention when undertaking medicine reconciliation include:
Parkinson’s Disease (PD) medicines – document the specific times of each PD medicine and the name of the different preparations
Warfarin – record where INR is checked e.g. GP or anticoagulation clinic, usual dose at home, indication, target INR and length of therapy
Steroids – record the length of course, whether it is long term maintenance, a short course or a reducing course
Cytotoxics –need careful documentation
For weekly / monthly treatments provide the day of the week or date of last dose
Depot injections – record dose and frequency and date / site of last administration
Methadone (for addictions management) – the dose must be confirmed with the GP or addictions team and the community pharmacy. Please note information relating to the patient being prescribed methadone may not be on the ECS.
As required medicines – ensure it is specifically highlighted that these medicines are not regular and give clear directions of the intended frequency (e.g. analgesics and hypnotics)
Hypnotics – often dose if changed frequently so always clarify specific dose is correct
Insulin – ensure that correct dose, formulation and device are prescribed
Clozapine – record date and time of last dose (do not prescribe if >48hours since last dose)
Lithium – prescribe by brand, ensure correct formulation is prescribed
This list is by no means exhaustive. 4.4 Communicate a complete list of current medication
4.4.1 A medicines reconciliation form must be completed for each patient with the
following information:
Patient name and CHI number
Sources of information used for the medication history
Generic name of all current medicines unless brand specific e.g. Uniphyllin for theophylline, Priadel for lithium carbonate
Short courses of medicines, for example steroids, antibiotics
Dose and frequency
Formulations / devices if applicable e.g. insulin devices, inhalers
Non-prescription medicines including over the counter / herbal / homeopathic medicines
Recently discontinued medicines if applicable
Concordance issues that may be apparent
Allergy status / adverse drug reactions and the nature of the reaction / allergy
Signature of doctor, nurse or pharmacist documenting the medication history
Time and date that medication history has been taken.

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 5 of 12 Review Due:
4.4.2 A plan for each medicine must be documented on the medicine reconciliation form or ECS using the Continue, Withhold and Stop columns and the reasons for this action. This will highlight intentional discrepancies between the medicines the patient was taking prior to admission and the medicines prescribed in the new care setting that have been changed intentionally and agreed with the consultant responsible for the patient’s care.
4.4.3 Discuss and ensure patient/carer understands any changes to the patient’s medication regimen.
4.4.4 Clear documentation will also highlight unintentional discrepancies (errors,
omissions or unintentional additions) between the medicines the patient was taking prior to admission and the medicines prescribed in their new care setting that is not a conscious change. The reason for a medicine being discontinued or withheld must be documented.
4.4.5 If the decision to withhold a medicine is made a follow up review date must be
planned at this stage. 4.4.6 All medicines from the patient’s medication history that are to be continued
must be accurately and legibly prescribed on the inpatient medicine chart by the prescriber in accordance with NHS Fife Code of Practice Medicines polices on prescribing (F3-1 / F3-2).
4.5 Medicines reconciliation on transfer
4.5.1 Medicines reconciliation must be undertaken prior to the transfer of a patient.
This includes the transfer of patients between wards and between hospitals. This must also be undertaken where the medicine chart needs to be re-written. Consideration should be given to medicines which can be stopped prior to transfer and medicines which have been temporarily withheld which may need to be restarted.
4.5.2 When starting, stopping or withholding a patient’s medicine the reasons for
this must be clearly documented on the medicine chart and medical notes. 4.5.3 Medical staff in critical care are responsible for reviewing medicines and
rewriting the Drug Prescription and Administration chart prior to the patient being transferred to a general ward.
4.6 Medicines reconciliation on discharge
4.6.1 When a patient is discharged from hospital, medicines reconciliation must be performed. This will ensure the transfer of accurate medication information between the care settings. The discharge prescription must contain an accurate list of all the medicines the patient is to take at home including the dose, frequency and route. Any medicines that have been stopped, started or any changes to the doses must be documented on the discharge prescription along with the reasons for the changes. Discuss and ensure patient/carer understands any changes to the patient’s medication regimen.
4.6.2 An Immediate Discharge Prescription Form must be completed for all
patients. 4.6.3 This must be completed by medical staff / non-medical prescribers.

