mental health services, university of copenhagen 1
TRANSCRIPT

Mental Health Services, University of Copenhagen
1
Early intervention in bipolar disorderLars Vedel Kessing, professor, DMSc.Psychiatric Center CopenhagenDenmark

Mental Health Services, University of Copenhagen
2
Disclosure:
Lars Vedel Kessing has within recent three years been a consultant for Lundbeck and AstraZeneca.
Mental Health Services, University of Copenhagen
3
Early intervention in bipolar disorder ?
A number of randomised trials have investigated the effect of combined pharmacological and psychological interventions and various health-service interventions in bipolar disorder
…….but none of the studies have specifically investigated the effect in the early stages of bipolar disorder.

Mental Health Services, University of Copenhagen
4
7 indications from observational studies that early intervention may improve course and outcome
1. Progressive course of illness with increasing risk of recurrence for every new episode (Kessing et al, 1998, 2004)

5
Progressive course of illness with increasing risk of recurrence for every new episode
Kessing et al, BJP 2004,185:372-377

Mental Health Services, University of Copenhagen
6
7 indications from observational studies that early intervention may improve course and outcome
1. Progressive course of illness with increasing risk of recurrence for every new episode (Kessing et al, 1998, 2004)
2. Delay to first treatment is associated with more time depressed, greater severity of depression, greater number of episodes and more days of ultradiancycling (Post et al, 2010)

Mental Health Services, University of Copenhagen
7
7 indications from observational studies that early intervention may improve course and outcome
1. Progressive course of illness with increasing risk of recurrence for every new episode (Kessing et al, 1998, 2004)
2. Delay to first treatment associated with more time depressed, greater severity of depression, greater number of episodes, more days of ultradian cycling (Post et al, 2010)
3. Response to lithium monotherapy decreases with the occurrence of multiple prior episodes (Kessing et al, 2011)

Mental Health Services, University of Copenhagen
8
7 indications from observational studies that early intervention may improve course and outcome
1. Progressive course of illness with increasing risk of recurrence for every new episode (Kessing et al, 1998, 2004)
2. Delay to first treatment associated with more time depressed, greater severity of depression, greater number of episodes, more days of ultradian cycling (Post et al, 2010)
3. Response to lithium monotherapy decreases with the occurrence of multiple prior episodes (Kessing et al, 2011)
4. The rate of response to lithium is increased when started at first psychatriccontact rather than at later contacts (Kessing et al, 2014)

Mental Health Services, University of Copenhagen
9
Rate of non-response to lithium when started following first versus later contacs
Kessing et al, British Journal of Psychiatry, 2014 Jul 10.
N= 4714: HR= 0.73, 95%CI: 0.67-0.90, p< 0.0001;

Mental Health Services, University of Copenhagen
10
7 indications from observational studies that early intervention may improve course and outcome (con´t)
5. Mood stabilizers prescribed for bipolar disorder may have neuroprotectiveabilities (Manji et al, 2000; Fountoulakis et al, 2008)

