mental health cover design 101210.ppt - mfi.org · 250 mental health professionals were trained in...
TRANSCRIPT

MENTAL HEALTH
T H E M E A D O W S F O U N D A T I O Napproved by The Meadows Foundation’s Board of Directors – April 2011

2
Introduction .................................................................................................................................................. 4
Meadows Foundation Mental Health Grantmaking 2001 ‐ 2010 ................................................................. 5
The 2001 Mental Health Plan ....................................................................................................................... 6
Guiding Principles ..................................................................................................................................... 6
Grantmaking Strategies ............................................................................................................................ 6
Financial Targets ....................................................................................................................................... 7
Program Goals ........................................................................................................................................... 7
Improve Early Identification, Intervention, and Prevention ................................................................. 7
Treatment ............................................................................................................................................. 8
Public Education and Erasing Stigma .................................................................................................. 10
Culturally Appropriate Services .......................................................................................................... 11
2001 – 2010 Program Highlights ................................................................................................................. 12
Early Identification, Intervention, and Prevention ............................................................................. 12
Treatment ........................................................................................................................................... 14
Public Education and Erasing Stigma .................................................................................................. 22
Mental Health in Texas ............................................................................................................................... 24
Mental Health and Mental Illness: Points on a Continuum ............................................................... 25
Influences, Treatment, and Recovery ................................................................................................. 25
Prevalence ........................................................................................................................................... 27
New Freedom Commission on Mental Health .................................................................................... 27
Transformation Progress .................................................................................................................... 28
Access to Mental Health Services ....................................................................................................... 29
Texas Priority Population .................................................................................................................... 29
Common Disorders ............................................................................................................................. 31
Special Populations ............................................................................................................................. 33
The Economic Costs of Mental Illness ................................................................................................. 44
Key Issues ............................................................................................................................................ 45
Workforce ....................................................................................................................................... 45
Direct Services ................................................................................................................................. 53
Technology ...................................................................................................................................... 58
Mental Health Strategic Plan – The Next Ten Years ................................................................................... 60
What Have We Learned and Where Are We Going? .................................................................................. 61
3
Direct Services ......................................................................................................................................... 62
Mental Health Research & Advocacy ...................................................................................................... 63
Workforce ............................................................................................................................................... 63
Work Plans .............................................................................................................................................. 65
Monitoring and Evaluation ..................................................................................................................... 65
References .................................................................................................................................................. 66
Appendix A .................................................................................................................................................. 73

4
Introduction
This document presents the Meadows Foundation Strategic Plan for Mental Health, 2011 – 2020.
Included in the plan is a summary of the 2001 Mental Health Plan that served as a guide for MFI
grantmaking through 2010, as well as progress toward the goals and objectives of the 2001 plan. Also
included is a look at the current state of mental health in Texas which assisted in developing our mental
health goals and strategies for the next ten years. The final section of the document contains the goals
and strategies for the next ten years.

5
Meadows Foundation Mental Health Grantmaking 2001 ‐ 2010

6
The 2001 Mental Health Plan
In November of 2001 a strategic plan for mental health was approved by the Meadows Foundation
Board of Directors. The overall goal was to improve the mental health of Texans by improving mental
health services in the state. In order to achieve this goal the Foundation chose to focus on four primary
areas: identify and prevent mental health problems particularly among children and other populations
who are at high risk of developing mental illness; improve treatment and assistance to persons with
mental illness that helps them transition to and maintain full function; ensure there are culturally
appropriate and effective services to minority communities through education and outreach efforts;
and erase the stigma of mental illness through programs and projects that increase awareness of
mental health issues among the general public, employers, funders, and policy makers.
Approved in the 2001 plan was a set of guiding principles, grantmaking strategies, financial targets, and
program goals for the Foundation to follow. A summary of the principles, strategies, and targets
follows, along with progress made towards reaching the targets and goals, where appropriate.
Guiding Principles
Build on our strengths and build on what we have been doing where appropriate:
- support of mental health agencies;
- mental health services to the homeless;
- parenting education; and
- child abuse and violence prevention.
Look for opportunities to leverage our dollars for maximum impact.
Provide a leadership role in the area of foundation support for mental health.
Identify partners with similar goals to participate in joint projects.
Look for opportunities to address the underlying causes of problems.
Grantmaking Strategies
Make grants on two levels: those designed to have a statewide impact and those that focus on
regional and community needs.
We will use our website, grant guidelines, and annual report to inform prospective grantees that we
are interested in funding projects in this area.
In addition to screening eligible proposals through the grant review process, we will be proactive in
identifying programs and projects that address the Foundation’s goals.

7
Financial Targets
The 2001 strategic plan set two financial goals. The first was to increase all grants to health, including
mental health, to 20% of all annual grantmaking (approximately $6.5 million per year). During the
period between 2001 and 2010 an average of $6.5 million per year was granted in the area of health,
meeting the targeted amount.
The second financial target was to award approximately 50% of the annual health grant dollars to
mental health. Between 2001 and 2010, 228 mental health grants totaling $27.7 million were awarded
accounting for 42% of all health grant dollars. Treatment grants accounted for the largest percentage of
mental health grants (85%), followed by identification and prevention (10%), and stigma related grants
(5%). No grants were awarded in the culturally appropriate area between 2001 and 2010.
Program Goals
Improve Early Identification, Intervention, and Prevention
Mental health is central to the health and well‐being of adults and children alike. Those living with
mental disorders must be identified early and linked with effective services and supports. Children
especially require early identification and intervention in order to accomplish age appropriate
developmental tasks such as establishing healthy interpersonal relationships, succeeding in school, and
making their way in the workforce. The burdens of many disorders include life‐long effects that
encompass high psychosocial and economic costs, not only for the person with a mental illness, but also
for their family, school, and community. The prevention of these disorders is one of the most effective
ways to reduce the burdens. For these reasons, five program strategies related to improving early
identification, intervention, and prevention of mental illness were laid out in the 2001 plan:
Support mental health screening efforts in a wide variety of settings, including primary health
care sites, schools, recreation centers, malls, churches, etc.
Support programs that encourage and enable parents to nurture their children’s social and
emotional development.
Support programs that reduce child abuse that can lead to severe emotional disorders.
Support violence prevention programs and early identification of those at risk.
Work with Texas agencies and state and regional non‐profits and national and local advocacy
groups to address mental health crisis interventions, ongoing screening, and treatment services
for at‐risk populations.
Between 2001 and 2010, 31 grants were awarded in improving identification, intervention, and
prevention totaling $2,838,407.
2,000 elementary and middle school children received mental health screenings.

8
19,262 families were served with child abuse and neglect prevention and intervention services,
including parenting classes to foster good parenting skills, and in‐home visits with the most high‐
risk families.
75 workshops were held, 5 TV shorts were produced, and over 10,000 children received mental
health booklets and DVDs ‐ all of which focused on the long‐term psychological consequences of
Hurricanes Katrina and Rita on young children.
One research center was established to conduct research on brain disorders and other
neuroscience projects.
250 mental health professionals were trained in infant mental health, parent‐child visitation,
parental substance abuse, and other issues.
20 staff were hired in an effort to continue or expand services to clients.
Early Identification, Intervention, and Prevention Lessons Learned
When the state faced across the board budget cuts, prevention programs were completely cut
off. Some programs faltered and disbanded while others with diversified funding sources
struggled through and survived. It is difficult to find funding for these programs when results
aren’t realized until far into the future.
The evidence‐based Nurse‐Family Partnership program receives a state appropriation to support
its expansion around Texas. As a result, some agencies are changing their programs to
incorporate an evidence‐based approach to attract funding.
There are many different prevention efforts around the state and few standardized methods of
evaluating the effectiveness of each.
Treatment
More than one in four American adults suffers from short‐term, clinically diagnosable mental disorders
in a given year. These disorders, which include depression, are the leading cause of disability among
U.S. workers under age 45. Unfortunately, less than half of those in need get treated. And those who
seek treatment typically do so after a decade or more of delays, during which time they are likely to
develop additional problems. To make things worse, the treatment that most people receive is usually
inadequate, which results in an escalation of costs to the individual and society in the form of lost wages
and productivity, incarceration, homelessness, and mortality. For these reasons, the following
treatment strategies were laid out in the 2001 plan:
Support research that leads to new medical treatments for brain disorders.
Support the development and dissemination of drug therapies that treat mental health
disorders.
Support programs that target homeless persons who have serious mental illness.

9
Support programs that provide supportive housing and vocational opportunities for persons
with mental illness to enable them to live productively and independently.
Increase mental health services for criminal justice and juvenile justice clients.
Support community‐based jail diversion programs for juveniles and adults with serious mental
illnesses.
Strengthen the mental health services delivery system by building the capacity of community‐
based agencies to provide mental health services.
Between 2001 and 2010, 187 grants were awarded for improving treatment totaling $23,342,396.
Over 88,000 children and adults served by mental health treatment programs.
Nine grants were awarded to direct service providers to provide over 4,500 Hurricane Katrina
evacuees with needed mental health services.
22 new buildings were acquired, 26 buildings were renovated, and 36 new homes and
supportive housing units were built to expand services for mentally ill children and adults.
Over 5,800 professionals and volunteers received training to work with abused and neglected
children.
One women's mental health center was established to provide diagnostic and treatment
services, research, and teaching opportunities to improve mental health services to girls and
women.
13 interactive video conferencing sites established to increase access to clinical supervision and
consultation.
Treatment Lessons Learned
The shortage of mental health professionals, especially in less urban areas, greatly impacts
access to treatment.
The use of technology has increased to help serve individuals in less populated areas.
Integrated primary and mental health care is a recognized best practice in Texas and around the
United States and can greatly impact the quality of life of a person with mental illness.
Because the Texas public mental health system restricts services to those who have severe
depression, bi‐polar disorder, and schizophrenia, smaller agencies are trying to serve everyone
else. Licensed social workers/professional counselors may be the best way to provide care to
large numbers of individuals in an affordable manner.
Jails and prison systems have a high percentage of inmates with mental illnesses. Some
counties are implementing specialized courts to ensure individuals are diverted to treatment
instead of the jail.
When MFI layers its support among various entities to advance a project, positive outcomes
result. MFI’s work in diverting individuals with mental illness from jail into community‐based

10
treatment included convening and participating in meetings, granting funds to strengthen an
instant messaging system used in the courts to identify individuals who receive mental health
treatment, and providing funds for re‐entry services benefitting ex‐offenders.
Public Education and Erasing Stigma
Mental disorders do not discriminate based on age, economic status, race, creed, or color. During the
course of a year, more than 57 million Americans are affected by one or more mental disorders. There
are numerous obstacles, however, that prevent these Americans from receiving the help they need.
Stigma is one of the more formidable barriers to seeking proper treatment, services, and supports
needed. Stigma and discrimination leads others to avoid living, socializing or working with, renting to, or
employing people with mental illnesses. Stigma leads to low self‐esteem, hopelessness, and
embarrassment. And it deters the public from seeking and wanting to pay for care. For these reasons,
two strategies related to educating the public and erasing the stigma of mental illness were laid out in
the 2001 plan:
Support programs and projects that disseminate information to targeted populations and the
general public on the cause and effects of mental disorders and the issues of access and
availability of effective treatment.
Work with state agencies, nonprofits and advocacy groups to improve access to care and
eliminate disparity between general health insurance coverage and mental health coverage.
Between 2001 and 2010, ten grants were awarded in public education and erasing stigma totaling
$1,097,558.
1,063 direct service providers were trained in identifying symptoms of mental illness.
One documentary on Texas children’s mental health was completed and aired on all 13 public
television stations in Texas. The film was distributed to 2,000 public and private mental health
organizations across the state.
Over 240,000 brochures were distributed highlighting symptoms and treatments for pre and
postnatal mental illnesses.
15,000 handbooks were disseminated to educate professionals, consumers, and advocacy
groups about the legal representation of mentally ill defendants.
Public Education and Erasing Stigma Lessons Learned
A long‐term, consistent media campaign to impact public attitudes about mental health has yet
to be developed.
It is difficult to address stigma in isolation. Studies have shown that compared to education,
direct contact with someone with a mental illness leads to significant changes in attitudes and
behavior that are maintained until a month later. The attitude change is greatest when the
contact is with a person who is living in the community with a job.

11
The concept of social inclusion is gaining acceptance in the mental health community. Social
inclusion enables all individuals to participate in all aspects of society, thus encouraging an
understanding and embracing of one’s differences and similarities.
Culturally Appropriate Services
As Texas demographics change, so does the mental health system consumer base. Public and private
mental health systems are unprepared for differences in language, traditions, cultural perspectives, and
preferences for services and supports. As a result, ethnic minorities are often underserved or
inappropriately served due to poor quality of care. For these reasons, the following strategies for
providing culturally appropriate services were laid out in the 2001 plan:
Support mental health programs that have proven to be successful in serving minority
populations.
Support training for mental health professionals working in minority communities.
Between 2001 and 2010, no grants were awarded in providing culturally appropriate services.
Culturally Appropriate Lessons Learned
Cultural appropriateness can be defined differently depending on the Texas region an agency is
working in.
There is a need for the mental health workforce to reflect the cultural and linguistic diversity of
mental health consumers.

12
2001 – 2010 Program Highlights
The following section highlights notable grants awarded between 2001 and 2010 with progress made to
date. A complete list of grants awarded is provided in the Appendix.
Early Identification, Intervention, and Prevention
University of Texas Health Science Center at San Antonio
($345,000 in 2001)
MFI funds went toward the creation of the South Texas Psychiatric Genetics Research Center to improve
the identification and treatment of patients with bipolar disorder. The Center is dedicated to locating
and identifying genes associated with mental illness and the development of safe and effective
treatments for patients with psychiatric disorders. Since its inception, the Genetics Research Center has
provided psychiatric therapy and laboratory genetics training to 48 students from UT San Antonio, local
high schools and the University of Texas‐Pan American via internships, fellowships and mentoring
assignments. From September 2001 through March 2006, 2,442 subjects were recruited for protocols
which consisted of interviews and donations of a blood sample for DNA analysis. The Center’s database
on family members who are relatives of bipolar and schizophrenic subjects now contains over 10,000
entries. Much of the Center’s work revolves around the study of schizophrenia and bipolar disorder in
Hispanic populations.
Exchange Clubs of Texas
(6 grants totaling $443,560)
The Exchange Club is the oldest community service organization for business professionals in the U.S. In
1979, the national organization established child abuse prevention as its service focus. Since then,
nearly 100 child abuse prevention centers, called EXCAP Centers, have been established in the U.S.
Between 2001 and 2010, the Exchange Clubs of Houston and DFW received over $440,000 in grants
from MFI. The clubs are dedicated to preventing child abuse and neglect by giving parents and children
the tools they need to build healthy and safe relationships. With the help of MFI funds, the clubs were
able to establish more positive and loving relationships between parents and children through
numerous programs focused on peer support, in‐home mentoring of at‐risk families, and family‐focused
skills programs. Within the last nine years the two clubs served over 10,000 clients in the Houston and
DFW areas.
University of Texas at Austin
($312,500 in 2006)
The Imaging Research Center (IRC), housed within the Institute for Advanced Technology (IAT) at The
University of Texas at Austin was established to host the operation of the University’s functional

13
Magnetic Resonance Imaging machine (fMRI). The IRC is a component of UT’s interest in expanding
neuroscience research, which the fMRI makes possible. The fMRI uses a magnetic field to create 3‐D,
high‐resolution pictures of the body which can be used to research the relationship between brain
function, psychology, and other physiological systems such as cardiovascular and immunology.
Research related to Alzheimer’s disease, Post‐Traumatic Stress Disorder, methamphetamine
dependence and depression, as well as other mental disorders will be conducted at the IRC. MFI’s gift
provided support for the first two years of IRC operations, freeing up researchers to focus on gathering
enough data to receive grants from national research funding entities to cover the future costs of the
fMRI technology. Between July 2006 and June 2008 the IRC conducted over 2,100 hours of scans as part
of 62 research projects. By the end of 2009, the imaging machine was being used an average of 1,300
hours per year.
Zero To Three
($100,000 in 2008)
The Washington D.C. based Zero To Three organization launched a pilot program in 2005 to provide
developmental and mental health services to foster children age zero to three in Fort Bend County. The
program, Texas’ Court Team, is led by a coordinator that works closely with judges, the county
attorney’s office, representatives from Child Protective Services (CPS), and area service providers to
minimize stress placed on children in foster care by improving the parent‐child relationship and
increasing the likelihood that the child will be reunited with the biological parents or placed with
relatives. With MFI funding, the agency was able to hire a second coordinator to help support the
group’s activities allowing the existing coordinator to provide more intensive mental health training to
Fort Bend providers as well as provide technical assistance to El Paso, Harris, and Bexar counties which
are interested in establishing similar court teams. In 2008‐2009, 100% of the young children in Fort
Bend County CPS custody were referred to the court team and all of the cases closed during the year
resulted in children reunified with parents or relatives. In addition, over 250 judicial, legal, mental
health, child welfare, and childhood professionals across Texas have received training on the mental
health needs of children.
Texas Association for Infant Mental Health
($25,000 in 2005)
The mission of the Texas Association for Infant Mental Health (TAIMH) is to promote awareness and
develop policies and practices related to the importance of early childhood development in the first five
years of life. In 2005, the Austin‐based group received a grant from MFI to enhance the professional
development and status of persons working with young children. The endorsement process verifies that
the individual has attained a certain educational level in the child development/infant mental health
field; participated in specialized in‐service trainings; worked with guidance from mentors or supervisors;
and acquired knowledge to promote the delivery of high quality, culturally sensitive, relationship‐based
services to infants, toddlers, preschool children, parents and other caregivers. The endorsement offers

14
individuals in the field a professional development plan and verifies their professional status to
employers. As of February 2010, 23 individuals had completed the endorsement process with an
additional 104 in the process of earning endorsements. MFI’s grant also provided TAIMH with an
opportunity to increase the executive director’s hours from 10 to 20 per week and hire a part‐time
administrative assistant to help market the endorsement, receive applications, develop training
programs for volunteers and applicants with universities and community colleges. The 300‐member
organization is also active in reviewing child care licensing standards for the state, hosts an annual
conference, and trains child care workers in Corpus Christi and Dallas.
Treatment
Children’s Mental Health Services
(80 grants totaling $8,168,050)
Between 2001 and 2010, 80 grants were made to provide services related to children’s mental health. A
majority of grants supported child advocacy and child guidance centers which provide services to
children who are either directly or indirectly affected by abuse and/or violence. Due to their
experiences, victims of abuse and violence tend to be emotionally and socially behind their peers.
Mental health services provided by these centers help children regain trust and establish healthy
relationships with others. Additional grants supporting children’s mental health provided for
professional development and training of mental health professionals and support services to parents of
children with mental health needs. In total, over 52,700 individuals were impacted.
Mental Health and the Criminal Justice System
(7 grants totaling $806,516)
The Dallas County Mental Health Diversion Court project began with a $157,000 grant to Mental Health
America (MHA) Dallas in 2001 to help coordinate community efforts to appropriately and effectively
serve persons with mental illness in the criminal justice system. In the fall of 2002, MFI held a meeting
of all interested community providers to determine the steps needed to implement and receive funding
for a mental health diversion court. MFI provided a $205,000 continuation grant to MHA Dallas in 2003
for this effort. In July 2004, two mental health diversion courts were initiated in Dallas County. The
program diverts eligible offenders with serious mental health problems out of the traditional criminal
justice system and into community‐based treatment. To be eligible, an offender must be 17 years or
older and charged with a non‐violent misdemeanor offense, or a non‐violent felon on probation charged
with technical violations (e.g. failure to report to a probation officer as scheduled). As of July 19, 2007 a
total of 135 offenders were diverted for misdemeanor offenses and 124 for felony offenses.
In an effort to improve the effectiveness of the Dallas County Mental Health Diversion Court a grant for
$40,000 was made in 2005 to the Dallas Area NorthStar Authority for support of an instant messaging
communications system. The use of instant messaging in the court process ensures smooth and timely

