mesotelioma: approccio chirurgico alla diagnosi … · journal of thoracic oncoloy, 2012...
TRANSCRIPT

MESOTELIOMA: APPROCCIO CHIRURGICO ALLA
DIAGNOSI E ALLA TERAPIA
L. SantambrogioCentro Trapianti di Polmone – Fondazione IRCCS Ca’ Granda,
Ospedale Maggiore Policlinico di MilanoUniversità degli Studi di Milano
1° Congresso Nazionale IART
Cremona, 7-8 Maggio 2015
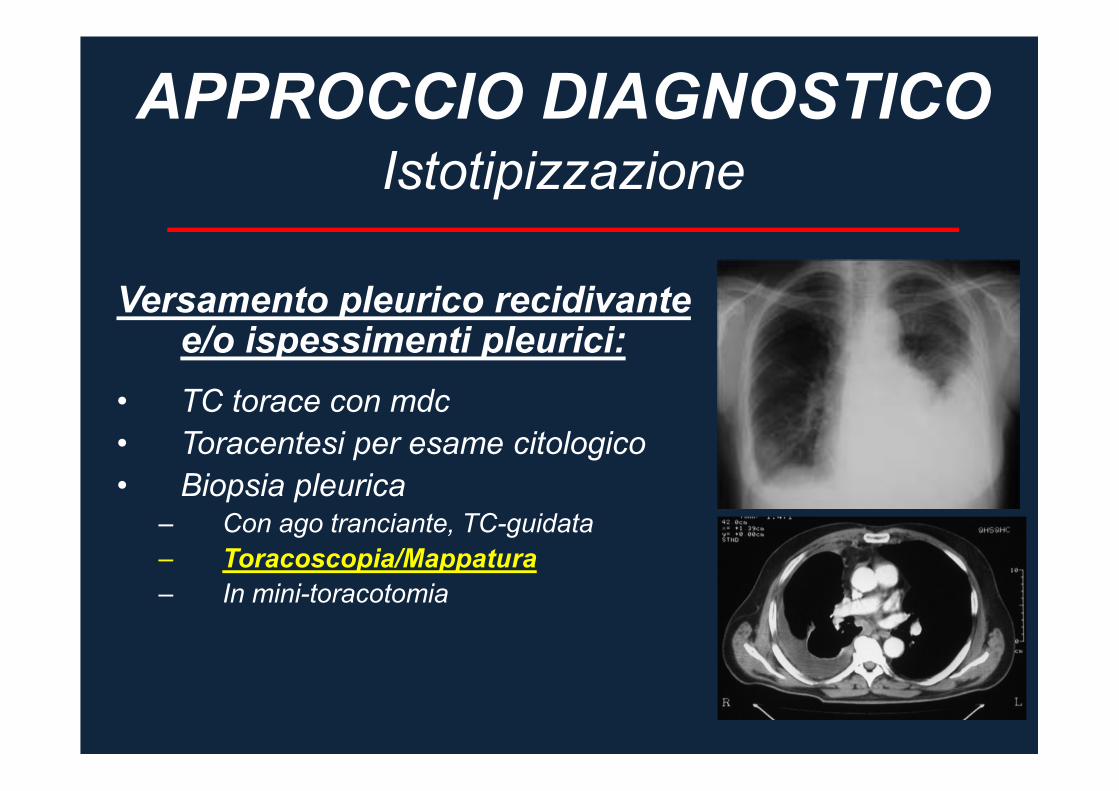
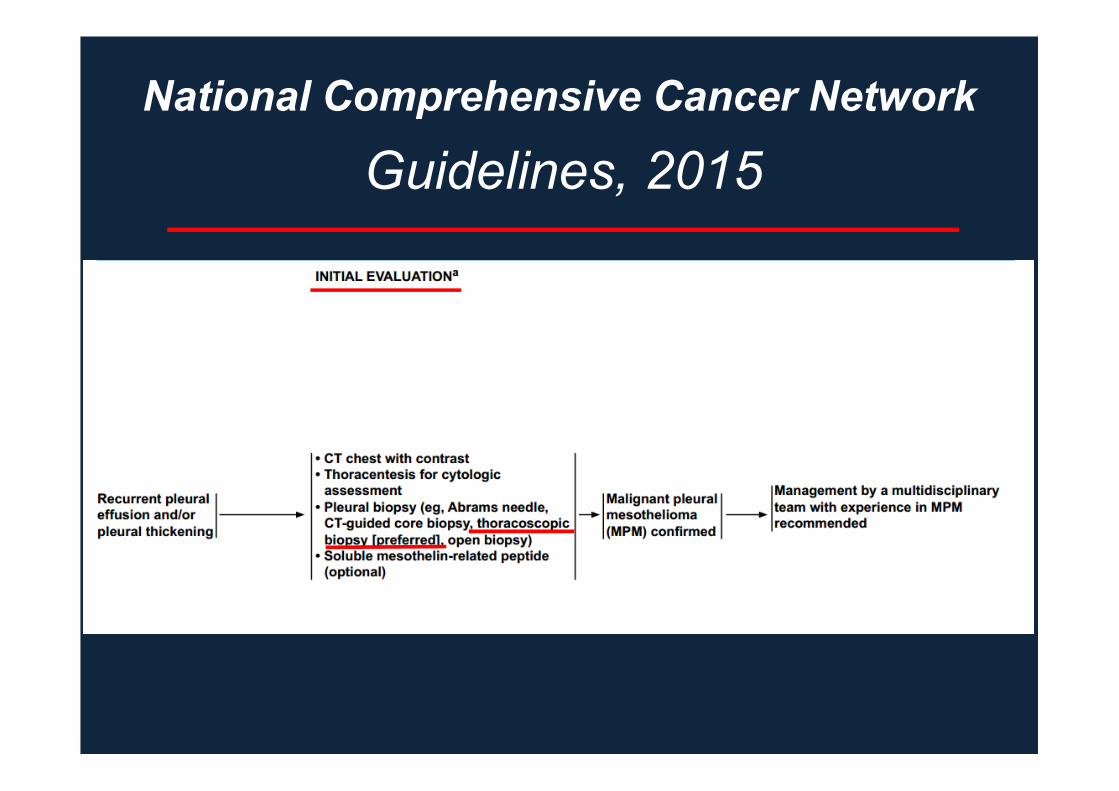
APPROCCIO DIAGNOSTICO
Versamento pleurico recidivante e/o ispessimenti pleurici:
• TC torace con mdc
• Toracentesi per esame citologico
• Biopsia pleurica– Con ago tranciante, TC-guidata
– Toracoscopia/Mappatura
– In mini-toracotomia
Istotipizzazione