Mental Health Services, University of Copenhagen
11
7 indications from observational studies that early intervention may improve course and outcome (con´t)
5. Mood stabilizers prescribed for bipolar disorder may have neuroprotectiveabilities (Manji et al, 2000; Fountoulakis et al, 2008)
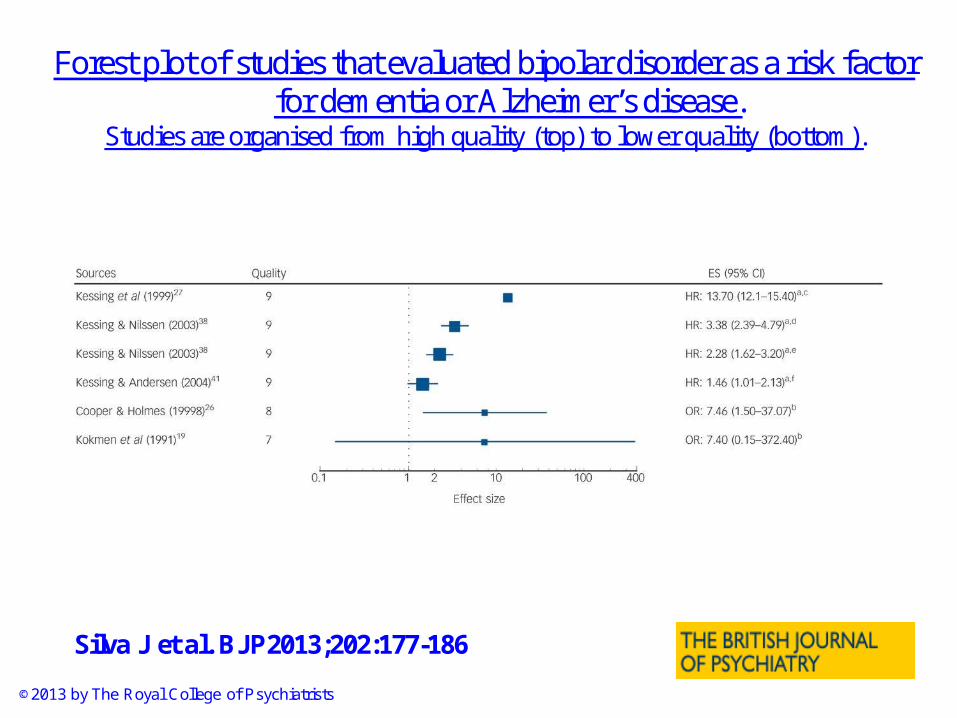
6. The prevalence of cognitive dysfunction may increase with affective episodes and the risk of dementia seems increased for patients with bipolar disorder (Silva et al, 2013)
12
Forest plot of studies that evaluated bipolar disorder as a risk factor for dementia or Alzheimer’s disease.
Studies are organised from high quality (top) to lower quality (bottom).
Silva J et al. BJP2013;202:177-186
©2013 by The Royal College of Psychiatrists

Mental Health Services, University of Copenhagen
13
7 indications from observational studies that early intervention may improve course and outcome (con´t)
5. Mood stabilizers prescribed for bipolar disorder may have neuroprotectiveabilities (Manji et al, 2000; Fountoulakis et al, 2008)
6. The prevalence of cognitive dysfunction may increase with affective episodes and the risk of dementia seems increased for patients with bipolar disorder (Silva et al, 2013)
7. Patients may profit from psychoeducation before potential cognitive disturbances may occur during the long-term course of illness (Berk et al, 2007).

Mental Health Services, University of Copenhagen
14
Specialized mood disorder clinics ?
It has been claimed that specialized bipolar units and programs such as, e.g., the Bipolar Disorders Programme at the Barcelona Hospital Clinic are needed to improve outcome and advance research in bipolar disorder (Vieta, 2012)
…..but there is no randomised trial on the effects of such specialized units.

Mental Health Services, University of Copenhagen
15
Treatment in a specialised outpatient mood disorder clinic versus standard treatment
in the early course of bipolar disorder: a randomised multicenter clinical trial within
The Mental Health Services in the Capital Region of CopenhagenDanmark
Lars Vedel Kessing, Hanne Vibe Hansen, Ellen Margrethe Christensen, Henrik Dam, Christian Gluud, Jørn Wetterslev, and The Early Intervention Affective Disorders (EIA) Trial Group*
* Members of the EIA Trial Group also encompass Klaus Damgård Jakobsen, Ejnar BundgaardLarsen, Martin Balslev Jørgensen, Maj Vinberg, Rikke Engel, Flemming Mørkeberg Nilsson, Nana Hengstenberg, Birgitte Bjerg Bendsen, Hans Mørch Jensen, Rie Lambæk Mikkelsen, Birgit Straasø, Jens Abraham.

Mental Health Services, University of Copenhagen
16
Early intervention in bipolar disorder
Aim:In a RCT to investigate whether treatment in a specialized bipolar unit program, combining optimised pharmacological treatment with group psychoeducation, early in the course of illness among patients discharged from their first hospitalisations for bipolar disorder improve long-term outcome compared with standard psychiatric outpatient treatment.

