metaphase-arrest technique applied to human cervical epithelium. ii. cell production rates in normal...
TRANSCRIPT

Cell TissueKinef. (1985) 18, 321-331.
Metaphase-arrest technique applied to human cervical epithelium. 11. Cell production rates in normal and
pathological cervical epithelium
David Ireland Regional Department of GynaecologicalOnco1og.v. Queen Elizabeth Hospital, Gateshead. Tvne and Wear, U.K.
(Received 24 Ju1.v 1984: revision accepted 3 December 1984)
Abstract. An application of the metaphase-arrest technique to human cervical epithelium, in uiuo, was utilized to obtain cell birth rate data for seventy-six patients with normal and pathological cervical epithelium. Mean cell production rates for basal and parabasal layers of normal .epithelium were 0.9 1 and 0.92 cells/1000 cells/hr respectively. Histologically normal epithelium adjacent to CIN (cervical intra-epithelial neoplasia) had a significantly higher rate for the parabasal layer compared to the ‘normal’ group (P < 0.05). Values for the lower two-thirds of CIN I11 were 8-10 times higher than for normal epithelium, with microinvasive carcinoma having the highest rates of all. Values for wart-affected cervical epithelium (NCWVI) were intermediate between normal and CIN, but there was activity in the superficial layer, possibly reflecting activity of the papilloma virus. Large variation in birth rates between individuals in the same histological category was noted for each group, this being particularly the case in six patients with early invasive carcinoma.
The data is used to attempt to elucidate some of the uncertainties surrounding the aetiology and biological behaviour of cancer of the cervix and its precursors. Sources of inaccuracy are emphasized and practical difficulties discussed.
In uiuo cell kinetic studies of human neoplasia have been severely restricted because of ethical considerations. Whilst there have been a few attempts to construct fraction of labelled mitoses curves (e.g. Frindel & Tubiana, 1968; Muggia, Krezoski & Hansen, 1974, studying skin tumours and carcinoma of bronchus respectively), most data have been obtained from in uitro labelling of biopsy material. Their relevance to the true in uiuo situation is uncertain. The metaphase arrest technique has however been successfully applied in uiuo to the study of human neoplasms particularly of the gut (e.g. Camplejohn, Bone & Aherne, 1973: Wright et al., 1977) and in the study of psoriasis (Duffill, Wright and Shuster, 1976). This stimulated the author to attempt to apply the technique to the human cervix in uiuo, a study which has been described (Ireland & Monaghan, 1984).
Metaphase accumulation was demonstrated following the intra-epithelial administration of vincristine sulphate at an optimum dose of 50 pg/ml. This study presents the cell
Correspondence: Dr D. Ireland, Regional Department of Gynaecological Oncology, Queen Elizabeth Hospital, Gateshead, Tyne and Wear, U.K.
321

322 D. Ireland
production rates irr riro of normal cervical epithelium, cervical intra-epithelial neoplasia (C IN 1. non-condylomatous wart virus infection (NCWVI) and early invasive carcinoma of the cervix.
S U B J E C T S A N D M E T H O D S
The technique is fully described in part I of the study. In summary, a pre-determined optimum dose of vincristine sulphate (50 pglml) was injected directly into cervical epithelium of patients with CIN. NCWVI, microinvasive and early invasive carcinoma, under colpo- scopic control. The patients had all been listed for cone biopsy, abdominal hysterectomy, or radical hysterectomy. For normal controls, patients having hysterectomy for benign uterine pathology were selected. Colposcopically normal cervical epithelium adjacent to CIN was also studied. I n all cases diagnosis was confirmed by subsequent histology. CIN is charac- terized by cytological atypia. disorganization and mitotic activity and describes the continuum of disease from CIN I , the mildest abnormality affecting only the lower layers through to CIN 111. where changes affect the full thickness of the epithelium (Richart, 1973). The diagnosis of NCWVI was made if koilocytosis and multiple nucleation was present in the upper portion of the epithelium, with or without atypia in the lower portions. These features have been associated with wart-virus infection (Meisels. Fortin & Roy, 1977).