(Butchart ‘79 – Brigham ‘93 – Sugarbaker ‘99)
STADIAZIONE
• PET
• RMN
• Mediastinoscopia
• EBUS
• Toracoscopia/Mappaggio pleurico
• Laparoscopia
In ogni caso, per le caratteristiche della malattia, la stadiazione clinica del MPM basata
sull’imaging è inaccurata.
La stadiazione definitiva può esserci solo dopo exeresi chirurgica

Esplorazione e biopsia
TORACOSCOPIA
Gli accessi toracoscopici dovrebbero essere effettuati nella sede della
potenziale successiva toracotomia
OTTICA COASSIALE

Mappaggio
TORACOSCOPIA
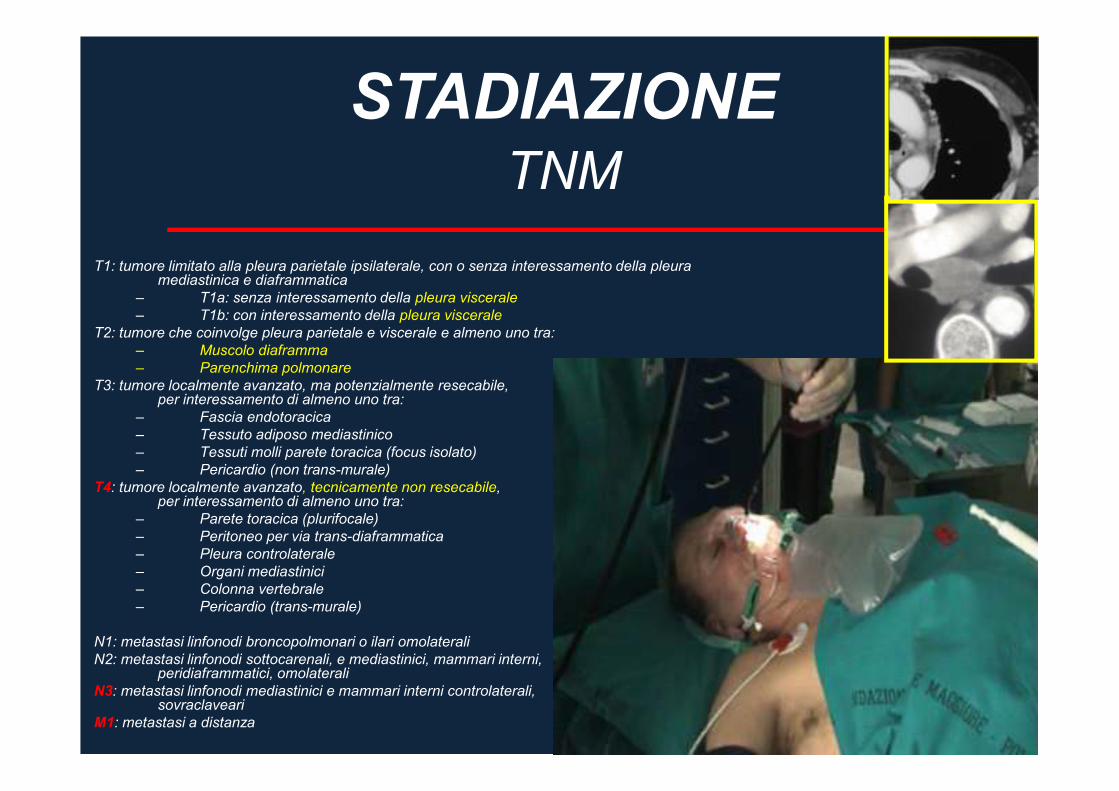
TNM
STADIAZIONE
T1: tumore limitato alla pleura parietale ipsilaterale, con o senza interessamento della pleura mediastinica e diaframmatica
– T1a: senza interessamento della pleura viscerale
– T1b: con interessamento della pleura viscerale
T2: tumore che coinvolge pleura parietale e viscerale e almeno uno tra:
– Muscolo diaframma
– Parenchima polmonare
T3: tumore localmente avanzato, ma potenzialmente resecabile, per interessamento di almeno uno tra:
– Fascia endotoracica
– Tessuto adiposo mediastinico
– Tessuti molli parete toracica (focus isolato)
– Pericardio (non trans-murale)
T4: tumore localmente avanzato, tecnicamente non resecabile, per interessamento di almeno uno tra:
– Parete toracica (plurifocale)
– Peritoneo per via trans-diaframmatica
– Pleura controlaterale
– Organi mediastinici
– Colonna vertebrale
– Pericardio (trans-murale)
N1: metastasi linfonodi broncopolmonari o ilari omolaterali
N2: metastasi linfonodi sottocarenali, e mediastinici, mammari interni, peridiaframmatici, omolaterali
N3: metastasi linfonodi mediastinici e mammari interni controlaterali, sovraclaveari
M1: metastasi a distanza

VALUTAZIONE CHIRURGICA
• Stadio clinico I-III
• Istologia epiteliale o mista
• Età, performance status
� Prove di funzionalità respiratoria
� Scintigrafia polmonare perfusoria
� Test da sforzo

Terapia
MESOTELIOMA PLEURICO
Il M.P. è un tumore:
– Chemioresistente
– Radioresistente
– La chirurgia da sola non offre buoni risultati
– Meglio le terapie multimodali
(N.Martini, 1996)


Terapia chirurgica
MESOTELIOMA PLEURICO
• Pleuropneumonectomia (Sugarbaker)
– Pneumonectomia extrapleurica con exeresi
pericardio e diaframma
– Linfoadenectomia mediastinica
• Pleurectomia / decorticazione
• Talcaggio pleurico (palliazione)
CHIRURGIA NEL MPM
Natura diffusa del MPM
� R0 impossibile
� ruolo fondamentale della terapia adiuvante e neoadiuvante
Chirurgia – Palliativa
– Citoriduttiva
– Radicale
Peculiarità

