methadone maintenance in the treatment of heroin addiction prop 36 claim meeting - oct 2003 joan e....
TRANSCRIPT
Methadone Maintenance in the Treatment of Heroin
Addiction
Methadone Maintenance in the Treatment of Heroin
Addiction
Prop 36 CLAIM Meeting - Oct 2003
Joan E. Zweben, Ph.D.Executive Director: 14th Street Clinic and EBCRP
Clinical Professor of Psychiatry; University of California, San Francisco
Prop 36 CLAIM Meeting - Oct 2003
Joan E. Zweben, Ph.D.Executive Director: 14th Street Clinic and EBCRP
Clinical Professor of Psychiatry; University of California, San Francisco
Questions & IssuesQuestions & Issues
How important is methadone in treating heroin addiction?
What is the rationale? What is the data? How do we decide when/if it can be
discontinued? What is included in the psychosocial
component of treatment?
Natural History of Heroin Addiction: A 33-Year Follow-up (1)
Natural History of Heroin Addiction: A 33-Year Follow-up (1)
581 male heroin addicts, admitted to Calif Civil Addicts Program, 1962-1964
CAP: compulsory drug tx for heroin-dependent criminal offenders
284 dead; 242 interviewed High rates of disability, hepatitis,
excessive drinking, cigarette smoking, marijuana use, other drug-related problems
(Hser et al, 2001)
Narcotics Addicts: A 33-Year Follow-up (2)