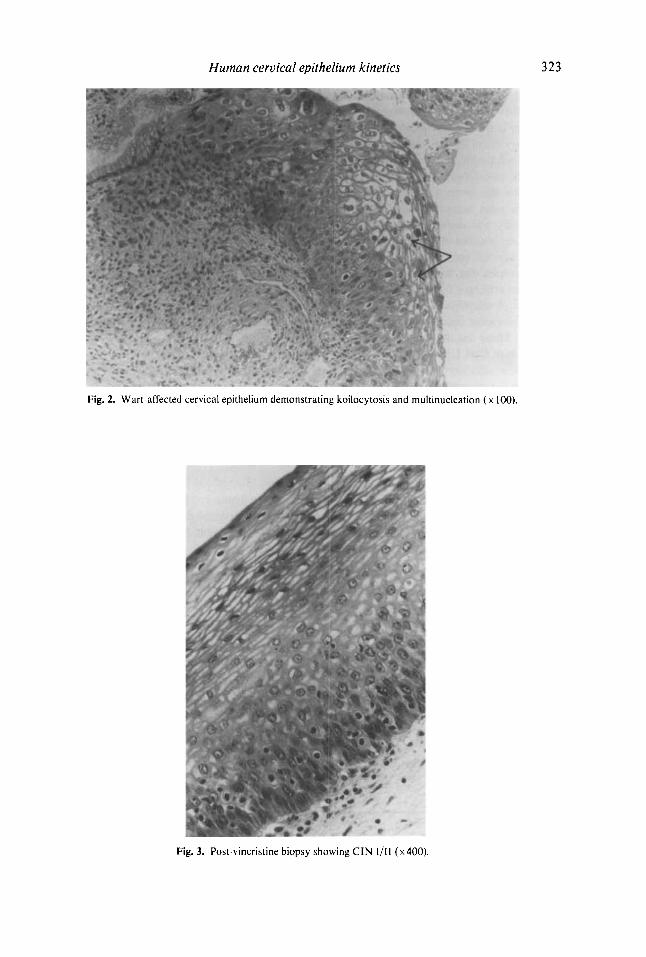
Figure 1 is a photomicrograph of normal cervical epithelium showing a single basal layer. a parabasal layer. and above these mature stratified squames. In contrast, Fig. 2 demonstrates koilocytosis (arrowed) and multinucleation. Figure 3 is a section obtained
Fig. 1. Histological appearance of normal cervical epithelium ( x400).
Human cervical epithelium kinetics
Fig. 2. Wart-affected cervical epithelium demonstrating koilocytosis and multinucleation ( x 100).
323
Fig. 3. Post-vincristine biopsy showing CIN 1/11 (~400).

324 D. Ireland
4 h after vincristine; the histological diagnosis is CIN 1/11, with metaphases clearly seen in the lower portion of the epithelium.
Serial biopsies were obtained during a 4-hr period following injection. Four 3 pm sections were obtained at 20 pm intervals from each biopsy and stained with haematoxylin and eosin. The metaphase index was plotted against time, the data fitted using least squares and the cell birth rate calculated from the slope of the line. A total of I12 patients was studied. Ethical permission has been obtained from the District Ethical Committee. Of the 112 patients, cell birth rates were not determined for thirty-six. In thirty of these patients, the lesion under study was demonstrated in one or two biopsies only. I n four others, accumulation of metaphases was not observed, and two patients found the technique too uncomfortable.
For normal epithelium, division was made into (i) basal (ii) parabasal and (iii) inter- mediate/superficial layers. For CIN, NCWVI and rnicroinvasive carcinoma, division was made into arbitrary thirds. The microinvasive category refers to areas of CIN 111 in association with foci of microinvasion. The foci themselves contained too few cells for counting. In all cases of invasive carcinoma. and in ten of those with C I N 111, division into thirds was not feasible. These results were therefore excluded from comparative studies, as were three subjects with CIN 1/11.
