melanonychia striata and the evaluation of pigmented nail streaks
TRANSCRIPT
NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT | 191www.podiatrym.com
IntroductionThe goal of this CME is to present
an introduction to the examination ofpigmented nails streaks, which areoften overlooked and poorly under-stood in everyday clinical practice.These seemingly benign lesions can
present a difficult clinical challengebecause subungual melanoma mustalways be involved in the differentialdiagnosis, and quite often a biopsybecomes necessary to confirm whatthe lesion is. Similarities and differ-ences between melanonychia striata
and subungual melanoma will be ad-dressed and clues to the diagnosis ofsubungual melanoma are empha-sized. Important biopsy techniquesapplicable are considered and the in-dication for different surgical ap-
Continued on page 192
Continuing
Medical Education
Goalsand Objectives
1) Identify appropri-ate hallmarks for dis-tinguishing betweenbenign pigmented nailstreaks and subungualmalignant melanoma.
2) Understand thebenefits of performingaccurate surgical nailbiopsies in order to as-sist the pathologist inproperly identifyingmalignant melanoma.
3) Recognize thecauses and simulatorsof pigmented nailstreaks and how thenail apparatus can be atrap to both the patientand the clinician, andwhy proof of diagnosisis necessary.
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $22.00 per topic) or 2) per year, for the special rate of $169 (you save $51).You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. You can also takethis and other exams on the Internet at www.podiatrym.com/cme.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earnedcredits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake thetest at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 198. Other than those en-tities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be ac-ceptable by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best ef-forts to ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of thisprogram is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts bynoted authors and researchers. If you have any questions or comments about this program, you can write or call us at:Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (pg. 198).—Editor
MelanonychiaStriata
and the Evaluationof PigmentedNail Streaks
BY PETER VANNUCCHI, DPM
Biopsy is the keyto distinguishing between a benign
and a malignant condition.
CONTINUING MEDICAL EDUCATION
www.podiatrym.com
CME
NAIL STREAKS
192 | NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT
proaches is emphasized inorder to assist the histopathologist
in interpreting nail biopsy specimens.Melanonychia striata and longitudi-nal melanonychia are synonymousterms used in the literature and inmost reports, but for purposes ofthis article, melanonychia striata willbe used as more precise and lesscumbersome.
MelanonychiaStriata
Melanonychia striata is character-ized by a tan, brown, or black longi-tudinal streak within the nail plateand is a relatively uncommon occur-rence. Melanonychia striata resultsfrom increased melanin deposits inthe nail plate. There are many causesand simulators of melanonychia stria-ta, and it is often impossible to differ-entiate one another by history andclinical inspection alone. More impor-tantly, subungual malignantmelanoma must always beincluded in the differentialdiagnosis (Figure 1).
If the causes ofmelanonychia striata are notapparent, then biopsy isnecessary. However, thismaxim poses a dilemma. Inorder to get accurate nailbiopsy, tissue must be ex-cused that is both adequatefor diagnosis and represen-tative of the underlyingpathologic process. In orderto minimize the risk of post-operative nail dystrophy,enough matrix must be pre-served to permit regenera-tion of a nail plate that isfunctionally and cosmetical-ly acceptable. Above all, anaccurate interpretation ofthe biopsy specimen re-quires broad experience inthe evaluation of disordersof the nail unit and itsmelanocyte system by thehistopathologist.
The Nail Apparatusand Its MelanocyteSystem
The nail plate is derivedfrom the nail matrix, a spe-
cialized germinative epithelium thatlies beneath the proximal nail foldand cuticle. The proximal matrix pro-duces the superior (upper) portion ofthe nail plate; the distal matrix pro-duces the inferior (lower) portion of
the nail plate (Figure 2).Melanonychia striata originates in
the nail matrix and results from in-creased deposition of the melanin
from melanocytes which migrate dis-tally as they transform into nail platecorneocytes. The linear band of themelanized corneocytes is visible inthe nail plate.
Melanocytes are normal con-
stituents of the nail apparatus, mi-grate to the nail matrix and bed dur-ing embryonic development. Fortu-nately, the majority of these
melanocytes are located inthe distal portion of the nailmatrix, and because of theirgreater density and activity,pigmented streaks are morelikely to originate in the dis-tal matrix. This has very im-portant surgical implicationsbecause it means that if asurgical biopsy is performedon the distal portion of thematrix and it later forms adefect, that defect will ap-pear on the under-portion ofthe nail plate and not on thetop, and therefore the nailplate surface remains intact.