Narcotics Addicts: A 33-Year Follow-up (2)
Between 1985-1986 to 1996-1997: Dead: 49% Abstinent: 20%-22% Incarcerated: 4%-7% Methadone maintenance: 2%-6% Occasional use: 2%-3% Lost to follow-up: 12
(Hser et al, 2001)
Opiate Dependency:Hidden Populations
Opiate Dependency:Hidden Populations
Subscribers of Private Insurance Plan:
Empire Blue Cross/Blue Shield, NYC estimated from opiate dependency
diagnosis on admission & AIDS cases insured 141,000 opiate users between
1982-1992 85,000 among current subscribers
(1992)(Eisenhandler & Drucker, 1993)
Treatment Outcome Data: Methadone
Treatment Outcome Data: Methadone
8-10 fold reduction in death rate Reduction of drug use Reduction of criminal activity Engagement in socially productive roles;
improved family and social function Increased employment Improved physical and mental health Reduced spread of HIV Excellent retention
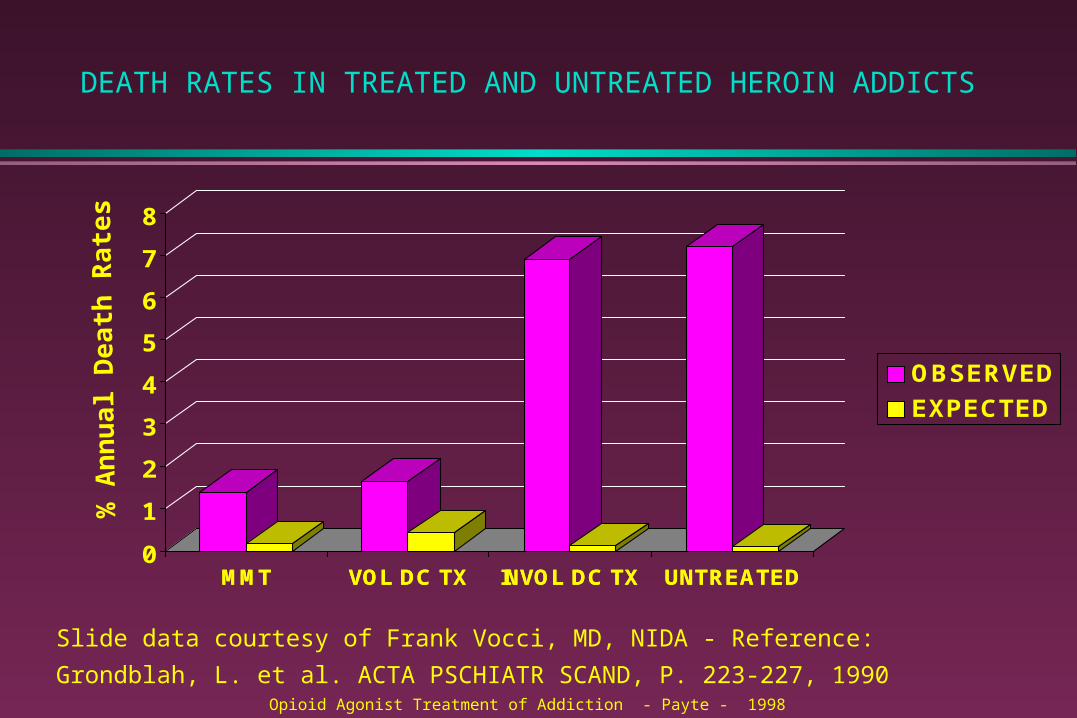
DEATH RATES IN TREATED AND UNTREATED HEROIN ADDICTS
MMT VOL DC TX INVOL DC TX UNTREATED0
1
2
3
4
5
6
7
8
MMT VOL DC TX INVOL DC TX UNTREATED
OBSERVED
EXPECTED
Slide data courtesy of Frank Vocci, MD, NIDA - Reference: Grondblah, L. et al. ACTA
PSCHIATR SCAND, P. 223-227, 1990
% A
nn
ua
l De
ath
Rat
es
Opioid Agonist Treatment of Addiction - Payte - 1998