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 6 of 12 Review Due:
4.6.4 Collect medicine information for accurately documenting a discharge prescription. This can include:
Current medicine chart and previous medicine charts if necessary
Medicine reconciliation form from admission
ECS record. 4.6.5 Confirm the discharge medication on the Immediate Discharge
Prescription Form
Complete a list of medication required at discharge with drug, dose and frequency and duration of treatment (if applicable)
Detail the supply method for each medicine, in particular whether hospital pharmacy dispensing is required (if Patients Own Drugs not available)
Document the reasons for stopping any medicines in hospital in the “Changes to Medication” section.
Document any medication started during admission along with the indication in the “Changes to Medication” section
Any medicine to be re-started following discharge (e.g. anti-platelet and anti-coagulants) must be clearly documented on the Immediate Discharge Prescription Form
Any medicines which are to be monitored or reviewed must be documented clearly on the Immediate Discharge Prescription Form
The Immediate Discharge Prescription Form must be clinically signed off by medical staff / non-medical prescriber.
4.6.6 Communicate discharge medication
If discharge medication is required from pharmacy the Immediate Discharge Prescription Form must be sent to pharmacy for dispensing
On return of dispensed medicines from pharmacy check against medicine chart and Immediate Discharge Prescription Form for accuracy
Send a copy of Immediate Discharge Prescription Form to GP surgery and community pharmacy e.g. fax, email etc.
Medicines are given to patient with appropriate counselling, especially where there have been changes to treatment.
It must be documented on the Immediate Discharge and Prescription Form that the patient and / or carer has been counselled on their discharge medication
Patients are given copy of the Immediate Discharge Prescription Form to hand into GP surgery.
4.6.7 A list of discharge medicines should be given to the patient or carer to aid
compliance with their medicines at home. 4.7 Outpatient Review
4.7.1 Any medicines stopped, started or altered must be clearly communicated to
the GP detailing the indication or reason for alteration. Discuss and ensure patient/carer understands any changes to the patient’s medication regimen
4.8 Medicine Reconciliation in Primary Care
4.8.1 Reconcile records at GP surgery after discharge or outpatient review following the processes developed from the Patient Safety Programme Primary Care Medicines Reconciliation Bundle.

Document in - APR 2014\Medicines Reconciliation Group - Request for group
representation v0 1 21 Apr 14 (2) (2).doc
Issue 0.1 6/1/14
Jonathan Bate Page 7 of 12 Review Due:
4.9 Consent
4.9.1
Consent for access to ECS. See Appendix 6.1. “Access to The Emergency Care Summary by Secondary Care Clinicians” for clarification of rights of access to the ECS.
5. RISK ASSESSMENT
5.1 The key risks involved in the implementation of this policy are:-
Lack of awareness of staff resulting in medicine not being supplied to patients on discharge.
Staff not being able to access clinical policies, procedures and guidance documents to ensure the delivery of safe and effective care.
5.2 These key risks, along with any others, are addressed through the robust
implementation of the policy led by the Code of Practice: Medicines Review Group Medical, Nursing, Pharmacy staff and Non-medical Prescribers.
6. RELATED DOCUMENTS
6.1 Access to The Emergency Care Summary by Secondary Care Clinicians. 20
December 2012.
6.2 Medicines Reconciliation on admission Flow Chart.
6.3 Medicines Reconciliation on discharge Flow Chart.
6.4 Example of Medicines Reconciliation Form.
7. REFERENCES
7.1 National Institute for Health and Clinical Excellence / National Patient Safety Agency. Technical patient safety solutions for medicines reconciliation on admission of adults to hospital. Department of Health. December 2007
7.2 www.patientsafetyalliance.scot.nhs.uk 7.3 NHS Tayside Medicine Reconciliation Steering Group, Medicines Reconciliation
Policy, May 2013, NHS Tayside. 7.4 The Scottish Government. Safer Use of Medicines. Medicine Reconciliation: Revised
Definition, Goals and Measures and Recommended Practice Statements for the Scottish Patient Safety Programme. 19 September 2013. SGHD/CMO(2013)18
7.5 Clark S, Birnie G. Letter to NHS Fife Consultants, Associate Specialists, Specialty Doctors and Trainees. “Access to the Emergency Care Summary By Secondary Care Clinicians” 20 December 2005. 2 pages.