15
communications among all the entities involved from the time an offender with mental illness is booked
into the jail system until they are diverted to a community treatment program. The system enables the
criminal justice system and community service providers to immediately respond to the needs of
individuals with mental illnesses who come into contact with the system.
A 2004 grant to Dallas County provided $53,000 for the county to contract with an outside organization
to review the quality and efficiency of health care services in the county jail. Regarding mental health
issues, the study assessed the jail’s intake processes and the diagnosis capability of the intake staff,
housing and services to inmates with mental illness within the jail, use of psychotropic drugs, and suicide
rates and the jail’s suicide prevention plan. The resulting report cited a litany of problems within the jail
including jail guards without medical training conducting medical screenings and a severely understaffed
medical team. In response to the report’s recommendations, the Dallas County Commissioner’s Court
established a committee to improve the conditions of the jail and contracted with additional consultants
to evaluate the necessary steps to meet the recommendations.
A $246,516 grant was awarded to El Paso County in 2005 to serve more offenders with mental illness in
the Mental Health Unit of the El Paso County Public Defender’s Office. The goal of the Mental Health
Unit is to move offenders with mental illness out of the criminal justice system as quickly and humanely
as possible. The therapeutic approach used by unit staff results in redirecting mentally ill offenders to
appropriate health care services in an effort to reduce rates of recidivism. Prior to MFI funding, the
Public Defender’s Office was able to serve approximately 32% of clients identified with severe
psychiatric problems. With MFI help, the percentage of clients aided increased and the results of the
program were enough to convince the County of El Paso to include the Mental Health Unit in their
annual budget.
Serving close to 9,000 homeless men, women, and children a year through health care and outreach
efforts, the Healthcare for the Homeless‐Houston (HHH) received a $105,000 grant in 2008 to expand
their services to reach even more people – those on the streets and those housed in the Harris County
Jail. For county jail inmates, HHH case management staff offer a continuum of care for homeless
persons transitioning from medical/mental health care in the jail system to the street. They also make
referrals for mental health, housing, job training and other support services to help to mitigate
recidivism. By the end of 2008, HHH had increased the number of jail inmates and releases served by
75%.
Mental Health America of Greater Dallas
(11 grants totaling $1,214,270)
Although a number of gifts have been given to Mental Health America (MHA) of Greater Dallas, three
grants awarded in the amount of $235,430 between September 2005 and January 2006 are particularly
noteworthy because they helped MHA coordinate mental health services for Hurricane Katrina
evacuees. The first grant was used to hire a Coordinator for a task force of mental health professionals
providing services to evacuees. The second grant enabled MHA to hire interviewers to assess the

16
psychiatric needs of Katrina evacuees in Dallas. The depth and urgency of need manifested by many of
the 580 individuals interviewed required immediate crisis intervention and/or case management.
Interviewers reported that besides mental health issues related to Post Traumatic Stress Disorder,
depression and/or adjustment disorders, evacuees needed immediate access to and help with
navigating critical social and health services for their families.
In response to these findings, a third grant was awarded in January 2006 to hire temporary case
management staff. Over 400 evacuees received case management services, including a referral packet
of information about medical, mental and social services in the Dallas area. Ninety percent of these
individuals (379) received mental health or medical services. Based on a follow‐up survey of the
evacuees, 90% showed an increased knowledge of referral sources in Dallas County. Many former
evacuees who have stayed in the area are receiving services as part of an agency’s regular program
efforts.
Mental Health America of Texas
($149,000 in 2005)
Mental Health America of Texas is a statewide organization that focuses on the prevention of mental
illness, education about mental health issues, and improving services for persons with a mental illness.
MFI’s grant to MHA Texas helped fund a pilot project focused on increasing access to mental health
treatment through the equalization of mental and physical health coverage in private insurance.
Funding enabled MHA to hire a staff person to encourage private corporations across the state to
voluntarily provide equal mental and physical health insurance coverage. Within the project’s two year
period (2006‐2008), 76,325 individuals received increased comprehensive mental health coverage.
Soon after, the Mental Health Parity and Addiction Equity Act of 2008 became federal law, requiring
health plans to cover treatment for mental illness on the same terms and conditions as medical
treatment. In sum, the new law requires that financial requirements (e.g., deductibles and co‐
payments) and treatment limitations (e.g., number of visits or days of coverage) that apply to mental
health benefits must be no more restrictive than the financial and treatment limitations that apply to
medical/surgical benefits. MHA Texas served as a policy advocate for the legislation, testifying for
different aspects of the law. The intent of this grant was realized on a national level and MHA continues
to serve as a resource for implementation of the legislation.
Mental Health America of Greater Houston
($58,000 in 2009)
MFI’s grant to Mental Health America of Greater Houston completed the budget for an evaluation study
into the effective strategies for developing and implementing integrated primary and mental health care
in Texas. An integrated health care system includes both physical and behavioral health care in the
same setting. Research shows that integration provides a more thorough level of care, improves
physical and mental health, and potentially lowers some health care costs. An integrated system

17
ensures primary care physicians have the necessary training and resources to treat mental health
problems and have access to mental health specialists when a referral is necessary. MHA is gathering
information from 10 providers that are currently providing integrated care. They will then examine the
different models that are used and analyze their effectiveness and how they overcame the financial and
interdisciplinary obstacles of integrating primary and behavioral health care systems. The end result will
be a template for organizations and the state to use in implementing an integrated care system in Texas.
A follow‐up study to determine improvements in care will be completed in 2012.
Metro Dallas Homeless Alliance
($1,500,000 in 2007 and $150,000 in 2009)
The Metro Dallas Homeless Alliance (MDHA) is a membership organization made up of 86 agencies that
meet routinely to collaborate on issues to fight homelessness. The organization’s purpose is to end
homelessness in Dallas through advocacy, planning, and education. MDHA’s largest success in serving
the homeless is through the Bridge Homeless Assistance Center. Based on three years of research and
observations of best practices, The Bridge runs on a state‐of‐the‐art model that provides a dynamic
entry point for homeless persons to access multiple services in one centralized site. With the capacity to
house 400 nightly, each individual is provided a case manager, medical care, counseling, and meals.
Nineteen area organizations collaborate to provide these services at The Bridge. MFI’s $1.5 million
grant in 2007 provided a quarter of the foundation support needed for the first year of operations and
encouraged others to join the effort. A second grant in 2009 went to support personnel costs of a new
Vice President of Strategic Initiatives. The vice president is responsible for building the organization’s
fund development efforts and overseeing government relations related to housing, planning,
development and communications. Since opening in May of 2008, The Bridge has provided services to
over 7,000 individuals, including securing 600 housing placements and 1,000 jobs. In addition, the
number of homeless individuals at The Bridge who now receive behavioral health care services has
increased by 31%, and the need for crisis related services, which are twice as expensive as regular
outpatient services, has decreased by 24%. Crisis related services include emergency room visits,
inpatient services, crisis stabilization, and crisis rehabilitation.
Lone Star Circle of Care
($225,000 in 2006 and $200,000 in 2010)
Lone Star Circle of Care began in 2002 under a management contract with People’s Community Clinic of
Austin (MFI grantee). In 2004, the organization was approved as a Federally Qualified Health Center
(FQHC) enabling access to federal grants, pharmaceutical discounts, and other governmental
reimbursements and programs. The clinic provides primary medical care, gynecological care, dental and
vision services as well as mental health screening to uninsured, working poor and medically underserved
individuals in Central Texas. MFI’s grant in 2006 enabled Lone Star to hire its first full‐time psychiatrist
to provide mental health services. The behavioral health department now has four board‐certified adult
psychiatrists, two licensed professional counselors, and four licensed clinical social workers. In 2009,

18
10,228 behavioral health‐related visits were provided to 1,653 unduplicated clients. MFI’s grant in 2010
went to support the clinic’s rapid expansion of its integrated health care model. Lone Star expects to
double the number of behavioral patient visits in 2010 (from 10,288 to 20,661) thanks to a new
partnership with Texas A&M Health Science Center in Round Rock. Approximately 30,000 SF of the new
A&M facility is dedicated to six clinics staffed and operated by Lone Star. To effectively serve patients,
Lone Star plans to add two additional psychiatrists to its behavioral health program and integrate an
additional 12 full‐time supporting psychotherapists into primary care clinics at Lone Star’s different
locations.
Texas Department of State Health Services, Mental Health and Substance Abuse Division
($239,000 in 2010)
In 2005, Texas was one of seven states awarded a federal Mental Health Transformation grant to
support the creation and/or expansion of the state’s treatment capacity by focusing on mental health
services that are consumer‐driven, recovery‐oriented, and supported through evidence‐based practices.
A portion of the grant was used to initiate a self‐directed care (SDC) pilot program in the Dallas area. An
SDC program enables consumers and families to play a larger role in choosing their own services,
treatments, and supports. Clients work with a case advisor to create a personalized recovery plan along
with an approved line item budget of up to $4,000 per year per client in which all expenditures are
clearly tied to recovery goals. The advisors help clients hire providers and make purchases that lead to
wellness. Although the model has not been widely used for people with severe mental illness, it has
shown good results for people with physical and developmental disabilities.
The SDC program became fully operational in May 2010 and has 88 clients who reside in the seven
counties in and around Dallas. Sixty‐six percent of the clients are female, 65% are minorities, and 50%
have annual incomes of less than $10,000. Each client can receive services for two years. The University
of Illinois at Chicago is evaluating the program. Once the evaluation is complete, the results will be used
to encourage the Department of State Health Services to expand the concept to other areas of Texas
and allocate part of the mental health budget to a self‐directed care model of service.
University of Texas Southwestern Medical School at Dallas
($810,000 in 2006)
MFI funding provided the University start‐up funding to establish the Women’s Mental Health Center
and to hire a nationally known expert to direct the center’s work which is focused on diagnosing and
treating psychiatric disorders affecting girls and women. The Women’s Center has focused primarily on
pregnancy and the peripartum period (period occurring during the last month of gestation or the first
few months after delivery). In its first year of operation, the center cared for over 900 girls and women.
Within the second year an additional 841 girls and women were served. By the third year of operation
the center doubled its original count and treated over 1,800 females. The center’s work is done in
collaboration with the community health care team at Parkland Hospital where community and home‐

19
based medical treatment and social services are provided to patients with severe medical illnesses and
psychiatric comorbidities. Work is also done in Parkland’s obstetric complications clinic in order to
address the mental health needs of patients. In addition, mental health services are provided to victims
of crime, domestic violence, torture and other traumatic events through Parkland’s Violence
Intervention Program. The center manages a multi‐disciplinary group of scientists investigating the
ethical challenges of perinatal mental health research and it is the first training site for a structured
therapy program that is used in perinatal depression.
Metrocare Services (Dallas County Mental Health and Mental Retardation)
($150,000 in 2010)
According to the Texas Department of State Health Services, the mental health workforce supply has
decreased in almost every geographic area of Texas and for almost every mental health profession. In
Texas and throughout the U.S., mental health workforce challenges include:
A shortage of workers across professional disciplines, especially in rural areas;
Difficulties recruiting new workers and retaining qualified staff;
The lack of cultural diversity among the existing workforce; and
Outdated educational content and teaching methods in professional and continuing education
for mental health providers.
In 2008, Metrocare joined forces with the Department of Psychiatry at the University of Texas
Southwestern Medical School (UTSW) to offer experiential training to psychiatry residents, psychology
students, nurse practitioners, medical assistants, and social workers. The objective was to provide
exposure to public sector mental health care and the development of professional networks within the
public sector to encourage mental health professionals to devote their careers to low‐income individuals
in need. The program offers rotations with homeless services, child and adolescent psychiatry, and dual
mental health‐developmental disability clinics for children.
To encourage more mental health professionals to enter public mental health, Metrocare expanded its
training program by offering: (1) one‐year fellowships to psychiatrists; (2) clinical training in autism and
behavior intervention; (3) training in psychiatric nursing; and (4) therapy sessions run by psychologists
for individuals with schizophrenia. MFI’s gift completed the funding needed for Metrocare to offer the
fellow and internship program to mental health practitioners and students to encourage them to offer
their skills to low‐income, less‐advantaged individuals with mental illnesses.
Turtle Creek Manor
(4 grants totaling $682,000)
Four grants totaling $682,000 were awarded to Turtle Creek Manor between 2001 and 2005. The
agency offers residential treatment services to individuals with dual diagnoses of mental illness and
chemical dependency. In 2001, MFI assisted with the merger of Herrin House and Turtle Creek Manor

20
and two programs to expand transitional housing and support services to clients who graduate from
Turtle Creek’s residential treatment program. The merger prevented the closure of Herrin House while
providing Turtle Creek Manor with a level of service it was missing between its residential program and
transitional living houses. The last grant in 2005 provided emergency support to keep the doors open
after the agency suffered governmental funding cuts. During 2005, Herrin House was sold and the
Routh Street Residential Treatment Center was renovated. By the end of 2005, the agency cut expenses
and enhanced revenues to the point that they are no longer in jeopardy of closing. In 2009, a total of
504 clients were served.
San Antonio Clubhouse
($90,000 in 2006)
The San Antonio Clubhouse is a professional self‐help program, operated by men and women recovering
from mental illness, in collaboration with professional staff. Clubhouse members engage with each
other to regain their productivity and self‐confidence, resume their lives, and re‐enter society.
Members spend their day in one of three work units: 1) the business unit to complete administrative
work; 2) the house unit to plan and prepare meals; and 3) the development unit to plan and provide
fundraising activities, community awareness, and outreach to non‐active members. The employment
program works with individuals to obtain transitional employment positions (entry‐level, 6‐9 month
positions) and supported employment positions where staff works closely with the employer and
employee to ensure job success. In 2008, thirty‐five members were aided by the employment programs
and placed in a job. In addition, participation in Clubhouse activities decreased psychiatric
hospitalization rates by 80%.
Arlington Life Shelter
($60,000 in 2002 and $199,000 in 2006)
The Arlington Life Shelter began a psychiatric telemedicine program in 2001 to provide timely mental
health services for homeless Arlington residents. The telemedicine program, which is done in
partnership with Mental Health Mental Retardation of Tarrant County, reduces the time needed to get
clients on prescribed medication from 6‐8 weeks to 7‐10 days. Once stabilized on medication, clients
are able to join the workforce and move into the agency’s two‐year transitional housing program. MFI’s
grant in 2002 enabled the program to expand from 62 patients to the program’s full capacity of 140
patients by 2004. The 2006 grant from MFI enabled the shelter to hire two part‐time counselors to
provide supplemental counseling to 48 residents in the telemedicine program and individual, family or
group counseling to 260 individuals and families who had mental health problems but did not qualify for
the telemedicine program.

21
The Network of Behavioral Health Providers
($25,000 in 2009 and $50,000 in 2010)
Sixty‐eight percent of Texas counties are designated as mental health professional shortage areas. A
recent report produced by the Network of Behavioral Health Providers found that low salaries, the
stigma of mental illness, and legislative restrictions are the major challenges for recruiting and retaining
behavioral health care personnel. It was also discovered that loan forgiveness and other incentive
programs do exist but are not well known by students or professionals in the disciplines. In an effort to
address this workforce shortage the Network designed a pilot program for Houston‐area high school and
community college students to encourage youth to study and enter behavioral health professions. The
first year of the pilot program focused on developing a behavioral health awareness curriculum for
grades 9‐11 and initiating a 10‐week psychiatric rotation for nursing students at a community college
specializing in health professions. During the first year, 678 students from a health professions magnet
high school participated in the program. A study completed at the end of the school year found that
careers as psychologists and psychiatrists were consistently preferred over social workers and
psychiatric nurses, although there was a greater recognition and knowledge about the roles of social
workers and psychiatric nurses compared to when the school year began. MFI’s 2010 grant provided
support for the second year of the program which will enable the Network to further develop its initial
efforts by expanding into additional high schools and college schools of nursing.
University of North Texas
($112,000 in 2009)
The unemployment rate for adults with serious mental illness is estimated at 90%. Many of these
individuals, however, would like to work. Unfortunately, there are few agencies within the state that
offer supportive employment services to individuals with serious mental illnesses due in part to the
stigma surrounding mental illness among employers. As a result, the Texas Department of Assistive and
Rehabilitative Services (DARS) approached the University of North Texas Department of Rehabilitation,
Social Work, and Addictions about initiating a supportive employment program specifically for
individuals with severe mental illness. The newly created program, Job Fit, provides supportive
employment services for youth and adults with mental illness in the North Texas region. The program
integrates vocational services with mental health services such as counseling and medication
management. Job Fit aims to provide rapid job placement as soon as possible after program entry and
to provide on‐going vocational support services throughout employment.

22
Public Education and Erasing Stigma
Texas Appleseed
($93,558 in 2001 and $81,000 in 2002)
In 2001, Texas Appleseed published two handbooks in English and Spanish for consumers and lawyers:
Finding Help When You’re in Trouble with the Law: A Handbook for Persons with Mental Illness and Their
Families and Mental Illness, Your Client and The Criminal Law. MFI’s grants totaling $174,558 were
awarded to Texas Appleseed to help disseminate the handbooks and to educate professionals,
consumers, and advocacy groups about the legal representation of mentally ill defendants. The
handbooks received the 2003 Ring of Honor Award from the Mental Health Association in Texas and
were replicated by Appleseed Centers in Georgia and Louisiana. In 2005, third editions of the two
handbooks were released, along with two new books: Opening the Door: Justice for Defendants with
Mental Retardation: A Handbook for Attorneys Practicing in Texas and Finding the Path to Equal Justice:
A Handbook for Defendants with Mental Retardation and Their Families. Between 2004 and 2009, over
17,000 handbooks were distributed around the state.
Mental Health America of Greater Houston
($86,000 in 2005)
In an effort to reach more people and increase the public’s understanding of mental illness, Mental
Health America of Greater Houston received an MFI grant in 2005 to hire a Community Outreach
Specialist. The Outreach Specialist’s activities greatly exceeded the agency’s expectations by 1)
increasing the number of direct service providers receiving MHA training in identifying the symptoms of
mental illness and making effective mental health referrals for clients from 300 in 2004 to 1,769 in 2008;
2) marketing an outreach program and building relationships within the faith community, including
members of the Muslim faith; and, 3) marketing and distributing English and Spanish brochures about
postpartum disorders, expanding distribution from 50,000 in 2004 to over 231,000 by 2009. The
postpartum depression brochure is now available in Vietnamese as well. A low‐literacy (fourth grade
reading level) version of the pamphlet was incorporated into the Texas Department of Health and
Human Services’ brochure entitled Information for Parents of Newborn Children, which is distributed
across the state.
Association for Community Television (KUHT)
($107,000 in 2003)
A 60‐minute television documentary titled Children on the Brink was produced to address issues
surrounding children’s mental health care in Texas. The film focused on several issues including the
importance of erasing the stigma of mental illness, preventative measures such as modern medications
and treatments, and the toll on families of those with a mental illness in an effort to build public
support for the stressful work that families and caregivers undertake. MFI supported final production

23
and outreach expenses of the project. The outreach component included collateral materials in English
and Spanish, and effectively helped establish the film as a central document for Texas‐based community
organizations. The documentary was broadcast on 12 of the state’s 13 public television stations and
over 2,000 videos were distributed to Texas legislators, community mental health centers, school
districts, residential treatment facilities, juvenile probation departments, and other individuals.

24
Mental Health in Texas

25
Mental Health in Texas
Mental Health and Mental Illness: Points on a Continuum
The 1999 U.S. Surgeon General’s Report on Mental Health defines mental health as a state of successful
performance of mental function, resulting in productive activities, fulfilling relationships with other
people, and the ability to adapt to change and to cope with adversity. From early childhood until death,
mental health is the springboard of thinking and communication skills, learning, emotional growth,
resilience, and self‐esteem – all of which are the ingredients of an individual’s successful contribution to
society.
On the other end of the continuum is mental illness, a term that refers collectively to all diagnosable
mental disorders. The Surgeon General’s report defines mental disorders as health conditions that are
characterized by alterations in thinking, mood, or behavior (or some combination thereof) associated
with distress and/or impaired functioning. These alterations contribute to a host of problems—patient
distress, impaired functioning, heightened risk of death, pain, and disability, or loss of freedom.
Texas law defines mental illness as an illness, disease, or condition, other than epilepsy, senility,
alcoholism, or mental deficiency, that:
Substantially impairs a person’s thought, perception of reality, emotional process, or judgment;
or
Grossly impairs behavior as demonstrated by recent disturbed behavior.
Influences, Treatment, and Recovery
Biological and Environmental Influences on Mental Health Years of research has revealed that an individual’s mental health is influenced by both biological and
environmental factors. The biological perspective views psychiatric disorders as a disease of the body,
specifically the brain. Brain imaging scans can reveal how specific regions of the brain are linked with
certain mental disorders by examining brain activity levels. Other research has linked schizophrenia
with abnormalities in the shape and asymmetry of the hippocampus, a part of the brain that is critical to
spatial learning and awareness, navigation and the memory of events.
Mental Health
Mental Illness
Severe Mental
Illness

26
Brain chemistry is a crucial element to proper mental functioning. Research has shown that the transfer
of chemicals in the brain, called neurotransmitters, is connected to some mental disorders. One of the
most widely supported theories in neurochemistry is the hypothesis that the positive symptoms of
schizophrenia are related to an excess of dopamine in the striatum. Additional research continues on
the link between depression and the neurotransmitters norepinephrine, serotonin, and dopamine.
In addition to biological factors, environmental factors, such as stress, influence mental health. If
individuals lack the coping resources to deal with excess stress they become vulnerable to breakdowns
in mental well‐being. Examples include stressors such as hunger and unstable family relationships which
are shown to contribute to a child’s anxiety and depression. A survey of adults who were once in foster
care revealed that 25% of those surveyed experienced Posttraumatic Stress Disorder which far exceeds
the national average of 4%.
Treatment and Recovery Despite the significant research related to biological and environmental influences on mental health,
cures for mental illness are currently limited, but successful treatments abound. In fact, between 70 and
90 percent of individuals diagnosed with a mental illness can experience relief from their symptoms and
improved quality of life with the help of medication and psychosocial treatments, such as therapy. Most
studies suggest that for major mental health disorders, a treatment approach involving both medication
and psychotherapy is more effective than either treatment method used alone.
Drug Therapy
A primary treatment for mental illness is psychoactive drugs, which are often categorized according to
the disorder for which they are primarily prescribed. For example, antidepressants are used to treat
various types of depression while mood‐stabilizing medications which include lithium are most
commonly used to treat bipolar disorder.
Psychotherapy
The second most common type of treatment is psychotherapy, or talk therapy, which helps individuals
develop effective coping mechanisms and problem solving skills. There are a variety of talk therapy
models, each designed to deal with different needs. Some examples include:
Cognitive Behavior Therapy: Changes problematic patterns of thinking or behavior;
Cognitive Analytical Therapy: Focuses on improving coping skills;
Dialectical Behavior Therapy: Focuses on learning how to react normally to emotional triggers;
Psychotherapy: Based on the client using their own insight to solve current problems;
Family Intervention: Engages the family unit as part of the therapy process;
Creative Therapies (e.g., art and drama): Used to deal primarily with emotional conflicts; and
Counseling: Being able to talk without fear of judgment or criticism.

