mental health & employmentstats.learningandwork.org.uk/events_presentations/intowork2016... ·...
TRANSCRIPT
Mental Health & Employment
6 Common Myths That Prevent
Effective Delivery
Kevin Moore, Future Path
Bob Kitchin, Twining Enterprise
www.future-path.co.uk/mythbusters
Terminology Used• “Common mental health problems”: Mild to
moderate anxiety &/or depression, phobias etc.
• “Severe & enduring mental health problems”: Severe anxiety/depression, personality disorders, psychotic disorders
• IAPT – Improving Access to Psychological Therapies; national network of local primary care services that provide talking therapies to people with common mental health problems
London-based local authority-funded provider
Use unique PACES© Model
At the heart of multi-agency approaches across 8 London
boroughs
Specialise in supporting people with common, often undiagnosed
mental health issues
Charity specialising in mental health & employment
IPS Centre of Excellence
Working in 14 London boroughs, embedded within
mental health teams
Services covering common and severe & enduring mental
health disorders

Common Ground• Similar values, ethics and ethos.
• IPS is a strong feature, but doesn’t define us.
• Strong willingness to work together.
• Co-located teams an essential feature.
• Both seen by funders as high performing, flexible, reliable partners.
• We’re on a mission…..
Myth OneThe Identification Myth
“we know who has mental health problems”

The 3 “Tells” That Support the Myth
Claimants will tell you
Referrers will tell you
You can tell
The Barnet Example
• MaPS service designed to identify and work with unemployed people with common mental health issues.
• 453 clients supported in under 2 years
• 74% mild to moderate depression
• 70% mild to moderate anxiety
• 64% both
• Just two percent were already receiving therapy
Myth extension; we need specialist provision for people with poor mental health
• Mental health issues are common
• 1 person in 4 will experience some form of mental health issue in any year
• Approximately 1 person in 100 will get a diagnosis of psychosis at some time in their lives
• Approximately 1 person in 100 will get a diagnosis of bipolar disorder at some time
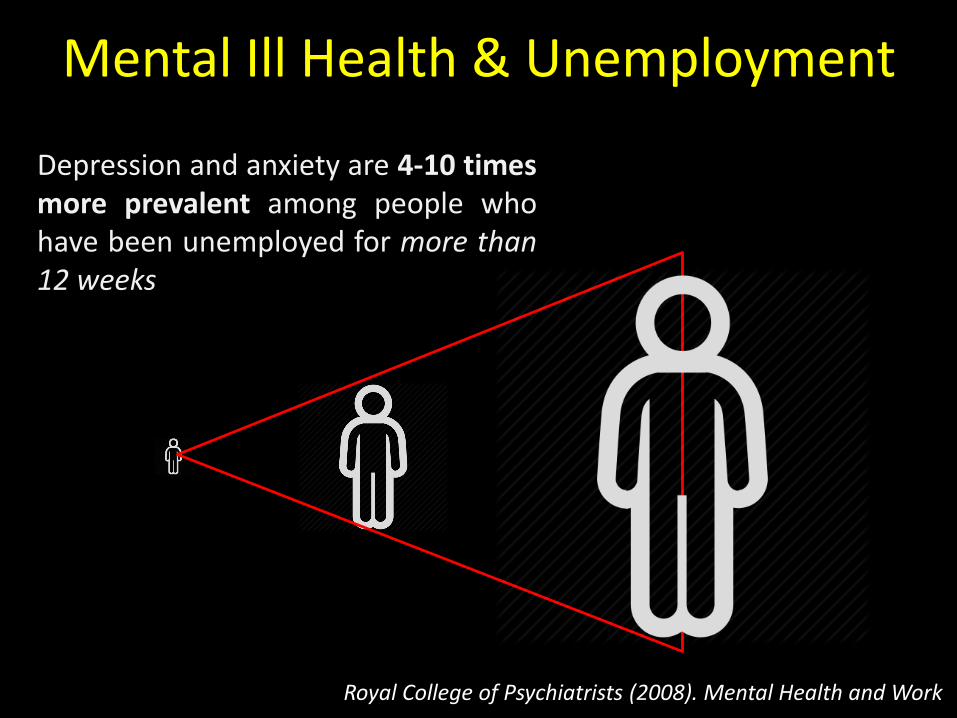
Mental Ill Health & Unemployment
Depression and anxiety are 4-10 timesmore prevalent among people whohave been unemployed for more than12 weeks
Royal College of Psychiatrists (2008). Mental Health and Work

