meningitis & meningococcal annual report of hepatitis b...
TRANSCRIPT
Meningitis & Meningococcal
Disease
Yorkshire and the Humber Regional Epidemiology Unit
Annual Report 2012
Published: December 2012
Hepatitis B and C
Annual report of hepatitis B and C surveillance in Yorkshire and the
Humber 2012
Vir
al Immunisation
Acute
Transm
ission
Vaccine
Chronic
Blood Borne
Treatment


HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 1
Reader Information Box
Document Purpose For information
Title Yorkshire and the Humber Hepatitis B and C Annual Report; 2012
Publication Date
Publication PDF format only
Target Audience Primary Care Trusts (commissioning and public health), Health Protection Units, National Treatment Agency, Clinical Commissioning Groups, NHS Commissioning Board, Public Health Observatory, Drug Action Teams, Laboratories, Prison Healthcare, Hospital Trusts, drug services, Local Authority Crime and Disorder Reduction Partnerships, Local Authority Public Health, primary care providers and service users
Circulation List Yorkshire and the Humber Health Protection Units, National Treatment Agency, Directors of Public Health, Yorkshire and the Humber Microbiologists, members of the Regional Hepatitis B and C Steering Group, Chief Executives of Local Authorities, Public Health Observatory leads, NHS Commissioning Board and Clinical Commissioning Group leads
Description The report provides an overview to stakeholders about hepatitis B and C activity during 2011 to assist with service developments
Superseded Documents N/A
Contact Details Dr Autilia Newton Regional Hepatitis Lead Health Protection Agency Block 2 C/o The Food and Environment Research Agency Sand Hutton, York YO41 1LZ Email: [email protected] Dr Louise Coole/Madeline Cox Regional Epidemiology Health Protection Agency Yorkshire and the Humber 6th Floor South East Quarry House Quarry Hill Leeds LS2 7UE Email: [email protected]
Suggested Citation Hepatitis B and C Annual Report 2012 Health Protection Agency Yorkshire and the Humber
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 2
Authors and lead contributors Cathie Railton (nee Gillies), Project Manager – Hepatitis B and C, HPA Yorkshire and the Humber Dr Autilia Newton, Consultant in Communicable Disease Control and Regional Lead for Hepatitis, HPA Yorkshire and the Humber Madeline Cox, Information Manager, HPA Yorkshire and the Humber Regional Epidemiology Unit Dr Louise Coole, Regional Epidemiologist, HPA Yorkshire and the Humber Regional Epidemiology Unit Adrian Wensley, Epidemiology and Surveillance Manager, HPA Yorkshire and the Humber Regional Epidemiology Unit
Acknowledgements We would like to gratefully acknowledge the work of all those who contributed information on hepatitis B and C in Yorkshire and the Humber, including Drug Action Teams, Primary Care Trusts, drug services, hospitals, laboratories, service users, the National Treatment Agency, The Hepatitis C Trust and Sentinel Surveillance of Hepatitis Testing (HPA).
Data sources Hepatitis C in the UK, Health Protection Agency Annual report, 2012 Estimates of Hepatitis C Prevalence, Burden, Treatment and Cost by PCT: Modelling Tool (HPA website) National Treatment Agency National Drug Treatment Monitoring System Yorkshire and the Humber Hospital Trust’s Data
Labbase, Lab data from Yorkshire and the Humber NHS Laboratories
Sentinel Surveillance of Hepatitis Testing, 2011
HPZone, HPA case management system
Concateno and Manchester NHS Laboratories
Hospital treatment data (RHBCSG hospital data collection survey, 2012)

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 3
Acronyms used Anti-HBc Anti-hepatitis B core antibody
APPHG All-Party Parliamentary Hepatology Group
AT Area Team
BBV Blood Borne Virus
CCDC Consultant in Communicable Disease Control
CCG Clinical Commissioning Group
DAAT Drug and Alcohol Action Team
DAT Drug Action Team
DBST Dried blood spot test
DH Department of Health
GPwSI General Practitioner with Special Interest
GUM Genitourinary Medicine
HBsAG Hepatitis B surface antigen
HCV Hepatitis C virus
HMP Her Majesty’s Prison
HPA Health Protection Agency
HPU Health Protection Unit
ID Infectious disease
IDU Injecting drug user
Liver QuEST Liver Quality Enhancement Service Tool
MDT Multi disciplinary team
NHS National Health Service
NICE National Institute for Health and Clinical Excellence
NTA National Treatment Agency
NHS CB NHS Commissioning Board
PCR Polymerase chain reaction
PCT Primary Care Trust
PHE Public Health England
PHEC Public Health England Centre
PHO Public Health Observatory
PHPQI Prison Health Performance Quality Indicator
PIP Prison Infection Prevention
PWIDs People who inject drugs
RAPS Rapid Access Prescribing Service
RCGP Royal College of General Practitioners
RHBCSG Regional Hepatitis B and C Steering Group
SCG Specialist Commissioning Group
SCN Strategic Clinical Network
SHA Strategic Health Authority
SpR Specialist Registrar
WHO World Health Organisation

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 4
Contents
Authors and lead contributors ........................................................................................... 2
Acknowledgements ........................................................................................................... 2
Data sources...................................................................................................................... 2
Acronyms used .................................................................................................................. 3
Tables ............................................................................................................................... 6
Figures .............................................................................................................................. 7
Foreword .......................................................................................................................... 9
Executive summary ......................................................................................................... 10
Introduction .................................................................................................................... 11
1. National developments ................................................................................................ 12
1.1. NHS changes................................................................................................................... 12
1.2. National hepatitis B and C developments ..................................................................... 12
1.2.1. The Department of Health’s National Liver Strategy ............................................. 12
1.2.2. NHS Liver Care......................................................................................................... 13
1.2.3. National standards framework for liver disease .................................................... 13
1.2.4. National HPA reports .............................................................................................. 14
1.2.5. Royal College of General Practitioners (RCGP) ....................................................... 16
1.2.6. National Institute for Health and Clinical Excellence (NICE) .................................. 17
1.2.7. The Hepatitis C Trust ............................................................................................... 17
1.2.8. HCV Action .............................................................................................................. 18
1.2.9. Developments in other regions .............................................................................. 18
2. Regional developments ............................................................................................... 20
2.1. Regional Hepatitis B and C Steering Group (RHBCSG) ................................................... 20
2.1.1. Yorkshire and the Humber Quality Standards Framework for Hepatitis B and C, March 2012 ....................................................................................................................... 20
2.1.2. Yorkshire and the Humber Guidance on testing for hepatitis B and C (with reference to HIV), March 2012 ......................................................................................... 20
2.1.4. Training ................................................................................................................... 21
2.1.5. Yorkshire and the Humber Hepatitis Project Launch, 29 March 2012 ................... 21
2.2. West and East Yorkshire Hepatology Network .............................................................. 21
2.3. The development of a Yorkshire and the Humber Liver Network................................. 22
2.4. PCT Hepatitis Leads ........................................................................................................ 22
2.5. World Hepatitis Day, 28 July 2012 ................................................................................. 23
2.6. Area specific developments ........................................................................................... 26

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 5
3. Mapping of services ..................................................................................................... 31
3.1. Drug service testing practice ......................................................................................... 31
3.2. Hepatitis C treatment and support group provision ..................................................... 34
3.3. Hepatitis B treatment provision .................................................................................... 37
3.4 Local hepatitis action groups (strategic/planning groups) ............................................. 38
4. Epidemiology of hepatitis B and hepatitis C .................................................................. 39
Introduction .......................................................................................................................... 39
Sentinel Surveillance for hepatitis C ..................................................................................... 39
Overview of hepatitis B and C activity .................................................................................. 39
National laboratory data on hepatitis B and C ................................................................. 39
Treatment services for hepatitis B and C in Yorkshire and the Humber .......................... 41
Hepatitis C ............................................................................................................................. 44
Regional laboratory data for hepatitis C ........................................................................... 44
Hepatitis C Testing and positivity rates through the hepatitis C sentinel surveillance scheme for Yorkshire and the Humber PCTs .................................................................... 47
Demographics of hepatitis C in Yorkshire and the Humber ............................................. 48
Virology profile.................................................................................................................. 53
Hepatitis C testing through alternative providers and methodologies ............................ 54
National Treatment Agency data ...................................................................................... 57
Hepatitis B ............................................................................................................................. 60
Hepatitis B laboratory data ............................................................................................... 60
Sentinel Surveillance for hepatitis B ................................................................................. 63
Hepatitis B demography ................................................................................................... 65
Transmission risks ............................................................................................................. 70
Source of positive samples ............................................................................................... 71
4.1.1. ................................................................................................................................. 71
Antenatal screening .......................................................................................................... 72
5. Commissioning ............................................................................................................ 73
5.1. Future commissioning arrangements ............................................................................ 73
5.2. Estimates of the future burden of hepatitis C in Yorkshire and the Humber and the costs of treatment ................................................................................................................. 73
6. Conclusion and recommendations ............................................................................... 75
6.1. Conclusion ...................................................................................................................... 75
6.2. Recommendations for 2013 .......................................................................................... 75
7. References ................................................................................................................... 76
NICE Technology appraisal 253, Hepatitis C (genotype 1) – boceprevir, 2012 .................... 76
NICE Technology appraisal 252, Hepatitis C (genotype 1) - telaprevir, 2012 ....................... 76
Appendix 1: Yorkshire and the Humber Hepatitis Project Launch – Agenda ...................... 77

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 6
Tables
Table 1: Number of people commencing treatment for Hepatitis C in 2011 by local authority of treatment ....................................................................................................................................... 42
Table 2: Number, and rate with confidence intervals per 100,000 resident population of laboratory confirmed cases of hepatitis C, in the Yorkshire and the Humber region, 2011 ......... 44
Table 3: Number of individuals tested and testing positive for anti-HCV in the Yorkshire and the Humber by PCT through the sentinel scheme, 2011* ................................................................... 47
Table 4: Percentage positive of hepatitis C by age group and region, reported via sentinel surveillance, 2005 – 2011 (except South West*) .......................................................................... 48
Table 5: Number of individuals tested and testing positive for anti-HCV in the Yorkshire and the Humber by ethnicity, 2011 ............................................................................................................ 52
Table 6: Number of individuals tested and testing positive for anti-HCV, HCV PCR and/or HCV genotype in the Yorkshire and the Humber by PCT , 2011* .......................................................... 53
Table 7: Number of individuals tested and testing positive for anti-HCV by Concateno Plc† and Sentinel surveillance, 2005 - 2011 ................................................................................................. 55
Table 8: Percentage of individuals testing positive by oral fluid for anti-HCV by Drug Action Team and year, 2005 - 2011 .................................................................................................................... 55
Table 9: Number of individuals tested and testing positive by dried blood spot for anti-HCV per PCT, 2010 - 2011† .......................................................................................................................... 56
Table 10: Injecting status of adults in drug treatment .................................................................. 57
Table11: Hepatitis C test status of adults in drug treatment - injectors only................................ 57
Table 12: Hepatitis C intervention status for adults in drug treatment - injectors only ............... 58
Table 13: Hepatitis C intervention status at latest episode in drug treatment journey (i.e. all those in treatment in 2011) ........................................................................................................... 58
Table 14: Hepatitis C intervention status with test date between 01/01/2011 and 31/12/2011 (all test dates) and for latest test date (individual number) .......................................................... 58
Table 15: Number of cases of hepatitis B, acute and chronic, reported via Labbase, by primary care trust and year, for the Yorkshire and the Humber region, 2006 – 2011 ............................... 60
Table 16: Cases of hepatitis B reported via Labbase in 2011, by number, rate and confidence intervals, for the Yorkshire and the Humber region ...................................................................... 61
Table 17: Number of individuals tested and testing positive for HBsAg in the Yorkshire and the Humber by PCT (excluding antenatal screening), 2010* ............................................................... 63
Table 18: Number of chronic and acute cases of hepatitis B reported through HPZone, by HPU, PCT and quarter, 2011 ................................................................................................................... 64
Table 19: Number of chronic, acute and unspecified cases of hepatitis B reported through HPZone, by HPU and diagnosis, 2011 ............................................................................................ 64
Table 20 Age-group and gender of individuals tested and testing positive for HBsAg in Yorkshire and the Humber by PCT (excluding antenatal screening) 2011* .................................................. 67
Table 21: Number of individuals tested and testing positive for HBsAg in the Yorkshire and the Humber by ethnicity (excludes antenatal screening) 2011 ........................................................... 69
Table 22: Number of women booked for antenatal care in the Yorkshire and the Humber region by year and number of women, offered, declining, tested and testing positive for hepatitis B .. 72
Table 23: HPA estimates for numbers infected with hepatitis C and genotype distribution by local authority ................................................................................................................................ 74
Table 24: HPA estimates for future burden of hepatitis C by local authority ............................... 74

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 7
Figures
Figure 1: Rate per 100,000 resident population of cases of hepatitis C by year and by region, reported via NHS laboratories, 2006 -2011 ................................................................................... 40
Figure 2: Rate per 100,000 resident population of cases of hepatitis B by year and by region, reported via NHS laboratories, 2006 - 2011 .................................................................................. 40
Figure 3: Number of cases treated (includes patients commencing treatment in 2010) by hospital for hepatitis B and C, 2011 ............................................................................................... 41
Figure 4: Number of patients being treated for hepatitis C by genotype in the Yorkshire and Humber region, by provider 2011 ................................................................................................. 43
Figure 5: Number and rate per 100,000 resident population of laboratory confirmed cases of hepatitis C for the Yorkshire and the Humber region, by year, 2006 - 2011 ................................. 44
Figure 6: Laboratory confirmed hepatitis C in the Yorkshire and the Humber region by PCT of residence; number of cases, rates per 100,000 resident population with confidence intervals, 2011 ............................................................................................................................................... 45
Figure 7: Rates per 100,000 resident population of laboratory confirmed hepatitis C by PCT in the Yorkshire and the Humber region 2011 .................................................................................. 46
Figure 8: Number of individuals tested and testing positive for anti-HCV in 1 sentinel laboratory in the Yorkshire and the Humber (January 2005 - December 2011)* ........................................... 47
Figure 9: Gender distribution of laboratory confirmed hepatitis C for the Yorkshire and the Humber region, 2011 ..................................................................................................................... 48
Figure 10: Number of cases and rate per 100,000 resident population of hepatitis C by age group and PCT, Yorkshire and the Humber region, reported via Labbase 2011 ..................................... 49
Figure 11: Age group and gender of individuals testing positive for anti-HCV in the sentinel laboratory in the Yorkshire and the Humber (2005-2011) ............................................................ 50
Figure 12: Number of young adults tested and testing positive for anti-HCV in the sentinel laboratory in the Yorkshire and the Humber (2005-2011) ............................................................ 50
Figure 13: Percentage positivity of specimens for anti-HCV in the Yorkshire and the Humber by ethnicity (2005 - 2011)* ................................................................................................................. 51
Figure 14: Number of individuals tested and percent testing positive for anti-HCV in the Yorkshire and the Humber by ethnicity 2011* .............................................................................. 51
Figure 15: Ethnicity breakdown of individuals tested for anti-HCV in the Yorkshire and the Humber 2011* ............................................................................................................................... 52
Figure 16: Genotype distribution among sentinel survey specimens, 2011 ................................. 53
Figure 17: Number of individuals tested and testing positive by oral fluid for anti-HCV in Yorkshire and the Humber DATs by Year, 2005 - 2011.................................................................. 56
Figure 18: Number of cases and rate per 100,000 resident population of cases of hepatitis B, acute and chronic, reported via Labbase, by year, for the Yorkshire and the Humber region, 2006 – 2011............................................................................................................................................. 60
Figure 19: Cases of hepatitis B reported via Labbase in 2011 by number, rate and confidence intervals for the Yorkshire and the Humber region ....................................................................... 62
Figure 20: Rates per 100,000 resident population of laboratory confirmed hepatitis B by PCT in the Yorkshire and the Humber region 2011 .................................................................................. 62
Figure 21: Number of cases of hepatitis B reported via HPZone for the Yorkshire and the Humber region by diagnosis and quarter, 2011 .......................................................................................... 63

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 8
Figure 22: Gender breakdown of cases of acute and chronic hepatitis B reported via Labbase, 2011, for the Yorkshire and the Humber region ............................................................................ 65
Figure 23: Percentage breakdown of cases of hepatitis B reported via HPZone in the Yorkshire and the Humber region, by diagnosis and gender, 2011............................................................... 65
Figure 24: Cases of acute and chronic hepatitis B reported via Labbase by age group and rate per 100,000 resident population, 2011, for the Yorkshire and the Humber region ............................ 66
Figure 25: Number of cases of acute and chronic hepatitis B reported via HPZone in the Yorkshire and the Humber region by age group, 2011.................................................................. 66
Figure 26: Number of individuals tested and percent testing positive for HBsAg in the Yorkshire and the Humber by age group and PCT (excluding antenatal screening) 2011 ............................ 67
Figure 27: Percentage of cases of acute hepatitis B reported via HPZone by ethnic group, 2011 68
Figure 28: Ethnicity breakdown of Individuals tested for HBSAg in the Yorkshire and the Humber (excludes antenatal screening) 2011 ............................................................................................. 68
Figure 29: Ethnicity breakdown of individuals testing positive for HBsAg in the Yorkshire and Humber region (excludes antenatal screening) 2011 .................................................................... 69
Figure 30: Ethnicity breakdown of individuals tested and testing positive for HBsAg in the Yorkshire and Humber region (excluding antenatal screening), 2011 .......................................... 70
Figure 31: Breakdown of most likely route of transmission for acute hepatitis B cases reported via HPZone in the Yorkshire and the Humber region, 2011 .......................................................... 71
Figure 32: Percentage of individuals tested for HBsAg in the Yorkshire and the Humber by primary service type (excluding antenatal screening) 2011 .......................................................... 71
Figure 33: Number of women tested and testing positive for hepatitis B in the Yorkshire and the Humber region by year, 2001 - 2011 ............................................................................................. 72
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 9
Foreword I am pleased to provide a foreword for the 2012 Annual Report on Hepatitis B and C in Yorkshire and
the Humber. Each year we are able to provide more comprehensive information on hepatitis B and
C activity across the region through our well established Hepatitis B and C Steering Group. This year
we have published guidance developed by the group to support providers and commissioners which
was launched at the event in March 2012 at Leeds Town Hall. The event was successful in attracting
national experts to speak as well as engage a range of stakeholders to attend from across the region.
During the latter part of 2012, our attention has turned to the many changes within the NHS and the
emerging structures of Public Health England (PHE) and the NHS Commissioning Board (NHSCB). In
response to this, work is now taking place across our region to further develop our structures and
merge our Hepatitis B and C Steering Group with the West and East Yorkshire Hepatology Network
to develop a Yorkshire and the Humber Liver Network (more details about this are included in the
report). A strategic group addressing liver issues is more encompassing than our current structures,
however it is important to note that this will not deflect our attention away from viral hepatitis, this
will remain a key priority for the region.
Finally, at this time of organisational change for both the NHS and wider public health, we are
working hard to ensure momentum on the work done so far in the region is not lost during this
transition period. In that respect, we are fortunate that the future Centre for Public Health England
and the three Area Teams of the NHS Commissioning Board will share the same footprint as the
current Yorkshire and the Humber region and our three heath protection teams. In addition to the
structures being developed across our region, discussions have already started to take place with
our Northern counterparts in the North East and the North West to look at how we can work
together to address liver disease over the coming years.
Dr Stephen Morton Regional Director Health Protection Agency