27
Regardless of the treatment approach selected, the availability of a trained mental health workforce is
critical to improving the mental health of Texans. A shortage of mental health care providers, such as
the one the state is currently facing, limits access to treatment making recovery practically impossible.
Prevalence
Prevalence is a measure of the total number of existing cases of a condition in the population at a given
time.
According to current estimates, approximately one in four adults in the U.S. (26.2%) suffers from
a diagnosable mental disorder in a given year. When applied to 2009 U.S. Census Bureau
estimates, this figure translates to 60.9 million people.
In Texas, approximately one in four adults (over 4.3 million people) has a mental illness.
An estimated 6% of Americans (1 in 17) live with a serious mental illness (SMI) which
substantially interferes with or limits one or more major life activities.
Mental illness can affect persons of any age, race, religion, or income – there is no
discrimination.
New Freedom Commission on Mental Health
In 2002, President Bush created the New Freedom Commission (NFC) on Mental Health to examine the
inadequacies of the mental health service system. The group was charged with making concrete
recommendations for improvements that the Federal government, State governments, local agencies,
and public and private health care providers could implement immediately. In the final report,
published July 2003, the Commission described mental health care in the United States as a “system in
shambles.” The report called for a fundamental transformation of the mental health care delivery
system – a system where services are consumer and family centered and give people access to
information regarding care options. The plan additionally called for implementing mental health care
that facilitates recovery and builds resiliency so that people with mental illnesses may function
successfully in a community setting. This transformed system represented a shift in the national
approach towards the delivery of mental health care.
The Commission identified the following six principles as the foundation for achieving a transformed
system:
1. Americans understand that mental health is essential to overall health.
2. Mental health care is consumer and family driven.
3. Disparities in mental health services are eliminated.
4. Early mental health screening, assessment, and referral to services are common practice.
5. Excellent mental health care is delivered and research is accelerated.
6. Technology is used to access mental health care and information.

28
In 2005, the State of Texas received a five‐year Mental Health Transformation State Incentive Grant
(MHTSIG) from the Substance Abuse and Mental Health Services Administration (SAMHSA). The
transformation project aims to “accomplish NFC/Texas Goals statewide through the use of mental
health infrastructure innovations1 that increase effective mental health services for all Texans.” In 2006
the Texas Comprehensive Mental Health Plan (CMHP) was developed to guide the transformation
efforts. The state continues to make progress on the principles presented in the CMHP and continues to
implement plans and develop infrastructure for system transformation to continue.
Transformation Progress
Despite the state’s efforts to improve the mental health system, the prospects for people living with
serious mental illnesses remain bleak. The mental health system in Texas is chronically under‐funded,
ranking 49th in the nation in public mental health expenditures per capita. And in 2009 the state
received a D grade from the National Alliance on Mental Illness (NAMI) regarding the state’s progress
toward transforming its mental health system of care. The report, which is a follow‐up to the first
report released in 2006, looks at the progress each state is making in terms of providing evidence‐based,
cost‐effective, recovery‐oriented services for adults living with serious mental illnesses. In 2006 the
state received a C grade. NAMI attributes the drop in grade level primarily to the state’s low
commitment to supportive housing, lack of a workforce development plan, and lack of cultural
competence. The report also includes a list of urgent needs:
Equitable funding for Local Mental Health Authorities;
Improve access to services in all areas;
Expand health insurance coverage to uninsured persons; and
Address cultural competence and workforce shortage.
Without a doubt, greater investment and strong political leadership is needed in order to truly
transform the state’s mental health system and move toward a system that is evidence‐based and cost‐
effective. If not, Texas will continue a backward slide to join the rank of states with a failing grade.
1 “Mental health infrastructure innovations” are defined as novel infrastructure or the novel use of infrastructure that
increases effective mental health services.

29
Texas Adult Population
18,362,951
Adults with Mental Illness
4.3M (23%)
MH Priority Population
467,226 (11%)
MH Priority Population Served
150,057 (32%)
Private Insurance
Mental Health & Substance Abuse Division of TDSHS
39 Community Mental Health
Centers
9 Mental Health State Hospitals
1 Youth Treatment Center
Nonprofit Organizations
Public Insurance (Medicaid,
Medicare, & CHIP)
Access to Mental Health Treatment
Access to Mental Health Services
Individuals in Texas can access mental health services in a number of ways, depending upon the care
that is needed and the financial situation of the individual. Many people receive services through
employer‐provided health plans. Approximately one‐quarter of Texas residents, however, are without
insurance and therefore rely on nonprofit agencies and public mental health centers for care. The public
mental health system in Texas, which is administered by the Texas Department of State Health Services
(TDSHS), includes 39 community mental health centers, one regional managed care plan (NorthSTAR),
nine state psychiatric hospitals, and a residential treatment center for youth, ages 13 through 17.
Community mental health centers provide services within a specific geographic area of the state. The
NorthSTAR Medicaid managed care plan serves seven counties in the Dallas area. Funding for the public
mental health system is appropriated by the Texas Legislature with additional funding coming from
block grants and other federal programs.
Texas Priority Population
Adults The Texas public mental health system assigns treatment
priority to the adult population with severe and
persistent mental illnesses (SPMI). SPMIs require crisis
intervention and ongoing, long‐term support and
treatment. In Texas, severe and persistent mental
illnesses include major depression, schizophrenia, and
bipolar disorder. And because resources are limited,
decisions related to admission into public mental
health services are based on the level of functioning
and needs of the individual. Data from 2009 indicates
that approximately 32% of the potentially eligible
population received services.

30
Texas Youth Population (age 9‐17) 3,342,820
Youth with Mental Illness 735,419 (22%)
MH Priority Population
167,141 (23%)
MH Priority Population Served
40,575 (24%)
Severe & Persistent Mental Illness (SPMI)
Bipolar Disorder
Schizophrenia
Major Depression
Children and Adolescents In the U.S., approximately 7.5 million children and adolescents are affected by mental, developmental,
or behavioral disorders. These can lead to school failure, alcohol or other drug use, violence, or suicide.
Early on‐set mental disorders have been strongly associated with
reduced educational attainment.
The Texas public mental health system prioritizes
children age three to 17 with a diagnosis of mental
illness who:
Have a serious functional impairment;
Are at risk of disruption of a preferred living
or child care environment due to psychiatric
symptoms; or
Are enrolled in special education because of a
serious emotional disturbance.
In 2009, an estimated 735,419 Texas youth age nine to 17
(22% of age group) had a mental illness at some time during the
year. An estimated 23% of these youth (167,141) fell within the priority population. An even smaller
number was actually served by the public mental health system (40,575 or 24% of the priority
population).

31
Common Disorders
Major Depression
Major depression is characterized by a depressed mood that can range from feelings of dullness or
apathy to total despair. Depression can severely impair a person’s ability to function in daily activities.
The most typical and obvious symptom is a loss of interest in people, events, activities, and things that
the person formerly enjoyed. People with major depression often experience changes in body functions
such as sleep disturbances, eating problems, energy loss or agitation.
Major depressive disorder affects 6.7% of adults, or approximately 14.8 million individuals in the
U.S., including an estimated 1.2 million in Texas.
An estimated one in four women and one in 10 men will report experiencing major depression
during their lifetime.
Prior to adolescence, boys and girls are equally likely to experience a depressive episode. After
age 15, women are twice as likely as men to experience major depression.
Major depression can occur at any age, from infants to the elderly.
Schizophrenia
Schizophrenia is in many ways the most severe form of mental illness. It can be a chronic and disabling
brain disease. People with untreated schizophrenia often suffer terrifying symptoms that evoke fear in
some and withdrawal for others (e.g., hearing internal voices not heard by others, and believing that
other people are reading their minds, controlling their thoughts, or plotting to harm them). Speech and
behavior can be so disorganized that it may be incomprehensible to others.
Approximately 2.4 million American adults (1.1%), including 202,000 Texans, have schizophrenia
in a given year.
Schizophrenia affects men and women with equal frequency.
Schizophrenia often first appears earlier in men (usually in their late teens or early 20s) than in
women, who are generally affected in their 20s or early 30s.
Bipolar Disorder
People with bipolar disorder experience severe mood swings, from a manic phase to a depressive phase.
During the manic period, the person may exhibit high amounts of energy, appear both euphoric and
irritable, speak rapidly and have a short attention span, and use poor judgment.
Bipolar disorder affects approximately 5.7 million adults nationwide, including 477,000 Texans,
which represents 2.6% of the adult population.
32
Bipolar disorder occurs with equal frequency in men and women.
Onset typically occurs before the age of 35.
This disorder occurs less frequently than major depression, affecting about one in 100 people.
Obsessive Compulsive Disorder
Obsessive compulsive disorder (OCD) is an anxiety disorder characterized by recurring thoughts and
behaviors. People with OCD may be plagued by persistent, unwelcome thoughts or images, or by the
urgent need to engage in certain rituals. They may be obsessed with germs or dirt and wash their hands
over and over, or feel the need to check things repeatedly.
Approximately 2.2 million Americans, including 18,000 Texans, age 18 and older have OCD.
The median age for onset is 19; however, the first symptoms usually appear in childhood or
adolescence.
Panic Disorder
People with panic disorder have feelings of terror that strike suddenly and repeatedly with no warning.
During a panic attack, people can experience chest pain, heart palpitations, shortness of breath,
dizziness, or abdominal distress.
While the exact cause of panic disorder is unclear, there appears to be a genetic connection. In
addition, there is a higher prevalence of onset during major life transitions.
Panic disorder affects about six million (2.7%) American adults each year. An estimated 500,000
Texas adults are affected.
Panic disorder is more common in women than men and usually starts at a young age.
The disorder is widespread, affecting approximately one in every 75 persons.
Post Traumatic Stress Disorder
Post‐Traumatic Stress Disorder (PTSD) is an anxiety disorder that can develop after exposure to a
terrifying event in which grave physical harm occurred or was threatened. Traumatic events that may
trigger PTSD include violent personal assaults, natural or human‐caused disasters, accidents, or military
combat.
Approximately 7.7 million American adults, or 3.5% of the population, have PTSD. An estimated
643,000 Texas adults are affected.
A 2008 study by RAND found that an estimated 18.5% (one out of every five) of those back from
deployment in Iraq and Afghanistan reported symptoms consistent with a diagnosis of post‐
traumatic stress disorder (PTSD) or depression.

33
Long‐Term Effects of Domestic Violence on
the Abused
• Anxiety
• Chronic Depression
• Dissociative States
• Drug and Alcohol Dependence
• Repeated Self‐Injury
• Suicide Attempts
Suicide
Suicide is a tragic and potentially preventable public health problem. In 2007, it was the 11th leading
cause of death in the U.S. Specifically within Texas, 11.2 out of every 100,000 persons died by suicide in
2007. The total number of suicides was approximately 2,488, or 1.5% of all deaths.
Adverse life events and depression may lead to suicide if combined with other risk factors such as:
Prior suicide attempt;
Family history of mental disorder or substance abuse;
Family history of suicide;
Family violence, including physical or sexual abuse;
Firearms in the home;
Incarceration; and
Exposure to the suicidal behavior of others, including family members, peers, movies, fiction,
and suicides covered by the media.
Special Populations
Victims of Traumatic Events Trauma is the psychological response to one or more harmful events
that exceed an individual’s ability to cope or effectively adapt.
Experiencing a traumatic event often leaves individuals feeling angry,
depressed, hopeless, and alone. Many individuals will withdraw from
friends, family, and previously enjoyed activities. Some of the more
prominent causes of trauma include child abuse and child neglect,
domestic violence, community/school violence, disasters, sexual
assault and rape, victims/witnesses of crime, and war zone trauma. In
many cases, individuals can effectively deal with the aftermath of a
traumatic event with the help of counseling, medication, or out‐
patient services.
Domestic Violence
Between 25 and 31 percent of U.S. women, or approximately 2.6 million Texas women, report being a
victim of domestic violence at some point in their lives. Domestic violence—sometimes referred to as
intimate partner violence, domestic abuse, or battering—includes actual or threatened physical or
sexual violence or emotional abuse between adults in an intimate relationship. Domestic violence may
include psychological threats, emotional abuse, sexual abuse, and/or physical violence. Women are

34
Short‐ and Long‐Term Effects of Domestic Violence on
Children
• Anxiety
• Nightmares
• Increased Aggression
• Intense worry about their safety
• Behavior problems in adolescence (e.g., juvenile delinquency, substance abuse)
• Emotional difficulties in adulthood (e.g., depression, anxiety disorders, PTSD)
victims of intimate partner violence at a rate about 5 times
that of males. Victim interventions, which are offered through
domestic violence service agencies, include the following:
Emergency services and shelters;
Support groups; and
Individual counseling. An estimated 3.3 million children are exposed to some form of
domestic violence each year. Being witness to such violence
poses a serious threat to a child's emotional, psychological,
and physical well‐being. To make matters worse, children
living in homes where domestic violence occurs are physically
abused and neglected at a rate 15 times higher than the
national average.
For children, interventions and treatments include group and individual therapy, and dyadic treatment
with their non‐offending parent. For most children, developing a strong relationship with the non‐
offending parent is key to helping a child heal from the effects of domestic violence. Many shelters and
domestic violence service agencies offer support groups for children. These groups are important tools
in helping children to recognize that they are not alone with their worries and fears. Mental health
treatment can give children and adolescents a chance talk about and make sense of their experiences in
the presence of a caring and neutral counselor.
Child Abuse and Neglect In 2009, the Texas Department of
Family Protective Services (DFPS)
confirmed approximately 80,000 cases
of child abuse or neglect involving
68,326 unduplicated victims. Of the
confirmed cases, the most common
type of abuse was neglectful
supervision (62%). The most likely
perpetrator of abuse/neglect was a
parent (78.1%), while the confirmed
victim was most commonly a female
(51.7%). Infants have the highest rates of abuse or neglect confirmations, followed by children between
the ages of one and three.
Physical Abuse17%
Sexual Abuse8%
Emotional Abuse1%
Abandonment<1%
Medical Neglect3%
Physical Neglect8%
Neglectful Supervision
62%
Refusal to Accept Parental
Responsibility1%
Type of Abuse/Neglect
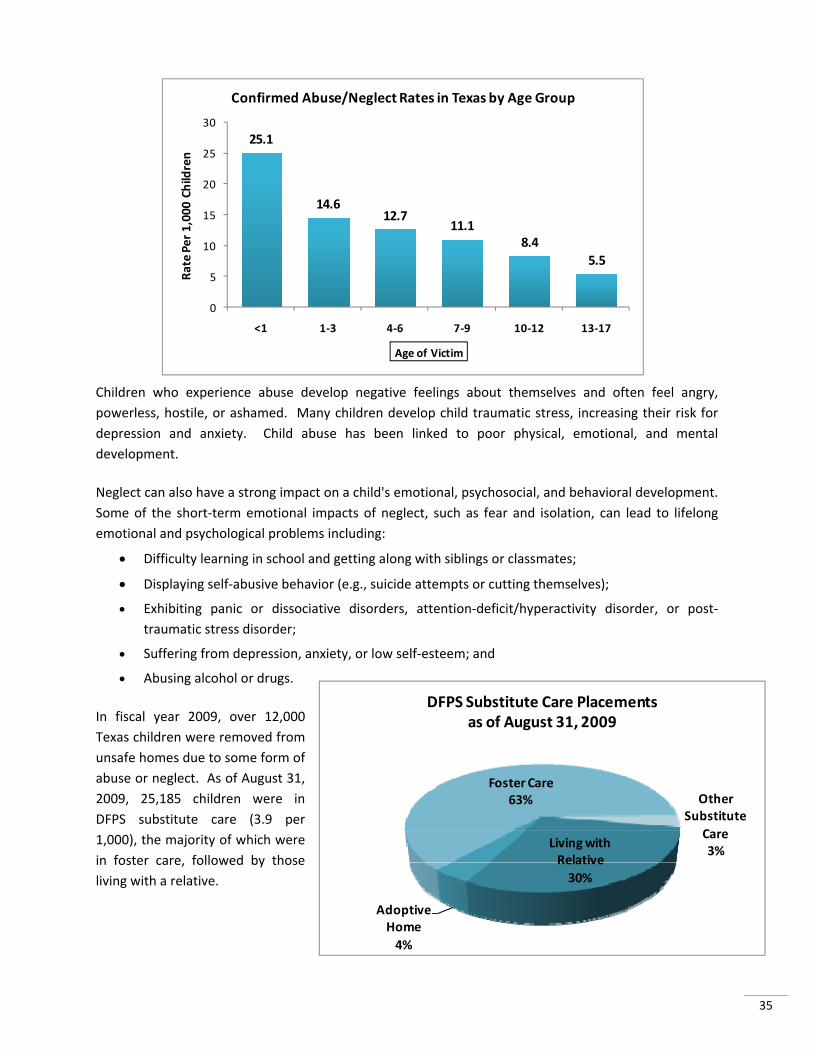
35
Children who experience abuse develop negative feelings about themselves and often feel angry,
powerless, hostile, or ashamed. Many children develop child traumatic stress, increasing their risk for
depression and anxiety. Child abuse has been linked to poor physical, emotional, and mental
development.
Neglect can also have a strong impact on a child's emotional, psychosocial, and behavioral development.
Some of the short‐term emotional impacts of neglect, such as fear and isolation, can lead to lifelong
emotional and psychological problems including:
Difficulty learning in school and getting along with siblings or classmates;
Displaying self‐abusive behavior (e.g., suicide attempts or cutting themselves);
Exhibiting panic or dissociative disorders, attention‐deficit/hyperactivity disorder, or post‐
traumatic stress disorder;
Suffering from depression, anxiety, or low self‐esteem; and
Abusing alcohol or drugs.
In fiscal year 2009, over 12,000
Texas children were removed from
unsafe homes due to some form of
abuse or neglect. As of August 31,
2009, 25,185 children were in
DFPS substitute care (3.9 per
1,000), the majority of which were
in foster care, followed by those
living with a relative.
25.1
14.612.7
11.18.4
5.5
0
5
10
15
20
25
30
<1 1‐3 4‐6 7‐9 10‐12 13‐17
Rate Per 1,000 Children
Age of Victim
Confirmed Abuse/Neglect Rates in Texas by Age Group
Living with Relative
30%
Adoptive Home
4%
Foster Care63% Other
Substitute
Care3%
DFPS Substitute Care Placements as of August 31, 2009

36
Being taken from home and placed in substitute care is a hard and stressful experience for any child.
Children living in substitute care are more likely to be economically disadvantaged, at risk for dropping
out, and in need of special education services. Research shows that between one‐half and three‐fourths
of the children entering foster care exhibit behavior or social competency problems that warrant mental
health care.
Foster children in Texas are enrolled in the STAR Health health‐care program once they enter state care.
STAR Health is a free health insurance program under which foster children have access to primary care
physicians, behavioral health clinicians, specialists, dentists, and vision services. STAR health benefits
also include coverage for hospitalizations, prescriptions and medical supplies, and telemedicine services.
Homeless Having an untreated mental illness makes it difficult to impossible to maintain employment, pay bills, or
keep supportive social relationships; all of which contribute to increasing a person’s risk for becoming
homeless. On a single night in January 2009, there were an estimated 36,761 homeless persons living in
an emergency shelter, transitional housing, or on the street in Texas. An estimated 19.5% of the 36,000
homeless are severely mentally ill.
Subpopulations of Texas Homeless, 2009
Subpopulation Sheltered Unsheltered Total
Chronically Homeless 2,741 3,279 6,020 (16.3%)
Severely Mentally Ill 4,392 2,775 7,167 (19.5%)
Chronic Substance Abuse 5,104 4,215 9,319 (25.4%)
Veterans 2,385 1,594 3,979 (10.8%)
Persons with HIV/AIDS 626 625 1,251 (3.4%)
Victims of Domestic Violence 4,050 5,917 9,967 (27.1%)
Unaccompanied Youth (Under 18) 591 893 1,484 (4.0%)
People with serious mental illnesses have a harder time overcoming homelessness than others. Because
their symptoms are ongoing and often untreated, it is extremely difficult to provide for themselves the
most basic of needs such as food, shelter, and safety. The severely mentally ill are homeless more often
and for longer periods of time than other homeless populations. And they are twice as likely to be
arrested or jailed, mostly for misdemeanors.
Veterans
Since October 2001, approximately 1.7 million military service members have been deployed for
Operations Enduring Freedom (OEF) and Iraqi Freedom (OIF) in Afghanistan and Iraq. The psychological
toll of these deployments, many involving prolonged exposure to combat‐related stress over multiple