Sometimes, it is possibleto identify the origin (proxi-mal or distal matrix) of pig-mentation in melanonychiastriata by inspection of thedistal nail plate tip after clip-ping. It is the simplest butleast precise method and isgenerally not a reimbursableprocedure. By inspection,pigment localized in the tophalf of the nail plate indi-cates proximal matrix origin,and with a subsequent biop-sy a more likely nail defect.When the pigment is in the
Continued on page 193
Continuing
MedicalEducation
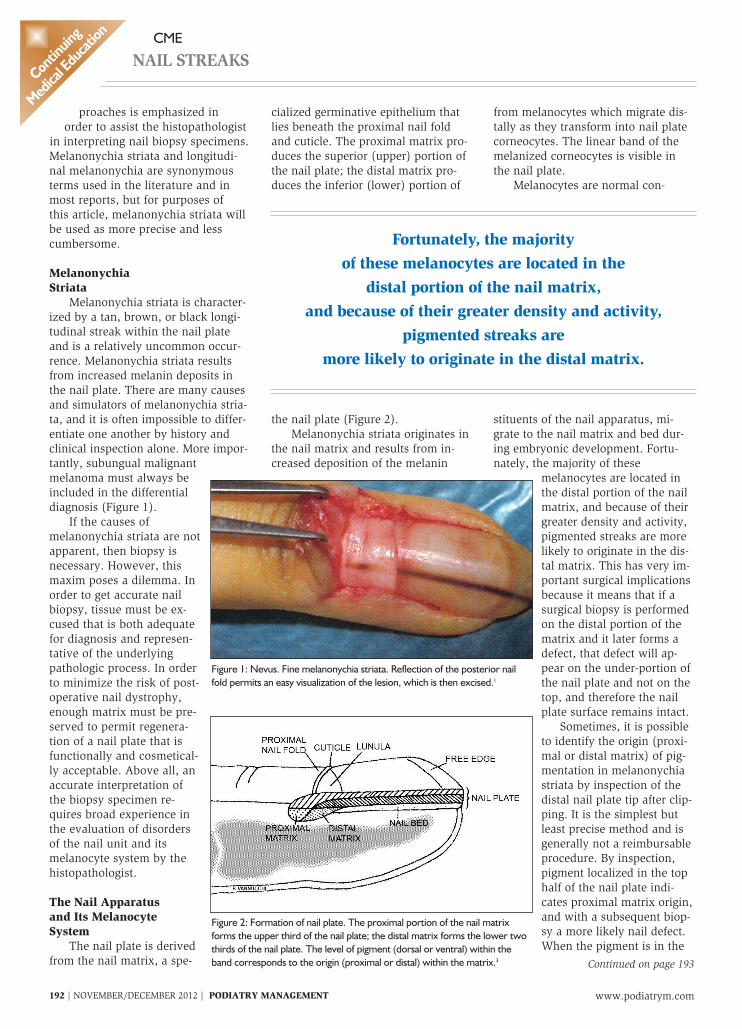
Figure 1: Nevus. Fine melanonychia striata. Reflection of the posterior nailfold permits an easy visualization of the lesion, which is then excised.1
Figure 2: Formation of nail plate. The proximal portion of the nail matrixforms the upper third of the nail plate; the distal matrix forms the lower twothirds of the nail plate. The level of pigment (dorsal or ventral) within theband corresponds to the origin (proximal or distal) within the matrix.3
Fortunately, the majorityof these melanocytes are located in the
distal portion of the nail matrix,and because of their greater density and activity,
pigmented streaks aremore likely to originate in the distal matrix.
NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT | 193www.podiatrym.com
CME
NAIL STREAKS
bottom half, post-operative dystrophyis less likely.
The level of pigment within theclipped nail specimen may be moreaccurately ascertained microscopi-cally with Fontana-Masson stainingof the nail clipping. This gives animportant clue to the pathologist asto precise origin of pigment produc-tion and to the appropriate surgical
procedure to be selected.4 But thesingle most important reason is todetermine whether there is a prima-ry melanoma present.