I n the results that follow, cell birth rates are expressed as cells11000 cells/hr. Confidence limits are not presented for each reading, but are wide in every case. A note was made of the patients’ oral contraceptive history. parity. and phase of the menstrual cycle. Those taking oral contraceptives at the time of the study are designated O.C. = 1, the remainder O.C. = 0.
R E S U L T S
Normal epithelium The data for eight patients in this group are presented in Table 1. The mean age of patients was 36 years (range 26-54 years). None had a history of cervical pathology. There was no significant difference between cell birth rates for the two layers. No mitotic activity was observed in the intermediate/superficial layers in any of the patients.
Table 1. Cell birth rates in eight patients with histologically normal epithelium
Birth rate (cells/1000 celk/hrj Patient no. Age Week in
( t i - 8 ) Basal Parabasal (years) O.C. Parity cycle
1 0.7 0 . 6 54 0 3 1 0 .3 0.4 39 0 3 4
3 0 . 7 I .o 39 0 2 1 4 0.9 0.8 32 0 1 4 > 0.8 1 . 1 28 1 2 2 6 I .o 1.7 29 I I 3 1 1 .7 1 .o 41 0 2 3 8 I . ? 0.8 26 0 2 3
1
Mean values 0.91 0.92 S.D. (0.41) (0.39)
~ ~ ~~~ ~ ~~
I , = 0.08. NS. O.C. = I : oral contraception used: O.C. = 0: oral contraception not used.

Human cervical epithelium kinetics 325
Histologically normal epithelium adjacent to CIN on the same cervix Biopsies were obtained from colposcopically normal epithelium adjacent to CIN on the same cervix. Results are presented in Table 2. The mean age of patients was 3 5 . 3 years (22-48 years). Normal and apparently normal epithelium were compared for both basal and parabasal layers. For the basal layer, there was no significant difference, but the difference reached significance for the parabasal layer ( f 1 9 = 2.82; P < 0.05).
Table 2. Cell birth rates in thirteen patients with histologically normal epithelium adjacent to CIN
Birth rate (cells/1000 cells/hr) Patient no. Age Week in
( n -- 13) Basal Parabasal (years) O.C. Parity cycle
9 4.1 2.3 22 0 2 2 10 0 . 4 6.1 48 0 5 1 I I 0.1 4.1 21 1 3 4 12 1.8 5.7 30 0 4 I 13 1.3 3.5 33 0 3 3 14 0 . 2 3 .1 28 I 2 1 15 1.2 3.9 39 1 3 2 16 2.2 2.9 27 1 1 2 17 0.8 0.6 32 0 2 3 18 0.8 1.8 48 0 7 3 19 1.2 1.2 4 s 0 3 4 20 1.3 0 .4 45 0 3 I 21 0.5 0.9 35 0 4 2
Mean values 1 . 1 5 2.81 (SD) (1.09) ( 1.84)
~~
I,, = 2.84: P < 0.05. There was in addition one subject with values of 9.2 and 11.0 cells/lOOO celldhr for basal and parabasal
layers respectively.
CIN 1/11 The mean values for these three patients were: lower third 4.6; middle third 5.2; upper third 0.0 cells/ 1000 cells/hr.
CIN 111 For the twenty patients with CIN 34.2 years (range 21-59 years). Although there was no difference the upper third were significantly
111, results are presented in Table 3. The mean age was Results show considerable variation between patients. between values for lower and middle thirds, values for lower than for the other two portions (by analysis of
variance). There was an obvious difference between CIN 111 and normal epithelium, the former having a cell birth rate eight to ten times higher.
Microinvasive carcinoma Values were obtained from six patients with microinvasive carcinoma. The mean age of patients in this group was 39.2 years (range 26-47 years). Birth rates are shown in Table 4.