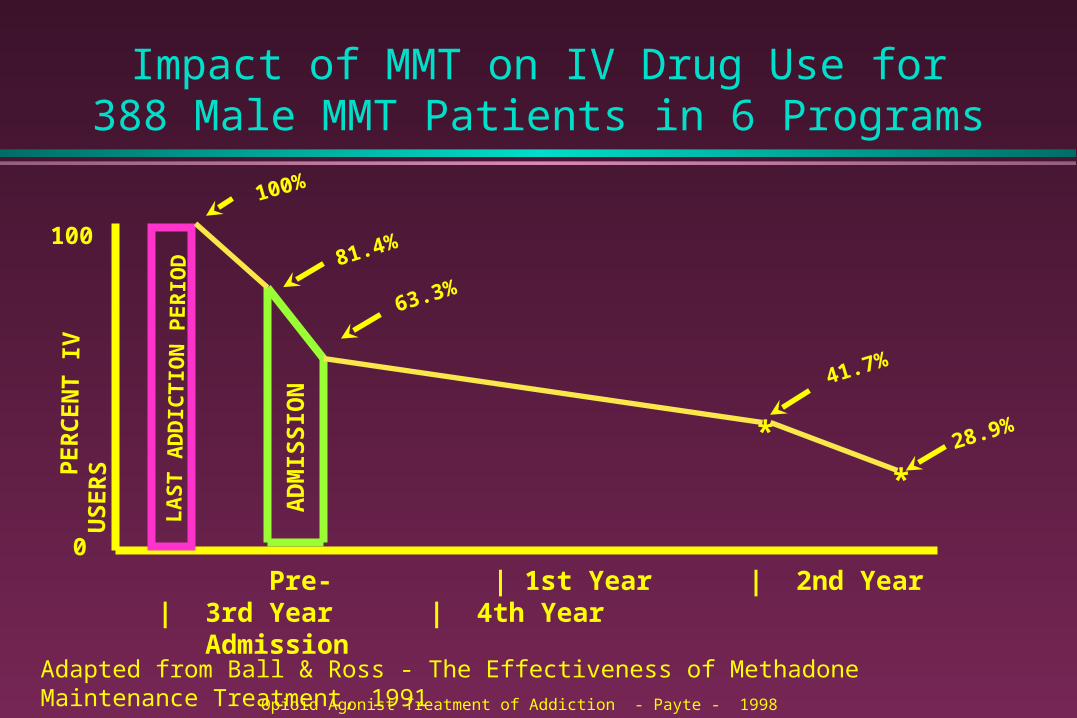
Impact of MMT on IV Drug Use for 388 Male MMT Patients in 6 Programs
P
ER
CE
NT
IV
US
ER
S
0
100
LA
ST
AD
DIC
TIO
N P
ER
IOD
AD
MIS
SIO
N
100%
81.4%
Pre- | 1st Year | 2nd Year | 3rd Year | 4th Year Admission
*
*
63.3%
41.7%
28.9%
Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991Opioid Agonist Treatment of Addiction - Payte - 1998
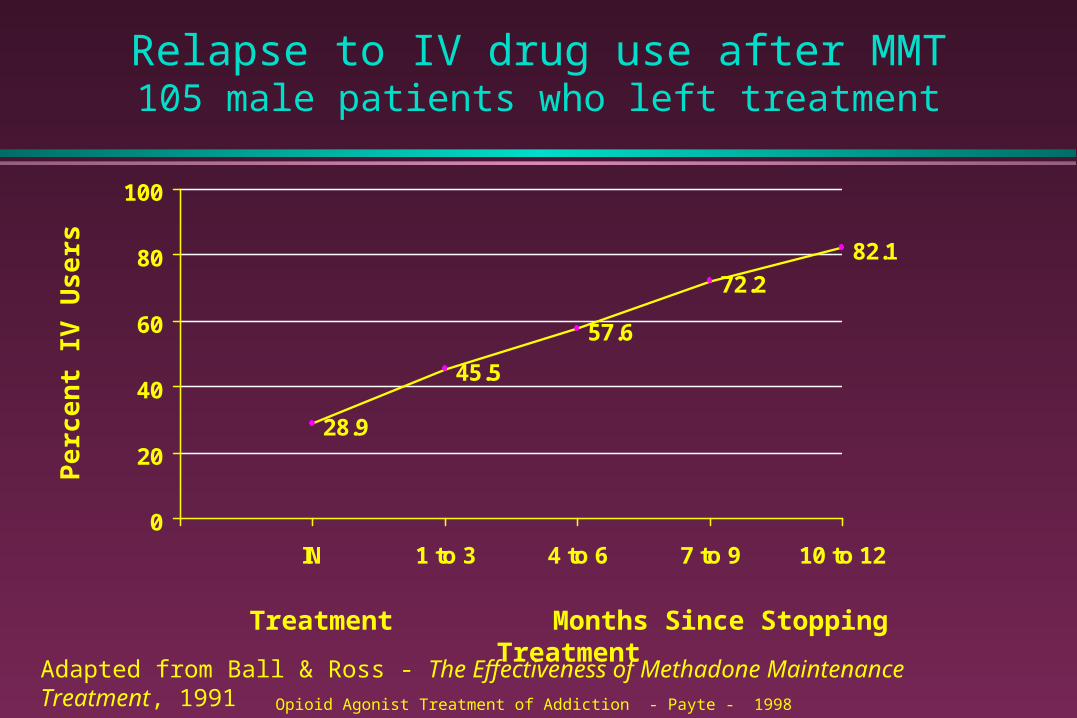
Relapse to IV drug use after MMT105 male patients who left treatment
28.9
45.5
57.6
72.2
82.1
0
20
40
60
80
100
IN 1 to 3 4 to 6 7 to 9 10 to 12
Pe
rce
nt
IV U
se
rs
Treatment Months Since Stopping Treatment
Opioid Agonist Treatment of Addiction - Payte - 1998
Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991
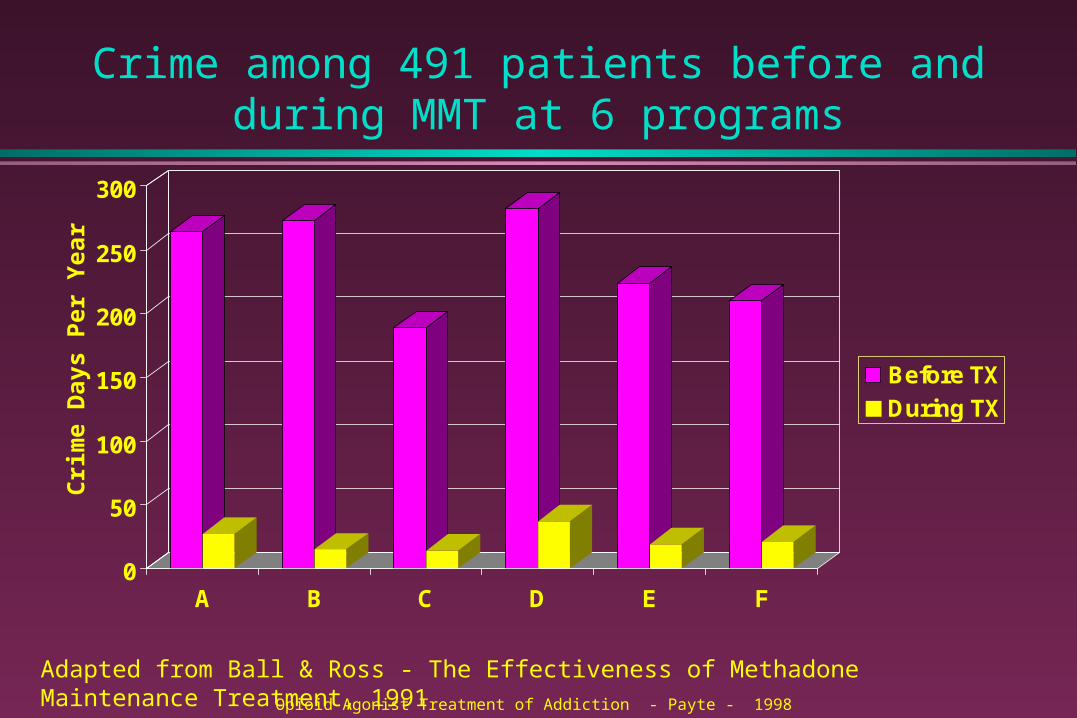
Crime among 491 patients before and during MMT at 6 programs
0
50
100
150
200
250
300
A B C D E F
Before TX
During TX
Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991
Cri
me
Day
s P
er Y
ear
Opioid Agonist Treatment of Addiction - Payte - 1998
Opioid Maintenance Pharmacotherapy - A Course for Clinicians - 1997
HIV DISEASE
• Role of MMTP
– Education, counseling, and testing -- prevention
– Decrease HIV transmission by decreasing needle sharing
– For HIV (+) patients, provide, refer, and coordinate treatment