37
212 210
174
119 116
0
50
100
150
200
250
Anxiety Disorders
Substance Abuse
Disorders
Major Depression
Mood Disorders
BH Disorders including PTSD
Rate per 100,000
‐‐‐‐‐‐Rate for Soldiers with no history of BH diagnosis = 13/100k
Suicide Rate for Soldiers Diagnosed with a Behavioral Health Disorder 2003 to 2008
rotations, is disproportionately high compared with the physical injuries of combat. A recent Pentagon
report indicates that in 2009 hospitalizations of military service members for mental disorders outpaced
those for injuries.
Unprecedented strain has been placed upon solders due to serving multiple and extended rotations, call
backs to service after leaving the military, and being held on active duty past an expected exit date. A
2008 study by the RAND Corporation found that an estimated 18.5%, or one out of every five returning
service members, reported symptoms consistent with a diagnosis of post‐traumatic stress disorder
(PTSD) or depression. The number of suicides among service members has increased every year since
2003. The Department of Veterans Affairs estimates that among veterans of all U.S. wars, 18 take their
own lives each day – an annual rate that is nearly twice the rate for civilians. A July 2010 report released
by the U.S. Army indicates that the suicide rate of soldiers is markedly higher for those diagnosed with
behavioral health disorders and PTSD than it is for soldiers who have no history of a behavioral health
diagnosis.
Through the Veteran’s Health Administration (VHA), inpatient and outpatient mental health services are
available to veterans through medical centers, community‐based outpatient clinics, and Readjustment
Counseling Centers (Vet Centers). A 2009 study conducted by RAND identified gaps in the military and
veteran’s health care systems, despite a large infusion of new funds into the Department of Defense
(DoD) and the VHA in recent years in support of improving care. Due to the gaps in the governmental
services available, many returning service members seek care in community settings as they reintegrate
into civilian life. Community‐based settings, however, aren’t without their own problems, including a
mental health workforce shortage and a lack of training in the most effective evidence‐based treatment
practices. Army representatives indicate that to end the shortage of mental health professionals within
the armed services, an additional 800 mental health counselors are needed. An even larger barrier to

38
accessing mental health care is the reluctance of military service members and veterans to seek mental
health care in the first place.
The military engagements in Iraq and Afghanistan have also adversely affected the family members of
military personnel. Many military families find themselves struggling to readjust into relationships and
parenting upon a soldier’s return home. Military divorce rates are on the rise, especially for female
service members. And with almost two million children affected by deployments more than half of the
spouses of military personnel report increased levels of fear, anxiety, and behavioral problems in their
children. Additional studies have shown that the partners of veterans with PTSD are more likely to
develop mental health problems in the future than partners of veterans without PTSD.
Texas is home to the third largest veteran population in the nation and as such, has an even larger
burden of care than most other states. There are 15 Veteran’s Affairs Vet Centers in Texas where
veterans and their families are eligible for services at no charge. State agencies and community‐based
organizations serve as a backup to help fill service gaps that veterans encounter with the VA centers.
Rural Residents Due to a chronic shortage of mental health providers, much of the burden of mental health care in rural
areas has shifted to the primary health care sector. Primary care clinicians, however, generally lack
training and time to provide proper mental health care. And with a shortage of mental health clinicians,
there are fewer experts to turn to for consultation and referrals. Rural residents, like their urban peers,
experience a wide range of mental health problems. Individuals living in rural areas, however, must
often overcome significant accessibility and availability issues compared to their urban counterparts.
Rural residents:
Travel farther to receive services;
Are less likely to have insurance coverage for mental health services;
Are less likely to recognize mental illnesses and are less knowledgeable of treatment options;
Enter care later, sicker, and with a higher level of cost; and
Have fewer available comprehensive services. The enormous size of Texas poses great difficulties for rural residents seeking access to mental health
care services. Of the 254 counties in Texas, 177 (70%) are rural counties. Rural Texas is home to over
three million people, and accounts for 213,297 of the 261,797 square miles of Texas land. Mental health
care services are in low supply in rural Texas due to a lack of resources and providers. Approximately
15% of Texans live in rural areas, while only 10% of primary care physicians practice in rural areas. For
many rural area Texans, it is not uncommon to travel 50 miles or more to see a doctor.
Approximately 90% of rural Texas counties are designated by the U.S. Department of Health and Human
Services as Mental Health Professional Shortage Areas (MHPSAs). In order to receive a MHPSA
designation, a geographic area must have:

39
A large population‐to‐mental‐health‐professional ratio;
Unusually high needs for mental health services; and
Mental health professionals in contiguous areas that are over utilized, excessively distant, or
inaccessible to residents of the area under consideration.
More detailed information related to MHPSA areas in Texas can be found in the Key Issues portion of
the report within the Workforce subject area.
The Criminalization of Mental Illness The lack of public mental health services often results in the inappropriate use of prisons as warehouses
for people with mental illness. The National Alliance on Mental Illness reports that jails and prisons are
the largest psychiatric wards in the nation, housing well over 350,000 inmates with serious mental
illness compared to approximately 70,000 patients living with serious mental illness in hospitals. This
criminalization of the mentally ill, where individuals with mental health needs are placed in the justice
system to access mental health services that are unavailable or inaccessible in the community, has been
evident at the adult level for some time; however, it is now occurring more frequently at the juvenile
level as well.
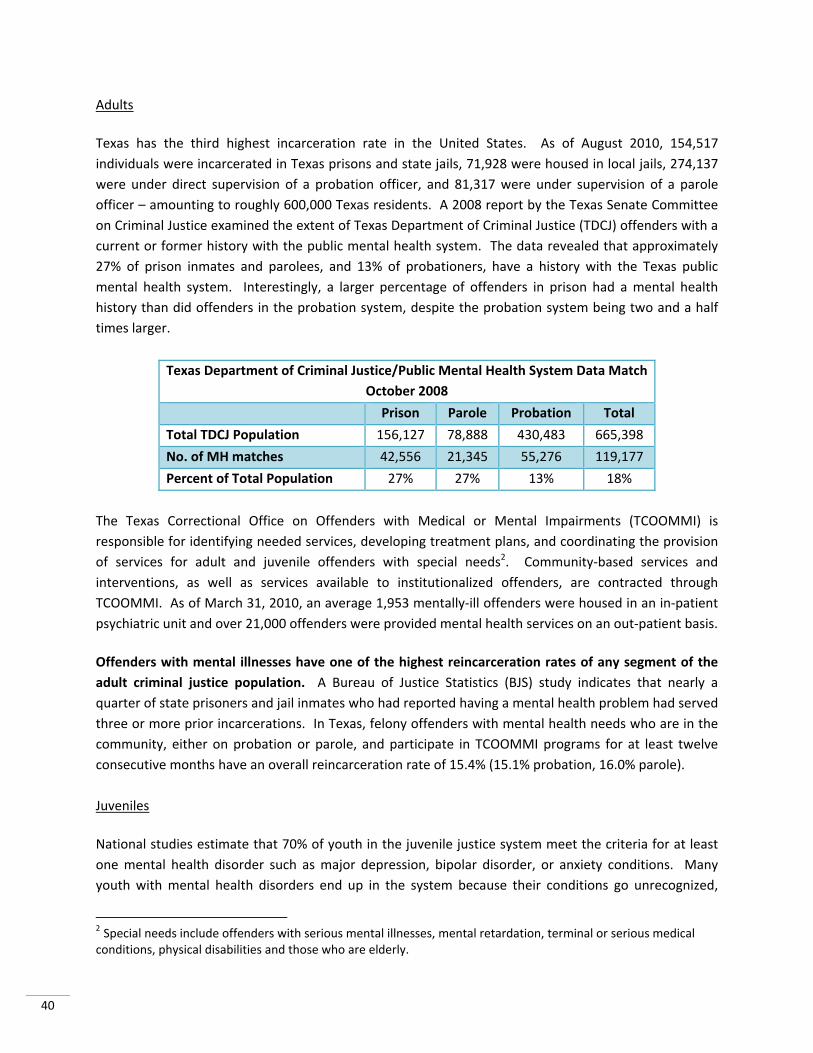
40
Adults
Texas has the third highest incarceration rate in the United States. As of August 2010, 154,517
individuals were incarcerated in Texas prisons and state jails, 71,928 were housed in local jails, 274,137
were under direct supervision of a probation officer, and 81,317 were under supervision of a parole
officer – amounting to roughly 600,000 Texas residents. A 2008 report by the Texas Senate Committee
on Criminal Justice examined the extent of Texas Department of Criminal Justice (TDCJ) offenders with a
current or former history with the public mental health system. The data revealed that approximately
27% of prison inmates and parolees, and 13% of probationers, have a history with the Texas public
mental health system. Interestingly, a larger percentage of offenders in prison had a mental health
history than did offenders in the probation system, despite the probation system being two and a half
times larger.
Texas Department of Criminal Justice/Public Mental Health System Data Match
October 2008
Prison Parole Probation Total
Total TDCJ Population 156,127 78,888 430,483 665,398
No. of MH matches 42,556 21,345 55,276 119,177
Percent of Total Population 27% 27% 13% 18%
The Texas Correctional Office on Offenders with Medical or Mental Impairments (TCOOMMI) is
responsible for identifying needed services, developing treatment plans, and coordinating the provision
of services for adult and juvenile offenders with special needs2. Community‐based services and
interventions, as well as services available to institutionalized offenders, are contracted through
TCOOMMI. As of March 31, 2010, an average 1,953 mentally‐ill offenders were housed in an in‐patient
psychiatric unit and over 21,000 offenders were provided mental health services on an out‐patient basis.
Offenders with mental illnesses have one of the highest reincarceration rates of any segment of the
adult criminal justice population. A Bureau of Justice Statistics (BJS) study indicates that nearly a
quarter of state prisoners and jail inmates who had reported having a mental health problem had served
three or more prior incarcerations. In Texas, felony offenders with mental health needs who are in the
community, either on probation or parole, and participate in TCOOMMI programs for at least twelve
consecutive months have an overall reincarceration rate of 15.4% (15.1% probation, 16.0% parole).
Juveniles
National studies estimate that 70% of youth in the juvenile justice system meet the criteria for at least
one mental health disorder such as major depression, bipolar disorder, or anxiety conditions. Many
youth with mental health disorders end up in the system because their conditions go unrecognized,
2 Special needs include offenders with serious mental illnesses, mental retardation, terminal or serious medical conditions, physical disabilities and those who are elderly.

41
community services aren’t available, or diversion from the system is not employed where appropriate.
Many also exhibit behavioral problems at school that result in disciplinary actions which can lead to
entrance into the juvenile justice system.
Juvenile’s who engage in delinquent behavior can be dealt with informally and returned home or
referred to the juvenile court. If the juvenile is adjudicated (i.e., sentenced) for his or her delinquent
conduct they may be placed on probation and released into the community or sent to a secure
correctional facility operated by the Texas Youth Commission (TYC). Approximately 95% of juveniles
sent to TYC have chronic delinquency problems and have exhausted their community‐based options.
The remaining 5% are sent directly to the agency’s care for serious offenses such as murder, armed
robbery, or aggravated sexual assault.
Juvenile probation intake is often viewed as the “gatekeeper” to juvenile court and plays a vital role in
determining whether a case is dismissed, diverted, or formally referred to juvenile court. The probation
intake process also constitutes one of the most critical points for identifying the need for mental health
services. Unfortunately, the traditional juvenile probation officer is not trained on how to identify or
work with this population of offenders. Impediments to supervising and enforcing treatment services
for offenders with mental illness include limited community resources, a lack of family and youth
support, and limited knowledge of intervention options and alternative problem solving skills.
The Texas Juvenile Probation Commission estimates that in FY 2008, 33.2% of juveniles under probation
supervision needed mental health services; however, only 37.4% of these offenders received services.
Juveniles on probation with mental health needs are often required to receive treatment through
TCOOMMI, which contracts with 21 community mental health agencies around the state. These services
include medication and monitoring, individual and/or group therapy, and family‐focused support
services. In FY 2008, over 2,100 youth were served in these community‐based programs.
The Texas Youth Commission (TYC) reports that the number of youth committed to a TYC secure facility
with severe mental health problems has increased greatly in recent years. In 2009, over one‐third (37%)
of the youth in TYC’s care were diagnosed with a serious mental health problem. TYC youth with mental
health needs can participate in a number of programs depending on the severity of need. The least
rigorous of programs are the general programs which include psychiatric and psychological support.
Youth with more severe mental health problems and illnesses may receive specialized treatment at the
Corsicana Residential Treatment Center. Youth with extremely severe problems are eligible for
admission to the Corsicana Stabilization Unit (CSU).
Similar to youth on probation, TYC parolees receive aftercare treatment services through the community
mental health programs under contract with TCOOMMI. In FY 2008, 425 TYC releases were served in
the community, up 207% from the 205 served in FY 2007.

42
Mental Health Courts
The establishment of mental health courts, which provide law enforcement, court, and corrections
systems with options other than arrest and detention of mentally ill offenders, has become increasingly
more popular over the last 20 years. These specialty courts link mentally ill offenders who would
normally be prison‐bound to long‐term community‐based treatment. Mental health courts rely on a
problem‐solving approach to court processing, the implementation of individual, community‐based
treatment plans, and on‐going judicial monitoring at which progress is periodically reviewed. The
benefits of establishing mental health courts include increasing public safety, improving the quality of
life for the offender, and making more effective use of limited criminal justice and mental health
resources.
An April 2010 evaluation of mental health courts in Dallas and Tarrant Counties showed strong impacts
on reducing repeat offending by participants of the programs. Notably, Tarrant County participants
were less than half as likely to reoffend within six months of sentencing compared to their peers not in
the program.
Cultural and Linguistic Diversity Texas is the seventh most diverse state in the nation. The Texas State Data Center (TSDC) estimates that
in 2008, Hispanics accounted for 37% of the state’s population and African Americans represented 12%,
for a total “minority” population of 49%. By 2015, TSDC projections show a combined African American
and Hispanic population accounting for over 51% of the Texas population. The state, however, is
extremely deficient in cultural and linguistic competence.
A 2001 U.S. Surgeon General report on mental health points out that culture—beliefs, norms, values,
and language—plays a key role in how people think about and experience mental illness, whether they
seek help, the quality of the services they receive, and the kinds of treatments that may work best for
them.
Numerous studies published by the Institute of Medicine and the National Alliance on Mental Illness
document that people from minority racial and ethnic communities have less access to mental health
services, are less likely to receive services, and often receive a poorer quality of care once in treatment –
despite the fact that the prevalence of mental disorders for minorities is similar to that for whites.
An effective way to reduce disparities in treatment and outcomes associated with minorities is to
provide care that is sensitive and responsive to cultural and linguistic differences. Otherwise, clinical
environments that do not respect, or are incompatible with, the cultures of the people they serve may
deter minorities from using services and receiving appropriate care.

43
Co‐occurring Disorders: Mental Illness and Substance Abuse In 2007, 28% of adults served in the Texas public mental health system were diagnosed with a co‐
occurring substance abuse disorder. Substance abuse is the most common co‐occurring condition
among adults with a mental illness.
For adults suffering from co‐occurring mental health and addiction disorders, treatment must occur for
both problems at the same time in order to reach full recovery. Research shows that co‐occurring
disorders are quite common.
Approximately 50% of individuals with severe mental disorders are affected by substance abuse.
Thirty‐seven percent of alcohol abusers and 53% of drug abusers also have at least one serious
mental illness.
Of all people diagnosed as mentally ill, 29% abuse either alcohol or drugs.
Because alcohol and drug addiction can cause symptoms that are similar to those associated with
mental disorders, such as depression, anxiety, and psychosis, physicians often fail to recognize the
presence of a co‐occurring problem. Individuals with co‐occurring disorders are more difficult to treat
as they are less stable and have a greater tendency to be noncompliant with medication. All of which
leads to a greater chance of relapse.
A study conducted by the National Institute of Mental Health shows that certain psychiatric disorders
increase an individual’s risk for substance abuse over the presence of other disorders.
Psychiatric Disorder Increased Risk for
Substance Abuse
Antisocial Personality Disorder 15.5%
Manic Episode 14.5%
Schizophrenia 10.1%
Panic Disorder 4.3%
Major Depressive Episode 4.1%
Obsessive‐compulsive Disorder 3.4%
Phobias 2.4%
Thus, someone suffering from antisocial personality disorder is at a 15.5% higher‐than‐average risk of
being an alcoholic or drug abuser. And someone who has an obsessive‐compulsive disorder is at a 3.4%
higher‐than‐average risk of being an alcohol or drug abuser.

44
The Economic Costs of Mental Illness
The direct and indirect costs of untreated or poorly treated mental disorders are substantial. The
indirect, or human, costs include reduced educational attainment, homelessness, high rate of medical
complications, and early mortality. The direct costs associated with mental illness include, among
others, losses in income and productivity, medical costs associated with treatment, incarceration costs,
and costs related to homelessness. A May 2009 assessment by The Perryman Group looked at the
adverse effects of severe mental health and substance abuse disorders on the Texas economy.
According to the analysis, the total impact of severe mental health and substance abuse issues on Texas
business activity amounts to losses of $269 billion in spending each year and 1.7 million permanent jobs.
The chart below details the costs to the state economy.
The report also highlights additional negative impacts to the state including $136 billion on gross
product, $83 billion on annual personal income, and $61 billion on annual retail sales. In addition, the
cost in terms of state tax dollars lost from the foregone activity and actual outlays (net of federal
matching and reimbursement funds) total $13 billion each year. The Perryman Group points out that if
all of these costs and losses could be eliminated, the Texas economy would be approximately 10% larger
than its current size.
Affordability and a lack of insurance is often the reason people have little or no access to care. And if
individuals are lucky enough to have insurance, current laws (such as exclusions due to pre‐existing
conditions) often create barriers to getting needed treatment. The Patient Protection and Affordable
Care Act of 2010 addresses many of the challenges people have in getting and keeping health care
coverage and offers meaningful benefits to millions of Texans who live with mental illness. Some of the
key provisions include:
‐$35,850
‐$79,734
‐$111,802
‐$4,487
‐$5,301
‐$32,169
‐$120,000 ‐$100,000 ‐$80,000 ‐$60,000 ‐$40,000 ‐$20,000 $0
Medical Expenses
Comorbidities and Disability
Lost Income and Productivity
Incarceration
Homelessness
Mortality
Billions of 2008 Dollars
Impact of Severe Mental Health and Substance Abuse Issues
on Business Activity in Texas

45
Psychiatrist A psychiatrist is a
physician with a doctor of medicine (M.D.) or osteopathic (D.O.) degree that provides a variety of medical services including medical and psychiatric evaluations, psychotherapy, treatment of psychiatric disorders, and can prescribe and monitor medications.
Psychologist Psychologists have either a master’s or
doctoral degree. Psychologists are able to provide many of the same services as a psychiatric, however, they are not able to prescribe or monitor medications. So
cial W
orker
Social workers can have a bachelor’s, master’s, or doctoral degree. Social work services include assessment and treatment, case management, supportive counseling, information and referral, hospital discharge planning, and psychotherapy.
Prohibits pre‐existing medical condition exclusions;
Extends dependent coverage up to 26th birthday;
Prohibits lifetime limits on benefits;
Establishes insurance exchanges to provide a range of choices in health coverage; and
Providing premium assistance when costs exceed certain percentages of income.
Key Issues
Workforce The current state of the Texas mental health workforce is in crisis. While a majority of counties in the
state are characterized by a shortage of mental health professionals, the state’s rural areas are impacted
the most. Leaders in the mental health industry point to extensive problems in recruiting, retaining, and
providing sufficient training of professionals. And despite being the seventh most diverse state in the
nation, racially, culturally, and linguistically diverse individuals are underrepresented in mental health
professions.
Mental Health Professionals Mental health professionals assist people dealing with psychological, emotional, and drug and alcohol
abuse problems. There are many different professions, each with its own training and area of expertise.
The most recognizable mental health careers are those of psychiatrist, psychologist, and social worker.
Additional careers in the mental health field include:
Psychiatric/Mental Health Nurse ‐ Nurses pursuing this specialization can have an associate’s,
bachelor’s, master’s, or doctoral degree. These nurses are able to provide a wide variety of
services depending on their education level and licensure. Services are very similar to those
provided by social workers except that certain levels of psychiatric nurses are allowed to
prescribe medication.