Talcaggio pleurico
CHIRURGIA PALLIATIVA
Comunque, primo tempo
indispensabile per EPP/P-D

Pleurectomia
CHIRURGIA PALLIATIVA

PNEUMONECTOMIA
EXTRA-PLEURICA

PNEUMONECTOMIA
EXTRA-PLEURICA

PNEUMONECTOMIA
EXTRA-PLEURICA

Legatura intrapericardica dei vasi
EPP
PNEUMONECTOMIA
EXTRA-PLEURICA

PNEUMONECTOMIA
EXTRA-PLEURICA

Patch pericardico
EPP

Patch su diaframma
EPP
PNEUMONECTOMIA
EXTRA-PLEURICA
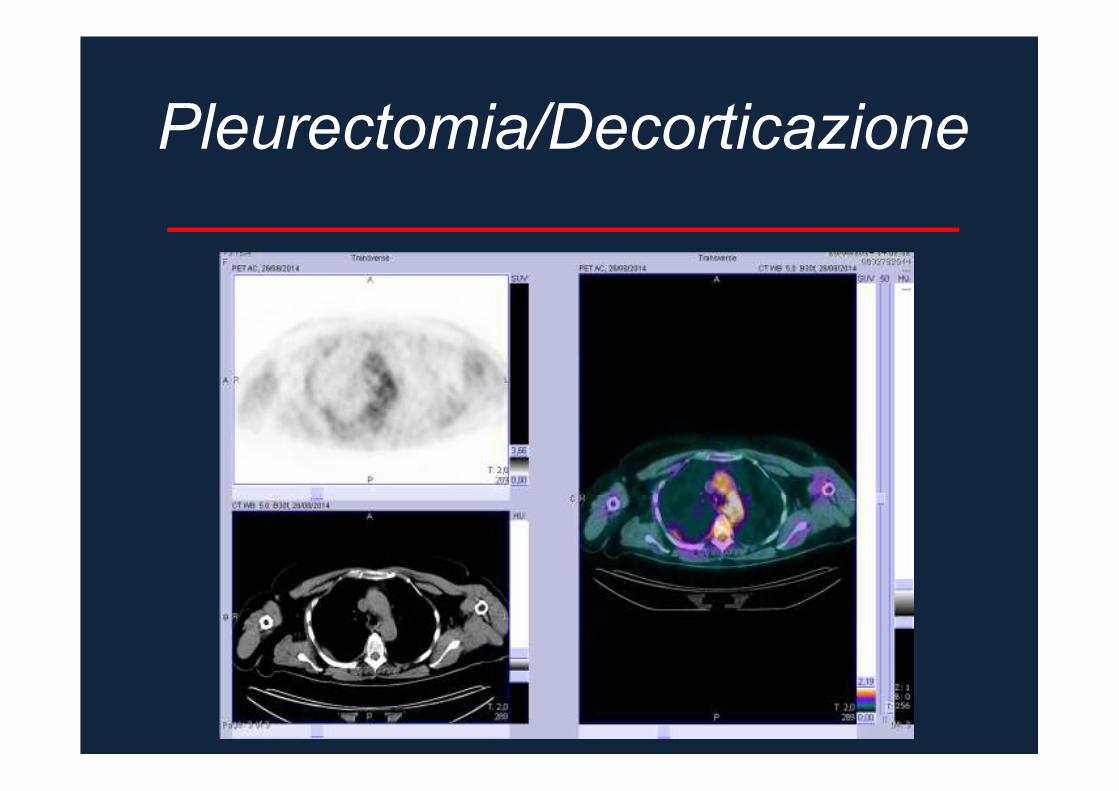
Pleurectomia/Decorticazione
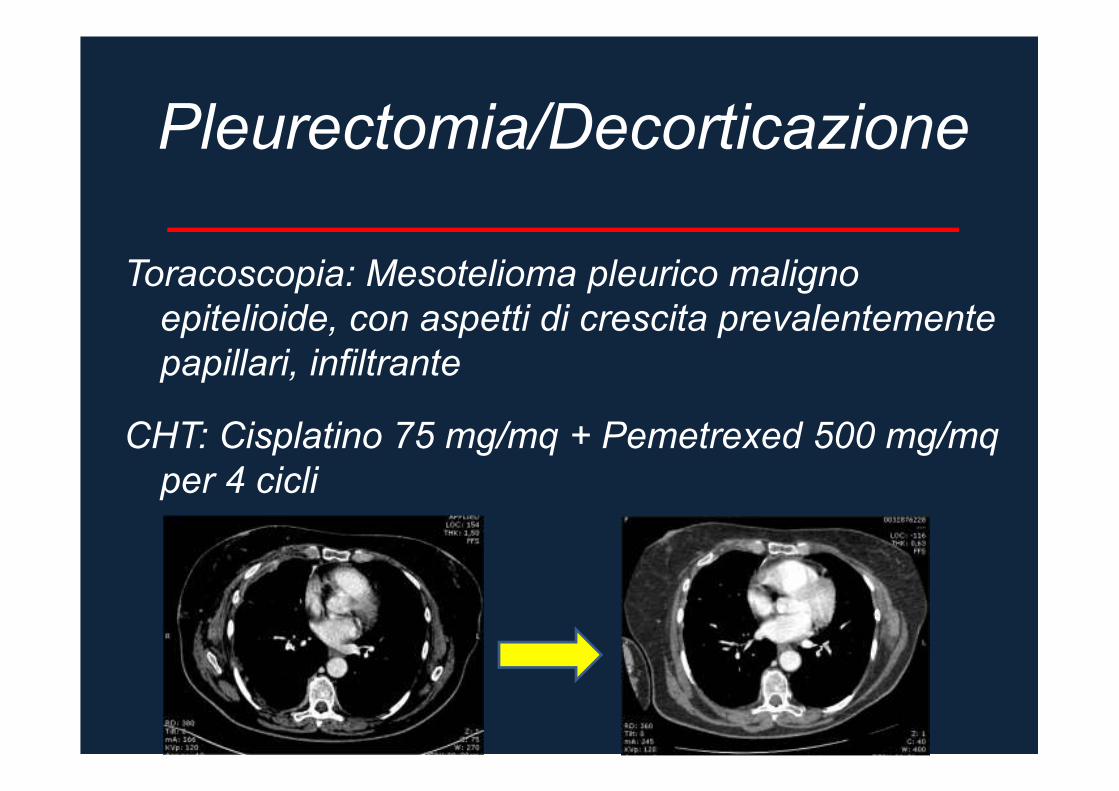
Toracoscopia: Mesotelioma pleurico maligno
epitelioide, con aspetti di crescita prevalentemente
papillari, infiltrante
CHT: Cisplatino 75 mg/mq + Pemetrexed 500 mg/mq
per 4 cicli
Pleurectomia/Decorticazione