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 10
Executive summary Since last year’s report ‘Hepatitis B and C: Annual report of hepatitis B and C surveillance in Yorkshire
and the Humber 2010/11’, there have been many developments which will affect the commissioning
of services for hepatitis B and C. The work of the Hepatitis B and C Steering Group has focussed on
how best to support stakeholders during this transitional period and has published a suite of
guidance documents for commissioners and providers of hepatitis B and C services.
Despite the many changes currently taking place both nationally and across our region, both
commissioners and providers have continued to work proactively in responding to hepatitis B and C.
For example, this year has seen the introduction in Leeds of a care pathway for prisoners being
released from prison into the community for hepatitis C treatment through a newly established
multi-disciplinary team (MDT), more areas have now started to introduce dried blood spot testing
(DBST) to enable more people to be tested and the HPA have continued to provide training to a
range of stakeholders to help raise awareness around blood borne viruses.
This 2012 report provides a detailed overview of service provision across all areas as well as an
analysis of the epidemiology of hepatitis B and C across Yorkshire and the Humber, and is intended
to help inform commissioning and service development.
NHS laboratory diagnoses of hepatitis C are now higher in Yorkshire and the Humber than any other
region with 1486 new diagnoses of current or past infection reported in 2011.There is variation
across the region with the highest numbers and rates observed in Leeds, Bradford and Doncaster
and Rotherham. In keeping with national epidemiology the highest burden is observed in males and
in those aged 25- 44 years of age. There are some indications from the sentinel surveys of a more
recent decrease in positivity rates in teenagers and young adults tested for hepatitis C. There is also
encouraging data on the coverage of hepatitis C testing in drugs service clients, important because
detection is critical to achieving the clinical management and control goals for this infection.
There were 660 new diagnoses of hepatitis B reported in Yorkshire and the Humber in 2011, which is
consistent with the levels of recent years. The highest rates are reported in Leeds, Doncaster, Hull,
Bradford and Kirklees. Diagnoses are most common among the 15- 44 age group. All regions outside
London are reporting similar rates of diagnosis. Of the reported cases in Yorkshire and the Humber
35 were known to be acute infections. Risk factors for transmission in these cases was most
frequently sexual exposure (heterosexual and MSM). The antenatal infection screening programme
for hepatitis B continues to work well and contributes to the detection of previously infected women
and the prevention of transmission of hepatitis B to newborns.
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 11
Introduction 2011-12 has been a year of transition towards major changes which will take place in the health
system from 01 April 2013. This will include the abolition of Primary Care Trusts (PCTs) and Strategic
Health Authorities (SHAs) and the transfer of many of their functions, including commissioning, to
local Clinical Commissioning Groups (CCGs), and the NHS Commissioning Board, nationally and
through its Regions and Area Teams. The Health Protection Agency, National Treatment Agency for
Substance Misuse and other public organisations including Public Health Observatories, will also be
abolished and their functions transferred to the new body Public Health England, and its Regions and
Centres. . All of these developments will result in changes in the commissioning of hepatitis B and C
nationally. This year’s report provides information on how the national health changes will affect the
commissioning and possibly delivery of hepatitis B and C services and also makes reference to the
work that is taking place both nationally and across the region which will support professionals
during this transitional period.
The report focuses on 2011 data from a number of sources but also details service developments
across Yorkshire and the Humber during 2011 and 2012 to date. Since the 2011 report there have
been many achievements across Yorkshire and the Humber in relation to hepatitis B and C including:
- The Regional Hepatitis B and C Steering Group has finalised the Quality Standards Framework and
Testing Guidance and also held an event in Leeds for stakeholders to raise awareness about the
work.
- In Leeds, a formal Multi-disciplinary Team has been introduced, made up of HMP Leeds, St James’s
Hospital and St Martin’s Healthcare to enable prisoners to be initiated on treatment for hepatitis C
in prison even when they are due for release before their treatment is due to end.
-In York, a hepatologist has been appointed, who previously worked in Leeds and has now submitted
a business case to the Board at York District Hospital regarding introducing hepatitis C treatment in-
house.
- North Lincolnshire services have successfully piloted and rolled out across all drug agencies dried
blood spot testing, which has resulted in an increase in referrals to the hepatitis C treatment service.
- There have also been new peer support groups established, for example in Kirklees HepCats, a
group for people with an interest in hepatitis C has been established and in Scunthorpe ‘C the
Difference’ has been introduced.
Whilst there have been many challenges for service providers and commissioners during 2011-12 it
is extremely positive that so much work has still taken place across the region to ensure that
patients affected by hepatitis B and C continue to receive good quality care and support. It is a credit
to the many professionals working in the field that they are able to continue to be proactive during
the national changes within the NHS and continue to improve the pathway for patients across
Yorkshire and the Humber.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 12
1. National developments
1.1. NHS changes Since writing last year’s regional report the national NHS changes have started to emerge. The key developments in relation to hepatitis B and C are that:
Public Health England will officially be introduced from 1 January 2013. Amongst other agencies, the Health Protection Agency (HPA), the National Treatment Agency (NTA) and Public Health Observatories (PHOs) will be abolished and their functions transferred to Public Health England;
Public Health England will have three main areas of work, namely health protection, health improvement and population health and knowledge and intelligence;
There will be 15 Public Health England local Centres in England. The current three Health Protection Unit (HPU) areas in Yorkshire and the Humber will become one centre (Yorkshire and the Humber), however the three current HPU offices will remain (South Yorkshire, North Yorkshire and the Humber and West Yorkshire);
The NHS CB will have 27 Area Teams, ten of which will lead on specialist areas;
PCT Directors of Public Health and current PCT public health functions will go into Local Authorities;
Each Local Authority will have a Health and Wellbeing Board which PHE can advise and influence;
Clinical Commissioning Groups will also be established with responsibility for commissioning services at local level.
1.2. National hepatitis B and C developments
1.2.1. The Department of Health’s National Liver Strategy
The Department of Health began developing England’s first National Liver Disease Strategy in 2010 in response to the rising incidence and burden of liver disease. The Office for National Statistics1 state that the most common causes of death are circulatory, cancer, respiratory and stroke but liver is fifth most common and is the only one that is rising. Various work is taking place nationally to address the burden of hepatitis B and C and ensure a more seamless approach in identifying, testing and treating people at risk of the diseases. It is hoped that the strategy will be published shortly.
1 http://www.ons.gov.uk/ons/dcp171778_239518.pdf

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 13
1.2.2. NHS Liver Care
NHS Liver Care2 has been created to provide a virtual working environment for professionals. It supports the work programme being led by Professor Martin Lombard, National Clinical Director for Liver Disease in England. The three main work streams are:
1. Service Configuration and Workforce 2. Pathways and System Levers 3. Optimising the Prevention Agenda
A new website3 was launched in 2012 as part of NHS Liver Care and includes information around liver disease. The organisation is also providing training for primary care around liver issues as well as supporting regions in the development of Liver Networks.
1.2.3. National standards framework for liver disease
A new standards framework for liver disease was launched in November 2012 with funding from NHS Liver Care. The standards have been developed as part of the Liver QuEST (quality enhancement service tool) project, which aims to support teams working in liver services. The standards are to be piloted by hepatology and gastroenterology services from November 2012 to March 2013 and then hopefully rolled out nationally thereafter. The pilot sites are as follows: Derriford Hospital, Plymouth Sheffield Teaching Hospitals Norfolk and Norwich University Hospitals NHS Trust Freeman Hospital, Newcastle Queen Elizabeth Hospital, Birmingham West Middlesex University Hospital NHS Hull CCG Gloucestershire Hospitals Foundation Trust Nottingham University Hospital County Durham and Darlington NHS Trust Royal Liverpool University Hospital A new website4 has also been set up to support the Liver QuEST system to support professionals to assess their progress in providing high quality liver care to patients. .
2 http://www.liver.nhs.uk/
3 http://www.livermatters.nhs.uk/
4 http://www.liverquest.org.uk/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 14
1.2.4. National HPA reports
Four key reports were released this year from the HPA. Each report is briefly described below. Hepatitis C in the UK report 20125 The 2012 report from the HPA explains that the most recent national estimates suggest that around 216,000 individuals are chronically infected with hepatitis C (HCV) in the UK with the most common genotypes being genotype 1 and genotype 3. Injecting drug use continues to be the most important risk factor for HCV infection in the UK and both hospital admissions and deaths from HCV-related end stage liver disease (ESLD) and hepatocellular carcinoma (HCC) are continuing to rise. In England, statistical modelling predicts that 15,840 individuals will be living with HCV-related cirrhosis or HCC in England in 2020 if left untreated. This year’s report lists eight public health recommendations which include the need for commissioners to consider expanding provision of treatment in non-traditional settings and also . CCGs and Local Authorities working together to ensure that patient pathways are in place so that infected individuals identified in drugs services can also access treatment services for hepatitis C.
National survey of hepatitis C services in prisons in England, July 20126
In partnership with Offender Health and the Department of Health’s National Liver Disease Strategy Team, the HPA’s Prison Infection Prevention (PIP) team carried out a national survey of hepatitis C services in prisons in England between September and November 2011. The key findings are detailed below.
National hepatitis C survey results
Total prisons surveyed 128
Number responded 110 86%
No. testing via DBST 11 10%
No. testing via venous blood 109 99%
No. testing via oral 2 2%
No. automatic PCR testing 44 40%
No. with written pathway in place 82 74%
No. treating via hospital outpatient 45 41%
No. treating via hospital in reach 59 54%
No. treating via prison doctor 22 20%
5 http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/HepatitisC/
6 http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/PrisonInfectionPreventionTeam/Guidelines/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 15
Of the 128 prisons in England that were invited to complete the survey, 110 responded (86%). The survey found that the overwhelming majority of prisons (109/110, 99%) use venous blood sampling for testing but 10% (11/110) also provide DBST. Only 40% (44/110) of blood samples are routinely
tested for polymerase chain reaction (PCR) if they have a positive antibody test result. 82/110 prisons (74%) of those surveyed have a written pathway in place to describe what happens following a positive hepatitis C result. Having a pathway in place is a requirement of the Prison Performance Quality Indicators (PHPQIs) and some of those that do not currently have a pathway are in the process of developing one. In terms of the service model for treatment, this varies considerably across England with 45/110 prisons (41%) referring prisoners to outpatient hospital appointments; 59/110 prisons (54%) have an in reach service provided by the local hospital and 22/110 (20%) of prisons providing treatment in house overseen by the prison doctor ((although it is not clear if this means that a prison doctor simply oversees treatment prescribed and/or provided elsewhere or whether they have a more directive role in the care of their patients). The vast majority of prisons 95/110 (86%) do provide follow up for prisoners being discharged into the community; however this may simply involve giving a letter to the prisoner to give to their GP on release. The HPA and Department of Health (DH) issued some good practice guidance in the survey and are now in the process auditing a sample of prisons based on this and other national guidance. A report is due out by April 2013. Sentinel surveillance of hepatitis testing in England7 The sentinel surveillance study of hepatitis testing in England began in 2002, and provides information on trends in testing, individual risk exposures and clinical symptoms, as a supplement to the routine surveillance of hepatitis A, B and C. The study collects information on hepatitis A, B and C testing carried out in participating sentinel centres regardless of test result and therefore can also be used to estimate prevalence in those individuals tested. A report is published every quarter detailing data from the 22 participating centres. The only laboratory that submits in Yorkshire and the Humber is Leeds. The quarterly report from the sentinel surveillance study of hepatitis testing in England for the period January to March 2012 shows that in Yorkshire and the Humber the number of individuals testing positive for hepatitis B surface antigen (HBsAg) (excluding antenatal screening) was 72/4,545 (1.6%) compared to 794/47,547 (1.7%) nationally. With regards to hepatitis C, the proportion of individuals testing positive for antibodies was the same in Yorkshire and the Humber 2.8% (113/3,992) as it was nationally (1,120 / 40,287).
7
http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/HepatitisSentinelTesting/GeneralInformation/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 16
Unlinked anonymous HIV and viral hepatitis monitoring among people who inject drugs: Update, July 20128 The unlinked anonymous HIV and viral hepatitis monitoring among people who inject drugs (PWIDs) is a voluntary unlinked anonymous survey which recruits injecting drug users through specialist agencies throughout England, Wales and Northern Ireland. People using these services that are either currently injecting drug users, or who have done so previously, are asked to take part in the survey by service staff. Those who agree to take part provide a biological specimen that is tested anonymously for HIV, hepatitis C and hepatitis B. Behavioural and limited demographic information is then collected through a brief anonymous subject-completed questionnaire linked to the specimen. The report shows that prevalence of antibodies to hepatitis C among the survey participants across England, Wales and Northern Ireland was 43% in 2011. Half of those with antibodies to hepatitis C remain unaware of their infection, even though four-fifths reported having been tested for it. The prevalence of anti-hepatitis B core antibody (anti-HBc) among the survey participants across England, Wales and Northern Ireland has declined since 2006. During the period 2001 to 2006 the anti-HBc prevalence fluctuated between 26% and 30%, before declining to 16% in 2011.
1.2.5. Royal College of General Practitioners (RCGP)
The RCGP has now introduced their Part Two Certificate in the Detection, Diagnosis and Management of Hepatitis B and C in Primary Care9. The training comprises of two parts:
Part one is a stand-alone e-module to enable a basic understanding of hepatitis B and C and contribute towards professional’s continuing professional development. Part One also includes a face-to-face training day which, completed together with the e-module, will form the components of the Part One Certificate;
Part Two consists of a face-to-face training day that will involve teaching of further knowledge and skills for clinicians seeking to provide an increased level of management for patients with hepatitis B and C.
The training is to be made available, not only to GPs working in primary care, but also to any professionals and patients with an interest in hepatitis B and C.
8 http://www.hpa.org.uk/hpr/infections/hiv_sti.htm#uam11 9 http://www.smmgp.org.uk/html/rcgp.php#Hepatitis