17
Early intervention in bipolar disorder
Specialized bipolar unit 2-year program:• Optimised pharmacological treatment: evidence focused
treatment in accordance with the guidelines from the British Association for Psychopharmacology, 2009 with focus on mood stabilising agents (lithium, valproate, lamictal and atypical antipsychotics)
• 3 sequential groups A) settling-in group: focus on the current clinical status
and beliefs and experiences in relation to the recent hospitalisation.
B) following remission: psychoeducation once a week for 15 weeks (shortened version ad modus F Colom)
C) discharge group: learn to live and identify early warning signals

Mental Health Services, University of Copenhagen
18
Early intervention in bipolar disorder
Inclusion: • Patients discharged from their first, second, or third
hospitalisation from an inpatient psychiatric ward with an ICD-10 diagnosis of single manic episode or bipolar disorder as the primary diagnosis.
• Comorbidity with alcohol or substance abuse and other psychiatric disorders were allowed.
• Age between 18 and 70 year old.
Exclusion: • moderate or severe dementia• poor understanding of Danish• any kind of commitment

Mental Health Services, University of Copenhagen
19
Early intervention in bipolar disorder
Primary outcome• Re-admission to psychiatric ward after discharge from the
index hospitalisation. Data on re-hospitalisation were obtained from the Danish Psychiatric Central Register
Secondary outcomes • Use of mood stabilizers (lithium or anticonvulsants), atypical
antipsychotics and/or antidepressants.
Tertiary outcome• Satisfaction with care (Verona Service Satisfaction Scale-
Affective Disorder (VSSS-A))

Mental Health Services, University of Copenhagen
20
Basic characteristics
The mood disorder clinic
Standard Treatment
N 72 86Sex, Female (%) 44 (61.1) 42 (48.8)
Median age at randomisation (quartiles)
37.6 (27.3-48.2) 35.2 (27.9-46.3)
Number of patients with or without previous admission before index hospitalisationWithout (%)With (%)
41 (56.9)31 (43.1)
40 (46.5)46 (53.5)
Mental Health Services, University of Copenhagen
21
Early intervention in bipolar disorder
Standard care
• local community mental health centre 56.5%
• private psychiatrist 24.7%
• local psychiatrist at the discharging ward 15.3%
• the general practitioner 3.5%

22
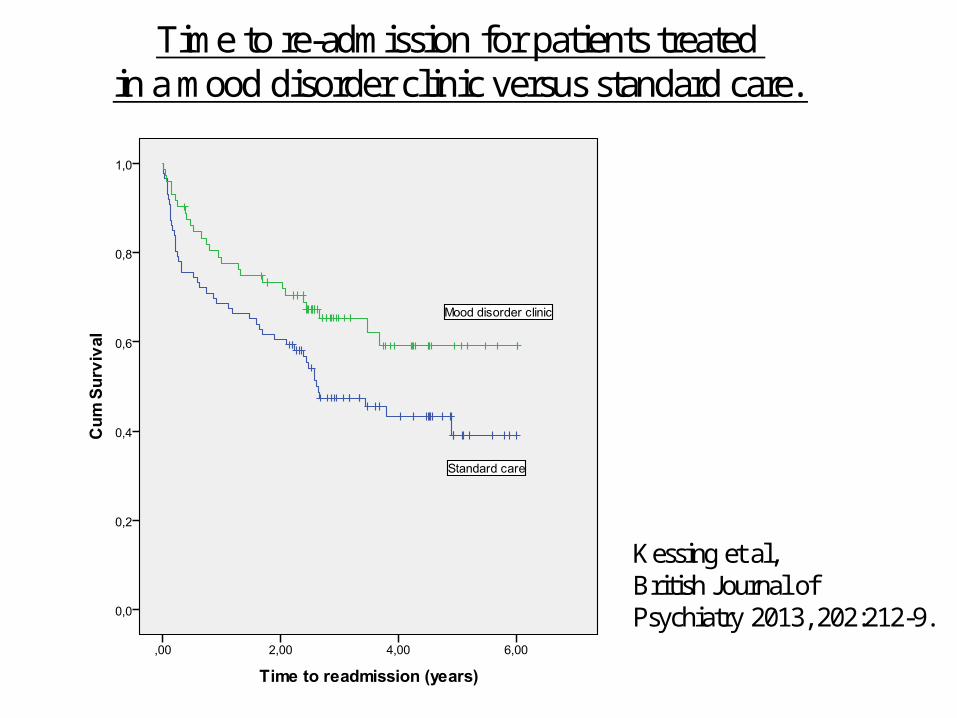
Time to re-admission for patients treated in a mood disorder clinic versus standard care.
p= 0.034
Adjusted for age, sex, psychiatric centre, and number of previouspsychiatric admissions:
HR 0.60, 95% CI 0.37 to 0.98; p= 0.043.
Kessing et al,British Journal ofPsychiatry 2013, 202:212-9.
1
23
Time to re-admission for patients treated in a mood disorder clinic versus standard care.
Kessing et al,British Journal ofPsychiatry 2013, 202:212-9.
2