3 26 D. Ireland
Table 3. Cell birth rates in twenty patients with C I N 111
Birth rate (cellsi'l000 cellsihr) Patient no. A F Week in
( t i = 20) Lower third Middle third Upper third (years) O.C. Parity cycle
2 2 23 24 2 5 26 27 28 29 30 31 32 _ . 7 7 34 3 5 36 37 38 39 40 41
hlean value\ (SD)
8 . 1 7.7 6.0 a 7
10 .7 4 . 0 5.9
8.4 18.4 4 . 3 6 .2 4 .3 5.9 6.1 6.2 5.4 6 . 7 4. I
16.3
2 . j
7.25 1 3 - 9 7 )
7.6 8 .2 6 . 4
16.2 7.9 5.5 3 . I 3.4 5 .O
18.8 8.6 6.7 4.3 3. I 7.9 5 .1 4.9
10.0 8 . 2 6 .9
7 .39 (3 .99 )
6 . 6 4 .2 I . 4 0.6 4 .4 0 . 7 0 . 2 0.4 1.4 0.3 1.4 2.9 0. I 0 .9 2.4 0.8 0 .9 1 . 1 2.6 0 .9
1.70 (1.70)
26 34 34 21 29 33 45 39 59 26 26 2 1 32 50 34 31 48 27 30 33
1 0 0 I 1 1 I 0 0 0 0 0 0 0 0 0 0 1 0 0
1 3 3 0 3 3 3 2 1 3 3 4 2 4 2 3 5 3 4 3
3 3 1 2 2 4 2 4 I 3 3 I 2 2 4 3 2 4 1 3
F , , , = 26.17:P < 0.001.
Table 4. Cell birth rates in six patients with microinvasive carcinoma -
Birth rate (cel1s;'IOOO cellslhr) Patient no. Age Week in
( ! I - 6 ) Lower third Middle third Upper third (years) O.C. Parity cycle
42 41 44 45 46 4'
Mean talues (SD)
4 .8 1 2 . 1 14.8 9.4 5.4 7 . 0
8.92 (3.95)
0 . 4 38 0 5 3 1 . 5 47 0 3 4 1.8 26 1 3 3 3.0 44 0 1 1 I . 4 42 0 6 I 0 . 9 38 0 5 1
1.50 (0.89)
F , ,,, -- 10.98: P < 0.01.
Non-condylomatous wart-virus infection Ten patients with NCWVI were included. The mean age was lower than the other groups (28.1 years. range 26-34 years). Birth rates are shown in Table 5. NCWVI, CIN and niicroinvasion were compared. The values for the lower two-thirds were significantly lower for NCWVI. but the difference betwccn microinvasion and CIN 111 was also just significant for the lower third.

Human cervical epithelium kinetics 327
Table 5. Cell birth rates in ten patients with NCWVI
Birth rate (cells/l000 cells/hr) Patient no. Age Week in (ti = 10) Lower third Middle third Upper third (years) O.C. Parity cycle
48 49 50 5 1 52 53 54 55 56 57
Mean values (SD)
2.3 2 .4 3 . 1 8.0 3.0 4 . 2 4 . 5 3.1 2 . 0 5. I
3.77 (1.80)
I .o 2.0 0 . 4 7 .2 1 .o 2.8 3 .O 2.1 1.4 3.0
2.39 (1.92)
0.0 1.5 1 . 5 1.7 0 .4 0 . 4 0 . 2 0 .8 0.1 0 . 2
0.68 (0.65)
28 34 30 26 30 24 24 33 26 26
0 0 0 0 0 0 0 0 0 0
2 1 2 4 1 2 2 1 2 2
4 1 2 4 3 4 1 2 3 4
F2,,R = 21.99: P < 0.01.