Distributionof Melanonychia Striata
Melanonychia striata occurs in77% of African-Americans morethan 20 years of age and in almost100% who are more than 50 yearsold. The thumbs and index fingersare common sites as well as thegreat toes. The more frequentlyused digits are subject to more trau-
ma and have a higher incidenceof melanonychia striata. Someauthors have linked trauma andfriction in both the causes ofmelanonychia striata and subun-gual melanoma.3,4,5 But to distin-guish the small numbers of pa-tients with subungual melanoma
from the larger group of patientswith non-specific melanonychiastriata is difficult. Both are alikein several ways. In the hand,each arises most often in thethumb, index fingers, or both.Melanonychia striata has beenreported to precede the onset of
subungual melanoma and may bean early sign. Both occur commonlyin dark pigmented people. By someestimates, 40% to 55% of subun-gual melanoma arise in the foot,and the majority occur in the greattoes. It is not known if it is becauseof trauma or because the greattoe offers a greater surface area.Approximately 3% of malignant
melanoma in Caucasians are subun-gual melanoma. Subungual melanomaoccurs mainly in older individualsover more than 50 years of age andappears with equal frequency in bothsexes.6
Clues to Diagnosing SubungualMelanoma
A thorough history and physicalexam can help distinguish the exoge-nous causes of a single band of sub-ungual melanoma. Common simula-tors include subungual hematomawhich usually migrates distally. For-
eign bodies, however, do notfollow this rule and require moreextensive evaluation.
Hutchinson’s SignHutchinson’s sign represents pig-
mentation of the nail fold either prox-imally or laterally and can be an im-
portant indicator for subungualmelanoma.7 But it is not pathog-nomonic.
Occasionally, pigmented nailstreaks that are dark brown simulatepigmentation of the overlying cuticleand proximal nail fold. This pigmen-tation is visible because of the cuticleand proximal nail fold’s transparency,and not because of melanin localiza-tion within the tissue. This so-calledpseudo-Hutchinson’s Sign can beidentified by careful inspection andgood lighting.
Other less prominent exceptionsmight include: periungual recurrenceof pigmentation after nail surgery orfor a nevus, and for malnutrition andminocycline therapy.
Periungual pigmentation and ex-tension, therefore, is a salient but notalways specific sign of subungualmelanoma, nor does the absence of aHutchinson’s sign mean that the le-sion is benign.
Other clues for the diagnosis ofsubungual melanoma are whenmelanonychia striata:
• Begin in a single digit during thesixth decade of life or after.
• Develop abruptly in a previous-ly normal nail plate.
• Become suddenly darker orwider.
• Occur in the thumb, index fin-ger, or great toe.
• Occur after digital trauma.• Occur in a single digit in a dark
pigmented patient, especially in thethumb or great toe.
• Demonstrate blurred, ratherContinued on page 194
Continuing
Medical Education
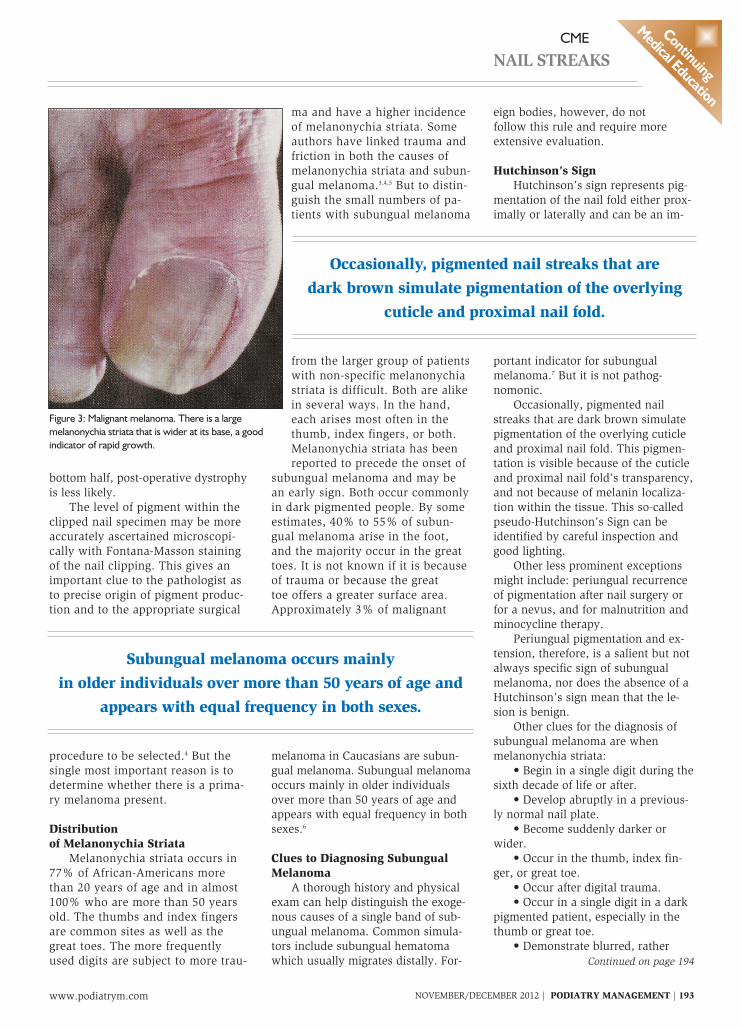
Figure 3: Malignant melanoma. There is a largemelanonychia striata that is wider at its base, a goodindicator of rapid growth.