24
Time to re-admission for patients treated in a mood disorder clinic versus standard care.
Kessing et al,British Journal ofPsychiatry 2013, 202:212-9.
3

Mental Health Services, University of Copenhagen
25
Early intervention in bipolar disorder
Mood disorder clinic Standard care P
Cumulated duration of hospitalisations(median (quartiles))
33.0 days (10.5-133.5) 49.0 days (21.0-127.5) 0.01

Mental Health Services, University of Copenhagen
26
Early intervention in bipolar disorder
Mood disorder clinic Standard care P
Use of :
Mood stabilizer(lithium / anticonv., %)
Antipsychotic (%)
Antidepressants (%)
59.0
59.5
42.9
32.4
34.9
37.2
0.001
0.01
0.5

Mental Health Services, University of Copenhagen
27
Early intervention in bipolar disorder
Mood disorder clinic Standard care P
Satisfaction with intervention(VSSS-A)
132.2 (SD: 16.9) 114.9 (SD: 31.6) 0.001

Mental Health Services, University of Copenhagen
28
Two-year treatment mean costs per patient in the Mood disorder clinic versus standard care (euro).
Total direct net costs when including saved hospitals beds:
Treatment in the mood disorder clinic was 3,194 euro less per patient than for standard care, corresponding to 11 % of the costs for standard care.

29
K
29 patients between 18 and 25 years of age• Patients between 18 and 25 years (HR 0.33, 95% CI 0.10 to1.07; p=0.064) • Patients 26 years or older (HR 0.68, 95% CI 0.40 to1.14, p=0.14).
Kessing et al,Journal Affective Disorders,2014 Jan;152-154:403-8.
1

30
K
29 patients between 18 and 25 years of age• Patients between 18 and 25 years (HR 0.33, 95% CI 0.10 to1.07; p=0.064) • Patients 26 years or older (HR 0.68, 95% CI 0.40 to1.14, p=0.14).
Kessing et al,Journal Affective Disorders,2014 Jan;152-154:403-8.
2
Younger adults treated in the mood disorder clinic used mood stabilizers and antipsychotics more than those treated in standard care.

Mental Health Services, University of Copenhagen
31
Early intervention in young patients with bipolar disorder
Young adults with bipolar disorder may benefit even more than older adults from early intervention combining pharmacological treatment and group psychoeducation.
Kessing et al, J Affect Disorders, 2014 Jan;152-154:403-8.

Mental Health Services, University of Copenhagen
32
Limitations
• Early intervention? - Half of the patients had had their first hospitalisation
ever.- High median age of 35.6 years at inclusion in the
study (although 25% were below 28 years and 25% above 47 years).
• Generalisation? - To bipolar I patients with the more severe disorders
leading to hospitalisation

Mental Health Services, University of Copenhagen
33
The first randomised trial onEarly intervention in bipolar disorder
Conclusion Treatment in a specialised mood disorder clinic early in the course of bipolar disorder substantially reduces psychiatric re-hospitalisations and increases satisfaction with care. And more so among young patients.
…and save total net costs.

Mental Health Services, University of Copenhagen
34
Thank you !