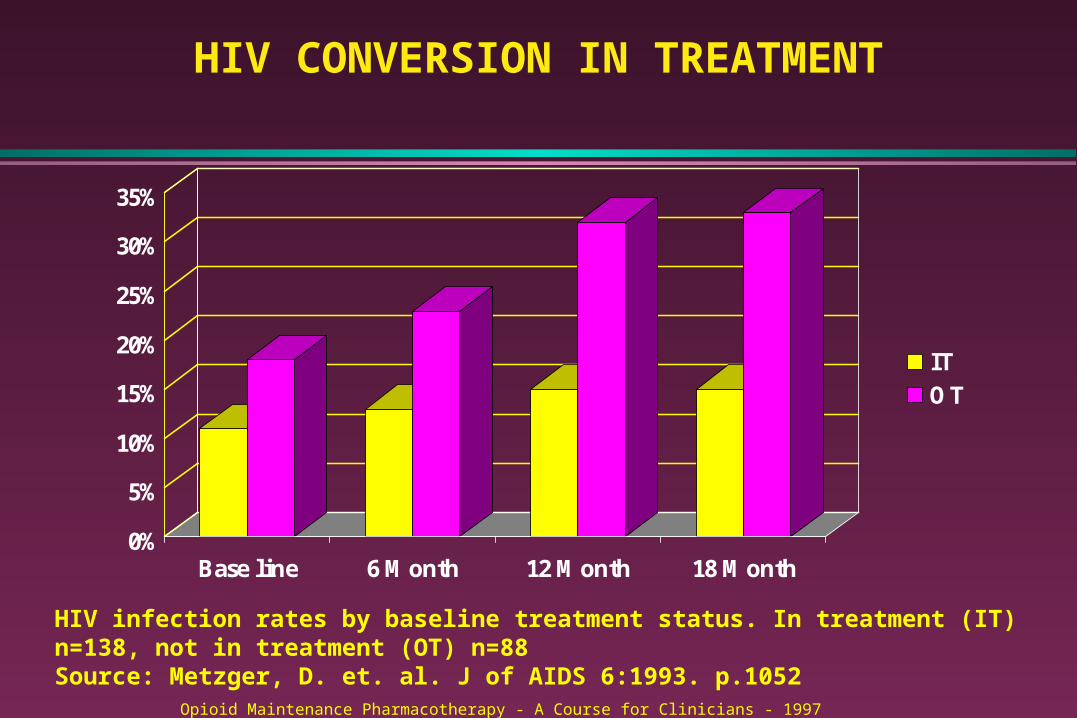
HIV CONVERSION IN TREATMENT
0%
5%
10%
15%
20%
25%
30%
35%
Base line 6 Month 12 Month 18 Month
ITOT
HIV infection rates by baseline treatment status. In treatment (IT) n=138, not in treatment (OT) n=88Source: Metzger, D. et. al. J of AIDS 6:1993. p.1052
Opioid Maintenance Pharmacotherapy - A Course for Clinicians - 1997

OPIOID MAINTENANCE
THERAPY
OPIOID MAINTENANCE
THERAPY
The Addiction Process:Barriers to Understanding
INFLUENCE OF THE STIGMA: difficulty understanding the complexity of
the disorder treatment is denied treatment is diminished treatment is discouraged treatment is conditional
“I Don’t Believe in Methadone”
Methadone is a medication,
not a religionJ. Thomas Payte, MD
Founding Chair, Methadone Treatment Committee, ASAM
Overview:Opioid Maintenance
Therapy
Overview:Opioid Maintenance
Therapy
Methadone (MMT) & levoacetylmethadol (LAAM), buprenorphine (soon)
most highly regulated history rationale for replacement therapy political influences diversion
OMT, ContinuedOMT, Continued
Strong empirical support for safety and efficacy (30 years of data)
valuable tool in reducing spread of HIV makes the pt accessible to interventions
for other problems hidden populations of heroin users medical maintenance and office-based
practice
What is Abstinence?