Pleurectomia/Decorticazione
destra

Pleurectomia/Decorticazione
sinistra

Pleurectomia/Decorticazione
sinistra

Pleurectomia/Decorticazione
sinistra

Terapia chirurgica
MESOTELIOMA PLEURICO
Pleurectomia/dec. Mortalità 1,5%
Morbidità 9%
Pleurectomia/dec.
+ impianto barre RT
Sopravv. media 12,6 mesi;
15 mesi se malattia non macroscopic.
visibile
Pleurectomia/dec.
+ CT intraop (Cispl.-Mit.)
+ CT sistemica
Nessun vantaggio
EPP
Solo terapia medica
Mortalità 6%; Sopravvivenza =
Sopravvivenza peggiore
Martini, 1998
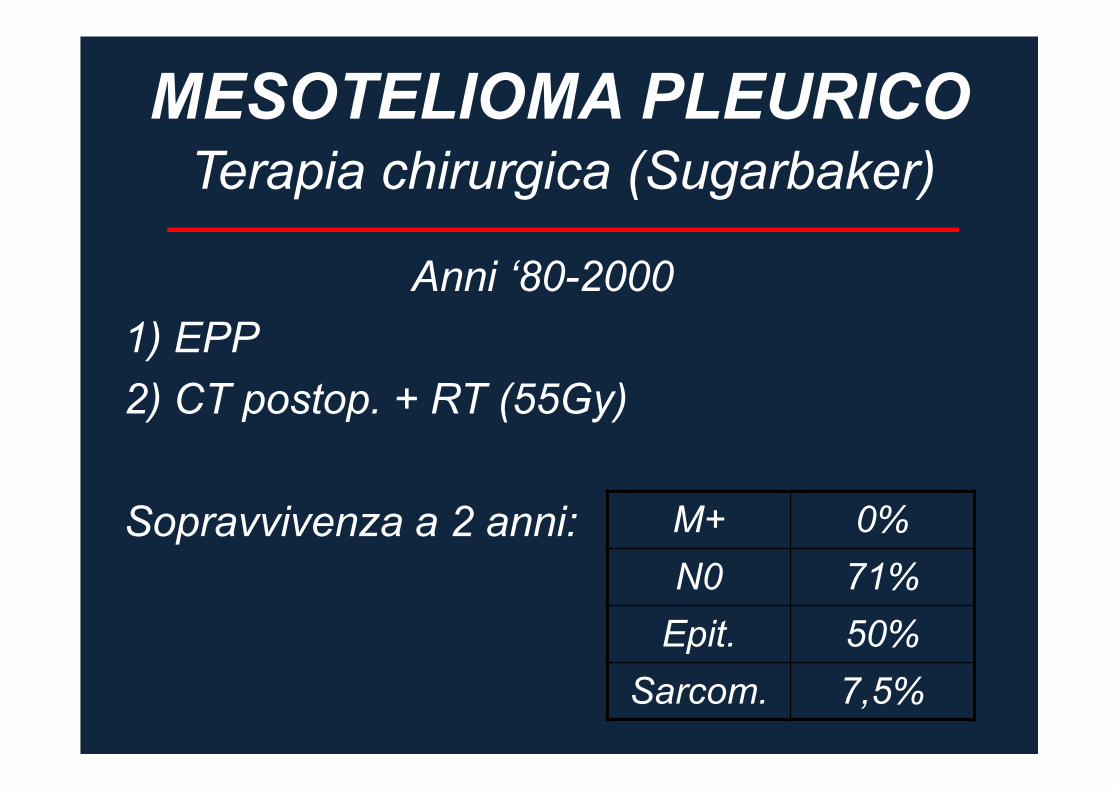
Terapia chirurgica (Sugarbaker)
MESOTELIOMA PLEURICO
Anni ‘80-2000
1) EPP
2) CT postop. + RT (55Gy)
Sopravvivenza a 2 anni: M+ 0%
N0 71%
Epit. 50%
Sarcom. 7,5%

In view of the high morbidity associated with EPP in this trial and in other non randomised studies
a larger study is not feasible. These data, although limited, suggest that radical surgery in the
form of EPP within trimodal therapy offers no benefit and possibly harms patients.

Lung Cancer, 2012
Extrapleural pneumonectomy for early stage
malignant pleural mesothelioma: a harmful
procedure.
Rena O, et al.
• Prospettico, non randomizzato (1998-2009)
• 77 pz con early stage MPM– 40 EPP
– 37 P/D
+ CHT-RT postoperatoria per entrambi i gruppi
“I, the present study suggests that P/D in a multimodal protocol ischaracterised by a lower morbidity and mortality, warranting abetter QoL up to recurrent disease and a longer survival afterrecurrence when compared with EPP. (I) When a diagnosis ofearly stage disease is made, I it should be proposed a lung-sparing procedure like the P/D in a multimodal protocol since theEPP should be confirmed to be superior in the disease control bydemonstrated evidences”

Annals of Thoracic Surgery, 2012
Quality of life after radical pleurectomy
decortication for malignant pleural mesothelioma.
Mollberg NM, et al.
• Prospettico (2010-2011)
• 28 PD radicale +/- CHT-RT
In conclusion, PD does not negatively impact minimally symptomatic
patients from baseline at intermediate follow-up. Patients who have
significant symptoms at baseline can have significant improvement
in their QoL after surgical resection.