46
Licensed Professional Counselors ‐ Licensed Professional Counselors have a master’s degree in
psychology, counseling or a related field and typically have two years of post‐graduate
experience. Generally provide services that include diagnosis and counseling.
Marriage and Family Therapists – Marriage and Family therapists have a master’s degree at
minimum. These therapists deal with many issues including substance abuse, eating disorders,
depression, and other mental and emotional problems.
Some of the most successful recovery programs nationwide are adding well‐trained peers and family
members to their workforce. Peer and family support has proven effective in developing and sustaining
a culture that stays focused on recovery practices. Peers are especially important in achieving recovery
and wellness as they share their common experiences and offer support and guidance during the
recovery process. Below are some ways in which incorporating peers (including family members) into
the workforce can increase a clinical team’s performance and outcomes:
Peers can reach out and engage people unwilling to use behavioral health services. This is
especially important because only 15% of people with serious mental illnesses are estimated to
receive minimally adequate treatment.
Peers who work alongside professional staff provide living proof that recovery is possible. This
can raise morale by providing evidence to service providers that people can and do recover.
Peers provide a living example of hope for others with mental illnesses. The “if I can do it, you
can do it” message doesn't even have to be spoken—it's right before their eyes. This often
allows peers to engage and bond with people who otherwise would be reluctant to trust and
use clinical services.
Peers can free up professional staff to do other tasks that can be done only by professionals
because of licensing issues and regulations.
Texas has a training and certification program for mental health consumers who want to become peer
specialists and help others with their recovery. Once the training is completed, individuals are eligible
for jobs as peer specialists in health care centers, residential treatment facilities, state hospitals, and
other places that serve consumers.
Recruitment
Texas is experiencing a shortage of mental health professionals that will likely continue to worsen in the
future as the aging workforce begins to retire and fewer people enter the profession. As a result,
recruiting individuals to train in the mental health professions has never been more urgent. The ability
to enter a profession, however, is contingent upon the capacity of the state’s institutions of higher
education. The following table highlights the number of Texas colleges and universities offering mental
health professional education in 2010.

47
Profession Bachelor Master Doctoral Residency Training
Psychiatric Residency Training N/A N/A N/A 103
(9 university‐based, 1 hospital‐based)
Psychology 35 33 13 N/A
Social Work 22 10 3 N/A
Substance Abuse Counseling 1 N/A N/A N/A
Marriage and Family Counseling N/A 4 2 N/A
During the 2008‐09 school year, Texas universities graduated the following:
10 doctoral level marriage and family counseling therapists;
46 Master’s degree marriage and family counseling therapists;
24 doctoral level social workers;
763 Master’s degree social workers;
28 doctoral level psychologists; and
182 Master’s degree psychologists.
Once graduate‐level schooling is complete, many students encounter difficulties in completing their final
stages of training due to a shortage of internship sites available in Texas. In 2009, approximately one in
four psychology Ph.D. graduates failed to find an available internship position during the initial
internship matching phase. And many licensed professional counselor interns who are required to
complete 3,000 hours of post‐master’s training find it difficult to locate a paid internship. As a result,
many end up working multiple jobs to piece together a living wage, lengthening the training process
considerably.
Despite the number of Texas colleges and universities offering education in mental health fields, state
agencies and other employers serving persons with mental disorders have a hard time recruiting mental
health professionals. A September 2009 examination of the supply of licensed, actively working mental
health professionals in Texas highlights the problem.
3 The nine Texas universities and one hospital that have psychiatric residency programs include: Texas A&M
University, Texas Tech‐El Paso, Texas Tech‐Lubbock, University of Texas Medical Branch, University of Texas‐
Houston, University of Texas‐Southwestern (Dallas), University of Texas‐Southwestern (Austin), University of
Texas‐San Antonio, Baylor University, and John Peter Smith Hospital in Tarrant County.

48
Licensed Professional
2009 Professional
Total
Ratio of Texas Population per Professional
Ratio of Professionals per 100,000 Population
Social Worker 16,574 1,501 66.6
Professional Counselor 14,876 1,672 59.8
Marriage and Family Therapist 2,789 8,919 11.2
Psychiatrist 1,634 15,223 6.6
Psychologist 6,316 3,938 25.4 Note: The 2009 projected Texas population is 24,873,773
As indicated in the table above, only one licensed psychiatrist is actively working for every 15,223 Texas
residents. Looking at the data in terms of a supply ratio reveals a ratio of 6.6 licensed psychiatrists for
every 100,000 Texas residents. The supply ratio in New York is 35 psychiatrists per 100,000 residents.
The Health Professions Resource Center (HPRC) of the Texas Department of State Health Services (DSHS)
periodically surveys various agencies and facilities that provide public health services to determine how
many public health workers are employed and how many more are needed. Such facilities include local
health departments, federally qualified community health centers, and Texas health and human services
enterprise agencies. The results for mental health professions from the most recent staffing survey are
highlighted in the table below.
Mental Health Profession
Staffed Full‐Time Positions
Staffed Part‐TimePositions
Total StaffedFTEs
Vacant Positions
Vacancies In FTEs
VacancyRate (%)
Psychiatrists 116 33 132.5 36 32.0 19.5
Licensed Social Workers 266 6 269.0 27 25.5 8.7
Unlicensed Social Workers 63 0 63.0 1 1.0 1.6
Psychologists & Psychological Associates 251 7 254.5 45 45.0 15.0
Other Mental Health Workers 2,783 78 2,822.0 288 278.5 9.0
Total 3,479 124 3,541 397 382 ‐
With vacancy rates as high as 20% and an overall short supply of qualified mental health professionals
working in the community health clinics results in long waiting lists. Over the past five years, the
number of persons on waiting lists for community mental health services in Texas has increased from
1,394 to 6,844, representing a 386% growth.

49
A major contributing factor to the increasing number of individuals on waiting lists is the small number
of persons removed from the list each month. During the third quarter of FY 2010, the average monthly
number of persons removed from waiting lists for community mental health services was 359,
representing a five‐year high.
Mental Health Professional Shortage Areas (MHPSAs) An overwhelming majority of Texas counties are designated as Mental Health Professional Shortage
Areas (MHPSAs). There are three different types of MHPSA designations, each with its own designation
requirements: Geographic Area, Population Groups, and Facilities. As of October 28, 2010, 200 of the
254 counties (79%) in Texas were designated as whole county HPSAs for mental health purposes. Over
80% of the 200 counties are rural counties. As a result of the lack of qualified mental health care
professionals:
An estimated 6.1 million Texans are underserved by mental health professionals.
An additional 160 psychiatrists are needed to achieve a population‐to‐psychiatrist ratio of
30,000:1 in all designated mental health HPSAs in order to remove the MHPSA designation.
An additional 511 core mental health professionals are needed to achieve a population‐to‐
practitioner4 ratio of 10,000:1 in all designated MHPSAs so that the Texas population is
adequately served.
The map below highlights the MHPSA designations of Texas counties.
4 Practitioners include psychiatrists, clinical psychologists, clinical social workers, psychiatric nurse specialists, and marriage and family therapists.
1,394 1,350
2,056 2,230 2,165 2,604
3,672 3,977
5,422
6,773 6,844
‐
2,000
4,000
6,000
8,000
Number of Persons on Waiting List for Community Mental Health
Services

50
A comparison between Texas and other states similar in population size highlights the magnitude of the
mental health workforce crisis the state is facing. Texas has a total of 352 HPSAs in the area of mental
health (includes total geographic areas, populations, and facilities) while California, the closest in the
number of MHPSA designations, has 296. Texas, by far, has the largest estimated unserved population
in terms of mental health needs.
State
Total MHPSA
Designations
Estimated Unserved
Population (10,000:1)
MH Practitioners Needed to:
Remove MHPSA
Designation5
Adequately Serve
Population6
New York 148 1.4 M 35 120
Florida 154 1.6 M 81 131
California 296 3.7 M 172 326
Illinois 130 4.4 M 125 420
Texas 352 6.2 M 160 511
5 The number of additional psychiatrists needed to achieve a population‐to‐psychiatrist ratio of 30,000:1 in all designated mental health HPSAs, resulting in their removal from designation. 6 The number of additional practitioners needed to achieve a 10,000:1 population‐to‐practitioner ratio so that the population is adequately served.

51
Workforce Training A 2007 report prepared for the Substance Abuse and Mental Health Services Administration (SAMHSA)
highlights three major concerns related to the training and education of the mental health workforce:
1. The content of current training and education offerings is often not relevant to
contemporary practice;
2. Teaching methods are ineffective in changing the actual practice patterns of the workers
being trained; and
3. Access to training and education is often limited, particularly in rural communities and for
culturally diverse populations.
According to the report, graduate education, the cornerstone of professional workforce development in
mental health, has not kept pace with recent changes and critical trends in the field including resilience‐
and recovery‐oriented approaches to care; interdisciplinary team‐based practice; and use of evidence‐
based treatment and guidelines. In fact, the basic approach to health care education has not been
revamped since 1910. As a result, recent graduates are viewed as ill prepared by their new employers
and require an estimated two years of post training experience in order to develop needed knowledge
and skills.
The Hogg Foundation’s 2007 report on the mental health workforce in Texas points out that the efforts
of the state’s colleges and universities to address the deficiencies in mental health professional
education and training is unknown. And although licensed mental health professionals are required to
participate in continuing education classes, the content guidelines of the continuing education programs
are limited and in no way require courses to focus on critical, emerging issues in the field.
The population growth within racially and ethnically diverse groups in Texas has lead to an increased
demand for delivering culturally and linguistically competent care as these various population groups
perceive and use mental health services differently. Cultural and linguistic factors affect whether people
seek mental health care, how they describe their symptoms, and the duration and quality of care they
receive. As such, the state needs a diverse and culturally‐competent mental health workforce to
provide appropriate and effective treatment.
In Texas, however, racial and ethnic minorities are badly underrepresented, relative to their proportion
of the Texas population, within core mental health professions. In fact, NAMI’s Grading the States 2009
report gave Texas a score of zero in the overall cultural competence score. The report additionally
found that “Texas has no plan or activities geared toward recruiting and developing a [culturally]
competent workforce.” A comparison of the 2009 racial and ethnic makeup of Texas residents and
psychiatrists reveals that the psychiatric workforce doesn’t mirror the ethnic distribution of the
population.

52
With a lack of diversity in the mental health professions, the existing workforce requires cross‐cultural
training. Cross‐cultural training has the potential to improve quality of care and service use among
racial and ethnic populations. In Texas, however, there are no uniform standards regarding cultural
competency training. In addition, little outcome measurement has been done so it is unknown how the
cultural training of the Texas workforce has benefited the state’s racial and ethnic populations.
Retention Research related to retaining qualified mental health professionals is limited in number and scope. A
recent national study indicates, however, that the turnover rate among the behavioral health workforce
(18.5%) appears to exceed that of teachers (13%) and nurses (12%). Additional retention studies
highlight turnover rates from as low as 13% for residential treatment center workers to a high of 73%
within community health organizations.
In the Hogg Foundation’s May 2007 report, The Mental Health Workforce in Texas: A Snapshot of the
Issues, the authors point out that anecdotally, public and private mental health employers in Texas
express serious concerns regarding retention among their mental health workers. One example
provided in the report is data from the Texas Department of State Health Services’ state‐run psychiatric
hospitals. In 2006, the state psychiatric hospitals experienced a 17% turnover rate among social
workers, a 20% turnover rate among psychiatric nurses, a 14% turnover among psychiatrists, and a 14%
turnover among psychologists. The Hogg Foundation concludes that statewide data on retention rates
and initiatives relating to retaining mental health workers in Texas are not available.
White46%
African American
12%
Hispanic38%
Other/Unknown
4%
TEXAS POPULATION
White64%
African American
4%
Hispanic12%
Other/Unknown
20%
PSYCHIATRISTS

53
Transitional Housing
Provides temporary housing to help individuals and
families transition to independent living within 24 months.
Permanent Housing
Provides housing with no definite length of stay that is intended to be a home as long as a person chooses
to live there.
Direct Services It used to be that a person with a serious mental illness was thought to have a permanently disabling
condition with little hope of recovery. This school of thought believed that people with a severe mental
health disorder could never get well enough to live normal lives, have normal relationships, and
contribute to their community. We now know, however, that with proper treatment and support
systems people can live with their mental illness, and often times recover, to lead full, productive lives.
Social Inclusion Social inclusion refers to the ability to help people with a mental illness live a full, productive life and
participate fully in their communities. Providing opportunities for individuals to participate in key areas
of economic, social, and cultural life allows the mentally ill to build a life beyond their illness, which in
turns helps promote recovery. People with severe mental health problems are often poor and have
little or no income. Many lack adequate housing and end up homeless. And others find it difficult to
participate in economically or socially valuable activities such as employment and education. The
beneficial effects of improving access to the basic necessities of life, such as housing, basic education,
and employment go beyond the recipient of the services, resulting in a more productive and unified
community.
Housing
Finding adequate and consistent housing can be difficult for individuals with mental illness. As a result,
many end up homeless, living on the streets or in shelters. Contributing to a lack of consistent housing
is the absence of appropriate treatment and support, which creates many challenges for maintaining
stable employment. Without a steady income, securing housing becomes even more of a challenge.
There are two primary publically provided (government or nonprofit) housing options for homeless
individuals suffering from mental illness: transitional housing and permanent housing.

54
Transitional and permanent housing facilities can be either supportive or non‐supportive. Supportive
housing facilities provide supportive services, allowing tenants to continue on their path to self‐
sufficiency and independent living. Examples of services include intensive case management, life skills
training, counseling services, basic health care, and employment and education services.
Permanent supportive housing has shown the most success at helping people establish independent
living. As a proven, national strategy for ending chronic homelessness for the most vulnerable
populations, more than 80% of residents in permanent supportive housing stay for at least one year,
incarceration rates decline by 50%, emergency room visits decrease by 50%, and earned income
increases by 50%. Aspects of a permanent supportive housing unit include:
The tenant pays no more than 30‐50% of household income towards rent.
The tenant has access to comprehensive services including medical, mental health, substance
abuse, employment, money management, and life skills.
The use of services is not a condition of ongoing tenancy.
The tenant signs a lease agreement and there are no limits on a person’s length of stay as long
as they abide by conditions of the lease.
In 2009, 4,468 or 2.2% of public mental health care consumers in Texas lived in some form of supportive
housing. The 2009 inventory of existing housing units in Texas totaled 7,070 permanent supportive
housing units (873 of which were under development) and 7,236 transitional units (44 of which were
under development). It is estimated, however, that the state faces a shortfall of over 18,000 permanent
and transitional housing units to meet the needs of homeless Texans.
Due to the limited supply of transitional and permanent housing, boarding houses have developed as an
affordable housing alternative for the mentally ill. An estimated 29% of boarding house residents are
afflicted with a mental disorder. A 2008 survey identified 845 boarding houses across the state;
however, boarding houses are exempt from state licensing so it is believed that many more are in
existence. And because state agencies do not have the authority to require inspection or oversight of
boarding houses, many establishments are unsanitary, not adequately heated or cooled, only offer food
sporadically, and are in need of critical repairs. Due to the poverty and disabilities associated with
mental illness, many boarding house residents have nowhere else to turn.
Employment Many individuals living with a mental health disorder are unemployed, despite a willingness and ability
to work. In fact, the unemployment rate for individuals with a serious mental illness is 90%, which is far
higher than the 50% unemployment rate for physically disabled individuals. The lack of available work is
due in part to a workforce that is uneducated about mental illness and discriminatory in its treatment of
individuals with mental illness. For those employers that do hire individuals with mental illness many
report an attendance and punctuality rate that exceeds the norm and the level of motivation, work
quality, and job tenure is as good as or better than that of other employees.

55
Physical Health Care
Mental Health Care
One model of rehabilitative services centered on providing employment opportunities for the mentally
ill is the “clubhouse model.” The clubhouse model, which focuses on the participation of club members
in their own recovery process, provides paid employment opportunities in local community businesses
for members who want work. Clubhouses have seen significant improvements in the well‐being of their
members, along with decreases in the number of hospitalizations and incarcerations. The International
Center for Clubhouse Development (ICCD) provides guidance and support, as well as certification, for
clubhouses across the United States and overseas. Texas is home to five clubhouses: Austin Clubhouse
in Austin; Our House San Antonio in San Antonio; St. Joseph Clubhouse and The Gathering Place in
Houston; and The Well Community in Dallas.
In 2009, approximately 16% of public mental health care consumers in Texas indicated they were
employed at the time of receiving services.
Integrated Health Care
Many individuals rely on their primary care physician to diagnose and treat mental health problems. In
fact, the majority of mental health treatment is provided by primary care physicians. Unfortunately, in
the primary care setting mental health problems are frequently undetected or treated at a level below
the recommended quality of care. And individuals with a mental illness who seek care from a mental
health professional are less likely to receive primary medical care. Because psychiatrists generally do
not conduct physical examinations or obtain and monitor vital signs, they fail to recognize more than
half of the existing medical conditions in their patients.
Many people will experience a combination of physical and mental health problems over their lifetimes
and go untreated, resulting in poorer outcomes. Individuals with illnesses such as diabetes and heart
disease, for example, are more prone to depression and anxiety which impairs their ability to follow
doctors’ orders, take medications, and make positive life changes. Higher mortality rates are another
consequence of mental illness as many forsake primary care treatment. Texans with severe mental
illnesses such as bipolar disorder and schizophrenia die nearly 30 years earlier than the general
population. Sadly, nearly two‐thirds of these deaths are
caused by treatable physical illnesses.
There is no health without mental health.
Mental health and physical health care should
be integrated at all levels. An integrated health
care approach does just that, including both
physical and behavioral health care in the same
setting. Research shows that integrated care
provides a more thorough level of care, improves
physical and mental health, and potentially lowers some
health care costs. As a result, integrated care has become a national movement.
Integrate
d
Health
Care

56
Referrals Physicians make
agreements with mental health providers, to whom they refer their patients with mental health needs.
Co‐location Physicians and
mental health professionals are housed in the same facility so that patients can receive medical and mental health services in the same clinic.
Collaborative Care Physicians partner
with mental health providers to collaborate in the treatment of individuals in the primary care setting.
Integrated health care can be defined in many ways and approaches to integrated care vary in the
extent to which they are truly integrated. The most common models of integrated health care focus on
referrals, co‐location of services, or collaborative care.
With the referral approach, physical health care providers develop agreements with mental health
providers, to whom they refer their patients with mental health needs. Researchers have found that
patients often fail to follow through with their mental health referral so the integrated referral approach
incorporates supports that are designed to increase the likelihood of follow through. Examples of
supports include free transportation, follow‐up reminders, and coordination of care between the
primary care and mental health care providers. In a co‐location model, physical health care providers
and mental health providers are housed in the same facility, with the idea that the proximity of these
services will make it easier for people to access care for their physical and mental health problems.
While co‐location allows for increased opportunities for collaboration between the mental health
specialist and primary care provider, co‐location alone does not ensure this collaboration exists.
Collaborative care partners physical health providers, behavioral health care managers, and consulting
psychiatrists in the primary care setting to manage the treatment of moderate to severe psychiatric
disorders. The care managers, which are trained mental health professionals, regularly monitor a
patient’s treatment response and meets regularly with the consulting psychiatrist. Collaborative care
may include brief psychotherapy, or simply medication management and patient education. Over 20
years of research supports collaborative care as the most effective model of integrated health care. It
has been shown to decrease mental health symptoms and improve psychosocial functioning and quality
of life.
In 2009 the Texas Legislature established the Integration of Health and Behavioral Health Services
Workgroup to recommend best practices in policy, training, and service delivery for the promotion of
integrated health care in Texas. The workgroup submitted its final recommendations to 81st Texas
Legislature in August 2010. Recognizing there are numerous barriers to integrated health care in Texas,
the final report highlights the barriers and offers possible solutions for each. The group concludes with a

57
call for the state to address the barriers impeding integration to more effectively meet the health care
needs of Texans.
Self‐Directed Care The profession of medicine has become more collaborative, with a greater emphasis placed on patient
self‐care and choice, and greater recognition of the contribution of patients as experts in their own
conditions. Self‐directed care seeks an active partner in the consumer regarding recovery decision
making and provides individuals with more choice and control over the services they receive. A self‐
directed support program allows a mentally ill person to:
live independently;
stay healthy;
have more control over their own life;
maintain the family unit;
participate in the community as an equal citizen;
have the best quality of life irrespective of illness or disability; and
retain maximum dignity and respect.
A mainstay of the self‐directed care model is the development of individualized recovery plans. The
recovery plans include goals related to treatment and person‐centered activities such as going back to
school, obtaining employment, or buying a home. A personal budget is then created which allows
individuals to choose the best ways to support and achieve their goals. Each program participant
receives guidance and support from program personnel to help purchase the services and goods
contained in their recovery plans. Research shows that participants of self‐directed care programs tend
to receive more services and exhibit higher consumer satisfaction than their non‐participating
counterparts.
Patient Protection and Affordable Care Act of 2010
On March 23, 2010, the Patient Protection and Affordable Care Act was signed into law by President
Barak Obama. When fully implemented, the law will provide access to health insurance coverage for
Americans who are currently uninsured. As currently written, the Act recognizes that prevention, early
intervention, and treatment of mental disorders are an integral part of improving and maintaining
overall health. The passage of the Act assures that mental health services provided to newly covered
individuals are provided at parity and consistent with the 2008 Mental Health Parity and Addiction
Equity Act.
Under the Affordable Care Act, the Medicaid program will play an increasing role in the financing and
delivery of mental health services. Although it is unclear at this point how health care reform will be
fully implemented, the Act expands Medicaid eligibility to individuals with incomes below 133% of the
federal poverty level in 2014. As more individuals become eligible to seek mental health care from