ESA (WRAG) Claims - Primary Condition
DWP: assessments completed December 2013 – February 2015

Doing the Maths
Overall ESA MH
83%4-10X more likelyJSA
ESA MH Primary
Condition
48.1%
ESA MH Secondary Condition
66%(Anecdotal)
Mental ill health is almost inevitable in unemployed people
who are claiming ESA, or who have been without work for 3 months or more. Your model needs appropriate support as
standard.
Myth TwoThe Well-Being Myth
“your level of mental ill health = your closeness to the labour market”


Myth extension; well-being is the same as diagnosis
Positive Well-Being
Negative Well-Being
Diagnosed
Undiagnosed

Myth ThreeThe Integration Myth
“the work & health sectors work well together…. it’s straightforward”

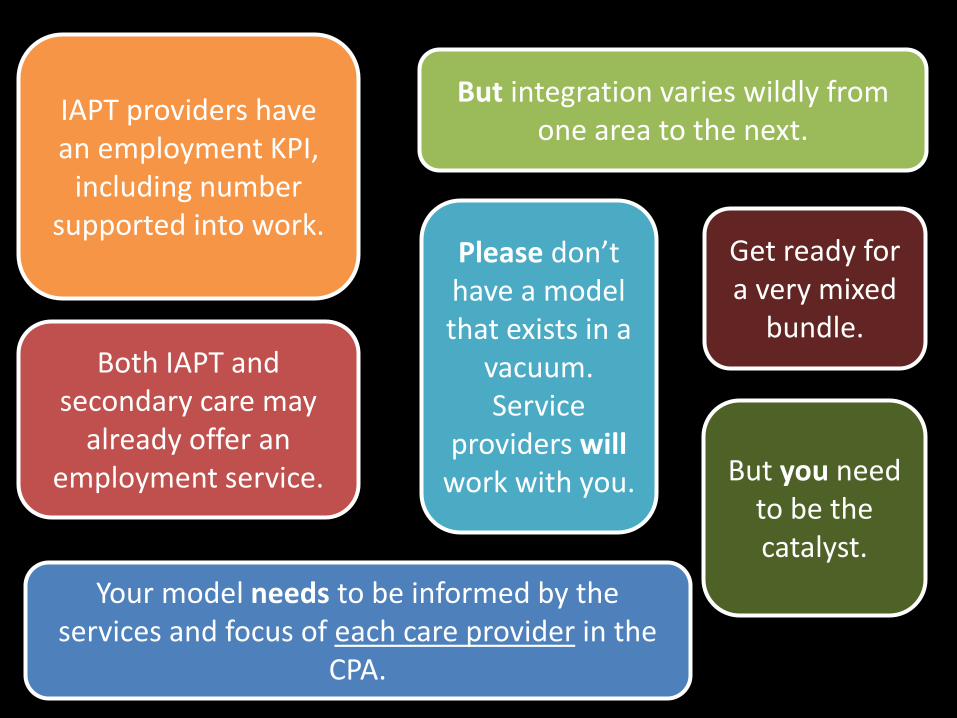
But integration varies wildly from one area to the next.
IAPT providers have an employment KPI,
including number supported into work.
Both IAPT and secondary care may
already offer an employment service.
Your model needs to be informed by the services and focus of each care provider in the
CPA.
Get ready for a very mixed
bundle.
Please don’t have a model that exists in a
vacuum. Service
providers willwork with you. But you need
to be the catalyst.
NHS Good – DWP Bad?
One of the biggest barriers toemployment that people withmental health problems face isthe low expectations that somemental health professionalshave of them.