Occasionally, pigmented nail streaks that aredark brown simulate pigmentation of the overlying
cuticle and proximal nail fold.
Subungual melanoma occurs mainlyin older individuals over more than 50 years of age and
appears with equal frequency in both sexes.
www.podiatrym.com
CME
NAIL STREAKS
194 | NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT
than sharp lateral borders.• Occur in a patient with a
history of malignant melanoma.
• Occur in a patient when the riskfor melanoma is increased (dysplasticnevus syndrome)8
• Are accompanied by nail dystro-phy such as partial nail destruction ordisappearances.
Some other important considera-tions include:
• Black bands may be importantconsideration in Caucasians for sub-ungual melanoma.
• However, in African-Americansjet-black bands are not unusual.
• Color variation and streakswithin streaks may suggest subun-gual melanoma, but they can be com-mon in multiple benign melanony-chia striata.
• Theoretically, wide bands sug-gest subungual melanoma, but thecritical width that signifies melanomahas never been established.
• Bands that do not extend all theway to the free end of the nail are un-likely to be melanomas because theydo not take their origin from the nailmatrix.
• Bands which are progressivelywider indicate rapid growth and are aconstant feature of subungualmelanoma (Figure 3).
• Multiple pigmented nail streaksare usually not neoplastic in origin.9
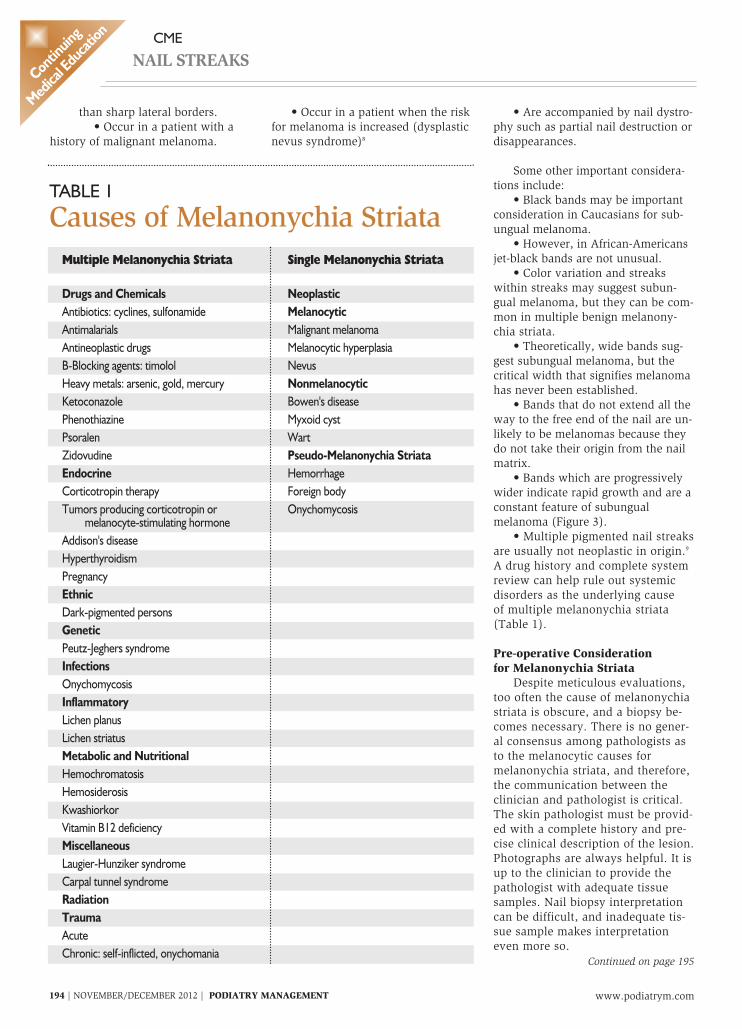
A drug history and complete systemreview can help rule out systemicdisorders as the underlying causeof multiple melanonychia striata(Table 1).
Pre-operative Considerationfor Melanonychia Striata
Despite meticulous evaluations,too often the cause of melanonychiastriata is obscure, and a biopsy be-comes necessary. There is no gener-al consensus among pathologists asto the melanocytic causes formelanonychia striata, and therefore,the communication between theclinician and pathologist is critical.The skin pathologist must be provid-ed with a complete history and pre-cise clinical description of the lesion.Photographs are always helpful. It isup to the clinician to provide thepathologist with adequate tissuesamples. Nail biopsy interpretationcan be difficult, and inadequate tis-sue sample makes interpretationeven more so.