Relationship with oral contraceptive intake, parity, and stage of the menstrual cycle Only in the CIN 111 group was there a sufficient number with a history of oral contraception for a statistical test to be performed; no significant association was detected between birth rate and such history. There was no correlation between birth rate and either parity or stage of the cycle.
Correlation between cell birth rate and patient’s age For each group the correlation coefficient between patient’s age and cell birth rate was determined. There is an apparent tendency for birth rate to decline with age, although only in the middle third of CIN 111 did this reach significance (Table 6).
Table 6. Correlation coefficient between cell birth rate and patient’s age
Birth rate (cells/ 1000 cells/hr) CIN NCWVI Microinvasion
Lower third -0.16 -0.47 -0.48 Middle third -0.56* -0.38 -0.37 Upper third -0.19 0 .47 0.15
Normal Apparently normal Basal -0.18 -0.49 Parabasal -0.47 -0.11
* P < 0.05.
Cell birth rates in early invasive squamous carcinoma Table 7 lists birth rates for six patients with invasive squamous carcinoma (stage lb, FIG0 classification). Division into thirds was not possible. One patient only had pelvic node metastases (patient 59). All patients are free of disease at least 1 year after radical surgery, except patient 62 who died from a cerebral haemorrhage. The mean birth rate was 7 . 0 cells/ 1000 cells/hr (range 2.9-13.2).

328 D. Ireland
Table 7. Cell birth rates for six patients with invasive squamous carcinoma
Birth rate Patient no. (cells/ 1000 cells!hr) Pelvic node status
- 58 2 . 9 '9 I ? . ? + 60 3.4 -
61 7 . 5 -
6 2 10.7 -
6 3 4 . 3 ~
Pelvic node status: + Pelvic nodes involved in turnour: - pelvic nodes not involved in turnour.
D I S C U S ST O N
Birth rate data was not obtained from all patients studied (36 out of 112). The major reason for exclusion was inadequate biopsy material. unavoidable with the in civo technique. and the imperfect correlation of colposcopic appearances with histology.
The precision of individual values has already been shown to be doubtful, confidence limits being wide (Ireland & Monaghan. 1984a). There is likely to be variation in cell proliferathe activity between different areas of apparently similar histological abnormality in the same cervix. Llatjos & Rubio (1983). studying rodent cervical epithelium, demon- strated that cell proliferation occurred in clusters rather than evenly throughout a strip of epithelium: in our study it was noted that mitotic activity was greater in certain areas than in others. Despite careful attention to technique, there remains the possibility that the agent fails to reach all parts of the lesion in optimum dosage. This problem was confirmed by the finding of the occasional anaphase or telophase in this project. The optimum may indeed be different for normal and pathological epithelium. as Pritchett et al. (1982). discovered in their work on human colo-rectal tumours in tissue culture. However. limitations on the number of subjects available for study and the difficulty in accurately defining optimum dose in riro preclude more detailed dose-response studies.
The counting technique is laborious and in addition to observer error, section thickness may influence the count. Abercrombie (1946) showed that larger cells tend to be scored more frequently than smaller ones. To minimize this problem. all sections were cut at 3 pm. A further unknown factor is whether the biopsy procedure initiates a tissue reaction which will affect subsequent biopsies.
As Wright & Appleton (1980) emphasize. it would be misleading to attempt to derive specific values such as turnover time or potential doubling time from already imprecise cell birth rate data. Howeker. results for CIN I11 suggest a turnover time of several days. with that for normal epithelium being considerably longer. These values are longer than those proposed by Richart (1963). who suggested a turnover time for CIN 111 of 12 hr. However. in that study unjustified assumptions were made, and the data are of questionable value. Averette. Weinstein & Frost ( 1970) using an in uivo tritiated thymidine technique, estimated the cell generation times for basal and parabasal layers of normal epithelium to be 30 days and 3 days respectively. They proposed that the basal cells functioned as a reserve compartment. with mitotic activity confined to the parabasal compartment. In this present study. similar birth rates were obtained for the two layers, indicating that both participate equally in cell division. contradicting the reserve-cell concept.