58
health care providers due to the Medicaid expansion, there will be a great need for increased access to
quality care.
Technology Technology is being used in new and innovative ways to address a number of issues discussed above,
including health care provider shortages and providing direct services. For Texans in remote areas, the
use of technology helps improve access and coordination of mental health care when services are
limited. The use of technology is also known to positively influence job satisfaction and thus improve
retention. Overall, technology can help insure people with mental disorders receive timely, appropriate,
and needed services.
Telemedicine
Telemedicine is the use of telecommunications technology to provide, enhance, or expedite health care
services, by accessing off‐site databases, linking clinics or physicians' offices to central hospitals,
transmitting medical data such as x‐rays or other diagnostic images for examination at another site, and
using audio and video equipment which permits real‐time interaction between a patient and
practitioner.
Telepsychiatry, which is the application of telemedicine to the field of psychiatry, is one of the most
successful discipline‐based telemedicine applications thus far. Telepsychiatry is the specific use of
videoconferencing between a patient and psychiatrist in two separate geographic locations. It is most
commonly utilized in isolated and medically underserved areas, as well as prisons. During fiscal year
2010, Community Mental Health Centers in Texas provided 22,600 mental health service encounters via
telemedicine means. The majority of these encounters were assessment related or medication visits.
In 2006, the state implemented a pilot project to allow Medicaid recipients residing in rural or medically
underserved areas to receive mental health services via telemedicine. An evaluation of the program
revealed increased access to mental health services and an increased use in telemedicine services. The
evaluation also indicated no significant difference in clinical outcomes for clients receiving services via
telemedicine versus those who received face‐to‐face services, therefore, highlighting the equal
effectiveness of both types of service delivery methods. A March 2008 survey of community mental
health clinics revealed, however, that only 50% of the clinics use telemedicine services. Since the
success of the pilot program, the use of telemedicine by Medicaid recipients has transitioned from pilot
status to general Medicaid telemedicine policy and the state Health and Human Services Commission
continues to encourage the use of telemedicine to increase access to care.
Electronic Health Records (EHRs)
The movement towards electronic health records (EHRs) is important in the success of mental health
care across the state. An EHR provides real time patient health information and an immediate health
history for providers. For people with mental illness, who often interact with large numbers of

59
providers, EHRs facilitate information exchange that increases the efficiency of care. The use of EHR
systems is also beneficial for mental health service providers. Benefits include improved reporting
capabilities, enhanced quality assurance, improved productivity, and reduced billing errors.
Texas state psychiatric hospitals have implemented the use of an electronic health records system that
tracks all components in the hospital, including patient admission, transfer, discharge, billing,
progress/care documentation, and pharmacy orders. Texas law allows for the exchange of state hospital
client information with community mental health providers to provide better care. Nationally, however,
only two in ten doctors and one in ten hospitals use a basic electronic record system.
Recognizing the importance of widening the use of health information technology, the U.S. Congress
passed the Health Information Technology for Economic and Clinical Health (HITECH) Act in February
2009. To qualify for the Medicare and Medicaid incentive payments authorized by the act, providers
must show “meaningful use” of EHRs, including patient demographic and medical history information,
clinical decision support, physician order entry, and information about health care quality. Physicians
can receive incentives of up to $44,000. Psychiatrists and nurse practitioners who provide mental
health services at community mental health centers are eligible for the incentive payments. The bill,
however, excludes clinical psychologists, clinical social workers, psychiatric hospitals, mental health
treatment facilities, and substance abuse treatment facilities from receiving incentive payments.

60
Mental Health Strategic Plan – The Next Ten Years

61
What Have We Learned and Where Are We Going?
Since the approval of mental health as an initiative in 2001, the Foundation has developed effective
partnerships with the public and private sector, and at the local and state level. Over the last ten years
we have made the most gains in the area of treatment, which is where the greatest area of opportunity
and need has been presented. We have also had considerable success in helping maintain child abuse
and domestic violence prevention programs during financial crises. While we have been less successful
in addressing the issue of stigma, it remains an important and relevant area. With our work in mental
health over the last ten years we have gained experience and insight in the following:
We are now poised for the next ten years to build upon our knowledge base, skill set, and relationships
to be even more programmatically effective.
We can contribute to providing better mental health services by supporting evidence‐based and best
practice models that demonstrate significant opportunity for improving the outcomes and increasing
access for Texans diagnosed with a mental illness. We recognize there is a growing need to increase the
size of the mental health workforce and retain qualified professionals to meet current and future
workforce needs. There is also a need to promote excellence in research and policy recommendations
in mental health and advocacy for those who need us most. Finally, we recognize there are
opportunities to find an intersection between our mental health grantmaking and grants to reduce
crime and recidivism.
While this plan does not specifically address services for individuals with cognitive disabilities (e.g.,
Asperger’s Disorder, Autism, Fragile X Syndrome, etc.), the Foundation will continue to support this
population and their needs as a part of our health‐related grantmaking activities.
It is recommended that the Foundation adopt the following overarching goal:
Meet the needs of individuals with mental illness and those at risk of developing mental illness throughout Texas.
Supportive Housing
Integrated Health Care
Diversion Programs
Peer and Family Support
Self‐directed Care

62
To achieve this goal, we recommend the adoption of the following objectives and strategies:
Direct Services ‐ Through our competitive grant process, support direct services to individuals with
mental illness and to those at risk of developing mental illness.
I. Objective 1: Increase public mental health services to serve an additional 37,000 adults, thus
raising the percentage of the adult priority population7 receiving services from the current 32%
in 2009 (150,057) to 40% (186,890) by 2020.
a. Strategy 1: Maintain and expand best practice treatment services with priority given to
full and partial Mental Health Professional Shortage Areas8.
i. Measure the number of proven treatment service programs supported.
ii. Measure the number of adults in the priority population served.
II. Objective 2: Increase public mental health services to serve an additional 10,000 youth, thus
raising the percentage of the youth priority population9 receiving public mental health services
from the current 24% in 2009 (40,575) to 30% (50,142) by 2020.
a. Strategy 1: Maintain and expand best practice treatment services with priority given to
full and partial Mental Health Professional Shortage Areas.
i. Measure the number of proven treatment service programs supported.
ii. Measure the number of youth in the priority population served.
III. Objective 3: Create alternative court systems to divert juveniles and adults from the criminal
justice system to appropriate community mental health systems10.
a. Strategy 1: Survey current court diversion systems throughout Texas.
b. Strategy 2: Based upon survey results, provide direct financial assistance to eliminate
service gaps within the diversion systems.
i. Measure the dollar amount given to eliminate service gaps.
c. Strategy 3: Identify communities without court diversion systems and promote the
development of appropriate systems (e.g., Dallas Mental Health Court funded by MFI).
i. Measure the number of new diversion systems developed.
IV. Objective 4: Maintain and expand proven intervention programs for individuals at high risk of
developing mental illness or severe emotional disorders.
a. Strategy 1: Priority given to programs providing counseling to adult and child victims of
trauma, abuse, and violence.
i. Measure the number of counseling programs supported.
ii. Measure the number of adult and child victims served.
7 The Texas public mental health system assigns treatment priority to the adult population with severe and persistent mental illnesses (SPMI). SPMIs include major depression, schizophrenia, and bipolar disorder. 8 There are three different types of Mental Health Professional Shortage Area designations, each with its own designation requirements: Geographic Area, Population Groups, and Facilities. 9 The Texas public mental health system prioritizes children age three to 17 with a diagnosis of mental illness who have a serious functional impairment; are at risk of disruption of a preferred living or child care environment due to psychiatric symptoms; and are enrolled in special education because of a serious emotional disturbance. 10 Recognizing the intersection of criminal justice and the mental health system, we will give special attention to programs and opportunities for creating more diversion courts.

63
b. Strategy 2: Priority given to parenting programs targeting families with young children
at high risk for abuse and neglect.
i. Measure the number of parenting programs supported.
ii. Measure the number of families served.
Mental Health Research & Advocacy – Establish the Meadows Mental Health Institute as a premier
resource and driver of change to create and promote a vision of high quality mental health care in Texas
through research, evaluation, training and policy development.
I. Objective: Establish a comprehensive mental health institute (a think tank) that takes a broad
view of mental health care with the capacity to:
a. Conduct expert research and evaluation in critical content areas facing mental health
care such as financial supports, service delivery models, workforce development (e.g.,
collect data on the race/ethnicity of mental health service providers, assess current
training programs, and determine turnover causes/rates among mental health
professionals), and other areas as changing circumstances require;
b. Disseminate research findings and policy recommendations through publications,
professional meetings, and public media to federal and state agencies, community and
faith‐based organizations, nonprofit and for‐profit companies, consumer and family
groups, and other mental health care stakeholders;
c. Develop practical applications/guides for practitioners; and
d. Promote advocacy around public policies that support appropriate funding levels for the
public mental health sector and the delivery of high quality mental health care.
Workforce ‐ Through our competitive grant process, recruit and retain mental health professionals to
meet current and future workforce needs.
I. Objective 1: Recruit at least 511 core mental health professionals11 to achieve a 10,000:1 ratio
in order to reach and maintain an adequate workforce to meet the mental health needs of
Texans.
a. Strategy 1: Support programs that provide exposure to mental health careers at the
secondary and postsecondary academic levels and to current professionals such as
social workers and nurses.
i. Measure the number of programs supported.
ii. Measure the number of people exposed to mental health careers.
iii. Measure the number of mental health professionals exposed to public mental
health career.
b. Strategy 2: Support programs that specifically recruit culturally diverse persons into
mental health careers.
11 As of March 6, 2011 the Office of Shortage Designation, Bureau of Health Professions, Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services reported a deficit of 511 core mental health professionals in Texas. The deficit of mental health professionals will fluctuate throughout the term of the strategic plan as the state gains or lose professionals in the field.

64
Improve MH of Texans
Direct Services
i. Measure the number of programs supported.
ii. Measure the number of culturally diverse people recruited into mental health
fields.
c. Strategy 3: Provide financial incentives to attract individuals into mental health
professional education programs and careers.
i. Establish academic scholarships and other incentives to schools of social work,
nursing, and medical schools to attract a larger pool of candidates for mental
health professions.
1. Measure the number of scholarships awarded for mental health fields.
ii. Expand residency and internship programs for mental health professionals.
1. Measure the number of residency and internship programs expanded.
d. Strategy 4: Provide financial incentives to mental health professionals specifically to
practice in rural areas.
i. Measure the number of new mental health professionals practicing in rural
areas.
I. Objective 2: Retain the level of mental health professionals needed to continue to meet the
population‐to‐core‐mental‐health‐professional of 10,000:1.
a. Strategy 1: Conduct a study to determine the turnover rates of mental health
professionals in Texas and what factors increase turnover rates.
b. Strategy 2: Identify points of intervention to address the findings of the retention study.

65
Advisory Committee
We propose establishing a Blue Ribbon Advisory Committee comprised of state and national expert
practitioners, policy advocates, consumers, and consumer family members to provide guidance and
expert advice on establishing and maintaining the mental health institute. We expect to convene this
group several times during the feasibility study and at least once annually thereafter to meet with staff
and the Board of Directors.
Work Plans Upon approval of the Mental Health Plan, MFI staff will develop annual work plans for its
implementation. For each strategy, work plans will identify key activities, expectations, and budgets.
Monitoring and Evaluation Special attention will be given to monitoring and evaluating mental health grants related to the plan. All
grantees will be expected to provide foundation staff with their goals and a plan to evaluate
their activities and goals. Program Officers will be assisted by the Research and Evaluation Specialist in
reviewing these plans to determine if they will provide adequate information to the foundation as it
relates to the foundation's goals.
Special reporting requirements will be developed to ensure the foundation receives timely and accurate
information over the term of the grant.
Staff will develop a set of indicators to report progress toward goals that will be posted to the Board
page of the website and used in briefings to the Board on a regular basis.
At least annually, the Board will review progress toward the annual targets and at least every three
years review progress toward the broader goals.

66
References
The 2001 Mental Health Plan
Kingsbury, K. (2008, May 9). Tallying Mental Illness’ Costs. Time. Retrieved May 29, 2010, from http://www.time.com/time/health/article/0,8599,1738804,00.html Medscape Psychiatry & Mental Health. (2004, December 9). How Stigma Interferes with Mental Healthcare: An Expert Interview with Patrick W. Corrigan, PsyD. Retrieved October 28, 2010, from http://www.medscape.com/viewarticle/494548 National Institute of Mental Health. (2009, August 6). Retrieved June 2, 2010, from http://www.nimh.nih.gov/health/topics/statistics/index.shtml The Perryman Group. (2009). Costs, Consequences, and Cures!!! An Assessment of the Impact of Severe Mental Health and Substance Abuse Disorders on Business Activity in Texas and the Anticipated Economic and Fiscal Return on Investment in Expanded Mental Health Services. Weiss, R. (2005, June 7). Study: US Leads in Mental Illness, Lags in Treatment. The Washington Post. Retrieved June 12, 2010, from http://www.washingtonpost.com/wp‐dyn/content/article/2005/06/06/AR2005060601651.html Mental Health in Texas Ackerman, K. (2010, July 26). Mental Health Providers Excluded From Health IT Initiatives. iHealthBeat. Retrieved August 12, 2010, from http://www.ihealthbeat.org/features/2010/mental‐health‐providers‐
excluded‐from‐health‐it‐incentives.aspx#ixzz0utmfcXwS, American Psychology Association. (2010). Answers to Your Questions about Panic Disorder. Retrieved July 14, 2010, from http://www.apa.org/topics/anxiety/panic‐disorder.aspx Anthony, William. Ashcroft, Lori (2007, May) The Value of Peer Employees. PHD Behavior Healthcare. Retrieved September 22, 2010, from http://www.behavioral.net/ME2/dirmod.asp?sid=&nm=Archives&type=Publishing&mod=Publications%3A%3AArticle&mid=64D490AC6A7D4FE1AEB453627F1A4A32&tier=4&id=D4BC4B2C7DF84D7F8524AF753B6B02E3 Burnam MA, Meredith LS, Tanielian T, and Jaycox LH, Mental Health Care for Iraq and Afghanistan War Veterans, Health Affairs, Vol. 28, No. 3, May/June 2009, pp. 771‐782 Cambridgeshire County Council. (2009). Self‐Directed Support. Retrieved October 12, 2010, from http://www.cambridgeshire.gov.uk/NR/rdonlyres/D45D0F18‐29E8‐4B0A‐93F7‐A2BBB19120B4/0/SelfDirectedSupportLeafletMay09.pdf Center for Public Policy Priorities. State of Texas Children, 2009‐2010 Kids Count Data. Retrieved September 3, 2010, from http://www.cppp.org/factbook09/texas_profile.php?fipse=99999 Cook, Adrian. (2010, May). Mental Health Survey Report for The Rees‐Jones Foundation.

67
Council of State Governments Justice Center. Criminal Justice/ Mental Health Consensus Project. (2008). Improving Responses to People with Mental Illness, The Essential Elements of a Mental Health Court. Retrieved September 20, 2010, from http://consensusproject.org/jc_publications/essential‐elements‐of‐a‐mental‐health‐court/mhc‐essential‐elements.pdf Foster, L. & Brown, R. (2003, March 26). Improving The Quality of Medicaid Personal Assistance Through Consumer Direction. HealthAffairs. Retrieved March 23, 2010, cited in presentation presented by Judith Cook & Sam Shore to The Meadows Foundation Gale, John A. Lambert, David. (2006, January‐February). Mental Healthcare in Rural Communities: The Once and Future Role of Primary Care. North Carolina Medical Journal. Retrieved September 15, 2010 from http://www.ncmedicaljournal.com/jan‐feb‐06/Gale.pdf Hogg Foundation. (2008). Connecting Body and Mind: A Resource Guide to Integrated Health Care in Texas and the United States. Retrieved October 8, 2010, from http://www.hogg.utexas.edu/uploads/documents/IHC_Resource_Guide1.pdf
Hogg Foundation. (2007). The Mental Health Workforce in Texas: A Snapshot of the Issues. Retrieved September 24, 2010, from www.uta.edu/ssw/file_download/59 Hogg Foundation. Consumer, Youth and Family Perspectives. Retrieved September 22, 2010, from http://www.hogg.utexas.edu/initiatives/consumer_youth_family.html Insel, Thomas. (2008, June). Assessing the Economic Costs of Serious Mental Illness. The American Journal of Psychiatry. Retrieved September 20, 2010, from http://ajp.psychiatryonline.org/cgi/content/full/165/6/663 Domestic Violence Statistics: Prevalence and Trends. (2001). Retrieved September 20, 2010, from http://www.findcounseling.com/journal/domestic‐violence/domestic‐violence‐statistics.html L. Aron, R. Honberg, K. Duckworth et al. (2009) Grading the States 2009: A Report on America’s Health Care System for Adults with Serious Mental Illness, Arlington, VA: National Alliance on Mental Illness. Marriage and Family Therapist degree and workforce information. Retrieved September 24, 2010, from http://www.texashotjobs.org/d10.aspx Martinez, Jr. O.(2010). Integrated Healthcare in Texas should be a priority. Retrieved October 25, 2010, from http://www.statesman.com/opinion/martinez‐integrated‐health‐care‐in‐texas‐should‐be‐610116.html?printArticle=y Mental Health America. (2010). Dual Diagnosis. Retrieved September 16, 2010, from http://www.mentalhealthamerica.net/index.cfm?objectid=C7DF9405‐1372‐4D20‐C89D7BD2CD1CA1B9 Mental Health Care for Children and Adolescents in Foster Care. (February 2006). Review of Research Literature Prepared for Casey Family Program.