Continued on page 195
Continuing
MedicalEducation
TABLE 1
Causes of Melanonychia StriataSingle Melanonychia Striata
NeoplasticMelanocyticMalignant melanomaMelanocytic hyperplasiaNevusNonmelanocyticBowen's diseaseMyxoid cystWartPseudo-Melanonychia StriataHemorrhageForeign bodyOnychomycosis
Multiple Melanonychia Striata
Drugs and ChemicalsAntibiotics: cyclines, sulfonamideAntimalarialsAntineoplastic drugsB-Blocking agents: timololHeavy metals: arsenic, gold, mercuryKetoconazolePhenothiazinePsoralenZidovudineEndocrineCorticotropin therapyTumors producing corticotropin or
melanocyte-stimulating hormoneAddison's diseaseHyperthyroidismPregnancyEthnicDark-pigmented personsGeneticPeutz-Jeghers syndromeInfectionsOnychomycosisInflammatoryLichen planusLichen striatusMetabolic and NutritionalHemochromatosisHemosiderosisKwashiorkorVitamin B12 deficiencyMiscellaneousLaugier-Hunziker syndromeCarpal tunnel syndromeRadiationTraumaAcuteChronic: self-inflicted, onychomania

NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT | 195www.podiatrym.com
CME
NAIL STREAKS
A biopsy has to be performed cor-rectly the first time; patients shouldnot be subjected to mutilating surgicalprocedures for a condition that mayprove totally benign. But at the sametime, the pathologist must be provid-ed with adequate tissue that repre-sents the disorder and adequate for
diagnosis in order to preclude post-operative recurrence.
No single biopsy method meetsthe needs of all patients. The follow-ing considerations may be helpful inselecting the appropriate biopsy pro-cedure.
• Post-operative nail dystrophy isless likely with distal matrix proce-dures than with proximal matrix biop-sies.
• Complete excision of melanony-chia striata with less cosmetic defor-mity when the band is located in thelateral third of the nail plate.
• When there is periungual spreadof pigmentation into the proximal andlateral nail folds, there is a greaterlikelihood of melanoma, and thereshould be less regard for cosmetic ap-pearance and more concern for com-plete lesion extirpation.
• Appearance and functional in-tegrity is less critical in the toes thanin the hands.
• Melanonychia striata is morelikely to represent subungualmelanoma in older patients and biop-sy should be performed more aggres-sively.
Biopsy MethodsAmong the many surgical proce-
dures for nail biopsies the one that isultimately selected will depend on:
• The likelihood of subungualmelanoma.
• Need to minimize risk of post-operative deformity.
• Location (medial or lateral) of
the pigmented nail streak within thenail plate.
• Band width and matrix origin(proximal or distal).
• Periungual pigmentation whenpresent with melanonychia striata thelikelihood of subungual melanoma isgreater.
Imaging studies, both x-raysand/or MRI’s, should be obtained,and the patient examined for lym-phadenopathy. All infected portionsof the nail apparatus (proximal andlateral nail folds, nail plate, nailbed, hyponychium and skin) are re-moved en bloc down to bone withrelative disregard for cosmetic ap-pearance to ensure complete biopsyand excision. The big advantage isthat the pathologist is able to studythe lesion in its entirety, render aprecise diagnosis, and draw salient
conclusions regarding prognosis.The conspicuous disadvantageis significant post-operativedeformity.
Lateral Portion of Nail PlateInvolvement
The preferred surgical techniqueis a lateral longitudinal biopsy whenmelanonychia striata involves pastthe lateral third of the nail plate. Thebig advantage is that all affected tis-sue of the nail apparatus are com-pletely removed, and the der-matopathologist can examine the le-sion in its entirety. Post-operatively,the patient is left with a narrowed
nail and a good to excellent cos-metic result.
Mid-portion of the Nail PlateInvolvement
When melanonychia striata liewithin the mid-portion of the nailplate, the chance for post-operativedystrophy is greater, and the selectionof optimal biopsy technique is moredifficult. It is important to establishpre-operatively the matrix origin(proximal or distal) of the streak. Be-cause the more proximal the origin,the greater the risk of nail dystrophy.As noted previously, the origin of thelongitudinal streak may sometimes bedetermined by clinical inspection ofthe nail plate tips or by microscopicexamination of Fontana-Massonstained clippings from the distal freeedge of the nail. But a more accuratemethod for establishing the origin ofthe pigmented streak is by makingsurgical relaxing incisions in the prox-imal nail fold and ascertaining theexact location by direct visualization(Figure 1)
These biopsies are best carriedout under ring block anesthesia atthe base of the digit. The biopsy isthen performed with a punch orscalpel. Punch defects smaller than
3mm in diameter need no suture.The punch is run through the softplate and matrix down to the bone,and the entire specimen is trans-ferred to the fixative. Care should betaken because the matrix tissue isvery friable. An antibiotic gauzedressing can then be applied.