Human cervical epithelium kinetics 329
Values may be compared with results from studies of other human epithelium. Wright et al. (1977) studying metaphase accumulation in human gastric carcinoma and adjacent normal mucosa found in both groups cell birth rates ranging from 3 to 24 cells/1000 cells/hr. Duffill et al. (1976) estimated cell production rates for psoriasis of 12.4 cells/1000 cells/hr, but with 95% confidence limits of 7.1-18.7 cells/1000 celldhr. The highest value in our series was 18.8 cells/1000 cells/hr in the middle third of the epithelium in a patient with CIN 111.
The higher cell production rates in CIN compared to normal cervical epithelium support the work of Rubio & Lagerlof (1974) who labelled sections from cone biopsies with tritiated thymidine followed by autoradiography. They noted a significant progressive increase in labelling from normal epithelium through to severe dysplasia.
The proponents of the multicellular origin of CIN (Coppleson & Reid. 1967; Johnson, 1969) suggest that the abnormality arises in a pre-determined field in the transformation zone containing a susceptible cell population. This was based on histological and colposcopic findings. A larger number of workers favour a unicellular origin. based on colposcopic, histological and glucose-6-phosphate dehydrogenase X-linked marker studies (Przybora & Plutowa, 1959; Richart, 1966; Smith, Townsend & Sparks, 1971). This present study shows a significantly higher cell production rate in histologically normal epithelium adjacent to CIN than for epithelium from a ‘normal’ cervix. This finding is in agreement with a study in which labelling indices were established for cervical punch biopsies (Ireland & Monaghan, 1985). A possible explanation could be that a substance diffuses from adjacent abnormal epithelium, stimulating basal and parabasal cells to proliferate more rapidly. No such growth factors have yet been isolated, however, and an alternative explanation may be that the apparently normal cells form part of a potentially neoplastic cervical epithelium, in which a biological perturbation precedes a histopathological change. This epithelium could then be susceptible to promotion by a carcinogen or other stimulus.
An agent currently receiving much attention as a possible promoter is the papilloma virus. The term NCWVI is used to describe changes thought to be induced in cervical epithelium by this virus. Typical histopathological, cytological and colposcopic changes have been described (koilocytosis, double nucleation, dyskeratosis) and the papilloma virus has been isolated from some of these lesions (Kirkup et al., 1982: Laverty et al., 1978: Meisels et al., 1977). Dysplastic changes are frequently noted in association with these observations. This study demonstrates birth rates for the lower two-thirds of NCWVI inter- mediate between normal and CIN 111. The majority exhibited histopathological atypia also in the lower two-thirds. It is not known whether such changes are co-incidental or are triggered by the papilloma virus. However, the demonstration of mitoses in association with the koilocytes in the superficial epithelial layers may be a reflection of viral incorporation into host DNA, stimulating cell division in normally mature, non-dividing superficial epithelium. This may explain the finding of Rubio & Lagerlof (1974) that. in their tritiated thymidine labelling experiment using cone biopsy sections, certain cases of mild to moderate dysplasia contained DNA-synthesizing cells in superficial layers. They suggested a disturbance in DNA regulation mechanisms by a carcinogenic agent.
Results in all groups in this study, particularly the CIN I11 group, show wide variation between individuals, with large standard deviations of the mean values. This may in part be explained by the suggestion of Dallenbach-Hellweg (1981) that there are two types of intra-epithelial neoplasia, one derived from the stratified squamous epithelium of the exocervix and the other developing on the basis of reserve-cell hyperplasia. The latter, she concludes, is characterized by a greater number of mitoses and more rapid proliferation, and may be

3 30 D. Ireland
the group that tend to invade early. Which preinvasive lesions regress and which progress to invasion is not known. and of course it would be unethical to leave patients untreated to resolve the issue. However. several studies (Fox, 1967: Gad, 1976; Murphy & Coleman, 1976) confirm that only a proportion of patients go on to develop invasive disease. This study does not help to identify which lesions are likely to go on to invasion. Practically, it is important to treat all preinvasive disease. and to include a margin of apparently normal tissue in the treatment field.