68
Models for Change. Mental Health/Juvenile Justice Action Network. Retrieved September 10, 2010 from http://www.modelsforchange.net/about/Action‐networks/Mental‐health‐Juvenile‐justice.html National Alliance on Mental Illness Texas. Disorders Affecting Children. Retrieved October 29, 2010, from http://www.namitexas.org/mental_illness/child_mental_illness.shtml National Alliance on Mental Illness Texas. (2003). Dual Diagnosis and Integrated Treatment of Mental Illness and Substance Abuse Disorder. Retrieved July 20, 2010, from http://www.nami.org/Template.cfm?Section=By_Illness&Template=/TaggedPage/TaggedPageDisplay.cfm&TPLID=54&ContentID=23049 National Alliance on Mental Illness Texas. (2010) Fast Facts about mental illness. Retrieved September 17, 2010, from http://www.nami.org/Template.cfm?Section=State_Advocacy&Template=/ContentManagement/ContentDisplay.cfm&ContentID=93161 National Alliance on Mental Illness Texas. (2010). Mental Health Professionals: Who They Are and How to Find One. Retrieved September 22, 2010, from http://www.nami.org/Content/ContentGroups/Helpline1/Mental_Health_Professionals_Who_They_Are_and_How_to_Find_One.htm National Alliance on Mental Illness Texas. (2009). State Report Card. Retrieved September 16, 2010, from http://www.nami.org/gtsTemplate09.cfm?Section=Grading_the_States_2009&Template=/contentmanagement/contentdisplay.cfm&ContentID=74934 National Center for Mental Health and Juvenile Justice. (2006). Blueprint for Change: A Comprehensive Model for the Identification and Treatment of Youth with Mental Health Needs in Contact with the Juvenile Justice System. Retrieved September 20, 2010, from http://www.ncmhjj.com/Blueprint/default.shtml National Center for PTSD. (2005). PTSD and Intimate Relationships. PTSD Research Quarterly. Retrieved July 20, 2010 from http://www.ptsd.va.gov/professional/newsletters/research‐quarterly/V16N4.pdf National Institute of Health. Panic Disorder. Retrieved July 14, 2010 from http://www.nlm.nih.gov/medlineplus/panicdisorder.html National Institute of Mental Health. (2009, August 6). Retrieved June 2, 2010, from http://www.nimh.nih.gov/health/topics/statistics/index.shtml National Institute of Mental Health. Obsessive Compulsive Disorder. Retrieved July 14, 2010, from http://www.nimh.nih.gov/health/topics/obsessive‐compulsive‐disorder‐ocd/index.shtml National Institute of Mental Health. Post‐Traumatic Stress Disorder (PTSD). Retrieved July 14, 2010 from http://www.nimh.nih.gov/health/topics/post‐traumatic‐stress‐disorder‐ptsd/index.shtml

69
National Institute of Mental Health. The Numbers Count: Mental Disorders in America 2010. Retrieved July 14, 2010, from http://www.nimh.nih.gov/health/publications/the‐numbers‐count‐mental‐disorders‐in‐america/index.shtml Northwestern University (2009, July 10). Map Of Your Brain May Reveal Early Mental Illness. ScienceDaily. Retrieved October 29, 2010, from http://www.sciencedaily.com /releases/2009/07/090709095431.htm New Freedom Commission on Mental Health, Achieving the Promise: Transforming Mental Health Care in America. Final Report. DHHS Pub. No. SMA‐03‐3832. Rockville, MD: 2003. Regent University, School of Psychology & Counseling. Trauma Support. Retrieved September 10, 2010, from http://www.regent.edu/acad/schcou/trauma/support/overview.htm Royal College of Psychiatrics Social Inclusion Scoping Group. (June 3, 2009). Making Psychiatric and Mental Health Services Fit for the 21st Century. Retrieved October 7, 2010, from http://www.rcpsych.ac.uk/pdf/social%20inclusion%20position%20statement09.pdf Secretary Kathleen Sebelius, Dept. of Health and Human Services. (2010, August 26). The New Momentum Behind EHRs. Kaiser Health News. Retrieved October 2, 2010, from http://www.kaiserhealthnews.org/Columns/2010/August/082610Sebelius.aspx
Substance Abuse and Mental Health Services Administration (SAMHSA). An Action Plan for Behavioral Health Workforce Development. Retrieved October 1, 2010, from http://www.samhsa.gov/Workforce/Annapolis/ExecSummaryWorkforceActionPlan.pdf Substance Abuse and Mental Health Services Administration (SAMHSA). (2008).Characteristics of State Mental Health Agency Data Systems. Retrieved October 5, 2010, from http://store.samhsa.gov/shin/content/SMA08‐4361/SMA08‐4361.pdf Substance Abuse and Mental Health Services Administration (SAMHSA). 2009 CMHS Uniform Reporting System Output Tables. Retrieved October 8, 2010, from http://www.samhsa.gov/dataoutcomes/urs/2009/Texas.pdf Substance Abuse and Mental Health Services Administration (SAMHSA). Resource Center to Promote Acceptance, Dignity and Social Inclusion. Employment (March 2009). Retrieved on October 27, 2010, from http://www.promoteacceptance.samhsa.gov/topic/employment/default.aspx Texas colleagues and universities offering mental health professional education in 2010. Retrieved September 24, 2010 from http://www.thecb.state.tx.us/ Texas Department of Criminal Justice. Texas Correctional Office on Offenders with Medical or Mental Impairments. Retrieved September 20, 2010, from http://www.tdcj.state.tx.us/tcomi/tcomi‐home.htm Texas Department of Criminal Justice. Texas Correctional Office on Offenders with Medical or Mental Impairments. (2009), Biennial Report. Retrieved September 20, 2010 from http://www.tdcj.state.tx.us/publications/tcomi/Biennial%20Report%202009%20FINAL.pdf

70
Texas Department of Criminal Justice. (2010) Agency Strategic Plan for the FY2011‐2015. Retrieved September 20, 2010 from http://www.tdcj.state.tx.us/publications/finance/FY_2011‐15_Agency_Strategic_Plan.pdf Texas Department of Family Protective Services. Data Book 2009. Texas Department of Mental Health and Mental Retardation. (2002, May). Strategic Plan, Fiscal Years 2003 – 2007. Texas Department of Rural Affairs. Rural Health Work Plan 2009. Retrieved September 13, 2010, from http://www.tdra.state.tx.us/pdfs/WORKPLAN_2009_FINAL_08_25_2009.pdf Texas Department of State Health Services. (2009, July). 17th Edition Texas Laws Relating to Mental
Health, Texas Administrative Code, Rule §571.003 ‐ Definitions, No. 14 Texas Department of State Health Services. (2008, December). Behavioral Health Services for Returning Veterans and Their Families: Services, Gaps, and Recommendations. Retrieved August 17, 2010 from http://www.mhtransformation.org/documents/reports/MHTWorkgroupReport_ReturningVeterans010809.pdf Texas Department of State Health Services. (2010, July). Behavioral Health Data Book. Retrieved September 27, 2010, from http://www.dshs.state.tx.us/mhsa/databook/DSHS%20Behavioral%20Health%20Data%20Book%20‐%20FY2010%20‐%20Quarter%203%20‐%2007‐02‐2010.pdf Texas Department of State Health Services. Health Professions Resource Center, Center for Health Statistics. Summary of Texas Public Health Professional Staffing Levels. Retrieved September 27, 2010, from http://www.dshs.state.tx.us/chs/hprc/pubhealth/summary.pdf Texas Department of State Health Services. Texas State Health Plan (2011‐2016). Retrieved October 22, 2010, from http://www.dshs.state.tx.us/chs/shcc/reports/SHP2011‐Draft.pdf Texas Department of State Health Services. (2009, September). Supply and Distribution Tables for State Licensed Health Professions in Texas. Retrieved September 27, 2010, from http://www.dshs.state.tx.us/chs/hprc/health.shtm Texas Department of State Health Services. (2005, June) Taking Care of Your Mental Health brochure. Retrieved July 14, 2010, from http://www.dshs.state.tx.us/mhnews/BrochuresMH1.shtm Texas Health and Human Services Commission. Health and Human Services System Strategic Plan 2009‐13, Volume 1. Texas Health and Human Services Commission. Report on Boarding Houses H.B. 116 January 2009. Retrieved October 11, 2010, from http://www.hhsc.state.tx.us/news/presentations/BoardingHouses_0109.pdf Texas Youth Commission. Overview of the Juvenile Justice System in Texas. Retrieved September 30, 2010, from http://www.tyc.state.tx.us/about/overview.html

71
Texas Task Force on Indigent Defense. (2010). Representing the Mentally Ill Offender. Retrieved October 15, 2010 from http://contentdm.ncsconline.org/cgi‐bin/showfile.exe?CISOROOT=/accessfair&CISOPTR=190 The Henry J. Kaiser Family Foundation. State Health Facts.org. Retrieved September 20, 2010, from http://www.statehealthfacts.org/comparetable.jsp?ind=760&cat=1&sub=150&yr=63&typ=3&sort=a The International Center for Clubhouse Development (ICCD).Clubhouse Directory. Retrieved on October 5, 2010, from http://www.iccd.org/clubhouseDirectory.php?state=Texas The National Child Traumatic Stress Network. What is Domestic Violence? Retrieved September 20, 2010, from http://www.nctsnet.org/nccts/nav.do?pid=typ_dv Three Ways to Recover from a Mental Illness. (2009, November 18). Retrieved October 12, 2010 from, http://www.livestrong.com/article/8124‐recover‐from‐mental‐illness/ Treatment and Therapy. (2010, October 5). Retrieved October 20, 2010, from http://www.rethink.org/living_with_mental_illness/treatment_and_therapy/index.html University at Albany School of Public Health. Center for Health Workforce Studies. New York Physician Workforce Supply and Distribution. Retrieved September 27, 2010, from http://chws.albany.edu/index.php?nyphysicians U.S. Army. (2010) Health Promotion Risk Reduction Suicide Prevention Report. Retrieved September 13, 2010, from http://usarmy.vo.llnwd.net/e1/HPRRSP/HP‐RR‐SPReport2010_v00.pdf U.S. Department of Health and Human Services. Administration for Children and Families.(2006). Child Neglect: A Guide for Prevention, Assessment and Intervention. Retrieved September 3, 2010, from http://www.childwelfare.gov/pubs/usermanuals/neglect/chapterthree.cfm U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. National Vital Statistics Report (2010, May 20). Retrieved September 7, 2010 from http://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_19.pdf U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. Health Data Interactive Website. Retrieved September 7, 2010 from http://www.cdc.gov/nchs/hdi.htm U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, 1999. U.S. Department of Health and Human Services. Health Resources and Services Administration. (2009). Shortage Designation HRSA. Retrieved September 15, 2010, from http://bhpr.hrsa.gov/shortage/

72
U.S. Department of Housing and Urban Development. (2009). HRE Continuum of Care Texas Homeless and Homeless Populations Report. Retrieved August 3, 2010, from http://www.hudhre.info/CoC_Reports/2009_tx_pops_sub.pdf U.S. Surgeon General Report. (2001). Retrieved September 15, 2010, from http://www.surgeongeneral.gov/library/mentalhealth/cre/execsummary‐6.html Zoroya, Gregg. (2010, May 16). Mental care stays are up in military. USAToday. Retrieved September 13, 2010, from http://www.usatoday.com/news/military/2010‐05‐14‐mental‐health_N.htm

73
Appendix A
MENTAL HEALTH
Treatment2001 MFI Grant Amount
Rusk County Chi ldren's Advocacy Center,
January
Toward renovating and equipping a
bui lding to provide a chi ld sens i tive
environment for treating chi ld abuse
victims
$60,450
The Bridge, Janaury Toward constructing a permanent home for
a chi ld advocacy center serving victims of
chi ld abuse
$100,000
Concho Val ley Center for Human
Advancement, MHMR Services for the
Concho Val ley, February
Toward constructing a new faci l i ty to
expand menta l health services to chi ldren
$250,000
Mental Health America of Greater
Dal las , March
To coordinate community efforts to
improve crimina l jus tice practices for
persons with menta l i l lness
$157,000
Patsy's House Chi ldren's Advocacy
Center, March
Toward purchas ing and renovating a
faci l i ty in which to offer services to chi ld
abuse victims
$25,000
Settlement Club, May Toward expanding res identia l , academic
and recreation faci l i ties for a res identia l
therapeutic program serving emotiona l ly
disturbed girl s
$247,000
American Gateways , May Toward establ i shing menta l health
services for economica l ly disadvantaged
immigrants and refugees
$125,350
Turtle Creek Manor, May Toward developing a pi lot trans itional
l i ving program for individua ls with
chemica l dependency and severe mental
i l lnesses
$250,000
Chi ldren's Advocacy Center of Hidalgo
County, July
Toward s tart‐up funds for a new program to
provide a chi ld sens i tive environment for
treating victims of chi ld abuse
$75,000
Concho Val ley Home for Girls , July Toward constructing a res idence, tra ining
center and administration/therapy
bui lding in which to expand res identia l
services for abused and neglected girl s
$150,000
Mental Health Association in Abi lene,
July
To ass is t in securing loca l support to meet
a projected operating shortfa l l
$30,000
MHMR of Concho Val ley for Concho
Val ley Community Resource
Coordination Group, July
Toward hiring a case manager to
coordinate services for multi ‐need chi ldren
and their fami l ies
$63,500

74
MENTAL HEALTH
Treatment2001 MFI Grant Amount
San Antonio Urban Ministries , September Toward constructing a res identia l faci l i ty
for menta l ly i l l women and their chi ldren
$250,000
Volunteer Services State Counci l
September
Toward a program to tra in s taff and
volunteers from 21 Mental Health Menta l
Retardation s tate faci l i ties in fundra is ing
to supplement services and programs to
Texans with menta l i l lness and menta l
retardation
$65,000
Planned Living Ass is tance Network of
North Texas , October
Toward developing and implementing a
l i ving ski l l s educationa l program for
people with severe and chronic menta l
i l lness and their fami l ies
$82,000
Turtle Creek Manor, October Toward costs associated with trans ferring
Herrin House faci l i ties and programs
serving mental ly i l l cl ients to Turtle Creek
Manor
$115,500
Youth and Fami ly Al l iance, October Toward expanding menta l health
counsel ing and socia l services to low‐
income fami l ies in North Austin
$100,000
17 $2,145,800
2002
Central Counties Center for Menta l
Health & Mental Retardation Services ,
January
Toward establ i shing a video conferencing
network to provide psychiatric eva luations
to individua ls with menta l retardation and
mental i l lness
$25,000
Advocacy Center for Chi ldren of
Galveston County, February
Toward constructing a new faci l i ty in which
to provide cris i s services for chi ld abuse
victims and their non‐offending fami ly
members
$48,000
Robert Beavers Fami ly Studies Center,
February
Toward expanding menta l health services
for economica l ly disadvantaged fami l ies
$119,000
Comal County Emergency Chi ldren's
Shelter, March
Toward constructing a bui lding in which to
provide an activi ty center and menta l
health assessment areas for abused,
neglected and abandoned chi ldren
$117,000
DePelchin Chi ldren's Center, March Toward renovating a res identia l emergency
shel ter for chi ldren and youth in Fort Bend
County
$200,000
G R E A T Kids W/ADHD, March Toward emergency operating support for a
school serving chi ldren diagnosed with
ADD/ADHD and other menta l i l lnesses
$115,000
Homeward Bound, March Toward s tart‐up funding for a substance
abuse treatment faci l i ty in South Dal las
speci fica l ly for Spanish‐speaking cl ients
$50,000
Advocacy Center for the Chi ldren of El
Paso, April
Toward constructing a bui lding in which to
provide services to chi ld victims of phys ica l
and sexual abuse
$75,000

75
MENTAL HEALTH
Treatment2002 MFI Grant Amount
Col l in County Chi ldren's Advocacy Center,
April
Toward reti ring the mortgage on a faci l i ty
in which services to chi ld victims of abuse
are provided
$100,000
NAMI Dal las , April Toward adding profess iona l s taff to
expand services to a la rger number of
individua ls with mental i l lness and their
fami l ies in Dal las
$225,000
Abused Chi ldren's Shelter, May Toward emergency operating support to
replace revenue losses suffered as a
resul t of di fficul t economic conditions and
to meet increas ing demand for services
$88,000
Lakes Regiona l MHMR Center, June Toward constructing a community mental
health and mental retardation center in
Terrel l
$200,000
NAMI Gulf Coast, June Toward emergency operating support to
provide educational services for
individua ls with mental i l lness and their
fami l ies
$62,000
Safe Tri ‐County Community Center
Ass is ting Women and Chi ldren, June
Toward hiring an additiona l counselor to
offer expanded menta l health services to
low‐income persons
$25,000
Woods ide Tra i l s Wilderness Experience
June
Toward purchas ing a van and a truck to
transport emotional ly disturbed boys from
the therapeutic camp to off‐s i te services
and activi ties
$26,500
Austin Harvard School , July Toward expanding a school for chi ldren
diagnosed with bipolar and attention
defici t hyperactivi ty disorders
$85,400
Arl ington Li fe Shelter, October Toward expanding a telemedicine program
that provides psychiatric services for
homeless persons
$60,000
Chi ldren's Bereavement Center of South
Texas , October
Toward expanding grief support services to
chi ldren and their fami l ies
$100,000
Garth House Mickey Mehaffy Chi ldren's
Advocacy Program, October
To provide menta l health counsel ing to
victims of chi ld abuse in Tyler County
$37,800
Settlement Club, November Toward renovating three res identia l
cottages for severely emotiona l ly
disturbed girl s that need intens ive therapy
and supervis ion
$50,000
Southwest Menta l Health Center,
November
Toward expanding a therapeutic care
faci l i ty to serve additional chi ldren with
serious psychiatric disorders
$190,000

76
MENTAL HEALTH
Treatment2002 MFI Grant Amount
Intervention Services Unl imited,
December
Toward emergency operating support to
continue providing mental health services
to school chi ldren and fami l ies
$150,000
La Fami l ia Del Paso, December Toward expenses associated with hiring a
new executive director to maintain services
for individua ls with menta l i l lness
$60,000
Li feNet Community Behaviora l , December Toward constructing five group homes in
which to provide permanent supportive
hous ing to homeless adults with menta l
i l lness
$300,000
24 $2,508,700
2003
Alamo Chi ldren's Advocacy Center dba
Chi ldSafe, January
Toward expanding chi ld abuse prevention
and intervention programs to keep up with
the growing demand for services
$150,000
Hospice of Midland, January Toward renovating a bui lding in which to
serve as a grief center for chi ldren
$96,000
Texas Tech Univers i ty Health Sciences
Center, January
Toward expanding health services in 73
colonias in southeast El Paso by adding
community outreach and menta l health
components to a school ‐based health
cl inic
$262,000
Chi ldren's Advocacy Center of Paris ,
March
Toward purchas ing a bui lding in which to
provide services to victims of chi ld abuse
$70,400
Boys & Girls Clubs of San Antonio, June Toward expanding a mental health
program for phys ica l ly and sexual ly abused
chi ldren
$135,000
Pastora l Counsel ing and Education
Center, June
Toward purchas ing new computers for the
s taff and therapists who provide menta l
health counsel ing
$31,600
Mental Health America of Greater
Dal las , July
Toward continuing efforts to implement
ja i l divers ion programs for persons with
mental i l lness
$205,000
Mosaic Fami ly Services , July Toward expenses for an emergency shel ter
and mental health program for women and
chi ldren refugees and immigrants who are
victims of fami ly violence
$165,000
Panhandle Cris i s Center, July Toward renovating a bui lding in which to
provide counsel ing services to victims of
fami ly violence and sexua l assaul t
$50,000

77
MENTAL HEALTH
Treatment2003 MFI Grant Amount
The Gathering Place, July Toward expanding a comprehens ive,
supportive employment program for
persons with menta l i l lness
$76,000
El Paso Chi ld Guidance Center,
September
Toward emergency funding to maintain
chi ldren's menta l health services
$50,000
Mental Health Association of Tarrant
County, September
Toward funding the pos i tion of a
development director over two years
$97,000
Turtle Creek Manor, October Toward s tart‐up costs associated with
expanding a trans i tional hous ing program
to include apartments for cl ients with
mental i l lness and chemical addiction
$104,500
Coasta l Bend Youth City, November Toward renovating five res identia l
cottages in order to expand an intens ive
therapeutic program for severely
emotiona l ly dis turbed chi ldren
$45,500
Northeast Texas Chi ld Advocacy Center,
November
Toward expanding the exis ting faci l i ty to
provide additional space for treating
victims of chi ld abuse
$47,500
15 $1,585,500
2004
Bo's Place, February Toward constructing a new faci l i ty
dedicated to serving bereaved chi ldren
$100,000
Samari tan Counsel ing Center of East
Texas , February
Toward operating support to replace
revenue losses suffered as a resul t of
recent state budget reductions
$37,000
Grayson County Chi ldren's Advocacy
Center, March
Toward s tart‐up costs for a new program to
serve abused and neglected chi ldren
$65,000
Navarro County Chi ldren's Advocacy
Center, March
Toward hiring staff to expand advocacy
services to abused and neglected chi ldren
$52,000
San Antonio Urban Ministries , June Toward constructing a second fami ly lodge
to provide hous ing and support to women
with severe mental i l lness and their
chi ldren
$176,000
St. Peter‐St. Joseph Chi ldren's Home,
June
Toward constructing a faci l i ty in which to
provide increased therapeutic programs for
abused and neglected chi ldren and to
provide additional mental health services
to low‐income community members
$200,000

78
MENTAL HEALTH
Treatment2004 MFI Grant Amount
Waterloo Counsel ing Center, June Toward establ i shing a graduate s tudent
tra ining program to provide menta l health
services to an expanded number of gay and
lesbian individuals
$15,000
Austin Chi ld Guidance Center, July Toward hiring a director of development to
divers i fy and increase the agency's funding
base to meet the demand for menta l
health services
$135,000
Houston/Trini ty Counties Chi ldren's
Advocacy Center, July
Toward increas ing program staff in order to
serve more chi ldren who are victims of
abuse and neglect
$63,000
Opportunity Center for the Homeless ,
July
Toward renovating space for use as a 15‐
bed 'sa fe zone' for homeless persons
recovering from substance abuse
$41,100
Volunteer Service Counci l for Wichita
Fa l l s State Hospita l , July
Toward campus renovations to improve the
effectiveness of a model psychiatric
treatment program
$75,000
National Al l iance for the Mental ly I l l ,
September
Toward constructing a 15‐unit multi ‐fami ly
hous ing complex for individuals with
chronic mental i l lness
$175,500
Arrow Project, October Toward campus infras tructure upgrades at
the Porter faci l i ty
$61,000
Chi ldren's Advocacy Center of Hidalgo
County, October
Toward establ i shing a satel l i te office to
serve abused chi ldren in Starr County
$61,000
Center for Success and Independence,
November
Toward expanding a res identia l treatment
faci l i ty for adolescents with psychologica l ,
emotiona l , and substance abuse disorders
$150,000
Dal las County, November To analyze the qual i ty and efficiency of
mental health and medica l care services
provided in the Dal las County Ja i l
$53,000
16 $1,459,600
2005
Turtle Creek Manor, February Toward emergency operating support $212,000
Youth and Fami ly Al l iance, February Toward constructing a youth and fami ly
counsel ing center in South Austin
$200,000
Phoenix Houses of Texas , March Toward emergency funding to maintain
res identia l substance abuse and mental
health services for adolescents in Austin
$107,000
Dal las Area NorthSTAR Authori ty ‐ North
Texas Behaviora l Health Authori ty, April
Toward funding to support an instant
messaging communications system as part
of a new mental health divert court
process
$40,000