Medication is compatible with 12-step participation if appropriately prescribed by physician knowledgeable about addiction
Pt on methadone is abstinent if not using illicit drugs and using legal ones as prescribed
It’s just another medication. Meds are a tool, not a solution
Dole: Receptor System Dysfunction
Endogenous ligand-narcotic receptor system is defective; hence high relapse rate
Stabilize blood level at 150-600 ng/mL This normalizes neurological and endocrine
functioning This treatment is corrective but not curative Future research: identify the specific defect and
repair it(Dole, JAMA 1988)
Genetic Factors
Recent studies show distinct genetic vulnerability to heroin and other opiates:
heroin had larger genetic influences unique to itself than marijuana, sedatives, stimulants, psychedelics (Tsuang et all; Merikangas et al; ARCHIVES 1998)
Alcoholism and drug disorders appear to be independent
Genetic factors impact the transition from drug use to abuse/dependence, not use itself
Diversion of Medication
political hot button key issue in formulating original regs IOM report: cannot document significant
public health or safety problem confusion about DAWN data difficulty of determining cause of death
(Rettig 1995)
Reasons for Diversion
selling take-homes to buy illicit drugs need to supplement income share with or sell to addicted friend/mate unwilling or unable to enter treatment low dose policies of some programs
IOM conclusion: risks of diverted methadone do not outweigh benefits of making MMT more available
(Rettig 1995)
PHARMACOTHERAPYPHARMACOTHERAPY
Methadone vs HeroinMethadone vs Heroin
Can be taken by mouth Slow onset of action No continuing increase in tolerance levels
after optimal dose is reached; relatively constant dose over time