Appendix 6.1
Fife NHS Board
Hayfield House
Hayfield Road
Kirkcaldy
Fife KY2 5AH
Telephone: 01592 643355
Fax: 01592 648142
www.show.scot.nhs.uk
Distribution: Date 20 December 2012
Your Ref
Consultants Our Ref SAC/ED
Associate Specialists
Specialty Doctors Enquiries to Dr Stella Clark
Trainees Extension 28143
Direct Line 01592 648143
Fax No 01592 648142
Email [email protected]
Dear Doctor
ACCESS TO THE EMERGENCY CARE SUMMARY BY SECONDARY CARE CLINICIANS
The purpose of this letter is to clarify rights of access to the Emergency Care Summary which contains
important information about current medication prescribed by a patient’s General Practitioner.
The content of this letter has been agreed by the NHS Fife Information Governance Group and the
National Emergency Care Summary Board. This letter provides information about:
When it is appropriate to use presumed consent for access
Access to the Emergency Care Summary in cases where the patient is unable to give informed
consent.
Situations where presumed consent is acceptable
In emergency situations patients referred by the following routes will have already given consent to the
Emergency Care Summary being accessed. These situations include:
Referral directly from NHS 24
Referral from the Primary Care Emergency Service
Direct referrals from General Practitioners in emergency situations
Where a recent referral from the General Practitioner is available in the Clinical Portal or Sci
Store
Where a patient is incapable of giving consent.
In summary, should a patient present in any of the ways described above the Emergency Care Summary
can be accessed using presumed consent.

Access to the Emergency Care Summary where patients are unable to consent due to incapacity
Secondary care clinicians require access to the information contained in the Emergency Care Summary in
both urgent situations and at times of transfer of responsibility through the inpatient care pathway. This
can cause concerns for clinical staff when a patient is incapable of consenting. The following paragraphs
outline the legal basis for consent in such situations:
During the first 24 hours of a patient’s admission access to the Emergency Care Summary, common law
provides legal protection for such an intervention when a patient is incapable of consenting. Following
advice from the Mental Welfare Commission the timeframe for such access is the first 24 hours of
admission. The first 24 of a patient’s admission enables clinical staff:
Consult with family members
Consult with a Power of Attorney or Guardian where either of these exist
Complete an Adults with Incapacity Act certificate in consultation with the family where this is
required.
Access to the Emergency Care Summary beyond 24 hours where the patient remains incapable of
giving informed consent must be supported by the completion of an Adults with Incapacity Act Section
47 medical certificate. Such a certificate must be completed in consultation with the patient’s family.
With the above guidance it is clear that Clinicians in secondary care can and should be accessing the
Emergency Care Summary.
A&E is the only place where patients are likely to attend hospital without having been referred by a
General Practitioner, NHS 24 or the Primary Care Emergency Service. A&E staff will therefore require
to continue asking a patient’s consent to access the Emergency Care Summary unless the patient is
incapable of giving consent.
With best wishes.
Yours sincerely
DR STELLA CLARK DR GORDON BIRNIE
Medical Director, Primary Care Medical Director, Operational Division
Appendix 6.2

Appendix 6.3

Patient Name: GP Name / Tel: CHI Number
EXAMPLE
Medicines Reconciliation
Source of medication history (Minimum 2 sources)
Patient Relative / Carer
GP Phone call
ECS Patient’s own drugs
Community Pharmacy
GP letter / Summary
Repeat Script
Other (please specify)
Admission Medicines Plan for medicines (Dr Complete)
Comments (Reason for alteration)
Name Dose Freq Continue Amend Withhold Stop
Allergies List any Over the Counter or alternative medicines
None known (Please circle)
Do medicines need further clarification
Yes No
List collected by:
Plan Approved by:
Designation: Date Designation Date
Compliance aid Yes No Type of compliance aid
Community Pharmacy Name / Tel Any other information / Comments e.g. family member deals with medication issues, GP not aware of OTC usage, liquid medicines required