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 17
1.2.6. National Institute for Health and Clinical Excellence (NICE)
NICE published its guidance on hepatitis B and C - ways to promote and offer testing to people at risk of infection in December 2012. Stakeholders were invited to comment on the draft guidance in August 2012. The guidance provides recommendations for good practice, based on the best available evidence of effectiveness, including cost effectiveness. It is aimed at commissioners, managers and practitioners with public health as part of their remit working within the NHS, local authorities and the wider public, private, voluntary and community sectors. In April 2012 NICE also recommended that both Boceprevir10 and Telaprevir11 in combination with Peginterferon Alfa and Ribavirin should be available as options for the treatment of genotype 1 chronic hepatitis C in adults with compensated liver disease. Across Yorkshire and the Humber some hospitals have started to use the new treatments, however many are still waiting for approval from commissioners before they can commence patients on the ‘triple therapy’.
1.2.7. The Hepatitis C Trust
The Hepatitis C Trust12 is a national UK charity for hepatitis C. It was founded and is now led by people with personal experience of hepatitis C and almost all of their Board, staff and volunteers either have hepatitis C or have had it and cleared it after treatment. The charity provides a number of functions nationally from awareness raising and training to providing direct services for those affected by hepatitis C. 2011/12 has seen many developments by The Trust including: The hepatitis C testing van In November 2011 The Trust launched their ‘testing van’ which tours the country, targeting high risk and hard to reach groups. Before visiting areas they work with local services to publicise the visit and ensure that the right facilities and onward referral steps are in place. The van visited Yorkshire and the Humber during October and November 2012 where they arranged sessions in York, Grimsby, Scunthorpe and Goole. The new service has proved a useful intervention to existing testing provision and has helped raise awareness nationally around hepatitis C. Pharmacy DBST In 2010 The Trust launched a programme for hepatitis C and hepatitis B (and in some areas HIV) testing in pharmacies where they trained pharmacists to offer DBST in 17 PCTs nationally. The service has helped to increase awareness amongst professionals and those affected by hepatitis C, and has been successful in identifying more people with the virus. Across Yorkshire and the Humber areas that have taken part in the project include Barnsley, East Riding and Doncaster.
10
http://guidance.nice.org.uk/TA253
12
http://www.hepctrust.org.uk/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 18
Peer to peer education programme In order to dispel the many myths around hepatitis C and encourage more individuals to access testing and treatment, The Trust now have a peer educator in place who is available to visit services to talk to people affected by hepatitis C. The educator usually visits drug services but can also attend prisons and other services to help raise awareness.
1.2.8. HCV Action
HCV Action is a UK-wide network of health professionals with an interest in hepatitis C bringing together specialists from across the patient pathway including consultants, nurses, GPs, pharmaceutical industry representatives and people living with the virus. The group aims to improve the quality of care for hepatitis C including increased prevention, diagnosis and treatment by commissioning research, developing various guidance to support professionals as well as hosting a website13 containing a range of resources and ‘promising practice’ which can be shared nationally. In October 2012, HCV Action launched a hepatitis C commissioning toolkit14 to support CCGs and public health commissioners. It aims to support professionals in commissioning for a key outcome of the ‘Improving outcomes and supporting transparency: public health outcomes framework for England, 2013-2016’15: to reduce mortality in people under 75 years from liver disease. The toolkit will help local authorities to address the growing public health burden of hepatitis C. It will also help commissioning groups to tackle the virus through promoting early diagnosis, treatment and support for patients.
1.2.9. Developments in other regions
The changes in the NHS have led to many developments around hepatitis, namely the importance of moving towards ‘Liver Networks’ across Public Health England Centre areas. In addition to developments across this region (which are detailed in Section 3) two other areas are developing a Liver Network. Greater Manchester Greater Manchester held an initial meeting in September where Dr Martin Prince, Lead Hepatologist, Manchester Royal Infirmary invited key clinicians from each hospital. The meeting was multi-disciplinary and included Gastroenterologists, Hepatologists, an Infection Diseases Physician, Addiction Psychologist, a GP and NHS manager. The aim of the meeting was to discuss and agree strategic solutions and to ensure that that liver disease is highlighted as a priority for the new commissioning structures post April 2013.
13
http://www.hcvaction.org.uk/
14 http://www.hcvaction.org.uk/Commissioning/Commissioning+Toolkit/Commissioning+toolkit
15 www.dh.gov.uk/health/2012/01/public-health-outcomes/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 19
The group agreed the following:
That a Liver Network which covers the Greater Manchester footprint should be developed;
Meetings should take place three times a year.
There will be an educational role for the Network (linked to Specialist Registrar [SpR] training and peer support).
The Network will develop responses to the commissioning environment.
They will build links/membership with CCGs and public health.
They will develop relationships with commissioners.
Develop a support structure for the Network in terms of management/administration and a clinical lead.
Whilst they will initially focus on direct clinical care the aim is that as structures are formalised they will be able to inform commissioners.
The group also agreed that the Network will need to:
Be a repository for local guidelines.
Identify guideline priorities.
Develop referral guidance for out-patients /specialist care.
Carry out an audit of alcohol services. Following the initial meeting an event was held in October 2012 which was attended by a range of clinicians and commissioners to discuss the Network with a wider audience. The conclusion to the day was that stakeholders support the development of a Greater Manchester Liver Network and that further work should be done to develop this and encourage more stakeholders to become engaged.
Another key development in Greater Manchester this year has been the publishing of the ‘Burden of Liver Disease and Inequalities in the North West of England16’ by the HPA. In October 2011, a multi-agency meeting for public health and intelligence staff (who will form part of PHE) was held. The meeting included representation from the HPA, North West PHP, the NTA, North West Cancer Intelligence Service and DH North West. They decided to carry out a collaborative piece of work to identify synergies across public health intelligence systems and liver disease was the chosen topic.
North East In December 2012 the North East held an event to establish a Liver Network and to address work
priorities for the next commissioning cycle. The Network will support work being led by the DH policy team and aim to:
Reduce variation in care.
Standardise liver care across the North East and Cumbria.
Develop pathways to ensure that excellent care is achieved.
Regions across the North have much work to do in establishing Liver Networks. However, discussions have taken place between the North East, Yorkshire and the Humber and Greater Manchester to look at better integrating the new structures to ensure that best practice can be shared.
16
http://www.hpa.org.uk/web/HPAweb&Page&HPAwebAutoListNameDesc/Page/1158945065208
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 20
2. Regional developments
2.1. Regional Hepatitis B and C Steering Group. Since its formal establishment in April 2010 the regional steering group has managed to achieve a number of goals. These include the development of the following:
2.1.1. Yorkshire and the Humber Quality Standards Framework for Hepatitis B and C, March 2012
The document provides a quality standards framework for hepatitis B and C for commissioners and providers to use when commissioning and/or delivering a new or existing service. It is divided into eight different sections and is intended to be used as stakeholders see fit in different areas, for example some areas may want to measure themselves against all eight standards; however other areas may want to just focus on one or two. The eight sections are as follows:
Strategic Planning and Partnerships.
Local Authorities.
Workforce.
Public Health.
NHS Commissioning.
Service Providers.
Offender Health.
Monitoring and Data Collection.
2.1.2. Yorkshire and the Humber Guidance on testing for hepatitis B and C (with reference to HIV), March 2012
In response to requests from stakeholders across the region the regional steering group developed this document to provide guidance for commissioners and providers on testing for hepatitis B and C.
2.1.3. Yorkshire and the Humber hepatitis project website17
The HPA now host a page on the website for the Yorkshire and Humber Hepatitis Project. It provides basic information about the work. Unfortunately the page does not include the guidance documents listed above and this is something that will need addressing during the transition to Public Health England.
17
http://www.hpa.org.uk/AboutTheHPA/WhatTheHealthProtectionAgencyDoes/LocalServices/YorkshireHumber
/Services/yorksHepatitisProject/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 21
2.1.4. Training
A number of training events led by the HPA for professionals working with individuals affected by hepatitis B and C have taken place during 2011-12. Events have varied from immunisation training for nurses to generic blood borne virus training for a range of professionals. Training has taken place in Hull, North Lincolnshire, North East Lincolnshire, York, North Yorkshire, Kirklees and Rotherham.
2.1.5. Yorkshire and the Humber Hepatitis Project Launch, 29 March 2012
The regional steering group arranged an event on 29 March 2012 for commissioners, planners and providers of hepatitis B and C services. The aims of the day were to:
Provide key stakeholders with guidance and support around the commissioning and provision of quality hepatitis B and C services.
Provide delegates with the opportunity to network and build links to share good practice.
Inform delegates about national and regional developments.
National experts presented at the conference including Professor Martin Lombard, National Clinical Director for Liver Disease, DH. Regional experts also presented on the day (agenda included as appendix) including a representative from the Grimsby Hepatitis C Support Group which was very well received. The event was oversubscribed with 88 people applying to attend the event. 65 attended the launch on the day in addition to 20 presenters, workshop facilitators and support staff. From the 36 evaluations received after the event: 1/36 (3%) rated the event as average 1/36 (3%) rated the event as good 19/36 (52%) rated the event as very good 14/36 (39%) rated the event as excellent 1/36 (3%) gave no comment The event achieved its aim which was to raise awareness amongst professionals and circulate the guidance documents produced by the regional steering group.
2.2. West and East Yorkshire Hepatology Network Links have been established with the West and East Yorkshire Hepatology Network which is chaired by Dr Rebecca Jones, Consultant, Leeds Teaching Hospitals NHS Trust. The Network includes representatives from across Yorkshire and the Humber with the exception of South Yorkshire, North Lincolnshire and North East Lincolnshire. The Network has now appointed a part time project manager to support their work. Achievements of the group so far include the development of the regional ‘Hepatitis C Guidelines and Treatment Protocols’ for use by hospital consultants and nurses and the Symposium on Liver Disease for General Practice Event which took place on 9 December 2011 in Leeds.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 22
2.3. The development of a Yorkshire and the Humber Liver Network In the publication ‘The Way Forward, Strategic Clinical Networks18’, the NHSCB announced that Strategic Clinical Networks should be developed based on the following conditions:
Cancer
Cardiovascular disease (incorporating cardiac, stroke, diabetes and renal
disease)
Maternity and children;
Mental health, dementia and neurological conditions
Whilst networks for the liver are not to be commissioned centrally at this present time, stakeholders across the region have agreed that there is still a need to introduce a formal ‘network’ across Yorkshire and the Humber whereby a range of stakeholders should be brought together to identify priorities and agree a work programme. This group will be made up of both clinicians and commissioners (as well as relevant others) and it is likely that the functions of the West and East Yorkshire Hepatology Network and the regional steering group will merge to create a more encompassing Yorkshire and the Humber Liver Network. It is hoped that by early 2013 the Terms of Reference for the new Network will be finalised and a work plan initiated to bring all work around the three key areas of the National Liver Strategy together.
2.4. PCT Hepatitis Leads As personnel has changed since the 2011 report, some hepatitis leads across PCTs have changed. The lead is responsible for acting as the link between regional strategic work and local delivery. However from April 2013 when PCTs are abolished the leads across Local Authority areas will have to be reviewed. As it currently stands the leads are as follows:
Barnsley: Dr Sharon Stoltz, Consultant in Public Health, NHS Barnsley
Bradford and Airedale: Dr Andrew O'Shaughnessy, Consultant in Public Health, NHS Bradford and Airedale
Calderdale: Gill Manojlovic, Head of Infection Prevention & Control, NHS Calderdale
Doncaster: Dr Rupert Suckling, Deputy Director of Public Health, NHS Doncaster
East Yorkshire: Dr Tim Allison, Director of Public Health, NHS East Yorkshire
Hull: Peter Dawson, Public Health Manager, NHS Hull
Kirklees: Jane O'Donnell, Deputy Director of Infection Control, NHS Kirklees
Leeds: Dr Simon Balmer, Consultant in Public Health, NHS Leeds
North East Lincolnshire: Mike Hardy, Project Development Manager, NHS North East Lincolnshire
North Lincolnshire: Natasha Philips, Commissioning Manager, NHS North Lincolnshire
18 www.commissioningboard.nhs.uk/files/2012/07/way-forward-scn.pdf

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 23
North Yorkshire and York:
Dr Martin Hawkings, Consultant in Public Health, NHS North Yorkshire and York
Rotherham: Kathy Wakefield, Nurse Consultant for Health Protection, NHS Rotherham
Sheffield: Dr Jeremy Wight, Director of Public Health, NHS Sheffield
Wakefield: Jeremy Mitchell, Commissioning Manager, NHS Wakefield
2.5. World Hepatitis Day, 28 July 2012
Last year’s regional report included details about the many activities that took place to mark World Hepatitis Day. This year there was also a range of activities organised by hospitals, drug services and commissioners.
Barnsley The local drug service and blood borne virus (BBV) support workers arranged a promotional stand in Barnsley town centre and offered advice and information along with promotional gifts to help raise awareness and reduce stigma around hepatitis C. They also worked with the hospital nurses to help raise awareness in the drug service. BBV screening and hepatitis A and B vaccinations were available throughout the day and volunteers were available to offer one to one support.
Bradford and Airedale The Physical Health Nursing Team arranged displays in all ten drug and alcohol services across Bradford and Keighley. This included information on where people can get tested, pre and post test information and referral into specialist services. BBV testing by mouth swab or blood samples were offered as well as vaccinations for hepatitis B and A at all services in the week leading up to World Hepatitis Day. Staff and volunteers at the alcohol services were also offered hepatitis awareness sessions.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 24
Doncaster Various awareness raising activities took place as well as a press release by Rotherham Doncaster and South Humber NHS Foundation Trust. Kirklees In addition to the usual testing offered at Lifeline drug services, the newly established local hepatitis C support group ‘HepCats’ arranged a ‘wheel of fortune’ quiz at both the Huddersfield and Dewsbury sites. There was also an article about hepatitis in the local papers to raise awareness and posters and leaflets were circulated to GP surgeries, pharmacies and other service providers. North East Lincolnshire In Grimsby there was a promotional stand in the Freshney Place Shopping Centre. Local professionals arranged a quiz, disseminated leaflets and gave away ‘gifts’ such as trolley tokens, pens, balloons and wrist bands. There was also a collection box for the local hepatitis C support group. Pelham Medical Centre developed a poster for the corridors to raise awareness around hepatitis in addition to putting it on their Facebook page. North Lincolnshire Scunthorpe ‘C the difference’ support group made themselves available in the town centre and arranged a quiz, circulated leaflets and gave away ‘gifts’ such as trolley tokens, pens, balloons and wrist bands.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 25
North Yorkshire Compass, Selby Staff, service users and volunteers from Compass Selby and its ‘Natural Highs’ service user group managed to do a three day climb of Scafell Pike between 27 - 29 July to mark World Hepatitis Day.
HARCAS, Hambleton and Richmondshire A poster presentation was held at the local drug service HARCAS and The Hub area at The Friarage Hospital Northallerton to promote World Hepatitis Day.
CODA, Craven This year CODA combined World Hepatitis Day with their second Craven Recovery Day. An event was held at a Greatwood Community Centre which featured lots of fun activities for families such as face painting, bouncy castle, stalls and local celebrities including Minnie Mouse, Fireman Sam, ‘The man with a pan on his head’ and Craven District Council’s Mayor. CODA staff were available throughout the day to provide advice and information about hepatitis.
Sheffield Two articles were published to mark World Hepatitis Day. One article (of a two part series) titled ‘Part 1: Detection and assessment of hepatitis C’ was written by Ray Poll, Nurse Consultant for the Journal of Practice Nursing and another article was written by Fran Rayner, Specialist Nurse for Viral Hepatitis for Independent Nurse.
Wakefield A newsletter to raise awareness about hepatitis was circulated to community centres, schools and voluntary services. The Well Being Nursing Team promoted testing at vaccinations at HMP New Hall and are also working in partnership with Turning Point to develop a hepatitis C support group in the community which will include education and advice on treatment and harm reduction.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 26
2.6. Area specific developments Barnsley A community clinic at Addaction has been in place since the start of 2012 at the harm reduction service whereby all new referrals from the team to the secondary care hospital provider receive their first appointment at the drug service. This has enabled more patients to engage in the first stages of treatment as the transition between diagnosis and treatment has been better supported. The success of this intervention is to be rolled out to outlying areas, including Penistone, Goldthorpe and Thurnscoe in an attempt to increase patients accessing treatment.
Addaction are also in the process of rolling out a BBV Peer Support Programme. Service users have been identified to be trained as peer educators and to deliver screening. It is envisaged that, as this project progresses, testing and treatment take up will increase. The peer educators will also be involved in awareness raising activities (e.g World Hepatitis Day) and will support the development of support groups.
Funded by the DAAT, the pharmacy pilot in Barnsley started in February 2011 and initially ran for six months. The service is specifically for people in drug and alcohol treatment services who visit the pharmacy as part of their drug treatment programme. They can access testing for hepatitis C at the pharmacies after which the client is asked to make an appointment (2-3 weeks later) to discuss their results. If they test positive for hepatitis C a referral for treatment is sent to the Specialist Unit at Barnsley Hospital. Six pharmacies were involved in the pharmacy pilot, although only three of the pharmacies carried out any testing (this was due to low uptake from service users). After the six month pilot the DAAT continued to fund the service as the pharmacies had surplus testing equipment, however it is planned to stop the provision at the end of March 2013 as only one pharmacy has carried out any tests since and these have been minimal.
During 2011:
17 individuals were tested of which 4 were found to be positive;
Of the 4 positive, 2 were genotype 1; 1 genotype 2; the other person’s genotype was not confirmed;
3 out of the 4 individuals attended a follow up appointment.
Bradford and Airedale The Primary Healthcare Nursing Team now see all substance misuse clients at entry into substance misuse services via the two new ‘Fresh Start Hubs’ where the clients have a comprehensive physical health assessment and BBV testing and vaccinations are offered. This has allowed the nurses to ensure they can focus their time accordingly between new assessments and the need to re test existing clients.
Doncaster NHS Doncaster staff have provided training on hepatitis awareness to local GPs, drug services, prisons, probation and the Drug Intervention Programme team. A twelve month pharmacy testing pilot in the community also started in March 2012 whereby ten pharmacies have been recruited (some are needle exchanges and some provide supervised consumption only) to trial testing for hepatitis C in a pharmacy setting.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 27
East Yorkshire The Hepatology and Infectious Diseases departments at Hull and East Yorkshire Hospitals Trust have obtained approval from the Drugs and Therapeutics Committee for the use of triple therapy with protease inhibitors for patients with genotype 1. The consultants are actively involved in several trials of the new treatments available, and a number of patients have agreed to take part in these. There is now a FibroScan available at the hepatitis clinic to enable staging of patients with viral hepatitis as an alternative to liver biopsy and the hepatitis clinic also has the benefit of an alcohol liaison nurse who can offer immediate assessment and signposting to treatment and support services.
The in house hepatitis C database, ‘C Thru’ is currently recording much of the Trust’s activities for hepatitis C patients and will assist in monitoring treatment outcomes for patients. Both specialist nurses attend regional and national hepatitis network meetings where best practice can be disseminated and shared.
Hull St Martin’s Healthcare were commissioned to start delivering the new community drug service J2R in July 2011. Since then an action plan has been implemented to increase vaccination and BBV testing in Hull and two clinicians have become trainers for the Part 1 of the new RCGP Certificate in the Detection, Diagnosis and Management of Hepatitis B and C in Primary Care. One of these clinicians is also a tutor for the Part 2 Certificate. A Part 1 face to face training day was held on 2nd May 2012 and another one is planned for October 2012.
A client induction programme has been developed within the service to increase take up of a comprehensive healthcare assessment which includes screening and vaccination for hepatitis. One of the hospital nurses is now also providing a weekly nurse led clinic at the service to increase uptake for treatment.
The Hospital Trust covering Hull is the same one as East Yorkshire and the developments noted above under ‘East Yorkshire’ are also relevant to Hull.
Kirklees HepCats is a new self help support group for people with an interest in hepatitis C which has been developed in Kirklees. They held a launch earlier in 2012 to help raise awareness amongst professionals and people affected by hepatitis C and make them aware of the new service on offer.
Hepatitis training has also been carried out by the HPA to the local drugs service provider and HIV service provider.
Leeds The community hepatitis C treatment pilot began in early 2012 at St Martin’s Healthcare Rapid Access Prescribing Service (RAPS) to allow handover of patients prior to release from HMP Leeds and HMP Wealstun. Monthly MDT meetings are held at St James’s Hospital under the clinical supervision Dr Mark Aldersley, Consultant Hepatologist. In addition to hospital representation, there is also representation from HMP Leeds, RAPS and any relevant others. Whilst this service has initially been introduced to continue hepatitis C treatment started in HMP Leeds or Wealstun, the plan is that the drug service will start to initiate treatment for hepatitis C amongst their community patients. Currently the capacity at the drug service is for a total of 6 patients to be on treatment at any one time.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 28
Additional work has been initiated around examining the needs of affected hep C communities in terms of peer and other social support structures. Leeds currently has two hepatitis C peer support groups, one aimed at the homeless and the other aimed at injecting drug users. Work is underway to identify best practice around the further development of such groups and also to identify suitable sources of funding or support, in order for effective work to continue.
A hepatitis B nurse has recently been appointed by St James’s hospital in an effort to improve the continuity of care and ensure uninterrupted supply of hepatitis B treatment. Nurse led clinics have now started for hepatitis B patients and there are plans in place to introduce homecare delivery of medications. Additional work has been started involving exploring the cultural and social reasons why members of certain ethnic minority groups do not present for testing or vaccination for hepatitis B. In partnership with the West and East Yorkshire Hepatology Network, new GP referral guidelines are being developed for hepatitis B and C which includes a more streamlined patient pathway. Furthermore, joint hospital MDT meetings have been taking place with the infectious disease team and there is a plan to introduce joint viral hepatitis clinics towards the end of 2012 which will include haematology and genitourinary medicine (GUM) colleagues.
North East Lincolnshire Efforts have been made to increase testing across North East Lincolnshire and following a dried blood spot testing pilot at The Junction there are now plans to roll this out to all drug services. Also, the hepatitis C nurse from the local hospital carried out testing on site at Birkwood Medical Centre for those patients who have difficult venous access.
The Grimsby hepatitis C support group continues to provide advice and support to people locally who are affected by hepatitis C. Two of the founding members have been pro active in helping to raise awareness both locally and nationally and attended and presented at the Yorkshire and Humber Hepatitis Project event in Leeds in March 2012.
At Addaction BBV screening and hepatitis B immunisations are now offered to all clients. All testing is carried out through venous blood sampling and there is a good pathway in place for referrals to the local hospital for positive results. The local support group and specialist nurse also regularly attend client group sessions to help raise awareness about hepatitis.
North Lincolnshire Dried blood spot testing has been successfully piloted and rolled out across all drug services and has resulted in an increase in referrals to the hepatitis C treatment service. Also, at the end of 2011 the Scunthorpe hepatitis C support group ‘C the Difference’ was formed. The group was initially started by four individuals who had undergone treatment for hepatitis C and wanted to help support other patients through treatment. They have visited various organisations locally to increase awareness about hepatitis C treatment and also offer support to anyone undergoing treatment.
North Yorkshire Contingency management for the completion of hepatitis B vaccinations is now in place at CRI Harrogate Compass Selby and CODA. Compass Selby also provide this to clients for undertaking hepatitis C testing.
At CRI, Harrogate there is now an increase in testing capacity due to the introduction of dried blood spot testing. This has in turn, increased the number of clients been tested for hepatitis. All staff