Pt on stable dose rarely experiences euphoric or sedating effects; is able to perceive pain and have emotional reactions; can perform; can perform daily tasks normally and safely
Methadone vs Heroin (2)Methadone vs Heroin (2)
Long acting; prevents withdrawal for 24-36 hours (4x-6x as long as heroin), permitting once-a day-dosing
At sufficient dosage, blocks euphoric effect of normal street doses of heroin
Medically safe when used on long-term basis (10 years or more)
(Physician’s Guide: Opioid Agonist Medical Maintenance Treatment; CSAT 2000)
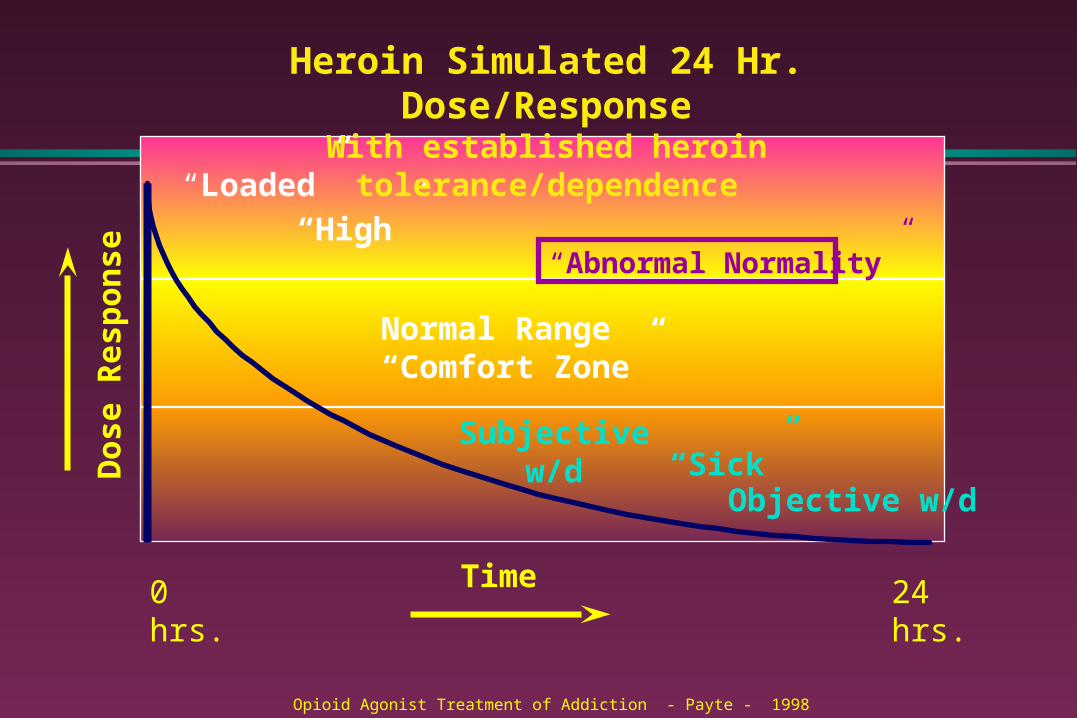
Do
se R
esp
on
se
Time
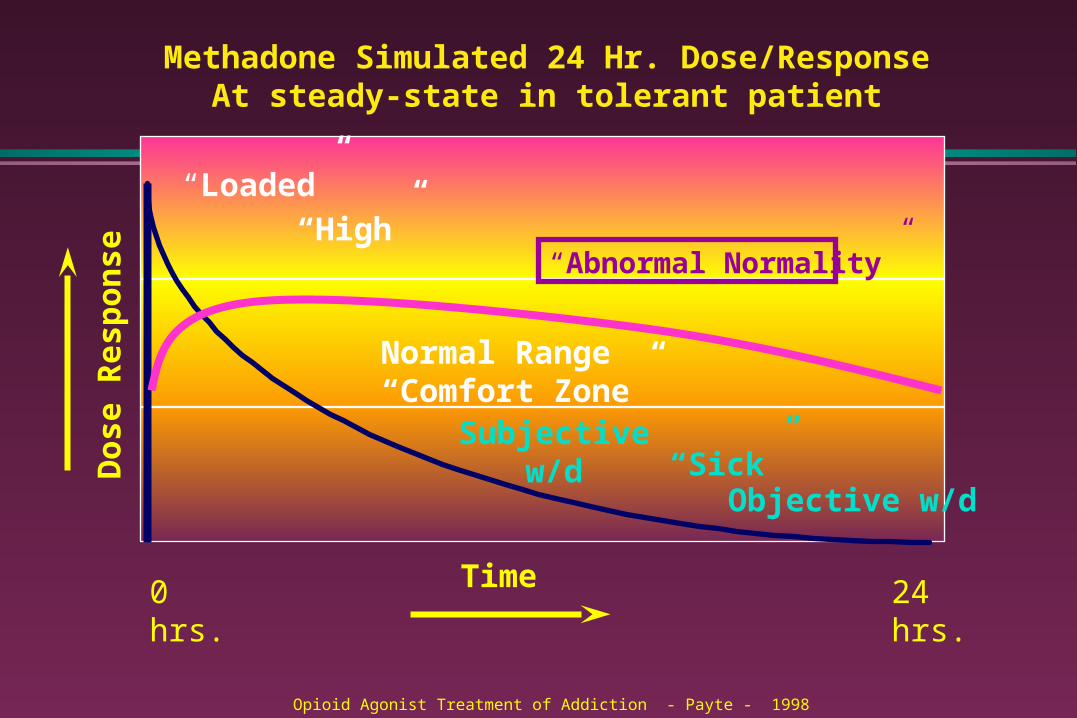
“Loaded” “High”
Normal Range“Comfort Zone”
“Sick”
Heroin Simulated 24 Hr. Dose/ResponseWith established heroin tolerance/dependence
0 hrs. 24 hrs.
“Abnormal Normality”
Subjective w/d
Objective w/d
Opioid Agonist Treatment of Addiction - Payte - 1998
Opioid Agonist Treatment of Addiction - Payte - 1998
GOALS FOR PHARMACOTHERAPY
• Prevention or reduction of withdrawal symptoms
• Prevention or reduction of drug craving
• Prevention of relapse to use of addictive drug
• Restoration to or toward normalcy of any physiological function disrupted by drug abuse
Source: MJ Kreek, Rationale for Maintenance Pharmacotherapy of Opiate Dependence, 1992
PROFILE FOR POTENTIAL PSYCHOTHERAPEUTIC AGENT
Effective after oral administration
Long biological half-life (>24 hours)
Minimal side effects during chronic administration
Safe, no true toxic or serious adverse effects
Efficacious for a substantial % of persons with the disorder (> 15-20%)
Opioid Agonist Treatment of Addiction - Payte - 1998
Source: MJ Kreek, Rationale for Maintenance Pharmacotherapy of Opiate Dependence, 1992
Do
se R
esp
on
se
Time
“Loaded” “High”
Normal Range“Comfort Zone”
“Sick”
Methadone Simulated 24 Hr. Dose/ResponseAt steady-state in tolerant patient
0 hrs. 24 hrs.