A number of recent reports have suggested a link between oral contraceptives and cervical cancer (e.g. Vessey. 1983). Few women in this study were oral contraceptive users; in the CIN group those taking oral contraceptives did not have higher rates. This suggests that in the group of women in this study, oral contraceptives do not significantly affect cell turnover. However, the between-patient variability for birth rates may mask a small difference. The tendency of cell birth rate to decline with age raises the likelihood of a hormonal influence; it is well established that oestrogens stimulate proliferation of the stratified squamous epithelium of the exocervix. with progestogens stimulating the columnar epithelium and the reserve cells beneath it (Dallenbach-Hellweg, 1981).
Values for invasive lesions are likely to be more imprecise because of tumour hetero- geneity. with greater mitotic activity at the growing edge compared to the relatively hypoxic, often necrotic central area. Results from the six patients studied show large variation between individuals. It may be significant that the highest value occurred in the one patient with pelvic node metastases. raising the possibility that the metaphase-arrest technique can be applied to predict which lesions carry a poor prognosis. More detailed knowledge of cervical cell kinetics is clearly essential if a more rational approach to the use of chemotherapy in advanced cervical cancer is to be achieved. Despite limitations, this technique does add to the data on human cervical cell proliferation in civo. allowing a dynamic parameter to be estimated which is not critically dependent on variables such as growth fraction and age distribution of the epithelium.
A C K N O W L E D G M E N T S
I am indebted to Dr David Appleton for performing the statistical analysis and for his invaluable advice throughout this project, and to Mr John Monaghan and Mr George Wilkinson for their encouragement and advice. Also I thank Mrs Shirley Cole, Miss Carol Rutherford, and Miss Deborah Steele for their meticulous preparation of the histological sections. This work was financed by the Evening Chronicle Laser Research Fund, and the colposcope provided by the North of England Cancer Campaign.
R E F E R E N C E S
A B E H C H O M B I ~ . M. ( 1946) Estimation of nuclear population from microtome sections. Anat. Rec. 94,239. AVERFTW. 1 i .E . . WEINSltlN. G.D. & FROST. P. ( 1970) Autoradiographic analysis of cell proliferation kinetics
CAMPLEJOHN. R.S.. BONE. G. & AHERNE. W. (1973) Cell proliferation in rectal carcinoma and rectal mucosa.
COPPLESON. M. & REID. B. (1967) Preclinical Carcinoma of the Cervix Uteri 1st edn. Pergamon Press, Oxford. D A L I - E N B ~ C H - ~ ~ E L L W E G . G. (1981) Structural variations of cervical cancer and its precursors under the influence
of exogenous hormones. In : Cerrical Cancer (Ed. by G. Dallenbach-Hellweg), p. 143. Springer-Verlag, N a v York.
DCFFILL. M.. WRIGHT. N.A. & SHUSTER. S . (1976) Cell population kinetics in psoriasis examined by three in riro techniques. Br. J . Dermatol. 94. 355.
in human genital tissues. Am. J. Obsrer. Gj.necol. 108. 8.
A stathmokinetic study. Eur. J . Cancer. 9. 577.

Human ceru ica 1 epithelium kinetics 33 1
Fox, C.H. (1967) Biologic behaviour of dysplasia and carcinoma in situ. Am. J. Obstet. Gynecol. 99, 960. FRINDEL, E. & TUBIANA, M. (1968) Cell proliferation kinetics in five human solid tumours. Cancer, 22,6 11. GAD, C. (1976) The management and natural history of severe dysplasia and carcinoma in situ of the uterine
cervix. Br. J. Obsfet. Gynaecol. 83, 554. IRELAND, D. & MONAGHAN, J.M. (1984a) The metaphase-arrest technique applied to human cervical epithelium.