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 29
offering pre and post test discussion are given regular training to ensure they are offering the most up to date advice. For those clients who test positive and would like to access treatment, a direct referral is made to St James’s Hospital, Leeds. In terms of vaccinations if clients do not attend for appointments the nurse and key worker will assertively outreach the client to encourage attendance. Outreach vaccination appointments are also provided for clients who are not able to attend the service. Rotherham The Viral Hepatitis Steering Group which includes representation from the PCT, CCG, DAT, hospital and public health is still in place. They have developed a shared care pathway for GP practices that have high referral rates for hepatitis B patients. A local support group is also in the process of being developed by the DAT.
Sheffield There have been many developments in the hospital this year, for example Professor Mike McKendrick retired in February and Dr Ben Stone was appointed as a new consultant Physician with a remit to lead on hepatitis for the Department of Infection and Tropical Medicine at the Royal Hallamshire Hospital. A trainee undertaking part 2 of the RCGP certificate in hepatitis undertook a placement in Sheffield and has successfully completed the course. Also, the hepatitis team has recently started some work with the Trust service development team using a Microsystems approach developed by the Dartmouth Academy in the USA to make changes that could improve accessibility for patients.
As a stakeholder Sheffield Teaching Hospitals Foundation Trust contributed to the consultation on the new NICE guidance for the testing and diagnosis of hepatitis B and C. Sheffield is also one of approximately 20 centres across the country enrolling patients onto the new national HCV UK study. Recruitment started in April and will cease in April 2014. As well as patients attending clinics, discharged patients (i.e. those who achieved SVR or naturally cleared) are invited to participate with anonymised demographic and clinical details put onto a database. Blood samples are taken and stored in Biobank. This will then be used as a resource for people to apply and do further research.
For the last few years Dr Alicia Vedio (Speciality Physician) and Fran Rayner (Specialist Nurse) have offered screening for hepatitis in ethnic minority populations. This has culminated in identifying persons with infection and engaging them into further clinical care where needed. In the last year a website has been developed to raise awareness about hepatitis among the public and staff. The website provides clear and simple information using short videos and is available in other languages. It can be accessed at http://hitsheffield.org/
Diagnostic service for blood borne virus testing (HBsAg, antiHBc, anti-HCV and anti-HIV) on dried blood spots was launched by the Sheffield virology service in September 2012. Oral fluid test (OFT) is available for anti-HIV only, HBV and HCV screening on OFT has been evaluated and it is hoped that this method for screening will also be available in near future.
Ray Poll (Nurse Consultant) was invited by Professor Martin Lombard to contribute to the development of standards for liver services (as detailed in 2.2.3 ‘National standards framework for liver disease’). Sheffield is one of the pilot sites for the initial evaluation of these standards and will be completed by April 2013.
Finally, the drugs harm reduction service is increasing access to testing for clients who are in drug treatment. Previously clients were only tested at the beginning of their treatment journey (as per

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 30
NTA targets); however they are now trying to test on a two yearly basis. An audit of these results shows that around 25% of clients have become hepatitis C positive since starting drug treatment.
York A new Consultant Hepatologist has been recruited to work at York District Hospital. The Consultant previously worked at St James’s, Leeds and is working with hospital management to develop an in house service to ensure that patients in York, Selby and Harrogate can access treatment for hepatitis C locally.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 31
3. Mapping of services
3.1. Drug service testing practice
PCT area
Oral (Y/N)
PCR tests following positive oral result
DBST (Y/N) Venous blood (Y/N)
Automatic testing for PCR if antibody positive? (Y/N)
Direct referral from drug service to hepatitis treatment provider? (Y/N)
Barnsley
Addaction
Yes Usually refer directly to hospital consultant for PCR bloods, however occasionally test for PCR prior to referral
To pilot shortly All staff now trained in harm reduction team to deliver DBST
Yes No Yes
Bradford and Airedale
Substance Misuse service (Fountains Hall – BDCT)
Yes PCRs and genotyping done by Physical Health Team Nurses
Finger prick test Yes Yes - samples are sent to Leeds laboratory
Yes plus hospital outreach clinic
Bridge Project Yes As above As above Yes As above Yes
Project 6 Yes As above As above Yes As above Yes
Bradford Community Drug and Alcohol Service
Yes As above As above Yes As above Yes
Airedale Community Drug and Alcohol Service
Yes As above As above Yes As above Yes
North Bradford Drugs Service (Eccleshill and Shipley)
Yes As above As above Yes As above Yes
Working Women’s Project (BDCT)
Yes As above As above Yes As above Yes
Lifeline Piccadilly Project Yes As above As above Yes As above Yes
DRR/DIP (DISC and s2f)
Yes As above As above Yes As above Yes
Kensington Street Health Centre (Dr Wilson and partners)
No N/A No Yes As above Yes

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 32
Calderdale
Substance Misuse Service
Yes Sent from Calderdale Hospital Foundation Trust to Leeds
No Yes Yes Yes
Doncaster
The Garage & Shared Care No Bloods for PCR taken at The Garage
No Yes (and capillary blood)
Yes Yes
Streetreach No Bloods for PCR taken at Streetreach
No Yes (and capillary blood)
Yes Yes
East Yorkshire
East Riding Partnership No N/A Yes No Yes Yes
DIP Team No N/A Yes (for substitute prescribed patients only)
No Yes Yes
Criminal Justice No N/A Yes No Yes Yes
Hull
Compass – Direct Access and Harm Reduction service
No N/A Yes No No Yes
CRI DIP N/A N/A N/A N/A N/A No – managed via CORS community Prescribing Service
DISC/ST Martin’s Healthcare J2R
No In house – venous blood sampling
No Yes Yes – one stage procedure for venous blood now in place
Yes plus hospital outreach clinic
Compass Clinic Hull
No N/A Yes No Yes Yes via the specialist Hepatitis Nurse who also performs the PCR
Kirklees
Lifeline Kirklees Yes DBS – Concateno
Yes Yes No - oral for antibody test and DBST for PCR
Yes
Leeds
St Martin’s Health Care Services
Yes Yes in house – venous blood sampling
No Yes Yes - also piloting capillary blood sampling for those with difficult venous access
Yes
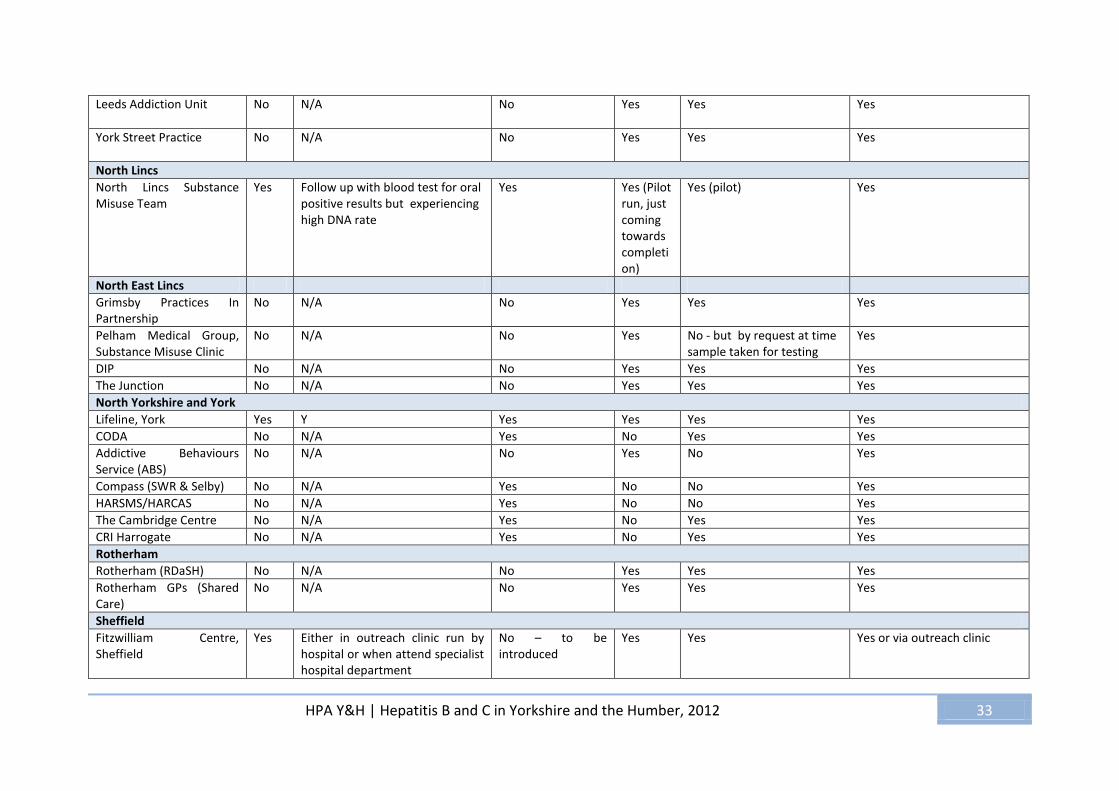
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 33
Leeds Addiction Unit No N/A No Yes Yes
Yes
York Street Practice No N/A No Yes Yes Yes
North Lincs
North Lincs Substance Misuse Team
Yes Follow up with blood test for oral positive results but experiencing high DNA rate
Yes Yes (Pilot run, just coming towards completion)
Yes (pilot) Yes
North East Lincs
Grimsby Practices In Partnership
No N/A No Yes Yes Yes
Pelham Medical Group, Substance Misuse Clinic
No N/A No Yes No - but by request at time sample taken for testing
Yes
DIP No N/A No Yes Yes Yes
The Junction No N/A No Yes Yes Yes
North Yorkshire and York
Lifeline, York Yes Y Yes Yes Yes Yes
CODA No N/A Yes No Yes Yes
Addictive Behaviours Service (ABS)
No N/A No Yes No Yes
Compass (SWR & Selby) No N/A Yes No No Yes
HARSMS/HARCAS No N/A Yes No No Yes
The Cambridge Centre No N/A Yes No Yes Yes
CRI Harrogate No N/A Yes No Yes Yes
Rotherham
Rotherham (RDaSH) No N/A No Yes Yes Yes
Rotherham GPs (Shared Care)
No N/A No Yes Yes Yes
Sheffield
Fitzwilliam Centre, Sheffield
Yes Either in outreach clinic run by hospital or when attend specialist hospital department
No – to be introduced
Yes Yes Yes or via outreach clinic

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 34
Guernsey House, Sheffield
Yes As above As above Yes As above As above
Wakefield
Spectrum Community Health CIC
Yes All positive antibodies are tested for HCV PCR by the well being nurses at Spectrum
No Yes Yes Yes
Turning Point (testing carried out by Spectrum nurses)
Yes All positive antibodies are tested for HCV PCR by the well being nurses at Spectrum
No Yes Yes Yes
3.2. Hepatitis C treatment and support group provision
AREA HOSPITAL TREATMENT COMMUNITY TREATMENT* PRISON PRISON(S) PROVIDING TREATMENT?
SUPPORT GROUP
Barnsley Yes - Barnsley Hospital Foundation Trust, Gastroenterology
Pending Due to success of joint working in new patient community clinic at John St a patient has now been identified to provide a pilot for community treatment
No N/A Yes to be developed through BBV peer educators who are currently being trained
Bradford & Airedale
Yes - Airedale General Hospital (Airedale Foundation NHS Trust) and Bradford Royal Infirmary (Bradford Teaching Hospitals NHS Foundation Trust)
No - Airedale Yes - Substance Misuse Service, Fountains Hall (service’s clients only)
No N/A No, but there is a quarterly information/support meeting at the Bridge Project
Calderdale Yes Calderdale Royal Hospital (nurse also covers South Kirklees)
Yes x 1 at health centre (part of hospital)
No N/A No
Doncaster Yes Doncaster & Bassetlaw Hospital
No – developments planned Moorland open and closed HMP Doncaster/ Marshgate HMP Lindholme
Yes – nurse in reach is provided in all prisons
Yes

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 35
East Yorkshire
Hull and East Yorkshire Hospitals NHS Trust - ID & Hepatology
Yes – drug services HMP Everthorpe HMP The Wolds HMP Full Sutton
Yes – consultant and nurse sessions
No
Hull Yes Hull and East Yorkshire Hospitals NHS Trust - ID & Hepatology (nurse also covers Scarborough, Whitby and Ryedale and East Riding)
Yes – drug services and recently introduced weekly in reach service at DISC
HMP Hull Yes Monthly nurse and consultant visits
No
Kirklees Yes* - Huddersfield Royal Infirmary Patients in Huddersfield (South Kirklees) are referred to HRI for treatment/patients in Dewsbury (North Kirklees) are referred to Leeds for treatment * Nurse also covers Calderdale
No No N/A Yes
Leeds Yes Leeds Teaching Hospitals
Yes – drug services (St Martin’s) started to treat in primary care through MDT from 2012 – continuing prison treatments but also plans to commence treatment
HMP Leeds HMP Wealstun HMP/YOI Wetherby
Yes Through prison based GP (not been needed at Wetherby as yet)
Yes x 2
York St Medical Practice;
Multiple Choice
North East Lincs
Yes Scunthorpe General Hospital (new Gastroenterologist in post)
No No N/A No
North Lincs Yes Scunthorpe General Hospital (new Gastroenterologist in post)
No No N/A No
NYY Out of area
Scarborough – Hull Royal Infirmary
Hambleton and Richmondshire - Friarage Hospital, Northallerton and St James Cook, Middlesbrough
Craven – Airedale General Hospital
York, Selby & Harrogate- Leeds Teaching Hospitals
Yes – health centre, Scarborough Yes – hospital, Northallerton No No
HMP Northallerton HMP Askham Grange
No - assessed and prescribed treatment through local hospital. Patients attend hospital outpatient clinic usually monthly for monitoring.
No
Rotherham Yes Rotherham NHS Foundation Trust
No No N/A Peer mentoring now in place

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 36
Sheffield Yes - Royal Hallamshire Hospital No but plans in early stages Yes via in reach Hospital based support provided to Doncaster prisons for Sheffield residents
Yes through the hospital
Wakefield Out of area Leeds Teaching Hospitals
Yes Spectrum Community Health CIC Well Being Nursing Team in the community with support from St James’ specialist nursing team
HMP Wakefield HMP New Hall (adults) HMP New Hall (juveniles)
Yes – HMP New Hall (adults) Prisoners seen as St James for the assessment, then prison healthcare oversee the treatment management, under hospital supervision.
No but in the process of setting one up. However buddying service in place where service users can talk to people who have undergone hepatitis treatment.
* Community provision is mainly through drug treatment services

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 37
3.3. Hepatitis B treatment provision
Area Hospital Treatment
Barnsley Yes – first referral has been made to and actioned by Barnsley Hospital recently
Bradford & Airedale
Yes x 2 Airedale General Hospital Bradford Hospital Trust
Calderdale Yes Calderdale Royal Hospital (nurse also covers South Kirklees)
Doncaster Yes - Doncaster & Bassetlaw Hospital
East Riding Yes - Hull and East Yorkshire Hospitals NHS Trust
Hull Yes - Hull and East Yorkshire Hospitals NHS Trust
Kirklees Yes - Huddersfield Royal Infirmary (South Kirklees) and St James’s, Leeds (North Kirklees)
Leeds Yes St James’s Hospital
North East Lincs Yes - Diana Princess of Wales, Grimsby
North Lincs Yes - Scunthorpe General Hospital, Scunthorpe
NYY Out of area Scarborough – Hull and East Yorkshire Hospitals NHS Trust H&R – Friarage Hospital Northallerton and St James Cook, Middlesbrough Craven – Airedale General Hospital York, Selby and Harrogate - Leeds Teaching Hospitals
Rotherham Yes - Rotherham NHS Foundation Trust. Patients may also choose to go to Sheffield
Sheffield Yes - Royal Hallamshire Hospital
Wakefield Out of area - Leeds Teaching Hospitals

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 38
3.4 Local hepatitis action groups (strategic/planning groups)
Area Local group Lead agency
Barnsley Yes x 2 Hospital led group – operational DAAT Harm Reduction Group – strategic Also, Lifeline are planning to put an operational group in place regarding work of BBV peer educators to feed into strategic meetings above
Bradford & Airedale
Yes Dr Moreea, Consultant, Bradford Royal Infirmary
Calderdale Yes Substance Misuse Service
Doncaster Yes DAT Harm Reduction Strategy Group
East Riding Yes DAT Treatment Group
Hull Yes DAT Treatment Forum
Kirklees Yes DAAT Harm Reduction Group
Leeds Yes x 2 Public Health focussing on prison and community treatment DAT Harm Reduction Strategy Group
North East Lincs Yes PCT
North Lincs Yes PCT
North Yorkshire and York
Yes x 2 County Substance Misuse Forum BBV Provider Group
Rotherham Yes PCT (includes hepatitis B and hospital representation)
Sheffield Yes (also monthly Clinical Hepatitis MDT meeting)
DAAT
Wakefield Yes DAT Harm Reduction Group

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 39
4. Epidemiology of hepatitis B and hepatitis C
Introduction This report includes data from a range of sources and whilst none of these will, in isolation, provide a complete record of all hepatitis B and hepatitis C infections; together they do provide a representative picture of the burden of these diseases and the trends in their epidemiology. Throughout this section the caveats around specific data sources that need to be considered in any interpretation of the data will be highlighted. A consequence of the various data sources in use is the risk of disagreement between figures which therefore need to be interpreted in the context of the datasets from which they are derived. The biggest challenge in reporting the epidemiology of hepatitis, especially for hepatitis C, is the incomplete nature of available intelligence due to the pool of undiagnosed infection.
Sentinel Surveillance for hepatitis C In 2002, the Sentinel Surveillance of Hepatitis Testing Study was set up to enhance routine surveillance of hepatitis C. It collects data on laboratory test results and demographic data for all individuals tested for hepatitis C antibody in 24 sentinel laboratories in England, covering approximately one third of the population.4 Limitations of the data include some duplication of individual patients and exclusion of dried blood spot, oral fluid, reference testing, and testing from hospitals referring all samples which do not have the original location identified. Individuals aged less than one year, in whom positive tests may reflect the presence of passively-acquired maternal antibody rather than true infection, are excluded. All data are provisional. There are two actively participating centres in Yorkshire and Humber, Leeds and Grimsby. Together they provide estimated population coverage of 20-39%. Whilst the data is not comprehensive for the whole region, it provides a helpful demographic and epidemiological profile of hepatitis C in the region.
Overview of hepatitis B and C activity National laboratory data on hepatitis B and C
A regional comparison of national laboratory data shows that the rate of hepatitis C diagnosed in NHS laboratories in Yorkshire and the Humber is the highest in the country. However, there may also be differential use of alternative diagnostic methods and non-NHS laboratories across different regions which will especially affect the hepatitis C data. Equivalent data for hepatitis B show the particularly high rate of hepatitis B in London, with Yorkshire and the Humber comparable to other regions outside of London with rates appearing to have plateaued over the last few years.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 40
Figure 1: Rate per 100,000 resident population of cases of hepatitis C by year and by region, reported via NHS laboratories, 2006 -2011
Figure 2: Rate per 100,000 resident population of cases of hepatitis B by year and by region, reported via NHS laboratories, 2006 - 2011
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
2006 2007 2008 2009 2010 2011
East Midlands
East of England
London
North East
North West
South East
South West
West Midlands
Yorkshire andHumberside
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
2006 2007 2008 2009 2010 2011
East Midlands
East of England
London
North East
North West
South East
South West
West Midlands
Yorkshire andHumberside
Source: Labbase – NHS Laboratory data
Source: Labbase – NHS Laboratory data