“Abnormal Normality”
Subjective w/d
Objective w/d
Opioid Agonist Treatment of Addiction - Payte - 1998
“Not Holding” Strategies
Cognitive, Behavioral Interventions Increased contact, counseling,
therapyAlter urinary pH? Is patient fixing? - Raise doseSplit Dose?
Opioid Agonist Treatment of Addiction - Payte - 1998
Payte - Khuri
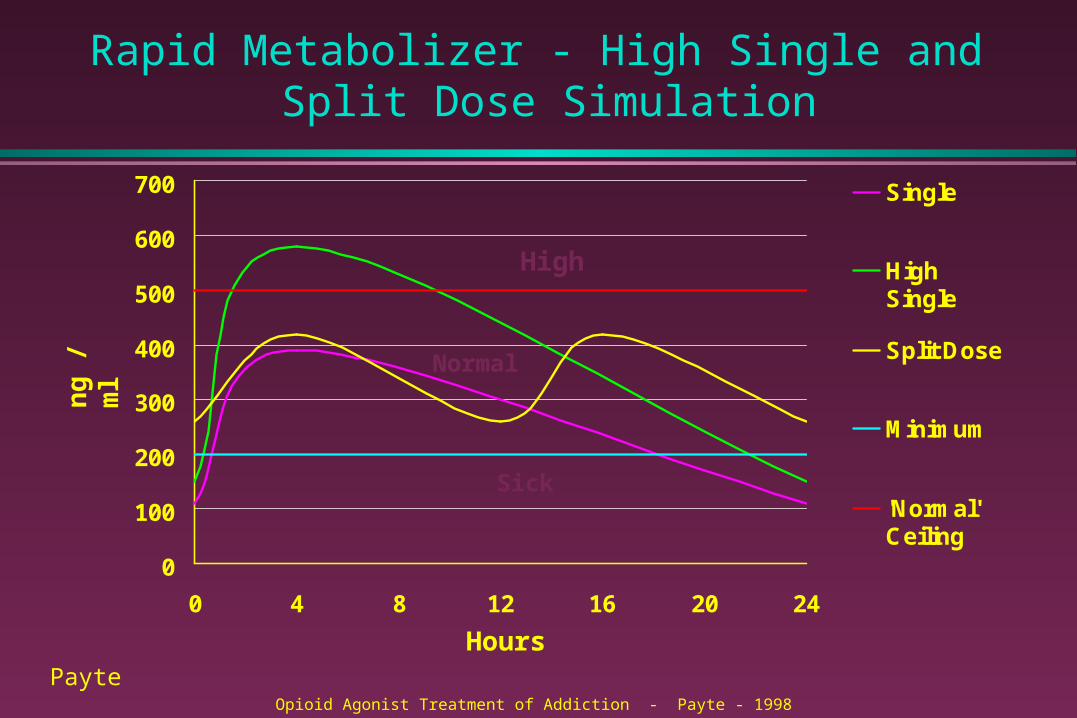
Rapid Metabolizer - High Single and Split Dose Simulation
0
100
200
300
400
500
600
700
0 4 8 12 16 20 24
Single
HighSingle
Split Dose
Minimum
'Normal'Ceiling
High
Normal
Sick
Opioid Agonist Treatment of Addiction - Payte - 1998
Payte
ng
/ m
l
Hours
TAPERING
how many remain abstinent? tapering readiness tapering strategies clonidine handling relapse
Buprenorphine (1)Buprenorphine (1)
1970’s - partial opioid agonist useful in opioid dependence treatment
1990’s - clinical trials long duration of action; smooth onset low physical dependence mild withdrawal syndrome good name on the street
Buprenorphine (2)Buprenorphine (2)
DATA 2000 permitted use in MD office FDA approved Subutex and Suboxone in
2002 Physicians must meet training
requirements: certified in addiction medicine, participated in clinical trials, or took 8 hour course by specified organizations
Buprenorphine (3)Buprenorphine (3)
SUBUTEX & SUBOXONE Sublingual tablets Suboxone has naloxone added to
discourage needle use Partial agonist: ceiling effect Expensive: $300/month at average dose Not interchangeable with methadone
Buprenorphine (4)Buprenorphine (4)
Poor oral bioavailability Sublingual administration requires
longer observation Abuse documented in Europe, Australia,
and New Zealand How much training should be required
for physicians to use it?