Journal of Thoracic Oncoloy, 2012
Prospective study on functional results after
lung-sparing radical pleurectomy in the
management of MPM.
Bölükbas S, et al.
• Prospettico (2010)
• 16 Radical pleurectomy + CHT-RT
Lung-sparing RP leads to significant improvement of pulmonary
function and perfusion after a recovery time of 2 months. Functional
results are better after preservation of the diaphragm. Preservation
of physiological reserve via lung-sparing RP might allow patients
with MPM to be eligible for further therapeutic options in the long
term.

A best evidence topic in thoracic surgery was written according to a structured protocol. The question addressed was whether extrapleural
pneumonectomy (EPP) is superior to supportive care in the treatment of patients with malignant pleural mesothelioma (MPM). Overall, 110
papers were found using the reported search, of which 14 represented the best evidence to answer the clinical question. The authors, journal,
date and country of publication, patient group studied, study type, relevant outcomes and results are tabulated. We conclude that EPP
confers no advantage to chemotherapy and palliative treatment in terms of survival and symptom
improvement. Ten studies evaluated the role of EPP in the management of MPM. The median survival was 13 months and perioperative
and 30-day mortality rates were 5.7% and 9.1%, respectively. There was a high morbidity rate of 37% including atrial fibrillation, empyema and
supraventricular arrhythmias. Disease recurred in 73% of patients at a median time of 10 months. Median hospital stay was 13 days and
intensive care unit stay was 1.5 days. At three months postsurgery, improvement in symptoms was achieved in 68% of patients. Significant
advantages were observed in patients with epithelial MPM (19 vs. 8 months, P-0.01) compared to non-epithelial MPM and with N2 disease (19
vs. 10 months) compared to N1 or N0 disease, respectively. Two studies reported outcomes after chemotherapy in patients with MPM. The
median survival was 13 months and symptoms improved in 50% of patients. Response rate of 21% was achieved and the median time to
disease progression was 7.2 months. Postoperative haematological toxicity was common and included neutropenia (25%), anaemia (5%) and
thrombocytopenia (7.4%). Two studies analysed palliative treatment in mesothelioma and reported a median survival of seven months and
improvement in symptoms in 25% of patients at one-year post-treatment. The 30-day mortality rate was 7.8% and complications
included prolonged air leak (9.8%) and empyema (4%). Median hospital stay was seven days. Overall, EPP shows no benefit in terms of
survival or symptom improvement which is compounded by its high operative mortality and recurrence rate.
EPP is a highly morbid operation with high perioperative mortality and recurrence rate. Although a number of
retrospective studies have shown a small benefit in survival with EPP, there is consensual agreement that even
in subgroups with the best prognostic indicators (epithelial histology and N0/N1 disease), EPP still results in
high complication rates with minimal symptomatic improvement. Great weight should be given to the initial
findings of the MARS trial, which has clearly demonstrated the detrimental effects of conducting radical EPP
surgery compared to conservative management.
Guidelines, 2015
National Comprehensive Cancer Network