I. Technique and dose-response studies. Cell Tissue Kinef. 17, 509. IRELAND, D. & MONAGHAN, J.M. (1985) A critical evaluation of three methods of studying cell proliferation
in human cervical epithelium. Obstet. Gvnecol. (in press). JOHNSON. L.D. ( 1969) The histopathological approach to early cervical neoplasia. Obstef. G.vnecol. Sun>.
24,135. KIRKUP, W., EVANS, AS., BROUGH, A.K., DAVIS, J.. O’LOUGHLIN, T., WILKINSON. G. & MONAGHAN, J.M.
(1982) Cervical intraepithelial neoplasia and ‘warty’ atypia-a study of colposcopic. histological and cytological characteristics. Br. J. Obstet. Gynaecol. 89, 571.
LAVERTY, C.R.. RUSSELL, P., HILLS, E. & BOOTH, N. (1978) The significance on non condylomatous wart virus infection of the cervical transformation zone. A review with discussion of two illustrative cases. Acta Cytol. 22. 195.
LLATJOS, M. & RUBIO. C.A. (1983) Kinetics of cell replication in the uterine cervix. IV. Loci of DNA- synthesising cells and arrested mitoses in the basal-layer. Acta Cytol. 27,454.
MEISELS, A., FORTIN, R. & ROY. M. (1977) Condylomatous lesions of the cervix. 11. Cytologic, colposcopic and histopathologic study. Acta Cytol. 21, 379.
MUGGIA. F.M., KREZOSKI, S.K. & HANSEN, H.H. (1974) Cell kinetic studies in patients with small-cell carcinoma of the lung. Cancer. 34, 1683.
MURPHY. W.M. & COLEMAN, S.A. (1976) The long term course of carcinoma in situ of the uterine cervix. Cancer, 38,957.
PRITCHETT, C.J., SENIOR, P.V., SUNTER. J.P., WATSON, A.J., APPLETON, D.R. & WILSON, R.G. (1982) Human colo-rectal tumours in short-term organ culture. A stathmokinetic study. Cell Tissue Kinet. 15,555.
PRZYBORA, L.A. & PLUTOWA, A. (1959) Histopathological topography of carcinoma in sifu of the cervix uteri. Cancer, 12,263.
RICHART, R.M. (1963) A radioautographic analysis of cellular proliferation in dysplasia and carcinoma in situ of the uterine cervix. Am. J . Obstet. Gynecol. 86,925.
RICHART, R.M. (1 966) Colpomicroscopic studies of cervical intraepithelial neoplasia. Cancer, 19. 395. RICHART, R.M. (1973) Cervical intraepithelial neoplasia. In: Parhology Annunl (Ed. by S. C. Sommers), p. 301.
RUBIO, C.A. & LAGERLOF, B. (1974) Autoradiographic studies of dysplasia and carcinoma in situ in cervical
SMITH, J.W., TOWNSEND. D.E. & SPARKS, R.S. (197 1) Genetic variants of glucose-6-phosphate dehydrogenase
VESSEY, M.P. (1983) Oral contraceptives and cervical cancer. Lancet, 2. 1358. WRIGHT, N.A. & APPLETON, D.R. (1980) The mataphase arrest technique. A critical review. Cell Tissue Kinet.
WRIGHT, N.A., BRITTON, D.C., BONE, G. & APPLETON, D.R. (1977) An in uiuo stathmokinetic study of cell
Appleton-Century-Crofts, New York.
cones, Acta Pathol. Microbiol, Scand. 82,4 1 1.
in the study of carcinoma of the cervix. Cancer, 28. 529.
13, 643.
proliferation in human gastric carcinoma and gastric mucosa. Cell Tissue Kinet. 10, 429.