Wide PlateNail Involvement
When a wide plate portion of thenail is pigmented, a large portion ofthe matrix would necessarily be in-volved. Under these circumstances,the underlying disease process is
The big advantage is thatthe pathologist is able to study the lesion
in its entirety, render a precise diagnosis, and drawsalient conclusions regarding prognosis.
Post-operatively,the patient is left with a narrowed nail and a good
to excellent cosmetic result.
Continued on page 196
Continuing
Medical Education

www.podiatrym.com
CME
NAIL STREAKS
196 | NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT
very serious. Depending on thecircumstances, partial longitudi-
nal biopsy, transverse elliptic exci-sion, or punch biopsies from select-ed areas of the matrix can be per-formed on the entire portion of thenail apparatus, and can be exerciseden bloc.
Malignant Melanoma of theNail Apparatus
Early diagnosis and surgical re-moval of the malignant melanoma ofthe nail and surrounding tissue isnecessary to improve currently poorsurvival rates. The initial assessmentstaging and follow-up are similar tothat for melanomas on other skinsites. Wide local incision of the le-sion is recommended. There are noclear surgical guidelines. For malig-nant melanoma in situ, complete ex-cision of the nail apparatus down tothe underlying bone is recommend-ed, followed by a full thickness skingraft. For invasive malignantmelanoma, amputation of the digit isrequired. There seems to be little
difference in survival between pa-tients treated with local proximal in-terphalangeal joint amputation com-pared to more proximal amputa-tions—provided that adequate exci-sion of the lesion is performed. Thelevel of amputation is chosen to ob-tain the best functional outcome.Therapeutic lymphadenopathy isadvised where there is clinical evi-dence of metastatic disease in re-gional lymph nodes.10 Thesemelanomas are known to metasta-size very rapidly to the brain andeye tissue.
Summaryand Conclusion
This article was written to helpthe clinician identify pigmented nail
streaks which are commonly seen andoften overlooked in everyday practice.These enigmatic benign lesions canpresent a difficult clinical challengebecause subungual melanoma mimicsmelanonychia striata, and biopsiesare often necessary to distinguish be-
tween the two. They should be per-formed for a single reason: to deter-mine whether there is a primarymelanoma.
If there is a pigmented longitudi-nal nail streak on a toe, then thesource of that streak is in the nail ma-trix, and that is where the biopsymust be performed. A biopsy doneanywhere else will result in no infor-mation that will help. The nail appa-ratus can be a trap for both the pa-
tient and the clinician, and proof ofdiagnosis is necessary. PM
Disclaimer: Any application of theinformation in this article in a profes-sional situation remains the profes-sional responsibility of the practition-er. The primary purpose of the author,Dr. Vannucchi is educational. Infor-mation presented and surgical tech-niques discussed are intended to in-form the reader about the knowledge,techniques, and experiences of the au-thor. A diversity of professional opin-ions may exist, and the views of theauthor are solely his own.
AcknowledgmentsMy appreciation is extended to
Patrick Vannucchi for editing and
preparation of this manuscript.
Endnotes1 Abimelel, P. Tumors of the nail Ma-
trix in Atlas of Hair and Nails. 1st. Ed Lon-don, Churchill Livingston. 2000. p. 145.
2 IBID p. 146
3 Norton, L.A. Incorporation of theThymidine-Mrthyl-H3 and glycine-2-H3 inthe nail Matrix and Bed of Humans. J In-vest Dermatol. 1971; 56: 61-68.
4 Baron, R. Surgery of the Nail. Derma-tol Clin. 1984; 2:271-284.
5 Kopy, A.W., Waldo, E. Melanony-chia Striata Australas. J. Dermatol. 1980;21:59-70.
6 Daly, J.M., Berlin, R., Urmacher, C.Subungual Melanoma: A 25 year review ofcases. J. Surg. Oncol. 1987; 35:107-112.
7 Mikhail, G.R. Hutchinson’s Sign. J.Dermatol Surg. Oncol. 1986; 12:519-521.
8 Clark Jr, W.C. The Dysplastic NevusSyndrome. Arch Dermatol. 1988; 124:207-210.
9 Leppard, B., Sanderson, R. V.,Behan, F. Subungual MalignantMelanoma. Difficult in Diagnosis. Br. MedJ. 1974; 31-32.
10 Abimelel, P. Tumors of the nail Ma-trix in Atlas of Hair and Nails. 1st. Ed Lon-don, Churchill Livingston. 2000. p. 147.