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 41
Treatment services for hepatitis B and C in Yorkshire and the Humber
During 2011, a survey was undertaken by the regional steering group with the acute trusts in Yorkshire and the Humber to explore where treatment services were in place and what outcomes had been achieved. Data quality and completeness varies between provider trusts but overall the results provide a useful window on hepatitis C and hepatitis B treatment services in Yorkshire and the Humber.
Numbers actually referred into the hospital, for assessment and consideration for treatment, have not been reported by all trusts. Of those who have reported this, some trusts report a relatively small number of pre-filtered referrals whilst others report two or three hundred referrals sometimes including PCR negative individuals. Figure 3 shows numbers treated by hospital in Yorkshire and the Humber during 2011. This data also includes those treated in both the community and prison.
Figure 3: Number of cases treated (includes patients commencing treatment in 2010) by hospital for hepatitis B and C, 2011
0 50 100 150 200 250
Airedale General Hospital
Barnsley Hospital Foundation Trust
Bradford Royal Infirmary
Calderdale Royal Hospital
Doncaster & Bassetlaw Hospital
Hull and East Yorkshire Hospitals
Huddersfield Royal Infirmary
Leeds Teaching Hospitals
St James Cook, Middlesbrough
Diana Princess of Wales Hospital, Grimsby
Scunthorpe General Hospital
Rotherham NHS Foundation Trust
Royal Hallamshire Hospital, Sheffield
Number of cases
Pro
vid
er
Hepatitis C Hepatitis B
Source: Hospital treatment data (RHBCSG hospital data collection survey, 2012)
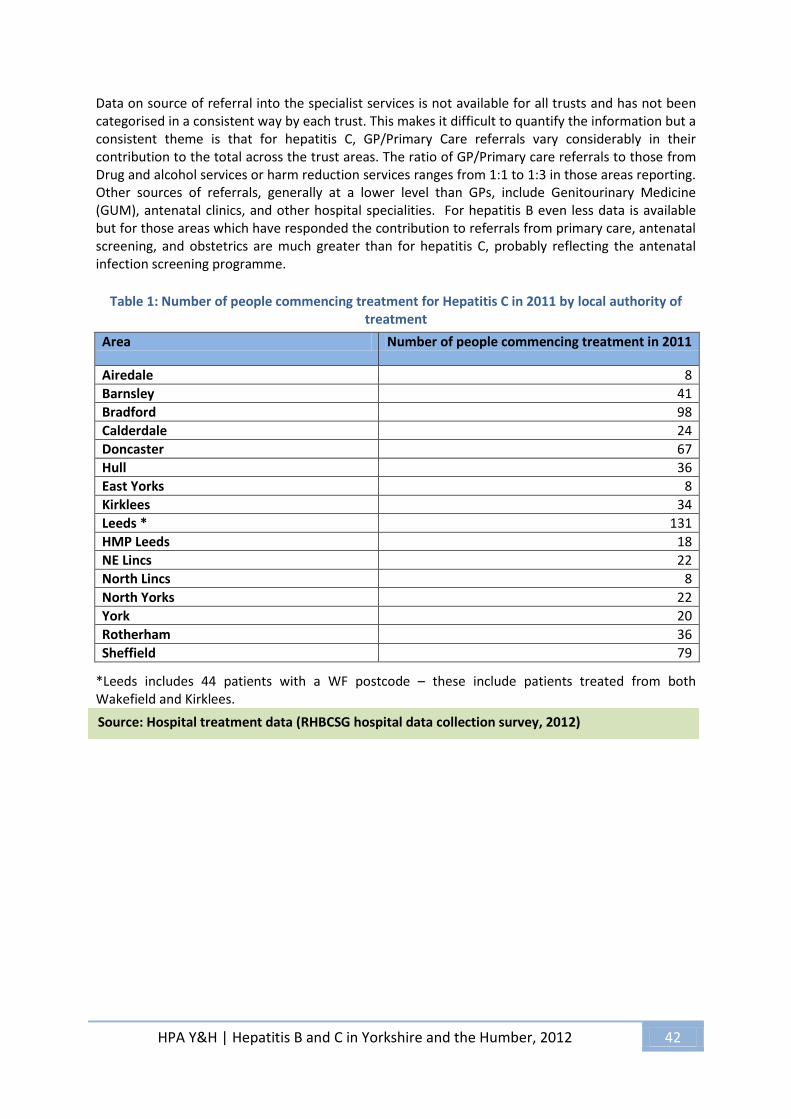
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 42
Data on source of referral into the specialist services is not available for all trusts and has not been categorised in a consistent way by each trust. This makes it difficult to quantify the information but a consistent theme is that for hepatitis C, GP/Primary Care referrals vary considerably in their contribution to the total across the trust areas. The ratio of GP/Primary care referrals to those from Drug and alcohol services or harm reduction services ranges from 1:1 to 1:3 in those areas reporting. Other sources of referrals, generally at a lower level than GPs, include Genitourinary Medicine (GUM), antenatal clinics, and other hospital specialities. For hepatitis B even less data is available but for those areas which have responded the contribution to referrals from primary care, antenatal screening, and obstetrics are much greater than for hepatitis C, probably reflecting the antenatal infection screening programme.
Table 1: Number of people commencing treatment for Hepatitis C in 2011 by local authority of
treatment
Area Number of people commencing treatment in 2011
Airedale 8 Barnsley 41 Bradford 98 Calderdale 24 Doncaster 67 Hull 36 East Yorks 8 Kirklees 34 Leeds * 131 HMP Leeds 18 NE Lincs 22 North Lincs 8 North Yorks 22 York 20 Rotherham 36 Sheffield 79
*Leeds includes 44 patients with a WF postcode – these include patients treated from both Wakefield and Kirklees.
Source: Hospital treatment data (RHBCSG hospital data collection survey, 2012)

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 43
Figure 4: Number of patients being treated for hepatitis C by genotype in the Yorkshire and Humber region, by provider 2011
0
50
100
150
200
250
Air
ed
ale
Gen
eral
Ho
spit
al
Bar
nsl
ey H
osp
ital
Fo
un
dat
ion
Tru
st
Bra
dfo
rd R
oya
l In
firm
ary
Cal
de
rdal
e R
oya
l Ho
spit
al
Do
nca
ster
& B
asse
tlaw
Ho
spit
al
East
Yo
rksh
ire
Co
mm
un
ity,
Ho
spit
al a
nd
Pri
son
Hu
ll, C
om
mu
nit
y, H
osp
ital
an
dP
riso
n
No
rth
Yo
rksh
ire
Co
mm
un
ity
Hu
dd
ers
fiel
d R
oya
l In
firm
ary
St J
ames
’s H
osp
ital
HM
P L
eed
s
Dia
na
Pri
nce
ss o
f W
ales
Ho
spit
al,
Gri
msb
y
Scu
nth
orp
e G
ener
al H
osp
ital
Ro
ther
ham
Ge
ne
ral H
osp
ital
(Ho
spit
al, O
utp
atie
nt)
Ro
yal H
alla
msh
ire
Ho
spit
al,
She
ffie
ld
Nu
mb
er
of
case
s
Provider
1 & 3 6 5 4 3 2 1
Source: Hospital treatment data (RHBCSG hospital data collection survey, 2012)

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 44
Hepatitis C
Regional laboratory data for hepatitis C
This data is derived from the results of blood tests processed through NHS/HPA laboratories. Figure 5 shows an increase in new reports of hepatitis C infection in 2011 after the gradual decline in preceding years.
Figure 5: Number and rate per 100,000 resident population of laboratory confirmed cases of hepatitis C for the Yorkshire and the Humber region, by year, 2006 - 2011
Table 2: Number and rate with confidence intervals per 100,000 resident population of laboratory confirmed cases of hepatitis C, in the Yorkshire and the Humber region, 2011
Primary Care Trust Number Rate Lower Upper Barnsley 75 32.95 25.92 41.31 Bradford and Airedale 244 47.6 41.81 53.96 Calderdale 27 13.32 8.78 19.38 Doncaster 173 59.53 50.99 69.09 East Riding of Yorkshire 6 1.77 0.65 3.86 Hull 5 1.89 0.62 4.42 Kirklees 73 17.81 13.96 22.4 Leeds 511 63.97 58.54 69.77 North East Lincolnshire 49 31.15 23.05 41.18 North Lincolnshire 21 13.02 8.06 19.9 North Yorkshire and York 56 6.98 5.27 9.07 Rotherham 103 40.46 33.02 49.06 Sheffield 95 17.1 13.84 20.91 Wakefield District 49 15.05 11.13 19.9 Yorkshire and Humber Region 1486 28.03 26.62 29.49
Source: Labbase – NHS Laboratory data
Source: Labbase – NHS Laboratory data

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 45
Figure 6: Laboratory confirmed hepatitis C in the Yorkshire and the Humber region by PCT of residence; number of cases, rates per 100,000 resident population with confidence intervals, 2011
Table 2 and Figure 6 show that there is considerable variation in the numbers and rates of new reports between PCTs in Yorkshire and the Humber. There does not appear to be an urban/rural pattern to this variation and it may reflect different service provision as much as true variation in population infection. Leeds PCT has a significantly higher number of new reports of hepatitis C than other PCTs in Yorkshire and the Humber, but adjusting for population size; Doncaster Bradford, and Rotherham also have crude rates in excess of 40 per 100,000 population. It is also important to note that this laboratory data includes hepatitis C antibody test results which may not reflect current infection.
0
10
20
30
40
50
60
70
80
0
100
200
300
400
500
600
Bar
nsl
ey
Bra
dfo
rd a
nd
Air
edal
e
Cal
de
rdal
e
Do
nca
ster
East
Rid
ing
of
York
shir
e
Hu
ll
Kir
kle
es
Leed
s
No
rth
Eas
t Li
nco
lnsh
ire
No
rth
Lin
coln
shir
e
No
rth
Yo
rksh
ire
an
d Y
ork
Ro
ther
ham
She
ffie
ld
Wak
efie
ld D
istr
ict
Rat
e p
er 1
00
,00
0 r
esid
ent
po
pu
lati
on
an
d c
on
fid
ence
in
terv
als
Nu
mb
er o
f ca
ses
PCTs by Rate
59.5 to 64 (2)33 to 59.5 (2)17.1 to 33 (4)13 to 17.1 (3)
1.7 to 13 (3)
Source: Labbase – NHS Laboratory data
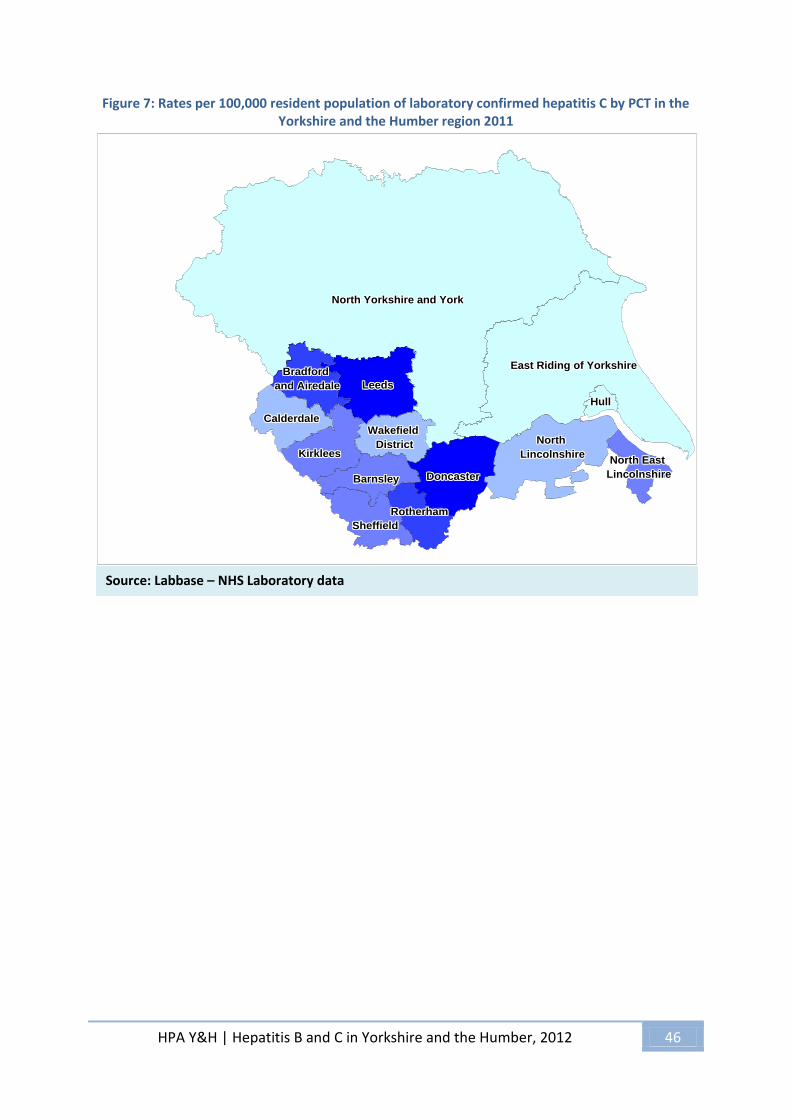
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 46
Figure 7: Rates per 100,000 resident population of laboratory confirmed hepatitis C by PCT in the Yorkshire and the Humber region 2011
North North North North North North North North North
LincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireNorth East North East North East North East North East North East North East North East North East
LincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshire
RotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherham
SheffieldSheffieldSheffieldSheffieldSheffieldSheffieldSheffieldSheffieldSheffield
BarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsley
KirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirklees
Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield
DistrictDistrictDistrictDistrictDistrictDistrictDistrictDistrictDistrict
Bradford Bradford Bradford Bradford Bradford Bradford Bradford Bradford Bradford
and Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedale LeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeeds
HullHullHullHullHullHullHullHullHull
East Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of YorkshireEast Riding of Yorkshire
CalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdale
North Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and York
DoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncaster
Source: Labbase – NHS Laboratory data
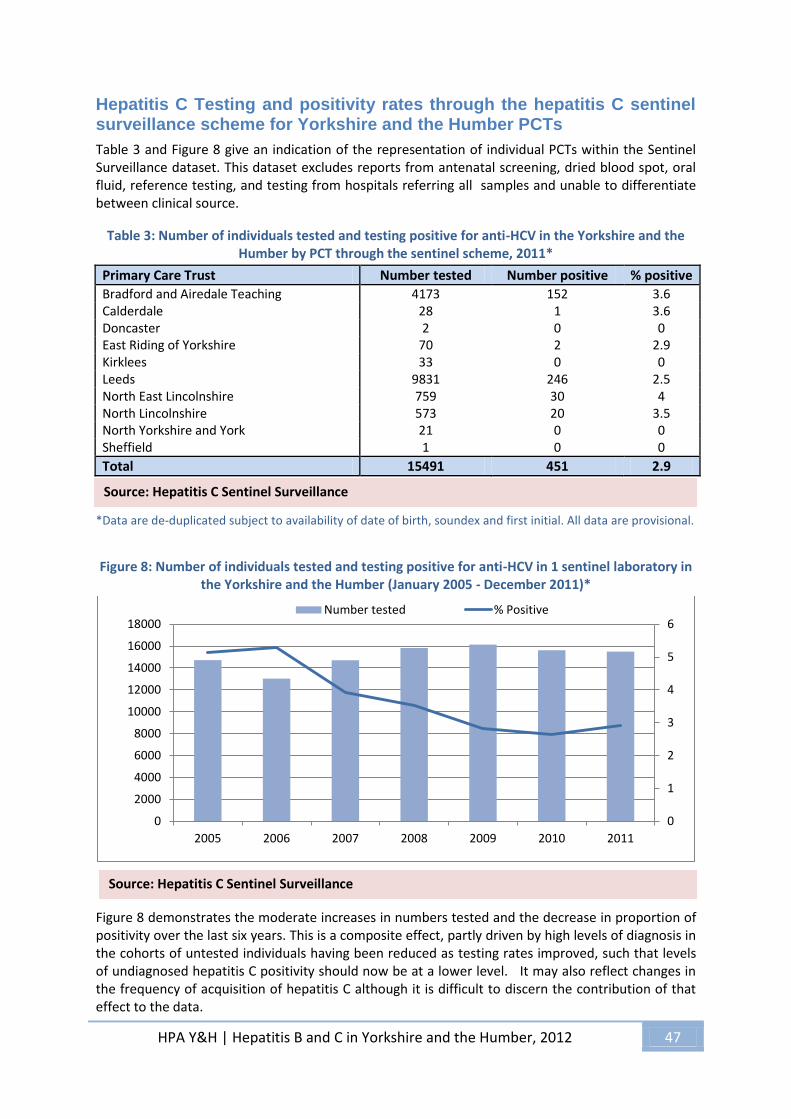
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 47
Hepatitis C Testing and positivity rates through the hepatitis C sentinel surveillance scheme for Yorkshire and the Humber PCTs
Table 3 and Figure 8 give an indication of the representation of individual PCTs within the Sentinel Surveillance dataset. This dataset excludes reports from antenatal screening, dried blood spot, oral fluid, reference testing, and testing from hospitals referring all samples and unable to differentiate between clinical source.
Table 3: Number of individuals tested and testing positive for anti-HCV in the Yorkshire and the Humber by PCT through the sentinel scheme, 2011*
Primary Care Trust Number tested Number positive % positive Bradford and Airedale Teaching 4173 152 3.6 Calderdale 28 1 3.6 Doncaster 2 0 0 East Riding of Yorkshire 70 2 2.9 Kirklees 33 0 0 Leeds 9831 246 2.5 North East Lincolnshire 759 30 4 North Lincolnshire 573 20 3.5 North Yorkshire and York 21 0 0 Sheffield 1 0 0
Total 15491 451 2.9 *Data are de-duplicated subject to availability of date of birth, soundex and first initial. All data are provisional.
Figure 8: Number of individuals tested and testing positive for anti-HCV in 1 sentinel laboratory in the Yorkshire and the Humber (January 2005 - December 2011)*
Figure 8 demonstrates the moderate increases in numbers tested and the decrease in proportion of positivity over the last six years. This is a composite effect, partly driven by high levels of diagnosis in the cohorts of untested individuals having been reduced as testing rates improved, such that levels of undiagnosed hepatitis C positivity should now be at a lower level. It may also reflect changes in the frequency of acquisition of hepatitis C although it is difficult to discern the contribution of that effect to the data.
0
1
2
3
4
5
6
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2005 2006 2007 2008 2009 2010 2011
Number tested % Positive
Source: Hepatitis C Sentinel Surveillance
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 48
Demographics of hepatitis C in Yorkshire and the Hu mber
Gender
Figure 9: Gender distribution of laboratory confirmed hepatitis C for the Yorkshire and the Humber
region, 2011
In keeping with national epidemiology, the burden of hepatitis C in Yorkshire and the Humber is
much higher among males than females with a ratio of approximately 2:1. The male predominance
may reflect the gender bias among some of the known risk associations for hepatitis C such as
injection drug use and having a custodial sentence.
Age Profile
Table 4: Percentage positive of hepatitis C by age group and region, reported via sentinel
surveillance, 2005 – 2011 (except South West*)
Region
Age Groups %
Positive
by Age
Group 1-14 15-24 25-34 35-44 45-54 55-64 65+ NK
East Midland 0.9 1.0 4.1 3.8 2.8 1.3 0.3 1.9 +N+N+N+N+N+N+N+� East of England 1.1 1.4 2.9 3.9 5.6 3.2 1.0 1.6 +N+N+N+N+N+N+N+� London 0.7 1.2 2.5 4.1 5.8 4.0 2.1 2.6 +N+N+N+N+N+N+N+� North East 0.7 1.5 3.5 3.6 2.6 1.1 0.7 0.9 +N+N+N+N+N+N+N+� North West 0.9 1.5 5.3 8.7 6.8 2.9 1.2 5.9 +N+N+N+N+N+N+N+� West Midlands 1.2 1.1 2.6 3.5 3.7 2.5 2.0 5.8 +N+N+N+N+N+N+N+� Yorkshire & Humber 1.0 1.7 5.5 5.2 4.9 2.5 1.1 5.1 +N+N+N+N+N+N+N+� South Central 0.0 0.9 2.6 4.2 5.4 2.7 0.4 3.8 +N+N+N+N+N+N+N+� South East 0.2 0.6 2.3 4.0 5.2 2.9 0.8 15.0 +N+N+N+N+N+N+N+� South West* 0.7 2.4 5.6 6.8 8.0 3.8 1.1 7.6 +N+N+N+N+N+N+N+�
*Data from April 2006 - December 2011
29%
67%
4%
Female
Male
NK
Source: Labbase – NHS Laboratory data
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 49
Table 4 shows the age distribution of hepatitis C cases which is consistent across the country in peaking between 25 and 54 years of age. Figure 10 shows the Yorkshire and Humber age distribution in numbers of cases and rates per 100,000. The YH peak is in the 25-34 year old age group, although there are still significant numbers of new diagnoses among those over 45 years of age, who may access a different range of diagnostic services than the younger cases. As most new infections are acquired via injecting drug use, which often begins in late adolescence and early adulthood, the number of positive tests in individuals aged 15 to 24 years (Figure 11) can be used as a proxy indicator of incidence.1 Figure 12 which presents Sentinel Surveillance data shows that whilst the numbers of tests done has remained steady for the last four years the percentage of positive results in 20-24 year old and especially in the 15-19 year olds has fallen steeply compared to the years before 2008, albeit slightly higher in 2011 than 2010. This indicates positive progress with preventative work with young adults and those new to injection drug use although the slight upturn in positivity in 2011 compared to 2010 adds a note of caution.
Figure 10: Number of cases and rate per 100,000 resident population of hepatitis C by age group and PCT, Yorkshire and the Humber region, reported via Labbase 2011
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
0
100
200
300
400
500
600
<1 01-04 04-09 10-14 15-24 25-34 35-44 45-54 55-64 > 65R
ate
pe
r 1
00
,00
0 r
esi
de
nt
po
pu
lati
on
Nu
mb
er
of
case
s
Number of Cases Rates per 100,000 resident population
Source: Labbase – NHS Laboratory data