Guidelines, 2015
National Comprehensive Cancer Network

Guidelines, 2015
National Comprehensive Cancer Network
Importanza dei Trials Clinici
MESOTELIOMA PLEURICO
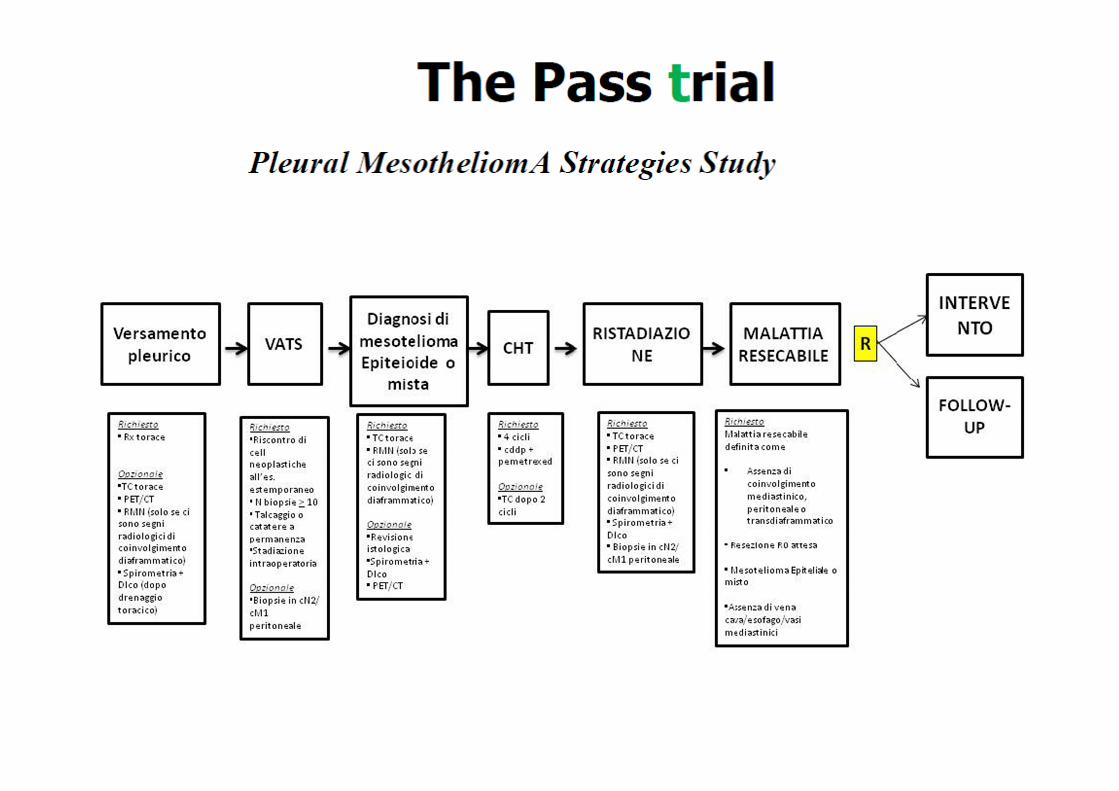
• The Pass trial (Pleural mesotheliomA
Strategies Study)
• Studio randomizzato prospettico
sull’efficacia del P/D (100 casi)
• Inizio Gennaio 2013
Importanza della ricerca di base
MESOTELIOMA PLEURICO
• Biobanca dei tessuti patologici
• Genomica
• Studio dei markers diagnostici/prognostici
Gary Lee YC, The Lancet 2014
Surgical resection of mesothelioma:
an evidence-free practice
• Extrapleural pneumonectomy (EPP) I has high postoperative mortality and morbidity. Extendedpleurectomy with decortication removes the samestructures but spares the lungI
• The MesoVATS trialI VAT-PP conferred no survival benefit over talc pleurodesis at 12 monthsI
• MARS (Mesothelioma And Radical Surgery) trialI median survival was 5 months shorter in the EPP group than in the no surgery groupI
• The more aggressive the procedure, the more complications it produces and the more detrimental it is to clinical outcomes.

Gary Lee YC, The Lancet 2014
Surgical resection of mesothelioma:
an evidence-free practice
• It often consists of multifocal tumours that can be histologically distinct (eg, epithelioid vs sarcomatoid) and has a predilection to spread along the pleural surfaces and invade deeper tissues, making complete surgical eradication practically impossible.
• I valuable evidence on the absence of benefit of surgical resection... Further forays into surgical resection of malignant pleural mesothelioma should be regarded as experimental, and should only be done within rigorous, high-quality clinical trials.

MESOTELIOMA PLEURICO
Il mesotelioma è una neoplasia maligna di cui
conosciamo molto della sua eziopatogenesi ma
abbiamo poche armi terapeutiche efficaci.
L’impressione è che qualunque terapia non cambi la
naturale evoluzione della malattia e che la
sopravvivenza dipenda dal momento della
diagnosi nell’ambito della naturale evoluzione della
malattia.
G. Chiappino

Conclusioni
MESOTELIOMA PLEURICO
• Sappiamo molto della eziopatogenesi del
mesotelioma e tra 20 anni si azzererà la
mortalità per scomparsa dell’amianto
nell’ambiente
• Per il tumore del polmone sappiamo molto
sulla eziologia da fumo. Perché non ci
applichiamo?
• Arriviamo sempre in ritardoI


Conclusioni
MESOTELIOMA PLEURICO