79
MENTAL HEALTHTreatment2005 MFI Grant Amount
Garth House Mickey Mehaffy Children's
Advocacy Program, April
Toward renovation of an additional facility and
hiring a full‐time counselor in order to expand psychiatric counseling to child victims of abuse and
neglect and their families
$108,000
Safe Tri‐County Community Center Assisting
Women and Children, April
Toward renovating a facility in which to provide
expanded mental health counseling services to women and children who have been abused
$63,000
Shelter Agencies for Families in East Texas, April Toward constructing a new facility in which to provide additional counseling services to victims of
domestic violence and sexual assault
$68,000
St. Jude's Ranch for Children, April Toward constructing two cottages in order to
increase residential therapeutic services to
additional children with severe emotional problems
$120,000
Travis County Domestic Violence and Sexual
Assault Center, April
Toward restoring two full‐time mental health
counselors to serve victims of sexual and domestic
violence
$160,000
Children's Advocacy Center of the Big Bend, June Toward adding on‐site mental health counseling for
victims of child abuse
$24,000
Texas Boys Ranch, June Toward constructing a new cottage to expand
therapeutic residential care services to neglected
and abused boys
$95,000
Journey of Hope Grief Support Center, July Toward adding staff in order to expand additional
grief support services to children, teens and their
families who have lost a loved one
$88,000
Alliance For Children, September Toward constructing a new facility to accommodate
more staff to serve children who are removed from
their homes due to abuse or neglect
$200,000
LifeNet Community Behavioral, September Toward extra costs associated with new state
mental health treatment guidelines and towards hiring additional staff in order to provide mental
health services to evacuees from Hurricane Katrina
$258,000
Mental Health America of Greater Dallas,
September
To hire a staff position in order to coordinate
mental health services to Hurricane Katrina evacuees in the Dallas area
$77,430
Samaritan Counseling Center of East Texas, September
For emergency funds to continue mental health counseling for the Katrina evacuees in Nacogdoches
and Lufkin
$37,000
Collin County Mental Health Mental Retardation
Center, October
Toward outreach services to identify Katrina
evacuees who are experiencing mental illness and to provide needed services
$25,000

80
MENTAL HEALTH
Treatment2005 MFI Grant Amount
El Paso County, November Toward expanding the capaci ty of Publ ic
Defender's Mental Health Unit to redirect
offenders with mental i l lnesses to needed
services and to reduce their rate of
recidivism
$246,516
Mental Health America of Greater
Dal las , November
Toward conducting a menta l health survey
of Katrina victims and providing referra ls to
mental health services
$75,000
Mental Health America of Texas ,
November
Toward a pi lot project to increase the
number of working Texans with health
insurance that includes menta l health
coverage
$149,000
Samari tan Counsel ing Center of
Southeast Texas , November
Toward emergency operating support as a
resul t of revenue losses due to Hurricane
Rita
$35,000
Mental Health Association of Tarrant
County, December
Toward hiring a case manager that wil l
assess and refer Katrina evacuees to loca l
providers
$25,000
22 $2,412,946
2006
El Buen Samaritano Episcopal Miss ion,
January
Toward hiring staff to expand mental
health and socia l service programs for low‐
income, uninsured Hispanic fami l ies
$160,000
Mental Health America of Greater
Dal las , January
To provide case managers to ass is t Katrina
evacuees in access ing needed medica l
and mental health services
$83,000
Samari tan Counsel ing Center of East
Texas , February
Toward continuing to provide counsel ing
and cris i s intervention services for
hurricane evacuees in East Texas
$30,000
The Univers i ty of Texas Southwestern
Medical Center at Dal las , February
Toward establ i shing a Women's Menta l
Health Center at UT Southwestern
diagnos ing and treating psychiatric
disorders affecting girl s and women
$810,000
Lone Star Circle of Care, March Toward expanding menta l health services
for uninsured and medica l ly underserved
individua ls in Wil l iamson County
$225,000
Mosaic Fami ly Services , March Toward bridge funding in order to mainta in
mental health and other emergency
services to victims of human trafficking as
the demand for services increases
$115,000
Alamo Chi ldren's Advocacy Center dba
Chi ldSafe, April
Toward emergency and bridge funding to
cover financia l losses and growing
demand as a resul t of the 2005 hurricanes
$108,000
Connections Individua l and Fami ly
Services , April
Toward support of a Development Director
pos i tion in order to divers i fy funding
sources
$51,000
Camp Agape, May Toward leas ing space for a summer
bereavement and grief counsel ing camp
program for chi ldren
$32,000
Chi ld Welfare Al l iance of Calhoun
County, June
Toward constructing a new bui lding to
serve victims of chi ld abuse, sexua l
assaul t and domestic violence
$25,000

81
MENTAL HEALTH
Treatment2006 MFI Grant Amount
Chi ld Welfare Al l iance of Calhoun
County, June
Toward constructing a new bui lding to
serve victims of chi ld abuse, sexua l
assaul t and domestic violence
$25,000
Chi ldren's Advocacy Center of Comal
County, June
Toward emergency operating support for a
newly establ i shed agency serving chi ld
victims of abuse and neglect
$18,000
Chi ldren's Home of Lubbock and Fami ly
Service Agency, June
Toward campus renovations to improve
therapeutic treatment services to abused
and neglected chi ldren
$89,500
Happy Hi l l Farm Chi ldren's Home, June Toward constructing three new group
res idences for emotiona l ly dis turbed youth
$238,000
Arl ington Li fe Shelter, July Toward expanding a mental health
program for homeless individua ls
$199,000
Fort Bend Family Health Center, July Toward expanding a mental health
program that targets Spanish‐speaking
cl ients and includes telepsychiatry
services
$81,000
Chi ldren's Advocacy Centers of Texas ,
September
Toward a new faci l i ty in which to tra in
personnel who serve abused and
neglected chi ldren
$150,000
Mental Health America of Greater
Dal las , September
Toward adding s taff in order to update and
expand consumer‐oriented programs and
educationa l ini tiatives for individuals with
mental i l lnesses in a seven‐county North
Texas area
$195,000
Center for Chi ld Protection, October Toward constructing a new, expanded chi ld
advocacy center
$214,000
For the Love of Chris ti , October Toward hiring an executive director to
ensure continui ty and growth of programs
for grieving individua ls and fami l ies
$57,000
San Antonio Clubhouse, November Toward expanding a rehabi l i tation
program for adults with severe and
pers is tent menta l i l lness
$90,000
20 $2,970,500
2007
Alamo Area Rape Cris i s Center, February Toward hiring a development director to
increase and divers i fy annual revenues
$81,000
Samari tan Counsel ing Center of
Southeast Texas , February
Toward hiring an additiona l counselor to
provide menta l health services to
individua ls and fami l ies
$40,000
El l i s County Chi ldren's Advocacy Center,
March
Toward constructing a new faci l i ty to serve
an expanded number of abused and
neglected chi ldren
$81,000

82
MENTAL HEALTH
Treatment2007 MFI Grant Amount
The Gathering Place, March Toward bridge funding for a new satel l i te
program offering increased services for
adults with severe and pers is tent menta l
i l lness
$67,500
Fort Bend County Chi ld Advocates , May Toward constructing a new faci l i ty to
provide expanded advocacy and support
services for abused and neglected chi ldren
$132,000
Samari tan Counsel ing Center of West
Texas , May
Toward hiring a therapist to provide
counsel ing and expand services to war
veterans and other individua ls in a 27‐
county rural area
$48,000
Chi ldren's Advocacy Center of Laredo‐
Webb County, June
Toward equipment for a newly constructed
faci l i ty for victims of chi ld abuse
$25,000
Women's Center of Tarrant County, June Toward constructing a la rger faci l i ty to
expand programs for victims of rape, abuse
and/or violence
$250,000
Gulf Bend Menta l Health Mental
Retardation Center, July
Toward technology to increase menta l
health services to people in a rura l area
with severe and/or pers is tent menta l
i l lness
$98,600
Col l in County Chi ldren's Advocacy Center,
September
Toward constructing an addition to a
faci l i ty to expand services to the growing
number of abused and neglected chi ldren
$200,000
Communities In Schools of San Antonio,
September
Toward expanding a pi lot program that
provides intens ive in‐school menta l health
services to students in need
$100,000
Fami ly and Chi ld Guidance Centers ,
September
Toward bridge funding whi le developing
susta inable revenues to support menta l
health services for indigent chi ldren and
adults in Dal las County
$150,000
Promise House, September Toward expanding a psychiatric treatment
program for homeless and at‐ri sk youth
$75,000
Metro Dal las Homeless Al l iance,
October
To launch a five‐year campaign to operate
a ci tywide, comprehens ive Homeless
Ass is tance Center
$1,500,000
Univers i ty of Texas Medical Branch at
Galveston, November
Toward continuing and expanding an
innovative model of del ivering menta l
health and substance abuse services to
the indigent population of Galveston and
Brazoria Counties
$375,000
15 $3,223,100

83
MENTAL HEALTH
Treatment2008 MFI Grant Amount
Cameron County Chi ldren's Advocacy
Centers , January
Toward bridge funding to support
counsel ing services for chi ld abuse victims
and their fami l ies
$75,000
Planned Living Ass is tance Network of
North Texas , January
Toward ini tiating a cognitive enhancement
therapy recovery program for individua ls
with severe mental i l lnesses
$234,000
Al l iance For Chi ldren, February Toward hiring the agency's fi rs t fund
development director
$145,000
Safe Tri ‐County Community Center
Ass is ting Women and Chi ldren, February
Toward hiring staff to expand a support
and treatment program for women and
chi ld victims of domestic violence
$30,000
NAMI Texas , April Toward bridge funding to hire new staff
and stabi l i ze services
$278,750
Scotty's House Brazos Val ley Chi ld
Advocacy Center, April
Toward constructing a faci l i ty to provide
increased advocacy services to abused and
neglected chi ldren
$86,000
Youth and Fami ly Al l iance, April Toward bridge funding for an adult mental
health program
$150,000
Depress ion and Bipolar Support Al l iance
Greater Houston (DBSA), May
Toward hiring an additiona l program
coordinator to expand support groups
$107,600
Healthcare For The Homeless ‐Houston,
May
Toward expanding menta l health services
to the homeless and individua ls
incarcerated or released from ja i l
$105,000
Lutheran Socia l Services of the South,
June
Toward expanding and improving
res identia l treatment at the Canyon Lake
faci l i ty to provide therapeutic and
educationa l services for youth with menta l
i l lness
$118,000
Fami ly and Chi ld Guidance Centers ,
September
Toward s tart‐up of a chi ldren's menta l
health cl inic to expand services to indigent
chi ldren and youth in the southern sector
of Dal las County
$150,000
Foundation For The Counci l On Alcohol
And Drug Abuse‐Houston, September
Toward expanding faci l i ties to provide
better access to counsel ing and
therapeutic services for individua ls
affected by alcohol and drugs
$300,000
Denton County Chi ldrens Advocacy
Network, Inc., October
Toward constructing a faci l i ty to meet the
increased need for services for chi ld
victims of abuse and their non‐offending
fami ly members
$150,000
Li feNet Community Behaviora l , October Toward renovating a faci l i ty to relocate the
main service office
$174,000
14 $2,103,350

84
MENTAL HEALTH
Treatment2009 MFI Grant Amount
Neighborhood Youth Services of
Richardson, January
Toward emergency operating funds due to
decreased government grants and
increased demand for counsel ing services
$53,000
Barrio Comprehens ive Fami ly Health
Care Center, February
Toward renovations to expand mental
health services
$50,000
Hi l l Country Community MHMR Center,
February
Toward furnishings and equipment for a
new menta l health cris i s s tabi l i zation unit
$25,000
Mental Health America of Greater
Dal las , March
Toward emergency operating support
during a time of economic cris i s
$225,000
Samari tan Pastora l Care & Counsel ing
Center of San Angelo, March
Toward increas ing the hours of a cl inica l
director to meet the growing need for
mental health services
$31,000
Community Partners of Dal las , April Toward bridge funding to reinstate and
expand menta l health services for victims
of chi ld abuse in Dal las County
$100,000
Sa lvation Army DFW Metroplex
Command, April
Toward a new program to trans i tion
homeless adults with mental i l lness to
s table hous ing
$150,000
Univers i ty of North Texas Health Science
Center at Fort Worth, April
Toward implementing a menta l health
screening tool to enhance treatment for
adult probationers
$105,400
Planned Living Ass is tance Network of
Central Texas , May
Toward ass is ting individuals trans i tion
from publ ic menta l health services to
community services
$39,000
Samari tan Center for Counsel ing and
Pastora l Care, May
Toward emergency operating funding to
cover a decrease in revenues whi le
meeting a growing need for menta l health
services
$105,000
Bexar County Detention Ministries , June Toward bridge funding to continue a
mental health therapy program for
individua ls released from ja i l /prison and
their fami ly members
$25,000
The Network of Behavioral Health
Providers , June
Toward a pi lot program to increase the
number of individua ls choos ing and
receiving education in the field of
behavioral health
$25,000
USA Cares , June Toward the financia l needs of mil i tary men
and women experiencing post traumatic
s tress disorder and/or traumatic brain
injury and their fami l ies
$250,000
Austin Chi ld Guidance Center, July Toward bridge funding to hire additional
s taff to meet the increas ing demand for
mental health services for low‐income and
working poor fami l ies
$100,000

85
MENTAL HEALTH
Treatment2009 MFI Grant Amount
Easter Sea ls ‐Central Texas , July Toward bridge funding to continue menta l
health services to cl ients with disabi l i ties
who are in a job tra ining program
$50,000
Mental Health America of Greater
Houston, July
Toward developing and eva luating
effective strategies for implementing
integrated primary health care and mental
health care in Texas
$58,000
Metro Dal las Homeless Al l iance,
September
Toward a new staff pos i tion to develop
and ini tiate funding and community
relations opportunities to benefi t the
homeless
$150,000
Mosaic Fami ly Services , October Toward emergency funding due to
decreased government revenues and
increased demand for services for victims
of domestic violence and human trafficking
$168,000
Univers i ty of North Texas , October Toward developing a supportive
employment program for individua ls with
mental i l lness
$112,000
Greater San Marcos Youth Counci l ,
November
Toward mainta ining emergency shel ter
and counsel ing services for chi ldren and
fami l ies in cris i s during the current
economic downturn
$24,000
Mental Health Association of Tarrant
County, November
Toward expanding a counsel ing program to
include fi rs t responders who need menta l
health services
$100,000
Project Trans i tions Toward hiring a case manager that wil l
assess and refer Katrina evacuees to loca l
providers
$57,000
22 $2,002,400
Treatment Total 165 $20,411,896
Early Identification, Intervention, and Prevention
2001
Univers i ty of Texas Health Science
Center at San Antonio, July
Start‐up funding to create the South Texas
Psychiatric Genetics Research Center to
improve the identi fi cation and treatment
of patients with bipolar disorder
$345,000
Texas Youth Commiss ion, November Toward expanding a pi lot program to
reduce chi ld abuse by providing parenting
tra ining and counsel ing for del inquent
parents in Dal las , Houston and San
Antonio
$112,000
2 $457,000

86
MENTAL HEALTH
Early Identification, Intervention, and Prevention
2002 MFI Grant Amount
Exchange Club Center for the Prevention
of Chi ld Abuse of DFW, February
Toward emergency operating support over
three years to employ caseworkers to
provide volunteer in‐home mentors for
chi ld abuse referra ls
$166,000
Parenting Cottage, February Toward bridge funding to establ i sh
parenting education programs for fami l ies
at ri sk of chi ld abuse
$62,000
Exchange Club Center for the Prevention
of Chi ld Abuse of DFW, June
Toward uti l i ty and jani toria l expenses
during the current economic downturn
$3,560
Univers i ty of Texas Health Science
Center at Houston, June
Toward supporting a pi lot after‐school
program serving chi ldren at ri sk for mental
health problems
$25,000
Escape Fami ly Resource Center of The
Exchange Clubs of Houston, November
Toward repairing and upgrading a faci l i ty
in which chi ld abuse and neglect
prevention services are provided
$49,000
5 $305,560
2003
Fami ly Outreach of Comal County,
November
Toward operating support to replace
revenue losses suffered as a resul t of
recent state budget reductions
$29,000
1 $29,000
2004
Exchange Club Center for the Prevention
of Chi ld Abuse of DFW, June
Toward emergency operating funds to
susta in the Dal las Healthy Fami l ies
Program
$150,000
1 $150,000
2005
Parenting Cottage, April To el iminate debt in order to provide chi ld
abuse prevention and fami ly support
services to more at‐risk fami l ies in
Lubbock County
$40,000
Escape Fami ly Resource Center of The
Exchange Clubs of Houston, June
Toward completing capi ta l improvements
to a faci l i ty serving chi ldren who are
victims of abuse
$25,000
Fami ly Outreach Corpus Chris ti , June Toward adding a bi l ingual program
director in order to expand programs for
fami l ies at ri sk of chi ld abuse and neglect
$20,000
Texas Association for Infant Menta l
Health, June
Toward s taffing and administrative
expenses associated with developing a
voluntary sys tem to enhance the
profess iona l development of providers of
services to very young chi ldren
$25,000
North Texas Publ ic Broadcasting (KERA‐
Channel 13), November
Toward providing educationa l and tra ining
materia ls to address the mental health
needs of chi ldren affected by the
hurricanes
$57,100
5 $167,100

87
MENTAL HEALTH
Early Identification, Intervention, and Prevention2006 MFI Grant Amount
Family Outreach Center of East Dallas, January Toward hiring an executive director in order to strengthen parenting education services to prevent
child abuse and neglect in East Dallas
$62,500
University of Texas at Austin, June Toward start‐up costs for the Imaging Research
Center to support basic and applied research on
brain disorders and other neuroscience projects
$312,500
2 $375,000
2007Ronald McDonald House Charities of El Paso,
June
Toward adding a mental health component to the
mobile unit that serves children in the Socorro
Independent School District and toward furnishing
and equipping a family room at a local hospital
$25,000
Parenting Cottage, July Toward expanding a program to prevent and treat
Fetal Alcohol Spectrum Disorder
$49,000
Any Baby Can, October Toward bridge funding for an in‐home program
assisting families with young children at high risk for
abuse, neglect or developmental delay
$125,000
Contact Crisis Line, November Toward hiring bilingual staff to serve more Spanish‐
speaking individuals in crisis
$87,500
4 $286,500
2008
Texas Christian University, TCU Institute of Child Development, January
Toward developing an outreach project to disseminate knowledge and training to
professionals and parents of children with
emotional and developmental problems
$215,000
Children's Advocacy Center of Tom Green County, May
Toward emergency funding to hire staff to advocate for and support children taken from the Eldorado
compound
$89,247
University of Texas at Dallas, July Toward initiating the Center for Children and
Families to offer a resource for parents and
professionals who seek guidance to meet the needs
of children from birth through adolescence
$350,000
Zero To Three, September Toward expanding a pilot program that provides
developmental and mental health services for children 0 ‐ 3 years old in foster care
$100,000
4 $754,247
2009
Exchange Club Center for the Prevention of Child
Abuse of DFW, January
Toward emergency operating support $50,000
Heart of Montgomery County, February Toward emergency operating support to continue a
suicide prevention program
$47,500

88
MENTAL HEALTH
Early Identification, Intervention, and Prevention
2009 MFI Grant Amount
Center For Publ ic Representation, July Toward replacing grant funding lost due to
the Madoff scheme in order to resume
reform ini tiatives in the juveni le jus tice
system
$34,000
Tip of Texas Fami ly Outreach, October Toward expanding chi ld abuse and neglect
prevention programs in the lower Rio
Grande Val ley to meet greater demand
created by the economic downturn
$30,000
Advocacy Incorporated, November Toward providing attorney services for long‐
term fos ter youth placed in state hospita ls
and correctional faci l i ties
$75,000
5 $236,500
29 $2,760,907
Public Education and Erasing Stigma
2001
Texas Appleseed, July Toward an indigent defense education
effort that focuses on menta l ly i l l crimina l
defendants
$93,558
1 $93,558
2002
Mental Health America of Texas , May Toward hiring development staff to bui ld
the agency's capaci ty
$225,000
Texas Appleseed, October Toward continuing an education effort to
improve lega l services for defendants with
mental i l lness
$81,000
2 $306,000
2003
Association for Community Televis ion
(KUHT), June
Toward developing and disseminating a
publ ic televis ion documentary on
chi ldren's menta l health in Texas
$107,000
1 $107,000
2005
Mental Health America of Greater
Houston, January
Toward increas ing publ ic understanding
and acceptance of menta l i l lness by
adding a Community Outreach Specia l i s t
$86,000
1 $86,000
2009
Mental Health America of Texas ,
September
Toward emergency operating support to
maintain menta l health services during
the current economic downturn
$150,000
1 $150,000
Public Education & Erasing Stigma Total 6 $742,558
Total for Mental Health 200 $23,915,361
Early Identification, Intervention, and Prevention Total