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 50
Figure 11: Age group and gender of individuals testing positive for anti-HCV in the sentinel laboratory in the Yorkshire and the Humber (2005-2011)
Figure 12: Number of young adults tested and testing positive for anti-HCV in the sentinel laboratory in the Yorkshire and the Humber (2005-2011)
0
200
400
600
800
1000
1200
1-14 15-24 25-34 35-44 45-54 55-64 65+ Unknown
Nu
mb
er
Age Group
Female Male Gender Unknown
-
500
1,000
1,500
2,000
2,500
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
2005 2006 2007 2008 2009 2010 2011
Nu
mb
er
of
you
ng
adu
lts
test
ed
Pro
po
rtio
n p
osi
tive
Year
15-19 % positive 20-24 % positive 15-19 tested 20-24 tested
Source: Hepatitis C Sentinel Surveillance
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 51
Ethnicity The Hepatitis C Sentinel Surveillance Scheme collects data on ethnicity. In Yorkshire and the Humber the decline in positive result rate is common to both South Asian and non-south Asian populations. Figure 14 reveals that far fewer specimens are submitted from patients of South Asian origin, although overall percentage positivity is common across both groups. Specimens from individuals of South Asian origin account for 15% of specimens.
Figure 13: Percentage positivity of specimens for anti-HCV in the Yorkshire and the Humber by ethnicity (2005 - 2011)*
*South Asian defined as someone with an ethnic origin of India, Pakistan and Bangladesh
Figure 14: Number of individuals tested and percent testing positive for anti-HCV in the Yorkshire
and the Humber by ethnicity 2011*
*South Asian defined as someone with an ethnic origin of India, Pakistan and Bangladesh
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
2005 2006 2007 2008 2009 2010 2011
% P
osi
tive
Year
No name available Non-South Asian origin South Asian origin
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0
2000
4000
6000
8000
10000
12000
No name available Non-South Asian origin South Asian origin
% P
osi
tive
Nu
mb
er
Test
ed
Ethnicity
Number tested % positive
Source: Hepatitis C Sentinel Surveillance
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 52
Table 5: Number of individuals tested and testing positive for anti-HCV in the Yorkshire and the Humber by ethnicity, 2011
Ethnicity No tested Number Positive
% Positive % Total tested
% Total Positive
No name available 1893 34 1.80 12.22 7.54
Non-South Asian origin 11259 350 3.11 72.68 77.61
South Asian origin* 2339 67 2.86 15.10 14.86
Total 15491 451 2.91
*South Asian defined as someone with an ethnic origin of India, Pakistan and Bangladesh
Figure 15: Ethnicity breakdown of individuals tested for anti-HCV in the Yorkshire and the Humber
2011*
*South Asian defined as someone with an ethnic origin of India, Pakistan and Bangladesh
Source: Hepatitis C Sentinel Surveillance
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 53
Virology profile
Table 6: Number of individuals tested and testing positive for anti-HCV, HCV PCR and/or HCV genotype in the Yorkshire and the Humber by PCT , 2011*
PCT
Nu
mb
er
test
ed
Nu
mb
er
po
siti
ve
% p
osi
tive
Nu
mb
er
test
ed
by
PC
R
Nu
mb
er
PC
R p
osi
tive
% P
CR
po
siti
ve
Nu
mb
er
HC
V g
en
o 1
Nu
mb
er
HC
V g
en
o 3
Nu
mb
er
HC
V g
en
o 2
or
4
Nu
mb
er
HC
V g
en
o 5
,6,7
and
10
Tota
l HC
V g
en
o
Tota
l HC
V g
en
o
Bradford and Airedale Teaching 4173 152 3.6 119 86 72.3 18 48 3 - 51 69
Calderdale 28 1 3.6 1 1 100 - 1 - - - 1
Doncaster 2 0 0 - - - - - - - - -
East Riding of Yorkshire 70 2 2.9 2 1 50 1 - - - - 1
Kirklees 33 0 0 - - - - - - - - -
Leeds 9831 246 2.5 190 145 76 48 49 8 1 58 106
North East Lincolnshire 759 30 4.0 23 13 56.5 5 6 1 - 7 12
North Lincolnshire 573 20 3.5 15 11 73 5 2 - - 2 7
North Yorkshire and York 21 0 0 - - - - - - - - -
Sheffield 1 0 0 - - - - - - - - -
Total 15491 451 2.9 350 257 73.4 77 106 12 1 118 196
Figure 16: Genotype distribution among sentinel survey specimens, 2011
39%
54%
6%
1%
HCV geno 1
HCV geno 3
HCV geno 2 or 4
HCV geno 5,6,7 and 10
Source: Hepatitis C Sentinel Surveillance
Source: Hepatitis C Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 54
Table 6 shows the PCT level breakdown of hepatitis C diagnostic activity via the sentinel survey in 2011. Across the region 2.9% of submitted specimens through the sentinel survey were positive for hepatitis C antibody. 73% of the 350 who were tested by PCR were positive indicating current infection.
Data on hepatitis C virus genome is incomplete but the proportions are consistent with national epidemiology with most cases being genotype 3, closely followed by genotype 1, and only small numbers of genotypes 2 and 4.
Hepatitis C testing through alternative providers and methodologies
Alternative approaches to the diagnosis of hepatitis C using less invasive techniques such as oral fluid testing or dried blood spot have increase in popularity because of their higher patient acceptability and their flexibility for use outside of traditional healthcare settings. Across the region agencies use two providers for dried blood spot testing, namely Concateno (private national organisation) and Manchester NHS Trust. Tables 7, 8 and 9, and Figure 17 present summary data from Concateno and Manchester NHS Trust which indicate the increase over time in the use of these techniques. Data on oral fluid testing is available from 2005 and whilst the numbers have increased the positivity rate has remained in the order of 20%. This is still significantly higher, 10 fold higher, than the positivity rate on specimens tested by serology or PCR via the sentinel system. This would be expected from the higher known prevalence of hepatitis C in the settings in which these are used, Both the oral fluid and dried blood spot tests are mainly used by drug services due to the difficulty with venous access amongst injectors as well as the lack of trained phlebotomy staff on site. Whilst venous blood sampling is the preferred test drug services have found that providing testing on site is much more effective than referring individuals to their GP or local hospital for a test because of the chaotic nature of their lifestyles. There is however a wide variation of positivity rate on oral fluid testing by drug action team and it would be interesting to explore if this reflects different protocols for testing or geographical variations in positivity. This may suggest that salivary antibody testing is being done in areas not dealing exclusively with drug users – possibly prisons or other community based projects. Thus, overall prevalence will be lower than the DBST which appears to be exclusively performed in drug users given the high antibody prevalence expected in this group. One of the issues emerging from increased use of these tests is that these positive results need to be considered alongside the declining numbers observed through the use of traditional blood tests. However, the two sets of figures can not be summed as individuals identified on oral fluid testing may well go on to have standard serology and PCR testing done via an NHS laboratory. In other words such individuals could appear in both sets of data. This complicates any attempt to explicitly quantify the number of new hepatitis C diagnoses but nevertheless provides a valuable insight on trend as well as an important opportunity to improve detection rates among high risk individuals.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 55
Table 7: Number of individuals tested and testing positive for anti-HCV by Concateno Plc† and
Sentinel surveillance, 2005 - 2011
Year
Sentinel surveillance
(venipuncture)*
Sentinel surveillance (dried blood
spot) §
Concateno Plc. (oral fluid) †
Concateno Plc. (dried blood
spot) † Combined
Num
ber
test
ed
Num
ber
posi
tive
% p
ositi
ve
Num
ber
test
ed
Num
ber
reac
tive
% r
eact
ive
Num
ber
test
ed
Num
ber
reac
tive
% r
eact
ive
Num
ber
test
ed
Num
ber
reac
tive
% r
eact
ive
Num
ber
test
ed
Num
ber
reac
tive
% r
eact
ive
2005 309 140 45.3 - - - 590 104 17.6 - - - 899 244 27.1
2006 529 206 38.9 - - - 686 143 20.8 - - - 1,215 349 28.7
2007 434 172 39.6 - - - 952 203 21.3 - - - 1,386 375 27.1
2008 534 145 27.2 - - - 1,302 301 23.1 - - - 1,836 446 24.3
2009 684 129 18.9 29 9 31.0 1,683 352 20.9 59 29 49.2 2,455 519 21.1
2010 695 109 15.7 74 22 29.7 1,751 316 18.0 243 118 48.6 2,763 565 20.4
2011 750 142 18.9 132 25 18.9 1,589 277 17.4 393 147 37.4 2,864 591 20.6
Total 3,935 1,043 26.5 235 56 23.8 8,553 1,696 19.8 695 294 42.3 13,418 3,089 23.0
Table 8: Percentage of individuals testing positive by oral fluid for anti-HCV by Drug Action Team
and year, 2005 - 2011
Drug Action Team
% Positive
2005 - 2011
Increase
or
decrease
on
previous
year
2005 2006 2007 2008 2009 2010 2011
Barnsley 37 27.6 17.2 29.5 41 27.3 0 ���N��������N������ N��������N��������N��������N������� �
Bradford 13.7 9.3 20.9 17.2 14.6 16.2 12.5 ��"N�$�%�&�'�(�)�*��N�+�,�-��N�.�/�0�1N�3�4�5�6N�8�9�:�N �
Calderdale 0 33 17.7 20.2 21.7 20.7 11.7 ��'�(�)�*�<N�=�>�?�4N�A�5�B�CN�E�F�G�HN�F�F�F�IN�K���L�N �
Doncaster - - 32.5 25.6 28 25.2 25.7 ��N�N�N�N�'�(�)�*�ON�P�����QN�S�T�U�VN�X�Y�Z�[N�[�]�Q�N ��
East Riding of Yorkshire 11.1 0 0 0 10 25 11.1 ��̂N�̀�a�&�N�N�N�N�N�N�N�N�b�c�d�e�fN�g�h�i�<N�j�k�l�N �
Kingston Upon Hull 12.7 25.2 6.3 10 9.2 3.7 5.7 ��mN�n�o�i�pN�q�r�s�tN�v�w�x�yN�y�z�{�|N�~�������������N ��
Kirklees 17.1 19.1 18.2 16.5 17.3 15.1 12.7 ���N��������N��������N�������BN�E�G����N������:N�$�%�&� �
Leeds 43.8 43.5 29.7 30.4 21 18.4 27.5 ���N��������N���k�l��N�����1��N�"������N��� �¡�¢�£�¤�¥�N ��
North East Lincolnshire 25 26.7 0 0 0 50 - ��¦N�§�§�̈�©N�ª�«�¬�N�N�N�N�N�N�N�N�'�(�)�*�N�®�̄�°� �
North Lincolnshire 75 0 9.7 26.8 16.2 23.3 12.4 ��N�®�̄�°���±���²�³N�́�µ�¶�·N�̧�z�|�¹N�»�x�¼�½N�¿�À�Á�N �
North Yorkshire 17 8 14 10.5 17.2 13.3 8.8 ��ÃN�Å�Æ�Ç�È�É�Ê�Ë�ÌN�Í���:�ÎN�Ï�Ð�Ñ�ÒN�Ó�Ô�Õ�ÖN�×�Ø���N �
Rotherham - - 62.5 23 32 - - ��N�N�N�N�'�(�)�*��N�Ù�Ú�Û�ÜN�Ý�Þ�¦�ßN�á�«�¬�N�N�N�N� �
Sheffield 0 0 14.7 36.2 26.1 19.9 20 ��N�N�N�N�b�c�d�e�mN�â�h�i��N�ã�ä����N�H�å�æ�çN�ç�4�A�N ��
Wakefield - - - 28.3 13.3 7.7 20.6 ��N�N�N�N�N�N�N�N�'�(�)�*�<N�é�ê�Ö�ëN�L�·�̧�ìN�í�î�ï�N ��
York - - - 22.2 29.5 23.3 32.7 ��N�N�N�N�N�N�N�N�ð�ñ�ò�ó�ôN�õ�ö�÷��N�X�ø�ù��N�ö�����N ��
Total 17.6 20.8 21.3 23.1 20.9 18 17.4 ��úN�ü�ý�þ�BN�E�G����N�������ÒN�Ó������N�����a��N��� �¡� �
Source: Concateno PLC and Sentinel Surveillance
Source: Concateno PLC.
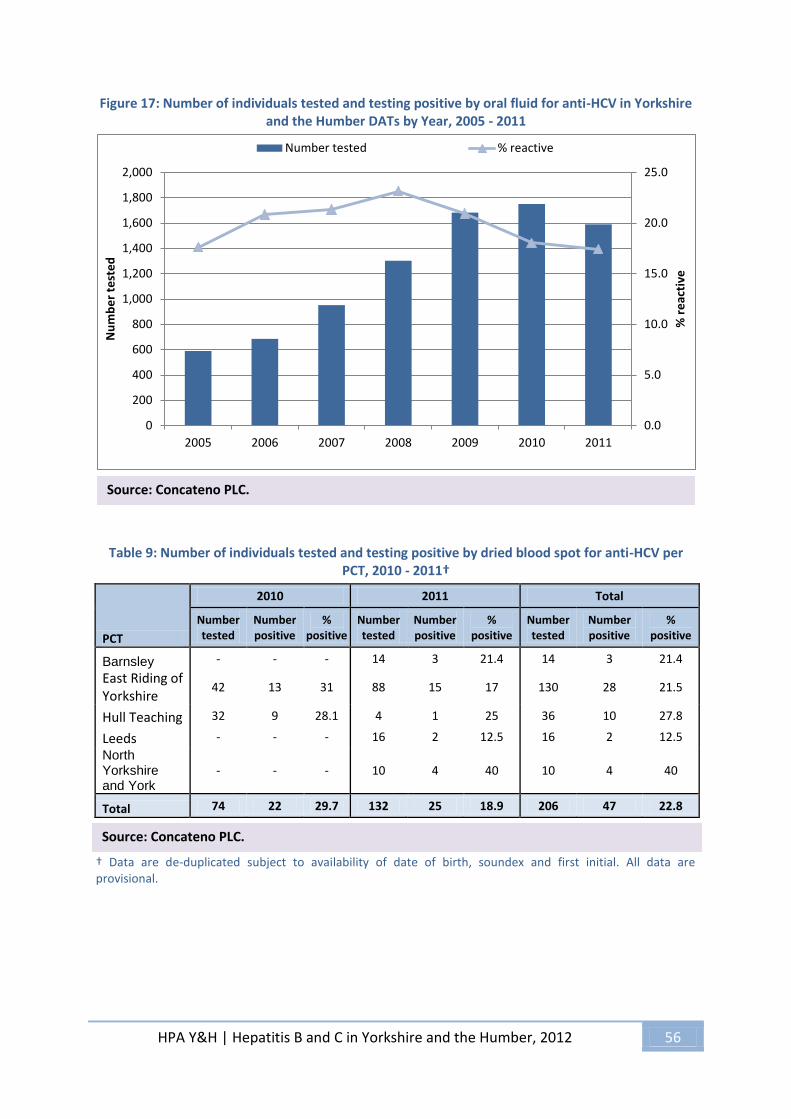
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 56
Figure 17: Number of individuals tested and testing positive by oral fluid for anti-HCV in Yorkshire and the Humber DATs by Year, 2005 - 2011
Table 9: Number of individuals tested and testing positive by dried blood spot for anti-HCV per
PCT, 2010 - 2011†
PCT
2010 2011 Total
Number tested
Number positive
% positive
Number tested
Number positive
% positive
Number tested
Number positive
% positive
Barnsley - - - 14 3 21.4 14 3 21.4
East Riding of Yorkshire
42 13 31 88 15 17 130 28 21.5
Hull Teaching 32 9 28.1 4 1 25 36 10 27.8
Leeds - - - 16 2 12.5 16 2 12.5
North Yorkshire and York
- - - 10 4 40 10 4 40
Total 74 22 29.7 132 25 18.9 206 47 22.8
† Data are de-duplicated subject to availability of date of birth, soundex and first initial. All data are provisional.
0.0
5.0
10.0
15.0
20.0
25.0
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2005 2006 2007 2008 2009 2010 2011
% r
eac
tive
Nu
mb
er
test
ed
Number tested % reactive
Source: Concateno PLC.
Source: Concateno PLC.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 57
National Treatment Agency data
The National Treatment Agency is a Special Health Authority, established in 2001 by the UK government to increase the availability, capacity and effectiveness of drug treatment in England. Their purpose is to get drug users into treatment, help them recover from dependency, and reintegrate them back into society. In light of the known association between injecting drug use and the risk of hepatitis C infection, the following tables have been included in this report to provide an insight into this area. However, it is important to note that this data only relates to those engaged in a structured intervention and therefore does not include those using open access or needle exchange services. Table 10 shows the injection status of newly presenting registered service users during 2010/2011 in England and in Yorkshire and the Humber. The percentage of those who are current injectors is 40% compared to those who are previous injectors. Table 11 provides information on hepatitis C testing within drugs services for users with a history of injecting showing that approximately 71% of service users have had a hepatitis C test, which compares well to the national figure of 60%. The definition of having had a test for the purpose of this data includes any hepatitis C test and does not imply confirmatory PCR has been undertaken. The test does not have to have been done within the reporting service and does not have to be recent.
Table 10: Injecting status of adults in drug treatment
2010-2011
Injecting status Newly presenting
Area National Yorkshire and Humber
Current injector 12,724 1,794
Previously injected 19,038 2,672
All current/previous injectors 31,762 4,466
Table11: Hepatitis C test status of adults in drug treatment - injectors only
2010-2011
All in treatment
National Yorkshire and Humber
Has a hepatitis C test recorded No. 67,395 12,202
% 59.79% 71.24%
Does not have a hepatitis C test recorded No. 45,320 4,927
% 40.21% 28.76%
Total 112,715 17,129