Additional ReadingBeaver, D. W., Brooks, S.E. The Nail
Colon Atlas of Clinical Diagnosis YearBook. Publishers Inc. Chicago
Pardo-Castello, V., Pardo, Osvaldo.Diseases of the Nails. Charles C Thomas.Springfield, IL 1960
Dr. Vannucchi re-ceived his professionaldegree from the NewYork College of Podi-atric Medicine, andcompleted his post-doc-toral studies at the Col-lege of Physicians andSurgeons of ColumbiaUniversity. He complet-
ed a surgical fellowship at Fairfield Hospital inShreveport, Louisiana. Dr. Vannucchi has beenin private practice in Corpus Christi, Texas,since 1972, as well as Dallas, Texas.
Continuing
MedicalEducation
The nail apparatuscan be a trap for both the patient and the clinician,
and proof of diagnosis is necessary
This article was writtento help the clinician identify pigmented nail streaks
which are commonly seenand often overlooked in everyday practice.
CME EXAMINATION
1) Which of the following state-ments regarding melanonychiastriata is correct?
A) Melanonychia striata ischaracterized by a tan, brown,or black longitudinal streakwithin the nail plate.B) There are many causes andsimulators of melanonychiaand it is often impossible todifferentiate one another sole-ly by history and clinical in-spection.C) If the causes of melanony-chia striata are not apparentthen biopsy is necessary torule out subungual malignantmelanoma.D) All of the above
2) Systemic disease(s) that cancause pigmented nail streaksinclude:
A) Addison’s DiseaseB) HypertensionC) Vitamin B12 DeficiencyD) All of the above
3) Which of the following is morelikely to produce a single digitmelanonychia striata rather thana multiple digit melanonychiastriata?
A) Malignant subungualmelanomaB) NevusC) Foreign BodyD) All of the above
4) Which of the following drugsdoes not cause multiple digitmelanonychia striata?
A) KetoconazoleB) Anti-malarialsC) RetinoidsD) Beta Blocking Agents
5) Which of the following is NOTa neoplastic cause for single bandmelanonychia striata?
A) OnychomycosisB) Metastatic MelanomaC) Basal Cell CarcinomaD) Verruca Vulgaris
6) Common non-neoplastic causes ofmelanonychia striata include:
A) PregnancyB) Subungual Foreign BodyC) Trauma and FrictionD) All of the above
7) Which of the following statementsregarding nail matrix is correct?
A) The nail plate is derived fromthe nail matrix which lies beneaththe proximal nail fold and cuticle.B) Melanonychia striata usually aris-es in the distal portion of the matrixand not the proximal portion.C) Both A and BD) Neither A or B
8) Melanonychia striata is morecommon in:
A) African-AmericansB) HispanicsC) CaucasiansD) Native Americans
9) In the foot subungual melanomaarises more commonly on the ______.
A) Great toeB) Second toeC) Third toeD) Fourth and fifth toe
10) Approximately what percentageof malignant melanomas are subun-gual in Caucasians?
A) 1%B) 3%C) 5%D) 10%
11) The median age at which subun-gual melanoma is diagnosed is_______.
A) 10 to 20 yearsB) 20 to 30 yearsC) 30 to 50 yearsD) More than 50 years
12) The male/female ratio of causesof subungual melanoma is approxi-mately_______.
A) 1 : 4B) 1 : 2C) 1 : 1D) 2 : 1
13) Of the following, the best stainfor melanoma pigment is the______.
A) S-100 immunoperoxidasestainB) Fontana-masson stainC) Methenamine stainD) Colloidal iron stain
14) Hutchinson's sign is ______.A) Pigment observed in periun-gual tissue.B) An important indicator ofsubungual melanoma but is notpathognomonic.C) Both A and BD) Neither A or B
15) When longitudinal nail streaksare dark brown and simulate pig-mentation of the overlying cuticleand proximal nail fold because ofthe skin's transparency, which ofthe following statements is correct?
A) The sign is referred to aspseudo-Hutchinson's signB) Periungual pigmentation issalient, but always specificC) Malnutrition and certaindrugs do not cause pigmentedbands and hyper-pigmentationD) After nail surgery for a be-nign nevus, periungual pig-mentation never occurs
16) When a nail biopsy is per-formed for melanonychia striatawhich of the following statementsis true?
A) Postoperative nail dystrophyis less likely with proximal ma-trix procedures than with distalmatrix biopsiesB) The entire source of the pig-ment production does not haveto be removedC) Biopsy should be performedmore aggressively in older pa-tients because the likelihoodfor subungual melanoma isgreaterD) Appearance and functionalintegrity is more important inthe toes than in the hands
Continued on page 198
SEE ANSWER SHEET ON PAGE 199.
NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT | 197www.podiatrym.com
Continuing
Medical Education
Continued on page <None>
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenient toenroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Manage-ment can be found on the Internet athttp://www.podiatrym.com/cme. Each lesson isapproved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of par-ticipation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may be earnedduring any 12-month period. You may select any 10in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instructionalmedia are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
Home Study CME credits nowaccepted in Pennsylvania
Continuing
MedicalEducation
CME EXAMINATION
www.podiatrym.com198 | NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT
17) Which of the following statements is correct?A) If you see a longitudinal pigmented nailstreak on the nail plate then the source of thatstreak is in the matrix and that is where youshould do your biopsyB) Excision of melanonychia striata is accom-plished more easily with less deformity whenthe streak is located on the lateral portion ofthe nail rather than on the middle portionC) Both A and BD) Neither A or B
18) Which of the following statements is correct?A) There are clear surgical guidelines for sub-ungual malignant melanomaB) Band width and matrix location eitherproximal or distal are important considera-tions for subungual biopsiesC) Periungual spread of pigmentation into theproximal or lateral skin folds is of no clinicalsignificanceD) Progressive widening of the pigmentedband in melanonychia striata is of no prognos-tic significance
19) Which of the following statements are impor-tant considerations for diagnosing subungualmelanoma?
A) Black bands area an important clue to sub-ungual melanoma in Caucasians but not inAfrican-AmericansB) Pigmented bands that do not extend to thefree end of the nailC) Pigmented bands demonstrate blurred,rather than sharp lateral bordersD) All of the above
20) Which of the following statements is correct?A) Early diagnosis and surgical removal of amalignant melanoma of the nail shows littleimportant survival ratesB) There are clear surgical guidelines for sub-ungual malignant melanomasC) Subungual malignant melanomas areknown to metastasize very rapidly to thebrain and eye tissueD) Periungual pigmentation along with darkblack bands of melanonychia striata in a Cau-casian patient over 50 years needs no x-raysor MRI’s because the cause is usually due totrauma.
See answer sheet on page 199.
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________ Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________ State_______________________ Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________ Soc. Sec.#______________________ Daytime Phone_____________________________
State License(s)___________________________ Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be chargedto your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $22.00 for each examsubmitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $169.00 (thus saving me $51 over the cost of 10 individualexam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must complete allinfo. on the front and back of this page and mail with your credit cardinformation to: Podiatry Management, P.O. Box 490, East Islip,NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or higher
on any examination will receive an official computer form stating thenumber of CE credits earned. This form should be safeguarded andmay be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will be noti-fied and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer form below.For each question, decide which choice is the best answer, and circlethe letter representing your choice.
(4) Complete all other information on the front and back of this page.(5) Choose one out of the 3 options for testgrading: mail-in, fax, or
phone. To select the type of service that best suits your needs,please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information and
mail with your credit card information to:
Podiatry ManagementP.O. Box 490, East Islip, NY 11730
PLEASEDONOTSENDWITH SIGNATURE REQUIRED, ASTHESEWILLNOTBEACCEPTED.
There is no charge for the mail-in service if you have already en-
ENROLLMENT FORM & ANSWER SHEET
� Continuing
Medical Education
rolled in the annual exam CPME program, and we receive this examduring your current enrollment period. If you are not enrolled, pleasesend $22.00 per exam, or $169 to cover all 10 exams (thus saving $51over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and fax
24 hours a day to 1-631-563-1907. Your CPME certificate will be datedand mailed within 48 hours. This service is available for $2.50 per examif you are currently enrolled in the annual 10-exam CPME program (andthis exam falls within your enrollment period), and can be charged toyour Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME program, thefee is $22 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free service.
Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Monday throughFriday. Your CPME certificate will be dated the same day you call andmailed within 48 hours. There is a $2.50 charge for this service if you arecurrently enrolled in the annual 10-exam CPME program (and this examfalls within your enrollment period), and this fee can be charged to yourVisa, Mastercard, American Express, or Discover. If you are not current-ly enrolled, the fee is $22 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information, pleasecontact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
Over, please NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT | 199www.podiatrym.com
�
ENROLLMENT FORM & ANSWER SHEET (continued)Continuing
MedicalEducation
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educationalobjectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
EXAM #9/12Melanonychia Striata and the
Evaluation of Pigmented Nail Streaks(Vannucchi)
www.podiatrym.com200 | NOVEMBER/DECEMBER 2012 | PODIATRY MANAGEMENT