Myth FourThe Recovery Myth
“people don’t recover from mental illness”

Ciompi in 1976 (228 patients with a diagnosis of schizophrenia followed up over 37 years) found:
• 26% experienced complete remission of symptoms
• 21% minor residual symptoms remained
• 23% intermediate course: symptoms arose episodically
The EPPIC study in 2005 (following 723 first episode psychosis patients over 7.5 years), demonstrated:
• Symptomatic remission in 37-59% of the group
• Social/Vocational recovery in 31% of the group
• Approximately 25% achieved both

Myth extension; work is something you do after recovery from MH problems
• Your role is not to refer claimants with mental health problems to health care and then wait for them to come back when they are well.
• MH professionals’ role is not to refer clients after they are well either.
• Recovery requires a “whole-person” approach

Traditional Treatment

Modern Treatment
“Employment - tough on mental illness and tough on the causes
of mental illness.”
- Farley Davidson, CEO Vauxhall and Southwark NHS

Recovery is not just about treatment
Employment Related Support & Mental Health Recovery Go Hand in Glove
• With the right training, your staff can proactively support recovery.
• Techniques that we have used successfully include:
Psycho-Education MindfulnessMotivational Interviewing
Low Level CBT NLPThe 5 Ways to
Well-Being

• Originally an Australian initiative, created by Betty Kitchener and Prof Antony Jorm.
• International initiative currently being delivered in 23 countries.
• The Department of Health encouraged all employers in England to provide MHFA training as one of three steps in its “No Health Without Mental Health” paper.
• In 2016 MHFA was recommended for all workplaces by Business in the Community.


Myth FiveThe Employment Myth
“work is something you endure once you are well”

Myth One; employment is harmful to people with mental health problems
• Employment contributes to improvement in health and well-being.
• There is no evidence that work is harmful to the mental health of people with serious mental health conditions.
• Effective recovery places employment at its core.

Myth Two; mental health employment discrimination is a thing of the past
• Over 25% of people think that someone with a mentalhealth condition should not have the same rights to a jobas anyone else.
• Less than 40% of employers would consider recruitingsomeone with a declared mental health condition (62%would consider recruiting someone with a physicaldisability).
However, 85% of employers who do employ people withmental health conditions do not regret doing so.

Myth SixThe Suicide Myth

Deaths in the UK Each Year (2014/15)
Road Traffic Accidents Known Suicides
6,2
33
1,7
13
SEVEN
TEENp
eo
ple every d
ay

Suicide Myths• People who talk about suicide are just trying to get attention.
• People who die by suicide usually talk about it first. They are in pain and often reach out for help because they do not know what to do and have lost hope. Always take talk about suicide seriously.
• Suicide always occurs without any warning signs.
• There are almost always warning signs.
• Once people decide to die by suicide, there is nothing you can do to stop them.
• Suicide can be prevented. Most people who are suicidal do not want to die; they just want to stop their pain.
• Asking someone if they’ve had thoughts of suicide might put the idea in their head.
• There is NO evidence to support this, in fact it suggests the absolute opposite.

• Identification
• Well-Being
• Integration
• Recovery
• Employment
What Does
Good Look Like?
Staff
Delivery Model
Structural

Staff
Proactively look for
signs and symptoms
Formally screen to
enable access to treatment
Are suicide and self-
harm aware
Monitor changes in well-being
Can advise clients on disclosure
and how to go about it

Tools used to quantify MH
progress/decline
Clients encouraged to report changes in
symptoms
Clients are supported into
work with “mental health friendly”
employers
Employers are encouraged to destigmatise, including through the Mindful Employer scheme
and Access to Work
Diagnosis not used to judge well-being
Support is integrated with a wide range of other,
positive recovery services
Bespoke MH interventions being
co-designed and co-delivered
Regular case-conferencing
between agencies
Support is joined up with family and social networks
In-work support is longer
Pre-employment support is rapid
DeliveryModel

StructuralCulture of
encouragement and disclosure
Stigma-free environment
Co-location at either, or preferably
both, your site & IAPT Relevant,
compliant data sharing
Clients’ overall well-being is the primary
concern of all agencies