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 58
Table 12: Hepatitis C intervention status for adults in drug treatment - injectors only
2010-2011
Recorded hepatitis C status Newly presenting
National Yorkshire and Humber
Offered and accepted No. 15,812 2,229
% 49.78% 49.91%
Offered and refused No. 9,638 1,669
% 30.34% 37.37%
Assessed as not appropriate to offer No. 3219 348
% 10.13% 7.79%
Not offered No. 1318 70
% 4.15% 1.57%
No recorded status No. 1,775 150
% 5.59% 3.36%
Total 31,762 4,466
Table 13: Hepatitis C intervention status at latest episode in drug treatment journey (i.e. all those
in treatment in 2011)
Hep C intervention Total %
Offered and accepted 9795 49.53%
Offered and refused 6949 35.14%
Not offered 372 1.88%
Assessed as not appropriate to offer 1900 9.61%
Missing data 759 3.84%
Total number in treatment 19775 100.00%
Table 14: Hepatitis C intervention status with test date between 01/01/2011 and 31/12/2011 (all test dates) and for latest test date (individual number)
Hep C intervention
Total Hep C interventions (all interventions with
test date in 2011) - could be double counted
%
Latest Hep C intervention during 2011 (individual number so not double
counted)
%
Offered and accepted
3913 60.74% 3207 66.70%
Offered and refused 1570 24.37% 973 20.24%
Not offered 64 0.99% 48 1.00%
Assessed as not appropriate to offer
787 12.22% 526 10.94%
Missing data 108 1.68% 54 1.12%
Total 6442 100.00% 4808 100.00%

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 59
Tables 12 - 14 present regional NTA data. Table13 is reporting information about the status of an individual, in terms of ever having a documented hepatitis C intervention. It indicates that almost 85% of service users with a treatment journey in 2011 had been offered a hepatitis C test as assessed at their latest episode of care during their treatment journey. 49% of service users had accepted the offer. In the majority of cases accepting an offer of a test is translated into actually having a hepatitis C test, but depending on service design there may be some attrition. Any one individual during a treatment journey may have contact and episodes of care with a number of services and the possibility exists for some duplication of testing. Table 14 is about service activity in the current/latest treatment journey and does not account for earlier interventions. It includes data on interventions for all episodes of care during 2011, and the figure of 3,913 incidences of a test being offered and accepted may include duplication where an individual has been receiving more than one episode of care during their treatment journey. The final columns in Table 14 also present the information for activity within 2011 but assessed for individuals at their latest episode of care in 2011. This number is lower than the intervention figures in Table 13 as the data refers just to 2011 and does not include any previously documented information on the intervention status of individuals.

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 60
Hepatitis B
This report contains information on hepatitis B from NHS/HPA laboratory data and from the Sentinel
Surveillance Scheme as with hepatitis C. The HPA case management system – HPZone- also provides
additional information on the burden of hepatitis B and epidemiological data.
Hepatitis B laboratory data
Table 15: Number of cases of hepatitis B, acute and chronic, reported via Labbase, by primary care
trust and year, for the Yorkshire and the Humber region, 2006 – 2011
Primary Care Trust 2006 2007 2008 2009 2010 2011 Trend
EAST RIDING OF YORKSHIRE PCT 2 1 10 5 8 7 ���N��� �¡�'�(�)�*�<N�j�k�l�� N�������� N�����N HULL TEACHING PCT 6 1 51 20 26 35 ���N��� �¡�'�(�)�*��N�Ù��� �� N�Ý���1�3N�������N NORTH EAST LINCS CARE TRUST 0 2 5 8 6 16 ��������²�³N�́�»���¶N�Ü���1�� N�������� N�g�h�i�N NORTH LINCOLNSHIRE PCT 2 14 8 9 8 9 ��'�(�)�*�<N�é�����¦N�̈�4�5�� N�������¦N�̈�4�5�N NORTH YORKSHIRE AND YORK PCT 4 2 5 18 11 6 ��� N� � �¡�! ���²�³�" N�$�%�&�ÒN�'�-�Ì�KN���(�)�N BARNSLEY PCT 0 10 3 1 29 19 ��¢�£�¤�*�̧N�¿�,�-��N�.��� �/ N�0�1�2��N�������N DONCASTER PCT 0 3 2 6 13 48 ����3���4�4N�4�4�4�4N�����²�tN�v�¹�6�ÎN�Ï�Ð�Ñ�N ROTHERHAM PCT 2 14 8 10 21 26 ��7 �8�9�í�: N�;�<�=�xN�y�¼�>�? N�@�A�B�öN�÷�C�D�N SHEFFIELD PCT 1 128 125 127 110 155 ��E �F�G�H�IN�I�I�Y�SN�I�I�I�Y N�Z����K N�������N BRADFORD AND AIREDALE
TEACHING PCT 12 6 57 69 92 67 ��� N� �3�¡�È�M�N�O�BN�P���Q�õ N��������N�+�,�ù�N CALDERDALE PCT 0 2 3 4 9 17 ��������S�TN�t�U�V�WN�X�¹�Y�µ N�[�\�]�̂N�_�̀�a�N KIRKLEES PCT 0 0 11 15 64 57 ��N�N�N�N�! ���S�³�WN�X�¹�Y�b N�c�H�Ñ��N�d�e���N LEEDS PCT 48 31 131 248 198 180 ��� N�4� �¡�b�f�g�h�þN�i�j�a�ON�P�k�ø�� N��l��N WAKEFIELD DISTRICT PCT 3 0 4 5 58 18 ��4N� �3�¡���3�����.N�.�.�.�m N�n�o�2�p N�q���r�N Yorkshire and Humber Region 80 214 423 545 653 660 ��! �s�³�́�g N�t�u�v�� N���Q�õ�öN�÷�C�D��N�������N
Figure 18: Number of cases and rate per 100,000 resident population of cases of hepatitis B, acute
and chronic, reported via Labbase, by year, for the Yorkshire and the Humber region, 2006 – 2011
0
2
4
6
8
10
12
14
0
100
200
300
400
500
600
700
2006 2007 2008 2009 2010 2011
Number of Cases Rate per 100,000 resident population
Source: Labbase – NHS Laboratory data
Source: Labbase – NHS Laboratory data

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 61
Table 16: Cases of hepatitis B reported via Labbase in 2011, by number, rate and confidence intervals, for the Yorkshire and the Humber region
Primary Care Trust Number Rate Confidence intervals
Lower Upper
EAST RIDING OF YORKSHIRE PCT 7 2.07 0.83 4.26
HULL TEACHING PCT 35 13.26 9.24 18.45
NORTH EAST LINCS CARE TRUST 16 10.17 5.81 16.52
NORTH LINCOLNSHIRE PCT 9 5.58 2.55 10.59
NORTH YORKSHIRE AND YORK PCT 6 0.75 0.27 1.63
BARNSLEY PCT 19 8.35 5.03 13.04
DONCASTER PCT 48 16.52 12.18 21.9
ROTHERHAM PCT 26 10.21 6.67 14.96
SHEFFIELD PCT 155 27.9 23.68 32.66
BRADFORD AND AIREDALE TEACHING PCT 67 13.07 10.13 16.6
CALDERDALE PCT 17 8.39 4.89 13.43
KIRKLEES PCT 57 13.91 10.53 18.02
LEEDS PCT 180 22.53 19.36 26.08
WAKEFIELD DISTRICT PCT 18 5.53 3.28 8.74
Yorkshire and Humber Region 660 12.45 11.52 13.44
Tables 15 &16 and Figure18 show the numbers (and rates) of cases of hepatitis B reported through NHS/HPA laboratories for Yorkshire and the Humber during 2011. This includes a combination of acute and chronic cases of the infection. Some of the chronic cases may be newly identified, whilst others may reflect repeat specimens in previously known infected individuals. The data is de-duplicated to remove multiple specimens from the same individual in the same year. There were 660 confirmed hepatitis B infections reported in 2011. HPZone data on cases reported to HPUs during 2011 indicate that there were 35 acute hepatitis B infections in Yorkshire and the Humber residents diagnosed in the year. The highest numbers of infections were confirmed in residents of Sheffield and Leeds but Doncaster, Hull, Bradford and Kirklees also have higher rates per 100,000 population than the regional average.
Source: Labbase – NHS Laboratory data

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 62
SShheeffffiieelldd
East Riding of East Riding of East Riding of East Riding of East Riding of East Riding of East Riding of East Riding of East Riding of
YorkshireYorkshireYorkshireYorkshireYorkshireYorkshireYorkshireYorkshireYorkshire
North North North North North North North North North
LincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshire
Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield Wakefield
DistrictDistrictDistrictDistrictDistrictDistrictDistrictDistrictDistrictKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirkleesKirklees
BarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsleyBarnsley
Bradford Bradford Bradford Bradford Bradford Bradford Bradford Bradford Bradford
and Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedaleand Airedale LeedsLeedsLeedsLeedsLeedsLeedsLeedsLeedsLeeds
North East North East North East North East North East North East North East North East North East
LincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshireLincolnshire
North Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and YorkNorth Yorkshire and York
RotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherhamRotherham
HullHullHullHullHullHullHullHullHull
CalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdaleCalderdale
DoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncasterDoncaster
SShheeffffiieelldd
Figure 19: Cases of hepatitis B reported via Labbase in 2011 by number, rate and confidence intervals for the Yorkshire and the Humber region
0
5
10
15
20
25
30
35
020406080
100120140160180200
EAST
RID
ING
OF
YOR
KSH
IRE
PC
T
HU
LL T
EAC
HIN
G P
CT
NO
RTH
EA
ST L
INC
S C
AR
ETR
UST
NO
RTH
LIN
CO
LNSH
IRE
PC
T
NO
RTH
YO
RK
SHIR
E A
ND
YOR
K P
CT
BA
RN
SLEY
PC
T
DO
NC
AST
ER P
CT
RO
THER
HA
M P
CT
SHEF
FIEL
D P
CT
BR
AD
FOR
D A
ND
AIR
EDA
LETE
AC
HIN
G P
CT
CA
LDER
DA
LE P
CT
KIR
KLE
ES P
CT
LEED
S P
CT
WA
KEF
IELD
DIS
TRIC
T P
CT
Rat
e p
er
10
0,0
00
re
sid
en
t p
op
ula
tio
n
Nu
mb
er
of
case
s
Source: Labbase – NHS Laboratory data
Source: Labbase – NHS Laboratory data
PCTs by Rate
59.2 to 63 (1)32.5 to 59.2 (4)15.1 to 32.5 (2)
6.9 to 15.1 (3)1.7 to 6.9 (4)
Figure 20: Rates per 100,000 resident population of laboratory confirmed hepatitis B by PCT in the Yorkshire and the Humber region 2011

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 63
Sentinel Surveillance for hepatitis B
The sentinel surveillance scheme described under hepatitis C also reports data on hepatitis B. The scheme does not fully represent the region but does provide an indication of positivity rates in submitted samples at least for West Yorkshire and Humber areas. The overall proportion of tests positive is 1.2% although this varies by geography and by age group with a peak among young adults. The samples included in this will include those taken for diagnostic and for screening purposes, although antenatal screening specimens are excluded. 0.3% of antenatal screening samples in Yorkshire and the Humber were positive during the same period.
Table 17: Number of individuals tested and testing positive for HBsAg in the Yorkshire and the Humber by PCT (excluding antenatal screening), 2010*
Primary Care Trust Number tested
Number positive % positive
Bradford and Airedale Teaching 4695 58 1.2
Calderdale 34 0 0
Doncaster 2 0 0
East Riding of Yorkshire 75 1 1.3
Kirklees 27 0 0
Leeds 11128 137 1.2
North East Lincolnshire 848 6 0.7
North Lincolnshire 640 2 0.3
North Yorkshire and York 21 0 0
Sheffield 1 0 0
Total 17471 204 1.2
Figure 21: Number of cases of hepatitis B reported via HPZone for the Yorkshire and the Humber region by diagnosis and quarter, 2011
0
20
40
60
80
100
120
140
160
180
1 2 3 4Quarters
Hepatitis B, acute Hepatitis B, chronic
Source: Hepatitis B Sentinel Surveillance
Source: HPZone

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 64
Breakdown of PCT/HPU
Table 18: Number of chronic and acute cases of hepatitis B reported through HPZone, by HPU, PCT and quarter, 2011
Health Protection Unit PCT Q1 Q2 Q3 Q4
North Yorkshire and the Humber
East Riding of Yorkshire 3 3 0 4
Hull 10 12 4 6
North East Lincolnshire 1 0 4 0
North Lincolnshire 3 1 1 3
North Yorkshire and York 13 9 7 14
South Yorkshire
Barnsley 3 4 6 0 Doncaster 13 27 26 20 Rotherham 4 5 10 6
Sheffield 21 11 30 37
West Yorkshire
Bradford and Airedale 25 29 14 18
Calderdale 4 8 5 11
Kirklees 7 14 14 11
Leeds 25 39 39 34
Wakefield District 2 6 4 5
Not Known (GUM samples) 1 2 0 0
Yorkshire and Humber Region 135 170 164 169
Table 19: Number of chronic, acute and unspecified cases of hepatitis B reported through HPZone, by HPU and diagnosis, 2011
Health Protection Unit Hepatitis B, acute Hepatitis B, chronic Hepatitis B, unspecified
North Yorkshire and Humber 11 85 2 South Yorkshire 9 209 5 West Yorkshire 15 301 1
Source: HPZone
Source: HPZone

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 65
Hepatitis B demography
Gender
There is a moderate male preponderance of hepatitis B cases in the laboratory data (Labbase) with a ratio of 3 males: 2 females. HPZone data allows a comparison between the profile of acute and chronic cases. For acute cases only 17% were female but for chronic cases 43% were female. This may reflect increased opportunity for asymptomatic diagnosis in well women with carriage who have been tested for other purposes. The acute diagnosis proportion is less likely to be biased by consulting behaviour.
Figure 22: Gender breakdown of cases of acute and chronic hepatitis B reported via Labbase, 2011, for the Yorkshire and the Humber region
Figure 23: Percentage breakdown of cases of hepatitis B reported via HPZone in the Yorkshire and
the Humber region, by diagnosis and gender, 2011
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Acute Chronic Unspecified
Pe
rce
nta
ge b
reak
do
wn
Diagnosis
Unknown
Male
Female
Source: Labbase – NHS Laboratory data
Source: HPZone