Naltrexone
antagonist; how it works who does it work for? accelerated withdrawal protocols Dole’s critique utility with alcoholics
Methadone in Pregnancy
Methadone in Pregnancy
Comprehensive MMT treatment with prenatal care improves neonatal outcome
Withdrawal is rarely appropriate during pregnancy
Methadone is not teratogenic; children have been followed into adulthood
Appropriate dosing is very important Breast feeding OK if no other drug use
Opioids and Chronic PainOpioids and Chronic Pain
Opioid tolerance & physical dependence DO NOT equal opioid addiction
Loss of Control Indices:
» Continued use despite adverse consequences
» Illicit or inappropriate drug seeking behavior
– In response to craving or drug hunger
– In the absence of pain or withdrawal
Pseudo Addiction- in chronic pain patient
Inadequate Treatment of Pain
“Apparent” Drug Seeking Behavior
» Effort to achieve adequate analgesia
» Early refill, doctor shopping, etc.
–Manipulation seen as “addictive behavior”
–May be seen as non-compliance
“Cured” by adequate treatment of pain
Opioid Agonist Treatment of Addiction - Payte - 1998
Chronic Pain Disorder
Opioid Tolerance Opioid Physical Dependence Absence of illicit or inappropriate drug
seeking behavior» No drug hunger in absence of pain» No loss of control
No “doctor shopping” Little tendency to escalate dose over time
Opioid Agonist Treatment of Addiction - Payte - 1998
PSYCHOSOCIAL TREATMENT ISSUES
PSYCHOSOCIAL TREATMENT ISSUES
Population Characteristics
Heterogeneity Readiness for recovery; motivation Psychiatric comorbidity Medical comorbidity
Program Characteristics
Program Characteristics
Medical component: assessment, dosing, client interactions
Individual counseling Group counseling Case management Staff training (ongoing)
What is Abstinence?
Medication is compatible with 12-step participation if appropriately prescribed by physician knowledgeable about addiction
Pt on methadone is abstinent if not using illicit drugs and using legal ones as prescribed
It’s just another medication. Meds are a tool, not a solution
Cognitive-Behavioral Therapy
Cognitive-Behavioral Therapy
Lends itself to controlled studies; strong support for its effectiveness
Especially useful to help establish abstinence, teach early recovery and relapse prevention skills
Emphasizes changing behavior and managing symptoms
Cognitive Behavioral Strategies (CBT)
Cognitive Behavioral Strategies (CBT)
MATRIX MODEL - Organizing Principles Create explicit structure and expectations Establish positive, collaborative relationship Teach information and CBT concepts Positively reinforce behavior change Provide corrective feedback when necessary Encourage self-help participation
CBT: MATRIX MODELCBT: MATRIX MODEL
Structure is essential: time scheduling, self-help meetings, exercise, work, treatment activities
Identify external and internal triggers and make a plan
Tools for managing cravings: thought stopping, visual imagery, change environment/behavior
TIP #33 has description, patient worksheets(Rawson 1999)
Clinical IssuesClinical Issues
Is Psychotherapy Useful?
Philadelphia group study, begun 1977 global psychiatric status ratings elements of drug counseling models of psychotherapy utilized benefits to low severity patients benefits to high severity patients
Dual Diagnosis Issues
depression trauma history; PTSD schizophrenia medication strategies
PTSD Influence in Early Tx
PTSD Influence in Early Tx
Aim: determine tx adherence relative to frequency of violence and PTSD in MMT pts, male & female
96 pts; over 2/3 exposed to one or more violent traumatic events
Trauma or PTSD did not predict dropout rates Those with current PTSD had significantly more
ongoing drug use at 3 months, especially cocaine
(Hein et al, 2000)
Continued heroin, alcohol, and other drug use
patient and provider expectations enhancing motivation cocaine use alcohol use medical comorbidity; AIDS, chronic pain controversies about discharge
Psychological Issues
AOD use in family of origin high frequency of childhood physical
and sexual abuse recognition and appropriate expression
of feelings issues of self-care, self-soothing
Women’s Issues
remove practical barriers: transportation, child care
intimate relationships as primary hazard sexual issues contraceptive practices
Family/Couples Work
engaging family, significant others education about addiction and MMT develop existing and new support
structures couples issues parenting classes
HIV/AIDSHIV/AIDS
impact on MMT staff; providing support regular assessment of staff attitudes and
knowledge integrating primary care promoting medication compliance impact of dementia on treatment
MMT and 12-Step Programs
benefits and hazards simulated meetings as a launching
strategy meetings in the community Vincent Dole and Bill W. other types of self-help advocacy groups
Making Residential Treatment Available to Methadone
Patients
Making Residential Treatment Available to Methadone
Patients
Some clients need higher level of care Issues for the methadone program Issues for the residential program Security issues Documentation issues Funding barriers