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 66
Age
Both the laboratory and the HPZone data show the peak age for hepatitis B positive reports to be in the 25 to 34 year old group, with the numbers starting to rise among the 15-24 year old group and falling off after 50 years of age. The sentinel surveillance data reveals that the positivity rate in those tested is highest in females in the 25-34 years bracket and falls sharply after 50. For males however, the peak starts earlier, is higher, and is more sustained into the fifties and sixties decades of life.
Figure 24: Cases of acute and chronic hepatitis B reported via Labbase by age group and rate per 100,000 resident population, 2011, for the Yorkshire and the Humber region
Figure 25: Number of cases of acute and chronic hepatitis B reported via HPZone in the Yorkshire and the Humber region by age group, 2011
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
0
50
100
150
200
250
300
0-<01 01-04 05-14 15-24 25-34 35-44 45-54 55-64 65+
0
50
100
150
200
250
300
0-<01 01-04 05-14 15-24 25-34 35-44 45-54 55-64 65+
Hepatitis B, acute Hepatitis B, chronic Hepatitis B, unspecified
Source: Labbase – NHS Laboratory data
Source: HPZone
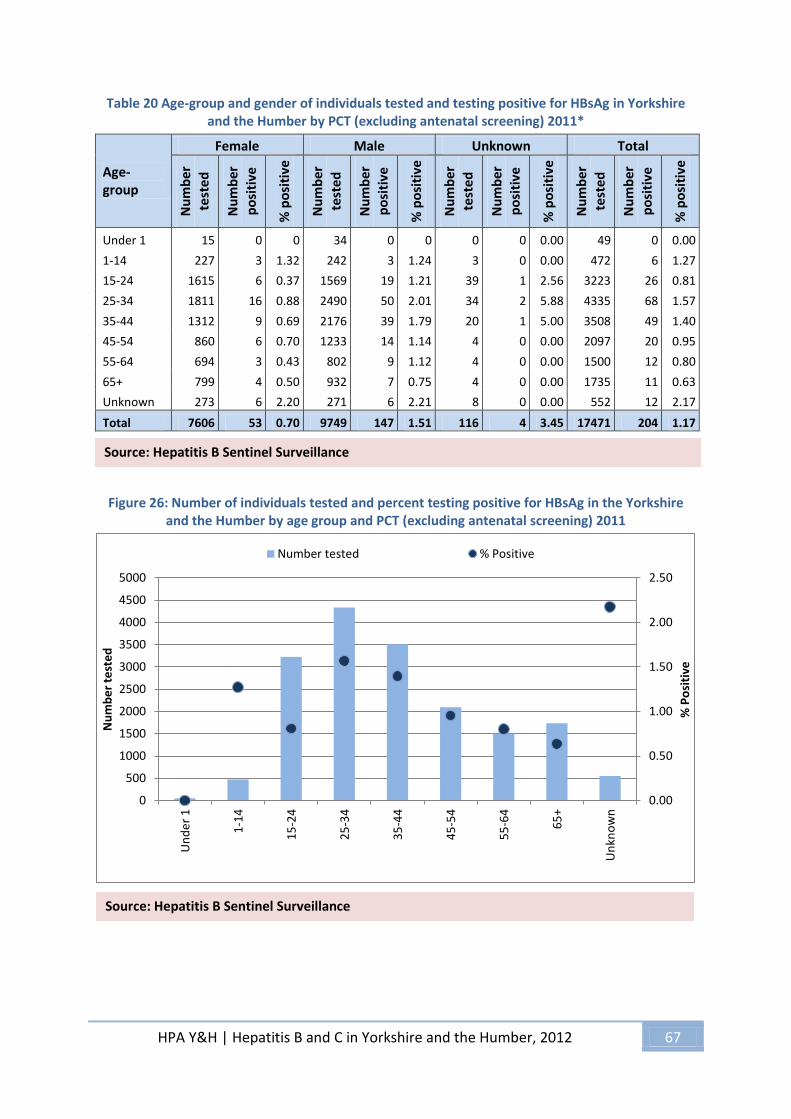
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 67
Table 20 Age-group and gender of individuals tested and testing positive for HBsAg in Yorkshire and the Humber by PCT (excluding antenatal screening) 2011*
Age-group
Female Male Unknown Total
Nu
mb
er
test
ed
Nu
mb
er
po
siti
ve
% p
osi
tive
Nu
mb
er
test
ed
Nu
mb
er
po
siti
ve
% p
osi
tive
Nu
mb
er
test
ed
Nu
mb
er
po
siti
ve
% p
osi
tive
Nu
mb
er
test
ed
Nu
mb
er
po
siti
ve
% p
osi
tive
Under 1 15 0 0 34 0 0 0 0 0.00 49 0 0.00
1-14 227 3 1.32 242 3 1.24 3 0 0.00 472 6 1.27
15-24 1615 6 0.37 1569 19 1.21 39 1 2.56 3223 26 0.81
25-34 1811 16 0.88 2490 50 2.01 34 2 5.88 4335 68 1.57
35-44 1312 9 0.69 2176 39 1.79 20 1 5.00 3508 49 1.40
45-54 860 6 0.70 1233 14 1.14 4 0 0.00 2097 20 0.95
55-64 694 3 0.43 802 9 1.12 4 0 0.00 1500 12 0.80
65+ 799 4 0.50 932 7 0.75 4 0 0.00 1735 11 0.63
Unknown 273 6 2.20 271 6 2.21 8 0 0.00 552 12 2.17
Total 7606 53 0.70 9749 147 1.51 116 4 3.45 17471 204 1.17
Figure 26: Number of individuals tested and percent testing positive for HBsAg in the Yorkshire and the Humber by age group and PCT (excluding antenatal screening) 2011
0.00
0.50
1.00
1.50
2.00
2.50
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Un
de
r 1
1-1
4
15
-24
25
-34
35
-44
45
-54
55
-64
65
+
Un
kno
wn
% P
osi
tive
Nu
mb
er
test
ed
Number tested % Positive
Source: Hepatitis B Sentinel Surveillance
Source: Hepatitis B Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 68
Ethnicity
Figure 27: Percentage of cases of acute hepatitis B reported via HPZone by ethnic group, 2011
Ethnicity data from HPZone is largely incomplete and it is not possible to conclude anything about ethnicity from the limited dataset. Using the Nanpam computer programme on the sentinel surveillance dataset to identify names of South Asian origin and comparing numbers tested to numbers positive there is a striking mismatch between the number of tests done and positivity. A much higher percentage (2.3) of individuals with South Asian names prove positive when tested compared to white British groups. The proportion of tests positive among the black or black British population is also raised at 7.9% although the numbers tested are smaller
Figure 28: Ethnicity breakdown of Individuals tested for HBSAg in the Yorkshire and the Humber (excludes antenatal screening) 2011
84%
0% 4%
3%
1%
0%
2% 0% 1% 2% 1%
2%
Unknown (533)
Bangladeshi (1)
Black African (27)
Chinese (21)
Indian (2)
Mixed White and Black African (1)
Not stated (11)
Other (2)
Other Asian (6)
Other White (13)
Pakistani (8)
White British (13)
63% 15%
1%
1%
20% White or White British
Asian or Asian British
Black or Black British
Other and/or Mixedethnicity
Unknown ethnicity
Source: HPZone
Source: Hepatitis B Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 69
Figure 29: Ethnicity breakdown of individuals testing positive for HBsAg in the Yorkshire and Humber region (excludes antenatal screening) 2011
Table 21: Number of individuals tested and testing positive for HBsAg in the Yorkshire and the Humber by ethnicity (excludes antenatal screening) 2011
Ethnicity Number tested
Number positive
% positive % known ethnicity
White or White British 10873 48 0.44 78.53
Asian or Asian British 2520 59 2.34 18.20
Black or Black British 190 15 7.89 1.37
Other and/or Mixed ethnicity 263 34 12.93 1.90
Unknown ethnicity 3421 48 1.40 -
Total 17267 204 1.181444 -
23%
29%
7%
17%
24%
White or White British
Asian or Asian British
Black or Black British
Other and/or Mixedethnicity
Unknown ethnicity
Source: Hepatitis B Sentinel Surveillance
Source: Hepatitis B Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 70
Figure 30: Ethnicity breakdown of individuals tested and testing positive for HBsAg in the Yorkshire and Humber region (excluding antenatal screening), 2011
Transmission risks
Figure 31 shows the most likely route of transmission ascertained by a health protection nurse or Consultant in Communicable Disease Control during their public health management of the case, and is based on information obtained from case interviews or from their attending clinician, where they have been able to do so. Disappointingly this is poorly completed the most likely route is not recorded for 37% of cases however this is a significant improvement from the 60% in 2010. Where most likely transmission risk has been recorded heterosexual exposure is the most commonly reported risk exposure for acute hepatitis B. The clinical source of positive specimens is shown in Figure 32. 42% are from GPs, and 34% from GUM services. Other significant sources include accident and emergency departments, prison health, drugs services and occupational health services which reflects where most diagnostic or screening activity is taking place, which in turn reflects what is known of the epidemiology and transmission risks for this infection. Although a history of injecting drug use is seldom documented among the cohort of acute hepatitis B infections in Yorkshire and the Humber in 2011 it is unknown if this risk is present among some of the individuals for whom exposure history was unavailable. The association of injection drug use especially sharing equipment is well established for hepatitis B. Provision of hepatitis B vaccination to clients of drugs services is an important and effective intervention to reduce this risk, made doubly important for those whose livers may already be at risk of damage from hepatitis C. However sexual transmission remains the most likely route of transmission for the majority of acute cases.
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
0
2000
4000
6000
8000
10000
12000
White or WhiteBritish
Asian or AsianBritish
Black or BlackBritish
Other and/orMixed ethnicity
Unknownethnicity
Number Tested % positive
Source: Hepatitis B Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 71
Figure 31: Breakdown of most likely route of transmission for acute hepatitis B cases reported via HPZone in the Yorkshire and the Humber region, 2011
Source of positive samples
Figure 32: Percentage of individuals tested for HBsAg in the Yorkshire and the Humber by primary service type (excluding antenatal screening) 2011
4.1.1.
34%
23% 3%
3%
37% Heterosexual exposure
Homosexual exposure
Other specified route
Skin piercing or tattooing
Unknown
1%
7%
42%
34%
13%
3% Accident and emergency
Drug dependency services
General practitioner
GUM clinics
Occupational health
Prison services
Source: HPZone
Source: Hepatitis B Sentinel Surveillance

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 72
Antenatal screening
Antenatal infection screening is now routinely offered to all women during pregnancy. There is a very high uptake of this test across the region. For women who are identified as positive, there is the opportunity to receive care for their infection and public health interventions for their contacts. The primary purpose of the programme however, is to identify at risk babies and protect them from vertical transmission through the early use of vaccine and in some circumstances immunoglobulin. This programme has been highly successful in interrupting vertical transmission of hepatitis B.
Figure 33: Number of women tested and testing positive for hepatitis B in the Yorkshire and the Humber region by year, 2001 - 2011
Source: Antenatal Screening Surveillance data
Table 22: Number of women booked for antenatal care in the Yorkshire and the Humber region by
year and number of women, offered, declining, tested and testing positive for hepatitis B
Year Booked Offered Declined Tested Positive
2001 41380 40970 4780 35272 82
2002 37290 36387 3437 33661 98
2003 49755 48690 3502 40465 101
2004 62732 52570 3581 50718 140
2005 62095 54572 3201 56210 185
2006 67822 66277 2127 63214 157
2007 68591 67747 1051 66954 234
2008 70532 70866 905 68428 296
2009 73056 68550 1082 70661 244
2010 71932 71734 456 70206 218
2011 68339 63921 334 66832 207
Source: Antenatal Screening Surveillance data
0
50
100
150
200
250
300
350
0
10000
20000
30000
40000
50000
60000
70000
80000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Number of Women tested Number of women testing positive

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 73
5. Commissioning
5.1. Future commissioning arrangements There remain uncertainties surrounding the future commissioning of hepatitis B and C services in the reformed health system. Services will be commissioned from different agencies over the coming months; however the multi agency work that has taken place across Yorkshire and the Humber will hopefully ensure that a clear framework is in place for the future commissioning of all parts of the hepatitis B and C pathway. In the documents Clinical Advisory Group for Prescribed Services: Final Recommendations, June 201219 and the Commissioning Fact Sheet for Clinical Commissioning Groups, July 201220 some details are provided about the future commissioning of hepatitis services. However, at the time of publishing this report the situation still remains unclear. Stakeholders will be informed of the new responsibilities for the commissioning of hepatitis services as soon as they are confirmed.
5.2. Estimates of the future burden of hepatitis C in Yorkshire and the Humber and the costs of treatment The HPA published a revised modelling tool in July 2011 to help DATs and Health and Wellbeing Boards with estimating the prevalence of HCV in their local population (the previous 2007 version was estimated at PCT level). The tool ‘Commissioning template for estimating prevalence of HCV by DAT and numbers eligible for treatment’21 is a useful source to look at local need in relation to prevalence, future burden and treatment and cost.
19 http://www.dh.gov.uk/health/files/2012/09/Clinical-Advisory-Group-for-Prescribed-Services.pdf 20
http://www.commissioningboard.nhs.uk/files/2012/07/fs-ccg-respon.pdf 21
http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/HepatitisC/EpidemiologicalData/

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 74
Table 23: HPA estimates for numbers infected with hepatitis C and genotype distribution by local authority
Genotype distribution
LA Total estimated infected as at 2005 RNA +ve 1 2 3 4 Other
Barnsley 791 585 263 43 256 19 4
Bradford & Airedale 2609 1930 869 141 846 64 12
Calderdale 605 447 201 33 196 15 3
Doncaster 1106 818 368 60 358 27 5
East Riding 684 506 228 37 222 17 3
Hull 1691 1251 563 91 548 41 8
Kirklees 1451 1074 483 78 470 35 6
Leeds 3106 2299 1034 168 1007 76 14
NE Lincs 526 389 175 28 170 13 2
North Lincs 506 374 168 27 164 12 2
North Yorks 1298 961 432 70 421 32 6
Rotherham 932 689 310 50 302 23 4
Sheffield 2083 1542 694 113 675 51 9
Wakefield 1145 848 381 62 371 28 5
York 725 537 242 39 235 18 3
Table 24: HPA estimates for future burden of hepatitis C by local authority
LA Estimated total
infected population (RNA+ve) as at 2005
Estimated Burden in 2015 Estimated total cost of
treating those
already identified
Estimated annual cost of
treating additional
cases
Mild Moderate Cirrhotic or
end stage
Died
Barnsley 585 321 186 24 54 £555,420 £78,299
Bradford & Airedale 1930 1057 614 82 177 £1,831,443 £258,183
Calderdale 447 245 142 19 41 £424,540 £59,849
Doncaster 818 448 260 35 75 £776,864 £109,446
East Riding 506 277 161 22 46 £480,127 £67,685
Hull 1251 685 398 53 115 £1,187,278 £167,374
Kirklees 1074 588 342 46 98 £1,018,460 £143,575
Leeds 2299 1259 731 97 211 £2,180,876 £307,444
NE Lincs 389 213 124 16 36 £369,069 £52,029
North Lincs 374 205 119 16 34 £354,971 £50,041
North Yorks 961 526 306 41 88 £911,505 £128,497
Rotherham 689 378 219 30 63 £654,024 £92,199
Sheffield 1542 844 490 66 141 £1,462,433 £206,163
Wakefield 848 464 270 36 78 £804,039 £113,347
York 537 294 171 23 49 £509,310 £71,799

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 75
6. Conclusion and recommendations
6.1. Conclusion 2011-12 has seen many changes both nationally and across the region in relation to the way that hepatitis B and C services are to be commissioned. During 2013 we will start to see these many changes being implemented. Work is taking place both locally and regionally to ensure that there is clarity regarding roles and responsibilities for the commissioning of these services and it is crucial that the regional network that has been built up is maintained to allow for discussion for the best way forward in the planning and delivery of local services. There have been many developments in service provision, which has allowed for better access to testing and treatment for patients, however there is still much work to do to ensure equity across the region. The development of a Liver Network in Yorkshire and the Humber will be an important step to providing a more encompassing arena for professionals to discuss liver issues. This will hopefully serve to provide more support to professionals working in liver care as well as be an expert resource for commissioners to seek guidance from in relation to alcohol, hepatitis and non-fatty liver disease.
6.2. Recommendations for 2013
i. The regional steering group and the West and East Yorkshire Hepatology Network should work together to create a Liver Network for Yorkshire and the Humber. This should include a range of stakeholders including commissioners, public health, service providers and service users.
ii. The regional steering group should review the Yorkshire and the Humber Testing Guidance and Quality Standards Framework during 2013 to ensure it is kept relevant and up to date.
iii. All regional guidance should be made available electronically for professionals to download; the regional steering group should explore the best way of doing this.
iv. The regional steering group should review the common dataset for the collection of information.
v. Commissioners and providers should ensure that automatic testing for PCR is carried out on all antibody positive results for hepatitis C. Where this is not possible (i.e. if oral tests are used) appropriate interventions should be in place to ensure that the patient is not lost to follow up or the pathway for access to PCR testing is not inaccessible.
vi. The regional steering group should introduce a system to ensure local HPUs are informed about all positive test results from drug services where private companies are being used.
vii. More accessible provision for hepatitis C treatment should be provided in Harrogate, York and Selby.
viii. All prisons should demonstrate that their pathway for vaccinations, testing and treatment are accessible and that services are equitable to those available in the community. Communication should be improved between prisons and the community in relation to testing and treatment and a clear pathway should be in place to enable continuation of treatment when patients return to the community.
HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 76
7. References
Department of Health, Improving outcomes and supporting transparency: public health outcomes framework for England, 2013-2016 HCV Action, Hepatitis C adult services commissioning toolkit, October 2012 Health Protection Agency and Department of Health, National survey of hepatitis C services in prisons in England, July 2012 Health Protection Agency North West, Burden of Liver Disease and Inequalities in the North West of England, 2012 Health Protection Agency, Commissioning template for estimating prevalence of HCV by DAT and numbers eligible for treatment, July 2011 Health Protection Agency, Hepatitis C in the UK report, 2012 Health Protection Agency, National Treatment Agency and NHS Yorkshire and the Humber, Guidance on testing for hepatitis B and C (with reference to HIV), March 2012 Health Protection Agency, National Treatment Agency and NHS Yorkshire and the Humber, Quality Standards Framework for Hepatitis B and C, March 2012 Health Protection Agency, Quarterly report from the sentinel surveillance study of hepatitis testing in England: data for January to March 2012 Health Protection Agency, Unlinked anonymous HIV and viral hepatitis monitoring among people who inject drugs: Update, July 2012 NHS Commissioning Board, The Way Forward, Strategic Clinical Networks, July 2012 NHS Commissioning Board, Commissioning fact sheet for clinical commissioning groups, July 2012 NHS Clinical Advisory Group for Prescribed Services: Final Recommendations, June 2012 NICE Technology appraisal 253, Hepatitis C (genotype 1) – boceprevir, 2012 NICE Technology appraisal 252, Hepatitis C (genotype 1) - telaprevir, 2012

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 77
Appendix 1: Yorkshire and the Humber Hepatitis Project Launch – Agenda
YORKSHIRE & THE HUMBER HEPATITIS B & C PROJECT LAUNCH 29 MARCH 2012, LEEDS TOWN HALL
AGENDA
SESSION 1: NATIONAL WORK Setting the Scene in the ‘New World’ Dr Stephen Morton, Regional Director Yorkshire & the Humber, HPA The National Liver Strategy – How Can We Achieve Change? Professor Martin Lombard, National Clinical Director for Liver Disease, Department of Health The Role of a Managed Network in Commissioning HCV Services Siobhan Fahey, Project Manager, NICE and Department of Health Hepatitis C in England and Monitoring Treatment Dr Helen Harris, Clinical Scientist (Epidemiology), HPA The Interface Between Primary and Secondary Care Dr Rebecca Jones, Consultant, Leeds Teaching Hospitals Questions to the Panel SESSION 2: TARGETTING HARD TO REACH GROUPS Testing Hard to Reach Groups Leila Reid, Research and Communications Manager, The Hepatitis C Trust Targeted Testing Amongst the South Asian Community in Bradford Dr Sulleman Moreea, Consultant, Bradford Royal Infirmary Peer Support for People affected by Hepatitis C – The Grimsby Experience Roger Tucker, Hepatitis C Support Group, Grimsby Treating People in Prison – A Joint Approach, The Leeds Model Dr Iain Brew, HMP Leeds Medical Officer and Dr Mark Hallam, Leeds Community Drugs Partnership Questions to the panel SESSION 3: WORKSHOPS

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 78
Workshops: Workshop A: Commissioning Supporting the commissioning of hepatitis services Siobhan Fahey, Project Manager, NICE and Department of Health & Becky Hug, Policy and Public Affairs Manager, The Hepatitis C Trust Workshop B: Treatment Putting strategy into practice – The Doncaster experience of setting up a treatment service Yvette Stones, Specialist Nurse – Viral Hepatitis, NHS Doncaster and Abid Mumtaz, Health Improvement Practitioner, Public Health, NHS Doncaster Workshop C: Testing Testing for Hepatitis - Which test to use? Antony Hale, Virologist, Leeds Teaching Hospitals & Lorraine Craig, Clinical Nurse Specialist, Nottingham Healthcare NHS Trust Workshop D: Peer Support Key considerations when trying to facilitate peer support Liz Butcher, Deputy Regional Manager, NTA Yorkshire and the Humber & Tina Tucker, Hepatitis C Support Group, Grimsby
Workshop feedback from groups Conclude and close

HPA Y&H | Hepatitis B and C in Yorkshire and the Humber, 2012 79